understanding a patient’s surgical journey - amta · 58 mtj/massage therapy journal spring 2014...
TRANSCRIPT

58
mtj
/mas
sage
ther
apy
jour
nal
spri
ng
201
4
Understanding a Patient’s Surgical JourneyWhat joint replacement surgery entails and the role massage therapy plays pre- and post-surgery
BY ANNIE MORIEN

ww
w.am
tamassage.org/m
tj 59
Joint Replacements

60
mtj
/mas
sage
ther
apy
jour
nal
spri
ng
201
4
Massage therapists serve an im-portant role in helping patient’s transition from pre-surgery pain to post-surgery rehabilitation. The goal of this article is to understand the most common causes of joint pain, non-surgical and surgical treatment options, and the effects of massage therapy before and af-ter joint surgery. In addition, this article describes current research regarding the various surgical ap-proaches, as well as joint replace-ment components (including metal-on-metal implants). By understand-ing patients’ pre-surgical journey of pain and disability, you can help them walk the post-surgical road to recovery.
Joint ReplacementOur focus will be on the two pri-mary joints involved in ambulatory movement: the hip and knee. The hip joint supports the body, and is important in balance and posture. The knee is the largest joint in the body and supports a signifi cant pro-
portion of body weight. Healthy hip and knee joints allow for smooth, unrestricted movement. Injury to the hip or knee, or change to these joints brought on by disease, often produces pain and disability. Over time, pain and dysfunction can become severe and signifi cantly limiting. When quality of life is compromised and all non-surgical treatments fail to alleviate the pain, an individual may decide to undergo a joint replacement, or arthroplasty, which is Latin for “joint repair.” Joint replacement entails replac-ing diseased parts of a joint with prosthetic implants. Surgeons per-formed more than 427,900 hip and 675,300 knee replacement opera-tions in the United States (Steiner, Andrews, Barrett & Weiss, 2012). By 2030, researchers predict the de-mand for hip and knee replacement surgery will increase by 175 per-cent and 674 percent, respectively (Kurtz, Ong, Lau, Mowat & Halpern, 2007).
Several factors account for the increasing demand for replacement surgery, including an aging “baby boom” population, increasing obe-sity and the demand for a better quality of life. Indeed, the increased demand for hip and knee replace-ment surgeries affects health care costs. Health economists estimate that the average hospital cost for the fi rst (primary) hip or knee re-placement falls between $18,000 and $19,000 (Steiner et al., 2012). A recent study suggested that total hospital charges could reach $80.2 billion by 2015 (Kim, 2008).
Osteoarthritis. Arthritis is the pri-mary cause of joint pain and dis-ability. Although more than 100 dif-ferent types of arthritis exist, osteo-arthritis (OA) is the most common type of arthritis worldwide, and the leading chronic illness in the Unit-ed States. An estimated 27 million Americans over age 25 have symp-toms of osteoarthritis (Lawrence, Felson, Helmick, Arnold, Choi, Deyo, Gabriel, Hirsch, Hochberg, Hunder, Jordan, Katz, Kremers & Wolfe, 2008). Pain from osteoar-thritis is the primary reason people undergo joint replacement surgery. According to the Arthritis Foun-dation, osteoarthritis most com-monly affects hip and knee joints (arthritis.org). One in four people will likely develop hip arthritis in their lifetime (Murphy, Helmick, Schwartz, Renner, Tudor, Koch, Dragomir & Kalsbeek, 2010) and one in two people will likely develop knee arthritis by age 85 (Murphy, Schwartz, Helmick, Renner, Tudor, Koch, Dragomir, Kalsbeek , Luta & Jordan, 2008). Although osteoarthritis is known as a degenerative joint disease (DJD), the condition is more com-plex than simply “wearing out” the joint. Osteoarthritic joints undergo
CONT
INUI
NG
EDUC
ATIO
N
M any patients struggle with joint pain and disability. Daily activities, such as rising from a chair, bending and walking are diffi cult. Although massage therapy decreases pain and improves quality of life in many people, some experience no relief from complementary therapies or from western medicine. Joint replacement surgery becomes the fi nal choice when all other options fail.

ww
w.am
tamassage.org/m
tj 61
chronic, progressive cycles of in-fl ammation and degeneration that affects the joint’s articular carti-lage, bone, synovium and ligaments. Over time, the cyclic low-grade in-fl ammation alters these structures, resulting in pain and dysfunction.
Risk FactorsResearch identifi es several factors for the development of osteoarthri-tis, including age, gender, joint trau-ma, obesity, genetics and muscle weakness. First, as people age, their risk of developing osteoarthritis in-creases until age 80 (at which point their risk levels off) (Buckwalter, Saltzman & Brown, 2004). Second, females face greater risk of develop-ing osteoarthritis, especially after age 50. Third, joint trauma that re-sults from prolonged, intense, high-level activity may increase the risk of developing osteoarthritis. Also, occupational activities, such as high impact loads, heavy lifting and jumping, to name a few, may lead to the development of osteoarthritis. Obesity, too, is an infl uential (yet modifi able) osteoarthritis risk fac-tor. Research suggests that two out of every three people who are obese will develop knee osteoarthritis (Lawrence, et al., 2008). A loss of approximately 11 pounds, however, decreases the risk of developing knee osteoarthritis by 50 percent (Felson, Zhang, Anthony, Naimark & Anderson, 1992). In addition to the extra weight exerted on joints, obesity is linked to the production of metabolic mediators involved in osteoarthritis. Research suggests that adipose tissue is a source of pro-infl ammatory and catabolic chemicals that promote synovial infl ammation, cartilage degrada-tion and bone remodeling (Sowers & Karvonen-Gutierrez, 2010). Evidence of a genetic infl uence stems from various sources, such as
epidemiological studies of families and twins, as well as molecular gene testing (Valdes & Spector, 2011). Family and twin studies suggest that certain osteoarthritic traits are inherited. For example, individual twins may develop osteoarthritis in the same joint, or have the same joint changes evident on x-ray. Also, specifi c genes may be associated with greater risk. Indeed, research-ers report combinations of certain high risk genes are associated with osteoarthritis incidence/prevalence. Finally, evidence links weak knee muscles with pain and dysfunction in people with osteoarthritis. In contrast, when quadriceps muscles are strengthened, osteoarthritis-associated symptoms improved (i.e., reduced pain and improved physical functioning) (Alnahdi, Zeni & Sny-der-Mackler, 2012). Likewise, mus-cles strengthened by practicing yoga improved symptoms of knee osteo-arthrtitis. Nambi and Shah (2013) demonstrated that Iyengar yoga, in combination with other techniques, reduced pain and improved func-tional ability. Certain yoga poses and movements also strengthen quadriceps, and increase both fl ex-ibility and blood fl ow.
Signs and Symptoms Osteoarthritis is typically a slow, chronic destruction of joints marked by varying levels of pain and stiffness. Initially, people with osteoarthritis experience brief (less than one hour) joint stiffness in the morning (after waking) or after pro-longed sitting. Over time, the pain and stiffness persist through the day, and eventually disrupts sleep at night and causes chronic dysfunc-tion. With hip osteoarthritis, pain oc-curs deep in the acetabulum (sock-et), and may extend to the groin or knee. With knee osteoarthritis,
Risk Factors For Developing Osteoarthritis
AGE. The number of people diag-nosed with OA increases with age.
GENDER. Women are diagnosed with OA more often than men, espe-cially after age 50.
JOINT TRAUMA. Repetitive or in-tense physical activity appears linked to OA.
OBESITY. Extra weight places sig-nifi cant stress on joints, increasing the risk of developing OA. Research also links obesity to elevated infl ammatory chemicals that may promote changes in cartilage, bone and synovium.
GENETICS. Family and twin stud-ies suggest that certain osteoarthritic traits are inherited, and specifi c genes are associated with greater risk.
WEAK MUSCLES. Weak knee mus-cles are associated with OA-related pain and dysfunction.

