zimbabwe assistance program in malaria annual report
TRANSCRIPT
ZIMBABWE ASSISTANCE PROGRAM IN MALARIA
ANNUAL REPORT
REPORTING PERIOD: OCT 1, 2018 – SEPT 30, 2019
SUBMISSION DATE: OCTOBER 30, 2019

Recommended Citation: ZAPIM Year Four Annual Report, October 1, 2018–September 30, 2019. Rockville, MD, U.S., and Harare, Zimbabwe. Zimbabwe Assistance Program in Malaria, Abt Associates.
Contract and Task Order Number: AID-613-A-15-00010
Submitted to: United States Agency for International Development/President’s Malaria Initiative
Submitted on: October 30, 2019
Abt Associates Inc. 1 6130 Executive Boulevard 1
1 Rockville, Maryland 20852 1 T. 301.347.5000 1 F. 301.913.9061
1 www.abtassociates.com

i
Contents LIST OF FIGURES ............................................................................................................................................................iii
LIST OF TABLES .............................................................................................................................................................. iv
ABBREVIATIONS AND ACRONYMS ................................................................................................................................... v
1. Executive Summary ............................................................................................................................................1
2. Background .........................................................................................................................................................4
2.1 Project Design.................................................................................................................................... 4
2.2 Zimbabwe Operating Context ........................................................................................................ 4
3. Technical Strategy ..............................................................................................................................................7
3.1 Target Districts for Implementation ............................................................................................. 7
3.2 Capacity Building ............................................................................................................................... 9
3.3 Community-Based Approach .......................................................................................................... 9
3.4 Using Data for Decision Making .................................................................................................... 10
3.5 Coordination and Integration of Activities for Impact and Sustainability ............................. 10
3.6 ZAPIM Quality Improvement ....................................................................................................... 10
3.7 Innovative Use of Digital Technology .......................................................................................... 11
3.8 Sustainability .................................................................................................................................... 11
4. Technical Activities .......................................................................................................................................... 13
4.1 Clinical Case Management ............................................................................................................ 13
4.1.1 Malaria case management and MIP trainings ......................................................................................................... 13
4.1.2 Malaria clinical mentorship ........................................................................................................................................ 14
4.1.3 Malaria death audit meetings .................................................................................................................................... 22
4.2 Community Case Management .................................................................................................... 23
4.2.1 CCM & MIP trainings .................................................................................................................................................. 24
4.2.2 Post training follow up ............................................................................................................................................... 26
4.2.3 Supportive supervision ............................................................................................................................................... 26
4.2.4 VHW Review meetings .............................................................................................................................................. 28
4.2.5 Issues/areas for improvement of the CCM program ......................................................................................... 29
4.2.6 procurements for VHWs .......................................................................................................................................... 30
4.2.7 A success story related to CCM activities in Mbire.......................................................................................... 31
4.3 Long Lasting Insecticide Treated Nets ........................................................................................ 31
4.3.1 Mass Distribution ......................................................................................................................................................... 32
4.3.2 Continuous Distribution of LLINs .......................................................................................................................... 44
4.4 Social and Behavioral Change Communication ......................................................................... 47
SBCC Areas of Intervention ...................................................................................................................... 47
4.4.1 Branding of the NMCP ............................................................................................................................................... 48
4.4.2 Development, printing and dissemination of malaria SBCC materials and communication facilitation
tools 48
4.4.3 Development and broadcasting of multimedia malaria communications (radio and audio)..................... 49
4.4.4 ADVOCACY FOR ACTION ON MALARIA CONTROL AND ELIMINATION BY COMMUNITIES,
COMMUNITY LEADERS AND STAKEHOLDERS – WORLD MALARIA DAY ...................................................... 50
4.4.5 Evidence gathering for improved SBCC programming ...................................................................................... 50
4.4.6 Production and publishing of NMCP reports on various thematic areas ..................................................... 51
Commented [EM1]: Audrey, please update the headings and link to the ToC (same for tables and figures). Ensure all headings
and sub-headings are consistent. Please also check that it is single spacing throughout the doc and left-justified text unless it is a table
or graphic or something.

ii
4.4.7 Community Based SBCC ACTIVITIES ................................................................................................................... 51
PARTICIPATION OF HCCS IN OUTREACH EDUCATION SESSIONS WITH COMMUNITIES .......................................... 56
CHALLENGES .................................................................................................................................................... 62
4.5 Monitoring & Evaluation/Operations Research .......................................................................... 62
4.5.1 Assessment of Drivers of Continuing Malaria Transmission in Angwa Ward, Mbire District,
Mashonaland Central Province ................................................................................................................................................ 62
4.5.2 National Malaria SM&E Plan ...................................................................................................................................... 63
4.5.3 EPR Preparedness and Response Guidelines ........................................................................................................ 63
4.5.4 Malaria SM&E Training Manual ................................................................................................................................. 63
4.5.5 CDCS .............................................................................................................................................................................. 64
4.5.6 MIS Alternative ............................................................................................................................................................. 64
4.5.7 Document and Review Training Gaps by Thematic Area ................................................................................. 65
4.5.8 Net Durability Study at Month 36 ........................................................................................................................... 65
4.5.9 Provincial Malaria Review Meetings ........................................................................................................................ 65
4.5.10 DQAs ........................................................................................................................................................................ 65
4.5.11 Weekly VHW Mobile Reporting Pilot in Mbire District .............................................................................. 66
4.5.12 RDT Registers for VHWs .................................................................................................................................... 67
4.5.13 Orientation of ZAPIM Staff in Global Information System Mapping ......................................................... 67
4.6 Malaria Elimination Activities in Lupane District, Matabeleland North ................................. 67
4.6.1 Enhanced Surveillance Training ................................................................................................................................ 67
4.6.2 Strengthening Foci Response .................................................................................................................................... 68
4.6.3 EHT Entomology Training ......................................................................................................................................... 69
4.6.4 Training in GIS Mapping ............................................................................................................................................. 70
4.6.5 ZAPIM Micro Plan for Elimination .......................................................................................................................... 71
5. Gender and Child Safeguarding ..................................................................................................................... 72
6. Environmental Compliance ............................................................................................................................ 73
6.1 Medical Waste ................................................................................................................................. 73
6.2 Liquid and Solid LLIN Waste ........................................................................................................ 73
6.3 Management of Public Health Medicines and Commodities .................................................... 73
7. ADMINISTRATIVE ACTIVITIES ..................................................................................................................... 74
7.1 Staffing and Management .............................................................................................................. 74
Conferences, Retreats, Trainings and Meetings ............................................................................. 74
7.2 ................................................................................................................................................................... 74
7.2.1 Annual Malaria Conference ....................................................................................................................................... 74
7.2.2 VHW Logistics System Redesign workshop ......................................................................................................... 74
7.2.3 Provincial Health Team Meetings and Data Management Workshop ........................................................... 75
7.2.4 National Malaria Vector Control Planning and Review Meeting, IRS Level I and II Trainings and IVM
Strategic Plan Development Workshop ............................................................................................................................... 75
7.2.5 Environmental Compliance Training ....................................................................................................................... 75
7.2.6 Year 5 Work Plan Development Meetings ........................................................................................................... 75
7.2.7 ZAPIM/NMCP Meetings ............................................................................................................................................ 75
7.2.8 Fundamentals of SM&E and Evaluation Methods of Malaria Programs .......................................................... 75
8. Challenges, Lessons Learned and Recommendations ................................................................................. 77
Annex A: Short-Term Technical Assistance ........................................................................................................... 79
Annex B: PMP Indicator/Year 4 Milestone Matrix .............................................................................................. 81
Annex C: Year 4 Activities Affected By Anticipated Delayed Release of Year 5 Funding ............................... 95

iii
LIST OF FIGURES
FIGURE 1: MAP OF ZIMBABWE SHOWING ZAPIM-TARGETED DISTRICTS .................................... 9 Figure 2: Mentorship Activities carried out by Different Districts ........ Error! Bookmark not defined.
Figure 3: Improvement in overall *competency in OPD in May 2019 compared to May 2018 baseline .................................................................................................................................. 17
Figure 4: Comparison of performance across districts ................................................................ 18 Figure 5: Parameters with notable performance improvement .................................................... 19 Figure 6: MENTORSHIP REVIEW DISCUSSION GROUPS ...................................................... 20 Figure 7: Mentorship Review Group Feedback Session .............. Error! Bookmark not defined. Figure 8: CCM TRAININGS MEAN SCORES BY DISTRICT, FEBRUARY-APRIL 2019 .......... 25 Figure 9: VHWs giving feedback on RDT/Medicine register documentationError! Bookmark not
defined. Figure 10: Solar powered light sourced by a VHW using her own funds in Mash. Central,
Chawarura clinic ..................................................................................................................... 27 Figure 11: Beneficiaries of the My Net My Life mass campaign displaying their just received LLINs ....... 32
Figure 12: Participants demonstrating how to hang a rectangular LLIN ......................................... Figure 13: Transport used in transporting LLINs from HFs to Distribution points in Mazowe
District ...................................................................................... Error! Bookmark not defined. Figure 14: The Provincial Field Officer sharing a lighter moment with some LLINs beneficiaries and some
women on the right socializing after getting their LLINs.............................................................. 41
Figure 15: MASS DISTRIBUTION OF LLINS 2016 AND 2019 ................................................... 42 Figure 16: LLINs Distributed Through CD Channel by Quarter Year 1-Year 4 ................................... 45
Figure 17 : Delayed presentation of a boy with severe malaria .... Error! Bookmark not defined. Figure 18: Kamativi HCC Nutrition Garden ................................... Error! Bookmark not defined. Figure 19: Showcasing some HCC activities ................................ Error! Bookmark not defined. Figure 20: Chart being used by Hwata HCC to track malaria cases in their area by month, week
& by village. ............................................................................................................................ 58 Figure 21: Breeding sites at Katoba River in Binga ...................... Error! Bookmark not defined. Figure 22: Larviciding at Katoba River in Binga ............................ Error! Bookmark not defined. Figure 23: Zimbabwe Malaria Foci Investigation and Response Algorithm ................................ 69 Figure 24: Community participation in larviciding during entomology training in Lupane, April
2019. ........................................................................................ Error! Bookmark not defined.

iv
LIST OF TABLES
TABLE 1: ZAPIM YEAR 5 IMPLEMENTATION PROVINCES AND DISTRICTS ................................... 8
Table 2: CM and MiP Trainees by Profession in ZAPIM focused provinces (February-March 2019) ...................................................................................................................................... 14
Table 3: HEALTH WORKERS MENTORED UP TO DATE (MAY 2018 TO AUGUST 2019) ..... 14 Table 4: Data collected and response rates during mentorship assessment ..... Error! Bookmark
not defined. Table 5: Recommendations from the mentorship review meeting .............................................. 21 Table 6: Findings and Recommendations from Death Audit Meetings ....................................... 23 Table 7: DISTRIBUTION OF CCM TRAINEES BY DISTRICT (FEBRUARY- APRIL 2019) ...... 24 Table 8: VHWs followed up after training, by district, April-June 2019 ........................................ 26 Table 9: VHWs Reached During Supportive Supervision ............................................................ 27 Table 10: VHW attendance at VHW review meetings by District, September 2019 ................... 29 Table 11: ROLES AND RESPONSIBILITIES OF MASS DISTRIBUTION STAKEHOLDERS IN MASS
DISTRIBUTION ........................................................................ Error! Bookmark not defined. Table 12: WARDS AND HEALTH FACILITIES WHICH PARTICIPATED IN MASS DISTRIBUTION OF
LLINS (2019) ............................................................................................................................ 35 TABLE 13: HEALTH WORKERS TRAINED ON MASS DISTRIBUTION BY DISTRICT AND GENDER
................................................................................................................................................ 36 Table 14 VILLAGE HEALTH WORKERS TRAINED BY DISTRICT AND BY GENDER ...................... 37 TABLE 15: NUMBER OF COMMUNITY MEMBERS SENSITIZED BY GENDER 2019 ......................... 38 TABLE 16: LLINS REGISTRATION DATA BY DISTRICT APRIL-MAY 2019 ...................................... 39
Table 17: LLIN DISTRIBUTION BY DISTRICT (JUNE-JULY 2019) ........................................... 41 .TABLE 18: SUCCESSES, CHALLENGES AND SOLUTIONS ............................................................. 43 TABLE 19: RECOMMENDATIONS ON MASS DISTRIBUTION ........................................................ 43 Table 20: CD of LLINs Oct 2018-Sept 2019 by District and Channel ................................................. 44 Table 21: Distribution by District and by Quarter October 2018-September 2019 ............................. 45 Table 22: Health Workers Trained in CD August 2019 ..................................................................... 46 Table 23: VHWs trained by HF and by Gender August 2019 ............................................................. 46
Table 24: key malaria behaviors and barriers identified during Explore phase for Binga and Hwange Districts. .................................................................... Error! Bookmark not defined.
Table 25: Distribution of HCCs Trained by District ...................................................................... 55 Table 26: Key findings and recommendations from DQAs, May-June 2019 .............................. 66

v
ABBREVIATIONS AND ACRONYMS
ACT Artemisinin-based combination treatment
AMC Annual Malaria Conference
ANC Antenatal care
CD Continuous distribution
CHW Community Health Worker
CM Case Management
CCM Community case Management
DHE District Health Executive
DHIS2 District Health Information System, Version 2
DMO District Medical Officer
DNO District Nursing Office
EHO Environment Health Officer
EHT Environment Health Technician
EPI Expanded Program on Immunization
EPR Emergency preparedness and response
ESDM Environmental sound design and management
HCC Health Center Committee
IRS Indoor residual spraying
LLIN Long-lasting insecticidal net
LSTM Liverpool School of Tropical Medicine
M&E Monitoring and evaluation
MCHIP Maternal and Child Health Integrated Program
MIP Malaria in pregnancy
MIS Malaria Indicator Survey
MoHCC Ministry of Health and Child Care
MPR Malaria program review
MSP Malaria Strategic Plan
N/A Not applicable
NIHR National Institute of Health Research
NMCP National Malaria Control Program
PEDCO Provincial Epidemiological Disease Control Office
PMD Provincial Medical Director
PMI President’s Malaria Initiative
PSI Population Services International
RA Research assistant
RBM Roll Back Malaria
RDT Rapid diagnostic test or testing
RHC Rural health center
SADC Southern African Development Community

vi
SBCC Social and behavior change communication
SMS Short message service
STI Sexually transmitted infection
STTA Short-term technical assistance
TBD To be determined
TOT Training of trainer
TrainSMART Training System Monitoring and Reporting Tool
TWG Technical working group
UMP Uzumba Maramba Pfungwe (District)
USAID United States Agency for International Development
VHW Village Health Workers
WHT Ward Health Team
ZAPIM Zimbabwe Assistance Program in Malaria

1
1. EXECUTIVE SUMMARY
This report presents the activities implemented by the Zimbabwe Assistance Program in Malaria
(ZAPIM) in support of the National Malaria Control Program (NMCP) during the project’s fourth year.
It covers the period October 1, 2018 to September 30, 2019. ZAPIM carried out these activities in eight
districts in Mashonaland Central Province, five districts in Mashonaland East Province and two in
Matabeleland North Province. Below is a summary of these Year 4 accomplishments that cover the
project’s intervention areas – case management (CM), malaria in pregnancy (MIP), social behavior change
communication (SBCC), long lasting insecticidal nets (LLINs), and monitoring and evaluation (M&E),
operational research (OR) and malaria elimination activities in Lupane District Matabeleland North
Province.
As a result of a delay in funding for Year 4, ZAPIM was unable to implement activities in the first quarter
of the year. The operating environment in the country changed towards end of June 2019 following
introduction of a new statutory instrument (SI 142) banning the use of the United States dollars for local
payments. As a result of this change, ZAPIM could not implement field activities in the month of July
2019. Further, due to yet another anticipated delay in release of Year 5 funding, the project had to slow
down implementation of activities and could not implement any field activities in September 2019.
Case Management (CM)
In Year 4 the project supported the training of 183 health care workers (HCW) in CM and MIP. The
majority of trained facility-based health care workers were newly recruited nurses. The trainers entered
the details of the trained health care workers into the Training System Monitoring and Reporting Tool
(TrainSMART) database in real time. Use of the database allows users to monitor training gaps and
ensure there are no repeat trainings of those already trained. ZAPIM worked with 25 district mentors in
the five districts (Mbire, Murewa, Mutoko, Binga and Hwange) to conduct mentorship visits to 134
mentees. ZAPIM also hosted a mentorship review meeting for the districts and other stakeholders to
assess the performance of the mentorship and map a way forward for the program. In Year 4 ZAPIM
provided technical and financial support for one malaria death audit meeting in each of the three
project-supported provinces.
Community Case Management (CCM)
ZAPIM trained 317 Village Health Workers (VHWs) in CCM and MIPand conducted post-training follow
up visits with 203 VHWs out of 282 VHWs trained in Mashonaland East and Mashonaland Central.
ZAPIM conducted district supportive supervisions with 132 VHWs in Binga and Hwange Districts,
meeting the VHWs at their respective health facilities and visiting 18 of these at their homes. ZAPIM
further trained 38 VHW peer supervisors in Mutoko and carried out post training follow up with 11 of
them. In addition, ZAPIM supported three district VHW review meetings in Mbire, Mutoko and
Centenary Districts. ZAPIM provided 200 VHWS in Mbire with lockable medicine cabinets to store
medicines.
Long-Lasting Insecticidal Nets (LLINs)
The project supported the distribution of 624,458 LLINs through mass distribution in 144 wards in 10
districts and 101,111 LLINs through continuous distribution (CD) channels. ZAPIM provided another
160,000 LLINs for distribution in Chimanimani and Chipinge Districts in response to cyclone Idai

2
induced flooding and participated in training 62 Environment Health Technicians (EHTs) in the two
districts for the distribution of the nets. ZAPIM supported the training of data collectors, provided
oversight of the field data collection, analyzed data, and developed the report for month 36 Net
Durability Study (NDS). ZAPIM is currently responding to comments from PMI to finalize the report.
Community Action Cycle (CAC)
In Year 4 ZAPIM trained eight Ward Health Teams (WHTs) in Binga and eight Health Centre
Committees (HCCs) in Hwange on Explore Health Issues and Setting Priorities, Planning Together and
Act Together phases of the community action cycle (CAC). The project further trained 26 HCCs in
Mashonaland Central and 34 in Mashonaland East on Evaluate Together phase of the CAC. Meanwhile
the participation of the HCCs in CAC has begun to bear fruit with some HCCs having reached out to
18,239 community members through village meetings. HCCs have participated actively in supporting
VHWs in their work by accompanying them on home visits, conducting village inspections and creating
health and hygiene clubs. As a result of the training support from ZAPIM, some HCCs have become
active in community lobbying for early ANC booking and early seeking of care in suspected malaria,
community surveillance against LLIN abuse and Indoor Residual Spraying (IRS) refusal and community
disease surveillance. ZAPIM supported HCC trainings on CAC has enabled HCCs to mobilize resources
like transport, allowances, meals and refreshments to support staff during mass distribution of LLINs and
IRS.
Social Behavior Change Communication (SBCC)
ZAPIM hosted a stakeholder meeting to help NMCP develop their branding concept. ZAPIM identified
a branding consultant from Abt Associates Inc. to carry out the stakeholder survey and spear head the
rebranding process. The actual branding process was postponed to 2020 due to the funding issues that
ZAPIM experienced and due to the economic challenges described in detail under Section 2.2 in this
report. ZAPIM developed and printed a leaflet “my net, my life” to promote the mass distribution of
LLINs and developed radio spots to promote LLINs and IRS. The project also supported the 2019
World Malaria Day Commemorations by providing technical assistance to the NMCP to publish a
malaria advertisement in the local newspapers. The project also provided financial and logistical support
for World Malaria Day Commemorations held in the three provinces in Shamva, Binga and Hwedza
Districts.
Surveillance Monitoring and Evaluation (SM&E)
During the reporting period, ZAPIM printed 1,400 copies of the Revised Epidemic Preparedness and
Response (EPR) Guidelines and 500 copies of the SM&E plan. The documents were distributed to the
provinces at the Annual Malaria Conference held in Mutare in June 2019. ZAPIM is currently developing
the training manuals for EPR and SM&E.
ZAPIM supported one malaria review meeting in each of the three provinces. These meetings are
platforms to review the malaria situation in the provinces, identify problems, find solutions, and plan for
improvements in the delivery of services and reporting of malaria data. ZAPIM supported the three
provinces to conduct data quality assessments (DQAs) at 47 selected health facilities in Binga (7),
Hwange (2), Murehwa (12), Goromonzi (12), Mbire (7) and Guruve (7).
Operational Research
ZAPIM worked with PMI, NMCP, and VectorLink to write the Assessment Report on Drivers of
Continuing Malaria Transmission in Angwa Ward, Mbire District. The report is currently being finalized.
The project completed the Case Drug Consumption Study (CDCS) report and printed 50 copies of the
report. The study sought to determine the factors that contribute to the observed disparity between
recorded malaria cases and the consumption of first-line artemisinin-based combination therapy in the

3
country. ZAPIM completed report writing on the 36-month NDS and is currently responding to
comments from PMI in order to finalize the report. ZAPIM submitted one late breaker abstract for each
of the researches for the American Society of Tropical Medicine and Hygiene (ASTMH) conference.
The project developed and shared a concept note with PMI on six alternatives to conducting a periodic
malaria indicator survey (MIS). The six options are: MIS within the Demographic and Health Surveys;
MIS (stand-alone), continuous MIS, strengthening the District Health Information System (DHIS2), a
‘hybrid’ approach between the last two options and using antenatal clinic attendants as a surrogate for a
population survey. ZAPIM shared short descriptions on each option and the advantages,
disadvantages/limitations, and likely cost implications.
VHW Reporting
MoHCC with support from ZAPIM trained and provided smart phones to 186 VHWs and 13 nurses in
Mbire District to enable VHWs to commence weekly mobile reporting on malaria data. Cellphone-
based reporting is expected to improve the timeliness and completeness of data from VHWs.
Malaria Elimination
ZAPIM supported training of 45 HCWs on enhanced surveillance and strengthening foci response in
Lupane District. EHTs and nurses from facilities with active malaria transmission in their catchment
areas were trained. The training was aimed at ensuring that the health care workers treat, notify, classify
and investigate all malaria cases according to national guidelines. In addition, the participants were
trained on foci mapping, foci classification, and appropriate responses to malaria foci in elimination. All
the 45 EHTs, environmental health officers (EHOs), and field orderlies in Lupane also received training
in entomology over a three-day period. The training included identification of vector breeding sites,
collection and transportation of female anopheles mosquitoes and use of larvicides to manage breeding
sites. ZAPIM supported training of the 45 EHTs in Lupane on geographic information system (GIS)
mapping to enable them to produce geocode-based electronic maps for mapping of malaria cases, vector
breeding sites and transmission foci in their catchment areas. This training will enable the EHTs to
produce more accurate maps that will replace hand drawn, estimated maps.
4
2. BACKGROUND
2.1 Project Design
The President’s Malaria Initiative was created in 2005 to reduce malaria-related mortality by 50 percent
in 15 high-burden countries in sub-Saharan Africa. The PMI’s commitment to combating malaria was
bolstered with the 2008 passage of the Tom Lantos and Henry J. Hyde Global Leadership against
HIV/AIDS, Tuberculosis, and Malaria Act (www.pmi.gov/about). In fiscal year 2011, Zimbabwe was
chosen to be a PMI country. The United States Agency for International Development (USAID)
previously had provided some limited support for IRS and commodity procurement (Zimbabwe Malaria
Operational Plan 2016). The PMI supports an array of malaria prevention and treatment activities in
Zimbabwe, including: LLIN procurement and distribution; IRS in high-burden areas; rapid diagnostic tests
(RDT), ACT, and sulphadoxine-pyrimethamine procurement and distribution; and the training of health
care workers in the diagnosis and treatment of malaria.
On September 25, 2015, Abt Associates and its partners Save the Children, Jhpiego, and the Liverpool
School of Tropical Medicine (LSTM) were awarded the ZAPIM project. This five-year project’s purpose
is to support the NMCP in providing comprehensive malaria prevention and treatment services to
Zimbabweans with the goal of reducing malaria morbidity and mortality. The project has five main
intervention areas: 1) CM/MIP, 2) LLINs), 3) SBCC, 4) OR, and 5) SM&E.
The project operated in 15 districts for the first three years in three provinces: Mashonaland Central
(Bindura, Centenary/Muzarabani, Guruve, Mazowe, Mbire, Mt Darwin, Rushinga and Shamva);
Mashonaland East (Goromonzi, Mutoko, Mudzi, Murehwa, and UMP); and Matabeleland North (Binga
and Hwange). In Year 4, the project scaled up to support pre-elimination work in Lupane District of
Matabeleland North.
This annual report provides a synopsis of the activities implemented in ZAPIM’s fourth year, covering
the period of October 1, 2018 through September 30, 2019. During the reporting period, As a result of
a delay in funding for Year 4, ZAPIM was unable to implement activities in the first quarter of the year.
Once the funding was obligated, the project was able to catch up and implement most of the approved
work-plan activities. However the changes in the regulatory framework in June 2019 detailed below led
to challenges that affected project implementation. Furthermore as the year progressed and there was
anticipated delay in the release of Year 5 funding, the project had to slow down implementation and
could not implement field activities in September 2019. Some Year 4 planned activities were thus
deferred to Year 5. The activities are detailed in Annex C.
2.2 Zimbabwe Operating Context As in previous years, Zimbabwe’s complex operating context was characterized by volatility, uncertainty
and ambiguity. Economic challenges continued to escalate and worsen throughout the year. Although
new monetary and fiscal policy statements were introduced, the economic situation did not improve,
instead they negatively impacted program implementation both at the project and staffing level. Inflation
was on the rise while the currency was depreciating fast and scarce thereby fueling the existence of a
parallel exchange rate market. Prices of goods and services in local currency increased drastically in line
with the U.S. dollar (USD) parallel market exchange rate. The project managed to mitigate against the
price increases by continuing to use the U.S dollar as the functional currency.

