wake county human services and environmental …€¦ · wake county human services and ... mr. tim...
TRANSCRIPT

1 of 3
www.wakegov.com
Wake County Human Services and Environmental Services Board
June 28, 2012 AGENDA
Human Services Ctr. - 220 Swinburne St. 2nd Fl., Rm. 2132
Standing Time: 7:30AM – 10:00AM Dianne Dunning, Chair
Pablo Escobar, Vice Chair
Purpose: Advocacy, Policy, Advisory, Accountability
All items on the Consent Agenda are considered to be routine and may be enacted by one motion. If a Board Member requests discussion on an item, the item will be removed from the Consent Agenda and considered separately.
7:35 am Human Rights/Consumer Affairs: Mr. Pablo Escobar, Chair Studies:
1. Latent Tuberculosis Infection - TBTC Study 33
2. NOVIOlencia - Latino Families for Safe Dates
Regional Networks Development Committee: Mr. Frank Eagles, Chair
7:40 am • Update on Regional Networks Committee Work Plan
7:45 am Overview of Wake County Transit Plan - Mr. Tim Maloney & Mr. Tim Gardiner, Wake County Planning, Development & Inspections
8:10 am Update on New Composition for Human Services Board - Ms. Denise Foreman, Assistant to the County Manager
7:30 am Meeting Called to Order
Invocation
Approval of Minutes: May 24, 2012
Next Board Meeting: July 26, 2012 220 Swinburne St., 2nd Fl., Rm. 2132
Consent Agenda
Regular Agenda

2 of 3
8:30 am LME Advisory Committee: Ms. Stephanie Treadway, Chair
• Update on Wake LME Closeout and Recent Actions by Wake County Commissioners re: Alliance Behavioral Healthcare (MCO) - Ms. Denise Foreman
• Update on Wrap Up Committee Meeting & History/Recognition - Ms.
Stephanie Treadway
Executive Committee: Dr. Dianne Dunning, Chair
8:45 am Recognition of Departed Board Member: --Mr. James B. Edgerton: January 19, 2010 - March 22, 2012
8:55 am FY12 - Q3 WCHS Data Report - Ms. Regina Petteway & Ms. CJ Harper
Public Health Committee: Mr. Benny Ridout, Chair
9:05 am • Review/Discuss Public Health Quarterly Report (Jan.-Mar. 2012) - (#2.4)
9:15 am HS&ES Directors' Q & A --Ongoing Activities
9:30 am Chair's Report
9:40 am Time Reserved for Input into WCHS Director's Annual Performance Evaluation Note: The Board may choose to go into closed session to provide input.
10:00 am Adjournment
Information Packet Items

3 of 3
Human Services Mission Statement
Wake County Human Services in partnership with the community will anticipate and respond to the public health, behavioral health and the economic and social needs of Wake County residents. We will coordinate and sustain efforts that assure safety, equity, access and well-being for all. - December 2006 _____________________________________________________________________________
Environmental Services Mission Statement
To protect and improve the quality of Wake County’s environmental and ensure a healthy future for its citizens through cooperation, education, management and enforcement. Environmental Services combines:
• water quality
• air quality
• solid waste (recycling, landfills, etc.)
• environmental health and safety (sanitation inspections, pest management, swimming pool regulations, animal control)
________________________________________________________________
FY 2011 Board’s Top Six Priorities:
#1 Prevent Child Abuse and Support Families
#2 Housing for Vulnerable Populations
#3 Obesity Prevention and Nutrition
#4 Access to Mental and Physical Health Services
#5 Protect Wake County’s Water Resources
#6 Human Capital Development (added 10/28/10)

Human Services and Environmental Services Board Quarterly Meeting Schedule
July 2012
SunSunSunSun MondayMondayMondayMonday TuesdayTuesdayTuesdayTuesday WednesdayWednesdayWednesdayWednesday ThursdayThursdayThursdayThursday FridayFridayFridayFriday SatSatSatSat
1 2
BOC 2pm----
3 4 County
Holiday) 5 6
9am-10:30am Social Services, Rm. 5032
7
8
9 10 11 12
8am – 10am Bd. Executive
Cmte. Rm. 5032
13
11:30am – 1:30pm
Environmental Services – Library Admin., 4020 Carya Dr.
14
15 16
No BOC Mtg. ----
17
18
Board Packet
Distribution
19
3:30pm – 5:15pm - Housing
& Cmty. Revitalization, Rm. 5032
20
LME Human Rights
Subcommittee (moved to MCO) __________
Noon – 2pm
Public Health, Rex Women Ctr., Rm. 100C*
21
22 23
12:45pm – 2pm HRC – Rm.
5032
24 25 26
7:30am – 10am HS & ES
Board Mtg. Rm. 2132
27 28
29 30 31
August 2012
SunSunSunSun MondayMondayMondayMonday TuesdayTuesdayTuesdayTuesday WednesdayWednesdayWednesdayWednesday ThursdayThursdayThursdayThursday FridayFridayFridayFriday SSSSatatatat
1
2
3
9am-10:30am Social Services,
Rm. 5032
4
5
6 BOC 2pm----
7
8
9
8am – 10am Bd. Executive
Cmte. Rm. 5032 __________
10:00 am – Noon Regional Networks Cmte. Rm. 5040
10
11:30am – 1:30pm
Environmental Services – Library Admin., 4020 Carya Dr.
11
12
13
14
15
16
3:30pm – 5:15pm - Housing
& Cmty. Revitalization, Rm. 5032
17
Noon – 2pm
Public Health, Rex Women Ctr., Rm. 100B
18
19
20 BOC 2pm----
21
22
23
7:30am – 10am HS & ES
Board Mtg. Rm. 2132
24
25
26
27
12:45pm – 2pm HRC – Rm.
5032
28
29
30
31
September 2012
SunSunSunSun MondayMondayMondayMonday TuesdayTuesdayTuesdayTuesday WednesdayWednesdayWednesdayWednesday ThursdayThursdayThursdayThursday FridayFridayFridayFriday SatSatSatSat
1
2 3 (County Holiday)
4
BOC 2pm----
5 6 7
9am-10:30am Social Services,
Rm. 5032
8
9
10
11 12 13
8am – 10am Bd. Executive
Cmte. Rm. 5032
14
11:30am – 1:30pm
Environmental Services – Library Admin., 4020 Carya Dr.
15
16 17
BOC 2pm----
18
19 20
3:30pm – 5:15pm - Housing
& Cmty. Revitalization, Rm. 5032
21
Noon – 2pm
Public Health, Rex Women Ctr., Rm. 100B
22
23 24
12:45pm – 2pm HRC – Rm.
5032
25 26 27
7:30am – 10am HS & ES
Board Mtg. Rm. 2132
28 29
30

Assignments to Committees
Executive Committee 2nd Thursday 8am – 10am
Rm. 5032
Community and Public Health 3rd
Friday, noon Rex Women Ctr.
Environmental Services
2nd Fri., 11:30am, Library Admin. Carya Dr.
Social Services 1st Friday
9am – 10:30am Rm. 5032
Dianne Dunning Pablo Escobar Frank Eagles Leila Goodwin Melissa Jemison Paul Norman Benny Ridout Stephanie Treadway Staff: Regina Petteway Joe Durham Ramon Rojano Joseph Threadcraft Bob Sorrels
Benny Ridout Burton Horwitz Sharon Foster Staff: Michelle Ricci Sue Lynn Ledford Brent Myers, EMS Peter Morris Regina Petteway Andre Pierce Yvonne Torres Community: Laura Aiken Kevin Cain Barbara A. Hughes Anne McLaurin Leena Mehta Ann Rollins Heidi Swygard Penny Washington
Leila Goodwin Dianne Dunning Frank Eagles Benny Ridout Melissa Jemison Jeff Smith Staff: Joseph Threadcraft Sue Lynn Ledford Deborah Peterson Andre Pierce Matt Roylance Community: Rodney Dickerson Les Hall Glenn Harris Suzanne Harris Don Haydon Bryan Hicks Lana Hygh Buck Kennedy Jacob Reynolds Bob Rubin Henk Schuitemaker Paula Thomas Liz Turpin Kenny Waldroup Julie Wilkins Phillip White John Whitson
Paul Norman Burton Horwitz Julian Smith Staff: Katherine Williams Giang Le Liz Scott Natasha Adwaters Martha Crowley Vielka Gabriel Warren Ludwig Jenny Wheeler Community: Lisa Bireline David Cottengim Pam Dowdy Lisa Draper Dudley Flood Glenn Harsh Marjorie Menestres Rick Miller John Parker Bob Robinson Georgia Steele Lynn Templeton Cherie Thierrault Brandon Trainer Tracy Turner Angie Welsh April Womack Marc Zarate
Affordable Housing & Community
Revitalization 3rd Thursday
3:30pm – 5pm, Rm. 5032
Regional Networks
Development Qtrly, Rm. 5040
Human Rights/ Consumer Affairs
4th Mon., 12:45-2pm Rm. 5032
Melissa Jemison Dianne Dunning Staff: Annemarie Maiorano Bob Sorrels Community: Emmett Curl Steven Hess Michele Grant Teresa Piner José M Serrano Mark Shelburne Trace Stone-Dino Yolanda Winstead
Frank Eagles Benny Ridout Staff: Darryl Blevins Rosena West Ross Yeager Regina Petteway Staff: Matt Burton Sharon Brown Andre Pierce Bob Sorrels Community: Arsenio Carlos, ERC Rev. Lenwood Long, NRC Eugenia Pleasant, NRC Lunette Vaughan, SRC
Pablo Escobar Kent Earnhardt Osama Said Staff: Brian Gunter Leticia Mendez Fabiola Sherman Community: Laura Goddard Naima Moussa Martha Pitts Olivia Simons Don Wiseman
HUMAN SERVICES AND ENVIRONMENTAL SERVICES
BOARD AGENDA ITEM
Agenda Date: June 28, 2012
Committee/Item: Human Rights-Consumer Affairs
Specific Action Requested: Review and recommend for approval the attached proposals for
participation in human research proposals by Wake County clients and/or staff.
Item Summary: Attached are proposals for:
1-Participation by clients and staff of the Communicable Disease clinic in a new approach to
treating patients with Latent Tuberculosis Infection (LTBI), and
2-Recruitment of Wake County client parents and teens for a dating violence prevention program
aimed at Latino families.
Purpose for Action: Complete Wake County’s Institutional Review protocols for the protection
of human subjects in research.
Next Steps: TBD
Attachments: Summary Sheet, Study summary for TTBC iAdhere , Study summary for
NOVIOlencia, signed Research Approval Checklists, IRB review data
Opportunities for Advocacy, Policy or Advisory: These are both innovative preventive
proposals. The TTBC 33 Iadhere study aims to prevent the development and spread of TB by
patients whose infection is latent, but requires intervention. The NOVIOlencia proposal seeks to
fill a void for the Latino population because no dating violence prevention efforts have been
designed for these families prior to this effort.
Connections to Other Committees: Public Health









HUMAN SERVICES AND ENVIRONMENTAL SERVICES
BOARD AGENDA ITEM
Agenda Date: June 28, 2012
Committee/Item: Regional Networks Committee
Specific Action Requested: Receive information
Item Summary (Ex: What are major points/data. Is it better or worse.):
Regional Network Committee’s Work Plan for the coming fiscal year. Primary focus is the
development of a Western Regional Community Advisory Committee
Purpose for Action (Ex: Proposed Solutions/Accomplishments):
To define the scope and tenure of work for the Regional Network Committee for the coming fiscal
year
Next Steps (Ex: What is next step for Board or staff):
Receive information
Attachments: RNC Work Plan
Opportunities for Advocacy, Policy or Advisory:

Wake County Human Services and Environmental Services Board Action Planning Worksheet
Date 05/11/12
Priority: Western Region Service Plan Plan Period: 4 Year Plan; 1 Year Strategy
Objective: Establish a coordinated service plan for Western Region citizenry
Strategies/Action Steps Person(s) responsible
Timetable
Start Date Anticipated Completion
Completion
1. Make use of available data to identify opportunities for meeting
citizens’ needs through an array of service strategies and enhanced partnerships within the Western Region.
2. Foster engagement in an intentional manner. Identify and
assemble a Western Regional Community Advisory Committee with representation from existing as-well-as potential partner organizations, entities currently providing services/resources within the community, and local leaders.
Regional Networks Committee and Wake County Staff Regional Networks Committee and Wake County staff and leadership
07/01/12 07/01/12
06/30/13 06/30/13
Performance Indicators (What are the indicators that will let you know you’re meeting your objective?)
Tracking or measuring system (How will you track/account for progress?)
Resource Requirements (What is needed to deliver the expected results)
1.) Update Data within the Western Regional
Assessment document produced in 2011 as new information/data is available.
Study current service provision demands and citizen service trends /dynamics in the Western Region creating a profile of how needs are met or if there are unmet needs.
2.) Identify and appoint a Western Regional
Advisory Committee of no less than six western citizens representing the aforementioned sectors.
Meet on a consistent basis.
1.) Notation and documentation with the Western
Regional Assessment materials to reflect date of update –keep the document relevant
Incorporate this level of analysis into the aforementioned document perhaps as an appendix.
2.) Once identified and vetted candidates to this Western Regional Community Advisory Committee will be appointed by the Regional Networks Committee and have a seat at its quarterly meetings
The Western Regional Advisory Committee will establish a regular meeting schedule and set its work plan
1.) County staff involved in data collection
from approved source data. County Staff time involved in collection, assessment, and detailing of information
2.) County Staff appointed to lead, coordinate and sustain this effort. Ancillary expenses to convene this group.

HUMAN SERVICES AND ENVIRONMENTAL SERVICES
BOARD AGENDA ITEM
Agenda Date: June 28, 2012
Committee/Item:
Specific Action Requested: For update and information purposes.
Item Summary
A draft version of the Wake County Transit Plan (the Plan) was completed late last year. The Plan is derived from various detailed engineering studies and analyses on bus and rail service in Wake County. Compilation of the Plan has been a collaborative effort among key stakeholders including Wake County, Triangle Transit, Capital Area Metropolitan Planning Organization (CAMPO), City of Raleigh Capital Area Transit, Cary C-Tran, Regional Transportation Alliance, and all municipalities. The Plan outlines the priorities for bus and rail service in Wake County and will be used to guide future regional bus and rail investments that may result from the possible creation of a regional revenue source along with assumptions for state and federal participation. At the Board of Commissioner’s November 14, 2011 Work Session, staff presented a draft version of the Wake County Transit Plan. Since that time, Wake County has been meeting with elected municipal officials and other stakeholders to gather feedback on the draft plan. Revisions to the draft Plan are currently underway. The approach to improve transit in our community is outlined in the Plan. It includes a Core Transit Plan that delivers increased bus service and commuter rail with locally generated funds and federal/state formula funds; and an Enhanced Plan that adds light rail only if we are successful in receiving competitive federal and state funds. The local revenue sources for the Plan include:
• A half-cent sales tax: The sales tax proposal must be placed on the ballot by the Board of Commissioners. If approved by voters, the sales tax would generate an estimated $56 million to $60 million annually in the early years of the plan. The sales tax does not apply to food, medicine, utilities and housing.
• A $10 increase in vehicle registration fees: The fee increase would happen if the Wake County Board of Commissioners approves a new $7 fee for vehicles, and the Triangle Transit Board of Trustees approves a $3 increase in existing fees.
The bus portion of the Plan extends service to all municipalities, adds commuter and local routes, increases the frequency of the routes, and streamlines the destinations and connections made. The result would be a near doubling of the number of buses on the road today, all in the first five

years. The bus services in the Plan would cost just over $330 million for both capital and operating. The financial model assumes bus services would receive a similar level of support from state and federal funds as they do today. The Plan includes several elements that would effect and improve service to special needs populations. First, the increase and streamlining of services proposed will make it easier and more efficient for all users to get to and from destinations. The frequency on some fixed route services will be as high as every 15 minutes and all local routes will run every 30 minutes. Second, the Plan proposes to construct sidewalks, shelters, and stations that will make it easier for all users to access the bus system. Third, the Plan includes funding to provide the required special bus services within ¾ mile of fixed transit lines. Lastly the Plan includes funding to augment or expand services currently provided to the rural areas of the County by the TRACS system. The team is still working on the details of how each of these elements will be implemented. Commuter rail would operate in the existing NC Railroad right-of-way from Garner to Durham (37 miles / 12 stations). Commuter rail would cost $650 million. Wake County’s share would be $330 million and Durham would pay $320 million. Commuter rail is projected to be in place in 2019 or 2020. If the commuter rail is implemented the bus lines will be adjusted as needed to connect with all stations. Additionally, should the area be successful in receiving competitive federal and state funding grants, then the first phase of the light rail system would be implemented from downtown Cary to north Raleigh (Millbrook Road) covering 13.9 miles with 16 stations. Light rail is estimated to cost $1.1 billion (2011 dollars) with operating costs at $14 million per year. This investment, particularly, is expected to have a heavy impact on where people choose to live and work and effect land development.
Purpose for Action:
For update and information purposes.
Next Steps:
Attachments: Powerpoint Presentation
Opportunities for Advocacy, Policy or Advisory:
Connections to Other Committees:
Wake County Transit PlanChoose how you move!Choose how you move!
June 28, 2012
Wake County
Human and Environmental Services
1

