world’s first device aims to treat vertigos3.amazonaws.com/zanran_storage/uwmedicine... · aims...
TRANSCRIPT

On Oct. 21 a patient at UW Medical Center became the world’s first recipient of an implanted device that aims to quell the disabling vertigo associated with
Ménière’s disease. The UW Medicine clinician-researchers who invented
the device hope its initial 10-person surgical trial will spur exploration of its usefulness against a broader group of balance disorders that torment millions of people worldwide.
The device being tested – essentially a cochlear implant with new electrodes and software – represents four-plus years of work by Drs. Jay Rubinstein and James Phillips of UW Medicine Otolaryngology-Head and Neck Surgery.
“What we’re proposing here is a potentially safer and more effective therapy than exists now,” said Rubinstein, a surgeon whose résumé also boasts a Ph.D. in bioengineering and multiple U.S. patents.
In the United States, Ménière’s affects less than 1 percent of the population. While Ménière’s occurs mostly in people between ages 30 and 50, it can strike anyone. Rubinstein has seen it develop in a child of 6 and a man of 86.
The disease affects hearing and balance with varying intensity and frequency. Its episodic vertigo is thought to stem from the rupture of an inner-ear membrane. Endolymphatic fluid leaks out of the vestibular system, causing havoc to the brain’s perception of balance.
Afflicted people must lie still and battle nausea for several hours while the membrane self-repairs and equilibrium is restored, said Phillips, director of the UW
World’s First Device Aims to Treat Vertigo UW Medicine Surgical Trial Could Advance Care of Vestibular Disorders
continued on page 8
Dr. Jay Rubinstein, center, performs the surgical implant Oct. 21 as Dr. Jennifer Hsia observes. UW Medicine clinicians and researchers developed the device, reprogramming a cochlear implant, to help Ménière’s patients avert disabling vertigo attacks. The implant’s looped antenna, at top, is about the size of a quarter.
Surgery photo by Clare McLean, UW Medicine; device image courtesy of Cochlear LTD.
UW MedicineTransplantExcellenceRecognized
UW Medical Center (UWMC) was the nation’s only transplant-services provider to earn two silver-level awards in the Health Resources and Services Administration’s (HRSA) recognition of outstanding transplant care. On Nov. 4 at the 2010 National Learning Congress, HRSA distributed one gold (Mayo Clinic in Jacksonville, Fla.), 10 silvers and
148 bronzes to U.S. hospitals based on scores in transplant rate, patient mortality while awaiting a donor organ, and post-operative survival. UWMC’s kidney and liver transplant programs earned silvers, and its kidney/pancreas transplant program earned a bronze. No other Pacific Northwest transplant service earned silver, though several received bronze awards.
Harborview Medical Center | UW Medical Center | Northwest Hospital & Medical CenterUW Neighborhood Clinics | UW School of Medicine | UW Physicians | Airlift Northwest
PAGE
CONSULT2 3 6Depression Common with
Brain Injuries, Study Shows Transfer Center ExpeditesPatient Moves, Consults W I N T E R 2 0 1 1 Contrast Agent Reveals
Malignant Gliomas Better

2
CoNsUlT
Two big red flags: That’s what Drs. Charles Bombardier and Jesse Fann waved in May with findings
about people who suffer traumatic brain injury (TBI): 53 percent experience major depression within a year of injury but only 44 percent of those with depression receive treatment for it.
“This should alarm people,” Bombardier said, “because the prevalence is so high and becoming depressed predicts poorer outcomes one year after TBI.”
The research, published by the Journal of the American Medical Association, exposes a problematic blind spot among health-care professionals who treat the 1.7 million people who sustain TBI every year. Physical and cognitive impairments are recognized consequences of TBI, but depression is only marginally on caregivers’ radar screens, Bombardier said.
