uva-dare (digital academic repository) functional … · doublefor mmnucleimostprominentinth...
TRANSCRIPT

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Functional recovery after liver resection
Veteläinen, R.L.
Link to publication
Citation for published version (APA):Veteläinen, R. L. (2006). Functional recovery after liver resection
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: http://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 28 May 2018

CL L a a SZ SZ u u
Reetaa Vetelainen
Dehaa Erdogan
Wilmarr de Graaf
Fiboo ten Kate
Peterr LM Jansen
Dirkk J Gouma
Thomass M van Gulik

hJ^l-^maa a


Introduction n < <
Hepatocellularr adenoma (HCA) is a benign solitary liver lesion which mostly occurs in young Ui
w o m a nn w i th a history of oral contraceptive use (OCC) and cessation of OCC may regress the nodule fD
sizee (1,2,3). Flejou et al def ined liver adenomatosis (LA) as the presence of multiple (arbitrary >10), o
adenomass scattered throughout normal liver parenchyma in a patient w i th no history of steroid g
therapyy or glycogen storage disease (4,5). Contradictory to Flejou, recent reports show female £
predominancee and relation w i th OCC (6,7). —*
Clinicall presentation of LA relates to the size of the largest nodule causing abdominal symptoms 5 *
(4).. Larger nodules of ten present wi th intralesional haemorrhage that may rupture w i th in the j£
peritoneall cavity (6,8). In literature, the preferred management for symptomatic patients is £2
resectionn of the larger tumor(s) (2,6,9). The potential risk of malignant transformation has also 2
warrantedd orthotopic liver transplantation as the recommended treatment (2,4). Recent reports,
however,, favor a more conservative approach and surgery is recommended for more aggressively
growingg lesions (5,7). In addition, less invasive embolization methods has been proposed. However,
duee to the rarity of the disease, the optimal management and prognosis remain unclear and there
aree no established guidelines for the management of patients wi th LA.
Diseasee etiology is also uncertain which hampers effective therapy of this disease. A recent study
reportss the presence of nonalcoholic steatohepatitis in a patient w i th LA (10) and there is also
growingg evidence of a connection between altered glucose metabolism and LA through germline
mutationss in hepatocyte nuclear factor (HNF) -1a (11,12). As altered glucose metabolism and
nonalcoholicc fat ty liver disease (NAFLD) are closely connected, a relationship between LA and
NAFLDD is also possible. The main focus of this study is to identify novel features associated w i th
LAA that may have impact on surgical management and the short and long-term prognosis of these
patients.. We also discuss innovative treatment strategies potentially applicable to patients wi th LA.
Materialss and methods
Thee patient database of Academic Medical Center (AMC) in Amsterdam between 1997 and
20066 was analyzed . For the definition of LA, the presence of multiple hepatic (>10) nodules and
thee exclusion of patients with glycogen storage disease or previous steroid therapy was used.
Thee definitive diagnosis was based on imaging studies and/or histopathology by an experienced
pathologist.. Furthermore, clinical status, laboratory and radiological evaluation, histopathology,
surgicall management and outcome were reviewed. All published case reports and series were
reviewedd and analyzed in detail (1-12, 14-44). A search in the Medline (1 January 1963 to January
2006)) was performed using MESH terms liver adenoma and liver adenomatosis. Patients from
ourr own series and from the literature were combined and analyzed by commercial computer
packagee (SPSS 10.1.).
163 3
Results s
Demographics s
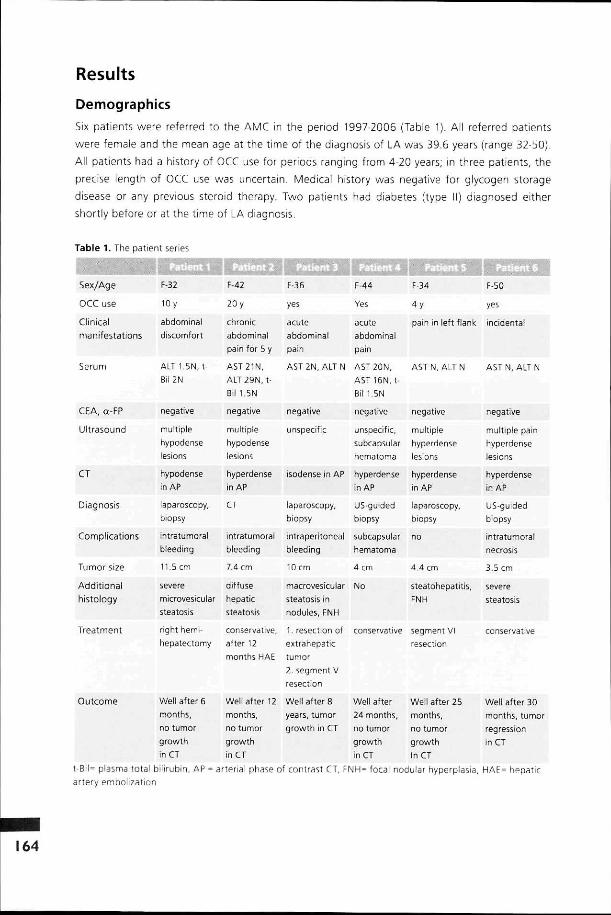
Sixx patients were referred to the AMC in the period 1997-2006 (Table 1). All referred patients
weree female and the mean age at the time of the diagnosis of LA was 39.6 years (range 32-50).
