what are the fundamental - sitcancer.org
TRANSCRIPT


What are the fundamental properties of curative anti-
tumor T cells?
Nicholas P. RestifoSITC
November 6, 2015
NIH Center for Regenerative
Medicine

Khajah, Int J Oncol, 2015
Surgery, radiation, and chemotherapy / targeted therapy can rapidly kill tumor cells but these modalities can fail to cure in the setting of metastatic
solid tumors . . .

Cancer Immunotherapy: Delayed gratificationAll patients (n=25) in TIL + TBI 12 Gy + HD IL-2
Months

Months
Cancer Immunotherapy: Delayed gratificationAll patients (n=25) in TIL + TBI 12 Gy + HD IL-2
Tumor rejection can be slow . . .
. . . but it can be complete and durable

Patterns of response to Ipilumumab in 4 patients with melanoma
Wolchok, et al, Clin Cancer Res, 2009

% persistence of the infused cells in peripheral blood
* CR + PR vs. NR < 0.001
T cell persistence at 1 month is highly correlated with objective clinical response
Rosenberg SA et al. Clin Cancer Res, 2011
25
14
1.5
Complete tumordestruction
> 30% tumordestruction
< 30% tumordestruction
Patient response status
0 40 60 80 10020
0
50
100
150
200
250
300
350
400
0 20 40 60 80
Tum
or S
ize
(mm
2)
Days post ACT
NT
Pcis-/- aCD8 D38
Pcis-/- aIgG D38
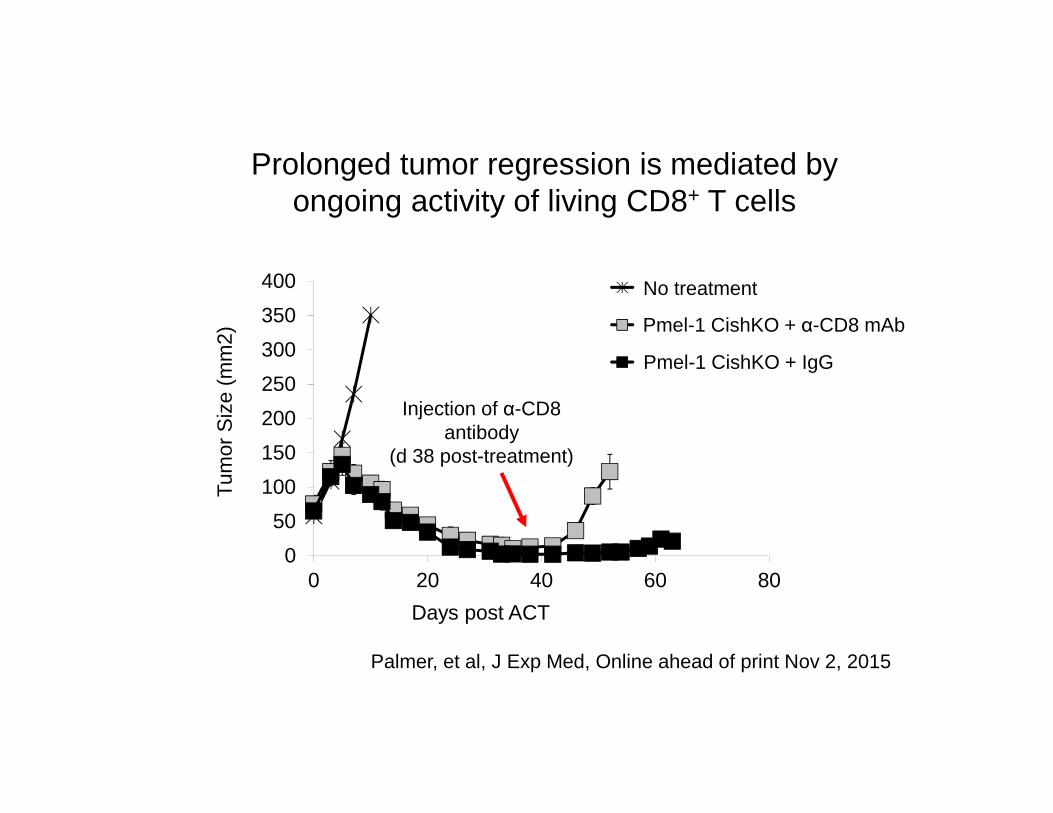
Prolonged tumor regression is mediated by ongoing activity of living CD8+ T cells
Injection of α-CD8 antibody
(d 38 post-treatment)
Pmel-1 CishKO + α-CD8 mAb
No treatment
Pmel-1 CishKO + IgG
Palmer, et al, J Exp Med, Online ahead of print Nov 2, 2015

How do we achieve the persistence of memory?