For primary-care providers (PCPs), a third finding of the study heightens
53% of Brain Injuries Cause Depression; Treatment lagsUW Medicine Study: Symptoms Can Emerge Long after Hospital Stay
Dr. Charles Bombardier, professor of rehabilitation medicine, left, and Dr. Jesse Fann, associate professor of psychiatry and behavioral sciences, led the study.
the issue’s relevance: Depression can emerge any time during the 12 months post-injury, which for many patients can be well past the end of outpatient medical and rehabilitative care.
“PCPs may be able to improve outcomes after TBI if they can recognize and treat depression in these individuals,” Bombardier said.
He and Fann, UW physicians based at Harborview, are leading a study of the effectiveness of telephone and in-person therapy for TBI patients with depression. The trial is recruiting patients from Washington, Alaska, Montana and Idaho, and will be open for two to three more years, said Fann, associate professor of psychiatry and behavioral sciences.
“We use cognitive behavioral therapy, which is the most evidence-based form of psychotherapy for depression. We’ve customized the therapy for people with TBI: for example, shorter sessions, more repetition, and we send people accompanying written materials to take advantage of both visual and verbal learning,” Fann said.
A psychologist counsels patients for 12 sessions spread over 16 weeks. Patients must have a qualifying injury and can self-refer or be referred by a health-care professional. Patients are paid $100 during the study; therapy sessions are free. Family members and significant others can join the sessions, if the patient wants. The counselor sends letters to the patients between sessions as reminders of key points covered.
“We’ve had patients call in from home, from work on a break. People in
the telephone counseling group can call in from anywhere, as long as they have about a half-hour to talk,” Fann said.
Patients can choose telephone or in-person counseling. A control group of patients will be randomly selected for usual care, which does not restrict the care that a person could receive outside the study.
A big unknown, Fann acknowledged, is whether TBI-related depression responds in the same way to the therapies that physicians routinely prescribe for depression associated with other causes.
TBI-Depression StudyTo learn about UW’s ongoing study of counseling for TBI patients with depression, contact research coordinator Kenneth Marshall: e-mail [email protected] or call 206.744.3609 (Seattle) or 866.577.1925 (elsewhere).
Rates of Major Depression after Traumatic Brain Injury
Time Since Traumatic Brain Injury, months
Depressed at injury (n=88) Preinjury history of depression,
not at injury (n=150) No history of depression (n=321)
Pati
ents
Wit
h M
ajor
Dep
ress
ion,
%
100 -
90 -
80 -
70 -
60 -
50 -
40 -
30 -
20 -
10 -
0 -1 2 3 4 5 6 8 10 12
“We think that depressed TBI patients should be treated with antidepressant medications or counseling, but these individuals may merit closer follow-up and more aggressive treatment than folks whose depression did not emerge through TBI,” he said.
Such attentive care is available at Harborview Medical Center and UW Medical Center, whose staffs have extensive experience in providing psychiatric and rehabilitation care to improve brain-injured patients’ lives.

3
UW MEDICINE
Around the clock, calls come from hospitals throughout the region: A patient is in our Emergency
Department but we’re not sure if we can manage the condition. Can you help?
In 2009, Harborview Medical Center admitted nearly 6,000 transferred patients, most needing care from the only Level I adult and pediatric trauma and burn center in Washington, Alaska, Montana and Idaho. Some 500 others were transferred to UW Medical Center.
UW Medicine’s Transfer Center facilitates consults and patient admissions with a “one call does it all” mindset. It is powered by a team of registered nurses whose resourcefulness is as prized as their clinical acumen.
During patients’ “golden hour” – the window in which care is most pivotal to a favorable outcome – they must understand the injury or condition, locate the appropriate consulting physician and complete a dozen other tasks to formally accept a patient into the system.
“A critical part of our job is not creating delays. If we have a rupturing aneurysm, time is a critical factor,” said Alida Coetzee, in her tenth year with the unit. “Our goal is to get the patient to the right physician at the right time.”
At outlying hospitals, emergency physicians responding to stroke, trauma and other serious conditions appreciate that the service facilitates conversations with specialists within a few minutes.
