xvi international aids conference toronto hiv epidemiology update based on plenary presentation c...
TRANSCRIPT







XVI International AIDS Conference
Toronto HIV Epidemiology Update
based on Plenary PresentationChris Beyrer MD, MPH
Johns Hopkins Bloomberg School of Public Health

Global HIV epidemic, 1990‒2005
Number of people living with HIV
% HIV prevalence, adult (15-49)
% HIV prevalence, adult (15‒49)
Number of peopleliving with HIV (millions)
0
10
20
30
40
50
1990 1995 2000 2005
0.0
1.0
2.0
3.0
4.0
5.0
Source: UNAIDS 2006
Bar indicates the range around the estimate
• 38.6 million living with HIV [33 to 46 million]
• 24.5 million in SS Africa
[21.6 to 27.4 million]
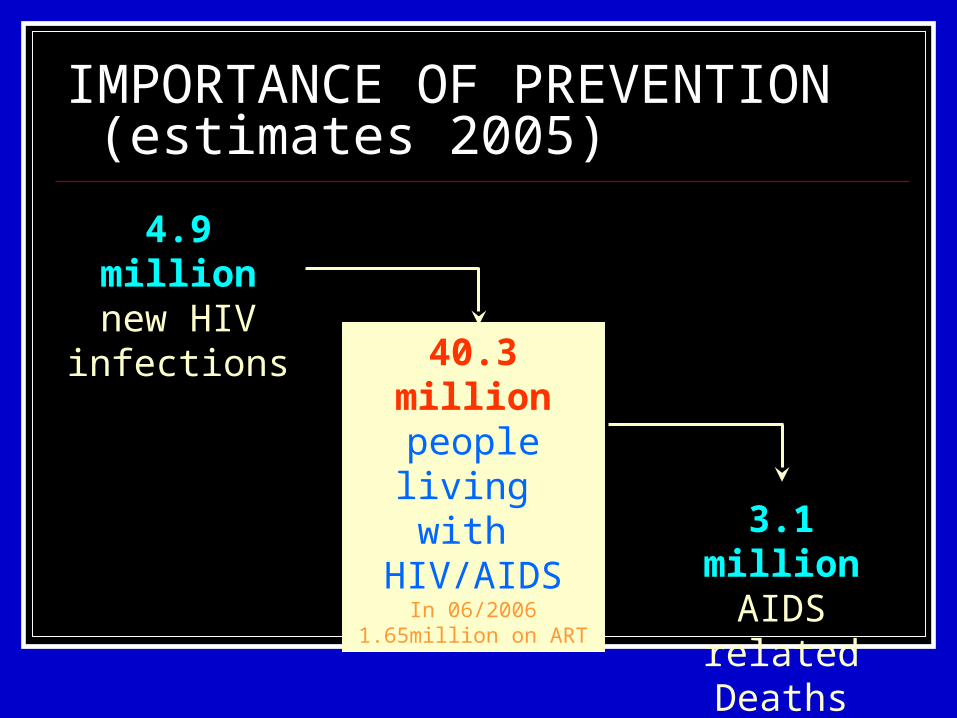
IMPORTANCE OF PREVENTION (estimates 2005)
40.3 millionpeople living
with HIV/AIDS
In 06/2006 1.65million on ART
3.1 millionAIDS related
Deaths
4.9 millionnew HIV infections

Prevalence main determinant of incidence
40 millionPeople living
with HIV/AIDS
3.1 millionAIDS related
deaths
4.9 millionNew HIV infections

A global view of HIV infection, 2005
Source: UNAIDS 2006 Report on the Global AIDS Pandemic
1.5 million200,000 in ‘05IDU
7.6 million830,000 in ‘05HeterosexualMSMIDU
12.1 million1.3 million in ‘05
Heterosexual

States with at least one site with HIV prevalence > 20% in IDU in 2006
• Belarus• Estonia • Kazakhstan• Russia • Ukraine• Serbia & Montenegro
• Iran
• Nepal• Indonesia
• Libya• Mauritius
• Kenya, Tanzania, Ghana, Nigeria**
• Burma• China• India
• Malaysia• Thailand• Vietnam
• Italy• Netherlands• Portugal• Spain
• Argentina• Brazil• Uruguay
• Canada• Puerto Rico• USA
**African States with at least one published report of IDU risks
Emergent Epidemics
Adapted from : Aceijas, et al, AIDS 2004 18:2295-2302
Established Epidemics

