vol. 37 issue 5 • september 2011...
TRANSCRIPT

OFFICIAL NEWSLETTER – SASKATCHEWAN UNION OF NURSES
Vol. 37 Issue 5 • September 2011
InsideCFNU celebrates 30 years ................................................ see page 2
NAC Update: 3D Internal Medicine (Pasqua Hospital) ...... see page 6
Moving PFCC Forward seminars ...................................... see page 8
SUN Memorial Scholarship ............................................ see page 18
Nurses and social media see page 10
CFNU celebrates 30 years of solidarity

2 • SASKATCHEWAN UNION OF NURSES ISSUE 5 • SEPTEMBER 2011
CFNU celebrates 30 years
During the week of June 13-17, 2011, 56 members of the Saskatchewan Union of Nurses (SUN) joined their fellow nurse unions
in Winnipeg, the birthplace of the Canadian Federation of Nurses Unions (CFNU), to celebrate 30 years of national solidarity.
During two days of education followed by two business days, over 800 nurses from across the country came together to learn, educate, inspire and shape the future of the nursing profession and the CFNU.
“This week brought nursing leaders together from across our country,” said Linda Silas, CFNU President, in a June 17, 2011 press release. “I am proud of the work we accomplished in setting CFNU’s direction forward in advancing nursing and patient care, and for nurses’ incredible show of solidarity for striking Air Canada and Canada Post workers. Nurses walked the picket lines, shoulder to shoulder, with CAW and CUPW workers as they continued their fight for fair and equitable collective agreements.”
“It’s hard to describe the power of 800 nurses in one room,” said Rosalee Longmoore, SUN President. “The energy, the passion, the conviction – it really is inspiring. The SUN members that attend Convention always leave with a new perspective on their profession and our health care system. They have a renewed sense of pride and determination to improve the public’s perception of RNs, RPNs, and RN(NP)s and health care at home. ”
A number of resolutions were approved by the assembly during Convention, including resolutions addressing nurse fatigue, models of care, succession planning, and the role of the RN. In support of the care of seniors, the assembly also passed a resolution to organize a national conference on the care of Canada’s seniors and vulnerable populations.
The following highlights are excerpts from the CFNU Convention Newsletter and have been re-printed with permission.
NurSeS wIeld ImportaNt power IN CaNadIaN health CareAfter a warm welcome to the Convention from
CFNU President Linda Silas, the opening plenary session Tuesday morning tackled the topic of leadership in Canadian nursing. Four nurses brought very different, and very personal, perspectives: Lesley Bell, from the Ontario Nurses’ Associaton, Roberta Dugas, from the New Brunswick Nurses Union, Jan Cibart from the Saskatchewan Union of Nurses and Mary Ferguson-Paré from the University of Toronto.
All the nurses highlighted the importance of nurses to the sustainability of our health care system. Nurses need to speak out to keep a high level of health care accessible to all Canadians.
Lesley Bell said nurses’ persistence will make a huge difference in the debate on the sustainability of our health system. If you feel you are not being paid attention to, keep making your points anyway, she said. “Keep putting it out.” It is the dripping water technique that will get results in the end.
“It’s hard to describe
the power of 800 nurses
in one room.”
Linda Silas, CFNU President,
opens Convention with words
of praise and inspiration.

ISSUE 5 • SEPTEMBER 2011 SASKATCHEWAN UNION OF NURSES • 3
New INterNet SoCIal medIa workShop grappleS wIth huge poteNtIal aNd wIth pItfallSIs it rude to use a smart phone in a meeting? In a
conversation? What if you’re using it as a diagnostic tool? These were some of the questions considered during a lively conversation Tuesday afternoon during the CFNU’s workshop on the use by unions of such on-line tools as Facebook, Twitter and YouTube, “Social Media, the New Tools for Change.”
The answers to these questions? They are not clear yet – and will likely have to be driven by a process of social consensus, suggested seminar facilitator Dave Cournoyer from the United Nurses of Alberta. But in the meantime, he argued, it’s important for trade unionists to cut others some slack, and assume they’re using social media tools to tune in, not out.
Unions need to aggressively use social media tools, Cournoyer argued, to counter the social media successes of forces in society who are opposed to unions and aim to obstruct the rights of working people. “It’s worked for conservative organizations,” he commented. “Why not progressive organizations like unions?” Used effectively, he concluded, they offer new ways for unions to connect with members, persuade non-members of our positions and generally go where Canadians want to be.
Not everyone is ready to embrace social media and all it has to offer. Many do not look at it as getting “live” information to take back to the members. And constantly tapping on a smart phone may seem rude to some. But many others see this not as a disrespectful form of communication, but rather as being “connected.”
Nurses’ unions need to be where our members are. Whether at home or just coming off a shift, they can check out the latest news through new media. Utilizing Facebook and other types of social media is not only an important part of on-line presence, using these channels can engage members and turn already engaged members into on-line activists.
Members are driving the conversation. More communication is being generated by the members themselves. They want to be heard and want to hear what is going on around them. This can get a conversation going that might otherwise have never been discussed. Summing up the workshop: the on-line conversations are happening, and if we are not participating with social media, these conversations will happen without us.
Members are driving the
conversation. They want to be
heard and want to hear what is going on around them.
The SUN delegation take a moment out to pose for a group shot during the CFNU Biennium.

4 • SASKATCHEWAN UNION OF NURSES ISSUE 5 • SEPTEMBER 2011
Better StaffINg – NurSeS ImproVINg Care for CaNadIaNSLinda Silas focused on the future and ways nurses
can improve the lives and care of Canadians in her address at the opening of the business meeting Thursday morning. She picked up on lessons on change from Australian nursing leader Brett Holmes, who spoke the day before.
“When nurse staffing levels in California hospitals increased substantially after mandated nurse-patient ratios, we know that reduced workload was associated with lower patient mortality, lower nurse burnout and better job satisfaction. We need strong language for decent staffing … as Brett said, why not in Canada? And I say, yes, it’s about time.”
Before she went on to talking about what nurses can do, Linda addressed what she called two shames in Canada. “In this rich country, the way we treat our aboriginal people is a shame, from their health care system, their housing to their education system. We have a second shame: the way we treat our seniors in
this country. Our long-term care sector is a mess and we need to fix it.”
But the core of Linda’s message to Canadian nurses was about making improvements. “We need to support a national pharmacare program … we need drugs for everyone who needs them not only those who can afford them,” she said. Silas said nurses are going to focus on primary health care. “Never mind a doctor for every Canadian. It should be a nurse for every Canadian and finally we would focus on prevention.”
“We know we need to address the overcapacity in our hospitals and the under-capacity in our workforce. We need to address the flaws in our medicare system and at the same time protect it and expand it. CFNU is important,” Linda Silas pointed out “as the national voice of the working nurses in Ottawa to promote solidarity with all health care workers and to leverage changes in Ottawa.”
New NatIoNal poll ShowS Very hIgh patIeNt approVal of NurSINg performaNCe deSpIte uNderStaffINg, NatIoNal NurSINg Shortage
A new national poll shows that Canadian patients overwhelmingly approve of treatment they receive from the nation’s nurses, despite the clearly visible nursing shortage in hospitals. The poll, conducted by Vector Poll in early June, for the Canadian Federation of Nurses Unions (CFNU) for its 30th Anniversary Biennial Convention held in Winnipeg, showed that nurses get a great report card from their patients.
The National Patients’ Report Card on Nurses found:
88% of respondents who saw a nurse the last time • they needed health care said they were listened to carefully and had their questions answered;84% of respondents say the nurse treated them with • respect and they felt the nurse cared about them;83% say the nurse knew and understood their health • needs;82% say the nurse addressed their needs quickly.• “Poll results showed Canadian patients respect and
value the care they receive from nurses, clearly seeing evidence that nurses are health care professionals with superior knowledge – and the ‘caring touch’ that those who are ill need,” said CFNU President Linda Silas,
RN. “The poll also showed that one third of patients noticed that the facility in which they sought treatment was understaffed with nurses, making the high approval ratings even more significant.”
Respondents also rated nurses very highly for being technically competent, for explaining procedures to patients, for helping patients understand their conditions and for quickly addressing their needs. Four in ten of those polled gave nurses a perfect score.
