vestibular migraine - university of texas medical branch · • could classic migraine or...
TRANSCRIPT
Vestibular Migraine
Matthew Yantis, MD
Faculty Mentors: Dayton Young, M.D. and
Tamoko Makishima, M.D., Ph.D.
The University of Texas Medical Branch (UTMB Health)
Department of Otolaryngology
Grand Rounds Presentation
May 22, 2013
Objectives
• Demonstrate the relevance of a primarily neurologic
diagnosis for an otolaryngologist
• Provide guidelines from which to conclude that a
patient likely has vestibular migraine
• Provide a differential diagnosis for diseases with
similar symptomatology
Outline
1. Terminology
2. Epidemiology
3. Pathophysiology
4. Symptomatology
5. Testing
6. Differential
7. Treatment
Terminology
• Vestibular Migraine
• Migraine Vestibulopathy
• Migrainous Vertigo
• Migraine Dizziness
• Migraine-Related Vertigo
• Migraine-Associated Vertigo
Entities Distinct from VM
• Basilar Migraine
• Meniere’s Disease
• Benign Paroxysmal Positional Vertigo (BPPV)
• Benign Recurrent Vertigo of Childhood
• Episodic Ataxia (Type 2)
What is VM?
• A manifestation of migraine -- not a distinct entity
• Vestibular center (peripheral or central) disturbed
before, during, or after migraine
Epidemiology
• Migraines
• Prevalence: 10% of population
• 11-17% of women, 4-6% of men
• 20% of women 30-49 years old
• Dizziness (vertigo and non-vestibular)