� The Issue
� The Process
� The Draft Plan
Presentation Overview
� The Draft Plan
� The Numbers
Wake County Transit Plan2

Wake County Population
Jurisdiction 1980 1985 2000 2010 2020 2035 2040
Apex 2,847 3,710 20,212 37,476 58,690 98,638 114,227
Cary 21,763 35,520 94,536 133,812 160,512 189,419 196,457
Fuquay-Varina 3,110 3,746 7,898 17,937 33,590 65,463 78,376
Garner 10,073 12,372 17,787 25,745 46,278 87,543 104,160
Holly Springs 688 746 9,192 24,661 34,875 52,478 59,024
Knightdale 985 1,267 5,958 11,401 27,922 63,422 78,145
Wake County Transit Plan3
Morrisville 251 580 5,208 18,576 22,615 27,400 28,707
Raleigh 150,255 194,228 276,094 402,825 490,982 596,038 624,939
Rolesville 381 586 907 3,786 8,560 18,696 22,879
Wake Forest 3,780 4,379 12,588 29,218 42,450 65,927 74,802
Wendell 2,222 2,663 4,247 5,845 12,908 27,845 33,998
Zebulon 2,055 2,794 4,046 4,433 9,444 19,970 24,294
Total Wake County 301,429 360,387 627,846 900,993 1,160,823 1,541,088 1,667,841

The Issue
R² = 0.999
1,200,000
1,600,000
2,000,000
2,400,000
Wake County Population
Wake County Transit Plan4
1980 1985 2000 2010 2020 2035 2040
Wake County Population 301,429 360,387 627,846 900,993 1,160,823 1,541,088 1,667,841
Source: US Census, North Carolina Demographer, Wake County Planning
-
400,000
800,000
1970
1972
1974
1976
1978
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
2020
2022
2024
2026
2028
2030
2032
2034
2036
2038
2040
Population (Projection) Population (Prior Years) US Growth Rate Trendline (Prior Years)

The Issue
R² = 0.99
450,000
600,000
750,000
900,000
Wake County - Total Employed
Wake County Transit Plan5
1980 1985 2000 2010 2020 2035 2040
Wake County Employment 153,581 198,260 357,153 418,320 507,851 641,846 695,453
Source: NC Employment and Security Commission , Wake County Planning
-
150,000
300,000
1970
1972
1974
1976
1978
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
2012
2014
2016
2018
2020
2022
2024
2026
2028
2030
2032
2034
2036
2038
2040
Employment (Projected Years) Employment (Prior Years) Trendline (Prior Years)


Previous Studies
The Process - Studies and Plans
Previous Studies
Wake County Transit Plan

2009 – Congestion Relief and Intermodal
Transportation 21st
The Process - Studies and Plans
Transportation 21st Century Fund
Wake County Transit Plan

� Involved Transit and Planning Professionals
� Engaged all 12 Wake County Municipalities
� Engaged Expert Transit Consultants
� Engaged the Public
The Draft Plan
Wake County Transit Plan10
� Engaged the Public �20+ Public Workshops
�74,000+ Unique Website views

The Draft Plan – Expanded Bus
�Existing Service Recognized as the Baseline
�More Frequent / Faster Service to Destinations
�Service to More Communities
�Capital - $171,450,000 (total)
�Operating – $27,309,000 (per year) (2020)
Wake County Transit Plan11
�Operating – $27,309,000 (per year) (2020)
�$3.64 Estimated Annual Operating Cost Per Trip
�35,000 New Daily Trips as a Result of New Service

Bus Plan – Service Hour Expansion
The Draft Plan - Bus
Existing
345,000 Bus HoursFirst Five Years
Year Six and beyond
Wake County Transit Plan12
- Triangle Transit- Capital Area Transit- Cary Transit- NCSU Wolfline
322,740 Additional Bus Hours
Year Six and beyond
102,000 Additional Bus Hours

Raleigh/ Cary
197,070 -
Rest of Wake
County 125,670 -
39%
Wake County Bus Plan Total Annual Hours 2017
Raleigh/ Cary
619,997 -57%
Rest of Wake
County 464,775 -
Wake County Population 2017*
The Draft Plan - Bus
Wake County Transit Plan13
197,070 -61%
39%57%
464,775 -43%
*Projection

Local Bus Routes Today
Wake County Transit Plan14

The Draft Plan – Local Bus
Wake County Transit Plan15
Local Routes 2020

Commuter Bus Routes Today
Wake County Transit Plan16

The Draft Plan – Commuter Bus
Wake County Transit Plan17
Commuter Routes 2020

The Draft Plan – Commuter Rail
�Greenfield Parkway in Garner to Durham (37 Miles)
�Trains 30 min apart in the mornings and afternoon
�Capital - $650,000,000 (total) / $330,000,000 (Wake)
�Operating – $10,900,000 (per year)
Wake County Transit Plan18
�Operating – $10,900,000 (per year)
�$6.44 Estimated Annual Operating Cost Per Trip
�6,900 Daily Trips anticipated in 2035

Commuter Rail Corridor
Presentation Title19

The Draft Plan – Light Rail �Downtown Cary to Millbrook Road (13.9 miles)
�Service every 10 minutes during peak hours and 20 minutes off-peak
�Capital - $1,100,000,000 (total)
�Operating – $14,170,000 (per year)
Wake County Transit Plan20
�Operating – $14,170,000 (per year)
�$2.97 Estimated Annual Operating Cost Per Trip
�15,900 Daily Trips anticipated in 2035

Light Rail Corridor
Presentation Title21

The Draft Plan – Transit Vision
The Numbers
• Federal and State funding (existing funding streams only)
• New and Expanded Bus Service, Shelters, Park-and-Ride Lots
• Nearly doubles existing bus service in first 5 years• Commuter Rail Service
CORE TRANSIT
PLAN
Wake County Transit Plan23
• Requires new federal and state financial participation that cannot be counted on
• Light Rail Service from downtown Cary to Millbrook Road
ENHANCED TRANSIT
PLAN

The Numbers
� Local Revenue
• Half-cent Local Sales Taxo Revenue estimated at $53.47 million in FY 2011
o Growth assumption:
Wake County Transit Plan24
o 1.0%.....FY 2012
o 1.5%.....FY 2013
o 2.0%.....FY 2014
o 2.5%.....future years

The Numbers
� Local Revenue
• New $7 county vehicle registration fee
• Increase from $5 to $8 regional vehicle registration fee
Wake County Transit Plan25
registration fee
• Existing 5% vehicle rental tax
• Fare box revenue

Local, Sales Tax; 2,133,552,449 ; 61%
Federal, FTA 5309 Grants; 90,710,757; 3%
Federal, All Other; 242,035,216; 7%
State, 290,855,760; 8%
Core Transit Plan Cumulative Revenue Totals (FY 2013-2040)
Wake County Transit Plan26
Local, Vehicle Registrations;
180,694,280; 5%
Local, Vehicle Rental Tax; 121,801,844; 3%
Local, Farebox; 268,196,951; 8%
Bonds; 170,000,000; 5%

Operating - Expanded Bus Service;
1,429,587,070 ; 51%
Capital - Rail Projects; 375,915,494; 13%
Core Transit PlanCumulative Expenditure Totals (FY 2013-2040)
Wake County Transit Plan27
Debt Service Payments;
255,419,728; 9%
Capital - Expanded Bus Service;
484,070,432 ; 17%
Operating - Rail Projects; 268,794,451;
10%

Policy Issues / Questions
• Need versus Cost
• County Priorities
• Choices and Tradeoffs
Wake County Transit Plan28
• Choices and Tradeoffs

Wake County Transit Plan“Working Schedule”
Task/Milestone Date
• Draft Wake County Transit Plan November 2011
• Input on the Plan / THOROUGH REVIEW January – May
Wake County Transit Plan29
• Develop Final Plan May - ?
• Referendum

Wake County Transit PlanChoose how you move!Choose how you move!
June 28, 2012
Wake County
Human and Environmental Services
30

RDU CONRAC Site, APM Link
& Possible APM Link between RDU & RTP

Current Legislation Current Model Filled/Vacant Term End Proposed Legislation Proposed Model Filled/Vacant
1 psychologist psychologist vacant 11/14/2011 1 psychologist psychologist vacant
2 pharmacist pharmacist filled (Ridout) 11/14/2012 2 pharmacist pharmacist filled (Ridout)
3 engineer engineer filled (Goodwin) 11/14/2014 3 engineer engineer filled (Goodwin)
4 dentist dentist filled (Horwitz) 11/14/2012 4 dentist dentist filled (Horwitz)
5 optometrist optometrist filled (Said) 11/14/2013 5 optometrist optometrist filled (Said)
6 veterinarian veterinarian filled (Dunning) 11/14/2013 6 veterinarian veterinarian filled (Dunning)
7 social worker social worker vacant 11/14/2014 7 social worker social worker vacant
8 registered nurse registered nurse vacant 11/14/2014 8 registered nurse registered nurse vacant
9 psychiatrist psychiatrist vacant 11/14/2011 9 psychiatrist psychiatrist vacant
10 other physician other physician filled (Foster) 11/14/2011 10 other physician other physician filled (Foster)
11 County Commissioners County Commissioner filled (West) - 11 County Commissioners County Commissioners filled (West)
12 consumer/MH consumer/MH filled (Earnhardt) 11/14/2011 12 consumer other HS consumer other HS filled (Ju. Smith)
13 consumer/DD consumer/DD filled (Je. Smith) 11/14/2012 13 consumer other HS consumer other HS vacant
14 consumer/SA consumer/SA filled (Treadway) 11/14/2012 14 consumer other HS consumer other HS new
15 family/MH family/MH filled (Greb) 11/14/2013 15 consumer other HS consumer other HS new
16 family/DD family/DD vacant 11/14/2014 16 general public general public filled (Eagles)
17 family SA family/SA filled (Jemison) 11/14/2013 17 general public filled (Escobar)
18 consumer other HS consumer other HS filled (Ju. Smith) 11/14/2014 18 general public filled (Norman)
19 consumer other HS consumer other HS vacant 11/14/2012 19 general public vacant
20 general public general public filled (Eagles) 11/14/2014 20
21 general public filled (Escobar) 11/14/2014 21
22 general public filled (Norman) 11/14/2012 22
23 general public vacant 11/14/2011 23
24 general public vacant 11/14/2011 24
25 general public vacant 11/14/2013 25
26 general public vacant 11/14/2013 26
Human Services Board Membership





Wake HS Quarterly Report by Service and Designated Indicator
FY 12 - Q3
PROGRAM or SERVICECaseload Size at end of Fiscal Year
FY 08 - FY 11
Indicator
Tracked
Q1
FY12
Q2
FY12
Q3
FY12
COMMENTS FROM PROGRAM ABOUT LEVEL OF CHANGE AND IMPACT ON SERVICE
DELIVERY (For this quarter only)
FY 08, 18,352
FY 09, 18,960
FY 10, 19,997
FY 11, 21,051
5% ↑ in caseload from FY 10 to FY 11
FY 08, 424
FY 09, 489
FY 10, 532
FY 11, 58310% ↑in number of wards in caseload from
FY 10 to FY 11FY 08, 1235 (Reports Made)
FY 09, 1294 (Reports Made)
FY 10, 1152 (Reports Made)
FY11, 247 (Reports Accepted**)
[Program began tracking new indicator in FY
11]
FY 08, 5,107 (Assessments for FY)
FY 09, 4,834 (Assessments for FY)
FY 10, 5,211 (Assessments for FY)
FY 11, 5,018 (Assessments for FY)
4% ↓in accepted assessments from FY 10
to FY 11
FY 08, 738 (New In Home Cases Opened)
FY 09, 817 (New In Home Cases Opened)
FY 10, 810 (New In Home Cases Opened)
FY 11, 844 (New In Home Cases Opened in FY)
4%↑ from FY 10 to FY 11
FY 08, 232
FY 09, 240
FY 10, 264
FY 11, 319
20 % ↑new placements from FY 10
Childcare Subsidy
FY 11 , 8,544 Caseload Count End of FY
(NOTE: The number children being served is
fairly static; it may change slightly
depending on funding)
**Counts Children
New Cases
Opened for
Service per
Quarter **Counts
Children
509 522 429
As of 6/1/12 the Child Care Subsidy Program will be supervised by Barbara Harris as we
continue to realign in preparation for NC FAST. NC FAST will be implemented in phases
to combine the eligibility for all DSS programs that include Food Assistance, Medicaid,
Child Care, Work First, etc. The Food Assistance Program implementation of NC FAST
will begin in the fall for Wake County.
Waiting list July 2008, 3,580
Waiting list July 2009, 6,689
Waiting list July 2010, 2,744
Waiting list July 2011, 5,495
100% ↑ from FY 10 to FY 11
920 905 1,046
3,566 applications were received this quarter, which is a 35% increase over the
previous quarter. Some of the increase was due to annual re-enrollment in Medicare
Part D drug plans and applications for help with drug costs, which automatically
generate Medicaid applications.
Adult GuardianshipWards Added
per Quarter39 29 23
Caseload has remained around 393, however trend is that the new cases are younger
and more difficult to serve.
Adult Medicaid New Cases
added per
Quarter
The number of Child Protective Services (CPS) assessments and assists in the first 3
quarters of FY2012 has decreased by 7% compared to the first 3 quarters of FY 2011.
Adult Protective ServicesAccepted
Reports per
Quarter**
67 68 67
191 183 182
Reports have been received in cycles, however number of reports accepted has been
consistent for 3 quarters this FY.
Child Welfare CPS
Assessments
Accepted
Assessments
per Quarter
1,106 1,137 1,294
The number of families referred to Child Protective Service (CPS) In-Home Services
during the first 3 quarters of FY 2012 has decreased 14% compared to the first 3
quarters of FY 2011.
Foster Care
New
Placements per
Quarter
**Counts
Children
81 78 99
The number of children entering foster care in first 3 quarters of FY 2012 increased by
7% compared to the first 3 quarters of FY 2011. This is on top of a 20% increase in FY
2011 compared to FY 2010. Staff and court officials report the increase in children
entering foster care (despite a decrease in Child Protective Service (CPS) reports
appears to be the result of higher numbers of children are at imminent risk of serious
harm.
Child Welfare In Home
New In-Home
Service Cases
Opened per
Quarter **Counts Cases
Opened for
Families
PROGRAM COMMENTS:
Childcare Subsidy
New Cases
Added to Wait
List per
Quarter
**Counts
Children
410 368 534
6/12/201212:38 PM Wake County Human Services Quarterly Report 1

Wake HS Quarterly Report by Service and Designated Indicator
FY 12 - Q3
PROGRAM or SERVICECaseload Size at end of Fiscal Year
FY 08 - FY 11
Indicator
Tracked
Q1
FY12
Q2
FY12
Q3
FY12
COMMENTS FROM PROGRAM ABOUT LEVEL OF CHANGE AND IMPACT ON SERVICE
DELIVERY (For this quarter only)
FY08, 36,558 cases
FY09, 41,495 cases
FY 10, 45,317 cases
FY 11, 47,870 cases
6% ↑ from FY 10 End of Year Caseload
FY 08, 20,416
FY 09, 25,998
FY 10, 27,816
FY 11, 28,166
1.2% ↑ in customers served from FY 10
FY 08, 19,866
FY 09, 25,892
FY 10, 30,408
FY 11, 35,809
18% ↑ from FY 10 End of Year Caseload
Calendar Year 2008, 37
Calendar Year 2009, 115
Calendar Year 2010, 84
Calendar Year 2011, 76
9.5% ↓ from Calendar Year '10 to '11
Calendar Year 2008, 321
Calendar Year 2009, 281
Calendar Year 2010, 285
Calendar Year 2011, 249
12.6% ↓ from Calendar Year '10 to '11
Calendar Year 2008, 1030
Calendar Year 2009, 1010
Calendar Year 2010, 1249
Calendar Year 2011, 1355
8.5%↑ from Calendar Year '10 to '11
Calendar Year 2008, 3121
Calendar Year 2009, 3590
Calendar Year 2010, 4530
Calendar Year 2011, 4748
5%↑ from Calendar Year '10 to '11
8,450 7,443 8,384
This quarter's figures are the total of applications approved from January 2012 through
March 2012. This represents an 11% increase from 2nd quarter to 3rd quarter.
However, this figure is also comparable to the 1st quarter figures.
Workforce Development
New & Repeat
Customers
Served by Job
Link &
Employment/
Vocational
Services
11,200** 8,911** 9,662
There was an increase in customer usage between Q2 and Q3. This increase is related
to seasonal variations following the November/December holidays. Also note,
effective July 1, 2012, the beginning of FY12, services from the Millbrook Center are
added into the counts for 'New and Repeat Customers' of Joblink and Employment
services. The "card swipe" system was implemented at Millbrook in FY12, creating an
increase in numbers captured for reporting using the new technology. Millbrook data
are a portion of each quarterly count shown. Counts of New and Repeat Customers for
the Millbrook Center by quarter are: Q1 - 2877; Q2 - 2210; Q3 - 2630.
Medicaid - Children and
Families
New Cases
Opened for
Services per
Quarter
PROGRAM COMMENTS: Case numbers for syphilis are similar to 2011 numbers.
Food and Nutrition (FNS)
New Cases
Opened for
Services per
Quarter
6,162 5,898 5,929
65 70 59
PROGRAM COMMENTS:
Syphilis ServicesNew Cases
being Served27 17 18
Numbers slightly down in Q3, yet total case numbers for HIV/AIDS may actually rise in
FY 2013--this would be in no small part due to the hiring of a staff member whose
primary purpose will be to work with WakeMed Raleigh Emergency Dept. on increasing
HIV testing there. Increased HIV screening will lead to many more HIV/AIDS cases
diagnosed.
Gonorrhea Services (New
this FY)
New Cases
being Served354 357 326
Case numbers remain very high, but with increased emphasis on expanded treatment
options (Expedited Partner Therapy and Field-Delivered Therapy), county may
experience less morbidity in FY 2013.
HIV/ AIDS Services *New Cases
being Served
Case numbers remain very high, but with increased emphasis on expanded treatment
options (Expedited Partner Therapy and Field-Delivered Therapy), county may
experience less morbidity in FY 2013.Chlamydia Services (New
this FY)
New Cases
being Served1290 1361 1062
6/12/201212:38 PM Wake County Human Services Quarterly Report 2

