what is functional training and what does it mean for the
TRANSCRIPT
ARE YOU EVEN FUNCTIONAL? WHAT IS FUNCTIONAL TRAINING AND WHAT DOES IT MEAN FOR THE MASTER’S ATHLETE?BRIAN JUSTIN, MKIN, CEP, CSCS
CLINICAL EXERCISE PHYSIOLOGIST/CERTIFIED STRENGTH AND CONDITIONING
SPECIALIST
WHAT IS FUNCTIONAL S&C?
• Function definition – 1. Capable of
operating or functioning. 2. Having or
serving a utilitarian purpose.
• Prescribing exercise is synonymous with
skill building for your clients. How do you
want them to move?
• “Functional” is dependent on what the
purpose of the training is.
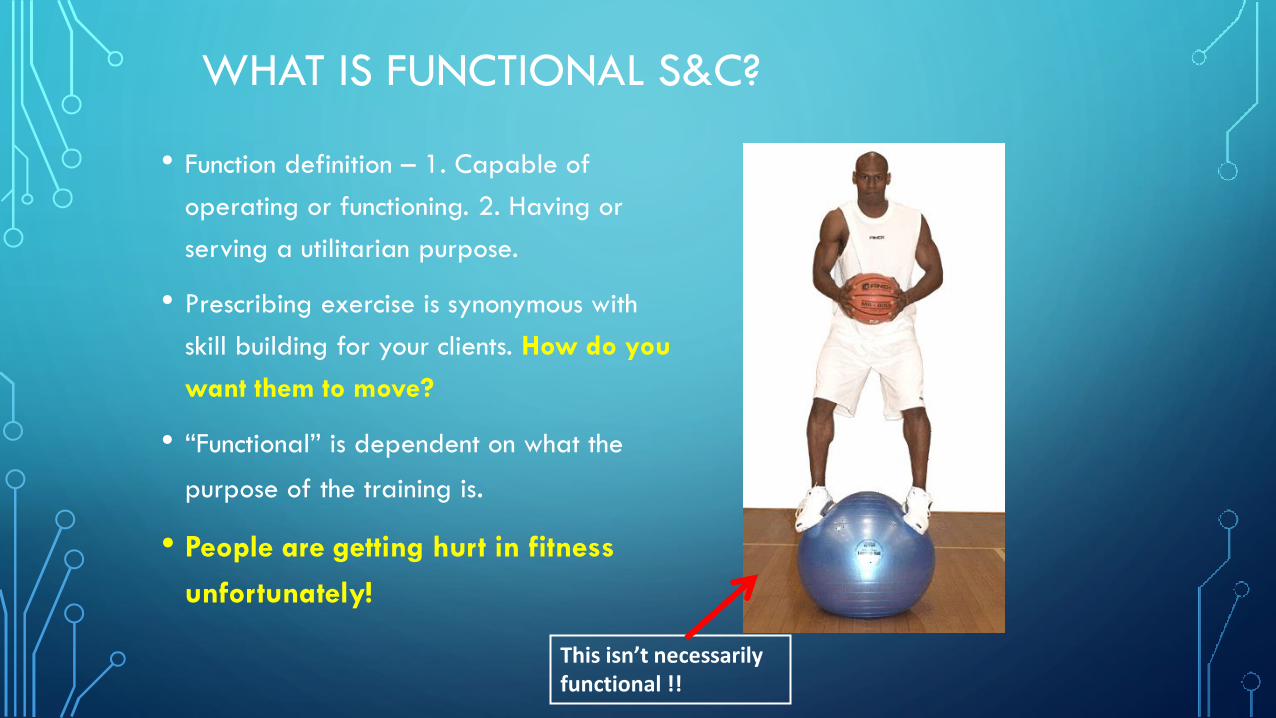
• People are getting hurt in fitness
unfortunately!
This isn’t necessarily functional !!
IMPORTANCE OF MOVEMENT: TO NULLIFY THE INSULTS TO THE BODY (LOUPOS, 2011)
Insult: Any experience, real or
imagined, that (dis)stresses or
offends the organism.
Minor level (frequent but less
impactful):
• Slumping posture
• Sub-optimal nutrition
• Stressful day at work
• Restless sleep
• Carrying a bag over one shoulder only
Medium Level: (rarer than minor but not
uncommon)
• Sprains/strains
• Coccyx impact
• Slow to resolve emotional trauma
• Jarring and bruising from sporting events
• Dean Juhan (book Job’s Body) – “ locomotor
patterns become individualized by one’s
unique pattern of experiences” or
“repeated gestures become postures, and
sustained postures become structures.
IMPORTANCE OF MOVEMENT: TO NULLIFY THE INSULTS TO THE BODY (LOUPOS, 2011)
Major Insults (infrequent):
• Broken bones
• Surgeries
• Automobile accidents
• Failed marriages
• Ruined careers
• Strokes
Combination of the Minor + Medium + Major insults – Athlete Lifestyle
management = Your movement behaviour and work capacity.
IMPLEMENTING FUNCTIONAL STRENGTH AND CONDITIONING
Characteristics of movement based
strength training:
• Environment we live in is considered.
• Muscle contraction spectrum is utilized.
• Bio-motor Profiles are addressed.
• Movement skill is taught (sequential
firing)
• Speed and amplitude (ROM) is
manipulated.
• Proprioceptive demand is challenged
Proprioceptive literacy (Loupos, 2011) – The brain’s ability to match
sensory feedback with a desired motor program.

THE ENVIRONMENT IN WHICH WE PLAY!
• Gravity
• Momentum (mass x speed)– Acceleration is an
increase in momentum and deceleration is a
decrease in momentum.