• 23-29% of population
• By chance (based on above): 3-4% have both symptoms
• Using stricter criteria, vertigo w/ migraine ~ 1% population
Pathophysiology of Migraines
Mostly theoretical
Theories include
• Vasospasm
• Cortical Spreading Depression
• Ion Channel Disorder http://www.youtube.com/watch?v=yZr9Joe85wg
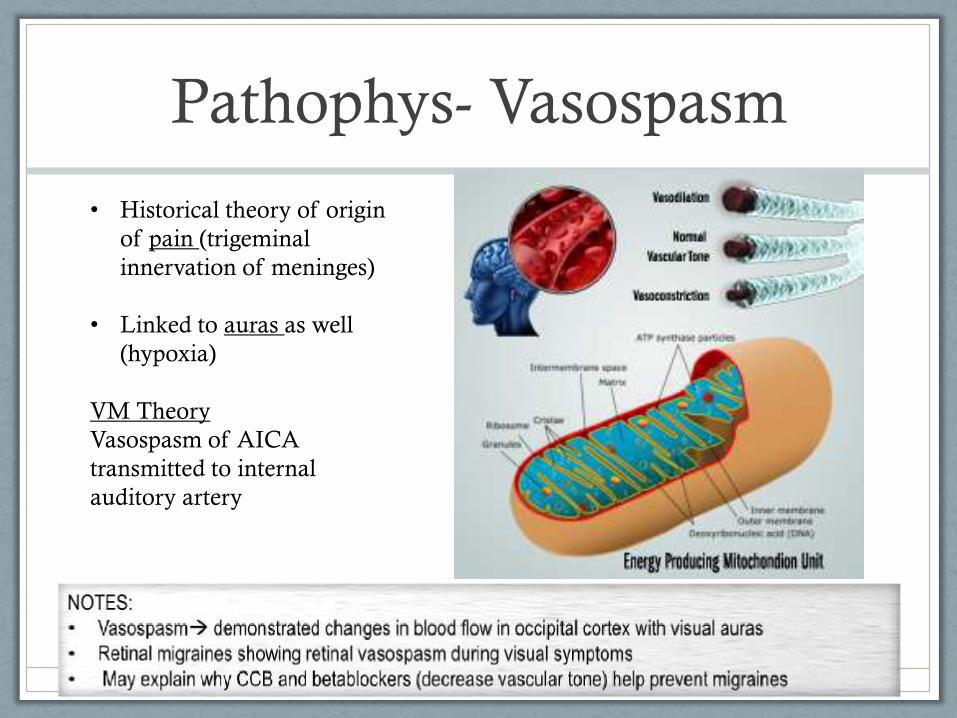
Pathophys- Vasospasm
http://www.migrelief.com/wp-content/uploads/2012/07/Science-Revised.png
• Historical theory of origin
of pain (trigeminal
innervation of meninges)
• Linked to auras as well
(hypoxia)
VM Theory
Vasospasm of AICA
transmitted to internal
auditory artery
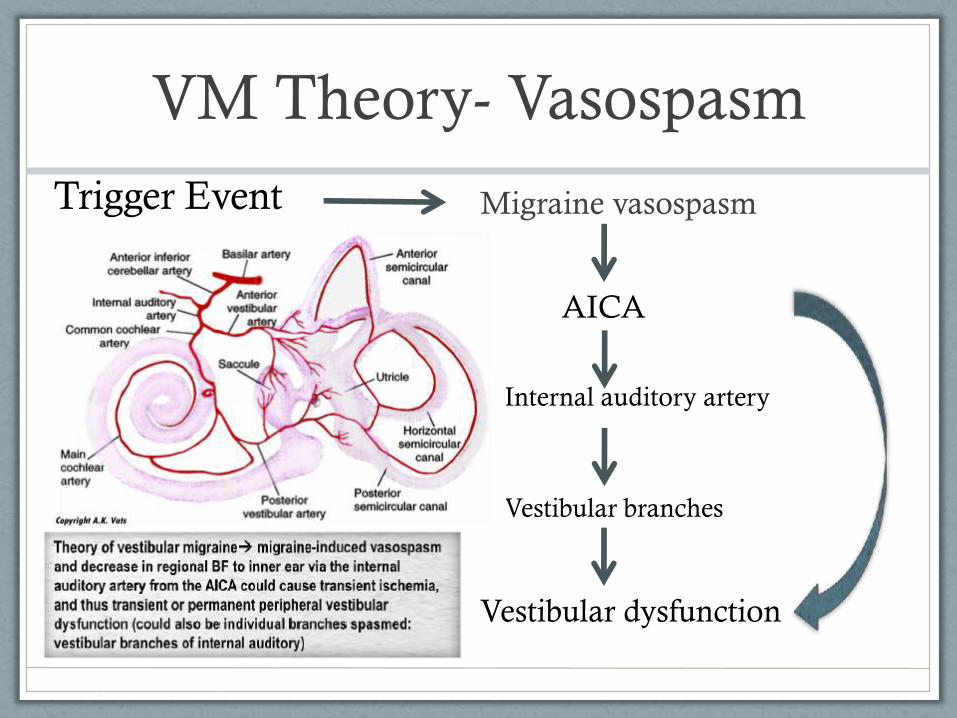
VM Theory- Vasospasm
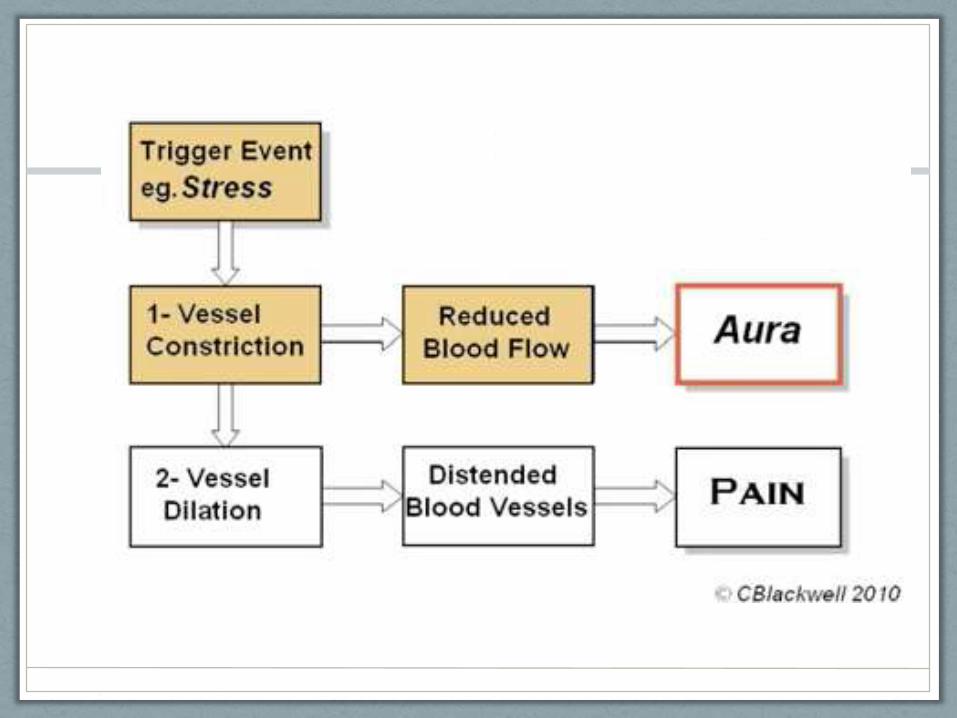
Migraine vasospasm
AICA
Trigger Event
Internal auditory artery
Vestibular branches
Vestibular dysfunction
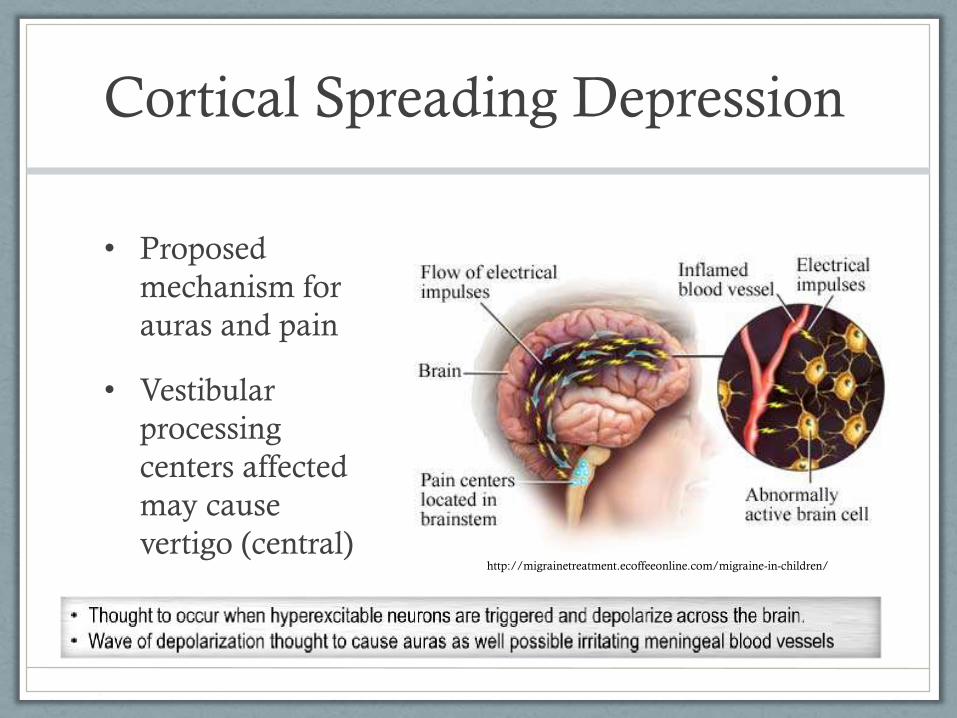
Cortical Spreading Depression
• Proposed
mechanism for
auras and pain
• Vestibular
processing
centers affected
may cause
vertigo (central)
http://migrainetreatment.ecoffeeonline.com/migraine-in-children/
Pathophys: Ion Channels
• Propranolol (BB) , Verapamil (CCB)
• Mutations of CACNA1A (Ca channel)
found in familial hemiplegic migraine
(FHM1) and episodic ataxia type 2 (EA-2)
• Could classic migraine or vestibular migraine have a
defective Calcium channel?