5
Below is a summary of the policy/regulation changes and how they impacted the program:
Policy/Regulation Impact on the project
Operationalization of the February 2018 ring-
fencing policy on Nostro foreign currency
accounts (FCAs) which seeks to separate
foreign currency accounts into two
categories, namely Nostro FCAs and Real
Time Gross Settlement (RTGS) FCAs by
October 15, 2018.
This resulted in delayed implementation of activities as the
project waited for the bank to put systems in place and provide
clear guidance on the how the project would be affected.
The Intermediated Money Transfer Tax was
reviewed upwards from 5 cents per
transaction to 2 cents per dollar transacted in
local currency effective October 1, 2018.
There was no direct impact on project implementation since the
tax is levied on local transactions. Even though the project
continued to use the US$ as the operational currency, the
increased tax resulted in a price hikes for goods and services.
New tax regulation on Paye As You Earn
(PAYE) for employees paid in foreign
currency was introduced by the Zimbabwe
Revenue Authority (ZIMRA.) The new
method involved converting the staff’s USD
salary to local currency at the prevailing
interbank rate in order to determine the
taxable bracket to apply. The interbank
exchange rate changes every day and month
thereby continuously eroding the net salary
of the employee.
Although there was no direct impact on project, staff net
incomes were severely eroded by between 11-15% and this
resulted in low staff morale. The project complied to the new
regulation but attempted to mitigate the situation by:
1. Reviewing staff benefits: increasing the daily meals
allowances and introducing a transportation allowance.
2. Reviewing staff salaries in line with the revised FSN
scale of June 4, 2019.
By the end of year, however, U.S$ denominated tax tables had
been re-introduced although staff salary net incomes could not
be re-instated to original levels.
Statutory Instrument (SI), 142 of 2019, was
introduced on June 24, 2019. The new
instrument banished the use of multi
currencies (including the USD) and
introduced a local currency. The local
currency is denoted in RTGS$ and bond
notes and is deemed as the sole legal tender
in Zimbabwe
The abrupt re-introduction of the local currency affected banks,
vendors and MoHCC partner allowances because adequate
change over time was not provided. The SI142 was silent on
treatment of funding from NGOs, Embassies and International
Organizations. The project could not implement activities or pay
MoHCC officials allowances for about a month in July 2019
while awaiting further guidance and while systems were being
put in place. The project subsequently continued to use the U.S$
as the operational currency since a waiver from SI142 was
granted for NGOs, Embassies and International Organizations.
Key activities planned for July 2019 that were affected by the policy changes, in particular, SI142 that had
to be deferred are as follows:
Affected Activity Planned Dates Actual Implementation Dates
Mentorship visit for Binga District 1-5 July 2019 5-9 August, 2019
Support supervision for Binga and Hwange
Districts
15 to 19 July Cancelled. Could not be done in Year
4
Post training follow up UMP VHWs
Post training follow up Mutoko peer supervisors
07-13 July 2019
21-26 July 2019
4-0 August, 2019
LLINs post distribution cluster review and
planning meetings
Training of VHWs on CD of LLINs
Data verification of Mass Distribution data
15-19 July
22-26 July
July-August, 2019
Cancelled. Was not done in Year 4.
August 2019 but coverage was low.
Only 100 were trained out of target of
1,000.
Cancelled. Was not done in Year 4.

6
CAC Evaluate Together Trainings:
Mbire District
Mt Darwin District
Shamva District
Activities to Document CAC in Mash East
1-6 July, 2019
8-13 July, 2019
5-20 July, 2019
For Mbire done 5-10 August. Cancelled
for Mt Darwin and Shamva and did not
happen in Year 4.
Was moved to August but the scope
was limited compare to original plan
CAC support supervision for Binga District 8-12 July, 2019 4-10 August
Supportive supervision for Lupane District 22-26 July, 2019 Cancelled. Could not be done in Year
4 as funding situation could not allow
for implementation in September 2019.
Provincial death audit and malaria review
meeting in Mash East
16-17 July, 2019 31 July-1 August
All the policy/regulation changes coupled with dealing with basics of fuel and power supply made
program implementation difficult and called for constant re-planning and re-strategizing. The country
started experiencing electricity load shedding which resulted in the project operating without power
supply and resorting to generator back up for extended hours on many occasions since June. This has
resulted in increased costs for fuel procurement, generator installation and maintenance. The power
outages also resulted in loss of internet connectivity which hampered communication for the project.
The project had to resort to using mobile phones which are more costly.

7
3. Technical Strategy
In Year 4, ZAPIM’s technical strategy was shaped by lessons learned over the past three years and the
project focused on consolidating already existing activities and building capacity for the MoHCC to
implement the activities in an efficient and sustainable manner. Firstly, ZAPIM continued implementing
CD of LLINs in addition to mass distribution. Further, ZAPIM continued to assist NMCP to address
challenging areas jointly identified by the NMCP and ZAPIM in the past years, namely SBCC
operationalization at the community level, improving commodity supplies and SS of VHWs, and
facilitating the use of death audit findings to improve the quality of malaria care. ZAPIM increased
integration and better coordination of activities within the project team and also with other partners
working in the same districts. For example, the project coordinated closely with Isdell Flowers and Wild
for Life on CCM in Binga and Hwange and with VectorLink in Mutoko and Mudzi. ZAPIM incorporated
capacity building activities for the NMCP at all levels of the health system to enhance programmatic
leadership and sustainability, including fostering a culture of continuous quality improvement by using
data for rapid decision making and action.
3.1 Target Districts for Implementation
In Year 4, ZAPIM continued to implement malaria control and prevention activities, focusing on the
same thematic areas of CM/MIP, LLIN, SBCC, and SM&E in the same 15 target districts in the three
focus provinces: Mashonaland East, Mashonaland Central, and two malaria control districts in
Matabeleland North (Table 1). In addition, ZAPIM started supporting malaria elimination work in Lupane
District in Matabeleland North Province. The level of implementation of activities across the thematic
arears varied according to the burden of malaria and existing gaps. Details of the activities implemented
are found under the various sections.

8
Table 1: ZAPIM Year 5 Implementation Provinces and Districts
Province Districts
Mashonaland Central 1. Mbire
2. Guruve
3. Centenary/ Muzarabani
4. Shamva
5. Rushinga
6. Bindura
7. Mt. Darwin
8. Mazowe
Mashonaland East 1. Goromonzi
2. Mutoko
3. Uzumba-Maramba-Pfungwe (UMP)
4. Murewa
5. Mudzi
6. Hwedza (LLIN activities only)
Matabeleland North 1. Hwange
2. Binga
3. Lupane (malaria elimination activities only)
Figure 1 shows the three provinces that ZAPIM targets, of which two, Mashonaland Central and
Mashonaland East, are high-malaria burdened.

9
Figure 1: Map of Zimbabwe Showing ZAPIM-Targeted Districts
3.2 Capacity Building
Central to ZAPIM across all thematic areas and activities is building capacity within the NMCP at all
levels (national, health facility and community) to implement sustainable, high-quality, evidence-based
programing in accordance with national and international standards for the control, prevention,
treatment, and reporting of malaria. Over the years, ZAPIM has built capacity through training of staff,
review and updating of technical guidelines and standard operating procedures (SOP), and development
of relevant job aids, supportive supervision (SS), and on-the-job training and mentoring. In Year 4,
ZAPIM continued support for these activities to build capacity within NMCP structures, and also
ZAPIM-supported communities, for effective activity implementation.
3.3 Community-Based Approach
The MoHCC emphasizes primary health care and a community-based approach to the delivery of health
services. In line with this approach, ZAPIM’s activities in Year 4 continued to build capacity at the
community and health facility levels. Since Year 2, ZAPIM has conducted community-based activities,
which involved training VHWs on CCM and LLIN distribution, as well as training health facility
personnel to conduct SS of VHWs and training VHWs to perform their own peer-to-peer supervision.
ZAPIM continued these community-focused efforts in Year 4, with emphasis on supervision and
mentorship geared towards strengthening CM of malaria and improving accountability of malaria
commodities supplied to VHWs. This community-based approach in Year 4 sought to strengthen

10
preventive efforts, especially by increasing uptake of LLINs during the mass distribution through
community sensitization and health education. Lastly, ZAPIM supported community empowerment
through the CAC approach through HCCs, and other community leaders, to encourage their active
participation in malaria prevention and treatment seeking.
3.4 Using Data for Decision Making
All ZAPIM-supported activities promote evidence-based decision making through international, national,
and local data sources—including ZAPIM research, assessments, and best practices from the past years.
In Year 4 ZAPIM used locally generated data, such as the MIS 2016, the Net Usage Assessment, Case
Drug Consumption Study (CDCS), Assessment of Drivers of Continued Malaria Transmission in Angwa
Ward, and the Net Durability Study, to inform programming, deployment of interventions including
LLINs, and training requirements. ZAPIM assisted the provinces and districts to use and analyze DHIS2
data for decision making, more particularly to identify, investigate, and respond to outbreaks. ZAPIM
used data obtained from various activities (including malaria review meetings, death audit meetings, SS
visits, and data quality assessments (DQAs) to inform training needs and plan interventions. To assess
the extent to which the trainings increased participants’ knowledge of CM/MIP, ZAPIM administered a
test before and after trainings. ZAPIM used data from the project’s Training System Monitoring and
Reporting Tool (TrainSMART) and the provinces to document CM/MIP trainings and to identify training
gaps.
3.5 Coordination and Integration of Activities for Impact and
Sustainability
ZAPIM offers a comprehensive package of support to the NMCP across key thematic areas that are
necessary for achieving the national strategic goals outlined in the NMSP. In Year 4, ZAPIM activities
were well coordinated across thematic areas to ensure the integration of activities for improved
efficiency and impact. Activities were layered and sequenced systematically in the supported districts to
complement each other and to share implementation costs. For example, malaria review meetings were
held back-to-back with the malaria death audits.
In addition to internal coordination and integration of activities, ZAPIM collaborated closely with other
implementing partners working in the same districts to ensure coordination and uniform standards for
activity implementation. For example, in Matabeleland North, ZAPIM coordinated CCM activities with
Isdell Flowers and Wild for Life, who are implementing similar activities in Hwange and Binga Districts.
In Mashonaland East, ZAPIM coordinated SBCC activities with the VectorLink project to support the
IRS program. ZAPIM also collaborated with CHAI in Lupane District.
3.6 ZAPIM Quality Improvement
In line with the PMI Malaria Operational Plan 2016, where it was identified as a key area, ZAPIM
incorporated quality assurance and improvement interventions into implementation of activities across all
technical areas—CM/MIP, LLINs, SBCC, and SM&E. It is important to emphasize that these interventions
are not entirely new as they were developed in collaboration with the NMCP to build on existing SS and
quality improvement processes at the provincial and district levels. The mentorship pilot program for
facility-based health care workers that started in Year 3 continued in Year 4. The mentorship review
meeting held in the last quarter of Year 4 will guide any improvements needed for the program going
forward. ZAPIM continues support for peer-to-peer mentoring for VHWs. Peer-to-peer mentoring is
particularly important as the project seeks to ensure sustainability of activities. ZAPIM used data quality
assessments, SS visits, and malaria review meetings to inform areas requiring improvements.

11
3.7 Innovative Use of Digital Technology
ZAPIM team also set up an electronic inventory for LLINs during the mass distribution. ZAPIM
continued the use of Short Message Services (SMS) reminders to facility-based health care workers post
CM trainings. ZAPIM supported training of EHTs on the DHIS2 Tracker and geographic information
system (GIS) in case investigations, notifications, and foci mapping in Lupane District. ZAPIM piloted
weekly mobile reporting by VHWs in Mbire in Year 4. In Year 5, ZAPIM will document the experiences
and lessons learned from the pilot, troubleshoot, and make any necessary adjustments to improve the
efficiency, timeliness, reliability, and completeness of the mobile reporting. ZAPIM will also make use of
the generated data for decision making to improve CCM programming in Mbire District.
3.8 Sustainability
In Year 4, ZAPIM continued to build capacity within the NMCP in a manner that ensures sustained
improvements to their activities in the fight against malaria. All ZAPIM activities were implemented
through the existing NMCP structures and the capacity of the structures were strengthened to enhance
independent future execution of the activities without partner support. In Year 4 ZAPIM targeted all
activities to address critical gaps and enhance long term sustainability within the NMCP structure down
to the community level.

13
4. TECHNICAL ACTIVITIES
4.1 Clinical Case Management In Year 4, ZAPIM supported MoHCC to conduct the following case management and MIP activities:
Trained a total of 183 health workers from Mashonaland East, Mashonaland Central and
Matabeleland North in CM and MIP
25 mentors reached a total of 134 mentees from 25 health facilities from Mbire, Murewa,
Mutoko, Hwange and Binga Districts
Support one malaria death audit meeting in each of the three ZAPIM supported provinces.
4.1.1 MALARIA CASE MANAGEMENT AND MIP TRAININGS In Year 4, ZAPIM continued to provide technical support for the training of health workers in malaria
case management and malaria in pregnancy. These trainings were timed to coincide with the malaria
season and targeted recently recruited nurses. The main objectives of the training were to help
participants understand the basic malaria situation in their areas of practice; acquaint them with the
treatment guidelines for malaria management as revised in 2014; and enable them to appropriately
diagnose and treat malaria patients including prevention and treatment of malaria in pregnancy.
Furthermore, ZAPIM used this platform to disseminate August 2018 policy changes in treatment of
severe malaria in all trimesters using intravenous artesunate and treatment of children weighing less than
five kilograms using ACTs. ZAPIM printed and distributed an addendum to participants for further
dissemination at their respective health facilities.
Out of a targeted 185 health workers, ZAPIM supported training of 183 (98.8%) including newly
recruited providers from the three provinces: Matabeleland North (33), Mashonaland Central (71), and
Mashonaland East (79) by 15 provincial trainers who also entered all the CM and MIP trainings into the
TrainSMART database. To assess whether these trainings resulted in improvement in knowledge
amongst participants, trainers administered a multiple choice malaria knowledge assessment
questionnaire before and after the training. Assessment results indicate general increase in knowledge
evidenced by median score increase from 65% to 72% in Matabeleland North, 65% to 78% in
Mashonaland Central, and 65% to 74.5% in Mashonaland East. Participants who performed poorly will
need ongoing support during supportive supervision and mentorship. Armed with skills gained from the
training, health workers are expected to have improved capacity to intervene appropriately when faced
with malaria cases hence contribute to reduction in malaria related morbidity and mortality. Table 2
below shows disaggregation of participants by type of cadre.

14
Table 2: CM and MIP Trainees by Profession in ZAPIM focused provinces (February-March 2019)
Cadre Male Female Total
Medical doctors 4 2 6
Registered general nurses 35 84 119
Primary care nurses 10 31 41
Nurse aides 0 1 1
Environmental Health Officer (EHO)/ EHTs 2 4 6
Pharmacy technicians 0 2 2
Lab scientists/technicians 2 2 4
Field orderlies* 0 1 1
Dispensary assistants 2 0 2
Data clerks 0 1 1
Total 55 128 183
*Field orderly: this is a cadre who reports to the EHT. They are involved in supervision of spray operators, larval source
management, water and sanitation, VHW support, and follow up of communicable disease cases including malaria and
tuberculosis
4.1.2 MALARIA CLINICAL MENTORSHIP
To support health care workers to implement their knowledge and skills obtained through CM and MIP
trainings and equip health care workers to provide the highest standard of malaria care, in May 2018,
ZAPIM commenced the malaria clinical mentorship pilot in Mbire, Murewa, Mutoko, Hwange and Binga
Districts. ZAPIM supported the training of 25 mentors, five from each district. The participants included
doctors, nurses, pharmacists and laboratory personnel with experience in malaria case management, MIP
and good interpersonal skills. Thus far, each district has conducted the following number of mentorship
visits: Mbire-5, Murewa-5, Mutoko-4, Hwange-3, and Binga-2. The program has reached 134 health
workers including nurses, EHTs, pharmacy technicians, and nurse aides. Table 3 below shows the number
of health workers mentored and disaggregated by district and cadre.
Table 3: Health Workers Mentored to Date (May) 2018 – August 2019)
Cadre Binga Hwange Mbire Mutoko Murewa Total
Nurses 31 16 10 31 13 101
Pharmacy Tech 0 0 0 0 1 1
EHTs 3 5 6 0 0 14
Nurse Aide 1 5 5 0 3 14
Dispensary assistants 0 1 0 0 0 1
Doctor 0 0 0 1 0 1
Microscopist 0 1 0 1 0 2
Total 35 28 21 33 17 134

15
Mentorship activities
During the first visit held in June 2018, mentors introduced the malaria mentorship program to
health facility staff. They explained the mentorship rationale, agreed on implementation
approaches and communication channels, provided sensitization on mentorship tools, and, in
instances where there were differing opinions agreed on how to tackle them. In addition, the
mentors used the Mentee Self-Assessment, Clinical Performance Assessment of Mentees by
Mentor, and Health Facility Assessment mentorship tools to conduct a baseline assessment of
the quality of care for malaria at selected sites. The teams used assessment findings to identify
challenges or gaps that mentors and mentees will address during program implementation.
Subsequent visits used case studies, record review, group discussions, demonstrations to
address the gaps identified e.g. demonstration on RDT, preparation of microscopy slides (thin
and thick smears), observing mentees while managing malaria cases to recognize good practices
and address shortfalls in history taking and examination of malaria case, mentorship on proper
documentation and reporting practices. For MIP, mentorship included review of ANC registers
to verify accuracy of gestational age calculation, eligibility for SP administration to pregnant
women. Some facilities were giving IPTp doses before 13 weeks gestation and before completing
28days after the last dose as recommended. In instances where health workers were not
adhering to IPTp guidelines, mentors reinforced the importance of administration of SP
according to guidelines. ZAPIM is currently supporting the development of IPTp job aids in the
form of a calendar to help correctly identify those eligible for the IPTp and will finalize this job
aid development in Y5.
The pictures below show some of the mentorship activities carried out by different districts during the
year.

16
Mentorship results and achievements
To assess mentorship results and achievements, ZAPIM technical staff and mentors collected and
reviewed data from various sources including summary of mentorship activities from mentorship
reports, feedback from mentors and mentees (collected through google forms), malaria record review
of registers including (OPD, IMNCI, ANC registers). Table 4 includes the data collected and response
rates during the mentorship assessment, comparing May 2018 with May 2019.
Table 4: Data collected and response rates during mentorship assessment
Assessment Data points Response
rate
Mentor feedback Common activities, satisfaction with mentorship approach, benefits of
mentorship, challenges mentees face during mentorship, how to
enhance sustainability of mentorship and recommendations for
improving mentorship
21 out 25
mentors (84%)
Mentee feedback Common activities, satisfaction with mentorship approach, benefits of
mentorship, challenges mentees face during mentorship and
recommendations for improving mentorship
49 out of 98
mentees (50%)
Malaria records review OPD and Integrated Management of Neonatal and Childhood Illness
(IMNCI) registers: Assessing malaria diagnosis, treatment and
recording practices using a simple checklist for all malaria clients in
the months of May 2018 and May 2019 (i.e. before and after
implementation of mentorship activities)
ANC register: Assessing adherence to IPTp and LLIN guidelines for all
pregnant women in the months May 2018 and May 2019 (i.e. before
and after implementation of mentorship activities)
Over 500
records
reviewed
Mentee feedback
Nearly half of the mentees (45%) received two mentorship visits. The most common activities that they
participated in during mentorship visits were clinical meetings (59%), side by side/bedside teaching

17
sessions (51%) and case observations and studies (43%). On enquiring about their satisfaction with the
mentorship program, 60% of mentees scored that they are very satisfied with the mentorship approach,
74% said mentorship helped them do their work better and 67% said that this has improved quality of
services. On asking about the benefits of mentorship, mentees reported that they benefited most from
learning new skills (97%), receiving direct support from the mentorship team (51%) and team problem
solving (44%). The most common challenge that mentees face during mentorship is systems issues (63%)
such as access to commodities and supplies followed by competing priorities. Mentees recommended
that mentorship is integrated with other activities (80%), using WhatsApp groups (56%) for sharing ideas
and prioritizing peak malaria season for mentorship (61%), rather than a regular activity the year round.
Mentor feedback
On enquiring about mentor satisfaction with mentorship program 62% scored “very satisfied”, 86% said
mentorship helped mentees do their work better and 67% said that this has improved quality of
services. Mentors reported that they benefited most from learning new skills themselves (86%) and
supporting service providers (mentees) (76%). The most common challenges that mentors faced was
the unavailability of transport (71%) and mentee unavailability (57%). Recommendations to make
mentorship more sustainable are; integration with other activities, prioritizing peak season for
mentorship, using WhatsApp and other means to provide virtual follow up. On asking mentors what
they recommend going forward the following themes came up: reduce and improve the “paperwork” /
forms / documentation of mentorship activities, strengthen consistency of approach across districts,
reward improved performance of facilities (positive competition), scale to other facilities in the district,
ensure that mentors are up to date and confident to reference latest guidance, develop local strategies
to address the transport barrier and develop local strategies to promote integration.
Findings from malaria records review
The three Figures below show changes in performance or competency between 2018 and 2019. Figure 2
shows that there were higher scores for OPD, IMNCI and ANC practices with respect to malaria
performance measures in 2019 compared to the 2018 baseline. Figure 3 shows the comparison of
performance across the districts: most districts improved average performance from 2018 to 2019.
Figure 3 shows change in competency across different services of clinical case management: there were
notable performance improvements between 2018 and 2019.

18
Figure 2: Improvement in overall competency across services in May 2019 compared to May 2018
baseline
*Competency in this case is measured by adherence to recommended practices as shown in the registers measured using a
checklist with different parameters including recording of vital signs, confirmation of HIV status, recording abnormal signs in
red, recording examination findings, malaria diagnosis, classification and correct documentation of malaria treatment
Figure 3: Showing improved average performance from 2018 to 2019 by district
57.6%53.2%
72.4%
63.3% 64.0%
76.4%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
OPD Average Score IMNCI Average Score ANC Average Score
2018 2019
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Hwange Binga Mutoka Murehwa Mbire
2018 2019

19
Figure 4: Parameters with notable performance improvement from 2018 to 2019
Malaria clinical mentorship review meeting
In September 2019, ZAPIM supported a two-day mentorship review meeting in the five mentorship
activity districts. This meeting was attended by Deputy Director NMCP, Mashonaland East and
Matabeleland North PEDCOs, PMI Malaria Advisors, four ZAPIM technical staff, DHE members and
mentors from five mentorship districts. The purpose of the meeting was to review the mentorship
program, including (using the information described above), the approach that was used as well as
highlight areas where mentees and mentors may need additional training or skills building. The meeting
also provided an important opportunity for stakeholders and participants to reflect on one year of
implementation experience and provide a platform to discuss three key themes:
Implementation: Overview of mentorship implementation; was this done according to the guide?
Achievements: Review of achievements; were goal and objectives met?
Recommendations: Recommendations based on implementation experience
The mentorship review meeting activities included the following
Overview presentation on mentorship design
District presentations from five districts on their experience of implementation, lessons learned,
successes and challenges and recommended way forward
Presentation on mentorship results and achievements
Group work and discussion focused on four main areas
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
OPD Vital Signs Index OPD Positive cases in red IMNCI Positive Cases inred
Confirm if takingCotrimoxizole
Patient eligible for IPTp
2018 2019

20
o Design of mentorship: Team formation, roles and responsibilities, site visits, supervision,
how can we make mentorship more cost effective, recordkeeping, documentation, peak
season vs low season
o Overcoming persistent mentorship challenges: Transport, commodities, availability of
mentees, turnover, persistent gaps in case management
o Meaningful results: How can we better capture and report improvement of performance
of health care workers and facilities due to mentorship
o Technology: How can we use technology more effectively
Malaria case management and MIP technical updates: To ensure that mentors were up to date
with case management and MIP technical updates, Matebeleland North PEDCO facilitated a
session during the review meeting where mentors discussed August 2018 policy changes in
treatment of severe malaria in all trimesters using intravenous artesunate and treatment of
children weighing less than five kilograms using ACTs.
The photos below illustrate a) the mentorship review discussion groups and b) the mentorship review
group feedback sessions. (Photos credit: ZAPIM)

21
Based on discussions during district presentations and group work, participants came up with the
following recommendations on some specific priority areas going forward (see Table 5).
Table 5: Recommendations from the mentorship review meeting
Priority Preliminary recommendations from workshop Responsibility
Increase cost
effectiveness of
mentorship
Train peer mentors at health facility level, reducing transport,
accommodation and per diem costs
Integrate mentorship visits with other programs where
appropriate (e.g. EPI, HIV)
Prioritize facilities and / or service providers for mentorship
determined by needs at a specific facility e.g. If a facility needs
mentorship on history taking/ physical examination only the
clinician participates in that visit rather than the whole team
Prioritize malaria season for mentorship by conducting 3 visits
during peak malaria season and 1 visit off season
Mentors
DHE
DHE, mentors
Improve availability
of transport DHE leads planning for mentorship visits and reviews progress
and challenges
DHE leads integration of mentorship visits with other programs
Peer mentors at health facility level
Mentors
DHE
Mentors, ZAPIM

22
Ensure mentee
availability during
mentorship visits
Collaborate with health facilities to schedule mentorship visits
Peer mentors at health facility level
Ensure team feedback after mentorship visit to include staff not
available during visit
Mentors, sister in charge
Mentors
Mentees
Strengthen
mentorship records
and reporting
Improve tools based on challenges noted
Consider electronic tools to support recording and reporting of
mentorship
ZAPIM, provincial executive
Strengthen strategic
use of technology in
mentorship
Use of electronic tools (but ensure security of data)
Explore affordable technologies such as WhatsApp, google forms,
ODK etc. working closely with NMCP
ZAPIM, mentors, NMCP
Most of these priorities will be addressed during Year 5 to ensure that the mentorship approach is
adapted and improved to meet real needs and realities.
4.1.3 MALARIA DEATH AUDIT MEETINGS ZAPIM provided technical and financial support for one-day malaria death audit meetings in May 2019 in
Mashonaland Central and Matabeleland North (Binga and Hwange) Districts and Mashonaland East in
August 2019. A total of 45 participants attended the meeting in Mashonaland Central, 43 participants in
Matabeleland North and 50 participants in August 2019. Participants included ZAPIM staff, PMI malaria
advisors, provincial health executives, district health executives, and health workers from selected
facilities. The purpose of the meetings was to discuss malaria deaths experienced during the period from
January to the time of death audit meeting. The process involved presentation of deaths experienced in
the provinces, identification of gaps in the management of these cases, and crafting of recommendations
to address these gaps in line with the MOHCC goal of reducing malaria deaths by at least 90 percent of
the 2015 figure by 2020.
Key findings from the death audit meetings are listed below and recommendations in Table 6:
Unavailability of malaria commodities at VHW level resulting in delayed access to care;
Misclassification of malaria cases as uncomplicated, yet signs of severe malaria existed resulting
inappropriate treatment of malaria patients;
Seeking treatment from traditional healers before visiting health facilities resulting in delayed
medical treatment;
Traditional practices were used to treat the patient, such as ‘scratching the throat’ which
unnecessarily harmed the patient and delayed treatment;
Unavailability of supportive equipment and diagnostic investigations such as pediatric catheters
and urea and electrolytes machine.