• Inertia – Being able to break the position of your
body or move objects.
• Impulse – (force x time applied) – Change in
momentum.
• Ground Reaction Forces – Generate forces from
the ground up
• 3 Planes of motion and associated plane of
stabilization – Sagittal, frontal, and transverse
plane.
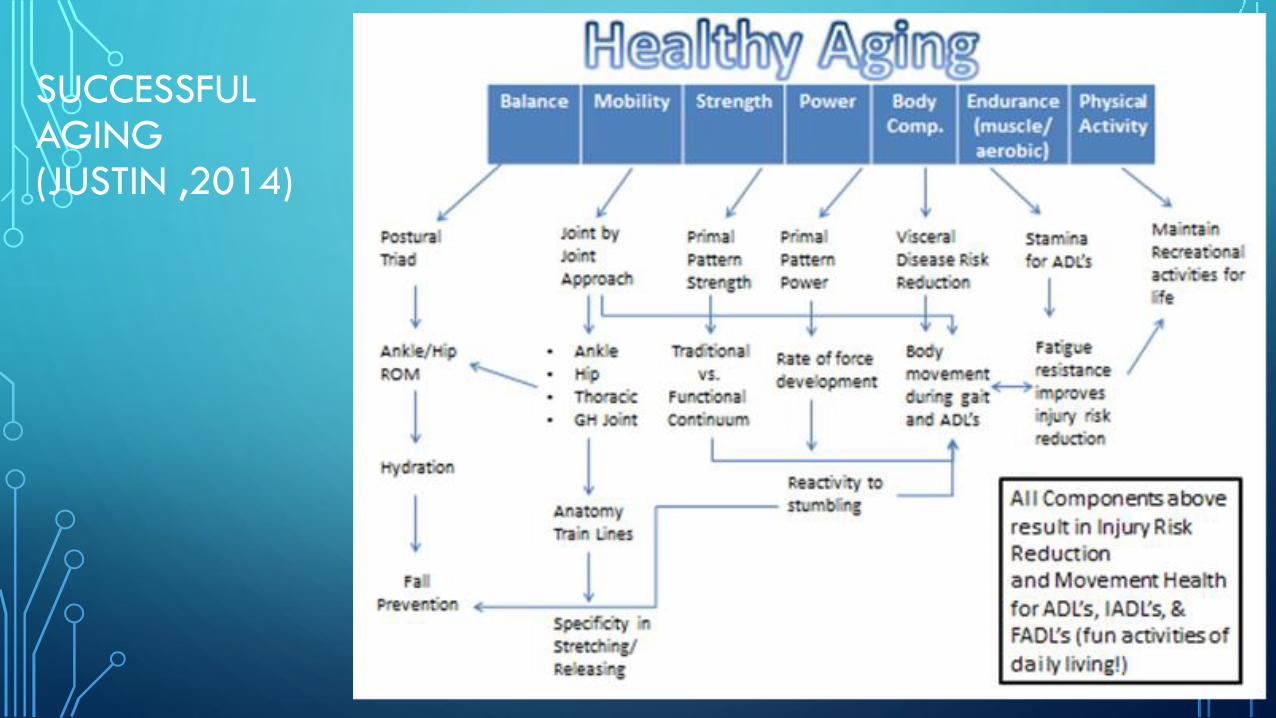
SUCCESSFUL AGING(JUSTIN ,2014)
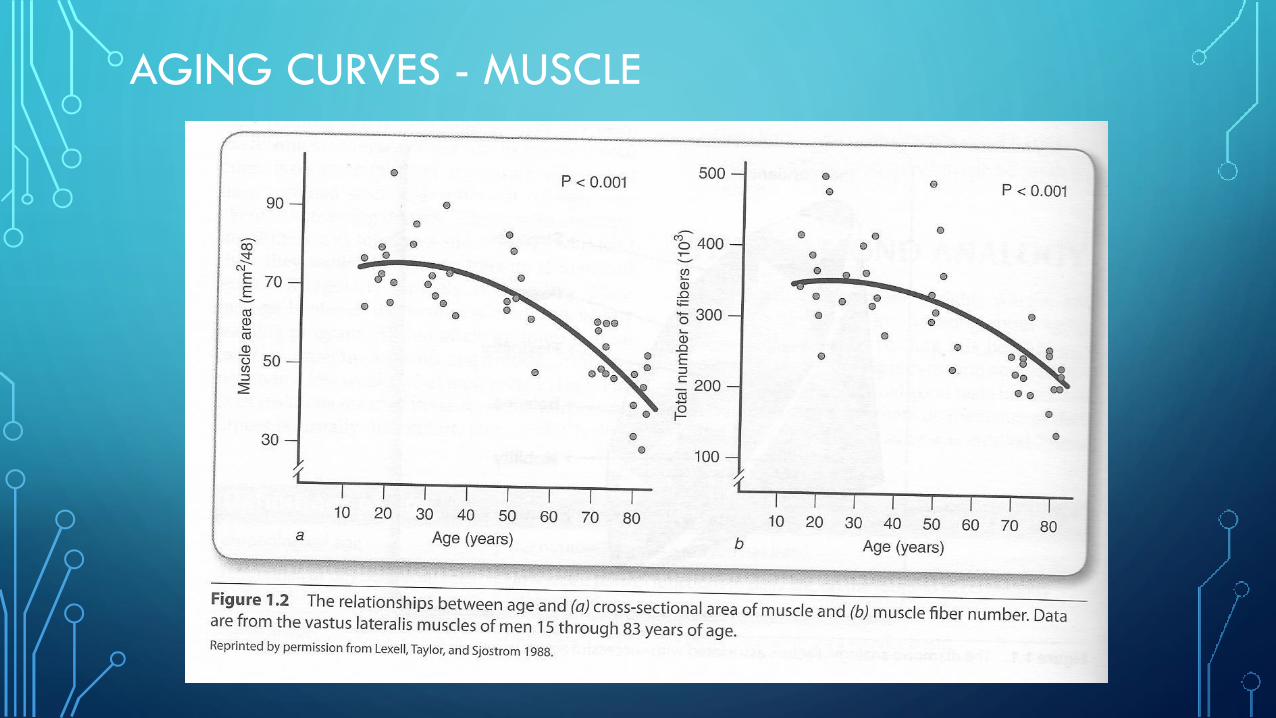
AGING CURVES - MUSCLE
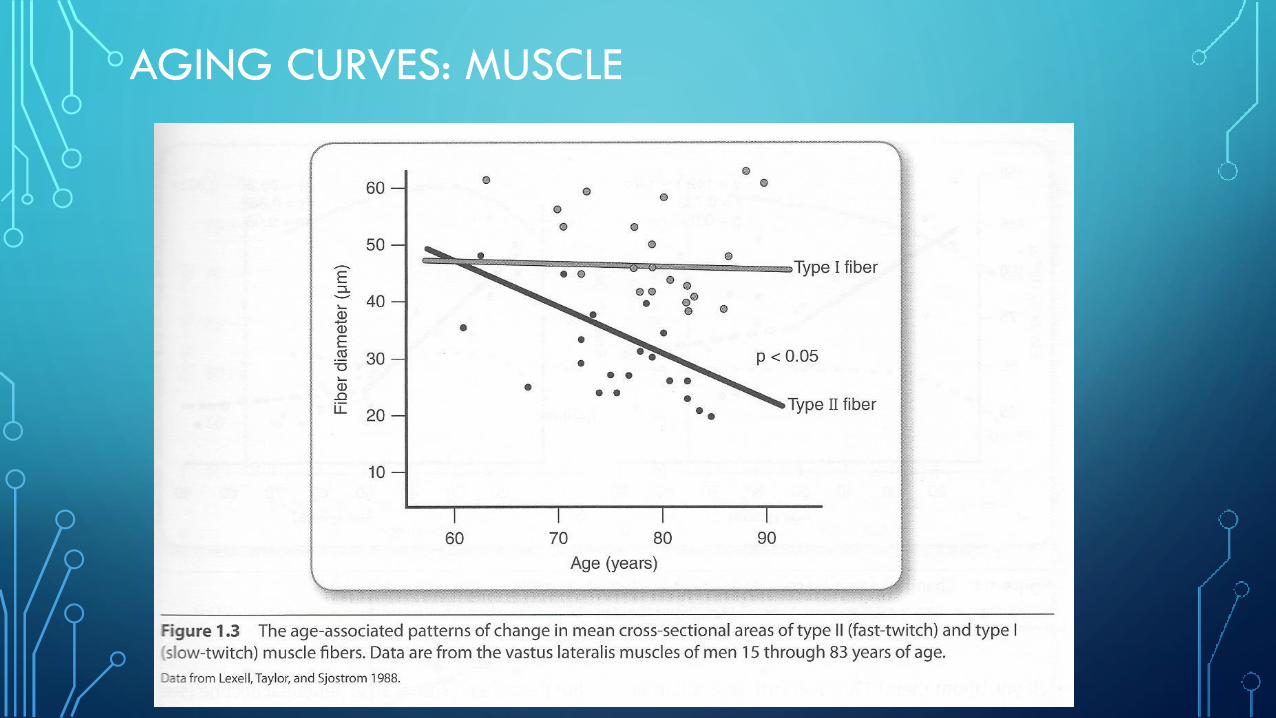
AGING CURVES: MUSCLE

AGING CURVES: BODY COMPOSITION

AGING CURVES: BONE MINERAL CHANGES

AGING CURVES: LIGAMENT STRENGTH
Load at failure is
less in ligaments
with age.

AGING CURVES:CARDIOVASCULAR FITNESS (VO2 PEAK)