The Transfer Center is “essential to the state medical system,” said Dr. Marcus Dubrow, an emergency-department doctor in Aberdeen, Wash. “When there’s no such system in place, you’re like a fisherman, casting around till you get the right person.”
Dubrow values the easy sharing of radiology images via the center’s virtual private network (VPN) online. “If we’re discussing a case, they see the same images we’re looking at and give an opinion, all in real-time.”
About 100 hospitals and clinics use the VPN, which has markedly changed Transfer Center-managed consults in recent years, said its director, April Delgado.
“Often the film will be here before the patient leaves the outside facility,” she said. “It’s critical for services like vascular surgery. If you have someone with a dissecting aneurysm, the vascular surgeons here want to see that CT scan and decide if a patient needs a procedure, which one, and approximate the size of the stent they might need. This allows us to start treating the patient sooner.”
Sometimes the UW Medicine physician recommends against immediate transfer, providing guidance to further stabilize the patient before travel or to enable the community hospital to manage the case.
The center also handles inpatient moves to UW Medical Center for tertiary and quarternary care for cancer, heart problems, and transplant care. These transfer volumes are trending up about 100 percent from 2009, said Delgado, who helped establish the transfer ser-vice in 1998. Northwest Hospital & Medical Center, the newest member of the UW Medicine health system, will increasingly be in the referral mix, too, she anticipates.
Delgado’s team of RNs bring poise to a demanding job.
With the clock ticking, their decisions must yield a definitive response for the patient, satisfy physicians on both ends of the consult, follow protocols, notify Airlift Northwest when needed, and ensure bed availability.
They also field UW Medicine’s Community Care Line, after-hours patient calls about symptoms, prescription dosages and other concerns.
“It’s exciting and really educational,” Coetzee said. “You hear some of the best physicians in the country talking about what needs to happen.” Reach the UW Medicine Transfer Center 24 hours a day: 888.731.4791.
savvy servesPatients in‘Golden Hour’ UW Medicine Transfer Center is Lifeline for Region
Alida Coetzee is one of several registered nurses that handle Transfer Center calls.
Harborview Medical Center received nearly 6,000 transferred patients in 2009.

4
CoNsUlT
The Agency for Healthcare Research and Quality has awarded UW Medicine researchers $24 million in patient- centered grants:• $11.7 million for Dr. David Flum, professor of surgery, to improve SCOAP (Surgical Care and Outcomes Assessment Program) patient registries to track outcomes and to measure quality and performance of surgical care across Washington.• $9.9 million to Dr. Jeffrey Jarvik, professor of radiology and neurosurgery, whose team will study low back pain diagnosis and treatment in elderly patients.• $2.45 million to Sean Sullivan, Ph. D., professor of pharmacy and health services. Sullivan, with scientists at Group Health, the Fred Hutchinson Cancer Research Center and the Veterans’ Administration, will provide enhanced training for researchers interested in comparative effectiveness.• $416,377 to Dr. Heidi Crane, assistant professor of medicine, to evaluate the comparative effectiveness of lipid-lowering and antihypertensive medications among HIV-infected individuals.
Inventive Physicians Honored Drs. Roy Martin and Yoky Matsuoka
are UW Medicine’s 2010 Inventors of the Year. Martin, research professor emeritus in bioengineering, developed a method to detect air emboli during neurosurgery. He helped to improve quantitative cardiac imaging and co-invented the popular Sonicare toothbrush. Matsuoka, director of the UW Center for Sensorimotor Neural Engineering, is developing an anatomically correct robotic hand to investigate the neural control of human hand movements. Matsuoka received a MacArthur Fellowship in 2007.
Study of Brain-Injured ChildrenDr. Monica Vavilala, UW associate
professor of anesthesiology and pediatrics, won a $2.7 million grant to examine how to increase the adoption of national guidelines to improve outcomes for children who have suffered traumatic brain injury. The National Institute of Neurological Disorders and Stroke is funding the five-year project.