• Link not found yet
What are the symptoms?
Clinical Symptoms
• Vertigo
• Migraine headaches
• Nausea/vomiting/motion sickness
• Photophobia/phonophobia
• Visual or other auras (e.g. scotomas, tingling sensation, auditory hallucinations)
• Tinnitus, temporary hearing loss*
What is “Dizziness”
• Vertigo = sensation of spinning or circular movement
• Oscillopsia
• Light-headedness
• Mental fog/lack of clarity
• Imbalance
• Causes: vestibular, psychogenic, cardiac (orthostatic), CNS origin (TIA), drug related, psychogenic
VM Symptoms- Vertigo
• Duration: seconds to weeks (commonly minutes to hours)
• Most often spontaneous (i.e. non-positional), but can be positional or due
to head motion intolerance *
• Rotational
• May be caused by visual stimuli (car chase scenes, repeating patterns on rugs)
• Definition of giddiness: adj; affected with vertigo, dizzy; Also, frivolous and lighthearted
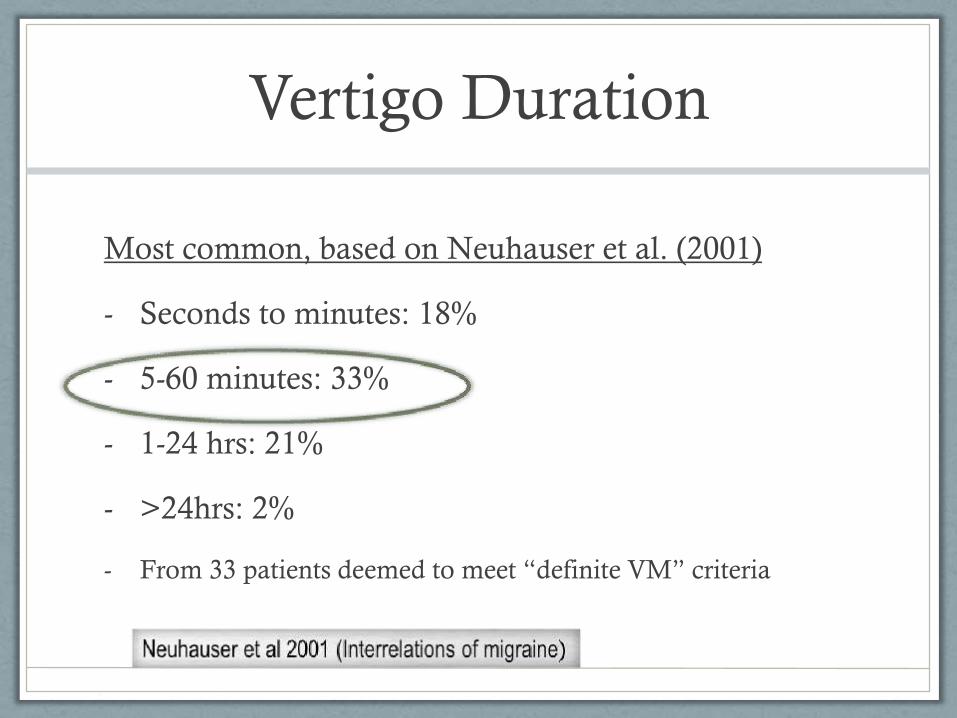
Vertigo Duration
Most common, based on Neuhauser et al. (2001)
- Seconds to minutes: 18%
- 5-60 minutes: 33%
- 1-24 hrs: 21%
- >24hrs: 2%
- From 33 patients deemed to meet “definite VM” criteria
Symptoms
33 patient’s symptoms breakdown during vertigo
• Photophotobia (70%)
• Phonophobia (64%)
• Visual and other aura (36%)
• Headache (94%) 2 patients without headache
• Always HA (45%), Sometimes HA (48%) Neuhauser et al 2001
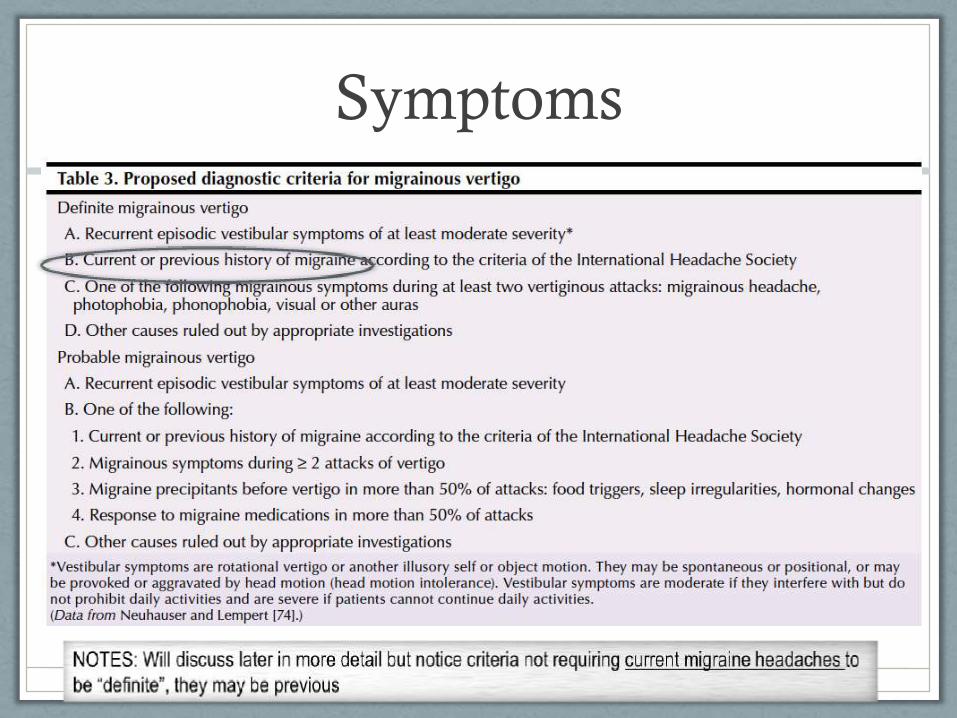
Symptoms
• Picture of Table – Neuhauser and Lempert –