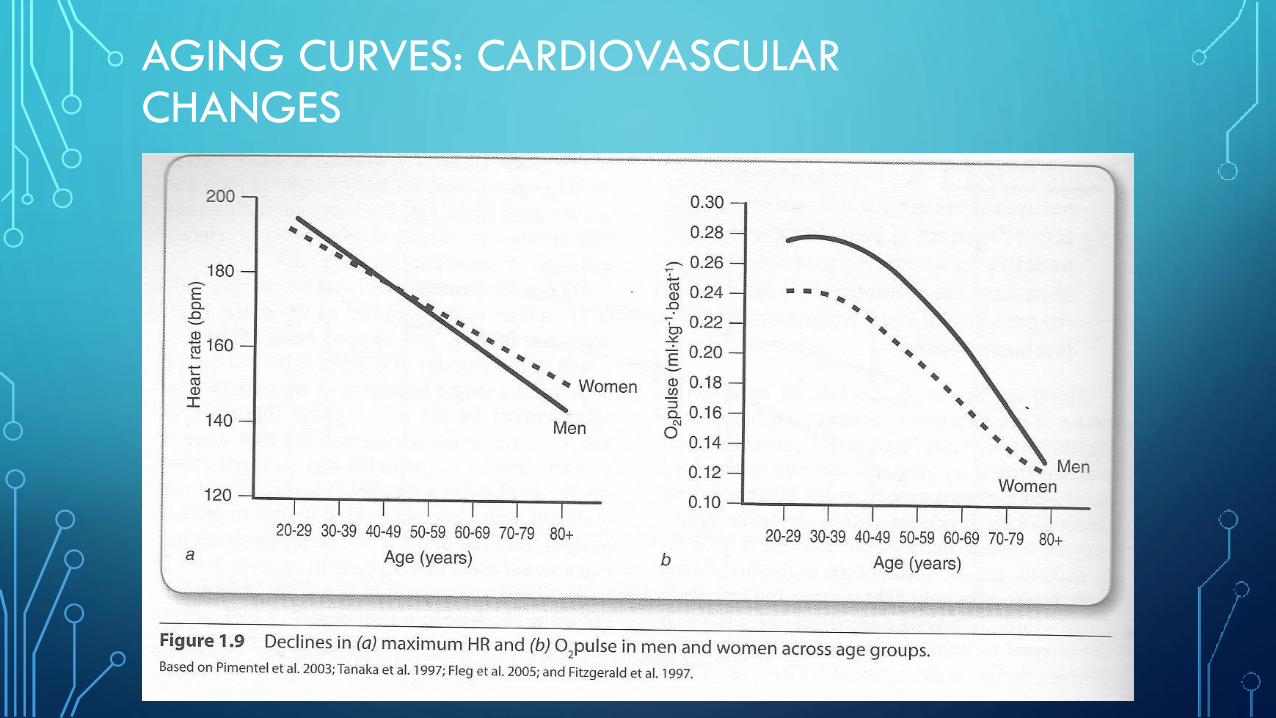
AGING CURVES: CARDIOVASCULAR CHANGES
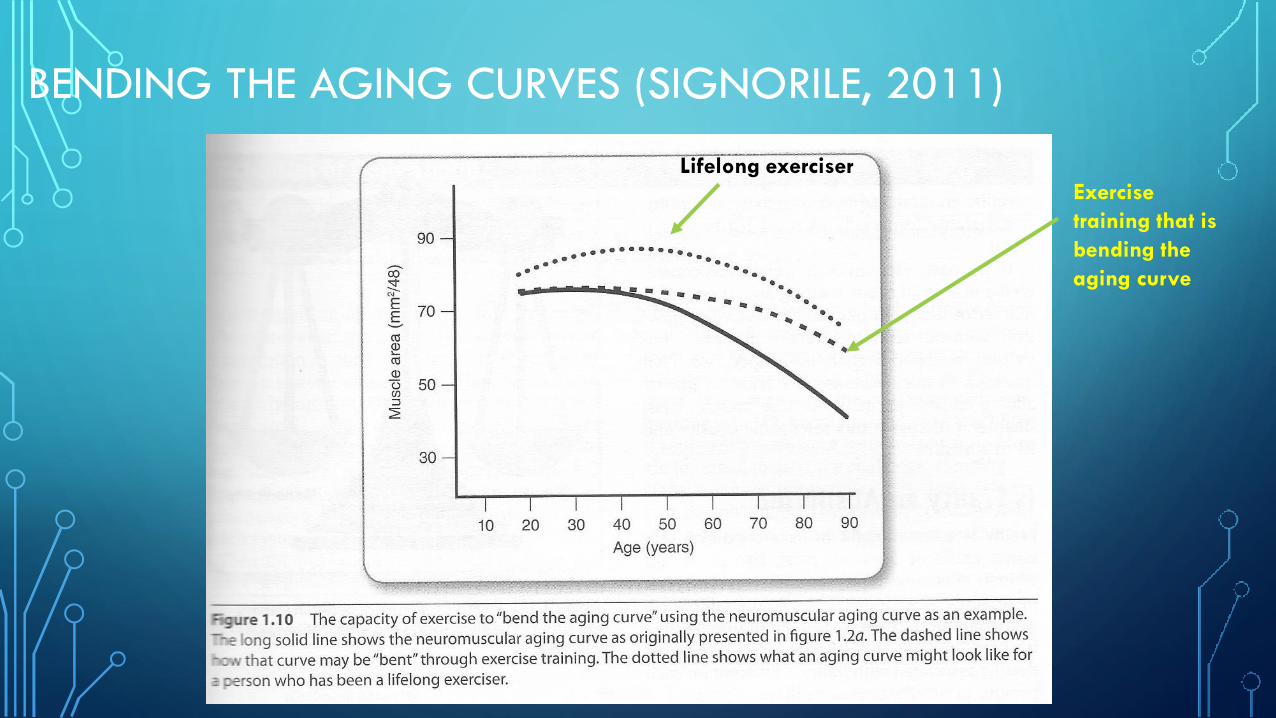
BENDING THE AGING CURVES (SIGNORILE, 2011)
Exercise
training that is
bending the
aging curve
Lifelong exerciser
SENESCENT CHANGES: KNEE
• Declining vascular supply and nutrition in the meniscus – gives rise
to complex tears.
•Osteoarthritis may be an issue.
• Important to observe the mobility of the hip and ankle
joints.

SENESCENT CHANGES: SHOULDERS
• Depth of the glenoid labrum decreases with age due to
degeneration forcing cartilage to bear the forces across the joint.
• Decrease in range of motion by a few degrees.
• Degeneration of rotator cuff tendons leads to pain and weakness in
the acromion region, biceps anteriorly, deltoid, or mid humerus.
• Activeand passive range of motion in internal rotation decreases with
age.
• Degenerative changes in the acromioclavicular joint are common
with increasing age.
SENESCENT CHANGES: SPINE
• The intervertebral disc undergoes alteration in its structure with maturation
and aging. The water content of the nucleus pulposus decreases and is
replaced by a fibrous material. The degeneration of the disc is a normal
process of aging and not pathological.
• Issues: segmental instability – work more on core efficiency
What are the fundamental motor programs?
