venous diseases zsolt pécsvárady [email protected] pécs
TRANSCRIPT


VV. saphaena maga. saphaena magaVV. saphaena parva. saphaena parva
Main Main perforaperforatorstors
Deep veinsDeep veins

I. Superficial thrombophlebitis
II. Deep venous thrombosis and pulmonal embolisation
III. Chronic venous insufficiency CVI

- Varicophlebitis / -thrombosis- Septic thrombophlebitis- Catether phlebitis- Flebitis migrans: Unknown origin in different location. Together with cancer, autoimmun or Buerger diseases.- Mondor disease: Unknown origin with spontaneous healing. associate with pancreas diseases.
I. Superficial thrombophlebitis
Hard, palpable veins. As these veins are not not flexible: stretching is painful
It is a painful but not dangerous disease with quick recovery.

II. Sign and symptoms of deep venous thrombosis
- Oedema of dependent leg- Pain- Cyanosis- Shining skin- Superficial collateral veins- Acut developement of the symptoms- Pain to press of deep veins, muscles around them- „Cord” feeling of thrombotic vein- Dorsalflexion of calf can cause pain in the gastrocnemic muscles ( Homans-sign ) - Inflate of the BP meter (on both calves) can cause pain in the dependent leg (Lowenberg jel)

Probability of DVT based on medical history and physical exmination
Clinical condition Score • active cancer 1 • plegia, plaster in the near past 1 • immobility or maior operation in the near past 1 • pressure sensitivity in the location of deep veins 1 • swelling of the whole leg 1 • >3 cm difference between the diameter of calves 1 • oedema 1 • collateral superficial veins 1 probability of other diagnosis -2
High probability >3; medium probability 1-2; Low probability 0
(Wels és munkatársai Lancet 1997; 350-1795)

Non invasive diagnosis of DVT
CUS= compression ultrasound test
Negative predictive value for proximal DVT is 98%
for distal DVT is just 40%
Low probability medium probability high probability 3-10% 15-30% >70% CUS negativ CUS negativ -D-dimer + D-dimer + D-dimer DVT can exclude DVT p value 3-5% DVT p value 20-30% without CUS
repeat CUS repeat CUS

Risk factors for DVT I.
• major orthopedic surgery ( hip, knee )
• malignant disease
• trauma, postoperative condition
• DVT or PE in medical history
• immobilization
• heart attack, heart failure
• stroke or paralysis
• infections, sepsis

Risk factors for DVT II.
• Age older than 40 yrs
• Obesity
• Varicositas
• Oral contraceptive, oestrogen treatment, gravidity
• Thrombophylia
APC resistency, Protein C and S, antithrombin III. insufficiency.
fibrin és plasminogen disturbances, myeloproliferatíve diseases
• Other serious diseases ( heart, lung, inflammatory bowel disease etc. )

III. Chronic venous insufficiency
C V I

Etiology of Primary Insufficiency
Heredity: most important risk factor
„ Varicose veins are the result of poorly selecting one’s grandparents” Sir William Osler MD

Epidemiology of CVI
- Varicositas in Europe: 25,2%
- CVI in Europe: 1,7 %
- Venous ulcer: 1 %

CVICVI = v = venous hypertensionenous hypertension
Causes:- reflux ( insufficiency of valves )- occlusion ( thrombosis )- disturbed lymphatic circulation- disturbed muscle pump function


Physiology of Venous Return
PumpCalf muscles provide the forceSinusoidal veins as chambers
ValvesMaintain unidirectional flow
Foot to heartSuperficial to deep

ClassificationClassification::
C. E. A. P.C. E. A. P.
C.E.A.P.
- clinical state (C), - etiology (E), - anatomical localization (A), - pathophysiology (P)

CEAP Clinical State
0 – No visible venous disease1 – Teleangiectasia or reticular veins2 – Varicose veins3 – Edema4 – Skin changes5 – Healed ulcer6 – Active ulcer

EEtioltiologyogy (E): (E):
Congenital ( Ec)Primer ( Ep)
Secundaer ( Es )
AnatAnatomyomy ( A ( ASS, A, ADD, A, APP ) )
Superficial ( A S )Deep ( A D )Perforators ( A P )

