usaid tb care ii bangladesh
TRANSCRIPT
This document has been developed by the TB CARE II project and is made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents of this document are the sole responsibility of University Research Co., LLC and do not necessarily reflect the views of USAID or the United States Government.
Grants SpotlightUSAID TB CARE II Bangladesh:
B ANG L AD E S H B ANG L AD E S H

Background ....................................................................................................1
Introduction to TB CARE II Bangladesh .......................................................1
Introduction to the Small Grants Program ...................................................2
The TB CARE II Bangladesh Small Grants Capacity Building Model .........4
Grantee Focus Areas .....................................................................................4
Intensified TB Case Finding .........................................................................4
Addressing TB among Vulnerable and High-Risk Populations .....................7
Linking with Private Providers ......................................................................8
Advocacy, Communication, and Social Mobilization Activities .....................9
Human Resource Department .................................................................. 10
Table of Contents

Background ....................................................................................................1
Introduction to TB CARE II Bangladesh .......................................................1
Introduction to the Small Grants Program ...................................................2
The TB CARE II Bangladesh Small Grants Capacity Building Model .........4
Grantee Focus Areas .....................................................................................4
Intensified TB Case Finding .........................................................................4
Addressing TB among Vulnerable and High-Risk Populations .....................7
Linking with Private Providers ......................................................................8
Advocacy, Communication, and Social Mobilization Activities .....................9
Human Resource Department .................................................................. 10
Table of Contents

USAID TB CARE II Bangladesh: Grants Spotlight 1
Background
Tuberculosis (TB) remains a major public health
problem in Bangladesh. Bangladesh currently
has the sixth highest TB burden in the word, with
approximately 350,000 new cases of TB in 2012. Of these,
the total number of all new TB cases detected was 164,855
– signifying that 53% of TB cases remain undetected every
year (WHO Global TB Report 2013). While Bangladesh
has made significant progress in the past several years
in increasing detection of smear positive TB, increasing
the rates of treatment success, and achieving nationwide
coverage of the directly-observed therapy short course
(DOTS) program, more remains to be done to detect a
larger proportion of cases and contain the spread of the
disease. Treatment adherence is also a major problem,
which is in part responsible for the increasing rates of
multidrug resistant TB (MDR TB) in the country. Currently,
MDR TB represents 1.4% of new and 29% of retreatment
cases. The total number of MDR TB cases among notified
pulmonary TB cases is estimated at 4,200. Because of
limited capacity for diagnosis, only a small proportion of
estimated MDR TB cases are identified. The situation is
same with the treatment of MDR-TB patients. The capacity
for in-patient treatment of MDR TB is far less than the
patients who need this service. As a result, a large number
of patients remain on waiting lists for treatment for MDR-TB.
Introduction to TB CARE II Bangladesh
TB CARE II Bangladesh, funded through the global
USAID TB CARE II Project, is designed to enhance the
capacity of the National TB Control Program (NTP) to
achieve its national objectives for preventing and controlling
TB. The project, implemented by University Research Co.,
LLC (URC) along with its global partners, leverages Global
Fund and Government of Bangladesh resources to facilitate
implementation of strategies to strengthen and expand
DOTS, Programmatic Management of Drug Resistant TB
(PMDT), and the overall health systems.
The specific objectives of the project include:
n Improving universal access to TB diagnosis and treatment;
n Working with Government of Bangladesh to reach
and sustain the global targets of > 70% case detection
and > 85% cure rates under DOTS;
n Providing high quality DOTS through all levels including
those of private providers;
n Improving programmatic management of MDR TB and
increasing access to MDR TB prevention and treatment
through community-based approaches;
n Strengthening diagnostic capacity for drug susceptible
and drug resistant TB;
n Strengthening health systems with an Upazila-based
approach for decentralized management of TB control
and prevention activities.
