view the q3 2008 newsletter - bcbswny.com€¦ · detailing your request (including language ......
TRANSCRIPT

Notice If a website link within this document does not direct you to the appropriate information or website location, please contact Provider Services by telephone. The Provider Services directory is located on the last page of this document.

STAT Newsletter
Volume 19 Third Quarter, 2008
2008-5976 WNY Page 1 CC 1501
Free CMEs for Physicians.........................1 Health Care Proxy ......................................1 Anticipatory Guidance Reminder .............2 Medical Services Protocol Updates .........3 Prescription Drug Formulary Updates.......................................................8 Radiation Safety Awareness Initiative ......................................................9 Hospital Coding: Present on Admission (POA) Indicator .....................11 Perceived Denials ....................................12 2008 – 2009 Vaccine Reimbursement Update.......................................................13 Opting Out of Medicare ...........................13 Quest Diagnostics Lab Exceptions ........14 Medicaid Managed Care and Family Health Plus Members Cannot Be Billed .........................................................16 Information on Provider “Gap” Reports .....................................................17 Member Rights and Responsibilities .....17 What’s New? Our Newer, Easier Provider Web Site! ...................................18 Updated UM Phone Prompts...................18 Provider Telephone and Web Site Reference Guide ................................. Back
Free CMEs for Physicians Enhanced cultural competency in healthcare professionals results in healthier patients, and health literacy and cultural competency for healthcare providers is a hot topic these days. Some of the most common misunderstandings between doctors and their patients are diagnosis, test results and prescription instructions. Understanding what you say to them about their health can mean the difference between your patients' compliance and non-compliance.
Inside This Issue
The Medical Society of the State of New York (MSSNY) is offering an online continuing medical education (CME) program for 2.0 American Medical Association (AMA) Physician's Recognition Award (PRA) Category 1 credits, designed to teach physicians how to provide their patients with healthcare information that is clearly understood. This free program can be found at www.mssny.org. In the lower right hand corner, click "New Cultural Competence CME Course," then "Online CME Program" at the bottom of the next screen. Click "New User" and use 7000 as the organization ID when registering. Health Care Proxy While your patients hope they’ll always be in a position to make their own healthcare decisions, there are occasions when a patient becomes unable to do so. A health care proxy allows individuals to make healthcare decisions in advance and to designate an agent (usually a family member) to make healthcare decisions for them if they become unable to do so. (continued on page 2)

Page 2
(continued from page 1) Take the opportunity to discuss the health care proxy process with your patients and stress the importance of appointing someone they trust to make healthcare decisions for them in the event they become incapacitated. Advise them that a health care proxy ensures that healthcare providers will follow their wishes. Remind your patients that the document must be signed in front of two witnesses and a copy placed in their health file, as well as given to a family member or friend. The health care proxy form is available free of charge from the New York State Department of Health web site at:
http://www.health.state.ny.us/professionals/patients/ health_care_proxy/index.htm.
The form is available in English, Spanish, Chinese and Russian. Assist your patients by having these forms available in your office. For those without computer access, call 1-877-878-8785 (toll-free), leave a message detailing your request (including language requested) and a copy of the free health care proxy will be sent to you. For a small fee, a health care proxy in numerous other languages can be obtained. It is available only at www.agingwithdignity.com and is available in the following languages: Albanian, Arabic, Bengali, Chinese Simplified, Chinese Traditional, Croatian, French, Gujarati, Haitian Creole, Hindi, Hmong, Japanese, Korean, Polish, Portuguese, Russian, Somali, Spanish, Urdu, and Vietnamese.
Anticipatory Guidance Reminder Recently, the New York State Department of Health studied adolescent care and the rate of physician discussions of anticipatory guidance with their patients. This study found a need to improve the rate at which adolescents receive this type of counseling, especially regarding tobacco use. Adolescent well care visits are important opportunities for direct communication between the adolescent and healthcare provider. Take the opportunity for discussion and/or screening of the topics listed below. Document the occurrence when each of these state-required topics is addressed.
• Body mass index • Nutrition • Exercise • Risk behaviors (e.g., sexual behavior, etc.) • Depression • Tobacco • Substance abuse
Page 3
Medical Services Protocol Updates The following clinical protocol update includes information on protocols that have been reviewed with revision or are new. Their effective date is October 1, 2008, unless otherwise noted. It also includes a listing of the protocols that have had an annual review resulting in no change to the guideline. Please note that some of this protocol update may not pertain to the members you provide care to, as it may relate to contracts that are not available in your geographic area. Protocol Summary New Policy: Clinical Trials • Routine services of qualifying clinical trials are eligible for coverage (usual edits apply, such as but not
limited to, prior approval, unbundling, investigational, contract in effect at time of service, etc.). • The item, device, drug or service that is the focus of the trial is not covered and will be rejected as
investigational if billed to BlueCross BlueShield. • For Senior Blue/Medicare PPO, claims for clinical trials should be submitted to original Medicare, not
BlueCross BlueShield. Annual Review with Guideline Change: 1. Cochlear Implant
• Guidelines added for bilateral cochlear implantation. • Clarification included that upgrades of existing, functioning systems to achieve aesthetic improvement or
to switch from a body-worn external sound processor to a behind-the-ear model are not medically necessary.
2. Dynamic Posturography
Changed guideline statement from "investigational" to "not medically necessary." 3. Hyperbaric Oxygen Therapy
Added soft-tissue radiation necrosis and osteoradionecrosis, as well as pre- and post-treatment for patients undergoing dental surgery of an irradiated jaw as medically appropriate indications. This addition eliminated the need for the separate Senior Blue/Medicare PPO policy statement.