Alll patients had a history of OCC use for periods ranging from 4-20 years; in three patients, the
precisee length of OCC use was uncertain. Medical history was negative for glycogen storage
diseasee or any previous steroid therapy. Two patients had diabetes (type II) diagnosed either
shortlyy before or at the time of LA diagnosis.
Tablee 1. The patient series
Sex/Age e
OCCC use
Clinical l manifestations s
Serum m
CEA,, a-FP
Ultrasound d
CT T
Diagnosis s
Complications s
Tumorr size
Additional l histology y
Treatment t
F-32 2
100 y
abdominal l discomfort t
ALTT 1.5N, t-Bil2N N
negative e
multiple e
hypodense e lesions s
hypodense e inn AP
laparoscopy, , biopsy y
intratumoral l bleeding g
11.55 cm
severe e microvesicular r
steatosis s
rightt hemi-hepatectomy y
F-42 2
200 y
chronic c abdominal l painn for 5 y
AST21N, , ALTT 29N. t-Bill 1.5N
negative e
multiple e hypodense e lesions s
hyperdense e inn AP
CT T
intratumoral l bleeding g
7.44 cm
diffuse e hepatic c steatosis s
conservative, , afterr 12
F-36 6
yes s
acute e abdominal l pain n
ASTT 2N, ALT N
negative e
unspecific c
isodensee in AP
laparoscopy. . biopsy y
intraperitoneal l bleeding g
100 cm
macrovesicular r
steatosiss in nodules,, FNH
1.. resection of
extrahepatic c
F-44 4
Yes s
acute e abdominal l pain n
AST20N, , ASTT 16N, t-Bill 1.5N
negative e
unspecific, , subcapsular r hematoma a
hyperdense e inAP P
US-guided d biopsy y
subcapsular r hematoma a
44 cm
No o
conservative e
F-34 4
4y y
painn in left flank
ASTT N, ALT N
negative e
multiple e hyperdense e lesions s
hyperdense e inAP P
laparoscopy, , biopsy y
no o
4.44 cm
steatohepatitis, , FNH H
segmentt VI resection n
F-50 0
yes s
incidental l
ASTT N, ALT N
negative e
multiplee pain hyperdense e lesions s
hyperdense e inAP P
US-guided d biopsy y
intratumoral l necrosis s
3.55 cm
severe e steatosis s
conservative e
monthss HAE tumor 2.. segment V resection n
Outcome e Welll after 6 months, , noo tumor growth h inCT T
Welll after 12 months, , noo tumor growth h inCT T
Welll after 8 years,, tumor growthh in CT
Welll after Well after 25 244 months, months, noo tumor no tumor growthh growth inn CT In CT
Welll after 30 months,, tumor regression n inCT T
t-Bil== plasma total bilirubin, AP = arterial phase of contrast CT, FNH= focal nodular hyperplasia, HAE= hepatic arteryy embolization
164 4

Diagnosticc modalities
Elevationn of liver enzymes and bilirubin was seen in four patients of our own series (table 1). In
alll patients, blood coagulation values were normal and tumor markers (CEA, a-fetoprotein) and
hepatitiss markers (B, C) negative. Five patients were symptomatic at the time of the LA diagnosis. In
patientt 6, LA was incidentally diagnosed during US-examination performed in relation with severe
obesitas.. One patient presented with an unspecific abdominal swelling and others with acute pain
inn the left flank, right epigastric area or unspecifically in the abdomen. The size of the largest tumors
rangedd from 3.5 cm to 11.5 cm without a direct relation with the severity of the symptoms as the
patientt with the largest single tumor had only abdominal discomfort and no actual pain.
Abdominall US was the initial imaging modality applied in all patients, followed by contrast-
enhancedd CT. The presentation of nodules in US and CT is summarized in Table 2. In patient
1,, US-guided liver biopsy was suspicious of hepatocellular carcinoma but additional diagnostic
laparoscopyy with a new biopsy was negative for malignancy. In patients 5 and 6, US-guided
biopsyy was performed and histopathology was typical of HCA, without signs of malignancy.
Additionally,, 99mTc-RBC scintigraphy was performed in patient 1, because unclear diagnosis
afterr US, CT and US-guided biopsy. Scintigraphy showed atypical findings for hemangioma; a
malignancyy could not be excluded.