TB CARE II Bangladesh is currently working to strengthen
community-based interventions for TB DOTS activities in
18 districts and parts of Dhaka and Khulna city corpora-
tions. The focus of the project’s community-based work is
to address programmatic gaps that are currently not being
addressed by the Global Fund or Government of Bangla-
desh activities. The project also complements the Global
Fund and GOB activities with main focus on strengthening
capacity and quality of the sputum microscopy services all
over the country. Developing national capacity for strength-
ening and expanding PMDT is a major technical focus of
the TB CARE II project. The project provides exclusive tech-
nical and logistics support to increase access to GeneXpert
services throughout the country and community-based
management of DR TB cases in 39 districts and three city
corporations. The project also supports activities to im-
prove the capacity of culture and DST services throughout
the country.

USAID TB CARE II Bangladesh: Grants Spotlight2
Introduction to the Small Grants Program
As a component of the project, TB CARE II Bangla-
desh supports nongovernmental, community based
organizations (NGOs) in urban and rural areas with
TB case notification rates below the national average to in-
crease detection and management of TB and MDR TB ser-
vices and to improve community knowledge and awareness
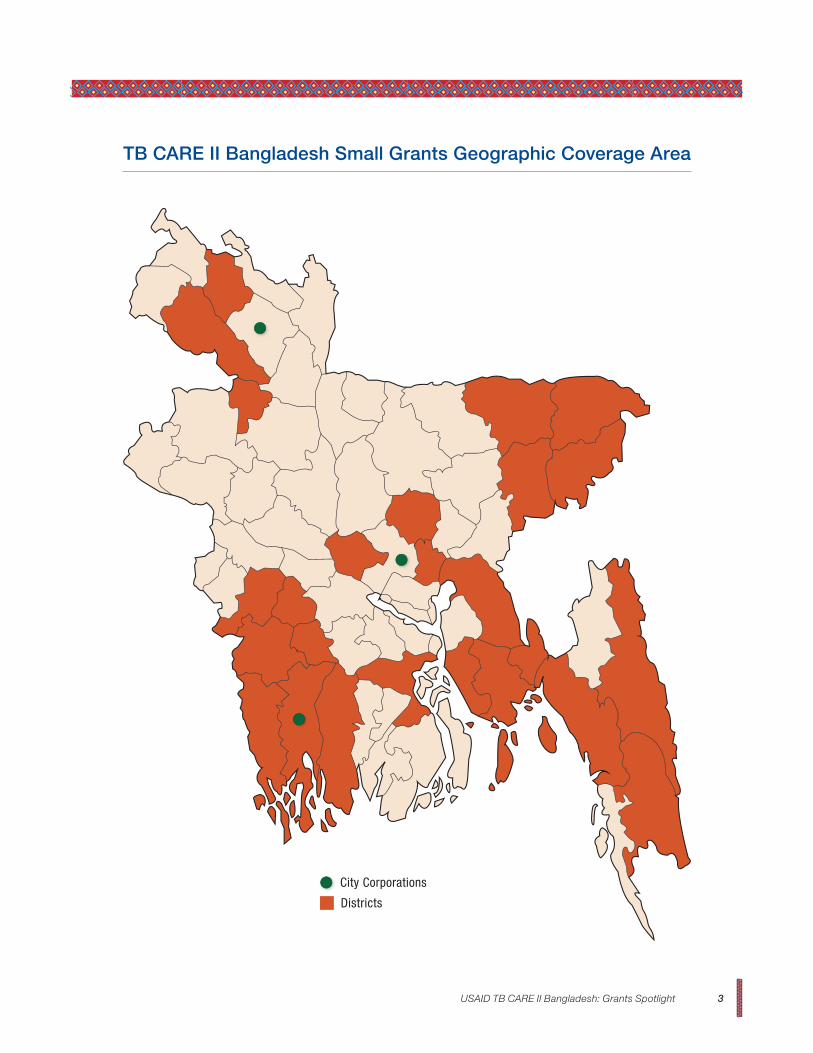
of TB and MDR TB. The geographic coverage varied under
different waves of grants as indicated in the table below.
