38 - sat am 2 - roy-chaudhry - bench to beside - future of ... · disclosures...
TRANSCRIPT

Disclosures
•Consultant/A dvisory Board:W L Gore,M edtronic,BardP eripheralVascular,CookM edical,A kebia,T VA
•FounderandChiefS cientificO fficer:Inovasc
•Grant/R esearchS upport:N IH,VA ,U niversity ofA rizona,N S F
•ClinicalT rialS upport:N IH,Bayer,A kebia,A bbvie,Baxter,VascularT herapies,P roteon,Corm edix
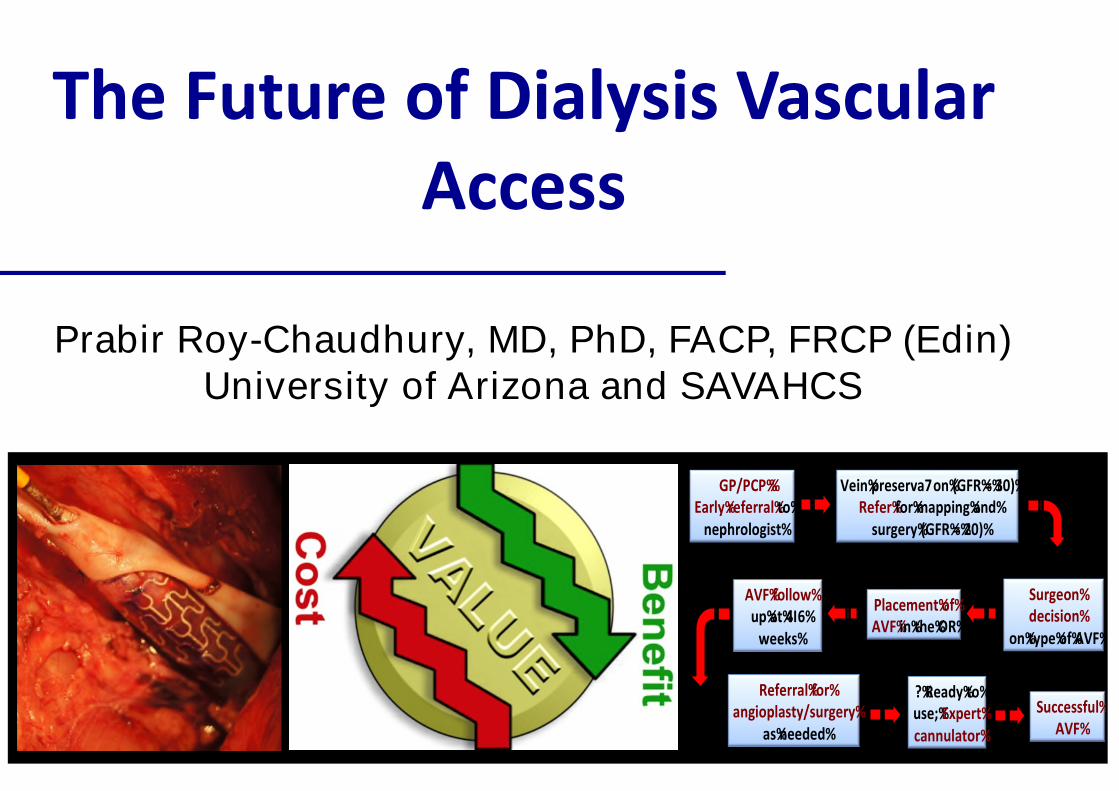
T heFutureofDialysisVascularA ccess
Prabir Roy-Chaudhury, MD, PhD, FACP, FRCP (Edin)University of Arizona and SAVAHCS
Artery
Vein
GP /P CP %%Early%referral%to%%
nephrologist%