For some of the benchmarks of good care measured by the poll, nurses were more productive and responsive than the public expected – especially with the nursing shortage.
“Patients give the highest marks to nurses working in facilities with what they view as ‘the right number’ of nurses,” noted Silas. “Nurses working in understaffed facilities rated the lowest, yet they still gave nurses high marks for their efforts when they’re overworked. In fact, 34% of respondents say they noticed the facility they used had too few nurses for the amount of work that had to be done.”
Full poll results are available on the CFNU’s web site at www.nursesunions.ca.
“Our long-term care sector is a mess and
we need to fix it. Never mind a doctor for
every Canadian. It should be a nurse for
every Canadian …”

ISSUE 5 • SEPTEMBER 2011 SASKATCHEWAN UNION OF NURSES • 5
oVertIme for NurSeS equalS more thaN 11,000 full-tIme joBSInformation from a new study shows that in 2010,
registered nurses and nurse supervisors publicly employed in Canada’s health care and social assistance sector, worked a total of 20,627,800 hours of overtime, equivalent to 11,400 full-time jobs.
On average, 14.5% of nurses worked unpaid overtime in 2010, up from 12.9% in 2008. Nurses reporting unpaid overtime worked 4.4 extra hours per week. This is 0.5 hours higher, on average, than in 2008.
For every week in 2010, 19,200 public-sector health care nurses, on average, were absent due to illness or
disability. Full-time nurses top all other occupations in rates of illness and disability-related absenteeism.
“We are not surprised by most of these figures, unfortunately,” said Silas. “They replicate a pattern established in a similar study covering 1987 to 2008. What is alarming is that though the percentage of nurses working paid overtime has decreased, from 21.4% in 2008 to 17.3% in 2010, the percentage of nurses working unpaid overtime has increased. This represents a further squeezing of labour from a workforce which continues to face layoffs.”
SoCIal determINaNtS of health – INVeStINg early payS offIn the jigsaw puzzle that health care has become,
experts speaking on the social determinants of health Wednesday concurred that healthy public policy should focus on optimizing the health of children, pre- and postnatal, as the single most important optimal return on investment. According to Darlene Girard, a panelist at the workshop, early childhood initiatives are the most promising way to improve health inequalities in a generation and Canada has a lot of work to do.
In a recent study, Canada tied for last place in an international comparison of the 26 wealthiest countries
in the world in regards to childhood poverty. Panelists were in agreement that social and health care policy across the board should be looked at with an “equity” lens with the view of creating social justice and the equitable distribution of resources.
A tour of community programs and initiatives reinforced the fact that investments in programs which foster the collective will and leadership, reduce child poverty and strengthen communities, pays off in the short and long term.
CFNU Biennium Inspiresdifferent personalities in the workplace, and how to develop healthy relationships. These workshops went well together and I gained valuable knowledge from both of which I will be able to apply in and out of my workplace.
Since the Convention, I have had plenty of opportunity to continue to learn about SUN, my workplace and what my role is. First and foremost, I finally made time to read the entire collective agreement for SUN, and not just the sections that relate to my personal situations. Due to this, I have been able to encourage other nurses that I work with to access their collective agreements during conversations when it is applicable. Also, I was able to share my experience and what I had learned at the CFNU Biennium at my last Local meeting and to show that I was enthusiastic about participating. I am proud to note that there were four new members present at the meeting and as a new member myself we were encouraged to continue to get involved. Lastly, I was able to make relationships with strong sisters and brothers in Saskatchewan and I look forward to developing these in the future.
I would like to sincerely thank SUN for sending me to the CFNU Biennium as a fully funded delegate. It was an inspiring event that I believe has been very appropriate to initiate my active involvement with the Union.
Staci Labrecque
Local 104, St. Joseph’s Hospital, Estevan
This year’s CFNU Biennium truly was a celebration of nurses and their unions as the CFNU’s 30th Anniversary had been commemorated throughout the entire week. The week was opened with a healthy walk followed by a high energy welcoming registration process. Being a first-time delegate to a nursing union convention, I had been apprehensive as of what to expect. However, immediately after meeting with some of the “spicy” sisters in my health region, I had no doubt that I would fit in. Truth be told, I had an overwhelming feeling of reassurance and belonging as I first witnessed over 800 active union members from around the country who care about the union and its future among the upcoming generations of nurses. Walking into the hall on Tuesday morning to witness this scene had been an empowering event that I hope to reflect on in many occasions in my nursing career.
I had the opportunity to attend two workshops during the Biennium. The first, called Young Workers: Our Leaders of Tomorrow, was actually what had initially caught my attention and drove me to sign up for the Convention. This workshop focused on current trends and issues for nurses under the age of 30 just entering into the union and the differences between generations and the implications of the same. Barriers of communication between the generations and how to overcome these were addressed. The second workshop was called Walking the Talk: Communication Compe tence. It had focused on tools to communicate effectively in the workplace,
6 • SASKATCHEWAN UNION OF NURSES ISSUE 5 • SEPTEMBER 2011
NURSING
ADVISORYNAC
PFCC creates a safer, more effective workplace 3D Internal Medicine Unit at Pasqua Hospital takes recommendations to Region’s Board
“The RNs on the 3D Unit at the Pasqua Hospital are committed to providing quality patient- and family-centred (PFCC) health care and being involved in creating a safer and effective workplace,” says Lorna Tourond, an RN and the 3D Medicine Unit Rep. Tourond goes on to say this is why the nurses took the Unit’s nursing practice concerns to the Regina Qu’Appelle Health Region Board of Directors on May 16, 2011.
BaCkgrouNd3D is an Internal Medicine Unit that encompasses
the study and practice of health promotion, disease prevention and diagnosis. Nursing care involves the treatment of adults from adolescents to the elderly during times of health and all stages of acute and chronic illnesses. Patients on an internal medicine unit typically have undifferentiated and/or multi-system disease processes and failures.
The registered nursing staff on 3D are qualified and responsible to deliver nursing care to patients requiring a broad range of general medicine services including but not limited to: Cardiac patients (Congestive heart failure, Angina, Myocardial Infarction, Hypertension, etc.); Endocrinology (Diabetes – both newly diagnosed and chronic); Gastroenterology (Crohn’s, Colitis); Rheumatology (Blood disorders); Geriatric Medicine; Infectious Diseases (HIV, Tuberculosis); Medical Oncology (Cancer); Pulmonology (COPD, Asthma, pneumonia) Critical Care Management and Nephrology (CRF, ARF).
The care the registered nurses (RNs) provide includes teaching, preserving function, advocating for patient needs and discharge planning; these functions often include the patient and their family. Patients on 3D typically require constant assessment and the RNs are responsible for the implementation of various interventions.
3D is a 32 bed unit with two (2) over-capacity beds which are regularly occupied approximately 90% of the time. There are four (4) teams on days which “should” each consist of one (1) RN and one (1) Licensed Practical Nurse (LPN) totalling eight (8) floor staff for 32-34 patients and one Charge Nurse designated to the desk. Each team provides patient care for seven (7) to ten (10) patients between the RN/LPN team. At night, staffing is decreased to five (5) RN/LPNs – the charge RN takes four (4) patients and the remaining patients are split between two (2) teams. Each team member cares for seven (7) to nine (9) patients. Each team on nights consists of only one nurse (an RN or LPN). This allows for one nurse to ‘float’ performing duties such as vital signs, blood sugars and whatever else she can do to assist the other nurses (admissions/discharges). Unfortunately this ‘float’ position is most often filled by an LPN so there is a narrower scope of practice that can be performed.
3D is also a “step down” unit for patients coming from the Intensive Care Unit (ICU). These patients are typically acutely ill with feeding tubes, catheters, pleural drains/chest tubes, central venous lines (CVL), peripherally inserted central catheter (PICC) and require close monitoring and frequent assessments. It is not uncommon for a patient fresh out of the ICU to be placed in a room with an elderly patient, perhaps awaiting long-term care (LTC) placement. Frequently, the mix of patients on the Unit and in each room requires the RN to alter her interventions or approach to accommodate the changing needs of the patients. Nurses on this Unit must be highly skilled and responsible to the needs of each patient.
The RNs work closely and in conjunction with physi cians, physiotherapy, occupational therapy, dieticians, LPNs, social workers, respiratory therapists, pharmacists, porters, unit clerks and the utilization coordinator to ensure the best possible outcomes for patients.
