updates in pcos research: facts & perspectives
TRANSCRIPT
UPDATES IN PCOS RESEARCH:FACTS & PERSPECTIVES
Daria Lizneva1Dept. of OB/GYN, Georgia Regent University Augusta, GA, United States2Dept. of Reproductive Health Protection, Scientific Center of Family Health and Human Reproduction, Irkutsk, Eastern Siberia, Russian Federation
1
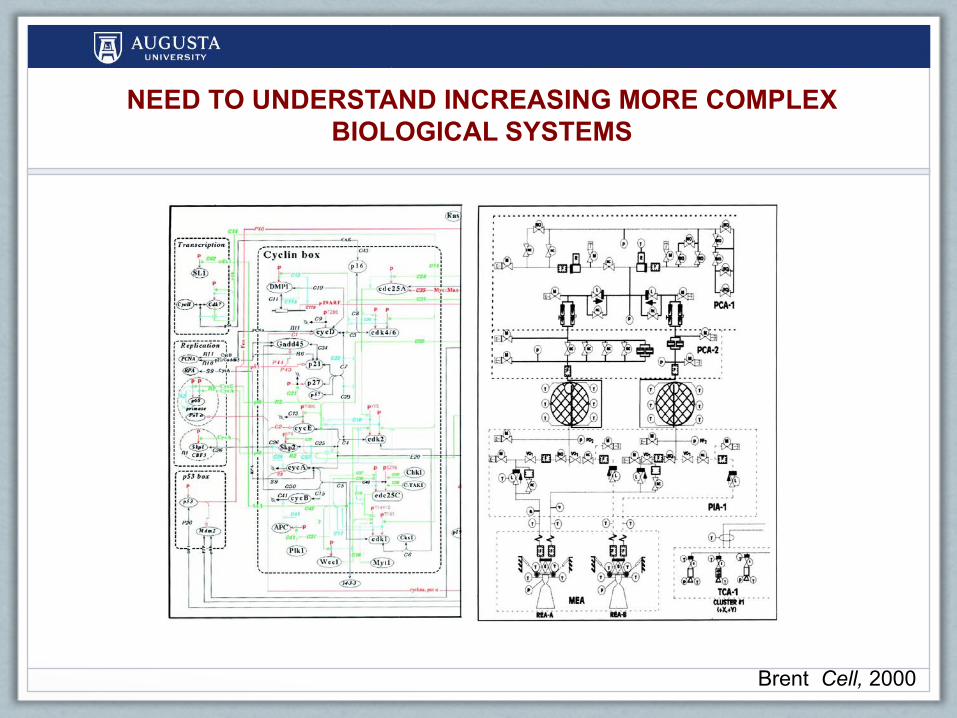
NEED TO UNDERSTAND INCREASING MORE COMPLEX BIOLOGICAL SYSTEMS
Brent Cell, 2000

MULTI- AND INTERDISCIPLINARY RESEARCH WILL BE REQUIRED TO SOLVE THE “PUZZLE” OF COMPLEX DISEASES AND CONDITIONS
• Genes• Behavior• Diet/Nutrition• Infectious agents• Environment • Society• ???

UPDATES IN PCOS: FACTS & PERSPECTIVES
4
§Evolutionary
§Epidemiologic
§Genetic
DETERMINANTS OF POLYCYSTIC OVARY SYNDROME

EVOLUTIONARY DETERMINANTS OF PCOS
• Reduced fertility and fecundity
• However, it has persisted hundreds of thousands of years with a significant prevalence (5-15% of female population)
5
PCOS: AN EVOLUTIONARY PUZZLE
PCOS: ADAPTIVE EVOLUTION
6
Metabolic Advantages = “Thrifty Gene Hypothesis”
Fessler DM, Natterson-Horowitz B, Azziz R. Fertil Steril. 2016 Jul;106(1)42-7; Escobar-Morreale, H.F., Luque-Ramirez, M., and San Millan, J.L. Endocr Rev. 2005; 26: 251–282; Shaw, L.M. and Elton, S. Br J Obstet Gynecol. 2008; 115: 144–148; Corbett, S.J., McMichael, A.J., and Prentice, A.M. Am J Hum Biol. 2009;21: 587–598
• Past: food shortage → “thrifty” phenotype conserved energy
• Multigenerational facultative adjustment to food scarcity
• No negative selection in populations with a long history of successful agriculture
• Prevalence of PCOS is too low to reflect the past positive selection