❑ Squatting
❑ Lunging
❑ Bend patterns
❑ Rotation and Anti-rotation
❑ Push and Pull (horizontal and vertical)
❑ Locomotion (walking, stepping, crawling, and running)
❑ Non-locomotion (balance and body sway)
❑ Manipulative skills (throw, catch, squeeze)
ROWING CONSIDERATIONS
• Lumbar spine injuries more common among men and chest/rib injuries among
women .
• Back extension movement produces 1/3 of the power during rowing stroke
(Wolf, 2020). Considerations: develop leg and hip power to manage the
imbalances.
• Maintenance of hamstring length is key to minimizing low back pain.
• Posterior hip dominant exercises such as loaded hip bridges can help manage
the pelvic rotations that occur between the catch and drive phase

QUICK FUNCTIONAL SCREENTHE FOLLOWING 5 TESTS WILL HELP GIVE YOU A WINDOW INTO YOUR
MOVEMENT

1. CLOSED CHAIN ANKLE DORSIFLEXION
Normal = 4 inch distance from the wall. (3-5 inches range)
1. Without wearing shoes, stand facing a wall with the foot pointed at the wall.
2. Keeping the midline of the kneecap in line with the midline of the foot and the heel on the floor, bend the knee and ankle until the knee touches the wall.
3. Repeat till you reach the maximum distance.
(Cressey, Hartman, and Robertson, 2009)

WHY DO WE CARE ABOUT ANKLE DORSIFLEXION?
• Restrictions at the ankle lead to knee pain.
• An immobile ankle causes the stress of landing to transfer to the
knee.
• Ankle restriction can affect squat mechanics for on land training.
• Ankle restriction can affect the catch phase of rowing – leading to
splayed legs, raised heels, or excessive lumbar flexion to compensate.
• Can lead to knee pain, ankle pain, and shin pain.
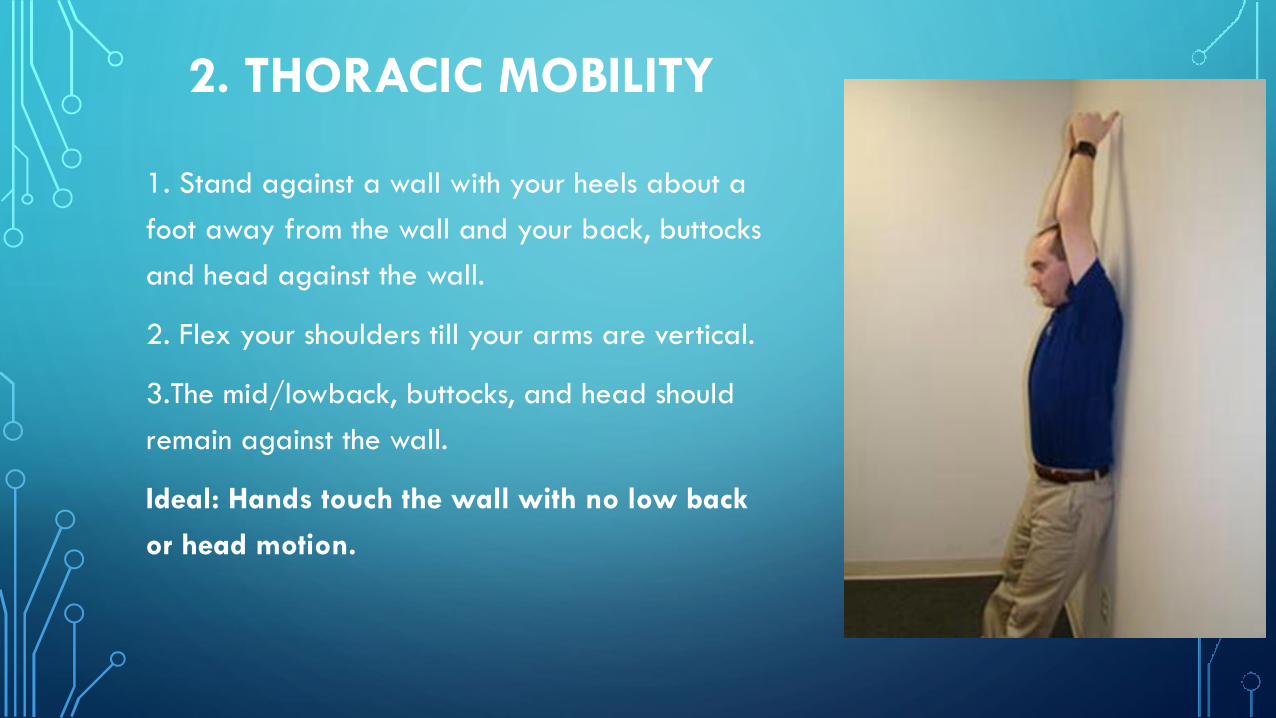
2. THORACIC MOBILITY
1. Stand against a wall with your heels about a
foot away from the wall and your back, buttocks
and head against the wall.
2. Flex your shoulders till your arms are vertical.
3.The mid/lowback, buttocks, and head should
remain against the wall.
Ideal: Hands touch the wall with no low back
or head motion.
WHY DO WE CARE ABOUT THORACIC MOBILITY?
• Restrictions at the thoracic spine can lead to low back pain.
• Can lead to excessive rounding during the stroke at the recovery and catch
(over-reaching at the catch).
• Hunchback posture – increases stress on the anterior side of the spine.