Individual Level Determinants for Parenteral HIV Infection
Needle sharing
Higher frequency of injection
Cocaine injection
Lack of opioid analogue therapy
MSM-IDU history
Injection use while incarcerated

Reported HIV cases in the Russian Federation and Ukraine, 1987–2005
1987 1989 1991 1993 1995 1997 1999 2001 2003 2005
0
50 000
100 000
150 000
200 000
250 000
300 000
350 000
400 000
30 000
45 000
60 000
75 000
90 000
105 000
120 000
15 000
0
Reported HIV cases
in the Russian FederationReported HIV cases
in Ukraine
Russian Federation
Newly reported cases
Cumulative (previous years)
Ukraine
Newly reported cases
Cumulative
Adapted from : Russian Federal AIDS Centre; Ukranian AIDS Centre and Ministry of Health of Ukraine, UNAIDS 2006 Report on the Global AIDS Pandemic

What are the Structural Drivers of Spread Across Eurasia?
Driver # 1Geographic proximity to overland drug trafficking routes
Driver # 2Limited use of HIV prevention measures with demonstrated efficacy for IDU transmission
Driver # 3Punitive and legalistic approaches to IDUs

Opiate seizures in Asia in 2004
Source : UNODC World Drug Report 2006
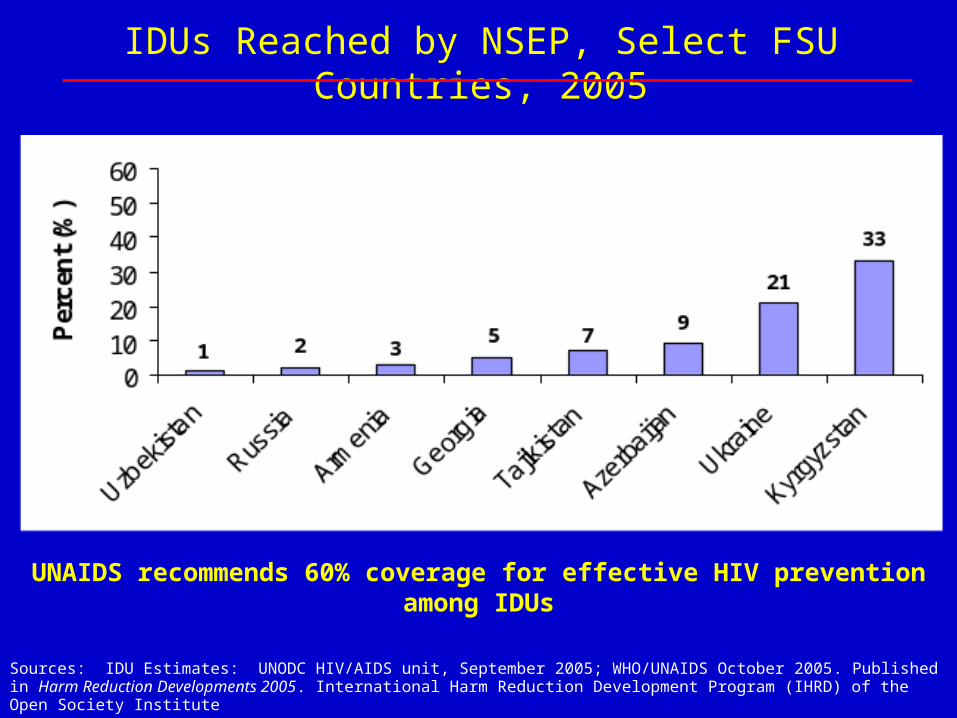
Sources: IDU Estimates: UNODC HIV/AIDS unit, September 2005; WHO/UNAIDS October 2005. Published in Harm Reduction Developments 2005. International Harm Reduction Development Program (IHRD) of the Open Society Institute
UNAIDS recommends 60% coverage for effective HIV prevention among IDUs
IDUs Reached by NSEP, Select FSU Countries, 2005
Structural limits on prevention & care for IDU
• US continues ban on federal funding for Needle Syringe Exchange Programs (NSEP) in US and globally
• Methadone Maintenance Therapy (MMT) remains illegal in many countries Ex: Russian Federation
• Across 50 developing countries, 34,000 IDU on ARV: 30,000 were in Brazil
Source: Aceijas, et al, Addiction, 2006

