uva-dare (digital academic repository) posttraumatic elbow ... filepart i current issues 30 abstract...
TRANSCRIPT

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Posttraumatic Elbow Stiffness
Lindenhovius, A.L.C.
Link to publication
Citation for published version (APA):Lindenhovius, A. L. C. (2009). Posttraumatic Elbow Stiffness.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 21 Jun 2019

����������� ���� ����������������� ����������� ����� �� ��� ������������������������������������������� � ������ ������������� ��������������� ���� �� � ��� ���� ����������������� ���������������
����������
�������������������������� �����

PART I CURRENT ISSUES
30
Abstract
Loss of motion is a common complication of elbow trauma. Restoration of joint motion in the
posttraumatic stiff elbow can be a difficult, time-consuming, and costly challenge. In this
review of the literature, the biologic response to trauma and the possible etiologic events that
may lead to fibrosis of the capsules and heterotopic ossification will be discussed, as well as
nonsurgical and surgical management of stiffness and expected outcomes of treatment.
Introduction
Stiffness of the elbow joint has long been recognized as a complication of elbow trauma.1-3
Hippocrates (400 BC) emphasized the importance of immediate reduction and recommended
immobilization in 90° of flexion: “an arm ankylosed in the extended position would be better
away for it would be of great hindrance and of little use to the patient”.4 Despite advances in
the management of injuries about the elbow, loss of elbow motion remains a common result.5-
7 restoration of joint motion in the posttraumatic stiff elbow can be a difficult, time-
consuming, and costly challenge. In this review of the literature, the biologic response to
trauma, the possible etiologic events that may lead to fibrosis of the capsules and heterotopic
ossification, nonsurgical and surgical management of stiffness, and expected outcomes of
treatment will be discussed.
Etiology
Loss of motion of the elbow is commonplace after elbow trauma.1,5-8 The etiology of
posttraumatic stiffness can be multifactorial and can include arthrosis9,10, heterotopic bone11-
13, or failure of fracture healing14-16 along with contracture of the soft tissues
around the elbow7. Why the elbow is so prone to contracture has been open to debate and
deserves further investigation. Regan and Reilly17 postulated 3 potential factors: (1) the
complex articular congruity and conformity of the elbow, (2) the brachialis muscle that covers
the anterior capsule, predisposing it to posttraumatic heterotopic ossification, and (3) the often
prolonged immobilization due to the difficult challenge of achieving stable fixation of
complex comminuted fractures.
Kay18 established a classification system of the stiff elbow based on the specific components
involved. According to his classification, type 1 involved soft tissue contracture; type 2, soft
tissue contracture with ossification; type 3, undisplaced articular fracture with soft tissue
contracture; type 4, displaced intra-articular fracture with soft tissue contracture; and type 5,
involved posttraumatic bony bars. Morrey9 classified stiffness on the basis of the anatomic
location of the contracture: intrinsic factors (intra-articular changes), extrinsic factors (extra-
articular changes), or a combination of the two. Intrinsic factors include intra-articular
adhesions, articular malalignment, loss of articular cartilage, or a multifaceted cause, whereas

LITERATURE REVIEW CHAPTER 2
31
extrinsic factors encompass contracture of the soft tissues (eg, the joint capsule or collateral
ligaments), heterotopic ossification, or extra-articular malunions. Because there is often more
than 1 anatomic structure involved, it is useful to use this classification. Mixed involvement is
most common (ie, extrinsic contractures will almost always have an intrinsic component).7
Most authors agree that prolonged immobilization can lead to capsular contracture19 and that
early active mobilization after the initial injury will be a factor in limiting residual stiffness.19-
21 Although several reports in the literature have described the beneficial effects of
manipulation therapy without exacerbation of heterotopic ossification22-25, there remains
some debate regarding the relationship of passive elbow mobilization and resultant
heterotopic ossification.21,26,27 We recommend that forceful and repeated manipulation of the
stiff elbow should be avoided as experimental models have shown the development of
heterotopic ossification under these circumstances27, yet gentle passive motion may be
indicated postoperatively11. In addition, multiple surgical interventions within the first weeks
after trauma11, thermal burns28,29, and associated head trauma30 have been suggested to
predispose for heterotopic ossification.
Soft Tissue Contracture
Pathophysiology
Contracture of the soft tissues around the elbow primarily concerns the capsule and the
ligaments. Animal models have demonstrated elevated numbers of myofibroblasts31,32 that
have highly contractile properties33 and increased proliferation of extracellular matrix34 in
experimentally induced contracture of knee and elbow capsules. In addition, increased
formation of collagen cross-links, together with decreased proteoglycan content and decreased
water content, may be characteristics of abnormal tissues in experimentally induced joint
contractures.35 All of the above may be related to the increased expression of transforming
growth factor beta (TGF-�) that was found in contracted rabbit elbow capsules.36 These
processes may result in scarring of the capsule by fibrosis with resultant contracture of the
joint.
It has been suggested that mechanical stimulation of injured periarticular structures, such as
may occur with efforts to gain or maintain motion, may contribute to tissue contracture37,38 by
an alteration in collagen synthesis.38 The medial collateral ligament may be prone to scarring
that results in stiffness because of the persistent stress it sustains as a consequence of the
carrying angle of the elbow.21 The exact mechanism that leads to contracture of the soft
tissues merits further investigation. Better understanding of the pathogenesis of the fibrotic
elbow capsule will potentially lead to more effective nonsurgical management of
posttraumatic stiff elbows in the future.
PART I CURRENT ISSUES
32
Heterotopic Ossification
Pathophysiology
Heterotopic ossification leading to loss of motion is uncommon after elbow trauma.26 When
associated with identified risk factors such as concomitant head trauma, the incidence
increases substantially.30 Heterotopic ossification is the inappropriate formation of mature
lamellar bone in soft tissues, which differs from the commonly seen periarticular
calcifications, in which amorphous calcium deposits form in soft tissues around the elbow
after injury.20,39 The formation of heterotopic bone is caused by pluripotential mesenchymal
stem cells that differentiate into osteoblasts (stimulated by, eg, trauma, surgery, or
inflammation), which produce osteoid40 that mineralizes into bone.41 This requires osteogenic
precursor cells, an inductive agent (most likely a growth factor), and an environment
conducive to osteogenesis.42 The heterotopic bone that subsequently develops is
histologically identical to native bone but is more metabolically active and does not have a
true periosteal layer.43
Prevention
Prevention of heterotopic ossification is based on 3 principles: (1) disrupting the signaling
pathways, (2) altering the relevant progenitor cells in the target tissue, and (3) modifying the
environment conducive to heterotopic osteogenesis.42 Anti-inflammatory drugs (for disruption
of inductive signal), preoperative irradiation (for disruption of responsive cells), and
postoperative etidronate (for disruption of conducive environment) may all have an inhibitive
effect.42
Nonsteroidal anti-inflammatory drugs (NSAIDs) inhibit the enzyme cyclooxygenase, which is
needed for the production of prostaglandins. Lowering prostaglandin levels raises the
threshold for heterotopic ossification44, because the induction of heterotopic ossification is
stimulated by prostaglandins together with bone morphogenetic proteins45. The use of
nonselective NSAIDs, such as indomethacin, ibuprofen, and naproxen, have all been related
to reduced formation of heterotopic bone, in particular in the hip.46-50 Although frequently
used8,21,51-53, the role of NSAIDs in prevention of heterotopic ossification around the elbow is
unclear, and a comparative trial is needed54. The possible beneficial role of selective NSAIDs
that inhibit cyclooxygenase 255,56 is uncertain because of the associated risk of serious
cardiovascular side effects57. Diphosphonates that interfere with the calcification of osteoid
are also considered a poor choice, as rebound calcification is to be expected after
discontinuation58, and side effects include serious gastrointestinal complaints and
osteomalacia59. Gene therapy with BMP antagonists might offer some potential for future
treatment, as a preventive effect on the formation of heterotopic bone has been shown in an
experimental animal model.60

LITERATURE REVIEW CHAPTER 2
33
An alternative prophylaxis is the use of low-dose irradiation within 72 hours after the trauma
to alter the progenitor cells in the target tissue. Stem cells are particularly radiosensitive, and
irradiation prevents them from differentiating into osteoblasts.61 A possible inhibiting effect
on the formation of heterotopic bone has been described with doses ranging from 600 to 1,000
cGy.62-65 The prevalence of radiation-induced osteosarcoma is low in humans.66 In addition, in
a retrospective review of medical records from a period of 50 years, radiation-induced bone
sarcoma was not reported with doses of less than 3,000 cGy.67 High doses of sodium
etidronate may inhibit the angiogenesis needed for the mineralization of bone matrix and
thereby reduce ossification68,69 but are not recommended as they predispose to osteomalacia
and impair the ossification of normal bone.70
Malunions and Nonunions
Intra-articular and extra-articular malunions and nonunions of the distal humerus, proximal
ulna, and radial head may cause pain, instability, and severe limitation of elbow function.
Extra-articular malunions of the distal humerus
The lateral column of the distal humerus is curved anteriorly with the lateral epicondyle
translated anteriorly with respect to the humeral diaphysis, whereas the medial column and
medial epicondyle are more in line with the diaphysis. The use of straight plates on the lateral
column of the distal humerus may lead to loss of anterior translation of the articular surface of
the distal humerus. This can result in a smaller axis of rotation that causes less space for the
coronoid and muscles and soft tissues during elbow flexion.71 The use of precontoured plates
on the lateral column may be helpful to restore the original anatomy of the distal humerus and
thereby prevent malunion.72,73 Treatment of a distal humerus fracture in which there is
metaphyseal comminution may lead to shortening in spite of bridging the comminution. This
may cause loss of the fossae, which results in limited flexion and extension.71 In addition,
implants, scar tissue, fracture callus, and heterotopic bone may obstruct the coronoid, radial,
and olecranon fossae. In the treatment of elbow stiffness due to malunion of a distal humerus
fracture, the fossae should be cleared of heterotopic bone, scar tissue, and implants with a burr
used to deepen or enlarge the fossae, even to the point of creating a hole through the distal
humerus using the Kashiwagi technique.74 An extra-articular osteotomy with subsequent bone
grafting and internal fixation may be considered in the case of an unsuccessful capsular
release and debridement of fossae.
Intra-articular malunions
Malunion of intra-articular distal humerus fractures is commonly associated with loss of
motion.75-77 Malunited anterior shearing articular fractures may be treated with osteotomy
and capsular release to restore motion.75 Uneven articular surfaces with subsequent