• Inconsistent handle heights – the inability to reach thoracic extension or
maintain a neutral thoracic spine under load causes uneven handle heights
and difficulty of a “soft hands” approach at the catch due to excessive over-
reaching as the rower is more rounded (they think they are neutral)
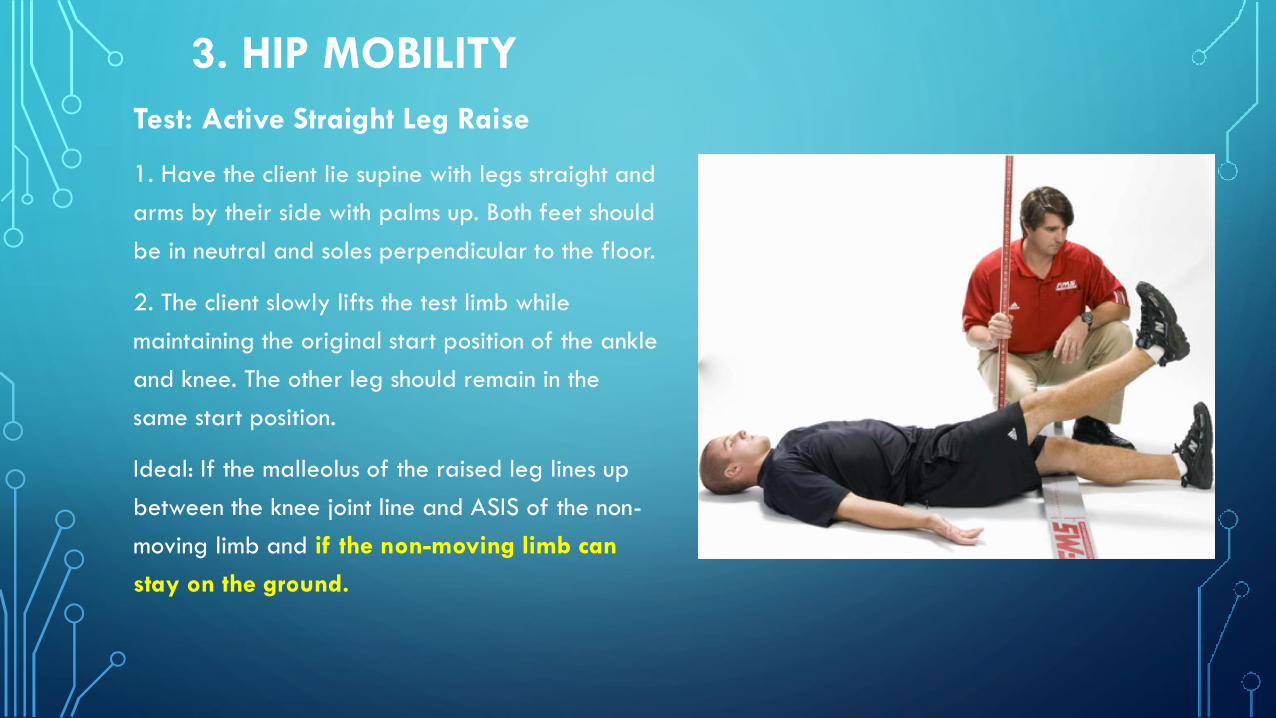
3. HIP MOBILITY
Test: Active Straight Leg Raise
1. Have the client lie supine with legs straight and
arms by their side with palms up. Both feet should
be in neutral and soles perpendicular to the floor.
2. The client slowly lifts the test limb while
maintaining the original start position of the ankle
and knee. The other leg should remain in the
same start position.
Ideal: If the malleolus of the raised leg lines up
between the knee joint line and ASIS of the non-
moving limb and if the non-moving limb can
stay on the ground.
HIP MOBILITY
Why do we care?
When hip mobility is deficient the lumbar spine or knee will compensate leading to
low back pain or knee pain.
You may see:
- Back arching from an anterior pelvic tilt
- Knee valgus
- Poor Gluteus function (next test)
- Slack hamstrings
- Tight hip flexors =anterior pelvic tilt = poor gluteus function/slack
hamstrings/excessive low back arch which leads to an inability to sit up in the boat.
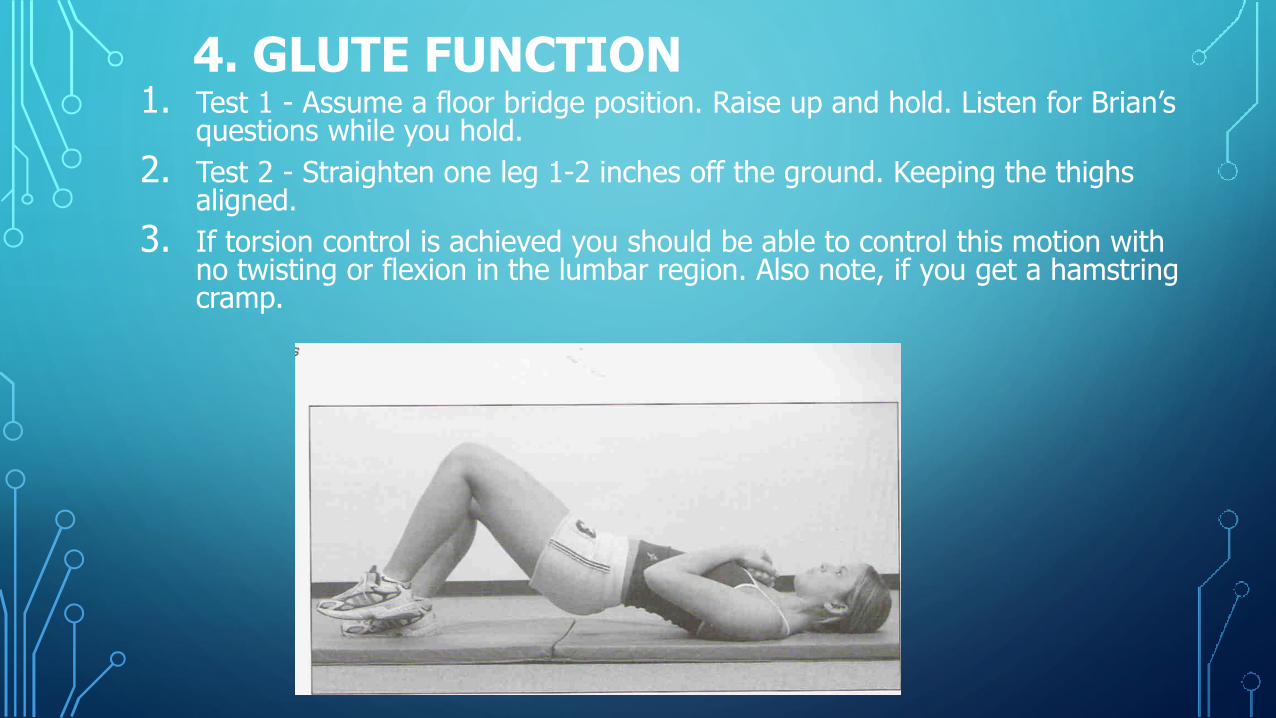
4. GLUTE FUNCTION1. Test 1 - Assume a floor bridge position. Raise up and hold. Listen for Brian’s
questions while you hold.