First-Responder TreatmentBrain-injured patients who received
out-of-hospital administration of hypertonic fluids as initial resuscitation did not experience better six-month neurologic outcomes or survival compared with patients who received a normal saline solution, according to a study by Dr. Eileen Bulger and colleagues at Harborview Medical Center. The study was published in JAMA.
NIH Names 2010 PioneersTwo UW Medicine researchers earned
National Institutes of Health Director’s Pioneer Awards this year. The awards provide up to $500,000 in direct costs, per year, for five years.
• Dr. Lalita Ramakrishnan is studying tuberculosis pathogenesis using the zebrafish model. She is an associate professor of medicine and microbiology and adjunct associate professor of immunology.
• Ram Samudrala, Ph.D., associate professor of microbiology, is working on a computational drug-discovery platform, which will first evaluate preclinical drug candidates for infections caused by all eight human herpes viruses.
MDA-Related Mutations Leo Pallanck, Ph.D., UW associate
professor of genome sciences, was awarded $312,699 by the Muscular Dystrophy Association for a three-year study of DNA mutations that lead to muscle weakness and wasting, exercise intolerance, seizures and stroke-like episodes.
Physician Liaison Team We’re here to assist you! Our team can meet with you to facilitate consultations, education or referrals to our providers. For details, contact one of our team members:
Voice: 206.598.5693 E-mail: [email protected] Web: uwmedicine.org/physician-liaison
Online Patient RecordsU-Link is a convenient way to access records of patients you refer to us. We now have expanded access for your support staff.
To enroll in U-Link, call 206.598.5693 or visit uwmedicine.org/u-link.
MedconWhen you need to confirm a diagnosis, obtain special information, or refer your patient for advanced care, Medcon operators will connect you with an expert UW physician. This free service is available 24 hours daily.
Voice: 800.326.5300 E-mail: [email protected]
Dr. David Flum discusses SCOAP’s mission at a conference. He won an $11.7 million award to track outcomes of surgical care across Washington State.
Agency Awards UW$24 Million in Grants
Research Briefs
Medical Programs
On-Air and Online
Among UW Medicine’s new programs at UWTV, the University of Washington’s award-winning channel:
• Inside Access: Minimally Invasive Cardiac Care Meet physicians and researchers pioneering noninvasive tech-niques for patients with heart malformations, failing valves and out-of-rhythm heartbeats.
• Grand Rounds: Geriatric Hip Fractures A panel of physicians discusses patients with hip fractures, the most serious osteoporosis-related concern affecting elderly people.
• Inside Access: Reshaping Vascular Surgery Program follows two patients whose lives were saved by endovascular techniques to repair abdominal aortic aneurysms.
• Mini-Med School: Is Your Doctor Really Hearing You? Patient communication informs decisions and healthy outcomes. A panel of UW Medicine physicians reflects on their experiences as patients.

Dr. Ganesh Raghu, UW professor of medicine, leads the pulmonary care team that kept Alicia Foss alive and viable for transplant.
5
UW MEDICINE
HelpingPatientssurvivethe WaitLung Team Kept Candidate Viable for Life-Saving Transplant
Alicia Foss dodged a bullet, some might say, when she survived childhood leukemia – though its
legacy almost killed her two decades later: Chemotherapy that worked so well also created an environment in which pulmonary fibrosis (PF), an incurable lung disease, developed and grew unnoticed until she was a high school senior.
In the time that followed, including four fretful years on the national organ-transplant wait list, Foss’ death drew closer with every shallow breath.
Fortuitously she became a patient of UW Medicine physician Dr. Ganesh Raghu, a world-recognized PF expert. From February 2006 until she received a double-lung transplant in April 2010, Foss’ health was maintained by UW Medical Center’s (UWMC) interstitial lung disease/pulmonary fibrosis team.
Their collective vigilance and experience likely slowed the disease’s progression and kept Foss and her transplant hopes alive during the wait.
