use of inhalers medicines optimisation workshop 14 th september 2015, holiday inn gatwick
TRANSCRIPT

Use of InhalersMedicines Optimisation workshop
14th September 2015, Holiday Inn Gatwick
To optimize the use of inhalers across Kent Surrey Sussex, to reduce the cost burden to the
NHS and maximise patient benefit of such medications through effective and appropriate
high quality care
Aim

1. To move forwards with optimising the use of inhalers across KSS
2. To agree specific ways forward and scope pieces of work
3. To share examples of good practice
4. To identify volunteers and partners for project work that is agreed
Objectives of this workshop

• NHSE set a medicines optimisation priority to all AHSN regions
• KSS AHSN hosted a MO event 19th May 2015 covering:– National view from NHSE– Polypharmacy– AF and HF medications
– Inhalers• Agreed to work up strategies and projects
The story so far…..
1. Need for spirometryspirometry competencies to be increased across all kinds of professionals, for accurate earlier diagnosis and ongoing effective monitoring
2. Need for improved effective use of inhalers by patients and their carers, through improved inhaler inhaler techniquetechnique capabilities and training
3. Need for appropriate, effective and responsible
inhaler prescribing inhaler prescribing in terms of both medication and devices
Agreed Priorities

Quality Assured Spirometry
Vikki KnowlesRespiratory Nurse Consultant
G & W CCG

Setting the scene● Spirometry is the recommended objective test
performed to identify abnormalities in lung volumes and air flow1.
● It is used in conjunction with physical assessment, history taking, blood tests and x-rays, to exclude or confirm particular types of lung disease, enabling timely diagnosis and treatment.

The Global view
● Standardisation of spirometry (2005) Eur Resp Journal 26: 319-338
● BTS NICE QS 10 (2011) COPD
STANDARDS DOCUMENTDiagnostic Spirometry in Primary Care
Proposed standards for general practice compliant with AmericanThoracic Society and European Respiratory SocietyRecommendations
A General Practice Airways Group (GPIAG)1 document, in association with the Association for Respiratory Technology & Physiology (ARTP)2 and Education for Health31 www.gpiag.org 2 www.artp.org 3 www.educationforhealth.org.uk
Mark L Levy, Philip H Quanjer, Rachel Booker, Brendan G Cooper, Stephen Holmes, Iain R Small

Quality Assurance
● Diagnostic spirometry should only be conducted by an operator trained and assessed to Association for Respiratory Technology and Physiotherapy (ARTP) or equivalent standards in the performance of spirometry by recognised training bodies.
● Interpretation of results may be performed separately. The interpreter must be trained and assessed to ARTP or equivalent standards in the interpretation of spirometry by recognised training bodies2.
Pitfalls in Spirometry: An Educational Piece Jo Congleton, Consultant Physician, Clinical Co-lead South of England (east) SHABreathing Matters Nov 2010
Other useful educational information
Restrictive Spirometry: An Educational Piece Jo Congleton, Consultant Physician, Clinical Co-lead South of England (east) SHABreathing Matters Sept 2011
QA Diagnostic spirometry for COPD. Ten minute tutorial (2013)www.copdexchange.co.uk
Issues re trainingARTP certification Gold standard but:
●Significant cost and time implications
●Practices may disengage with spirometry training
●Increased referrals to separate spirometry service
QA Spirometry training
●Silver standard training
●Alternative way of achieving a safe and cost effective service
●Practical to achieve across a CCG
●Starting point for those practices wishing to achieve the ARTP certification
Risk of poor quality spirometry
● Incorrect diagnosis
● Poor patient outcomes
● Inappropriate use of inhaled treatment with increased risk of side effects for no benefit.