HUMAN SERVICES AND ENVIRONMENTAL SERVICES
BOARD AGENDA ITEM
Agenda Date: Executive Committee: June 14, 2012
HS & ES Board: June 28, 2012
Committee/Item: Public Health Committee/Public Health Quarterly Report January – March
2012
Specific Action Requested: Receive Public Health Quarterly Report
Item Summary: The Public Health Quarterly Report is published by WCHS Public Health
Division and highlights program data such as disease trends, program participation and
outcomes. This quarterly report includes data from the first quarter of calendar year 2012.
Purpose for Action (Proposed Solutions/Accomplishments):
Public Health Accreditation requires that “The local health department shall analyze and note
reportable events occurring within the community and shall report atypical incidence, if any, to the
Division and the local board of health” (Benchmark 2 Activity 2.4).
Next Steps:
Accept quarterly report and use as needed to inform discussions, decisions and advocacy efforts
related to public health.
Attachments: Public Health Quarterly Report January – March 2012
Opportunities for Advocacy, Policy or Advisory: (see next steps)
Connections to Other Committees: Environmental Services

1 1
W A K E C O U N T Y W A K E C O U N T Y W A K E C O U N T Y W A K E C O U N T Y
H U M A N S E R V I C E SH UM A N S E R V I C E SH UM A N S E R V I C E SH UM A N S E R V I C E S
P U B L I C H E A LT H P U B L I C H E A LT H P U B L I C H E A LT H P U B L I C H E A LT H
Q U A R T E R LY Q U A R T E R LY Q U A R T E R LY Q U A R T E R LY R E P O R T R E P O R T R E P O R T R E P O R T
J A N U A R YJ A N U A R YJ A N U A R YJ A N U A R Y ———— M A R C H 2 0 1 2M A R C H 2 0 1 2M A R C H 2 0 1 2M A R C H 2 0 1 2
Wake County Human Services Public Health Division 10 Sunnybrook Road P.O. Box 14049 Raleigh, NC 27620-4049 www.wakegov.com
MAY 18, 2012
P u b l i c H e a l t h Prevent · Promote · Protect
Ramon Rojano, Human Services Director Sue Lynn Ledford, Public Health Division Director
Editor-in chief: Edie Alfano–Sobsey, Public Health Epidemiologist
Editorial Staff: Roxanne Deter, Public Health Nurse and
Carla Piedrahita, Public Health Educator
Design and Layout: Michelle Ricci, Public Health Educator

2 2
Table of Contents
Topic Page
Introduction 3
County Health Rankings 4
Tobacco Use
Quitline Use 7
School Health
School Nurse to Student Ratio 8
School Staff Training 9
School Health Services 10
Outreach
National Association of Counties (NACo) Prescription Drug Discount Card
Program
11
Infectious Disease and Foodborne Illness
Reportable General Communicable Disease Investigations 12
Critical Violations at Wake County Restaurants/Food Stands 12 & 13
Emergency Preparedness
Strategic National Stockpile Plan 13
Sexually Transmitted Infections
Integrated Testing Services 14 & 15
Pregnancy Rates
Pregnancy Rates for 15-19 Year Olds in Wake County 16 & 17
Wake County Prenatal Clinic Clients 2009—2011 18
Healthy North Carolina 2020 Objectives 19 & 20
Acknowledgements 21

3 3
Introduction
Wake County Human Services (WCHS), an accredited health department, continues to strive to
perform the three core functions of assessment, policy development and assurance and the 10 public
health essential services (see Figure 1). This report helps fulfill public health essential services:
• Number 1: Monitor health status to identify community health problems and
• Number 3: Inform, educate, and empower people about health issues.
Figure 1
Information is provided on a quarterly basis about health and safety trends for Wake County residents,
providers, policy makers and community partners to better inform decision making. Strategies used
by WCHS Public Health programs and services to improve health outcomes are also featured in these
reports. For additional information, point of contact information is provided for each area.
This issue highlights the results of the national County Health Rankings. See inside how WCHS
ranked!

4 4
County Health Rankings
For the third year in a row, Wake County has been named “Healthiest County” in North Carolina,
according to a report released on April 3, 2012 by the University of Wisconsin Population Health
Institute and the Robert Wood Johnson Foundation (See Figure 2). Community members such as
businesses, government, faith-based organizations, health care, educational systems, and public health
work together with philanthropists and investors to achieve these outstanding results.
The report assesses the overall health of counties in all 50 states by using a standard formula to
measure how healthy people are and how long they live. Counties are ranked within each state. The
findings ranked Wake first in overall health outcomes and second for other health factors among all
100 North Carolina counties.
The four measures used to assess the level of overall health for North Carolina by County were:
• The rate of people dying before age 75
• The percent of people who report being in fair or poor health
• The number of days people report being in poor physical and poor mental health and
• The rate of low-birth-weight infants.
The report also looked at factors that affect people’s health within four categories:
• Health behavior
• Clinical care
• Social and economic factors
• Physical environment (see Table 1).
Data Source: County Health Rankings and Roadmaps www.countyhealthrankings.org
Figure 2
1

5 5
Wake County Health Outcomes and Health Factors
2012 Wake County Error Margin National Benchmark* North Carolina Rank ( of 100)
HEALTH OUTCOMES 1
Mortality 1
Premature Death 5,212 5, 042-5,382 5,466 7,961
Morbidity 1
Poor or fair health 12% 11-13% 10% 18%
Poor physical health days 2.6 2.4-2.9 2.6 3.6
Poor mental health days 2.5 2.3-2.7 2.3 3.4
Low birthweight 7.7% 7.6-7.9% 6.0% 9.1%
HEALTH FACTORS 2
Health Behaviors 2
Adult smoking 15% 14-17% 14% 22%
Adult obesity 26% 24-28% 25% 29%
Physical inactivity 18% 17-20% 21% 25%
Excessive drinking 15% 13-16% 8% 13%
Motor vehicle crash death rate 11 11-12 12 19
Sexually transmitted infections 394 84 445
Teen birth rate 30 29-30 22 50
Clinical Care 4
Uninsured 14% 13-15% 11% 18%
Primary care physicians 835:1 631:1 859:1
Preventable hospital stays 51 49-53 49 64
Diabetic screening 89% 86-91% 89% 87%
Mammography screening 73% 71-76% 74% 70%
Social and Economic Factors 3
High school graduation 84% 78%
Some college 77% 76-78% 68% 61%
Unemployment 8.4% 5.4% 10.6%
Children in poverty 15% 13-17% 13% 25%
Inadequate social support 18% 16-20% 14% 21%
Children in single parent households 26% 25-28% 20% 34%
Violent crime rate 333 73 448
93
Air pollution-particulate matter days 3 0 1
Air pollution-ozone days 7 0 6
Access to recreational facilities 15 16 11
Limited access to healthy foods 6% 0% 10%
Fast food restaurants 52% 25% 49%
Physical Environment
*90th percentile, i.e. only 10% are better. NOTE: Blank values reflect unreliable or missing data.
Data Source: County Health Rankings and Roadmaps www.countyhealthrankings.org
Table 1

6 6
County Health Rankings
Although Wake County achieved a high health ranking, several areas to explore for improvement
have been identified from this and other Wake County reports (such as the Wake County Community
Assessment, and State of the County Report) based on weight of health factor, trend, comparison to
NC state average or magnitude of difference from a national benchmark. These include:
• Children in poverty (Increased from 11% in 2008 to 15% in 2010.)
• Obesity (Since 2006, 25% or more of Wake county residents are obese.)
• Violent Crime (The violent crime rate was 333/100,000 population from 2007-2009 ;
almost 5 times higher than the national benchmark of 73/100,000 population.)
• Excessive Drinking ( Fifteen percent (15%) of Wake county adults participate in heavy or
binge drinking compared to 13% of adults in NC from 2004 - 2010. This is about twice as
high as the national benchmark.)
• Sexually Transmitted Infections (Increased from 365/100,000 population in 2008 to
394/100,000 population in 2009; almost 5 times higher than the national benchmark of
84/100,000 population.)
• Physical Environment (Wake County’s physical environment ranked 93rd out of 100
counties because of unhealthy environmental conditions based on air pollution, access to
recreational facilities, limited access to healthy foods and number of fast food restaurants.)
AREAS FOR IMPROVEMENT
Contact: Edie Alfano-Sobsey, Public Heath Division 919-212-9674 [email protected]

7 7
Tobacco Use
Data Source: NC Quitline Monthly Data Reports
The purpose of the Quitline is to provide NC citizens a FREE cessation resource to aid in quitting
tobacco use. The Quitline offers 24/7 counseling sessions either by phone and/or online. Quit coaches
call people who are referred to the Quitline by healthcare providers. While supplies last, callers who
enroll and qualify are offered FREE nicotine replacement therapy (NRT) medication in the form of
patches, gum or lozenges. The Quitline number is 1-800-784-8669 (1-800-QUITNOW).
During the first three months of 2012, enrollment in the Quitline increased compared to the same time
in 2011 and 2010 (see Figure 4). The Centers for Disease Control and Prevention (CDC) Office of
Smoking and Health, the NC Department of Health and Human Services (DHHS), and Wake County
Human Services Project ASSIST (American Stop Smoking Intervention Study) collectively provided
multiple media campaigns during the months of January-March. The media outlets used were radio,
television, web ads and local newspapers. The campaign began in January and DHHS and CDC ads
continue to air. Figure 3 is a reflection of the importance of social media in public health. Educating
the public on available resources like the Quitline is essential to getting people the support needed to
quit using tobacco.
5240
159
36
57
144
180
111
167
0
20
40
60
80
100
120
140
160
180
200
2010 2011 2012
Number of Wake County Residents Registered With Quitline
During January-March 2010-2012
Jan
Feb
March
Figure 3
Contact: Sonya Reid, Health Promotion Chronic Disease Prevention Section 919-250-4553 [email protected]
QUITLINE USE

8 8
School Health
Figure 4
STUDENT TO SCHOOL NURSE RATIO
The Wake County Human Services School Health Program promotes the health, safety and
educational success of students in the Wake County Public School System (WCPSS). The WCHS
School Health Program does this by partnering with WCPSS, families, physicians, hospitals and
community agencies using evidence based practices and professional standards of care. This
partnership includes: training school staff with no medical background to perform medical procedures
and administer medications; responding to health concerns that interfere with academic success; and
assisting families in accessing needed resources. Additionally, the program promotes the public
health and safety of Wake County residents through emergency preparedness and the prevention,
investigation and control of communicable diseases in the school system.
The student to school nurse ratio is a measure used across the state of North Carolina and the United
States to assure students are healthy and able to participate in school. The student to school nurse
ratio is significantly higher in Wake County as compared to the recommended standard as well as to
other North Carolina counties (see Figure 4). In Wake County, the number of students per school
nurse is over twice the average of other North Carolina counties.
24052198
20471918 1897
1593 15711340 1340
1226 1175 1,201
19902172 2188 2239 2253 2298 2286
21632371
22672383 2,317
0
500
1000
1500
2000
2500
3000
Number of Student s
to One Nurse
Number of Public School Students Per School Nurse
Wake County and North Carolina
Trend from 1999-2000 to 2010-2011 School Years
North Carolina
Wake
Note: The standard student to school nurse ratio of 750 students to one school nurse nurse has been adopted by the North Carolina Public
Health Taskforce, the North Carolina Department of Public Instruction and teh NC Division of Public Health and is based on recommendations
made by the American Academy of Pediatrics, the Centers for Disease Contol and Prevention, and the National Association of School Nurses.
Source: NC Annual Survey of School Health Services, NC DHHS

9 9
School Health
Figure 5
SCHOOL STAFF TRAINING
12361542
18942111
2663
3180
35573881 3793
0
500
1000
1500
2000
2500
3000
3500
4000
4500
Number Of Procedures School Nurses
Trained WCPSS Non-Medical School Staff to Perform
2002-2003 through 2010-2011 School Year
Procedures
School Year
Data Source: Wake County Human Services School Based Public Health Nursing Program
Monthly Report
Use of epinephrine auto injectors
for severe allergy makes up 57%
of the medical procedures
performed in the schools (see
Figure 6); food allergies are the
most prevalent type of allergy.
Comprehensive preventive and
emergency care plans are
developed by the school nurse
and school staff is trained to give
medication through injections,
insulin pumps, rectal
suppositories and inhalers.
Data Source: Wake County Human Services School Based Public Health Nursing
Program Monthly Report
The number of procedures
school nurses train non-
medical staff to perform
increased 300% over a nine
year time span (see Figure
5).
Figure 6
Epinephrine
Auto Injector
57%
Diabetes
Re lated
Proc edure
27%
Diastat (Rectal
Valium)
7%
Nebulizer
Treatment
4%
Other
5%
Types of Procedures Wake County Public Schools

10 10
School Health
SCHOOL HEALTH SERVICES
The large number of assessments and counseling is attributed to assessment of each student referred to
the nurse with corresponding counseling when a health concern is identified. From October to
December, assessments increase significantly due to vision screening. As the year progresses, services
that take more time to complete such as case management, follow up of students referred for health
concerns and working with families to help their child access care increase (see Figure 7).
Figure 7
Contact: Roxanne Deter, Public Health Division 919-250-4637 [email protected]
9703
16511
13291
7725
8385
5958
5699
5317
3707
2072
1848
1457
0 2000 4000 6000 8000 10000 12000 14000 16000 18000
Jan-Mar 2012
Oct-Dec-2011
Jul-Sept 2011
Number of Services
Number of School Based Public Health Nurse and Dental Hygienist Services Including
Assessment, Counseling, Referral and Follow Up to Secure Care for Wake County
Public School Students
Quarterly Service Activity 2011-2012 School Year
Case Mananged
Services/Family
Intervetions/Home Visits
Follow up/Referral/Assurace
Student Secures Care
Health Counseling
Assessment of Health
Conditions
Source: Wake County Human Services School Based Monthly Reports

11 11
Outreach
The National Association of Counties (NACo) Prescription Drug Discount Card Program was initiated
in Wake County in September 2007. The card is ready for immediate use, with no form to fill out or
fee for enrollment, and provides a discount for prescription medications that are not already covered
by insurance or other prescription discount program. Cards can be obtained from card displays located
at Wake County government buildings with public access, including regional centers, public libraries,
town halls, and at retail pharmacies throughout Wake County. Table 2 shows card usage and price
savings in Wake County from 2008 –2011.
NATIONAL ASSOCIATION OF COUNTIES (NACo) PRESCRIPTION DRUG DISCOUNT
CARD PROGRAM
Calendar Year Total Utilizers Avg. Price Savings Percent of Price
Savings
2008 55,888 $13.83 25.44%
2009 52,836 $14.33 26.84%
2010 46,389 $14.77 27.74%
2011 38,163 $14.51 27.81%
Total 193,276 $14.36 26.95%
Total Utilizers – gives an indication of how many residents the program is helping
Average Price Savings – Average price savings per prescription
Percent of Price Savings – Percentage price savings per prescription
Data Source: National Association of Counties www.naco.org
Contact: JoAnn Douglas, Immunization Outreach 919-250-4518 [email protected]
Table 2