• Eggers 223

What Tests To Run?
Don’t Forget.....
Look in the...
&
Testing
• Specific exam tests: Dix-Hallpike, Vestibulo-ocular reflex, Romberg
• Battery of other tests: audiogram, ABR, VEMP, video-oculography/VNG, water calorics
• Some relevant findings on nystagmography
• MRI when still unsure
• Goal: primarily rule out other
identifiable causes of vertigo
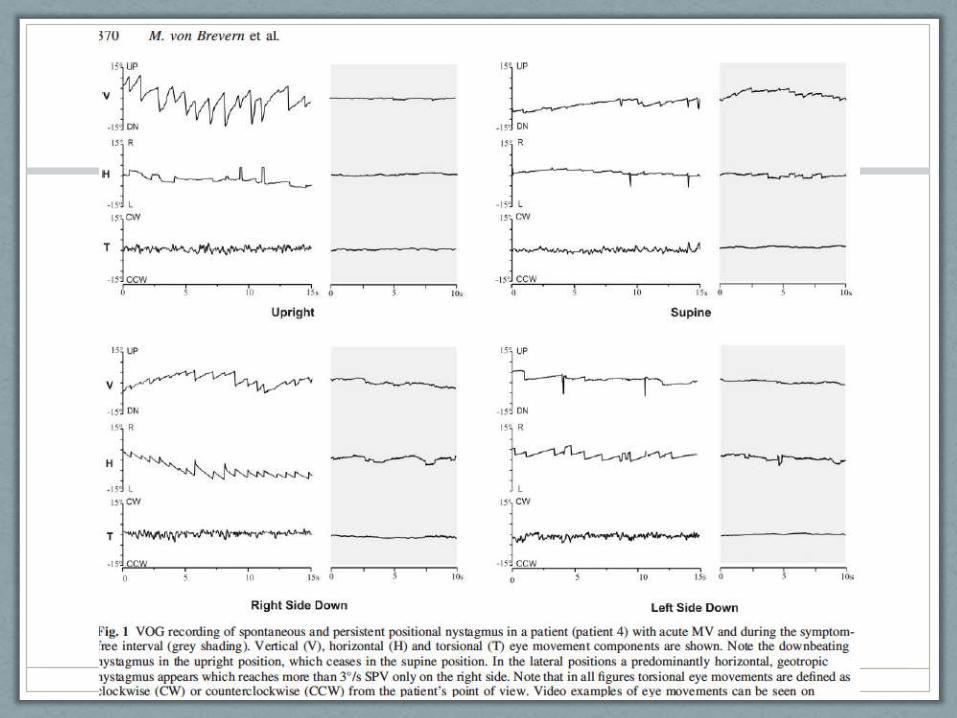
Testing- Nystagmus
Video-oculography of 20 VM patients (von Brevern et. al 2005)
• Found pathological spontaneous and positional nystagmus in 70% of pts during acute VM attack
• Spontaneous (central origin) or positional (peripheral origin)
• 70% also had positive Romberg
*No hearing loss noted
http://work.thaslwanter.at/Projects/Images/Thomas_and_VOG.jpg
http://mozyrko.pl/2009/10/08/eye-tracking-odmiany-rozne-metody-pomiaru/
Diagnosis of VM
• No official agreed upon criteria
• Difficult: no pathognomonic exam signs, no
biomarkers, no lab tests, lots of symptom overlap
• Only diagnostic criteria that includes “vertigo” as a
symptom is the International Headache Society’s
criteria for basilar type migraine
• Important to try to rule out other causes of vertigo
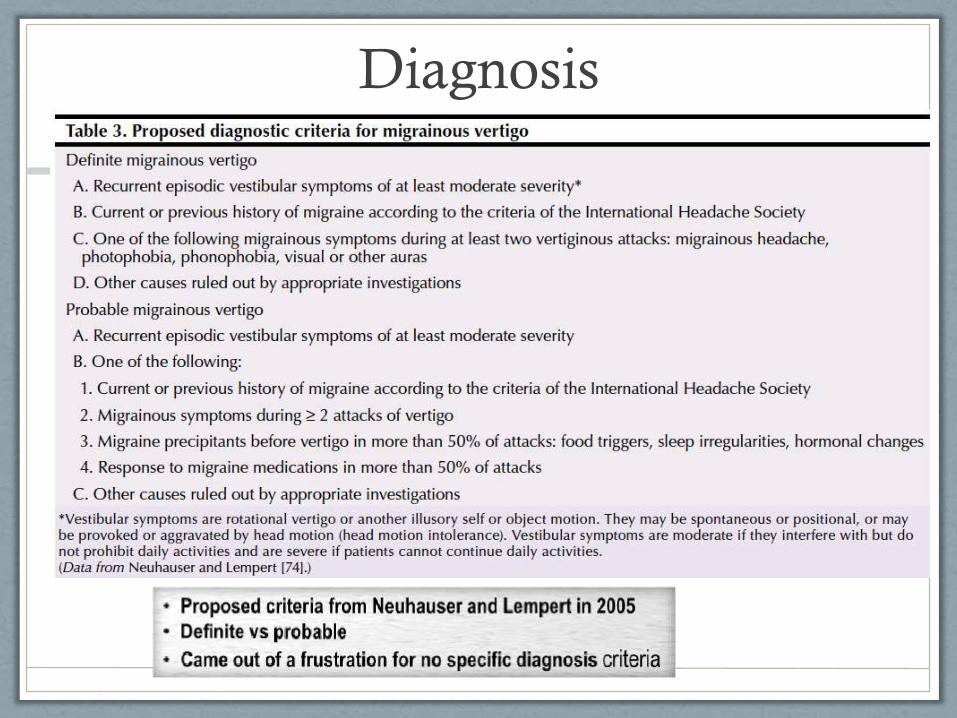
Diagnosis
• Picture of Table – Neuhauser and Lempert –
• Eggers 223
Differential Diagnosis
Basilar migraine
Meniere’s Disease
Benign Paroxysmal Positional Vertigo
And many more!
Basilar migraine
• What it is:
• Subtype of migraine (usually occipital pain)
• Sx’s = vertigo (60%), ataxia, parasthesias, dysarthria
• Why it’s not VM:
• BM diagnosis criteria requires at least two posterior circulation symptoms, lasting 5-60 minutes, and immediately followed by a migraine
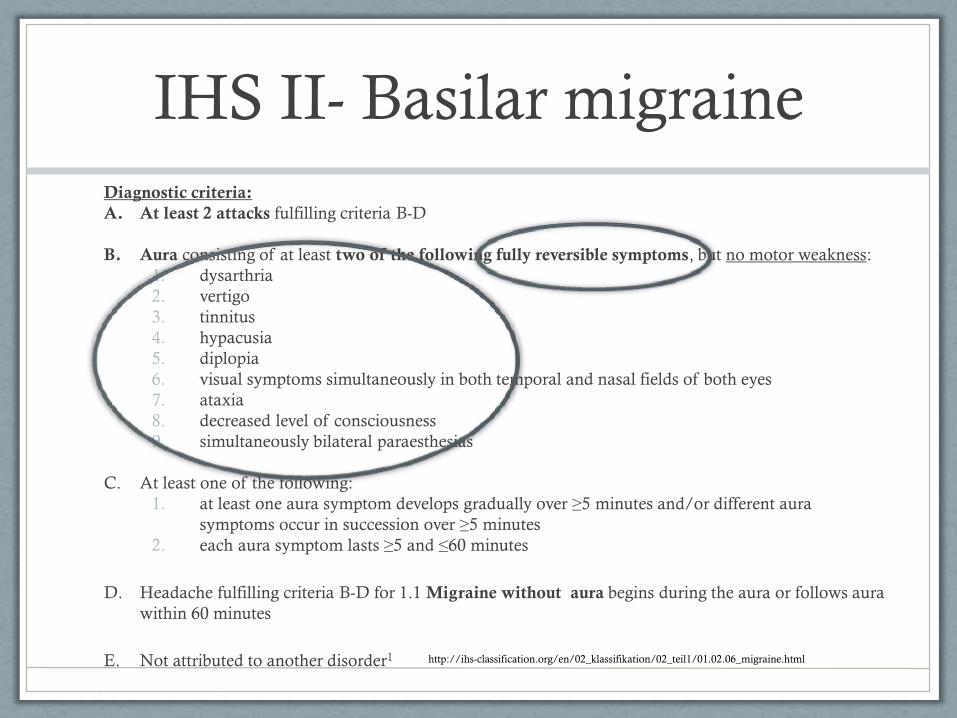
IHS II- Basilar migraine
Diagnostic criteria:
A. At least 2 attacks fulfilling criteria B-D
B. Aura consisting of at least two of the following fully reversible symptoms, but no motor weakness:
1. dysarthria
2. vertigo
3. tinnitus
4. hypacusia
5. diplopia
6. visual symptoms simultaneously in both temporal and nasal fields of both eyes
7. ataxia
8. decreased level of consciousness
9. simultaneously bilateral paraesthesias
C. At least one of the following:
1. at least one aura symptom develops gradually over ≥5 minutes and/or different aura
symptoms occur in succession over ≥5 minutes
2. each aura symptom lasts ≥5 and ≤60 minutes
D. Headache fulfilling criteria B-D for 1.1 Migraine without aura begins during the aura or follows aura
within 60 minutes
E. Not attributed to another disorder1 http://ihs-classification.org/en/02_klassifikation/02_teil1/01.02.06_migraine.html
Meniere’s Disease
• What is it:
• Vertigo episodes lasting 20 min to 24 hrs with often unilateral hearing sx’s including tinnitus and hearing fluctuation/loss (low frequency)
• Why it’s not VM:
• Hearing loss is possible with VM, but typically does not progress to profound.
