using ema methods in social epidemiology research thomas w. kamarck, ph.d. university of pittsburgh...
TRANSCRIPT

USING EMA METHODS IN SOCIAL USING EMA METHODS IN SOCIAL EPIDEMIOLOGY RESEARCHEPIDEMIOLOGY RESEARCH
Thomas W. Kamarck, Ph.D.Thomas W. Kamarck, Ph.D.
University of PittsburghUniversity of Pittsburgh
EMA Workshop:EMA Workshop:
Pittsburgh Mind-Body CenterPittsburgh Mind-Body Center
July 10, 2006July 10, 2006

COLLABORATORSCOLLABORATORS
Saul Shiffman, Ph.D.Saul Shiffman, Ph.D.
Matthew F. Muldoon, M.D., M.P.H.Matthew F. Muldoon, M.D., M.P.H.
Kim Sutton-Tyrrell, R.N.,Dr.P.H.Kim Sutton-Tyrrell, R.N.,Dr.P.H.
Chad J. Gwaltney, Ph.D.Chad J. Gwaltney, Ph.D.
Denise L. Janicki, Ph.D.Denise L. Janicki, Ph.D.
Barbara Anderson, Ph.D.Barbara Anderson, Ph.D.
Joseph Schwartz, Ph.D.Joseph Schwartz, Ph.D.
This study was funded by NHLBI Grant HL56346.

PURPOSE OF THIS STUDY

PSYCHOSOCIAL FACTORS AND DISEASE RISK
• Job Stress
• Low Social Support
• Hostility, Depression
Questionnaires, interviews
vs. EMA methods

RATIONALE FOR USE OF EMA
WHY USE EMA AS A TOOL FOR
SOCIAL EPIDEMIOLOGY?
• These methods are well suited for measuring the frequency and duration of risk exposure.
- Retrospective questionnaires require use of estimation heuristics that may be inaccurate, biased . - Momentary reports, sampled frequently throughout the day, should capture representative sample of risk exposure.

WHY USE EMA AS A TOOL FOR
SOCIAL EPIDEMIOLOGY?
• Opportunity to explore some of the mechanisms by which psychosocial risk factors may contribute to disease.
Stress Physiology -Acute effects of stress on body’s physiology may be observable in real time.
Disease
-Time-averaged effects of such changes may be linked with alterations in disease state

DECISIONS ABOUT STUDY DESIGN

SAMPLE CHARACTERISTICS

PITTSBURGH HEALTHY HEART PROJECTPITTSBURGH HEALTHY HEART PROJECT
Sample N=337Age 50-70
Healthy (no history of CVD)Unmedicated (no meds for BP, cholesterol)
51 % female, 16 % nonwhite25 % HS or less, 57 % BA or greater

MEASURES

PITTSBURGH HEALTHY
HEART PROJECT
• Atherosclerosis
• Ultrasound measurements visualize thickness of the artery walls as indicator of carotid artery atherosclerosis.


EMA ASSESSMENT:
CONTENT AND TEMPORAL FRAME

FIVE PSYCHOLOGICAL PROCESSES LINKED FIVE PSYCHOLOGICAL PROCESSES LINKED WITH STRESS, ACUTE BP CHANGES AND WITH STRESS, ACUTE BP CHANGES AND
CV RISKCV RISK
• NEGATIVE AFFECTNEGATIVE AFFECT• AROUSALAROUSAL• TASK DEMANDTASK DEMAND• TASK CONTROLTASK CONTROL• SOCIAL CONFLICTSOCIAL CONFLICT

TASK DEMANDTASK DEMAND
Activity last 10 minutesActivity last 10 minutesRequired working hard?Required working hard?
NO==================YESNO==================YES
Required working fast?Required working fast?NO==================YESNO==================YES
Juggled several tasks at once?Juggled several tasks at once? NO==================YESNO==================YES
DECISIONAL CONTROLDECISIONAL CONTROLActivity last 10 minutesActivity last 10 minutes
Could change activity if you chose to?Could change activity if you chose to? NO==================YESNO==================YES
Choice in scheduling this activity?Choice in scheduling this activity? NO==================YESNO==================YES
Adapted from Karasek
Job Content Questionnaire