62
mtj
/mas
sage
ther
apy
jour
nal
spri
ng
201
4
crepitus (a crackling or grinding noise) may be heard with move-ment, and joints may swell and be-come infl amed. Affected joints undergo cycles of infl ammation, ineffective repair and degeneration that results in detrimental changes in cartilage and bone. Chronic loss of carti-lage and hypertrophic changes in bone leads to bone-on-bone ero-sion. Bony deformities called osteo-phytes form on articulating bones. These changes are evident, along with joint space narrowing, when viewed on an x-ray. Degeneration of cartilage and appearance of osteo-phytes causes pain, loss of range-of-motion and altered gait. In addition to cartilage and bone changes, muscles become tight in an attempt to protect the affected joint. In the hip, shortened muscles (erector spinae, iliopsoas and rectus femoris) produce an anterior pelvic tilt, resulting in abnormal joint load-ing and gait changes. In the knee, tight hamstrings produce chronic knee fl exion, and weak quadriceps alter knee stability. In general, osteoarthritis produces a cycle of dysfunction. Because os-teoarthritis causes joint pain, the pa-tient avoids movement of the affect-ed joint. The reduction in movement produces muscle tightness, which leads to muscle weakness, restricted range-of-motion and more pain.
Diagnosis and TreatmentMedical providers make a diagnosis of osteoarthritis after careful exam-ination and the evaluation of tests. A thorough medical history and physical exam reveal much about the patient’s condition, and x-rays provide visual evidence of joint de-terioration. Unless the diagnosis is in question, MRIs (magnetic reso-nance imaging) or blood tests are unnecessary.
Non-surgical treatment. Treatment for osteoarthritis should start with safe, non-invasive therapies before advancing to surgical treatment. Non-surgical treatment includes conservative measures such as strengthening exercises, activity modifi cation, weight loss, manual therapy, and the use of a cane or walker. Pharmacological treatment includes NSAIDS (non-steroidal anti-infl ammatory drugs) such as over-the-counter Ibuprofen and prescription COX2-inhibitors such as Celebrex. Surgeons usually pre-scribe Tramadol for pain rather than opioid-based prescription drugs. Several studies report positive re-sults using massage therapy to treat patients with hip and knee osteoar-thritis. For example, one case study reported massage helped a young adult with hip osteoarthritis (Cook & Heiderscheit, 2009). Therapists applied massage for three months to the patient’s iliopsoas muscle. The treatment reduced the pa-tient’s pain and increased range-of-motion, strength, and function at a three-month follow-up. A second study found that 20-minute massage applied twice weekly for 12 weeks improved knee symptoms (pain, stiffness, func-tion) in patients with osteoarthritis (Atkins & Eichler, 2013), and a third study reported that Swedish mas-sage applied to knee muscles one to two times per week (for eight weeks) resulted in signifi cant reduction in pain and stiffness, as well as in-creased physical functioning and ROM (Perlman, Sabina, Williams, Njike & Katz 2006). However, for those people who do not respond to non-surgical treat-ments, have joint damage evidence via x-ray, and experience signifi -cant pain and disability that affects quality of life, surgery may become necessary. Ultimately, though, the
CONT
INUI
NG
EDUC
ATIO
N
“Although osteoarthritis is known as a degenerative joint disease, the condition is more complex than simply ‘wearing out’ the joint.
ww
w.am
tamassage.org/m
tj 63
patient—not the surgeon—makes the decision on whether to have sur-gery.
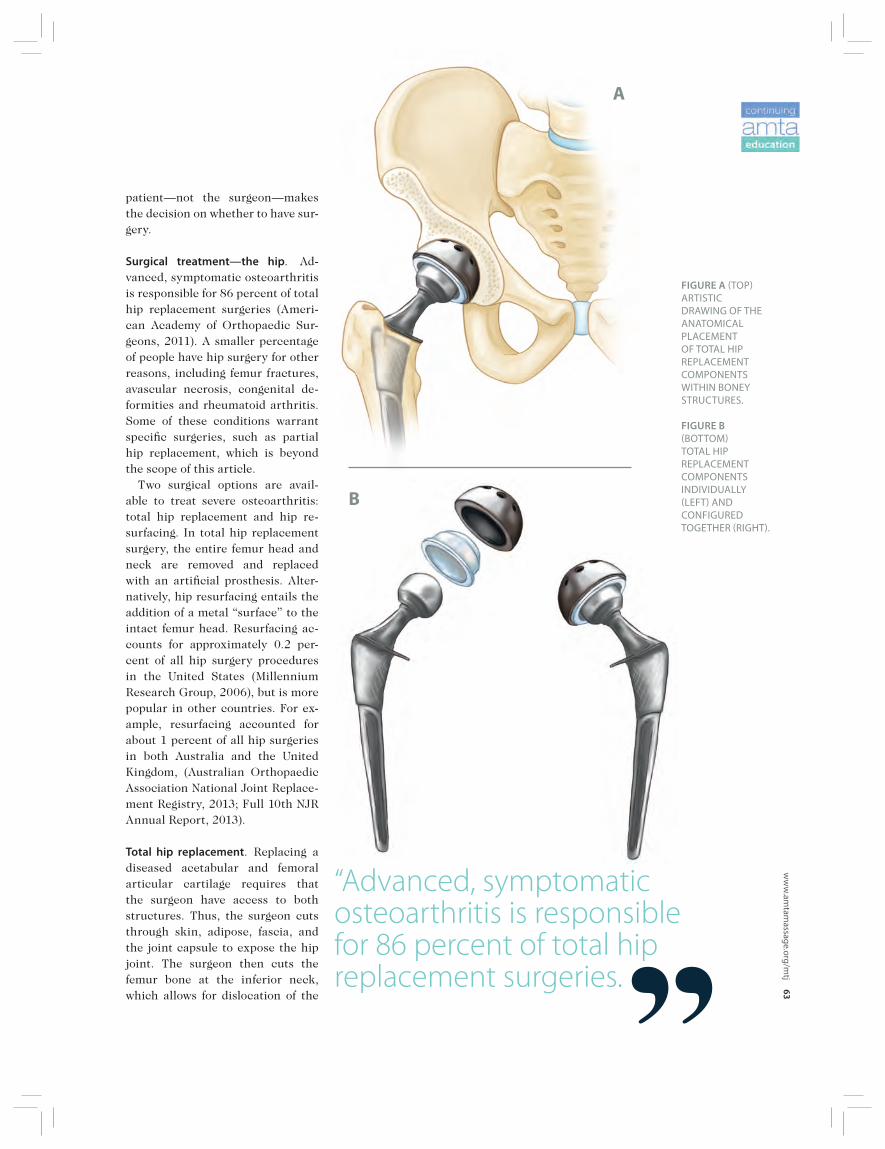
Surgical treatment—the hip. Ad-vanced, symptomatic osteoarthritis is responsible for 86 percent of total hip replacement surgeries (Ameri-can Academy of Orthopaedic Sur-geons, 2011). A smaller percentage of people have hip surgery for other reasons, including femur fractures, avascular necrosis, congenital de-formities and rheumatoid arthritis. Some of these conditions warrant specifi c surgeries, such as partial hip replacement, which is beyond the scope of this article. Two surgical options are avail-able to treat severe osteoarthritis: total hip replacement and hip re-surfacing. In total hip replacement surgery, the entire femur head and neck are removed and replaced with an artifi cial prosthesis. Alter-natively, hip resurfacing entails the addition of a metal “surface” to the intact femur head. Resurfacing ac-counts for approximately 0.2 per-cent of all hip surgery procedures in the United States (Millennium Research Group, 2006), but is more popular in other countries. For ex-ample, resurfacing accounted for about 1 percent of all hip surgeries in both Australia and the United Kingdom, (Australian Orthopaedic Association National Joint Replace-ment Registry, 2013; Full 10th NJR Annual Report, 2013).
Total hip replacement. Replacing a diseased acetabular and femoral articular cartilage requires that the surgeon have access to both structures. Thus, the surgeon cuts through skin, adipose, fascia, and the joint capsule to expose the hip joint. The surgeon then cuts the femur bone at the inferior neck, which allows for dislocation of the
“Advanced, symptomatic osteoarthritis is responsible for 86 percent of total hip replacement surgeries.
FIGURE A TOP ARTISTIC DRAWING OF THE ANATOMICAL PLACEMENT OF TOTAL HIP REPLACEMENT COMPONENTS WITHIN BONEY STRUCTURES.
FIGURE B BOTTOM TOTAL HIP REPLACEMENT COMPONENTS INDIVIDUALLY LEFT AND CONFIGURED TOGETHER RIGHT.
A
B