PART I CURRENT ISSUES
34
incongruency of the ulnotrochlear articulation can lead to stiffness and arthrosis. The
preservation of appropriate contact between the medial trochlea and the anteromedial facet of
the coronoid process and between the capitellum and the radial head is considered important
in maintaining a mobile joint.78 Malunited fractures of the radial head typically present as
forearm stiffness rather than ulnohumeral stiffness and radiocapitellar or radioulnar arthrosis78
and in most instances can be treated successfully by radial head resection.79,80
Arthrosis and stiffness after intra-articular fractures of the proximal ulna can be related to both
instability as well as joint incongruity.78 Adequate restoration of the normal anatomy of the
ulnotrochlear notch and the coronoid process is important to prevent arthrosis and instability
of the elbow.81-83 Lack of the coronoid as an anterior buttress can result in malalignment with
subsequent anterior subluxation of the distal humerus.78,84-86 Inadequacy of the coronoid is
difficult to treat.85,87 The use of an osteoarticular autograft or allograft may prove useful to
restore the coronoid84-86,88, particularly for small coronoid fractures that are part of a terrible
triad injury85.
Nonunions
Nonunion after intra-articular fractures of the distal humerus occurs usually at the
supracondylar level rather than at the intra-articular level.16,78,89 Nonunited distal humeral
fractures may lead to pain, instability, and stiffness, the latter in many patients caused by
motion occurring at the nonunion site16 with ankylosis or near-ankylosis of the joint itself.90,91
Intra-articular nonunions add to incongruity, increased articular adhesions, and presence of
malpositioned articular fragments that have limited blood supply.15,78 A combination of
debridement of the nonunion site, realignment and stable internal fixation, autogenous bone
grafting, elbow capsulectomy, and an intensive postoperative rehabilitation program have
been shown to result in improvements in union rate and elbow function.14-16,91-93 In the older
patients with limited demands, a total elbow arthroplasty may be considered. Epicondylar
nonunions may contribute to instability94, but motion usually is not an issue78.
Unstable nonunion of the proximal ulna is infrequently seen after olecranon fracture-
dislocations and posterior Monteggia fractures.95,96 As with distal humeral nonunions,
capsulectomy in conjunction with stable fixation of the nonunion may reduce stress on the
nonunion site and restore motion. If there is an additional nonunion of the coronoid process, it
may be internally fixed when the fragment is large and reconstructed when the fragment is
small or absent.78,84-88 Nonunion may also be the result of a neglected or inadequately treated
simple olecranon fracture95,97 or an ununited olecranon osteotomy96. Fortunately, significant
loss of motion is not common78,95,97, and an eventual surgical intervention would consist of
debridement, bone grafting, and internal fixation but may not be necessary in all patients78.
Recently, satisfactory results for treatment of olecranon nonunions during total elbow
arthroplasty were reported98.

LITERATURE REVIEW CHAPTER 2
35
Nonunions of nonsurgically treated (isolated) radial head fractures are uncommon99,100 and in
general cause little or no pain and usually do not interfere with motion99, therefore surgical
treatment of the nonunion may not be needed78,99. Nonunions of surgically treated radial head
fractures are usually caused by broken or loose implants and lead to restricted forearm
rotation and pain.101,102 Removal of radial head and implants usually relieves pain and restores
motion.101 In view of the fact that total elbow arthroplasty has the potential risk of loosening
over time as well as requiring marked limitation of function, it has been indicated primarily
for older patients whose major problem is a painful stiff elbow.9,103,104
Assessment
A functional arc needed to perform most basic daily activities is defined as an arc of flexion
from 30° to 130° and an arc of forearm rotation from 50° of pronation to 50° of supination.105
However, the functional impairment depends on the individual requirements of each
patient.106
It is important to understand the original injury and initial treatment as well as other
associated conditions such as neurologic dysfunction, infection, and ipsilateral limb
injury.106,107 In most cases, posttraumatic stiffness is not painful, especially at rest, and pain
usually is not present during flexion and extension. Pain with motion suggests the presence of
arthrosis and/or ulnar nerve dysfunction106, whereas patients with pain at rest and a history of
surgery are at risk for a lowgrade infection; therefore, laboratory studies should include a C-
reactive protein level and an erythrocyte sedimentation rate107. The elbow should be aspirated
prior to surgery if these values are abnormal and warmth or other evidence of inflammation is
present. The ulnar nerve is commonly involved in elbow trauma and deserves special attention
during the examination of the entire upper extremity.
Although anteroposterior and lateral radiographs are sufficient in most patients107, assessment
may be more complete with computed tomography (CT) scans65 and even more with 3-
dimensional CT scans, particularly when heterotopic bone is present11,53,106,108 (Fig. 1).
Although magnetic resonance imaging (MRI) defines the soft tissues around the elbow, it is
not considered useful in the evaluation of elbow contracture because it does not define the
heterotopic ossification and joint anatomy as well as CT imaging.20
Heterotopic ossification presents as local soft-tissue swelling, warmth and tenderness, easily
mistaken for infection, cellulitis, thrombophlebitis, tumor, or soft tissue (nonosseous)
calcification.20,39,42 The end points of motion become rigid or abrupt instead of compliant as
seen with some soft tissue contractures, and motion at the limits may be painful.20 Pain
through the central flexion arc suggests joint incongruity or degeneration of the ulnotrochlear

PART I CURRENT ISSUES
36
Figure 1. (A–C) Three-dimensional reconstruction of CT scans clearly depict the heterotopic bone around the elbow which may be helpful for operative planning. (Images courtesy of David Ring, MD, PhD.)
joints or the radiocapitellar joint in the case of pain through the central arc of forearm
rotation.20 Heterotopic ossification can manifest from 2 to 12 weeks after the inciting event
(trauma, surgery, burn, or neurologic insult).109 The maturity of the heterotopic bone as well as
the time since onset is important for the timing of eventual surgical intervention. Technetium-
99m bone scans are no longer used to evaluate bone metabolic activity, because they do not
provide useful prognostic information.39,65 The progression of heterotopic ossification should
be evaluated radiographically; a cloudy periarticular density may be seen within several
weeks after injury and subsequent maturity is indicated by smooth, well-demarcated cortical
margins and defined trabecular markings20, generally about 3 to 6 months after its
appearance7,39. Although early excision of heterotopic bone was not recommended because
this was thought to predispose to recurrence110, most authors do now agree that surgical
excision can safely proceed as soon as maturity is seen radiographically65,106,111,112.
Advantages of early resection include minimizing capsular and ligamentous contracture,
muscle atrophy, and cartilage degeneration, and allowing a more rapid functional recovery53.
In skeletally immature individuals, nonbridging heterotopic bone may resorb over time,
therefore it may be wise to wait longer in children.20
The classification system of Hastings and Graham113 is useful for clinical assessment,
treatment, and operative planning. Class I represents heterotopic ossification not causing
functional limitation and is therefore clinically insignificant, although prophylactic treatment
may be considered. Patients with class II heterotopic bone have a functional limitation of
motion: class IIA represents ulnohumeral limitation less than a (100°) flexion arc from 30° to
130°, class IIB concerns limitation of forearm rotation less than a (100°) arc from 50°
pronation to 50° supination, and class IIC concerns heterotopic bone causing limitation in
both planes. Patients with class III heterotopic ossification have ankylosis that prevents either
C B A

LITERATURE REVIEW CHAPTER 2
37
ulnohumeral motion, forearm rotation, or both. It may be useful to subclassify class III
according to the planes of limited motion: class IIIA no ulnohumeral motion, class IIIB no
forearm rotation, and class IIIC no motion in either direction.20
Heterotopic bone was traditionally considered a complicating factor for surgical release and
associated with poor outcomes, in particular in presence of a complete bony bridge.114-116
However, more recent studies have suggested that patients with nonbridging heterotopic
ossification that complicates capsular contracture may regain even more motion after surgical
release than patients with a capsular contracture alone.8,21
Nonsurgical Treatment
If posttraumatic stiffness develops in spite of precautionary measures such as early active
motion, it has the potential for successful nonsurgical treatment. Regaining joint motion in the
most time-efficient manner is critical for return to function, control of rehabilitation costs,
and to prevent the need for additional surgery.
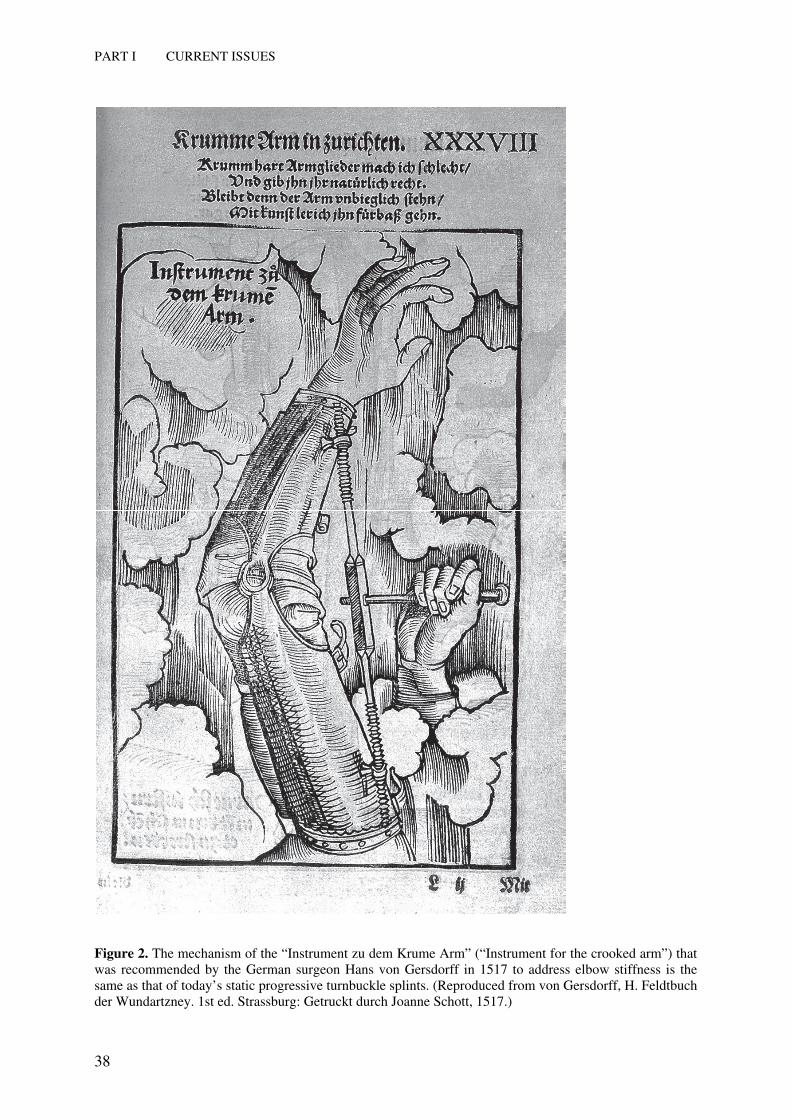
The use of turnbuckle-like splints to restore motion of the posttraumatic stiff elbow was
described in the Medieval era by the German surgeon Hans von Gersdorff (1455–1529)3 (Fig.
2). Today, adjunctive splinting devices are still added to the traditional rehabilitation program
and may help to prevent the need for surgical intervention. Splints are especially effective in
patients with contractures of relatively short duration and little articular involvement.19
Satisfactory restoration of motion with use of static progressive turnbuckle splints (that apply
a static stress relaxation force to the elbow tissues, which is sequentially increased as motion
is achieved) has been described in several studies.117-121 Dynamic splints that apply a constant
prolonged force to the tissues as additional motion is achieved are a popular alternative with
satisfactory results reported.21,122-124
Surgical Treatment
If nonsurgical treatment fails to restore a functional arc of motion, surgical treatment may be
considered.8,19,106,125,126 Traditionally, surgery has been offered to patients with flexion
contractures or extension contractures of at least 30°. However, the justification of surgical
intervention is highly individualized, and the patient’s needs and the ability of the surgeon to
realize these expectations should be considered, with a mutual assessment of risks and
benefits of the intervention.20,64,107 There should be radiographic union of the fractures, and
the patient must have the ability and motivation to complete a rigorous and prolonged
postoperative elbow rehabilitation program.20,64,127
Surgical release of the elbow has proved to be an effective way to restore motion, both with
an open procedure5,8,9,19,21,52,125,126,128-142 and after arthroscopic release143-151. Good functional
results after an open release for posttraumatic stiffness have been described in several case
PART I CURRENT ISSUES
38
Figure 2. The mechanism of the “Instrument zu dem Krume Arm” (“Instrument for the crooked arm”) that was recommended by the German surgeon Hans von Gersdorff in 1517 to address elbow stiffness is the same as that of today’s static progressive turnbuckle splints. (Reproduced from von Gersdorff, H. Feldtbuch der Wundartzney. 1st ed. Strassburg: Getruckt durch Joanne Schott, 1517.)