Since April 2012, TB CARE II has supported 11 grantees
for periods of one-to-two years each. These grantees have
carried out a range of community-based activities, including:
n Tracing contacts to identify and refer presumptive
(suspected) TB and MDR TB cases among children
and adult members of active and cured TB and
MDR-TB patients;
n Sputum collection and transportation systems for
people living in remote areas with no easy access to
microscopy centers;
n Identifying and referring presumptive MDR TB cases to
GeneXpert sites for testing;
n Diagnosis and management of smear negative and
extra-pulmonary TB (EPTB) cases;
n Providing isoniazid preventive therapy (IPT) for children;
n Engaging and developing capacity of graduate and
non-graduate (village doctors) private doctors,
homeopaths, herbal practitioners and traditional
healers in TB screening and referral;
Grant WavesNo. of
Awards Made Areas Covered Award Period
Wave 1 3 15 districts: Manikganj, Gazipur, Narayanganj, Feni, Chittagong, Rangamati, Dinajpur, Joypurhat, Sunamganj, Jessore, Khulna, Barisal, Rangpur city corporation, and 157 tea gardens in Sylhet, Moulvibazar and Habiganj districts;
April 2012 to June 2014; activities in tea gardens from April 2012 to March 2014
Wave 3 9 16 districts: Bagerhat, Narail, Jhenaidah, Noakhali, Magura, Shatkhira, Comilla. Laxmipur, Nilphamari, Bandarban; Dhaka and Khulna city corporations;
April 2013 to March 2015
Sole source 2 BPA: 17 districts of Dhaka division for child TB training;
DAB: BIRDEM hospital and district level outpatient facilities for detection of TB among diabetic patients
September 2013 to July 2014
April 2013 to March 2015
n Developing capacity of maternal and child health (MCH) and family planning (FP) workers in screening and referral of presumptive TB cases;
n Coordinating with the NTP/NGOs to initiate early initiation of TB treatment and DOTS services;
n Counselling TB patients and family members on treatment adherence, side effects management, infection prevention, follow up services, etc.
n Financial support to poor patients for diagnosis of smear negative and EPTB;
n Developing capacity of NGO staff/volunteers in TB screening, referral, DOTS, counselling, contact tracing, and data collection and recording;
n Organizing community meetings to educate people about TB, importance of early diagnosis and treatment adherence, social barriers and stigma related to TB;
n Organizing drama, folk songs, and rallies to promote awareness and counter stigma about TB;
n Developing and engaging peers (cured TB patients);
n Organizing advocacy meeting with local community leaders to engage them in supporting communication activities
Grants are given to local NGOs with a proven track record or interest in the area of TB and MDR TB management. Through the grants program, these organizations have been able to provide TB education, screening and treatment ser-vices to formerly unreached or underserved populations.
USAID TB CARE II Bangladesh: Grants Spotlight 3
TB CARE II Bangladesh Small Grants Geographic Coverage Area
City Corporations
Districts

USAID TB CARE II Bangladesh: Grants Spotlight4
The TB CARE II Bangladesh Small Grants Capacity Building Model
Grantee Focus Areas
While the primary goal of the small grants
program is to provide TB services to people,
the program has also acted as a capacity-
building mechanism for local NGOs, helping them build
their technical, financial and management systems. It
also helps them establish and cultivate collaborative
partnerships with the NTP and other NGOs to sustain and
expand the provision of services after the grant ends.
With about half of TB cases remaining undetected
each year in Bangladesh, improving TB case
detection through intensified case finding efforts
is a critical activity that nearly all TB CARE II grantees
actively engage in. Grantees engage in door-to-door
campaigns, household visits to contacts of known TB
patients and defaulters (contact tracing) and community
mobilization events to screen individuals for TB, identify TB
suspects, and refer them for diagnosis and treatment. As a
result, grantees are helping to improve the case notification
and case detection rates in the districts where they work.