64
mtj
/mas
sage
ther
apy
jour
nal
spri
ng
201
4
joint (the femur head and neck are discarded). The surgeon inserts a metal spike into the femur, and at-taches an artifi cial ball to the spike. Sometimes the surgeon applies spe-cial cement to secure the spike in the bone. The surgeon then reshapes the acetabulum with special tools that ream the socket, and then inserts a metal cup that is either cemented in place or fi xed with screws (the lat-ter process is called cementless). In some replacement systems, the sur-geon inserts a liner into the artifi -cial acetabulum. The spike and acetabular cup are typically made of a metal alloy (tita-nium, cobalt-chrome, etc.), and the artifi cial ball is composed of ceram-ic or metal alloy. The liner is made of polyethylene (plastic), ceramic or metal.
Candidates for total hip replace-ment. The best candidates for total hip replacement are people who are healthy, within normal weight and have solid bones. Healthy patients have strong immune systems that combat infections and stress. Be-cause normal weight patients place less stress on joints (additional weight on the new joint increases the risk that the artifi cial joint may fail), surgeons often encour-age patients with body mass index (BMI; body mass divided by height squared) greater than 35 to lose weight before surgery. Additionally, good candidates
should have solid bones, or an abun-dance of hip and femur bone (called bone stock). The surgeon needs plenty of solid bone in order to im-plant the artifi cial components. And fi nally, total hip replacement candi-dates can be any age, but risk of the new implant failing increases by 40 percent with each decade after 65 years of age.
Hip resurfacing. Similar to total hip replacement, the surgeon cuts through all joint-related tissues, dislocates the joint, and reshapes (reams) the acetabulum. In con-trast to total hip replacement, the surgeon does not remove the femur head and neck. Rather, the surgeon reshapes the femur head, which is then covered with a metal cap (sur-face overlay) and secured (cement-ed). The metal cap and acetabular cup are made of a metal alloy (typically cobalt-chrome). [Note: Future de-signs are likely to replace the metal cap with ceramic or similarly hard material.]
Candidates for hip resurfacing. The best candidates for hip resurfacing are people who are healthy, within normal weight and have solid bones. Additional evidence suggests that males fare better than female pa-tients, and prosthesis failure rates are higher in women than in men, making women poor candidates for resurfacing. When comparing men and wom-
en, a recent study reported that “resurfacing failure rates in women were unacceptably high,” and rec-ommend that “resurfacing proce-dures are not undertaken in wom-en” (Smith, Dieppe, Howard, Blom; on behalf of the National Joint Reg-istry for England and Wales. 2012). The reason women have higher failure rates is unclear, but some re-search suggests that a small femoral head (typically implanted in wom-en) may be problematic and bone loss (commonly seen after meno-pause) can contribute to increased risk of femoral neck fracture. Or, a combination of both of these factors may be at play. In 2012, an FDA advisory panel suggested that young males are the best resurfacing candidates, and surgeons should use large-diameter femoral heads. Although surgeons do not stipu-late an age cut-off, the typical re-surfacing patient is under age 60. People over age 60 can receive re-surfacing surgery provided they have solid bone stock.
Replacement or Resurfacing—Which is Better?Both total hip replacement and re-surfacing have advantages and dis-advantages.
The advantages of total hip replacement:Currently, the outcomes for total hip replacement implants are bet-ter than resurfacing. In general,
CONT
INUI
NG
EDUC
ATIO
N
“Both total hip replacement and resurfacing have advantages and disadvantages.

ww
w.am
tamassage.org/m
tj 65
FIGURE A. XRAY OF PATIENT’S RIGHT HIP SHOWING OSTEOARTHRITIS.
FIGURE B. XRAY OF RIGHT HIP WITH NONMETAL TOTAL HIP REPLACEMENT.
FIGURE C: XRAY OF LEFT HIP WITH METALONMETAL TOTAL HIP REPLACEMENT.
FIGURE D: XRAY OF LEFT HIP WITH HIP RESURFACING COMPONENTS.
C
A
D
B

66
mtj
/mas
sage
ther
apy
jour
nal
spri
ng
201
4
total hip replacement implants re-main functional for longer periods than most resurfacing implants, and present fewer issues related to implant failure (discussed in greater detail later in this course). Surgeons can adjust a patient’s leg length to match the other leg during hip replacement surgery, too, which is nearly impossible to address during resurfacing surgery because the femur anatomy is pre-served and there is less ability to ad-just the length of the components. Certain conditions, including avascular necrosis, Perthe’s dis-ease, slipped capital epiphysis or high grade hip dysplasia, make hip replacement one of the only viable options, as resurfacing isn’t an ap-propriate treatment. Most total hip replacement im-plants do not have metal articu-lating with metal, whereas all hip resurfacing implants have metal-on-metal contact. Concerns related
to metal-on-metal implants include elevated blood levels of metal ions and adverse tissue reactions.
The advantages of hip resurfacing:Surgeons do not remove the femur head and neck, thus preserving more bone compared to total hip re-placement. However, this advantage may be negated if extra acetabular bone is removed to accommodate the large metal cap. The stress load (force across the joint) on articulating surfaces may be better in resurfacing than total hip replacement, too, which possi-bly decreases bone loss over time (Kishida, Sugano, Nishii, Miki, Ya-maguchi & Yoshikawa, 2004). In general, patients who undergo re-surfacing may have better hip ab-duction, joint proprioception and lower dislocation rates. Although surgeons and implant manufacturers promote the idea that patients can return to an active
CONT
INUI
NG
EDUC
ATIO
N
FIGURE A: ACETABULAR COMPONENT SHOWING METAL SHELL. FIGURE B: ACETABULAR COMPONENT SHOWING INSIDE LINER.
lifestyle after resurfacing sur-gery, this idea remains unclear. High impact activities (running, singles tennis) may, in fact, has-ten the implant failure. You need to remember that im-plant components in both total hip replacement and resurfac-ing consist of an artifi cial femur ball (or cap) that articulates with the artifi cial acetabulum. The ball (or cap) and acetabulum are made of either metal, polyethyl-ene or ceramic. Each femur-ace-tabulum combination or system, is described as metal-on-metal, metal-on-polyethylene or ceram-ic-on-ceramic. Currently, all re-surfacing systems use metal-on-metal, while approximately 35 percent of total hip replacement systems use metal-on-metal sys-tems. The metal-on-metal systems can wear, corrode and release metal debris. Reports of elevated
A B

ww
w.am
tamassage.org/m
tj 67
metal ions and tissue damage have raised concern among patients, doctors and government agencies. Metal ions in blood and urine are detected weeks to years following surgical implant of these compo-nents. Metal debris can cause ad-verse local tissue reactions near the implant, such as pseudotumors (non-malignant growths), which can cause pain and dysfunction (Bisschop, Boomsma, Van Raay, Tiebosch, Maas & Gerritsma, 2013). Metal-on-metal implants may be more problematic in poorly func-tioning implants. According to Hal-lab and colleagues (2001) (and cited in Basko-Plluska, et al., 2011) “the prevalence of metal allergy was ap-proximately 25% among patients with a well-functioning hip arthro-plastic implant and 60% among pa-tients with a failed or poorly func-tioning implant.” According to the authors, it’s unclear “whether metal allergy causes device failure or whether device failure causes metal allergy.” However, the concerns linked to metal-on-metal implants are nei-ther simple nor easy to evaluate. Some patients with these implants develop pain and tissue damage, for example, whereas others remain as-ymptomatic. And symptoms do not always correlate with the absolute amount of metal ions in tissues. The FDA recommends that as-ymptomatic patients with metal-on-metal implants follow up with their orthopedic doctor every one to two years, and patients that de-velop symptoms should seek medi-cal evaluation. Symptoms include changes in skin (a new rash), ner-vous system (hearing or vision im-pairment), mental status (depres-sion or cognitive defi cits), and kid-ney (impairment) or thyroid (weight change, fatigue) function.
Surgical approaches for the hip. The location of the incision for total hip replacement and resurfacing deter-mines the type of approach the sur-geon uses. Although there are mul-tiple approaches, the anterior and posterior approaches are the focus of this article. We’ll also focus some time on the less invasive surgery ap-proach. Each approach is named accord-ing to the location of the incision, with reference to the great trochan-ter. For example, the posterior ap-proach incision is made posterior to the greater trochanter.
Posterior Approach. The posterior or traditional approach is the most widely used in the United States. The patient is placed in the prone position or on the side (lateral decu-bitus). The surgeon makes a 10- to 12-inch, curved incision over the buttocks (posterior to the great-er trochanter). The surgeon cuts through the gluteus maximus, ex-ternal rotator muscles and the pos-terior joint capsule. Compared to other approaches, the advantages of the posterior ap-
proach are its long and successful history, the large, visual exposure of the acetabulum and femur it pro-vides and the fact that the abductor muscles are not cut. The disadvantages include the fact that the patient’s gluteus maxi-mus and short external rotator muscles are cut (and may or may not be reattached), increasing the risk of posterior dislocation. The sciatic nerve is at risk of being in-advertently cut, as well, and the incision is long (compared to the other approaches). Because of the risk of dislocation, the patient must follow strict hip precautions. These include limited hip fl exion and in-ternal rotation up to one year after surgery.
Anterior Approach. The patient is placed in the supine position and the surgeon makes a 7- to 10-inch linear (straight) incision anterior to the greater trochanter, separating the vastus lateralis and rectus femo-ris (or rectus femoris and sartorius). The surgeon then cuts through the anterior joint capsule. The advantages of the anterior
Advantages of Total Hip Replacement and Hip ResurfacingTOTAL HIP REPLACEMENT: > Better outcomes > Ability to alter leg length> Appropriate for certain conditions > No metal-on-metal issues (in non-metal implants)
HIP RESURFACING:> Bone preservation> More natural hip stress load> Better hip abduction, joint proprioception > Low dislocation rate