LITERATURE REVIEW CHAPTER 2
39
series5,8,9,19,21,52,125,126,128-142, with an average minimal improvement in ulnohumeral motion
from 21° up to a maximum average improvement of 66°.9,21
Results of arthroscopic release have been reported less widely, and only few papers143-145,148
report results for posttraumatic stiffness separately from those for stiffness originating from
other causes. In the ones that do report results separately143-145,148 average improvements from
29°145 up to 70°144 have been reported. Although the safety of arthroscopy is still being
studied, in particular with regard to iatrogenic nerve damage, the application of this approach
may be extended to even the most severe contractures. The choice between both techniques
depends on the extent of the pathology and the experience of the surgeon.107 The need for
articular reconstruction, as is usual after an intra-articular fracture, is an indication for open
release, because articular involvement makes an arthroscopic release more difficult. In
addition, previous anterior transposition of the ulnar nerve may preclude use of the
anteromedial portal and as a consequence be a contraindication for arthroscopic release.152,153
Other treatment modalities include an interposition arthroplasty when extensive loss of the
articular surface is present, especially in younger patients.9,89,103,107,154-158 In older patients with
very stiff or ankylosed elbows with extensive articular involvement, a total elbow arthroplasty
may be considered.89,107,155,157
A young age9,136 and arthrosis19 have been associated with less favorable outcomes after a
contracture release, whereas patients with heterotopic ossification due to burns or head injury
seem to have better functional outcomes8,53. However, Bae and Waters139 reported results of
contracture release in adolescents that were virtually similar to those reported for adults. The
timing of surgery has also been associated with the outcomes. The longer the intervention is
delayed, the more contracted muscles and tendons become the articular cartilage may also
suffer, particularly when there is complete ankylosis of the elbow.53 Therefore, patients should
preferably be treated within 1 year after onset of stiffness, as better functional results may be
expected then.21,51,53
Open Contracture Release
Depending on the plane of elbow contracture, the location of previous elbow incisions, the
need for nerve decompression, and the location and extent of heterotopic ossification, the
surgeon can choose between medial, lateral, and anterior approaches. Either a posterior
midline incision or separate medial and lateral incisions will permit both posteromedial and
posterolateral arthrotomies and access to the ulnar nerve and anterior elbow via deep lateral
and medial approaches.7 Separate medial and/or lateral skin incisions may be useful to avoid
skin flap devascularization in the case of previous incisions or if there is concern about the
integrity of the soft tissue covering the elbow. Avoidance of injury to the median, radial,
posterior interosseous, and ulnar nerves is of utmost importance.64

PART I CURRENT ISSUES
40
Good results have been described with use of a lateral approach8,51,52,125,126, often referred to
as the lateral column procedure8,159. It is a highly versatile approach, although the ulnar nerve
will often need to be exposed on the medial side to ensure its safety. The lateral column
procedure may be used to address extrinsic contracture of the anterior and posterior capsules
with articular involvement of the radiohumeral joint.8 If articular involvement requires
attention to structures other than the radiohumeral joint, this exposure is inadequate.107,159
A medial approach may be used to address limited medial articular pathology with
involvement of the ulnar nerve, presence of heterotopic bone on the medial side, and
ossification or deficiency of the medial collateral ligament (MCL).107,133 Although an
advantage of this approach is the direct view on the ulnar nerve, a drawback is that the radial
nerve is at risk at the depth of exposure on the far side anteriorly. The median nerve is farther
away from the capsule than the radial nerve.160 This limited exposure may not be effective
when there is articular involvement.107
An anterior approach, which has been reported in several articles19,132,142 for the correction of
flexion contractures, has only very limited indications and may only be used for an isolated
flexion contracture with normal full flexion and no evidence of bony abnormalities at the
olecranon or in the olecranon fossa. Neurovascular structures are at risk when using the
anterior approach19,125,126, and an additional posterior release may frequently be needed132,136.
Regardless of the approach that is used, every attempt is made to preserve the lateral collateral
ligaments and the anterior oblique band of the MCL.20,21,133 This greatly facilitates
rehabilitation and virtually eliminates the potential for postoperative instability. Only in long-
standing and very severe cases may a partial release of the anterior oblique band of the MCL
and the lateral collateral ligaments be indicated.18
The most common complications of open contracture release include neuropathies, infection,
and recurrence of elbow stiffness and/or heterotopic bone.1,8,12,19,20,52,53,125,127,128,132,134,
135,137,138,142
Lateral column procedure
Either a lateral or midline posterior incision is used, fasciocutaneous flaps are elevated and
started proximally, and the lateral supracondylar ridge of the humerus is exposed by
reflecting the extensor carpi radialis longus (ECRL) anteriorly off the humerus and the triceps
off the humerus posteriorly.159 The dissection is continued for 2 to 3 cm distally through the
common extensor tendon from the epicondyle in a line toward Lister’s tubercle. This
generally passes in the interval between the ECRL and the extensor carpi radialis brevis
(ECRB), along the anterior edge of the extensor digitorum communis. The entire anterior soft
tissues are then reflected anteriorly off the capsule, which can then be excised. The release
should continue right to the level of the collateral ligaments. The coronoid and radial fossae
are cleaned, and spurs and loose bodies are removed. On the posterior side of the elbow, the
LITERATURE REVIEW CHAPTER 2
41
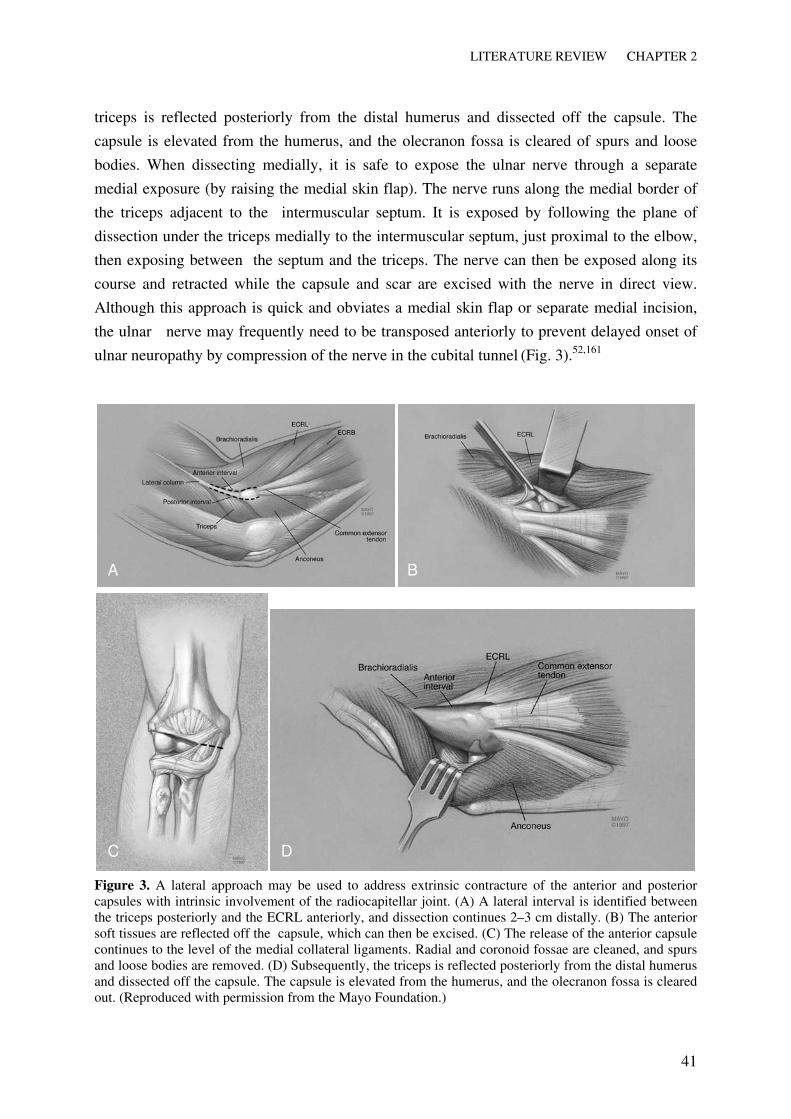
triceps is reflected posteriorly from the distal humerus and dissected off the capsule. The
capsule is elevated from the humerus, and the olecranon fossa is cleared of spurs and loose
bodies. When dissecting medially, it is safe to expose the ulnar nerve through a separate
medial exposure (by raising the medial skin flap). The nerve runs along the medial border of
the triceps adjacent to the intermuscular septum. It is exposed by following the plane of
dissection under the triceps medially to the intermuscular septum, just proximal to the elbow,
then exposing between the septum and the triceps. The nerve can then be exposed along its
course and retracted while the capsule and scar are excised with the nerve in direct view.
Although this approach is quick and obviates a medial skin flap or separate medial incision,
the ulnar nerve may frequently need to be transposed anteriorly to prevent delayed onset of
ulnar neuropathy by compression of the nerve in the cubital tunnel (Fig. 3).52,161
Figure 3. A lateral approach may be used to address extrinsic contracture of the anterior and posterior capsules with intrinsic involvement of the radiocapitellar joint. (A) A lateral interval is identified between the triceps posteriorly and the ECRL anteriorly, and dissection continues 2–3 cm distally. (B) The anterior soft tissues are reflected off the capsule, which can then be excised. (C) The release of the anterior capsule continues to the level of the medial collateral ligaments. Radial and coronoid fossae are cleaned, and spurs and loose bodies are removed. (D) Subsequently, the triceps is reflected posteriorly from the distal humerus and dissected off the capsule. The capsule is elevated from the humerus, and the olecranon fossa is cleared out. (Reproduced with permission from the Mayo Foundation.)
A B
C D