DIARY OF AMBULATORY BEHAVIORAL DIARY OF AMBULATORY BEHAVIORAL STATES (DABS)STATES (DABS)
• OTHER TIME-VARYING DETERMINANTS OF CARDIOVASCULAR ACTIVITY• POSTURE• ACTIVITY• SUBSTANCE USE

SAMPLING STRATEGY

PITTSBURGH HEALTHY
HEART PROJECT
AUTOMATED BP AND
ELECTRONIC DIARY ASSESSMENTS
45 mins45 mins
4 mos apart

ASSESSMENT METHODS OR DEVICES


WHY DID WE USE AN ELECTRONIC DIARY?
Electronic diary responses are time-stamped.
• Allowed us to synchronize behavioral and physiological data.
•Critical, given the rapid fluctuations in blood pressure that occur in daily life.

COMPLIANCE ANDCONSIDERATIONS FOR
INCREASING COMPLIANCE

WHY DID WE USE AN ELECTRONIC DIARY?
Time stamp also ensured that the questions were
answered in a timely fashion and allowed us to
check on compliance.


The average participant completed interviews
during 88 % of all possible 45-minute intervals
during waking hours throughout the
6-day monitoring period.
81 % of ABP assessments were valid.

DATA ANALYSIS

DATA ANALYSES
CAROTID ATHEROSCLEROSIS
Conventional GLM approach.
AMBULATORY BLOOD PRESSURE ANALYSES
Multilevel modeling (SAS Proc Mixed).
-- Ability to handle time varying covariates.
--Ability to model autocorrelation effects.
--Ability to tolerate unbalanced designs.

MAIN FINDINGS

WITHIN-PERSON ASSESSMENTSWITHIN-PERSON ASSESSMENTS
Five multi-item scales as measures of psychosocial demand.
SBP b t p
• Negative Affect .38 4.90 < .0001
• Arousal .57 8.52 <.0001
• Task Demand .22 3.59 .0003
• Decisional Control -.10 2.28 .02
• Social Conflict .43 5.97 <.0001
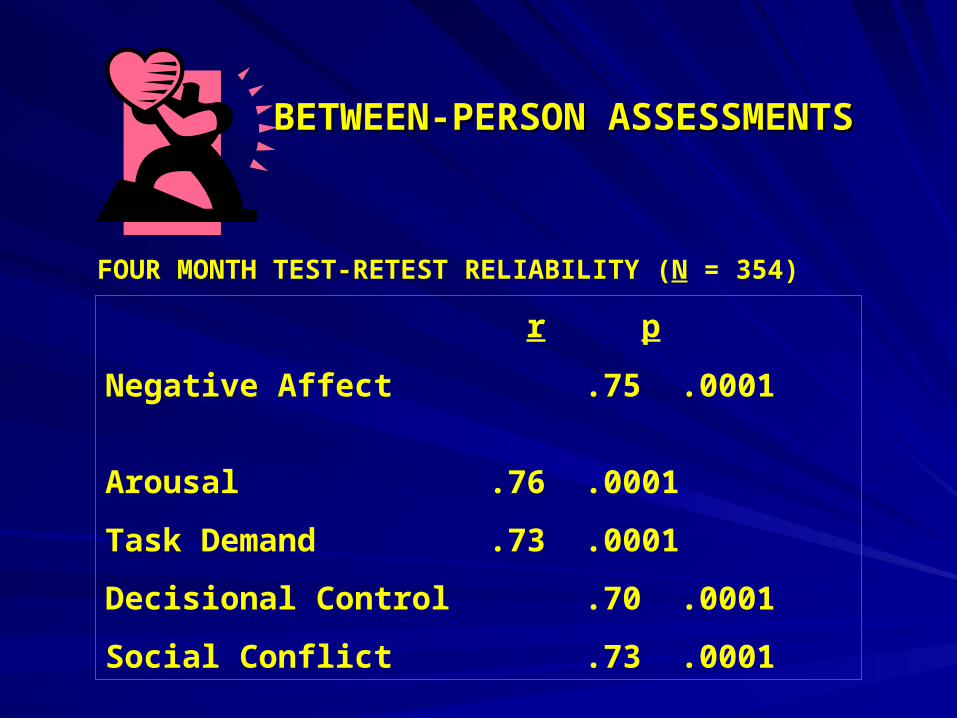
BETWEEN-PERSON ASSESSMENTSBETWEEN-PERSON ASSESSMENTS
FOUR MONTH TEST-RETEST RELIABILITY (N = 354)
r p
Negative Affect .75 .0001
Arousal .76 .0001
Task Demand .73 .0001
Decisional Control .70 .0001
Social Conflict .73 .0001