Left to right: Erin West, 3D RN, Board presenter,
Jessica Wright, 3D RN, Board presenter, Katherine Gibbons,
3D RN, Board presenter, Laurelle Pachal, Regina Base
Hospital Rep, Lorna Tourond, 3D RN, Board presenter,
Bev Miller, Local 106 President.
ISSUE 5 • SEPTEMBER 2011 SASKATCHEWAN UNION OF NURSES • 7
PFCC creates a safer, more effective workplace 3D Internal Medicine Unit at Pasqua Hospital takes recommendations to Region’s Board
The 3D Unit is almost always full; running a census of over 90% for the year of 2010. An average of one-third of the patients (approximately nine patients) were waiting placement to a long-term care facility or private care home in 2010. The majority of ICU patients are transferred directly to Medicine and often need close monitoring and significant RN intervention.
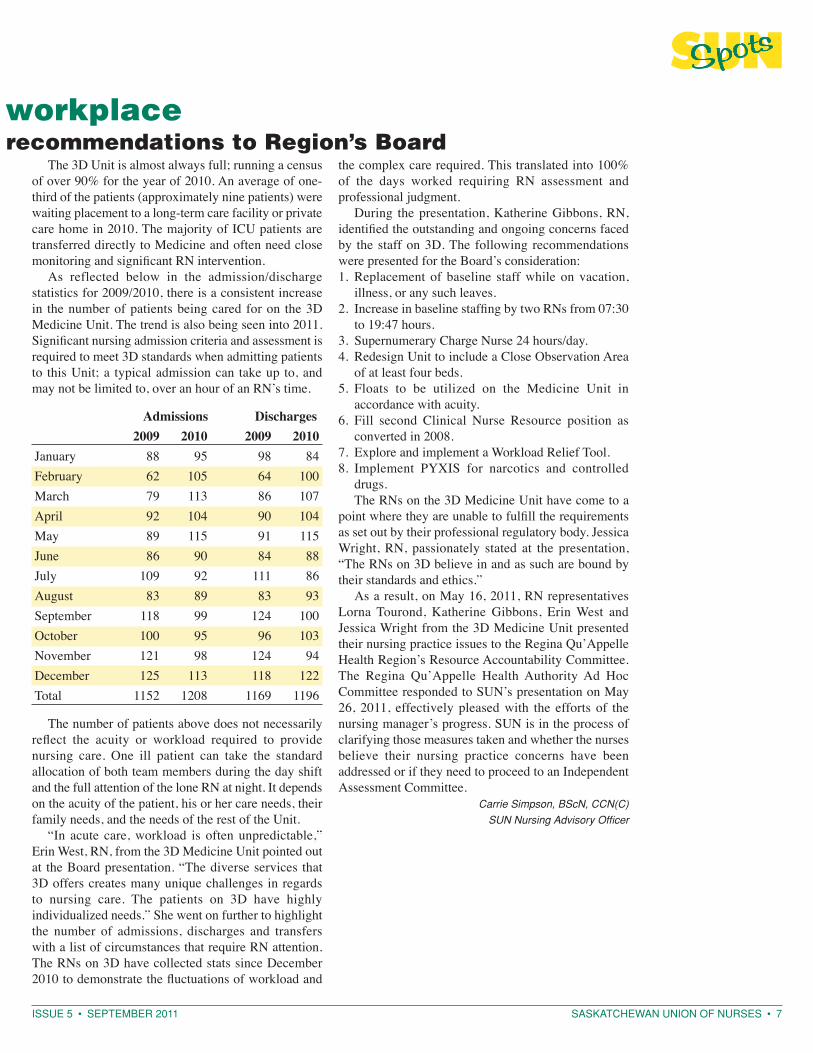
As reflected below in the admission/discharge statistics for 2009/2010, there is a consistent increase in the number of patients being cared for on the 3D Medicine Unit. The trend is also being seen into 2011. Significant nursing admission criteria and assessment is required to meet 3D standards when admitting patients to this Unit; a typical admission can take up to, and may not be limited to, over an hour of an RN’s time.
Admissions Discharges 2009 2010 2009 2010January 88 95 98 84February 62 105 64 100March 79 113 86 107April 92 104 90 104May 89 115 91 115June 86 90 84 88July 109 92 111 86August 83 89 83 93September 118 99 124 100October 100 95 96 103November 121 98 124 94December 125 113 118 122Total 1152 1208 1169 1196
The number of patients above does not necessarily reflect the acuity or workload required to provide nursing care. One ill patient can take the standard allocation of both team members during the day shift and the full attention of the lone RN at night. It depends on the acuity of the patient, his or her care needs, their family needs, and the needs of the rest of the Unit.
“In acute care, workload is often unpredictable,” Erin West, RN, from the 3D Medicine Unit pointed out at the Board presentation. “The diverse services that 3D offers creates many unique challenges in regards to nursing care. The patients on 3D have highly individualized needs.” She went on further to highlight the number of admissions, discharges and transfers with a list of circumstances that require RN attention. The RNs on 3D have collected stats since December 2010 to demonstrate the fluctuations of workload and
the complex care required. This translated into 100% of the days worked requiring RN assessment and professional judgment.
During the presentation, Katherine Gibbons, RN, identified the outstanding and ongoing concerns faced by the staff on 3D. The following recommendations were presented for the Board’s consideration:
Replacement of baseline staff while on vacation, 1. illness, or any such leaves.Increase in baseline staffing by two RNs from 07:30 2. to 19:47 hours. Supernumerary Charge Nurse 24 hours/day.3. Redesign Unit to include a Close Observation Area 4. of at least four beds.Floats to be utilized on the Medicine Unit in 5. accordance with acuity.Fill second Clinical Nurse Resource position as 6. converted in 2008.Explore and implement a Workload Relief Tool.7. Implement PYXIS for narcotics and controlled 8. drugs.The RNs on the 3D Medicine Unit have come to a
point where they are unable to fulfill the requirements as set out by their professional regulatory body. Jessica Wright, RN, passionately stated at the presentation, “The RNs on 3D believe in and as such are bound by their standards and ethics.”
As a result, on May 16, 2011, RN representatives Lorna Tourond, Katherine Gibbons, Erin West and Jessica Wright from the 3D Medicine Unit presented their nursing practice issues to the Regina Qu’Appelle Health Region’s Resource Accountability Committee. The Regina Qu’Appelle Health Authority Ad Hoc Committee responded to SUN’s presentation on May 26, 2011, effectively pleased with the efforts of the nursing manager’s progress. SUN is in the process of clarifying those measures taken and whether the nurses believe their nursing practice concerns have been addressed or if they need to proceed to an Independent Assessment Committee.
Carrie Simpson, BScN, CCN(C)
SUN Nursing Advisory Officer
8 • SASKATCHEWAN UNION OF NURSES ISSUE 5 • SEPTEMBER 2011
Moving patient- and family-centred care forward in SaskatchewanSince the Saskatchewan
Ministry of Health
announced its mandate
and framework for bringing
patient and family-
centred care (PFCC) to the
forefront of health care
in Saskatchewan, SUN
continues to be leaders
in the PFCC movement in
the province. SUN’s goal
is to provide as much
information about PFCC,
to as many people as we
can to ensure system-
centred care is a thing of
the past. In order to do
that we need to continue
educating one another on
what PFCC means, who can
make a difference in PFCC,
and how we can continue
to improve upon PFCC.
On June 6 and 7, 2011, SUN hosted two one-day seminars focusing on enhancing and developing the practical tools necessary for frontline health care providers to deliver the patient- and family-centred care they want to provide. Over 400 participants, over the two days, were captivated by the personal stories, experiences and lessons learned shared by Julie Moretz, Director, Special Projects, and Joanna Kauffman, Information Specialist, from the Institute of Patient- and Family-Centered Care (IPFCC) in Maryland, USA.
Engaged in the learning process, participants learned how to invoke change from the frontlines – being patient- and family-centred is more than how we deliver the care, it is also about how that care is perceived. Moretz and Kauffman spoke of how frontline care providers are the leaders of PFCC; they are the ones that have the ability to make a huge difference in the care their patients receive, just by involving their patients and their families.