12 12
I n f e c t i o u s D i s e a s e s a n d F o o d b o r n e I l l n e s s
+Number reported by NC
Electronic Disease Surveillance
System (NCEDSS) on May 2,
2012.
*Foodborne Illness includes
campylobacter, E. coli shiga toxin
producing , hepatitis A, salmonella
and shigella.
**Tickborne Illness includes
Rocky Mountain spotted fever,
Lyme disease and ehrlichiosis.
***Hepatitis B includes new
infections, long term infections and
those acquired through pregnancy/
birth.
Figure 8
REPORTABLE COMMUNICABLE DISEASE INVESTIGATIONS
0
10
20
30
40
50
60
70
Foodborne
Illness*
Tickborne
Illness**
Hepatitis
B***
31 29
6867
16
47
Investigations
Reportable Communicable Disease Investigations+
January - March 2011 and 2012
Jan-Mar 2011
Jan-Mar 2012
Figure
9
CRITICAL VIOLATIONS AT WAKE COUNTY RESTAURANTS/FOOD STANDS
Data Source: Wake County Environmental Services
The average number of critical violations per inspection decreased during the last quarter
(January to March 2012) for the first time in several years (see Figure 9), possibly due to increased
outreach and educational activities by the Wake County Environmental Health and Safety Division
staff .
More foodborne illness and fewer tickborne illness and hepatitis B investigations were conducted in
the first quarter of 2012 compared to the first quarter of 2011 (see Figure 8).
0.0
0.5
1.0
1.5
2.0
2.5
Jan
-10
Fe
b-1
0
Ma
r-10
Ap
r-10
Ma
y-1
0
Jun
-10
Jul-1
0
Au
g-1
0
Se
p-1
0
Oct-1
0
No
v-1
0
De
c-10
Jan
-11
Fe
b-1
1
Ma
r-11
Ap
r-11
Ma
y-1
1
Jun
-11
Jul-1
1
Au
g-1
1
Se
p-1
1
Oct-1
1
No
v-1
1
De
c-11
Jan
-12
Fe
b-1
2
Ma
r-12
Average
Number
of
Critical
Violations
Average Number of Critical Violations per Inspection at Wake
County Restaurants from January 2010 to March 2012
Contact: Ruth Lassiter, Communicable Disease Surveillance Section, 919-212-7344 [email protected]

13 13
I n f e c t i o u s D i s e a s e s a n d F o o d b o r n e I l l n e s s
Figure 10
CRITICAL VIOLATIONS AT WAKE COUNTY RESTAURANTS/FOOD STANDS
Data Source: Wake County Environmental Services
Number of Cri=cal Viola=ons Associated with CDC Risk Factors*
at Wake County Restaurants/Food Stands January—March 2012
*CDC Risk Factors
Items 1-5: Poor Personal
Hygiene
Items 6-9: Food from
Unsafe Source
Items 10-12: Cross
Contamination/
Contaminated Equipment
Item 13: Final Cook
Time
Items 14-18: Holding/
Time-Temperature
Contact: Andre Pierce, Wake County Environmental Services 919-865-7440 [email protected]
E m e r g e n c y P r e p a r e d n e s s
During the first quarter of 2012, the Wake County Strategic National Stockpile (SNS) Plan was
completely re-written to comply with the CDC Technical Analysis Review (TAR) of such plans.
The SNS Plan provides information on how to request the CDC stockpile of medications and support
equipment during a biological incident, how the materials are to be received and how the materials
are to be distributed to the entire population of Wake County within a 48 hour “window”. The
previous Wake County SNS Plan was an “operational” plan which did not meet the requirements of
the current CDC TAR. The re-write provides extensive details about actions to be taken should the
SNS be required in Wake County and many details on possible scenarios for medication distribution
to the population of Wake County in the event a terrorist incident.
Contact: Brian McFeaters, Public Health Emergency Preparedness Section 919-212-9394 [email protected]
STRATEGIC NATIONAL STOCKPILE PLAN
"Critical Violation Risk Factors” are those that increase the chance of developing food-borne illness
and are categorized by CDC as poor personal hygiene (1-5), food from unsafe source (6-9), cross
contamination/contaminated equipment (10-12), inadequate final cook temperature (13), improper
holding/time-temperatures (14-18). Figure 10 shows that most of the critical violations involved
cross contamination of foods and contaminated equipment.

14 14
Sexually Transmitted Infections (STIs)
Table 3
The number of cases reported from Wake County to the NC Division of Public Health for calendar
year 2010 to 2011 decreased for syphilis (9.5%) and HIV/AIDS ( 12.6%) but increased for gonorrhea
(8.5%) and chlamydia (5%). New cases reported from January to March 2012 were syphilis (18),
HIV/AIDS (59), gonorrhea (326) and chlamydia (1062).
Testing services for HIV, syphilis, chlamydia, gonorrhea, and hepatitis C are integrated by offering
simultaneously to clients at community as well as clinical testing sites. Integrated testing increases
detection and treatment of all STIs in high risk populations. This enhanced testing is made possible
through the CDC Program Collaboration and Service Integration (PCSI) and other grant funding.
Tables 3, 4, and 5 show the number of tests performed at community sites and the positivity test rates
for HIV, syphilis, gonorrhea, chlamydia and hepatitis C comparing October thru December 2011 to
January thru March 2012.
Number of Tests and Test Posi=vity Rate (%) at Non-Tradi=onal Tes=ng Sites in Wake
October-December 2011 January- March 2012
Test Number Tested % Posi>ve Number Tested % Posi>ve
HIV 500 9.6 743 13.5
Syphilis 682 0.1 737 0
Gonorrhea 500 1.4 511 1.4
Chlamydia 680 0.4 511 9.2
Hepa>>s C 39 12.8 90 13.3
Data Source: Wake County Human Services HIV/STD Community Program
INTEGRATED TESTING SERVICES
Non-traditional testing sides are community locations where HIV/STD counseling and testing
services would not customarily be provided (churches, shelters, colleges, and universities).

15 15
Sexually Transmitted Infections (STIs)
Number of Tests and Test Posi=vity Rate (%) at Substance Abuse Centers in Wake County
October -December 2011 January -March 2012
Test Number Tested % Posi>ve Number Tested % posi>ve
HIV 90 0 86 0
Syphilis 91 0 86 0
Gonorrhea 61 0 63 0
Chlamydia 61 0 63 1.6
Hepa>>s C 76 15.8 48 21
Data Source: Wake County Human Services HIV/STD Community Program
Number of Tests and Test Posi=vity Rate (%) at Expanded Tes=ng Sites* in Wake County
October -December 2011 January -March 2012
Test Number Tested % Posi>ve Number Tested % Posi>ve
HIV 406 6.9 406 0.2
Syphilis 407 2 406 3.2
Gonorrhea 406 2.5 405 2.7
Chlamydia 406 6.9 405 7.9
Hepa>>s C* 0 0 0 0
Data Source: Wake County Human Services HIV/STD Community Program
Table 4
Table 5
* Jails, detention. Hepatitis C testing is not offered at Expanded Testing Sites.
Contact: Yvonne Torres, HIV/STD Community Section 919-250-4479 [email protected]

16 16
Pregnancy Rates
PREGNANCY RATE FOR 15-19 YEAR OLDS IN WAKE COUNTY AND NORTH
CAROLINA
Figure 12
Figure 11
From 2006 to 2010, both North Carolina and Wake County saw their pregnancy rates for ages 15-17
and ages 18-19 decline (see Figures 11 and 12) .
23.321.9 22.6
19.4
18.6
35.1 34.832.5
30.1
26.4
0
5
10
15
20
25
30
35
40
2006 2007 2008 2009 2010
Rat
e P
er
10
00
Pregnancy Rate per 1,000 Age 15-17
Wake County and North Carolina 2006-2010
Wake
North Carolina
Source: North Carolina State Center for Health Statistics
72.8 75.7
64.4 63.3 59.5
101.3 101.693.1
83 81.6
0
20
40
60
80
100
120
2006 2007 2008 2009 2010
Rat
e P
er
10
00
Pregnancy Rate per 1,000 Age 18-19
Wake County and North Carolina 2006-2010
Wake
North
Carolina
Source: North Carolina State Center for Health Statistics
17 17
Figure 13
Pregnancy Rates
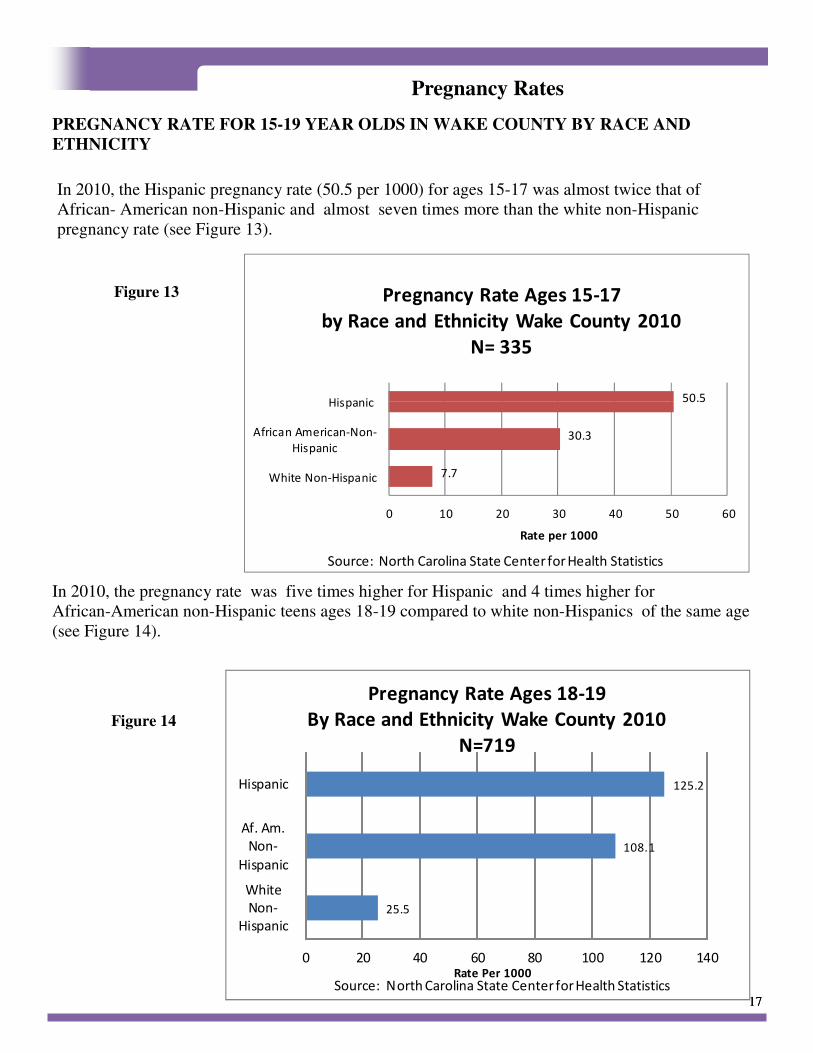
PREGNANCY RATE FOR 15-19 YEAR OLDS IN WAKE COUNTY BY RACE AND
ETHNICITY
Figure 14
In 2010, the Hispanic pregnancy rate (50.5 per 1000) for ages 15-17 was almost twice that of
African- American non-Hispanic and almost seven times more than the white non-Hispanic
pregnancy rate (see Figure 13).
In 2010, the pregnancy rate was five times higher for Hispanic and 4 times higher for
African-American non-Hispanic teens ages 18-19 compared to white non-Hispanics of the same age
(see Figure 14).
25.5
108.1
125.2
0 20 40 60 80 100 120 140
White
Non-
Hispanic
Af. Am.
Non-
Hispanic
Hispanic
Rate Per 1000
Pregnancy Rate Ages 18-19
By Race and Ethnicity Wake County 2010
N=719
Source: North Carolina State Center for Health Statistics
7.7
30.3
50.5
0 10 20 30 40 50 60
White Non-Hispanic
African American-Non-
Hispanic
Hispanic
Rate per 1000
Pregnancy Rate Ages 15-17
by Race and Ethnicity Wake County 2010
N= 335
Source: North Carolina State Center for Health Statistics

18 18
Figure
Pregnancy Rates
WAKE COUNTY HUMAN SERVICES PRENATAL CLIENTS BY AGE 2009-2011
The Wake County Human Services Prenatal Clinic served more teens each year from 2009-2011 (see
Figure 15).
0
20
40
60
80
100
120
140
160
2009 2010 2011
0 08
26
188
17
51
25
53
80
57
98
157
Unduplicated Number
Calendar Year
Number Of Prenatal Clients Ages 15 - 19
Wake County Human Services 2009-2011
Age 15
Age 16
Age 17
Age 18
Age 19
Figure 15
Contact: Roxanne Deter, Public Health Division 919-250-4637 [email protected]
Source: Wake County Human Services Patient Care Management System.

19 19
Healthy North Carolina 2020 Objectives
Tobacco Use Current 2020 Target
1. Decrease the percentage of adults who are current smokers 20.3% (2009) 13.0%
2. Decrease the percentage of high school students reporting current use of any tobacco
product
25.8% (2009) 15.0%
3. Decrease the percentage of people exposed to secondhand smoke in the workplace in
the past seven days
14.6% (2008) 0%
Physical Activity and Nutrition Current 2020 Target
1. Increase the percentage of high school students who are neither overweight nor obese 72.0% (2009) 79.2%
2. Increase the percentage of adults getting the recommended amount of physical activity 46.4% (2009) 60.6%
3. Increase the percentage of adults who consume five or more servings of fruits and
vegetables per day
20.6% (2009) 29.3%
Injury and Violence Current 2020 Target
1. Reduce the unintentional poisoning mortality rate (per 100,000) population 11.0 (2008) 9.9
2. Reduce the unintentional falls mortality rate (per 100,000) population 8.1 (2008) 5.3
3. Reduce the homicide rate (per 100,00) population 7.5 (2008) 6.7
Maternal and Infant Health Current 2020 Target
1. Reduce the infant mortality racial disparity between whites and African Americans 2.45 (2008) 1.92
2. Reduce the infant mortality rate (per 1,000 live births) 8.2 (2008) 6.3
3. Reduce the percentage of women who smoke during pregnancy 10.4% (2008) 6.8%
Sexually Transmitted Diseases and Unintended Pregnancy Current 2020 Target
1. Decrease the percentage of pregnancies that are unintended 39.8% (2007) 30.9%
2. Reduce the percentage of positive results among individuals aged 15 to 24 tested for
chlamydia
9.7% (2009) 8.7%
3. Reduce the rate of new HIV infection diagnoses (per 100,000) population 24.7% (2008) 22.2
Substance Abuse Current 2020 Target
1. Reduce the percentage of high school students who had alcohol on one or more of the
past 30 days
35.0% (2009) 26.4%
2. Reduce the percentage of traffic crashes that are alcohol-related 5.7% (2008) 4.7%
3. Reduce the percentage of individuals aged 12 years and older reporting any illicit drug
use in the past 30 days.
7.8%
(2007-2008)
6.6%
Every ten years since 1990, the state of North Carolina sets objectives aimed at improving the health of North
Carolinians. Below are the objectives that are set for the year 2020 organized by focus area. The Wake
County Human Services Public Health Report is organized to align with selected Healthy North Carolina
2020 Focus Areas and Objectives For more information about North Carolina’s health objectives and how
they are decided, visit the North Carolina Division of Public Health web page at http://publichealth.nc.gov/
hnc2020/objectives.htm.