COPD in KSS
68,000 people diagnosed; 55,000 undiagnosed68,000 people diagnosed; 55,000 undiagnosed
1,891 deaths in 2010equating to a DSR of 21.92 (against England rate of 25.19)
1,891 deaths in 2010equating to a DSR of 21.92 (against England rate of 25.19)
1,557 years of life lost1,557 years of life lost
Standardised LoS 6.3 daysbelow national average 6.4,
however, reducing to best area’s (London) could save 3,196 bed days
Standardised LoS 6.3 daysbelow national average 6.4,
however, reducing to best area’s (London) could save 3,196 bed days
49,504 bed days49,504 bed days
KSS spend £46.6m on inhaled corticosteroids in 2010KSS spend £46.6m on inhaled corticosteroids in 2010Ageing population will mean
these figures will worsen

Spirometry in Primary Care● Unlike many medical tests during which the patients
remain passive, spirometry testing requires co-operation and an almost athletic breathing manoeuvre.
● With submaximal effort, the results are erroneous (false positive and false negative for disease or change in severity).
● The misclassification rate is about 5% in most research and sub-speciality settings , but has been shown to be higher in primary care settings.
● The most common cause of error is inadequate spirometry training and experience of the person performing the test
Common Errors● Sub maximal inhalation
● Excessive extrapolated volume
● Slow start
● Cough
● Early termination
● Variable effort
● Cessation of airflow – glottis closure
● Leak
● Extra breaths

Local spirometry provision
● How does your service stack up?
● Have you used a QA checklist to assess the quality of the service being provided.
● Who carries out spirometry?
● What training have the HCP’s providing spirometry undertaken?
What happens in other areas
● Leicester ask practices to submit 10 traces to RCT lead for approval.
● Stockport had a spirometry LES initially but this created problems when the HCP leading it left.
● Moved towards accrediting a limited number of local practitioners (ARTP) and maintaining register but reaccreditation proving a problem.
Supportive documents
● Commissioning Toolkit
● Service Specifications
● Read costing tool for spirometry

Spirometry and Assessment Service Model
Net cost QALY Gains
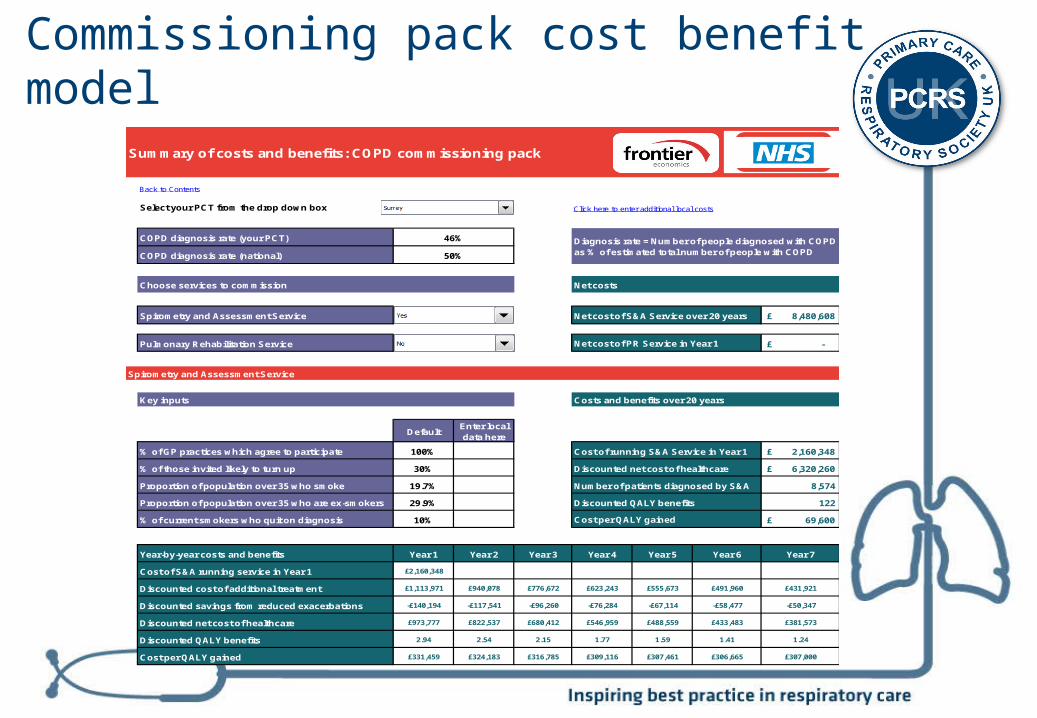
Summary of costs and benefits: COPD commissioning pack
Back to Contents
Select your PCT from the drop down box Click here to enter additional local costs
COPD diagnosis rate (your PCT)
COPD diagnosis rate (national)
Choose services to commission Net costs
Spirometry and Assessment Service 8,480,608£
Pulmonary Rehabilitation Service -£
Spirometry and Assessment Service
Key inputs Costs and benefits over 20 years
DefaultEnter local data here
% of GP practices which agree to participate 100% Cost of running S&A Service in Year 1 2,160,348£
% of those invited likely to turn up 30% Discounted net cost of healthcare 6,320,260£
Proportion of population over 35 who smoke 19.7% Number of patients diagnosed by S&A 8,574
Proportion of population over 35 who are ex-smokers 29.9% Discounted QALY benefits 122
% of current smokers who quit on diagnosis 10% 69,600£
Year-by-year costs and benefits Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Year 7
Cost of S&A running service in Year 1 £2,160,348
Discounted cost of additional treatment £1,113,971 £940,078 £776,672 £623,243 £555,673 £491,960 £431,921
Discounted savings from reduced exacerbations -£140,194 -£117,541 -£96,260 -£76,284 -£67,114 -£58,477 -£50,347
Discounted net cost of healthcare £973,777 £822,537 £680,412 £546,959 £488,559 £433,483 £381,573
Discounted QALY benefits 2.94 2.54 2.15 1.77 1.59 1.41 1.24
Cost per QALY gained £331,459 £324,183 £316,785 £309,116 £307,461 £306,665 £307,000
46%
50%
Diagnosis rate = Number of people diagnosed with COPD as % of estimated total number of people with COPD
Net cost of S&A Service over 20 years
Net cost of PR Service in Year 1
Cost per QALY gained
Commissioning pack cost benefit model