The seminars focused on more than just how the front line care providers can make a difference for the patients, but also on how to face the systemic and inter-professional challenges and barriers they face on a daily basis. Additional areas explored were, but not limited to:
practices and programs that support partnerships • with patients and families; practical strategies for advancing patient- and • family-centred care;how patient- and family-centred care improves • safety, quality and the experience of care;
Joanna Kauffman speaks to the participants about PFCC from the perspective of a front line nurse.

ISSUE 5 • SEPTEMBER 2011 SASKATCHEWAN UNION OF NURSES • 9
Moving patient- and family-centred care forward in Saskatchewannursing leadership qualities, actions, and strategies • for advancing the practice of patient- and family-centred care in a variety of settings; methods for dealing with resistance of staff • colleagues;the difference between system-centred, patient-• focused, family-focused, and patient- and family-centred care; implications of patient- and family-centred care for • the health care system; andthe emerging issues in nursing related to patient- • and family-centred care.The Moving Patient- and Family-Centred Care
Forward seminars were not about teaching registered nurses and other health care providers how to provide PFCC. The seminar was about reminding them that the small things matter, like involving the patient/family, asking them questions, and listening to what they have to say. It was about encouraging and empowering participants to have a voice, and how to hold on to that voice when faced with adversity. These PFCC seminars were meant to re-energize the frontlines with a new found passion for PFCC and how they deliver it. According to the feedback from the participants, it looks like we were on the right track. Participants told us that:
Listening to patient and family is vital to providing • quality carePFCC is the right thing to do• That we do not need permission to make change, • I can do what I feel is best for the patient, when I know what the patient’s needs are
Patient and family are the team leaders!• I have been doing a lot of little things along PFCC • but I haven’t been expressing out loud to patients, families or staff the why. I have been working at a whisper now I have a voice!When I heard “The moment of truth” is the moment • that your patient decides whether or not you are what you say you are – patient care is much more successful with trustWe pretend we are, we ask families/residents what • they want and need but do we really listen, do we really careAlways, ALWAYS remember: It’s not about me or • the system, it’s about the patient and their familyThe overwhelming response to the seminars and
the positive feedback is proof that the frontline care providers appreciate and understand the philosophies and goals of PFCC. Their willingness to learn new and improved skills and techniques proves that PFCC will become less of an initiative and more of a reality and norm for our health care system – from the patients and families to the frontline care providers to the administrators.
The June 2011 seminars were attended by Registered Nurses, Registered Psychiatric Nurses, Nurse Prac ti tioners, Licensed Practical Nurses, Nurse Managers, Nursing Instructors and Professors, profes sional associations and regional administrators. Thank you to the Saskatchewan Ministry of Health, Saskatchewan Registered Nurses Association (SRNA) and Saskatchewan Association of Licensed Practical Nurses (SALPN) for sponsoring the event.
Referring to her own personal experiences, Julie Moretz talks about the impact PFCC has on the patient and their family.
Julie Moretz speaks freely to a participant about PFCC.
10 • SASKATCHEWAN UNION OF NURSES ISSUE 5 • SEPTEMBER 2011
The Assistant Canadian Commissioner of Privacy has stated, “Social networking sites are a cultural phenomenon. In the last five years, the popularity of these sites has exploded, with millions of people around the world joining them to keep in touch with their friends and family and to meet new people. They represent a dramatic shift in the way people communicate and their use raises interesting questions about long held views on what it means to have a private life or a sense of ‘privacy’.”1
Given the above, it is no surprise that we are now faced with the need to consider how social networking sites affect the profession of nursing. Clearly, if SUN members are making use of such technology, it is wise to consider some of the ways such technology could affect a nurse’s profession and career.
Employees who use Facebook, My Space, Twitter, personal blogs and other forms of electronic communication are at risk of sometimes confusing freedom of speech with freedom from potential workplace and other legal consequences.
The potential employment related problems could include:
breaching a duty of loyalty to the employer;• theft of company time;• insubordination;• breach of personal health information and privacy • laws.The potential other legal problems could include:an action for defamation filed in a civil court, if a • nurse libels or defames a manager, co-worker or patient, the same as might be the case if this occurred in any other form of publication;criminal charges may be laid if employees harass or • intimidate co-workers.Facebook postings, e-mails, and any other traceable
forms of communication can be used as evidence in court or in an arbitration hearing.
However, before considering the issues more thoroughly, please take note of the following fact summaries which we will use as examples for our discussion:
During his/her time off, an employee lets off some 1. steam about his/her workplace by posting his/her opinions on a personal blog;While off work and in bed suffering from a migraine 2. headache, an employee accesses his/her Facebook site from his/her cell phone;
An employee snaps a picture of a patient undergoing 3. a procedure and subsequently posts that picture on his/her Facebook page; andAn employee engages in inappropriate conduct 4. while off duty and while wearing his/her uniform. The employee’s behaviour is photographed and the picture of the employee is posted on an internet site.What do all of the above scenarios have in common?
These are all cases which resulted in the termination of the employees in question.
Although nurses may, like many employees, think that their employers no longer have control over their actions once they leave the workplace, nothing could be further from the truth. This is particularly so in regard to professions such as nursing where nurses are expected to uphold certain standards of practice whether or not they are on duty.
The facts are, whatever you post, you are accountable for, and electronic rants are not only public, they may form a permanent record as well.
As nurses in Saskatchewan know, they are bound by certain standards of practice which are enforced by their respective professional associations. For instance, among other things, Registered Nurses are required to promote and uphold the ethical standards of the nursing profession, which includes:
Preserving the Dignity of patients; and• Understanding ethical and legal considerations in • maintaining client confidentiality in all forms of communication: written, oral, and electronic.2
1PIPEDA Case Summary #2009-008, [2009] C.P.C.S.F. No. 8, p. 3 2Section 3(80) of the Standards and Foundation Competencies for the Practice of Registered Nurses 3Section 4(2) of the Licensed Practical Nurses Act and The Registered Nurses of Manitoba Act
Facebook and Twitter – An ounce of prevention is worth a pound of cure
ISSUE 5 • SEPTEMBER 2011 SASKATCHEWAN UNION OF NURSES • 11
Since there is nothing within the RN Standards of Practice which limits the applicability of practice standards to the time while nurses are at work, it is important that nurses remember and abide by such standards even after they have left the workplace. Accord ingly, when using such internet social networking tools as Facebook and Twitter, nurses would be wise to keep their standards of practice in mind.
The above is particularly true since both professional colleges for RNs and LPNs in Manitoba advise that they (the Colleges) “must carry out its activities and govern its members in a manner that serves and protects the public interest.” 3 In other words, if a nurse’s use of sites such as Facebook and Twitter could be seen to act against the public interest, or to contravene applicable nursing standards of practice, a nurse may find herself in trouble with her respective professional college and/or employer.
For instance, take the case above-noted as example #3 (employee who took a picture of a patient undergoing a procedure and posted it on Facebook). This fact scenario involved a couple of nurses from the United States who were dismissed from their jobs. Although, in that particular case, the picture taken by the nurses was allegedly of an x-ray that did not identify a patient, the fact remains that what was posted on Facebook was considered inappropriate and therefore resulted in the nurses’ dismissal.
Given the standards of practice here in Saskatchewan, dismissal does not seem surprising in
the above-noted case. Frankly, had this incident taken place in Saskatchewan, it would not have been surprising if the nurses’ professional association(s) also investigated the matter and imposed discipline of some sort on the nurses as a result of arguable breaches of the nurses’ standards of practice.
Although the above is an extreme example of how social internet sites can land a nurse into hot water, it illustrates that nurses must be careful as to what they post on and how they use sites like Facebook during their personal time. To do otherwise could result in unnecessary discipline including termination, and/or investigation and sanction by the nurse’s professional licensing body.
Nurses should be aware that spending time on Facebook while at work or chatting with friends on Twitter can result in an allegation of theft of an employer’s time. Employees should understand that they can’t carry on personal activities on-line during working hours. This is especially so if they are using company-owned equipment. Posting personal information about co-workers on-line could also infringe on the co-workers right to privacy.
Insubordination on-line, in various forms, such as name-calling and personal rudeness, even though it may occur outside of the workplace, can still be grounds for discipline and possible dismissal.