7
Immune Advantages = “Hygiene Hypothesis”
Fessler DM, Natterson-Horowitz B, Azziz R. Fertil Steril. 2016 Jul;106(1):42-7; Escobar-Morreale, H.F., Luque-Ramirez, M., and San Millan, J.L. Endocr Rev. 2005; 26: 251–282; Vasunilashorn, S., Crimmins, E.M., Kim, J.K., Winking, J., Gurven, M., Kaplan, H. et al. Am J Hum Biol. 2010; 22: 731–740
• Past: pathogen-rich ancestral environments → disease protection offered by ↑ inflammatory state
• Contemporary small societies with ↑ pathogens → no capacity for facultative adjustment of inflammation
PCOS: ADAPTIVE EVOLUTION

8
Reproductive Longevity Advantages
Fessler DM, Natterson-Horowitz B, Azziz R. Fertil Steril. 2016 Jul;106(1):42-7. Saxena, R., Bjonnes, A.C., Georgopoulos, N.A., Koika, V., Panidis, D., and Welt, C.K. Hum Reprod. 2015; 30: 1697–1703; Perry, J.R., Hsu, Y.H., Chasman, D.I., Johnson, A.D., Elks, C., Albrecht, E. et al. Hum Mol Genet. 2014; 23: 2490–2497; Schmidt, J., Brännström, M., Landin-Wilhelmsen, K., and Dahlgren, E. J Clin Endocrinol Metab. 2011; 96: 2178–2185; Wild, S., Pierpoint, T., Jacobs, H., and McKeigue, P. Hum Fertil (Camb). 2000; 3: 101–105
• PCOS ~ associated with enhanced reproductive longevity• PCOS locus near RAD50 - DNA double-strand break repair• ↑ AMH in PCOS - larger ovarian primordial follicle pool
• Studies do not confirm later age at menopause
PCOS: ADAPTIVE EVOLUTION
9
Musculoskeletal Advantages
Fessler DM, Natterson-Horowitz B, Azziz R. Fertil Steril. 2016 Jul;106(1):42-7.Escobar-Morreale, H.F., Luque-Ramirez, M., and San Millan, J.L. Endocr Rev. 2005; 26: 251–282Shaw, L.M. and Elton, S. Br J Obstet Gynecol. 2008; 115: 144–148Corbett, S.J., McMichael, A.J., and Prentice, A.M. Am J Hum Biol. 2009;21: 587–598
• Greater muscle mass, bone density, possible aggressiveness → favored survival in the past
• Difficult to understand how increased androgenization at the cost of reduced fertility enhanced overall ‘fitness’
PCOS: ADAPTIVE EVOLUTION

10Kemper, K.E., Saxton, S.J., Bolormaa, S., Hayes, B.J., and Goddard, M.E. Selection for complex traits leaves little or no classic signatures of selection. BMC Genomics. 2014; 15: 246
PCOS: ADAPTIVE EVOLUTION
However, LITTLE evidence for a strong positive selection of PCOS-
susceptibility alleles
(e.g. prevalence would be higher)
PCOS: NON-ADAPTIVE EVOLUTION
11
Persistence theory
Fessler DM, Natterson-Horowitz B, Azziz R. Fertil Steril. 2016 Jul;106(1):42-7; Kemper, K.E., Saxton, S.J., Bolormaa, S., Hayes, B.J., and Goddard, M.E. BMC Genomics. 2014; 15: 246 Legro, R.S., Kunselman, A.R., Demers, L., Wang, S.C., Bentley-Lewis, R., and Dunaif, A. J Clin Endocrinol Metab. 2002; 87: 2134–2138; Casarini, L. and Brigante, G; J Clin Endocrinol Metab. 2014; 99: E2412–E2420; Casarini, L., Simoni, M., and Brigante, G. Reprod Biomed Online. 2016; 32: 350–361
• PCOS was Asymptomatic• or• PCOS traits were in Balance in the population:
• one group has a ‘fitness’ advantage / another has a ‘fitness’ disadvantage• e.g. “good for men / bad for women”, where several
genetic loci associated with the disorder differently modulate the reproductive parameters of men vs. those of women
• Little data is yet available

12
Source population
UPDATES IN PCOS:EPIDEMIOLOGIC PERSPECTIVE
13
PCOS in source population
TO STUDY• Disease Frequency• Measures of Association (Risks)• Causality
UPDATES IN PCOS:EPIDEMIOLOGIC PERSPECTIVE