Achieving QA Spirometry
Silver standard
●2 full days attendance
●Submission of portfolio
●Local assessment
●Annual half day attendance to maintain QA

Morning session – Day 1
● Introduction in to the rationale for performing spirometry followed by:
● Practical session on performing spirometry to include:
● Preparation of equipment
● Review of different spirometers (Attendees asked to bring along spirometer they use where possible.
● Calibration techniques
● Patient preparation
● Information on Contraindications
● Practical Assessment
Afternoon session – Day 1
● Introduction into interpretation
● Review all the spirometry strips from the morning assessment (QA)
● Within 6 weeks submit portfolio, 5 cases, calibration log and pre test check list.
Day 2 Interpretation day
● GP and PN to attend with portfolio containing 3 spirometry tracings.
● GP part of protected learning QA: One GP per practice to attend
● Morning session
● Introduction to interpretation of spirometry results with link to diagnosis.
● Review of spirometry tracings brought to day; Assess quality of tracing and interpretation of results
● Afternoon session
● Assessment of 5 cases to complete the day
● Certificate of attendance if passed
Maintaining QA Spirometry
● Annual half day attendance for all staff who have completed initial QA spirometry sessions.
● Submission and review of 5 cases
● Information / signposting - ARTP Gold standard accredited spirometry courses.

The Next Step● How would you define a QA spirometry
service?
● Do you think the silver standard level offers a robust first step to achieving QA spirometry?
● What is your preferred model of delivery?
● Should we be insisting on ARTP qualification across the CCG within all GP practices?

Follow us on Social Media
@PCRSUK
https://www.facebook.com/PCRSUK
Inhaler Technique
How do we get it right and improve technique,
knowledge and understanding of both HCP’s and patients?
Jo Wookey KSS AHSN Respiratory programme co lead.