A major concern is that most verbal complaints about a boss or co-worker are usually confined to a few trusted friends or family members. But once posted in cyberspace they can immediately circulate around the world, and become a permanent record. This causes such postings to be considered even more serious in their damaging effects and subsequent consequences.
In summary, generally speaking, Facebook and similar sites can be fun pastimes that have nothing to do with the workplace. However, in some cases, if a sufficient connection can be made to a nurse’s activity on such sites to her nursing profession, the nurse could find herself facing discipline, termination, licensing and other legal issues.
As a rule of thumb, before using social networking sites like Facebook, a nurse should ask herself if anything she is writing and/or posting could cause her difficulty with her employer and/or professional college. If she is unsure how to answer that question, a quick call to her local union rep or SUN Provincial could help prevent potential pitfalls in the future.
Re-printed with permission from Manitoba Nurses’ Union (MNU)
Facebook and Twitter – An ounce of prevention is worth a pound of cure
12 • SASKATCHEWAN UNION OF NURSES ISSUE 5 • SEPTEMBER 2011
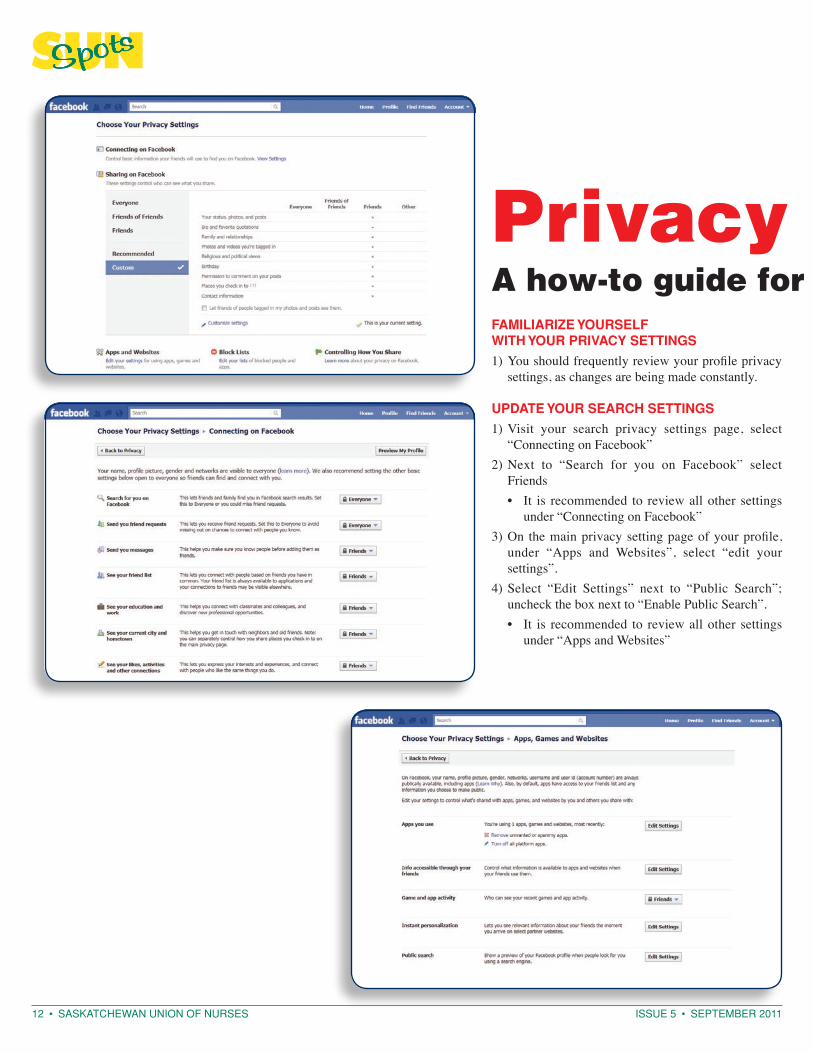
Privacy Protection 101A how-to guide for FacebookfamIlIarIze yourSelf wIth your prIVaCy SettINgS
You should frequently review your profile privacy 1) settings, as changes are being made constantly.
update your SearCh SettINgS
Visit your search privacy settings page, select 1) “Connecting on Facebook”Next to “Search for you on Facebook” select 2) Friends
It is recommended to review all other settings • under “Connecting on Facebook”
On the main privacy setting page of your profile, 3) under “Apps and Websites”, select “edit your settings”.Select “Edit Settings” next to “Public Search”; 4) uncheck the box next to “Enable Public Search”.
It is recommended to review all other settings • under “Apps and Websites”
ISSUE 5 • SEPTEMBER 2011 SASKATCHEWAN UNION OF NURSES • 13
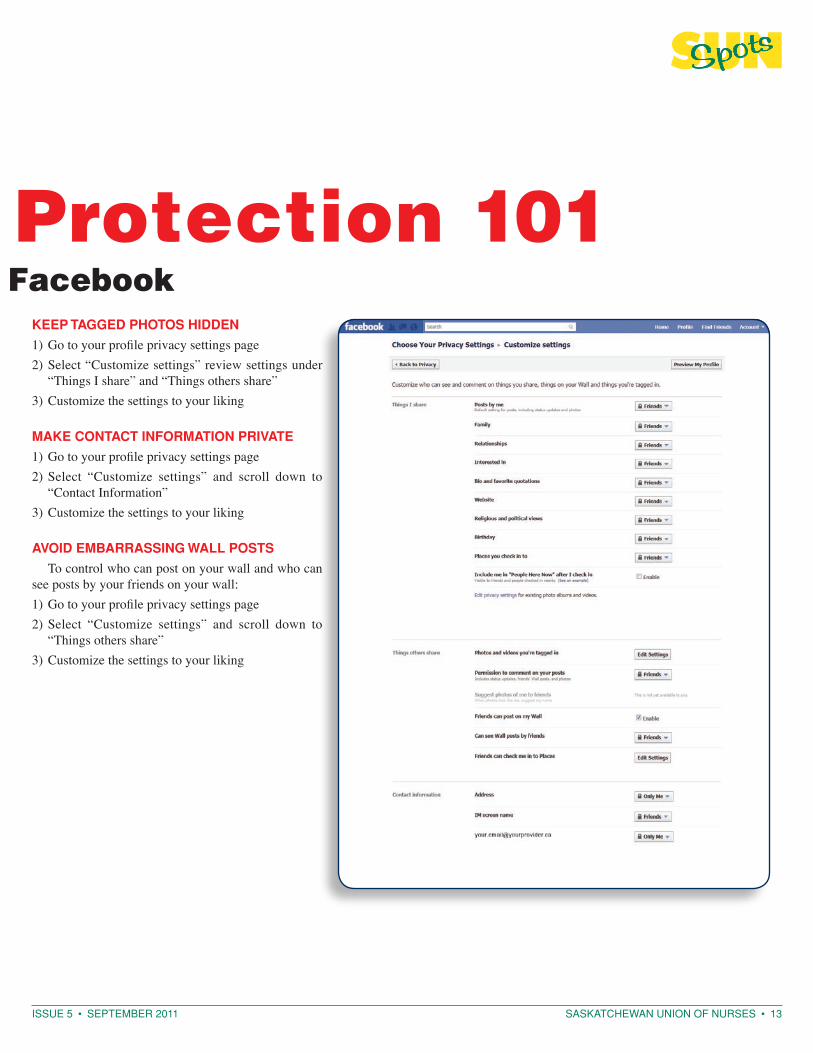
Privacy Protection 101A how-to guide for Facebook
keep tagged photoS hIddeN
Go to your profile privacy settings page1) Select “Customize settings” review settings under 2) “Things I share” and “Things others share”Customize the settings to your liking 3)
make CoNtaCt INformatIoN prIVate
Go to your profile privacy settings page1) Select “Customize settings” and scroll down to 2) “Contact Information”Customize the settings to your liking 3)
aVoId emBarraSSINg wall poStS
To control who can post on your wall and who can see posts by your friends on your wall:
Go to your profile privacy settings page1) Select “Customize settings” and scroll down to 2) “Things others share”Customize the settings to your liking3)
14 • SASKATCHEWAN UNION OF NURSES ISSUE 5 • SEPTEMBER 2011
Facebook (and other social media networks) and the Registered Nurse
aS a regIStered NurSe what do I Need to kNow aBout uSINg faCeBook?