PART I CURRENT ISSUES
42
Medial column approach
The medial column approach162 is conceptually similar to the lateral column procedure. The
medial antebrachial cutaneous nerve is protected and the ulnar nerve is freed up and
transposed anteriorly. The anterior half of the origin of the flexor pronator muscles are
reflected from the medial supracondylar ridge. From there, the common flexor-pronator
tendon is split longitudinally for 2 cm distally. The brachialis and the anterior portion of the
flexor-pronator group are dissected subperiosteally off the anterior humerus and capsule from
proximal to distal. The capsule can then be excised. If there is concern about the safety of the
radial nerve, a separate limited exposure can be made on the lateral side as described above to
resect the lateral capsule under direct vision. The posterior release from the medial side is
identical to that decribed for the lateral column procedure, except that the ulnar nerve must be
first transposed. If there is difficulty to release the posterolateral capsule to restore adequate
flexion, a separate lateral exposure may be required (Fig. 4).
Figure 4. A medial approach may be used to address medial articular pathology with involvement of the ulnar nerve, heterotopic ossification on the medial side, and ossification or deficiency of the MCL. The ulnar nerve is at direct view using this approach. It is conceptually similar to the lateral approach. The anterior half of the origin of the the flexor pronator muscles are reflected from the medial supracondylar ridge, and from there, the common flexor-pronator is split for 2 cm distally. The brachialis and the anterior portion of the flexor-pronator group are dissected subperiostally off the humerus and the capsule. The capsule can then be excised. (Reproduced with permission from the Mayo Foundation.)
Anterior approach19,132
A curvilinear anterior skin incision is used, starting proximally at the lateral side and
continuing distally on the medial side. The structures in the anterior aspect of the elbow are
exposed, taking care to protect the medial and lateral antebrachial cutaneous nerves. The
brachial artery is identified and protected together with the median, radial, and
musculocutaneous nerves. Starting medially, an interval between the flexor muscle origin and
the biceps tendon is developed. Using a blunt retractor, the brachialis muscle is dissected from
the joint capsule. A curved clamp is then passed from medial to lateral in the interval between

LITERATURE REVIEW CHAPTER 2
43
the brachialis muscle and the capsule. The interval between the biceps tendon and the
brachioradialis is then exposed, and the interval between the brachialis and the capsule is
further developed by blunt dissection. Placing a retractor deep to the brachialis allows direct
visualization of the entire anterior capsule, which can then be excised entirely.132 Sometimes,
sharp release of the brachialis may be needed to increase extension. The wound is closed over
suction drains and a bulky dressing and plaster splint are applied.
Heterotopic bone
Surgical resection of heterotopic bone is only indicated when the bone blocks motion39 and is
a technically challenging procedure20. Anterior heterotopic bone most commonly forms
beneath the brachialis muscle and is not continuous with the anterior articular surface. For
resection of anteriorly located heterotopic bone, a medial, lateral, or combined medial and
lateral approach65 may be chosen. In case of extensive anterolateral ossification, it is
important to identify the radial nerve and the posterior interosseous nerve. The median nerve
is most commonly protected by the brachialis muscle. Motion-limiting heterotopic bone in the
region of the proximal radioulnar joint requires special attention. The normal cortices of the
proximal forearm bones need to be defined, and iatrogenic injury to the lesser sigmoid notch
of the proximal ulna should be avoided. Posterior heterotopic bone is often in continuity with
the joint, beneath the triceps, and most commonly leads to ankylosis.39 Resection of
posteriorly located heterotopic bone requires elevation of the triceps from the olecranon. If
there is posteromedial involvement, extra attention should be paid to the ulnar nerve. After the
resection of the heterotopic bone, the surgeon continues with the elbow capsular release as
described above.
Complete bony ankylosis is a uniquely challenging problem, because the joint may be entirely
encased in bone.64,163 The capsule is usually distinct from the heterotopic bone anteriorly but
not posteriorly. It may be difficult to identify the junction between the heterotopic bone and
the original articular anatomy. An osteotome is used to resect the heterotopic bone in layers,
until the joint is encountered; quick and sharp blows with the osteotome will usually separate
the heterotopic bone from the underlying host bone along the anatomic planes. Some gentle
manipulation is needed intraoperatively. Because of the risk of an iatrogenic fracture, this
must be performed with great care. The limited force (applied with 2 fingers) is placed close
to the elbow. A hinged external fixator may be considered when there is a tendency for the
elbow to subluxate or dislocate after excision.64 Synostosis that is limited to the radial head or
neck level may best be treated with radial head resection.20 Results of resection of a proximal
radioulnar synostosis112,114,115 and complete bony ankylosis12,164 are not as promising as are
the results of excision of nonbridging heterotopic bone.

PART I CURRENT ISSUES
44
Arthroscopic Contracture Release
Only a small number of retrospective case series have been published over the past
decades.143-150 At the present time, arthroscopic release is best indicated in limited
contractures without complicating factors such as the presence of heterotopic bone or
neuropathies. Arthroscopic release of the stiff elbow should only be performed by surgeons
with a high level of experience and training. In spite of difficulties and risks that are
associated with arthroscopy, indications and techniques are evolving rapidly. A factor that
complicates the procedure is the limited intra-articular volume capacity that results from the
capsular contracture.165,166 This can obscure access and visualization of the joint145 and puts
the neurovascular structures at risk for iatrogenic injury by instruments165. Surgeons should
therefore be aware of the special techniques that are being developed when using the
arthroscopic approach to address stiff elbows. Some authors106,167 recommend the use of
retractors in the joint to facilitate the arthroscopic release of the capsule. This will add to
visualization and may permit more complex contractures to be addressed safely, without
damage to nerves. The surgeon may have to use multiple portals for the scope, shaver/cutter,
and the retractors.
Release of the posterior capsule168
A view is established (with the scope in the posterolateral portal and the shaver in the
posterior portal, or the scope in the direct midlateral and/or the shaver in the posterolateral
portal) by debriding the olecranon fossa. The capsule is elevated from the distal humerus with
use of a shaver or periosteal elevator, which further
increases the working space. A retractor may be used to maintain this space. In case of
synovitis, a synovectomy is performed. Osteophytes and loose bodies are removed, and
subsequently the posterolateral capsule is resected with a shaver or radiofrequency ablation
device, which is most easily done through the posterolateral portal. If there remains a lack of
flexion, the posteromedial capsule is released as well, and if needed, the posterior band of the
MCL may also be released. Given the anatomic location of this band near the cubital tunnel,
the ulnar nerve is at significant risk when this release is performed. Identification of the ulnar
nerve (arthroscopically or through a small incision167) during the posteromedial release is
paramount, retractors should be used, and release should be performed along the olecranon as
the nerve is closer to the medial epicondyle than to the olecranon. Eventually, the ulnar nerve
may be fully exposed or transposed during or prior to the release.
Anterior capsule release168
The first step, assessing the joint cavity, may be the most challenging part of the procedure.
Three anterior portals are established, starting with the scope and shaver in the anterolateral
and proximal anteromedial portals169-172 and a retractor in the proximal anterolateral portal. If

LITERATURE REVIEW CHAPTER 2
45
needed, a second retractor can be inserted through the anteromedial portal.106 The next step is
to create a view and to establish a working space. This involves identifying a sufficient
amount of normal articular anatomy to permit orientation and then stripping the capsule off
the humerus and supracondylar ridges. A synovectomy is performed and the capsule is
debrided. Loose bodies and osteophytes are removed, and abnormal bone is recontoured. The
capsule is now clearly delineated as a structure before it is cut. The capsule is divided from
medial to lateral with a wide-mouthed duckbill punch, as the plane of dissection between the
capsule and the brachialis muscle is more distinct on the medial side. The capsulotomy is
continued down to the level of the collateral ligaments on each side, and then the
capsulectomy is performed on the medial side, extending from proximal to distal. The final
step is the proximal and distal excision of the lateral capsule. During this part of the
procedure, the radial nerve, located just anterior from the radial head and between the
brachialis and ECRB, is unprotected and at risk (Fig. 5). The efficacy of the procedure may be
dependent on the completeness of the capsular excision.106
Figure 5. Transverse section of a normal elbow before and after distention. Capsular distention places the nerves away from surgical instruments in the normal elbow. In the stiff elbow, the capsular compliance is limited, and particularly the radial nerve is at risk for iatrogenic injury. (Reproduced with permission from Chantal Lichaa O’Driscoll.)
Interposition Arthroplasty
Whereas total elbow replacement may be a viable option to restore motion and relieve pain in
the older and less active patient with severely damaged articular surface89,107,155, interposition
arthroplasty may be indicated to restore function and relieve pain in younger and more active

PART I CURRENT ISSUES
46
patients, withstanding the functional demands.17,154,156,158,173,174 The goal of interposition
arthroplasty is to preserve functional stability and to reduce the likelihood of reankylosis by
interposing a substance between the resected bone ends.174 Resurfacing materials may include
autologous fascia lata from the thigh, autologous skin, or an allograft such as an Achilles’
tendon.156,158,173,175
When the ulnar nerve is symptomatic, a medial interval may be chosen.156,176 Otherwise, a
lateral interval is used. A posterior skin incision or previous incision may be used followed by
development of a Kocher’s interval between anconeus and extensor carpi ulnaris. The origins
of the common extensor muscle mass and the lateral ligament complex are released from their
origin on the humerus. The anterior and posterior ligaments and capsules are excised. The
radial head is preserved if forearm rotation is painless. A burr is used to remove a small
amount of bone to contour the articular surfaces of the distal humerus and ulna; this
accommodates the Achilles’ tendon allograft
and concentric fluid joint motion. However, the medial and lateral trochlear ridges should be
left intact, as these add to the inherent stability of the elbow.177 Drill holes are placed from
posterior to anterior in the distal humerus. The graft is contoured the size of the distal humerus
and draped over the trochlea and capitellum, and sutures are placed through the drill holes to
secure the graft.9,174 Ligaments are repaired; this may be done with suture anchors or excess
graft if Achilles’ tendon was used. When an articulated external fixator is applied, only a
minimal amount of bone needs to be resected, which helps prevent instability.158,178,179 The
triceps is reattached, and the interval is closed.
Few articles describe the outcome of interposition arthroplasty. Results have been reported
with various success for inflammatory158,178 and (post)traumatic conditions.9,103,158,176 Elbow
instability is associated with a poor outcome.103,158,176 Complications may include bone
resorption, nerve dysfunction, heterotopic ossification, triceps rupture, instability, infection,
seroma formation at the fascial donor graft site, and long-term failure.158,173,174 In cases of
failed interposition arthroplasty, later revision to a total elbow arthroplasty may result in a
satisfactory end result.158,180
Total Elbow Arthroplasty
Total joint replacement can be a salvage procedure for very stiff or ankylosed elbows with
considerable articular involvement in the older and less active patient, especially if there are
no other treatment options available anymore.89,107,155 Patients should have reasonable
expectations and be able to comply with an intensive postoperative rehabilitation program.6 In
elbows with posttraumatic contracture, which are often complicated by deficient bone stock,
deformity, and capsuloligamentous instability, linked designs are usually
recommended.6,10,107,155,157,177,181,182 These semiconstrained hinge devices are thought to limit