23
Table 6: Findings and Recommendations from Death Audit Meetings
Findings Recommendations Responsibility
Unavailability of malaria
commodities at VHW level
resulting in delayed access
to care
Ensure malaria commodities are adequately
distributed to VHWs
Health facilities to order adequate
commodities for VHWs
District Pharmacy Managers to assist health
facilities in verifying that they order
adequate commodities
Provincial Pharmacist to assist in
redistribution of commodities across
districts
Health facility nurse in charge
District Pharmacist
Provincial Pharmacist
Misclassification of malaria
cases as uncomplicated yet
there are signs of severe
malaria
Emphasize malaria classification and differing
treatment protocols during malaria case
management trainings, mentorship and
supportive supervision
Develop clerk sheet to guide health workers
on history taking, physical examination and
classification of malaria cases
Malaria Case Management
trainers
District and Provincial Health
Executives
ZAPIM Case Management
specialists
Seeking treatment from
traditional healers before
visiting health facilities
including traditional
practices such as
‘scratching the throat’
Conduct community meetings with
traditional and religious leaders and
traditional healers to promote early referral
of suspected malaria cases for diagnosis and
treatment and understanding of harmful
practices
Educate communities on early care seeking
behavior and understanding of harmful
practices
Improving health worker attitudes (including
VHWs) which may be deterrent to accessing
care from the formal system.
Health Promotion Officer,
ZAPIM SBCC Specialists,
ZAPIM Provincial
Coordinator
Malaria Case Management
trainers, ZAPIM Case
Management Specialists and
Unavailability of supportive
equipment and
investigations such as
pediatric catheters and
urea and electrolytes
machines and reagents
Procure supportive equipment
Advocate for procurement of urea and
electrolyte machines and reagents
Health Center Committees,
Provincial Medical Director
In Year 5, ZAPIM will prioritize addressing the identified challenges as described in the table above. For
challenges beyond ZAPIM’s scope of work such as procurement of equipment, we will play an advocacy
role to with the responsible authorities. ZAPIM will continue to support death audits meetings in Year 5.
4.2 COMMUNITY CASE MANAGEMENT ZAPIM’s approach to community case management includes several interventions in an effort to promote
quality case management at the village level. The interventions implemented by ZAPIM in Year 4 include:
CCM & MIP trainings
Post training follow up
Commented [EM2]: Word missing

24
Supportive supervision which encompasses local health facility staff supervision, VHW peer
supervisors, EHT- led supervision, and orientation of health workers on VHW supportive
supervision process and tools
VHW review meetings
4.2.1 CCM & MIP TRAININGS
ZAPIM supported the MoHCC VHW trainers to train a total of 317 Village Health Workers (VHWs) in
CCM and MIP between February and April 2019. This is the period when most cases of malaria are
experienced and the newly trained VHWs were able to practice during the peak period. Table 7 shows
the distribution of the trained VHWs by district.
Table 7: Distribution of CCM Trainees by District (February – April 2019)
District Target Achievement
Binga 40 35(88%)
Mudzi 80 77(96%)
Goromonzi 40 40(100)
Centenary 80 80(100%)
UMP 80 85(106%)
Mbire 80 0
Total 400 317 (79%)
The facilitators assessed the participants’ knowledge of malaria prevention and control through pre and
post- test evaluations. In all groups, participants gained knowledge as evidenced by higher mean scores in
the post test results although there were participants who did not attain the 50% pass mark in the post
test. At the end of training facilitators revised the pre and post- test highlighting the correct responses to
the questions so that VHWs understood where they failed to respond correctly. It is during these revision
sessions that the VHWs indicated that they failed to follow the instructions on the test which required
one answer for some questions and multiple answers for others. ZAPIM has shared with NMCP concerns
regarding layout of the test paper so that it can be revised, for example grouping questions into sections
and giving appropriate instructions. NMCP indicated that this would be done when the training manuals
are being revised. However over 75% of the VHWs attained a sound understanding of signs and symptoms
of uncomplicated and severe malaria to enable them to provide quality case management in the
community. The facilitators also assessed all the participants on RDT testing and all were able to perform
the procedure according to the required guidelines.
The VHWs were attached at their clinics soon after the training for five days under the supervision of the
HF staff. This is a necessary requirement as per training guidelines so that VHWs put into practice skills
of patient assessment and RDT testing learned in the classroom. ZAPIM also provided the VHWs
participant manuals to take home after the training so that they continue to refer whenever necessary and
adhere to guidelines. Figure 5 below shows the performance of all groups trained.

25
Figure 5: CCM Trainings: Mean Scores of Training Participants by District (February – April 2019)
VHWs who did not attain the 50% pass mark continued to receive support at the clinic during their
monthly meetings and were also targeted during the post training follow up and supportive supervision
visits to strengthen their knowledge and skills. From the follow up and supportive supervision visits, HF
staff and trainers are confident these VHWs are able to assess and manage malaria cases according to
guidelines.
The trainings also involved practice on documentation in RDT/malaria register, proper hygienic hand
washing following the ten steps for infection prevention, assessment of a sick child and RDT testing.
Below are two VHWs giving feedback to the group on documentation in the RDT register using a hand
drawn chart of the RDT/malaria register. Facilitators provided the necessary feedback to ensure VHWS
took home the correct information.
VHWs giving feedback on RDT/medicine register documentation
Facilitators used the flip chart (above) to demonstrate how to properly fill out theRDT/medicines register
and requested that ZAPIM procure an A1 size chart of the register. ZAPIM followed up the request and
procured five A1 size charts of the RDT/medicines register which have been used by the Provincial
0
10
20
30
40
50
60
70
80
90
mea
n s
core
s (%
)
pre test post test

26
Coordinators to reinforce to HF staff how VHWs use the register. This was done during selected
scheduled district meetings for Mbire, Centenary and Mutoko districts and will continue in the other
districts in Year 5. Regarding the use of the A1 chart, one nurse from Centenary had this to say: “I have
seen the registers used by VHWs, but I was not sure there was a section for the staff to fill in. Thank you for taking
us through this RDT/medicines register.”
4.2.2 POST TRAINING FOLLOW UP
According to the World Health Organization (WHO)/UNICEF course on Integrated Management of
Childhood Illness for first-level health workers,1 follow up is the second component of training which
should take place four to six weeks after the initial training. The three day course which the VHWs go
through is designed to equip them with the skills and knowledge to manage patients more effectively in
the community. However the VHWs may find it difficult to begin using these skills hence they need help
to transfer what they have learned in the classroom to their community where they work from. This is
achieved through the five day VHW attachment at the clinic that takes place within four weeks post
training after which a follow up visit is conducted by trainers four to six weeks after the training.
The objectives of post training follow up are; to reinforce skills on assessment of patient (adult and sick
child) and help VHWs transfer these skills to community work. ZAPIM supported trainers from four
districts (Centenary, Goromonzi, Mudzi and UMP) to conduct post training follow up for VHWs trained
in 2019 as shown in the table below.
Table 8: VHWs followed up after training, by district, April-June 2019
District Dates of
training
Dates of follow
up
Target Achievement
Centenary 19-24 March 09-15 June 77 68 (88%)
Goromonzi 12-16 March 03-07 June 40 24 (60%)
Mudzi 26 Feb-03 March 05-11 May 80 59 (74%)
UMP 07-14 April 04-10 August 85 52 (61%)
Total 282 203(64%)
The follow-up team included one staff from the facility responsible for supervising the VHWs where
feasible, two VHW trainers and ZAPIM staff. All the VHWs trained completed their post training
attachment and are contributing significantly in malaria case management. Trainers were able to support
a total of 203 VHWs at their respective health facilities and fifty (25%) received home visits to assess
storage of malaria commodities, waste management and suitability of space used for consultations.
Home visits were only conducted for VHWs who had medicines and RDTs at their homes on the day of
the visit.
4.2.3 SUPPORTIVE SUPERVISION
The post training follow up is followed by regular ongoing supportive supervision. Ideally supportive
supervision should be ongoing however this has not been happening as expected due to competing
priorities at facility level, lack of transport at district level and non-availability of fuel for motorized EHTs.
The objectives of the supportive supervision are to:
Strengthen the skills of VHWs by evaluating their ability to assess cases, perform RDTs, give
appropriate treatment and refer severe cases
Support the VHWs in proper storage of malaria medicines, RDTS and other supplies
Support the VHWs in proper record keeping
Support the VHWs in solving problems related to their role in CCM
1 https://apps.who.int/iris/bitstream/handle/10665/66095

27
4.2.3.1 SUPPORTIVE SUPERVISION BY DISTRICT SUPERVISORS
ZAPIM provided technical support and covered allowances for supervisors from Binga and Hwange to
enable them to conduct supportive supervision of VHWs trained in 2017-2018. The approach was to visit
VHWs in their homes and provide the support however the DNO’s office informed the VHWs to
assemble at the health facilities thus affected the number of VHWs visited at home. All the VHWs (132)
who assembled at the facilities were supported and 18 eventually visited at home. The table below
summarizes the distribution of VHWs supported at health facilities and at homes.
Table 9: VHWs Reached During Supportive Supervision in February 2019
District VHWs supported at health
facilities
VHWs reached at
homes
Binga 91 6
Hwange 41 12
Total 132 18
During the supportive supervision visits, VHWs indicated that they provide services during the night
and have challenges with lighting and requested ZAPIM to support them with solar lamps.
In Mashonaland Central the Community Health Nurse from Centenary reported the same issue and
mentioned that one VHW from Chawarura Clinic realizing the need for good lighting during case
management at night bought a solar powered light using her own resources. This solar powered
light serves as a light source and can recharge mobile phones. ZAPIM will explore the possibility of
supplying VHWs with solar powered lights in Year 5 if funding permits (see photo).
4.2.3.2 VHW PEER SUPERVISOR TRAINING, APRIL 2019
Peer supervision is a cost effective way of supporting VHWs. A peer supervisor is selected by other
VHWs under the guidance of the nurse in charge at the facility. According to the MoHCC VHW peer
supervisor guidelines 2016, the selection is based on the performance of the VHW in case management
and also considers the following; reliability, honesty, empathy, approachability and good interpersonal
communication skills. In Mutoko 40 peer supervisors were selected at 12 clinics in high malaria burden
areas. In 2019 ZAPIM supported the District VHW trainers to train 38 VHW peer supervisors. The
training aimed to equip the VHW peer supervisors with knowledge and skills to conduct supportive
Solar powered light sourced by a VHW using her
own funds in Mashonaland Central, Chawarura
Clinic

28
supervision of their peers. This included the ability to conduct observation of a peer providing services,
active listening, coaching, giving feedback and developing an action plan.
4.2.3.3 VHW PEER SUPERVISORS POST TRAINING FOLLOW UP, AUGUST 2019
ZAPIM supported two VHW trainers from Mutoko District to conduct post training follow up of VHW
peer supervisors. A subset of supervisors was visited and the approach was to: 1) visit the peer
supervisor at their home and see if their quality of care is still up to standard, review their peer
supervision reports and action plans developed and 2) visit a peer’s home to observe the SS process.
The following was achieved:
A total of 11 peer supervisors were followed up at their homes. Their registers and action plans
were reviewed. All 11 had conducted at least one peer supervisory visit to their peers, and thus
30 peers were visited before the follow up date.
Six peer supervisors were observed actually providing support to their peers and they all
provided their support in a stress free manner, used the SS checklist appropriately, identified
gaps in their peers’ performance and provided constructive feedback. The other five peer
supervisors had simulations of a support visit and facilitators were taken through how the peer
supervisors had conducted the supervision. The review of action plans indicated that the peer
supervisors were able to report the work they were doing.
Six VHWs supervised by the peers during the follow up indicated that the strategy is good as it
provides an opportunity for the peers to support and teach each other.
4.2.3.4 EHT LED SS
ZAPIM is supporting MoHCC to revitalize the EHT led supervision of VHWs in three districts namely
Mbire, Mutoko and UMP where selected motorized EHTs will provide SS to VHWs. The Provincial
Coordinator for Mash East organized fuel for the 10 EHTs from the two districts and they are currently
conducting their baseline visits. Reports will be shared by the end of October 2019. For Mashonaland
Central availability of petrol in Mbire District is a challenge. The Provincial Coordinator is working
closely with the PEDCO to ensure the petrol for the eight EHTs selected is safely delivered to the
District by first week of October. Detailed reports regarding this activity will be produced in the first
quarter of Year 5.
4.2.3.5 ORIENTATION OF HCWS TO VHW SUPPORTIVE SUPERVISION PROCESS AND
TOOLS, MAY 2019
UMP is one of the malaria high-burdened districts supported by ZAPIM and has trained 271 VHWs in
community case management. However ZAPIM noted that staff at health facilities in UMP were not well
versed with the tools and job aids used by the VHWs during malaria community case management.
Therefore, ZAPIM supported the orientation of 18 health workers including six nurses and 12 EHTs in
UMP to equip them with the knowledge and skills to provide supportive supervision to VHWs.
4.2.4 VHW REVIEW MEETINGS These meetings provide VHWs with a platform to share their experiences, successes, and challenges.
The meetings also provide the HF staff and DHE opportunity to hear the issues from the community
from representatives of VHWs. In Year 4 ZAPIM supported three districts, Mbire, Centenary and
Mutoko to hold their VHW review meetings. These meetings integrated all community activities
supported by ZAPIM (CCM, LLINs and SBCC). The meetings were generally well attended with DHEs
well represented. Table X shows attendance by district

29
Table 10: VHW attendance at VHW review meetings by District, September 2019
District VHWs Nurses EHTs DHE
members
Total
Mutoko 18 17 4 5 44
Mbire 13 13 6 4 36
Centenary 13 13 8 5 39
Total 44 43 18 14 119
4.2.5 ISSUES/AREAS FOR IMPROVEMENT OF THE CCM PROGRAM
The following achievements, issues and challenges were identified and recommendations were
discussed during the post training follow up, supportive supervision and VHW review meetings:
Achievements
VHWs contribute significantly to malaria case management across all districts.
Malaria commodities were available throughout the year in the districts although were often not
in adequate amounts to allow a consistent supply to VHWs. ZAPIM will continue to lobby for
adequate supplies for VHWs to enable communities to access early testing and treatment.
VHWs are able to identify cases that need urgent referral thus preventing deaths from malaria.
All VHWs reached were making use of their registers: RDT/Medicine register, improvised adult
consultation register and the sick child registers, documentation in the registers was good.
All the VHWs were recording page totals and monthly totals in the RDT/Medicines registers.
Adult consultation registers: Although improvised, the VHWs followed a standardized format,
given by facilitators, to capture adult patient information. Generally, these registers were well
written with the required information captured.
Areas for improvement
Generally there is need for the consistent and adequate supply of RDTs and malaria medicines to
VHWs across all the districts. This will enable VHWs to maintain their skills and knowledge in
malaria case management at optimum. In Year 5 ZAPIM will continue to lobby for adequate
supplies through the NMCP and GHSC.
VHWs not suppled with rectal artesunate, zinc and oral rehydration solution (ORS), gloves and
cotton wool. HFs were encouraged by the DHEs to provide VHWs with all commodities to
facilitate provision of integrated community case management. ZAPIM’s CCM specialist shared
the 2014 memo from the MoHCC Permanent Secretary that authorized VHWs to give ORS and
zinc. Following the meetings, VHWs are now receiving zinc and ORS, rectal artesunate, gloves
and cotton wool.
Over 75 percent of the VHWs were not indicating the opening and closing stocks in the
RDT/malaria medicines register. This is a persistent gap among VHWs across all districts and
requires continued support from the health facility, District and ZAPIM staff. In Year 5, ZAPIM
Provincial Coordinators will make use of the laminated A1 RDT/medicine register job aid to
reinforce the importance of this information during selected monthly nurses’ meetings in the
districts.
The main gap in the adult consultation register was that VHWs were not indicating the duration
of illness. ZAPIM discussed with the VHWs and corrected this. ZAPIM highlighted to the VHWs
that the duration of illness is crucial to assist them to identify how early the community members

30
seek treatment when they suspect malaria. ZAPIM reminded the VHWs that individuals should
seek treatment within 24 hours of suspecting malaria to avoid complications.
VHWs were referring patients with fever who tested RDT negative for malaria to health facilities
as per the guidelines but most of these patients were not reporting to health facilities despite the
VHWs having explained the importance of further assessment. The HF staff will support VHWs
in giving information to the communities in the on-going sensitization meetings in the districts.
Use of IEC materials in English yet some community members may not understand the language.
The District Health Promotion officers are working with health facilities and ZAPIM SBCC team
to produce IEC materials in Shona.
Health facility staff were not conducting VHW supervision in the community due to competing
priorities especially for the nurses. EHTs now supporting the VHWS to ensure quality community
case management services however they have reported transport challenges. In Year 5 ZAPIM
will continue the provision of fuel to the selected 18 EHTs from high burdened wards in Mbire
(8), Mutoko (5) and UMP (5).ZAPIM will also strengthen the VHW peer to peer support.
Some trained VHWs absconding duties or relocating to urban areas thus compromising availability
of CCM services in affected areas. HF staff were advised by the DHE members to provide
information to the district regarding VHWs. HF staff are to report all VHWs who are not active
each month giving the reasons so that those persistently unable to provide services can be
replaced.
Outdoor activities like stream bank cultivation, artisanal mining along Mazowe and Nyadire Rivers
in UMP in Mashonaland East, and sleeping outdoors due to extreme temperatures are
predisposing community members to mosquito bites. The District is mapping where the artisanal
miners are and will share with the PEDCO and ZAPIM so that the miners are considered for
LLINs.
Depending on available funding, gaps in CCM training for VHWs and EHTs will be considered in
ZAPIM-supported Year 5 trainings for selected malaria high burdened districts.
4.2.6 PROCUREMENTS FOR VHWS ZAPIM supported the MoHCC, Mbire District in Mashonaland Central with procurement and
distribution of 200 medicine cabinets for the safe and secure storage of commodities at the community
level. Three cabinets were lost within the district during transportation at the time of distribution and
the incident was reported at Mahuwe Police station by the DHIO. The three cabinets have not been
recovered to date. The ZAPIM Provincial Coordinator will continue to follow up the issue with the
police until the case is closed. ZAPIM also supported the MoHCC and Mashonaland Central Province
with procurement and distribution of 186 smart phones to VHWs who provide CCM in Mbire District.
This support from ZAPIM will enable mobile reporting of weekly malaria data by VHWs (see SM&E
section 4.5.11). The phones were well received by the DHE, HF staff and VHWs as they also provide
easier means of communication between the facility and VHWs. For example HFs have created
WhatsApp groups with their VHWs thus information is travelling faster than before. The phones also
provide a light source for VHW during case management at night.

31
4.2.7 A SUCCESS STORY RELATED TO CCM ACTIVITIES IN MBIRE
4.3 LONG LASTING INSECTICIDE TREATED NETS In an effort to reduce malaria morbidity and mortality and to strengthen health systems, Zimbabwe
adopted the 2007 World Health Organization recommendation calling for universal coverage of the
entire population at risk of malaria.
According to Zimbabwe’s National Malaria Control Strategy of 2016-2020, the country deploys Long
Lasting Insecticidal Treated Nets (LLINs) in areas with Annual Parasite Incidence (API) of 2-4/1,000
population. Whilst those with an API of 5 and above benefit from Indoor Residual Spraying (IRS) and
those with an API of less than 2 are put on surveillance and Social Behavior Change Communication
(SBCC) interventions. The country, however also recognizes the existence of special communities
where some populations live in areas with an API that requires Indoor Residual Spraying (IRS) as the
choice of intervention but reside in unsprayable structures/rooms. In this regard, ZAPIM in Year 4
supported the MOHCC in distributing LLINs to cater for this special community population, who reside
mostly along the border with Mozambique.
VHW Itariya Butau (Photo credit: ZAPIM)
On 17 April 2019, a pregnant woman (six months pregnant) visited VHW Itariya Butau of Chikafa clinic in Mbire
District, complaining of fever, headache and loss of appetite. The VHW did an RDT and confirmed malaria. She
had the woman startcommenced the woman on artemether-lumefantrine and instructed her on how to take the
medicine. As a norm following the clinical protocol, after two days the VHW made a follow up visit to the patient,
and noted that the woman’s condition was not improving. The VHW reassessed the woman and found she was
now developing jaundice and was not feeding well. Mrs. Butau counselled the woman and her family and referred
them urgently to Chikafa clinic. The family took the pregnant woman to the clinic where she was further referred
to Chitsungo Hospital, the designated District hospital, after receiving pre referral treatment. On arrival at the
hospital the woman was transferred to Parirenyatwa Hospital for further treatment for severe anemia, renal
failure and jaundice. The woman stayed at Parirenyatwa hospital for two months, recovered and was discharged.
Although she lost her unborn child she is grateful her life was saved. The woman said: “VHWs are important
because they stay close to the people so I went there first. They also give free services.”

32
In Year 4 ZAPIM supported the NMCP in conducting both Mass and Continuous Distribution of LLINs
under the theme “My Net My Life”. The following were the major achievements:
Trained of 348 Health Workers (HWs) on mass distribution and 29 on Continuous Distribution
(CD)
Ten districts were supported in training 1,632 Village Health Workers (VHWs) on Mass
Distribution and 100 HWs on CD of LLINs
A total of 28,592 people comprising of community leaders and ordinary community members
were sensitised prior to conducting mass distribution activities
Distributed 624,458 blue and white rectangular LLINs through mass distribution covering
993,852 people
Supported the distribution of 101,111 rectangular LLINs through CD channels
Supported NMCP in training 62 EHTs who were involved in distributing LLINs to Cyclone Idai
affected communities in Chimanimani and Chipinge Districts of Manicaland Province.
4.3.1 MASS DISTRIBUTION
ZAPIM supported the 2019 Mass Distribution campaign of LLINs to ensure universal coverage of the
targeted populations in 10 districts of Bindura, Centenary, Guruve, Goromonzi, Mazowe, Mbire, Mt
Darwin, Murewa, Rushinga and Shamva. ZAPIM strategically established LLINs 421 distribution points
consisting of both static and outreach points in the communities so that beneficiaries were within 10 km
radius of the outreach points. This was to ensure that the 967,141 targeted populations are covered.
The photo below shows some of the beneficiaries of the 2019 mass campaign happily holding their
LLINs. The wards which benefited from the campaign had either 1) benefited from the 2016 mass
distribution campaign 2) new wards which were not sprayed in 2018/2019 season or 3) had some special
populations living along the border with Mozambique. These communities are considered to be special
due to their socio –economic activities as they live in temporary homes in Mozambique or along
perennial rivers where they are involved in streambank cultivation. They have two homes one
temporary and one permanent and spend a greater part of the year residing at the former between
October and July of each year. They also reside far away from others and health facilities and are at
greater risk of getting malaria than their counterparts who reside in the villages and have their houses
sprayed annually. These communities are normally left out of most health programs as they reside far
away from health facilities.
The broad objective for the 2019 campaign was to increase ownership, access, correct and consistent
utilization of LLINs and eventually reduce malaria transmission. Specific targets were:
1. To replace the LLINs distributed in 2016 by July 30, 2019;
2. To provide an LLIN to every registered sleeping space in the targeted 144 wards in 10 districts
by the 30th of July 2019.
In line with the above objectives the mass distribution campaign of 2019 which started on June 10, 2019
was completed on July 5, 2019. A total of 624,458 (99.9%) sleeping spaces against a target of 625,283
were covered.
:

33
Beneficiaries of the My Net My Life mass campaign displaying their just received LLINs
4.3.1.1 LLINS MASS DISTRIBUTION PREPARATORY ACTIVITIES
Prior to the commencement of the Mass Distribution campaign, ZAPIM developed a guidance document
along with several tools to facilitate activity execution, data capture and reporting in order to
standardize implementation of mass distribution activities. The following tools were developed:
LLIN 10: this form was used by the Village Health Workers (VHWs) to collect household
information. Key information collected included number of people in the household, number of
sleeping places, inside and outside, number of LLINs available and required;
Form LLIN 11: used by HF staff to consolidate information by village from Form number 10;
Form LLIN 12: a district summary of data by ward for the household registration data;
Form LLIN 13: a summary of LLINs distributed by ward for each district;
Form 7: used to assess LLINs coverage and challenges in utilization of LLINs.
These tools were used from village level up to national level. This ensured that data transmission was
standardized. Another tool used at national level by ZAPIM LLIN/Vector Control Specialist was the
LLINs Daily Master Tracker. This tool completed by VHWs and EHTs was used to monitor the daily
performance of districts and to identify and resolve challenges faced in the field.
4.3.1.2 LLINS COORDINATION
For effective implementation and coordination, ZAPIM and the NMCP outlined the roles and
responsibilities of the various players who were involved in LLINs distribution right from the onset. The
modus operandi was that supervisors and LLIN distributors were responsible for running the distribution
activities in their respective areas of operation. Each ward had six VHWs, one Environmental Health
Technician (EHT) and one nurse. Each distribution point also had two security guards. Secondly each
district had an LLIN focal person who coordinated the distribution activities and reported to the
District Environmental Health Officer (DEHO). The LLINs focal person communicated with the ZAPIM
LLINs/Vector Control Specialist on a daily basis and provided daily updates to ZAPIM. At operational

34
level the EHTs and nurses were responsible for ensuring that all appropriate and useful information on
LLINs reached the targeted audiences through ward and village meetings and household visits. They also
supervised and supported LLINs distribution activities at ward level. Table 11 outlines the roles and
responsibilities of each structure at each level of the health system.
Table 11: Roles and Responsibilities of Mass Distribution Stakeholders
Level Key Coordination Staff Key roles
National NMCP
ZAPIM
GHSC
Coordination of Mass Distribution activities
Logistical and technical support
Training of personnel in Mass Distribution
Development of guidelines and tools
Support and supervision
Delivery of LLINs to district holding points
Provincial Provincial Field Officer (PFO)
Provincial Environmental Health
Officer (PEHO)
ZAPIM Provincial Coordinator
Coordination of activities
Supporting districts
Logistical support
Training support
Provincial level sensitization
District District Medical Officer (DMO)
District Environmental Health
Officer
Environmental Health Officer
(LLINs Focal person)
District planning
Logistics coordination
Support and supervision of ward personnel
Documentation and reporting
Training support
District level sensitization
Health Facility (HF) Environmental Health Technician
Nurse
Training of VHWs
Community sensitization
Supporting VHWs (sensitization meetings and
household registration)
LLINs distribution
Community Leaders Village Heads
Health Centre Committee Community sensitization
Supporting work of VHWs
Developing community policing measures.
Overseeing distribution of LLINs
Community VHWs
Community sensitization
Household registration
Selection of distribution points
Supporting distribution activities

35
4.3.1.3 MASS DISTRIBUTION PARTICIPATING DISTRICTS, WARDS AND HEALTH FACILITIES
The 2019 Mass Distribution campaign was implemented in the same areas where LLINs were distributed
in 2016 with new areas being added. However no LLINs were distributed in IRS areas as per national
policy, except in circumstances where concurrence for such targeted distribution was reached with the
NMCP and provinces. These special areas were in Centenary, Mbire and Rushinga Districts and are
located along the border with Mozambique. These communities are considered to be special due to
their socio-economic activities. They are engaged in stream bank cultivation, gold panning, charcoal
making in the forests and relocate to Mozambique for farming between October and June of each year.
As a result they are left of the IRS program and have to be provided with LLINs although the rest of the
communities benefit from IRS. Table 12 below indicates the number of wards and HFs by district which
participated in the 2019 Mass Distribution campaign.
Table 12: Wards and Health Facilities that participated in Mass Distribution of LLINs
(2019)
Province District Districts
Wards
LLINs
Wards
# of distribution points used Health
Facilities in
LLINs Wards
Static Outreach
Mash Central Bindura 22 10 8 5 8
Centenary 29 16 7 12 8
Guruve 24 14 11 8 12
Mazowe 35 25 21 78 20
Mt. Darwin 40 16 9 20 9
Rushinga 25 9 6 3 7
Mbire 17 4 5 8 5
Shamva 29 16 13 20 12
Total 221 110 80 154 81
Mash East Goromonzi 25 17 13 97 13
Murewa 34 17 13 64 13
Total 59 34 26 161 26
Total 10 280 144 106 315 107
A total of 107 Health Facilities (HFs) covering 144 (51%) wards participated in the 2019 LLINs mass
distribution campaign. This is 10 wards more than those which participated in 2016. Mazowe District
had the largest number with 25 out of 35 wards participating in LLIN distribution. This was followed by
Goromonzi and Murewa at 17 wards each and Mt Darwin and Shamva with 16 wards each. Mbire was
the least with four wards involved in the Mass Distribution campaign.
4.3.1.4 MASS DISTRIBUTION TRAINING
The VHWs were trained over the course of one day on the mass distribution of LLINs. The facilitators
were drawn from the districts, provinces and ZAPIM. In some cases HFs decided to engage all the
trained VHWs in their wards for the purposes of properly executing the program. However no
additional financial and logistical resources were provided by ZAPIM outside the six VHWs targeted.
The trainings covered the following topics:
National Malaria Program goal and objectives for malaria and Vector Control
Malaria prevention and control with a focus of LLINs and how they work
LLINs distribution methods-mass and continuous distribution
Demonstration on how to properly hang the rectangular net