4. Implantation of Intrastromal Corneal Ring Segments
Added medically appropriate criteria for patients with keratoconus. Prior approval is required.
5. Keratoprosthesis Previously indicated as medically appropriate for Senior Blue/Medicare PPO, but will now be considered investigational. (continued on page 4)

Page 4
(continued from page 3) 6. Measurement of Exhaled Nitric Oxide and Exhaled Breath Condensate in the Diagnosis and
Management of Asthma and Other Respiratory Disorders, and Semi-Implantable Middle Ear Hearing Aid for Moderate to Severe Sensorineural Hearing Loss Remain investigational, but the reason has been updated to indicate that literature does not support improvement in health outcomes.
7. Outpatient Pulmonary Rehabilitation
• Title and guidelines changed to clarify protocol pertains to outpatient pulmonary rehabilitation. • The word "obstructive" was removed from the first sentence in the guideline, therefore making the service
appropriate for chronic pulmonary disease rather than only for chronic obstructive pulmonary disease. 8. Rhinomanometry and Acoustic/Optical Rhinometry
Policy now applies to optical rhinometry as well as acoustic. 9. Stereotactic Radiosurgery
Added to and re-worded guidelines. 10. Subtalar Arthroereisis
Remains investigational, but the reason has been updated to indicate it has not been proven as effective as established alternatives.
11. Surgery for Morbid Obesity
Added a statement in guidelines that says endoscopic procedures for weight gain after bariatric surgery are considered investigational.
12. Vertebral Fracture Assessment with Densitometry
Included guidelines for when this is medically appropriate for Senior Blue/Medicare PPO. Clinical Protocols Reviewed Without Change: The following clinical protocols were reviewed in May and did not require revision to their guidelines. Previous effective dates remain accurate. • Ambulance (emergency) • Blood or Marrow Transplantation • Cognitive Rehabilitation • Diagnosis and Medical Management of Obstructive Sleep Apnea Syndrome • End Diastolic Pneumatic Compression Boot as a Treatment of Peripheral Vascular Disease or Lymphedema • Fetal Surgery for Prenatally Diagnosed Malformations • Functional Neuromuscular Stimulation to Provide Ambulation • Low-Level Laser Therapy as a Treatment of Carpal Tunnel Syndrome • Lysis of Epidural Adhesions • Magnetoencephalography/Magnetic Source Imaging • Mechanical Insufflation-Exsufflation as an Expiratory Muscle Aid (continued on page 5)

Page 5
(continued from page 4) • Minimally Invasive Surgery for Snoring, Obstructive Sleep Apnea Syndrome/Upper Airway Resistance
Syndrome • Nerve Graft in Association with Radical Prostatectomy • Osteochondral Autografts and Allografts in the Treatment of Focal Articular Cartilage Lesions • Percutaneous Vertebroplasty and Kyphoplasty • Plasma Exchange (Plasmapheresis) • Sensory Integration Therapy • Serum Antibodies for the Diagnosis of Inflammatory Bowel Disease • Surgical Management of Obstructive Sleep Apnea Syndrome/Upper Airway Resistance Syndrome • Surgical Ventricular Restoration • Transesophageal Endoscopic Therapies for Gastroesophageal Reflux Disease • Vagus Nerve Stimulation • Videofluoroscopic Evaluation of Velopharyngeal Dysfunction • Wearable Cardioverter-Defibrillators as a Bridge to Implantable Cardioverter-Defibrillator Placement The following clinical protocols were reviewed in July and did not require revision to their guidelines. Previous effective dates remain accurate. • Adjustable Banding as a Treatment of Plagiocephaly • Ambulatory Event Monitors and Mobile Cardiac Outpatient Telemetry • Artificial Intervertebral Disc: Cervical Spine • Artificial Intervertebral Disc: Lumbar Spine • Cardiac Rehabilitation • Computer-assisted Musculoskeletal Surgical Navigational Orthopedic Procedure • Continuous or Intermittent Monitoring of Glucose in the Interstitial Fluid • Corneal Topography/Computer-Assisted Photokeratoscopy • Cosmetic vs. Reconstructive Services • Cutaneous Electrogastrography (EGG) • Electrical Stimulation for the Treatment of Arthritis • Electrostimulation and Electromagnetic Therapy for the Treatment of Chronic Wounds • Endovascular Grafts for Abdominal Aortic Aneurysms • Gait Analysis • Genetic Testing for Familial Alzheimer’s Disease • Implantable Bone-Conduction and Bone-Anchored Hearing Aids • Interspinous Distraction Devices (Spacers) • Maze Procedure • Salivary Estriol as Risk Predictor for Preterm Labor • Selective Internal Radiation Therapy for Primary and Metastatic Tumors of the Liver • Thermography • T-Wave Alternans (continued on page 6)

(continued from page 5) Billing Reminders: As part of national coding guidelines, the most specific CPT/HCPCS code should always be used, when one exists. Here are some codes that apply to Medical Protocols: Artificial Intervertebral Disc: Cervical Spine 0090T Total disc arthroplasty (artificial disc), anterior approach, including diskectomy to prepare interspace
(other than for decompression), cervical; single interspace 0092T Each additional interspace 0093T Removal of total disc arthroplasty, anterior approach; single interspace, cervical; single interspace 0095T Each additional interspace 0096T Revision of total disc arthroplasty, anterior approach; cervical; single interspace 0098T Each additional interspace Artificial Intervertebral Disc: Lumbar Spine 22857 Total disc arthroplasty (artificial disc), anterior approach, including discectomy to prepare interspace
(other than for decompression), lumbar, single interspace 0163T Each additional interspace 22862 Revision including replacement of total disc arthroplasty (artificial disc) anterior approach, lumbar, single
interspace 0165T Each additional interspace 22865 Removal of total disc arthroplasty (artificial disc), anterior approach, lumbar, single interspace 0164T Each additional interspace Clinical Trials • HCPCS
Billed once on each claim with a 0.00 charge: S9988 Services provided as part of a Phase I clinical trial S9990 Services provided as part of a Phase II clinical trial S9991 Services provided as part of a Phase III clinical trial
• ICD 9 Diagnosis Billed for each service that is provided to treat the condition, for which the investigational device, drug, or service is being provided: V70.7 Examination of participant in a clinical trial
• Additional Indicators Either the Q0 or Q1 modifier is billed on each service that is provided: Q0 Investigational clinical service provided in a clinical research study that is an approved clinical
research study Q1 Routine clinical service provided in a clinical research study that is in an approved clinical research
study Condition code 30 is available for inpatient claims to indicate the admission includes qualifying trial services.
