undernutrition in the uk - british nutrition foundation in the... · undernutrition in the uksarah...
TRANSCRIPT
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
87
Blackwell Science LtdOxford UKNBUNutrition Bulletin0141-96842003 British Nutrition Foundation
2003
28
Original Article
Undernutrition in the UKSarah Schenker
Correspondence
Dr Sarah Schenker PhD SRD Nutrition Scientist British Nutrition Foundation 52ndash54 High Holborn London WC1V 6RQ UK E-mail sschenkernutritionorguk
The British Nutrition Foundation is registered as a company limited by Guarantee No 898651 Registered Charity No 251681 VAT No 381 7380 37
BRIEFING PAPER
Undernutrition in the UK
Sarah Schenker
British Nutrition Foundation London UK
SUMMARY1 INTRODUCTION2 DEFINITION AND CLASSIFICATION OF UNDERNUTRITION3 CAUSES OF UNDERNUTRITION
31 Causes in the community32 Effect of disease on nutritional status33 Reaching hospital
4 EXTENT OF THE PROBLEM OF UNDERNUTRITION5 COST OF THE PROBLEM OF UNDERNUTRITION6 WHY THE PROBLEM OF UNDERNUTRITION IS EXACERBATED IN HOSPITALS
61 Hospital food and feeding62 Drugndashnutrient interactions
7 WHAT CAN AND IS BEING DONE
71 Changes within the NHS72 Improvements in hospital food73 Improvements in the provision of hospital food74 Improvements in the nutrition education of health professionals and care workers75 Community initiatives
8 SCREENING FOR UNDERNUTRITION
81 Nutritional screening and assessment of patients in hospitals82 Measurement of nutritional status83 Body composition84 Biochemical assessment85 Functional assessment86 Nutritional screening and assessment of patients in the community87 Recommendations
9 SPECIALISED FEEDING10 CONCLUSIONS
ACKNOWLEDGEMENTSREFERENCESAPPENDIX 1 USEFUL ADDRESSES AND WEBSITESAPPENDIX 2 SPECIALISED FEEDING
88
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Summary
There is a nutritional component to most illnesses (whether poor nutrition leads todisease or disease adversely affects nutritional status) and their treatment ofteninvolving all the health care professions Undernutrition can adversely affect everysystem of the body such as the muscular system (resulting in fatigue lethargy anddecreased peripheral and respiratory muscle strength) the immune system (predis-posing to and delaying recovery from infection) and psycho-social function (causinganxiety depression and self-neglect)
As a consequence undernutrition consumes a disproportionate amount of healthcare resources It is estimated that 70 of undernutrition in the UK goes unrecog-nised and untreated and that in the community 5 of the population have a bodymass index (BMI) less than 20 kgm
2
In hospitals this figure rises to 20ndash25 It isimportant to recognise that not all people with low BMI are undernourished somemay be perfectly healthy There are difficulties in defining undernutrition becausethe anthropometric measurements used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have been based on healthy young indi-viduals and are applied to the whole population However the three key elementsthat help define undernutrition or risk of undernutrition are assessment of chronicprotein-energy status history of weight loss and underlying risk factors includingdisease and disabilities
Patients may be malnourished on admission to hospital as a result of a variety ofdisease-related social or psychological factors Mental illnesses such as depressionand dementia cause anorexia Malignancy and acute or chronic physical diseasereduce appetite and alter the taste smell and preferences for different types of foodInfections and malignant disease may also increase nutritional requirements Neu-rological and mechanical impairment of swallowing and diseases of the gastrointes-tinal tract affect nutritional intake Factors such as social isolation and poverty canplay an important role and disability and immobility can interfere with food pur-chase and preparation Taste appreciation also alters with ageing
It is reported that 40 of all patients admitted to hospitals are undernourishedhalf of them severely so Nutritional status tends to worsen during hospital stay andis associated with a worse outcome of the disease and prolonged hospital stay Stud-ies have shown that 40 of hospital food is wasted which results in patients receiv-ing only 70 of their energy and protein requirements Because many patients aredischarged from hospital in a worse nutritional state than they entered a furthergroup of undernourished individuals are discharged into the community setting upa vicious circle This can largely be prevented or treated with appropriate screeningand management
Weight loss often continues in many patients during their hospital stay for manyreasons These include surgical treatments and investigations that impair appetite orthe ability to eat (while increasing nutritional requirements) or treatments and pro-cedures that require a period of nil-by-mouth beforehand which reduces intakeFrustratingly sometimes a patient may be nil-by-mouth all morning only to havethe treatment delayed or postponed to a later date Often when the patient returnsto the ward no meal has been saved for them (due to lack of communication or lack
Undernutrition in the UK
89
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
of suitable facilities to store it if it was hot) and there may be no other food availableto them
A major contributor to the worsening nutritional status during hospitalisationhowever is the inadequacy of current catering and feeding practices Hospital cater-ing is beset with all sorts of seemingly trivial problems that add up to one hugeproblem For example the wrong food may arrive for a patient because they werenot able to choose it themselves or they have been given a meal chosen by somebodyelse occupying the bed before them The meal that does come is difficult to eat
eg
the provision of individual butter packs that are difficult for frail arthritic fingers toopen
Although special techniques of enteral and parenteral nutrition support are indi-cated for a minority of patients with failure of swallowing or gastrointestinal func-tion the majority of patients are dependent on hospital food to sustain them duringillness In many hospitals the three meals provided may be of a reasonable standardas the catering officers struggle on the tight budget they have but the range andquality of the snacks (essential to meet increased requirements in many patients) letthem down In many cases proprietary oral supplements or sip feeds may be ofvalue but they should not become a convenient substitute for adequate and appro-priate food provision
Hospital menus and meals should provide sufficient choice to offer healthy bal-anced appetising nutrition for all patients Menus should be designed to meet theneeds of particular patient groups
eg
elderly people children and ethnic minori-ties Adequate choice should be available to meet these needs Special attentionshould be given to the requirements of sick and nutritionally vulnerable patientsand appropriate special therapeutic diets for those who need them should be pro-vided A range of meals specially fortified in energy and protein should also be avail-able in every hospital and snacks and nourishing drinks should be kept in the wardand routinely offered between meals The timing of meals should be reviewed andmade more relevant to patientsrsquo customary meal patterns All methods of food prep-aration
eg
in-house cook-serve or brought-in cook-chill (with ward regeneration)have proved successful but each is highly dependent on the method of distributionand serving With proper management a bulk trolley bedside service servespatientsrsquo needs best Nutritionally vulnerable patients should be placed in wardswith kitchen areas or near ward kitchens so that special meals or snacks can beprepared for them or when possible patients can access the kitchen themselves Theprimary responsibility of the nutritional care of in-patients rests with the nurses incharge of the ward therefore food should be served by nurses supported wherenecessary by other grades of staff trained for this purpose
eg
ward hostesses diettechnicianshelpers Assistance with eating must be provided where necessary Plateor tray collection should be supervised by nursing staff to enable patientsrsquo foodintake to be monitored
Many studies have shown the benefits of nutritional intervention Therefore thepresence of disease whether in hospital or the community should be seen as anindication of the need for nutritional screening to identify those at particular riskand those who might benefit from some form of nutritional intervention In which
90
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
1 Introduction
Serious attention to the problem of undernutrition inhospitals was first given in 1992 with the publication ofthe Kingrsquos Fund report
A Positive Approach to Nutri-tion as Treatment
(Kingrsquos Fund 1992) The report statedthat 66 of all hospital patients were malnourished andcited evidence that undernutrition in hospital patientshad both clinical and financial implications The organ-isation of food and nutrition services in hospitals wasreviewed and a number of recommendations forimproving care were made
Two years later McWhirter amp Pennington (1994)showed that 40 of adults admitted to hospital hadsome degree of undernutrition and in half of them thiswas severe Patients continued to lose weight duringtheir time in hospital yet only 5 were referred for die-tetic help Those who did receive dietetic support gainedweight proving that once identified the problem couldbe treated McWhirter amp Pennington identified a num-ber of contributing factors to the widespread existenceof undernutrition Most importantly they showed thefailure of nurses and doctors to identify patients at riskand to recognise obvious signs and symptoms of under-nutrition There was often no reference in the medicalnotes to the nutritional status of the patient on admis-sion and 23 of patients were not weighed on admis-sion and throughout their stay Also no mention wasmade of the patientrsquos appetite or food intake
Following the publication of the Kingrsquos Fund report anumber of reports have produced recommendationsspecifically addressing the management of food andnutrition in hospitals (Bond 1997 Burke 1997) Thesecover such issues as staff roles and responsibilities train-ing standards for hospital food and the identificationand assessment of undernutrition The latest tworeports
Managing Nutrition in Hospital A Recipe forQuality
(Nuffield Trust 1999) and
Hospital Food asTreatment