36
Safe disposal of net plastic bags
Net aeration, maintenance, care and repair including beneficial repurposing for old torn nets
Community policing measures aimed at promoting net use and discouraging misuse of nets
Data collection using the various forms LLIN 10,11, 12 and 13
Net follow ups using form LLIN 07
The trainings were done in a participatory and interactive way and the methods used were:
Presentations and Discussions
Practical work on using the data collection tools
Group work
Role play
Demonstrations on various ways of hanging the rectangular net
District orientation trainings were conducted for the people directly involved in sensitization,
registration and distribution of LLINs. This included mainly the Environmental Health Technicians
(EHTs) and nurses from beneficiary wards or HFs, key district personnel (District Medical Officers,
Administrators/Stores managers, District Environmental Health Officers, EHOs, Health Promotion
Officers and District Nursing Officers) were trained as trainers for the ward level personnel. The
district orientation trainings were held from April 8 – May 17, 2019. Major outcomes of these district
trainings included: development of ward level action plans, identification and mapping of distribution
points and development of strategies for effective implementation of the mass distribution. Table 13
below indicates the number of health workers (HWs) trained by gender and district.
Table 13: Health Workers Trained on Mass Distribution (by district and gender)
ZAPIM trained a total of 348 HWs on mass distribution. Goromonzi trained 34 (85%) of the HWs as
others were engaged in other district health programs. However the district provided on-the-job
training for those who had missed the district level trainings. ZAPIM provided technical and logistical
support for the districts and provinces to hold one-day orientation trainings for HWs. The trainings
were held in hospital and rural district council boardrooms (free venues). After the district trainings the
HWs were then tasked with the training of VHWs. Table 14 shows the number of VHWs trained by
district and by gender.
District Date Target Males Females Total
Bindura 4/8/2019 25 14 13 27
Rushinga 4/11/2019 20 15 3 18
Shamva 4/12/2019 30 21 19 40
Mazowe 4/9-10/2019 60 30 36 66
Centenary 4/11/2019 30 25 14 39
Guruve 4/12/2019 35 24 14 38
Mbire 4/13/2019 10 6 3 9
Mt Darwin 4/26/2019 40 20 19 39
Goromonzi 5/17/2019 40 14 20 34
Murewa 5/17/2019 40 9 29 38
Total 330 178 170 348
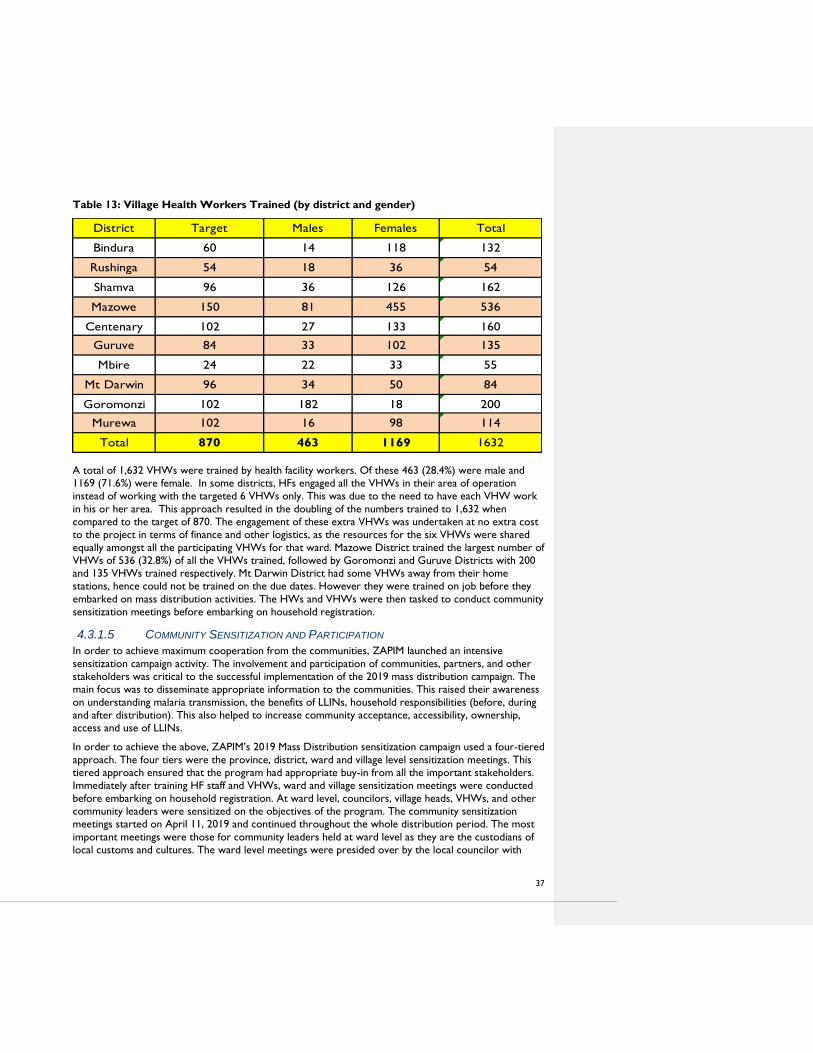
37
Table 13: Village Health Workers Trained (by district and gender)
A total of 1,632 VHWs were trained by health facility workers. Of these 463 (28.4%) were male and
1169 (71.6%) were female. In some districts, HFs engaged all the VHWs in their area of operation
instead of working with the targeted 6 VHWs only. This was due to the need to have each VHW work
in his or her area. This approach resulted in the doubling of the numbers trained to 1,632 when
compared to the target of 870. The engagement of these extra VHWs was undertaken at no extra cost
to the project in terms of finance and other logistics, as the resources for the six VHWs were shared
equally amongst all the participating VHWs for that ward. Mazowe District trained the largest number of
VHWs of 536 (32.8%) of all the VHWs trained, followed by Goromonzi and Guruve Districts with 200
and 135 VHWs trained respectively. Mt Darwin District had some VHWs away from their home
stations, hence could not be trained on the due dates. However they were trained on job before they
embarked on mass distribution activities. The HWs and VHWs were then tasked to conduct community
sensitization meetings before embarking on household registration.
4.3.1.5 COMMUNITY SENSITIZATION AND PARTICIPATION
In order to achieve maximum cooperation from the communities, ZAPIM launched an intensive
sensitization campaign activity. The involvement and participation of communities, partners, and other
stakeholders was critical to the successful implementation of the 2019 mass distribution campaign. The
main focus was to disseminate appropriate information to the communities. This raised their awareness
on understanding malaria transmission, the benefits of LLINs, household responsibilities (before, during
and after distribution). This also helped to increase community acceptance, accessibility, ownership,
access and use of LLINs.
In order to achieve the above, ZAPIM’s 2019 Mass Distribution sensitization campaign used a four-tiered
approach. The four tiers were the province, district, ward and village level sensitization meetings. This
tiered approach ensured that the program had appropriate buy-in from all the important stakeholders.
Immediately after training HF staff and VHWs, ward and village sensitization meetings were conducted
before embarking on household registration. At ward level, councilors, village heads, VHWs, and other
community leaders were sensitized on the objectives of the program. The community sensitization
meetings started on April 11, 2019 and continued throughout the whole distribution period. The most
important meetings were those for community leaders held at ward level as they are the custodians of
local customs and cultures. The ward level meetings were presided over by the local councilor with
District Target Males Females Total
Bindura 60 14 118 132
Rushinga 54 18 36 54
Shamva 96 36 126 162
Mazowe 150 81 455 536
Centenary 102 27 133 160
Guruve 84 33 102 135
Mbire 24 22 33 55
Mt Darwin 96 34 50 84
Goromonzi 102 182 18 200
Murewa 102 16 98 114
Total 870 463 1169 1632
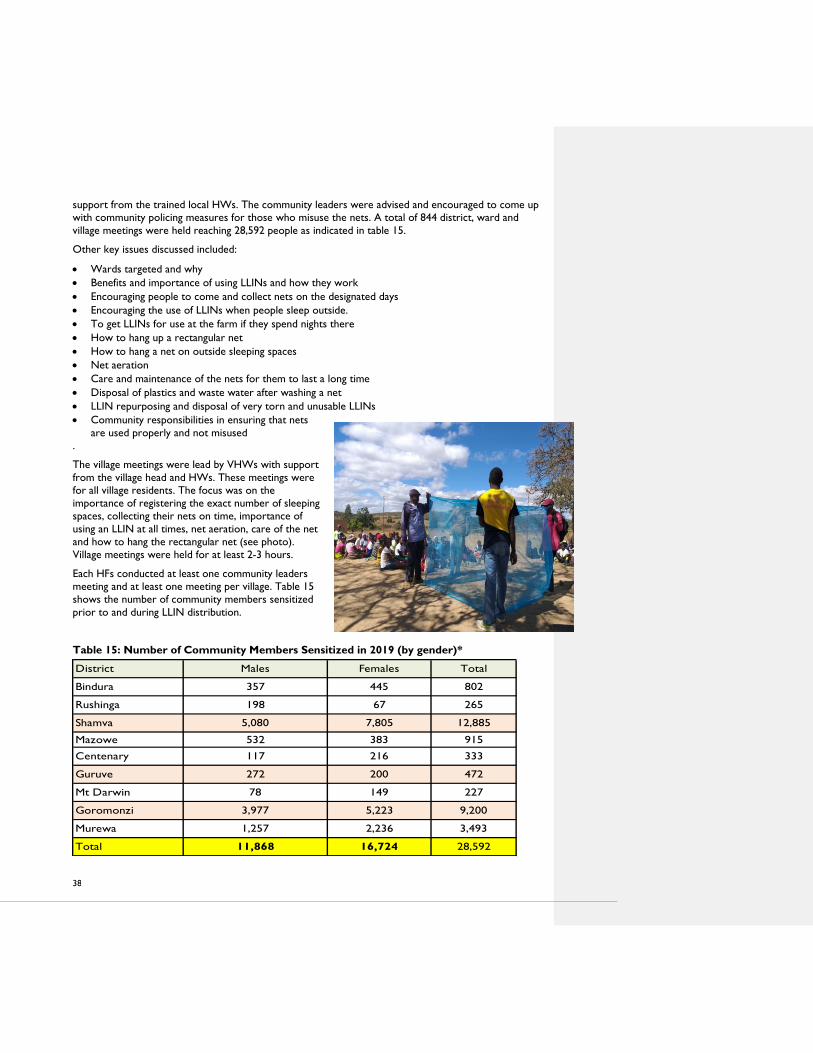
38
support from the trained local HWs. The community leaders were advised and encouraged to come up
with community policing measures for those who misuse the nets. A total of 844 district, ward and
village meetings were held reaching 28,592 people as indicated in table 15.
Other key issues discussed included:
Wards targeted and why
Benefits and importance of using LLINs and how they work
Encouraging people to come and collect nets on the designated days
Encouraging the use of LLINs when people sleep outside.
To get LLINs for use at the farm if they spend nights there
How to hang up a rectangular net
How to hang a net on outside sleeping spaces
Net aeration
Care and maintenance of the nets for them to last a long time
Disposal of plastics and waste water after washing a net
LLIN repurposing and disposal of very torn and unusable LLINs
Community responsibilities in ensuring that nets
are used properly and not misused
.
The village meetings were lead by VHWs with support
from the village head and HWs. These meetings were
for all village residents. The focus was on the
importance of registering the exact number of sleeping
spaces, collecting their nets on time, importance of
using an LLIN at all times, net aeration, care of the net
and how to hang the rectangular net (see photo).
Village meetings were held for at least 2-3 hours.
Each HFs conducted at least one community leaders
meeting and at least one meeting per village. Table 15
shows the number of community members sensitized
prior to and during LLIN distribution.
Table 15: Number of Community Members Sensitized in 2019 (by gender)*
District Males Females Total
Bindura 357 445 802
Rushinga 198 67 265
Shamva 5,080 7,805 12,885
Mazowe 532 383 915
Centenary 117 216 333
Guruve 272 200 472
Mt Darwin 78 149 227
Goromonzi 3,977 5,223 9,200
Murewa 1,257 2,236 3,493
Total 11,868 16,724 28,592
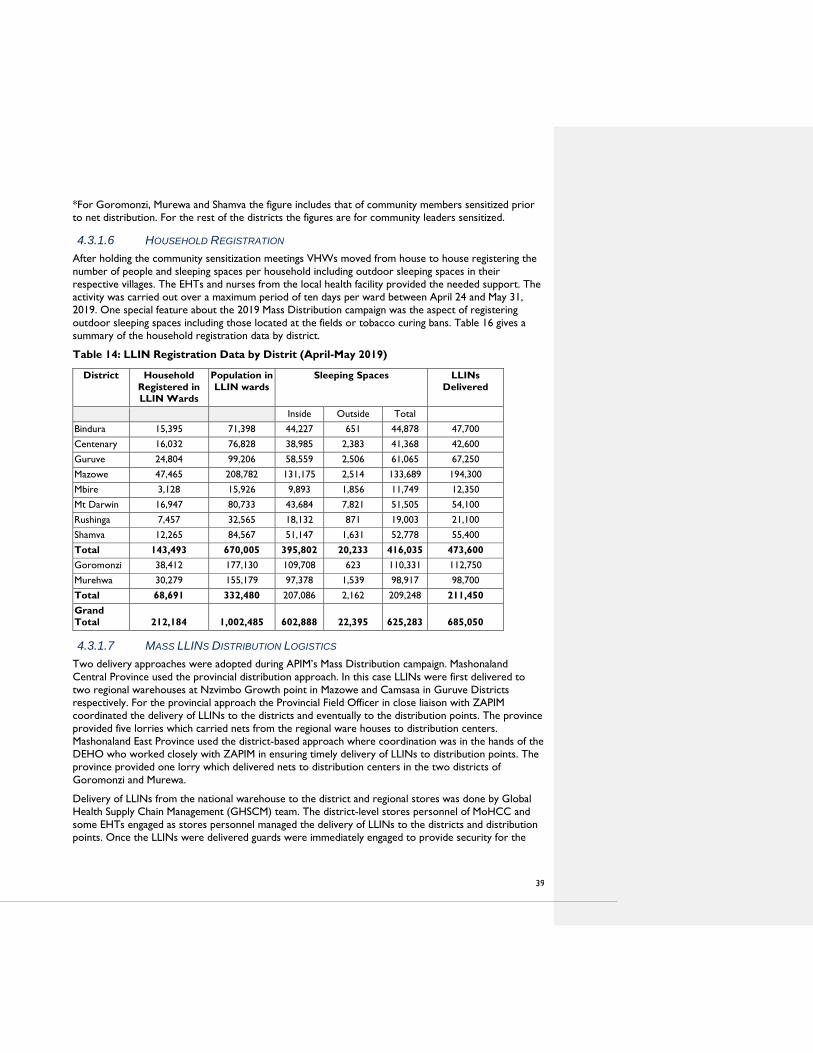
39
*For Goromonzi, Murewa and Shamva the figure includes that of community members sensitized prior
to net distribution. For the rest of the districts the figures are for community leaders sensitized.
4.3.1.6 HOUSEHOLD REGISTRATION
After holding the community sensitization meetings VHWs moved from house to house registering the
number of people and sleeping spaces per household including outdoor sleeping spaces in their
respective villages. The EHTs and nurses from the local health facility provided the needed support. The
activity was carried out over a maximum period of ten days per ward between April 24 and May 31,
2019. One special feature about the 2019 Mass Distribution campaign was the aspect of registering
outdoor sleeping spaces including those located at the fields or tobacco curing bans. Table 16 gives a
summary of the household registration data by district.
Table 14: LLIN Registration Data by Distrit (April-May 2019)
District Household
Registered in
LLIN Wards
Population in
LLIN wards
Sleeping Spaces LLINs
Delivered
Inside Outside Total
Bindura 15,395 71,398 44,227 651 44,878 47,700
Centenary 16,032 76,828 38,985 2,383 41,368 42,600
Guruve 24,804 99,206 58,559 2,506 61,065 67,250
Mazowe 47,465 208,782 131,175 2,514 133,689 194,300
Mbire 3,128 15,926 9,893 1,856 11,749 12,350
Mt Darwin 16,947 80,733 43,684 7,821 51,505 54,100
Rushinga 7,457 32,565 18,132 871 19,003 21,100
Shamva 12,265 84,567 51,147 1,631 52,778 55,400
Total 143,493 670,005 395,802 20,233 416,035 473,600
Goromonzi 38,412 177,130 109,708 623 110,331 112,750
Murehwa 30,279 155,179 97,378 1,539 98,917 98,700
Total 68,691 332,480 207,086 2,162 209,248 211,450
Grand
Total 212,184 1,002,485
602,888
22,395
625,283
685,050
4.3.1.7 MASS LLINS DISTRIBUTION LOGISTICS
Two delivery approaches were adopted during APIM’s Mass Distribution campaign. Mashonaland
Central Province used the provincial distribution approach. In this case LLINs were first delivered to
two regional warehouses at Nzvimbo Growth point in Mazowe and Camsasa in Guruve Districts
respectively. For the provincial approach the Provincial Field Officer in close liaison with ZAPIM
coordinated the delivery of LLINs to the districts and eventually to the distribution points. The province
provided five lorries which carried nets from the regional ware houses to distribution centers.
Mashonaland East Province used the district-based approach where coordination was in the hands of the
DEHO who worked closely with ZAPIM in ensuring timely delivery of LLINs to distribution points. The
province provided one lorry which delivered nets to distribution centers in the two districts of
Goromonzi and Murewa.
Delivery of LLINs from the national warehouse to the district and regional stores was done by Global
Health Supply Chain Management (GHSCM) team. The district-level stores personnel of MoHCC and
some EHTs engaged as stores personnel managed the delivery of LLINs to the districts and distribution
points. Once the LLINs were delivered guards were immediately engaged to provide security for the

40
LLINs. As per the guidance document districts,
distribution of LLINs to beneficiaries was done
within two days of delivery. This led to cut down on
costs and unforeseen risks. Stock cards were used
to manage the stocks of LLINs. Various modes of
transport were used from the HFs to outreach
points. The provinces, ZAPIM and the private sector
provided transport which distributed LLINs to
various designated distribution points. The mode of
transport provided ranged from lorries, twin cabs,
pick-up trucks, tractors, motorbikes and scotch
carts as seen in the photo (right), ZAPIM provided
fuel for the MOHCC lorries, while the private
sector provided vehicles and fuel at their cost as
seen in the photo (below).
4.3.1.8 MASS DISTRIBUTION MODEL AND DISTRIBUTION TO BENEFICIARIES
This was the second mass distribution supported by ZAPIM. Lessons were drawn from the 2016 mass
distribution campaign including the adoption of a village-based distribution model by taking the nets to
the people, assigning villages specific days and time to collect their nets, establishing LLINs outreach
points and providing LLINs even for outside sleeping spaces. LLINs outreach points were established in
areas which were 10km or more from the nearest health facility. A total of 421 distribution points were
established consisting of 106 static facilities (HFs) and 315 outreach points. This is a big increment when
compared to the 2016 mass campaign when 180 distribution points were used. Distribution of LLINs to
beneficiaries started on the 10th of June 2019 and was completed on July 5, 2019. The Provincial Field
Officer for Mashonaland Province was always on the ground as seen in in the photos below, shares a
lighter moment with some beneficiaries of the 2019 mass distribution campaign LLINs.

41
The LLINs in 2019 were distributed over an 8 day period. Table 17 shows the LLIN distribution
coverage by district.
Table 15: LLIN Distribution by District (June-July 2019)
Population Total Nets Distributed
District H/H
Covered Targeted Covered Inside Outside Total
Bindura 16,136 71,398 75,824 46,898 1,087 47,985
Centenary 16,763 76,828 76,265 38,781 2,023 40,804
Guruve 23,650 99,206 92,937 55,833 2,017 57,850
Mazowe 47,465 208,782 203,123 128,008 1,118 129,126
Mbire 4,690 15,926 15,926 9,887 1,733 11,620
Mt Darwin 17,109 80,733 82,744 45,426 6,454 51,880
Rushinga 7,747 32,565 33,060 19,006 1,364 20,370
Shamva 17,763 84,567 86,188 52,579 2,174 54,753
Total 151,323 670,005 666,067 396,418 17,970 414,388
Goromonzi 40,068 177,301 175,427 109,956 1,737 111,693
Murewa 31,879 155,179 151,768 97,217 1,160 98,377
Total 71,947 332,480 327,195 207,173 2,897 210,070
Grand Total 223,270 1,002,485 993,262 603,591 20,867 624,458

42
The 2019 Mass Distribution covered a total of 223,270 Households and 624,458 sleeping spaces. Of the
624,458 LLINs distributed, 20.867 (3%) were for covering outside sleeping spaces. This was the first
time in the history of mass distribution campaigns in the country that outside sleeping spaces were
specifically earmarked for LLINs distribution. These spaces included those at the fields, along stream
banks, at the tobacco curing barns and at small scale miners (gold panners) locations. The total
population covered was 993,262 out of a target population of 1,002,485 (99.1%). When compared to
the Mass Distribution of 2016 there has been an increase in the coverage for all key figure indicators.
Figure 5 shows a comparison of coverage between the 2016 campaign and the 2019 campaign.
Figure 2: Mass Distribution of LLINs (2016 and 2019 campaigns)
In 2019, a total of 993,262 people were covered by LLINs. This is a 16% increase in population coverage
when compared to 854,385 population covered in 2016. A total of 624,458 LLINs were distributed in
2019 which is an 11% increase compared to the 562,489 LLINs that were distributed in 2016. The
difference in coverage between 2016 and 2019 may be due to the fact that in 2019 outside sleeping
spaces were considered for LLINs distribution which was not the case in 2016. Furthermore, the 2019
mass campaign included ten more wards than in 2016.
LESSONS LEARNED AND RECOMMENDATIONS
ZAPIM has the following lessons learned from the 2019 Mass Distribution Campaign:
o Using a simple theme My Net My Life that resonated with the community members ensured
their buy in. Furthermore the beneficiaries were kept engaged during the distribution process as
they were constantly reminded of the benefits of using a net irrespective of its color, shape and
place of use.
o The use of appropriate communication structures (councilors, health centre committees,
VHWs, traditional/village leaders and local leadership and schools) to notify beneficiaries,
ensured that word reached all the targeted communities.
o The aggressive approach adopted in LLINs promotion is beginning to bear fruit as most
communities are requesting and are using LLINs for malaria prevention.
o The appointment of a LLIN focal person at district level improved communication, coordination
and implementation of activities.
o Tobacco farmers and gold panners preferred LLINs instead of IRS.
o The use of the daily master tracker ensured that LLINs distribution was monitored on a daily
basis by districts and ZAPIM and challenges quickly resolved.
Table 18 below captures the success, challenges and proposed solutions following the 2019 Mass
Distribution Campaign.
0
200000
400000
600000
800000
1000000
1200000
Population Covered LLINs Distributed Sleeping SpacesCovered
2016
2019

43
Table 16: Successes, Challenge and Solutions of the 2019 Mass Distribution Campaign
Successes Challenges Solutions
People received instruction on use of the
LLIN, how it works, how to hang the LLIN
including handling, care and maintenance
of the LLIN
LLINs were provided to outside sleeping
spaces unlike in previous years were
LLINs were only meant for use inside
houses only
LLINs were brought closer to the people
by establishing outreach LLINs distribution
points
The distribution was very orderly as
villages were given specific days for LLINs
collection
The village based approach also ensured
that people received appropriate messages
in small numbers
Community leaders actively supported the
program by holding sensitization meetings
and some accompanied their villagers to
the distribution points
Religious communities/objectors accepted
the program as they also collected the
LLINs
The 5% contingency minimized shortage
of LLINs as this covered those missed
during registration.
Some people were
out of the ward
during registration
Some registered
households had
travelled and hence
were missed
Names wrongly
omitted during the
transfer of data from
the VHWs books to
the main register
Border challenges
between districts on
registration of
beneficiaries
Temporary shortage
of LLINs
Those
households
(H/Hs) which
did not receive
LLINs will be
covered by CD.
HFs should
verify data from
VHWs at all
times
There should be
inter- district
meetings to
harmonize
operations along
the district
boundaries.
The 5%
contingency was
used to cover
the gap.
The following are the recommendations (Table 19) to address these challenges and indicates who has
responsibility for addressing these challenges going forward.
Table 17: Recommendations for LLIN Mass Districution
Challenges Recommendations Responsibility
o Local partners failed to provide the
promised vehicles to service outreach
points
o Future project to consider hiring private
transport for delivering nets from HFs to
outreach points
o The activity to be accorded a national
event so that resources are availed from
provincial to districts level
o Engage business and farming
communities/organizations in all
developmental programs from the
planning stage
ZAPIM/NMCP
NMCP/PMDs
MOHCC/ZAPIM
o Timing of campaign did not coincide with
timing of peak transmision season, when
protection is needed
o Future campaigns should be done
between March and May for impact
NMCP/ZAPIM
o Delays in daily reporting and sending data
by districts
o Provinces should take charge and play an
active role in LLIN activities in the same
way they conduct IRS operations
PEHO/DEHO

44
o Appearance of people who had not
registered prior to net distribution due
to some past false promises by other
organizations
o Conduct an intensive awareness campaign
prior to household registration
o Organizations should fulfil their promises
to the communities
ZAPIM/NMCP/PMDs
Partner organisations
o Workers not released to receive LLINs
on the scheduled distribution dates
o Continue to engage local leaders and
employers on best distribution methods
for these communities
DEHO/ZAPIM
o Low collection rates in peri-urban areas
as people were at work (formal and non-
formal) as they could not get time off to
collect their nets.
o Engage business community and also
conduct some intense awareness
campaigns prior to net distribution
DEHOs/HPOs
The provision of LLINs for outdoor sleeping places and the establishment of LLINs distribution points
closer to the people by adopting the village/farm based distribution model was a huge success. The
leadership role played by MoHCC personnel at the provincial, district and HF levels enabled the
campaign to achieve the desired objectives within the stipulated time frame. Future mass distribution
should consider establishing outreach points to bring the nets closer to the people. VHWs conducted
door-to-door household registration and educating beneficiary households for LLINs. In this year’s mass
distribution campaign the chief mobilizers were the village heads/kraal heads and councilors. The
program has been successful in making people aware about malaria in general and LLINs in particular.
Through this multipronged approached, acceptance of the program has been very encouraging and
ZAPIM and the MOHCC will build on this success for future campaigns.
4.3.2 CONTINUOUS DISTRIBUTION OF LLINS
In Year 4, ZAPIM continued to support the MOHCC and NMCP in implementing the CD activities in 11
districts. The districts are Bindura, Centenary, Guruve, Mazowe, Mbire, Mt Darwin, Rushinga and Shamva
in Mashonaland Central Province. In Mashonaland East Province three districts namely Goromonzi,
Hwedza and Murewa are supported. Table 20 indicates the number of LLINs distributed as from October
2018 to September 2019 by district and by channel.
Table 18 Continuous Distribution of LLINs, Oct 2018-Sept 2019 (by District and Channel)
District EPI ANC Community Total
Bindura 1,170 1,302 2,500 4,972
Centenary 492 1,147 10,883 12,522
Guruve 1,139 1,141 8,854 11,134
Mazowe 3,360 4,954 12,144 20,458
Mbire 178 224 3,047 3,449
Mt Darwin 2,668 3,226 13,391 19,285
Rushinga 140 186 1,122 1,448
Shamva 789 841 5,390 7,020
Goromonzi 2,044 1,625 9,354 13,023
Hwedza 35 196 891 1,122
Murewa 232 713 5,733 6,678
Total 12,247 15,555 73,309 101,111

