what gold standard for rifampicin testing?: the future of molecular testing tag meeting, manila,...
TRANSCRIPT

What Gold Standard for What Gold Standard for Rifampicin Testing?:Rifampicin Testing?:
the future of molecular testingthe future of molecular testing
TAG Meeting, Manila, 9-12 December 2014
Richard LumbMycobacterium Reference Laboratory, SA Pathology
Adelaide, South Australia
Plan of Presentation
• Introduction• Molecular concepts regarding rifampicin and resistance • Does DST methodology matter?• Frequency of discrepant results
– false-resistance– false-susceptibility
• Does low-level rifampicin resistance matter?• Extraordinary claims require extraordinary evidence• Resistance and other gene mutations• Implications for Programs• Concluding comments
Introduction
• Amplification of drug resistance is caused by human activity
• Mycobacteria genes have a low (≈10-6-10-8) level of spontaneous mutation– Any mycobacterial population will have a small
number of organisms naturally drug resistant and usually with resistance to a single drug
– Inadequate anti-TB regimen provides selection pressure for drug resistant strains to amplify and become the dominant strain
• MDR/XDR-TB is the step-wise accumulation of mutations; is not achieved in a single mutation
Molecular Concepts of Rifampicin Resistance
• Rifampicin resistance arises due to mutation(s) in the gene (rpoB) encoding the β-subunit of RNA polymerase– Rifampicin physically blocks RNA synthesis– Mutations reduce affinity for the rifampicin binding site
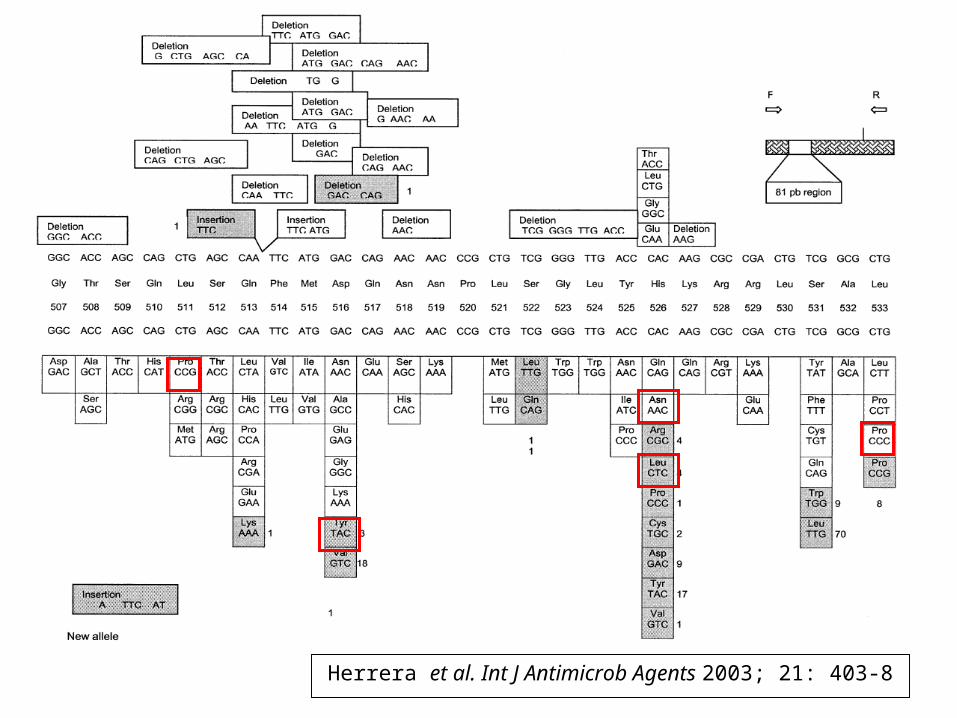
≈ 97% of mutations associated with rifampicin resistance occur within an 81bp ‘hotspot’ region
– Also known as rifampicin-resistant determining region or RRDR
• Codons 507-533
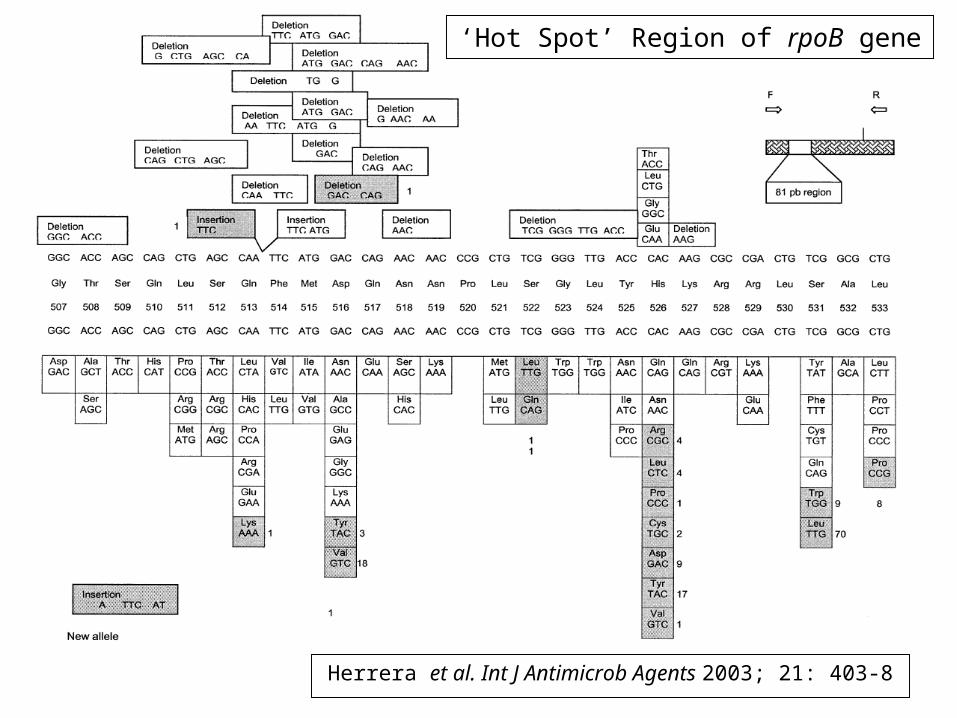
Herrera et al. Int J Antimicrob Agents 2003; 21: 403-8
‘Hot Spot’ Region of rpoB gene
Molecular Concepts of Rifampicin Resistance
• Phenotypic testing for rifampicin considered to be very reliable; until now…
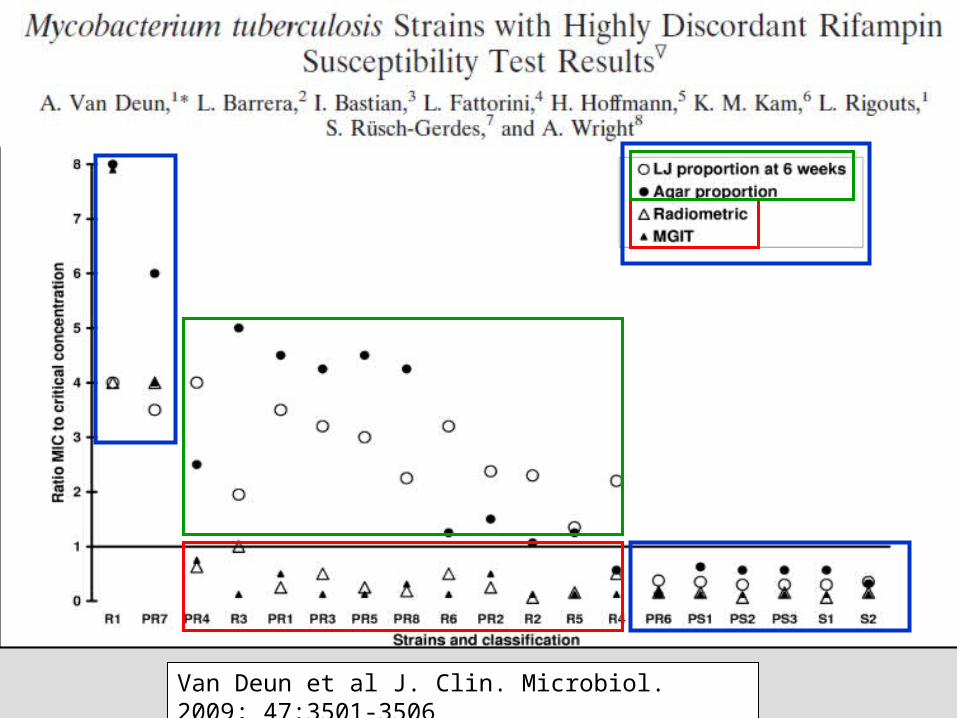
Does DST Methodology Matter?• Research revealed a subset of isolates with
highly discordant RIF results
Van Deun et al J. Clin. Microbiol. 2009; 47:3501-3506
Van Deun et al J. Clin. Microbiol. 2009; 47:3501-3506
Does DST Methodology Matter?