There are no modifiers or condition codes to use for non-qualifying trials. Non-qualifying trials should not be billed to BlueCross BlueShield.
(continued on page 7)
Page 6
(continued from page 6) End Diastolic Pneumatic Compression Boot as a Treatment of Peripheral Vascular Disease or Lymphedema There are no specific CPT/HCPCS codes for this service. It might be reported as a series of CPT codes which describe the individual components of the overall therapy such as: 92971 Cardioassist-method of circulatory assist; external 93041 Rhythm ECG, one to three leads; tracing only without interpretation and report Evaluation and Management codes Or it might be report as: 99199 Unlisted special service, procedure or report Note: The following HCPCS code was created specifically for external counterpulsation as a treatment of
chronic refractory angina, and not for the compression boot: G0166 External counterpulsation, per treatment session
Implantation of Intrastromal Corneal Ring Segments 0099T Implantation of intrastromal corneal ring segments Interspinous Distraction Devices (Spacers) 0171T Insertion of posterior spinous process distraction device (including necessary removal of bone or ligament
for insertion and imaging guidance), lumbar, single level 0172T Each additional level Selective Internal Radiation Therapy for Primary and Metastatic Tumors of the Liver S2095 Transcatheter occlusion or embolization for tumor destruction, percutaneous, any method, using yttrium-
90 microspheres Subtalar Arthroereisis S2117 Arthroereisis, subtalar
Page 7

Prescription Drug Formulary Updates The following is a summary of recent changes to the prescription drug formulary. For a complete list of the medications we manage and the corresponding clinical coverage criteria under prescription drug benefits, please refer to our web site at www.bcbswny.com. FDA warning on estriol compounds – change in coverage Based on recent information from the U.S. Food and Drug Administration (FDA), retail purchases of compounded bio-identical hormone therapy products with estriol are no longer covered. Why these products are no longer covered On January 9, 2008, the FDA sent warning letters to several compounding pharmacies that have made unproven claims about the safety and effectiveness of their compounded bio-identical hormone products. The FDA is concerned that the claims aren’t supported by medical evidence and are false and misleading. In addition, the FDA warned all pharmacies about compounding with estriol. The FDA’s opinion is that pharmacies shouldn’t compound with estriol unless they have a valid investigational new drug application on file with the FDA. As of July 15, 2008, members who chose to purchase one of these products began paying the full price. Members who were utilizing an estriol compound were notified of this coverage change by letter on May 29, 2008, and were encouraged to ask their physicians if one of the many other oral or topical FDA-approved estrogen products may be right for them.
Medications now available over the counter (OTC) – change in coverage The following medications are now available over the counter (OTC) and are therefore no longer covered under the prescription drug benefit: Zyrtec®, Miralax® and Glycolax. New prior authorization requirements As of January 21, 2008, the following medications required prior authorization: Topamax® and Zonegran®. As of May 1, 2008, the following medications required prior authorization: Singulair®, Accolate®, Zyflo® and Zyflo CR®. Coverage criteria for these medications are available online. Review of oral anti-diabetic medications, statins and ARBs – new quantity limits We recently reviewed the drug classes oral anti-diabetic medications, statins and angiotensin receptor blockers (ARBs) and, as a result, we are placing quantity limits on prescriptions for oral anti-diabetic medications, statins and ARBs, effective June 1, 2008. For a number of reasons, members may take prescription drugs in ways that may unnecessarily increase the number of pills taken. Quantity limits encourage more effective prescribing of drugs and make it easier for patients to comply with providers' recommendations. Some patients' prescriptions may need to be adjusted in order to maintain their medications at the appropriate dosage. If a provider determines that a patient’s current prescription must be maintained, he or she can do so through the prior authorization approval process. (continued on page 9)
Page 8

(continued from page 8) Step edit changes Soon to come The following medications no longer have a step edit requirement in place:
Prescriptions written by nephrologists, oncologists and hematologists for recombinant erythropoietin agents are currently exempt from needing prior authorization. This specialist edit will be removed. Effective September 1, 2008, prior authorization for the medications Epogen®, Procrit® and Aranesp® will be required for all providers. Coverage criteria for these medications are available online.