68
mtj
/mas
sage
ther
apy
jour
nal
spri
ng
201
4
approach are less muscle damage because muscles are spread/sepa-rated. There is also a low risk of dis-location (because external rotator muscles are not cut), and it’s more cosmetically appealing because a smaller incision is used. The disadvantage is this approach is more technically demanding for the surgeon. The anterior approach makes it diffi cult for the surgeon to align the femur with the prosthetic implant, thus increasing the risk of fracture to the femur. Although the risk of dislocation is low, the surgeon may place the patient on hip precautions, limit-ing hip hyperextension and exces-sive external rotation up to one year post-surgery, for example. Note that hyperextension and external rota-tion are movements used in some yoga poses (i.e., warrior pose), thus caution is warranted.
Less invasive surgery. This approach incorporates small incisions and minimally invasive techniques. Typically, small incision indicates that the incision is about half the length of the conventional (ante-rior and posterior, for example) approach. Minimally invasive usu-ally indicates use of an innovative technique that produces less tissue trauma. In some medical clinics,
“less invasive surgery may include unique pre- and post-operative pathways for anesthesia, nursing care and rehabilitation” (American Association of Hip and Knee Sur-geons; accessed 11/01/13). In hip replacement surgery, one type of less invasive surgery uses a single, small (4- to 6-inch) capsular incision and minimal muscle de-tachment, and has various names, including mini-anterior, mini-pos-terior, and mini-anterolateral sur-gery. A second, less invasive tech-nique incorporates two small (2- to 4-inch) incisions, one anterior and the other posterior to the greater trochanter. The anterior incision allows the surgeon access to the fe-mur, whereas the posterior incision allows access to the acetabulum. This technique is called the two-incision minimally invasive surgery. Advantages of the less invasive surgery are smaller, cosmetically appealing incisions, and less muscle damage. Also, the phrase “minimal-ly invasive” provides a psychologi-cal advantage. In other words, some people equate the word “minimal” to “less pain.” Less invasive surgery, however, potentially has more complications. First, a small incision produces a re-stricted visual fi eld for the surgeon
and can result in greater tissue trauma and nerve damage. Second, the surgeon may fi nd that learning and applying the less invasive sur-gery is more technically demand-ing, requiring different instruments and specialized equipment. Additionally, some less invasive surgery techniques may result in implant mis-alignment, fracture and prolonged time in the operating room. For the patient, more blood loss and extended time under anes-thesia can occur.
Complications and RevisionHip replacement surgery carries sig-nifi cant risk of negative outcomes. During the surgery (and soon after) there is risk of blood clots, fracture, infection, nerve injury, signifi cant blood loss and complications relat-ed to anesthesia. Long-term com-plications include metal sensitivity, leg length differences, nerve palsy, scarring and pain. Complications associated with metal-on-metal hip implants are elevated metal ion lev-els in the joint, blood and systemic reactions, and possible transport of metal ions across the placenta. There is an increased risk of femo-ral neck fracture in hip resurfacing. Some implants fail, necessitating a second hip replacement called a “revision” surgery. With a revision,
CONT
INUI
NG
EDUC
ATIO
N
“Less invasive surgery incorporates small incisions and minimally invasive techniques.

ww
w.am
tamassage.org/m
tj 69
part or all of the implant compo-nents are replaced. In the United States, approximately 50,000 revi-sions occur each year (Steiner et al., 2012). Revision surgery is more complex than the primary surgery, typically requiring a larger incision and deli-cate removal of the old components and cement. Replacing (grafting) bone from a bone bank might also be necessary. The reasons for revision surgery are complex and involve multiple factors related to the patient, sur-geon and implant. Patient-related factors include young age, highly active, diagnosed with infl amma-tory disorders) such as avascular necrosis and rheumatoid arthritis), multiple comorbidities (sickle cell anemia and poor bone quality, for example) and prone to infections. Surgeon-related factors range from less experience (fewer sur-geries) to incorrect placement of implants, while implant-related factors include instability (implant movement) and bearing surface fail-ure (i.e., the once-smooth surface cracks or becomes rough). This fail-ure results in bone separation (os-teolysis) and the implant loosening, two common reasons for revision (Prokopetz, Losina, Bliss, Wright, Baron & Katz, 2012). In general, the longevity or surviv-al of the patient’s implant is longer after primary surgery than after a revision surgery. Most primary total hip replacement implants survive 15 to 20 years. The longevity of the revision surgery is more variable: 35 percent to 100 percent fail within 10 years. A higher failure rate oc-curs in younger patients (Springer, Fehring, Griffi n, Odum & Masonis, 2009) because patients less than 65 years of age tend to be more active, weigh more and live longer than older counterparts. Advancements
in the technology of new implant designs, computer-assisted surger-ies and more experience with mini-mally invasive surgery will likely increase the longevity of revision surgery.
Surgical treatment—the knee. Nine-ty-seven percent of total knee re-placements are performed because of advanced, symptomatic osteoar-thritis (American Academy of Or-thopaedic Surgeons, 2011). A small percentage of patients undergo sur-gery due to ligament injuries, rheu-matoid arthritis, dislocation and fractures. Patients have two surgical op-tions to treat severe osteoarthritis: total and partial knee replacement. In total knee replacement surgery, the distal femur, tibial plateau, and cruciate ligaments are removed and replaced with artifi cial prosthe-ses. In contrast, only small areas of the knee (e.g., small sections of the tibia, femur or patella) are re-moved and replaced in partial knee replacement surgery.
Total knee replacement. With total knee replacement, the surgeon cuts through skin, adipose, fascia and the joint capsule; some surgeons in-vert or pull the patella to the side. Once the articular cartilage is ex-posed, the surgeon cuts through and removes the ends of the distal femur and proximal tibia bones. In most cases the surgeon removes the anterior and posterior cruciate liga-ments, although some tibial compo-nent designs allow retention of liga-ments. If the patella contains ex-tensive osteoarthritic damage, the surgeon removes and resurfaces the posterior side (patellar component). The surgeon inserts metal fi tted components over the femur (femo-ral component) and tibia (tibial component), securing each compo-
Advantages of Total Knee and Partial Knee Replacement SurgeryTOTAL KNEE REPLACEMENT:> Longer prosthesis survival> Better adjustment of leg length and
knee angle deformities > Successful history > Appropriate for certain conditions
(torn ACL, extensive osteoarthritis damage, and rheumatoid arthritis)
PARTIAL KNEE REPLACEMENT:> Small incision> Greater bone preservation> Less traumatized tissue and blood
loss> Lower dislocation rate> Quicker recovery> More natural feel during movement
and greater range of motion