45
In Year 4 a total of 101,111 LLINs were distributed in the 11 ZAPIM supported districts. Mazowe District
distributed the highest number of LLINs with 20,458 (20%) followed by Mt Darwin with 19,285 (20%) and
Centenary with 12,522(13%). Hwedza distributed the least 1,122 (1%), Rushinga followed with 1,448 (1%)
and Mbire with 3,449(3%). For distribution by channel the community channel remain the major channel
with 73,309(74%) followed by ANC with 13,606 (14%) and lastly the EPI channel with 11,109 (12%). The
analysis by quarter in Table 10 indicates that the highest uptake was during the 1st and 2nd quarters of Year
4. The second quarter had the highest number of LLINs 39,015 (41.5%). Distribution in quarters 3 and 4
were affected by the mass distribution campaign.
Table 19: Distribution by District and by Quarter, October 2018-September 2019
District Q1 Q2 Q3 Q4 Total
Bindura 1,270 2,580 321 801 4,972
Centenary 2,286 5,303 3,976 957 12,522
Guruve 1,230 4,760 3,477 1,667 11,134
Mazowe 4,749 10,202 2,904 2,603 20,458
Mbire 1,143 1,568 385 353 3,449
Mt Darwin 7,837 6,642 1,516 3,290 19,285
Rushinga 73 427 439 509 1,448
Shamva 2,424 3,486 682 428 7,020
Goromonzi 7,376 405 1,815 3,427 13,023
Hwedza 146 56 355 565 1,122
Murewa 508 3,586 644 1,940 6,678
Total 29,042 39,015 16,514 16,540 101,111
Starting in April 2016 when ZAPIM started supporting the NMCP in rolling out CD a total of 261,240
LLINs have been distributed to the communities through the continuous distribution channels. Figure 5
shows the distribution by year and quarter. Over the last four years the trend has been that the uptake
of LLINs is highest during the second quarter of the year (January-March). This period coincides with the
starting of the peak malaria transmission period.
Figure 5: LLINs Distributed Through CD Channel by Quarter Year 1-Year 4

46
4.3.2.1 CONTINUOUS DISTRIBUTION TRAINING OF HWS AND VHWS
CD training of HWs and VHWs only targeted HFs which commenced CD of LLINs this year. These
facilities were located in Rushinga (5 HFs), Centenary (1 HF) and Mbire (1HF). A total of 29 HWs and
100 VHWs as indicated in Tables 22 and 23 were trained in CD of LLINs.
Table 20: Health Workers Trained in Continuous Distribution (August 2019)
Dates District HF covered Health Workers Trained
M F Total
19-23/08/2019 Rushinga 5 17 6 23
8/29/2019 Centenary 1 1 1 2
8/27/2019 Mbire 2 2 2 4
Total 8 20 9 29
Table 21: VHWs trained by HF and by Gender (August 2019)
Date Health
facility
Wards
covered VHWs Trained Comments
Target M F Total
The VHWs who missed the CD
trainings were trained by the EHT and
Nurse who had attended the CD
trainings
19/08/2019 Mafigu 1 11 6 1 7
20/08/2019 Mukosa 2 11 5 5 10
21/08/2019 Chimandau 2 14 4 8 12
22/08/2019 Nyatsato 1 14 9 4 13
23/08/2019 Nhawa 2 24 12 12 24
27/08/2019 Chidodo 1 16 6 10 16
29/08/2019 Chiwenga 1 18 7 11 18
Total 7 10 108 49 51 100
Year 1 Year 2 Year 3 Year 4
Quarter 1 0 2964 10226 29042
Quarter 2 0 8013 54329 39015
Quarter 3 25411 6127 29809 16514
Quarter 4 998 8465 20958 9371
0100002000030000400005000060000
Quarter 1 Quarter 2 Quarter 3 Quarter 4

47
Challenges: Continuous Distribution Training of HWs and VHWs
Refresher courses for those trained in 2016 and some new trainings were not conducted due to
the time required to implement the the mass distribution campaign. This was further affected by
the economic situation as the trainings scheduled for the last quarter of Year 4 had to be
postponed.
The timely payment of mass distribution participants was affected by the directives from Central
Government which affected the established Ecocash payment method.
Non availability of transport and fuel at the district and ward level affected the establishment of
more LLINs outreach points as planes.
4.4 SOCIAL AND BEHAVIORAL CHANGE COMMUNICATION In Year 4 of ZAPIM, the SBCC thematic area pursued the vision stated in the Zimbabwe Malaria
Communication Strategy 2016–2020: “To have a malaria free Zimbabwe through empowered
communities who have knowledge and skills to protect themselves from malaria.” The program also
began implementing activities in support of the country’s drive towards malaria elimination and
continued to offer support for the strengthening of the NMCP’s SBCC program for malaria control.
The socio-ecological model remained the theoretical model that informed the ZAPIM SBCC approach.
ZAPIM designed and applied interventions that address not only individual practice and behavior, but
also the norms, beliefs, and socioeconomic and structural determinants influencing the demand for and
use of malaria services.
Selection of activities was based on the NMCP’s strategic behavior change priorities, which included
community awareness and adoption of lifestyle actions for the following: early illness identification and
timely health-seeking behavior, correct and consistent use of LLINs, IRS uptake, personal protection
against malaria infection, and appropriate epidemic-conscious behavior during high transmission season.
The activities were also aligned to the communication objectives in the National Malaria Communication
Strategy 2016–2020 under the areas of advocacy, vector control, CM, surveillance, cross-border
initiatives, special populations, and malaria branding and messaging.
The community-based approach of CAC mobilization model was applied to ensure intensification of
malaria community action planning and the effective implementation of those activities.
SBCC Areas of Intervention
The following areas of intervention were implemented in Year 4. Activities were conducted in
collaboration with the NMCP national, provincial, and district levels as well as the national SBCC
subcommittee:
1. Branding of the NMCP
2. Development, printing and dissemination of malaria SBCC materials and communication facilitation
tools
3. Development and broadcasting of multimedia malaria communications (radio)
4. Advocacy and communications for malaria elimination
5. Evidence gathering for improved SBCC programming
6. Production and publishing of NMCP reports on various thematic areas
7. Supporting communities for self-driven malaria actions through the CAC process and other
community-based approaches (including community dialogue forums)
48
4.4.1 BRANDING OF THE NMCP ZAPIM provided support to the NMCP to reposition the NMCP into a brand that is strategic. Through
this exercise the NMCP sought to:
Understand how it is perceived by others within the MoHCC and among the communities it
serves
Define how it wants to be perceived given its current achievements and situation
Make a plan to accomplish the re-branding.
During the reporting period ZAPIM convened a number of working sessions and consultative processes
that resulted in the following branding timeline:
Phase 1: Outline the Brand Strategy Concept and engage stakeholders.
Phase 2: Conduct data collection
Phase 3: Perform data analysis and articulate conclusions
Phase 4: Translate the research into the brand
Phase 5: Senior level review process of the brand
Phase 6: Launch and roll out the brand
To date ZAPIM has supported NMCP to achieve Phase 1 of the pathway. ZAPIM will continue to
provide support in Year 5. ZAPIM facilitated two key branding consultative sessions with stakeholders
and secured a branding specialist to oversee the process. Draft data collection to facilitate Phase 2
(Conduct data collection) were also developed. Phase 2 is expected to commence in January 2020
(Quarter 2 of Year 5).
4.4.2 DEVELOPMENT, PRINTING AND DISSEMINATION OF MALARIA SBCC
MATERIALS AND COMMUNICATION FACILITATION TOOLS
The following SBC materials were developed and printed during this period:
• Development of LLIN promotional leaflet - My net my life.
ZAPIM developed and distributed a leaflet to promote LLIN usage in communities. The 6 panel A4 size
Shona language leaflet was themed "My net, my life" based on the promotional by-line used in promoting
the LLINs at distribution. ZAPIM distributed 5,000 copies of the leaflet in Mashonaland Central. The
ZAPIM community level officers in collaboration with MOHCC staff distributed the leaflet in Mbire
Centenary and Rushinga Districts where the "My net, my life" slogan was coined and used as a byline by
the distribution teams. The project further printed 200 copies of the leaflet and distributed it at key
events such as the Mashonaland East Agricultural Show and community level meetings conducted by
ZAPIM.
Reprinting of the Communication guide for the introduction of rectangular nets for distribution in
Manicaland in response to Cyclone Idai.

49
The Cyclone Idai that affected the country in March 2019 called for an immediate response in terms of
malaria prevention. The NMCP deployed LLINs as a matter of urgency and ZAPIM supported the efforts
through providing LLINs and 500 copies of LLIN introduction communication guidelines for use by health
workers. Health workers and other active volunteers used the communication guide in educating
community members on the correct use, care and correct hanging instructions of the LLINs.
Development of material for malaria elimination areas (Lupane)
ZAPIM made a commitment to assist the NMCP with the development and printing of material to be used
in sensitizing communities in malaria elimination districts since most communication materials for malaria
behavior change and tools were developed for malaria control districts. ZAPIM supported Lupane district
to draft and develop Ndebele language material for targeting the elimination districts. ZAPIM will be
supporting the process of developing and printing of such materials. The drafted materials include:
o Flipchart tool for VHWs to use in educating communities on malaria prevention in elimination
settings,
o Behavior change communication leaflet
o Wall painting posters messaging
o A flow chart malaria guide for use by health-workers in elimination districts
ZAPIM will discuss the drafted materials with PMI and make necessary adjustments before printing them
in Year 5.
4.4.3 DEVELOPMENT AND BROADCASTING OF MULTIMEDIA MALARIA
COMMUNICATIONS (RADIO AND AUDIO)
In partnership with VectorLink, ZAPIM conducted radio based IRS sensitization activitis from mid-
October to November 2018 to encourage uptake of IRS services by communities. The radio spot
messages included content on: announcing the spraying season and that the program is conducted free
of charge, encouraging participation in IRS by allowing spray operators to spray homes and rationale for
chemical rotation.
ZAPIM developed a 60-second radio advertisement using three voices (artists) which was aired on one
national radio station (National FM -11 slots) and one provincial radio (Diamond FM -22 slots).
In September 2019, the project developed a radio spot to promote use of LLINs amongst populations
that received LLINs through the CD and the 2019 Mass Distribution campaign. The message raises
awareness on the LLINs as a malaria intervention for use indoors and outdoors, encouraged correct and
consistent use of LLINs and gave tips on correct care of the net to avoid adverse effects. ZAPIM has
paid for the radio spot to commence broadcasting in October2019 on three radio stations, namely
National FM (27 slots), Radio Zimbabwe (30 slots) and Diamond FM (24 slots). The project has made
bookings to continue broadcasting the radio spot into the peak malaria season (November and
December). The radio spots are aimed to reach over eighty percent of the population targeted by the
IRS and LLIN interventions nationally.
In addition ZAPIM continued to support and monitor dissemination of malaria control messages for the
Chikunda speaking ward of Chapoto via the Malaria Control audio book gadget. ZAPIM ensured that the
ZAPIM Provincial Coordinator made routine and regular follow ups with VHWs and Chapoto Health
facility regarding community level use of the Dipa gadget. The Provincial Coordinator ensured the gadget

50
reached targeted villages particularly sections of Mariga village where most of the Doma ethnic group live.
He also brought feedback on broken down gadgets and noted the gap for purposes of replenishment.
4.4.4 ADVOCACY FOR ACTION ON MALARIA CONTROL AND ELIMINATION BY COMMUNITIES, COMMUNITY LEADERS AND STAKEHOLDERS – WORLD MALARIA DAY
In Year 4, ZAPIM focused on the critical role of community level stakeholders and leaders in support of
malaria control and elimination activities through advocacy and awareness efforts. ZAPIM supported
malaria commemorative events and provided malaria information materials for communities such as
LLIN messaging banners, and leaflets copies on malaria facts and IPTp sourced from NMCP. The
commemorative events were used as forums for community leaders to drum up support for malaria
positive behaviors within their respective communities.
ZAPIM supported World Malaria Day commemorations at the national level and in three ZAPIM
supported provinces. ZAPIM supported the national level World Malaria Day newspaper supplement by
inserting advertorial materials highlighting malaria support provided through USAID ZAPIM in the
Sunday Mail April 25, 2019 and provided technical support for the national level malaria advocacy press
conference arranged by the NMCP SBCC and MOHCC Public Relations Department. ZAPIM’s Chief of
Party (COP) Noe Rakotondrajaona attended the press conference. ZAPIM supported the provincial
leveI commemorations in Matabeleland North, Simatelele Ward in Binga District on June 6, 2019,
Mashonaland East Province on June 13, 2019 at Goneso Clinic in Hwedza District, and Mashonaland
Central, Centenary District at Hoya Clinic on May 24, 2019. ZAPIM provided financing, technical and
material assistance and attendedthe commemorations. The COP and provincial coordinator attended
the Mashonaland East commemorations and the COP gave a speech, ZAPIM was represented by the
respective Provincial Coordinators in Mashonaland Central and East. Key issues that emerged as
advocacy points by community leaders and stakeholders at these events include:
The need to scale up malaria control activities along borders of malaria control and elimination
districts (Buhera Hwedza Border)
Encouraging people to spread the message of malaria elimination in the elimination district such
as Hwedza
Encouraging people in areas covered by IRS to support IRS teams during spraying season
Encouraging people to act on malaria through the Community Action Cycle community
mobilization model
Encouraging the local authorities to partner with MOHCC on health issues
Complimenting VHWs in assisting government efforts for health for all
Encourage use of LLINs in outdoor sleeping spaces in districts where the sleeping practice is
prevalent
4.4.5 THE SBCC THEMATIC AREA WILL TAKE INTO ACCOUNT THESE KEY
OBSERVATIONS IN THE DESIGN OF FUTURE PROGRAMMING BEYOND YEAR
4.EVIDENCE GATHERING FOR IMPROVED SBCC PROGRAMMING
In Year 4 ZAPIM continued to develop and finalize the report for the Assessment of the drivers of
continuing malaria transmission in the Angwa Ward, Mbire District. The report was developed and
extensively reviewed by ZAPIM, PMI and NMCP. The final draft report was submitted to PMI and
NMCP for review. NMCP and ZAPIM commenced the development of a follow on plan that takes into
account the key findings and recommendations from the assessment. NMCP intends to use the plan to

51
make malaria program improvements in the ward, including SBCC program improvements. The plan will
be included in the final published report and inform future programming across thematic areas.
4.4.6 PRODUCTION AND PUBLISHING OF NMCP REPORTS ON VARIOUS
THEMATIC AREAS
SBCC facilitated the production of print-ready copies of the following reports and guidelines on behalf of
the NMCP:
Malaria Epidemic Preparedness Guidelines
Surveillance Monitoring and Evaluation Plan
Assessment to determine the factors that contribute to the observed disparity between malaria case and
first-line artemisinin-based combination therapy consumption in Zimbabwe
The SBCC thematic area provided services to ensure design and layout of the documents, cover designs,
ensuring NMCP approval processes and printing of final copies.
4.4.7 COMMUNITY BASED SBCC ACTIVITIES
The main activities supported during year 4 were training of health center committees (HCCs)
in the following CAC phases : CAC Explore Health Issues and Setting priorities, CAC Plan
Together, CAC Act Together, CAC Evaluate Together, Supportive Supervision post training on
each phase, and activities facilitated by HCCs after the CAC trainings .
4.4.7.1 CAC EXPLORE HEALTH ISSUES AND SETTING PRIORITIES TRAININGS
ZAPIM supported Binga and Hwange Districts in Matabeleland North to start training on the CAC in
2018. This process started with orientation of District Health Executives from the two districts and staff
drawn from the participating facilities on CAC. Eight ward health teams in Binga (54 participants) and
eight health center committees in Hwange (80 participants) were trained on the CAC Explore Health
Issues and Setting Priorities, and the Plan Together phases. During these trainings, the communities
were assisted to develop their own community action plans. Training in Binga was conducted from 13 May to17 May 2019 and in Hwange from 8 April to 12 April 2019.
The CAC Explore Health Issues and Setting Priorities phase is the third phase of the cycle that seeks to
equip communities with relevant knowledge and skills to analyze their malaria situation, to prioritize
malaria issues in terms of importance and changeability. An assessment tool was used before the CAC
Explore Health Issues and Priorities Setting training to assess the participant’s perceived roles compared
to the roles as outlined in the HCC training manual, achievements, challenges and perceived top
conditions in their areas compared to the actual top diseases as reflected by facility data. The findings
will be used as baseline. Communities identified the following issues in Table 24 below, and were
assisted to understand the cause-effect relationship of these issues through use of participatory and conceptual tools such as community mapping and problem tree.
Table 24 Malaria Behaviors and Barriers Identified During Explore phase for Binga and Hwange Districts
Key malaria behavior Barriers identified

52
From the barriers identified, the communities were assisted to develop draft malaria community action
plans. The main strategies adopted by HCCs for
addressing these barriers include raising awareness
through conducting targeted outreach education activities
prioritizing areas experiencing more malaria cases
,formulation of community policy to minimize misuse of
nets or refusal of IRS, identification of mosquito breeding
sites , mobilizing resources for malaria activities such as
additional food stuff for spray operators, fuel , supporting
minor repairs for motor-cycle for EHTs and prioritizing
procurement of anti-malaria commodities. Before
introduction of the CAC, ward health teams did not have
malaria plans nor did they conduct outreach education
sessions. Presentation of the national malaria targets
were shared with the ward health teams and this was
compared with each respective facility’s malaria burden
which helped communities to appreciate that malaria was
indeed a problem they should aggressively address. Some
of the common issues identified by the communities that
contributed to malaria transmission include: active mosquito breeding sites; large numbers of community
members who sleep outdoors at night to guard their crops from wild animals; and individuals who sleep
in unsprayable structures (sleeping structures which are constructed of poles and are elevated to ensure
adequate ventilation as the area experiences high temperatures most of the times). The photo to the right shows the delayed presentation of a boy with severe malaria.
Late ANC booking
Fear to be tested for HIV and bearing the burden to disclose
results to partner when one is positive
Ashamed to disclose that pregnancy was unplanned.
Teen pregnancies and fear of being reported to police
Inadequate knowledge on benefits of booking early
Long distances to travel to clinic
Fear of losing unborn baby due to fear of being bewitched.
Ashamed to disclose person responsible for pregnancy
Delays in seeking
treatment/
Beliefs that illness is caused by witch craft. (See photograph
below Figure of a 6 year old boy brought to Chitse clinic
unconscious and father holding a bottle with water and stones
inside bottle; an indication that they had visited a faith healer and
in the process delayed seeking treatment.
Long distance to travel to clinics.
Flooded rivers during rainy season
Refusal or missing IRS
Skin irritations/itchiness
Causes dirty walls
Insecticide perceived as ineffective to kill other insect pests
Perceptions that mosquito density increases soon after spraying.
Involves labor to pack and unpack in some households
Late notifications by spray teams
Some homes being missed because spray operators are not
familiar with areas being sprayed
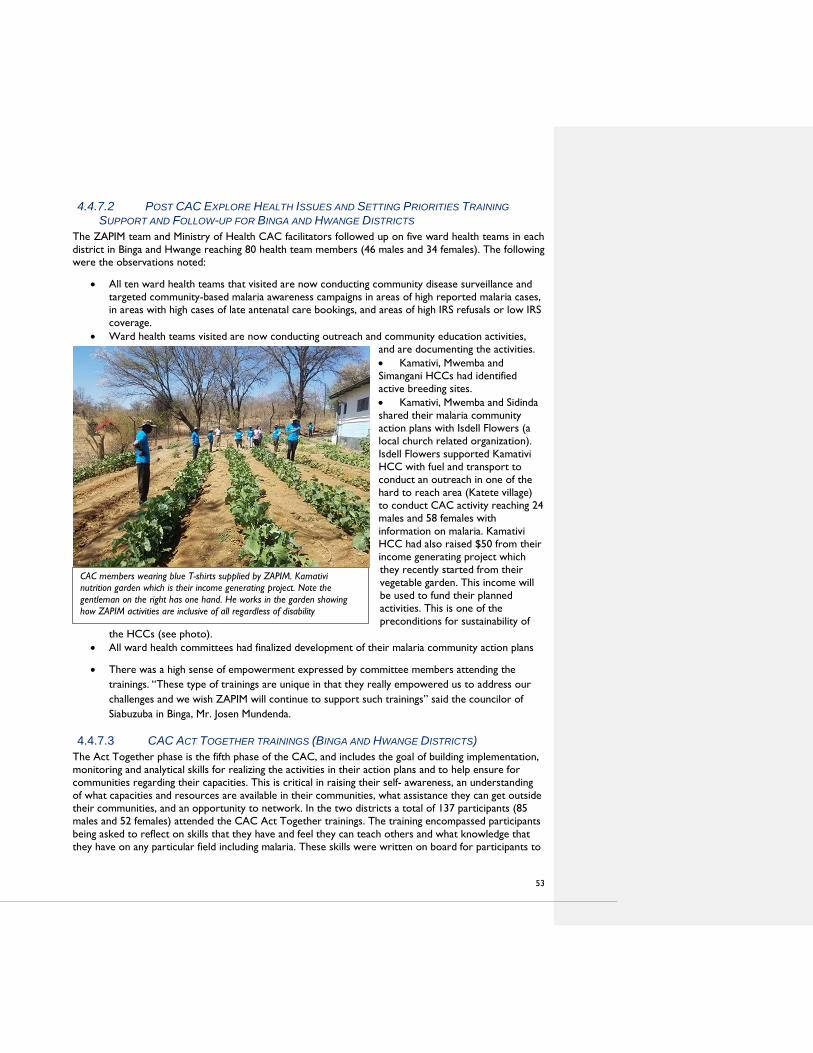
53
4.4.7.2 POST CAC EXPLORE HEALTH ISSUES AND SETTING PRIORITIES TRAINING
SUPPORT AND FOLLOW-UP FOR BINGA AND HWANGE DISTRICTS
The ZAPIM team and Ministry of Health CAC facilitators followed up on five ward health teams in each
district in Binga and Hwange reaching 80 health team members (46 males and 34 females). The following were the observations noted:
All ten ward health teams that visited are now conducting community disease surveillance and
targeted community-based malaria awareness campaigns in areas of high reported malaria cases,
in areas with high cases of late antenatal care bookings, and areas of high IRS refusals or low IRS
coverage.
Ward health teams visited are now conducting outreach and community education activities,
and are documenting the activities.
Kamativi, Mwemba and
Simangani HCCs had identified
active breeding sites.
Kamativi, Mwemba and Sidinda
shared their malaria community
action plans with Isdell Flowers (a
local church related organization).
Isdell Flowers supported Kamativi
HCC with fuel and transport to
conduct an outreach in one of the
hard to reach area (Katete village)
to conduct CAC activity reaching 24
males and 58 females with
information on malaria. Kamativi
HCC had also raised $50 from their
income generating project which
they recently started from their
vegetable garden. This income will
be used to fund their planned
activities. This is one of the
preconditions for sustainability of
the HCCs (see photo).
All ward health committees had finalized development of their malaria community action plans
There was a high sense of empowerment expressed by committee members attending the
trainings. “These type of trainings are unique in that they really empowered us to address our
challenges and we wish ZAPIM will continue to support such trainings” said the councilor of
Siabuzuba in Binga, Mr. Josen Mundenda.
4.4.7.3 CAC ACT TOGETHER TRAININGS (BINGA AND HWANGE DISTRICTS)
The Act Together phase is the fifth phase of the CAC, and includes the goal of building implementation,
monitoring and analytical skills for realizing the activities in their action plans and to help ensure for
communities regarding their capacities. This is critical in raising their self- awareness, an understanding
of what capacities and resources are available in their communities, what assistance they can get outside
their communities, and an opportunity to network. In the two districts a total of 137 participants (85
males and 52 females) attended the CAC Act Together trainings. The training encompassed participants
being asked to reflect on skills that they have and feel they can teach others and what knowledge that
they have on any particular field including malaria. These skills were written on board for participants to
CAC members wearing blue T-shirts supplied by ZAPIM. Kamativi
nutrition garden which is their income generating project. Note the
gentleman on the right has one hand. He works in the garden showing
how ZAPIM activities are inclusive of all regardless of disability

54
have an overall vision of their collective skills and talents. The second part of the assessment involved
the committees in groups to list all the planned activities in their malaria plans and identify the
knowledge, skills and resources needed to implement each activity and to identify whether it is available
in the community or whether they would need to source it from outside their community. Find below the major findings from the capacity assessments:
While assessing the individual capacity on existing knowledge and skills, the community shared
that they are a rich source of diverse skills and knowledge, including counselling, planning, selling
and marketing, gardening, mobilizing communities, leadership, support groups, and coaching
football.. The participants realized that there are a lot of underutilized skills amongst committee
members that they could can harness when implementing their action plans.
During HCC’s capacity assessments, all the HCCs and WHTs had inadequate knowledge on
malaria causes, transmission, signs and symptoms of simple and severe malaria, comprehensive
options on malaria prevention methods, comprehensive knowledge on IRS, insecticides use,
safety issues, benefits of spraying, and benefits of early booking for Ante Natal Care. The
facilitators addressed the gaps identified though this requires constant reminding given their
varying levels of comprehension. Lack of educational materials and jobs aids in the local language
to support such trainings is an added challenge. To address this challenge the Health Promotion
Officer for Binga developed a flier in Tonga and had followed the entire processes of pre-testing the material and is awaiting support from ZAPIM for printing.
Sidinda and Kamativi attempted to write proposals seeking support from partners with Kamativi
having yielded positive results whereby they received support from Isdell Flowers in the form of
fuel and transport to conduct outreach education session with one of the hard to reach Katete
village reaching an audience of 82 (24 males; 58 females) HCCs are found in poor resource
settings and for them to implement their activities ; it requires resources such as transport to
travel to remote areas, refreshments, or to pay for some of the inputs necessary for them to
implement their planned activities.
Before introduction of the CAC, all HCC meetings mainly focused on procurement issues,
infrastructural development, and hardly addressed the local disease burden, strategies for
interventions or the need to conduct outreach education meetings with affected communities.
The HCC chairpersons, secretary and treasurer had clearly defined roles in carrying out
activities with communities on malaria prevention. However the rest of the committee
members do not have clear roles. As a result ZAPIM recommended the formation of sub-
committees for monitoring and evaluation, resource mobilization and publicity that would
provide updates on their progress in implementing malaria plans and other health related issues
This helps to ensure that everyone has a role to play and share responsibilities.
All participants during the CAC Act Together trainings expressed appreciation on the micro
teaching demonstrations which participants performed and the subsequent feedbacks from the
district CAC facilitators which served to provide information gaps on general malaria, benefits of
ANC early booking, IRS and on guidance in responding to frequently asked questions from the community on key malaria issues.
4.4.7.4 CAC EVALUATE TOGETHER TRAININGS MASHONALAND EAST AND
MASHONALAND CENTRAL
The CAC Evaluate Together phase seeks to institutionalize the participation of project beneficiaries in
monitoring and evaluation of their own community activities and community action plans at all stages of
the project cycle. In addition to fostering inclusivity, other benefits of this approach include supporting