Why is so important?
4 of the top 5 costliest drugs to the NHS are Respiratory inhalers
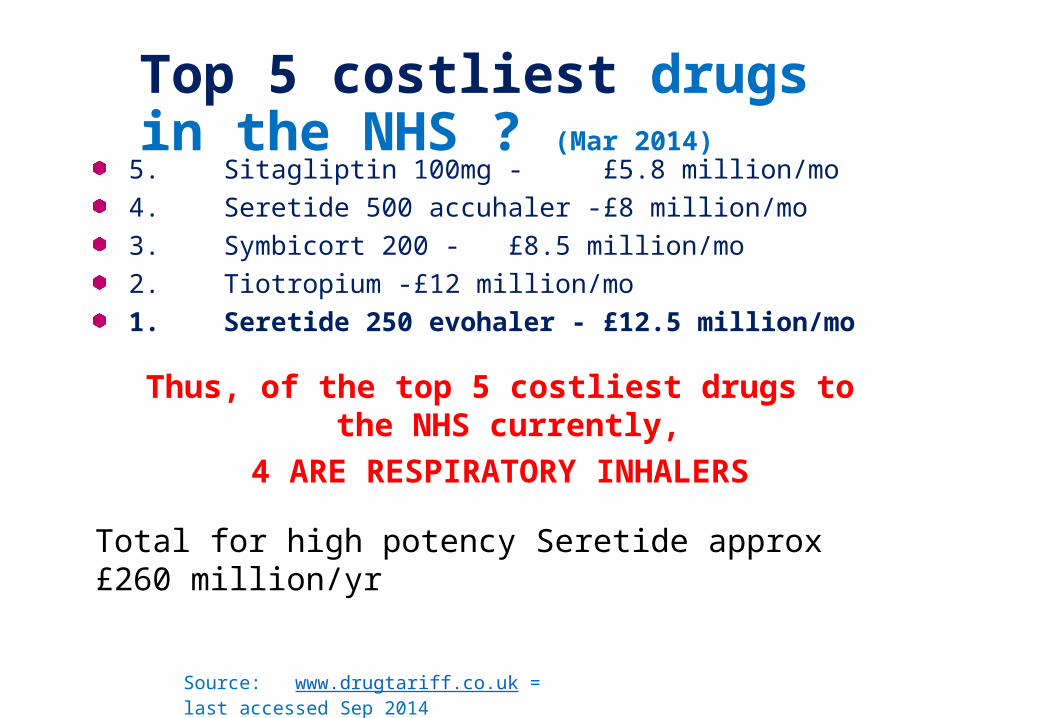
Top 5 costliest drugs in the NHS ? (Mar 2014)
Source: www.drugtariff.co.uk = last accessed Sep 2014
5. Sitagliptin 100mg - £5.8 million/mo4. Seretide 500 accuhaler - £8 million/mo3. Symbicort 200 - £8.5 million/mo2. Tiotropium - £12 million/mo1. Seretide 250 evohaler - £12.5 million/mo
Thus, of the top 5 costliest drugs to the NHS currently,
4 ARE RESPIRATORY INHALERS
Total for high potency Seretide approx £260 million/yr
Why is it so important?
• 90% of patients have the wrong technique.• Poor technique means patients aren’t getting the dose they
require• Think its ineffective• Doesn’t help symptom management• Keep changing inhalers or stepped up onto inappropriate regimes
• Studies have shown between 70-94% of HCP’s unable to demonstrate ability to use inhale correctly
• If we can’t do it right how can the patient??
Therefore, it is a costly mistake to both the patient and the NHS getting it wrong!
What do we need to do?• Improve the knowledge of all HPC’s
• Understanding the different devices, how they work, pro’s & con’s
• Patient appropriate device selection• Use of spacers- the correct type for the correct device• Understanding of the prescribing guidelines• Improve skills in teaching inhaler technique• Check and re-check inhaler technique at every opportunity
• Improve patient knowledge and technique• Provide patients with information about their device• Ensure carer/partner knows how to use the device• Involve them in the selection of the device