Photo: Hans Jürgen Burkard

MSM Trends in High and Low Income Country Settings

Estimated Number of HIV/AIDS Diagnoses, by Transmission Category — 33 States, 2001–2004.
* Statistically significant
Source: Espinoza, CDC, 2005
−9.1*
2.7
−3.9*
% Δ / year
−3.4* 0
5000
10000
15000
20000
2001 2002 2003 2004
Year of Diagnosis
HIV
/ A
IDS
MSM
IDU
MSM/IDU
HC

Trends HIV among MSMmid ’90- now
HAART introduced, resulting in dramatic improvement of survival of AIDS patients, as well as reduction in AIDS cases
HIV/AIDS becomes a “chronic disease” and “less visible”
Rise in “unsafe sex” and STI , including outbreaks of Syphylis and LGV

Sexual orientation of male syphilis cases registered in the sentinel
network of clinicians, Belgium, Oct 2000 - Jan 2003
0
5
10
15
20
25
Oct 2000-Jan 2001 Oct 2001-Jan 2002 Oct 2002-Jan 2003
Period of registration
Number of active syphilis cases
MSM
Het.men
From: IPH, Belgium

Possible explanations for increased risk behaviour
HAART changed the face of the epidemic: less AIDS and less deaths
Prevention fatigue: challenge of maintaining safe sex for an extended period
Changing environment : internet as new way of recruiting partners