Rigouts et al J. Clin. Microbiol. 2013; 51:2641-2645
Does DST Methodology Matter?
• Phenotypic testing misidentifies isolates with low-level RIF resistance as susceptible
• Xpert MTB/RIF and Line Probe Assays both detect mutations associated with RIF-resistance
• Associated with specific mutations– 511Pro, 516Tyr, 526Asn, 533Pro, 572Phe & likely
other rare mutations• Liquid culture much more likely to miss such
mutations than solid media DST• False-susceptibility in liquid culture
[Rigouts et al JCM 2013;51:2641-2645] [Van Deun et al JCM 2009;47:3501-3506]
–
Herrera et al. Int J Antimicrob Agents 2003; 21: 403-8
Frequency of Discrepant Results
• How frequently does low-level RIF-resistance occur?
Van Deun et al J. Clin. Microbiol. 2013; 51:2633-2640
Frequency of Discrepant Results
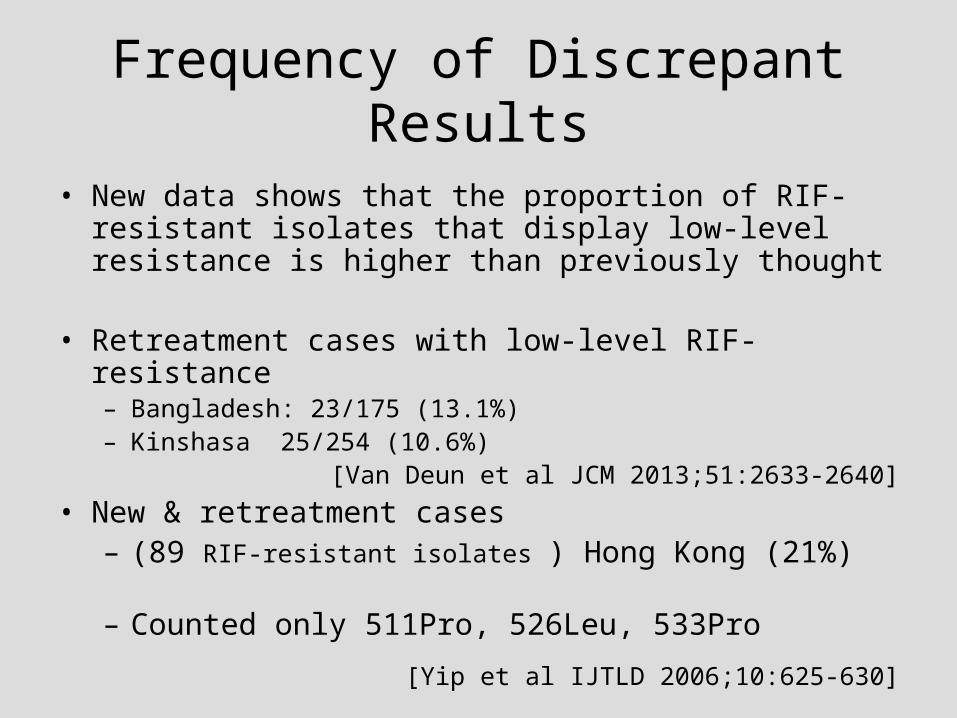
• New data shows that the proportion of RIF-resistant isolates that display low-level resistance is higher than previously thought
• Retreatment cases with low-level RIF-resistance– Bangladesh: 23/175 (13.1%) – Kinshasa 25/254 (10.6%)
[Van Deun et al JCM 2013;51:2633-2640]
• New & retreatment cases– (89 RIF-resistant isolates ) Hong Kong (21%) – Counted only 511Pro, 526Leu, 533Pro
[Yip et al IJTLD 2006;10:625-630]
Frequency of Discrepant Results Molecular False-Resistance
• Silent mutations– Mutation results in a base change but no change to
the amino acid encoded and no change to protein structure
– Change will not be detected phenotypically– Are detected by molecular testing
• Frequency of silent mutations varies– <0.5% by Van Deun et al 2013– <1% in TBPANNET (Italy) Cirillo (GLI-2014)
Frequency of Discrepant Results Molecular False-Susceptibility
• Mutations occurring within the rpoB gene but outside the ‘hot spot’– ‘Hot spot’ covers codons 507-533– Rare mutations occurring outside ‘hot spot’
• 535Ser and 536Ser (<1%)• 572Phe (≈2%)• Likely to be others
Does low-level RIF-resistance matter?