(BAPEN 1999) are in almost complete agree-ment as to causes and consequences of undernutrition inhospitals and their subsequent recommendations forimproving the current situation (see Section 7)
Despite an increased awareness and widespread dis-cussion of the issue there is little evidence of generalimprovement in practice either in the provision andorganisation of nutrition care or in the prevalence ofundernutrition among patients The Nuffield Trust(1999) and BAPEN (1999) reports highlighted the con-tinued confusion of roles and responsibilities over nutri-tional care a lack of enforcement of existing guidelinesand a lack of status awarded to the whole area of foodand nutrition in hospitals
The functional clinical and economic consequencesof undernutrition have been well reviewed and demon-strated repeatedly They include impaired mental andphysical function greater risk of death increased com-plication rates during illness and following surgery anddelayed recovery with prolonged convalescence and
case implementing measures such as improved staff training nutritional screeningand assessment and monitoring combined with better catering practices will resultin most patientsrsquo nutritional requirements being met Fortified meals between-mealsnacks and adequate ward staffing have all been shown to contribute to achievingthis goal which leads to better clinical outcome less waste a shorter hospital stayand a more cost-effective service
Recently a number of schemes and initiatives have been set up to help prevent orcombat malnutrition both in hospitals and the community These include the launchof
Better Hospital Food a new menu for the National Health Service
and the estab-lishment of the Malnutrition Advisory Group a group of experts convened to raiseawareness and understanding of issues of undernutrition Community initiativesinclude the establishment of the Neighbourhood Renewal Unit for deprived neigh-bourhoods Sure Start ndash set up to operate local programmes for children and parentsliving in areas of high poverty and Healthy Living Centres ndash set up to run schemessuch as luncheon clubs for older people
Undernutrition in the UK
91
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
hospital stay In some patients undernutrition may bethe main condition that precipitates hospital admissionTrials of nutritional intervention by oral or artificialmeans have shown that in many patients the clinicalconsequences of undernutrition can be avoided orreversed by appropriate nutritional care (Beier-Holgersen amp Boesby 1996 Keele
et al
1995 Larsson
et al
1990 Rana
et al
1992)
2 Definition and classification of undernutrition
Undernutrition can be defined as a disturbance of formor function arising from the deficiency of one or morenutrients Undernutrition can be mild or severe helpful(if it results in appropriate weight loss in someone whois obese) or dangerous Weight loss is a manifestation ofenergy depletion The least essential tissues suffer firstthe adipose tissue cells lose fat which is oxidised to pro-vide energy Essential nutrients protein and micronutri-ents are likely to be depleted at the same time The bodystores of some micronutrients are large while require-ments for others are lower when energy intake isreduced In children who have relatively higher proteinrequirements than adults serious depletion of proteinaccompanies undernutrition
The consequences of protein depletion are apparent intwo main ways somatic protein depletion ndash the loss oftissue as general wasting of muscles and visceral proteindepletion ndash protein loss from the liver pancreas and gutWhen protein is lost from skeletal muscle the musclefibres shrink and the spaces between them are filled withan extracellular watery gel In older people some of theexcess fluid collects in the legs during the day as oedemaIf the loss is not too severe the oedema will disappearwhen the person lies down
In undernutrition the skeleton retains its outward sizeand shape but the fatty marrow disappears and isreplaced with aqueous material The skin loses proteinand becomes easily infected this with the loss of sub-cutaneous fat gives it a loose hanging appearance Theinternal organs particularly the liver lose mass Theheart and kidneys tend to lose mass in parallel withthe rest of the body but the brain retains its size andstructure The gut becomes thin and weight is lost fromboth muscle and mucosa
In spite of these structural changes organ functionand body systems remain normal until a great deal ofweight has been lost The resting metabolic rate per kilo-gram body weight is not greatly reduced in moderateundernutrition but in starvation both metabolic rateand body temperature fall Pulse rate and arterial blood
pressure are low in undernutrition as the body adaptsphysiologically In moderate undernutrition the gutfunctions normally provided there is no infection butin severe undernutrition diarrhoea can be severe (evenwithout infection) and the resulting dehydration canprove fatal
The presence of undernutrition in adults is assessed interms of degrees of weight loss An easy (but not thebest) index is body mass index (BMI) (see Section 833)defined as weight (in kilograms) divided by the square ofthe height (in metres)
ie
weightheight
2
Table 1 givesvalues for defining adult grades of undernutrition
The most sensitive indicator of undernutrition in chil-dren is failure to achieve normal growth compared witha lsquonormalrsquo reference growth rate for the age and sex ofthe child Progression of growth is an important param-eter and can be assessed in terms of height and weightor in infants weight and head circumference in relationto reference standards for age New reference standards(Freeman
et al
1995) have been published to replacethose compiled in the 1950s which take into accountthe upward shift in the average weight and height ofchildren in recent decades However a number of diffi-culties are associated with the use of these data Firstlychildren who cross centiles but never actually reach thecut-off centile defining failure to thrive are not identi-fied For example infants considered large at birthmight fail to grow but because they do not reach thecut-off centile failure to thrive will not be diagnosedSecondly infancy is naturally a period of centile crossing(large for gestational age infants grow more slowly thanthose of small for gestational age) So identifying failureto thrive depends on being able to distinguish poorgrowth from natural changes in growth rate To addressthis problem Cole (1997) has developed a chart thatcan be used to detect growth faltering over any period of4 weeks or longer
Table 1
Classification of undernutrition in adults by body mass index (BMI)
BMI (kgm
2
) Classification
gt
20 Normal185ndash20 Marginal undernutrition17ndash185 Mild undernutrition16ndash17 Moderate undernutrition
lt
16 Severe undernutrition
92
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
3 Causes of undernutrition
Undernutrition is the consequence of a dietary intakethat does not meet nutritional needs and may resultfrom one or more of the following decreased dietaryintake increased nutritional requirementslossesimpaired ability to absorb or utilise nutrients
Undernutrition usually has a slow onset resultingfrom periods of weeks or months when intake has notmatched requirements However in conditions of acutemetabolic stress where nutritional demands are highutilisation of energy and nutrients are disturbed andoral intake is likely to be compromised nutritionaldepletion can occur rapidly and be severe
Many factors can impair dietary intake Theseinclude
bull difficulties with shopping (both access and affordabil-ity) andor preparing cooking or eating food resultingfrom illness lack of mobility or povertybull reduced appetite as a result of the effects of illness orassociated anxiety or depressionbull symptoms associated with a disease or its treatment
eg
nausea vomiting sore mouth abdominal discom-fort or diarrhoeabull lack of interest in food as a result of social isolationsignificant life change (such as bereavement) or mentalillnessbull inadequate or unappetising meals or the provision ofinappropriate foodbull repeated fasting for diagnostic or treatmentproceduresbull problems associated with skipping mealsbull difficulties with eating or chewing
eg
ill-fitting den-tures or poor oral hygiene
bull swallowing difficultiesbull difficulty with self-feeding (
eg
owing to disability ordisorders such as Parkinsonrsquos disease) or inadequatehelp given to those unable to self-feedbull sedation semiconsciousness or coma
These factors can be separated into effects of lifestyleand effects of disease and consequent treatment and areexplored in greater detail below
31 Causes in the community
In this briefing paper causes in the community are con-fined to those undernourished individuals who mayhave previously been patients in hospital and have beendischarged while undernourished or people with onsetof a disease that has yet to be diagnosed or treated andwill enter hospital in due course
311 Poverty
One in four of the UK population nearly 14 millionpeople live in households with incomes below theEuropean poverty line of half the average incomeApproximately 96 million of these people are in house-holds that receive income support and the remainderlive on low or insecure wages Diets in low-incomehouseholds are characterised by less dietary varietywhich is itself associated with poorer nutrient profiles
National Food Survey results have consistently shownlower nutrient intakes in the lowest income groups com-pared to the highest In addition the Dietary and Nutri-tional Survey of British adults (Gregory
et al
1990)found that men and women who were unemployed orliving in households claiming benefit or in social classesIV and V had significantly lower intakes of many vita-mins (especially vitamin C
b
-carotene and vitamin E)and minerals (especially iron) than people not in thesecategories Data from the new NDNS of adults can befound on the FSA website (httpwwwfoodgovuk)
In the National Diet and Nutrition Survey (NDNS) ofyoung children (Gregory
et al
1995) those from man-ual social classes or from less-advantaged homes (wherethe head of the household was unemployed or claimedbenefits) had lower intakes andor blood levels of
b
-carotene niacin vitamin C iron calcium phosphorusand potassium than those from non-manual or more-advantaged households Preschool children from single-parent families had lower levels of
b
-carotene andvitamin C In the NDNS of young people (Gregory
et al
2000) those who received free school meals (and were
Key points