“Alicia’s pulmonary fibrosis was bad. She had very limited life expectancy and no options other than lung transplant,” said Raghu, medical director of UWMC’s lung transplant program.
“In a person with longstanding fibrosis, their lung volume’s functional capacity keeps decreasing, their lungs and chest get smaller and the oxygen requirement goes up. They develop pulmonary hypertension, then fluid retention, and then they die. Medical management is very challenging.”
Every two to three months,
Foss’ parents ferried her from rural Kennewick, Wash., to Seattle. Raghu reassessed her dwindling lungs and recalibrated medications to address changes in inflammation, fibrosis, oxidant-antioxidant balance and pulmonary hypertension.
Raghu likened his tailored care to navigating a wintertime, pre-dawn drive on an interstate: “You must always be alert because you know black ice is there though you cannot see it.”
To extend the analogy across his transplant candidates, Raghu pilots cars that need new engines. He can only estimate his fuel supply and the nearness of his destination. He must take the car as far as it can go, accelerating and break judiciously, taking curves at optimal angles and speeds, and anticipating perils that could doom the trip.
Foss was among the 25 percent of U.S. lung-transplant candidates who wait more than 36 months for donor organs. Few transplant candidates elude the stress that comes with waiting.
“We provide counseling to the patients and families, to give hope,” Raghu said. “When you cannot walk a few steps without shortness of breath and you require supplemental oxygen, you wonder whether a transplant will indeed happen.”
In 2007, Foss got the call saying that matching donor lungs had been located, but learned, upon reaching the hospital, that they were not healthy.
“It was tough,” she said. “Just hearing that you need a lung transplant is emotional in itself. There were ups and downs. The support from everybody is what kept me going.”
Emphysema, cystic fibrosis, any end-stage pulmonary disease including fibrosis, sarcoidosis, and hypertension
are conditions that can warrant lung transplant.
A widespread team keeps these patients alive, Raghu said. Physicians, nurses, coordinators, pharmacists, respiratory and rehabilitation therapists, social workers and the surgical team led by Dr. Michael Mulligan – all contribute to lung-transplant patients’ survival rate, which at UWMC is superior to the rate nationwide.
Patients’ compliance and willingness to endure makes a difference, too, Raghu said.
In April, after a four-year wait on the national transplant list, Alicia Foss was on a f light to receive a set of donor lungs at UW Medical Center.
“The patient and family are the main team players,” he said. “Motivation, encouragement when things are not well, holding hands – all of that matters.” To refer a patient or learn more, call the Lung Transplantation clinic at 206.598.5668.

6
CoNsUlT
Within a few months, UW Medicine’s neurosurgeons will be able to offer a therapeutic
advantage to patients with highly lethal malignant gliomas: 5-aminolevulinic acid (5-ALA), a specialized contrast agent that “paints” tumor cells, revealing them in the operating room.
Tumor tissue can be difficult to distinguish from normal brain tissue, said Dr. Richard G. Ellenbogen, UW Medicine’s chair of neurological surgery. 5-ALA, taken orally by the patient before surgery, is preferentially absorbed by cancer cells, which glow when the tumor is exposed to a blue fluorescent light.
5-ALA is in use in Europe, the Pacific Rim and Canada, and more recently, a handful of U.S. cancer centers. Randomized studies have documented a twofold increase in the amount of malignant glioma tissue removed when 5-ALA is used, which, in turn, improves survival among patients.
“We want to emulate that success,”
Ellenbogen said. UW Medicine is home to one of the nation’s most prominent National Cancer Insitute (NCI)-funded platforms for brain-tumor study.
Dr. Dan Silbergeld, chief of neurological surgery at UW Medical Center (UWMC), sought and received the U.S. Food and Drug Administration’s approval to use 5-ALA locally. He operates on more than 200 brain-tumor patients a year.