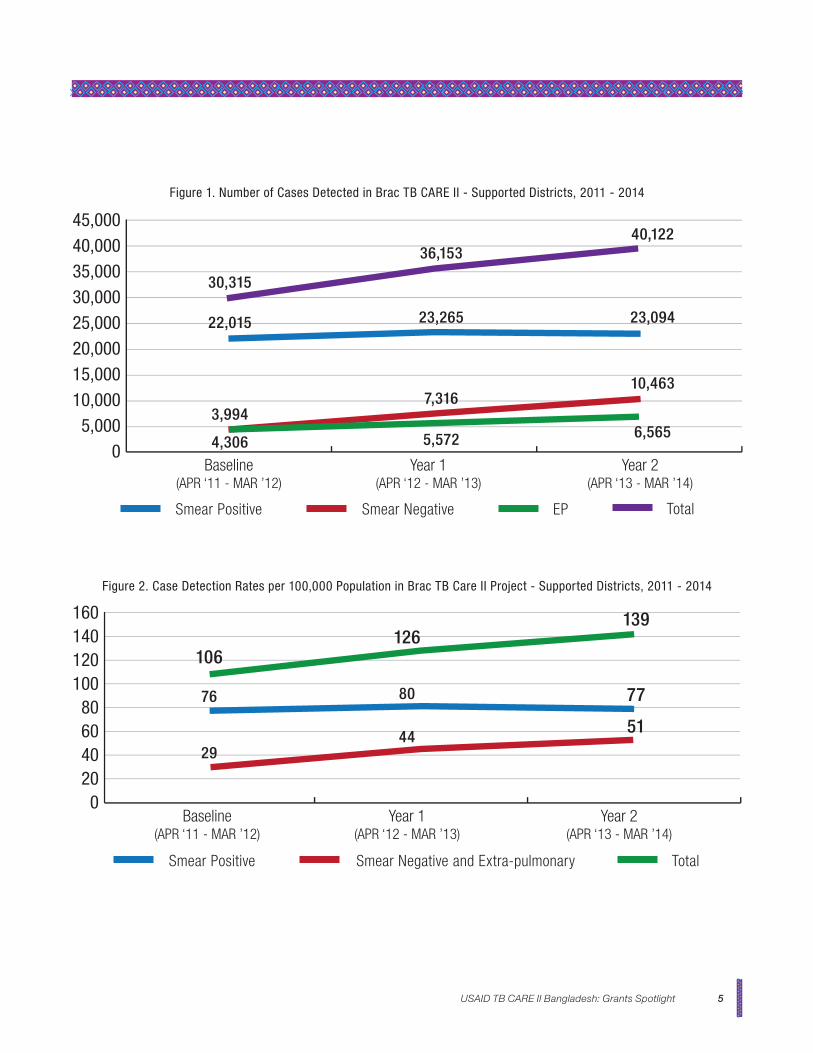
Through TB CARE II project support, grantee BRAC was
able to identify an additional 56,302 in 27 months over its
2011 baseline (Figure 1) - increasing case detection rates for
all cases from a baseline of 106 per 100,000 population to
139 per 100,000 population in 2014 (Figure 2).
Case detection of TB among the tea garden population has
always been lower than other parts of the country. With the
financial and technical support of the TB CARE II project,
HEED Bangladesh was able to streamline its strategies for
Intensified TB Case Finding
Intensified case finding (ICF)
Health workers, NGO staff, and/or
community volunteers screen individuals for
TB by asking a series of symptom screening
questions. When the symptom screen is
positive, sputum samples of suspected TB
cases are collected for diagnostic testing.
If the laboratory test confirms a diagnosis
of TB, the patient is put on appropriate
treatment and their contacts are in turn
screened and tested for TB.
TB case detection and raising community awareness and
implement them in a systematic manner among this target
population. As a result, since beginning of the project in
April 2012, case detection and notification of all forms of TB
has increased significantly compared to the baseline.