70
mtj
/mas
sage
ther
apy
jour
nal
spri
ng
201
4
nent with special cement or using a procedure called press-fi t fi xation, which allows for bone ingrowth. A plastic spacer (also called an outlay) is inserted between the metal femur and tibia components. The femoral component is typi-cally an alloy of cobalt-chromium; the tibial component (also called a tray) may be cobalt-chrome or tita-nium. Some companies use a new metal called oxidized zirconium. The spacer (outlay) is made of a hard polyethylene (plastic). The pa-tellar component is made of metal or plastic.
Candidates for total knee replace-ment. People who are healthy, within normal weight and have solid bones are good candidates for total knee replacement. Healthy pa-tients have strong immune systems that combat infections and stress. Again, normal weight patients place less stress on joints, so patients with body mass index (BMI; body mass divided by height squared) greater than 35 are encouraged to lose weight before surgery. Patients also need good bone stock to secure the implants. Candidates for total knee re-placement can be any age, but risk increases with age. Total knee re-placement surgery is contraindi-cated in patients with infections, compromised immune systems, renal insuffi ciency, allergy to metal implants and some other condi-tions. Total knee replacement sur-gery may be contraindicated in patients with major psychiatric dis-orders (including dementia), as well as neurological and muscular disor-ders because these conditions make rehabilitation diffi cult.
Partial knee replacement. Similar to total knee replacement, partial
knee replacement surgery entails incisions through all joint-related tissues, although the incision may be smaller. In contrast to total knee replacement, only the arthritic-damaged surfaces are replaced or resurfaced (and the healthy carti-lage is retained) in partial knee re-placement surgery. There are two major types of par-tial knee replacement systems: uni- and bicompartmental knee replace-ments surgeries. Unicompartmental surgery replaces a single area of the knee, such as the medial, lateral or patellar articulating surfaces. Bicompartmental surgery involves replacing two articulating surfaces. Typically, the cruciate ligaments re-main intact in both uni- and bicom-partmental surgeries. The component materials used in partial replacement systems are similar to total knee replacement systems and include cobalt-chrome, titanium or oxidized zirconium.
Candidates for partial knee replace-ment. Only 10 percent to 15 percent of patients are suitable for partial knee replacement. Partial knee replacement is appropriate for pa-tients with small arthritic areas, typically confi ned to one side of the knee and with mild varus (“bow-legged”) or valgus (“knock-knees”) deformity. Similar to total knee replacement, patients should be in good health, appropriate weight (BMI less than 35) and have good bone stock. Partial knee replacement surger-ies are not appropriate for patients with a torn anterior cruciate liga-ment, extensive osteoarthritis dam-age and rheumatoid arthritis. This surgery is also contraindicated in patients with infections, compro-mised immune systems and some other conditions.
CONT
INUI
NG
EDUC
ATIO
N
“Ninety-seven percent of total knee replacements are performed because of advanced, symptomatic osteoarthritis.

ww
w.am
tamassage.org/m
tj 71
“Knee replacement surgery carries risk of short- and long-term complications.

72
mtj
/mas
sage
ther
apy
jour
nal
spri
ng
201
4
Total or Partial Knee Replace-ment—Which is Better?Both total and partial knee replace-ment surgeries have advantages and disadvantages.
The advantages of total knee replacement:Total knee replacement compo-nents remain functional for lon-ger periods than most partial knee components. For example, the nine-year failure rate for total knee re-placement surgery ranges from 2.9 percent to 6.7 percent compared with 11.6 percent to 16 percent re-ported for partial knee replacement surgery (Full 10th NJR Annual Re-port, 2013). Surgeons correct leg length and varus/valgus deformities better with total knee replacement surgery. Moreover, surgeons are more famil-iar, and commonly perform, total knee replacement surgeries. Finally, patients with a torn an-terior cruciate ligament, extensive osteoarthritis damage and rheu-matoid arthritis can undergo total knee replacement surgery, whereas partial knee replacement surgery is not appropriate for these condi-tions.
The advantages of partial knee re-placement:Surgeons typically use smaller in-cisions and remove less bone with partial knee replacement surgeries. Because of less tissue disruption, patients experience less blood loss, lower dislocation risk, and recover quicker from surgery. Some patients report a more “natural feeling” knee and greater range-of-motion after receiving partial knee replacement.
Implant material concerns. Knee re-placement components wear-out, produce debris and create metal sensitivity in some patients. Poly-
ethylene wear is evident by the pro-gressive growth of infl ammatory tis-sue in and around the joint. The im-plant wear may be dependent on the manufacturer, implant design, skill of the surgeon and activity level of the patient. Some knee replacement implants have problems with metal debris and corrosion. Savarino and col-leagues (2010) measured serum chromium metal ion levels in pa-tients that had stable or unstable components and reported that ion levels were signifi cantly higher in patients with unstable components than in patients with stable compo-nents.
Surgical approaches—the knee The location of the incision for to-tal and partial knee replacements determines the type of approach the surgeon uses. There are two conventional approaches, medial and lateral, and a third technique called less invasive. Each approach is named according to the location of the incision in reference to the patella. Scholars greatly debate the ad-vantages and disadvantages of each approach, and various opinions re-sult. Because of this complexity, the pros and cons of each approach are beyond the scope of this article.
Medial approach. With the patient in the supine position, the surgeon makes an 8- to 12-inch incision medial to the patella through skin and adipose; with the knee bent, a second incision is made through the joint capsule. To expose the knee’s articulating surfaces, some surgeons cut or lift a small segment of the distal quadriceps (rectus femoris or vastus medialis). This techniques is commonly known as midvastus split or subvastus. In contrast, some surgeons do not cut
the quadriceps, known as quad-sparing.
Lateral approach. With the patient in the supine position, the surgeon makes an 8- to 12-inch incision lateral to the patella, and with the knee bent, a second incision is made through the joint capsule. Surgeons either cut or spare the vastus latera-lis and rectus femoris muscles.
Less invasive surgery. Similar to hip replacement surgery, “less in-vasive surgery” incorporates small incisions and minimally invasive techniques. The surgeon typically makes a 4- to 6-inch incision, com-pared with the conventional 8 to 12 inches. In addition, the surgeon main-tains minimal tissue trauma with small incisions to the extensor muscles and/or the suprapatellar bursa, a technique called mini-mid-vastus or mini-subvastus. Sparing the extensor muscles is called mini quad-sparing. Unfortunately, the multiple names for similar surgeries create confusion in the media and research literature.
Complications and RevisionsKnee replacement surgery carries risk of short and long-term compli-cations. During (and soon after) the surgery, there is risk of blood clots, fracture, infection, nerve injury, signifi cant blood loss and complica-tions related to anesthesia. Long-term complications are aseptic (no infection) component loosen-ing, wound infection, polyethylene component wear, instability, pain and stiffness, osteolysis (bone loss), and bone-implant misalignment (Dalury, Pomeroy, Gorab & Adams, 2013). Additionally, there is risk of leg length differences, nerve palsy, scarring and pain. If a complication results in the
CONT
INUI
NG
EDUC
ATIO
N