< < O O T T P P Q. Q. O O 3 3 O O
P P r t t O O 1/1 1
C C
Tablee 2. Review of patient characteristics
Age e
Male e
Female e
OCC C Yes s
Tumorr characteristics
Primary y
symptoms s
Tumorr size
Bleeding g
N o / / incidental l
Acutee pain
Chronicc pain
Pain# #
Hepatomegaly y
Non-specific c
Gll -symptoms
Meann (range) (nn of patients)
No o
ITN N
ITB* *
IPB** *
94 4
34.0(12-75) )
12%% (11)
88%% (83)
52% % (43/83) )
26%% (24)
43%% (40)
16%% (15)
9%% (8)
31%% (29)
7%% (7)
47%% (44)
2%% (2)
26%% (24)
20%% (19)
21%% (20)
37.77 (14-75)
5%% (1)
95%% (19)
50%% (10)
25%% (5)
30%% (6)
25%% (5)
15%% (3)
40%% (8)
15%% (3)
3.6(2--4.5)09) )
65%% (13)
5%% (1)
20%% (4)
10%% (2)
53%% (51)
33.9(12--54) )
12%% (6)
88%% (45)
57%% (29)
22%% (11)
59%% (30)
6%% (3)
8%% (4)
20%% (10)
4%% (2)
7.8(5-15) ) (51) )
47%% (24)
2%(1) )
26%% (13)
26%% (13)
26%% (23)
32.3(13--
53) )
17%% (4)
83%% (19)
22%% (5)
35%% (8)
17%% (4)
35%% (8)
4%% (1)
48%% (11)
8%% (2)
unknown n
30%% (7)
28%% (7)
16%% (4)
25%% (24)
32.5(13--53) )
17%% (4)
83%% (20)
54%% (13)
100%% (24)
13%% (3)
5.4(3-8) )
(15) )
67%% (16)
4%(1) )
13%% (3)
8%% (2)
75%% (70)
34.77 (12-75)
10%% (7)
90%% (63)
44%% (31)
57%% (41)
23%% (16)
11%% (8)
37%% (26)
10%% (7)
7.0(2-15) ) (55) )
40%% (29)
3%% (2)
30%% (21)
24%% (17)
165 5

Variables s Totall Tumor size 1 Tumor J Unknown j Asymptomatic <5cm<5cm I size j j Symptomatic
53%% (51) 26% (23) 25% (24) 75% (70)
Age e
Male e
Female e
OCC C Yes s
Tumorr characteristics
Primary y
symptoms s N o / /
incidental l
34.0(12-75) )
12%% (11)
88%% (83)
52% % (43/83) )
26%% (24)
37.7(14-75) )
5%(1) )
95%% (19)
50%% (10)
25%% (5)
33.99 (12-54) )
12%% (6)
88%% (45)
57%% (29)
22%% (11)
32.33 (13-
53) )
17%% (4)
83%% (19)
22%% (5)
35%% (8)
32.5(13-53) )
17%% (4)
83%% (20)
54%% (13)
100%% (24)
34.7(12-75) )
10%% (7)
90%% (63)
44%% (31)
Managementt and Outcome
Surgicall treatment
Initiall management consisted of surgical resection of the largest lesion in three patients (patients 1,
33 and 5). In patient 1, preoperative right portal vein embolization (PVE) was performed to increase
remnantt liver volume in the presence of severe steatosis. Subsequently, right hemihepatectomy
extendedd with resection of half of segment 4a was performed without complications. In patient
3,, a LA lesion hanging from the liver was resected laparoscopically and was complicated by
bleeding.. At subsequent laparotomy, the largest nodule located in the segment 5 was resected
becausee of intended pregnancy. The patient has been asymptomatic during a follow-up time of
88 years; however, the size and number of nodules have slightly increased on CT. Also in patient
5,, the largest nodule located in segment 6 was resected without complications. Follow-up of 25
monthss has been uneventful and patient is pain-free.
Conservativee treatment
Initially,, three patients (patients 2, 4 and 6) were observed including cessation of OCC medication.
Inn patient 2, the diameter of the largest nodule had increased after 12 months on follow-up
CT.. Because the patient also had abdominal discomfort, percutaneous selective embolization of
thee nodule via the hepatic artery was undertaken. Follow-up of 12 months was uneventful and
noo change in nodule size or number were detected on CT. Patient 4 who presented with an
intrahepaticc bleeding was treated conservatively and after 2 months, resolution of a subcapsular
hematomaa was seen on CT with signs of recent bleeding. In addition, multiple lesions (0 2-4
cm)) were detected in segments 2-4. Follow-up was uneventful for 24 months and the patient is
currentlyy symptom-free. Patient 6 was observed and after withdrawal of OCC, reduction of lesion
sizee was observed. At 30 months after diagnosis of LA, no nodules were detected on CT.