USAID TB CARE II Bangladesh: Grants Spotlight 5
Figure 1. Number of Cases Detected in Brac TB CARE II - Supported Districts, 2011 - 2014
0
10,0005,000
Baseline(APR ‘11 - MAR ’12)
Year 1(APR ‘12 - MAR ’13)
Year 2(APR ‘13 - MAR ’14)
20,00015,000
25,00030,000
40,00035,000
45,000
30,315
22,015
3,994
4,306
7,316
5,572
23,265
36,153
10,463
6,565
40,122
23,094
Smear Positive Smear Negative EP Total
Figure 2. Case Detection Rates per 100,000 Population in Brac TB Care II Project - Supported Districts, 2011 - 2014
0
4020
Baseline(APR ‘11 - MAR ’12)
Year 1(APR ‘12 - MAR ’13)
Year 2(APR ‘13 - MAR ’14)
8060
100120
160140
106
76
29
126
80
44
139
77
51
Smear Positive Smear Negative and Extra-pulmonary Total
USAID TB CARE II Bangladesh: Grants Spotlight6
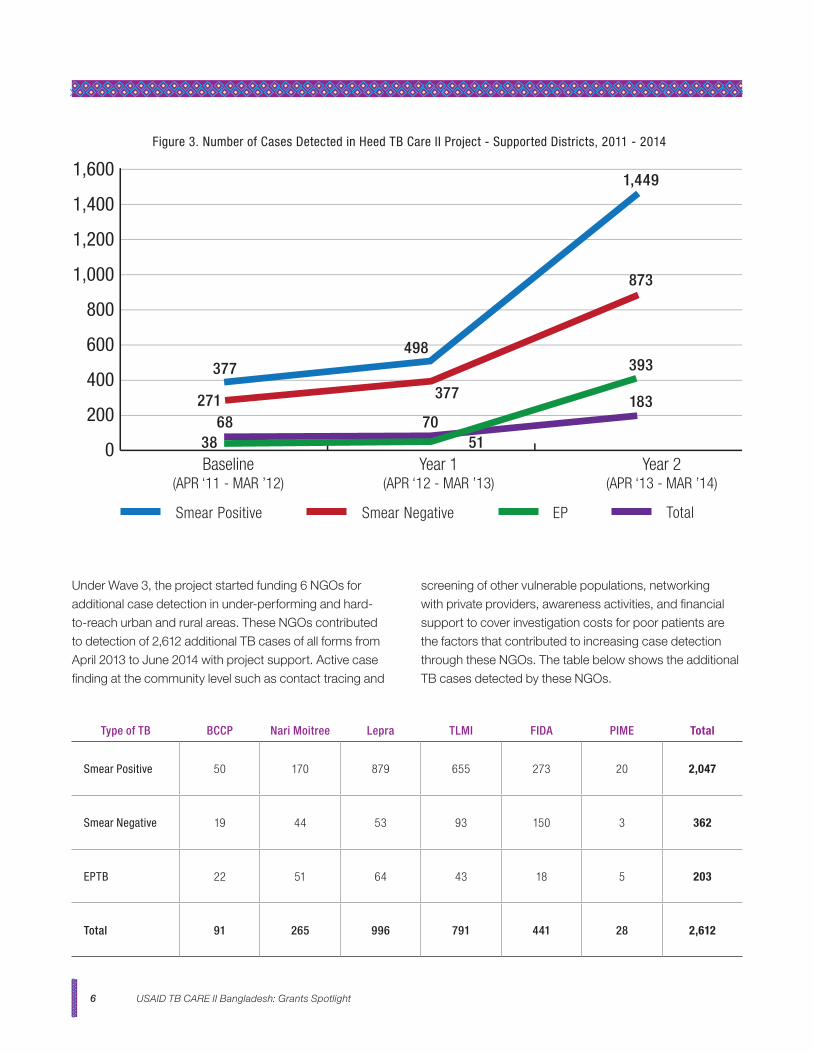
Under Wave 3, the project started funding 6 NGOs for
additional case detection in under-performing and hard-
to-reach urban and rural areas. These NGOs contributed
to detection of 2,612 additional TB cases of all forms from
April 2013 to June 2014 with project support. Active case
finding at the community level such as contact tracing and
screening of other vulnerable populations, networking
with private providers, awareness activities, and financial
support to cover investigation costs for poor patients are
the factors that contributed to increasing case detection
through these NGOs. The table below shows the additional
TB cases detected by these NGOs.