ww
w.am
tamassage.org/m
tj 73
If a complication results in the failure of the implant, a second sur-gery—or revision—is necessary. A recent study reported that many of the revisions that occurred within fi ve years of surgery were the result of infection, and instability/mal-position. Revisions after fi ve years resulted from implant wear, loos-ening, and instability/malposition (Dalury, et al., 2013). The longevity or survival of total knee replacement implants in pa-tients at 10 years ranged from ap-proximately 90 percent to 95 per-cent (Gøthesen, Espehaug, Havelin, Petursson, Lygre, Ellison, Hallan & Furnes, 2013), although survival is dependent on factors such as type of implant and surgeon experi-ence. (Australian Orthopaedic As-sociation National Joint Replace-ment Registry. Annual Report. Adelaide:AOA; 2013). Patient-related factors, such as age, also infl uence the longevity of the implant. At fi ve years, implant survival rates were lowest (92 per-cent) in patients aged 55 years or younger, compared with patients age 56 to 65 years (95 percent) and 65 years or older (97 percent) (Ju-lin, Jämsen, Puolakka, Konttinen & Moilanen, 2010). The age-related risk may refl ect a higher activity level, greater obesity or other fac-tors. Other patient-related risks associated with implant longevity are poor patient health, comorbidi-ties (e.g., diabetes), and higher body mass index (Paxton, Inacio, Khatod, Yue & Namba, 2010). The rate of revision is higher af-ter partial knee replacement. At ten years, an average 16.5 percent revision rate was reported for par-tial replacements, compared with 6.2 percent revision rate after total knee replacement (Pabinger, Berg-hold, Boehler & Labek, 2013).
Post-Surgery—Hip and Knee Rehabilitation and ConditioningMassage and physical therapy play an important role in a patient’s re-covery from hip and knee replace-ment surgery. Hospital-based mas-sage therapists provide individu-alized therapy that is dependent on the patient’s needs, massage therapist’s training and hospital’s protocol. For example, the massage therapist may address a patient’s pain and edema by applying gentle back, foot or hand massage, or use manual lymphatic drainage. Hospi-tal protocol may dictate the appli-cation of massage once or twice per day until discharge of the patient. The hospital-based physical ther-apists provide therapy directed at post-surgical ambulation. For exam-ple, the physical therapist encour-ages the patient to conduct simple “muscle-waking” exercises, such as gluteal contractions, ankle circles, and heel slides (hip replacement patients), as well as quadriceps con-tractions, ankle pumps, and heal slides (knee replacement patients). In time, the patient learns how to safely move to the edge of the bed, rise from a chair, and walk with crutches or a walker. Before discharge from the hospital, the patient must demonstrate (using
crutches or a walker) the ability to walk a short distance, and ascend and descend stairs safely. Some doctors require patients to continue to use a walker or crutches for four weeks (hip replacement) or six to eight weeks (knee replacement) af-ter surgery. After discharge from the hospital, the patient will either go home or to an inpatient rehabilitation center. Patients that go home presumably have a partner or family member to assist the patient with dressing changes, meals and bathing. Physi-cal therapists may come to the pa-tient’s house several days per week to ensure the patient is moving properly and performing exercises. Patients that go directly to inpatient rehabilitation facilities have nurs-ing staff trained to change wound dressings, assist in bathing and gen-eral ambulation, and physical thera-pists trained to properly strengthen and rehabilitate hips and knees. Approximately two weeks after hip or knee surgery, patients at-tend outpatient physical therapy programs. Physical therapy is an essential part of the rehabilitation process. Patients participate in outpatient physical therapy for sev-eral weeks to increase strength and range-of-motion. A recent study demonstrated that the combination
“Massage and physical therapy play an important role in a patient’s recovery from hip and knee replacement surgery.

74
mtj
/mas
sage
ther
apy
jour
nal
spri
ng
201
4
of physical therapy and (modifi ed) asana yoga benefi tted total knee re-placement patients (Bedekar, Prab-hu, Shyam, Sancheti & Sancheti, 2012). Specifi cally, the patients reported “better pain relief, less stiffness and better function.” The authors reported the yoga exercises did not produce any adverse effects. Following outpatient therapy, the patient can resume normal activi-ties, although some surgeons sug-gest patients practice precautions for approximately six months to one year post-surgery. For example, hip precautions following a posterior approach include avoiding greater than 90-degree hip fl exion, crossing legs and inversion of the feet. Knee
precautions include an avoidance of deep knee bends, and knee twist-ing and kneeling.
Current Research—Benefi ts of Massage Therapy on Surgical PatientsJoint replacement surgery. Research supports the use of massage therapy as a therapeutic benefi t to replace-ment patients. For example, a re-cent study reported that combined massage and relaxation techniques benefi ted patients that underwent either total hip or knee replace-ment surgery (Büyükyılmaz & Aştı, 2013). Applications of 10-minute back massages (effl eurage and petrissage)
and relaxation (rhythmic respira-tion, muscle relaxation exercises and listening to music) twice daily after surgery resulted in decreased anxiety and pain in patients, com-pared to patients receiving only conventional care. Likewise, manual lymphatic drainage assists in functional re-covery following joint replacement. A recent study examined the ef-fects of manual lymphatic drainage in post-knee replacement patients (Ebert, Joss, Jardine & Wood, 2013). One group of patients received a standard 30-minute session (plus standard care) and a second group received only standard care. The authors reported that greater knee
“Research supports the use of massage therapy as a therapeutic benefi t to replacement patients.
CONT
INUI
NG
EDUC
ATIO
N

ww
w.am
tamassage.org/m
tj 75
fl exion occurred in patients who received manual lymphatic drain-age (compared with patients that did not) four days post-surgery and six weeks after surgery. Moreover, manual lymphatic drainage patients reported “improved feeling of well-being and a more relaxed physical and/or mental state.”
Massage and other surgeries. The benefi ts of massage therapy are known to help various post-surgi-cal patients. For example, massage reduced pain and anxiety, and in-creased a sense of well-being in post-mastectomy patients (Drackley, Degnim, Jakub, Cutshall, Thomley, Brodt, Vanderlei, Case, Bungum, Cha, Bauer & Boughey, 2012) and reduced pain, anxiety and tension in patients following cardiac sur-gery (Cutshall, Wentworth, Engen, Sundt, Kelly & Bauer, 2010; Braun, Stanguts, Casanelia, Spitzer, Paul, Vardaxis & Rosenfeldt, 2012). Manual lymphatic drainage decreased swelling and pain fol-lowing surgical mastectomy (For-chuk, Baruth, Prendergast, Hol-liday, Bareham, Brimner, Schulz, Chan & Yammine, 2004), improved lymphedema in post-bariatric sur-gery patients (Bertelli, de Oliveira, Gimenes & Moreno, 2013) and in heart failure patients (Leduc, Crasset, Leleu, Baptiste, Koziel, Delahaie, Pastouret, Wilputte & Leduc, 2011), and decreased foot volume and improved quality of life in patients with chronic venous dis-ease (Molski, Kruczyński, Molski & Molski, 2013). Massage therapy may infl uence the progressive nature of scar tissue too. Martínez Rodríguez and Galán del Río (2013) proposed that specif-ic scar modeling techniques might alter the formation of scar tissue due to myofascial injury. Further, Roh and colleagues (2007) reported
improvement in scar-related char-acteristics, such as skin pigmenta-tion, pliability and vascularity and scar height after daily massage for three months. Moreover, massage produced a signifi cant decrease in depression in patients with burn scars (Roh, et al., 2007).
Being Mindful Before and After SurgeryThe massage therapist must always work within the scope of practice when dealing with patients. Com-municate with the patient’s surgical team (surgeon, physician assistant, physical therapist) to determine pre-surgical contraindications and when to initiate post-surgical mas-sage therapy. Remember, too, you need to be mindful of the patient’s needs be-fore and after joint surgery, and plan ahead to best address each issue. Prior to surgery, the patient likely has high stress and anxiety, and fl uctuating mood. The massage therapist can provide relaxation techniques and a safe environment to promote a sense of well-being. The pre-surgical patient likely has relentless joint pain and mus-cle stiffness. Hydrotherapy soothes and warms muscles and joint struc-tures; gentle massage increases heat and circulation to the affected area. Joint mobilization with deep pressure is contraindicated because of increased risk of tissue irritation. Also, avoid contact with the surgical site within 48 hours of surgery. The patient is probably also tak-ing pain and/or anti-infl ammatory medications, so be aware of medica-tion side effects and possible altered sensation. After surgery, the patient may experience a psychological roller coaster of emotions, including relief once the surgery is complete. How-ever, if the outcomes of the surgery
“Communicate with the patient’s surgical team (surgeon, physician assistant, physical therapist) to determine pre-surgical contraindications and when to initiate post-surgical massage therapy.