Young MSM (<20y) sexually active earlier , and never exposed to AIDS as a killer disease
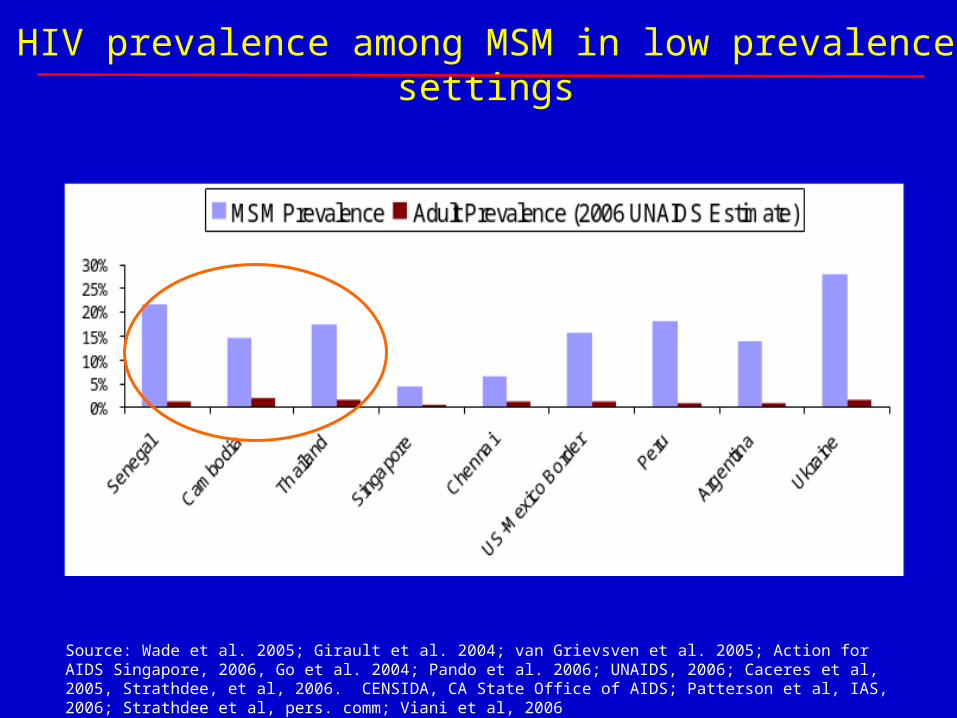
Source: Wade et al. 2005; Girault et al. 2004; van Grievsven et al. 2005; Action for AIDS Singapore, 2006, Go et al. 2004; Pando et al. 2006; UNAIDS, 2006; Caceres et al, 2005, Strathdee, et al, 2006. CENSIDA, CA State Office of AIDS; Patterson et al, IAS, 2006; Strathdee et al, pers. comm; Viani et al, 2006
HIV prevalence among MSM in low prevalence settings
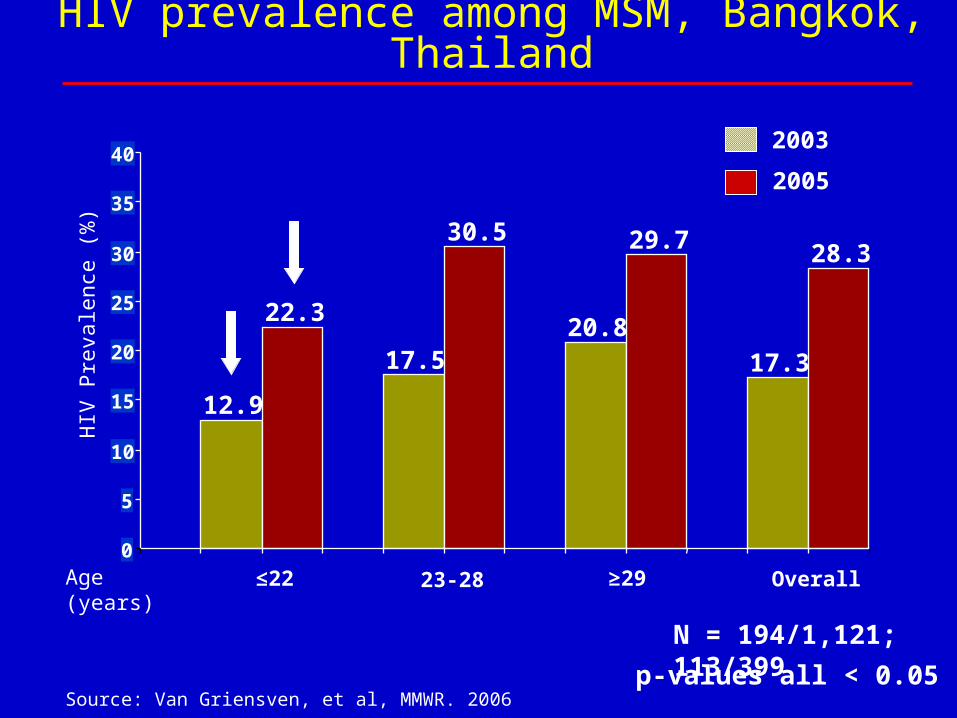
HIV prevalence among MSM, Bangkok, Thailand
Age (years)
2003
2005
≤22 23-28 ≥29
N = 194/1,121; 113/399
Overall
Source: Van Griensven, et al, MMWR. 2006
12.9
22.3
17.5
30.5
20.8
29.7
17.3
28.3
0
5
10
15
20
25
30
35
40
HIV
Pre
vale
nce
(%)
p-values all < 0.05

MSM structural risk contexts
• Criminalization and stigma limit MSM access to HIV prevention, treatment and care
• MSM understudied in emerging contexts: MSM not included in national HIV surveillance in Thailand, Vietnam, Senegal
• Only one African study (Wade, et al) of MSM risk and HIV rates
• Fewer than 1 in 10 MSM worldwide have access to necessary prevention services
Sources: UNAIDS; USAID, 2004; Wade 2005; Go 2006 personal communication; HRW; UNAIDS 2006

