update on diagnosis and management of fetal … · neonatal and fetal ga-adjusted ÒnormalÓ...
TRANSCRIPT

www.fetalmedicinebarcelona.org/
UPDATE ON DIAGNOSIS AND MANAGEMENT OF
FETAL GROWTH RESTRICTIONEduard Gratacos
Center for Maternal-Fetal Medicine and NeonatologyHospital Clinic & Hospital Sant Joan de Deu - University de Barcelona
www.fetalmedicinebarcelona.org

www.medicinafetalbarcelona.org/
Neonatal and Fetal GA-adjusted “normal” weight in the same population

www.medicinafetalbarcelona.org/
SGA Unknown (constitutional + others)
IUGRPlacental insufficiency
ISOLATED FETAL SMALLNESS = POORER PROGNOSISPerinatal and Long-term Outcomes
Exclude extrinsic cause
Exclude primary fetal defect
Poor perinatal outcome + IUFD(Doppler) Signs of adaptation
Perinatal outcome normal - No IUFDNO signs of adaptation
FGR vs. SGA: DIFFERENT MANAGEMENT

www.medicinafetalbarcelona.org/
UtA >p95
CPR <p5(<p15)
EFW CENTILE <3
0%
10%
20%
30%
40%
50%
8%11%
40%
Controls All normal Any abnormal
%
Prognostic criteria of “poor outcome”-SGACS for distress and/or neonatal acidosis
N=509 SGA + 509 controls
Figueras 2013

www.medicinafetalbarcelona.org/
IUGR = abnormal CPR or UtA or EFW<p3early vs late-onset IUGR
Savchev 2013

Red Line EARLY IUGRRed Line LATE IUGR
www.medicinafetalbarcelona.org/
RATIONALE FOR A STAGE-BASED APPROACH TO THE MANAGEMENT OF FGR
PLACENTAL DISEASE HYPOXIA ACIDOSIS SERIOUS INJURY DEATH
cardiac ischemiaDiastolic failure
Systolic cardiac failure
Centralization
Increment placental impedance
cCTG: reduced STV
Diagnostic/chronic markersEarly and Late IUGR
Prognostic/Acute markersEarly IUGR
IVIIIIIIStage fetal deterioration
HIGHMODERATELOWRisks of prematurity

www.medicinafetalbarcelona.org/
1. Identify small fetus
2. FGR vs. SGA
3. Early vs. Late
4. Parameters for fetal follow-up
5. Stage-based management protocol

www.medicinafetalbarcelona.org/
1. Identify small fetus
2. FGR vs. SGA
3. Early vs. Late
4. Parameters for fetal follow-up
5. Stage-based management protocol
Return

www.medicinafetalbarcelona.org/
Neonatal and Fetal GA-adjusted “normal” weight in the same population

Mula 2013, Lobmaier 2013www.medicinafetalbarcelona.org/
IMPROVING DETECTION: THE DEFINITION OF “RESTRICTION”Birthweight inverse relation with perinatal outcome AND brain-cardiac remodelling
!
INTEGRATED 3T SCREENING FOR LATE-PREGNANCY COMPLICATIONSLate-PE, Late-IUGR, Stillbirth

www.medicinafetalbarcelona.org/
1. Identify small fetus
2. FGR vs. SGA
3. Early vs. Late
4. Stage-based management protocol
Return

www.medicinafetalbarcelona.org/
SGA Unknown (constitutional + others)
IUGRPlacental insufficiency
ISOLATED FETAL SMALLNESS = POORER PROGNOSISPerinatal and Long-term Outcomes
Exclude extrinsic cause
Exclude primary fetal defect
Poor perinatal outcome + IUFD(Doppler) Signs of adaptation
Perinatal outcome normal - No IUFDNO signs of adaptation
FGR vs. SGA: DIFFERENT MANAGEMENT

www.medicinafetalbarcelona.org/
Constitutionally small Placental insufficiency Extrinsic cause
Primary fetal defect
SGA FGR
The discovery of UA and hemodynamics of IUGR
FGR = abnormal UA Doppler
20 30 4025 35
0
N cases
N cases
UA Doppler +(EARLY-ONSET)
UA Doppler N(LATE-ONSET)
Savchev 2013