Effector function/CytoxicityGlycolytic metabolism
Senescence
Anti-tumor activityProliferative capacityStemness/Persistence
Increasing cellular differentiation; decreasing anti-tumor effectiveness after ACT
Stem cell-like capacity for each persisting T cell clonotype
Adapted from Restifo, Blood, 2014; Gattinoni, et al, Nat Med, 2009 & 2011
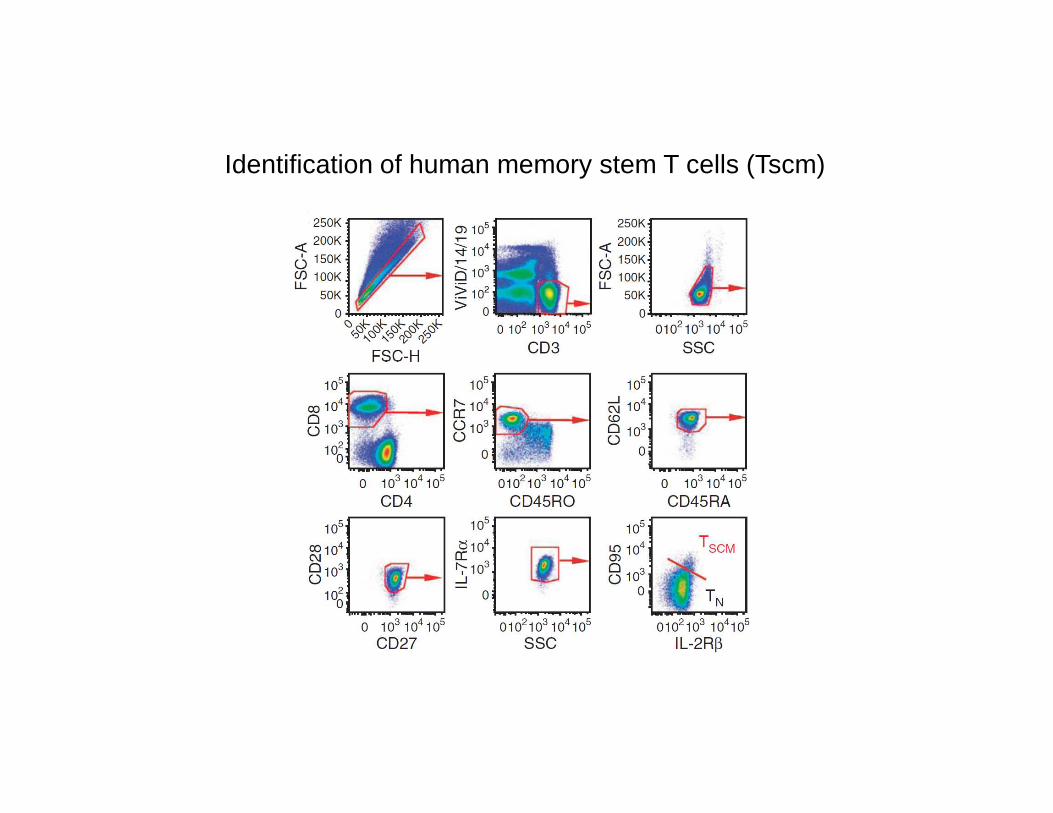
Identification of human memory stem T cells (Tscm)


Measuring mitochondrial membrane potential (∆ψm) in individual living cells using tetramethyl rhodamine methyl ester (TMRM)
∆ψm
Sukumar, Cell Metabolism, In Press

Measuring mitochondrial membrane potential (∆ψm) in individual living cells using tetramethyl rhodamine methyl ester (TMRM)