Formulary anticholinergic urinary agents available on Tier 2: Detrol® and Detrol LA® Non-formulary Proton Pump Inhibitor (PPI) available on Tier 3: Zegerid® Generic Fosamax® now available
The medication alendronate (generic Fosamax®) is now commercially available. Brand Fosamax® has been moved to Tier 3, and alendronate is now formulary on Tier 1, at the lowest cost to members. Radiation Safety Awareness Initiative We are pleased to inform you that BlueCross BlueShield of Western New York will begin a radiation safety awareness initiative in September in conjunction with National Imaging Associates (NIA), our nationally recognized radiology benefits manager. We are taking this proactive approach in order to improve patient safety and raise awareness regarding radiation exposure. As you know, radiation exposure from medical imaging is a rapidly growing patient safety issue. Patients are exposed to nearly six times more radiation from medical diagnostic tests than they were in 1980. The largest contributors to the increase in medical radiation exposure are CT scans and nuclear medicine. How is your patient identified? "At-risk" patients are those with cumulative radiation exposure equal to, or over, a level that has been identified as detrimental to long term health, thus, putting them at an increased risk of developing radiation-associated complications such as cancer. They are identified through radiology claims which are provided to NIA by BlueCross BlueShield twice a year for analysis of radiation exposure based on those claims. How am I notified if one of my patients is identified at-risk? You will be notified by telephone or by an online alert at the time a radiology procedure is reviewed for preauthorization. A provider alert letter will also be sent via fax or mail. Note: The patient’s level of radiation exposure does not impact the preauthorization or decision-making process for requested imaging studies. (continued on page 10)
Page 9
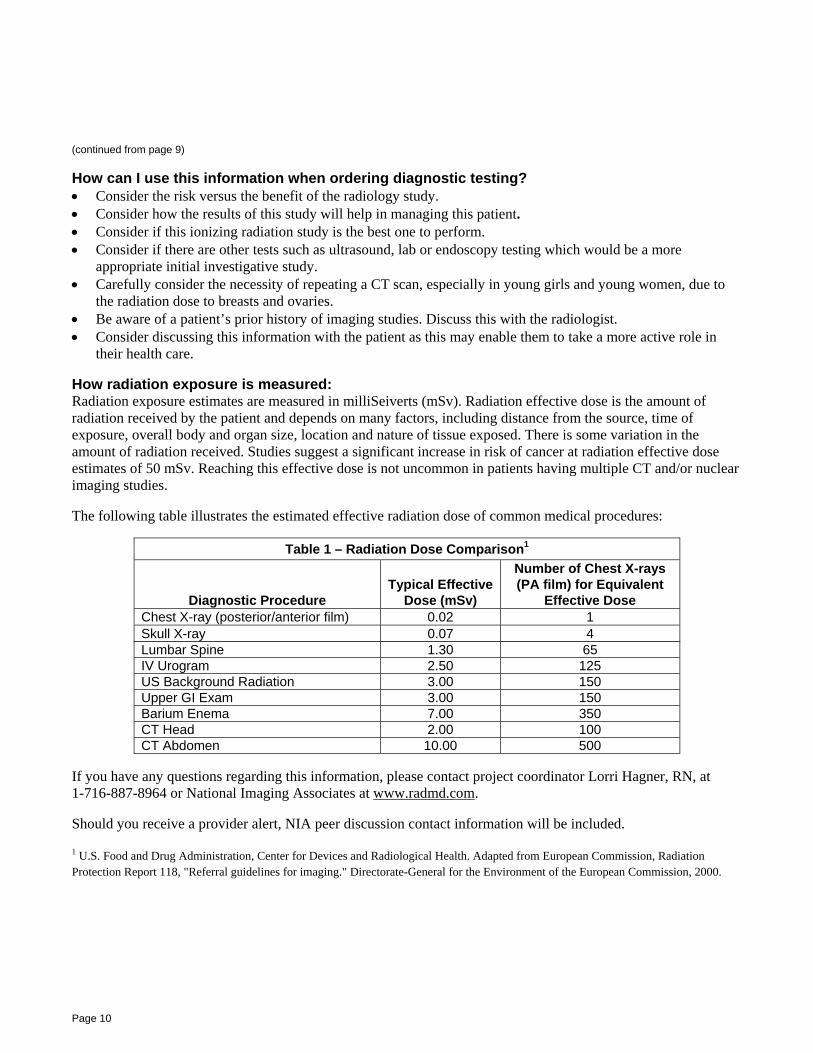
(continued from page 9) How can I use this information when ordering diagnostic testing? • Consider the risk versus the benefit of the radiology study. • Consider how the results of this study will help in managing this patient. • Consider if this ionizing radiation study is the best one to perform. • Consider if there are other tests such as ultrasound, lab or endoscopy testing which would be a more
appropriate initial investigative study. • Carefully consider the necessity of repeating a CT scan, especially in young girls and young women, due to
the radiation dose to breasts and ovaries. • Be aware of a patient’s prior history of imaging studies. Discuss this with the radiologist. • Consider discussing this information with the patient as this may enable them to take a more active role in
their health care. How radiation exposure is measured: Radiation exposure estimates are measured in milliSeiverts (mSv). Radiation effective dose is the amount of radiation received by the patient and depends on many factors, including distance from the source, time of exposure, overall body and organ size, location and nature of tissue exposed. There is some variation in the amount of radiation received. Studies suggest a significant increase in risk of cancer at radiation effective dose estimates of 50 mSv. Reaching this effective dose is not uncommon in patients having multiple CT and/or nuclear imaging studies. The following table illustrates the estimated effective radiation dose of common medical procedures:
Table 1 – Radiation Dose Comparison1
Diagnostic Procedure Typical Effective
Dose (mSv)
Number of Chest X-rays (PA film) for Equivalent
Effective Dose Chest X-ray (posterior/anterior film) 0.02 1 Skull X-ray 0.07 4 Lumbar Spine 1.30 65 IV Urogram 2.50 125 US Background Radiation 3.00 150 Upper GI Exam 3.00 150 Barium Enema 7.00 350 CT Head 2.00 100 CT Abdomen 10.00 500
If you have any questions regarding this information, please contact project coordinator Lorri Hagner, RN, at 1-716-887-8964 or National Imaging Associates at www.radmd.com. Should you receive a provider alert, NIA peer discussion contact information will be included. 1 U.S. Food and Drug Administration, Center for Devices and Radiological Health. Adapted from European Commission, Radiation Protection Report 118, "Referral guidelines for imaging." Directorate-General for the Environment of the European Commission, 2000.