How do we do this? Examples….• Train the trainer
• Isle of Wight project-• HCPs were instructed on how to use the inhalers themselves, and then
trained to measure a patient's ability to use their prescribed inhaler. • Emergency admissions due to asthma reduced by 50%, and deaths by
75%. PCT • Bronchodilator spend down by 20%• Hospital inpatient costs for asthma-related admissions have fallen by
66% • South West inhaler training project-
• training ambassadors( primary and secondary nurses and pharmacists) supported by on-line competency and then running further training sessions locally to other HCP’s
• Consistent messages• ITT East Sussex
• Trained the trainers• Learnt that targeting specific groups/ organisation was more effective
than a “mass marketing” approach with better uptake.• Have delivered workshops to practice nurses, ACNPs, school staff,
domiciliary care workers and housing support workers and more recently nursing and therapy teams in HWLH.
• Getting engagement is key

Examples…•Online training
• Greater Manchester inhaler improvement innovation project- WIRES Podcasts hosted by Wessex AHSN
• Medicines.org.uk- video’s showing use of inhaler + info on each device and medication
• Pharma websites

Examples
•On-line information/resources
• BLF• Asthma uk• Local CCG websites hosting information• Local pharmacy websites


How shall we do this across KSS?? Build on Train the trainer? Agreed standardised training for the region- slide set? Consistent messages? Accredited training/competency sets? combining training with MUR’s- utilise pharmacists? Develop regional on-line resource- utilising existing resources? Patient/carer information
Over to you…………..

Responsible Respiratory Prescribing Messages
Draft update for discussionHelen Marlow, Lead Primary Care Pharmacist and NICE Medicines and
Prescribing Centre Associate
August 2015

Responsible Prescribing in COPD (old
messages)
South East Coast Principles
Do the right things: Smoking cessation is the most effective intervention for COPD Pulmonary rehabilitation reduces admissions and health care
resource use, improves exercise capacity and health related quality of life
Prescribe according to guidelines
Do the right things right:
Ensure correct inhaler technique most patients don’t know how to use their inhaler and many health care professionals who teach the use of MDI cannot demonstrate it correctly
Use a spacer when using an MDI correctly a max of 15% of the drug enters the lung. With a spacer this can be increased up to 30%
Use an ICS patient safety card

What are we trying to achieve?
Maximise value
Porter ME; Lee TH NEJM 2010;363:2477-2481; 2481-2483

The challenge for the NHS is to get more for less in an era of “no more money”.
To do this, the NHS needs to shift from lower value interventions to higher value interventions
Right Care
“clinicians will need to accept that they are responsible for the stewardship of resources and not just their use” Sir Muir Gray BMJ Oct 6 2012
Do the right thing
Do the right thing right
Doing the right thing right first time should deliver quality and value
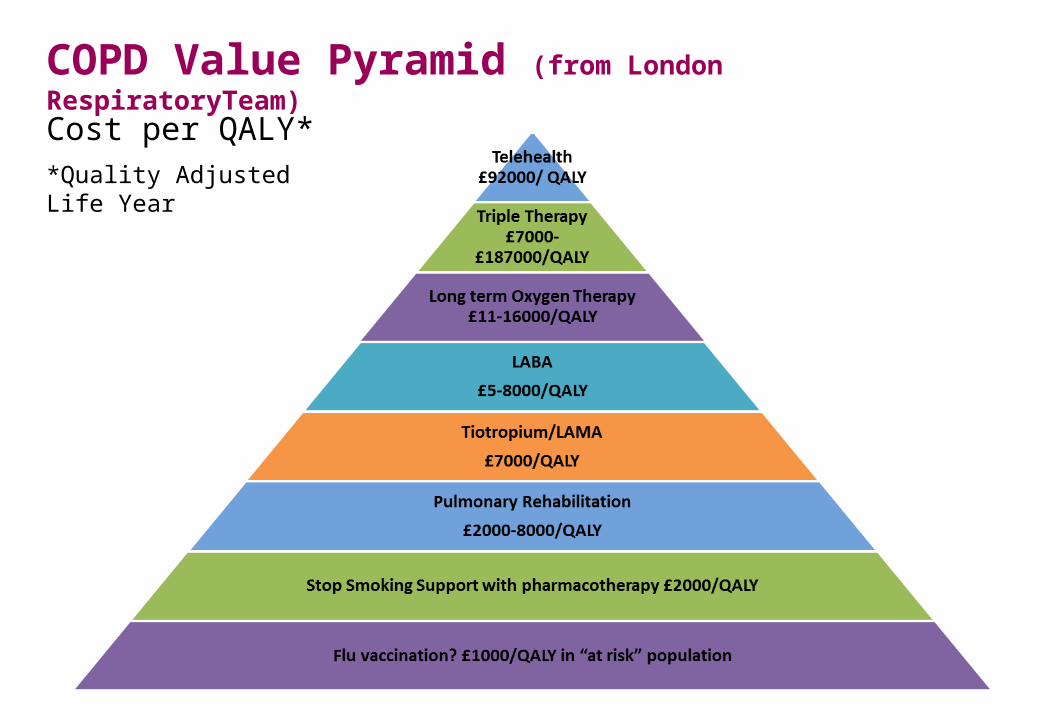
COPD Value Pyramid (from London RespiratoryTeam)
Cost per QALY**Quality Adjusted Life Year