bull Moderate undernutrition leads to fat loss generalwasting of muscles and loss of protein from internalorgansbull Internal organs can function normally in moderateundernutrition but with severe undernutrition gutfunction breaks down causing malabsorption diar-rhoea and infection This can be fatalbull There are a number of methods for the assessmentof undernutrition BMI is routinely used in adultsand growth reference standards are used in children
Undernutrition in the UK
93
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
therefore from households in receipt of benefits) hadlower vitamin and mineral intakes (Buttriss 2002)
Similar findings have been reported from other large-scale surveys in the UK such as the Scottish HeartHealth Study in which the data were controlled forsmoking and education level (Bolton-Smith
et al
1991)and the 36-year follow-up to the National Birth CohortStudy (Braddon
et al
1988) The survey of nutrientintakes in Northern Ireland found similar nutrientdifferences by occupational social class (Barker
et al
1989) These findings are comparable with those fromsmaller surveys looking at nutrient intakes in differentsocioeconomic circumstances (Calvert
et al
1994Moynihan
et al
1993) including the homeless (Rushdenamp Wheeler 1993) A study by Dowler amp Calvert (1995)of nutrient intakes in lone-parent households showedthat where parents had lived for some time on incomesupport and particularly where they had fixed regulardeductions for debt recovery nutrient intakes were halfof the levels of those not living in such circumstances
In terms of dietary variety and overall dietary pat-terns those in poorer households consume less fruitjuice lean meat oily fish and wholemeal products andfewer salads and are more likely to eat white breadpotatoes cheaper fatty meats beans eggs and chips(Anderson amp Hunt 1992 Gregory
et al
1995Whichelow
et al
1991) Those on lower incomes have amuch less diverse food base so their diet is more likelyto lack variety
Many foods that are integral to a healthy diet are per-ceived as a luxury by those on low incomes and are anlsquoexpensiversquo form of energy such foods include fruitsvegetables and fish In addition many healthier alterna-tives carry a price premium
eg
wholemeal bread fatsand spreads low in saturates and lean meat However inaddition to price many factors influence the purchasingand consumption patterns in low-income householdswhich are related to their poor financial status such aslimited food preparation facilities Low income is alsooften associated with lack of knowledge and skillsrelated to food nutrition and cooking
Policies adopted by government local authorities andfood retailers can influence which foods are availableand accessible to people with low incomes For examplethere is the issue of price variability between shopsFood is generally more expensive in corner shops con-venience stores and small independent supermarketsthan in large supermarkets Piachaud amp Webb (1996)found that on average basic foodstuffs cost 24 morein small stores than in supermarkets taking super-market own brands into account the differences in costs
were 60 They calculated that people living in ahousehold on benefits would have to spend 25 moreof their income on food if they could not get to a largesupermarket or street market
Access to shopping facilities in areas where low-income households are concentrated is restricted interms of the physical difficulties or cost of travelling toshops and by a lack of choice of shops Thereforeaccess to a healthy diet becomes a particular problemfor low-income households The number of food retailoutlets is continually decreasing mainly at the expenseof shops such as small grocery retailers butchers fish-mongers and greengrocers The number of large retailoutlets has also decreased mainly because of theincrease in the number of superstores located on the out-skirts of towns and designed for access primarily by carEconomies of scale allow food sold in supermarkets tobe cheaper and cover a wider range than that in smallerhigh street stores The 1998 Independent Inquiry intoInequalities in Health report (Acheson 1998) foundparadoxically that a basket of food cost more in dis-advantaged areas than in affluent areas
The price of a healthy diet and the variation betweenprices of some foods is therefore of major concern forthose living on low incomes Many of the poorest peoplein the UK are concentrated in local authority housing ininner cities and there is evidence to suggest a continuinggeographical polarisation of income inequalities Inmany of these areas shops and banks have withdrawnpartly because the residents spend so little and partlybecause of the retail concentration in superstores(defined as having a total floor surface area of more than7620 m
2
) designed primarily for car access The risein vandalism is another contributing factor In a bidto resolve these problems the supermarket chainSomerfield operates a policy of maintaining small- andmedium-sized high street shops to serve local commu-nities and not to build large out-of town superstoresMany deprived sectors of society suffer from a lack ofaccess to good shopping facilities and in particularfresh fruit and vegetables To avoid these lsquofresh fooddesertsrsquo Somerfield opted to offer a free delivery serviceto village shops and small local stores Unfortunatelythe company had to close some of these small stores insome areas due to vandalism
312 Social and physical factors
Some of the social factors that influence food choice andeating patterns are listed below
94
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Figure 1
Guidelines for estimating the approximate energy and nitrogen requirements for an adult patient receiving artificial nutritional support Reproduced from Garrow
et al
2000 Reproduced with permission from Elsevier
bull Budgeting skillsbull Cultural traditionsbull Religious beliefsbull Educationbull Nutritional knowledgebull Lack of cooking facilities
eg
families housed in bed-and-breakfast accommodationbull Habitsbull Likes and dislikesbull Previous food experiencebull Willingness to experimentbull Time availablebull Eating alonebull Depressionbull Bereavement
For example a recently widowed man may not only besuffering the effects of bereavement and depressionwhich are likely to reduce appetite but he may also sud-denly find himself having to cope alone If his wife hadalways been responsible for shopping cooking and pro-viding food the widower may have difficulty budgetingfor food preparing and cooking food and may find thenew experience of eating alone all too painful
Poor dentition is another factor The NDNS of peopleaged 65 years and over (Finch
et al
1998) reported thatpeople with no natural teeth or few natural teeth ate amore restricted range of foods influenced by their per-ceived inability to chew The survey showed an associ-ation between oral function and nutrient intake andnutritional status Subjects without their own teeth wereless likely to choose foods that need chewing such asfruit and vegetables had lower intakes of iron vitaminsC and E and retinol and had lower plasma levels of vita-min C This was particularly true of those who lived invarious forms of residential care Physical disabilitiesalso influence a personrsquos ability to shop prepare andcook food Something as simple as opening a can ofbaked beans is far from simple for someone witharthritic hands
32 Effect of disease on nutritional status
321 The nutritional requirements of illness
Tissue repair imposes demands on nutritional supplyand an increased activity of body defence mechanismsmay also increase nutritional needs Despite this illhealth is often associated with a decreased desire forfood and decreased nutritional intake
Various changes in the metabolism of carbohydratefat and protein can be observed in illness Proportionalto the severity of illness there is an increase in the bodyrsquosenergy requirement and also an increase in urinarynitrogen loss (Cuthbertson 1980) The scale of thesechanges can be seen in Fig 1 This response to illnesshas been termed a stress response and the state ofincreased energy and protein needs a hypermetabolicstate
The metabolic response to illness traditionally hasthree phases ebb flow and anabolic although these canbe moderated with drug treatment The ebb phase onlylasts for a few hours and there is a depression of meta-bolic function and a reduction in energy expenditure In
Undernutrition in the UK
95
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
the flow phase metabolic rate increases and energyreserves in the form of fat stores are mobilised Visceraland muscle tissue provide amino acids that can be usedfor gluconeogenesis providing glucose for the brain andred blood cells and for wound-healing mechanismsHormonal changes appear to be important determinantsof the stress response Simply stated insulin stimulatesglucose uptake and metabolism and glycogen fat andprotein synthesis During starvation insulin levels arelow and other hormones are effective in mobilisingbody stores (
ie
promote glycogen fat and proteinbreakdown and stimulate gluconeogenesis and ketoge-nesis) In the stress response there is an increased secre-tion of catabolic hormones Especially important arethe glucocorticoids catecholamines and glucagon Theactions of insulin seem to be opposed by the catabolichormones leading to a state of insulin resistance(Cuthbertson 1980)
Another fundamental event is the production of themediator interleukin-1 a polypeptide produced byphagocytic cells (white blood cells that help fight infec-tion) A number of direct effects collectively termed theacute-phase response are ascribed to interleukin-1These include fever which is one of the strategies thebody uses to fight infection and the induction of muscleprotein breakdown leading to increased blood levels ofthe acute-phase proteins prealbumin retinol-bindingprotein (RBP) and C-reactive protein (Casati
et al
1998)
In simple starvation the breakdown of body fat isreversed by feeding with glucose In the hypermetabolicpatient it is found that fat breakdown continues despitegiving glucose and that gluconeogenesis and glucoseoxidation also occur at increased rates Hence theincreased gluconeogenesis can increase the amount ofcarbohydrate that is required to obviate protein break-down Achievement of energy balance fails to alleviatecatabolism in critically ill patients Therefore provisionof energy intake to match energy expenditure is unnec-essary during the flow phase and may even be unhelpful(Frankenfield
et al
1997)The increased nitrogen loss observed in stressed