Type of TB BCCP Nari Moitree Lepra TLMI FIDA PIME Total
Smear Positive 50 170 879 655 273 20 2,047
Smear Negative 19 44 53 93 150 3 362
EPTB 22 51 64 43 18 5 203
Total 91 265 996 791 441 28 2,612
Figure 3. Number of Cases Detected in Heed TB Care II Project - Supported Districts, 2011 - 2014
0
200
Baseline(APR ‘11 - MAR ’12)
Year 1(APR ‘12 - MAR ’13)
Year 2(APR ‘13 - MAR ’14)
600
400
800
1,000
1,400
1,200
1,600
377
68271
498
1,449
873
393
183377
5170
38
Smear Positive Smear Negative EP Total
USAID TB CARE II Bangladesh: Grants Spotlight 7
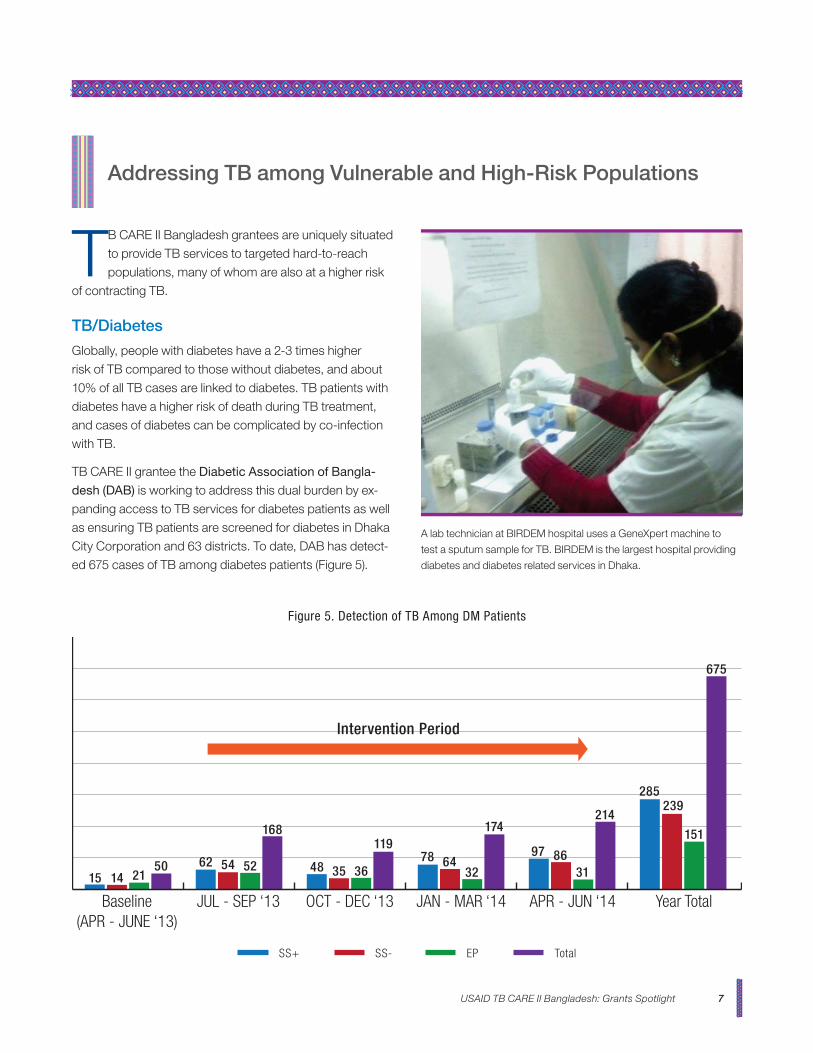
Baseline(APR - JUNE ‘13)
JUL - SEP ‘13 OCT - DEC ‘13 JAN - MAR ‘14 APR - JUN ‘14 Year Total
Figure 5. Detection of TB Among DM Patients
15 14 2150 62 54 52 48 35 36
11978 64
32
174
97 8631
214
285239
151
675
168
SS+ SS- EP Total
TB CARE II Bangladesh grantees are uniquely situated
to provide TB services to targeted hard-to-reach
populations, many of whom are also at a higher risk
of contracting TB.
TB/Diabetes
Globally, people with diabetes have a 2-3 times higher
risk of TB compared to those without diabetes, and about
10% of all TB cases are linked to diabetes. TB patients with
diabetes have a higher risk of death during TB treatment,
and cases of diabetes can be complicated by co-infection
with TB.
TB CARE II grantee the Diabetic Association of Bangla-
desh (DAB) is working to address this dual burden by ex-
panding access to TB services for diabetes patients as well
as ensuring TB patients are screened for diabetes in Dhaka
City Corporation and 63 districts. To date, DAB has detect-
ed 675 cases of TB among diabetes patients (Figure 5).