Responsible Prescribing in COPD (old
messages)
South East Coast Principles
Do the right things: Smoking cessation is the most effective intervention for COPD Pulmonary rehabilitation reduces admissions and health care
resource use, improves exercise capacity and health related quality of life
Prescribe according to guidelines
Do the right things right:
Ensure correct inhaler technique most patients don’t know how to use their inhaler and many health care professionals who teach the use of MDI cannot demonstrate it correctly
Use a spacer when using an MDI correctly a max of 15% of the drug enters the lung. With a spacer this can be increased up to 30%
Use an ICS patient safety card


Asthma – potential RRP messages
Do the right things: Smoking cessation is the most effective intervention for COPD Personalised asthma action plans improve outcomes and may
reduce readmission rates
Do the right things right: Titrate dose of inhaled preventative therapy to optimise asthma
control and minimise risk of side effects Know the equivalent dose of ICS when changing to a combination
inhaler Check adherence to and use of preventer and reliever therapy, to
identify patients at risk of severe exacerbations Use an ICS patient safety card

COPD – potential RRP messagesDo the right things: Smoking cessation is the most effective intervention for COPD Flu vaccination reduces the risk of COPD exacerbations Pulmonary rehabilitation reduces admissions and health care resource
use, improves exercise capacity and health related quality of life Prescribe according to guidelines Provide individualised self management plan and exacerbation rescue
pack, to patients with COPD exacerbations
Do the right things right: Encourage a trial of therapy, if it does not work don’t be afraid to stop it Use an ICS patient safety card for patients on high dose ICS Reserve ICS for more severe COPD and frequent exacerbations to
minimise risk of harm and optimise benefit

Inhalers - – potential RRP messagesDo the right things:With the patient, decide the best device for them assess their ability to inhale, let them see, touch and feel the inhaler, then describe, show and provide written information
Do the right things right:
Ensure correct inhaler technique most patients don’t know how to use their inhaler and many health care professionals who teach the use of MDI cannot demonstrate it correctlyUse a spacer when using an MDI correctly a max of 15% of the drug enters the lung. With a spacer this can be increased up to 30%Prescribe inhalers by brand, so patient receives correct inhaler deviceRationalise inhaler devices for an individual patient, avoid mixing too many DPI devices (check evidence)Re-check inhaler technique often, inhaler technique deteriorates over time, and lots of patients think they are using their inhalers correctly when they are not
Updating messages
• Do we have any new evidence / important issues in practice to include?
• Do we need separate messages for asthma and COPD?
• Messages need to be relevant and valid
• How should they be presented?
What do you think?