Histopathology y
Inn all our patients the histopathology of the nodules met with the previously reported criteria
forr benign adenoma (13). All nodules showed cell plate 1-3 layers thick in the reticulin stain with
intactt reticulin pattern. The lesional hepatocytes showed cellular proliferation, variable sized and

double-formm nuclei most prominent in the largest nodules. In the nodules, the arterialization, small
arteries,, derived {CD-34 positive cells) from sinusoidal beds. The non-lesional hepatic parenchyma
showedd intact architecture with regular central veins and portal fields. In the portal fields and
aroundd central veins inflammatory cells with segment patterned nuclei were present.
Inn three patients, a resection specimen and in two patients, a representative needle biopsy was
availablee for histopathological evaluation. In patient 4, a biopsy obtained under US-guidance was
consideredd inadequate for reliable evaluation.
Inn patients 1 and 3, presenting with the largest tumors, i.e. 11.5 cm and 10 cm, respectively, the
tumorss were macroscopically encapsulated with intratumor necrosis. The smaller tumors were
mostlymostly encapsulated and well demarcated from the surrounding hepatic parenchyma.
Inn 4 patients, steatosis was present in the non-lesional hepatic parenchyma surrounding the
nodules.. In all patients steatosis was of the severe type, involving more than 60% of all hepatocytes.
Patientt 1 presented with severe, centrilobularly focated, mtcrovestcular steatosis, patient 3 with
severee macrovesicular steatosis and patient 6 with severe micro- and macrovesicular steatosis.. In
patientt 5, steatosis had developed into steatohepatitis with fibrosis. In addition, patients 3 and
55 had also a single FNH lesion among multiple LA nodules. The overall non-lesional parenchyma
showedd intact cellular architecture with regular central veins and portal fields in all patients.
Discussion n
Demographics s Wee report the largest review so far of 94 patients with LA collected to date, consisting of all
publishedd case reports and all small series including our own series (Table 2). Only descriptive data
analysiss was performed because of the heterogeneous source of data. Strong female predilection
inn incidence of LA suggested in literature was also seen in our review (6,7). Of all patients, 52%
off females had a history of OCC use. Eight patients were younger than 18 years and 12% were
malee (Table 2). As estrogen/progesterone-positive and negative receptors can be unevenly found
inn LA nodules, it seems that the role of exogenous estrogen is not important in induction of LA
butt might play a role in disease progression (5). In our analysis a slightly higher incidence of OCC
usee was seen in females with larger tumor sizes, i.e. > 5cm.
Etiology y Thee etiology of LA remains unclear and a variety of predisposing conditions have been suggested.
Congenitall or acquired hepatic vascular abnormalities tend to occur more often in patients with
FNHH and HCA. Of all patients, 8 had a concomitant single lesion of FNH and some presented with
co-extstingg vascular malformations suggesting some role for vascular abnormalities (6,7,23,29).
Thee first connection between LA and diabetes was reported in 1978 (19). Interestingly, 2 of our
ownn patients had diabetes {type II) diagnosed at the time of LA diagnosis. Unfortunately, diabetes
wass assessed only in few reviewed studies (10,11,12,19). Recent studies report a familial autosomal
transmissionn of LA in one family and a familial type of LA linked with germline mutations of HNF-1a
inn two families (6,12). These mutations are associated with a rare form of diabetes, a non-ketotic
typee present in patients younger than 25 years (11-12). HNF - la mutation could present a genetic
predispositionn and LA would develop in presence of another factor because the expression of

thee mutation phenotype was variable within the families (12). This can be a vascular anomaly or
somaticc mutation in another allele. Unfortunately, HNF - la detection by immunohistochemistry is
nott yet possible in paraffin-preserved tissue samples and therefore, this analysis was not possible
inn our own patient series.
Thee etiology of NAFLD has close connection with western lifestyle and is therefore considered
aa rising clinical challenge (45). An association between LA and NAFLD was recently suggested
(10).. Interestingly 18% of all LA patients had steatosis, varying from mild to steatohepatitis. In
ourr own series, 5 of 6 patients had steatosis along with LA. Three patients had histologically
confirmedd steatosis; one patient had severe macrovesicular, one severe microvesicular and one
hadd combined micro- and macrovesicular steatosis. In addition, one patient had diffuse steatosis
diagnosedd by US. Furthermore, one patient had steatohepatitis, which is second ever published
inn the literature (10).
LAA nodules typically show steatosis but it seems that the co-existence of non-tumoral steatosis
hass increased during the last years. This might in part be explained by increased risk factors for
steatosiss and recognition of steatosis as a potential risk factor in liver surgery. However, LA is
diagnosedd also in young, lean adults and children. Furthermore, the microvesicular type of steatosis
iss not commonly connected with obesity-related steatosis as opposed to the macrovesicular type.
Thee microvesicular steatosis is often seen in patients with more acutely induced steatosis, such as
byy toxins or drugs. Glycogen storage disease induces rapid and massive LA, presenting often in
childrenn younger than 5 years (2). Therefore, considering all these aspects, etiology of LA has a
potentiall connection to deranged hepatic glucose metabolism with a yet unknown mechanism.
Furtherr research is needed to unravel this aspect.