Vein%preserva7on%(GFR %=%30)%R efer%for%m apping%and%
surgery%(GFR %=%20)%
S urgeon%decision%
on%type%of%A VF%
P lacem ent%of%A VF%in%the%O R %
A VF%follow %up%at%4I6%
w eeks%
R eferral%for%angioplasty/surgery%
as%needed%
?%R eady%to%use;%Expert%cannulator%
S uccessful%A VF%
+ +
+++
+ +
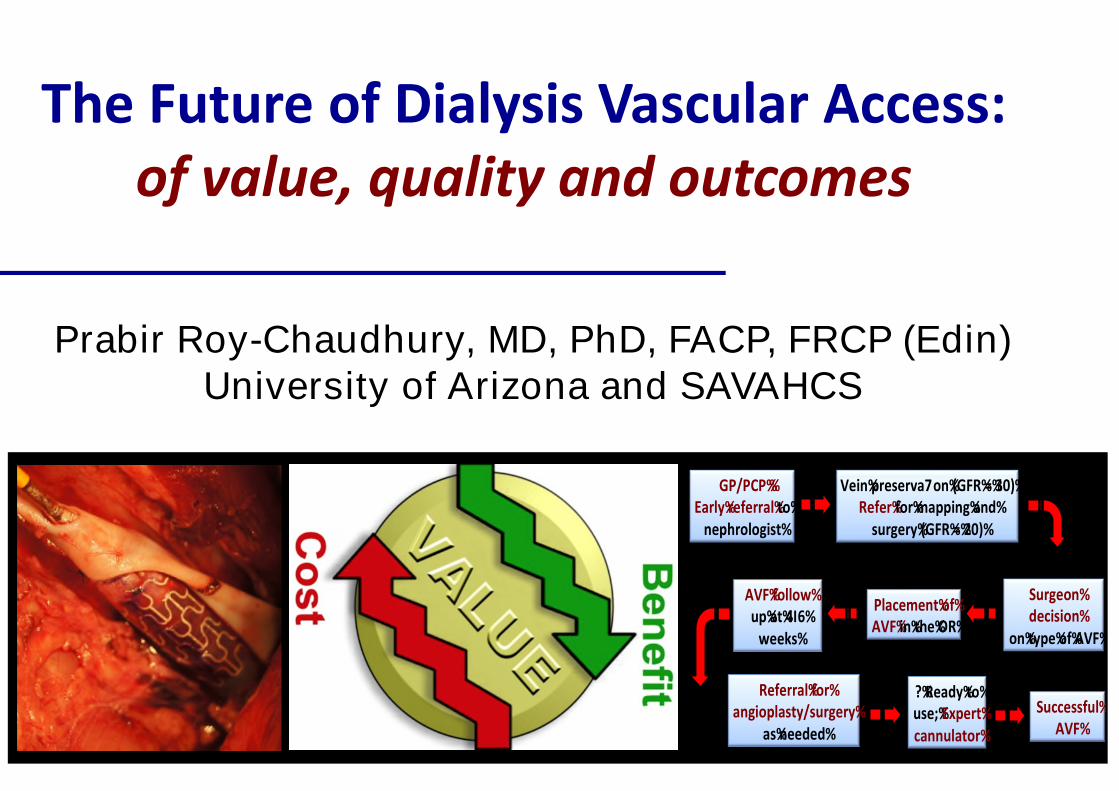
T heFutureofDialysisVascularA ccess:of value, quality and outcomes
Prabir Roy-Chaudhury, MD, PhD, FACP, FRCP (Edin)University of Arizona and SAVAHCS
Artery
Vein
GP /P CP %%Early%referral%to%%
nephrologist%
Vein%preserva7on%(GFR %=%30)%R efer%for%m apping%and%
surgery%(GFR %=%20)%
S urgeon%decision%
on%type%of%A VF%