PathoPathopysiologypysiology ( PR, PO, PRO )( PR, PO, PRO )
reflux (PR) 81 %,occlusion ( PO) 2 %,
combination of these 17 %, ** 3.5x risk ** of signs

Patterns of Reflux
1. Truncal reflux saphenous related
up to 5/6 of varicose veins2. Non-truncal Reflux
at least 1/6 of varicose veins3. Deep and perforator reflux
Not common alone but increases with severity of disease

Venous tests:
- Percussion test ( reflux )- Trendelenburg test ( reflux )
- Perthes test ( occlusio )

Continous wave (Continous wave ( CW ) Doppler CW ) Doppler inin venous diagnosisvenous diagnosis
Proximalis “A Proximalis “A soundsound”” Distalis “A Distalis “A soundsound””NormNormaal l venous flowvenous flow 0 0 ++RefluxReflux ++ ++Distal occlusioDistal occlusionn 00 00 animáció
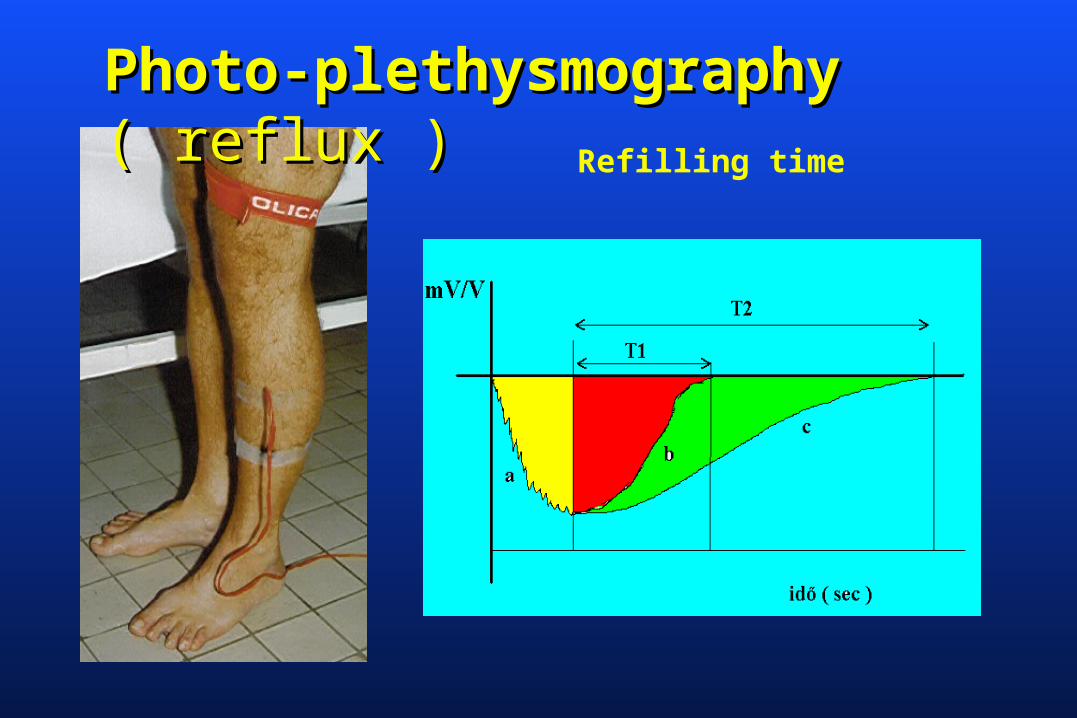
Photo-plethysmographPhoto-plethysmography y ( reflux )( reflux )
Refilling time

Strain-gauge plethysmographStrain-gauge plethysmographyy( Occlusion )

Color duplex ultrasound( IVUS ? )
Valsalva manoverCompression tests

Phlebography
AscendalóDescendalóVaricography
MR Venography ?

Conclusions
- CVI results from venous hypertension usually related to primary reflux in the superficial veins- Heredity is primary risk factor
Multiparity increases chance of its expression- Stigmata can vary
Depends on veins involvedCosmetic to limb threateningMost patiens have symptoms
- Disease occurs in patternsCategorization most important first step