Thee diagnosis tntn 43% of all analyzed patients with LA (including the literature and our own series), clinical
presentationn was with acute pain. However, in contrast to previous reports, the diagnosis was
fortuitouss in 25% of patients. Early diagnosis is vital, as hemorrhage is a common complication
inn patients with LA. In literature, an overall bleeding rate from 46% to 63% is reported (4,5) In
ourr analysis, the overall bleeding rate was 46% and had in two cases led to death (6, 23). In
54%% of symptomatic patients, intraperitoneal or intratumoral bleeding was present at the time of
diagnosis.. The actual prevalence of hemorrhage is difficult to estimate as symptomatic patients
aree more likely to seek medical help thus creating a selection bias. However, of all asymptomatic
patientss with incidentally discovered LA, only 8% had intraperitoneal and 13% had intratumoral
bleeding. .
Inn patients with intra-abdominal bleeding, LA is diagnosed on CT or during emergency laparotomy.
However,, in less acute patients the diagnosis is more complicated. As seen in our series (Table
1)) and in literature, plasma liver enzymes are unreliable with poor correlation with LA. Most
symptomaticc patients presented with epigastric or abdominal pain or discomfort of acute or chronic
onsett (Table 2). Additional symptoms include gastrointestinal complaints and hepatomegaly
(4,6,32).. During diagnostic work-up, several differential diagnoses might emerge, because of
diversityy of the LA tissue components such as necrosis, fat, calcification and hemorrhage, present
ass a variety of hypo-, iso- and/or hyperdense radiological features. Grazioli et al concluded that
thee most useful method for initial diagnosis is multiphase-helical CT or MRI (7). Most adenomas
weree uniformly or heterogeneousiy hyperattenuatmg lesions during the arterial phase like in our
series.. However, noncontrast images are needed for identification of local fat and hemorrhage
andd portal phase images for evaluation of vascular anomalies (7). A potential modality to identify
co-existingg steatosis is nuclear magnetic resonance spectroscopy ('H-MRS) providing a sensitive
andd quantitative technique to measure intrahepatic fat content (46). The obvious advantage of
'H-MRSS is that it samples noninvasively a considerably larger liver volume than standard liver
biopsy.. With ^-MRS the analysis of various liver lobes and/or regions is also possible, diminishing
thee bias introduced by heterogeneity of distribution of hepatic fat (46,47).
Evenn though imaging is useful in lesion identification, the total number of lesions detected during
surgeryy is usually higher because of the extensive number of small adenomas usually scattered
throughoutt the liver (43). Together with multiphase-helical CT or MRI, histopathology of several
noduless should be the gold standard for definitive diagnosis of LA. Only single core biopsy of
onee nodule might be misleading or even non-diagnostic due to co-existing parenchymal diseases
and/orr to different lesion components. For an accurate diagnosis and a reliable exclusion of
malignancy,, several biopsies should be taken preferably during laparoscopy or laparotomy to
ensureensure the control of any bleeding. It should be taken into account that the bleeding risk after
singlee biopsy is 0.7% (49) and is likely higher in LA patients because of the hypervascular structure
off the nodules. Intratumoral bleeding was already present in 26% of all LA patients at the time
off diagnosis.
< < n n ? ?
v v a. a. n n o o 3 3 O O I/) )
CI I C C -: : O O 3 3
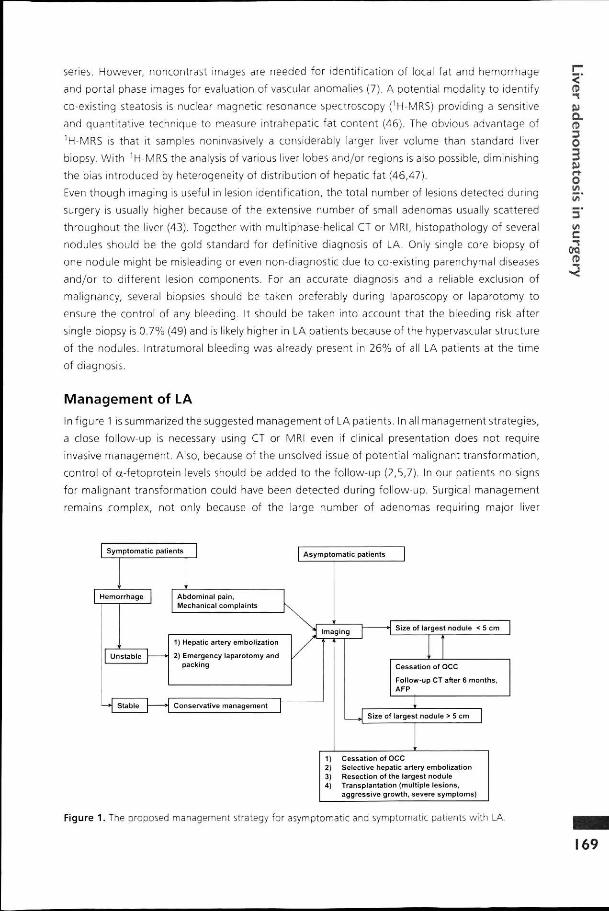
Managementt of LA
Inn figure 1 is summarized the suggested management of LA patients. In all management strategies,
aa close follow-up is necessary using CT or MRI even if clinical presentation does not require
invasivee management. Also, because of the unsolved issue of potential malignant transformation,
controll of «-fetoprotein levels should be added to the follow-up (2,5,7). In our patients no signs
forr malignant transformation could have been detected during follow-up. Surgical management
remainss complex, not only because of the large number of adenomas requiring major liver
Symptomat icc patients
Hemorrhage e Abdominall pain, Mechanicall complaints
1)) Hepatic artery embol izat ion
2)) Emergency laparotomy and packing g
Conservativee management
Asymptomat icc patients
Imaging g Sizee of largest nodule < 5 cm
Cessationn of OCC
Fol low-upp CT after 6 months, AFP P
Sizee of largest nodule > 5 cm
1)) Cessat ion of OCC 2)) Selective hepatic artery embol izat ion 3)) Resect ion of the largest nodule 4)) Transplantat ion (mult iple lesions,
aggressivee growth, severe symptoms)
Figuree 1. The proposed management strategy for asymptomatic and symptomatic patients with LA.