HIV prevalence in adults in Africa
Source : UNAIDS, 2006

Region Country
Population-based survey
prevalence (%) (year)
Adjusted 2003 HIV
prevalence (%) in current
report
2005 HIV prevalence (%)
in current report
Trend in prevalence
SOUTH
Botswana 25.2 (2004) 24.0 24.1 Stable
Lesotho 23.5 (2004) 23.7 23.2 Stable
South Africa 16.2 (2005) 18.6 18.8 Increasing
EAST
Burundi 3.6 (2002) 3.3 3.3 Decline in capital city
Rwanda 3.0 (2005) 3.8 3.1 Decline in urban areas
Tanzania 7.0 (2004) 6.6 6.5 Stable
Uganda 7.1 (2004-5) 6.8 6.7 Stable
WEST
Burkina Faso 1.8 (2003) 2.1 2.0 Decline in urban areas
Cameroon 5.5 (2004) 5.5 5.4 Stable
Ghana 2.2 (2003) 2.3 2.3 Stable
Guinea 1.5 (2005) 1.6 1.5 Stable
Senegal 0.7 (2005) 0.9 0.9 Stable
Sierra Leone 1.5 (2005) 1.6 1.6 Stable
HORN Ethiopia 1.6 (2005) (1.0-3.5) (0.9-3.5) Decline in urban areas
Adult HIV prevalence in Sub-Saharan Africa, 2003 and 2005.
Source: UNAIDS 2006 Report on the Global AIDS Epidemic
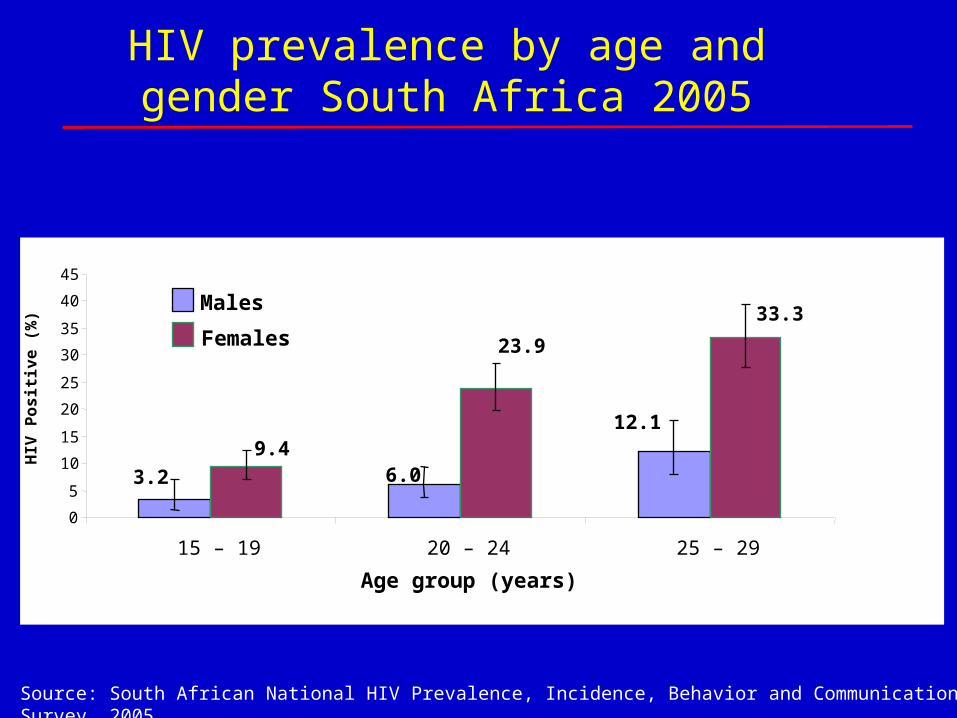
HIV prevalence by age and gender South Africa 2005
12.1
6.03.2
33.3
23.9
9.4
0
5
10
15
20
25
30
35
40
45
15 – 19 20 – 24 25 – 29
Age group (years)
HIV
Po
sit
ive
(%
)
Males
Females
Source: South African National HIV Prevalence, Incidence, Behavior and Communication Survey, 2005

Ecological Model for HIV Risk in Southern Africa
Individual Risks for HIV Infection
Widening Risk Contexts for HIV Infection Beyrer & Baral, 2006
Condom Usage, Circumcision, HSV-2/GUD, Viral Load, Acute Infection, Age of Coital Debut, Marriage, ARV Status