The SRNA Standards and Foundation Competencies for Registered Nurses (2007) states, the Registered Nurse (RN) “understands ethical and legal considera-tions in maintaining client confidentiality in all forms of communication: written, oral, and electronic” [#80] (p. 10).
Facebook is a useful social networking tool that RNs need to approach cautiously. RNs must be aware that providing patient health information (PHI) that was collected through the provision of care is a breach of confidentiality when posted on sites like Facebook. Infor mation posted to Facebook about a patient experience or care provided could lead to identification of the patient through association (for example: knowledge that you are an RN, who you work for, and what depart ment you work in). The use of PHI on Facebook is outside the scope of the intended use and purposes for which the information was collected. In some cases RNs may not be aware the information they provide in an update to their personal page may be shared beyond those intended recipients. The basic ‘rule of thumb’ for PHI use and disclosure is whether the receiver of the information has a ‘need to know’.
The CNA Code of Ethics for Registered Nurses (2008) identifies RNs’ ethical responsibilities regarding maintaining privacy and confidentiality as follows, “Nurses respect the right of people to have control
over the collection, use, access and disclosure of their personal information” (p. 15). Be aware of your organiza tional policies, procedures, and processes including how to manage a privacy breach.
If you are aware of a breach of privacy on a social networking site like Facebook, the Code of Ethics states, “Nurses intervene if others inappropriately access or disclose personal or health information of persons receiving care” (CNA, 2008, p. 16). This can involve discussing your concern with your co-worker, manager/supervisor, Privacy Officer, and the SRNA Competence Assurance Advisor.
Learn more about Privacy and Confidentiality of PHI:
Canadian Nurses Association (CNA) • www.cna-aiic.ca/cna/Canadian Nurses Protective Society (CNPS): • InfoLaw Bulletins www.cnps.caOffice of the Privacy Commissioner • (Saskatchewan) www.oipc.sk.caOffice of the Privacy Commissioner (Federal) • www.priv.gc.ca
Erika T. Vogel, RN
SRNA Nursing Advisor, Practice
Re-printed with permission from the Saskatchewan Registered Nurses’ Association (SRNA); originally published in the SRNA NewsBulletin, Summer 2010
Social networking etiquette Do not disclose any personal health information 1. about a patient which would breach the Personal Health Information Act. Anyone who wrongfully releases such information is guilty of an offence and subject to a fine of up to $50,000;Refrain from venting about your employer on 2. your social networking site;Remove any negative remarks about your 3. employer or colleagues, posted by others, from your social networking site;Do not post any pictures to your social 4. networking site that could bring your workplace and/or employer into disrepute (e.g. wearing your work uniform out while chugging your favourite alcoholic drink is not a good idea, particularly since such conduct could be caught on video or in a photograph);
Do not intimidate and/or harass co-workers or 5. your employer on your social networking site;Do not log-in and access your social networking 6. site while on sick leave or disability leave if such access could cause your employer to question why you are not at work;Do not access your social networking site from 7. work; andRemember anything you post or write on the 8. internet is something your employer, your professional college, and members of the general public can access. Even though a site may seem private, a court or tribunal can order access to materials posted on such sites in cases involving defamation, dismissal, harassment, etc.
Re-printed with permission from Manitoba Nurses’ Union (MNU)

ISSUE 5 • SEPTEMBER 2011 SASKATCHEWAN UNION OF NURSES • 15
Prairie School for Union Women – reviews and praiseThere were ten workshops to choose from during
the Prairie School for Union Women (PSUW) on June 12-16, 2011. The course I attended – Everyday Activism – was full of valuable information; the following is only but a summary.
Activism: to change something in your world • causing social change.People usually have a passion or interest because of • a life experience they have had.People decide to take on one thing and devote their • time to it.Communities can be building connections to make • a change.Depending on where a person is in their life, their • focus on activism will change. Example: kids’ activities, church, work, sports, community, unions, and politics.If you want to decide what to get involved in, go for • issues that get you mad because you’ll have a lot of energy to do it.Network with people so they know your credentials • which can help with opportunities to become involved.Being an activist can cost you time and money.• In unions, some members will only get involved if a • strike vote is happening.Recognize the barriers that other people face.• Equity: no matter where we are active, keep the • barriers down for people to become involved.Not everyone comes from the same point of • privilege; a lot of workers are non-unionized and have no one to stand up for them – no rights or benefits.Recognize who can’t be active and why.•
for uNIoN work:Get people involved.• Use the first coffee break of the day to get the • message out.Find a common ground or issue that most members • would be interested in.Have food at meetings.• People are emotional beings in regard to how they • feel about different issues.Build a network of people to get involved.• Spread the word and encourage people to get • involved.
to Be aN aCtIVISt:Support people from other unions; by picketing with • them and/or bringing them food.Start a petition about a cause or issue you are • concerned about.
Talk about and be aware of what is going on in • politics and work issues.Support a political party.• Talk to the MLA representing your area about issues • that concern you.Become more involved in your own union.•
It was beneficial to get to know women from other unions at PSUW – 140 women, representing the various unions attended the school put on by the SFL.
Thank you to SUN for providing me the funding to attend.
Diane Fehr, Local 286 President
Saskatoon Health Region Homecare and Public Health
Thank you so much for the opportunity to attend the Prairie School for Union Women; I was honoured to participate in the workshop “Freedom from Violence”. It was a fantastic experience and I highly recommend it to any union woman debating attendance. The School unites women from a large number of unions and women who share a piece of themselves; the school bringing us together to make our world a better place. By uniting workers and showing us how to make our world a better place, PSUW is extremely relative to our own union – SUN.
The course I attended, “Freedom from Violence”, was facilitated by a social worker and a justice worker for the offenders. This course has opened my eyes and my heart to others with problems dealing with violence in its many forms. We also had Occupational Health and Safety (OH&S) representatives from the Saskatchewan Federation of Labour (SFL) come to address any work issues we may have to face. This course is absolutely valuable and I highly recommend it to all.
At the end of the day, we concluded with the question “What can we do once we leave this course?” The options are numerous - each of the participants, myself included, picks only one of “what we can do”, we will touch the lives of many and hopefully make positive changes in our immediate circles.
I ask that you keep this opportunity open for as many registered nurses as possible to attend. I am willing to speak at the Annual Meeting to promote the PSUW.
I also took the course with the SFL at the Spring School for Collective Bargaining. Now, because of the great influence of the SFL and the education I received, I have run and acquired a position on the provincial Negotiations Committee.
Thanks so much once again – I do put to use all the education you have offered and I have taken.
Yvonne Hotzak, Local 238
Norquay Health Centre

16 • SASKATCHEWAN UNION OF NURSES ISSUE 5 • SEPTEMBER 2011
Next Up: Shaping the next generationIt is hard to put into words what this program
has meant to me. I received an e-mail from SUN encouraging members to apply the very day that I was out for lunch with an old nursing professor of mine. We had been talking about my plans for the future and what I was hoping to achieve. The e-mail advertising Next Up really spoke to the core values that I believe in; social justice, community building and what my role as a registered nurse can play in these. I have long believed that health and the environment are deeply intertwined and I felt that I might be able to gain some skills and experience through this program that would be of use to me in my career as an RN.
Next Up offers participants a variety of ways to learn and experience the progressive values of the program. For seven months we met every Tuesday night to discuss a range of topics and meet a presenter with knowledge and expertise on the subject. Most often these presenters were local community members and we truly formed bonds with them that have lasted outside of the sessions – through working on projects together, organizing events and even just seeing each other out and about and being able to say hi. The topics covered a full spectrum of issues, but all touched on the idea of fostering community, progressive leadership, and what role we might play as young leaders in identifying areas to work on and improve. Some topic examples were: treaties and Aboriginal relations; economics; governance (municipal, provincial and federal); climate change; trade unions; anti-poverty work; advocacy; the social determinants of health; engaging First Voice people – to name only a few.