14
PCOS in source population
PCOS seeking medical care
UPDATES IN PCOS:EPIDEMIOLOGIC PERSPECTIVE

UPDATES IN PCOS:EPIDEMIOLOGIC PERSPECTIVE
15
PCOS seeking medical care
PCOS in source population
TO STUDY• Diagnostic modalities• Treatment options
16
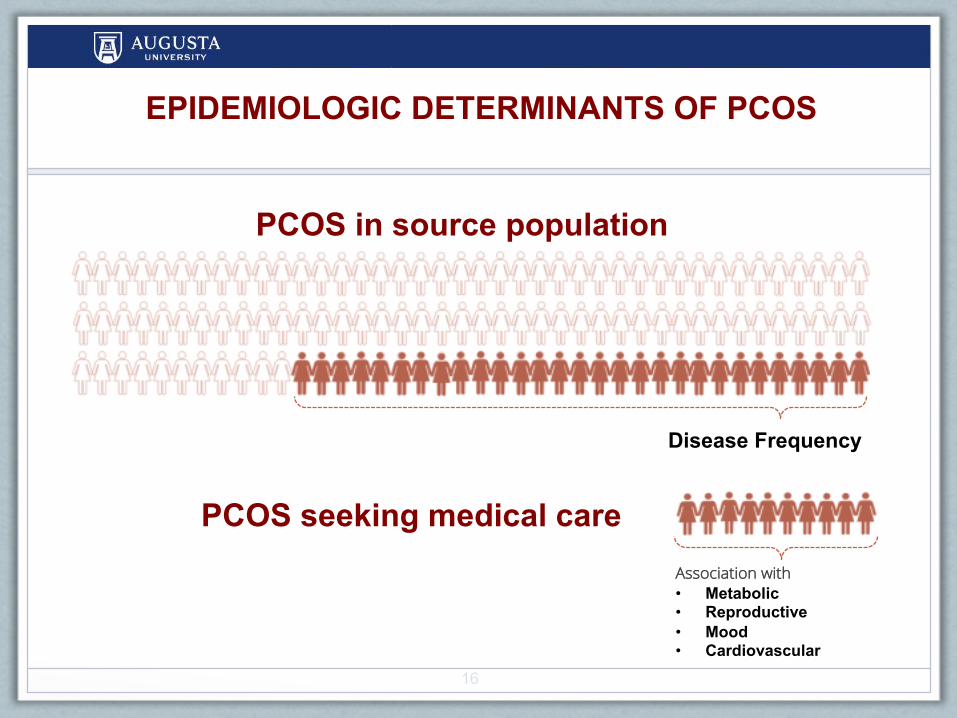
PCOS seeking medical care
PCOS in source population
Disease Frequency
Association with• Metabolic• Reproductive• Mood• Cardiovascular
EPIDEMIOLOGIC DETERMINANTS OF PCOS