www.medicinafetalbarcelona.org/
0
10
20
30
40
Neonatal acidosis CS for distress Abnormal NBAS Any
%
Figueras 2011
SGA: proportion of perinatal adverse outcomes in 376 consecutive cases

www.medicinafetalbarcelona.org/
IMPACT OF NON-DETECTED IUGR ON LATE FETAL MORTALITYBarcelona2005-2010
0%
10%
20%
30%
40%
50%
FGR Unknown Others
25%30%
45%
Classification of stillbirth by relevant condition at birth (ReCoDe): population-based cohort studyGardosi et al. BMJ 2005 and 2013
IUGR as relevant condition identified in 43-60%
Overall stillbirth rate (/ 1000 births) 4.2, but only 2.4 in non-SGA pregnancies, increasing to 9.7 with antenatally detected IUGR and 19.8 in not detected IUGR.

www.medicinafetalbarcelona.org/
UtA >p95
CPR <p5 EFW CENTILE <3
0%
10%
20%
30%
40%
50%
8%11%
40%
Controls All normal Any abnormal
%
Prognostic criteria of “poor outcome”-SGACS for distress and/or neonatal acidosis
N=509 SGA + 509 controls
Figueras 2012

www.medicinafetalbarcelona.org/
Distribution of cases when IUGR = abnormal UA Doppler
Savchev 2013

www.medicinafetalbarcelona.org/
Distribution of cases when IUGR = abnormal CPR or UtA or EFW<p3
Savchev 2013
www.medicinafetalbarcelona.org/
1. Identify small fetus
2. FGR vs. SGA
3. Early vs. Late
4. Stage-based management protocol
Return

www.fetalmedicinebarcelona.org/
IUGR
SGA?
20 30 4025 35
0
3
6 %
IUGR= low CPR or high UtA or EFW<p3 or low PlGF
EARLY IUGR (1%) LATE IUGR (5-7%)
PROBLEM: MANAGEMENT PROBLEM: DIAGNOSIS
Placental disease: high (UA+, PE high) Placental disease: low (UA-, PE low)
Hypoxia ++: systemic CV adaptation Hypoxia +/-: central CV adaptation
Tolerance to hypoxia. Natural history Low tolerance: no natural history
High mortality and morbidity Low mortality but poor long outcome.
32w @diagnosis

www.medicinafetalbarcelona.org/
FETAL DETERIORATION IN PLACENTAL INSUFFICIENCY
PLACENTAL DISEASE COMPENSATED HYPOXIA DECOMPENSATED HYPOXIA SERIOUS INJURYDEATH
cardiac ischemiaDiastolic failure
Systolic cardiac failure
Centralization
Increment placental impedance
growth
MIDDLE CEREBRAL A. <p5
CPR <p5
DUCTUS VENOSUS >p95 and a-
CTG ABNORMAL
UTERINE A. >p95
cCTG: reduced short-term variability
Ao ISTHMUS >p95
UMBILICAL A. >p95

www.medicinafetalbarcelona.org/
FETAL DETERIORATION IN PLACENTAL INSUFFICIENCY EARLY VS LATE IUGR (>34s)
PLACENTAL DISEASE COMPENSATED HYPOXIA DECOMPENSATED HYPOXIA SERIOUS INJURYDEATH
cardiac ischemiaDiastolic failure
Systolic cardiac failure
growth
UMBILICAL A. >p95
DUCTUS VENOSUS >p95 and a-
CTG / BPP ABNORMAL
Placental injury <30%
mild hypoxiano cardiovascular adaptation
minimal tolerance to hypoxia
MIDDLE CEREBRAL A. <p5
CPR <p5
UTERINE A. >p95
Ao ISTHMUS >p95
Centralization
Increment placental impedance

www.fetalmedicinebarcelona.org/
IUGR
SGA?
20 30 4025 35
0
3
6 %
IUGR= low CPR or high UtA or EFW<p3 or low PlGF
EARLY IUGR (1%) LATE IUGR (5-7%)
PROBLEM: MANAGEMENT PROBLEM: DIAGNOSIS
Placental disease: high (UA+, PE high) Placental disease: low (UA-, PE low)
Hypoxia ++: systemic CV adaptation Hypoxia +/-: central CV adaptation
Tolerance to hypoxia. Natural history Low tolerance: no natural history
High mortality and morbidity Low mortality but poor long outcome.
32w @diagnosis

www.medicinafetalbarcelona.org/
1. Identify small fetus
2. FGR vs. SGA
3. Early vs. Late
4. Parameters for fetal follow up
4. Stage-based management protocol
Return

umbilical arterynormal and anormal hemodynamics
DS
Cardiac pump normal function
Cardiac pump abnormal function
Placental status
<30%
placenta + cardiac ischemia

middle cerebral arterynormal and abnormalhemodynamics
[marked vasodilation]
[normal waveform]
[mild vasodilation]
Normal oxygenation
hypoxia

www.medicinafetalbarcelona.org/
30 % venous return
REFLECTS DIASTOLIC PRESSURE IN RIGHT (AND LEFT) HEART

ductus venosusnormal and abnormal hemodynamics
Venous vessel: pulsation due to retrograde pressure
S DA
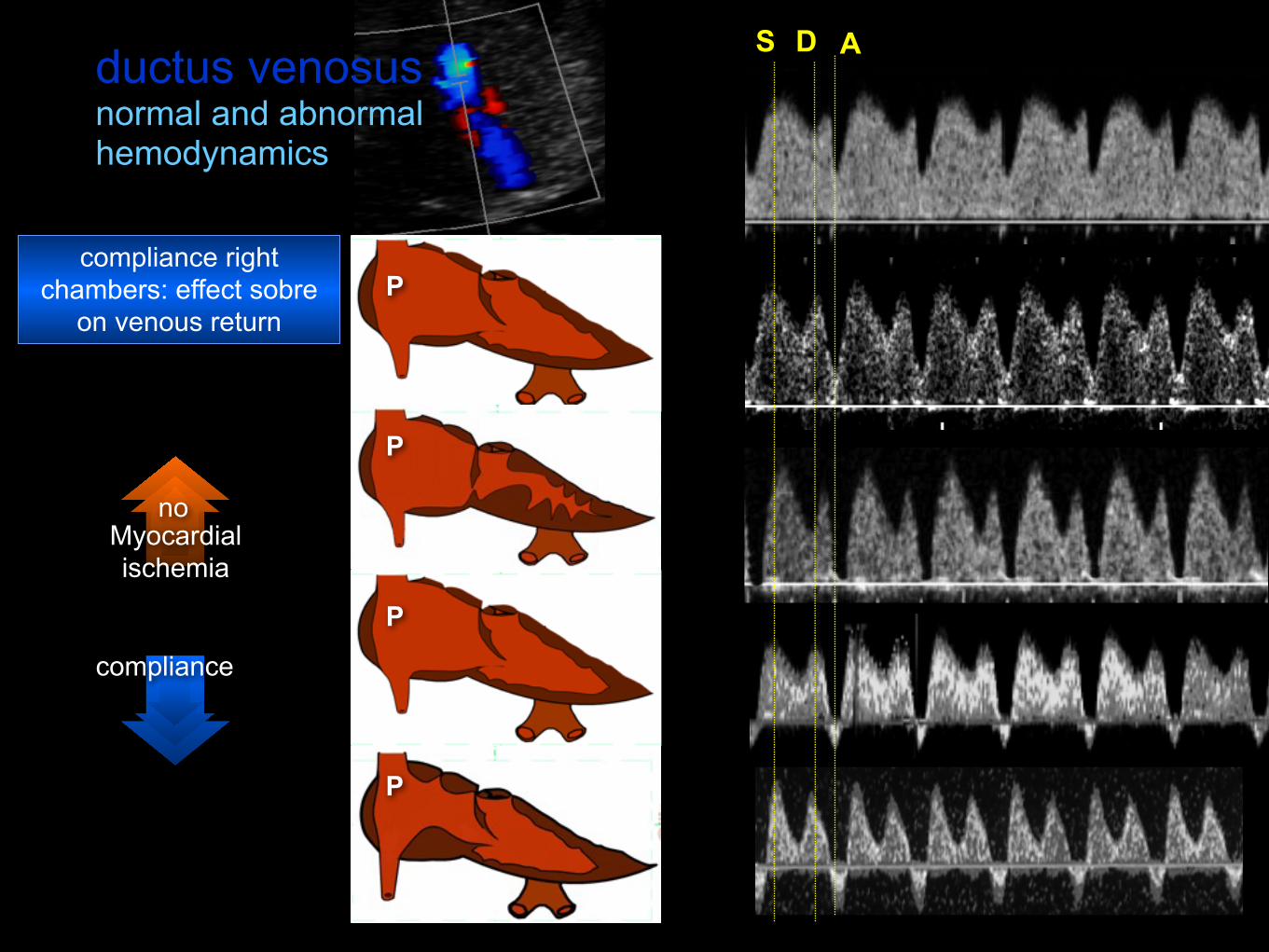
ductus venosusnormal and abnormal hemodynamics
compliance right chambers: effect sobre
on venous return
DS A
P
P
P
P
Myocardial ischemia
compliance
no




Perinatal >90% 30-‐40% <10%Mortality
www.medicinafetalbarcelona.org/
<26 26-28 >28
Baschat 2003Hecher 2003 Grivell 2009Cruz-‐Lemini 2012
Early-onset IUGRPROBLEM #1: MORTALITY
DVa (rev)
Yes No
60%
19%
cCTG-‐STV<3 ms
Pathological CGT

Perinatal >90% 30-‐40% <10%Mortality
www.medicinafetalbarcelona.org/
<29 29-32 >32.0
Fouron 2004Del Rio 2008Cruz-‐MarOnez 2012
Early-onset IUGRPROBLEM #2: (NEUROLOGICAL) MORBIDITY
0
15
30
45
60
(%)
ControlsIUGR antegrade AoIIUGR retrograde AoI
ControlsIUGR DV<5 z-scoreIUGR DV>5 z-score
**
Brain US anomalies in 30w IUGR

www.medicinafetalbarcelona.org/
1. Identify small fetus
2. FGR vs. SGA
3. Early vs. Late
4. Parameters for fetal follow up
5. Stage-based management protocol
Return

www.medicinafetalbarcelona.org/
IUGR = abnormal CPR or UtA or EFW<p3
Savchev 2013

Red Line EARLY IUGRRed Line LATE IUGR
www.medicinafetalbarcelona.org/
RATIONALE FOR A STAGE-BASED APPROACH TO THE MANAGEMENT OF FGR
PLACENTAL DISEASE HYPOXIA ACIDOSIS SERIOUS INJURY DEATH
cardiac ischemiaDiastolic failure
Systolic cardiac failure
Centralization
Increment placental impedance
cCTG: reduced STV
Diagnostic/chronic markersEarly and Late IUGR
Prognostic/Acute markersEarly IUGR
IVIIIIIIStage fetal deterioration
HIGHMODERATELOWRisks of prematurity

www.medicinafetalbarcelona.org/
Protocol IUGRFirst step: UtA + CPR + EFW = SGA or IUGR
CPR<p5
Ut A >p95
MCA<p5
DV (a rev)
CGT decelerations of reduced short-term
variability
REDV DV >p95
I low EFW (<p3) or mild placental resistance / redistribution
III Severe placental resistance / redistribution
III Severe hemodynamic adaptation - Low suspicion acidosis
IV High suspicion of acidosis - High risk of death
AEDV AoI >p95

Delivery Any Ome 30 34 37
Mort. >90% 50% <10%Morb. >90% 50%
www.medicinafetalbarcelona.org/
<26w 26-28 28-32 32-34 34-37
CriteriaDV(a-‐)
cCTG abn.CTG dec.
DV>p95UV puls REDV
(a) AEDV(b) AoI>95 CPR>p95
UtA>p95MCA<p5
EFW<p3
Stage IV III II I
Mode CS CS CS or LI LI
IUGRManagement protocol according to severity stages
Follow-‐up Hours/Daily 1-‐2 d 2/w 1/w







www.medicinafetalbarcelona.org/
The main goal in FGR is identification
Small fetus (EFW<p10) must be divided in: FGR (placenta, poor perinatal and long-term outcome)
SGA (we don’t know, perinatal outcome N, poor long term)
Early and late-onset FGR (GA 32s) represent two distinct phenotypes of the same disease
Clinically, a single stage-based protocol allows optimizing decisions in all cases