LITERATURE REVIEW CHAPTER 2
47
excessive loading of the bone-cement interface by allowing soft tissues to absorb some of the
forces.183
The technique is challenging and, in the case that no triceps-sparing approach is used, the
reattachment of the triceps is crucial. Specific techniques depend on the implants that are
used, presence of previous incisions, and the surgeon’s preference.184 However, in all cases,
the ulnar nerve should be identified, released from surrounding scar and soft tissue, and
eventually transposed.107,155,157,181,185 Aggressive soft tissue release that involves the collateral
ligaments, and posterior and anterior capsules, and often includes the origins of the common
flexors and extensors, is needed to balance soft tissue distortion of the joints.107,157 Adequate
bone may need to be resected to optimize the outcome; if there is complete osseous ankylosis,
the joint line may be established with a sagittal microsaw or small osteotome to create a space
as close to the center of rotation of the ulnohumeral joint as possible to offer the best
biomechanical and functional condition for the implant.157 In addition, it may be needed to
resect the radial head and heterotopic bone and to re-create an adequate medullary canal with
use of a small burr.157,184
Although preoperative presence of heterotopic bone157 and deformity10 have been associated
with a less favorable outcome, total elbow replacement for the treatment of posttraumatic
arthritis is associated with substantial functional improvement and pain relief in most
cases6,10,155,186,187. However, complications such as ulnar nerve dysfunction, mechanical
failure, loosening, infection, triceps disruption, and fracture (particularly in older women188)
may be seen frequently and result in the need for revision surgery and eventual unsatisfactory
outcomes6,10,98,155,157,186-201. Some of these complications157 may be attributed to the stress that
components are exposed to (which may depend on the activity level of patients with
posttraumatic arthritis187) and the typically high number of previous surgeries that patients
with posttraumatic arthritis have undergone10,190, which increases the risk for wound
complications or infection187,197,200.
Postoperative Management and Rehabilitation
Although the rehabilitation program for each of the surgical procedures has its unique
features, the postoperative management should be aimed at (1) restoring a functional arc of
motion, (2) regaining muscle power, and (3) reincorporating the limb into functional
activities.177 Most authors start mobilization of the elbow within 2 days after an open
contracture release8,51,52,64,65,125,126,128,133,134,137,202, which may be enhanced
by sufficient pain control8,125,127,132,202,203. Continuous passive motion (CPM) is used by many
authors5,8,9,51,52,125,132,134,135,142,203,204. However, there have been only 2 studies that investigated
the role of CPM in the postoperative management of operative elbow release, one of these
presumably being an extended follow-up of the other with new patients added.132,142 In both
studies, patients had a release for extension loss. In the first study142, a significant greater

PART I CURRENT ISSUES
48
improvement in flexion (and not extension) was found in patients that used CPM compared
with the control group that did not use CPM. This study may have been somewhat biased, as
some of the patients that were treated with CPM had had a more extensive release than did
patients in the other cohort. In addition, patients in the control group were not mobilized until
10 days postoperatively. In the second study132, a significant greater ulnohumeral arc was
found in patients that used CPM. In this study, it was not specified after how many days the
patients in the control group were mobilized. Patients in the cohort that used CPM had
substantially stiffer elbows preoperatively than did patients in the control group. A potential
advantage of CPM would be that it can be used to flex and extend the elbow until the
extremes of motion that were achieved in the operating room are reached. On the other hand,
there has been concern about the formation or recurrence of heterotopic ossification after
forceful manipulation of the elbow21,27, as described above. At our institution, CPM is
prescribed according to the preference of the treating surgeon.64 Continuous passive motion
should not be used if reconstruction of the ligaments was performed.205 Further research
should define the role of CPM in the postoperative management after elbow contracture
release.
Aggressive rehabilitation should be continued at least until no additional gains in motion are
made. A static progressive turnbuckle splint8,9,65,107,119,128,203,206 or a dynamic splint21,52,65,125
may be very helpful to restore a functional arc of motion. Some authors recommend the use of
NSAIDs52 or low-dose irradiation8,21,51,113 postoperatively to prevent recurrence of heterotopic
bone.
When an interposition arthroplasty is performed, motion may be started early. The external
fixator is removed under anesthesia after about 6 to 8 weeks with examination to determine
motion and stability. Gentle manipulation may be performed after removal of the external
fixator. In patients who had a total elbow arthroplasty, the rehabilitation program depends on
the implant that was used, the status of the triceps tendon, the stability as assessed in the
operating room, and the status of the ulnar nerve.182 In patients that have a linked prosthesis,
as is usually the case in the treatment of posttraumatic stiffness, the elbow is rarely unstable.
Regardless of the type of prosthesis, however, all patients will have to comply with guidelines
for upper-limb restrictions (for instance, a 5-lb lifetime weight limit for lifting).182 Gentle
passive stretching may begin for both flexion and extension after about 6 weeks, and gentle
strengthening exercises may be begun after 10 weeks, particularly addressing the triceps. If
the triceps was reflected and reattached during surgery, triceps contraction should be avoided
for 1 month. If the ulnar nerve was not transposed, compression of the nerve during flexion
should be avoided.182 Static progressive or dynamic splinting is rarely indicated after a total
elbow arthroplasty. Return to full activity may be indicated after 12 weeks.
In spite of the lack of knowledge about the pathology underlying the causes of posttraumatic
elbow stiffness, the pessimistic attitude toward surgical intervention for stiff elbow that

LITERATURE REVIEW CHAPTER 2
49
dominated the orthopedic literature of the 20th century has turned more optimistic over the
past 2 decades by the introduction of challenging but relatively safe and effective procedures
to restore elbow function. Heterotopic bone can successfully be resected with only little risk
for complications and good functional outcomes, unless there is complete ankylosis of the
elbow or synostosis of the proximal radioulnar joint.
References
1. Wilson PD. Capsulectomy for the relief of flexion contractures of the elbow following trauma. J Bone Joint Surg 1944;26:71– 86. 2. Doornberg JN, Jupiter JB. The posttraumatic stiff elbow: a historical perspective of treatment. In: Jupiter JB, ed. The stiff elbow. 1st ed. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2006:1–7. 3. Von Gersdorff H. Feldtbuch der Wundarztney. Strassburg: Getruckt durch Joanne Scott, 1517. 4. Smith GE, Jones FW. Report on the Human Remains. Cairo, Egypt: National Printing Department, 1910. 5. Heirweg S, De Smet L. Operative treatment of elbowstiffness: evaluation and outcome. Acta Orthop Belg 2003;69:18 –22. 6. Figgie MP, Inglis AE, Mow CS, Figgie HE III. Total elbow arthroplasty for complete ankylosis of the elbow. J Bone Joint Surg 1989;71A:513–520. 7. Jupiter JB. Assessment and management of the stiff elbow. J Musculoskel Med 2005;22:692– 698. 8. Mansat P, Morrey BF. The column procedure: a limited lateral approach for extrinsic contracture of the elbow. J Bone Joint Surg 1998;80A:1603–1615. 9. Morrey BF. Post-traumatic contracture of the elbow. Operative treatment, including distraction arthroplasty. J Bone Joint Surg 1990;72A:601–618. 10. Schneeberger AG, Adams R, Morrey BF. Semiconstrained total elbow replacement for the treatment of post-traumatic osteoarthrosis. J Bone Joint Surg 1997;79A:1211–1222. 11. Casavant AM, Hastings H II. Heterotopic ossification about the elbow: a therapist’s guide to evaluation and management. J Hand Ther 2006;19:255–266. 12. Ring D, Jupiter JB. Operative release of complete ankylosis of the elbow due to heterotopic bone in patients without severe injury of the central nervous system. J Bone Joint Surg 2003;85A:849–857. 13. Yang SC, Chen AC, Chao EK, Yuan LJ, Lee MS, Ueng SW. Early surgical management for heterotopic ossification about the elbow presenting as limited range of motion associated with ulnar neuropathy. Chang Gung Med J 2002;25:245–252. 14. McKee M, Jupiter J, Toh CL, Wilson L, Colton C, Karras KK. Reconstruction after malunion and nonunion of intraarticular fractures of the distal humerus. Methods and results in 13 adults. J Bone Joint Surg 1994;76B:614–621. 15. Ring D, Jupiter JB. Operative treatment of osteochondral nonunion of the distal humerus. J Orthop Trauma 2006;20: 56–59. 16. Helfet DL, Kloen P, Anand N, Rosen HS. Open reduction and internal fixation of delayed unions and nonunions of fractures of the distal part of the humerus. J Bone Joint Surg 2003;85A:33–40. 17. Regan WD, Reilly CD. Distraction arthroplasty of the elbow. Hand Clin 1993;9:719 –728. 18. Kay NR. Arthrolysis of the post-traumatic stiff elbow. In: Stanley D, Kay NR, eds. Surgery of the elbow. London: Arnold, 1998;228 –234. 19. Urbaniak JR, Hansen PE, Beissinger SF, Aitken MS. Correction of post-traumatic flexion contracture of the elbow by anterior capsulotomy. J Bone Joint Surg 1985;67A: 1160–1164. 20. Viola RW, Hastings H II. Treatment of ectopic ossification about the elbow. Clin Orthop Relat Res 2000;370:65– 86. 21. Itoh Y, Saegusa K, Ishiguro T, Horiuchi Y, Sasaki T, Uchinishi K. Operation for the stiff elbow. Int Orthop 1989;13:263–268. 22. Duke JB, Tessler RH, Dell PC. Manipulation of the stiff elbow with patient under anesthesia. J Hand Surg 1991; 16A:19–24. 23. Stover SL, Hataway CJ, Zeiger HE. Heterotopic ossification in spinal cord-injured patients. Arch Phys Med Rehabil 1975;56:199 –204. 24. Wharton GW, Morgan TH. Ankylosis in the paralyzed patient. J Bone Joint Surg 1970;52A:105–112.