76
mtj
/mas
sage
ther
apy
jour
nal
spri
ng
201
4
This mtj article serves as the basis for the AMTA Online Course of the same name. To register for the course and receive continuing education hours, please visit amtamassage.org/learn.
AMTA RESOURCE
or recovery fall short of expecta-tions, the patient may experience frustration and depression. The massage therapist can provide com-fort and empathy through engaged listening and a calm environment. Gentle massage of the head, hands and feet can sooth and distract the patient. Also, the post-surgical patient will have signifi cant tissue trauma. The muscles and new joint must relearn to function and support the body once again. The massage therapist can provide brief, gentle touch to distal sites to help decrease pain and anxiety. Manual lymphatic drainage enhances lymph fl ow and decreases edema. Avoid the surgical site because of risk of infection and pain. Be aware of post-surgical compli-cations and joint precautions. The surgeon will provide the patient with instructions regarding possible post-surgical complications, such as symptoms of a blood clot and infec-tion. Also, depending on the type of surgery and approach, the surgeon will provide hip or knee precau-tions. Follow the precautions when applying massage, stretching, pas-sive and active movements. The post-surgical patient will likely take medication for pain, blood clot prevention and infection. Once again, be aware of possible side effects, and the patient’s level
of pain and sensation. Blood thin-ners are meant to prevent clots, but they also increase the risk of skin bruising. Therefore, adjust the pres-sure of the massage accordingly. If any unexplained swelling or pain arises, immediately refer the pa-tient to the medical provider. Also, make note of any co-mor-bidities that may infl uence your massage, such as diabetes and pe-ripheral neuropathy. Massage can alter blood glucose levels and possi-bly hasten fatigue, and neuropathy can alter the level of sensation. The massage therapist must adapt both the massage (and awareness) to the each patient’s circumstances. Once the risk of infection has passed, the message therapist can initiate scar therapy with gentle intent. The massage therapist may perform assisted, then passive movements of the patient’s affected limb. Continue lymphatic drainage and support healing through aware-ness and touch.
In SummaryOsteoarthritis is a complex con-dition characterized by the slow, chronic destruction of joints, and is the primary cause of joint pain and disability. Aging, gender, joint trau-ma, obesity, genetics, and muscle weakness are risk factors for devel-oping osteoarthritis. Non-surgical treatments to alleviate osteoarthrit-
ic pain include strengthening exer-cises, activity modifi cation, weight loss, manual therapy, acupuncture and the use of a cane or walker. Joint replacement surgery is an op-tion only when the osteoarthritis signifi cantly affects the patient’s quality of life and loss of function interferes with daily activities. Joint replacement surgery is com-mon worldwide and successfully al-leviates symptoms of osteoarthritis. Many factors infl uence the outcome of replacement surgery, such as pa-tient-characteristics (age, activity level and co-morbidities, for exam-ple), prosthesis, surgical skill and post-surgery rehabilitation. Surgical options are available for osteoarthritic hips and knees (e.g., total hip replacement, hip resurfac-ing; total and partial knee replace-ment). Total hip and total knee replacement surgeries are more common and have a longer survival rate than do resurfacing and partial knee replacement. Massage therapy plays an impor-tant role in the patient’s pre- and post-surgical journey. Massage helps to decrease pain, anxiety, edema, and muscle stiffness, and increase mobility and sense of well-being. Manual lymphatic draining, specifi c muscle massage, stretch-ing, and scar tissue massage are important techniques that massage therapists can incorporate into the
CONT
INUI
NG
EDUC
ATIO
N

ww
w.am
tamassage.org/m
tj 77
patient’s rehabilitation plan. Aware-ness and compassion are impera-tive. As a part of the health care team, massage therapists provide a valuable service to the patient’s road to recovery. ■
REFERENCESSteiner C, Andrews R, Barrett M, Weiss A.
HCUP Projections: Mobility/Orthopedic
Procedures 2011 to 2012. 2012. HCUP Pro-
jections Report # 2012-03. ONLINE Septem-
ber 20, 2012. U.S. Agency for Healthcare
Research and Quality. Available: http://
www.hcup-us.ahrq.gov/reports/projec-
tions/2012-03.pdf
Kurtz S, Ong K, Lau E, Mowat F, Halpern
M. Projections of primary and revision hip
and knee arthroplasty in the United States
from 2005 to 2030. J Bone Joint Surg Am.
2007 Apr;89(4):780-5.
Kim S. Changes in surgical loads and
economic burden of hip and knee re-
placements in the US: 1997-2004. Arthritis
Rheum. 2008 Apr 15;59 (4):481-8.
Lawrence RC, Felson DT, Helmick CG, Ar-
nold LM, Choi H, Deyo RA, Gabriel S, Hirsch
R, Hochberg MC, Hunder GG, Jordan JM,
Katz JN, Kremers HM, Wolfe F; National
Arthritis Data Workgroup. Estimates of the
prevalence of arthritis and other rheumatic
conditions in the United States. Part II. Ar-
thritis Rheum. 2008 Jan;58(1):26-35.
The Arthritis Foundation, www.arthritis.
org (accessed 10/14/13).
Murphy LB, Helmick CG, Schwartz TA,
Renner JB, Tudor G, Koch GG, Dragomir AD,
Kalsbeek WD, Luta G, Jordan JM. One in
four people may develop symptomatic hip
osteoarthritis in his or her lifetime. Osteoar-
thritis Cartilage. 2010 Nov;18(11):1372-9.
Murphy L, Schwartz TA, Helmick CG,
Renner JB, Tudor G, Koch G, Dragomir A,
Kalsbeek WD, Luta G, Jordan JM.Lifetime
risk of symptomatic knee osteoarthritis. Ar-
thritis Rheum. 2008 Sep 15;59(9):1207-13.
Buckwalter JA, Saltzman C, Brown T. The
impact of osteoarthritis: implications for re-
search. Clin Orthop Relat Res. 2004 Oct;(427
Suppl):S6-15.
Felson DT, Zhang Y, Anthony JM, Nai-
mark A, Anderson JJ. Weight loss reduces
the risk for symptomatic knee osteoarthri-
tis in women. The Framingham Study. Ann
Intern Med. 1992 Apr 1;116(7):535-9.
Sowers MR, Karvonen-Gutierrez CA
The evolving role of obesity in knee os-
teoarthritis. Curr Opin Rheumatol. 2010
Sep;22(5):533-7.
Valdes AM, Spector TD. Genetic epide-
miology of hip and knee osteoarthritis. Nat
Rev Rheumatol. 2011 Jan;7(1):23-32.
Alnahdi AH, Zeni JA, Snyder-Mackler
L. Muscle impairments in patients with
knee osteoarthritis. Sports Health. 2012
Jul;4(4):284-92.
Nambi GS, Shah AA. Additional eff ect of
iyengar yoga and EMG biofeedback on pain
and functional disability in chronic unilat-
eral knee osteoarthritis. Int J Yoga. 2013
Jul;6(2):123-7.
Cook KM, Heiderscheit B. Conservative
management of a young adult with hip
arthrosis. J Orthop Sports Phys Ther. 2009
Dec;39(12):858-66.
Atkins DV, Eichler DA. The eff ects of self-
massage on osteoarthritis of the knee: a
randomized, controlled trial. Int J Ther Mas-
sage Bodywork. 2013;6(1):4-14.
Perlman AI, Sabina A, Williams AL, Njike
VY, Katz DL. Massage therapy for osteoar-
thritis of the knee: a randomized controlled
trial. Arch Intern Med. 2006 Dec 11-25;
166(22):2533-8.
United States Bone and Joint Initiative:
The Burden of Musculoskeletal Diseases
in the United States, Second Edition. Rose-
mont, IL: American Academy of Orthopae-
dic Surgeons; 2011.
2006 estimates suggested by Millenni-
um Research Group; http://mrg.net/News-
and-Events/Press-Releases/QUARTERLY-
ORTHOPEDIC-RECONSTRUCTIVE-IMPLANT-
MARKET.aspx (accessed 10/16/13).
Australian Orthopaedic Association Na-
tional Joint Replacement Registry. Annual
Report. Adelaide:AOA; 2013.
Full 10th NJR Annual Report 2013; avail-
able at www.njrcentre.org.uk (accessed
10/31/13).
Smith AJ, Dieppe P, Howard PW, Blom
AW; on behalf of the National Joint Regis-
try for England and Wales. Failure rates of
metal-on-metal hip resurfacings: analysis
of data from the National Joint Registry for
England and Wales. Lancet. 2012 Nov 17;
380(9855): 1759-66.
Kishida Y, Sugano N, Nishii T, Miki H, Ya-
maguchi K, Yoshikawa H. Preservation of
the bone mineral density of the femur after
surface replacement of the hip. J Bone Joint
Surg Br. Mar 2004;86(2):185-9.
Bisschop R, Boomsma MF, Van Raay JJ,
Tiebosch AT, Maas M, Gerritsma CL. High
Prevalence of Pseudotumors in Patients
with a Birmingham Hip Resurfacing Pros-
thesis: A Prospective Cohort Study of One
Hundred and Twenty-nine Patients. J Bone
Joint Surg Am. 2013 Sep 4;95(17):1554-60.
Hallab N, Merritt K, Jacobs JJ. Metal sen-
sitivity in patients with orthopaedic im-
plants. J Bone Joint Surg Am. 2001 Mar;83-
A(3):428-36; Direct quote, p. 69, from
Basko-Plluska JL, Thyssen JP, Schalock PC.
Cutaneous and systemic hypersensitivity
reactions to metallic implants. Dermatitis.
2011 Mar-Apr;22(2):65-79. Review.
American Association of Hip and Knee
Surgeons. http://www.aahks.org/patients/
resources/MIS_Patients.pdf; (accessed
11/01/13).
Prokopetz JJ, Losina E, Bliss RL, Wright J,
Baron JA, Katz JN. Risk factors for revision of
primary total hip arthroplasty: a systematic
review. BMC Musculoskelet Disord. 2012
Dec 15;13:251.
Springer BD, Fehring TK, Griffi n WL,
Odum SM, Masonis JL. Why revision total
hip arthroplasty fails. Clinical Orthopaedics
and Related Research. 2009;467:166–173.
Savarino L, Tigani D, Greco M, Baldini
N, Giunti A. The potential role of metal
ion release as a marker of loosening in
patients with total knee replacement: a
cohort study. J Bone Joint Surg Br. 2010
May;92(5):634-8.
Dalury DF, Pomeroy DL, Gorab RS, Ad-
ams MJ. Why are total knee arthroplas-
ties being revised? J Arthroplasty. 2013
Sep;28(8 Suppl):120-1.
Gøthesen O, Espehaug B, Havelin L, Pe-
tursson G, Lygre S, Ellison P, Hallan G, Furnes