Page 10

Hospital Coding: Present on Admission (POA) Indicator Effective October 1, 2008, BlueCross BlueShield of Western New York will now require "Present on Admission" (POA) values on all claim submissions from acute care hospitals. Please ensure that valid POA values are submitted on electronic or paper claim forms. Claims submissions received without valid POA values indicated will be returned. The following information from the UB-04 Data Specifications Manual is provided to help you understand how and when to code POA indicators. General Reporting Requirements • "Present on Admission" is defined as a condition present at the time the order for inpatient admission occurs. • Conditions that develop during an outpatient encounter, including emergency department, observation or
outpatient surgery, are considered as present on admission. • A POA indicator is assigned to the principal and secondary diagnoses (as defined in Section II of the Official
Guidelines for Coding and Reporting) and the external cause of injury codes. As determined by the Centers for Medicare and Medicaid Services (CMS) and the National Uniform Billing Committee (NUBC), the reporting options and definitions for POA values are as follows.
Reporting Options and Definitions
Y = Yes. (Condition present at the time of inpatient admission.)
N = No. (Condition not present at the time of inpatient admission.)
U = Unknown. (Documentation is insufficient to determine if the condition was present at the time of inpatient admission.)
W = Clinically Undetermined. (The provider is unable to clinically determine whether the condition was present at the time of inpatient admission or not.)
1 = Unreported/Not used – exempt from POA reporting. (This code is the equivalent of a blank on the UB-04. Since it has been determined that blanks are undesirable when submitting electronically, this POA indicator should be utilized instead of a blank.)
The POA appears in the last (or eighth) position of the diagnosis code field on a UB-04 paper claim and in the K3 segment of the 837 Institutional electronic claim submission.
Page 11
Perceived Denials We recognize, appreciate and support your efforts to manage the care of your Medicare Advantage HMO and Medicare PPO patients in a prudent, cost-effective manner. However, the Centers for Medicare & Medicaid Services (CMS) require that when a member perceives a denial of treatment or care, he/she is entitled to certain appeal rights under federal law. This includes situations in which the member's request is made directly to the provider and one of the following conditions exists:
• The member disagrees with your prescribed course and/or type of treatment.
• You decline to provide a course of treatment and/or type of treatment that the member is requesting.
• You discontinue a course of treatment or reduce a course of treatment.
Examples of Denial Some examples of a perceived denial are: • A patient asks to be referred to a radiologist for
an MRI but you feel that an MRI is not necessary.
• A new prescription drug comes out on the market and one of your patients would like you to prescribe it for him/her. You decline to write the prescription at the present time because the American Medical Association and the Food and Drug Administration have not yet approved the drug for use in the senior population.
• A patient asks to be referred to a dermatologist for the treatment of a rash. You decline to refer the patient because you can effectively treat him/her yourself.
• A patient is receiving physical therapy services and you determine that physical therapy is no longer necessary.
Your Responsibility When a perceived denial occurs, the following must take place: • You must contact the Use Management
department (previously known as the Medical Management department) the day that the denial occurs to apprise the Medicare Advantage HMO and/or Medicare PPO of the situation. It is your responsibility to ensure that our members are informed of their right to appeal.
• We will then issue a letter stating the details of the denial, including a description and reason for the denial. The letter will inform the member of the clinical rationale, as well as the right to obtain reconsideration, and the procedure for requesting reconsideration. You will receive a copy of this letter at the same time the letter is sent to the member.
• The member will be advised that he/she can appeal if they do not agree with our decision about their health care.
Please contact our Use Management department at 1-716-884-2942 or 1-800-677-3086 if you have any questions about perceived denials.