• Permanence of hearing loss
VM vs Meniere’s: Reality
• Significant overlap, making diagnosis difficult
• Prevelance of migraine in Meniere’s patient
• Migraine symptoms like aura up to 45% Meniere’s
patients experience during vertigo (Radke et al. 2002)
• Lempert et al. (2013) if criteria for Meniere’s met
(audiogram), should diagnose as Meniere’s (not
VM)
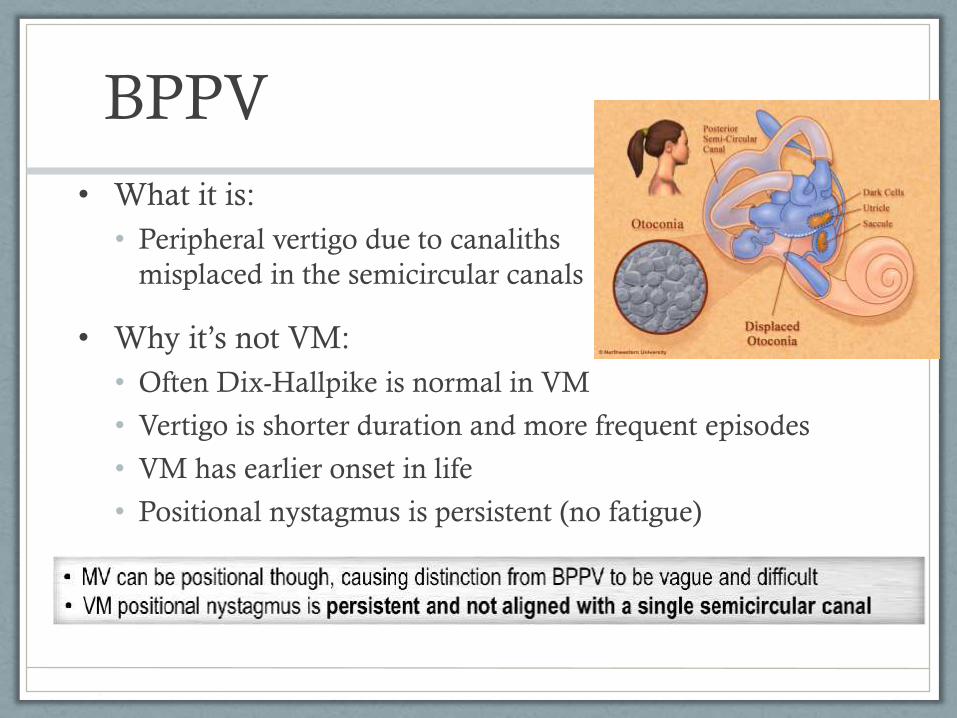
BPPV
• What it is:
• Peripheral vertigo due to canaliths
misplaced in the semicircular canals
• Why it’s not VM:
• Often Dix-Hallpike is normal in VM
• Vertigo is shorter duration and more frequent episodes
• VM has earlier onset in life
• Positional nystagmus is persistent (no fatigue)
How Can We Treat It?
Treatment
• Classic migraine treatment
• Abortive methods
• Prophylaxis
• Symptomatic (e.g N/V)
• Trigger avoidance
• Vestibular migraine-specific treatment
• Physical therapy
• Limited drug trials (zolmitriptan, topiramate)
Treat- Abortive
• Triptans (sumatriptan, rizatriptan)
• Zolmitriptan vs placebo in treating specifically VM in
10 patients inconclusive (Neuhauser et al. 2003)
• Combo pills:
• Fioricet (butalbital, acetaminophen, caffeine)
• Fiorinal (butalbital, aspirin, caffeine)
Treat- Prophylaxis
• Antihypertensives: BB’s (propranolol, metoprolol,
atenolol), CCB’s (verapamil)
• Antidepressants: TCAs (nortriptyline)
• Anticonvulsants: topiramate, lamotrigine
Treat- Symptoms
Nausea--> suppress the vestibular system
• promethazine, ondansetron (antiemetics)
• dimenhydrinate, meclizine (antihistamines)
• benzodiazepines (short course)
• metoclopramide *
Phono/photophobia removal of stimuli
Treat- Triggers
• Avoidance is the key!