20 20
Mental Health Current 2020 Target
1. Reduce the suicide rate (per 100,000 population) 12.4 (2008) 8.3
2. Decrease the average number of poor mental health days among adults in the past 30
days
3.4 (2008) 2.8
3. Reduce the rate of mental health related visits to emergency departments (per 100,000)
population
92.0 (2008) 82.8
Oral Health Current 2020 Target
1. Increase the percentage of children aged 1-5 years enrolled in Medicaid who receive
any dental service during the previous 12 months
46.9% (2008) 56.4%
2. Decrease the average number of decayed, missing or filled teeth among kindergartners 1.5 (2008-09) 1.1
3. Decrease the percentage of adults who have had permanent teeth removed due to tooth
decay or gum disease
47.8% (2008) 38.4%
Environmental Health Current 2020 Target
1. Increase the percentage of air monitor sites meeting the current ozone standard of 0.075
ppm
62.5%
(2007-09)
100.0%
2. Increase the percentage of the population being served by community water systems
(CWS) with no maximum contaminant level violations (among persons on CWS)
92.2% (2009) 95.0%
3. Reduce the mortality rate from work-related injuries (per 100,000 equivalent full time
workers )
3.9 (2008) 3.5
Infectious Disease and Foodborne Illness Current 2020 Target
1. Increase the percentage of children aged 19-35 months who receive the recommended
vaccines.
77.3% (2007) 91.3%
2. Reduce the pneumonia and influenza mortality rate (per 100,000 population) 19.5% (2008) 13.5%
3. Decrease the average number of critical violations per restaurant/food stand 6.1 (2009) 5.5
Social Determinants of Health Current 2020 Target
1. Decrease the percentage of individuals living in poverty 16.9% (2009) 12.5%
2. Increase the four year high school graduation rate 71.8%
(2008-09)
94.6%
3. Decrease the percentage of people spending more than 30% of their income on rental
housing
41.8% (2008) 36.1%
Chronic Disease Current 2020 Target
1. Reduce the cardiovascular disease mortality rate (per 100,000 population) 256.6 (2008) 161.5
2. Decrease the percentage of adults with diabetes 9.6% (2009) 8.6%
3. Reduce the colorectal cancer mortality rate (per 100,000 population) 15.7 (2008) 10.1
Cross Cutting Current 2020 Target
1. Increase average life expectancy (years) 77.5 (2008) 79.5
2. Increase the percentage of adults reporting good, very good, or excellent health 81.9% (2009) 90.1%
3. Reduce the percentage of non-elderly uninsured individuals (aged less than 65 years) 20.4% (2009) 8.0%
4. Increase the percentage of adults who are neither overweight nor obese 34.6% (2009) 38.1%

21 21
We wish to thank all staff for their daily efforts toward improving the health and safety of the citizens
of Wake County.
Contributors to this Public Health Quarterly Report are:
Edie Alfano-Sobsey
Roxanne Deter
JoAnn Douglas
Brian McFeaters
Andre Pierce
Michelle Ricci
Ronda Sanders
Ramsay Hoke
Yvonne Torres
May 18, 2012
A c k n o w l e d g e m e n t s

INFORMATION
ITEMS
• Board Fund Report (Separate)
• Articles
• Housing Multi-Family Development Loans
• LME Financial Reports 6-19-12
• Committee Reports/Minutes
• Commissioners’ Agenda Items Related to HS&ES June 2012

Proposed psychiatric hospital in Wake years away By John Murawski - [email protected]
The News & Observer - May 30, 2012
On any given day WakeMed hospital in Raleigh is caring for mentally ill residents who may be suicidal, psychotic and dangerous. These patients spend anywhere from several days to several weeks down the hall from people recovering from physical illnesses, car wrecks and other accidents because there’s nowhere else for them to go.
Relief may be on the way. UNC Health Care’s proposal, announced last week, to build a 28-bed psychiatric hospital in Wake County is designed to address the problem of mentally ill patients who are crowding emergency rooms and hospital wards throughout Wake County and the region.
“They will stay in the emergency department for hours and days,” said Jack Naftel, vice-chair of clinical affairs in the psychiatry department at UNC-Chapel Hill. “Just imagine someone with a heart attack waiting days to get upstairs for a bed.”
But despite the pressing need, the $30 million hospital could take at least several years to become reality.
Indeed, there’s no guarantee it will win all necessary approvals, although rival WakeMed, which often challenges other hospitals for available beds, has already signed off on the project. That’s because the hospital is part of the deal UNC and WakeMed hammered out to get WakeMed to drop its hostile takeover bid for UNC-owned Rex Hospital. WakeMed officials have long argued that their facilities treat a disproportionate share of the region’s poor, uninsured and mentally ill.
Still, the public handshakes and photo ops belie the hurdles ahead. Simply preparing all the necessary paperwork to submit applications to build a hospital is expected to take a year. It may also require fending off opposition from such health care providers as Holly Hill Hospital, a cross-town competitor and the only private hospital in the county that specializes in psychiatric services.
Groundwork
But first UNC must persuade state officials to increase their need projections for psychiatric beds in Wake County, a number that sets a limit on hospital construction.
In this case, however, much of the groundwork for UNC’s proposal has already been done. UNC and Wake County spent nine months researching need and concluded that 28 more beds are needed in the county, the same amount proposed for the new UNC hospital, said Wake County Manager David Cooke.
That study shows that the psychiatric beds will generate revenue from a newly created financial source: the Affordable Care Act, dubbed by some as Obamacare. The controversial law, which is

being reviewed by the U.S. Supreme Court and could be overturned this summer, would reduce the number of uninsured individuals and expand Medicaid coverage, providing “a much increased revenue stream to support Medicaid substance abuse services” that are in high demand by the mentally ill.
The state is currently estimating a need for just 12 psychiatric beds in its draft 2013 medical facility projection. UNC will request a revision of the final projection to at least 28 new psychiatric beds. Revising the annual limit by petition happens almost every year, usually in the area for hospice beds, and is often granted, said Julie Henry, a spokeswoman for the N.C. Department of Health and Human Services.
The state’s 2012 projection set the limit at 37 beds, and Holly Hill Hospital requested approval to add the full allotment to its facility. A hearing on that request will be held in Raleigh in June. Neither WakeMed nor Rex is objecting to Holly Hill’s application.
If the state does change its 2013 need estimate, UNC – which has not determined where it will build the facility – would have to win approval for the beds through the state’s certificate of need process. It’s not clear whether Holly Hill will view a new mental health hospital in the same county as a competitive threat. Holly Hill officials did not return calls. But a fight would not be surprising in the contentious world of hospitals.
“I would assume Holly Hill would do everything to position itself for a competitive advantage,” said mental health activist Ann Akland, a board member of the Wake County chapter of the National Alliance for Mental Illness. “I doubt they would be overjoyed with UNC entering Wake County.”
Wait times for psychiatric beds have been growing statewide since North Carolina halved the number of beds in its mental hospitals as part of a reform launched in 2001. Dorothea Dix Hospital, which once housed 300 psychiatric beds in Raleigh, is slated to close and now has just 30 patients left. Most of the patients have been moved to Central Regional Hospital, the facility built in Butner to replace Dix, about 40 miles north of Raleigh.
“It was almost like re-institutionalizing all of those people out on a reservation,” Akland said.
The state currently has 2,594 licensed psychiatric beds at county, state and private institutions. But not all are staffed, and some are designated for youth or have other restrictions.
‘If we had 28 beds …’
Putting the 28 needed beds in the Dorothea Dix building is not an option because the aging facility would not meet modern building standards and would have to be renovated, officials said.
The problem of mentally ill patients overflowing to hospitals has become more acute especially in the last several years, said Jim Hartye, manager of behavior health services in the WakeMed

system. He said WakeMed treats between five and 18 mentally ill patients a day, with an average stay of 2.5 to 3 days, with “some staying multiple weeks.”
Hartye said that at WakeMed the patients are assigned to rooms and are visited by a staff psychiatrist, but the hospital is not a psychiatric unit that provides comprehensive treatment to the mentally ill. He said it’s especially difficult to transfer patients who are disruptive or violent, or those who are older and ill.
“I don’t think there’s ever such a thing as ‘solve’ in the mental health profession,” Hartye said. “If we had 28 beds that can take patients who are highly complex, then that would be a huge help.”
Murawski: 919-829-8932


HUMAN SERVICES AND ENVIRONMENTAL SERVICES
BOARD AGENDA ITEM
Agenda Date: June 28, 2012
Committee/Item: Housing and Community Revitalization/Multifamily Housing
Development Loans
Specific Action Requested: Information Only. To receive an update on funding
recommendations made by the Housing and Community Revitalization Committee
Item Summary:
**On June 4th The Wake County Board of Commissioners approved the following loans: The applications recommended for funding are:
1. Timber Spring Apartments, Garner – 48 units for seniors
Developer: Evergreen Construction Company
Evergreen Construction Company has requested funding of up to $480,000 on behalf of the ownership entity to be formed, Timber Spring Housing Associates, LLC, for the construction and permanent financing of Timber Spring Apartments. Timber is located in Garner, near the intersection of Timber Drive and New Rand Road. The Mayor of Garner has written a letter of support for the development. The loan terms requested for the Wake County loan are 1% interest during construction and 1% interest for the permanent loan with a 30 year term. At least $198,339 would be repaid over 29 years; the remainder would be repaid as a balloon in year 30. During construction, Wake County would hold second lien position with a bank construction loan in first lien position. In the permanent phase, Wake County would hold third lien position with a bank loan in first lien position and a NC Housing Finance Agency loan in second lien position. The funding source for this loan would be Federal HOME and Federal HOPWA funds.
Lender Funding Request
Bank $ 750,000 NC Housing Finance Agency Loan $ 720,000 Wake County $ 480,000 State Tax Credit Loan $ 572,177 Federal Tax Credit Equity $ 4,307,752 Total $ 6,829,929 The bank loan has not yet been secured because the development is in the early stages, however, banks generally need to be in first lien position and will not subordinate to public lenders. Per the County’s lien position policy, Wake County has

asked NC Housing Finance Agency to share second lien position. The NC Housing Finance Agency has declined this request. The development will add 12 units affordable to seniors earning at or below 30% AMI (currently $19,200 per year for a two person household) and 12 units affordable to seniors earning at or below 40% AMI (currently $25,570 per year for a two person household). The remaining 24 units will be affordable to seniors earning at or below 60% AMI (currently $38,400 per year for a two person household). Evergreen Construction expects construction to be complete before December 31, 2014.
2. Willow Creek Apartments, Cary – 53 units for seniors
Developer: DHIC, Inc.
DHIC, Inc. has requested funding of up to $530,000, on behalf of the ownership entity to be formed, Willow Creek Seniors, LLC, for the construction and permanent financing of Willow Creek Apartments. Willow Creek is located in Cary, near the intersection of Davis Drive and Morrisville Parkway. The Cary Town Manager has written a letter of support for this development. The loan terms requested for the Wake County loan are 1% interest during construction and 1% interest for the permanent loan with a 21 year term. At least $207,037 would be repaid on an annual basis over 20 years; the remainder would be paid as a balloon in year 20. During construction, Wake County’s loan would hold second lien position with a bank construction loan in first lien position. In the permanent phase, Wake County would hold third lien position with a bank loan in first lien position and the NC Housing Finance Agency loan in second position. The funding source for the loan would be Federal HOME funds.
Lender Funding Request
Bank $ 500,000 NC Housing Finance Agency Loan $ 795,000 Wake County $ 530,000 NeighborWorks Loan $ 250,000 State Tax Credit Loan $ 718,879 Federal Tax Credit Equity $4,652,692 Deferred Developer Fees $ 44,689 Total $7,491,260 The bank loan has not yet been secured because the development is in the early stages, however, banks generally need to be in first lien position and will not subordinate to public lenders. Per the County’s lien position policy, Wake County has asked NC Housing Finance Agency to share second lien position. The NC Housing Finance Agency has declined this request. The development will add a total of 14 units affordable to seniors earning at or below 30% AMI, (currently $19,200 per year for a two person household) and seven units affordable to seniors earning at or below 40% AMI, (currently $25,570 for a two person household). The remaining 32 units will be affordable to seniors earning at or below 60% AMI (currently $25,570 per year for a two person household).

DHIC, Inc. expects construction to be complete before December 31, 2014.
3. Holly Woods Apartments, Holly Springs - 64 units for Families in Holly
Springs
Developer: Halcon Development
Halcon Development has requested funding of up to $640,000 of behalf of Holly Woods LLC, the ownership entity to be formed for the construction and permanent financing of Holly Woods Apartments. Holly Woods Apartments is located in on Lassiter Road near the intersection of Sunset Lake Road in the town of Holly Springs. The Holly Springs Town Manager has written a letter of support for this development. The developer has requested Wake County funds for permanent and construction financing. During construction, Wake County’s loan would hold second lien position with a bank construction loan in first lien position. In the permanent phase, Wake County would hold second lien position with a bank loan in first lien position. The loan terms requested for the Wake County loan are 1% interest during construction and 1% interest for the permanent loan with a 30 year term. At least $230,157 would be repaid on an annual basis over 25 years; the remainder would be paid as a balloon in year 30. The funding source for this loan would be County CIP funds.
Lender Funding Request
Bank $2,550,000 Wake County Loan $ 640,000 State Tax Credit Loan $ 724,108 Federal Tax Credit Equity $5,167,044 Total $9,097,235 The bank loan has not yet been secured because the development is in the early stages, however, banks generally need to be in first lien position and will not subordinate to public lenders. The development will add a total of 16 units affordable to families earning at or below 30% AMI, (currently $23,950 per year for a four person household) and 17 units affordable to families earning at or below 50% AMI (currently $39,950 for a four person household). The remaining 31 units will be affordable to families earning at or below 60% AMI (currently $47,940 for four person household). Halcon, Inc. expects construction to be complete before December 31, 2014.
4. Whitehall Apartments, Wendell – 24 units for Seniors
Developer: Lucius Jones
Lucius Jones has requested funding of up to $240,000 on behalf of the ownership entity to be formed, Whitehall Housing Associates, LLC, for the construction and permanent financing of Whitehall Apartments. Whitehall is located on East Fourth Street in Wendell. The Mayor for the Town of Wendell has written a letter of support for this development. The developer has requested Wake County funds for permanent and construction financing. During construction, Wake County’s loan would hold second lien position with a bank construction loan in first lien position. In the permanent phase, Wake County would hold third lien position with a bank loan in first lien position and the
NC Housing Finance Agency loan in second position. The loan terms requested for the Wake County loan are 1% interest during construction and 1% interest for the permanent loan with a 30 year term. At least $117,045 would be repaid on an annual basis over 25 years; the remainder would be paid as a balloon in year 30. The funding source for this loan would be Federal CDBG and County CIP funds.
Lender Funding Request
Bank $ 175,000 NC Housing Finance Agency Loan $ 360,000 Wake County Loan $ 240,000 State Tax Credit Loan $ 291,498 Federal Tax Credit Equity $ 2,194,549 Deferred Developer Fee $ 45,000 Owner investment $ 100 Total $ 3,306,147 The bank loan has not yet been secured because the development is in the early stages, however, banks generally need to be in first lien position and will not subordinate to public lenders. Per the County’s lien position policy, Wake County has asked NC Housing Finance Agency to share second lien position. NC Housing Finance Agency has declined this request. The development will add a total of six units affordable to seniors earning at or below 30% AMI, (currently $19,200 per year for a two person household) and six units affordable to seniors earning at or below 40% AMI, (currently $25,570 for a two person household). The remaining 12 units will be affordable to seniors earning at or below 60% AMI (currently $38,400 for a two person household). Lucius Jones expects construction to be complete before December 31, 2014.
5. Granite Falls Apartments, Rolesville – 72 units for Families
Developer: Granite Falls LLC
Granite Falls LLC has requested funding of up to $720,000 for the construction and permanent financing of Granite Falls Apartments. Granite Falls is located off Rogers Road in Rolesville. The Mayor for the Town of Rolesville has written a letter of support for this development. During construction, Wake County’s loan would hold second lien position with a bank construction loan in first lien position. In the permanent phase, Wake County would hold second lien position with a bank loan in first lien position. The loan terms requested for the Wake County loan are 1% interest during construction and 1% interest for the permanent loan with a 30 year term. At least $494,500 would be repaid on an annual basis over 29 years; the remainder would be paid as a balloon in year 30. The funding source for this loan would be Federal HOME and County CIP funds.