Page 12
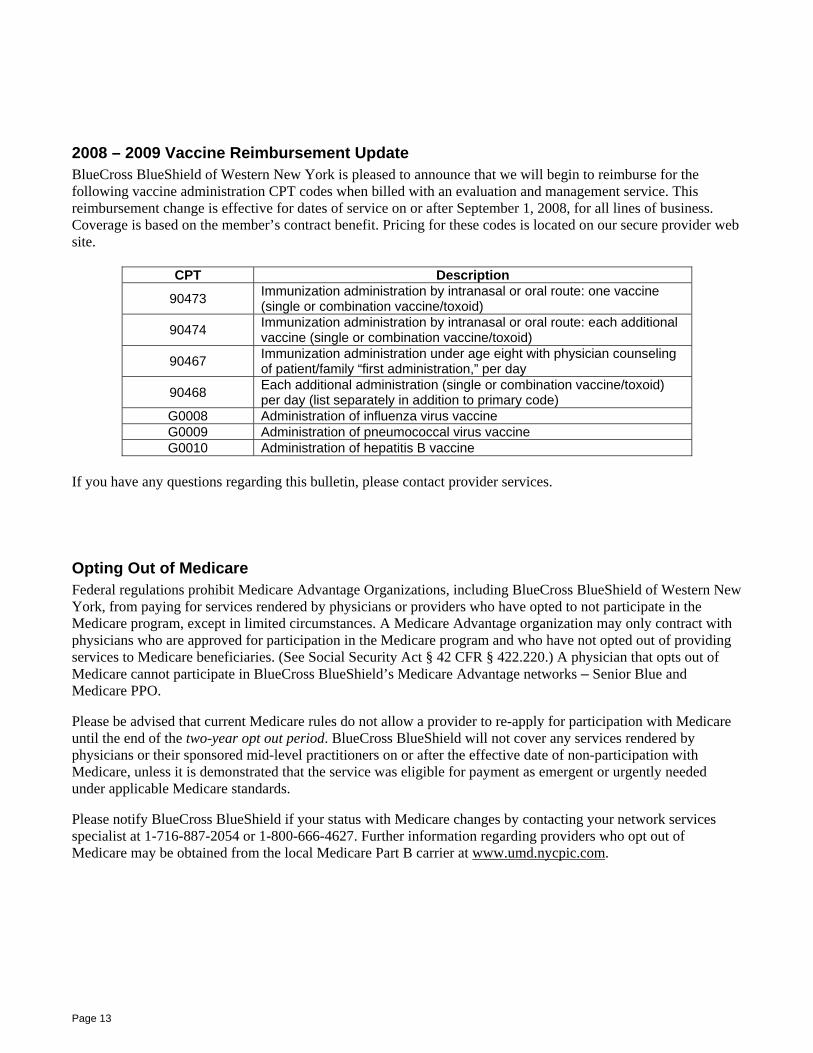
2008 – 2009 Vaccine Reimbursement Update BlueCross BlueShield of Western New York is pleased to announce that we will begin to reimburse for the following vaccine administration CPT codes when billed with an evaluation and management service. This reimbursement change is effective for dates of service on or after September 1, 2008, for all lines of business. Coverage is based on the member’s contract benefit. Pricing for these codes is located on our secure provider web site.
CPT Description
90473 Immunization administration by intranasal or oral route: one vaccine (single or combination vaccine/toxoid)
90474 Immunization administration by intranasal or oral route: each additional vaccine (single or combination vaccine/toxoid)
90467 Immunization administration under age eight with physician counseling of patient/family “first administration,” per day
90468 Each additional administration (single or combination vaccine/toxoid) per day (list separately in addition to primary code)
G0008 Administration of influenza virus vaccine G0009 Administration of pneumococcal virus vaccine G0010 Administration of hepatitis B vaccine
If you have any questions regarding this bulletin, please contact provider services. Opting Out of Medicare Federal regulations prohibit Medicare Advantage Organizations, including BlueCross BlueShield of Western New York, from paying for services rendered by physicians or providers who have opted to not participate in the Medicare program, except in limited circumstances. A Medicare Advantage organization may only contract with physicians who are approved for participation in the Medicare program and who have not opted out of providing services to Medicare beneficiaries. (See Social Security Act § 42 CFR § 422.220.) A physician that opts out of Medicare cannot participate in BlueCross BlueShield’s Medicare Advantage networks – Senior Blue and Medicare PPO. Please be advised that current Medicare rules do not allow a provider to re-apply for participation with Medicare until the end of the two-year opt out period. BlueCross BlueShield will not cover any services rendered by physicians or their sponsored mid-level practitioners on or after the effective date of non-participation with Medicare, unless it is demonstrated that the service was eligible for payment as emergent or urgently needed under applicable Medicare standards. Please notify BlueCross BlueShield if your status with Medicare changes by contacting your network services specialist at 1-716-887-2054 or 1-800-666-4627. Further information regarding providers who opt out of Medicare may be obtained from the local Medicare Part B carrier at www.umd.nycpic.com.