[Williamson et al IJTLD 2011;16:216-220]
3/3 patients with low level RIF-resistance failed Cat-1
Does low-level RIF-resistance matter?
Pang et al IJTLD 2014;18:357-362
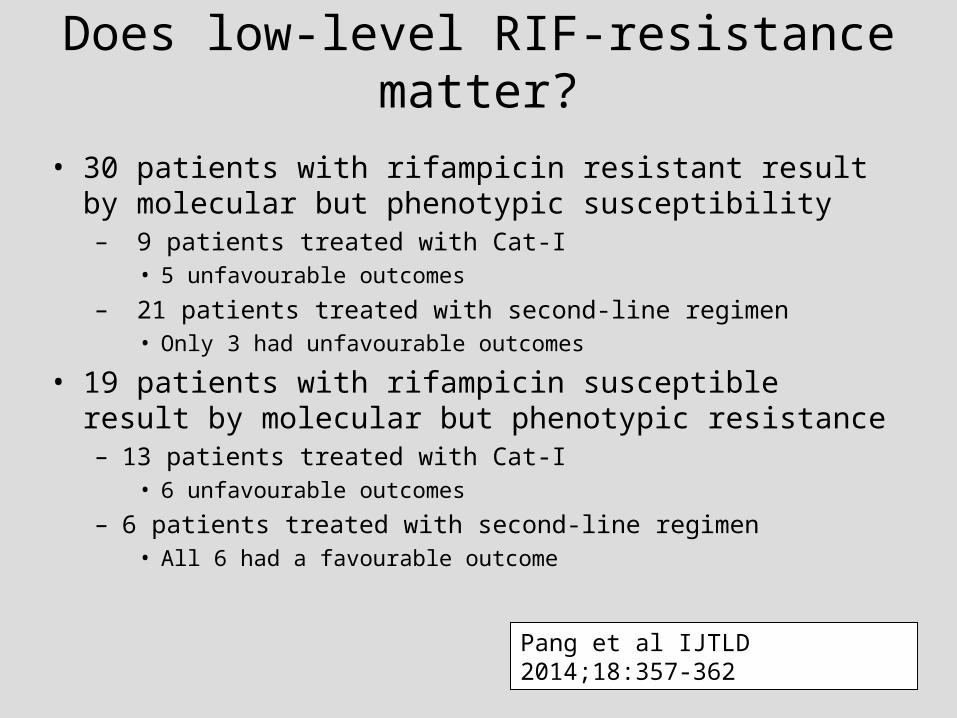
Does low-level RIF-resistance matter?
• 30 patients with rifampicin resistant result by molecular but phenotypic susceptibility – 9 patients treated with Cat-I
• 5 unfavourable outcomes
– 21 patients treated with second-line regimen• Only 3 had unfavourable outcomes
• 19 patients with rifampicin susceptible result by molecular but phenotypic resistance– 13 patients treated with Cat-I
• 6 unfavourable outcomes
– 6 patients treated with second-line regimen• All 6 had a favourable outcome
Pang et al IJTLD 2014;18:357-362
Does low-level RIF-resistance matter?
• Globally, an additional 37,000+ MDR-TB/year go unrecognised!