patients can be accounted for by both a depression ofprotein synthesis and an increase in the rate of proteinbreakdown Provision of adequate protein stimulatesprotein synthesis but it also stimulates breakdown(Campbell 1999)
In the anabolic phase catabolism eventually declinesand is coupled with an increase in appetite and ability tomove This phase provides the opportunity for nutri-tional therapy to restore muscle mass and increase pro-tein synthesis
33 Reaching hospital
On reaching hospital dietary intake may be furtherreduced by one or more of the following problems
bull Confusionbull Fearbull Depressionbull Dysphagia (inability or reduced ability to swallow)bull Loss of appetite taste smell or thirstbull Poor dentitionbull Constipation which is caused by reduced mobilityand the fear that eating will make it worsebull Discomfortbull Dislike of the type of food availablebull Difference in routine and meal patternbull Problems with feedingbull Lack of staff available to help with feeding
Key points
Factors influencing poor dietary intake includebull loss of appetitebull disease or recurrent illness and consequenttreatmentbull impaired ability to absorb or utilise nutrientsbull poverty resulting in lack of car ownership or alter-native transport leading to limited access to bulk buy-ing low-cost foodbull poor housing with poor food storage and prepara-tion facilitiesbull problems of shopping and lack of preparation andcooking skillsbull less education leading to less knowledge and moti-vation to make healthy diet choicesbull unemployment so there is less money available forexpenditure on foodbull social isolation depression and bereavement lowself-esteem
4 Extent of the problem of undernutrition
Undernutrition among patients in UK hospitals wasdocumented in the mid-1970s (Bistrian
et al
1974 Hill
et al
1977) and it remains a common and often unrec-ognised problem that contributes to patient morbidityand mortality (Lennard-Jones 1992 McWhirter ampPennington 1994 Potter
et al
1998)
96
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Many studies over the last 30 years have since empha-sised the presence of disease-related undernutrition inhospitalised patients (Bistrian
et al
1974 Corish
et al
2000 Hill
et al
1977 Kelly
et al
2000 McWhirter ampPennington 1994) However there is controversy aboutits exact prevalence in the hospital setting One of themajor reasons for this is that there is no universal agree-ment about the definition of undernutrition Becausevarious workers have used different criteria to screen forundernutrition the reported magnitude of the problemhas been highly variable ranging from 10 to 60
Corish
et al
(2000) have screened for undernutritionin patients admitted to two teaching hospitals in DublinTo ensure more reliable comparisons they used thesame criteria employed by McWhirter amp Pennington(1994) in a Dundee hospital 6 years earlier In both stud-ies patients were classified as undernourished if theyhad a BMI
lt
20 kgm
2
and a triceps skinfold thicknessor mid-arm muscle circumference (MAMC) below the15th percentile The incidence of undernutrition innewly admitted patients in Dublin was reported to bemore than threefold lower (11) than in Dundee(40)
This striking difference has led other experts in thefield to question the criteria for defining undernutritionElia amp Stratton (2000) suggest that anthropometric cut-off values should not be used as a diagnostic label ofundernutrition but rather to classify an individualrsquosrisk of undernutrition Some healthy subjects have aBMI
lt
20 kgm2 (especially young adults) and are per-fectly well In addition anthropometric criteria alonesuggest a chronic protein-energy deficiency status How-ever a patient showing substantial recent weight loss(eg greater than 10 weight loss over 3ndash6 months) isat risk of undernutrition and impaired bodily functionseven though the anthropometric cut-off values may nothave been reached
The standard data used for anthropometry requireregular review so that they achieve the right balancebetween reflecting what is the norm (which may not bedesirable) and what is desirable (which may not beappropriate to the current generation) Unlike BMIwhich is a fixed criterion percentile values can showsubstantial change over time For example the referencevalues provided by Bishop et al (1981) for arm anthro-pometry were established in the USA about 30 yearsago The secular trends in obesity over that period meanthat these reference values may no longer apply Fur-thermore the choice of the percentile cut-off for use aspart of the screening tool to classify patients as under-nourished may be inappropriately high (since 15 ofthe reference population falls below this cut-off)
While the picture may be incomplete with regard tothe prevalence of undernutrition in hospitals it is clearthat disease-related undernutrition remains a significantclinical problem in hospitals
However the problem of disease-related undernutri-tion is not confined to people in hospital Within thecommunity up to 10 of people with cancer or otherchronic diseases may be significantly malnourished(Edington et al 1996) and many elderly people are alsoat high risk of undernutrition As a result people arecommonly admitted to hospital nutritionally depletedIn a study conducted in four hospitals in EnglandEdington et al (2000) found that one in every fivepatients admitted was malnourished Patients wereassessed using anthropometric measurements and BMIand by recording history of unintentional weight lossThis figure is likely to be an underestimate because it didnot include those who were too ill on admission to beassessed Kelly et al (2000) estimated that undernutri-tion among acute hospital admissions goes unrecognisedin 70 of cases
Once in hospital undernutrition is likely to get worseIn the study by McWhirter and Pennington two-thirdsof the 500 patients who had been assessed on admis-sion and were reassessed on discharge had lost weightA study on a random sample of 150 in-patients foundapproximately half of them to be either at moderate riskor high risk of undernutrition (Reilly et al 1995) Theprevalence and level of risk is probably higher amonghigh dependency medical surgical geriatric and paedi-atric patients (Reilly et al 1995) As illness and hospi-talisation are frequently associated with weight lossdeterioration in nutritional status is inevitable unlessaction is taken to prevent it
Key points
bull It is estimated that 70 of all undernutrition in theUK goes unrecognised and untreatedbull In the community 5 of the population have aBMI lt 20 kgm2 In hospitals this figure is 20ndash25bull It is estimated that 40 of adults and 15 of chil-dren admitted to hospital are malnourished half ofthese severely so and many others become malnour-ished during their stay in hospitalbull It is estimated that at any one time approximately66 of hospital patients are malnourished
Undernutrition in the UK 97
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
5 Cost of the problem of undernutrition
Undernutrition primarily results in loss of body tissue(depletion of body fat stores and muscle wasting) How-ever because nutrient intake is so closely correlatedwith energy intake a deficiency of energy is likely toresult in an inadequate intake of protein vitamins min-erals and trace elements This can cause widespreadmetabolic physiological and functional effects whichmay include
bull Impaired immune function and hence increased sus-ceptibility to infection and sepsis Infection will furtherimpair a malnourished statebull Delayed wound healingbull Increased risk of pressure sores particularly due toloss of cushioning fat storesbull Muscle wasting and weakness which may affect
ndash Respiratory function impaired respiratory musclestrength makes it difficult for a patient to cough andexpectorate effectively so increasing the risk of chestinfection It may also be more difficult to wean apatient off a ventilatorndash Cardiac function this may be impaired resulting inreduced cardiac output and risk of heart failurendash Mobility weakness of skeletal muscles delays areturn to full mobility Reduced mobility increases therisk of thromboembolism and bedsores
bull Altered structure of the small intestine which mayresult in malabsorptionbull Increased risk of postoperative complicationsbull Apathy and depression leading to loss of morale andreduced will to recoverbull General sense of weakness and illness which impairsappetite and physical ability to eat and hence tends toperpetuate and worsen any undernutrition
In summary undernutrition causes considerable mor-bidity delays recovery and increases the risk of death ABMI at or below the 15th percentile has been shown tobe a significant and independent predictor of death inseriously ill patients (Galanos et al 1997) There is alsoan economic cost in terms of increased need of nursingcare and extended hospital stay
There is clear evidence that correcting undernutritionhas many benefits (Potter et al 1998) Improvements inbody weight status and anthropometric parameters areassociated with improvement in immune function(Chandra 1992 Dionigi et al 1988) wound healing(Haydock amp Hill 1987) and muscle function (Fiataroneamp Evans 1993) and in clinical outcomes such asrecovery time and incidence of postoperativecomplications
Hospitals spend approximately pound15 billion on foodannually and studies conducted in one hospital foundthat 30ndash40 of food is discarded (Kelly 1999) This isconsistent with national estimates that 30ndash50 of hos-pital food is wasted with a monetary value calculated tobe pound45 million each year (Edwards amp Nash 1997Fenton et al 1995) With the inclusion of labour andoverheads this cost rises to pound144 million annuallyThere is also the hidden cost of the extra ill health asso-ciated with undernutrition Some hospitals also typicallyspend approximately pound800 000 on enteral andparenteral nutrition (see Sections 92 and 93) TheKingrsquos Fund (1992) report calculated that provision ofcomprehensive nutrition support would result in a 5-day reduction in hospital stay for approximately 10of patients The consequent saving was estimated to bepound266 million annually in the UK A review conducted byBond (1997) in the USA showed a clear relationshipbetween undernutrition and prolonged hospital stayWhen nutritional intervention was introduced 2 daysearlier than usual the result was a 1-day shortening ofhospital stay It was calculated that a more aggressivenutritional intervention policy would save the averagehospital $1 million per year
Key points