P lacem ent%of%A VF%in%the%O R %
A VF%follow %up%at%4I6%
w eeks%
R eferral%for%angioplasty/surgery%
as%needed%
?%R eady%to%use;%Expert%cannulator%
S uccessful%A VF%
+ +
+++
+ +
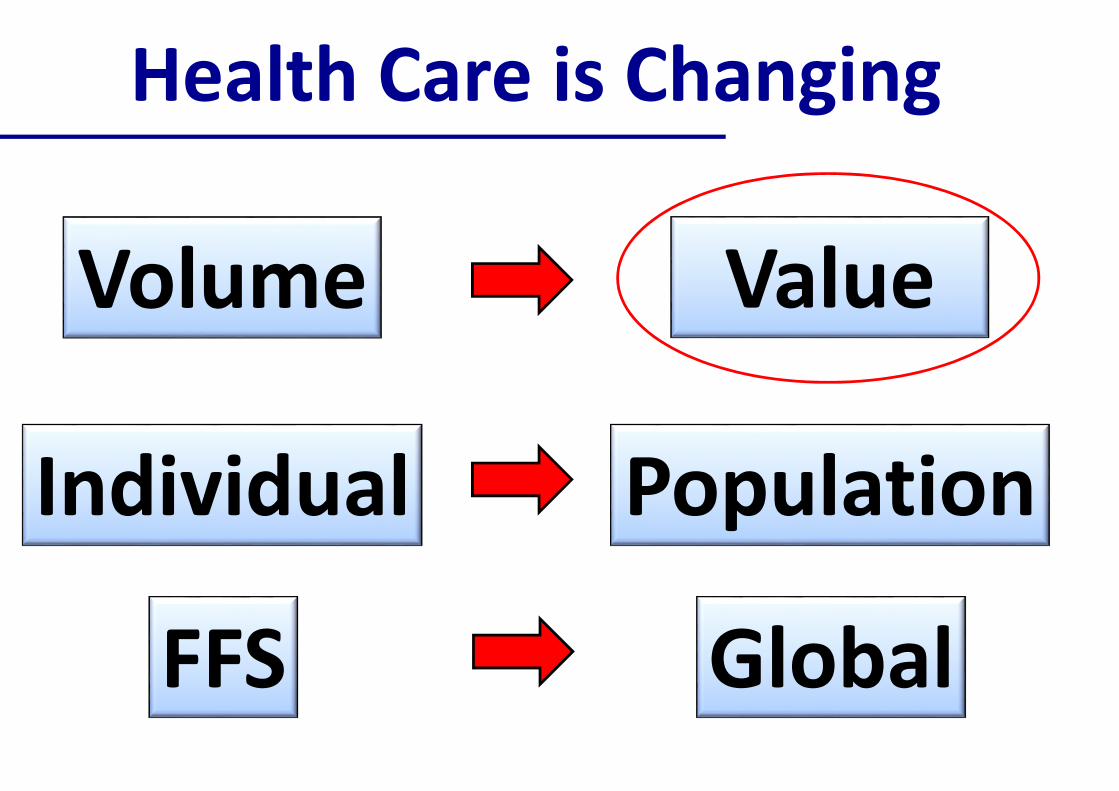
HealthCareisChanging
Volum e Value
Individual P opulation
FFS Global
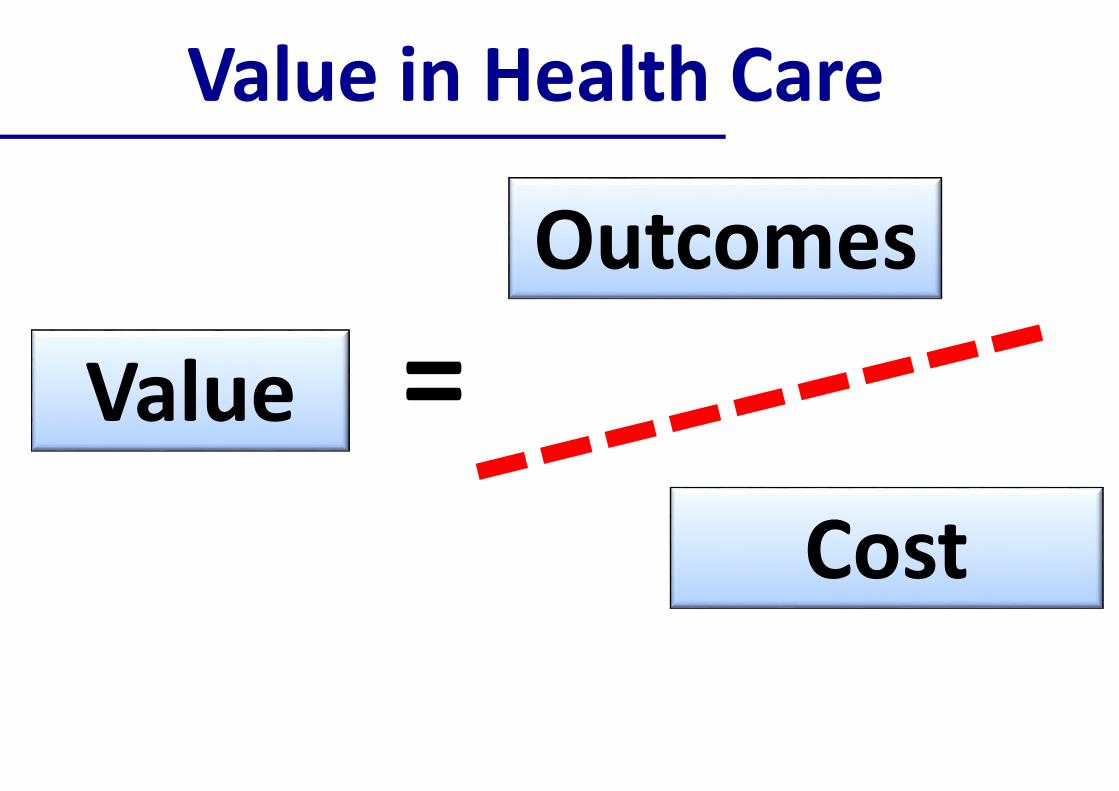
ValueinHealthCare
Value
O utcom es
Cost
P oorValueinvascularaccesscare
P oorValue
BadO utcom es
Cost
How do we improve VALUE invascular access care = INNOVATION
T echnology innovation
P rocessofcareinnovation
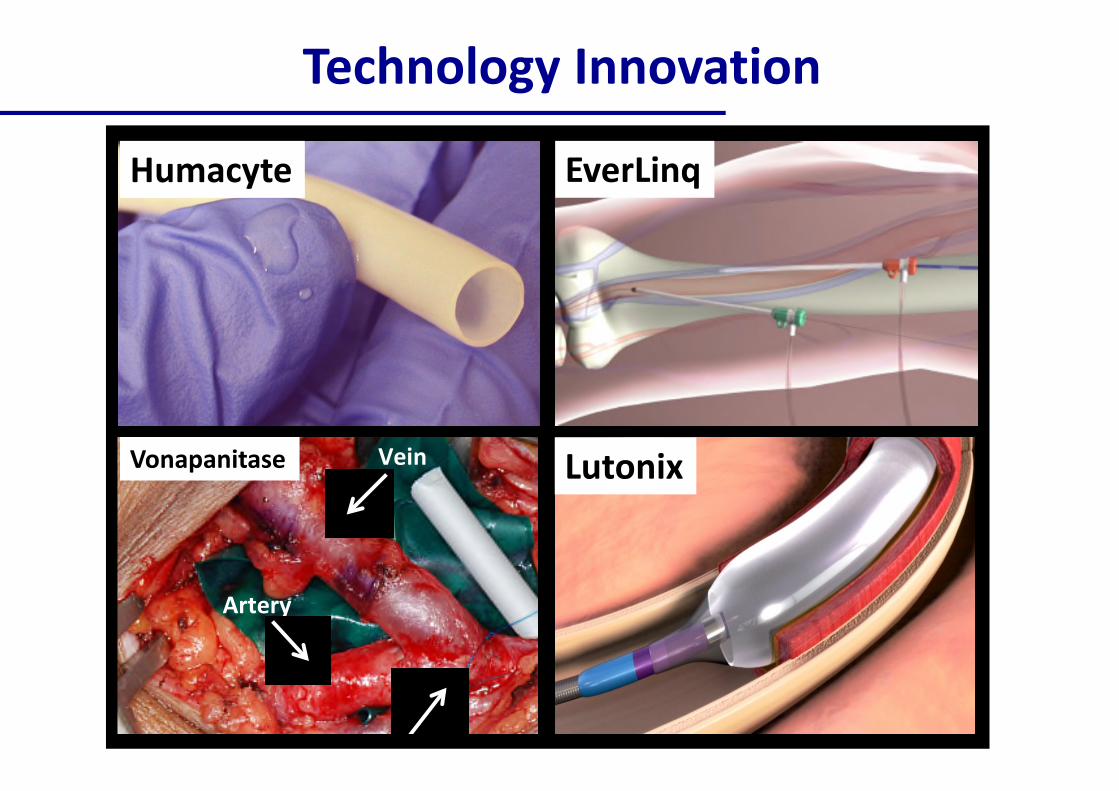
T echnology Innovation
EverL inqHum acyte
Vein