17
Are PCOS patients seeking medical care representative of the
disorder?

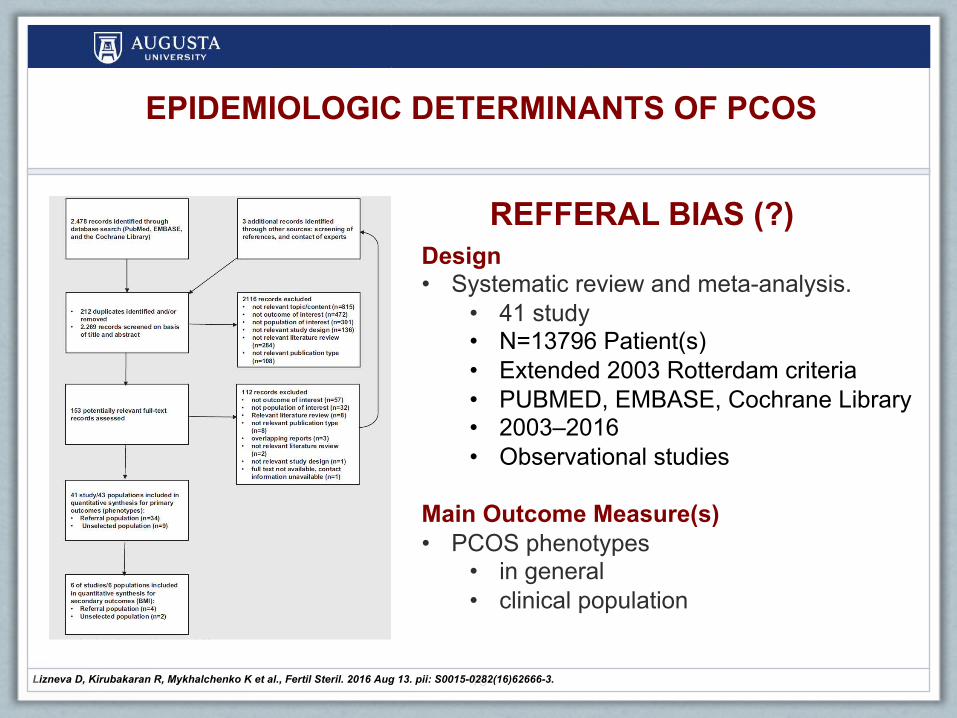
REFFERAL BIAS (?)
18
EPIDEMIOLOGIC DETERMINANTS OF PCOS
3 original study – general and clinical PCOS • same region / same center / same tools
USA (NIH PCOS) Ezeh et al.• ↑ prevalence of the more severe PCOS phenotypes• greater BMI• more severe hirsutism• more pronounced hyperandrogenemia
China (Rott 2003 PCOS) Ma et al.• ↑ prevalence of PCOS phenotype A and• ↑ rate of menstrual dysfunction
Spain (Functional HA) Luque-Ramírez et al. • ↑ more hirsute, • ↑ % clinical and biochemical HA, • ↑ % obesity• ↑ % prevalence of PCOS
U. Ezeh, B.O. Yildiz, R. Azziz. J Clin Endocrinol Metab, 98 (2013), pp. E1088; M. Luque-Ramirez, M. Alpanes, R. Sanchon, E. Fernandez-Duran, A.E. Ortiz-Flores; H.F. Escobar-Morreale. Eur J Endocrinol, 173 (2015), pp. 603–610; Y.M. Ma, Chin Med J (Engl), 123 (2010), pp. 2185–2189
REFFERAL BIAS (?)
19Lizneva D, Kirubakaran R, Mykhalchenko K et al., Fertil Steril. 2016 Aug 13. pii: S0015-0282(16)62666-3.
EPIDEMIOLOGIC DETERMINANTS OF PCOS
Design• Systematic review and meta-analysis.
• 41 study• N=13796 Patient(s)• Extended 2003 Rotterdam criteria• PUBMED, EMBASE, Cochrane Library• 2003–2016• Observational studies
Main Outcome Measure(s)• PCOS phenotypes
• in general • clinical population