PART I CURRENT ISSUES
50
25. Garland DE, Razza BE, Waters RL. Forceful joint manipulation in head-injured adults with heterotopic ossification. Clin Orthop Relat Res 1982;169:133–138. 26. Thompson HC III, Garcia A. Myositis ossificans: aftermath of elbow injuries. Clin Orthop Relat Res 1967;50:129 –134. 27. Michelsson JE, Rauschning W. Pathogenesis of experimental heterotopic bone formation following temporary forcible exercising of immobilized limbs. Clin Orthop Relat Res 1983;176:265–272. 28. Hoffer MM, Brody G, Ferlic F. Excision of heterotopic ossification about elbows in patients with thermal injury. J Trauma 1978;18:667– 670. 29. Hunt JL, Arnoldo BD, Kowalske K, Helm P, Purdue GF. Heterotopic ossification revisited: a 21-year surgical experience. J Burn Care Res 2006;27:535–540. 30. Garland DE, O’Hollaren RM. Fractures and dislocations about the elbow in the head-injured adult. Clin Orthop Relat Res 1982;168:38–41. 31. Hildebrand KA, Zhang M, van Snellenberg W, King GJ, Hart DA. Myofibroblast numbers are elevated in human elbow capsules after trauma. Clin Orthop Relat Res 2004;419:189 –197. 32. Unterhauser FN, Bosch U, Zeichen J, Weiler A. Alphasmooth muscle actin containing contractile fibroblastic cells in human knee arthrofibrosis tissue. Winner of the AGA-DonJoy Award 2003. Arch Orthop Trauma Surg 2004;124:585–591. 33. Hinz B, Mastrangelo D, Iselin CE, Chaponnier C, Gabbiani G. Mechanical tension controls granulation tissue contractile activity and myofibroblast differentiation. Am J Pathol 2001;159:1009 –1020. 34. Hildebrand KA, Zhang M, Hart DA. High rate of joint capsule matrix turnover in chronic human elbow contractures. Clin Orthop Relat Res 2005;439:228 –234. 35. Akeson WH, Amiel D, Abel MF, Garfin SR, Woo SL. Effects of immobilization on joints. Clin Orthop Relat Res 1987;219:28 –37. 36. Hildebrand KA, Zhang M, Hart DA. Myofibroblast upregulators are elevated in joint capsules in posttraumatic contractures. Clin Orthop Relat Res 2007;456;85–91. 37. Trudel G, Uhthoff HK, Brown M. Extent and direction of joint motion limitation after prolonged immobility: an experimental study in the rat. Arch Phys Med Rehabil 1999;80:1542–1547. 38. Matsumoto F, Trudel G, Uhthoff HK. High collagen type I and low collagen type III levels in knee joint contracture: an immunohistochemical study with histological correlate. Acta Orthop Scand 2002;73:335–343. 39. Cohen MS. Heterotopic ossification of the elbow. In: Jupiter JB, ed. The stiff elbow. 1st ed. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2006:31– 40. 40. Friedenstein AJ, Chailakhyan RK, Gerasimov UV. Bone marrow osteogenic stem cells: in vitro cultivation and transplantation in diffusion chambers. Cell Tissue Kinet 1987;20:263–272. 41. Fijn R, Koorevaar RT, Brouwers JR. Prevention of heterotopic ossification after total hip replacement with NSAIDs. Pharm World Sci 2003;25:138 –145. 42. Kaplan FS, Glaser DL, Hebela N, Shore EM. Heterotopic ossification. J Am Acad Orthop Surg 2004;12:116 –125. 43. Wlodarski KH. Bone histogenesis mediated by nonosteogenic cells. Clin Orthop Relat Res 1991;272:8 –15. 44. DiCesare PE, Nimni ME, Peng L, Yazdi M, Cheung DT. Effects of indomethacin on demineralized bone-induced heterotopic ossification in the rat. J Orthop Res 1991;9:855–861. 45. Ono I, Inoue M, Kuboki Y. Promotion of the osteogenetic activity of recombinant human bone morphogenetic protein by prostaglandin E1. Bone 1996;19:581–588. 46. Neal BC, Rodgers A, Clark T, Gray H, Reid IR, Dunn L, et al. A systematic survey of 13 randomized trials of non-steroidal anti-inflammatory drugs for the prevention of heterotopic bone formation after major hip surgery. Acta Orthop Scand 2000;71:122–128. 47. Jockheck M, Willms R, Volkmann R, Sell S, Weller S, Kusswetter W. Prevention of periarticular heterotopic ossification after endoprosthetic hip joint replacement by means of diclofenac. Arch Orthop Trauma Surg 1998;117:337–340. 48. Reis HJ, Kusswetter W, Schellinger T. The suppression of heterotopic ossification after total hip arthroplasty. Int Orthop 1992;16:140 –145. 49. Gebuhr P, Soelberg M, Orsnes T, Wilbek H. Naproxen prevention of heterotopic ossification after hip arthroplasty.A prospective control study of 55 patients. Acta Orthop Scand 1991;62:226 –229. 50. Vielpeau C, Joubert JM, Hulet C. Naproxen in the prevention of heterotopic ossification after total hip replacement. Clin Orthop Relat Res 1999;369:279 –288.

LITERATURE REVIEW CHAPTER 2
51
51. Boerboom AL, de Meyier HE, Verburg AD, Verhaar JA. Arthrolysis for post-traumatic stiffness of the elbow. Int Orthop 1993;17:346 –349. 52. Cohen MS, Hastings H II. Post-traumatic contracture of the elbow. Operative release using a lateral collateral ligament sparing approach. J Bone Joint Surg 1998;80B:805– 812. 53. Tsionos I, Leclercq C, Rochet JM. Heterotopic ossification of the elbow in patients with burns. Results after early excision. J Bone Joint Surg 2004;86B:396–403. 54. Ellerin BE, Helfet D, Parikh S, Hotchkiss RN, Levin N, Nisce L, et al. Current therapy in the management of heterotopic ossification of the elbow: a review with case studies. Am J Phys Med Rehabil 1999;78:259 –271. 55. Simon AM, Manigrasso MB, O’Connor JP. Cyclo-oxygenase 2 function is essential for bone fracture healing. J Bone Miner Res 2002;17:963–976. 56. Zhang X, Schwarz EM, Young DA, Puzas JE, Rosier RN, O’Keefe RJ. Cyclooxygenase-2 regulates mesenchymal cell differentiation into the osteoblast lineage and is critically involved in bone repair. J Clin Invest 2002;109:1405–1415. 57. Kearney PM, Baigent C, Godwin J, Halls H, Emberson JR, Patrono C. Do selective cyclo-oxygenase-2 inhibitors and traditional non-steroidal anti-inflammatory drugs increase the risk of atherothrombosis? Meta-analysis of randomized trials. Brit Med J 2006;332:1302–1308. 58. Garland DE. A clinical perspective on common forms of acquired heterotopic ossification. Clin Orthop Relat Res 1991;263:13–29. 59. Warren SB. Heterotopic ossification after total hip replacement. Orthop Rev 1990;19:603– 611. 60. Glaser DL, Economides AN, Wang L, Liu X, Kimble RD, Fandl JP, et al. In vivo somatic cell gene transfer of an engineered Noggin mutein prevents BMP4-induced heterotopic ossification. J Bone Joint Surg 2003;85A:2332–2342. 61. Rubenstein JH, Salenius SA, Blitzer PH, Katin MJ, Dosoretz DE. Prevention of heterotopic bone formation with low dose radiation therapy. J Fla Med Assoc 1992;79:828–832. 62. Burd TA, Lowry KJ, Anglen JO. Indomethacin compared with localized irradiation for the prevention of heterotopic ossification following surgical treatment of acetabular fractures. J Bone Joint Surg 2001;83A:1783–1788. 63. Heyd R, Strassmann G, Schopohl B, Zamboglou N. Radiation therapy for the prevention of heterotopic ossification at the elbow. J Bone Joint Surg 2001;83B:332–334. 64. Ring D, Jupiter JB. Excision of heterotopic bone around the elbow. Tech Hand Up Extrem Surg 2004;8:25–33. 65. McAuliffe JA, Wolfson AH. Early excision of heterotopic ossification about the elbow followed by radiation therapy. J Bone Joint Surg 1997;79A:749–755. 66. Virtanen A, Pukkala E, Auvinen A. Incidence of bone and soft tissue sarcoma after radiotherapy: a cohort study of 295,712 Finnish cancer patients. Int J Cancer 2006;118:1017–1021. 67. Kim JH, Chu FC, Woodard HQ, Melamed MR, Huvos A, Cantin J. Radiation-induced soft-tissue and bone sarcoma.Radiology 1978;129:501–508. 68. Yin M, Pacifici M. Vascular regression is required for mesenchymal condensation and chondrogenesis in the developing limb. Dev Dyn 2001;222:522–533. 69. Spielman G, Gennarelli TA, Rogers CR. Disodium etidronate: its role in preventing heterotopic ossification in severe head injury. Arch Phys Med Rehabil 1983;64:539–542. 70. Kaplan FS, Hahn GV, Zasloff MA. Heterotopic ossification: two rare forms and what they can teach us. J Am Acad Orthop Surg 1994;2:288 –296. 71. Kapandji IA, ed. The physiology of joints. 5th ed. Edinburgh, Scotland: Churchill Livingstone, 1982. 72. Yang KH, Park HW, Park SJ, Jung SH. Lateral J-plate fixation in comminuted intercondylar fracture of the humerus. Arch Orthop Trauma Surg 2003;123:234 –238. 73. Schemitsch EH, Tencer AF, Henley MB. Biomechanical evaluation of methods of internal fixation of the distal humerus. J Orthop Trauma 1994;8:468–475. 74. Antuna SA, Morrey BF, Adams RA, O’Driscoll SW. Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: long-term outcome and complications. J Bone Joint Surg 2002;84A:2168–2173. 75. McKee MD, Jupiter JB, Bamberger HB. Coronal shear fractures of the distal end of the humerus. J Bone Joint Surg 1996;78A:49–54. 76. Ring D, Jupiter JB, Gulotta L. Articular fractures of the distal part of the humerus. J Bone Joint Surg 2003;85A:232–238.