A rtery
Vonapanitase L utonix
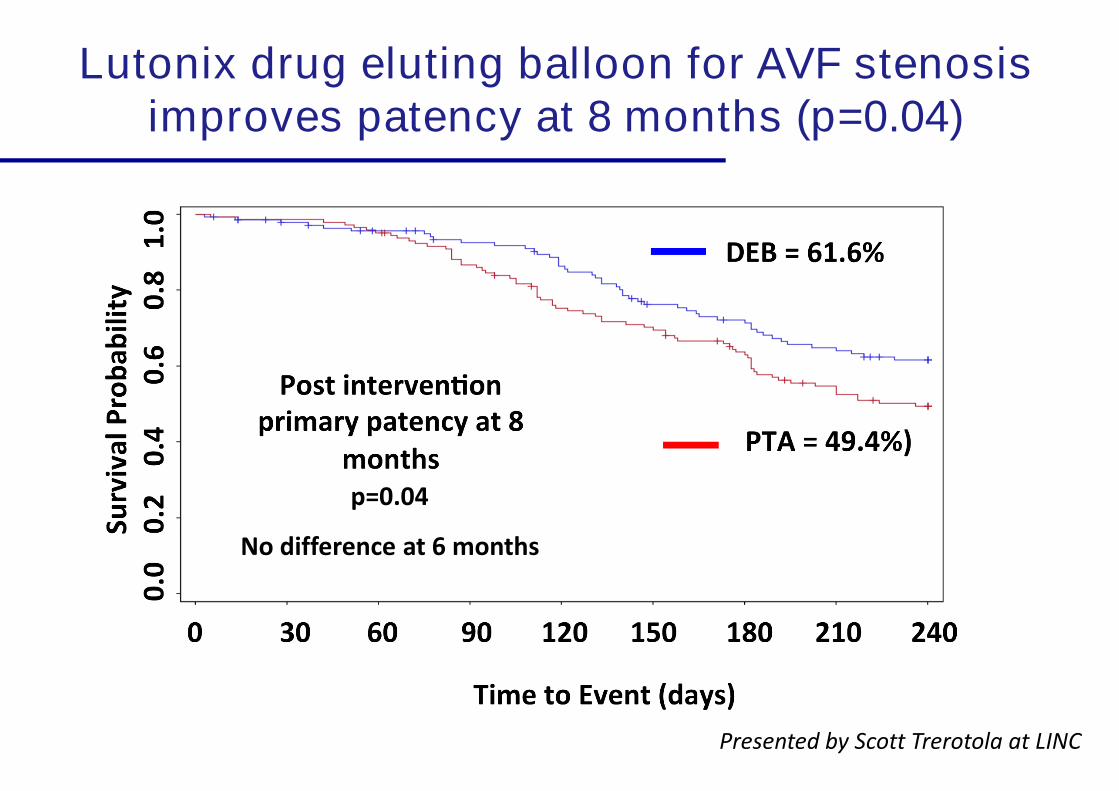
Lutonix drug eluting balloon for AVF stenosisimproves patency at 8 months (p=0.04)
P resentedby S cottT rerotolaatL IN C
N odifferenceat6m onths
p=0.04
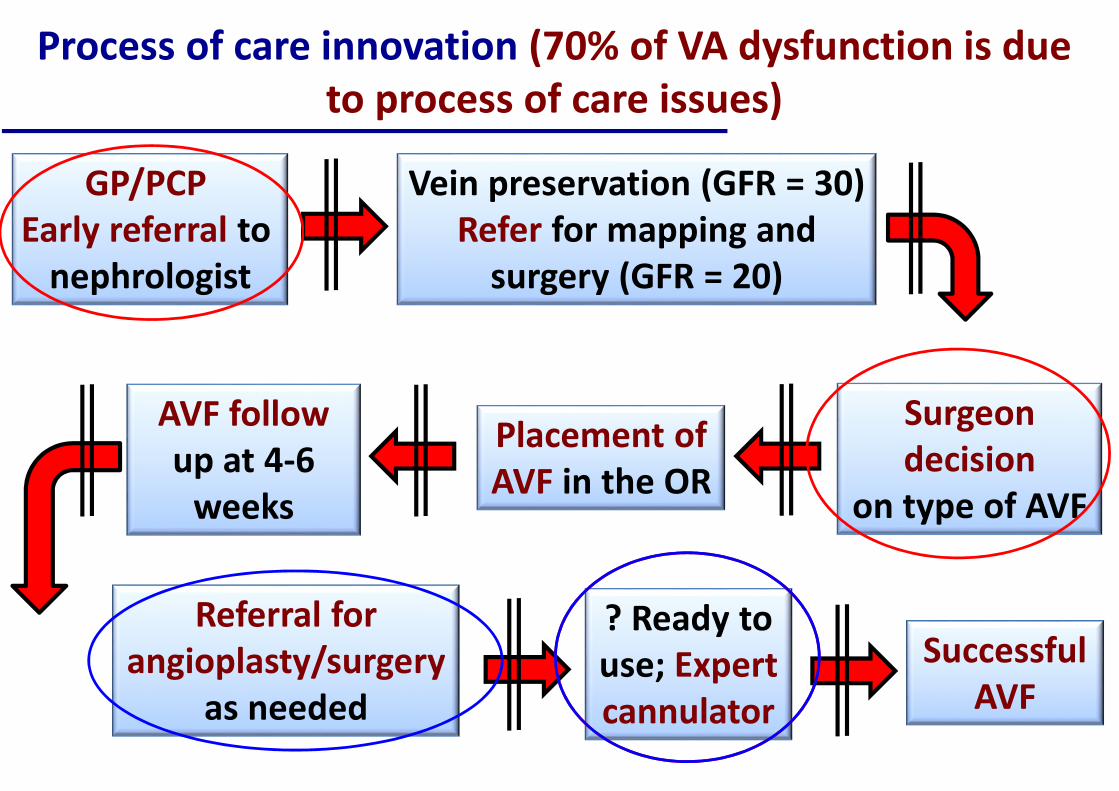
P rocessofcareinnovation(70% ofVA dysfunctionisduetoprocessofcareissues)
S urgeondecision
ontypeofAVF
P lacem entofAVFintheO R
AVFfollowupat4-6
w eeks
R eferralforangioplasty/surgery
asneeded
? R eady touse;Expertcannulator
S uccessfulAVF
Veinpreservation(GFR = 30)R eferform appingand
surgery (GFR = 20)
GP /P CPEarly referralto
nephrologist