”The goal of surgery for malignant gliomas is to safely remove as much of the tumor as possible. The addition
of 5-ALA has helped neurosurgeons achieve this goal. We are excited to bring this technology to the Northwest,” Silbergeld said.
For decades, malignant gliomas, which constitute more than 50 percent of brain tumors in adults, have seemed immune to medicine’s best efforts. The introduction of 5-ALA at UWMC, combined with another research breakthrough at UW – nanoparticles that not only light up tumor cells but also have potential to kill them – is energizing neurosurgeons and scientists here.
Exploiting Nanoparticles’ Size, Strength
A flurry of recent research here and elsewhere demonstrates nanoparticles’ promise as a vehicle to identify and the treat tumors. Thousands of times thinner than a human hair, nanoparticles safely cross the blood-brain barrier, which is impermeable to conventional chemotherapy drugs.
UW Professor Miqin Zhang, principal investigator for the NCI nanoplatform studies, has devoted years to deciphering how to exploit nanoparticles medically. Her research suggests that, despite its lack of size, a nanoparticle might be nature’s smallest pack mule.
“We decorate the nanoparticle with a specific chemical ligand that recognizes and targets only the tumor.
Now our research is focused on the nanopaticle therapies – particles to carry genes, chemo drugs and small interfering RNA molecules, to try to kill the tumors,” Zhang said.
As a professor of materials science/engineering, neurological surgery and radiology, she is magnificently qualified to generate, rationalize and prioritize ideas.
“It helps me to see the problems, and how to solve them,” Zhang said of her rounded perspective. “The engineer thinks a different way from the doctor. Dr. Miqin Zhang’s research team has developed a nanoparticle
that can reveal glioblastomas and deliver drug therapy to them.
New Agent to Reveal Malignant Gliomas Surgeon Receives OK to ‘Paint’ Brain Tumors; Nanoparticle Research Shows Early Promise
Brain tumor tissue (a) under normal lighting and (b) under f luorescence with 5-ALA, which reveals tumor tissue as pink. Dr. Dan Silbergeld, UW professor of neurological surgery, anticipates using 5-ALA with glioma patients in coming months. Tissue images courtesy of Springer-Verlag Wien.
continued on page 7

7
UW MEDICINE
UW Medicine Health System launched its new brand- positioning campaign in
September. The campaign’s main goal is to increase consumer awareness of the services that UW Medicine provides to improve health throughout the region.
Advertising to support the brand campaign features compelling stories that capture the extraordinary care patients experience from UW Physicians at Harborview Medical Center, UW Medical Center, Northwest Hospital & Medical Center, UW Neighborhood Clinics and Airlift Northwest.
“The mission of UW Medicine is to improve the health of the public, locally and globally. That is unique in the Pacific Northwest,” said Dr. Paul Ramsey, chief executive officer of UW Medicine and dean of the UW School of Medicine.
During the past year, UW Medicine’s marketing team worked closely with the firm DNASeattle on strategies to build the public’s understanding of the system’s health-care resources. The brand-development process included extensive market research,
UW Medicine EmphasizesBroad skill set, Unique RoleBrand is Positioned to Educate Public
which revealed that consumers view all health-care professionals as somewhat similar.
“This key insight confirmed the need to design an effective method to communicate health information to the public so that they can understand UW Medicine’s depth and breadth,” said Johnese Spisso, chief health system officer of UW Medicine. “Ours is the only health-care system in the region that provides primary care through the most complex quarternary care.
“We want our community to understand that our world-class health system is available to them and that they can benefit from its clinical care, teaching and research that are improving health outcomes around the world.”
The campaign features stories of patients, health-care professionals and staff that give meaning to the brand statement: “From here, we change the world.” Each story shows how local medical advances have ripple effects extending far beyond the Puget Sound region.
Information about the UW Medicine health system, its benefits and how new patients can access its world-class health care will be shared in various venues.
UW Medicine’s Marketing and Commu- nications team unveiled the new brand campaign and its supporting stories to a group of physicians, senior leaders and staff at Meany Hall in late September.