2. Test 2 - Straighten one leg 1-2 inches off the ground. Keeping the thighs aligned.
3. If torsion control is achieved you should be able to control this motion with no twisting or flexion in the lumbar region. Also note, if you get a hamstring cramp.
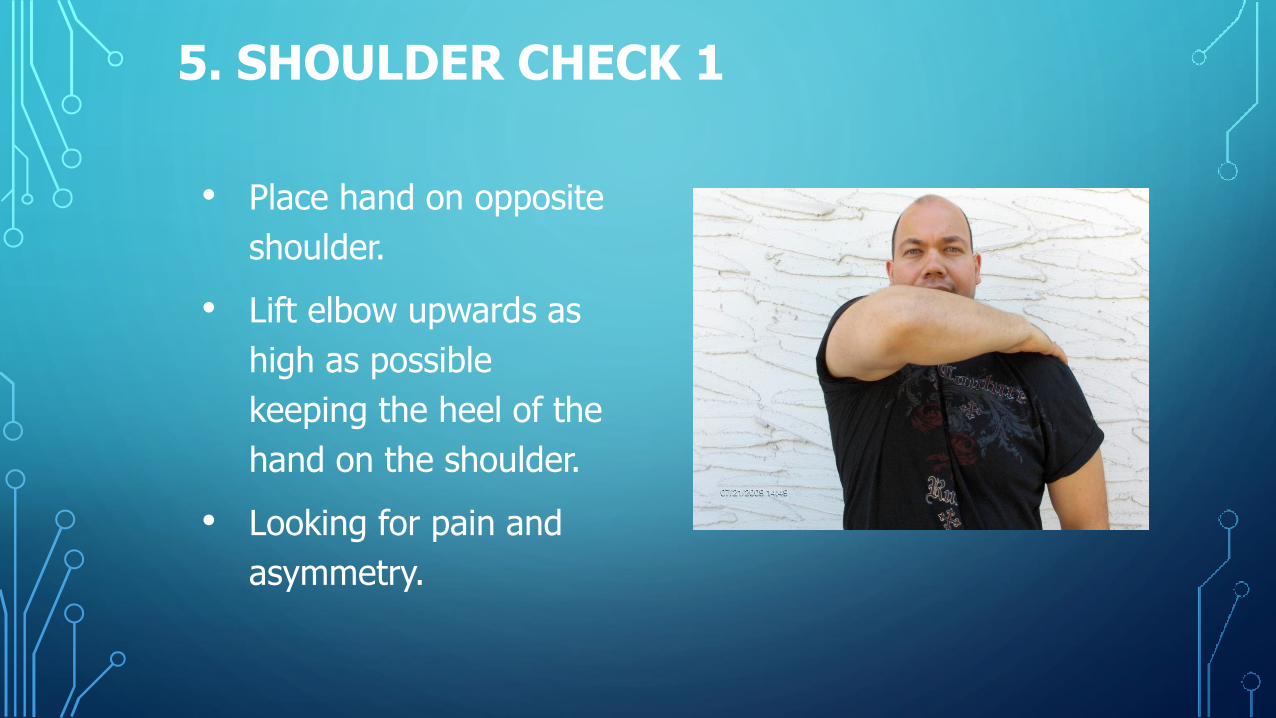
5. SHOULDER CHECK 1
• Place hand on opposite
shoulder.
• Lift elbow upwards as
high as possible
keeping the heel of the
hand on the shoulder.
• Looking for pain and
asymmetry.