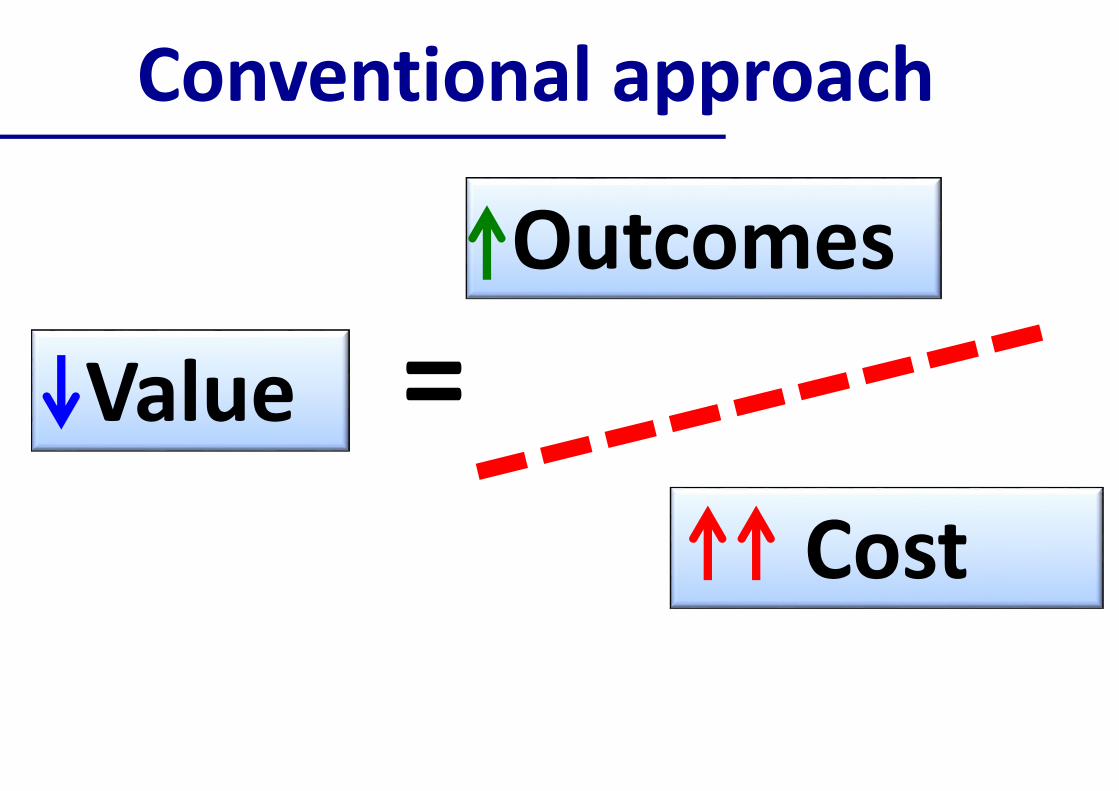
Conventionalapproach
Value
O utcom es
Cost
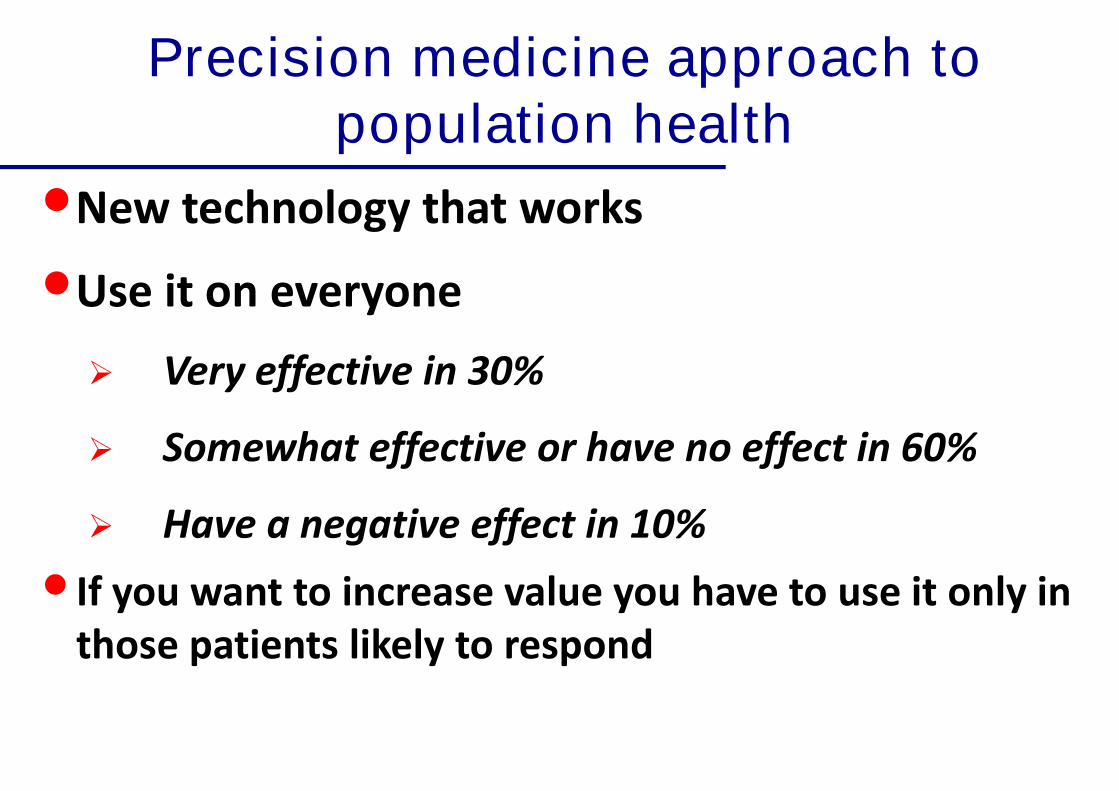
Precision medicine approach topopulation health
•N ew technology thatw orks
•U seitoneveryone
Very effective in 30%
Somewhat effective or have no effect in 60%
Have a negative effect in 10%
•Ifyou w anttoincreasevalueyou havetouseitonly inthosepatientslikely torespond
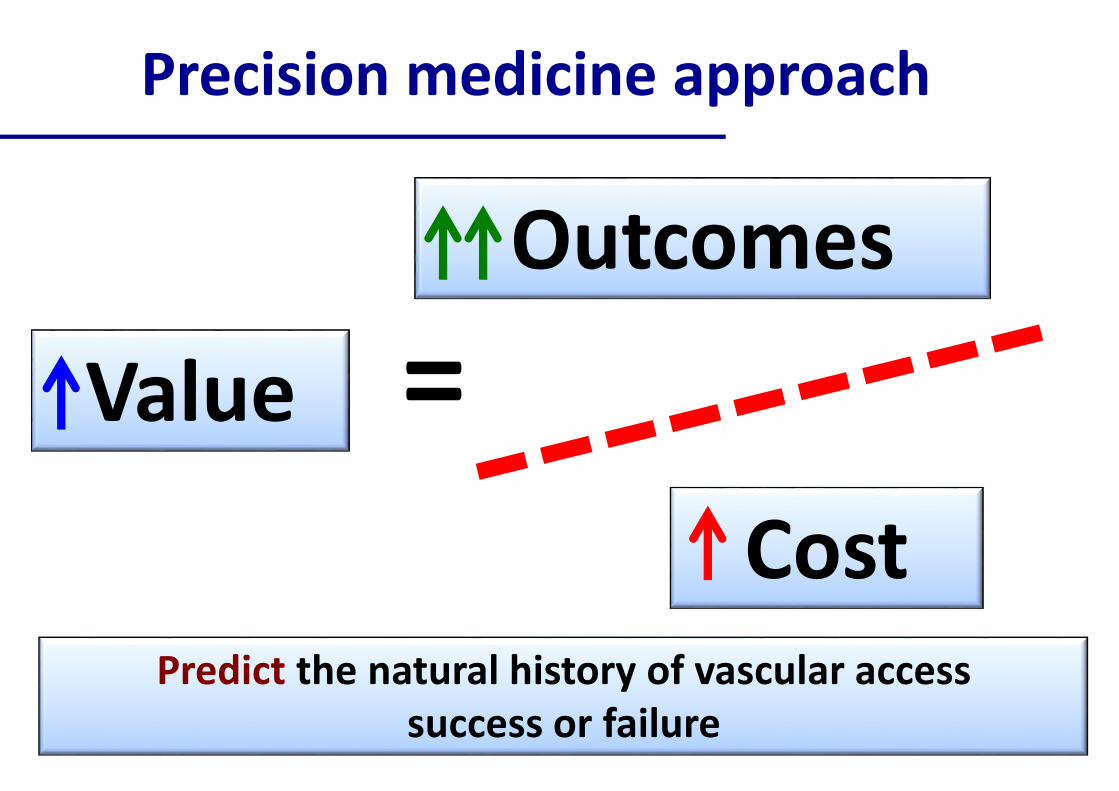
P recisionm edicineapproach
Value
O utcom es
CostP redictthenaturalhistory ofvascularaccess
successorfailure
Real world evidence generation forvascular access
•Com ingtogetheroftheclinicalcareandclinicalresearchenterprises