69 9

resectionn but also because of the risk of hemorrhagic complications during surgery. Large
adenomas,, particularly superficial, have a higher risk of bleeding with a mortality rate of 7%. In
emergency,, i.e. in case of rupture of the bleed into the peritoneal cavity, selective angiography of
thee hepatic artery with embolization is recommended (50). In case of extensive bleeding, either
excisionn of the bleeding tumor or packing has been recommended (12,44). In our review, an
equall number of symptomatic and asymptomatic patients were primarily resected (57% vs. 54%)
andd in both groups, an equal number of secondary interventions were performed (21% vs 17%).
Inn patients with tumors >5 cm, 59% was resected compared to 35% of smaller tumors. In larger
tumors,, secondary interventions were needed in 25% of patients vs. 8% if the size was less than
55 cm. However, 40% of smaller tumors continued to grow during follow-up. Interestingly, after
surgeryy in patients with tumors > 5 cm, the remaining tumors remained stable. Of all analyzed
patientss (94), tumor(s) showed regression during follow-up only in three patients.
Liverr resection should be considered when a nodule is larger than 5cm, if malignancy cannot be
ruledd out or when a larger nodule presents with severe pain. For the most aggressively growing
tumors,, OLT has been considered too (6,7). Still, a selection of patients can benefit from extensive
resectionn without any negative effect on outcome as we noticed no difference in the long-term
outcomee of conservatively or surgically treated patients. Resection can be preceded by PVE to
increasee the future remnant liver volume consequently decreasing the risk of postoperative liver
failuree and complications. However, as PVE increases hepatic arterial blood supply, an increase in
thee volume of hyperarterialized LA is possible, as found in our patient 1. Therefore, the addition
off sequential arterial embolization (TAE) or the combination therapy, i.e. TAE followed by
percutaneouss ethanol injections, might be preferred (51). In patient 4, an elective hepatic artery
embolizationn was sufficient to induce tumor regression.
Inn any patient with LA considered for liver resection, potentially co-existing steatosis should be
acknowledged.. This is because of the impact of liver steatosis on the outcome of liver surgery.
Evidencee is accumulating that all grades of steatosis, even the mildest, potentially affect the
recoveryrecovery of patients after transplantation and liver resection (52,53,54). It is noteworthy in this
connectionn that in our own series of 6 patients, 5 featured severe type of steatosis.
Conclusion n
LAA is a progressive, benign parenchymal disease mainly occurring in females. There is a potential
linkk with hepatic steatosis with implications for the management of patients with LA. Noninvasive
diagnosiss is difficult because of the variety of tissue components. Management should primarily
bee conservative with careful follow-up.
Referencee list 1.. Edmondson HA, Henderson B. Liver cell adenoma associated with the use of oral contraceptives.
NN Eng J Med 1976; 294:470-472.
2.. Leese T, Farges 0, Bismuth H. Liver cell adenomas Ann Surg 1988; 208:558-564.

3.. Bulher H, Provino M, Akovbianstz, et al. Regression of liver cell adenoma. A follow-up of three consecutivee patients after dicontunuation of oral contraceptive use. Gastroenterology 1982; 82:534-536. .
4.. Flejou JF, Barge J, Menu Y, et al. Liver cell adenomatosis. An entity distinct from liver cell adenoma? Gastroenterologyy 1985; 89; 1132-1138.
5.. Ribeiro A, Burgart U, Nagorney DM, Gores GJ. Management of liver adenomatosis: results with conservativee surgical approach. Liver Transplant Surg 1998; 4:388-398.