A low mitochondrial membrane potential marks self-renewing hematopoietic stem cells
Long-term reconstitutionIn lethally irradiated hosts
LT-HSC (Lin - c-kit + Sca+) (0.75% of population)Congenically labeled with CD45.1
cKit
Sca1TMRM

CD45.2 (competitor total bone marrow cells)
CD
45.1
(so
rted
for ∆ψ
m)
39 5
51 91
Low ∆ψm High ∆ψm
Low mitochondrial membrane potential marks self-renewing hematopoietic stem cells
Transplantation into lethally irradiated recipients (CD45.2) using: -- 300 CD45.1 (low or high membrane potential) Lin- Sca1+ c-Kit+ cells along with
-- 3 X105 CD45.2 competitor total bone marrow cells (CD45.2)
Reconstitution of host lymphocytes

Adoptive transfer into irradiated C57BL/6
rVV hgp100 challenge
Pmel TCR transgenic
spleen
Hgp100peptide
Phenotype and function of
CD8+ T cells
High∆ψ
Low∆ψ
CD44 CD69CD27 IL7Rα KLRG1
CD8-Naive Low ∆ψ High ∆ψ
Characterization of CD8+ T cells sorted based on ∆Ψm
TMRM

RNA-seq ‘volcano plot’ of cells sorted based on mitochondrial membrane potential

CD
8+T
hy-1
.1+
T c
ells
(10
6 )
Time after transfer (days)
Bcl6 Tcf7 Lef1 Klf2
Prdm1 Eomes Prf1 GzmbE
xpre
ssio
n re
lativ
e to
Act
-b(1
03)
Low ∆ψ High ∆ψHigh ∆ψLow ∆ψ
0 5 10
0
4
8
12
******
**
Mitochondrial membrane potential (∆ψm) segregates short-lived effector from memory T cell precursors

Low ∆ψ High ∆ψ
% P
ersi
sten
ce C
D8+
Thy
1.1+
0.01
0.1
1
10
100 *
Thy
1.1
SSC
High ∆ψ
Low ∆ψ
Low ∆ψm CD8+ T cells demonstrate increased long-term in vivo persistence (300 days)

∆ψm segregates long-lived memory T cells from short-lived effectors in vivo after infection
CD
44
CD62L
TSCM
TCMTEM

Low ∆ψm cells identify ‘metabolically fit’ T cells within sorted populations of TCM and Tc17

0.4 0.1
0.299.2
4.0 3.5
8.084.4
6.4 15.7
33.244.8
IFN
-γ
IL-17A
SS
C
IFN-γ
IL17
-F
IL-17A
Low ∆ψm High ∆ψm
% IL
-17A
+
CD
8+ T
cel
ls%
IL-1
7A+
CD
4+ T
cel
ls%
IFN
-γ+
CD
4+ T
cel
ls
Unstim0.4 0.0
0.399.3
1.3 0.3
24.174.4
0.1 0.3
74.325.2
58.914.62.5
Tc17
Th1
Th17
Low ∆ψHigh ∆ψm
High-∆Ψm is associated with effector cytokine production in T cells
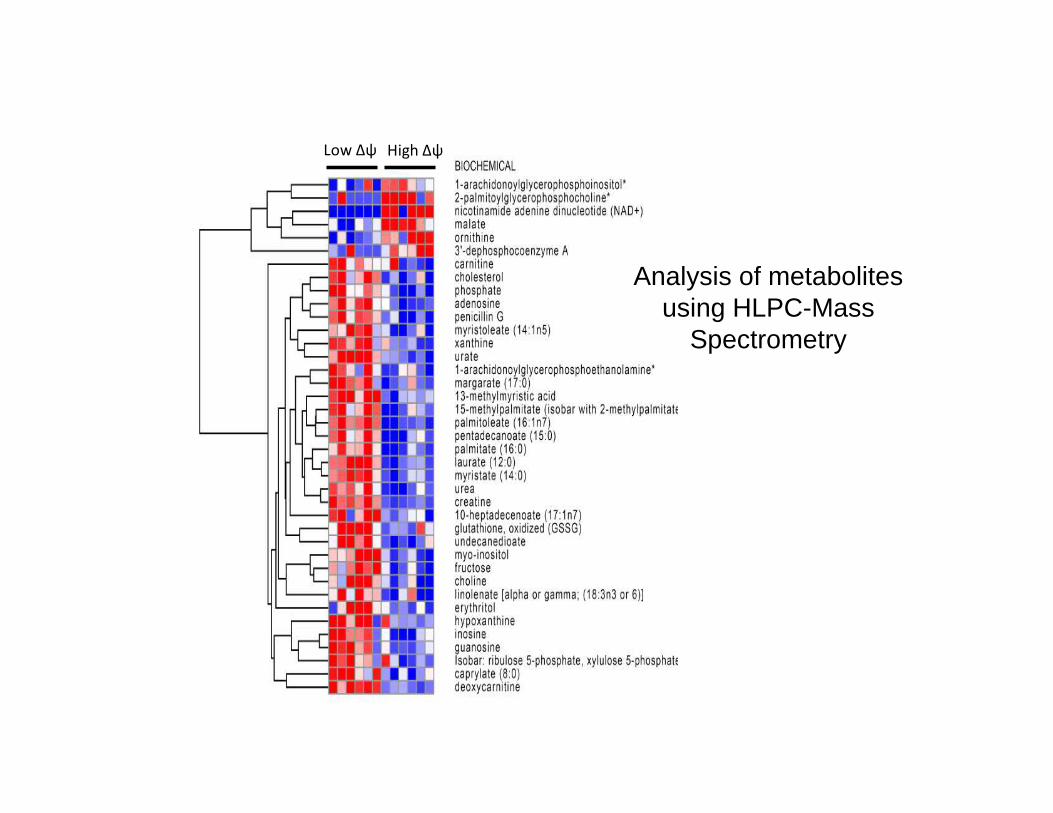
Analysis of metabolites using HLPC-Mass
Spectrometry
Low Δψ High Δψ