•S tandardofcareclinicaldatathatisgeneratedevery day isusedforclinicalresearchandprocessofcareim provem ent(learninghealthsystem )
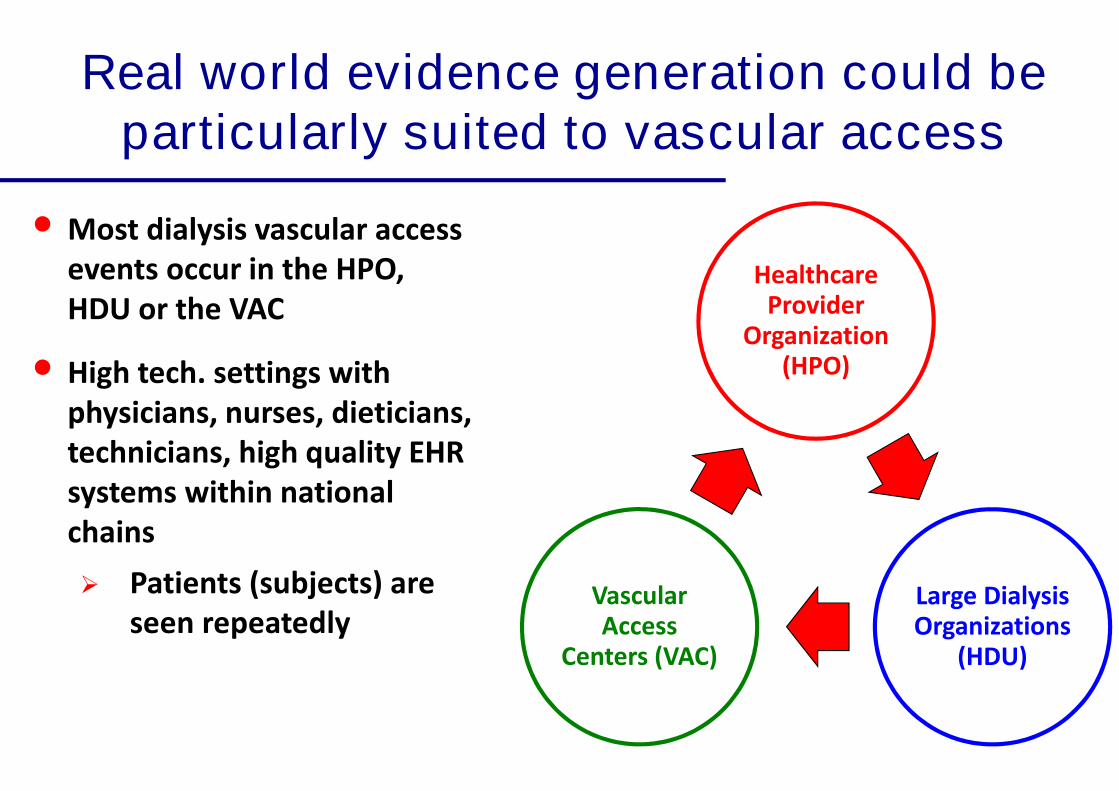
Real world evidence generation could beparticularly suited to vascular access
HealthcareP rovider
O rganization(HP O )
L argeDialysisO rganizations
(HDU )
VascularA ccess
Centers(VAC)
• M ostdialysisvascularaccesseventsoccurintheHP O ,HDU ortheVAC
• Hightech.settingsw ithphysicians,nurses,dieticians,technicians,highquality EHRsystem sw ithinnationalchains
P atients(subjects)areseenrepeatedly
O verallVisionandGoal
•Createatripartitepartnershipbetw eenHP O ’s,L DO ’sandVAC’s