We also had monthly skills-building workshops – full day intensive training sessions. The topics that were covered in these workshops included facilitation training; anti-oppression training; conflict resolution and transformation; creative activism and media
engagement; and self-care in activism (or how to stay in it for the long haul). These workshops introduced us to speakers from all over the country and have given me many tools, which have been very beneficial to me in all facets of my life, not just my “activist” life. Who among us would not benefit from being more aware of our own conflict triggers, privilege, and ways of handling difficult situations? In the same vein, who among us would not benefit from a deeper understanding of how we engage the media, our fellow colleagues and our patients?
One of the greatest strengths of this program is the bridge building that it offers to participants and members of the community. We have met, and worked with, so many amazing people doing fantastic work in Saskatoon and throughout the province. I know that had it not been for Next Up I would never have had the opportunity to meet many of these people and become engaged in the projects they are working on.
For me personally, Next Up has been a driving force behind much of the work I find myself engaged in today – working with municipal politicians on a variety of civic issues (currently recycling); working with the Saskatchewan Federation of Labour on the Labour Issues campaign; working on Releasing Time to Care™ projects and Patient- and Family-Centred Care projects in my workplace.
Prior to this program I was a politicized, but disengaged, youth. I had a lot of knowledge, passion and potential but I felt as though I was feeling my way around in the dark, searching for ways to apply it. Next Up has helped me to narrow down my focus and identify ways that I can directly impact the world as a citizen, as a nurse and as an informed individual. It has also helped me gain the confidence to start engaging other people around these issues and provided me with many, many connections to people whose experience and opinions I can draw on to support me.
I believe that Next Up has the potential to shape the next generation of progressive leaders and build bridges within a very splintered progressive movement. The program has helped me to grow into myself and allowed me to do that growing within a supportive community.
I would not hesitate to recommend this program to other interested individuals and I am thanking you from the bottom of my heart for having the vision and the generosity to have supported it in its inaugural year. I hope that you will see the value in this program, as I do.
Karen Rooney, RN
SUN Member
*This article has been published as it was submitted to the SUN Board of Directors.

ISSUE 5 • SEPTEMBER 2011 SASKATCHEWAN UNION OF NURSES • 17
O HS �
Dear SUNSpots Editor, I read Norma Wallace’s report on adverse reactions
to Bitrex with interest (SUNSpots, May 2011). As noted in the report, there is little research on adverse reactions during fit testing. In addition to the Youakim reference, the only other reported adverse reactions to Bitrex (denatonium benzoate) that I was able to find was a journal article about a 30 year old male gardener who developed contact urticaria and asthmatic symptoms following exposure to products containing denatonium benzoate (Bjorkner, 1980).
I work as an Occupational Health Nurse in Cypress Health Region and fit testing has been part of my nursing role since 2005. I first became interested in this adverse reaction phenomenon in 2008 after three workers I tested had a reaction to the Bitrex. I also had reports from another tester in our region about two (2) other workers who had reacted. After searching the literature and reading more about denatonium benzoate, I re-evaluated our screening process for fit testing. Since changing the screening questionnaire to better reflect some of the risk factors I had identified, we were able to eliminate all reactions except one (n= 1500) in 2009. Some of the additional risks included reactions to local/topical anesthetics, chemical/perfume and/or household chemical sensitivities.
Bitrex is a trade name. Other names for denatonium benzoate include benzenemethanaminium, N-{2-{2,6-dimethylphenl)amino]-2-oxoethyl}N,N-diethyl-, benzoate. Denatonium benzoate is used not only to prevent animals and children from drinking substances such as anti-freeze, but it is also a denaturant for alcohol in cosmetics; as a denaturant it acts as an astringent, solvent and/or viscosity decreasing agent. Cosmetic agents that may have denatonium benzoate can include eyeliner, eye shadow, mascara and eye makeup remover, perfumes and colognes, hair conditioners, hair colour, foundations, deodorants, and suntan products. The US Cosmetic Ingredient Review (CIR) Expert Panel released their report on the safety assessment of alcohol denaturants including denatonium benzoate in 2007. Their findings were that denatonium benzoate was non-irritating and not sensitizing. (see reference list to access this report.) One weakness in their findings is that researchers used lidocaine to make their case. Lidocaine has an almost identical molecular structure to denatonium benzoate except that the lidocaine molecule is smaller.
I endorse Ms. Wallace’s advice that anyone who believes that they have had a reaction during fit testing should report it to someone in their OH&S department. I would discourage closing your eyes during qualitative
testing because of the qualitative nature of this type of testing requires both verbal and non-verbal communication. Using goggles or safety glasses would be preferred and in fact, will help ensure the fit as most often we wear both in actual practice. Also, washing your face especially around your mouth after testing is good practice. Change or wash your tunic or shirt as soon as you can as well. I find that after I have tested that the denatonium benzoate clings to my clothing.
Denatonium benzoate has a CAS number (3734-33-6) so there are means to let the authorities know of a problem. The Ministry of Labour Relations and Workplace Safety had been documenting and reporting incidents for us. Since I have been fit testing, 3M, the major supplier of fit testing solutions, has changed their labeling to reflect Bitrex as a WHMIS controlled product. The label shows it as a Class D2 – other toxic effects. Other substances that can be used to test qualitatively include irritant smoke and saccharin. Both of these have been implicated as carcinogens thus the rationale for using Bitrex. It is not clearly understood why healthcare workers seem to have such a high incidence of reactions. Other industries have used Bitrex without incident.
I am working on a research project about this phenomenon and a question that I am continuing to work on is why do healthcare workers experience reactions to Bitrex and how can we reduce the risk? While I have identified some risk factors for reactions, I am very interested in stories from healthcare workers who have experienced reactions to Bitrex during fit testing. Any readers who would like to contact me with their experiences are welcome to by e-mailing me at one of the following: [email protected] or [email protected]
Mary Anderson, RN BSN COHN(C)
ReferencesBjorkner, B. (1980). Contact urticaria and asthma from denatonium
benzoate (Bitrex). Contact Dermatitis, 6,(7), 466 – 471 Retrieved from Ebscohost.
Andersen, F. (2008). Final report of the safety assessment of alcohol denat., including SD alcohol 3-A, SD alcohol 30, SD alcohol 39, SD alcohol 39B, SD alcohol 40-C, and the denaturants, quassin, brucine sulfate/ brucine, and denatonium benzoate. International Journal of Toxicology, 27(Suppl.1)1-43 doi: 10.1080/10915810802032388
Youakim, S. (2007) Adverse reactions associated with respirator fit testing of health care workers in British Columbia, Canada: a review of compensation claim cases. Archives of Environmental & Occupational Health, 62, (4), 197-200. Retrieved from Ebscohost.
18 • SASKATCHEWAN UNION OF NURSES ISSUE 5 • SEPTEMBER 2011
SUN Memorial Scholarship The SUN Memorial Scholarship Fund was initiated
at the request of the family of one of SUN’s former presidents, upon her passing. Annually, the trustees of the SUN Memorial Scholarship Fund award two $750 bursaries to first or second year students enrolled in a Registered Nursing education program in Saskatchewan, one at each of the SIAST Wascana and Kelsey campuses. In addition, SUN also offers the same scholarship to first or second year students enrolled in the Registered Nursing education program at the First Nations University in Prince Albert.
SUN is pleased to announce the winners of the 2011 SUN Memorial Scholarships. Congratulations to:
Kim Strinja • SIAST, Wascana Campus (Regina) (photo unavailable)Amie-Lee Rusk • SIAST, Kelsey Campus (Saskatoon)
Amie Rusk Merissa Azure
Merissa Azure • First Nations University, Prince Albert CampusSUN wishes our scholarship winners, and all
registered nursing students, the best of luck in their studies and in their careers as registered nurses.
SUN ends provincial-wide approval The recruitment of Internationally Educated Nurses,
an issue which engages SAHO, RHAs, SUN and the Provincial Government, has been prominent on all our respective agendas for some time.
In 2002, recognizing the acute nursing shortage, government and SAHO were advised that SUN was prepared to indicate province-wide approval for the recruitment of Internationally Educated RNs and RPNs.
SUN’s requirement was that Employers inform the Union, in advance, of their request for a visa from Human Resources Department of Canada (HRDC). Should SUN then have an objection to the issuance of a specific visa, we would inform the employer and, if required and as appropriate, HRDC. We advanced this streamlined process to HRDC and were assured in 2002, that this procedure would satisfy the requirements of the department.