bull Between 30 and 50 of hospital food is wastedbull On average food intake is less than 75 of thatrecommended particularly among the elderlybull The monetary value of hospital food wasted eachyear in England alone is calculated to be pound45 millionBy including labour and overheads this cost rises topound144 millionbull There is also the hidden cost of the extra ill healthassociated with undernutrition because it increasesthe risk of complications lowers resistance to infec-tion impairs physical and mental functioning anddelays recovery
6 Why the problem of undernutrition is exacerbated in hospitals
In more than 60 of patients nutritional status deteri-orates during their stay in hospital with those whoare malnourished on admission particularly affectedPennington (1998) demonstrated that progressive nutri-tional depletion occurs for up to 8 weeks after curativesurgery (eg a heart by-pass operation) This thereforeindicates the need to consider nutritional status fromonset of illness through to complete recovery including
98 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
time after discharge However undernutrition remainsundetected in the majority of patients affected becausemany clinicians and nurses still do not consider nutri-tion to be an important factor in the management of dis-ease (Schenker 2000) and so do not routinely monitornutritional status and body weight Economic analysishas demonstrated that appropriate nutritional treatmentis cost-effective but benefits will only be achieved withhigh standards of nutritional care Multi-professionalnutritional support teams best conduct such treatmentbut there is continuing evidence of poor practice anda high incidence of treatment-related complicationswhich negate the benefits of nutritional treatments(Schenker 2000) In the hospital or institutional settingtherefore the problems that cause undernutrition maybe compounded by the fact that nutritional consider-ations may receive little attention from medical andnursing staff Lack of awareness of the prognostic sig-nificance of undernutrition and lack of knowledgeamong doctors and nurses regarding its assessment andmanagement (Nightingale amp Reeves 1999) may meanthat it is neither looked for nor taken into account whentreatment priorities are being set In particular theremay be failure to
bull identify those with or at risk of nutritional depletionbull identify nutritional requirements especially whenthese are increased because of fever surgery or injurybull provide food of an appropriate quality compositionand consistencybull encourage food intake food is of no benefit if noteatenbull monitor what is actually consumed in some circum-stances direct observation of food and fluid consump-tion is essentialbull identify those whose nutritional needs are not beingmet (through regular weighing or the use of otheranthropometric measurements)bull correct inadequate intake
61 Hospital food and feeding
The following factors have been identified as causes forpoor dietary intake in hospital patients
611 Problems with ordering
bull Menus lack clarity dishes should be described accu-rately so that patients have a reasonable idea of what toexpectbull Help with ordering should be available (but in manycases is not) where there are problems with a patientrsquoscomprehension speech or language
bull Menus are often not printed in languages other thanEnglish This is a particular problem in areas with a highimmigrant population Illiteracy may limit usefulness oftranslated menus Verbal translation may be betterbull Ordering from the menu too far in advance A patientmay be discharged after they have ordered food for thenext day resulting in the bedrsquos new occupant receivingfood chosen by someone else which may be unsuitableSame day ordering systems reduce waste and encourageconsumptionbull Patientsrsquo orders are not checked to ensure that thefood received and the portions requested are correct Inthis respect ward hostesses or feeding care attendantsmay be helpful however this does have financialimplicationsbull Inefficient ordering systems and poor two-way com-munication between the wards and the catering depart-ment lead to waste eg food sent to patients who havebeen discharged transferred or have died Such trays arethen either wasted or given to another patient wholeaves most of it because it was not their choice
612 Menu choice
bull Menus do not always take account of the needs tastesand customary eating habits of different groups ofpatients These will vary according to age race or cul-ture or the disease processbull Menus often do not take account of those needingfortified andor modified-consistency mealsbull Inappropriate promotion of lsquohealthy eatingrsquo eglow-fat diets in undernourished or nutritionally at-riskpatientsbull Some elderly patients often adopt a grazing habit andrequire frequent small volume high energy densityfeeds and snacksbull Special needs Although some disease-specific menuseg for renal failure may be provided from a dietkitchen it may be cost-effective to be able to supplementthe standard menu with high-energy high-proteinadditionsbull Nutritional needs and appetites of children differfrom those of adults and also vary according to ageMeals should be made attractive to children
613 Appropriate food choices
bull Food suitable for lsquohealthy eatingrsquo by the overweightpatient with cardiovascular disease is inappropriate forthe depleted malnourished patientbull Pureacuteed or semisolid diets are required by patientswith neurological or mechanical dysphagia who may be
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients
88
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Summary
There is a nutritional component to most illnesses (whether poor nutrition leads todisease or disease adversely affects nutritional status) and their treatment ofteninvolving all the health care professions Undernutrition can adversely affect everysystem of the body such as the muscular system (resulting in fatigue lethargy anddecreased peripheral and respiratory muscle strength) the immune system (predis-posing to and delaying recovery from infection) and psycho-social function (causinganxiety depression and self-neglect)
As a consequence undernutrition consumes a disproportionate amount of healthcare resources It is estimated that 70 of undernutrition in the UK goes unrecog-nised and untreated and that in the community 5 of the population have a bodymass index (BMI) less than 20 kgm
2
In hospitals this figure rises to 20ndash25 It isimportant to recognise that not all people with low BMI are undernourished somemay be perfectly healthy There are difficulties in defining undernutrition becausethe anthropometric measurements used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have been based on healthy young indi-viduals and are applied to the whole population However the three key elementsthat help define undernutrition or risk of undernutrition are assessment of chronicprotein-energy status history of weight loss and underlying risk factors includingdisease and disabilities
Patients may be malnourished on admission to hospital as a result of a variety ofdisease-related social or psychological factors Mental illnesses such as depressionand dementia cause anorexia Malignancy and acute or chronic physical diseasereduce appetite and alter the taste smell and preferences for different types of foodInfections and malignant disease may also increase nutritional requirements Neu-rological and mechanical impairment of swallowing and diseases of the gastrointes-tinal tract affect nutritional intake Factors such as social isolation and poverty canplay an important role and disability and immobility can interfere with food pur-chase and preparation Taste appreciation also alters with ageing
It is reported that 40 of all patients admitted to hospitals are undernourishedhalf of them severely so Nutritional status tends to worsen during hospital stay andis associated with a worse outcome of the disease and prolonged hospital stay Stud-ies have shown that 40 of hospital food is wasted which results in patients receiv-ing only 70 of their energy and protein requirements Because many patients aredischarged from hospital in a worse nutritional state than they entered a furthergroup of undernourished individuals are discharged into the community setting upa vicious circle This can largely be prevented or treated with appropriate screeningand management
Weight loss often continues in many patients during their hospital stay for manyreasons These include surgical treatments and investigations that impair appetite orthe ability to eat (while increasing nutritional requirements) or treatments and pro-cedures that require a period of nil-by-mouth beforehand which reduces intakeFrustratingly sometimes a patient may be nil-by-mouth all morning only to havethe treatment delayed or postponed to a later date Often when the patient returnsto the ward no meal has been saved for them (due to lack of communication or lack
Undernutrition in the UK
89
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
of suitable facilities to store it if it was hot) and there may be no other food availableto them
A major contributor to the worsening nutritional status during hospitalisationhowever is the inadequacy of current catering and feeding practices Hospital cater-ing is beset with all sorts of seemingly trivial problems that add up to one hugeproblem For example the wrong food may arrive for a patient because they werenot able to choose it themselves or they have been given a meal chosen by somebodyelse occupying the bed before them The meal that does come is difficult to eat
eg
the provision of individual butter packs that are difficult for frail arthritic fingers toopen
Although special techniques of enteral and parenteral nutrition support are indi-cated for a minority of patients with failure of swallowing or gastrointestinal func-tion the majority of patients are dependent on hospital food to sustain them duringillness In many hospitals the three meals provided may be of a reasonable standardas the catering officers struggle on the tight budget they have but the range andquality of the snacks (essential to meet increased requirements in many patients) letthem down In many cases proprietary oral supplements or sip feeds may be ofvalue but they should not become a convenient substitute for adequate and appro-priate food provision
Hospital menus and meals should provide sufficient choice to offer healthy bal-anced appetising nutrition for all patients Menus should be designed to meet theneeds of particular patient groups
eg