Lender Funding Request
Bank $ 1,816,660 Wake County Loan $ 720,000 State Tax Credit Loan $ 941,316 Federal Tax Credit Equity $ 6,162,369 Total $ 9,640,346 The bank loan has not yet been secured because the development is in the early stages, however, banks generally need to be in first lien position and will not subordinate to public lenders. The development will add a total of 18 units affordable to families earning at or below 30% AMI (currently $39,950 for a four person household). The remaining 54 units will be affordable to Families earning at or below 60% AMI (currently $47,940 for four person household). Granite Falls LLC expects construction to be complete before December 31, 2014.
Next Steps:
North Carolina Housing Finance Agency will decide which developments receive tax credits by August 15th
Attachments:
Opportunities for Advocacy, Policy or Advisory:
Connections to Other Committees:





1
Wake County Human Services Board
Social Services Advisory Subcommittee
Friday, May 4, 2012
9:00 am – 10:30 am
Swinburne Building, Room 5032
Minutes
Board Members:
Paul Norman
Guest:
Lisa Cauley
Committee Members:
Angie Welsh
Anna Troutman
Dudley Flood
Marjorie Menestres
Staff:
Janny Flynt
Katherine Williams
Liz Scott
Nikki Lyons
Vielka Maria Gabriel
Warren Ludwig
Agenda
Item
Discussion, Conclusions, Recommendations Action,
Follow-up
Responsible
Party
Due Date
I. Welcome
&
Introductions
The meeting was called to order at 9:00 p.m.
Paul
Norman
II. Review
and approval
of the
minutes
Minutes were reviewed and were accepted.
Vielka
Gabriel

2
III. Business
Discussion
And Updates
Child Abuse Prevention Summit Update:
• Summit was held on April 23, 2012 – 8:30 am – 12:00 noon - JC Railston Arboretum
• 106 Attended the summit
• Committee is scheduled to meet next week at the Safe Child office on West Morgan
St. to discuss the outcomes of the summit.
Follow Up Discussion: Child Welfare – Presented by Warren
• Warren’s recapped and update of Lisa Cauly brief presentation to the WCHS Board in
April regarding the upcoming Child and Family Services Review (CFSR).
o CFSR Round III
� Children’s Bureau intends to start Round III of the CFSR in 2012
� North Carolina is scheduled to be the second state reviewed
� Wake County expects to be one of the counties reviewed
� Reviewers are likely to talk with community leaders including WCHS
Board Members
o CFSR Round III has not been scheduled at this time for NC (Wake County).
Round II had not been published. It is a requirement of the Commissioners to
have this document published for review prior to its next review. At this time
Wake County may be delayed until 2013
• Community Child Protection Team: Volunteers are needed to join the team.
o Reviews child death cases not only CPS related
o Has a public health component to make recommendations to reduce child
mortality cases
o The meetings are detailed and very informative regarding the child including
the history of the family (education, siblings, siblings, ect.)
o Group meets the 3rd Thursday of each month.
Action,
Follow-up
Committee
will present
in June the
full report
Responsible
Party
Marjorie &
Ann
Warren

3
Follow Up Discussion: Child Welfare – Presented by Warren
• Family Finding –
o Children’s Home Society (CHS) received a Clark Foundation grant for Family
Finding
o 7 staff will be working to support families of children entering into foster care
o The Family Finding Goals
� Decrease length of stay in foster care through reunification and relative
placements
� Safely divert children from foster care
� Provide foster your with family connections and support
� Improve CFSR performance in areas of engaging relatives and
achieving permanence
� Improve compliance with Federal Fostering Connections law
• First Fostering Bright Futures Graduate: Veronica Armstrong is the first to graduate
from Wake Tech through the Fostering Bright Future. Veronica will be attending
UNC Greensboro in the fall.
Action,
Follow-up
Responsible
Party
Warren
HCD Updates:
• PowerPoint presentation attached
Action,
Follow-up
Responsible
Party
Katherine
W.
V. Next
Meeting
Friday, June 1, 2012
9- -10:30 am ~ Swinburne Building, Board Room. –
Action,
Follow-up
Responsible
Party
VI.
Adjournment
The meeting adjourned at 10:35 am.

Human Services Regional Networks Committee Board - Minutes May 10, 2012
1
Committee Charge: Create advocacy, awareness, and community and political support for the need and value of regional networks of care.
Members Present Human Services Staff Present Agenda
Frank Eagles Benny Ridout
Eugenia Pleasants, NRC CAC Rep
Kat Herndon-Lee, SRC CAC Rep
Bob Sorrels Ross Yeager
Darryl Blevins
Kris Ramsundar Rosena West
Andre Pierce
RNC Secretary
Cindy Rice
I. Call To Order/Welcome II. Western Region Advisory Group
III. Western Region Assessment
-Next Steps -Role of Regional Network Committee -
-Role of Staff IV. Southern Regional Center Update
V. Eastern Regional Center Update
VI. Northern Regional Center Update VII. Millbrook Human Services Center Update
VIII. Good of the Order IX. Adjourn
Agenda Item Discussion Conclusions, Recommendations Action, Follow-up Responsible Party
Due Date
I. Call to Order/Welcome
by Chair
Meeting called to order by Mayor Frank Eagles (Chair).
II. Western Region
Advisory Group
Mayor Eagles had a discussion with Ramon Rojano and
shared his thoughts that an Advisory Committee is key for further development of the Regional Network in the
west. Mayors are in favor a regional center but are
fearful of the pushback from town council & citizens.
Bob Sorrels stated that a Community Advisory Committee is needed in the west regardless of having a
building. Services are already there and we have
integrated intentions. Whether it is a storefront, rented space or a new building we need the same concept as
we have in the other regions and Millbrook.
Form a Community
Advisory Committee for the west
Regional Networks
Committee/Human Services Staff
ASAP
(July-Sept.)

2
Agenda Item Discussion Conclusions, Recommendations Action, Follow-up Responsible
Party
Due Date
III. Western Region Assessment
• Next steps
• Role of Regional
Network Committee
• Role of Staff
Ross Yeager requested clarification with the next steps, role of the Regional Networks Committee and role of
the staff so he can have a better understanding as to his role in moving forward with the west.
Who would be the key people in recruiting/identifying Community Advisory Committee members for the west? Staff could recommend or identify names of key
stakeholders in the western communities to the
Regional Networks Committee including a Chair that is a community member. The staff members located in
the west could serve as staff support to the committee and assist with keeping the Community Advisory
Committee enlightened and engaged. They currently
have relationships with area non-profits & key stakeholders established.
Darryl Blevins indicated that it is critical to appoint
someone to be lead when working with the Community Advisory Committee. There are many facets to the
committee around available services, keeping the
committee members mobilized as outlined in their work plans, and on-going input into service planning. The
concept maybe somewhat different from other regional centers.
Bob Sorrels reminded the Committee of the “Common Cause”, bringing integrated services to a region (not a
building). We currently have a foundation High House/Cornerstone to build upon. The purpose of the
Community Advisory Committee is to advocate for community needs and let the community know what is
already there.
Should we review the Community Advisory Committee functions and/or bi-laws?

3
Agenda Item Discussion Conclusions, Recommendations Action, Follow-up Responsible
Party
Due Date
Each Regional Center has different action plans and/or functions. The west will have their unique action plan
and/or functions as well.
Kris stated that it has been his experience with a community approach that a Community Advisory
Committee is needed.
Are the Committees self-governed? The Regional Network Committee flowchart shows that Human Services/Environmental Services Board oversees
the Regional Network Committee; the Regional Network
Committee oversees the activities of the Community Advisory Committee.
The development of a Community Advisory Committee
and assignment of staff liaisons to Community Advisory Committee has been recommended to the Board. The
Regional Networks Committee will need to submit an
Action Plan outlining the activities that will be undertaken to develop the Committee and submit to
the Human Services Board.
Mayor Frank Eagles has advocated for a Western
Regional Center at the Mayors Association meetings and had discussions with the Mayors of Cary and
Morrisville. It seems that the mayors are having difficulty understanding the service area maps. Mayor
Eagles encouraged them to communicate with their Planning Department.
There would have to be interest in both the public & political arena for this topic to get more attention. The
Mayors’ convincing David Cooke & others builds momentum resulting in serious dialog. As a Human
Services Department, we will continue to deliver
services in all space available offering integrated services for the next 2-3 years. If a Center is built
before that time frame, it would require interest and
Send Action Plan
information to Jonica Hinton before the next
Board Executive Committee meeting.
Mayor Eagles & Ross Yeager
June 1

4
Agenda Item Discussion Conclusions, Recommendations Action, Follow-up Responsible
Party
Due Date
work from the mayors.
Location is key. It doesn’t have to be in Cary. One advantage is that Cary has transportation, C-Tran and
TTA links to Amtrak then to Swinburne.
An important next step is to identify what services are needed/wanted. You can always customize services.
Regional Centers offer same service package but may be different due to uniqueness of needs/demands. The
west has an abundance of resources and is very large.
It is important to build a provider network. Some providers already there include: town services, WTCC,
Employment Security Commission and Dorcas Ministries. Staff and the Community Advisory
Committee can build upon what is already there.
Human Services leaders and David Cooke recently
visited Cornerstone. A storefront expansion was suggested by David Cooke. There is 1700 sq ft
available across the hall from the space we have at Cornerstone. High House offers Mental Health services
only and with the changes to Mental Health we are
unsure of the future. One concept could be to partner with Dorcas Ministries housing Medicaid staff. The CAC
can promote what can be done at these strategic sites.
Benny Ridout suggested that we look to the future (10-15 years). We do not need overlapping of service
areas.
IV. Southern Regional
Center Update
Community non-profits and Southern Regional Center are working together to form a Community Collaborative for the
Fuquay-Varina area. SWFCA (Southern Wake Faith
Community in Action) made up of 12-13 churches
initiated the initiative to encourage relations with area non-profits, local government and community

5
Agenda Item Discussion Conclusions, Recommendations Action, Follow-up Responsible
Party
Due Date
members.
Three priorities include:
• Development of a cooperative provider network
• Build on the Community Resource Connection
model “No Wrong Door for Information”
• Implementing community based Human Capital
Development Strategies, mentoring, coaching, skill building, financial planning, etc.
Project 100 Service Integration
Southern Regional Center is working to develop a plan to incorporate more HCD strategies into daily service
delivery. A better outcome for families is the ultimate goal.
V. Eastern Regional Center
Update
The Action Plan for the Eastern Regional Center Community Advisory Committee is complete. The plan includes: Marketing Services: Eastern Wake TV will spotlight ERC and the 10 year anniversary to be aired on East Wake TV. (Mayor Eagles suggested for Darryl to contact Mayor Matheny to see if he would be interested in being in a video). Community Advisory members will attend council meeting(s) to promote services. Health Promotions for Seniors: Focus on the safety and well-being of community members. ERC Community Advisory Committee members will partner with Sonya Reid, Health Promotions, to develop strategies. Faith partnership; increase service coordination to address service gaps.

6
Agenda Item Discussion Conclusions, Recommendations Action, Follow-up Responsible
Party
Due Date
ERC will celebrate and host a 10 year celebration on October 26
th. Committees and sub-committees for this
event have been formed. Save a date cards will be sent out this month. Darryl will be deploying for military duty at the end of June. Sonya Peterkin, Operations Manager will fill in during his absence.
VI. Northern Regional
Center Update
This was the first year NRC was an early voting site.
Three thousand eight hundred thirty-three (3,833) citizens voted.
The April 21st rabies/microchip clinic was extremely successful and is always a popular community event.
Engaging activities with staff (Amazing Grace-a spin off
from the TV series Amazing Race) around Service
Integration. These activities begin Monday, May 21st. Staff will learn about services offered from other
divisions.
VII. Millbrook Human
Services Center Update
LME will be moving out of the Millbrook building.
Millbrook is currently forming their Community Advisory
Committee. Three meetings have been held with community, business and faith partners to recruit
members. Kris will send all completed applications directly to Mayor Eagles for approval.
Forward CAC
applications to Mayor
Eagles directly. Chair (Mayor Eagles) will
endorse.
Kris Ramsundar
VIII. Good of the Order
IX. Adjourn After hearing no further business, Mayor Eagles
adjourned the meeting. The group will next assemble on Thursday, August 9th, 10am, Swinburne 5040.

DRAFT
1
Environmental Services Committee
May 11, 2012
Library Administration – Wake County Office Park
11:30 a.m. Wake County Board of Commissioner
Present
Human Services Board Members
Present:
Leila Goodwin
Frank Eagles
Melissa Jemison
Human Services Board Members
Absent: Clarence (Benny) Ridout
Jeffrey Smith
Kent Earnhardt
Dianne Dunning
Community Members Present:
Donald Haydon
Ed Buchan
Community Member Absent:
Buck Kennedy
Les Hall
Rodney Dickerson
Bob Rubin
Henk Schuitemaker
Phillip White
Bryan Hicks
John Whitson
Suzanne Harris
Julian Prosser
Paula Thomas
Kenny Waldroup
Glenn Harris
Liz Turpin
Julie Wilkins
Staff Present:
Joseph Threadcraft
Matt Roylance
Andre Pierce
Deborah Peterson
Sue Ledford
John Roberson
Ed Duke
Staff Absent:
Britt Stoddard
Sarah Williamson-Baker
Guests/Others:
Shivani Garg (UNC Chapel Hill Intern)

DRAFT
2
Agenda Item
Discussion, Conclusions, Recommendations Action, Follow-up Responsible Party Due
Date
I. Call to Order
II. Minutes
III. Introduction of
Environmental
Services Committee
Members
Chair Leila Goodwin called the meeting to order at 11:50 A.M.
The April 13, 2012 minutes were approved as written.
Highlights Committee members introduced themselves to Shivani Garg, a UNC
Chapel Hill Intern shadowing Sue Lynn Ledford. Shivani will be
applying to the UNC Chapel Hill Public Health program next year.
Sue Lynn informed committee members that there will be multiple
college interns attending some of the meetings this summer. Interns
will come from East Carolina University, N.C. State University, UNC-
Greensboro, UNC-Winston Salem, Shaw and UNC Chapel Hill. Staff
has been encouraged to allow interns to be a part of their workplace.
Even if this requires some additional time, Sue Lynn reminded
committee members how important it was to cultivate the next Public
Health generation.
Committee
Member
Leila Goodwin
Sue Lynn Ledford

DRAFT
3
Agenda Item
Discussion, Conclusions, Recommendations Action, Follow-up Responsible Party Due
Date
IV. Public Health
Update
Highlights
• The Ecoli State Fair Report is still being finalized. When
complete Sue Lynn will provide a copy to committee members.
• There is a new Communicable Disease (CD) Nurse. Currently
the CD Program is in a transition period while training is taking
place and if issues arise there is a very stable core team
available to assist client/staff.
• There is an increase in vector borne diseases. Staff is
conducting work in the communities to get educational
information out to the public. Sue Lynn encouraged committee
members to utilize the materials available through the
Communicable Disease Program. If there are any venues that
committee members feel this information could be used, please
contact the Communicable Disease Team.
• There was an issue with a rabid fox in Zebulon. Six people
were exposed. Two of the victims were children. Three of the
people involved received treatment. Because of this incident
staff saw an increase in the number of residents attending the
rabies vaccination and microchip clinic held at the Wake
County Eastern Regional Center on Saturday, May 5, 2012.
Two hundred and fifteen animals were vaccinated.
Sue Lynn Ledford

DRAFT
4
Agenda Item
Discussion, Conclusions, Recommendations Action, Follow-up Responsible Party Due
Date
IV. Public Health
Update (Continued)
Highlights (Continued)
• There has been an increase in bat exposure. There have been
pets that have been euthanized due to exposure.
• There were several cases of Salmonella in Buncombe County
that was related to tofu and some other unpasteurized
vegetarian products. There were 2 or 3 restaurants involved.
There were a total of over 60 cases related to this incident. One
case involved a Wake County resident. There were six
different states involved. There was a voluntary recall on some
of the products.
• Parrott owned by a Wake County resident diagnosed by
veterinarian to have died from Chlamydophila psittaci (type of
bird flu). Because this is the second bird owned by this
resident to die from this disease, there will be a more thorough
investigation conducted involving staff and a state veterinarian.

DRAFT
5
Agenda Item
Discussion, Conclusions, Recommendations Action, Follow-up Responsible Party Due
Date
IV. Public Health
Update (Continued)
V. Animal Services
Division Update
Highlights (Continued)
• May 18, 2012 – Symposium/Training held on Mass Fatality
Response (Cultural Issues as it relates to Death and Burial) –
Because of the increase cultural variables in Wake County
there were questions/issues arising that violated the death and
burial laws in the vital records section. Wake County wants to
be sensitive to cultural needs but at the same time the County
must abide by state laws. This training is designed to help vital
records staff, hospitals, funeral homes, etc.
Highlights
• Animal Services Director Position – No candidate chosen from
first set of interviews. 2nd set of interviews conducted. (Since
the May 11, 2012 meeting Dr. Jennifer Federico has been hired
as the new Animal Services Director effective June 1, 2012.
Dr. Federico is a veterinarian with a background in shelter
medicine who has worked as one of the Wake County Animal
Center's veterinarians for approximately one year. She has
tremendous knowledge of animal health and medical issues, as
well as an excellent understanding of how the Wake County
Animal Center operates.)
Matt Roylance

DRAFT
6
Agenda Item
Discussion, Conclusions, Recommendations Action, Follow-up Responsible Party Due
Date
V. Animal Services
Division Update
(Continued)
VI. Proposed Food
Code Changes
Highlights (Continued)
• TNR Ordinance – Because staff and the Cat Committee could
not come to an agreeable ordinance, the Board of
Commissioners requested staff work with the Cat Committee to
develop two versions for their review. One issue is that staff
would like to have a registered contact should there be issues
with one of the colonies of cats. (At the time of this May 11,
2012 meeting an agreement had not been reached on this
registered contact issue. These draft ordinances were brought
before the Board of Commissioners at their May 21, 2012
meeting. Update to be given at the next meeting.)
Highlights
• FDA prepares a food code every 4 years. The Conference for
Food Protection met this year. During this Conference each
state had 2 votes. North Carolina voted for food codes this
year. North Carolina regulators and industries participate in
this very involved, extensive and technical process.
Andre Pierce

DRAFT
7
Agenda Item
Discussion, Conclusions, Recommendations Action, Follow-up Responsible Party Due
Date
VI. Proposed Food
Code Changes
(Continued)
Highlights (Continued)
• In 2009, Wake County conducted an assessment of the North
Carolina rules as compared to the 2005 FDA Food Code and
the practices of the North Carolina rules were 50% compliant
with the 2005 FDA Food Code.
• There were some gaps identified in the in the State rules. They
involved:
(1) Barehanded Contaminant
(2) Cold Holding Temperatures
(3) Date Marking
(4) Employee Health Policies
(5) Consumer Advisory
(6) Special Food Processes
(7) Emerging Science
• When North Carolina adopts the 2009 Food Code it will be
used as a model for operating. In North Carolina the rule
making is centralized. Counties do not have the authority to
develop ordinances on food codes. In some States this is not
the case and therefore when going from one jurisdiction to
another there maybe complications in interpreting the rules.