55
teamwork, enabling project beneficiaries and external evaluators to see issues from different perspectives, promoting data analysis, building skills, and facilitating critical dialogue.
The ZAPIM team and district CAC facilitators supported six districts, namely Goromonzi, Mudzi,
Mutoko, Centenary, Bindura and Mbire to train HCCs on the CAC Evaluate Together phase. The
Arcturus Mine Clinic in Mashonaland East is no longer functional following closure of the mine by Mine
Authorities which has led to the dissolving of the HCC. Therefore, the total number of HCCs where
CAC was introduced in Mashonaland East and Mashonaland Central is now 83 in the 8 districts which
have a combined total of 152 facilities. All the HCCs trained on the CAC Evaluate Together phase were
assigned to develop evaluation plans for their 2018 malaria plans and proceeded to implement the
evaluation plans, analyze the results and share the findings with the community. Furthermore, The
PEDCO for Mashonaland East has also assigned the CAC facilitators in Mash East to document the
effectiveness of CAC In order to do this ZAPIM worked with the CAC facilitators to develop data
collection too and pre-testing of the data collection tools was done in Mudzi. Results of the pre-testing
still being analyzed by the time of writing this report. Below is a table summarizing the state of CAC trainings in the 3 provinces to date.
Table 22: Distribution of HCCs Trained by District
Province District CAC phase
Target
Trained Facilities in
the district
Mashonaland
East
Mudzi
CAC Explore Health Issues and
Set Priorities
14
14
27
CAC Plan Together 14 14
CAC Act Together 14 14
CAC Evaluate Together 14 14
CAC Prepare to Scale Up 14 0
Mutoko
CAC Explore Health Issues and
Set Priorities
11 11
24 CAC Plan Together 11 11
CAC Act Together 11 11
CAC Evaluate Together 11 11
CAC Prepare to Scale Up 11 0
Goromonzi
CAC Explore Health Issues and
Set Priorities
10 10
23 CAC Plan Together 10 10
CAC Act Together 10 10
CAC Evaluate Together 10 9
CAC Prepare to Scale Up 9 0
Mashonaland
Central
Mbire
CAC Explore Health Issues and
Set Priorities
5 5
13 CAC Plan Together 5 5
CAC Act Together 5 5
CAC Evaluate Together 5 4
CAC Prepare to Scale Up 5 0
Centenary
CAC Explore Health Issues and
Set Priorities
12 12
13 CAC Plan Together 12 12
CAC Act Together 12 12
CAC Evaluate Together 12 12
CAC Prepare to Scale Up 12 0

56
Bindura
CAC Explore Health Issues and
Set Priorities
10 10
17
CAC Plan Together 10 10
CAC Act Together 10 10
CAC Evaluate Together 10 10
CAC Prepare to Scale Up 10 0
Mt Darwin
CAC Explore Health Issues and
Set Priorities
9 9
19
CAC Plan Together 9 9
CAC Act Together 9 9
CAC Evaluate Together 9 0
CAC Prepare to Scale Up 9 0
Shamva
CAC Explore Health Issues and
Set Priorities
13 13
16 CAC Plan Together 13 13
CAC Act Together 13 13
CAC Evaluate Together 13 0
CAC Prepare to Scale Up 13 0
Matabeleland
North
Binga
CAC Explore Health Issues and
Set Priorities
8 8
15 CAC Plan Together 8 8
CAC Act Together 8 8
CAC Evaluate Together 8 0
CAC Prepare to Scale Up 8 0
Hwange CAC Explore Health Issues and
Set Priorities
8
8
18 CAC Plan Together 8 8
CAC Act Together 8 8
CAC Evaluate Together 8 0
CAC Prepare to Scale Up 8 0
Grand total 10 99 185
4.4.7.5 ACHIEVEMENTS:
PARTICIPATION OF HCCS IN OUTREACH EDUCATION SESSIONS WITH COMMUNITIES
The HCCs, during implementation of the CAC, visited areas/villages that had reported high malaria cases,
to carry out informational sessions on malaria prevention with communities. The topics for discussion
were based on an analysis of health data from the clinics. This is a good practice which needs to be
strengthened as SBCC interventions should be evidence-based and targeted. The HCC’s used dialogue,
demonstrations, community mapping, and other participatory approaches to involve participants while
filling in information gaps and addressing misconceptions on the causes of malaria, signs and symptoms,
insecticides used in spraying, the aeration of nets, net hanging, and net care.
In response to HCC members presentations, the communities agreed to act on issues such as identifying
and eliminating mosquito breeding sites, conducting outreach distribution of nets to identified remote
areas (such as in Chinyani and Always), and strengthening community policing against the misuse of nets.
HCCs also continue to work through village committees (a committee chaired by village head), to
accompany VHWs during village inspections and door to door visits, coordinate with village based malaria
agents, participate in health and hygiene clubs addressing malaria and during monthly ward assembly
meetings, carry out village drama groups and through church meetings, or have one on one discussions
with community members. Observations by CAC facilitators and testimonies from some village heads

57
during supportive supervision and during trainings show that communities now report fewer incidences
of skin itchiness (one of the key barriers for not using nets) resulting from sleeping in nets not properly
aerated.
Village heads are also playing a key role in prevention, including enforcing their by-laws against net misuse
and mobilizing resources, including seconding community volunteers for malaria activities. Some village
heads speak confidently and are aware of the number of houses not sprayed, and understand related
challenges associated with IRS refusal, demonstrating that they would have participated in the programs.
More than 18,239 participants from 78 communities were reached during outreach education sessions
facilitated by HCCs. However, some of the HCCs had not documented their outreach sessions, so more
people than the number mentioned were actually reached. The HCC’s were encouraged to document
their outreach activities, in which case ZAPIM provided all the trained HCCs with stationery. Find below photos with captions from the field demonstrating how the HCCs work:
Takuramombe drama group: an initiative of Dendera HCC. Chidikamwedzi HCC during an outreach.
HCC chair Mr. Mustang giving a presentation
HCC members participated in overseeing the distribution of LLINs in Goromonzi.
HCC member leading a discussion in Mugwiza village in Shamva District.
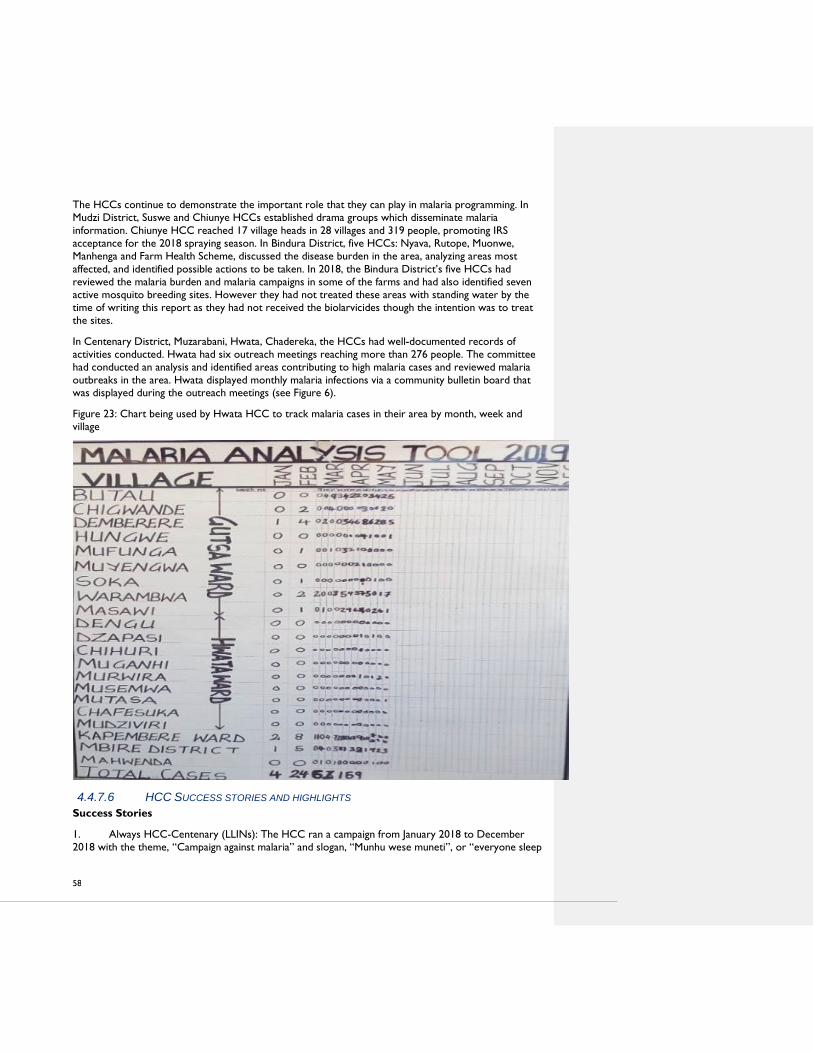
58
The HCCs continue to demonstrate the important role that they can play in malaria programming. In
Mudzi District, Suswe and Chiunye HCCs established drama groups which disseminate malaria
information. Chiunye HCC reached 17 village heads in 28 villages and 319 people, promoting IRS
acceptance for the 2018 spraying season. In Bindura District, five HCCs: Nyava, Rutope, Muonwe,
Manhenga and Farm Health Scheme, discussed the disease burden in the area, analyzing areas most
affected, and identified possible actions to be taken. In 2018, the Bindura District’s five HCCs had
reviewed the malaria burden and malaria campaigns in some of the farms and had also identified seven
active mosquito breeding sites. However they had not treated these areas with standing water by the
time of writing this report as they had not received the biolarvicides though the intention was to treat
the sites.
In Centenary District, Muzarabani, Hwata, Chadereka, the HCCs had well-documented records of
activities conducted. Hwata had six outreach meetings reaching more than 276 people. The committee
had conducted an analysis and identified areas contributing to high malaria cases and reviewed malaria
outbreaks in the area. Hwata displayed monthly malaria infections via a community bulletin board that was displayed during the outreach meetings (see Figure 6).
Figure 23: Chart being used by Hwata HCC to track malaria cases in their area by month, week and
village
4.4.7.6 HCC SUCCESS STORIES AND HIGHLIGHTS
Success Stories
1. Always HCC-Centenary (LLINs): The HCC ran a campaign from January 2018 to December
2018 with the theme, “Campaign against malaria” and slogan, “Munhu wese muneti”, or “everyone sleep

59
under a net.” During the campaign, the HCC conducted several community meetings in its catchment
area and reached 625 people (324 males and 301 females). The HCC produced accompanying reports
and videos during their outreach. One specific action the HCC took was to identify four farms that
were contributing more malaria cases in their area. Challenges these four farms face with these specific
areas include long distances to travel to the health clinic, the nearest farm being 24 km from the health
clinic. This effectively limits the ability to collect nets and access other health services, like ANC. In
response, the HCC managed to source transport to carry the nets to the village health worker to
distribute the nets to the affected farms. Additionally, the HCC had requested to have the all standing
water in these farms to be treated with larvicides. The HCC successfully reviewed its 2018 malaria
activities, produced a detailed annual report, and used the lessons learned and challenges to plan for 2019.
2. Chiriseri HCC-Bindura (LLINs): The HCC carried out a number of good practices, including a
well-written malaria plan and well documented achievements. The village head reported that they use a
neighbor-to-neighbor approach to monitoring, which requires each community member to take
responsibility of their neighbor health concerns to ensure that any suspected fever cases are reported to
the VHW. With this approach, they did not encounter any severe cases in 2018 compared to 2017
when they experienced an outbreak with reported community deaths. Due to the village committee‘s
monitoring efforts, all 6 pregnant women in 2018 were booked early for Ante Natal Care and ensured
that they receive nets. The HCC also conducted a successful door-to-door education campaign that
reached 45 of 63 households in Nhevera village and discussed malaria, net aeration, net hanging, misuse
of nets, and monitoring of net use. All households visited reported using nets. Highlights
HCC’s advocacy role in community policing measures
HCCs have demonstrated their capacity to effectively discourage negative practices through the
enactment of local policies against misuse of nets, wanton refusal of IRS, and delays in booking early for
ANC mothers. For example in Chidikamwedzi, with support from the HCC the community identified 2
individuals who were misusing nets and were asked to do community work at the clinic to increase their
awareness on the importance of malaria prevention. This has gone a long way in mitigating against
misuse of nets in the area. This demonstrates the effectiveness of malaria prevention when village heads
are involved and take ownership. Some HCCs have not received similar support from the local leadership thereby requires continuous advocacy with the leadership.
HCC’s participation in community resource mobilization
One of the indicators of success for community action groups is whether communities can mobilize
resources needed to implement their planned activities. Establishing income generating projects is one
way to ensure that the groups are financially sustainable after ZAPIM or partners leave. All the HCCs
receive Results Based Funds (funds which clinics receive based on their performance on certain
indicators) and in a way some of the committees do not appreciate the importance of raising additional
funds. RBF cannot be used for other activities. However some HCCs have heeded this advice and have
started income generating projects such as vegetable gardening, small shops, and selling printed health
cards. HCC’s use the profits to fund their malaria activities, such as repairing EHT’s motorcycle for
David Nelson HCC in Centenary; they also occasionally provide fuel and lunch allowances to the EHT
and Nurse when they do outreach malaria activities, giving fuel support to EHT’s malaria activities for
example Chibuli HCC in Mt Darwin which provided the EHT with 200 liters and Farm Health Scheme in
Bindura which allocates 3 liters per week to the EHT to support malaria activities, air time to the VHW
coordinator and refreshments to VHWs doing LLINs mass distribution activities in Goromonzi . Based
on the capacity assessments done during the CAC Act Together trainings, all the HCCs need capacity
building on resource mobilization including developing successful proposals. Only Kamativi HCC had received support from a local partner (Isdell Flowers).

60
HCC’s participation in community disease surveillance Communities play a significant role if they are well capacitated, to conduct disease surveillance activities
for malaria prevention and control. After CAC training, communities have participated in analysis of
areas most affected by malaria and have initiated targeted education sessions in the respective areas
while others have supported outbreak investigations, and subsequent implementation of interventions as
well as in identification of mosquito breeding sites and the treatment of such standing water. Activities
such as the identification of breeding sites and their treatment when implemented on a wide scale has
high potential of reducing risk of mosquito bites and malaria in particular. Below are photos and captions
of an HCC treating mosquito breeding site at Katoba River in Binga in Binga (Sinansengwe HCC).

61
Katoba Larviciding photos
A) Some of the identified breeding sites at Katoba River
B) With Katoba community members and 2 CAC Members collecting Larvae

62
Photo B above shows HCC Chair Mr. Moses Siamubeze (green shirt) and the EHT Philan Ncube all in
khaki showing larvae to villagers
EHT Philani Ncube demonstrating how to apply larviciding chemicals
CHALLENGES
Despite the achievements noted above, there are other HCCs that have shown slow progress in
generating quality malaria plans, implementation of activities, and documentation of activities despite
receiving the same training. The total number of such HCCs could not be computed given that these
observations were obtained during post training supportive supervision visits which were limited to five
HCCs per district visit. The expectation was that district CAC facilitators would in addition to the
support provided by ZAPIM integrate this activity as they perform their routine work. For example the
standard practice is that the EHT or nurse is the secretariat of HCC and should document all activities
but is not the case in some facilities. The slow progress observed on the HCCs could be attributed to:
low motivation, poor attendance of committee meetings, long distances to travel to clinic without
reliable transport, and inadequate support from facility staff and CAC facilitators, or improvised
equipment for entomology. After a half day training on a CAC phase, not all HCC members will
automatically comprehend all the issues and apply them given that they have diverse educational
backgrounds. Additional support or training may not be permissible due to limited budgets. The above
challenges can be easily addressed if both district CAC facilitators and local staff fully embrace and
integrate the approach in their routine work and by providing frequent onsite trainings during the HCC
scheduled monthly meetings and support visits to the HCCs.
4.5 MONITORING & EVALUATION/OPERATIONS RESEARCH
4.5.1 ASSESSMENT OF DRIVERS OF CONTINUING MALARIA TRANSMISSION IN
ANGWA WARD, MBIRE DISTRICT, MASHONALAND CENTRAL PROVINCE
ZAPIM continued to develop a report on the assessment of drivers of continuing malaria transmission in
the Angwa Ward in Mbire District during the year. The project worked with the NMCP to review and
refine the report. The report was submitted to PMI for further review and approval. The report is

63
expected to inform future programing as per findings from the assessment. Some of the findings were
also used during the development of ZAPIM’s Year 5 work plan.
4.5.2 NATIONAL MALARIA SM&E PLAN
ZAPIM worked with the NMCP to finalize the malaria SM&E Plan. The project supported the printing of
five hundred copies. The NMCP used the annual malaria conference platform to distribute 500 copies of
the Malaria SM&E Plan to the NMCP’s provincial and district offices.
4.5.3 EPR PREPAREDNESS AND RESPONSE GUIDELINES
The Emergency Preparedness and Response (EPR) guidelines were finalized during the year. ZAPIM
printed 1,600 copies of the guidelines and the NMCP distributed about 800 copies to the provincial and
district offices at the annual malaria conference. The remainder was set aside for the orientation of the
rapid response teams and health workers on the revised guidelines. The project also continued to have
discussions with the NMCP on the best approach to orient the rapid response teams and health
workers. The NMCP requested ZAPIM to work with the Provincial Epidemiology and Disease Control
Officer for Mashonaland East Province to come up with the training schedule and materials. The training
will be scenarios-based to enhance practical application of the principles in the guidelines. The
development of the scenarios and training materials is on-going and will be finalized in October 2019.
The trainings were initially scheduled for August and September 2019 before the peak malaria season.
However, due to budgetary constraints, these were rescheduled for the first and second quarters of
Year 5.
4.5.4 MALARIA SM&E TRAINING MANUAL
Following the successful development of the new Malaria SM&E Plan, ZAPIM offered to support the
revision to the SM&E Training Manual. The SM&E Training Manual and training materials need to be
revise to align with the new Malaria SM&E Plan, the revised EPR Guidelines, the new World Health
Organization Malaria SM&E Reference Manual, USAID/PMI M&E documents, and other relevant M&E
documents. This prudent step to align materials is meant to enhance the quality of SM&E trainings and
ensure that implementation processes occur at all levels. The facilitator’s guide and participant’s manual
will form part of the SM&E Training Manual.
In order to kick start this task, ZAPIM supported a three-day workshop from May 2-4, 2019. The
workshop involved key malaria stakeholders in building consensus on the contents and format of the
new SM&E training manual as well as coming up with a draft facilitator’s training manual. It began with an
experience-sharing session to identify issues with use of the previous manual. Some of the main issues
noted include:
Inconsistencies between the old training manuals and new tools
Time allocation and shortages of funds compromise quality of trainings
Practical hands-on experiences at times not accommodated as the training materials might not
be available
Training delivery methods not well customized to the content
Given the increased need/use of technology, there will be need to increase the length of
trainings to accommodate hands-on learning
Trainees should be those cadres that will actually use the information and skills in their day-to-
day work on the ground
Post-training follow-up is usually not done
Pre- and post-evaluations on the training sometimes not done.

64
The participants utilized the above reference resources – NMCP’s 2016-2020 Malaria Strategic Plan and
accompanying SM&E plan, the EPR guidelines, WHO guidelines, among other documents. Given the
limited face-to-face time, the development process consisted of group sessions to plan the modules,
develop modular structure and content areas, and then flesh-out the contents including examples and
emphasize areas for training sessions and tools to the new SM&E Plan and other relevant documents.
The SM&E training manual will cover a total of seven modules:
Learning Module 1: Overview of malaria SM&E system in Zimbabwe
Learning Module 2: Introduction to SM&E fundamentals
Learning Module 3: M&E program cycle and M&E tools
Learning Module 4: M&E log frame development, results framework and indicators
Learning Module 5: Data management 1- Collection, collation and submission
Learning Module 6: Data management 2- Data analysis, presentation and use, and dissemination
Learning Module 7: Data quality assurance
The NMCP requested ZAPIM to continue developing the SM&E Manual so that it will be ready for
review by other partners during the SM&E sub-committee meeting or any other forum to be convened
in the first quarter of Year 5. ZAPIM will share a solid draft of the SM&E Training Manual before the end
of October 2019.
4.5.5 CDCS
The CDCS report was reviewed and finalized during the year. The CDCS Report was submitted to PMI
for final review before printing and dissemination. A total of 50 copies of the report were printed and
will be distributed to key partners at national and sub-national levels. MOHCC requested ZAPIM to
present the findings of the study since they were relevant in the redesigning of the VHW logistics
system. All relevant partners acknowledged the relevance and importance of the findings and the
recommendations of the assessment as they have great potential to help strengthen the delivery of
malaria services in the facility and community, Health Management Information System (HMIS), and
Logistics Management Information System (LMIS), thus improving the quality of malaria data reporting.
ZAPIM will continue to work with the NMCP in reviewing the final findings, and taking action on the
areas that need improvement. The recommendations of the assessment are expected to help strengthen
the Health Management Information System (HMIS) and Logistics Management Information System, thus
improving the quality of data reported on malaria.
4.5.6 MIS ALTERNATIVE
Zimbabwe conducted MIS exercises in 2008, 2012, and 2016. Zimbabwe has a heterogeneous malaria
epidemiology which requires a carefully considered national survey methodology. This transmission
variability, and the fact that Zimbabwe is overall a malaria low prevalence country, has brought about
discussions among malaria stakeholders on the most appropriate type of national survey to measure
malaria indicators. During the third quarter of the year, ZAPIM assisted the NMCP to look for other
examples of countries that are developing unique alternative methods to the standard MIS. Six options
were identified, namely: MIS within the Demographic and Health Surveys; MIS (stand-alone), continuous
MIS, strengthening the DHIS2, a ‘hybrid’ approach between the last two options and antenatal care
attendees as a surrogate for a household survey. ZAPIM developed a brief description for each option
and its advantages, disadvantages/limitations, and likely cost implications. Where appropriate,
experiences from elsewhere on the use of the proposed options were mentioned. The brief is intended
to be the starting basis for further discussions with the NMCP, PMI and other partners to decide on
which option(s) to pursue. Once the partners have chosen a method(s), ZAPIM will develop a detailed
proposal for it in Year 5. Based on time, resources, and NMCP availability, ZAPIM will facilitate NMCP’s
development of a high-level suggested roadmap to implementation.

65
In the meantime, however, a decision has been made to integrate the 2020 MIS into the Demographic
and Health Survey. ZAPIM will work with NMCP and other stakeholders to develop an appropriate
methodology, review the protocol, questionnaires and the draft report.
4.5.7 DOCUMENT AND REVIEW TRAINING GAPS BY THEMATIC AREA
ZAPIM devised a systematic approach of assisting the NMCP and provinces to establish a reliable
database on training gaps by thematic area. ZAPIM took advantage of other activities that it supported,
such as the provincial and district malaria review meetings, to gather and update the database
information. In Year 5, the ZAPIM provincial coordinators will work closely with the provincial and
district staff to quantify and verify the number and type of staff positions, active employees, and staff
training history in order to more accurately identify actual training gaps.
4.5.8 NET DURABILITY STUDY AT MONTH 36
Month 36 is the last time point of the Net Durability Study. ZAPIM trained field staff and collected data
in February 2019 with support from NMCP and NIHR. Soon after the field work, the project cleaned
the data and also prepared the ground work for data analysis. Data analysis and report writing were
conducted in quarters 3 and 4. The first draft report was submitted to NMCP and PMI for review. The
project responded to the comments and re-submitted the report to PMI for further review and
approval. Meanwhile, an abstract has been developed, reviewed and approved by NMCP and PMI. It has
since been submitted for the ASTMH Conference which is scheduled for November 2019.
4.5.9 PROVINCIAL MALARIA REVIEW MEETINGS
ZAPIM provided both financial and technical support to Mashonaland Central, Mashonaland East and
Matabeleland North provinces to undertake malaria review meetings. A total of 134 participants (99% of
target) attended the meetings. Participants were drawn from the PMD’s Offices, DHEs, and health
facilities. The main objectives of the review meetings were to:
Review the malaria situation in the provinces.
Share progress in the implementation of malaria interventions in the two provinces
Share and discuss the DQA findings and recommendations. It was also a platform to discuss the
quality of data which is generated both at community and facility levels
Share and discuss the revised EPR guidelines
Share best practices among the districts and health facilities
ZAPIM also used this opportunity to share and discuss the remaining activities up to the end of
September 2019, covering all ZAPIM thematic areas. The proposed VHW mobile reporting pilot in
Mbire District was one of the activities presented at the Mashonaland Central provincial malaria review
meeting and the provincial leadership accepted it. There was a consensus that NMCP, ZAPIM and
MOHCC lower level structures should learn from the pilot as there is great potential to cascade the
initiative in other districts in the country.
4.5.10 DQAS
During the year, ZAPIM supported the three provinces to conduct DQAs at selected health facilities in
the districts. A total of 32 health facilities: Binga (4), Hwange (6), Rushinga (6), Mt Darwin (6) and Mudzi
(10) participated in the DQAs. The main objectives of the DQA were to:
Conduct onsite data verification of selected malaria indicators at sampled health facilities in
various districts
Verify indicator data against primary source documents, document the reasons for variance and
ensure that the data is updated

66
Assess whether the selected health facilities have adequate data collection and reporting tools
Assess whether some of the facilities are still in malaria outbreak status
Assess the availability of updated outbreak thresholds at health facilities.
Ensure that the environmental compliance component is integrated into the DQAs
The DQAs were conducted together with the provincial and district staff. The team members used this
platform to provide on-the-job coaching and mentoring. Table 26 highlights some of the key findings and
recommendations.
Table 23: Key findings and recommendations from DQAs, May-June 2019
Key Findings Recommendations
Although improvised, registers (T12 and IMNCI) were
in place and in use
ZAPIM assisted the three provinces to come up with
standard registers. The districts were requested to print
these registers using RBF resources, whilst awaiting
standard registers from MOHCC
All the T5 forms were in place and well filed Health facilities were encouraged to keep up the good
work
T5 forms were being submitted and entered into the
DHIS2
The district offices were requested to verify the data
before entering into DHIS2
VHW data was being incorporated into the rapid
disease notification system
Health facilities were encouraged to keep up the good
work
Malaria cases were managed according to the national
malaria treatment guidelines
Health facilities were encouraged to keep up the good
work
Data discrepancies between the T12 and T5 and the
DHIS2
The district offices were requested to verify the data
before entering into DHIS2
Low index of suspicion with most cases that qualify to
be malaria suspects being missed for malaria RDT
All suspected cases to tested for malaria
Patients treated based on clinical diagnosis because of
stock out of RDTs.
There is need to properly document and ensure that
such patients are not considered as confirmed cases
Binga District hospital incinerator had broken down The district was encouraged to mobilize resources and
expedite the repair or replacement of the incinerator if
it is beyond repair
4.5.11 WEEKLY VHW MOBILE REPORTING PILOT IN MBIRE DISTRICT
ZAPIM provided financial and technical support in piloting the weekly mobile reporting by VHWs in
Mbire District. Mashonaland Central Province’s Mbire District—one of the highest malaria burden
districts in the country, was selected, in consultation with the NMCP and the PMD’s Office. Mbire
District has a total of 13 health facilities. Timely reporting will assist the district to detect, investigate,
and respond to any reported epidemic. ZAPIM supported this initiative through the design of the
system, using Open Data Kit (ODK) platform, pretesting the system, orientation of one hundred and
eighty-six VHWs and twenty-six health facility staff (13 nurses and 13 EHTs) in the district and the
procurement of cellphones. ZAPIM, NMCP, PMD and DMO’s offices were represented during the
pretesting and training exercises. The system works offline during data entry and only requires the
mobile network to be active when the VHW is ready to send the data through SMS to the health facility.
VHWs started reporting to their respective health facilities from the fourth week of August 2019.
However, a total of 61mobile lines were mistakenly deactivated by Econet before some of the VHWs
started reporting and this affected the reporting rate on a weekly basis (67%). Econet failed to re-