REFFERAL BIAS (?)
20Lizneva D, Kirubakaran R, Mykhalchenko K et al., Fertil Steril. 2016 Aug 13. pii: S0015-0282(16)62666-3.
EPIDEMIOLOGIC DETERMINANTS OF PCOS
Design• Systematic review and meta-analysis.
• 41 study• N=13796 Patient(s)• Extended 2003 Rotterdam criteria• PUBMED, EMBASE, Cochrane Library• 2003–2016• Observational studies
Main Outcome Measure(s)• PCOS phenotypes
• in general • clinical population
21
EPIDEMIOLOGIC DETERMINANTS OF PCOS
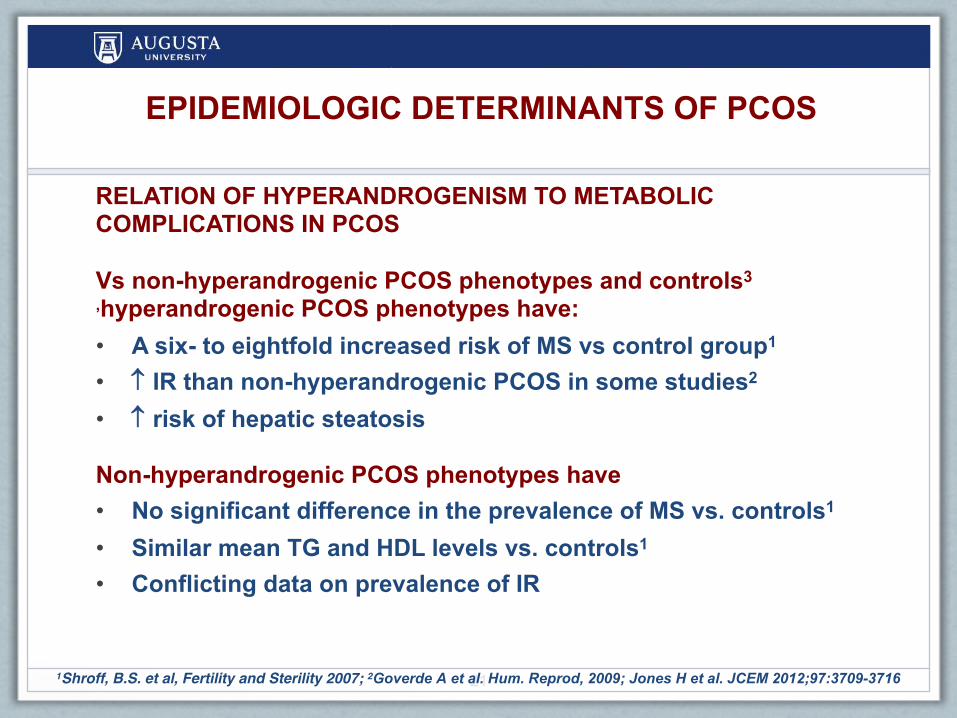
RELATION OF HYPERANDROGENISM TO METABOLIC COMPLICATIONS IN PCOS
Vs non-hyperandrogenic PCOS phenotypes and controls3 ,hyperandrogenic PCOS phenotypes have:• A six- to eightfold increased risk of MS vs control group1
• IR than non-hyperandrogenic PCOS in some studies2
• risk of hepatic steatosis
Non-hyperandrogenic PCOS phenotypes have• No significant difference in the prevalence of MS vs. controls1
• Similar mean TG and HDL levels vs. controls1