That is often a barrier, but I think we do pretty well to bridge the gap here at UW,” she said.
One confounding issue she and other researchers have met is tumor-cell variation: More than 70 biologically unique brain cancers exist.
“If we use antibodies (against the tumors), then we have to use many types that recognize individual tumor varieties. But now we use a specific tumor-targeting ligand called chlorotoxin, which recognizes almost all brain tumor varieties,” Zhang said.
Zhang; Ellenbogen; Donghoon Lee, a research associate professor of radiology; and a small cadre of UW scientists developed multifunctional nanoparticles studded with chlorotoxin Cy.5.5. It binds specifically to, and slows the invasion of, malignant gliomas. The chlorotoxin compound must demonstrate efficacy in animal tests before it can be considered for treating humans.
“We’ve done something that National Institutes of Health has wanted us to do – ally engineers with neurosurgeons to produce a compound such as chlortoxin-Cy.5.5, which we can take from the research lab and use to help patients,” Ellenbogen said.
Although the chlorotoxin’s clinical use might be years away, the other tumor-painting diagnostic, 5-ALA, will soon benefit patients here. Zhang acknowledged her enthusiasm at the prospect.
“This is very challenging work but that’s what makes it satisfying, too,” she said. “It’s exciting, the feeling that we’re getting close to solving some big problems for people with cancer.” To refer a patient or learn more about 5-ALA, call UWMC’s Neurological Surgery Clinic at 206.598.9449.
Aligning bioengineers and neurosurgeons keeps UW Medicine at the forefront of brain-cancer research, said Dr. Richard Ellenbogen, UW professor and chairman of neurological surgery.
BRAIN CANCER from page 6
UW MEDICINECoNsUlT
CoCHlEAR DEVICE TREATs VERTIGo from page 1
Dizziness and Balance Center. Because the attacks come with scant warning, a Ménière’s diagnosis can cause people to change careers and curb lifestyles.
Many patients respond to first-line treatments of medication and changes to diet and activity. But when those therapies fail, destructive procedures have been the only option. In essence, the person sacrifices function in the affected ear to halt the vertigo – much like a pilot who shuts down an erratic engine during flight. Forever after, the person’s balance and, often, hearing are based on one ear’s function.
Phillips and Rubinstein’s device preserves hearing and balance in the affected ear.
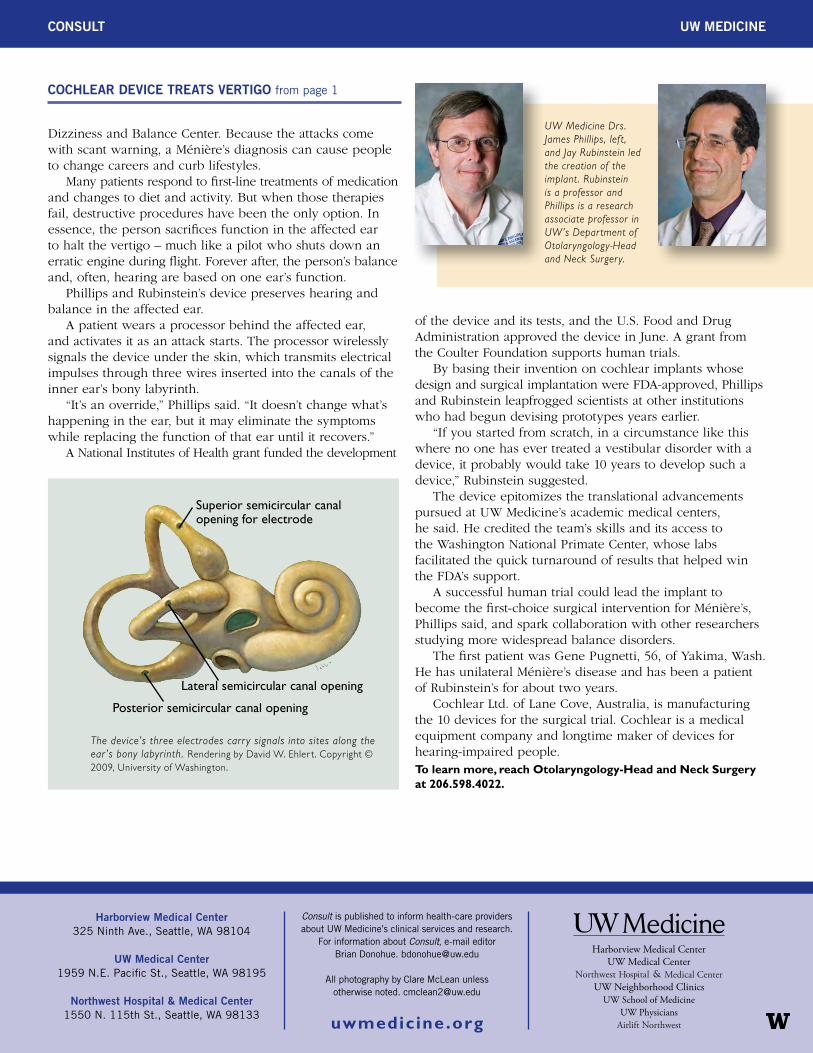
A patient wears a processor behind the affected ear, and activates it as an attack starts. The processor wirelessly signals the device under the skin, which transmits electrical impulses through three wires inserted into the canals of the inner ear’s bony labyrinth.