• Symptom diary
• Dietary modifications
• Avoid: caffeine, alcohol
• Situational/environmental
• Hormonal: menstrual cycles
• Weather changes
• Lack of sleep, dehydration, stress

Kramer 2013
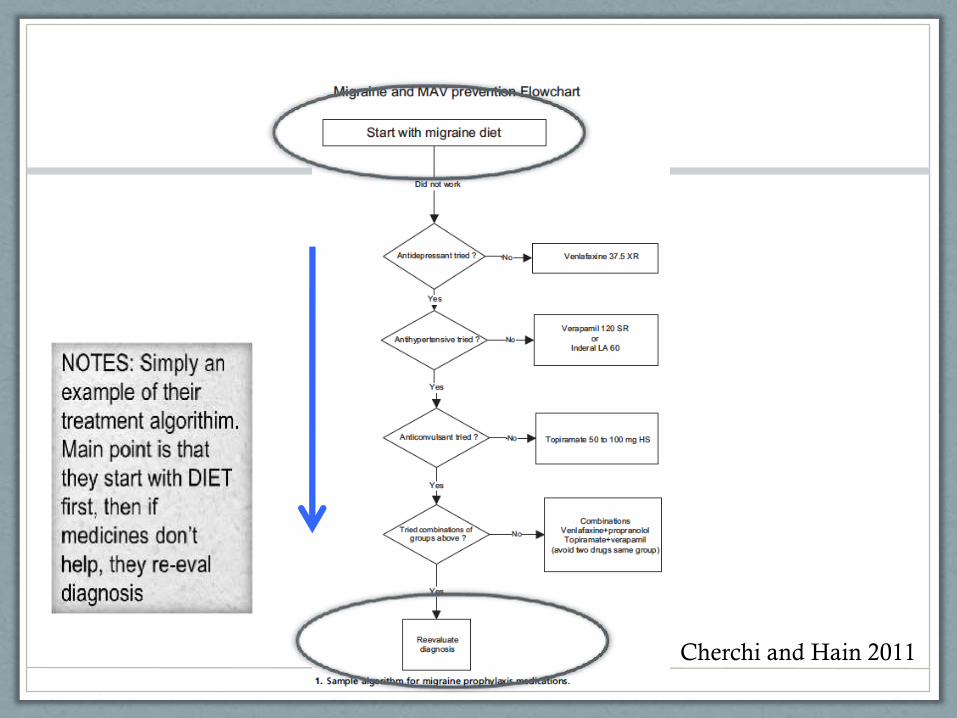
Cherchi and Hain 2011
Treat- Physical Therapy
• Found to be effective specifically for VM
Whitney et al. (2000); retrospective case series of 39 pts
• Initial vestibular functioning testing before rehab
• Treated with vestibular rehab (strength/stretching, habituation,
balance/gait training)
• Completed questionnaires pre- and post treatment (symptom
severity rating 0-100, dizziness handicap inventory, dynamic
gait index, # of falls)
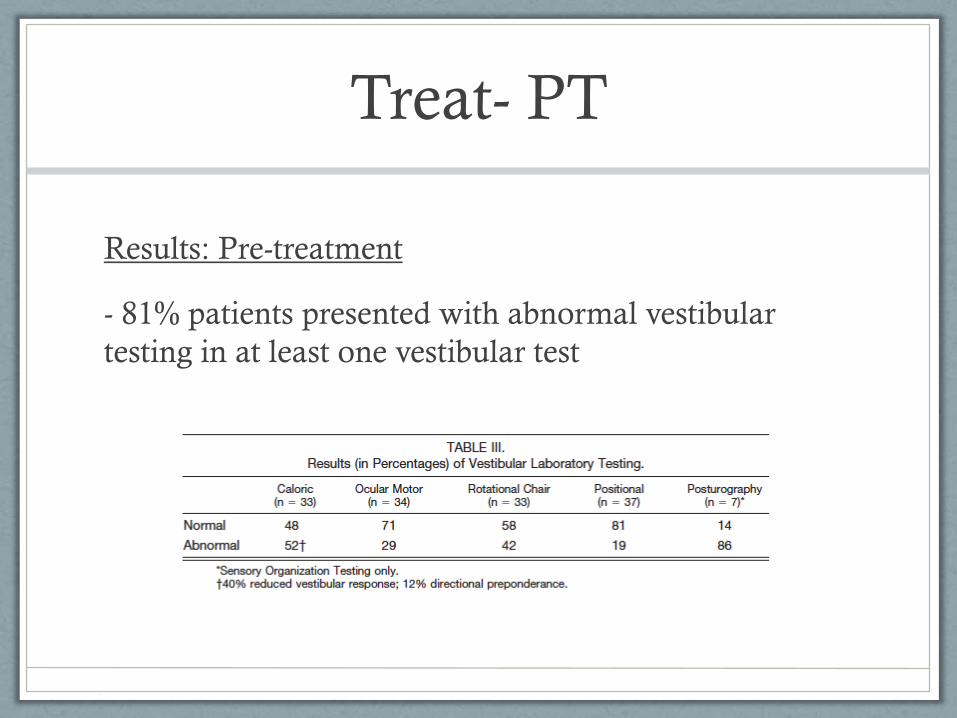
Treat- PT
Results: Pre-treatment
- 81% patients presented with abnormal vestibular
testing in at least one vestibular test
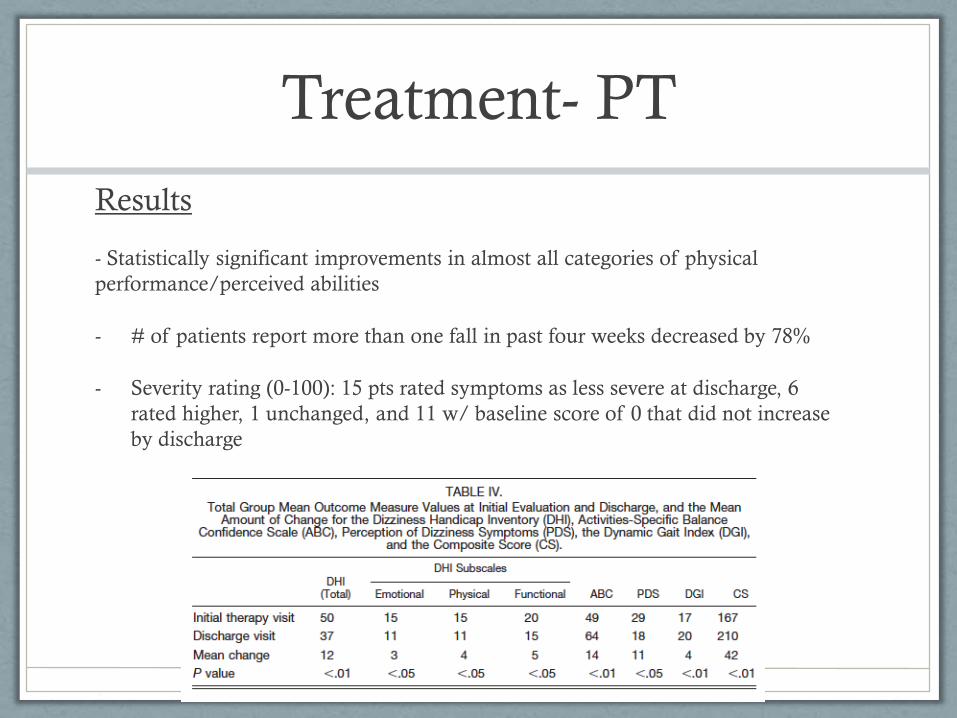
Treatment- PT
Results
- Statistically significant improvements in almost all categories of physical
performance/perceived abilities
- # of patients report more than one fall in past four weeks decreased by 78%
- Severity rating (0-100): 15 pts rated symptoms as less severe at discharge, 6
rated higher, 1 unchanged, and 11 w/ baseline score of 0 that did not increase
by discharge
Treatment- PT
Conclusion
- Offer vestibular rehab to patients with VM
- 35/39 patient had improved scores
Summary- VM
• Common manifestation of migraine and common
cause of vertigo
• Still not well defined as a specific disease process
• No consensus on diagnosis
• Treatment mostly for migraine (triggers, abortive
and prophylactic meds, physical therapy)
What Happens Next
• Need accepted diagnostic criteria
• Will require better pathophys understanding
• 2014 criteria for VM supposed to be published in the
IHS’s International Classification of Headache
Disorders