• Conflicting data on prevalence of IR
1Shroff, B.S. et al, Fertility and Sterility 2007; 2Goverde A et al. Hum. Reprod, 2009; Jones H et al. JCEM 2012;97:3709-3716
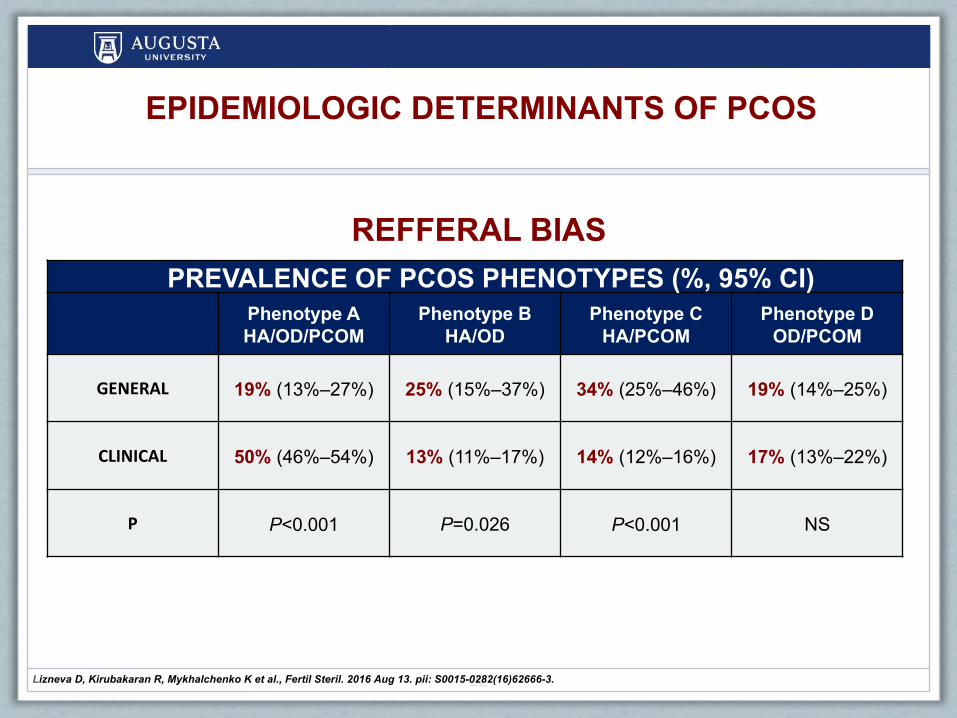
REFFERAL BIAS
22
PREVALENCE OF PCOS PHENOTYPES (%, 95% CI)Phenotype AHA/OD/PCOM
Phenotype BHA/OD
Phenotype CHA/PCOM
Phenotype DOD/PCOM
GENERAL 19% (13%–27%) 25% (15%–37%) 34% (25%–46%) 19% (14%–25%)
CLINICAL 50% (46%–54%) 13% (11%–17%) 14% (12%–16%) 17% (13%–22%)
P P<0.001 P=0.026 P<0.001 NS
Lizneva D, Kirubakaran R, Mykhalchenko K et al., Fertil Steril. 2016 Aug 13. pii: S0015-0282(16)62666-3.
EPIDEMIOLOGIC DETERMINANTS OF PCOS
23Lizneva D, Kirubakaran R, Mykhalchenko K et al., Fertil Steril. 2016 Aug 13. pii: S0015-0282(16)62666-3.
EPIDEMIOLOGIC DETERMINANTS OF PCOS
23
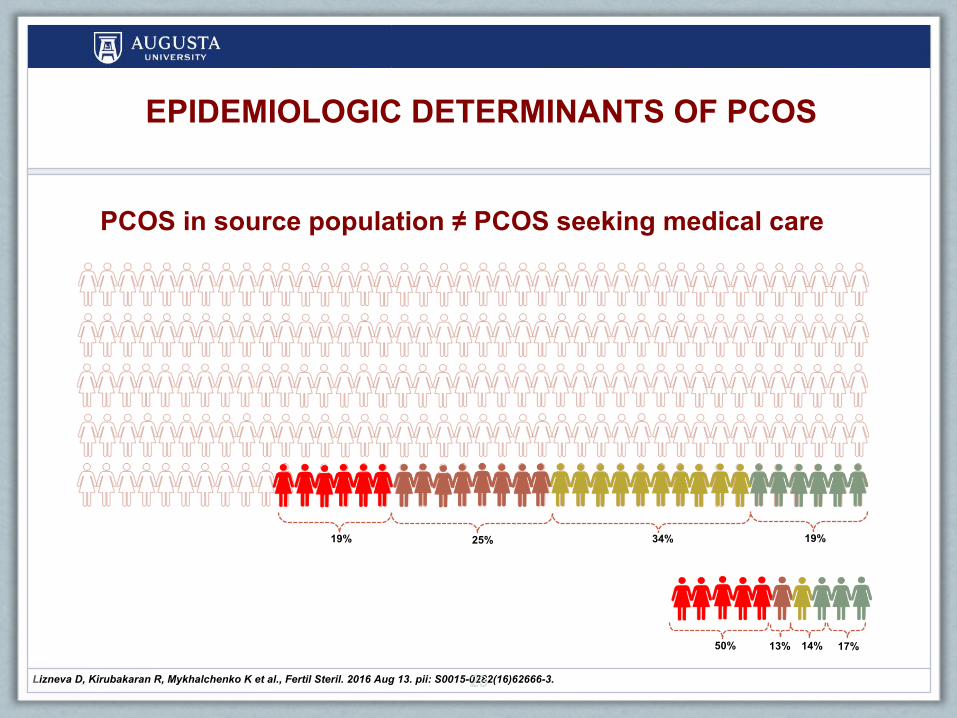
PCOS in source population ≠ PCOS seeking medical care
50% 13% 14% 17%
19% 25% 34% 19%