“It’s an override,” Phillips said. “It doesn’t change what’s happening in the ear, but it may eliminate the symptoms while replacing the function of that ear until it recovers.”
A National Institutes of Health grant funded the development
of the device and its tests, and the U.S. Food and Drug Administration approved the device in June. A grant from the Coulter Foundation supports human trials.
By basing their invention on cochlear implants whose design and surgical implantation were FDA-approved, Phillips and Rubinstein leapfrogged scientists at other institutions who had begun devising prototypes years earlier.
“If you started from scratch, in a circumstance like this where no one has ever treated a vestibular disorder with a device, it probably would take 10 years to develop such a device,” Rubinstein suggested.
The device epitomizes the translational advancements pursued at UW Medicine’s academic medical centers, he said. He credited the team’s skills and its access to the Washington National Primate Center, whose labs facilitated the quick turnaround of results that helped win the FDA’s support.
A successful human trial could lead the implant to become the first-choice surgical intervention for Ménière’s, Phillips said, and spark collaboration with other researchers studying more widespread balance disorders.
The first patient was Gene Pugnetti, 56, of Yakima, Wash. He has unilateral Ménière’s disease and has been a patient of Rubinstein’s for about two years.
Cochlear Ltd. of Lane Cove, Australia, is manufacturing the 10 devices for the surgical trial. Cochlear is a medical equipment company and longtime maker of devices for hearing-impaired people.To learn more, reach Otolaryngology-Head and Neck Surgery at 206.598.4022.
UW Medicine Drs. James Phillips, left, and Jay Rubinstein led the creation of the implant. Rubinstein is a professor and Phillips is a research associate professor in UW’s Department of Otolaryngology-Head and Neck Surgery.
The device’s three electrodes carry signals into sites along the ear’s bony labyrinth. Rendering by David W. Ehlert. Copyright © 2009, University of Washington.
Superior semicircular canal opening for electrode
Lateral semicircular canal opening
Posterior semicircular canal opening
Harborview Medical Center 325 Ninth Ave., Seattle, WA 98104
UW Medical Center 1959 N.E. Pacific St., Seattle, WA 98195
Northwest Hospital & Medical Center 1550 N. 115th St., Seattle, WA 98133
Consult is published to inform health-care providers about UW Medicine’s clinical services and research.
For information about Consult, e-mail editor Brian Donohue. [email protected]
All photography by Clare McLean unless otherwise noted. [email protected]
uwmedicine .org
UW MEDICINECoNsUlT