ventilator setup and management for suspected and
TRANSCRIPT

Guideline No:
Guideline:
Disclaimer This document is available on-line as a stimulus for interchange of knowledge and ideas in the field of Neonatal and
Paediatric Retrieval. It is provided "as-is" and without support or warranty of any kind. Many of our guidelines may not be appropriate for use in retrieval settings other than NETS NSW, especially in non-Australian environments.
This document reflects what is currently regarded as safe practice. However, as in any clinical situation, there may be
factors which cannot be covered by a single set of guidelines. This document does not replace the need for the
application of clinical judgement to each individual presentation.
Approved by: SCHN Policy, Procedure and Guideline
Committee
Date Effective: Review Period: 3 years
Team Leader: Area/Dept: NETS
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 1 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
VENTILATOR SETUP AND MANAGEMENT FOR
SUSPECTED AND CONFIRMED COVID-19
PATIENTS
PRACTICE GUIDELINE ©
DOCUMENT SUMMARY/KEY POINTS
In suspected or confirmed COVID- 19 patients:
Use of a closed suction system must be used for all intubated patients
Bacterial/Viral filters must be added to all ventilation circuits except in the first 14 days of
life in neonates born to women with COVID-19 or risk factors for COVID-19
Bacterial/Viral filters must be attached to emergency bag-mask equipment except in
neonates ≤ 14 days of life.
PPE for airborne precautions must be worn during aerosol generating procedures
(AGPs)
Avoid disconnection of the ventilation circuit once connected to the patient Only in an emergency should manual ventilation be performed Only in an emergency should open suction be performed
Avoid aerosol generating procedures, i.e. ventilator circuit disconnection, open
suctioning, nebulization (unless it is nebulization via the Aerogen)
Includes process for safe sequence of surfactant administration if required
CHANGE SUMMARY

Guideline No:
Guideline:
Disclaimer This document is available on-line as a stimulus for interchange of knowledge and ideas in the field of Neonatal and
Paediatric Retrieval. It is provided "as-is" and without support or warranty of any kind. Many of our guidelines may not be appropriate for use in retrieval settings other than NETS NSW, especially in non-Australian environments.
This document reflects what is currently regarded as safe practice. However, as in any clinical situation, there may be
factors which cannot be covered by a single set of guidelines. This document does not replace the need for the
application of clinical judgement to each individual presentation.
Approved by: SCHN Policy, Procedure and Guideline
Committee
Date Effective: Review Period: 3 years
Team Leader: Area/Dept: NETS
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 2 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
This is a new guideline
READ ACKNOWLEDGEMENT
NETS clinical staff are to read and acknowledge they understand the contents of this
guideline.

Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 3 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
Preparation for ventilation circuit setup
Appropriate PPE
COVID-19 pack (Neonatal or Paediatric) in retrieval bag (see attachment 1 for content list)
Only take the items you require from the retrieval bag to the patient area
To minimise contamination of the COVID-19 pack and retrieval bags, avoid taking into the patient care area. If this is unavoidable, keep bags at least 2 meters away from the patient
Only a clean person to access retrieval bags
Do not discard unused items from COVID-19 pack – return into retrieval bag
Equipment Required
1. Appropriate sized inline suction system
Ambu Cath closed system suction catheter (with elbow – sizes ≥FG7) - see picture 1
OR
Ambu Cath closed system suction catheter (without elbow – FG6) and Air Life Neo-Verso Airways Access Adaptor® (Y-adapter) - see picture 2
Picture 1
Picture 2

Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 4 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
OR
Halyard closed suction system (with elbow – all sizes) – see picture 3
2. 2x Bact-Trap™ filter (wet circuits) OR 1x green HME (dry circuit). No
Bact-Trap™ filter at ETT end of circuit in neonates ≤ 14 days of life
3. 1x Bact-Trap™ or HME filter for bagging circuit except in neonates
aged ≤ 14 days
4. ETCO2 sampling line
5. Appropriate ventilation circuit
6. ETT clamp
Setting Up
Prepare ventilator and circuit before entering patient area:
Set up ventilator and perform leak test
Set ventilation parameters and confirm with test lung - anticipate
higher pressures, longer inspiratory times and appropriate breath rate
for I:E ratio, to account for large dead space
Activate standby/turn off ventilator and cover inline suction with clean
glove or plastic bag until ready to attach to patient
Leave test lung in the retrieval bag to remain clean
Ensure ETCO2 monitor is turned on prior to intubation
Picture 3
Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 5 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
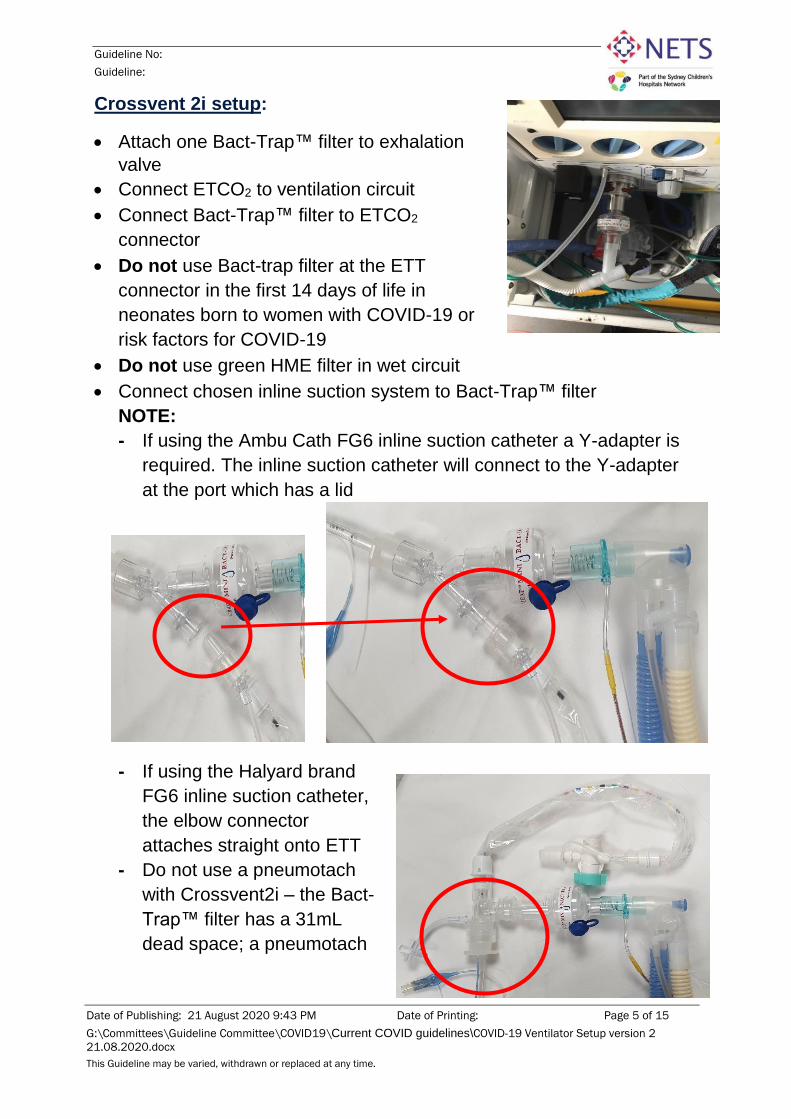
Crossvent 2i setup:
Attach one Bact-Trap™ filter to exhalation
valve
Connect ETCO2 to ventilation circuit
Connect Bact-Trap™ filter to ETCO2
connector
Do not use Bact-trap filter at the ETT
connector in the first 14 days of life in
neonates born to women with COVID-19 or
risk factors for COVID-19
Do not use green HME filter in wet circuit
Connect chosen inline suction system to Bact-Trap™ filter
NOTE:
- If using the Ambu Cath FG6 inline suction catheter a Y-adapter is
required. The inline suction catheter will connect to the Y-adapter
at the port which has a lid
- If using the Halyard brand
FG6 inline suction catheter,
the elbow connector
attaches straight onto ETT
- Do not use a pneumotach
with Crossvent2i – the Bact-
Trap™ filter has a 31mL
dead space; a pneumotach

Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 6 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
will increase dead space further
- Without the pneumotach, only CMV mode can be used with the
Crossvent 2i ventilator
Hamilton-T1 ventilator setup:
Attach one Bact-Trap™ filter to exhalation housing
Attach a bacterial/viral filter to pre-humidification tubing, as per usual practice (use the clear filter provided with adult circuit or Bact-Trap™ filter or HME filter)
Connect ETCO2 to ventilation
circuit/flow sensor
Connect Bact-Trap™ filter to ETCO2
connector (Do not use green HME
filter in wet circuit)
Connect chosen inline suction system to Bact-Trap™ filter
Inline Suction set up with Y-adaptor Inline Suction set up with elbow

Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 7 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
Oxylog ventilator setup:
The Oxylog 3000+ ventilator has a single limb dry circuit
Connect ETCO2 to ventilation circuit
Attach appropriate sized green viral/bacterial HME to ETCO2
connector
NOTE:
- Cannot use a Bact-Trap™ filter
as it is not a HME and does not
provide any passive
humidification
- Only one viral filter that also
provides passive humidification
is required for the Oxylog
ventilator. If you need to
remove/replace an
additional/incorrect filter, clamp
ETT before breaking the closed
circuit
Attach appropriate size Inline
suction system to HME

Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 8 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
Connecting to patient
1. The ideal situation is a successful first attempt intubation, connecting
straight onto the ventilator circuit without giving manual breaths
If attaching ventilator setup immediately after intubation, ETT
clamping is not required
Following successful intubation attach the ventilator circuit setup
to the patient ETT and start mechanical ventilation
Confirm ETT position looking for chest rise, ETCO2 waveform,
misting of the ETT and auscultation
2. If the patient has needed emergency bagging immediately after
intubation, the following sequence needs to be performed to connect
onto the NETS ventilator circuit:
Cease giving breaths and give PEEP only
Clamp ETT to maintain PEEP and minimise exhaled volumes
Turn off gas flow to the bagging circuit, this may be achieved
simultaneously with ETT clamping
Disconnect the bagging circuit and filter
Connect ventilator circuit setup to ETT from the inline suction
Unclamp ETT
Start ventilator

Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 9 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
Managing ventilation disconnections
Transition to receiving hospital ventilator:
For a successful and risk-free transition, the NETS team should always
be leading the discussion for disconnection and connection onto the
receiving ventilator
Complete clinical handover to the receiving team
Transfer patient to receiving bed as per NETS General Retrieval
Guidelines
Ensure receiving ventilator circuit is ready:
- The receiving team may be happy to keep the NETS inline
suction and filter in place, OR
- The receiving team may want to connect their own inline
suction and filter
NETS team to perform the disconnection and connection sequence:
1. Turn off NETS ventilator at the end of expiration
2. Clamp ETT
3. Disconnect NETS circuit from the pre-determined connection point
- Either at the ETT connector, thus removing NETS inline
suction and filter, OR
- At the filter, thus leaving the inline suction and filter still
connected to the patient ETT
4. Connect the receiving ventilator circuit setup
5. Unclamp ETT
6. Start receiving ventilator
Emergency bagging during mechanical ventilation:
Manual ventilation should be avoided wherever possible. However, if
emergency bagging is required:
1. Activate ventilator stand-by at the end of expiration to stop gas flow
2. Clamp ETT
3. Disconnect only the ventilator circuit from the ETCO2 connector,
leaving the inline suction, filter and ETCO2 attached to patient ETT

Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 10 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
4. Attach only the bagging system
onto ETCO2 connector (there
should be only 1 filter in the
system)
5. Unclamp ETT
6. Turn on gas flow to bagging
system
When ready to recommence mechanical ventilation: 1. Cease giving breaths and give PEEP only
2. Clamp ETT to maintain PEEP and minimise exhaled volumes
3. Turn off gas flow to the bagging system, this may be achieved
simultaneously with ETT clamping
4. Disconnect the bagging circuit from the ETCO2 connector
5. Connect ventilator circuit to ETCO2 connector
6. Unclamp ETT
7. Restart ventilator
Emergency bag-mask ventilation:
If emergency bag-mask ventilation is required,
there should always be a viral/bacterial filter
attached between the bagging system and mask
except in the first 14 days of life in a neonate.
In infants, use HME filters with the smallest
possible dead space at the bagging system
interface. Small HME filters are included in the
neonatal COVID-19 pack
A 2-hand technique should be used to ensure a
tight seal over the patient nose and mouth, with
another team member giving manual breaths

Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 11 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
Surfactant Administration
Prepare surfactant as per NETS Surfactant Administration policy
Surfactant administration needs to occur with minimal risk of AGPs –
avoid manual ventilation if possible
Remember to treat the baby normally however if truly suspicious of, or
with confirmed vertical transmission of COVID-19, have a low
threshold to add muscle relaxation to prevent the baby coughing and
therefore aerosolizing when surfactant is administered
Place a clear sterile drape over the baby head for secretion control
during administration
Use any one of the situations below as guidance:
Administration immediately after intubation:
- If the patient is stable enough, the surfactant may be given as one
aliquot immediately after intubation prior to connecting to the
ventilation circuit and commencing initial mechanical ventilation
- Consider higher pressures and longer iTime may be required
initially given the extra dead space with inline suctioning.
Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 12 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
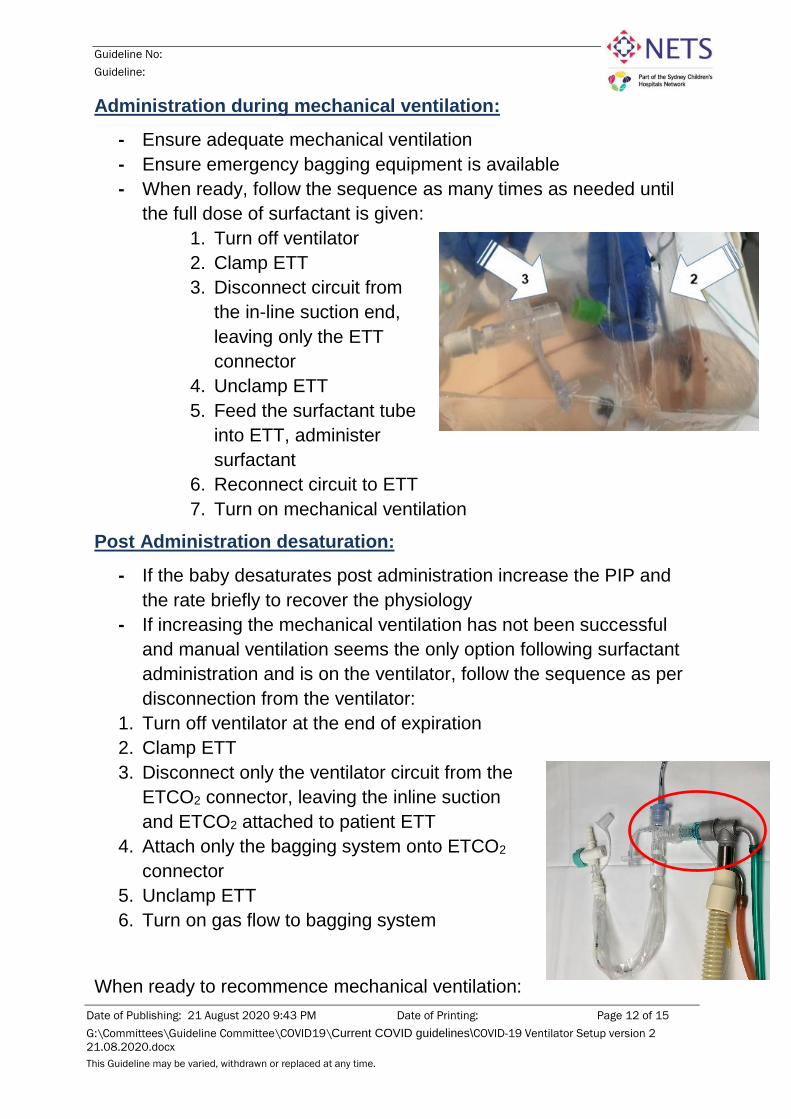
Administration during mechanical ventilation:
- Ensure adequate mechanical ventilation
- Ensure emergency bagging equipment is available
- When ready, follow the sequence as many times as needed until
the full dose of surfactant is given:
1. Turn off ventilator
2. Clamp ETT
3. Disconnect circuit from
the in-line suction end,
leaving only the ETT
connector
4. Unclamp ETT
5. Feed the surfactant tube
into ETT, administer
surfactant
6. Reconnect circuit to ETT
7. Turn on mechanical ventilation
Post Administration desaturation:
- If the baby desaturates post administration increase the PIP and
the rate briefly to recover the physiology
- If increasing the mechanical ventilation has not been successful
and manual ventilation seems the only option following surfactant
administration and is on the ventilator, follow the sequence as per
disconnection from the ventilator:
1. Turn off ventilator at the end of expiration
2. Clamp ETT
3. Disconnect only the ventilator circuit from the
ETCO2 connector, leaving the inline suction
and ETCO2 attached to patient ETT
4. Attach only the bagging system onto ETCO2
connector
5. Unclamp ETT
6. Turn on gas flow to bagging system
When ready to recommence mechanical ventilation:

Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 13 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
1. Cease giving breaths and give PEEP only
2. Clamp ETT to maintain PEEP and minimise exhaled volumes
3. Turn off gas flow to the bagging system, this may be achieved
simultaneously with ETT clamping
4. Disconnect the bagging circuit from the ETCO2 connector
5. Connect ventilator circuit to ETCO2 connector
6. Unclamp ETT
7. Restart ventilator
Trouble shooting
ETCO2 readings will be unreliable due to the large dead space in the ventilation circuit setup – use for ETT placement and trends in increasing or decreasing CO2
Anticipate the need for higher pressures, longer inspiratory times and appropriate I:E ratios to overcome dead space
Assess patient for ventilator asynchrony – have low tolerance for appropriate levels of sedation and muscle relaxation
Change Bact-Trap™/HME if excessively wet (viral filtration is not guaranteed when wet)
When changing between ventilator and manual circuits, there should only be one viral/bacterial filter at the patient interface – more than one filter will increase the dead space significantly. The exception to this is with the neonate aged 14 days and under.
References
1. Agency for Clinical Innovation (2020). Aerosol generating respiratory therapies.
2. AMPA (2020). AMPA Position Statement. https://www.ampa.org/
3. Australian and New Zealand Intensive Care Society (2020). ANZICS COVID-19 Guidelines. Version 1. Melbourne: ANZICS https://www.anzics.com.au/wp-content/uploads/2020/03/ANZICS-COVID-19-Guidelines-Version-1.pdf
4. Australian Government Department of Health (2020).Information for aeromedical retrieval of patients with COVID-19 https://www.health.gov.au/sites/default/files/documents/2020/03/coronavirus-covid-19-information-for-aeromedical-retrieval-of-patients.pdf
5. Brewster D, Chrimes N, Do T, Fraser K, Groombridge C, Higgs A, Humar M, Leeuwenburg T, McGloughlin S, Newman F, Nickson C, Rehak A, Vokes D and Gatward J (2020). Consensus statement: Safe Airway Society principles of airway management and tracheal intubation specific to the COVID-19 adult patient group. The Medical Journal of Australia.

Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 14 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
https://www.mja.com.au/journal/2020/212/10/consensus-statement-safe-airway-society-principles-airway-management-and
6. Clinical excellence commission (2020). Infection prevention and control practise handbook. http://www.cec.health.nsw.gov.au/__data/assets/pdf_file/0010/383239/IPC-Practice-Handbook-2020.PDF
7. Clinical excellence commissions (2020). Infection Prevention and Control Novel Coronavirus 2019 (2019-nCoV) – Hospital setting https://intranet.schn.health.nsw.gov.au/files/attachments/7714/infection-control-ncov-2019-hospital-setting-v2.pdf
8. Medtronic (2019). Effective humidification. Effective protection. DAR™ filter HMEs. https://www.medtronic.com/content/dam/covidien/library/us/en/product/ventilator-filters/dar-breathing-filter-hme-sellsheet.pdf
9. NSW Ambulance (2020). Clinical Practice standard – Aeromedical operations AO.CLI.23- Novel Coronaviruseshttps://nswhems.files.wordpress.com/2020/03/ao.cli_.23-novel-coronaviruses-approved-by-aed-11-03-2020.pdf
10. SCHN (2015). Airway suction in PICU-CHW Practice Guideline. http://webapps.schn.health.nsw.gov.au/epolicy/policy/1934/download
11. SCHN (2019). Respiratory support in neonates – GCNC – CHW. Practice Guideline http://webapps.schn.health.nsw.gov.au/epolicy/policy/4507/download
12. Matava CT et al (2020) Pediatric airway management in COVID-19 patients- Consensus guidelines from the Society for Pediatric Anaesthesia’s Pediatric Difficult Intubation Collaborative and the Canadian Pediatric Anaesthesia Society. Anesth Analg DOI:10.1213/ANE.00000000000004872 Accessed via https://www.schn.health.nsw.gov.au/files/attachments/matava-pediatric_airway_managemen-anesth_analg.pdf
13. NSW Government. Clinical Excellence Commission (25Jun2020). Safety Notice 006/20. Use of Viral filters for respiratory care in neonates.
14. Shalish W, Lakshminrusimha S et al. (2 May 2020). COVID-19 and neonatal respiratory care: current evidence and practical approach. Am J Perinatol. doi:10.1055/s-0040-1710522.
15. Terheggen U, Heiring C, Kjellberg M, et al. European consensus recommendations for neonatal and paediatric retrievals of positive or suspected COVID-19 patients [published online ahead of print, 2020 Jul 7]. Pediatr Res. 2020;10.1038/s41390-020-1050-z. doi:10.1038/s41390-020-1050-z
Attachment:

Guideline No:
Guideline:
Date of Publishing: 21 August 2020 9:43 PM Date of Printing: Page 15 of 15
G:\Committees\Guideline Committee\COVID19\Current COVID guidelines\COVID-19 Ventilator Setup version 2
21.08.2020.docx
This Guideline may be varied, withdrawn or replaced at any time.
COVID-19 Packs - List of Contents
Copyright notice and disclaimer
The use of this document outside Sydney Children's Hospitals Network (SCHN), or its reproduction in whole or in part, is subject to acknowledgement that it is the property of SCHN. SCHN has done everything practicable to make this document accurate, up-to-date and in accordance with accepted legislation and standards at the date of publication. SCHN is not responsible for consequences arising from the use of this document outside SCHN. A current version of this document is only available electronically from the Hospitals. If this document is printed, it is only valid to the date of printing.