24Lizneva D, Kirubakaran R, Mykhalchenko K et al., Fertil Steril. 2016 Aug 13. pii: S0015-0282(16)62666-3.
GENERALPOPULATION:3studies CLINICALPOPULATION:2studies
REFFERAL BIAS: BMI
0.53 kg/m2, 95% CI, 0.39, 0.66 kg/m2, P<0.001
0.18 kg/m2,95% CI, 0.15, 0.51 kg/m2, P=0.30
EPIDEMIOLOGIC DETERMINANTS OF PCOS
PCOS PCOSCONTROL
CONTROL

25
Does the current data confirm the “Persistence Hypothesis’ (i.e.
PCOS was essentially asymptomatic in prehistory)?

26
Eastern Siberia Settings§ Scientific Center of Family
Health Protection and Human Reproduction
§ Two regions:Ø Irkutsk ØUlan-Ude
§ 4 cites
§ Collected at baseline
§ 2015 - 2017 years
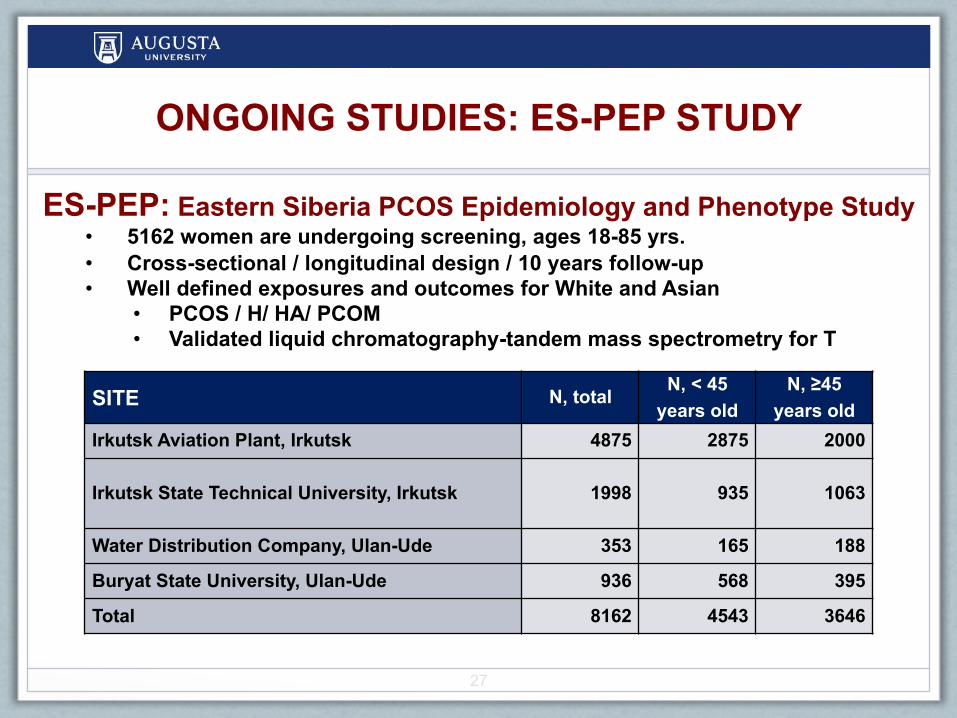
ONGOING STUDIES: ES-PEP STUDY
ONGOING STUDIES: ES-PEP STUDY
27
SITE N, total N, < 45 years old
N, ≥45 years old
Irkutsk Aviation Plant, Irkutsk 4875 2875 2000
Irkutsk State Technical University, Irkutsk 1998 935 1063
Water Distribution Company, Ulan-Ude 353 165 188
Buryat State University, Ulan-Ude 936 568 395
Total 8162 4543 3646
ES-PEP: Eastern Siberia PCOS Epidemiology and Phenotype Study• 5162 women are undergoing screening, ages 18-85 yrs.• Cross-sectional / longitudinal design / 10 years follow-up• Well defined exposures and outcomes for White and Asian
• PCOS / H/ HA/ PCOM • Validated liquid chromatography-tandem mass spectrometry for T

28
Race
Caucasian (Russian)
Asian (Buryat ~ northern subgroup / Mongols)
vs
ONGOING STUDIES: ES-PEP STUDY
29
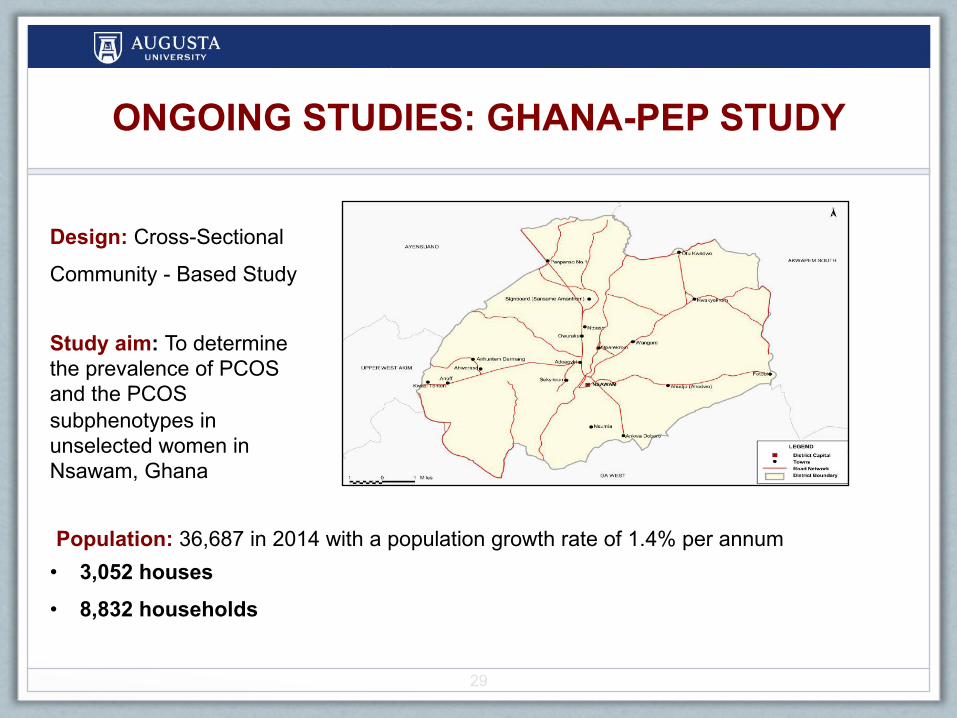
ONGOING STUDIES: GHANA-PEP STUDY
Design: Cross-Sectional
Community - Based Study
Study aim: To determine the prevalence of PCOS and the PCOS subphenotypes in unselected women in Nsawam, Ghana
• 3,052 houses• 8,832 households
Population: 36,687 in 2014 with a population growth rate of 1.4% per annum