DRAFT
8
Agenda Item
Discussion, Conclusions, Recommendations Action, Follow-up Responsible Party Due
Date
VI. Proposed Food
Code Changes
(Continued)
VII. Solid Waste 10
Year Plan Update
Highlights (Continued)
Proposed Schedule for FDA Code Adoption:
5/16/12----------Commission for Public
6/21/12----------Rules Review Commission
7/01/12----------Adoption
9/1/12------------Implementation
Highlights
• The Solid Waste 10 Year Plan has been approved by Cary,
City of Raleigh, Fuquay-Varina and Zebulon. Short
presentations are scheduled to be for the other Towns.
• Goal – Submit to the State by June 30, 2012
John Roberson

DRAFT
9
Agenda Item
Discussion, Conclusions, Recommendations Action, Follow-up Responsible Party Due
Date
VIII. Update on Septic
System Subcommittee
IX. Adjourn
Highlights
• The Septic System Subcommittee contains members of the
Public Health Committee and Environmental Services
Committee. They’ve had two meetings thus far. Leila
Goodwin will send copies of the work plan which shows future
scheduled meetings. Currently this committee is in education
mode and has had several experts to come in and speak to the
group. There will be stakeholders input build into this process.
There will be point where the Septic System Subcommittee
will come before the Environmental Services Committee with a
presentation and ideas and start getting feedback on the
direction they may be headed.
THE JUNE ENVIRONMENTAL SERVICES COMMITTEE
MEETING WILL BE CANCELLED. THE NEXT MEETING IS
SCHEDULED FOR FRIDAY, JULY 13, 2012 @ THE LIBRARY
ADMINISTRATION BUILDING, WAKE COUNTY OFFICE
PARK, ROOM 102,
4020 CARYA DRIVE.
Leila Goodwin

Wake County Human Services Board LME Advisory Committee Meeting Community Services Center – 401 E. Whitaker Mill Road, Rm. 210
Minutes – May 15, 2012
Members Present: Staff Present: Guests/Community:
Ms. Stephanie Treadway, Committee Chair / HS Board
Mr. Pablo Escobar, Committee Vice Chair / HS Board
Dr. Jim Hartye, Horizons Healthcare / WakeMed
Ms. Melissa Jemison, HS Board
Members Absent:
Dr. Kent Earnhardt, HS Board / HRC
Ms. Rhonda Spence, Advocate
Ms. Crystal Farrow, Crisis Services Director
Ms. Denise Foreman, Assistant to the County Manager
Mr. Paul Gross, HS Finance Officer
Dr. Carlyle Johnson, LME Administrator
Ms. Beth Nelson, Networks Development
Mr. Ramon Rojano, HS Director
Mr. Grady Britt, Advocate
Mr. Tad Clodfelter, SouthLight, Inc.
Agenda Item
Discussion, Conclusions, Recommendations, Follow-up
Call to Order The LME Advisory Committee meeting, facilitated by Ms. Stephanie Treadway, opened at 12:05 p.m.
Approval of Minutes
Upon motion by Mr. Pablo Escobar, seconded by Ms. Melissa Jemison, the committee approved the April 17, 2012, committee minutes.
Agenda Items
Agenda: •Business/Finance Report •New Item: Crisis Services & DHSR •Consultant’s WCBHS Strategic Planning Final Report •LME Director/Administrator Updates •MCO Transition Updates •Good of Order

Agenda Item
Discussion, Conclusions, Recommendations, Follow-up
LME Budget/ Finance Report
Mr. Paul Gross and Ms. Beth Nelson presented the LME Monthly Financial Reports as of May 15, 2012. The committee reviewed and discussed the reports. Highlights included:
• Mr. Gross said last month the LME projection for Purchase of Services UCR overspending was $800,000. However, this month, the new projection is $722,956. Mr. Gross estimated the projection at fiscal year end to be between $580,000 - $590,000. Within the next few days, the county will transfer uncommitted LME Systems Administration dollars to cover the overspending.
• HHH inpatient expenditures are on target with FY12 budget projections (under by $1,192). HHH is expected to open additional beds on June 1st, and this could impact the figure during June for the FY12 budget. Demand is high at HHH.
• The state has fixed the glitch in their system for funding drawdown of IPRS UCR earnings in the Child Mental Health category, and the LME has drawn down the earnings at 100%.
Discussion on County Budget FY13: • Ms. Foreman said the county plans to have a funding cap for the MCO and Co./HHH contract. The county, MCO, and HHH
are in re-negotiations with the Co./HHH contract and anticipate having it finalized by June 30.
• Ms. Crystal Farrow said the question will be what to do with unfunded Wake County clients—this is still an unfilled gap in the continuum.
Committee Request: Suggested that the county approach the state for 3-way contracts. Urged to act fast, because State Legislators are considering these contracts now and the opportunity may be gone by next week.

Agenda Item
Discussion, Conclusions, Recommendations, Follow-up
Discussion of Consultant’s Wake County Behavioral Health Strategic Planning Final Report
A Steering Committee with representation from Wake County, the University of North Carolina Health Care System (UNC Health Care), and the North Carolina Department of Health and Human Services (NCDHHS) commissioned a consultant team in August 2011 to analyze behavioral health services in Wake County. The overall purpose of the project was to identify gaps and plan for how best to utilize county resources to meet anticipated growth in the behavioral health population in need of services amidst the challenges associated with federal health care reform as well as local and state changes in the service management and delivery system for this population. Seven (7) key strategic objectives were identified. The full report and the county manager’s presentation can be viewed at the Board of Commissioner’s meeting agenda page: Work Session May 14, 2012. One outcome of the study was a proposed framework for an enhanced partnership between Wake County, UNC Health Care, and Alliance Behavioral Healthcare (MCO). A formal agreement among the parties is being developed with many details yet to be determined prior to consideration by the Board of Commissioners, currently slated for an August 2012 meeting. Discussion: • The county provides $20 million in local dollars for MH/DD/SA services. The county asked UNC to advise them on how to
use the $20 million. UNC has many years of expertise in mental health services.
• The committee discussed the background, overview, key findings, and recommendations of the final report. Ms. Foreman said the report provides good data to help inform decisions. The primary goal is to not have any conflicts of interest in WCBHS as of January 1, 2013. There are opportunities for improvements and partnerships for the spectrum of services. Wake County, UNC and MCO are at the table and will work together.
• UNC will help with the transition. The transition period is 18 – 24 month.
• Ms. Foreman said the county is trying to be transparent and trying to share as much information upfront as possible. There are many details to work out. She pointed out that the county could wait until September when the plan has been developed, but it would not be as inclusive. She said the county preferred to get input first, because we don’t know all of the answers.
• Mr. Tad Clodfelter and Dr. Jim Haryte commented that some oversight is needed to ensure no cherry picking of services. Mr. Rojano said the MCO Board has oversight and that committee members are free to discuss it with them.

Agenda Item
Discussion, Conclusions, Recommendations, Follow-up
New Item: 24-hr. Stay Issue with Crisis Services and Department of Health Services Regulations Mr. Ramon Rojano and Ms. Crystal Farrow
Mr. Rojano and Ms. Farrow gave an overview of a new situation that happened this week.
24-hour Stay Issue at Crisis Services: The new manager of the Guilford Center phoned Department of Health Services Regulations asking if they needed a license to keep people more than 24 hours at the crisis center. This call prompted an investigation and DHSR found that Wake was also holding patients for more than 24 hours in a non-licensed facility (WakeBrook downstairs). DHSR toured WakeBrook on May 1.
DHSR defines stays over 24 hours as a licensed facility.
Ms. Farrow said the single largest contributing factor is the state hospital level of care. The lack of state beds is forcing Crisis Services to hold people longer. Mr. Rojano said this is ten percent of the people served. Ms. Farrow said Crisis Services is near to doubling its budget for overtime and staffing.
If Crisis Services cannot hold people beyond 23 hours, they would need to send the patients to the ED, in which they would start over on the wait list.
Jan.-April, 2012: total visits to Crisis Services total 1,819, of those 734 patients were sent to an inpatient setting. The total number that stayed longer than 23 hours was 181 (or 10%) people, of this group the average length of stay was over three days per person, with the longest length of stay being 16 days.
One out of ten is adolescent. The new PRTF Facility in Garner, opening in September, will help with adolescent services.
Also, on July 1, it will be the Alliance Behavioral Healthcare (MCO) responsibility to make these decisions.
Wake County told DHSR that the solution would need to come from the state.
After the meeting with Wake County, DHSR said they would discuss the situation with the DHHS Secretary to see what route to pursue.
Good of Order • Chair Treadway asked if the MCO would be setting up an advisory committee. The committee agreed that the question for the MCO Board is how do you see the MCO Board staying in touch with Wake County issues.
• Chair Treadway said that she wants the HS&ES Board and BOC to recognize the Mental Health Authority for providing 50 years of services. She has asked Dr. Johnson to prepare a resolution in recognition. Mr. Rojano offered to assist. This item was moved to the June Board meeting agenda.
• Dr. Johnson announced that Alliance Behavioral Healthcare (MCO) will be hosting several Town Hall Meetings to provide information and to answer questions. The meetings are open to providers, advocates, and consumers. He offered to email information about the meeting being held on May 29.
Meeting Adjourned
Meeting adjourned at 2:07 pm. Next meeting is June 19, 2012, CSC 12:00 pm– 2:00 pm

Public Health Committee Meeting Minutes –18 May, 2012
Committee Members Present: Benny Ridout, Leena Mehta, Barbara Ann Hughes, Penny Washington, Sharon Foster, Anne McLaurin, Ann Rollins, Burton Horwitz, Barbara Ann Hughes, Lynette Tolson Staff Members Present: Peter Morris, Randy Marsh, Andre Pierce, Edie Alfano-Sobsey, Michelle Ricci Guests: Kristina Wharton, (NCSU
Agenda Items
• Welcome • Approval of Minutes • Chair’s Privilege • Human Services and Environmental Services Board (Board) Advocacy
Agenda • Obesity/Overweight • Public Health Quarterly Report • Behavioral Health Update
Welcome and Call to Order Benny Ridout
Benny called the meeting to order. Benny welcomed new committee member, Lynette Tolson. Committee members and staff introduced themselves.
Approval of Minutes
Benny asked for a motion to approve the minutes. Barbara Ann Hughes made a motion that was seconded by Penny Washington. The minutes were unanimously approved.
Chair’s Privilege Benny Ridout Update on Wastewater Treatment Systems (Septic Tank) Subcommittee
The first meeting of the wastewater treatment system subcommittee focused on the problem of failing septic systems and where they are located in Wake County. The second meeting was a visit to the NC State farm to observe working septic systems and learn more about how they function. A report was made on the causes of septic tank failures; maintenance is a primary issue. Some homeowners are not aware that they have septic systems. The subcommittee will be discussing ways to address septic tank failures and developing recommendations to move to the Board and County Commissioners. Discussion included:
• Noting individual and community consequences of failed septic systems both
in terms of disease and effects on the drinking water supply.
• Next steps include a review of literature and studies. Edie Alfano-Sobsey and
a representative from the NC Department of Public Health will make a
presentation at the next meeting.
• The benefits of visiting the facility at the NC State were increased
understanding and realization of the quality of the facility. People from
different parts of the country train there.
• The close tie between septic tanks and wastewater management.
• The importance of and venues for education about septic systems. Realtors
do provide information from the County about septic tanks and their
maintenance.

Public Health Committee Meeting Page 2
Advocacy Agenda Sharon Foster
Purpose: Continue discussion on the Board advocacy priority “Decrease disparities in key disease indicators such as infant mortality and chronic disease morbidity and mortality.” Action: Identify strategies to engage stakeholders in this advocacy item. The Board has several priorities in each of the divisions in Human Services. The one that bubbled up from Public Health Committee is “Decrease disparities in key disease indicators such as infant mortality and chronic disease morbidity and mortality.” The Executive Committee has asked that the audience and the specifics of how this will be accomplished be identified. When speaking with the Legislative Committee, the focus was on use of better technology, specifically through NC FAST, as a way to get clients and providers through the Medicaid system expediently. This combined with making reimbursement more competitive will increase the economic feasibility of taking Medicaid clients for both medical and dental providers. Advocacy efforts also support the educational campaigns that increase enrollment. There are many uninsured children who would qualify for Medicaid Health Choice; parents may be unaware they are eligible or have not taken the time to enroll. The enrollment form is 2 pages and the state has been able to enroll more children than any other state.
Stakeholders identified for further education so far are:
• Physicians need to be at the top of the list—especially those practitioners who may not participate in grand rounds types of educational offerings.
• The Wake Delegation. The advocacy work group foresees meeting with the delegation a couple of times a year to educate about disparities and advocate for ways to decrease them.
• Community groups such as community advisory councils. Sue Lynn has been making presentation to the faith community about disparities in heart disease, hypertension, obesity, cancer etc.
Discussion included:
• The North Carolina Council of Churches has partners in Health and Wellness that covers an 8 county district. Poe Center for Health Education partnered with the Council; a registered dietitian wrote a four series health and wellness curriculum for faith based organizations that included the organization as well as the hostess.
• Focusing on 2-3 disease disparities. The number one priority is obesity. Take this as our chronic disease for adults and children. Addressing this impacts other chronic diseases and infant mortality as well.
• STI’s. Addressing this disparity would impact infertility issues as well. Physicians are quantitated on how many of their female patients are screened for STI’s. One of the challenges in screening sexually active females in a pediatric practice is that the test goes on the parent’s bill which affects confidentiality.
• Conversations about Medicaid need to be more specific. While everyone is looking for better Medicaid rates, that may not happen because of the budget. For example, if the focus is on maintaining Medicaid rates for children, for dental Medicaid for dentists who see children, it’s a much easier audience

Public Health Committee Meeting Page 3
than if the focus is on Medicaid rates for providers. • Overhead for the average dental office is 65 to 75%. Participation in Medicaid
has been decreasing; there has not been any adjustment upward in a number of years. The costs of dentistry are much smaller but they are an important part of overall heath. More children are missing school from dental problems than any other reason.
• Medicaid will likely have to make cuts due to lack of money. If Medicaid reimbursements are increased, where will the cuts be elsewhere? That needs to be considered in advocacy.
• Someone needs to advocate for increasing taxes to get more revenue and the health of our population is important to do that
• Ann Rollins offered to send information about HB 503 along with talking points to Michelle to forward to committee members if members want to advocate on something that will have an impact in the next few weeks.
• The talking points address that getting more Medicaid may not be possible; the Board and Committee can advocate for maintaining and making it more efficient and use other means like advocacy in the faith community at the grass roots level without funding to help address issues such as obesity.
• Are there Spanish speaking advocates to work with Spanish churches? The Latino community is impacted by health disparities and there are great educational needs.
• School based health centers were suggested however that may limit efforts as those centers don’t address STDs.
• There was a bill in the legislature recently because of a parent whose child was being treated for an STD without the parent’s knowledge. Advocacy efforts should proceed with care in this area.
• Adult clinics should be able to screen those who are sexually active but the younger population 15-19 with very high chlamydia rates is not being screened because of confidentiality issues.
• Do the schools have wellness policies, are they being implemented and monitored. That may not take additional funding.
• The Legislature may do more with tobacco prevention than previously thought; can address comments to Wake County representatives
• One third of the Child Fatality Task Force’s recommendations are related to infant mortality reduction their agenda could be sent out.
• Additional stakeholders might be Parks and Recreation, the Y, Poe Center, Boys and Girls Club
• The medical home concept is spreading. To become a medical home one must participate in quality improvement initiatives. When initiatives are met, reimbursements increase. That is a positive way to entice physicians into developing strategic plans in client care.
Overweight/Obesity Benny Ridout Leena Mehta
Purpose: Continue discussion from March meeting on Committee activities to address Board and Committee priority of overweight /obesity. Action: As determined by discussion. Leena provided the following outline of the strategic planning process for the Healthy Weight Stakeholders group. The group is ready to move into the gap/analysis and prioritization phase of its work having been successful in the discovery phase. Leena highlighted each phase for the committee. WAKE COUNTY HEALTHY WEIGHT PROGRAM (DRAFT SHELL FOR PLANNING)
I. Discovery Phase
Public Health Committee Meeting Page 4
a. Purpose
b. Vision
c. Possible Assumptions & Barriers
d. Data or Information Gathering
e. Stakeholder Impact Analysis
f. Gap Analysis
g. Prioritization for Approach in Phases
II. Planning Phase (TBD)
a. Determine Phases
b. Taskforce Governance
c. Partnerships/Collaborations
d. People, Process, Technology
e. Communications/Training
III. Design & Development Phase (TBD)
IV. Implementation (TBD)
DISCOVERY PHASE:
PURPOSE:
Prevent overweight and obesity in Wake County by:
• Promoting a healthy living environment
• Build an agenda for community health improvement
• Assess Wake County health status in general
• Making healthy weight initiatives visible in the community
• Tracking behaviors -lifestyle, nutrition, and exercise of people living in Wake
County
• Empower people to assess their health status
VISION:
Build a healthy community in Wake County where all residents are able to live, work,
play in a healthy environment and maintain a healthy lifestyle.
SCOPE OF PROGRAM:
(What is healthy environment and how can it be provided so that Wake County
residents may live, work, and play to create and maintain a healthy lifestyle)
ASSUMPTIONS (possible, depending on the Plan Phase TBD):
• Support from Wake County Schools
• Support from Food and Beverage Industry
• Support from local Hospitals
• Support from local places of worship
• Support from Foundations (business organizations and philanthropic)
• Support from stakeholders mentioned below

