what's cooking in health policy, market inquiries and other...
TRANSCRIPT

What's cooking
in health policy,
market inquiries
and other curiosities
Health law and ethics update
Follow us on twitter or our twitter-feed
www.ekconsulting.co.za
@EKConsulting1
The abbreviated abbreviates
1. HMI & PMB charges
2. Medical devices & medicines
3. NHI
4. OHSC & CON
5. DSPs, and other med scheme cases
6. Global fees
7. HPCSA matters
8. Malpractice
HMI ….

“So, who is this Peter?” …
“and who are the Departments of Silly
Questions?”

Where we are in HMI… • Timelines:
– First set of hearings (Feb, March & May),
should be 6 sets
– Provision report of Aug 2016 postponed
• OECD/WHO Report (next slide): 30 August
round table
– Is used to make case for (further) price
regulation & in NHI White Paper
• PMB up-coding and charging more
• DSPs & co-payments

Reply by WHO “After careful review of all comments, we find no substantive
issues related to the data and analysis that alter the main
findings and conclusions of the WHO/OECD report, namely
that:
• Prices in South African private hospitals are high
relative to South Africa's income level, and on par with
the OECD average and much higher income
European countries (i.e., France, U.K, and Germany).
• Prices in South African private hospitals are increasing
above the rate of increase for other goods and
services in the South African economy
• Prices in South African private hospitals are
unaffordable for the vast majority of South Africans •
even higher income groups”
Bestmed, BHF and DoH
addressed this at HMI

Indications of possible
recommendations • Implementation of non-implemented provisions
of NHA (incl RPL, info on quality, etc.)
• Patient RIGHTS: – PMB info,
– info on quality and
– info on pricing
• Implementation of PMB Review
• Doctor employment by hospital
• Address technology… (“when last were you in Chicago?”)
• Role of brokers and administrators(?)

Medical devices & Medicines

The SAHPRA Project
• Acts 72 of 2008 and 14 of 2015
(amending the current Medicines Act)
• Regulations still outstanding
• MCC will become SAHPRA
• Device “establishments” (importers,
manufacturers, distributors) must apply
for licence BEFORE 1 March 2017
(under current Act)

Medical devices Will also be subject to:
• Section 18A: No bonus, rebate or incentive
scheme (unless declared acceptable - MoH)
• Section 18B: No sampling, unless for exhibition
or appraisal purposes (regs)
• Section 18C: Marketing Codes
• SO:
– Product placement in facilities? (capex, etc.)
– Free goods (e.g. glucometer free + strips sold)?
– Differential pricing and discounts? (e.g. implants,
sutures, etc.)

Developments in medicines
• SEP and a second SEP)
• IP:
– Bolar provision & parallel importation &
mandatory generic substitution
– Voluntary licensing
• IP - DTI – new framework
– Search and Examination of patents
– Different criteria for patentability
– Compulsory licensing

NHI White Paper: re-cap
Work Streams 1. NHI Fund: (Prof McIntyre)
2. NHI Benefits (Dr Yogan Pillay)
• Draw on PHC, HIV/TB, NCDs, EMS & hospital
packages – public sector
• Health technology assessment
3. Purchaser-provider split (Dr Anban Pillay)
• Providers: mix of public and private
• Independent multidisciplinary group practices
• Results-based purchasing & contracting
• Registration of facilities
• DRG’s and capitation
• Incentives for providers to contract

Work Streams 4. Medical schemes (Mr Vishal Brijlal)
• Unified information system
• Only complementary benefits (?) – MSA to change
• Tax subsidies towards NHI Fund (DTC)
5. Finalise NHI Policy Paper (Dr Thulare)
6. Strengthen District Health System (Mr
Morewane)
• Shift from hospital care to PHC
• DHM (District Health Management) Offices
• Consider demographics & epidemiology
• Coordination of services, referral system

And now?
• Davis Tax Committee asking for input on
NHI tax – hearings begin Nov
• White Paper to be finalised
• Various regs, e.g. on EMS have been
finalised, some laws still to go through
Parliament
• Consultation through Work Streams
• Financing Paper still outstanding (DTC?)

OHSC and the CON

OHSC – Office of Health
Standards Compliance
• http://www.ohsc.org.za



National Health Act, s36
You’d need a CON to —
• Establish (start a new “health establishment” (incl
pharmacies), occ health clinic, what equipment, staffing,
etc.),
• Construct (developers, builders)
• Modify (existing practice, etc.)
• Acquire (BUY! -buyers gets CON, not seller provides
CON to buyer)
• Renew (x number of years, whereas x ,20yrs)
a health establishment or health agency
The issuing or renewal may be made subject
to:
“compliance by the holder with national operational
norms and standards (OHSC) for health
establishments and health agencies, as the case
may be; and any condition regarding—
(i) the nature, type or quantum of services to be
provided by the health establishment or health agency;
(ii) human resources and diagnostic and therapeutic
equipment and the deployment of human resources or
the use of such equipment;
(iii) public private partnerships;
(iv) types of training to be provided …; and
(v) any criterion contemplated in subsection (3).”