6.. Chiche L, Dao T, Salame E, et al. Liver adenomatosis: reappraisal, diagnosis and surgical management:: eight new cases and review of the literature. Ann Surg 2000; 231:74-81.
7.. Grazioli L, Federle MP, Ichikawa T, Batzano E, Nalesnik M, Madariaga J. Liver adenomatosis: clinical, histopathologicall and imaging findings in 15 patients. Radiology 2000; 216:395-402.
8.. Brander WL, Vosnides G, Ogg CS, et al. Multiple hepatocellular tumours in a patient treated with orall contraceptives. Virchows Arch A Path Anat Histol 1976; 370:69-76.
9.. Brophy CM, Bock JF, West AB, et at. Liver cell adenoma: diagnosis and treatment of a rare hepatic neoplasticc process. Am J Gastroenterol 1989; 84:429-432.
10.. Brunt EM, Wolverson MK, Bisceglie AM. Benign hepatocellular tumors (adenomatosis) in nonalcoholicc steatohepatitis: a case report. Sem Liv Dis 2005; 2:230-236.
11.. Bluteau O, Jeannot E, Bioulac-Sage P, et al. Bi-allelic inactivation of TCF1 in hepatic adenomas. Natt Gen 2002; 32:312-315.
12.. Bacq Y, Jacquennin E, Balaband C, et al. Familial liver adenomatosis associated with hepatocyte nuclearr factor 1" inactivation. Gastroenterology 2003, 125:1470-1474
13.. Jenkins RL, Johnson LB, Lewis D. Surgical approach to benign liver tumors. Sem üv Dis 1994; 14:178-189. .
14.. Monges H, Payan H, Legre M, Vignoli R, Considerations on a case of benign multinodular adenomaa of the liver. Arch Mai Appar Dig Mai Nutr 1963; 52:725-737.
15.. Monaco P, Halgrimson J, MacDermott WV. Multiple adenoma (hamartoma) of the liver treated byy subtotal (90%) resection; morphological and functional studies of regeneration. Ann Surg 1964;; 159:513-519.
16.. Bertrand G, Saint-Andre JP, Simard C, Pillet J, SulzerJ. Nodular liver hyperplasia after oral contraception.. 2 new cases. Nouv Presse Med 1975; 4:2276.
17.. Bisson A, Duron JJ, Fagnietz PL, Pinadau Y, Germain A. Hepatic adenomatosis and oral contraceptives.. Surgical aspects. Nouv Presse Med 1974; 3:2079-2082.
18.Caguett R, Guillausseau PJ, Louvel A, et al. Polyadématose hépatique. Un nouveau cas. Nouvelle Pressee Med 1976; 5:1474-1476.
19.. Foster JH, Berman MM. The malignant transformation of liver cell adenomas. Arch Surg 1994; 129:712-717. .
20.. Mariani AF, Livinstone AS, Perreiras RV, Van Zuiden PE, Schiff ER. Progressive enlargement of an
hepaticc cell adenoma. Gastroenterology 1979; 77:1319-1325.
21.. Lui AK, Hiratza LF, Hirose FM. Multipfe adenomas of the liver. Cancer 1980; 45:1001-1004.
22.. Sinha MR, Prasad SB. Multiple adenomas of the liver. J Indian Med Assoc 1982; 79:16-18.
23.. Chen KTK, Bocean JJ. Multiple hepatic adenomas (letter). Arch Pathol Lab Med 1983; 107:274-275. .
24.. Kalra PA, Guthrie JA, Dibble JB, Turney JH, Brownjohn AM. Hepatic adenomas induced by norethistronee in patients receiving renal dialysis. Br Med J (Clin Res Ed) 1987, 294:808.
25.. Leborgne J, Lehur PA, Horeau JM, et al. Problemes therapeutiques lies aux ruptures de volumineuxx adenomas hepatiques de siege central: a propos de trois observations. Chirurgie 1990;; 116:454460.
26.. Lei K, Han JK, Kim SH, Han MC. MR findings in liver adenomatosis. Gastrointest Radiol 1991; 16:234-236. .

27.. Lui AFK, Hiratzka LF, Hirose FM. Multiple adenomas of the liver. Cancer 1980;45:1001-1004.
28.. Kahn SS, Fink M, King S. Case report: liver adenomatosis presenting as multiple calcified masses. Clinn Radiol 1992;45:206-207.
29.. Le Bail B, Joinahole H, Deugnier Y, et al, Liver adenomatosis with granulomas in two patients
onn long-term oral contraceptives. Am J Surg Pathol 1992; 16:982-987. 30.. Propst A, Propst T, Waldenberg P, et al. A case of hepatocellular adenomatosis with a follow-up
off 11 years. Am J Gastroenterol 1995; 90:1345-1346.
31.. Arsenault TM, Johnson CD, Gorman B, et al. Hepatic adenomatosis.mayo Clin Proc 1996, 71:478-480. .
32.. Barcet S, Frering V, Partensky C. Resection hépatique pour adenoma et adénomatose hépatique. Lyonchirr 1996, 92:6-12.