However, in light of many varied experiences for our members and local leaders, lack of information from Employers in advance of their recruitment initiatives – recruitment to other than permanent positions – it has been determined that effective immediately SUN is withdrawing province-wide approval for future recruitment of Internationally Educated RNs and RPNs.
The effect of this change will require all Employers to comply with Article 27.08 prior to recruiting and filling positions.
Article 27.08 of the SUN/SAHO Collective Agreement reads:
Foreign-trained Registered Nurses or Registered Psychiatric Nurses may be recruited to fill vacant positions, upon confirmation in writing, by the Employer to the Union that:
All Articles/Letters of Understanding in the a) Collective Agreement have been exhausted regarding filling of vacancies; The Employer has offered specific nursing training, b) including orientation and training for certifiable skills at the Employer’s expense to Registered Nurses or Registered Psychiatric Nurses in the Regional Health Authority and/or bargaining unit, and; The Employer has advertised Locally, Provincially c) and Nationally. This change in practice is in no way meant to
compromise any SUN members who are Internationally Educated Nurses currently employed throughout the province. SAHO and Employers have been notified.
Your Employment Relation Officer will be able to assist with any questions you may have.
ISSUE 5 • SEPTEMBER 2011 SASKATCHEWAN UNION OF NURSES • 19
Fall 2011 Regional Workshops10 locations to choose from …
September 19 Swift CurrentSeptember 21 WeyburnSeptember 29 Regina La RongeOctober 4 LloydminsterOctober 5 RosetownOctober 6 SaskatoonOctober 12 Yorkton Prince AlbertOctober 13 Tisdale
Visit our web site for workshop details www.sun-nurses.sk.ca
register on-line today
2011 Education ConferenceNovember 2 and 3, 2011TCU Place, Saskatoon
Registration is now open! Registration Deadline: October 21, 2011Conference details can be found on-line at
www.sun-nurses.sk.ca Register on-line today!
United WayThe Canadian Federation of Nurses Unions (CFNU) and SUN encourage all registered nurses to support the 2011 United Way Centraide campaign.
These annual campaigns bring together much needed resources for communities – financial and human energy. We’ve seen what economic crisis can do to individuals, families and entire communities. It’s by working together and supporting one another, that we can strengthen and protect the health and prosperity for our communities.
Union members have continued to be extremely generous in responding to the needs of their community, but it’s not over and we need to continue working closely with United Way Centraide.
www.unitedway.ca
2011 Innovators Conference: Moving Patient- and
Family-Centred Care ForwardRamada Hotel & Convention Centre, Regina
September 27th, 2011
Keynote Speaker: Dr. Mary Ferguson-Paré “Leading from where you stand”2011 Patient and Families First Challenge ShowcaseInnovation and Leadership in Patient- and Family-Centred Care Panel
Mireille Brosseau • Program Lead, Patient and Citizen Engagement Canadian Health Services Research Foundation (CHSRF)Kevin Fenwick • Saskatchewan OmbudsmanPetrina McGrath, RN • Vice-President, Inter professional Practice and Chief Nursing Officer Saskatoon Health Region
PLUS 18 exciting and innovative approaches to patient- and family-centred care.
More conference details can be found on-line at www.sun-nurses.sk.ca
Plan to attend the 2011 SUN Bargaining Conference
Meet Your Negotiations Committee November 15, 2011
Reception 7:00 – 10:00 pm; Cash barBargaining Conference November 16-17, 2011
Delta Regina Hotel Registration opens mid-September
20 • SASKATCHEWAN UNION OF NURSES ISSUE 5 • SEPTEMBER 2011
Return Undeliverable Canadian Addresses to:2330 2nd Avenue Regina, SK S4R 1A6Telephone: 306-525-1666 Toll Free: 1-800-667-7060Fax: 306-522-4612E-mail: [email protected] site: www.sun-nurses.sk.ca Publication Agreement Number – 40065076
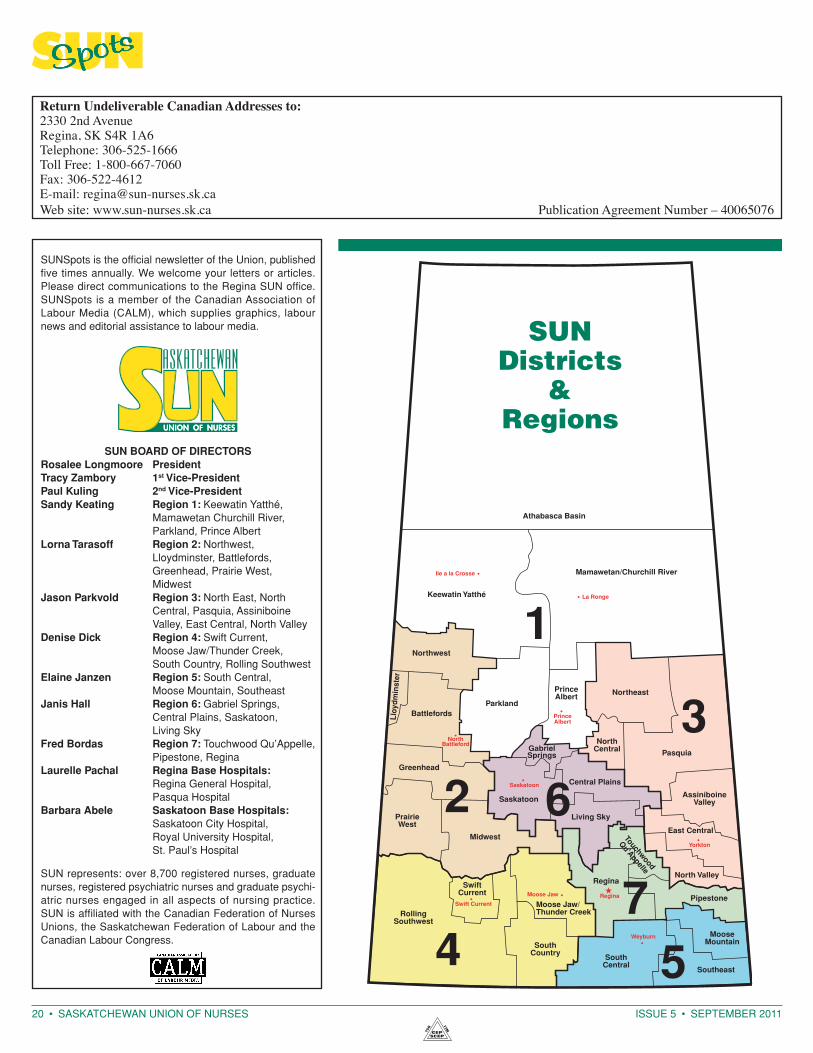
SUN Districts
& Regions
SUN represents: over 8,700 registered nurses, graduate nurses, registered psychiatric nurses and graduate psychiatric nurses engaged in all aspects of nursing practice. SUN is affiliated with the Canadian Federation of Nurses Unions, the Saskatchewan Federation of Labour and the Cana dian Labour Congress.
SuN Board of dIreCtorSrosalee longmoore president tracy zambory 1st Vice-president paul kuling 2nd Vice-president Sandy keating region 1: Keewatin Yatthé,
Mamawetan Churchill River, Parkland, Prince Albert
lorna tarasoff region 2: Northwest, Lloydminster, Battlefords, Greenhead, Prairie West, Midwest
jason parkvold region 3: North East, North Central, Pasquia, Assiniboine Valley, East Central, North Valley
denise dick region 4: Swift Current, Moose Jaw/Thunder Creek, South Country, Rolling Southwest
elaine janzen region 5: South Central, Moose Mountain, Southeast
janis hall region 6: Gabriel Springs, Central Plains, Saskatoon, Living Sky
fred Bordas region 7: Touchwood Qu’Appelle, Pipestone, Regina
laurelle pachal regina Base hospitals: Regina General Hospital, Pasqua Hospital
Barbara abele Saskatoon Base hospitals: Saskatoon City Hospital, Royal University Hospital, St. Paul’s Hospital
SUNSpots is the official newsletter of the Union, published five times annually. We welcome your letters or articles. Please direct communications to the Regina SUN office. SUNSpots is a member of the Canadian Association of Labour Media (CALM), which supplies graphics, labour news and editorial assistance to labour media.