78
mtj
/mas
sage
ther
apy
jour
nal
spri
ng
201
4CO
NTIN
UING
ED
UCAT
ION
cemented primary total knee replacement:
a report from the Norwegian Arthroplasty
Register 1994-2009. Bone Joint J. 2013
May;95-B(5):636-42.
Julin J, Jämsen E, Puolakka T, Konttinen
YT, Moilanen T. Younger age increases
the risk of early prosthesis failure follow-
ing primary total knee replacement for
osteoarthritis. A follow-up study of 32,019
total knee replacements in the Finnish
Arthroplasty Register. Acta Orthop. 2010
Aug;81(4):413-9.
Paxton EW, Inacio MC, Khatod M, Yue EJ,
Namba RS. Kaiser Permanente National To-
tal Joint Replacement Registry: aligning op-
erations with information technology. Clin
Orthop Relat Res. 2010 Oct;468(10):2646-
63.
Pabinger C, Berghold A, Boehler N,
Labek G. Revision rates after knee replace-
ment. Cumulative results from worldwide
clinical studies versus joint registers. Os-
teoarthritis Cartilage. 2013 Feb;21(2):263-8.
Bedekar N, Prabhu A, Shyam A, Sancheti
K, Sancheti P. Comparative study of con-
ventional therapy and additional yogasa-
nas for knee rehabilitation after total knee
arthroplasty. Int J Yoga. 2012 Jul;5(2):118-22.
Büyükyılmaz F, Aştı T. The eff ect of re-
laxation techniques and back massage on
pain and anxiety in Turkish total hip or knee
arthroplasty patients. Pain Manag Nurs.
2013 Sep;14(3):143-54).
Ebert JR, Joss B, Jardine B, Wood DJ.
Randomized trial investigating the ef-
fi cacy of manual lymphatic drainage to
improve early outcome after total knee
arthroplasty. Arch Phys Med Rehabil. 2013
Nov;94(11):2103-11.
Drackley NL, Degnim AC, Jakub JW, Cut-
shall SM, Thomley BS, Brodt JK, Vanderlei
LK, Case JK, Bungum LD, Cha SS, Bauer BA,
Boughey JC. Eff ect of massage therapy for
postsurgical mastectomy recipients. Clin J
Oncol Nurs. 2012 Apr;16(2):121-4.
Cutshall SM, Wentworth LJ, Engen D,
Sundt TM, Kelly RF, Bauer BA. Eff ect of
massage therapy on pain, anxiety, and
tension in cardiac surgical patients: a pilot
study. Complement Ther Clin Pract. 2010
May;16(2):92-5.
Braun LA, Stanguts C, Casanelia L,
Spitzer O, Paul E, Vardaxis NJ, Rosenfeldt
F. Massage therapy for cardiac surgery pa-
tients--a randomized trial. J Thorac Cardio-
vasc Surg. 2012 Dec;144(6):1453-9.
Forchuk C, Baruth P, Prendergast M, Hol-
liday R, Bareham R, Brimner S, Schulz V,
Chan YC, Yammine N. Postoperative arm
massage: a support for women with lymph
node dissection. Cancer Nurs. 2004 Jan-
Feb;27(1):25-33.
Bertelli DF, de Oliveira P, Gimenes AS,
Moreno MA. Postural drainage and manual
lymphatic drainage for lower limb edema
in women with morbid obesity after bariat-
ric surgery: a randomized controlled trial.
Am J Phys Med Rehabil. 2013 Aug;92(8):697-
703.
Leduc O, Crasset V, Leleu C, Baptiste N,
Koziel A, Delahaie C, Pastouret F, Wilputte
F, Leduc A. Impact of manual lymphatic
drainage on hemodynamic parameters in
patients with heart failure and lower limb
edema. Lymphology. 2011 Mar;44(1):13-20.
Molski P, Kruczyński J, Molski A, Molski S.
Manual lymphatic drainage improves the
quality of life in patients with chronic ve-
nous disease: a randomized controlled trial.
Arch Med Sci. 2013 Jun 20;9(3):452-8.
Martínez Rodríguez R, Galán del Río F.
Mechanistic basis of manual therapy in
myofascial injuries. Sonoelastographic
evolution control. J Bodyw Mov Ther. 2013
Apr;17(2):221-34.
Roh YS, Cho H, Oh JO, Yoon CJ. Eff ects
of skin rehabilitation massage therapy
on pruritus, skin status, and depression in
burn survivors. Taehan Kanho Hakhoe Chi.
2007 Mar;37(2):221-6.
STATEMENT OF OWNERSHIP, MANAGEMENT AND CIRCULATION
(Required by 39 U.S.C. 3685) Date of fi ling: 1114Title of publication: Massage Therapy Journal Publication No: 0895-0814Frequency of issue: quarterly No. of issues published annually: 4Annual subscription price: $25
Complete mailing address of known offi ce of publication:American Massage Therapy Association, 500 Davis St., Suite 900, Evanston, IL 60201-4695. Owner: American Massage Therapy Association, 500 Davis St., Suite 900, Evanston, IL 60201-4695.
Complete mailing address of headquarters or general business of the publisher: same as above.
Names and addresses of publisher and editor: publisher, American Massage Therapy Association; managing editor, Michelle Vallet, 500 Davis St., Suite 900, Evanston, IL 60201-4695. Owner: American Massage Therapy Association, 500 Davis St., Suite 900, Evanston, IL 60201-4695.
Known bondholders, mortgagees, and other security holders owning or holding 1 percent or more of total amount of bonds, mortgages, or other securities: None. The purpose, function, and nonprofi t status of this organization and the exempt status for federal income tax purposes have not changed during the preceding 12 months.
Heading for numbers in red: Average No. copies each issue during preceding 12 months. Heading for blue numbers: No. copies in single issue published nearest to fi ling date
Total No. of copiesPaid and/or requested circulation 51,486 51,385 Paid/requested outside-county mail subscriptions 50,455 50,354 Paid in-county subscriptions 0 0
Sales through dealers and carriers, street vendors, counter sales and other non- USPS paid distribution 0 0Other classes mailed through the USPS 0 0
Total paid and/or requested circulation 50,455 50,354Free distribution by mail Outside-county 31 31 In-county 0 0 Other classes mailed through the USPS 0 0Free distribution outside the mail 0 0Total free distribution 31 31Total distribution 50,486 50,385Copies not distributed 1,000 1,000Total 51,486 51,385Percent paid and/or requested circulation 100 100
I certify that the statements made by me above are correct and complete: Michelle Vallet, Managing Editor