Low ∆ψm cells display increased fatty acid metabolites
carnitineacetyl
carnitinedeoxy
carnitine
palmitate palmitoleate margarate
linolenate caprylate laurateSca
led
Inte
nsity
Low Δψ
High Δψ

Low ∆ψm cells display a metabolic profile of memory CD8+ T cells
EC
AR
(m
M/p
H)
Exp
ress
ion
rela
tive
to A
ct-b
(10
3 )
Cpt1a Slc2a1
Basal ExtracellularAcidifcation Rate
Low ∆ψ High ∆ψ

Low ∆ψm cells display a metabolic profile of memory CD8 + T cells

Low ∆ψm CD8+ T cells control established tumor even when sorted from an established T cell culture
**
High ∆ψ
Low ∆ψ
No Treatment

Low ∆ψm CD8+ T cells demonstrate increased autoimmune vitiligo
Low Δψm High Δψ

Low ∆ψm cells:
1. Are more stem cell-like
2. They burn fats not glucose
3. They have more spare respiratory capacity
4. The persist longer
5. They control established tumor better
High ∆ψm cells make more cytokines, but why do they die?

CD8+ T cells with low ∆ψm have decreased checkpoint

CD8+ T cells with low ∆ψm have decreased levels of reactive oxygen species (ROS)
DCFDA is a cell-permeable non-fluorescent probe. 2′,7′-Dichlorofluorescin diacetate is de-esterified intracellularly and turns to highly fluorescent 2′,7′-dichlorofluorescein upon oxidation.
DC
FD
A
Bulk CD8 TCM Tc17 Th1 Th17 LT-HSC
Low ∆ψm High ∆ψm

High ∆ψm CD8+ T cells display increased DNA damage
Stain for γ-H2AX, a marker for dsDNA breaks