Addressing TB among Vulnerable and High-Risk Populations
A lab technician at BIRDEM hospital uses a GeneXpert machine to
test a sputum sample for TB. BIRDEM is the largest hospital providing
diabetes and diabetes related services in Dhaka.
Intervention Period
USAID TB CARE II Bangladesh: Grants Spotlight8
¹ Banu, S.et al. PLoS One. 2010 May 21;5(5):e10759. http://www.ncbi.nlm.nih.gov/pubmed/20505826
TB in Prisons
Prisoners are at a heightened risk for TB because of over-crowded, cramped living conditions and inadequate diets often found in prison settings. Prison health care systems are often ill equipped to deal with TB patients and patients often lack access to TB diagnostics and treatments. A 2010 study of Dhaka Central Jail, the largest prison in Bangla-desh, found a prevalence rate of sputum-positive pulmonary TB of 2,227/100,000¹.
TB CARE II partner BRAC used funding from a Wave 1 grant to conduct enhanced screening in twelve prisons within the project target districts. As a result, 2554 prison inmates were tested for TB and 96 cases of TB were diagnosed. Of these, 94 prisoners were registered for TB treatment.
TB in Children
TB remains a serious threat to children’s health in many parts of the world. The WHO estimates that children account
for around 500,000 new cases of TB annually, and that
In Bangladesh, more than half of TB patients seek care
in the private sector, both formal and informal. Therefore,
private medical practitioners and traditional healers must
be well-equipped to screen patients for TB and referral
them for diagnosis and treatment. TB CARE II Bangladesh
grantees are currently playing an important role in linking
private and public sector providers to ensure effective
referral and proper diagnosis and treatment follow up for
Linking with Private Providers
up to 74,000 children die from TB each year. Of the
total number of TB cases detected in Bangladesh, only
3% are childhood TB cases – compared with 9-11%
globally – signifying that many cases of childhood TB in
Bangladesh are left undetected and untreated.
Through intensified case finding and contact tracing,
eight TB CARE II grantees have detected 692 cases
of TB in children. Two grantees, BRAC and LEPRA
have also been actively engaged in the provision of INH
prophylaxis to prevent TB from developing in children
who have been in close contact with a TB patient. BRAC
had a total of 541 children registered in April – June 2013
complete the full course of INH prophylaxis during the
Wave 3 grant period.
TB CARE II grantees are actively engaged in contact
tracing and referral of childhood TB cases, as well as in
provision of isoniazid preventive therapy (IPT) for eligible
children under five.
FY 12 (Apr - Sep ‘12) FY 13 FY 14 (Oct ‘13 - Jul ‘14) Total
Child contacts <5 year evaluated for IPT 1,642 2,965 2,996 7,603
Children <5 year registered for IPT 587 545 321 1,453
Children <5 years completed INH - 1,049 78 1,127
TB CARE II small grantee Family Income Development Association
(FIDA) conducts an orientation session for non-graduate private
providers on TB screening and referral. Through a Wave 3 TB CARE II
Bangladesh grant, FIDA was able to reach 20 graduate and 150 non-
graduate private providers.
USAID TB CARE II Bangladesh: Grants Spotlight 9
TB patients in line with the NTP DOTS strategy. Grantees
also conduct advocacy meetings and networking events
with private health care providers to increase their support
for TB control and prevention efforts. Since 2012, TB CARE
II Bangladesh have reached 7599 graduate and 12,801
non-graduate providers with orientation and training on
proper TB screening and referral practices. These private
health practitioners are now poised to effectively aid TB
control efforts. For example, from April 2013 – March 2014,
the 61 private medical doctors trained by grantee LEPRA
referred 704 TB suspects for diagnosis and follow up.
TB CARE II small grantee LEPRA oriented 61 private medical doctors
on TB screening and referral from Sirajgong, Pabna, and Natore dis-
tricts. These providers in turn referred 704 TB suspects for diagnosis
and follow up.