DSPs
CMS v Genesis (SCA)
• What is it about?
– Scheme not paying for prostheses (not
available in state sector)
– Scheme saying its rules say state = DSP
and/or they only have to pay up to level of
state care
– Reversal of benefits already paid
SCA = Supreme Court of Appeal

Q: Can the scheme rules override the Act and regulations?
A: No, scheme cannot contract out of legal framework
Q: Can the scheme say it only pays up to the level available in
public sector?
A: No, it has to pay in full
Q: Can the scheme say the state is their DSP but not appoint
them?
A: No, you cannot oblige members to go to state and then
there is little or no cost to the scheme
Q: Can the scheme only appoint the state as their DSP?
A: No, as it would go against objective of the PMBs and the
law
Q: can scheme say they don’t pay for prostheses not available
in state?
A: No, if reasonable and part of treatment

CMS Appeals Board: Punative
Co-payments: ICPA v CMS • History:
– Schemes impose penalty co-payments when
members elect to use not network/DSP
providers (even where services, fees, etc. are
the same)
• Schemes of the opinion that if no penalty co-
payment, no incentive to use DSPs
• ICPA: CMS to have penalty co-payment
system declared Undesirable Business
Practice (Section 61) = ruling of Appeal
Board

SCA case:
Sechaba, Gen-health
• Schemes do NOT have a free choice to
now pay provider, then pay member
• At par 25:
– If it is owing to the provider, it must be paid
to the provider
– People become members exactly so that
scheme will pay up to benefits, only when
patient chose to pay provider themselves,
should scheme pay patient
Global fees
• Medical schemes going out on tender
• Hospitals incorporating professional
fees in their services
• Some models a hit with the HMI
• HPCSA rules:
– No fee sharing (rule 7)
– No subcontracting (rule 18)
– Possible exploitation (rule 22)
• Proposals for amendments to ethical
rules?

HPCSA


Findings
• Failure to perform to an adequate
standards to ensure an effective and
sufficient administration
• Failure to ensure appropriate operations
management
• Mismanagement, maladministration,
irregularities in professional conduct
inquiries
• Also structure of HPCSA with 12 Boards
is problematic

Latest from HPCSA Hearings
• Can your PROVE that: you have
obtained –
– informed consent and
– informed BILLING consent?

Malpractice
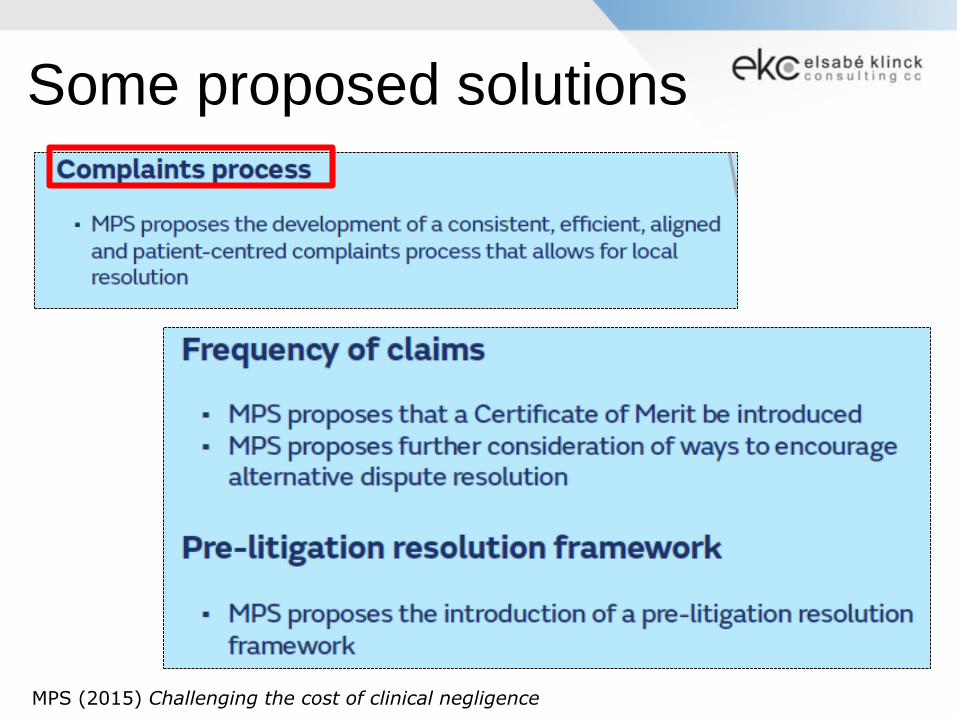
Some proposed solutions
MPS (2015) Challenging the cost of clinical negligence

Thank you!
Follow us on twitter or our twitter-feed
www.ekconsulting.co.za
@EKConsulting1