High ∆ψm CD8+ T cells elevated levels of biomarkers of ‘physiological age’
Cdkn1a Cdkn2a
Exp
ress
ion
rela
tive
to A
ct-b
(103
)
Low ∆ψm
High ∆ψm
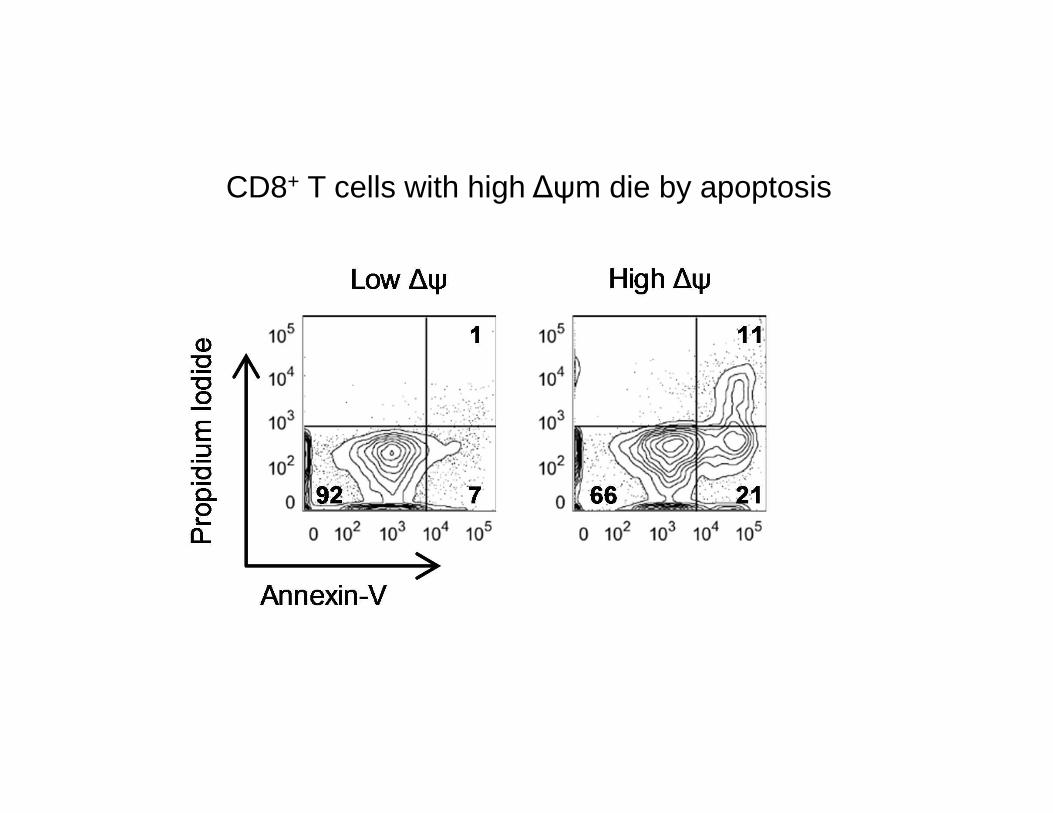
CD8+ T cells with high ∆ψm die by apoptosis

� Low ∆Ψm CD8+ T cells demonstrate long-term in vivopersistence and superior anti-tumor activity
� Low ∆Ψm T cells display metabolic signature of memory CD8+ T cells
� High-∆Ψm is associated with effector cytokine production in T cells, followed by DNA damage, senescence and death.
� Low ∆Ψm identifies metabolically fit cells among HSC and CD8+ TCM subsets
SUMMARY

THE VISION: What is required to bring cell-based therapies to the many patients who need them?
1. Concerted commitment to basic science.2. Concerted effort to create vector and cell production
laboratories for patients.3. Robust technology transfer: open sourcing & industrial
partners.

Restifo Lab:Past and present
Madhu SukumarRahul RoychoudhuriDouglas C PalmerChristopher A. KlebanoffNick AcquavellaJoe CromptonNick KlemenTori YamamotoZhiya YuRobert EilJenny PanShashank PatelDavid CleverGautam MehtaRaul VizcardoLinda TranDevi Gurusamy
Toren Finkel:Jie Liu
Leonard Lab:Warren LeonardRosanne SpolksiPeng Li
David Stroncek:Franco MarincolaEna Wang
Richard Siegel:Madhu RamaswamyAnthony C. Cruz
Luca Gattinoni:Luca GattinoniYun Ji
NIH Pharmacy:George GrimesGopal Poti
Clinical Team:Udai KammulaRick SherryStephanie GoffPaul RobbinsSteve FeldmanRobert SomervilleSteve Rosenberg
James Yang:Ken-ichi HanadaQiong Wang
Rosenberg Lab:Eric TranAlena Gross
John O’Shea:Golnaz VahediVittorio Sartorelli
Francis Collins:Stephen C. J. Parker
Larry Samelson:Lakshmi Balagopalan