elderly people children and ethnic minori-ties Adequate choice should be available to meet these needs Special attentionshould be given to the requirements of sick and nutritionally vulnerable patientsand appropriate special therapeutic diets for those who need them should be pro-vided A range of meals specially fortified in energy and protein should also be avail-able in every hospital and snacks and nourishing drinks should be kept in the wardand routinely offered between meals The timing of meals should be reviewed andmade more relevant to patientsrsquo customary meal patterns All methods of food prep-aration
eg
in-house cook-serve or brought-in cook-chill (with ward regeneration)have proved successful but each is highly dependent on the method of distributionand serving With proper management a bulk trolley bedside service servespatientsrsquo needs best Nutritionally vulnerable patients should be placed in wardswith kitchen areas or near ward kitchens so that special meals or snacks can beprepared for them or when possible patients can access the kitchen themselves Theprimary responsibility of the nutritional care of in-patients rests with the nurses incharge of the ward therefore food should be served by nurses supported wherenecessary by other grades of staff trained for this purpose
eg
ward hostesses diettechnicianshelpers Assistance with eating must be provided where necessary Plateor tray collection should be supervised by nursing staff to enable patientsrsquo foodintake to be monitored
Many studies have shown the benefits of nutritional intervention Therefore thepresence of disease whether in hospital or the community should be seen as anindication of the need for nutritional screening to identify those at particular riskand those who might benefit from some form of nutritional intervention In which
90
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
1 Introduction
Serious attention to the problem of undernutrition inhospitals was first given in 1992 with the publication ofthe Kingrsquos Fund report
A Positive Approach to Nutri-tion as Treatment
(Kingrsquos Fund 1992) The report statedthat 66 of all hospital patients were malnourished andcited evidence that undernutrition in hospital patientshad both clinical and financial implications The organ-isation of food and nutrition services in hospitals wasreviewed and a number of recommendations forimproving care were made
Two years later McWhirter amp Pennington (1994)showed that 40 of adults admitted to hospital hadsome degree of undernutrition and in half of them thiswas severe Patients continued to lose weight duringtheir time in hospital yet only 5 were referred for die-tetic help Those who did receive dietetic support gainedweight proving that once identified the problem couldbe treated McWhirter amp Pennington identified a num-ber of contributing factors to the widespread existenceof undernutrition Most importantly they showed thefailure of nurses and doctors to identify patients at riskand to recognise obvious signs and symptoms of under-nutrition There was often no reference in the medicalnotes to the nutritional status of the patient on admis-sion and 23 of patients were not weighed on admis-sion and throughout their stay Also no mention wasmade of the patientrsquos appetite or food intake
Following the publication of the Kingrsquos Fund report anumber of reports have produced recommendationsspecifically addressing the management of food andnutrition in hospitals (Bond 1997 Burke 1997) Thesecover such issues as staff roles and responsibilities train-ing standards for hospital food and the identificationand assessment of undernutrition The latest tworeports
Managing Nutrition in Hospital A Recipe forQuality
(Nuffield Trust 1999) and
Hospital Food asTreatment
(BAPEN 1999) are in almost complete agree-ment as to causes and consequences of undernutrition inhospitals and their subsequent recommendations forimproving the current situation (see Section 7)
Despite an increased awareness and widespread dis-cussion of the issue there is little evidence of generalimprovement in practice either in the provision andorganisation of nutrition care or in the prevalence ofundernutrition among patients The Nuffield Trust(1999) and BAPEN (1999) reports highlighted the con-tinued confusion of roles and responsibilities over nutri-tional care a lack of enforcement of existing guidelinesand a lack of status awarded to the whole area of foodand nutrition in hospitals
The functional clinical and economic consequencesof undernutrition have been well reviewed and demon-strated repeatedly They include impaired mental andphysical function greater risk of death increased com-plication rates during illness and following surgery anddelayed recovery with prolonged convalescence and
case implementing measures such as improved staff training nutritional screeningand assessment and monitoring combined with better catering practices will resultin most patientsrsquo nutritional requirements being met Fortified meals between-mealsnacks and adequate ward staffing have all been shown to contribute to achievingthis goal which leads to better clinical outcome less waste a shorter hospital stayand a more cost-effective service
Recently a number of schemes and initiatives have been set up to help prevent orcombat malnutrition both in hospitals and the community These include the launchof
Better Hospital Food a new menu for the National Health Service
and the estab-lishment of the Malnutrition Advisory Group a group of experts convened to raiseawareness and understanding of issues of undernutrition Community initiativesinclude the establishment of the Neighbourhood Renewal Unit for deprived neigh-bourhoods Sure Start ndash set up to operate local programmes for children and parentsliving in areas of high poverty and Healthy Living Centres ndash set up to run schemessuch as luncheon clubs for older people
Undernutrition in the UK
91
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
hospital stay In some patients undernutrition may bethe main condition that precipitates hospital admissionTrials of nutritional intervention by oral or artificialmeans have shown that in many patients the clinicalconsequences of undernutrition can be avoided orreversed by appropriate nutritional care (Beier-Holgersen amp Boesby 1996 Keele
et al
1995 Larsson
et al
1990 Rana
et al
1992)
2 Definition and classification of undernutrition
Undernutrition can be defined as a disturbance of formor function arising from the deficiency of one or morenutrients Undernutrition can be mild or severe helpful(if it results in appropriate weight loss in someone whois obese) or dangerous Weight loss is a manifestation ofenergy depletion The least essential tissues suffer firstthe adipose tissue cells lose fat which is oxidised to pro-vide energy Essential nutrients protein and micronutri-ents are likely to be depleted at the same time The bodystores of some micronutrients are large while require-ments for others are lower when energy intake isreduced In children who have relatively higher proteinrequirements than adults serious depletion of proteinaccompanies undernutrition
The consequences of protein depletion are apparent intwo main ways somatic protein depletion ndash the loss oftissue as general wasting of muscles and visceral proteindepletion ndash protein loss from the liver pancreas and gutWhen protein is lost from skeletal muscle the musclefibres shrink and the spaces between them are filled withan extracellular watery gel In older people some of theexcess fluid collects in the legs during the day as oedemaIf the loss is not too severe the oedema will disappearwhen the person lies down
In undernutrition the skeleton retains its outward sizeand shape but the fatty marrow disappears and isreplaced with aqueous material The skin loses proteinand becomes easily infected this with the loss of sub-cutaneous fat gives it a loose hanging appearance Theinternal organs particularly the liver lose mass Theheart and kidneys tend to lose mass in parallel withthe rest of the body but the brain retains its size andstructure The gut becomes thin and weight is lost fromboth muscle and mucosa
In spite of these structural changes organ functionand body systems remain normal until a great deal ofweight has been lost The resting metabolic rate per kilo-gram body weight is not greatly reduced in moderateundernutrition but in starvation both metabolic rateand body temperature fall Pulse rate and arterial blood
pressure are low in undernutrition as the body adaptsphysiologically In moderate undernutrition the gutfunctions normally provided there is no infection butin severe undernutrition diarrhoea can be severe (evenwithout infection) and the resulting dehydration canprove fatal
The presence of undernutrition in adults is assessed interms of degrees of weight loss An easy (but not thebest) index is body mass index (BMI) (see Section 833)defined as weight (in kilograms) divided by the square ofthe height (in metres)
ie
weightheight
2
Table 1 givesvalues for defining adult grades of undernutrition
The most sensitive indicator of undernutrition in chil-dren is failure to achieve normal growth compared witha lsquonormalrsquo reference growth rate for the age and sex ofthe child Progression of growth is an important param-eter and can be assessed in terms of height and weightor in infants weight and head circumference in relationto reference standards for age New reference standards(Freeman
et al
1995) have been published to replacethose compiled in the 1950s which take into accountthe upward shift in the average weight and height ofchildren in recent decades However a number of diffi-culties are associated with the use of these data Firstlychildren who cross centiles but never actually reach thecut-off centile defining failure to thrive are not identi-fied For example infants considered large at birthmight fail to grow but because they do not reach thecut-off centile failure to thrive will not be diagnosedSecondly infancy is naturally a period of centile crossing(large for gestational age infants grow more slowly thanthose of small for gestational age) So identifying failureto thrive depends on being able to distinguish poorgrowth from natural changes in growth rate To addressthis problem Cole (1997) has developed a chart thatcan be used to detect growth faltering over any period of4 weeks or longer
Table 1
Classification of undernutrition in adults by body mass index (BMI)
BMI (kgm
2
) Classification
gt
20 Normal185ndash20 Marginal undernutrition17ndash185 Mild undernutrition16ndash17 Moderate undernutrition
lt
16 Severe undernutrition
92
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
3 Causes of undernutrition