• Without better understanding of disease, may be
inappropriate to establish criteria to diagnose as a
stand-alone disease process
http://www.migraine-aura.org/content/e24966/e22874/e23697/index_en.html
Bibliography
• Baloh. Neurotology of migraine. Headache 37:615-621, 2002.
• Brackman, Shelton, Arriaga: Otologic Surgery 3rd edition.
• Brevern et al. Acute migrainous vertigo: clinical and oculographic findings. Brain 128:365-374, 2005.
• Cha et al. Migraine associated vertigo. Journal of Clinical Neurology 3:121-126, 2007.
• Cherchi and Hain. Migraine-associated vertigo. Otolaryngology Clinic Of North America 44:367-375,
2011.
• Cherian. Vertigo as a migraine phenomenon. Curr Neurol Neurosci Rep 13:343-349, 2013.
• Cohen et al. Migraine and Vestibular Symptoms—Identifying ClinicalFeatures That Predict “Vestibular
Migraine”. Headache 51:1393-1397, 2011.
• Eggers. Migraine-related vertigo: diagnosis and treatment. Current Pain and Headache Reports 11:217-
226, 2007.
• Glasscock-Shambaugh: Surgery of The Ear
• IHS Webite http://ihsclassification.org/en/02_klassifikation/02_teil1/01.02.06_migraine.html
• Lempert and Neuhauser. Migrainous vertigo. Neurol Clin 23:715-730, 2005.
• Lempert et al. Vestibular migraine: Diagnostic criteria. Journal of Vestibular Research 2012; 22: 167-172
• Neuhauser H, Leopold M, von Brevern M, et al. The interrelations of migraine, vertigo, and migrainous
vertigo. Neurology 2001; 56(4):436-41
• Peter Weber: Vertigo and disequilibrium: A practical guide to diagnosis and management
• Porta-etessam et al. Neuro-otological symptoms in patients with migraine. Neurologia 26:100-104, 2011.
• Thomas Brandt: Vertigo and Dizziness: Common complaints
• Whitney et al. Physical therapy for migraine-related vestibulopathy and vestibular dysfunction with
history of migraine. Laryngoscope 110:1528- 1534, 2000.