Williamson et al IJTLD 2011;16:216-220
NASA scientist 'finds alien fossils on meteorite' [1996]
“Extraordinary claims require extraordinary evidence”
Carl Sagan (Cosmologist)
Extraordinary Claims Require Extraordinary Evidence
• Multiple examples where a reported ‘MDR-TB’ (or worse) actually MTB plus environmental mycobacteria or MTB plus non-mycobacteria contaminant…
• High income/low TB prevalent countries and with high quality laboratories– E.g-1: Thought to have XDR but only had MDR-TB…– E.g-2: Diagnosed with XDR-TB but was subsequently found to be
INH-resistant MTUB plus MAC…
• Cryptic environmental mycobacteria a higher risk in liquid culture DST than in solid media DST
• MDR/XDR-TB result has potentially life-changing implications for the patient, family and community
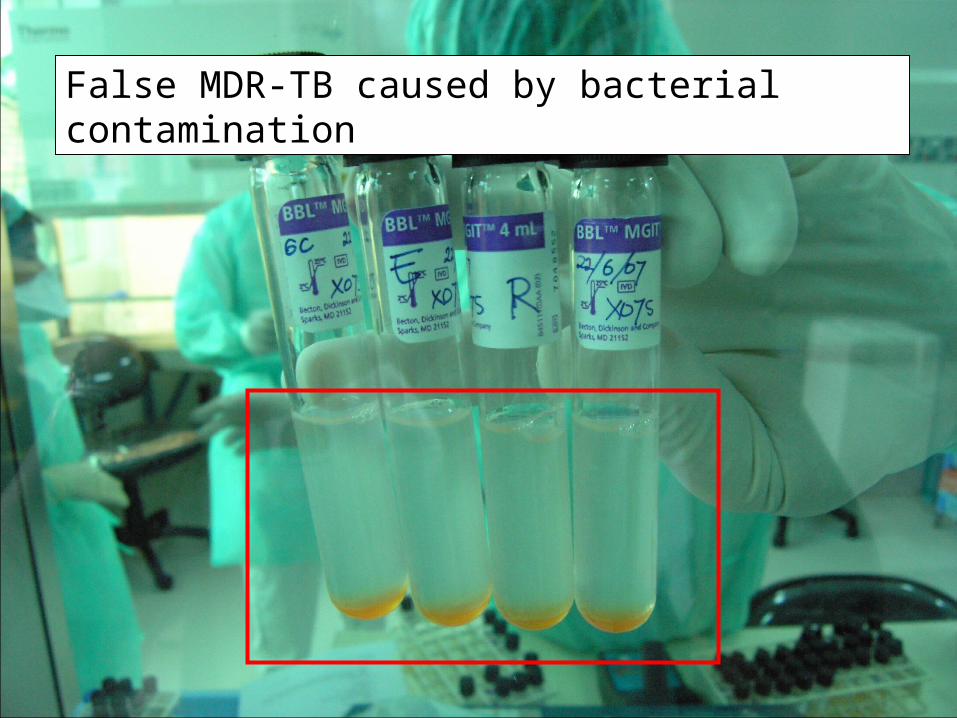
False MDR-TB caused by bacterial contamination
Resistance and Other Gene Mutations
• Mutations associated with resistance incompletely understood– Mutations in pncA have strong association with
pyrazinamide resistance• Sensitivity 80-90% of molecular with phenotypic
– InhA and katG mutations associated with 70-90% of INH resistance but varies between- and within- countries
– EmbB codon 306 mutations found in 30-68% of ethambutol-resistant strains
– Some mutations associated with resistance to second-line anti-TB drugs recognised but incomplete
Implications for Programs
• Molecular testing beyond Xpert and LPA is the future– More mutations associated with drug resistance are
being defined– Countries need to be planning/developing extended
molecular capacity for TB diagnostics– Whole Genome Sequencing (WGS) a reality and
being used now as a diagnostic tool for TB• Price/test falling very fast• Capacity of new machines increasing quickly• Bioinformatics presents a bigger challenge• Multiplatform capacity
– Rapid/reliable specimen/isolate shipment strategy
Concluding Remarks - 1
• Mutations within rpoB exert variable effects upon results obtained by phenotypic DST
• The effect of a mutation within rpoB upon the rifampicin MIC depends upon – the amino acid change induced by the mutation– location of the mutation in the rpoB gene
• Low-level (borderline) resistance to rifampicin is strongly associated with treatment failure when a standard first-line treatment regimen in used
• Detection of mutations in the rpoB gene, and especially within the ‘hot spot’, correlate better with treatment outcome
Concluding Remarks - 2
• Sequencing the entire rpoB gene may give the best correlation with treatment outcome
• Countries will require molecular capacity that goes beyond Xpert and Line Probe Assays – Technology, training, and gaining ‘hands-on’
experience must be part of National Strategic Plans• Must be included in funding cycles
– Will change country requirements for DST laboratories
– For fast turnaround, rapid, safe, and reliable specimen/isolate shipment strategies to higher-level laboratories is vital

Is the sun setting on phenotypic DST testing…?