Undernutrition is the consequence of a dietary intakethat does not meet nutritional needs and may resultfrom one or more of the following decreased dietaryintake increased nutritional requirementslossesimpaired ability to absorb or utilise nutrients
Undernutrition usually has a slow onset resultingfrom periods of weeks or months when intake has notmatched requirements However in conditions of acutemetabolic stress where nutritional demands are highutilisation of energy and nutrients are disturbed andoral intake is likely to be compromised nutritionaldepletion can occur rapidly and be severe
Many factors can impair dietary intake Theseinclude
bull difficulties with shopping (both access and affordabil-ity) andor preparing cooking or eating food resultingfrom illness lack of mobility or povertybull reduced appetite as a result of the effects of illness orassociated anxiety or depressionbull symptoms associated with a disease or its treatment
eg
nausea vomiting sore mouth abdominal discom-fort or diarrhoeabull lack of interest in food as a result of social isolationsignificant life change (such as bereavement) or mentalillnessbull inadequate or unappetising meals or the provision ofinappropriate foodbull repeated fasting for diagnostic or treatmentproceduresbull problems associated with skipping mealsbull difficulties with eating or chewing
eg
ill-fitting den-tures or poor oral hygiene
bull swallowing difficultiesbull difficulty with self-feeding (
eg
owing to disability ordisorders such as Parkinsonrsquos disease) or inadequatehelp given to those unable to self-feedbull sedation semiconsciousness or coma
These factors can be separated into effects of lifestyleand effects of disease and consequent treatment and areexplored in greater detail below
31 Causes in the community
In this briefing paper causes in the community are con-fined to those undernourished individuals who mayhave previously been patients in hospital and have beendischarged while undernourished or people with onsetof a disease that has yet to be diagnosed or treated andwill enter hospital in due course
311 Poverty
One in four of the UK population nearly 14 millionpeople live in households with incomes below theEuropean poverty line of half the average incomeApproximately 96 million of these people are in house-holds that receive income support and the remainderlive on low or insecure wages Diets in low-incomehouseholds are characterised by less dietary varietywhich is itself associated with poorer nutrient profiles
National Food Survey results have consistently shownlower nutrient intakes in the lowest income groups com-pared to the highest In addition the Dietary and Nutri-tional Survey of British adults (Gregory
et al
1990)found that men and women who were unemployed orliving in households claiming benefit or in social classesIV and V had significantly lower intakes of many vita-mins (especially vitamin C
b
-carotene and vitamin E)and minerals (especially iron) than people not in thesecategories Data from the new NDNS of adults can befound on the FSA website (httpwwwfoodgovuk)
In the National Diet and Nutrition Survey (NDNS) ofyoung children (Gregory
et al
1995) those from man-ual social classes or from less-advantaged homes (wherethe head of the household was unemployed or claimedbenefits) had lower intakes andor blood levels of
b
-carotene niacin vitamin C iron calcium phosphorusand potassium than those from non-manual or more-advantaged households Preschool children from single-parent families had lower levels of
b
-carotene andvitamin C In the NDNS of young people (Gregory
et al
2000) those who received free school meals (and were
Key points
bull Moderate undernutrition leads to fat loss generalwasting of muscles and loss of protein from internalorgansbull Internal organs can function normally in moderateundernutrition but with severe undernutrition gutfunction breaks down causing malabsorption diar-rhoea and infection This can be fatalbull There are a number of methods for the assessmentof undernutrition BMI is routinely used in adultsand growth reference standards are used in children
Undernutrition in the UK
93
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
therefore from households in receipt of benefits) hadlower vitamin and mineral intakes (Buttriss 2002)
Similar findings have been reported from other large-scale surveys in the UK such as the Scottish HeartHealth Study in which the data were controlled forsmoking and education level (Bolton-Smith
et al
1991)and the 36-year follow-up to the National Birth CohortStudy (Braddon
et al
1988) The survey of nutrientintakes in Northern Ireland found similar nutrientdifferences by occupational social class (Barker
et al
1989) These findings are comparable with those fromsmaller surveys looking at nutrient intakes in differentsocioeconomic circumstances (Calvert
et al
1994Moynihan
et al
1993) including the homeless (Rushdenamp Wheeler 1993) A study by Dowler amp Calvert (1995)of nutrient intakes in lone-parent households showedthat where parents had lived for some time on incomesupport and particularly where they had fixed regulardeductions for debt recovery nutrient intakes were halfof the levels of those not living in such circumstances
In terms of dietary variety and overall dietary pat-terns those in poorer households consume less fruitjuice lean meat oily fish and wholemeal products andfewer salads and are more likely to eat white breadpotatoes cheaper fatty meats beans eggs and chips(Anderson amp Hunt 1992 Gregory
et al
1995Whichelow
et al
1991) Those on lower incomes have amuch less diverse food base so their diet is more likelyto lack variety
Many foods that are integral to a healthy diet are per-ceived as a luxury by those on low incomes and are anlsquoexpensiversquo form of energy such foods include fruitsvegetables and fish In addition many healthier alterna-tives carry a price premium
eg
wholemeal bread fatsand spreads low in saturates and lean meat However inaddition to price many factors influence the purchasingand consumption patterns in low-income householdswhich are related to their poor financial status such aslimited food preparation facilities Low income is alsooften associated with lack of knowledge and skillsrelated to food nutrition and cooking
Policies adopted by government local authorities andfood retailers can influence which foods are availableand accessible to people with low incomes For examplethere is the issue of price variability between shopsFood is generally more expensive in corner shops con-venience stores and small independent supermarketsthan in large supermarkets Piachaud amp Webb (1996)found that on average basic foodstuffs cost 24 morein small stores than in supermarkets taking super-market own brands into account the differences in costs
were 60 They calculated that people living in ahousehold on benefits would have to spend 25 moreof their income on food if they could not get to a largesupermarket or street market
Access to shopping facilities in areas where low-income households are concentrated is restricted interms of the physical difficulties or cost of travelling toshops and by a lack of choice of shops Thereforeaccess to a healthy diet becomes a particular problemfor low-income households The number of food retailoutlets is continually decreasing mainly at the expenseof shops such as small grocery retailers butchers fish-mongers and greengrocers The number of large retailoutlets has also decreased mainly because of theincrease in the number of superstores located on the out-skirts of towns and designed for access primarily by carEconomies of scale allow food sold in supermarkets tobe cheaper and cover a wider range than that in smallerhigh street stores The 1998 Independent Inquiry intoInequalities in Health report (Acheson 1998) foundparadoxically that a basket of food cost more in dis-advantaged areas than in affluent areas
The price of a healthy diet and the variation betweenprices of some foods is therefore of major concern forthose living on low incomes Many of the poorest peoplein the UK are concentrated in local authority housing ininner cities and there is evidence to suggest a continuinggeographical polarisation of income inequalities Inmany of these areas shops and banks have withdrawnpartly because the residents spend so little and partlybecause of the retail concentration in superstores(defined as having a total floor surface area of more than7620 m
2
) designed primarily for car access The risein vandalism is another contributing factor In a bidto resolve these problems the supermarket chainSomerfield operates a policy of maintaining small- andmedium-sized high street shops to serve local commu-nities and not to build large out-of town superstoresMany deprived sectors of society suffer from a lack ofaccess to good shopping facilities and in particularfresh fruit and vegetables To avoid these lsquofresh fooddesertsrsquo Somerfield opted to offer a free delivery serviceto village shops and small local stores Unfortunatelythe company had to close some of these small stores insome areas due to vandalism
312 Social and physical factors
Some of the social factors that influence food choice andeating patterns are listed below
94
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Figure 1
Guidelines for estimating the approximate energy and nitrogen requirements for an adult patient receiving artificial nutritional support Reproduced from Garrow
et al
2000 Reproduced with permission from Elsevier
bull Budgeting skillsbull Cultural traditionsbull Religious beliefsbull Educationbull Nutritional knowledgebull Lack of cooking facilities
eg
families housed in bed-and-breakfast accommodationbull Habitsbull Likes and dislikesbull Previous food experiencebull Willingness to experimentbull Time availablebull Eating alonebull Depressionbull Bereavement
For example a recently widowed man may not only besuffering the effects of bereavement and depressionwhich are likely to reduce appetite but he may also sud-denly find himself having to cope alone If his wife hadalways been responsible for shopping cooking and pro-viding food the widower may have difficulty budgetingfor food preparing and cooking food and may find thenew experience of eating alone all too painful
Poor dentition is another factor The NDNS of peopleaged 65 years and over (Finch
et al