33.. Gokhale R, Whitington PF. Hepatic adenomatosis in an adolescent. J Pediatr Gastroenterol Nutr 1996;; 23:482-486.
34.. Cristaldi M, Rovati M, Conte D, Elli M, Lesma A, Mezzabotta M, Vago L, Taschieri AM. Primary liverr adenmatosis. Dig Surg 1998; 15:75-78.
35.. Oberti F, Rifflet H, Flejou JF, et al.Association d'une adénomatose hépatique et d'une sclerose hépatopotatee chez une femme atteinte d'incontinentia pigmenti. Gastroenterol Clin Biol 1997; 21:147-151, ,
36.. Ye MQ, Surianawata A, Ben Haim M, Parsons R, Schwartz ME. A 42- year old woman with liver massess and long- term use of oral contraceptives. Sem Liver Dis 1999; 19:339-344.
37.. Caballes RL, Caballes RA. Multiple hepatocellular adenomas in a patient with a history of oral contraception.. Int J Gyn Obst 1999; 64:177-180.
388 Yoshidome H, McMasters Km, Edwards MJ. Management issues regarding hepatic adenomatosis. Amm Surg 1999; 65:1070-1076.
39.. Yunta PJ, Moya A, San-Juan F, Lopez-Andujar R, De Juan M, Orbis F, Mir J. A new case of hepatic adenomatosiss treated with orthotopic liver transplantation. Ann Chir 2001; 126:672-674.
40.. Suarez AA, Brunt EM, Di Biseglie AM. A 35 year old woman with progesterone implant contraceptionn and multiple liver masses. Semin Liver Dis 2001; 21:453-459.
41.. Jovine E, Biolchini F, Talarico F, Lazzari A, Lerro FM, Selleri S, Landolfo G, Martuzzi F. Intrahepatic rupturee of caudae lobe adenoma in liver adenomatosis. J Hepatobiliary Pancreat Surg 2004; 11:324-329. .
42.. Lee SH, Hahn ST. Treatment of multiple hepatic lesions using transarterial chemoembolization. Cardiovascc Intervent Radiol 2004; 27:563-566.
43.. Lepreaux S, Laurent C, Blanc JF, Trillaud H, Le Bail B, Trouette H, et al. The identification of small noduless in iiver adenomatosis. J Hepat 2003; 39:77-85.
44.. Skarupa DJ, Ellison C, Vitellas KM, Frankel WL. Hepatocellular adenomatosis is a rare entity that mayy mimic other hepatocellular lesions. Ann Diag Pathol 2004; 8:43-49.
45.. Marchesini G, Bugianesi E, Forlani G, et al. Nonalcoholic fatty liver, steatohepatitis and the metabolicc syndrome. Hepatology 2002; 35:1485-1493.
46.. Thomas EL, Hamilton G, Patel N, et al. Hepatic triglycerides content and its relation to body adiposity:: a magnetic resonance imaging and proton magnetoc resonance spectroscopy study. Gutt 2005; 54:122-127.
47.. Browning JD, Szczepaniak LS, Dobbins R, et al. Prevalnece of hepatic steatosis in an urban populationn in the United States: impact of ethnicity. Hepatology 2004; 40:1387-1395.
48.. Wheeler PG, Melia W, Dubbins P, et al. Non-operative arterial embolisation in primary liver tumours.. Br Med J 1979; 2:242-244.
49.. McGill DB, Rakela J, Zinsmeister AR, et al. A 21-year experience with major hemorrhage after percutaneouss liver biopsy. Gastroenterology 1990; 99:1396-1400.
50.. Shortell CK, Schwartz SI. Hepatic adenoma and focal nodular hyperplasia. Surg Gynecol Obstet 1991;; 173:426-31.

51.. Tanaka K, Nakamura 5, Numata K, Kondo M, Morita K, Kitamura T, Saito 5, Kiba T, Okazaki ül H,, Sekihara H. The long term efficacy of combined transcatheter arterial embolization and Q percutaneouss ethanol injection in the treatment of patients with large hepatocellular carcinoma "* andd cirrhosis. Cancer 1998; 82:78-85. K
52.. Belghiti J, Hiramatsu K, Benoist S, et al. Seven hundred forty-seven hepatectomies in the 1990s: 2 ann update to evaluate the actual risk of liver resection. J Am Coll Surg 2000; 191:38-46. O
3 3 53.. Kooby DA, Fong Y, Suriawinata A, et al. Impact of steatosis on perioperative outcome following £
hepaticc resection. J Gastrotntest Surg 2003; 7:1034-1044. w.
54.. Little SA, Jarnagin WR, DeMatteo RP, et al. Diabetes is associated with increased perioperative I/I I mortalityy but equivalent long-term outcome after hepatic resection for colorectal cancer. J C Gastrr Surg 2002; 6:88-94. 0Q
re re
173 3
. '« f t . . '"'' '"'..,
r r