BETWEEN-PERSON ASSESSMENTSBETWEEN-PERSON ASSESSMENTS
120
122
124
126
128
130
132
134
1st quartile 2nd quartile 3rd quartile 4th quartile
Task Demand
1st quartile 2nd quartile 3rd quartile 4th quartile
Decisional Control
Systolic Blood
Pressure
(mmHg)
Demand Control
Sys
toli
c B
loo
d
Pre
ssu
re (
mm
Hg
)
120
122
128
124
126
130
132
134
0.75
0.77
0.79
0.81
0.83
0.85
0.87
0.89
Mean Ratings of Task Demand by Quartile
Me
an
Ca
roti
d IM
T (
mm
)
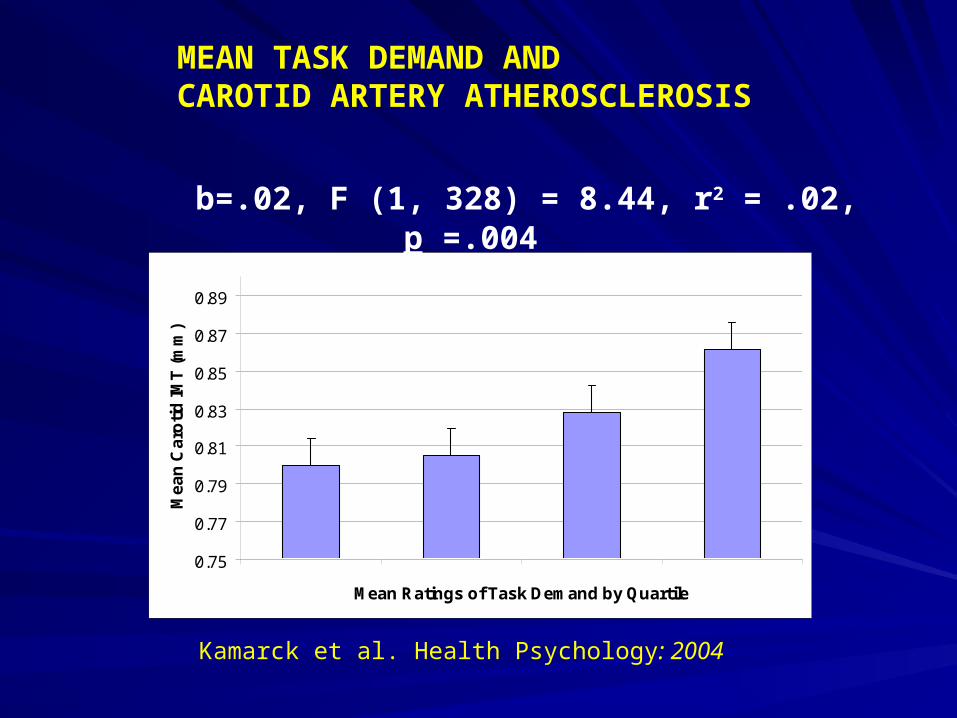
b=.02, F (1, 328) = 8.44, r2 = .02, p =.004
Kamarck et al. Health Psychology: 2004
MEAN TASK DEMAND ANDCAROTID ARTERY ATHEROSCLEROSIS