Public Health Committee Meeting Page 5
CONSTRAINTS/BARRIERS (perceived):
• Policies at School, Work, and Community
• Accessibility to affordable fruits and vegetables
• Physical Activity time in Schools
• Vending machines
• Super sizes
STAKEHOLDERS:
• Wake County Department of Health:
o Data Subcommittee:
� BRFSS (Behavioral Risk Factor Surveillance System)
� NC-NPASS (NC Nutrition & Physical Activity Surveillance
System)
� NC-CHAMP (NC Child Health Assessment & Monitoring
Program)
� NCSU/EFNEP – Families, Food and Health Project
� NC State Health Plan (for teachers and employees)
� WIC
� CCHC – Child Care Health Consultant for Child Care Centers,
including Pre Schools, in general
� Child Care Centers
� Wake Health Services
� Wake County employees (active and retired)
o Wake County Marketing/Branding
� Community Dashboard (for measures tracked)
� ? web portal designers and developers
• NC Advocates of Health in Action (AHA) Coalition
• Eat Smart Move More
• Be Active North Carolina
• Local Hospitals:
o Wake Med
� Pediatric Diabetes Program
o Rex
• CCWJC - Community Cares of Wake and Johnson Counties (Network of 122
practices)
• Wake County Policymakers (Commissioners)
• Foundations:
o ? Health organizations
o Philanthropic organizations
o Robert Wood Johnson Foundation
• ?Farmers Market Association
• ?Urban/City Planning
• ?Parks and Recreation
• ?Food and Beverage Industry
• ? Restaurant Association

Public Health Committee Meeting Page 6
• Local Churches, Temples, Synagogues
• Local YMCAs
GAP ANALYSIS:
What is the Health Status today based on all the data that is gathered and
available?
What are the gaps to meet our Vision for Wake County community?
How do we move towards meeting the Vision? What are the priorities?
PRIORITIZATION:
• At Individual Level (?Schools, Employers, Doctor’s Offices, Health
Insurance):
o Health Coaching Programs to modify behaviors and meet
healthy weight goals
• At Family Level (available through churches, YMCAs, Social
Workers…):
o Family education on healthy living
o Interventions at group level to help support each other
• Social Networks:
o Church, Temple, Synagogue
o Employment worksite
o School
o YMCA
o Media
• At Community Level:
o Policy makers
o Hospitals
o County Health Department
o Grocery Stores
o Restaurants
o Farmers Market
REFERENCES:
Child Obesity Taskforce unveils Action Plan
http://www.letsmove.gov/sites/letsmove.gov/files/TaskForce_on_Childhood_O
besity_May2010_FullReport.pdf
[5 Simple Steps to Success: for Parents, Schools, Mayors & Local Officials,
Community Leaders, Chefs, Kids, and Health Care Providers]
Discussion: • Where do preschools and child development centers fall? They can make a
significant impact. • The USDA SNAP connection has published out a social ecological model. It
is already developed and there is no charge for it. • The Youth Risk Behavioral Surveillance System (YRBSS) is a gap—Wake
County Public Schools do not participate. There have been meetings with the

Public Health Committee Meeting Page 7
public school system over the past few months and there is agreement on the part of the school system to participate in part of the YRBSS. Ten thousand dollars is needed for that effort.
• WCHS is developing a 2 year strategic plan for the agency that should be completed by fall. The goals have been approved and the plan is at the point of developing agency wide and program objectives. It is fully anticipated that there will be an agency objective that addresses obesity. One of the problems is lack of data. Another issue is identifying a target.
• Not all stakeholders are using the same outcome data. Consistent collection of data using the same definition for perhaps two data points would save time and effort.
Benny thanked Leena for her work on the planning draft and report to the committee.
Public Health Quarterly Report Edie Alfano Sobsey
Purpose: Public Health Accreditation requires that the "local health department shall analyze and note reportable events occurring within the community and shall report atypical incidence, if any to the Division and the local Board of Health (Benchmark 2, Activity 2.4). Action: Accept quarterly report; recommend report to Human Services and Environmental Services Board. Use as needed to inform discussions, decisions, and advocacy efforts related to public health. Edie reviewed the January – March 2012 Public Health Quarterly Report highlighting:
• The Community Health Rankings. Counties were ranked among other counties in North Carolina and rankings are from the community-- not solely public health. Outcome indicators are available nationally and statewide; Wake County’s indicators should be identified as a result of the strategic planning process.
• The differences in each report are due to some data being available annually and some quarterly. The format may change after the strategic planning process with the development of targets so movement toward targets can be tracked.
Discussion included: • Current efforts that impact the physical environment ranking (air quality
program, auto emissions program, mass transit, etc.) • Food violations being reported to Public Health and Environmental Services
Committees. It was noted that the Food Code passed in the Legislature on May 17.
• Current adult obesity data locally is about the same based on behavioral risk factor surveillance study.
Benny asked for a motion to accept the report and recommend it to the Board. Penny made a motion that was seconded by Barbara Ann Hughes. The report was unanimously accepted. It was noted that the Public Health Accreditation process is danger of being eliminated because of budget cuts. The mandate for accreditation will still exist and if funding is cut, counties will have to absorb those costs. Also of concern is that funding will be eliminated and the mandate will be for national accreditation which will cost an estimated $30,000 to $40,000 for a county the size of Wake. Currently it is estimated that the state accreditation process costs about $12,000 for each county. Advocates are asking that the program be funded if the mandate remains or to remove the mandate if funding is removed.

Public Health Committee Meeting Page 8
Behavioral Health Update Randy Marsh
Purpose: Provide committee members with an update on changes in Behavioral Health programs and services. Action: As determined by discussion. Since the last update to the committee, UNC has agreed to work with Wake County. The specifics of what and when are still unknown at this time. Wake County Behavioral Health provided UNC with a large amount of data about its programs and services to UNC’s strategic planning department. UNC has in turn requested additional information to decide how to work with Wake. In the meantime Behavioral Health is building a relationship with the new managed care organization that will begin its work on July 1. There are some areas of concern when considering the integration of behavioral health services in the Human Services agency. One is a conflict of interest statement by the Division of Medical Assistance (DMA) because there are Commissioner appointed Wake County representatives on the board of the new managed care organization (MCO). For that reason Wake County cannot be a provider of Medicaid or federally funded services that are managed through the MCO. If that conflict of interest holds, Wake Behavioral Health will have to stop providing Medicaid services. A question about that conflict extending to social workers in public health providing behavioral health services has been posed --will the new MCO be responsible for managing their Medicaid spending? There’s a DMA clinical coverage policy 8I which is behavioral health services provided in a public health department and all the other number 8 policies are mostly covered by the MCO. The MCO is consulting DMA about that and the outcome is pending. Also of concern is the potential loss of non-treatment behavioral health expertise in the provision of public health services related to tobacco use prevention and substance abuse, as well as in social services. Wake County has been able to totally fund a Master’s level psychologist with expertise in substance abuse and mental health to work in Clinic A through Ryan White funds. She can continue to provide services regardless of the behavioral health transition. At the same time a 2/10 time position (about 8 hours) is being lost. There has been little discussion given to the potential loss of behavioral health services that are integrated into both public health and social services and how those services can be carved out and retained. Discussion:
• Priorities for tobacco/addictions/diseases and obesity are all related to behavioral health.
• The legislature mandated this to save money and managed care saves money by cutting services.
• This is a different time with health information technology. Medicaid is paying based on outcomes—it is time to look how everyone can work together instead of as individuals. As in the case of obesity, there are many in the community working on the same issue. Perhaps Public Health can pull the community together in a convener role. How can the community take care of its needs in a way it has never been done before?

Public Health Committee Meeting Page 9
Benny asked Dr. George Corvin and Jim Bernstein, new Wake representatives to the MCO board, to represent mental health on the public health committee however the board of the MCO board thought it would be a conflict of interest. Dr. Corvin may be able to recommend someone else.
Adjournment Benny thanked committee members for their participation and adjourned the meeting.
Public Health Division Director’s Report
Public Health Committee Updates
Friday, May 18, 2012
Sue Lynn Ledford RN BSN MPA
Public Health Division
1. Cultural Issues Related to Death and Mass Fatalities Preparedness is being conducted today, Friday, May 18, 2012
from 10am to 2 pm. The training is at the WakeMed Andrews Center. The invitees include a variety of people from
public health, hospitals, emergency operations, funeral homes, Hospice, NC PH Preparedness, medical examiners,
faith based groups and law enforcement.
2. BP Zebulon Tobacco Violation. BP Zebulon has filed Petition to appeal the 3/14/12 ruling. This is scheduled for June
and we will keep the Committee informed with status updates.
3. Healthy Weight Stakeholders meeting was held 5/15/12 with good attendance. We heard from the Data and
Marketing Committees. AHA’s new Director, Sheree Vodicka, was welcomed on board and was introduced to the
Stakeholders group. She is off to a great start and has been meeting with many in the community. Leena Mehta
was present and outlined a plan for the next steps in our Strategic Plan. The group has been successful in the Data
and Investigation or Discovery Phase and is now ready to move into the next phase of Gap Analysis Prioritization
Exercises. Leena will update the Public Health Committee on those plans at this month’s meeting. .
4. State Fair Task force on E. Coli outbreak meeting updates
a. Final recommendations have been submitted to Commissioner Troxler and will be released in near future
b. Recommendations will include
i. Logistical changes in layout of Kelly and other buildings to segregate animals from human contact
ii. Will NOT prevent public viewing and access to animal education portals
iii. Increased education and hand wash access points
c. Wake County Public Health Division will be conducting an “Observation Study” of 3 different hand washing
stations during the Got to be NC event May 18-20, 2012. The purpose is to evaluate and compare the
utilization and effectiveness of the various types of stations and inform the State Fair plans.
5. Health Disparities presentations have been conducted in past few weeks to raise awareness and encourage a
community call to action. Presentations have been made to:
a. Strengthening the Black Family
b. N & O (interview)
c. Raleigh Community Advisory Council Leaders
d. Wake Missionary Baptist Church Association and
Public Health Committee Meeting Page 10
e. Latino Faith Initiative
Additional presentations have been planned
6. Multiple interns from ECU, UNC-CH, NCSU, UNC-G, UNC-W, Shaw, etc. are on site for the summer.
7. WCHS Strategic Planning process (next 2 year plan) is underway and there will be request for feedback from the
Public Health Committee as the process moves forward. Michelle and Sue Lynn will be coordinating with Benny.
Epi Team
8. Communicable Disease Update
a. There is a new staff nurse on board in CD Section.
b. Vector borne diseases are seeing an increase as is usual for this time of year. The following items are
available to groups or locations that would have a need for posters or brochures:
• 2012 Lyme disease surveillance memo for health care providers
• 2012 Arboviral disease surveillance memo for health care providers
• 2012 Tick-borne Rickettsial disease surveillance memo for health care providers
• Tick borne illness poster (though developed with the former DENR/PHPM staff, the content
is still appropriate)
• Wake County tick bite prevention poster. Developed last year by Wake County staff, the
poster is good public information and in English and Spanish.
c. There was another rabid fox incident this month involving several people. The incident occurred at Zebulon
park on 5/4/12; 6 people evaluated for exposure (2 were children) and 4 are receiving post exposure
prophylaxis.
d. There has been an increase in bat exposures: 4 positive last week and this warrants public being more alert
and encouraged to make sure household pets are vaccinated even if they are kept indoors.
e. The salmonella outbreak in Buncombe County has been linked to tempeh and tofu consumption. Two or 3
restaurants are involved (there is not a state law for pasteurization for these food items). There are
approximately 60 cases as of last week, 1 was from Wake County and total of 5 states were involved. There
has been a voluntary recall of the food items by the company.
f. Recent case of Chlymdiophilia psittaci (type of bird flu) in a household pet --Senegal parrot. The Wake
County pet owner did have another bird that tested positive in 2007. Carl Williams, State DVM has
communicated to resident regarding the positive test and possible transmission to humans. WCHS- PH
Division will be investigating further to fully trace back information.
g. One hundred and ten people were screened for TB at an area elementary school due to a student exposure.
No disease spread has been detected.
Other
9. Ricin scare in April, 2012 with law enforcement and Wake Med was resolved without further incident. (After action
did yield some recommendations for communication pathways to be better defined.)
10. The Raleigh US Postal Services building is conducting an Anthrax Drill on June 14, 2012. Public Health will participate.
11. Sue Lynn attended the National Public Health Services and Systems Research Conference in April. Speakers
included: CDC Director Dr. Thomas Friedan, Dr. Harvey Fienberg, President of the Institute of Medicine, and Debra
Perez PH.D, Assistant Vice President of the Robert Woods Johnson Foundation, Richard Umbdenstock, President and
CEO of the American Hospital Association, Association of State and Territorial Health Officials Executive Director and

Public Health Committee Meeting Page 11
National Association of City and County Health Officials Executive Director as well as many other distinguished
health leaders. The conference was full of cutting edge Population Health research info and promises to be helpful
to WCHS as we evolve into a more data-driven agency.
12. See advocacy info from the North Carolina Association of Local Health Directors below:
NCALHD North Carolina Association of Local Health Directors
Advocacy Talking Points
Consolidated Governance of Local Health Departments (LHD)
North Carolina can create a public health system that allows integration of local services while protecting the health of
North Carolinians. In order to do so, the public’s health must be the focus of all decisions made by policy makers.
Introduction: Current Environment for counties
1. Counties currently have the authority to physically consolidate local DSS and LHD by:
• Combining local DSS and LHD staff and programs in one building
• Utilizing the same registration area for clients of DSS and LHD
2. Counties currently have authority over LHD budget by:
• Controlling the county portion of the LHD budget
• Bringing LHD financials under the county finance system
• Appointing all Board of Health members
3. Counties currently have authority over LHD staff (local health director) by:
• Appointing all Board of Health members. G.S. 130A-35 (b)
• Board of Health appoints a local health director after consulting with the county board of commissioners. G.S.
130A-40 (a).
What North Carolina needs to do in the interest of the public’s health
1. Preserve Boards of Health –
a. Who bring a level of expertise to the table based on their particular profession - (NCGS 130A -35).
b. Are by statute responsible for protecting and promoting the public’s health – (NCGS 130A – 39).
c. Has the authority to Adopt Rules, including all municipalities – allowing them to take a leadership role in
critical public health issues; providing a buffer between decisions made and the local BOCC’s. – (NCGS 130A
– 39).
d. Serves many functions: i NACCHO 2011 survey of the nation’s 2,568 LHD

Public Health Committee Meeting Page 12
i. (87%) Advise Elected Officials on Policies, Programs, and Budgets.
ii. (81%) Set Policies, Goals, and Priorities that Guide the LPH.
iii. (65%) Hire and Fire the Agency Top Executive.
2. When considering a change in the governance of a local DSS and LHD, county board of commissioners should
collaborate with and have support of local boards of health and local boards of social services. (In current legislation
for multi county authority, G.S. GS 130A-36.) The county board of commissioners should consult with the local
board of health concerning such an important local public health decision.
3. Local Human Services Director should meet the same education and experience requirements as found in G.S.
130A-40 (a).
a. Value of having regulated education and experience requirements for the position (NCGS 130A-40).
b. Who have the legal authority to act when people’s health is in question (NCGS 130A-41)
c. Factors which enable the role and enshrine a duty to serve every person equally and fairly in the
enforcement of laws, rules or policies relating to health.
And which provides a buffer between the Health Department and the County when controversial decisions affecting the
public’s health are made
i NACCHO Research Brief. Local Health Department Job Losses and Program Cuts: Findings from January 2011 Survey and 2010
National Profile Study. Available at
http://naccho.org/topics/infrastructure/lhdbudget/loader.cfm?csModule=security/getfile&PageID=198106; June 2011