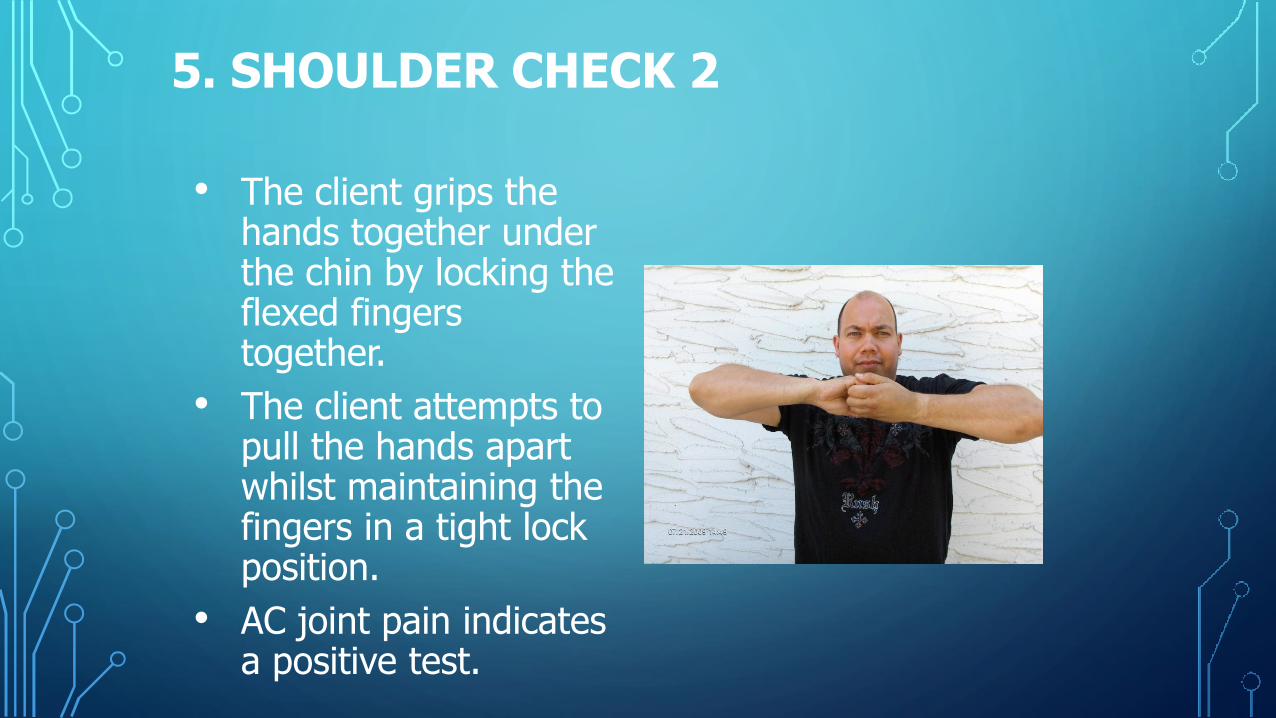
5. SHOULDER CHECK 2
• The client grips the hands together under the chin by locking the flexed fingers together.
• The client attempts to pull the hands apart whilst maintaining the fingers in a tight lock position.
• AC joint pain indicates a positive test.
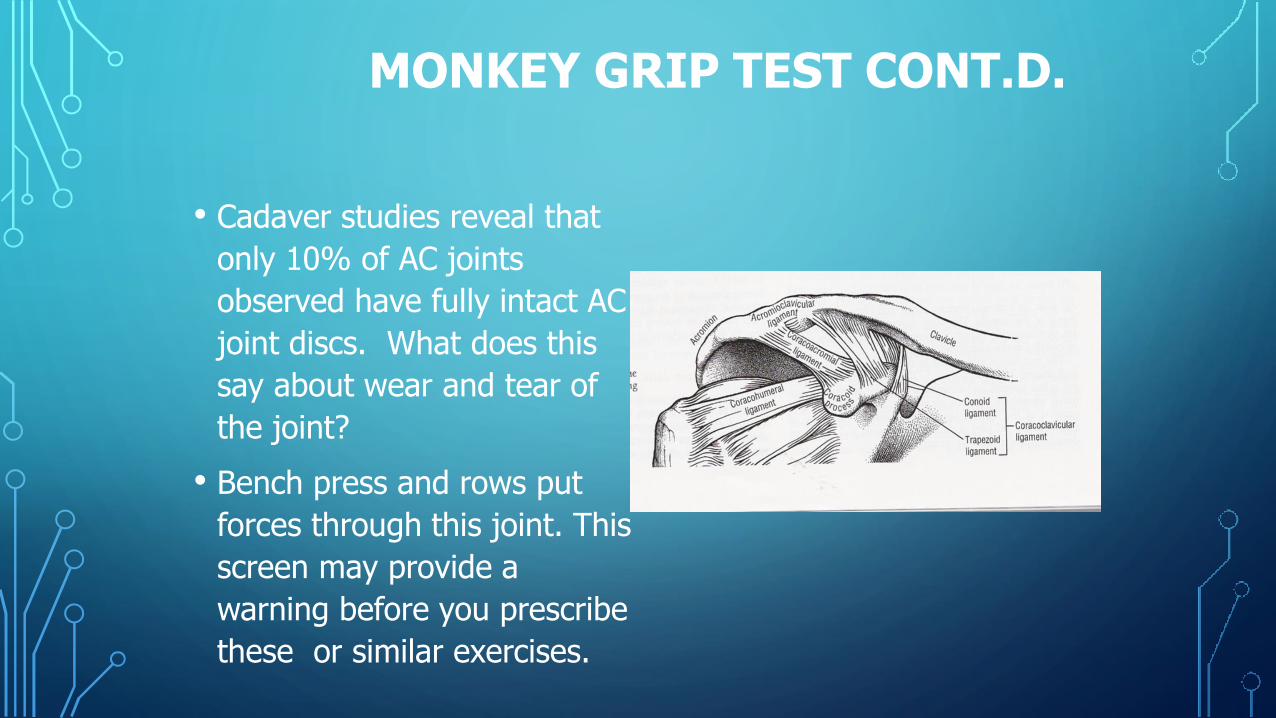
MONKEY GRIP TEST CONT.D.
• Cadaver studies reveal that
only 10% of AC joints
observed have fully intact AC
joint discs. What does this
say about wear and tear of
the joint?
• Bench press and rows put
forces through this joint. This
screen may provide a
warning before you prescribe
these or similar exercises.

ANY QUESTIONS?