• Task Demand ratings were associated with atherosclerosis even among those who were not employed during the study (n=141).
(b=.02, p=.03, r2= .03).
• Among employed Ss (n=152), association did not differ as a function of whether ratings were derived from inside or outside of the workplace.
Work: (b=.02, p=.02, r2= .03).
Nonwork: (b=.02, p=.05, r2= .02).
MEAN TASK DEMAND AND
CAROTID ARTERY ATHEROSCLEROSIS
Kamarck et al. Health Psychology: 2004

• Scales from the Karasek Job Content Questionnaire were not significantly associated with atherosclerosis among the employed.
• No significant gender differences in the association between Task Demand and carotid atherosclerosis.
MEAN TASK DEMAND AND
CAROTID ARTERY ATHEROSCLEROSIS
Kamarck et al. Health Psychology: 2004

Mean ABP partially mediated the association between Task Demand and Carotid Atherosclerosis
Demand Carotid Atherosclerosis
Demand
Amb SBP
b = .02, p = .0006
b =.01, p = .05
Amb SBP
CONTROLLING FOR DEMOGRAPHIC COVARIATES AND CLINIC PRESSURE, N=336
Carotid Atherosclerosis

Demand Mean Amb SBP
Demand
p < .01
p = .28
Momentary SBP
Mean Amb SBP
p < .0001
Effects of Task Demand on Mean ABP are completely accounted for by its effects on momentary ABP.

•Individuals show momentary ABP elevations when faced with activities that are perceived as demanding,
•These momentary elevations translate into higher mean ABP for those whose Task Demand ratings are consistently highest,
•Such mean ABP elevations, in turn, may increase risk for atherosclerosis over time.

LESSONS LEARNED

WHAT ARE THE LESSONS LEARNED FROM THESE FINDINGS?
1. We can collect multiple days of ambulatory blood pressure data on a large community-based sample.
2. Self-report and physiological data may be successfully linked using EMA methods, allowing us to examine some of the behavioral determinants of rapidly fluctuating physiological processes.
3. Our ability to obtain a representative sample of experience throughout daily life allows us to test important models of psychosocial risk and cardiovascular disease.

WHAT ARE THE LESSONS LEARNED FROM THESE FINDINGS?
4. It is possible that EMA assessments may capture the frequency and duration of effects more effectively than a measurement method that relies on retrospective self-report.
5. This is the first study examining ambulatory blood pressure as a mediator accounting for the relationship between Demand/Control and increased cardiovascular risk.

CHALLENGES

WHAT ARE SOME OF THE CHALLENGES INVOLVED IN THIS WORK?
1. EMA monitoring with ambulatory blood pressure involves a substantial effort for the participants.
Strategies for streamlining data collection procedures should be investigated.
2. Challenges with respect to maintaining participant comfort during ambulatory blood pressure monitoring.
e.g.,Oscillometric system should be considered.
WHAT ARE SOME OF THE CHALLENGES INVOLVED IN THIS WORK?
3. These methods are time consuming for staff.
Need to plan for adequate staffing, support.
4. Concerns about generalizability.
These methods exclude those whose routines cannot handle interruption.
5. Occasional technical difficulties.
Increased integration between self-report and physiological data collection systems would be desirable.

CONCLUSIONCONCLUSION
•
• These methods can provide valuable information These methods can provide valuable information about person-environment transactions not about person-environment transactions not available from interviews or questionnaires.available from interviews or questionnaires.
• Such intensive sampling methods will find an Such intensive sampling methods will find an important place at the table in future social important place at the table in future social epidemiological research.epidemiological research.