PART I CURRENT ISSUES
52
77. Goodman HJ, Choueka J. Complex coronal shear fractures of the distal humerus. Bull Hosp Jt Dis 2005;62:85– 89. 78. Ring D. Elbow stiffness associated with malunion or nonunion. In: Jupiter JB, ed. The stiff elbow. 1st ed. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2006:41–49. 79. Goldberg I, Peylan J, Yosipovitch Z. Late results of excision of the radial head for an isolated closed fracture. J Bone Joint Surg 1986;68A:675–679. 80. Broberg MA, Morrey BF. Results of delayed excision of the radial head after fracture. J Bone Joint Surg 1986;68A:669–674. 81. Doornberg JN, Ring DC. Fracture of the anteromedial facet of the coronoid process. J Bone Joint Surg 2006;88A:2216–2224. 82. Doornberg J, Ring D, Jupiter JB. Effective treatment of fracture-dislocations of the olecranon requires a stable trochlear notch. Clin Orthop Relat Res 2004;429:292–300. 83. Regel G, Weinberg AM, Seekamp A, Blauth M, Tscherne H. Complex trauma of the elbow. Orthopade 1997;26:1020–1029. 84. Ring D, Jupiter JB. Reconstruction of posttraumatic elbow instability. Clin Orthop Relat Res 2000;370:44 –56. 85. Ring D, Hannouche D, Jupiter JB. Surgical treatment of persistent dislocation or subluxation of the ulnohumeral joint after fracture-dislocation of the elbow. J Hand Surg 2004;29A:470–480. 86. Moritomo H, Tada K, Yoshida T, Kawatsu N. Reconstruction of the coronoid for chronic dislocation of the elbow. Use of a graft from the olecranon in two cases. J Bone Joint Surg 1998;80B:490–492. 87. Papandrea RF, Morrey BF, O’driscoll SW. Reconstruction for persistent instability of the elbow after coronoid fracture-dislocation. J Shoulder Elbow Surg 2007;16:68–77 88. Esser RD. Reconstruction of the coronoid process with a radial head fragment. Orthopedics 1997;20:169 –171. 89. Knight RA. The management of fractures about the elbow in adults. Instr Course Lect 1957;14:123–141. 90. Ackerman G, Jupiter JB. Non-union of fractures of the distal end of the humerus. J Bone Joint Surg 1988;70A:75–83. 91. Pugh DM, McKee MD. Advances in the management of humeral nonunion. J Am Acad Orthop Surg 2003;11:48–59. 92. Jupiter JB, Goodman LJ. The management of complex distal humerus nonunion in the elderly by elbow capsulectomy, triple plating, and ulnar nerve neurolysis. J Shoulder Elbow Surg 1992;137– 46. 93. Ring D, Gulotta L, Jupiter JB. Unstable nonunions of the distal part of the humerus. J Bone Joint Surg 2003;85A:1040–1046. 94. Gilchrist AD, McKee MD. Valgus instability of the elbow due to medial epicondyle nonunion: treatment by fragment excision and ligament repair—a report of 5 cases. J Shoulder Elbow Surg 2002;11:493– 497. 95. Papagelopoulos PJ, Morrey BF. Treatment of nonunion of olecranon fractures. J Bone Joint Surg 1994;76B:627– 635. 96. Ring D, Jupiter JB, Gulotta L. Atrophic nonunions of the proximal ulna. Clin Orthop Relat Res 2003;409:268 –274. 97. Waldram MA, Porter KM. Late treatment of non-union of fracture of the olecranon. Injury 1987;18:419–420. 98. Marra G, Morrey BF, Gallay SH, McKee MD, O’Driscoll S. Fracture and nonunion of the olecranon in total elbow arthroplasty. J Shoulder Elbow Surg 2006;15:486–494. 99. Cobb TK, Beckenbaugh RD. Nonunion of the radial neck following fracture of the radial head and neck: case reports and a review of the literature. Orthopedics 1998;21:364–368. 100. Akesson T, Herbertsson P, Josefsson PO, Hasserius R, Besjakov J, Karlsson MK. Primary nonoperative treatment of moderately displaced two-part fractures of the radial head. J Bone Joint Surg 2006;88A:1909–1914. 101. Ring D, Quintero J, Jupiter JB. Open reduction and internal fixation of fractures of the radial head. J Bone Joint Surg 2002;84A:1811–1815. 102. Heim U. Combined fractures of the radius and the ulna at the elbow level in the adult. Analysis of 120 cases after more than 1 year. Rev Chir Orthop Reparatrice Appar Mot 1998;84:142–153. 103. Knight RA, Van Zandt IL. Arthroplasty of the elbow: an end result study. J Bone Joint Surg 1952;24A3:610–618.
LITERATURE REVIEW CHAPTER 2
53
104. Cobb TK, Morrey BF. Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. J Bone Joint Surg 1997;79A:826–832. 105. Morrey BF, Askew LJ, Chao EY. A biomechanical study of normal functional elbow motion. J Bone Joint Surg 1981; 63A:872–877. 106. O’Driscoll SW. Clinical assessment and open and arthroscopic surgical treatment of the stiff elbow. In: Jupiter JB, ed. The stiff elbow. 1st ed. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2006:9 –19. 107. Morrey BF. The stiff elbow with articular involvement. In: Jupiter JB, ed. The stiff elbow. 1st ed. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2006:21–30. 108. Libicher M, Freyschmidt J. Radiological diagnosis in contracted elbow joint. Value of CT and MRI. Orthopade 2001;30:593– 601. 109. Orzel JA, Rudd TG. Heterotopic bone formation: clinical, laboratory, and imaging correlation. J Nucl Med 1985;26:125–132. 110. Pittenger DE. Heterotopic ossification. Orthop Rev 1991;20:33–39. 111. Viola RW, Hanel DP. Early “simple” release of posttraumatic elbow contracture associated with heterotopic ossification. J Hand Surg 1999;24A:370–380. 112. Jupiter JB, Ring D. Operative treatment of post-traumatic proximal radioulnar synostosis. J Bone Joint Surg 1998;80A:248–257. 113. Hastings H II, Graham TJ. The classification and treatment of heterotopic ossification about the elbow and forearm. Hand Clin 1994;10:417– 437. 114. Vince KG, Miller JE. Cross-union complicating fracture of the forearm. Part I: adults. J Bone Joint Surg 1987;69A:640–653. 115. Failla JM, Amadio PC, Morrey BF. Post-traumatic proximal radio-ulnar synostosis. Results of surgical treatment. J Bone Joint Surg 1989;71A:1208–1213. 116. Jupiter JB. Heterotopic ossification about the elbow. J Am Acad Orthop Surg 1991;40:41– 44. 117. Gelinas JJ, Faber KJ, Patterson SD, King GJ. The effectiveness of turnbuckle splinting for elbow contractures. J Bone Joint Surg 2000;82B:74 –78. 118. Schultz-Johnson K. Static progressive splinting. J Hand Ther 2002;15:163–178. 119. Doornberg JN, Ring D, Jupiter JB. Static progressive splinting for posttraumatic elbow stiffness. J Orthop Trauma 2006;20:400–404. 120. Green DP, McCoy H. Turnbuckle orthotic correction of elbow-flexion contractures after acute injuries. J Bone Joint Surg 1979;61A:1092–1095. 121. Bonutti PM, Windau JE, Ables BA, Miller BG. Static progressive stretch to reestablish elbow range of motion. Clin Orthop Relat Res 1994;303:128 –134. 122. Shewring DJ, Beaudet M, Carvell JE. Reversed dynamic slings: results of use in the treatment of post-traumatic flexion contractures of the elbow. Injury 1991;22:400–402. 123. Dickson RA. Reversed dynamic slings. A new concept in the treatment of post-traumatic elbow flexion contractures. Injury 1976;8:35–38. 124. Richard R, Shanesy CP III, Miller SF. Dynamic versus static splints: a prospective case for sustained stress. J Burn Care Rehabil 1995;16(3 Pt 1):284 –287. 125. Husband JB, Hastings H II. The lateral approach for operative release of post-traumatic contracture of the elbow. J Bone Joint Surg 1990;72A:1353–1358. 126. Kraushaar BS, Nirschl RP, Cox W. A modified lateral approach for release of posttraumatic elbow flexion contracture. J Shoulder Elbow Surg 1999;8:476–480. 127. van Eijck GJ, Poets JJ, van der Werken C. Surgical arthrolysis for posttraumatic stiffening of elbow and knee joints. Neth J Surg 1991;43:252–257. 128. Ring D, Adey L, Zurakowski D, Jupiter JB. Elbow capsulectomy for posttraumatic elbow stiffness. J Hand Surg 2006;31A:1264–1271. 129. Cikes A, Jolles BM, Farron A. Open elbow arthrolysis for posttraumatic elbow stiffness. J Orthop Trauma 2006;20:405–409. 130. Tan V, Daluiski A, Simic P, Hotchkiss RN. Outcome of open release for post-traumatic elbow stiffness. J Trauma 2006;61:673– 678. 131. Marti RK, Kerkhoffs GM, Maas M, Blankevoort L. Progressive surgical release of a posttraumatic stiff elbow. Technique and outcome after 2–18 years in 46 patients. Acta Orthop Scand 2002;73:144 –150. 132. Aldridge JM III, Atkins TA, Gunneson EE, Urbaniak JR. Anterior release of the elbow for extension loss. J Bone Joint Surg 2004;86A:1955–1960.
PART I CURRENT ISSUES
54
133. Wada T, Ishii S, Usui M, Miyano S. The medial approach for operative release of post-traumatic contracture of the elbow. J Bone Joint Surg 2000;82B:68 –73. 134. Amillo S. Arthrolysis in the relief of post-traumatic stiffness of the elbow. Int Orthop 1992;16:188 –190. 135. Chantelot C, Fontaine C, Migaud H, Remy F, Chapnikoff D, Duquennoy A. [Retrospective study of 23 arthrolyses of the elbow for post-traumatic stiffness: result predicting factors]. Rev Chir Orthop Reparatrice Appar Mot 1999;85:823–827. 136. Stans AA, Maritz NG, O’Driscoll SW, Morrey BF. Operative treatment of elbow contracture in patients twenty-one years of age or younger. J Bone Joint Surg 2002;84A:382–387. 137. Weizenbluth M, Eichenblat M, Lipskeir E, Kessler I. Arthrolysis of the elbow. 13 cases of posttraumatic stiffness. Acta Orthop Scand 1989;60:642– 645. 138. Gosling T, Blauth M, Lange T, Richter M, Bastian L, Krettek C. Outcome assessment after arthrolysis of the elbow. Arch Orthop Trauma Surg 2004;124:232–236. 139. Bae DS, Waters PM. Surgical treatment of posttraumatic elbow contracture in adolescents. J Pediatr Orthop 2001;21:580 –584. 140. Park MJ, Kim HG, Lee JY. Surgical treatment of posttraumatic stiffness of the elbow. J Bone Joint Surg 2004;86B:1158–1162. 141. Olivier LC, Assenmacher S, Setareh E, Schmit-Neuerburg KP. Grading of functional results of elbow joint arthrolysis after fracture treatment. Arch Orthop Trauma Surg 2000;120:562–569. 142. Gates HS III, Sullivan FL, Urbaniak JR. Anterior capsulotomy and continuous passive motion in the treatment of post-traumatic flexion contracture of the elbow. A prospective study. J Bone Joint Surg 1992;74A:1229–1234. 143. Ball CM, Meunier M, Galatz LM, Calfee R, Yamaguchi K. Arthroscopic treatment of post-traumatic elbow contracture. J Shoulder Elbow Surg 2002;11:624–629. 144. Jones GS, Savoie FH III. Arthroscopic capsular release of flexion contractures (arthrofibrosis) of the elbow. Arthroscopy 1993;9:277–283. 145. Timmerman LA, Andrews JR. Arthroscopic treatment of posttraumatic elbow pain and stiffness. Am J Sports Med 1994;22:230 –235. 146. Nowicki KD, Shall LM. Arthroscopic release of a posttraumatic flexion contracture in the elbow: a case report and review of the literature. Arthroscopy 1992;8:544 –547. 147. Kim SJ, Kim HK, Lee JW. Arthroscopy for limitation of motion of the elbow. Arthroscopy 1995;11:680–683. 148. Kim SJ, Shin SJ. Arthroscopic treatment for limitation of motion of the elbow. Clin Orthop Relat Res 2000;375:140–148. 149. Kelly EW, Bryce R, Coghlan J, Bell S. Arthroscopic debridement without radial head excision of the osteoarthritic elbow. Arthroscopy 2007;23:151–156. 150. Strobel MJ, Eckardt OA, Eichhorn HJ. Arthroscopic therapy in limited mobility of the elbow joint. Orthopade 2001;30:610–618. 151. Phillips BB, Strasburger S. Arthroscopic treatment of arthrofibrosis of the elbow joint. Arthroscopy 1998;14:38–44. 152. McGinty JB. Operative arthroscopy. New York: Raven Press, 1991:583– 603. 153. Parisien JS. Techniques in therapeutic arthroscopy. New York: Raven Press, 1993:21.1–21.14. 154. Morrey BF. Posttraumatic stiffness: distraction arthroplasty. Orthopedics 1992;15:863– 869. 155. Aldridge JM III, Lightdale NR, Mallon WJ, Coonrad RW. Total elbow arthroplasty with the Coonrad/Coonrad-Morrey prosthesis. A 10- to 31-year survival analysis. J Bone Joint Surg 2006;88B:509 –514. 156. Hausman MR, Birnbaum PS. Interposition elbow arthroplasty. Tech Hand Up Extrem Surg 2004;8:181–188. 157. Mansat P, Morrey BF. Semiconstrained total elbow arthroplasty for ankylosed and stiff elbows. J Bone Joint Surg 2000;82A:1260–1268. 158. Cheng SL, Morrey BF. Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg 2000;82B:233–238. 159. Cohen MS, Hastings H II. Operative release for elbow contracture: the lateral collateral ligament sparing technique.Orthop Clin North Am 1999;30:133–139. 160. Thoreux P, Blondeau C, Durand S, Masquelet AC. Anatomical basis of arthroscopic capsulotomy for elbow stiffness. Surg Radiol Anat 2006;28:409–415.