TB CARE II grantees engage in a variety of advocacy, communication, and social mobilization (ACSM) activi-ties designed to 1) increase knowledge and awareness
of local leaders about the burden of TB disease and its impact on communities and families with TB patients, and promote their active participation in TB control, care and prevention activities; 2) improve community knowledge of TB prevention strategies as well as TB symptoms to motivate communi-ty members to seek care from health workers when TB is suspected; and 3) mobilize communities to reduce stigma
associated with TB and provide support for TB patients.
Advocacy, Communication, and Social Mobilization Activities
Sample BCC materials designed by grantee BCCP.
Outreach to Community Leaders
One of TB CARE II grantee Nari Maitree’s main project objectives was to mobilize communities to increase aware-ness about TB and encourage timely utilization of TB ser-vices in 14 wards of Dhaka City Corporation. Nari Maitree organized a series of advocacy meetings and orientation sessions with a variety of influential community leaders, including ward commissions, slum leaders, teachers at local madrasahs and orphanages, as well as with family members of current TB patients. Over the course of the one year grant, Nari Maitree was able to reach 90 teachers, 420 ward commissioners and slum leaders, 360 community leaders, and 210 family members of TB patients.
Behavior Change Communications
Grantee the Bangladesh Center for Communication Pro-grams (BCCP) received a TB CARE II grant to implement advocacy and social awareness interventions in 5 wards of Dhaka City Corporation. As part of its grant, BCCP de-signed and developed behaviour change communication (BCC) materials including posters, brochures, booklets, and stickers on TB topics including childhood TB, MDR TB, and infection control which they distributed during communi-ty-based events.
BCCP also hosted 146 video screening, where huge crowds gathered in the slum area of Mirur, Dhaka to learn about TB symptoms and be encouraged to visit the nearby clinic for a cough test.
USAID TB CARE II Bangladesh: Grants Spotlight10
Grantee Nari Maitree holds a TB orientation session for teachers from
Dhaka City madrasahs and orphanages. An informational meeting for
families of TB patients.BCCP hosts a street drama to inform community members about the
symptoms of TB.
Pre-Service Training in TB for Intern Doctors
URC awarded a sub-grant to Research, Training and
Management (RTM) International to conduct pre-service
training on programmatic management of TB for intern
doctors. Through this project, 1,308 intern doctors from 10
public and private medical college hospitals participated in
this training. The participants also received various training
materials including national guidelines on TB and child TB,
and handbook on TB control.
Child TB Training
To improve capacity of service providers to address child-
hood TB, TB CARE II awarded a sole source sub-grant to
the Bangladesh Pediatric Association (BPA) to train doctors
and health care workers from Dhaka division to improve
their skills in screening, diagnosis, and management of
child TB.
Human Resource Department
A child TB training supported by TB CARE II.
Drama and Folk Songs
Several grantees, including BCCP and Leprosy Mission
International – Bangladesh reached out to their communi-ties through street performances, dramas, and folk songs. Leprosy Mission hosted 20 events in 2013 – 2014, which drew 17,992 participants to learn about early signs and symptoms of TB. As a result, 79 TB suspects came forward to access TB services.
USAID TB CARE II Bangladesh: Grants Spotlight 11
Type of Training Number Trained Participants
Training of Facilitators (Trainers) 70 Pediatricians from Medical College and District Hospitals
4-day training on Diagnosis and management of child TB
544Government doctors - UHFPO, Peditric Consultant, Medial Officer
1-day Orientation of on Child TB 15 District Civil Surgeons
1-day Orientation on National Child TB Guidelines 622 Private graduate doctors from upazilas and districts
1-day Orientation on screening and referral of children with TB symptoms
8,345Health Assistant, SACMO, Health Inspector, Program Organizer
The training content and duration were tailored to meet
varying needs of the participants. A total of 544 doctors,
including paediatricians from sub-district hospitals and
medical college hospitals, attended the four-day training
with focus on diagnosis and management of child TB. The
one-day orientation on national guidelines for management
of child TB was conducted for 622 private medical doctors.
Additionally, 8,345 health workers, most of whom work at
the community level, were oriented on screening and refer-
ral of presumptive child TB cases.

For more information, please visit:
http://tbcare2.org or http://www.urc-chs.com/