• L everagetheirintrinsicEM R andsam plesizestrengthstocollectstandardizedvascularaccessdatafieldsacrosstheentirespectrum ofvascularaccesscare(creation/m aintenance/abandonm ent)
•Developuniform datastandardsonclinical,dem ographic,biologicalandprocessofcareparam eters
Benefitsofdevelopingsuchacom prehensiveR EA L T IM Edataset
• Identify clinicaland biologicalpredictorsofdialysisaccesssuccessandfailure(stratify patientsintohighandlow riskgroups)
• Incentivize processofcareinnovationinvascularaccess
• Facilitate pragm aticclinicaltrialsforvascularaccess(interventionw ithacoordinatorinoneunitbutnottheother:clusterrandom ization)
• R ealw orld realtim edatabasetocollectoutcom edataw ithm inim aladditionalcost
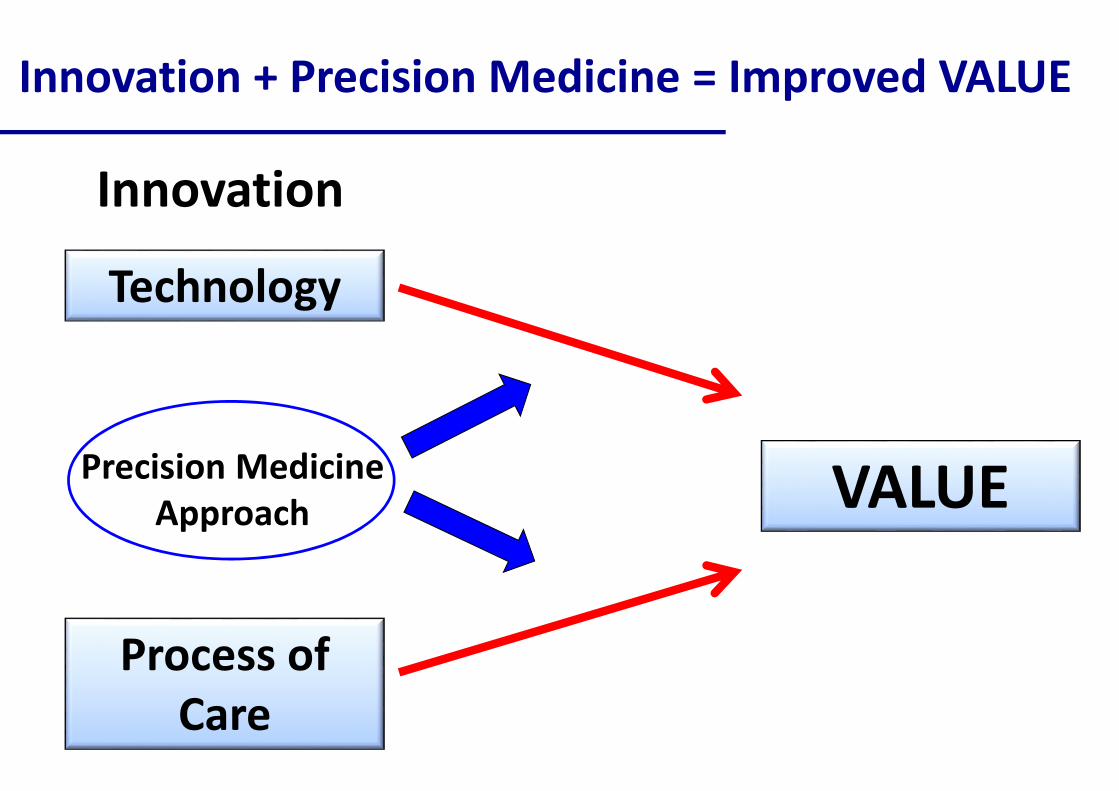
Innovation+ P recisionM edicine= Im provedVA L U E
T echnology
P rocessofCare
VA L U EP recisionM edicineA pproach
Innovation
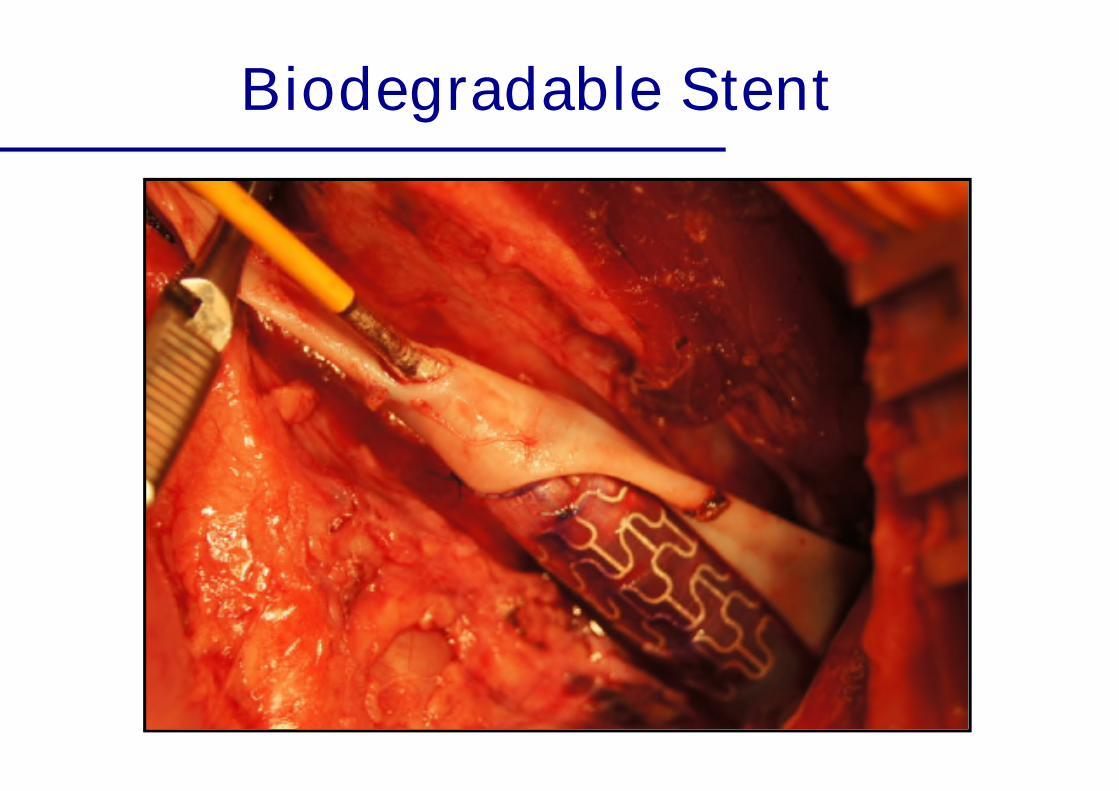
Biodegradable Stent
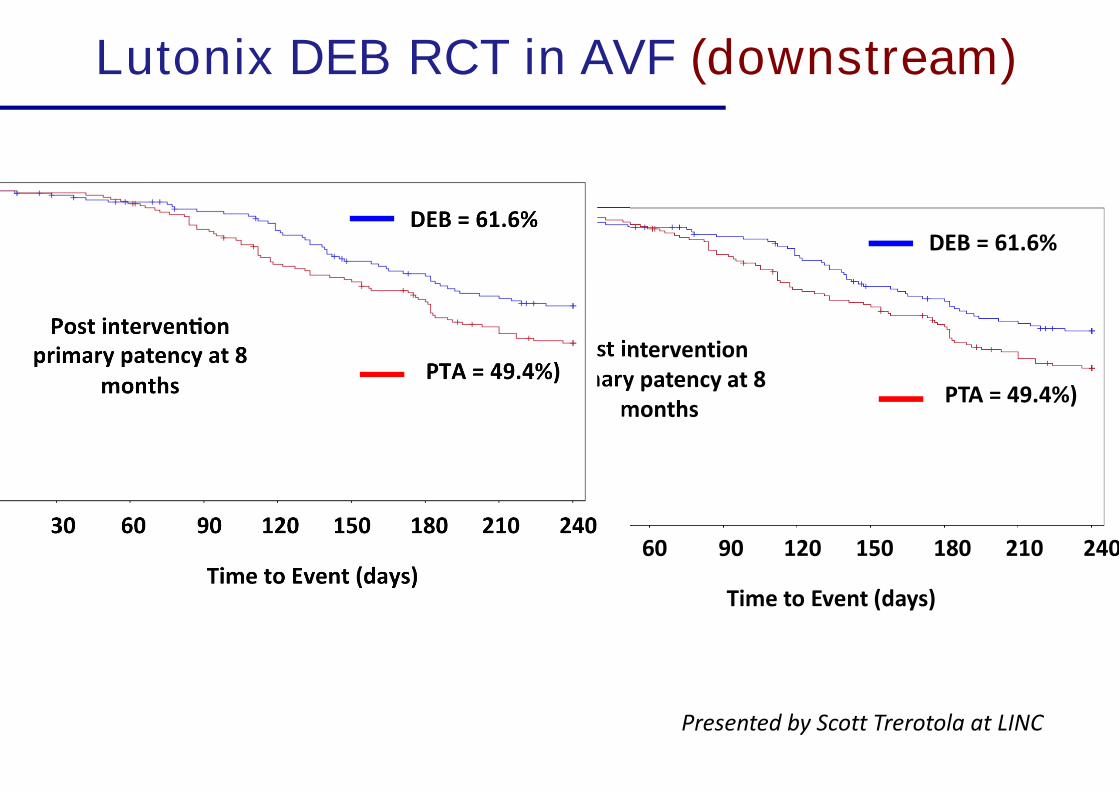
Lutonix DEB RCT in AVF (downstream)
0 30 60 90 120 150 180 210 240
0.0
0.2
0.4
0.6
0.8
1.0
Surv
ival
Pro
bab
ility
T im etoEvent(days)
P T A = 49.4% )
DEB = 61.6%
P ostinterventionprim ary patency at8
m onths
P resentedby S cottT rerotolaatL IN C