30
GENETIC DETERMINANTS OF PCOS:GWAS
B.C. Fauser, B.C. Tarlatzis, R.W. Rebar et al. Fertil Steril, 97 (2012), pp. 28–38.e25. R.S. Legro, S.A. Arslanian, D.A. Ehrmann et al. J Clin Endocrinol Metab, 98 (2013), pp. 4565–4592
LOCUS NEAREST GENE SNP P DISCOVERY REPLICATION
1 2p16.3 LHCGR rs13405728 7.55 × 10−21 CHN SRD, EUR, EGY, IND, ARB, CHN2 2p16.3 FSHR rs2268361 9.89 × 10−13 CHN EUR, ARB, CHN
rs2349415 2.35 × 10−12 CHN3 2p21 THADA rs13429458 1.73 × 10−23 CHN EUR, CHN4 2q34 ERBB4 rs1351592 1.2 × 10−12 EUR5 5q31.1 RAD50 rs13164856 3.5 × 10−9 EUR6 8p32.1 GATA4 rs804279 8.0 × 10−10 EUR7 9q33.3 DENND1A rs2479106 8.12 × 10−9 CHN EUR
8 9q22.32 C9orf3 rs4385527 5.87 × 10−9 CHN CHN, EUR9 11p14.1 FSHB rs11031006 1.9 × 10−8 EUR EUR, CHN10 11q22.1 YAP1 rs1894116 1.08 × 10−22 CHN EUR, CHN
rs11225154 7.6 × 10−11 EUR CHN11 12q14.3 HMGA2 rs2272046 1.95 × 10−21 CHN EUR12 12q13.2 RAB5B/SUOX rs705702 8.64 × 10−26 CHN EUR13 12q21.2 KRR1 rs1275468 1.9 × 10−8 EUR14 16q12.1 TOX3 rs4784165 3.64 × 10−11 CHN EUR15 19p13.3 INSR rs2059807 1.09 × 10−8 CHN EUR16 20q13.2 SUMO1P1 rs6022786 1.83 × 10−9 CHN
31
GENETIC DETERMINANTS OF PCOS:GWAS
B.C. Fauser, B.C. Tarlatzis, R.W. Rebar et al. Fertil Steril, 97 (2012), pp. 28–38.e25. R.S. Legro, S.A. Arslanian, D.A. Ehrmann et al. J Clin Endocrinol Metab, 98 (2013), pp. 4565–4592
The potential for gene discovery to improve diagnosis and treatment of PCOS is promising, though there is much to be
done in the field before the current findings can be translated to the clinic

32
SUMMARY
• Persistence theory
• Need longitudinal data for PCOS in general
population to understand
• Causation
• Risks
• Further explore genetic/epigenetic factors1Shroff, B.S. et al, Fertility and Sterility 2007; 2Goverde A et al. Hum. Reprod, 2009; Jones H et al. JCEM 2012;97:3709-3716

ACKNOWLEDGMENTS
USA
RUSSIA
1Dept. of Obstetrics and Gynecology, Medical College of Georgia, Georgia Regents University, 2Dept. of Medicine, Medical College of Georgia, Georgia Regents University, Augusta 3Dept. of Reproductive Health Protection, Scientific Center of Family Health and Human Reproduction, 4Department of Population, Family and Reproductive Health, School of Public Health, University of Ghana, Legon, Accra,
Ghana.
Ricardo Azziz 1,2
Yen Hao Chen1
33
Larisa Suturina3
Adanu RM4

Igor Stravinsky, 1951: “The Rake's Progress”Tom Rakewell deserts Anne Trulove by marrying Baba the Turk, the famous bearded lady