LITERATURE REVIEW CHAPTER 2
55
161. O’Driscoll SW, Horii E, Carmichael SW, Morrey BF. The cubital tunnel and ulnar neuropathy. J Bone Joint Surg 1991;73B:613– 617. 162. Mezera K, Hotchkiss RN. Fractures and dislocations of the elbow. In: Bucholz RW, Heckman JD, eds. Rockwood and Green’s fractures in adults. 5th ed. Philadelphia: Lippincott Williams & Wilkins, 2001:921–952. 163. Ring D, Jupiter JB. Operative release of ankylosis of the elbow due to heterotopic ossification. Surgical technique. J Bone Joint Surg 2004;86A(Suppl 1):2–10. 164. Baciu CC, Dobre I, Mirsu F, Duma A. [Long-term results of mobilization by bone resection in patients with posttraumatic total stiffness and ankylosis of the elbow. Study and results of 39 operations]. Rev Chir Orthop Reparatrice Appar Mot 1990;76:375–382. 165. Gallay SH, Richards RR, O’Driscoll SW. Intraarticular capacity and compliance of stiff and normal elbows. Arthroscopy 1993;9:9 –13. 166. O’Driscoll SW, Morrey BF, An KN. Intraarticular pressure and capacity of the elbow. Arthroscopy 1990;6:100 –103. 167. Kelly EW, Morrey BF, O’Driscoll SW. Complications of elbow arthroscopy. J Bone Joint Surg 2001;83A:25–34. 168. Jupiter JB, O’Driscoll SW, Cohen MS. The assessment and management of the stiff elbow. Instr Course Lect 2003;52:93–111. 169. Lindenfeld TN. Medial approach in elbow arthroscopy. Am J Sports Med 1990;18:413– 417. 170. Lynch GJ, Meyers JF, Whipple TL, Caspari RB. Neurovascular anatomy and elbow arthroscopy: inherent risks. Arthroscopy 1986;2:190 –197. 171. Marshall PD, Fairclough JA, Johnson SR, Evans EJ. Avoiding nerve damage during elbow arthroscopy. J Bone Joint Surg 1993;75B:129 –131. 172. Miller CD, Jobe CM, Wright MH. Neuroanatomy in elbow arthroscopy. J Shoulder Elbow Surg 1995;4:168 –174. 173. Froimson AI. Fascial interposition arthroplasty of the elbow. In: Morrey BF, ed. The elbow. 1st ed. New York: Raven Press, 1994:329 –342. 174. Wright PE, Froimson AI, Stewart M J. Interposition arthroplasty of the elbow. In: Morrey BF, ed. The elbow and its disorders. 2nd ed. Philadelphia: W.B. Saunders, 1993:611–622. 175. Froimson AI, Silva JE, Richey D. Cutis arthroplasty of the elbow joint. J Bone Joint Surg 1976;58A:863–865. 176. Fox RJ, Varitimidis SE, Plakseychuk A, Vardakas DG, Tomaino MM, Sotereanos DG. The compass elbow hinge: indications and initial results. J Hand Surg 2000;25B:568–572. 177. Modabber MR, Jupiter JB. Reconstruction for post-traumatic conditions of the elbow joint. J Bone Joint Surg 1995;77A:1431–1446. 178. Ljung P, Jonsson K, Larsson K, Rydholm U. Interposition arthroplasty of the elbow with rheumatoid arthritis. J Shoulder Elbow Surg 1996;5(2 Pt 1):81– 85. 179. Morrey BF. Distraction arthroplasty. Clinical applications. Clin Orthop Relat Res 1993;293:46 –54. 180. Blaine TA, Adams R, Morrey BF. Total elbow arthroplasty after interposition arthroplasty for elbow arthritis. J Bone Joint Surg 2005;87A:286–292. 181. Gramstad GD, King GJ, O’Driscoll SW, Yamaguchi K. Elbow arthroplasty using a convertible implant. Tech Hand Up Extrem Surg 2005;9:153–163. 182. Szekeres M, King GJ. Total elbow arthroplasty. J Hand Ther 2006;19:245–253. 183. O’Driscoll SW, An KN, Korinek S, Morrey BF. Kinematics of semi-constrained total elbow arthroplasty. J Bone Joint Surg 1992;74B:297–299. 184. Moro JK, King GJ. Total elbow arthroplasty in the treatment of posttraumatic conditions of the elbow. Clin Orthop Relat Res 2000;370:102–114. 185. McKee MD, Jupiter JB, Bosse G, Goodman L. Outcome of ulnar neurolysis during post-traumatic reconstruction of the elbow. J Bone Joint Surg 1998;80B:100 –105. 186. Schneeberger AG, Meyer DC, Yian EH. Coonrad-Morrey total elbow replacement for primary and revision surgery: a 2- to 7.5-year follow-up study. J Shoulder Elbow Surg 2007;16(suppl):544 –554. 187. Kraay MJ, Figgie MP, Inglis AE, Wolfe SW, Ranawat CS. Primary semiconstrained total elbow arthroplasty. Survival analysis of 113 consecutive cases. J Bone Joint Surg 1994;76B:636–640. 188. Hildebrand KA, Patterson SD, Regan WD, MacDermid JC,King GJ. Functional outcome of semiconstrained total elbow arthroplasty. J Bone Joint Surg 2000;82A:1379–1386.
PART I CURRENT ISSUES
56
189. Sneftrup SB, Jensen SL, Johannsen HV, Sojbjerg JO. Revision of failed total elbow arthroplasty with use of a linked implant. J Bone Joint Surg 2006;88B:78–83. 190. King GJ, Adams RA, Morrey BF. Total elbow arthroplasty: revision with use of a non-custom semiconstrained prosthesis.J Bone Joint Surg 1997;79A:394–400. 191. Thillemann TM, Olsen BS, Johannsen HV, Sojbjerg JO. Long-term results with the Kudo type 3 total elbow arthroplasty. J Shoulder Elbow Surg 2006;15:495– 499. 192. Athwal GS, Morrey BF. Revision total elbow arthroplasty for prosthetic fractures. J Bone Joint Surg 2006;88A:2017–2026. 193. Lee BP, Adams RA, Morrey BF. Polyethylene wear after total elbow arthroplasty. J Bone Joint Surg 2005;87A: 1080–1087. 194. Celli A, Arash A, Adams RA, Morrey BF. Triceps insufficiency following total elbow arthroplasty. J Bone Joint Surg 2005;87A:1957–1964. 195. van der Lugt JC, Geskus RB, Rozing PM. Limited influence of prosthetic position on aseptic loosening of elbow replacements: 125 elbows followed for an average period of 5.6 years. Acta Orthop 2005;76:654–661. 196. Figgie MP, Su EP, Kahn B, Lipman J. Locking mechanism failure in semiconstrained total elbow arthroplasty. J Shoulder Elbow Surg 2006;15:88 –93. 197. Wolfe SW, Figgie MP, Inglis AE, Bohn WW, Ranawat CS. Management of infection about total elbow prostheses. J Bone Joint Surg 1990;72A:198–212. 198. Wright TW, Hastings H. Total elbow arthroplasty failure due to overuse, C-ring failure, and/or bushing wear. J Shoulder Elbow Surg 2005;14:65–72. 199. Schneeberger AG, Hertel R, Gerber C. Total elbow replacement with the GSB III prosthesis. J Shoulder Elbow Surg 2000;9:135–139. 200. Yamaguchi K, Adams RA, Morrey BF. Infection after total elbow arthroplasty. J Bone Joint Surg 1998;80A:481–491. 201. Gutow AP, Wolfe SW. Infection following total elbow arthroplasty. Hand Clin 1994;10:521–529. 202. Davila SA, Johnston-Jones K. Managing the stiff elbow: operative, nonoperative, and postoperative techniques. J Hand Ther 2006;19:268 –281. 203. Morrey BF. Surgical treatment of extraarticular elbow contracture. Clin Orthop Relat Res 2000;370:57– 64. 204. Breen TF, Gelberman RH, Ackerman GN. Elbow flexion contractures: treatment by anterior release and continuous passive motion. J Hand Surg 1988;13B:286 –287. 205. O’Driscoll SW. Continuous passive motion. In: Morrey BF, ed. The elbow and its disorders. 3rd ed. Philadelphia:Saunders, 2000:147–149. 206. Morrey BF. The posttraumatic stiff elbow. Clin Orthop Relat Res 2005;431:26-35.



����� ����������������
