unicef flour fortification strategy & action plan · unicef flour fortification strategy &...
TRANSCRIPT

UNICEF Flour Fortification Strategy & Action Plan
Proposed by Laila Luopa, Health Communications Intern
July 2013
Supporting Organizations:
Emory University, Rollins School of Public Health
TABLE OF CONTENTS
FINAL REPORT .................................................................................................................................. 3
APPENDIX A: SWOT Charts .......................................................................................................... 6
APPENDIX B: Logic Models ......................................................................................................... 10
APPENDIX C: 4 P’s of Marketing ............................................................................................... 14
APPENDIX D: Logos ....................................................................................................................... 16
APPENDIX E: Key Communications Messages ..................................................................... 17
APPENDIX F: External Communications Plan ..................................................................... 19
APPENDIX G: TV Media Strategy .............................................................................................. 21
APPENDIX H: Health Provider’s Toolkit ................................................................................ 24
APPENDIX I: Grant Proposal ...................................................................................................... 27
APPENDIX J: Economics of Fortification ................................................................................ 33
FINAL REPORT
1. Mission Statement The communications strategy is a framework to guide all internal and external communications in the process of passing legislation regarding flour fortification, fortifying flour, and educating/marketing to target audiences in Armenia.
2. Current Status To address the worsening situation in regard of micronutrient deficiency, in 2008 UNICEF initiated a national discussion on the need and feasibility of fortifying flour with iron and folic acid in Armenia as a public health intervention in addressing micronutrient deficiencies. As a result of UNICEF’s intensive advocacy, a Steering Committee under the authority of the Prime Minister with high representation from concerned ministries, National Assembly and international organizations was established to coordinate all activities regarding the flour fortification initiative in the country. A Concept Note and a Plan of Action Budget on Implementation of Flour Fortification Program in Armenia was approved by the Government as a legal basis for implementation of flour fortification activities. The needs of eight major milling companies (which supply about 85% of the total flour needs in the country) have been assessed and UNICEF has procured the required number of feeders to be installed in the mills. In addition, the country has already drafted legislative framework for sanctioned production of fortified flour, which includes legislation and technical standards for production. The proposed mandatory flour fortification law will be raised again to Parliament in August 2013. The legislation was brought before Parliament twice before but both times it was tabled for later action. UNICEF Armenia is hopeful that the law will be passed before the start of 2014 as support has been found in the President and Prime Minister.
3. Process of the Development of the Strategy Prior to leaving at Atlanta, I read as much as I could about Armenian culture and flour fortification best practices. I also met with several people to discuss this project, including: Sarah Zimmerman, Flour Fortification Initiative (FFI) Communications Coordinator; Becky Handforth, FFI Europe Associate; Helena Pachón, FFI Senior Nutrition Scientist; Bob Baldwin, FFI Senior Advisor; and Quentin Johnson, FFI Technical Coordinator. I continued to consult with those listed during my time in Armenia. In addition, I prepared a preliminary marketing campaign for Armenian flour millers as a part of a social marketing class I took Spring 2013. In Armenia, I worked primarily with UNICEF Armenia’s Health & Nutrition Program Officer, Liana Hovakimyan, and the Assistant Health & Nutrition Program Officer, Mihran Hakobyan. Together we identified four target audiences for our communications campaign:
Policy Makers
Millers Consumers Healthcare providers
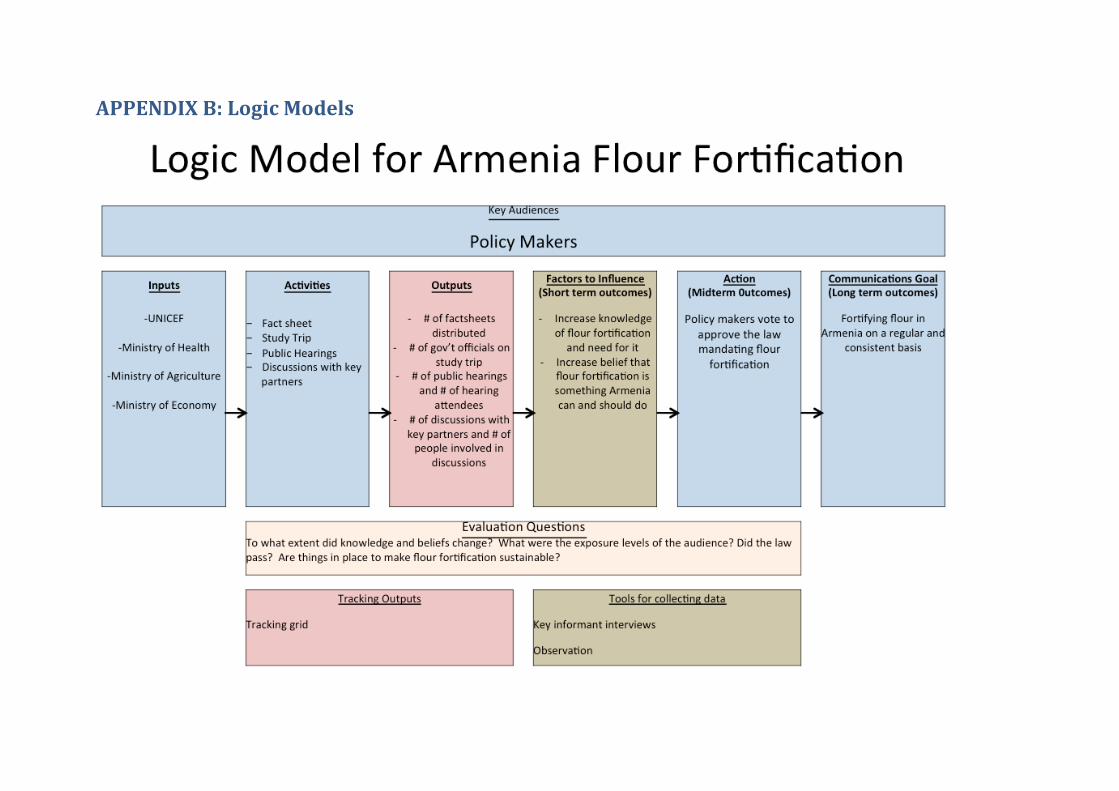
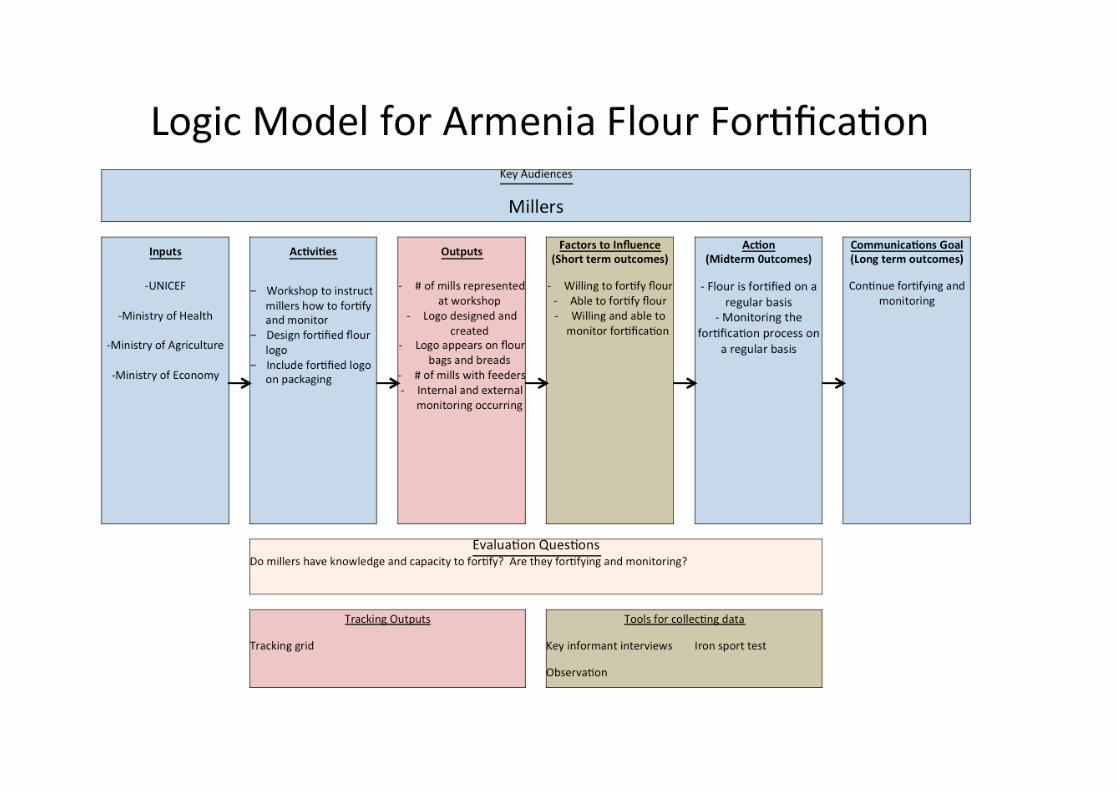
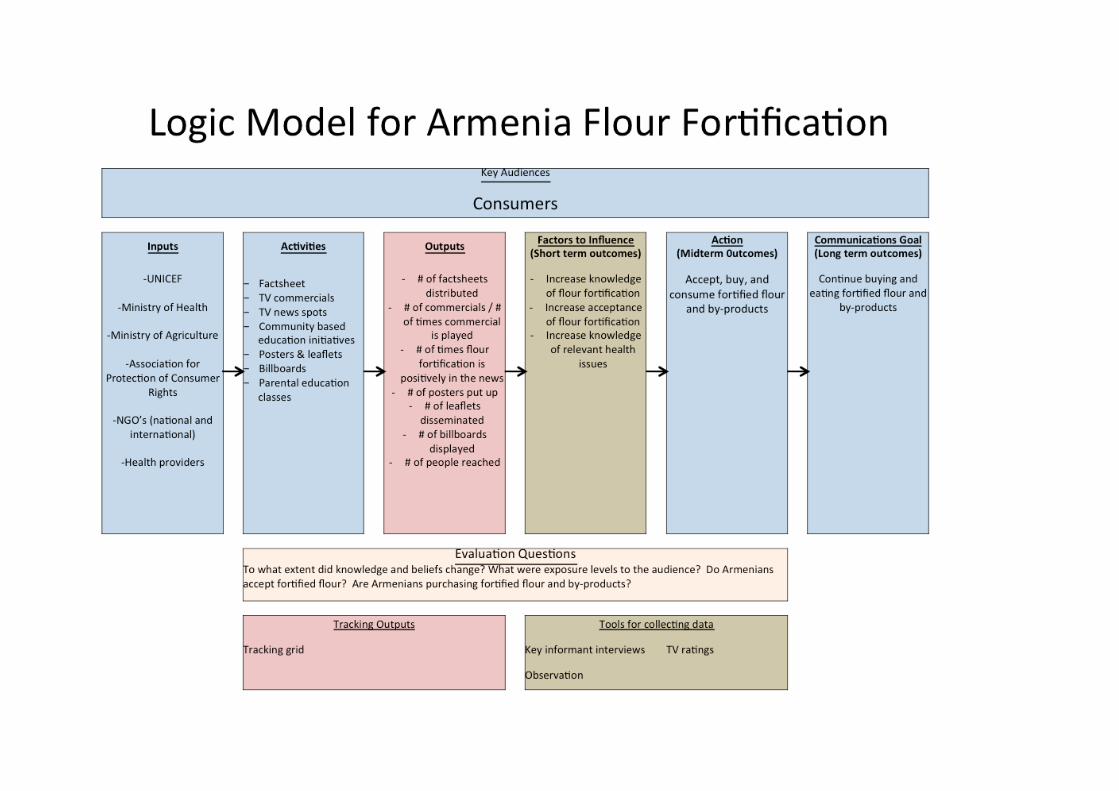
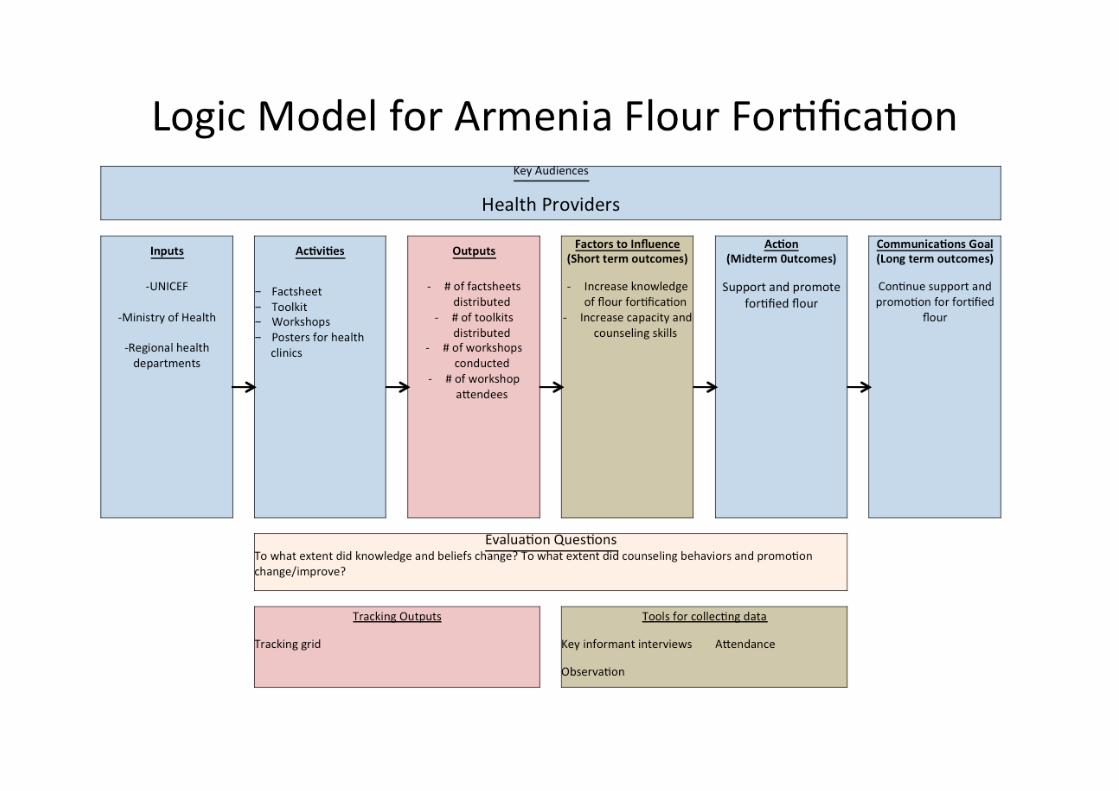
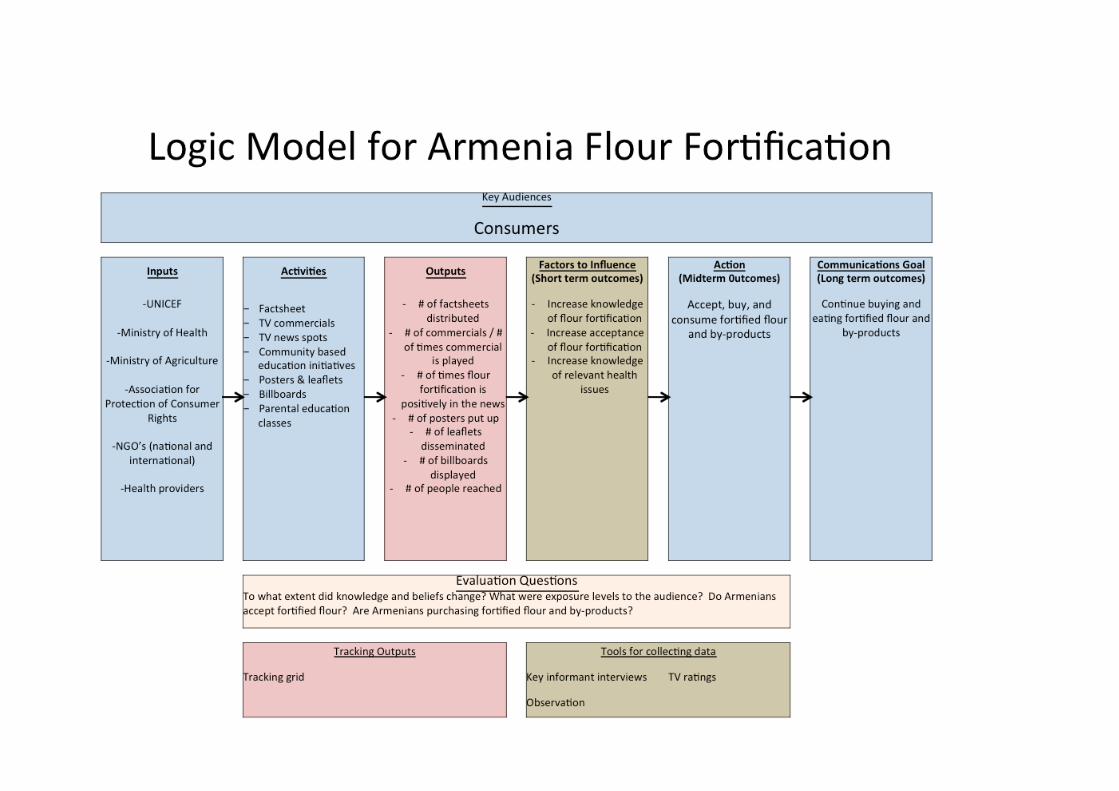
To assist my understanding of the situation, I did a literature review of all materials related to flour fortification in Armenia and visited a flourmill and several bakeries to see more about how flour is made, acquired, and used by Armenians. To map out the current situation of flour fortification amongst target groups, the Nutrition and Health UNICEF staff (Liana and Mihran) assisted me in creating Strengths, Weaknesses, Opportunities, and Threats (SWOT) charts for each audience. Please see Appendix A. From there, we developed logic models that detail the activities, goals, and indicators of the campaign for each target audience. Please see Appendix B. I applied the 4 P’s of Marketing (Product, Price, Place, Promotion) to each of the target audiences and their goals. This helped to identify the challenges with each audience. Please see Appendix C.
4. The Campaign One of the most important pieces of the campaign will be the logo that will go on the bags of flour, and our campaign materials that will signal to consumers that flour has been fortified. The logo will be used primarily on the 25 kilogram bags of flour and potentially on smaller bags prepared for consumers. Bakers and consumers buy bags of flour. Most bread that is made by bakers and sold in stores is unpackaged; therefore the logo cannot be placed on bread packaging, as there is none. Liana, Mihran, and I felt that the logo’s target audience is women as they are the ones who buy groceries and manage their family’s health. Using UNICEF staff as a focus group, I designed three logos that will be voted on by the government ministries to determine which will be best for our campaign. I also suggest conducting focus groups to see what messages each logo sends and what resonates most with women of reproductive age, our primary consumer target audience as they are the ones who buy groceries and take care of the family’s health. Please see Appendix D for logo designs. It is also important to note that even with the best logo, how the logo communication is designed and rolled out will play a key role in brand perception. I also made a list of key communications messages for the flour fortification campaign. Please see Appendix E. This document can help inform all future communications materials and help to keep messages consistent. I wrote a communication action plan to guide activities when a grant has been secured and UNICEF is ready to engage in flour fortification communications with external audiences: consumers and health providers. This is a prioritized list that includes cost estimates. Please see Appendix F. We decided that TV would be the primary mode to deliver our communications messages, thus I created an additional TV media strategy. Using research on TV
usage by USAID, I highlighted important goals and suggested activities. Please see Appendix G. In addition to these materials, we identified a need to build capacity amongst health providers, so that they will be well prepared to counsel patients and respond to questions regarding flour fortification. Thus I created a health providers’ toolkit that will be distributed along with pre-existing fact sheets. Please see Appendix H. When it comes time to begin our campaign, I would recommend starting focus groups or a pilot program to test and ensure the effectiveness of our campaign. In addition, it will be important to tie this campaign to the success of iodized salt. The population, including government, view salt iodization in their country as a strong success and an effective public health measure. By highlighting the similarities of these two initiatives, it can positively affect views on flour fortification.
5. Other materials
I drafted a grant proposal that can be used to request funds for the remaining parts of the project. Please see Appendix I. To assist with particular campaign messages to policy makers, I compiled a small list of resources that discuss the economic benefits of fortification in general and specific to Armenia. Please note that this document is not my own work. It is the highlights of several studies for UNICEF’s easy reference. See Appendix J. One of the biggest obstacles for this campaign will be the increase in bread prices, especially for policy makers and consumers. As it is not addressed anywhere else in the materials I have prepared for the campaign, I wanted to do so here. Bread prices have increased three times within the last year, and UNICEF felt that another small increase would blend in with those increases. The information gathered on the economics of fortification (Appendix J) is to assist specifically in this area. Educating consumers on the cost and benefits of fortification will help increase acceptance. In addition, comparing the flour fortification to salt iodization will illustrate how spending a little bit more on fortified food can be an effective public health measure.
6. Follow Up The UNICEF Armenia Health & Nutrition section has requested that I continue to work on this project. Pending available funds, I will join UNICEF Armenia and government representatives on their study tour to Canada in October 2013. I have also been invited to return to Armenia once the law is passed to assist with implementation of this project. The timing for this is yet to be determined.
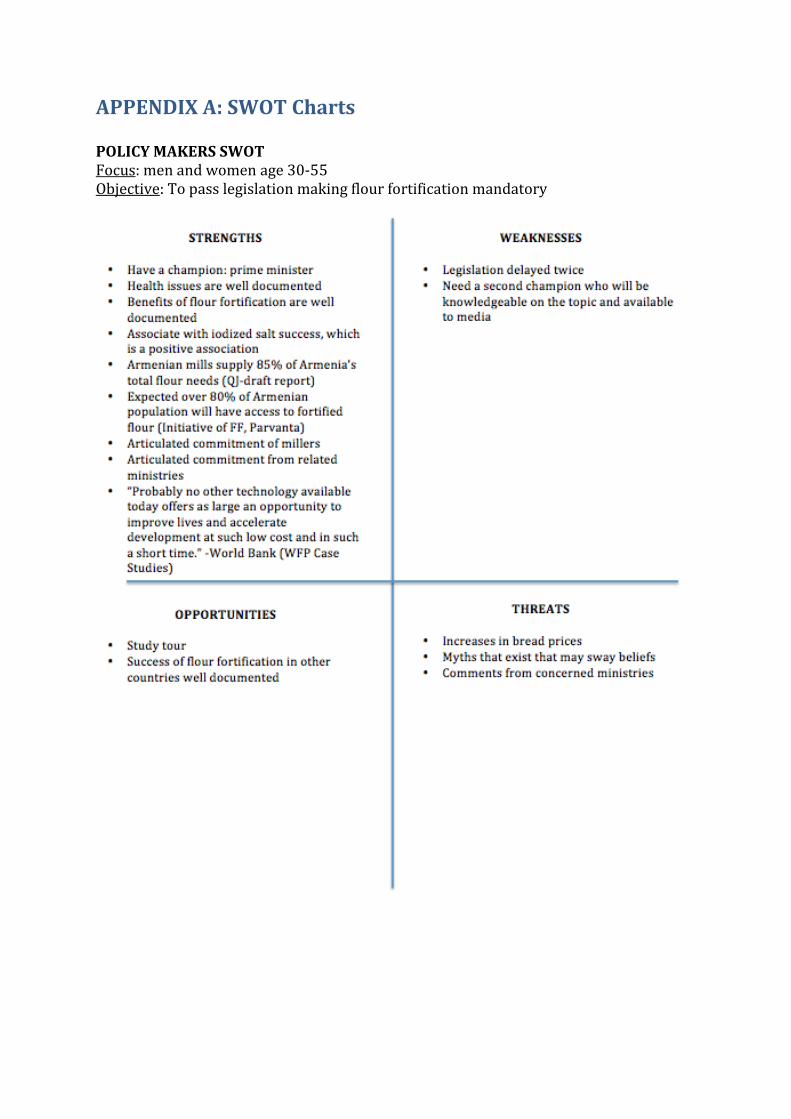
APPENDIX A: SWOT Charts POLICY MAKERS SWOT Focus: men and women age 30-55 Objective: To pass legislation making flour fortification mandatory
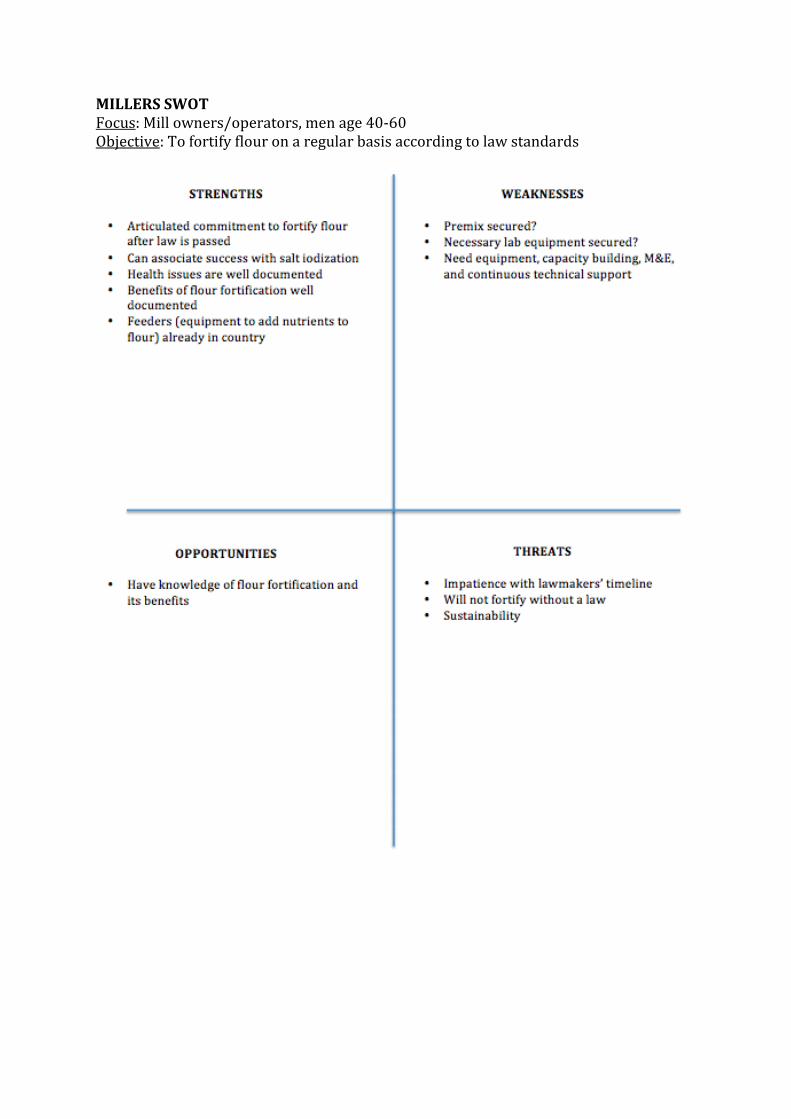
MILLERS SWOT Focus: Mill owners/operators, men age 40-60 Objective: To fortify flour on a regular basis according to law standards
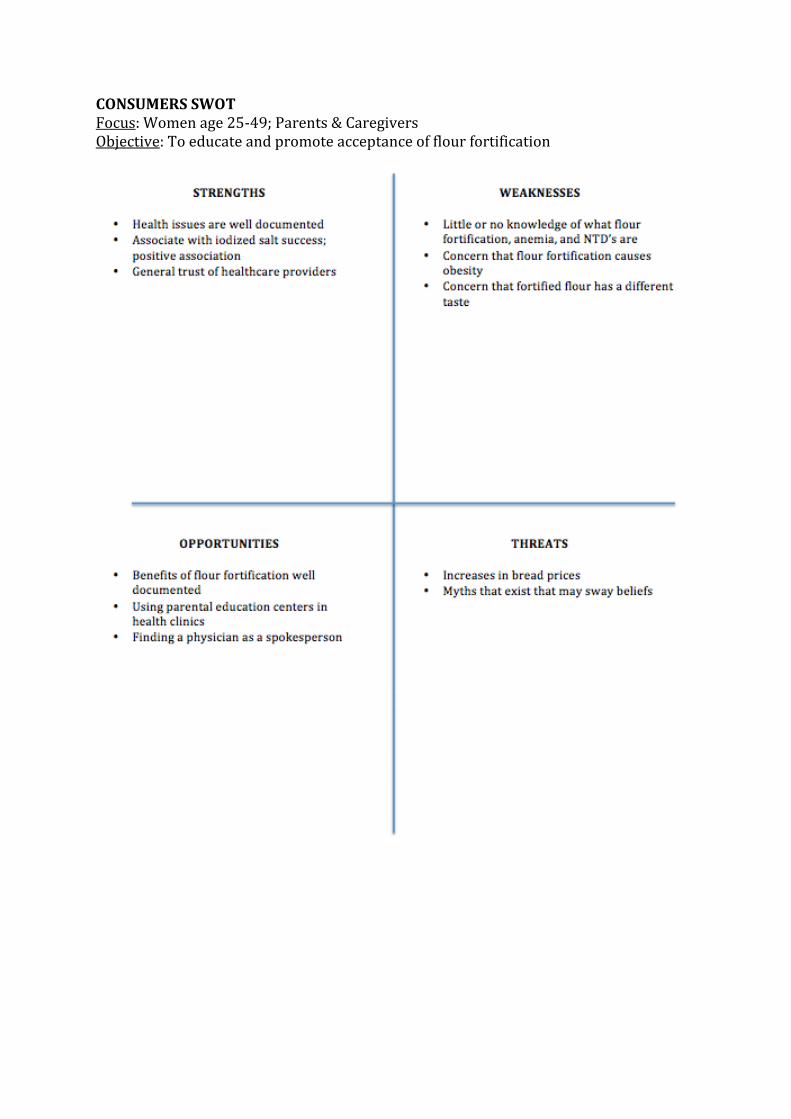
CONSUMERS SWOT Focus: Women age 25-49; Parents & Caregivers Objective: To educate and promote acceptance of flour fortification
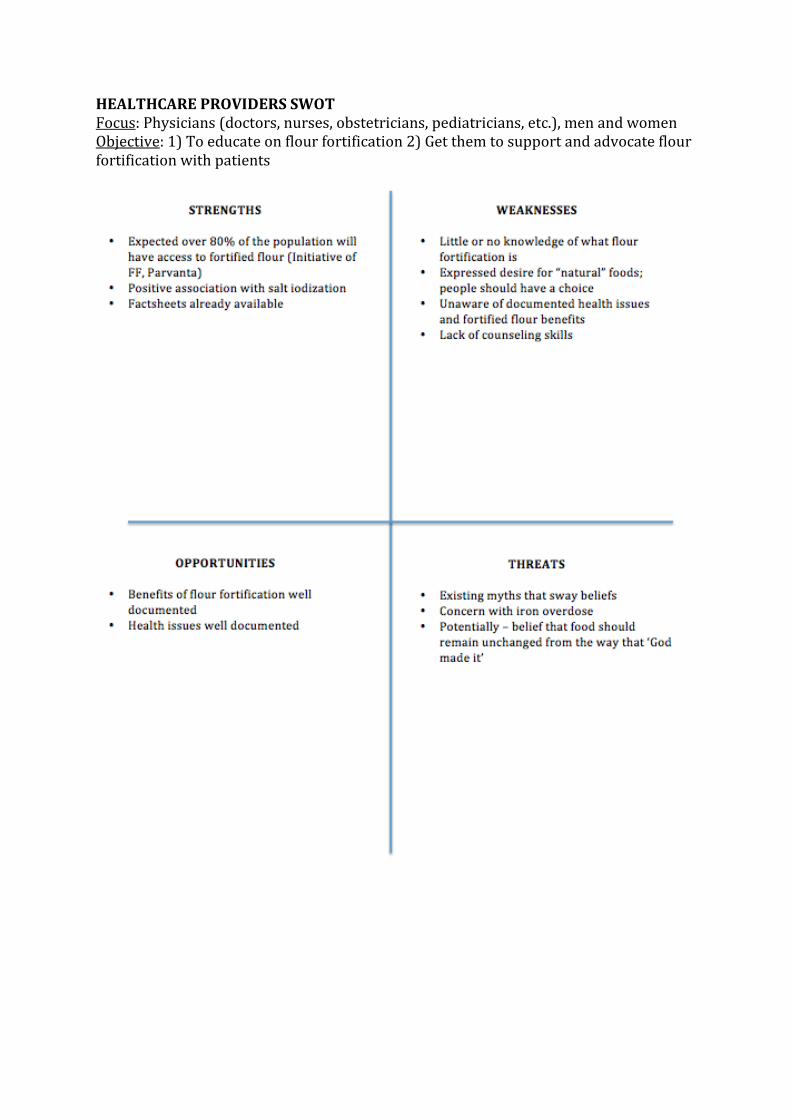
HEALTHCARE PROVIDERS SWOT Focus: Physicians (doctors, nurses, obstetricians, pediatricians, etc.), men and women Objective: 1) To educate on flour fortification 2) Get them to support and advocate flour fortification with patients
APPENDIX B: Logic Models
APPENDIX C: 4 P’s of Marketing
4 P’s OF MARKETING FOR FLOUR FORTIFICATION IN ARMENIA Product, Price, Place, Promotion
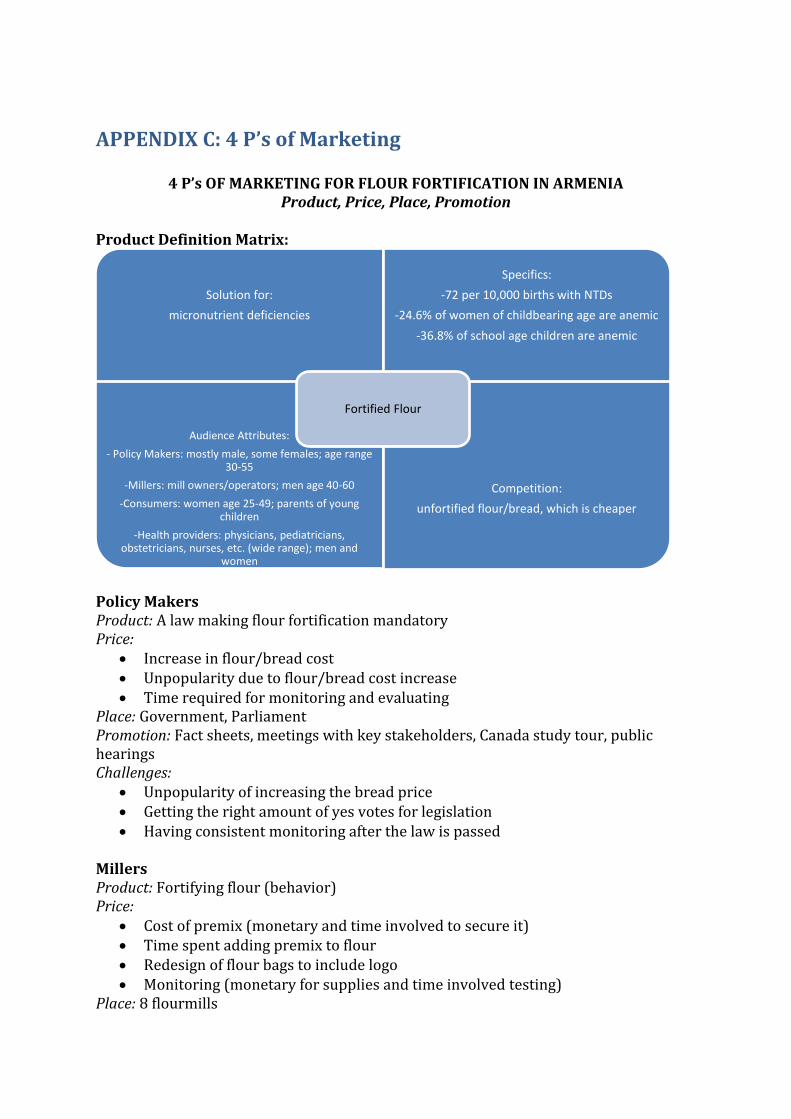
Product Definition Matrix:
Policy Makers Product: A law making flour fortification mandatory Price:
Increase in flour/bread cost Unpopularity due to flour/bread cost increase Time required for monitoring and evaluating
Place: Government, Parliament Promotion: Fact sheets, meetings with key stakeholders, Canada study tour, public hearings Challenges:
Unpopularity of increasing the bread price Getting the right amount of yes votes for legislation Having consistent monitoring after the law is passed
Millers Product: Fortifying flour (behavior) Price:
Cost of premix (monetary and time involved to secure it) Time spent adding premix to flour Redesign of flour bags to include logo Monitoring (monetary for supplies and time involved testing)
Place: 8 flourmills
Solution for:
micronutrient deficiencies
Specifics:
-72 per 10,000 births with NTDs
-24.6% of women of childbearing age are anemic
-36.8% of school age children are anemic
Audience Attributes:
- Policy Makers: mostly male, some females; age range 30-55
-Millers: mill owners/operators; men age 40-60
-Consumers: women age 25-49; parents of young children
-Health providers: physicians, pediatricians, obstetricians, nurses, etc. (wide range); men and
women
Competition:
unfortified flour/bread, which is cheaper
Fortified Flour
Promotion: Workshop to educate on how to fortify and monitor Challenges:
Getting the money for and securing premix Investment of time with fortifying and monitoring
Consumers Product: Accepting, buying, and consuming fortified bread/flour Price:
Higher bread/flour cost Feared change in lavash, an important piece of culture
Place: bakeries, shops Promotion: TV commercials & news coverage, billboards, community activities, posters, leaflets Challenges:
Justifying increase in price Dispelling myths about fortified flour Assuring that there will be no difference in flour/bread quality and that culture
will be maintained Creating a brand around the new logo
Health Providers Product: Supporting and promoting fortified flour Price:
Time and effort to remember to discuss fortified flour with patients Place: Health clinics Promotion: Factsheet, toolkit, posters for health clinic Challenges:
Having health providers retain the information Having health providers remember to counsel patients in regard to fortified flour
APPENDIX D: Logos FINAL DRAFTS OF LOGOS Below are the final three logos for the campaign that will be voted on by the government. A) Reads: Fortified Flour for a Healthy Family
B) Reads: Fortified Flour for a Healthy Family
C) Reads: Fortified Flour for Better Health
APPENDIX E: Key Communications Messages KEY MESSAGES FOR FLOUR FORTIFICATION COMMUNICATIONS IN ARMENIA Focusing on health problems:
Health problems from vitamin and mineral deficiencies, such as iron-deficiency anemia (IDA) and neural tube defects (NTDs), can be easily prevented.
o A deficiency of folic acid may also cause fatigue, and women with insufficient folic acid levels have a higher risk of children being born with NTDs.
o The use of fortified wheat flour can ease symptoms of iron deficiency anemia and lower the risk of having a baby born with birth defects.
o Weakness and fatigue are the most common signs of anemia, which is most frequently caused by not consuming enough iron. Other nutritional deficiencies, such as folic acid deficiency, can also cause anemia. .
o Even if you do not have iron deficiency anemia or are not a woman of childbearing age, it is still important to consume adequate amounts of vitamins and minerals. Foods made with fortified flour can help accomplish that.
Focusing on fortified flour (the product): Buy and consume fortified flour to prevent iron and folic acid deficiencies.
o Consuming fortified grains can prevent health problems associated with iron and folic acid deficiency. It is not a medicine or a cure for anemia or babies born with NTDs.
o Appropriately fortified grains are safe for everyone, including very young children, pregnant women, or ill persons.
o Fortified foods do not taste, look, or feel any different than unfortified foods. The quality of a product (for example, bread, pasta, etc.) made with fortified flour is the same as unfortified. Nutrients added to fortified flour have no color, odor, or taste.
o People do not need to eat more fortified flour than usual to experience the health benefits. The amount of vitamins and minerals added in each country is based on the normal eating patterns. To make sure flour is fortified, one should read the label on the package or look for the fortified logo.
Focusing on women:
Women who have IDA or do not get enough folic acid during pregnancy have an increased risk for an NTD-affected baby, miscarriages, perinatal death, and maternal death.
o Consuming fortified flour is good for the mother’s and the baby’s health. o IDA in pregnancy is a risk factor for preterm delivery and low birth
weight. o Children who are born prematurely are at increased risk for health
complications such as breathing problems, intellectual disabilities, and hearing loss.
o A mother’s IDA can put the child at risk for having anemia later in life.
Focusing on Children:
Children can be greatly affected by IDA, because their bodies are growing and developing.
o School children with IDA may have increased weakness and fatigue. o Iron deficiency can impair the development of children, affecting them
mentally, emotionally, and physically. o IDA can impair children’s school achievement.
Focusing on general population:
Men, women, and children who do not get enough of the vitamin and minerals they need can have serious health problems.
o IDA causes increased fatigue and thus lower productivity. o Folic acid may lessen the risk for heart attacks and cardiovascular disease. o Spina bifida, the most common NTD, has no cure. Children with spina
bifida have some degree of paralysis. They often need multiple surgeries and therapy, which adds to the family’s and the state’s healthcare costs. While there is no cure, spina bifida can be prevented by getting enough folic acid.
Focusing on national impacts:
The hidden effects of IDA, NTDs, and other vitamin and mineral deficiencies can impact the social and economic progress of nations.
o Adults with anemia can have diminished strength and fatigue, which decreases their ability to work and provide for their family.
o Babies with NTDs can increase healthcare costs for families and for the country.
o If a country has high anemia rates, then it can affect their production and economic status.
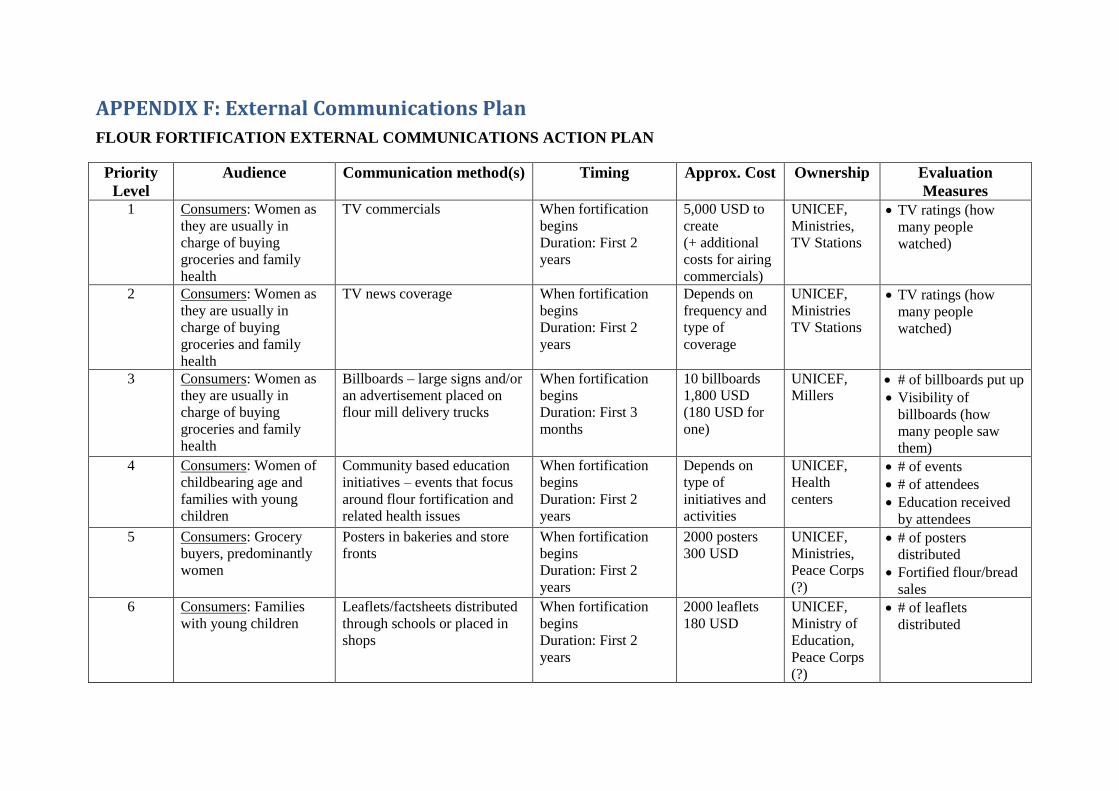
APPENDIX F: External Communications Plan
FLOUR FORTIFICATION EXTERNAL COMMUNICATIONS ACTION PLAN
Priority
Level
Audience Communication method(s) Timing Approx. Cost Ownership Evaluation
Measures 1 Consumers: Women as
they are usually in
charge of buying
groceries and family
health
TV commercials When fortification
begins
Duration: First 2
years
5,000 USD to
create
(+ additional
costs for airing
commercials)
UNICEF,
Ministries,
TV Stations
TV ratings (how
many people
watched)
2 Consumers: Women as
they are usually in
charge of buying
groceries and family
health
TV news coverage When fortification
begins
Duration: First 2
years
Depends on
frequency and
type of
coverage
UNICEF,
Ministries
TV Stations
TV ratings (how
many people
watched)
3 Consumers: Women as
they are usually in
charge of buying
groceries and family
health
Billboards – large signs and/or
an advertisement placed on
flour mill delivery trucks
When fortification
begins
Duration: First 3
months
10 billboards
1,800 USD
(180 USD for
one)
UNICEF,
Millers # of billboards put up
Visibility of
billboards (how
many people saw
them)
4 Consumers: Women of
childbearing age and
families with young
children
Community based education
initiatives – events that focus
around flour fortification and
related health issues
When fortification
begins
Duration: First 2
years
Depends on
type of
initiatives and
activities
UNICEF,
Health
centers
# of events
# of attendees
Education received
by attendees
5 Consumers: Grocery
buyers, predominantly
women
Posters in bakeries and store
fronts
When fortification
begins
Duration: First 2
years
2000 posters
300 USD
UNICEF,
Ministries,
Peace Corps
(?)
# of posters
distributed
Fortified flour/bread
sales
6 Consumers: Families
with young children
Leaflets/factsheets distributed
through schools or placed in
shops
When fortification
begins
Duration: First 2
years
2000 leaflets
180 USD
UNICEF,
Ministry of
Education,
Peace Corps
(?)
# of leaflets
distributed
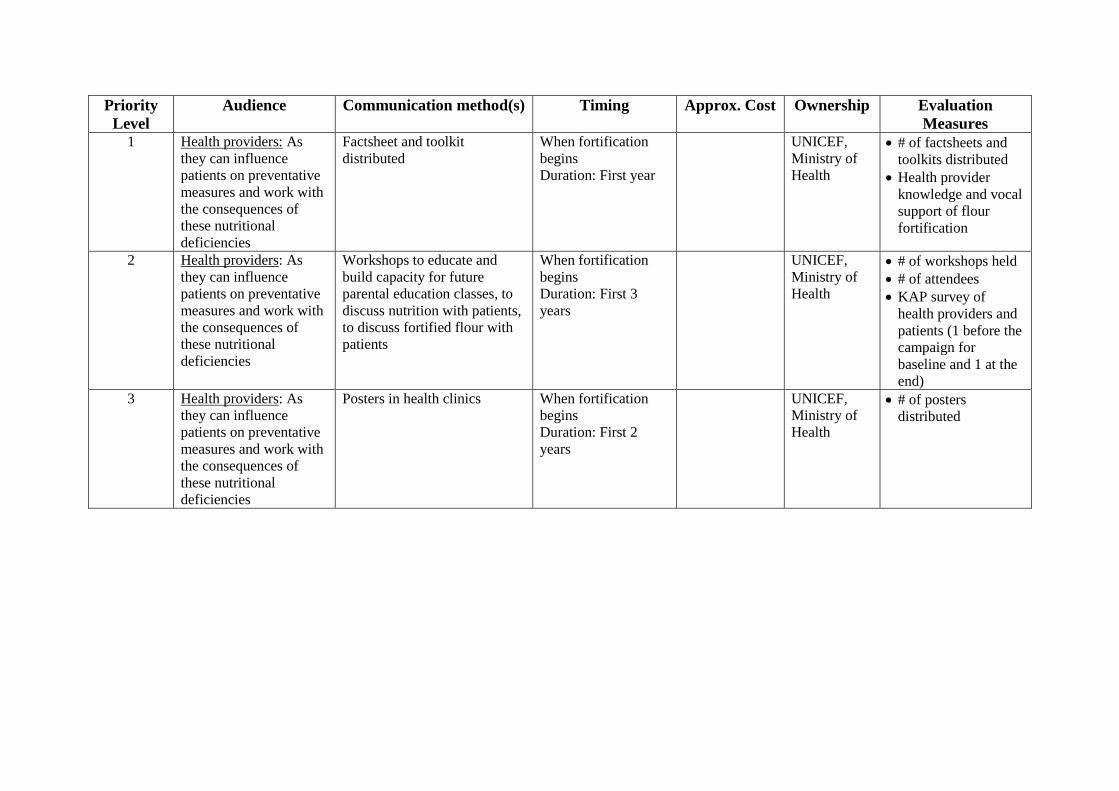
Priority
Level
Audience Communication method(s) Timing Approx. Cost Ownership Evaluation
Measures 1 Health providers: As
they can influence
patients on preventative
measures and work with
the consequences of
these nutritional
deficiencies
Factsheet and toolkit
distributed
When fortification
begins
Duration: First year
UNICEF,
Ministry of
Health
# of factsheets and
toolkits distributed
Health provider
knowledge and vocal
support of flour
fortification
2 Health providers: As
they can influence
patients on preventative
measures and work with
the consequences of
these nutritional
deficiencies
Workshops to educate and
build capacity for future
parental education classes, to
discuss nutrition with patients,
to discuss fortified flour with
patients
When fortification
begins
Duration: First 3
years
UNICEF,
Ministry of
Health
# of workshops held
# of attendees
KAP survey of
health providers and
patients (1 before the
campaign for
baseline and 1 at the
end)
3 Health providers: As
they can influence
patients on preventative
measures and work with
the consequences of
these nutritional
deficiencies
Posters in health clinics When fortification
begins
Duration: First 2
years
UNICEF,
Ministry of
Health
# of posters
distributed
APPENDIX G: TV Media Strategy
ARMENIA FLOUR FORTIFICATION TV MEDIA STRATEGY Objectives:
To inform the general public that flour fortification is a mandatory law in Armenia
To educate the general public on what flour fortification is and why it’s important
To encourage the general public to purchase and consume fortified flour and by-products
Key messages:
Health problems from vitamin and mineral deficiencies, such as iron-deficiency anemia (IDA) and neural tube defects (NTDs), are widespread in Armenia and can be easily prevented with fortified flour.
Fortified flour is essentially the same as regular flour except that it has added vitamins and minerals for better health.
Buy and consume fortified flour to prevent iron and folic acid deficiencies. Target audience:
Women as they are most likely to purchase flour and handle the family’s healthcare needs
Key stakeholders:
UNICEF Ministry of Health Ministry of Finance Ministry of Agriculture Association for Protection of Consumer Rights
Supporting Research & TV Targets: (Source: http://internews.am/sites/default/files/ArMediaSurveyReport.pdf , 2011) The following points highlight why the use of TV is important in this campaign and where campaign efforts should be targeted.
A huge majority of Armenians (90%) say that TV is their most important news source, followed by 6% who prefer the Internet, 2% radio, and 1% citing newspapers as the most important source.
The frequency of news consumption by source shows that national TV is the daily news source for a vast majority of Armenians.
Most popular channels: Viewership of H1 is high, with 80% of Armenian households watching it daily, however, Shant TV is the most frequently watched single channel, with 82% tuning in daily.
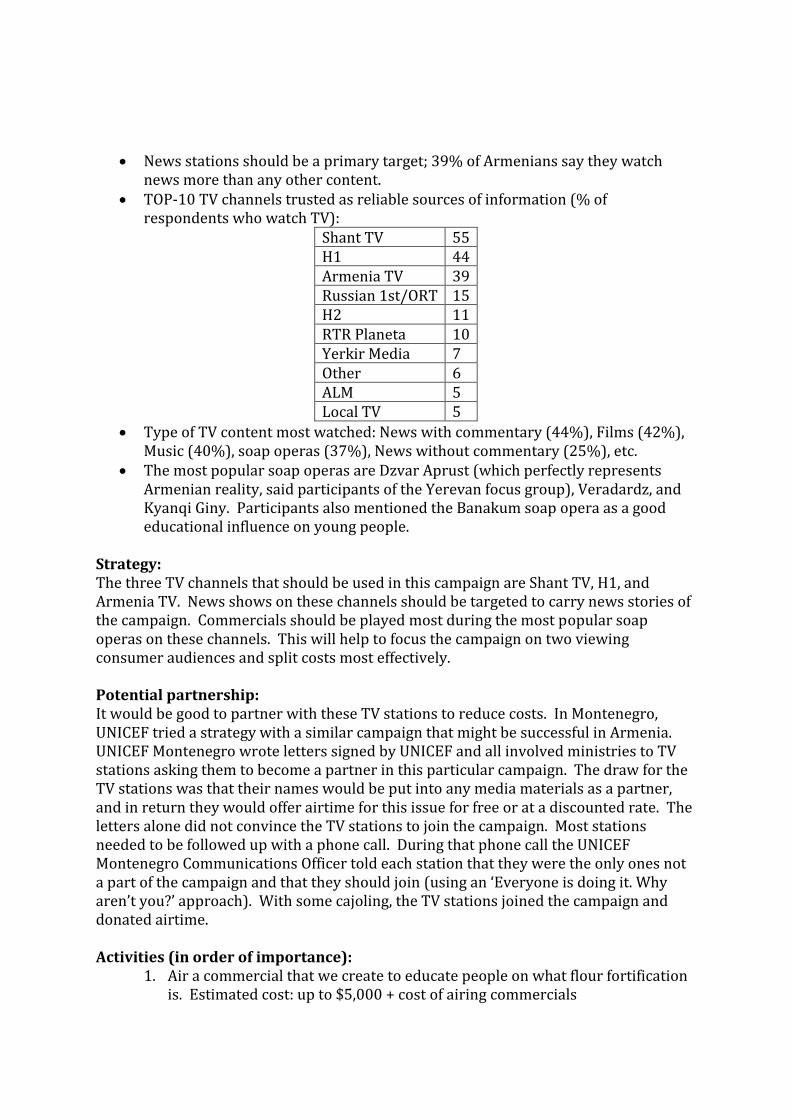
News stations should be a primary target; 39% of Armenians say they watch news more than any other content.
TOP-10 TV channels trusted as reliable sources of information (% of respondents who watch TV):
Shant TV 55 H1 44 Armenia TV 39 Russian 1st/ORT 15 H2 11 RTR Planeta 10 Yerkir Media 7 Other 6 ALM 5 Local TV 5
Type of TV content most watched: News with commentary (44%), Films (42%), Music (40%), soap operas (37%), News without commentary (25%), etc.
The most popular soap operas are Dzvar Aprust (which perfectly represents Armenian reality, said participants of the Yerevan focus group), Veradardz, and Kyanqi Giny. Participants also mentioned the Banakum soap opera as a good educational influence on young people.
Strategy: The three TV channels that should be used in this campaign are Shant TV, H1, and Armenia TV. News shows on these channels should be targeted to carry news stories of the campaign. Commercials should be played most during the most popular soap operas on these channels. This will help to focus the campaign on two viewing consumer audiences and split costs most effectively. Potential partnership: It would be good to partner with these TV stations to reduce costs. In Montenegro, UNICEF tried a strategy with a similar campaign that might be successful in Armenia. UNICEF Montenegro wrote letters signed by UNICEF and all involved ministries to TV stations asking them to become a partner in this particular campaign. The draw for the TV stations was that their names would be put into any media materials as a partner, and in return they would offer airtime for this issue for free or at a discounted rate. The letters alone did not convince the TV stations to join the campaign. Most stations needed to be followed up with a phone call. During that phone call the UNICEF Montenegro Communications Officer told each station that they were the only ones not a part of the campaign and that they should join (using an ‘Everyone is doing it. Why aren’t you?’ approach). With some cajoling, the TV stations joined the campaign and donated airtime. Activities (in order of importance):
1. Air a commercial that we create to educate people on what flour fortification is. Estimated cost: up to $5,000 + cost of airing commercials
2. Have the flour fortification campaign covered by the news. Have government representatives and the Association for Protection of Consumers Rights representatives speak about the campaign. Estimated cost: Depends on type of news segment
3. Use a trial run with bakers using fortified flour as a media opportunity to show that fortified flour has the same baking, taste, feel, and smell as unfortified flour. This could also be covered by the news or it could be done on a popular cooking show
4. Highlight millers’ commitment to fortifying flour and their social responsibility in a news story
5. Going on a talk show to discuss flour fortification
APPENDIX H: Health Provider’s Toolkit HEALTH PROVIDER’S TOOLKIT
1. What do iron and folic acid do for the body? Iron helps in the production of red blood cells and carries oxygen to the body cells, helps in synthesis of DNA and electron transport. Iron metabolism helps to protect the body against infections and promotes efficient functioning of the brain, aids in physical activity and productivity. It prevents some premature births. Folic Acid, also known as Vitamin B9, helps to produce and maintain new cells and therefore prevents neural tube defects. It also helps to make normal red blood cells and thus prevents one type of anemia.
2. Who are the most vulnerable to micronutrient deficiencies? Why? Children and women of reproductive age are most vulnerable, but generally everyone needs nutrients for good health. Children need to eat nutritious meals several times a day, because their bodies are growing. Women of reproductive age require extra nutrients during pregnancy and while breastfeeding. These nutrients are needed for the mother’s wellbeing, the development of the fetus during pregnancy, and for the baby during breastfeeding.
3. What are other sources of micronutrients? The best sources of iron are meat, fish, and poultry. Other sources include lentils, leafy greens, and nuts. It is important to note that peoples’ ability to absorb nutrients from some of these sources can be inhibited by other components in the food. Folic acid is present many foods. However, women would have to consume an unrealistic amount of these foods to get the dietary equivalent of 400 micrograms of folic acid a day, which is the amount recommended to reduce the risk of a pregnancy affected by a neural tube defect. To get the dietary equivalent of 400 micrograms of folic acid a day, a person would need to consume one of the following:
• 44½ medium ripe tomatoes • 17½ cups of orange juice • 19½ cups of raw green beans • 5½ cups of black beans • 200 medium red apples
4. How can you identify flour that is fortified?
Look for fortified flour logo on your bags of flour. (Picture of final logo)
5. When can you talk to patients about fortified flour? What can you say to them?
When a woman is of childbearing age or a couple is newly married When a woman or couple comes in for counselling on having children
Encourage the woman to bake with fortified flour or eat bread
(and other baked goods such as lavash, croissants, pizza crust, etc.) made with fortified flour to ensure that she gets enough folic acid. The time when folic acid is most critical is in the third and fourth week of pregnancy, which is often before women even know that they are pregnant.
When a woman is pregnant or parents have young children
Encourage the mother to feed her children foods made with
fortified flour, because iron and folic acid assists in their brains’ development and their wellbeing.
When anemia is present in an individual or there is a high prevalence in
the region
Encourage anemic patients to consume bread (and other baked goods such as lavash, croissants, pizza crust, etc.) made with fortified flour along with other foods rich in iron. Please note that if a patient is prescribed medication for anemia, then fortified flour should NOT replace medication.
6. What are the consequences of too little or no folic acid and iron?
Too little folic acid during the third and fourth weeks of pregnancy can result in neural tube defects (NTDs), of which spina bifida is the most common. Children born with spina bifida will undergo a lifetime of surgeries and face many health issues. Spina bifida cannot be cured. Iron deficiency leads to fatigue and decreased work and academic performance. With a high prevalence of anemia, production and the economy can suffer.
7. How can you respond to patients’ worries about safety or side effects of fortified flour?
It is highly unlikely that anyone will get an excess amount of vitamins and minerals from fortified foods. No side effects on health have been reported in the studies published on fortified flour. Studies and research in countries with long histories of fortification have established overwhelming evidence of the protective effect of fortification. In addition, the body regulates iron and folic acid levels by eliminating any excess of these nutrients in a person’s waste.
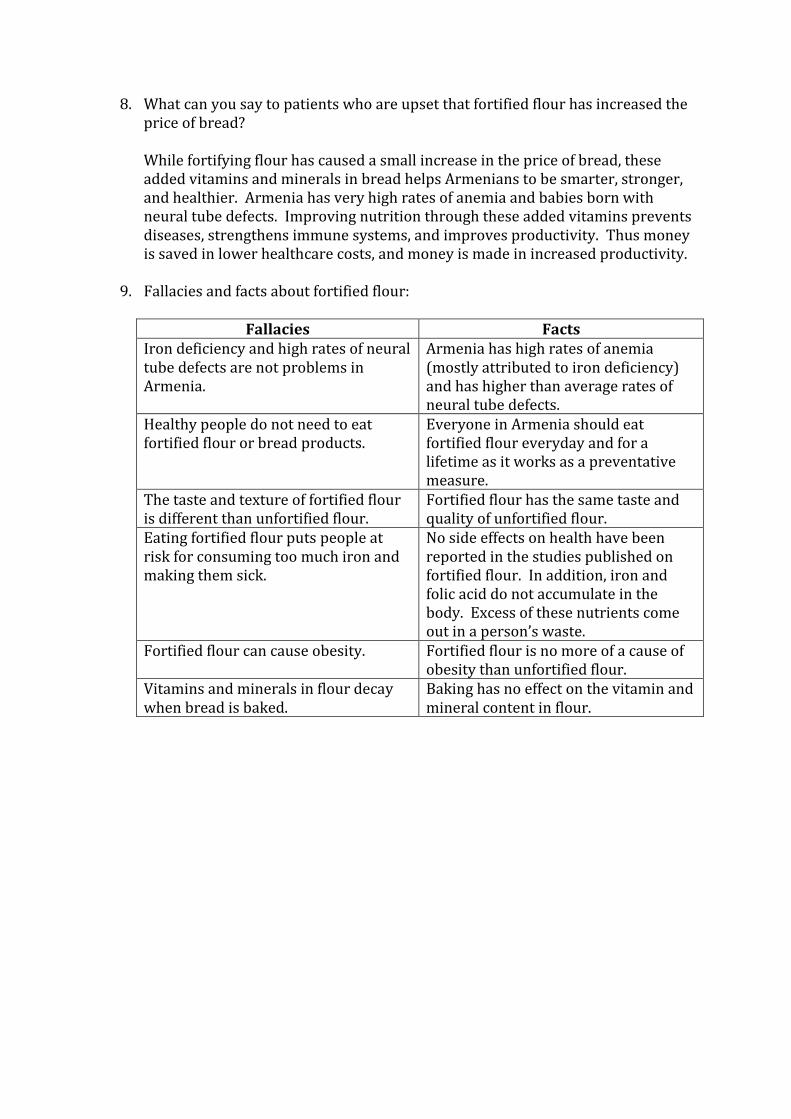
8. What can you say to patients who are upset that fortified flour has increased the price of bread? While fortifying flour has caused a small increase in the price of bread, these added vitamins and minerals in bread helps Armenians to be smarter, stronger, and healthier. Armenia has very high rates of anemia and babies born with neural tube defects. Improving nutrition through these added vitamins prevents diseases, strengthens immune systems, and improves productivity. Thus money is saved in lower healthcare costs, and money is made in increased productivity.
9. Fallacies and facts about fortified flour:
Fallacies Facts Iron deficiency and high rates of neural tube defects are not problems in Armenia.
Armenia has high rates of anemia (mostly attributed to iron deficiency) and has higher than average rates of neural tube defects.
Healthy people do not need to eat fortified flour or bread products.
Everyone in Armenia should eat fortified flour everyday and for a lifetime as it works as a preventative measure.
The taste and texture of fortified flour is different than unfortified flour.
Fortified flour has the same taste and quality of unfortified flour.
Eating fortified flour puts people at risk for consuming too much iron and making them sick.
No side effects on health have been reported in the studies published on fortified flour. In addition, iron and folic acid do not accumulate in the body. Excess of these nutrients come out in a person’s waste.
Fortified flour can cause obesity. Fortified flour is no more of a cause of obesity than unfortified flour.
Vitamins and minerals in flour decay when bread is baked.
Baking has no effect on the vitamin and mineral content in flour.

APPENDIX I: Grant Proposal GRANT PROPOSAL (Budget to be completed and grant to be submitted to a funding source by UNICEF staff) Background While Armenia makes all efforts to be on track to meet health-related MDGs, the size and magnitude of health issues facing children and young people remains considerable, and more efforts need to be concentrated by the Government and international partners to ensure further progress. There is a need for enhanced engagement, innovative equity approaches as well as the allocation of additional resources to address mother and child health needs in general with a particular focus on infant and young children nutrition and prevention of micronutrient deficiencies. Armenia has a high prevalence of the nutritional deficiencies: anemia and folic acid deficiencies that cause neural tube defects (NTDs). According to the 2005 Demographic and Health Survey (DHS), 24.6% of non-pregnant women of childbearing age in Armenia are anemic. The prevalence is even higher in pre-school children at 36.8%.1 While anemia can be caused by many factors, the anemia in Armenia is largely due to iron deficiency.2 The 2011 DHS estimated that one-fifth of perinatal mortality and one-tenth of maternal mortality are attributable to iron deficiency. A 2006 report by the March of Dimes estimated that NTDs have a prevalence rate of 72 per 10,000 births in Armenia.3 This number is high in comparison to other nations; countries that fortify flour with folic acid report less than 10 NTDs per 10,000 births.4 Regular consumption of bread, noodles, and other products made with fortified flour helps to fill the gap between dietary consumption and daily nutritional needs without requiring behavior change on the part of the consumer. For example, if women consume at least 400 micrograms of folic acid daily for at least one month before they become pregnant, 50-70% of NTDs can be prevented.5 Nevertheless many pregnancies are unplanned, and many women do not comply with the advice to take a daily supplement. Flour fortification can circumvent this challenge by helping to ensure that any woman who consumes bread or other flour-based products receives an additional supply of folic acid. Armenia has very high flour consumption at 311 grams per person per day,6 which means flour-based foods are a natural choice for the food vehicle to deliver extra micronutrients to the population.
1 ICF Macro 2011. MEASURE DHS STATcompiler. USAID. http://www.statcompiler.com. Accessed February 24, 2012.
2 Food and Agriculture Organization of the United Nations. Nutrition Country Profile Republic of Armenia. Food and
Agriculture Organization of the United Nations. http://www.bvsde.paho.org/texcom/nutricion/arm.pdf. Published 2005. Accessed February 7, 2013. 3 March of Dimes. Global Report on Birth Defects. March of Diems Birth Defects Foundation.
http://www.marchofdimes.com/downloads/BirthDefectsExecutiveSummary.pdf. Published 2006. Accessed February 7, 2013. 4 Zimmerman S. Fifteen Years of Fortifying with Folic Acid: Birth Defects are Reduced and Healthcare Expenses Averted.
Sight and Life. 25(3) 2011:54-59. 5 Center for Disease Control and Prevention. Recommendations for the use of folic acid to reduce the number of cases of
spina bifida and other neural tube defects. MMWR 1992; 41 (No. RR-14). 6 Flour Fortification Initiative. Country Profile: Armenia.
http://www.ffinetwork.org/country_profiles/country.php?record=1. Accessed February 7, 2013.
These public health issues also translate into economic losses for the country. Using available statistical data on anemia and NTDs into economic models developed by the World Bank and Asian Development Bank, an initial estimate of economic losses in Armenia is 49 million USD per year. In addition to the global economic crisis of 2008/2009 which caused a contraction in the Armenian economy of 14% GDP in 2009/2010, the global food price crisis has resulted in significant economic hardship in the country. The UN has identified Armenia as one of the countries of the former Soviet Union where public health indicators such as anemia will worsen over the next few years and will limit Armenia’s ability to reach its Millennium Development Goals. The high food prices are expected to result in increased food insecurity in the country. This means that the population will need to have access staple foods that have sufficient micronutrients available through fortification. Current Status To address the worsening situation in regard of micronutrient deficiency, in 2008 UNICEF initiated a national discussion on the need and feasibility of introduction of flour fortification with iron and folic acid in Armenia as one of the most effective public health interventions in addressing micronutrient deficiencies. As a result of UNICEF’s intensive advocacy, a Steering Committee under the authority of the Prime Minister with high representation from concerned ministries, National Assembly and international organizations has been established to coordinate all activities regarding the flour fortification initiative in the country. A Concept Note and a Plan of Action Budget on Implementation of Flour Fortification Program in Armenia was approved by the Government as a legal basis for implementation of FF activities. The needs of 8 major milling companies (which supply about 85% of the total flour needs in the country) have been assessed and UNICEF has procured the required number of feeders to be installed in the mills. In addition, the country has already drafted legislative framework for sanctioned production of fortified flour, which includes legislation and technical standards for production. The proposed law will be raised again to parliament in August 2013. UNICEF Armenia is hopeful that the law will be passed before the start of 2014 as support has been found in the President and Prime Minister. Now that these key pieces are in place, additional financial support is needed to ensure the sustainability and success of flour fortification in Armenia. Funding is needed for help with communications, monitoring, and evaluation costs. Goals & Objectives The overall goal is to support the Government of Armenia in ensuring better access to healthy food through the initiation of sustainable production of fortified flour. Within 4 years, our aim is to have 85% of wheat flour at production and wholesale/retail levels fortified by iron and folic acid. At least 50% of general population, including 500,000 women of childbearing age and children will be consuming iron and folic acid in fortified flour. As a result, nutrition status of women and children will be improved and health problems caused by micronutrients deficiencies will be prevented. Iron deficiency anemia among women of childbearing age and children and NTDs in newborns will be reduced by at least 20% in four years following nationwide implementation of the flour fortification program.

The project goals and objectives are as follows:
Goals & Objectives Indicators 1. Assist millers with preparation to begin
fortifying.
a. Secure the initial quantity of premix, which will be enough for the first year of production, within two months of legislation being passed.
Amount of premix secured Date premix is purchased
b. Train staff of the milling companies on how to fortify flour in accordance with standards established by the government within two months of legislation passing.
Number of mills represented at training
Date training is completed Conduct survey after the
training to assess miller education during training
2. Establish a quality control system. a. Ensure that the government
creates standards with which fortification levels must comply before fortification begins.
Quality standards are included in legislation
b. Establish the internal and external quality control system to monitor the compliance of the fortified flour with national standards on quality and safety in cooperation with the Ministry of Health and Ministry of Agriculture before fortification begins.
The government has a system and timeline to monitor fortification levels
Mills have a system and timeline to monitor fortification levels
3. Carry out a flour fortification communications campaign.
a. Improve the awareness of population on availability of fortified flours and its advantages in preventing of anemia and NTDs.
Consumers purchase fortified flour
Consumers accept and support fortified flour as assessed through KAP survey
b. Improve the knowledge and counseling capacities of health providers in regards to fortified flour and the prevention of micronutrient deficiencies.
The percentage of health providers who received the health provider toolkit (our goal: 70%)
Health providers support and promote fortified flour as assessed through KAP survey
Activities To ensure the production of fortified flour in the country, the funds to be received
within the framework of this proposal are essential to support the establishment of equipped production lines in mills and procurement of premixes compliant with national standards. There are a total of 8 flourmills that have sufficiently large enough rated daily capacity to be able to fortify flour at an industrial level. It is estimated that these mills supply about 85% of the total flour needs in the country, which makes about 272,000 metric tons. In order to start up the production of fortified flour, all milling companies need to be provided with initial quantity (for the 1st year of production) of premix. In addition, the staff of milling companies should be trained on how to fortify the flour to be in accordance with standards established in the country. The quality assurance system will be developed and introduced to monitor the quality of produced fortified flour and its compliance with national standards. The system will incorporate both internal (at production level) and external (at wholesale and retail levels, in public catering enterprises, etc.) monitoring, which will be conducted jointly by the Ministry of Health (State Hygiene and Anti-Epidemic Inspectorate) and Ministry of Agriculture (State Food Security Service) based on the monitoring standards. Capacities of both organizations will be improved through provision of laboratory equipment required for determining premix levels within the flour and training of relevant staff on monitoring methodologies. In addition, a standard system of self-control of quality of produced flour by milling companies will be developed and introduced in all 8 mills, and to ensure effectiveness of the self-control system milling companies will be provided with laboratory equipment and staff training. A multi-targeted public awareness campaign on advantages of fortified flour will be conducted through all communication channels and using different methodologies and techniques. To ensure the effectiveness of public awareness, UNICEF in collaboration with American University of Armenia has conducted an assessment of population knowledge, perceptions and attitude in relation to micronutrient deficiencies and fortified food. Results of the assessment as well as UNICEF’s strong experience in public communication on prevention of micronutrient deficiencies (gained during implementation of IDD/USI program) served a basis for development of audience-centered communication strategy on promotion of flour fortification. Capacities of health providers working at primary health care facilities, who are considered by population as one of the most reliable source of information on health related issues, will be improved on prevention of micronutrient deficiencies to enable them to provide population of their respective communities with adequate counselling and support. Please see attached log frames for more details on communications activities. Assumptions
That the flour fortification law passes. Without the law, none of the other plans can move forward. However, the situation looks favorable for the law to pass.
Changes in official posts of the Government due to political instability may also impede the smooth implementation of the project.
Lack of funds to procure initial supply of premixes and undertake complementary activities makes it impossible to start up the production of fortified flour as neither Government nor milling industry are currently in the position to provide funds for mentioned activities. In the result all preparation to initiate the program might be wasted.
Due to the current economic crisis and the food price crisis in the country the
increased cost due to flour fortification is a sensitive political issue in the country.
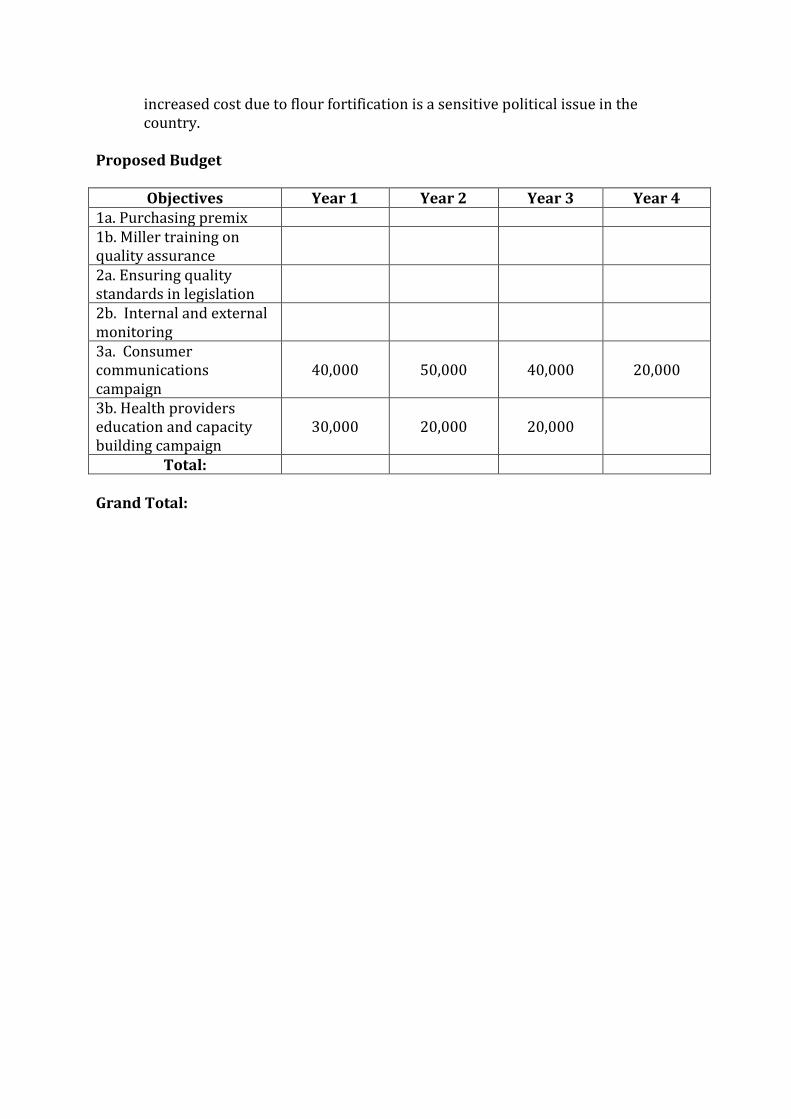
Proposed Budget
Objectives Year 1 Year 2 Year 3 Year 4 1a. Purchasing premix 1b. Miller training on quality assurance
2a. Ensuring quality standards in legislation
2b. Internal and external monitoring
3a. Consumer communications campaign
40,000 50,000 40,000 20,000
3b. Health providers education and capacity building campaign
30,000 20,000 20,000
Total: Grand Total:
APPENDIX J: Economics of Fortification OVERVIEW OF ECONOMIC COSTS OF FORTIFICATION IN ARMENIA The following document contains highlights of several documents that may be a helpful reference in the campaign. None of this is my own work. All relevant reports are available in the digital Appendix J folder. 1) Economic impact of flour fortification. A presentation by Sue Horton. October 2012. Costs of deficiency: iron Iron: in developing countries anemia is associated with
5% lower productivity (light manual labour) 17% lower productivity (heavy manual labour) 4% lower productivity (other work) – related to one-half standard deviation LOWER
score on cognitive tests (7-8 IQ points)
Costs of deficiency: folate • Human costs are paramount; • Economic costs also large: Yi et al (2011) review:
o Annual direct cost/patient/year €43,000 in 2003 for NTDs and €12-54,000 for spina bifida in US
o Spain annual medical costs/patient/year €3,500 spina bifida o Other costs for spina bifida are at least twice this (special education, lost productivity of
individual) o Parents also less able to work, lose additional income
2) Horton S and Ross J. The economics of iron deficiency. Food Policy. 2003, 28: 51-75. [Please note: The underlined figures are different from the original 2003 article. A second article was published in 2003, because the first article contained a calculation error. Both articles are in Appendix J.] Illustrative calculations for 10 developing countries suggest that the median value of annual
physical productivity losses due to iron deficiency is around $2.32 per capita, or 0.57% of
GDP. Median total losses (physical and cognitive combined) are $3.64 per capita, 0.81% of
GDP. Using a cost of $1.33 per case of anemia prevented, from one of the few effectiveness
studies of national fortification, allows us to calculate the benefit-cost ratio for long-term iron
fortification programs. The median value is 6:1 for the 10 countries examined and rises to
8.7:1 including the discounted future benefits attributable to cognitive improvements.
[The 10 developing countries are: Bangladesh, India, Pakistan, Mali, Tanzania, Egypt, Oman,
Bolivia, Honduras, and Nicaragua.]
3) Armenia Provisional BCR Scenario. Prepared by FFI affiliates. Unpublished.
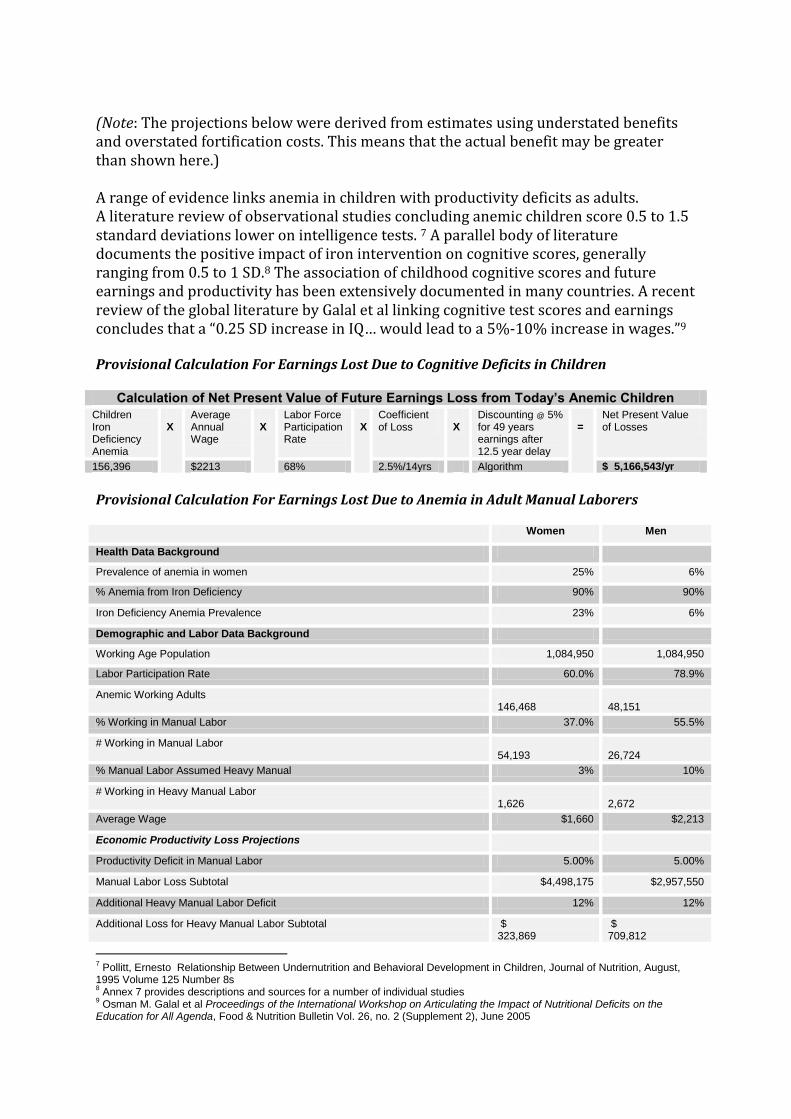
(Note: The projections below were derived from estimates using understated benefits and overstated fortification costs. This means that the actual benefit may be greater than shown here.) A range of evidence links anemia in children with productivity deficits as adults. A literature review of observational studies concluding anemic children score 0.5 to 1.5 standard deviations lower on intelligence tests. 7 A parallel body of literature documents the positive impact of iron intervention on cognitive scores, generally ranging from 0.5 to 1 SD.8 The association of childhood cognitive scores and future earnings and productivity has been extensively documented in many countries. A recent review of the global literature by Galal et al linking cognitive test scores and earnings concludes that a “0.25 SD increase in IQ… would lead to a 5%-10% increase in wages.”9 Provisional Calculation For Earnings Lost Due to Cognitive Deficits in Children
Calculation of Net Present Value of Future Earnings Loss from Today’s Anemic Children
Children Iron Deficiency Anemia
X
Average Annual Wage
X
Labor Force Participation Rate
X
Coefficient of Loss
X
Discounting @ 5% for 49 years earnings after 12.5 year delay
=
Net Present Value of Losses
156,396 $2213 68% 2.5%/14yrs Algorithm $ 5,166,543/yr
Provisional Calculation For Earnings Lost Due to Anemia in Adult Manual Laborers Women Men
Health Data Background
Prevalence of anemia in women 25% 6%
% Anemia from Iron Deficiency 90% 90%
Iron Deficiency Anemia Prevalence 23% 6%
Demographic and Labor Data Background
Working Age Population 1,084,950 1,084,950
Labor Participation Rate 60.0% 78.9%
Anemic Working Adults 146,468
48,151
% Working in Manual Labor 37.0% 55.5%
# Working in Manual Labor 54,193
26,724
% Manual Labor Assumed Heavy Manual 3% 10%
# Working in Heavy Manual Labor 1,626
2,672
Average Wage $1,660 $2,213
Economic Productivity Loss Projections
Productivity Deficit in Manual Labor 5.00% 5.00%
Manual Labor Loss Subtotal $4,498,175 $2,957,550
Additional Heavy Manual Labor Deficit 12% 12%
Additional Loss for Heavy Manual Labor Subtotal $ 323,869
$ 709,812
7 Pollitt, Ernesto Relationship Between Undernutrition and Behavioral Development in Children, Journal of Nutrition, August,
1995 Volume 125 Number 8s 8 Annex 7 provides descriptions and sources for a number of individual studies
9 Osman M. Galal et al Proceedings of the International Workshop on Articulating the Impact of Nutritional Deficits on the
Education for All Agenda, Food & Nutrition Bulletin Vol. 26, no. 2 (Supplement 2), June 2005
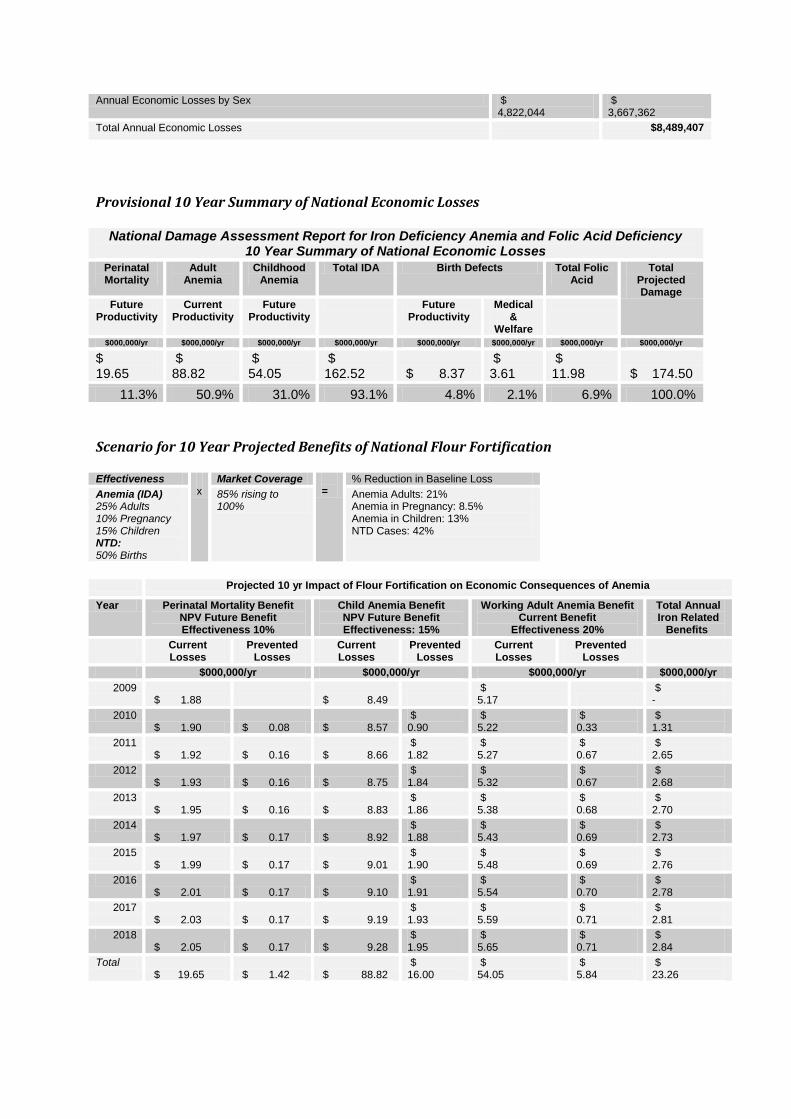
Annual Economic Losses by Sex $ 4,822,044
$ 3,667,362
Total Annual Economic Losses $8,489,407
Provisional 10 Year Summary of National Economic Losses
National Damage Assessment Report for Iron Deficiency Anemia and Folic Acid Deficiency 10 Year Summary of National Economic Losses
Perinatal Mortality
Adult Anemia
Childhood Anemia
Total IDA Birth Defects Total Folic Acid
Total Projected Damage
Future Productivity
Current Productivity
Future Productivity
Future Productivity
Medical &
Welfare
$000,000/yr $000,000/yr $000,000/yr $000,000/yr $000,000/yr $000,000/yr $000,000/yr $000,000/yr
$ 19.65
$ 88.82
$ 54.05
$ 162.52 $ 8.37
$ 3.61
$ 11.98 $ 174.50
11.3% 50.9% 31.0% 93.1% 4.8% 2.1% 6.9% 100.0%
Scenario for 10 Year Projected Benefits of National Flour Fortification Effectiveness
x Market Coverage
= % Reduction in Baseline Loss
Anemia (IDA) 25% Adults 10% Pregnancy 15% Children NTD: 50% Births
85% rising to 100%
Anemia Adults: 21% Anemia in Pregnancy: 8.5% Anemia in Children: 13% NTD Cases: 42%
Projected 10 yr Impact of Flour Fortification on Economic Consequences of Anemia
Year Perinatal Mortality Benefit NPV Future Benefit Effectiveness 10%
Child Anemia Benefit NPV Future Benefit Effectiveness: 15%
Working Adult Anemia Benefit Current Benefit
Effectiveness 20%
Total Annual Iron Related
Benefits
Current Losses
Prevented Losses
Current Losses
Prevented Losses
Current Losses
Prevented Losses
$000,000/yr $000,000/yr $000,000/yr $000,000/yr
2009 $ 1.88 $ 8.49
$ 5.17
$ -
2010 $ 1.90 $ 0.08 $ 8.57
$ 0.90
$ 5.22
$ 0.33
$ 1.31
2011 $ 1.92 $ 0.16 $ 8.66
$ 1.82
$ 5.27
$ 0.67
$ 2.65
2012 $ 1.93 $ 0.16 $ 8.75
$ 1.84
$ 5.32
$ 0.67
$ 2.68
2013 $ 1.95 $ 0.16 $ 8.83
$ 1.86
$ 5.38
$ 0.68
$ 2.70
2014 $ 1.97 $ 0.17 $ 8.92
$ 1.88
$ 5.43
$ 0.69
$ 2.73
2015 $ 1.99 $ 0.17 $ 9.01
$ 1.90
$ 5.48
$ 0.69
$ 2.76
2016 $ 2.01 $ 0.17 $ 9.10
$ 1.91
$ 5.54
$ 0.70
$ 2.78
2017 $ 2.03 $ 0.17 $ 9.19
$ 1.93
$ 5.59
$ 0.71
$ 2.81
2018 $ 2.05 $ 0.17 $ 9.28
$ 1.95
$ 5.65
$ 0.71
$ 2.84
Total $ 19.65 $ 1.42 $ 88.82
$ 16.00
$ 54.05
$ 5.84
$ 23.26

Projected 10 yr Impact of Flour Fortification on Economic Consequences of Folic Acid
NPV of Lost Productivity from Mortalities and Disabilities
Current Medical & Welfare Losses
Total Annual Folic Acid
Related Benefits Current Losses Prevented Losses
Current Losses Prevented Losses
$000,000/yr $000,000/yr $000,000/yr $000,000/yr $000,000/yr
2009 $ 0.8 $ 0.3 $0.0
2010 $ 0.8 $ 0.2 $ 0.3 $ 0.1 $0.2
2011 $ 0.8 $ 0.3 $ 0.4 $ 0.1 $0.5
2012 $ 0.8 $ 0.3 $ 0.4 $ 0.1 $0.5
2013 $ 0.8 $ 0.4 $ 0.4 $ 0.2 $0.5
2014 $ 0.8 $ 0.4 $ 0.4 $ 0.2 $0.5
2015 $ 0.8 $ 0.4 $ 0.4 $ 0.2 $0.5
2016 $ 0.9 $ 0.4 $ 0.4 $ 0.2 $0.5
2017 $ 0.9 $ 0.4 $ 0.4 $ 0.2 $0.5
2018 $ 0.9 $ 0.4 $ 0.4 $ 0.2 $0.5
$ 8.4 $ 3.0 $ 3.6 $ 1.3 $4.3
Provisional Benefit Cost Analysis Based on the 10-year projected benefits as well as the 10 year financial analysis a Benefit Cost presentation is shown below. Benefits of $27.6 million and fortification cost of $6.17 million yield net benefits of $21.4 million and indicate a 10 year benefit cost ratio of 4.5 For each $1 invested in flour fortification, $4.5 will be returned as a mix of lower medical and welfare expenditures, improved current productivity of manual laborers and greater future today’s productivity of children.
Benefit Cost Analysis
Benefits Costs Benefit- Cost Annual Net Benefits
Cumulative Net Benefits
$000,000 $000,000 Ratio $000,000 Net Benefits $000,000
2009 $0.000 $0.54 - -$0.540 -$1
2010 $1.555 $0.69 2.3 $0.864 $0
2011 $3.140 $0.60 5.3 $2.543 $3
2012 $3.172 $0.60 5.3 $2.569 $5
2013 $3.203 $0.61 5.3 $2.595 $8
2014 $3.235 $0.61 5.3 $2.621 $11
2015 $3.268 $0.62 5.3 $2.648 $13
2016 $3.300 $0.63 5.3 $2.675 $16
2017 $3.333 $0.63 5.3 $2.702 $19
2018 $3.367 $0.64 5.3 $2.729 $21
27.6 $6.17 4.5 $21.4