67
activate the lines and issued new lines on the last week of September 2019. ZAPIM and DMO’s office
are making frantic efforts to ensure that the affected VHWs receive the new mobile lines before the
second week of October 2019.
4.5.12 RDT REGISTERS FOR VHWS
As per request from the three provinces, ZAPIM printed 1,160 copies of RDT registers for VHWs. The
project will start distribution of the printed copies in April 2019.
4.5.13 ORIENTATION OF ZAPIM STAFF IN GLOBAL INFORMATION SYSTEM MAPPING
As part of partner collaboration, ZAPIM requested the Clinton Health Access Initiative to orient ZAPIM
technical staff on Quantum Geographic Information System mapping. This is one of the steps that
ZAPIM has taken as it prepares to collaborate with the Clinton Health Access Initiative on implementing
elimination activities in the country. This orientation will enable staff to map the coverage of
interventions supported by the project. As the project started moving into malaria elimination work,
mapping of cases becomes a key activity in surveillance and monitoring of malaria foci.
4.6 MALARIA ELIMINATION ACTIVITIES IN LUPANE DISTRICT, MATABELELAND NORTH ZAPIM started implementing malaria elimination activities in Lupane District in Year 4. Zimbabwe has
been implementing malaria elimination work since 2012, beginning with seven districts in Matabeleland
South and growing to 20 districts in 2015. The National Malaria Strategic Plan or NMSP (2016-2020) aims
to implement malaria elimination in 30 districts by 2020. Zimbabwe is currently on track to reach this
target as another eight districts were added to the list following a capacity assessment done in 2018.
To develop a plan of elimination activities to support in Year 4, ZAPIM met with the Matabeleland North
provincial team, Lupane District staff, Clinton Health Access Initiative (CHAI), and the NMCP focal person
for elimination to understand where ZAPIM support could be most beneficial and to harmonize and
coordinate approaches where possible. ZAPIM, CHAI, and NMCP held several meetings to identify,
discuss, and better coordinate the elimination activities. Following these meetings, ZAPIM created a micro
plan that it shared with PMI before finalization. In Year 4 ZAPIM supported the following key areas:
Enhanced surveillance trainings for nurses and EHTs. This training gave HCWs an overall
understanding of their roles and the scope of activities in malaria elimination and the national
guidelines for malaria elimination.
Strengthening foci response. This training equipped HCWs with the knowledge and skills
needed to proactively and reactively respond to potential and existing malaria transmission foci—
in accordance with the national guidelines.
Entomology training for EHTs. ZAPIM worked with Vector Link and Adeline Chan from
CDC to identified key areas for the entomology training. The training gave cadres the theoretical
and practical skills they need for active and routine vector surveillance of breeding sites and adult
vectors within their communities.
Geographic Information System (GIS) mapping. ZAPIM also supported training in
electronic mapping of malaria cases, vectors, vector breeding sites and malaria transmission foci.
4.6.1 ENHANCED SURVEILLANCE TRAINING
ZAPIM supported enhanced surveillance training for all the environmental health cadres in Lupane District
(18 EHTs, three Environmental Health Officers (EHOs), and four Field Officers). The training took place
in Bulawayo from March 18-20. Twenty-four of the participants were from Lupane District, including the

68
District Environmental Health Officer (DEHO) and five new EHTs who were recruited in 2019. The
Provincial Field Officer also participated in the training. The facilitators included the Provincial
Epidemiology and Disease Control Officer (PEDCO), the Provincial Environmental Health Officer (PEHO),
and DEHOs for Umguza, Bubi, and Tsholotsho Districts.
The training covered the following topics:
Overview of malaria in Zimbabwe generally and Lupane District specifically
Introduction to malaria elimination
Basic malaria epidemiology and transmission
Approaches and tools specific to malaria elimination programs
Introduction to key concepts in pre elimination
Community-based surveillance and preparedness for malaria elimination
Malaria investigation and surveillance in elimination
Road map to elimination from advanced control to the prevention of re- introduction phase
Foci classification group work
Entomological surveillance
Pre-elimination indicators, data tools, and timelines (including group work)
DHIS2 tracker
Tracker practical
Case management in elimination
o RDT testing practical
o Slide collection practical
As part of the training, the participants developed and discussed ward-level and district-level malaria
elimination plans.
4.6.2 STRENGTHENING FOCI RESPONSE
ZAPIM provided technical and financial support for this two-day training held on April 1 and 2, 2019.
The training was attended by 17 EHTs, two EHOs and six nurses. The nurses included the District
Community Health Nurse and five nurses selected from Dongamuzi, Jotsholo, Dandanda, Fatima and
Gwayi Clinics with active foci. Training topics included case management for elimination, case
investigation and classification, active case finding, foci mapping, foci classification, SBCC, and vector
control responses to local malaria cases. The case management training emphasized the use of single
dose primaquine for clearance of gametocytes to cut out malaria transmission and the active surveillance
and reporting of any primaquine related side effects. The trainer highlighted the importance of active
case finding and performance of microscopy in all RDT positive cases. Other key learning points were
notification of cases within 24 hours, classification of cases within 72 hours and foci investigations within
seven days. The training taught the participants the classification of cases as follows:
Local: malaria cases acquired within the elimination district by mosquito borne
transmission. The alternative terms are indigenous, introduced or autochthonous case.
Imported: malaria cases originating from a malarious area outside of the 28 malaria
elimination districts.
Intraported: malaria cases acquired from a malarious area outside the district but within
another malaria elimination district.
The training was guided by the Zimbabwe Malaria Foci Investigation and Response Algorithm shown in
Figure 7 below.

69
Figure 7: Zimbabwe Malaria Foci Investigation and Response Algorithm
The participants were taught the classification of foci as per WHO 2017 guidelines as follows:
Active foci: where there is ongoing transmission where locally acquired cases have been
reported in current calendar year.
Cleared foci: where there has been no local malaria transmission for more than three years
and which is no longer considered residual non-active.
Residual, non-active foci: where transmission was interrupted recently (i.e., one to three
years). The last local case was detected in the previous calendar year or up to three years
earlier.
During the training, participants had a practical session in which they were placed into groups and given
information for RDT positive cases from the nearby Gwayi Clinic. They were then tasked to conduct case
follow up, investigations, classification and foci mapping around the identified cases.
4.6.3 EHT ENTOMOLOGY TRAINING
All the environmental health cadres in Lupane District (19 EHTs, the DEHO, two EHOs, and three Field
Orderlies) attended the three-day training in Lupane from April 3 to 5, 2019. ZAPIM coordinated with
trainers from VectorLink, Africa University, National Institute of Health Research (NIHR) and Adeline
Chan from the Centers for Disease Control and Prevention, Atlanta. The training focused on essential
skills required for routine vector surveillance for elimination and active response to malaria cases. The
topics covered included identification and staging of vector mosquito larvae, identification of adult female
anopheles mosquitoes and differentiation from male anopheles and culicine mosquitoes. The participants
received training related to the identification of vector breeding sites, larval scooping, methods of

70
collecting adult mosquitoes, preservation and transport of mosquitoes and biolarviciding. There were
practical sessions on larval scooping, setting up of Centers for Disease Control and Prevention light
traps, Pyrethrum Spray Catch (PSC), use of suction tubes, using Prokopack aspirators (PPA) and
biolarviciding.
The advantages and disadvantages of each method of collecting mosquitoes were also discussed. These
included the need for expensive equipment and functional batteries for PPA versus the cheaper PSC.
The PSC needs adequate reliable supply of the pyrethrum spray cans. Given the limited availability of the
PPA and the challenges of batteries even when the aspirators are available, the district was encouraged
to get enough pyrethrum spray cans for use and to ensure ready access to the available equipment for
the EHTs.
During the training, the participants had a practical session on biolarviciding at breeding sites in
Maganganga. The community of the area was involved in the biolarviciding session as part of the
community engaged in the areas that was started through the CAC process. The photo below shows
the community involvement in biolarviciding of a breeding site.
Going forward, ZAPIM will consider redesigning the entomology training to allow for more days (i.e., five
to seven), develop a standard training manual, and ensure availability of adequate equipment and mosquito
specimens for the training and better instruction on biolarviciding.
4.6.4 TRAINING IN GIS MAPPING
ZAPIM supported the training of 25 EHTs from Lupane District on Geographic Information System
(GIS) mapping for quality mapping of malaria cases, vectors, vector breeding sites, and malaria
transmission foci. The training occurred in Bulawayo from April 15 to 17, 2019. In the past, facilities
have been relying on hand drawn maps. Training in GIS mapping allows for more accurate mapping using
geo-codes that are obtained using the DHIS2 Tracker tablets that are used in cases investigations and
notification in elimination districts.
Community participation in larviciding during entomology training in Lupane,
April 2019.

71
4.6.5 ZAPIM MICRO PLAN FOR ELIMINATION
ZAPIM developed a micro plan for supporting elimination activities in Lupane District with inputs from
PMI. PMI encouraged ZAPIM to learn from current implementation efforts to improve future
implementation. The micro plan will guide ZAPIM’s activities in Year 5. Based on the micro plan, ZAPIM
will promote uniform, quality training of all partners and trainers to ensure there is a full array of
training (including MOP-UP) materials, standard operating procedures, and any other tools/job aids for
CM, SM&E, SBCC and vector control in elimination, including refresher trainings. ZAPIM will review the
need for job aids and tools including support for slide preparation. There is a need to improve on the
quality of entomology trainings by allowing more time and more hands on access and use of key
equipment by the trainees. ZAPIM will institute supportive supervision visits, elimination specific review
meetings and data quality audits.

72
5. GENDER AND CHILD
SAFEGUARDING Gender equality and child safeguarding remained key guiding principles for ZAPIM in Year 4. ZAPIM took
the opportunity to re-commit to gender equality and raise consciousness amongst its entire staff through
participating in the #Better for balance campaign held on International Women’s Day 2019. The campaign
which was supported by Abt Associates in all countries of operation saw ZAPIM personnel at all levels
and across gender supporting it overwhelmingly. The scheduled occasion was well attended and
supported by male staff and a genuine interest was shown as all levels of staff from Directors to support
staff such as the drivers from both ZAPIM and Vectorlink projects discussed issues of gender equality
openly and objectively. ZAPIM also participated in celebrating the 100 year achievements of Save the
Children’s work in child protection the world over and in Zimbabwe.
ZAPIM implemented the Year 4 activities in full consideration of gender issues with an emphasis on the
protection of its employees from sexual harassment. There was no reported incidence of any form of
discrimination based on sexual orientation. The project allowed equal participation of women and men in
all the trainings conducted across the thematic areas. LLINs were distributed to both women and men.
All activities were implemented in a gender sensitive manner. During the development of SBCC materials,
both men and women were engaged under equal contractual terms. Language used in the trainings and on
all materials developed was gender sensitive.
During Year 4, both women and men undertook the practice and perception of malaria key interventions.
Pregnant women were given LLINs during antenatal visits and counseled to regularly sleep under an LLIN
to protect her and the unborn child. Women played a leading role in making sure that their children slept
under nets, and they were typically the frontline caregivers, who sought treatment for their children. All
proposed SBCC interventions were designed to align with gender norms in the community while focusing
on empowering women to carry out the recommended behaviors for malaria treatment, prevention,
control, and elimination.
In Year 4, the program continued to be vigilant in all activities related to the existing child safeguarding
policy and ensured child safety in implementation of all program activities. The program oriented all staff
in compliance with the child safeguarding policy. No incidents of child violations or child rights violations
were reported during this reporting period. The program made deliberate efforts to ensure that activity
schedules and venues considered suitable travel times for parents and child minders travelling to and from
the ZAPIM–related activity and allowed time to care for children. Mothers brought their infants to the
short community-based workshops. Furthermore, breaks were established throughout the activities to
enable mothers to breastfeed their babies at suitable times. In the case of residential workshops, mothers
who needed to bring babies did so and provided a childminder. The safety and welfare of children was of
utmost importance.
Children remained important beneficiaries for ZAPIM-led malaria prevention services. The LLINs
continuous distribution systems continued to ensure children’s sleeping spaces were covered and LLIN
distribution for children remained a priority.

73
6. ENVIRONMENTAL COMPLIANCE
Health programs, including those supported by ZAPIM, may have negative environmental effects. To
ensure the optimal environmental protection, USAID-funded projects, programs, and activities must
have measures in place to mitigate any anticipated environmental effects. ZAPIM focus areas that could
have potential negative effects on the environment include the following:
Generation of medical waste at both health facility and community levels
Disposal of LLIN solid and liquid waste
Management of public health medicines and commodities
6.1 MEDICAL WASTE If medical waste generated from health facility and community case management is not properly handled,
stored, and disposed there is risk of disease transmission. As with the previous years, in Year 4, ZAPIM
technical staff supported health facilities and community health workers in infection prevention. Through
case management trainings, ZAPIM trained health workers on infection prevention using measures such
as wearing gloves when handling medical waste, avoiding recapping of sharps, proper disposal of sharps
into puncture proof sharps containers, and disaggregation of medical waste in color coded bins. At the
community level, the program also trained VHWs on proper handling of medical waste as they are
expected to bring medical waste to health facilities for proper disposal every month. Apart from
trainings, the program uses supportive supervision visits to mitigate identified gaps in handling and
disposal of medical waste and to ensure implementation of suggested measures. In the future, ZAPIM
will integrate environmental compliance into quarterly data quality assessments.
6.2 LIQUID AND SOLID LLIN WASTE The distribution of LLINs generates solid waste from LLIN packages. Considering the high volume of
nets the program distributes, there is potential harm to the environment if proper disposal procedures
are not followed. Washing of nets at the household level may also lead to contamination of water
sources if communities are not taught the proper disposal of water from LLIN washing. To mitigate the
negative environmental effects of liquid and solid waste VHWs and health workers are trained on
proper disposal of waste from LLINs. LLIN packaging is cut into small pieces and buried in a pit 50-100
cm deep, away from water bodies. Nets should not be washed in rivers or dams but should be washed
in a dish and water should be disposed in a pit. The program gives this information to community
members during LLIN distribution.
6.3 MANAGEMENT OF PUBLIC HEALTH MEDICINES AND COMMODITIES ZAPIM supports activities at both the health facility and community level where medicines and
commodities such as malaria medicines, testing kits, syringes, gloves, etc. are distributed. There is a risk
of children ingesting improperly secured medicines. Medicines may also expire; and using expired
medicines may result in poor treatment outcomes. It is therefore necessary to have good medicines and
commodities management practices in place. Through malaria trainings and supportive supervision,
health workers are taught proper storage of medicines, ways of avoiding drug expiration (e.g.,
quantification of stocks and proper handling of expired drugs). During supportive supervision visits for

74
VHWs, ZAPIM assisted with the identification and return of expired medicines from the VHWs to the
health facilities for supervised destruction by the health care staff.
7. ADMINISTRATIVE ACTIVITIES
7.1 STAFFING AND MANAGEMENT In Year 4, ZAPIM continued to build on the established decentralized management approach and
implemented activities with high quality through careful planning and strong communication. ZAPIM
worked through existing MoHCC provincial and district-level staff and structures to continue building
capacity within the government and ensure that project activities consider local context and respond to
local needs. All levels of the NMCP received this approach with great appreciation and this
strengthened coordination and collaboration in project implementation.
During Year 4, Dr. Noe Rakotondrajaona continued as the project’s Chief of Party, Dr. Anthony
Chisada as Technical Director and Angeline Zengeni as the Finance and Administration Director. The
project recruited three provincial coordinators and two new drivers.
In Year 4, ZAPIM benefitted from several short-term, technical assistance assignments from Abt
Associates, Save the Children and Jhpiego. Details of these visits and remote support are in Annex A.
7.2 CONFERENCES, RETREATS, TRAININGS AND MEETINGS
7.2.1 ANNUAL MALARIA CONFERENCE
The ZAPIM Chief of Party, Technical Director, M&E/OR Manager, Senior CM Specialist, SBCC Specialist
and LLIN Specialist attended the national annual malaria conference hosted by NMCP in Mutare from
June 24 to June 27, 2019. ZAPIM presented on malaria death audits, NMCP branding, Angwa assessment
and month 24 NDS results. The other presentations supported by ZAPIM were the CDCS presented by
Mr. Sanyanga from the DPS and community dialogues presented by the NMCP SBCC focal person. The
major take-away message from the conference was the need to make use of the key findings from these
activities to implement evidence-based programming.
7.2.2 VHW LOGISTICS SYSTEM REDESIGN WORKSHOP
ZAPIM Technical Director and the M&E/OR Manager attended the VHWs logistic system redesign
workshop hosted by Chemonics in Mutare form May 22 to May 24, 2019. This was a consultative
workshop with stakeholders from the NMCP, MOHCC Health Information department, DPS, ZAPIM,
PMI, Chemonics, Mhuri/Imuli, NatPharm, provinces and districts. The workshop also included focus
group discussions with VHWs. The purpose of the workshop was to understand the gaps and challenges
of the current VHW logistic system in preparation for the system’s re-design. ZAPIM presented the key
VHW-related finding from the CDCS for the stakeholders’ consideration in the re-design of the system.
Chemonics engaged a consultant to facilitate the workshop and develop a new design for the system.
The new system, once fully developed, will be piloted in selected districts guided by a protocol which
Chemonics is currently developing. The re-design is expected to deal with the challenges of VHW stock
management, stock outs, reporting and use of data from VHWs among other issues. By end of
September 2019, the consultant had developed draft training manual for system users and supervisors
and system design standard operating procedures. The two documents were circulated to the
stakeholders for stakeholders for review

75
7.2.3 PROVINCIAL HEALTH TEAM MEETINGS AND DATA MANAGEMENT
WORKSHOP
ZAPIM participated in the Provincial Health Team Meetings in Mashonaland Central and Matabeleland
North provinces, and data management workshop in Mashonaland Central. The project was represented
by the Provincial Coordinators and presented project achievements to date, planned upcoming activities
and data quality issues for the provinces. The meetings and workshop were also used as a platform to
review the performance of the malaria program in the provinces. The ZAPIM Provincial Coordinator in
Matabeleland North used this forum to hold discussions with Wild 4 Life, one of the malaria
implementing partners in the province, and agreed on areas for collaboration in Binga District. ZAPIM
shared the supportive supervision tools with Wild 4 Life to ensure same standard in the activities. The
activities for the two projects will be coordinated to avoid overlap in the same geographical areas and
also to ensure that all the wards in the district are covered.
7.2.4 NATIONAL MALARIA VECTOR CONTROL PLANNING AND REVIEW
MEETING, IRS LEVEL I AND II TRAININGS AND IVM STRATEGIC PLAN
DEVELOPMENT WORKSHOP
The ZAPIM LLINs Specialist participated in the planning and review meeting in Masvingo from
September 2 to 6, 2019. The meeting reviewed vector control in the country including LLINs. He also
provided technical support in the development of IVM Strategic Plan and IRS Level I training between
September 9 and September 20, 2019. The Provincial Coordinators in Mashonaland Central and
Mashonaland East participated in the IRS Level II training from September 23 to 27, 2019.
7.2.5 ENVIRONMENTAL COMPLIANCE TRAINING
The LLIN/Vector Control Specialist, Case Management Specialist, and Data Quality and Reporting
Officer attended an Environmental Compliance training hosted by USAID. The training aimed to
familiarize participants with key terms and definitions used in environmental compliance and highlight
USAID’s policies, standards, and procedures. New USAID regulations require that implementing
partners include Climate Risk Management in their proposals and implementation plans and strategies.
Since the training, ZAPIM is now emphasizing the importance of integrating environmental compliance
into all thematic areas.
7.2.6 YEAR 5 WORK PLAN DEVELOPMENT MEETINGS
ZAPIM met with the three provinces to gather their views on the priorities for Year 5. NMCP endorsed
the proposed priorities with minimal changes. The project made it clear to the provinces and NMCP
that the final activities to implement in Year 5 depend on the available budget and PMI approval. The
project presented the consolidated work plan to NMCP before submitting to PMI.
7.2.7 ZAPIM/NMCP MEETINGS
ZAPIM held regular meetings with NMCP leadership to give updates on the implementation of ZAPIM-
supported activities and discuss program achievements and challenges.
7.2.8 FUNDAMENTALS OF SM&E AND EVALUATION METHODS OF MALARIA
PROGRAMS
The ZAPIM Data Quality and Reporting Officer attended a ten-day training session on fundamentals of
SM&E and evaluation methods of malaria programs at the University of Ghana from June 24 to July 05,
2019. The training involved plenary sessions, discussions, group work, and hands-on experience. This

76
training is beneficial to the project particularly in the implementation of evidence-based programming for
elimination work in Lupane District.

77
8. Challenges, Lessons Learned and
Recommendations
The following is a list of challenges that the ZAPIM project faced in Year 4 and some recommendations
for how to mitigate or avoid these challenges in the future.
Some facilities are giving IPTp doses before 13 weeks gestation and before
completing 28 days after last dose as recommended: Mentees were instructed on the
importance of adhering to clinically established guidelines. ZAPIM is currently supporting the
development of IPTp job aids in the form of a calendar.
Shortage of malaria commodities (RDT kits, Dextrose 50%, sulfadoxine-
pyrimethamine, and ACTs): ZAPIM encouraged the District Managers to redistribute
commodities from facilities with low malaria burden to those with high burden and also ensure
that malaria commodities are enough to distribute to VHWs. The provinces were also
requested to assess the magnitude of the problem and document for possible discussion at
higher level meetings (e.g., CM subcommittee, PMI meeting, Provincial Health Team meetings,
etc.). Through the mentorship program, facilities were encouraged to calculate minimum and
maximum stocks and reminded on when to do an emergency order and what they should do
when commodities ordered are not delivered by Zimbabwe Assistance Pull System.
Low index of suspicion with most cases that qualify to be malaria suspects being
missed for malaria RDT: Give emphasis on importance of testing all fever cases during
training, supportive supervision or mentorship so that no suspected cases are missed
Delay treatment seeking behavior: Seeking treatment from traditional healers before
visiting health facilities including traditional practices such as ‘scratching the throat’ in still a
common practice. There is a need to conduct community meetings with traditional healers to
promote early referral of suspected malaria cases for diagnosis and treatment and understanding
of harmful practices and to educate communities on early care seeking behavior and
understanding of harmful practices.
Unavailability of transport for mentorship program: Involve the DHE in planning
mentorship visits and also integrate mentorship visits into other programs. In some instances,
mentees were not on site during mentorship visits. This can be mitigated by involving health
facilities in scheduling mentorship visits. In addition, there is need to train peer mentors at
health facility level in Year 5 to cut on transport challenges
Threshold graphs not distributed at the beginning of the year in some health
facilities: Through the provincial malaria review and death audit meetings, there was a
consensus that the provincial and district offices need to calculate the threshold values and give
them to facilities at the beginning of the malaria season so that facility staff can plot their graphs
on time.
Timing of LLIN mass distribution campaign was after the peak malaria season: Future campaigns should be conducted just before the peak malaria season for impact.
VHW commodities: During the VHW supportive visits, ZAPIM worked with the district to
ensure that VHWs without commodities were supplied with RDT kits, cotton wool, latex
examination gloves, Sharps boxes and malaria medicines. The health centers are encouraged to
continue supplying VHWs with adequate commodities.

78
VHW stock documentation: The documentation of stock in VHW registers is still a
challenge with most not recording the opening and closing stock. ZAPIM emphasized these
issues in the trainings and supportive visits. Health facility staff were encouraged to monitor and
support VHWs more closely on these issues. ZAPIM staff will continue to train VHWs on this
to ensure they are proficient and routinely document stock correctly.
Health facility staff support for VHWs. In 50% of the facilities visited during supportive
supervision visits, staff were not meeting with VHWs when they came to clinics with their
monthly reports. ZAPIM continues to orient facility-based health workers on VHW supervision
and encourages them to create time for this. The DNOs in the affected districts were
encouraged to ensure that clinic staff were effectively supporting VHWs.
NDS mosquito bioassays: National Institute of Health Research (NIHR) did not have enough
mosquito colonies to conduct bioassays for the month 36 NDS. ZAPIM and NIHR arranged for
the bioassays to be done at DeBeers Laboratory in Chiredzi.
Nurse involvement in elimination training. ZAPIM noticed that nurses had limited
involvement in the trainings for enhanced surveillance in Lupane District, while an emphasis was
placed on EHTs. This has resulted in challenges with the implementation of case investigations,
active case finding, and the adequate supply of commodities to EHTs. ZAPIM discussed the
issues with the province and district staff and agreed to involve nurses in future trainings and
foster better elimination work collaboration between the two professionals.
EHT clinical skills. EHTs experience challenges in doing newly-required clinical work in the
community for which they are untrained, such as preparing blood slides for microscopy
examination for malaria parasites. ZAPIM-supported trainings emphasized skill development with
thorough RDT simulations and practical sessions to help participants carry out these activities.
Limited access of entomology equipment to EHTs: Entomology equipment was mainly
kept at district level yet the EHTs need to use them on a daily basis. This included even simple
items like magnifying glasses. The DEHO was encouraged to decentralize the entomology
equipment to ensure that the EHTs are able to carry out the entomology work.
Operating Environment: The volatile and complex operating environment as described in
the background section of this annual report, coupled with the delayed release of Year 4 funding
and anticipated delay of funding for Year 5 meant some planned activities were either delayed or
could not be implemented in Year 4.
SBCC subcommittee meeting scheduling and funding: Convening of subcommittee
meetings was are highly dependent on the NMCP programming year. While ZAPIM planned and
was ready to support the NMCP on the technical meetings that guide SBCC programming
nationally, mutual prioritization was not possible. In future ZAPIM should place the onus of
convening these meetings on NMCP and depend on GFTAM funding to support the meetings.
Fuel access in the field. Lupane District experiences challenges obtaining petrol for EHTs to
carry out community activities for elimination and servicing of motorbikes. The district was
encouraged to continue lobbying for these through the MoHCC structures, which are primarily
responsible for fuel access. ZAPIM will assist in some cases if the fuel is used for specified, well-
defined malaria elimination actives and with proper accountability. The challenges with
supporting this are in ensuring that the support is used for malaria activities and that issued
coupons can be redeemed into liquid fuel in the field.
ZAPIM has experienced challenges exchanging coupons for liquid fuel in the field due to limited outlets
fuel outlets. The project has resorted to using jerry cans to carry extra fuel for field work, which has
resulted in limited reach in some communities. The project acquired more jerry cans in Year 4 and
acquired some coupons from a second supply (Petrotrade) in addition to the usual supplier (Redan).