Page 13
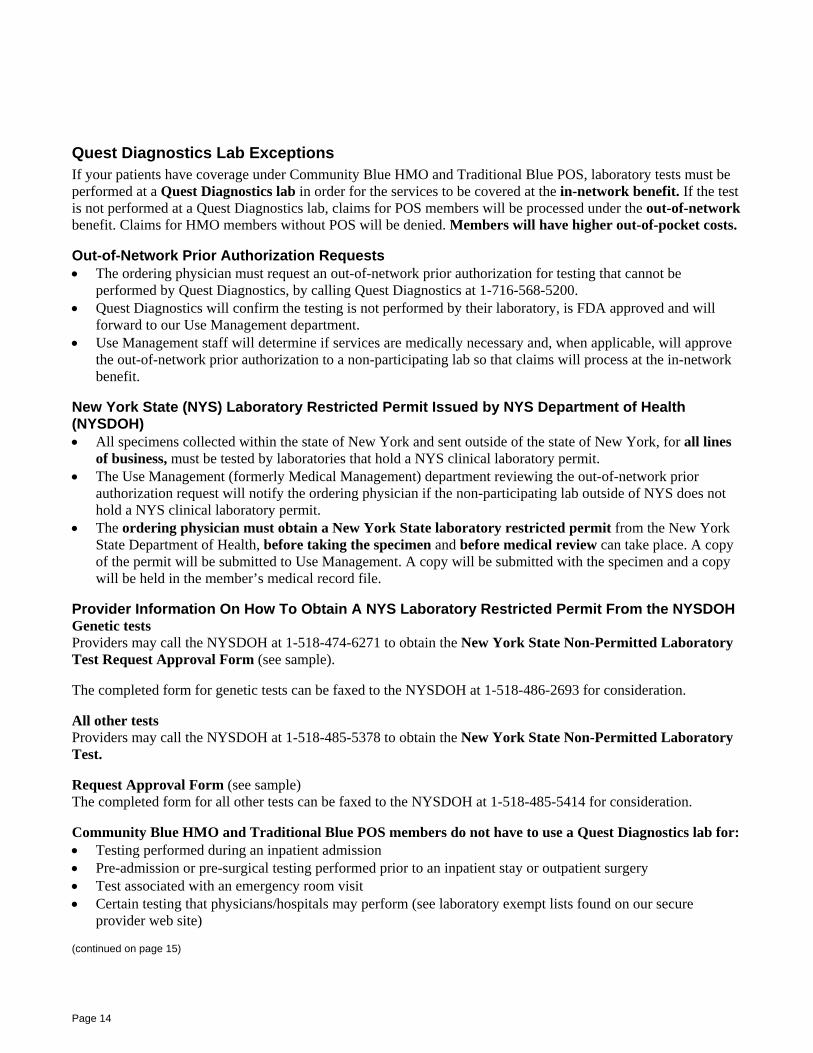
Quest Diagnostics Lab Exceptions If your patients have coverage under Community Blue HMO and Traditional Blue POS, laboratory tests must be performed at a Quest Diagnostics lab in order for the services to be covered at the in-network benefit. If the test is not performed at a Quest Diagnostics lab, claims for POS members will be processed under the out-of-network benefit. Claims for HMO members without POS will be denied. Members will have higher out-of-pocket costs. Out-of-Network Prior Authorization Requests • The ordering physician must request an out-of-network prior authorization for testing that cannot be
performed by Quest Diagnostics, by calling Quest Diagnostics at 1-716-568-5200. • Quest Diagnostics will confirm the testing is not performed by their laboratory, is FDA approved and will
forward to our Use Management department. • Use Management staff will determine if services are medically necessary and, when applicable, will approve
the out-of-network prior authorization to a non-participating lab so that claims will process at the in-network benefit.
New York State (NYS) Laboratory Restricted Permit Issued by NYS Department of Health (NYSDOH) • All specimens collected within the state of New York and sent outside of the state of New York, for all lines
of business, must be tested by laboratories that hold a NYS clinical laboratory permit. • The Use Management (formerly Medical Management) department reviewing the out-of-network prior
authorization request will notify the ordering physician if the non-participating lab outside of NYS does not hold a NYS clinical laboratory permit.
• The ordering physician must obtain a New York State laboratory restricted permit from the New York State Department of Health, before taking the specimen and before medical review can take place. A copy of the permit will be submitted to Use Management. A copy will be submitted with the specimen and a copy will be held in the member’s medical record file.
Provider Information On How To Obtain A NYS Laboratory Restricted Permit From the NYSDOH Genetic tests Providers may call the NYSDOH at 1-518-474-6271 to obtain the New York State Non-Permitted Laboratory Test Request Approval Form (see sample). The completed form for genetic tests can be faxed to the NYSDOH at 1-518-486-2693 for consideration. All other tests Providers may call the NYSDOH at 1-518-485-5378 to obtain the New York State Non-Permitted Laboratory Test. Request Approval Form (see sample) The completed form for all other tests can be faxed to the NYSDOH at 1-518-485-5414 for consideration. Community Blue HMO and Traditional Blue POS members do not have to use a Quest Diagnostics lab for: • Testing performed during an inpatient admission • Pre-admission or pre-surgical testing performed prior to an inpatient stay or outpatient surgery • Test associated with an emergency room visit • Certain testing that physicians/hospitals may perform (see laboratory exempt lists found on our secure
provider web site) (continued on page 15)
Page 14
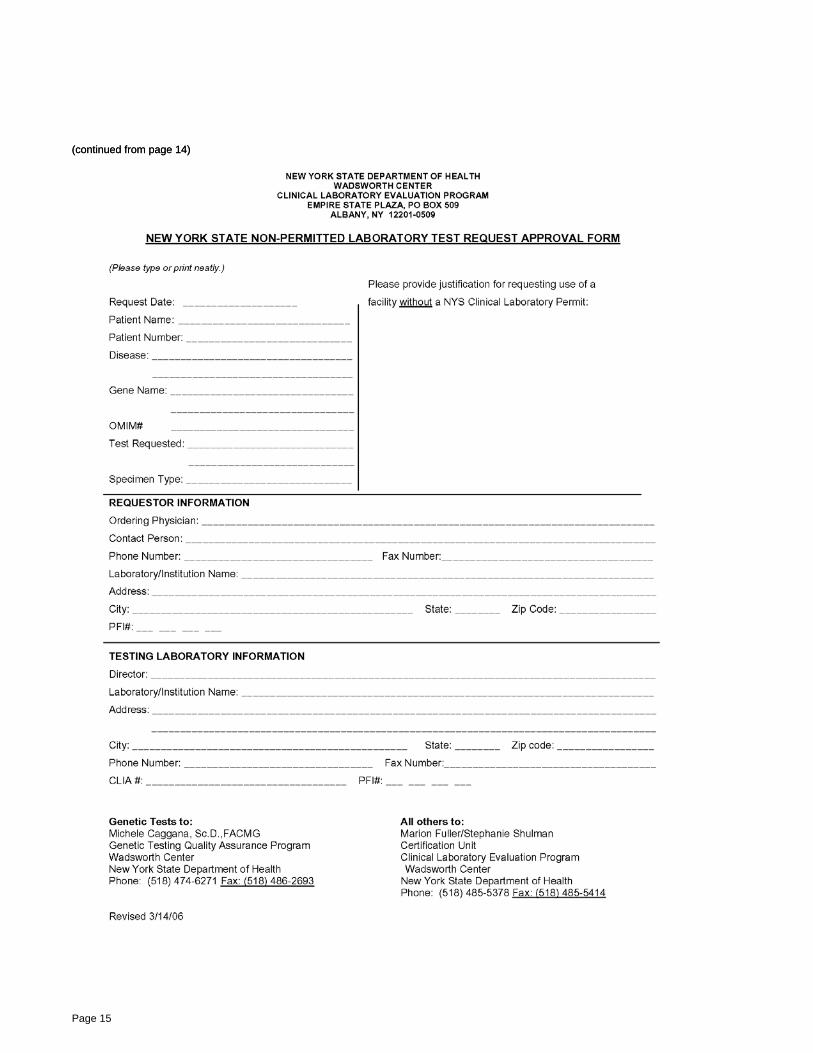
(continued from page 14) (continued from page 14)
Page 15

Medicaid Managed Care and Family Health Plus Members Cannot Be Billed When a provider accepts a Medicaid Managed Care or Family Health Plus member as a patient, the provider agrees to bill the managed care plan for services covered by the contract. The provider is prohibited from requesting any monetary compensation from the recipient, or his/her responsible relative, except for any applicable Family Health Plus copayments. A provider may charge a Medicaid Managed Care or Family Health Plus member only when both parties have agreed prior to the rendering of the service that the recipient is being seen as a private pay patient. This must be a mutual and voluntary agreement. It is suggested that the provider maintain the patient’s signed consent to be treated as private pay in the patient record. The prohibition on charging a Medicaid Managed Care or Family Health Plus member applies when a participating provider fails to submit a claim to the recipient’s managed care plan within the required timeframe. It also applies when a claim is