79
ANNEX A: SHORT-TERM TECHNICAL
ASSISTANCE
Project staff provided the following short-term technical assistance (STTA) during Year 4:
Name Position Dates Scope of Work
Ekpenyong Ekanem ZAPIM M&E Specialist,
Abt Associates
April 1-13, 2019 and
May 2-4, 2019
Provide technical
assistance in NDS at
month 36 data analysis
and development of
SM&E Training Manual
Jeanne Koepsell Save the Children CCM
Advisor, Digital Health
and Innovation Lead
May 20-22, 2019 Provide technical
support to CCM
activities
Chantelle Allen Jhpiego Quality
Improvement Advisor
June 09-15,2019 Provide technical
support for case
management (malaria
clinical mentorship and
Y5 work plan
development) and
development of EPR
training package
Ffyona Patel ZAPIM Technical
Program Officer, Abt
Associates
July 7 – 12, 2019 Provide technical
support to the project
including Year 5
workplan development.
Kinsen Talukder ZAPIM Project Finance
Analyst, Abt Associates
July 21 – 26, 2019 Provide finance and
administrative support
including Year 5 budget
formulation


81
ANNEX B: PMP INDICATOR/YEAR 4 MILESTONE
MATRIX
# Indicator/ Milestone
Type Targets/ Benchmarks
Results Comments/ Problems
Encountered
Next Steps
Baseline (year and source)
Oct 2018 – Sept 2019
YR 4 Results
Year 4 Cumulative
Results
Percent of Annual Target
Achieved
CM Number of malaria deaths
PMP 392 (HMIS 2016)
N/A 353 353 Not applicable (N/A)
The baseline and results are national. Cumulative deaths from ZAPIM Districts/Provinces were reported from Matabeleland North (5)- Lupane (1) and Binga (4), Mashonaland Central (39)- Centenary (4), Guruve (8), Mazowe (1) , Mbire (6), Mt darwin (9), Rushinga (4) and Shamva (7), Mashonaland East (54)- Goromonzi (1), Marondera (4), Hwedza (2) , Mudzi (26), Murewa (8), Mutoko (8) and UMP (5)
Scale up malaria interventions and also continue to support malaria death investigations in the affected provinces.

82
CM Incidence of malaria
PMP 17/1,000 (HMIS 2016)
N/A 21/1,000 N/A ZAPIM supported provinces, Mashonaland Central and Mashonaland East were amongst the three provinces that reported high number of cases. The most affected ZAPIM supported districts were Mudzi, Goromonzi, Mt Darwin, Mbire, Bindura, Centenary, and Mutoko. These districts were suspected to be experiencing malaria outbreaks.
ZAPIM continues to priotize high-impact interventions to contribute to the reduction of malaria districts experiencing malaria outbreaks.
CM Proportion of women who received two or more doses of Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) during ANC
PMP 35% (MIS
2012)
N/A 37% 37% N/A The figure of 37% is according to the 2016 MIS.
MCHIP carried out an assessment in Manicaland to determine the causes for the low uptake of IPTp. ZAPIM continued to rely on assessment findings and recommendations to improve the program
CM Proportion of under-five children who sought treatment within 24 hours of onset of fever
PMP 68.8% (MIS
2012)
N/A 50% 50% N/A 50% is according to the 2015 ZDHS. The new National Malaria Strategic Plan is being costed and will inform the targets.
The indicator is not well reported in the 2016 MIS preliminary report and therefore the 2015 ZDHS report has been used as a reliable source document.
CM Percentage of suspected malaria cases that receive a parasitological test
PMP 99.8% (HMIS 2016)
100% 100% 100% 100% Need to encourage communities that any suspected malaria case should be tested.
The HFs and community health workers (CBHWs) should continue to exhibit high compliance and acceptable practices.

83
CBHWs are adhering to the guidelines.
CM Percentage of confirmed malaria cases that receive first-line antimalarial treatment according to national policy
PMP 93% (HMIS 2016)
100% 100% 100% 100% The indicator only captures ACTs given; other anti malarial medicine given to complicated cases are not documented in the DHIS2 system.
The results show that the level of access to treatment of deserving cases for first-line treatment increased in quarter.
CM+CCM Number of health workers (including VHWs) trained in malaria case management (ACT, MiP/IPTp, RDT, microscopy, medicine management)
PMP 896 (Year 1 ZAPIM Annual Report)
760 538 538 71% 183 health facility workers, 317 VHWs and 38 VHW peer supervisors were trained CM. The target was not achieved due to inadequate funding.
Additional health workers will be trained in Year 5.
CM Number of planned malaria-related SS of health facility workers conducted
PMP 0 (2016) 15 9 9 60% Prioritized mentorship program during the year.
To be integrated into mentorship program in Year 5.
CM Number of districts with outbreak response plans
PMP 0 (2016) 15 15 15 100% All districts plans feed into the provincial plans.
As part of the outbreak response initiative, ZAPIM will continue to support all districts to ensure they have robust plans to quickly respond to any outbreaks. ZAPIM supported the production of the EPR guidelines. In Year 5, ZAPIM will support training of RRT members in selected districts. It is anticipated that this will go a improve the

84
quality of the outbreak response plans.
CM Functional training database (TrainSMART) for current and future trainings
Year 4 mileston
e
0 (2016) 1 1 1 100% Database was maintained throughout the year.
Database to be maintained beyond the life span of the project.
CM NMCP CM/MiP subcommittee quarterly meetings supported
Year 4 mileston
e
1 (2016) 2 0 0 0% Rescheduled for Q1- Year 5.
ZAPIM will continue to engage NMCP so that subcommittee meetings are held as planned.
CM Malaria case and drug consumption assessment findings disseminated
Year 4 mileston
e
0 (2016) 1 1 1 100% Report was finalized and key results disseminated at different forums.
Need to follow up on the implementation of the recommendations.
CM Number of staff trained in CM/MIP reached with SMS information reminders and quizzes
Year 4 mileston
e
0 (2016) 200 0 0 0% Deferred to Year 5 because of inadequate funds.
To be implemented in Year 5.
CM Supportive supervision tools and job aids reviewed and updated with NCMP
Year 4 mileston
e
0 (2016) 500 500 500 100% ZAPIM did not support the printing of revised treatment charts because of inadequate funds.
ZAPIM will support review of any relevant tools in Year 5 as per recommendations from SS and mentorship program.
CM Number of on the job mentorship visits to six districts conducted
Year 4 mileston
e
0 (2016) 3 6 6 200% 25 health facilities were visited, with a total of 98 health workers mentored.
Need to continue updating action plans based on discussions and proposed actions to be taken.
CM Number of mentorship review meetings conducted
Year 4 mileston
e
0 (2016) 2 1 1 50% The review meeting focused on the approach that was used and highlighted areas where mentees
Need to follow up on the recommendations of the meeting.

85
and mentors need additional training or skills building
CM External mentorship assessment conducted
Year 4 mileston
e
0 (2016) 1 0 0 0% This will be guided by the recommendations from the mentorship review meeting.
To be guided by the recommendations from the mentorship review meeting.
CM Number of malaria death investigation/ malaria death audit meetings with NMCP, hospitals and PMDs, DMOs, and Matrons in attendance
Year 4 mileston
e
2 (2016) 6 3 3 50% One meeting was conducted in each province. The target was not achieved due to inadequate funding.
Need to follow up on the recommendations of the meeting. More death audit meetings to be conducted in Year 5.
CCM Number of facility- based health workers oriented on supportive supervision process and tools
Year 4 mileston
e
0 (2016) 25 18 18 72% The orientation targeted selected health workers from health facilities in UMP District.
These will act as focal persons for VHW supervision at their respective centers.
CCM Number of VHWs and potential VHW peer supervisors followed up (post-training follow-up)
Year 4 mileston
e
0 (2016) 280 203 203 73% Follow up VHWs in four districts, Centenary, Goromonzi, Mudzi and UMP. Other VHWs could not be followed up in the last quarter of the year because of inadequate funds.
Additional VHWs will be followed up in Year 5.
CCM Number of meetings with School Health Coordinators conducted as part of post-training follow-up
Year 4 mileston
e
0 (2016) 3 0 0 0% Deferred to Year 5 because of inadequate funds.
To be implemented in Year 5.

86
CCM Number of training manuals and job aids (facilitators and participant manuals, medicine supply and accountability register, RDT job aid and monthly reporting book) printed
Year 4 mileston
e
0 (2016) 370 1,440 1,440 389% Copies printed in Q2 were sufficient to cover the trained cadres in Q3.
Additional copies will be printed as per need in Year 5.
CCM Number of bi-annual district VHW review meetings conducted (eight districts)
Year 4 mileston
e
0 (2016) 16 3 3 19% Conducted in three districts only, Centenary, Mbire and Mutoko. Implementation affected because of the other competing activities and inadequate funds.
Additional meetings will be conducted in Year 5.
CCM Number of items procured for the VHWs (medicine boxes & torches)
Year 4 mileston
e
0 (2016) 200 200 200 100% 200 medicine boxes were procured for all VHWs in Mbire District. Three cabinets were lost within the district during transportation at the time of distribution.
Need to monitor the use of medicine boxes.
CCM Number of EHTs and nurses supported to conduct VHW supportive supervision including LLIN CD
Year 4 mileston
e
0 (2016) 60 10 10 17% Piloted in Mbire, Mutoko and UMP were selected motorized EHTs provided SS to VHWs.
To be scaled up in Year 5.
CCM Number of coordination meeting with other Malaria Partners on CCM
Year 4 mileston
e
0 (2016) 1 1 1 100% Met with Wild 4 Life and Isdell Flowers to discuss how community activities can be coordinated
Need to follow up on areas to share or leverage resources

87
LLIN Proportion of population that slept under an insecticide treated net the previous night
PMP 49% (MIS
2012)
N/A 54% 54% N/A The figure of 54% is according to the MIS 2016.
Need to assess the performance of the indicator through ZDHS/MIS that is scheduled for 2020
LLIN Proportion of children under-five who slept under an LLIN the previous night
PMP 8% (ZDHS
2010-11) 49.6%
(MIS 2012)
N/A 17.5% (ZDHS 2015)
33% (MIS
2016)
17.5% (ZDHS 2015)
33% (MIS
2016)
N/A It is important to note the different methologies used for MIS and ZDHS.
Need to assess the performance of the indicator through ZDHS/MIS that is scheduled for 2020. However, there is need to scale up the interventions which promote net usage among children.
LLIN Proportion of women of child bearing age who slept under an LLIN the previous night
PMP 49.1% (MIS
2012)
N/A 36% (MIS
2016)
36% (MIS 2016)
N/A Only 36% of women slept under an LLIN the previous night, which was a substantial decrease compared to the 49% in the 2012 MIS.
Need to assess the performance of the indicator through ZDHS/MIS that is scheduled for 2020. However, there is need to scale up the interventions which promote net usage among women aged 15-49 years.
LLIN Proportion of households in ZAPIM target districts with one or more LLINs
PMP 46.4% (MIS
2012)
N/A 58% (MIS
2016)
58% (MIS 2016)
N/A The baseline and results are national.
Need to assess the performance of the indicator through ZDHS/MIS that is scheduled for 2020.
LLIN LLIN Continuous distribution system rolled out in ZAPIM target districts
PMP 10 (Year 1 ZAPIM
Annual Report)
11 11 11 100% This was complimented by the mass distribution program
To be done throughout the year
LLIN Net durability study findings produced and recommendations adopted for future
PMP 0 (2016) 1 1 1 100% The project the study and submitted the final report to PMI for approval.
The recommendations will be adopted for future distribution planning.

88
distribution planning
LLIN Number of trainers trained on continuous LLIN distribution
PMP 0 (2016) 120 29 29 24% The target was not achieved due to inadequate funding.
To be trained in Year 5 when funds are available
LLIN Number of people (LLIN Distributors) trained in LLIN routine/continuous distribution
PMP 1,358 (2016)
1020 100 100 10% The target was not achieved due to inadequate funding.
To be trained in Year when funds are available
LLIN Number of trainers trained on Mass LLIN distribution
Year 4 mileston
e
0 (2016) 330 348 348 105% The target was surpassed at no extra cost.
Ensure that the trainers provide effective training.
LLIN Number of people (LLIN Distributors) trained in LLIN mass distribution
Year 4 mileston
e
0 (2016) 870 1,632 1,632 188% HFs engaged all the VHWs in their area of operation instead of working with the targeted 6 VHWs only. This was done at no extra cost to the project
Ensure that the VHWs distribute the LLINs in an efficient manner.
LLIN Number of LLINs distributed (mass + CD)
PMP 573,950 (2016)
816,225 725,569 725,569 89% A total of 725,569 LLINs were distributed. Of these, 624,458 were distributed through mass campaign and 101,111 through continuous channels
Distribution will continue as per need
LLIN Number of ANC clinics implementing LLIN routine distribution
PMP 0 (2016) 98 98 98 100% All ANC clinics continue to implement LLIN routine distribution.
All ANC clinics will continue to implement LLIN routine distribution.
LLIN Number of vector control subcommittee
Year 4 mileston
e
1 (2016) 2 0 0 0% Rescheduled for Q1- Year 5.
ZAPIM will continue to engage NMCP so that subcommittee meetings are held as planned.

89
meetings supported
SBCC SBCC repository (on-line data base) of malaria messages and delivery methods established
PMP 0 (2016) 1 0 0 0% This falls under the portfolio of the mainstream MoHCC.
ZAPIM will no longer support the activity.
SBCC Number of persons trained in SBCC
PMP 1066 (2016)
803 554 554 69% The trainings focused on CAC Explore health issues and setting priorities as well as CAC Evaluate Together.
Additional trainings will be conducted in Year 5.
SBCC Rapid assessment- Knowledge, Attitude and Practice Surveys of the Mbire community completed
PMP 0 (2016) 1 1 1 100% The project worked with NMCP to review and refine the report.
The report is expected to inform future programing as per findings from the assessment. Some of the findings were also used during the development of Year 5 work plan.
SBCC Commemoration of the SADC Community Malaria Day supported
Year 4 mileston
e
1 (2016) 1 1 1 100% Press conference was held together with the Minister of Health and Child Care
ZAPIM will continue to support future commemorations.
SBCC World Malaria Day Campaign supported in 3 provinces
Year 4 mileston
e
3 (2016) 3 3 3 100% World Malaria Day commemorations were supported at national level and in three ZAPIM supported provinces.
ZAPIM will continue to support future commemorations.
SBCC SBCC materials and tools in local languages (including leaflets & posters) for
Year 4 mileston
e
0 (2016) 3 3 3 100% Project printed LLIN promotional leaflet, My net, My life. Support was also rendered towards the
ZAPIM will continue to support material production for different thematic areas.
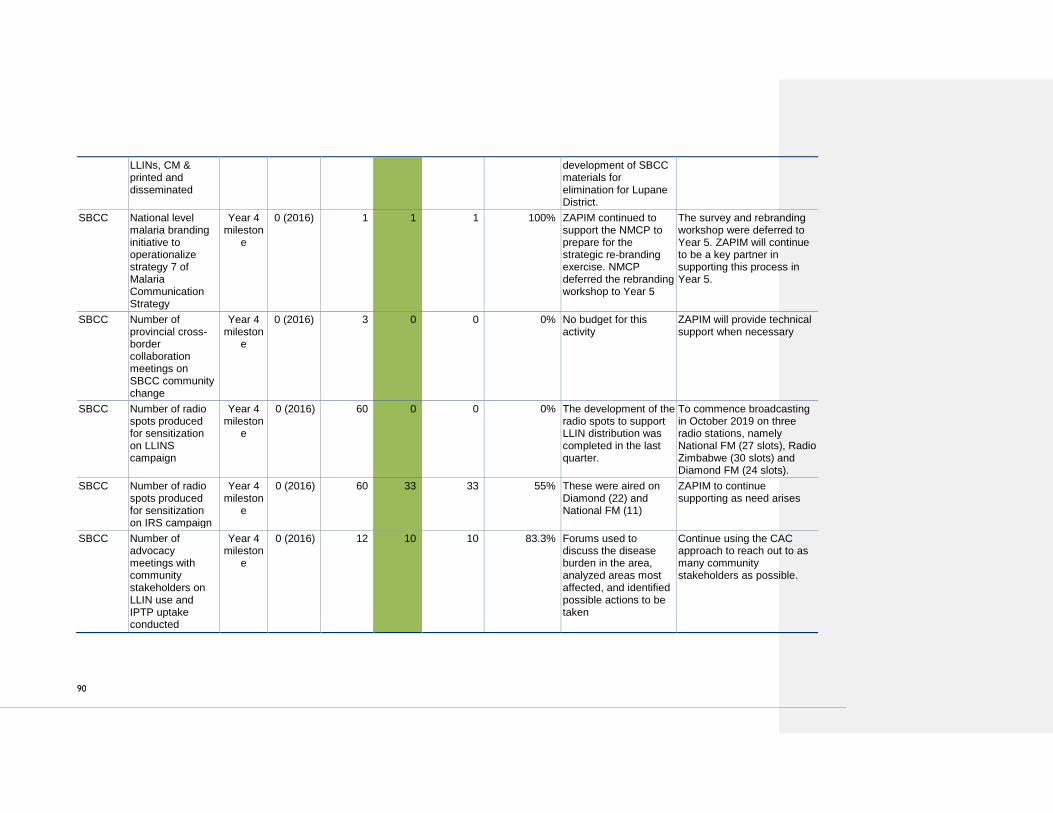
90
LLINs, CM & printed and disseminated
development of SBCC materials for elimination for Lupane District.
SBCC National level malaria branding initiative to operationalize strategy 7 of Malaria Communication Strategy
Year 4 mileston
e
0 (2016) 1 1 1 100% ZAPIM continued to support the NMCP to prepare for the strategic re-branding exercise. NMCP deferred the rebranding workshop to Year 5
The survey and rebranding workshop were deferred to Year 5. ZAPIM will continue to be a key partner in supporting this process in Year 5.
SBCC Number of provincial cross-border collaboration meetings on SBCC community change
Year 4 mileston
e
0 (2016) 3 0 0 0% No budget for this activity
ZAPIM will provide technical support when necessary
SBCC Number of radio spots produced for sensitization on LLINS campaign
Year 4 mileston
e
0 (2016) 60 0 0 0% The development of the radio spots to support LLIN distribution was completed in the last quarter.
To commence broadcasting in October 2019 on three radio stations, namely National FM (27 slots), Radio Zimbabwe (30 slots) and Diamond FM (24 slots).
SBCC Number of radio spots produced for sensitization on IRS campaign
Year 4 mileston
e
0 (2016) 60 33 33 55% These were aired on Diamond (22) and National FM (11)
ZAPIM to continue supporting as need arises
SBCC Number of advocacy meetings with community stakeholders on LLIN use and IPTP uptake conducted
Year 4 mileston
e
0 (2016) 12 10 10 83.3% Forums used to discuss the disease burden in the area, analyzed areas most affected, and identified possible actions to be taken
Continue using the CAC approach to reach out to as many community stakeholders as possible.

91
SBCC Number of SBCC Sub-Committee meetings conducted
Year 4 mileston
e
1 (2016) 2 0 0 0% Rescheduled for Q1- Year 5.
ZAPIM will continue to engage NMCP so that subcommittee meetings are held as planned.
Elimination
Number of health workers trained in enhanced surveillance
Year 4 mileston
e
0 (2016) 25 24 24 96% The participants were drawn from Lupane District where ZAPIM is supporting elimination work
Training will enhance the capacity of health workers to effectively carry out malaria elimination activities in the district
Elimination
Number of environmental health workers trained in entomology
Year 4 mileston
e
0 (2016) 25 25 25 100% The training gave cadres the theoretical and practical skills they need for active vector surveillance of breeding sites and adult vectors within their communities
The skills will be essential for routine vector surveillance for elimination and response to malaria cases
Elimination
Number of environmental health workers trained in GIS
Year 4 mileston
e
0 (2016) 25 25 25 100% The project supported the training of 25 EHTs from Lupane District on GIS mapping for quality mapping of malaria cases, vectors, vector breeding sites, and malaria transmission foci.
Trained health workers are expected to map malaria cases, vectors, vector breeding sites, and malaria transmission foci
Elimination
Number of health workers trained in foci response
Year 4 mileston
e
0 (2016) 25 25 25 100% The training equipped health workers with the knowledge and skills needed to proactively and reactively respond to potential and existing malaria transmission foci—in accordance with the national guidelines for malaria elimination
Trained health workers are expected to proactively and reactively respond to potential and existing malaria transmission foci.

92
M&E Malaria M&E training manual revised
Year 4 mileston
e
0 (2016) 1 1 1 0% The project supported a workshop which kick started the process of developing the malaria SM&E training manual
To finalize the facilitator’s training manual and participants’ manual in Year 5.
M&E Number of districts and health facility staff trained in M&E, supportive supervision, epidemic alert protocols (EPR/IDSR)
PMP 10 (2016) 90 0 0 0% The trainings will be guided by the M&E training manual to be finalized in Year 5
To be implemented as soon as the M&E training manual is updated
M&E ZAPIM M&E database updated
Year 4 mileston
e
0 (2016) 1 1 1 100% The M&E Database was updated on a regular basis.
M&E Database will continue to be updated throughout the projecet lifespan and to be used to monitor the performance of the project.
M&E Number of national, provincial and district data quality assessments (DQAs) conducted
Year 4 mileston
e
0 (2016) 6 3 3 50% A total of 32 health facilities: Binga (4), Hwange (6), Rushinga (6), Mt Darwin (6) and Mudzi (10) participated in the DQAs. The target was not achieved due to inadequate funding.
Additional districts and health facilities to be covered in Year 5
M&E Number of provincial and district planning and review meetings conducted
Year 4 mileston
e
0 (2016) 6 3 3 50% The project all the provinces to undertake malaria review meetings. The target was not achieved due to inadequate funding.
The project will support additional malaria review meetings in Year 5.
M&E M&E Plan for the National Malaria Strategy printed and distributed
Year 4 mileston
e
0 (2016) 500 500 500 100% The project supported the printing and distribution of the SM&E Plan
The project will continue using different platforms at provincial and district level to disseminate key document.

93
M&E Revised EPR guidelines printed and distributed
Year 4 mileston
e
0 (2016) 1,600 1,600 1,600 100% NMCP requested ZAPIM to revise the number of copies to be printed
These were distributed to partners and provinces at the Annual Malaria Conference. The guidelines will guide the training of RRTs.
M&E Number of district staff trained in the revised EPR guidelines
Year 4 mileston
e
0 (2016) 80 0 0 0% Deferred to Year 5 because of inadequate funds.
To be implemented in Year 5.
M&E Malaria Research Agenda developed and printed
Year 4 mileston
e
0 (2016) 1 0 0 0% Discussions with NMCP to develop the agenda underway
To be implemented in Year 5.
M&E Number of RDT registers for VHWs printed
Year 4 mileston
e
0 (2016) 1,000 1,160 1,160 116% Printed as per provinces’ request
Distributed to all provinces as per need.
M&E Number of cellphones procured to pilot weekly mobile data reporting by VHWs
Year 4 mileston
e
0 (2016) 200 200 200 100% Agree with NMCP and national health information department on parameters to be reported.
VHWs started reporting to their respective health facilities from mid-August 2019.
M&E Number of VHWs trained in weekly mobile data reporting (through SMS)
Year 4 mileston
e
0 (2016) 186 186 186 100% All active VHWs were trained to report to the health facility on a weekly basis.
VHWs started reporting to their respective health facilities from mid-August 2019. Non-active VHWs are likely to be targed for CCM training in Year 5. This will be followed by training in weekly mobile data reporting. Health facility staff prepared to lobby with HCCs to take over the initiative after the ZAPIM Project
M&E Alternative to MIS developed and explored
Year 4 mileston
e
0 (2016) 1 1 1 100% Five options were identified and a short description of the approach for each
The brief is intended to be the starting basis for further discussions with the NMCP, PMI and other partners to

94
option and the advantages, disadvantages/limitations, and likely cost were articulated
decide on which option(s) to pursue. Once the internal partners have made a choice on a method(s) to pursue further, ZAPIM will develop a detailed proposal in Year 5.
M&E Number of Surveillance, M&E and OR Sub-Committee meetings supported
Year 4 mileston
e
0 (2016) 2 0 0 0% Rescheduled for Q1- Year 5.
ZAPIM will continue to engage NMCP so that subcommittee meetings are held as planned.

95
ANNEX C: YEAR 4 ACTIVITIES
AFFECTED BY ANTICIPATED DELAYED
RELEASE OF YEAR 5 FUNDING
THEMATIC
AREA
AFFECTED ACTIVITY COMMENTS
CM EPR training
Supportive supervision
CM subcommittee meeting support
Death audit meetings
ZAPIM intended to carry out training of 80
RRT members in October
Matabeleland North requested support for SS
but project could not provide
NMCP planning to have this meeting in
October. ZAPIM will not be able co-fund this
activity with other partners
Managed one death audit meeting for each
province instead of the planned 2 per province
CCM CCM training of VHWs
CCM post training follow up for Binga
Supportive supervision
VHW review meetings
Mbire trainings x 2 groups postponed
Follow up was affected by changes in monetary
policies. Then subsequently budget issues
Only one visit conducted for Binga and Hwange
districts instead of 2 visits to each of the 11
CCM supported districts
Only 3 meetings held one per each district
instead of the planned 16 (2 per district in 8
districts)
LLINs Training of HWs and VHWs on CD of
LLINs
Net follow ups after Mass Distribution
Community Leaders’ engagement
meetings for LLINs uptake
District supportive visits
91 HWs and 920 VHWs could not be trained
No follow up was done
None carried out
None carried out

96
SBCC Re-print malaria BCC communication
facilitation tools for health personnel
and CBHWs in 1 district
Re-print copies of My net my life (20
000)
Development of 1 Ndebele language
leaflet on net use (translation of My
net my life)
Conduct a follow-on rapid assessment
of Dipa la Malaria and replenishment
of gadgets in Chapoto ward
Fully develop malaria elimination
material (partly – illustrator
procurement deferred)
VHW Flipchart in Shona Language could not be
printed
All the activities will be implemented in Year 5
Community
SBCC CAC Evaluate Together trainings for
Mt Darwin (9 HCCs)and Shamva (13
HCCs)
Lupane CAC Elimination support
trainings
Support Advocacy community
dialogue meetings with leaders to
promote LLINs utilization and uptake
of IPTp.
Support post Angwa assessment
dissemination of findings and roll out of
short term interventions.
Documentation of CAC activities
All the activities will be implemented in Year 5
Elimination Supportive supervision for Lupane
district
Elimination review meeting
The supportive supervision could not happen in
July as plan. It could not be done in September
either.
The elimination review was scheduled for
September and could not happen as the project
could not carry out field activities in
September.
M&E/OR One last round of DQAs in each
province
One provincial malaria review meeting
per province
Support training of RRTs in revised
EPR guidelines-
Support SM&E Sub-Committee
Meeting
Support printing and distribution of
T12/ OPD Registers- MoHCC NHIS
department yet to finalize them though
All the activities are now earmarked for Year 5
Commented [EM3]: Are all other activities postponed to Year 5?