submitted to the recipient’s managed care plan and the claim is denied for reasons other than that the patient was not eligible for coverage on the date of service. A Medicaid Managed Care or Family Health Plus member must not be referred to a collection agency for collection of unpaid medical bills or otherwise billed, except for applicable Family Health Plus copayments, when the provider has accepted the recipient as a Medicaid Managed Care or Family Health Plus patient. Providers may, however, use any legal means to collect applicable unpaid Family Health Plus copayments. If a problem arises with a claim submission, the provider must first contact provider service at 1-877-327-1395. If the managed care plan is unable to resolve an issue because some action must be taken by the recipient’s local department of social services (e.g., investigation of recipient eligibility issues), the provider must contact the local department of social services for resolution. Details can be found online at http://www.health.state.ny.us/health_care/medicaid/program/update/2006/apr2006.htm. For questions regarding Medicaid Managed Care or Family Health Plus, please call the Division of Managed Care and Program Evaluation at 1-518-473-0122. For questions regarding Medicaid fee-for-service, please call the Division of Financial Planning and Policy at 1-518-473-2160.
Page 16
Information on Provider “Gap” Reports As a service to our practitioners, we have been distributing "gap" reports twice a year. The intent of the reports is to aid the practitioner in addressing certain preventive health and condition monitoring standards in their practice. This tool is not tied to any incentive program — it is a communication, based on claims review, which indicates a gap in care and, in some cases, simply a reminder of the potential need for counseling or testing.
The cover letter of the report outlines its purpose and the time periods associated with the report, as well as how the information is gathered.
We received several returned reports with comments on them indicating a lot of time and effort has been spent by you and your office staff. There is no need to reply to these reports. They are simply a tool for your practice to use as you wish.
If there are questions regarding the data provided, please call us at the number listed on the gap report. We have used your comments to refine the reports and modify data gathering strategies to meet the needs of our practitioners.
Member Rights and Responsibilities Our members have certain rights to help protect them and responsibilities that we ask they assume. We encourage all of our participating providers to review these policies. The most current version of our Member's Rights and Responsibilities is available on our provider web site at www.bcbswny.com. Paper copies are available upon request by contacting our Provider Services Department.
Page 17

What’s New? Our Newer, Easier Provider Web Site! In an ongoing effort to provide access to information and resources in a secure and consistent manner, we have improved our provider portal. We want to make it easy for you to find the information you need so that you can make the best decisions for your patients. With this in mind, we are launching an all new provider section of our web site. Please take some time and explore the provider section to familiarize yourself with the new navigation and content layout. When you sign in, you’ll notice we’ve integrated our public and secure sites to ensure a seamless experience. We’re making these changes online to increase the availability of content and promote self-service for you and your office. Updated UM Phone Prompts For your convenience, we have posted an updated Use Management phone menu on our provider web site. The menu is in .pdf format and can be easily printed.
Page 18


Provider Telephone and Web Site Reference Guide
Provider Services 1-800-950-0051 or 1-716-884-3461 (Traditional) 1-800-950-0052 or 1-716-882-2616 (Managed Care) 1-877-327-1395 (Government Programs)
Network Services 1-800-666-4627
Use Management (formerly Medical Management) 1-800-677-3086 or 1-716-884-2942
Health Care Quality Improvement 1-877-878-8785
Web Site www.bcbswny.com