1998) reported thatpeople with no natural teeth or few natural teeth ate amore restricted range of foods influenced by their per-ceived inability to chew The survey showed an associ-ation between oral function and nutrient intake andnutritional status Subjects without their own teeth wereless likely to choose foods that need chewing such asfruit and vegetables had lower intakes of iron vitaminsC and E and retinol and had lower plasma levels of vita-min C This was particularly true of those who lived invarious forms of residential care Physical disabilitiesalso influence a personrsquos ability to shop prepare andcook food Something as simple as opening a can ofbaked beans is far from simple for someone witharthritic hands
32 Effect of disease on nutritional status
321 The nutritional requirements of illness
Tissue repair imposes demands on nutritional supplyand an increased activity of body defence mechanismsmay also increase nutritional needs Despite this illhealth is often associated with a decreased desire forfood and decreased nutritional intake
Various changes in the metabolism of carbohydratefat and protein can be observed in illness Proportionalto the severity of illness there is an increase in the bodyrsquosenergy requirement and also an increase in urinarynitrogen loss (Cuthbertson 1980) The scale of thesechanges can be seen in Fig 1 This response to illnesshas been termed a stress response and the state ofincreased energy and protein needs a hypermetabolicstate
The metabolic response to illness traditionally hasthree phases ebb flow and anabolic although these canbe moderated with drug treatment The ebb phase onlylasts for a few hours and there is a depression of meta-bolic function and a reduction in energy expenditure In
Undernutrition in the UK
95
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
the flow phase metabolic rate increases and energyreserves in the form of fat stores are mobilised Visceraland muscle tissue provide amino acids that can be usedfor gluconeogenesis providing glucose for the brain andred blood cells and for wound-healing mechanismsHormonal changes appear to be important determinantsof the stress response Simply stated insulin stimulatesglucose uptake and metabolism and glycogen fat andprotein synthesis During starvation insulin levels arelow and other hormones are effective in mobilisingbody stores (
ie
promote glycogen fat and proteinbreakdown and stimulate gluconeogenesis and ketoge-nesis) In the stress response there is an increased secre-tion of catabolic hormones Especially important arethe glucocorticoids catecholamines and glucagon Theactions of insulin seem to be opposed by the catabolichormones leading to a state of insulin resistance(Cuthbertson 1980)
Another fundamental event is the production of themediator interleukin-1 a polypeptide produced byphagocytic cells (white blood cells that help fight infec-tion) A number of direct effects collectively termed theacute-phase response are ascribed to interleukin-1These include fever which is one of the strategies thebody uses to fight infection and the induction of muscleprotein breakdown leading to increased blood levels ofthe acute-phase proteins prealbumin retinol-bindingprotein (RBP) and C-reactive protein (Casati
et al
1998)
In simple starvation the breakdown of body fat isreversed by feeding with glucose In the hypermetabolicpatient it is found that fat breakdown continues despitegiving glucose and that gluconeogenesis and glucoseoxidation also occur at increased rates Hence theincreased gluconeogenesis can increase the amount ofcarbohydrate that is required to obviate protein break-down Achievement of energy balance fails to alleviatecatabolism in critically ill patients Therefore provisionof energy intake to match energy expenditure is unnec-essary during the flow phase and may even be unhelpful(Frankenfield
et al
1997)The increased nitrogen loss observed in stressed
patients can be accounted for by both a depression ofprotein synthesis and an increase in the rate of proteinbreakdown Provision of adequate protein stimulatesprotein synthesis but it also stimulates breakdown(Campbell 1999)
In the anabolic phase catabolism eventually declinesand is coupled with an increase in appetite and ability tomove This phase provides the opportunity for nutri-tional therapy to restore muscle mass and increase pro-tein synthesis
33 Reaching hospital
On reaching hospital dietary intake may be furtherreduced by one or more of the following problems
bull Confusionbull Fearbull Depressionbull Dysphagia (inability or reduced ability to swallow)bull Loss of appetite taste smell or thirstbull Poor dentitionbull Constipation which is caused by reduced mobilityand the fear that eating will make it worsebull Discomfortbull Dislike of the type of food availablebull Difference in routine and meal patternbull Problems with feedingbull Lack of staff available to help with feeding
Key points
Factors influencing poor dietary intake includebull loss of appetitebull disease or recurrent illness and consequenttreatmentbull impaired ability to absorb or utilise nutrientsbull poverty resulting in lack of car ownership or alter-native transport leading to limited access to bulk buy-ing low-cost foodbull poor housing with poor food storage and prepara-tion facilitiesbull problems of shopping and lack of preparation andcooking skillsbull less education leading to less knowledge and moti-vation to make healthy diet choicesbull unemployment so there is less money available forexpenditure on foodbull social isolation depression and bereavement lowself-esteem
4 Extent of the problem of undernutrition
Undernutrition among patients in UK hospitals wasdocumented in the mid-1970s (Bistrian
et al
1974 Hill
et al
1977) and it remains a common and often unrec-ognised problem that contributes to patient morbidityand mortality (Lennard-Jones 1992 McWhirter ampPennington 1994 Potter
et al
1998)
96
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Many studies over the last 30 years have since empha-sised the presence of disease-related undernutrition inhospitalised patients (Bistrian
et al
1974 Corish
et al
2000 Hill
et al
1977 Kelly
et al
2000 McWhirter ampPennington 1994) However there is controversy aboutits exact prevalence in the hospital setting One of themajor reasons for this is that there is no universal agree-ment about the definition of undernutrition Becausevarious workers have used different criteria to screen forundernutrition the reported magnitude of the problemhas been highly variable ranging from 10 to 60
Corish
et al
(2000) have screened for undernutritionin patients admitted to two teaching hospitals in DublinTo ensure more reliable comparisons they used thesame criteria employed by McWhirter amp Pennington(1994) in a Dundee hospital 6 years earlier In both stud-ies patients were classified as undernourished if theyhad a BMI
lt
20 kgm
2
and a triceps skinfold thicknessor mid-arm muscle circumference (MAMC) below the15th percentile The incidence of undernutrition innewly admitted patients in Dublin was reported to bemore than threefold lower (11) than in Dundee(40)
This striking difference has led other experts in thefield to question the criteria for defining undernutritionElia amp Stratton (2000) suggest that anthropometric cut-off values should not be used as a diagnostic label ofundernutrition but rather to classify an individualrsquosrisk of undernutrition Some healthy subjects have aBMI
lt
20 kgm2 (especially young adults) and are per-fectly well In addition anthropometric criteria alonesuggest a chronic protein-energy deficiency status How-ever a patient showing substantial recent weight loss(eg greater than 10 weight loss over 3ndash6 months) isat risk of undernutrition and impaired bodily functionseven though the anthropometric cut-off values may nothave been reached
The standard data used for anthropometry requireregular review so that they achieve the right balancebetween reflecting what is the norm (which may not bedesirable) and what is desirable (which may not beappropriate to the current generation) Unlike BMIwhich is a fixed criterion percentile values can showsubstantial change over time For example the referencevalues provided by Bishop et al (1981) for arm anthro-pometry were established in the USA about 30 yearsago The secular trends in obesity over that period meanthat these reference values may no longer apply Fur-thermore the choice of the percentile cut-off for use aspart of the screening tool to classify patients as under-nourished may be inappropriately high (since 15 ofthe reference population falls below this cut-off)
While the picture may be incomplete with regard tothe prevalence of undernutrition in hospitals it is clearthat disease-related undernutrition remains a significantclinical problem in hospitals
However the problem of disease-related undernutri-tion is not confined to people in hospital Within thecommunity up to 10 of people with cancer or otherchronic diseases may be significantly malnourished(Edington et al 1996) and many elderly people are alsoat high risk of undernutrition As a result people arecommonly admitted to hospital nutritionally depletedIn a study conducted in four hospitals in EnglandEdington et al (2000) found that one in every fivepatients admitted was malnourished Patients wereassessed using anthropometric measurements and BMIand by recording history of unintentional weight lossThis figure is likely to be an underestimate because it didnot include those who were too ill on admission to beassessed Kelly et al (2000) estimated that undernutri-tion among acute hospital admissions goes unrecognisedin 70 of cases
Once in hospital undernutrition is likely to get worseIn the study by McWhirter and Pennington two-thirdsof the 500 patients who had been assessed on admis-sion and were reassessed on discharge had lost weightA study on a random sample of 150 in-patients foundapproximately half of them to be either at moderate riskor high risk of undernutrition (Reilly et al 1995) Theprevalence and level of risk is probably higher amonghigh dependency medical surgical geriatric and paedi-atric patients (Reilly et al 1995) As illness and hospi-talisation are frequently associated with weight lossdeterioration in nutritional status is inevitable unlessaction is taken to prevent it
Key points
bull It is estimated that 70 of all undernutrition in theUK goes unrecognised and untreatedbull In the community 5 of the population have aBMI lt 20 kgm2 In hospitals this figure is 20ndash25bull It is estimated that 40 of adults and 15 of chil-dren admitted to hospital are malnourished half ofthese severely so and many others become malnour-ished during their stay in hospitalbull It is estimated that at any one time approximately66 of hospital patients are malnourished
Undernutrition in the UK 97
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
5 Cost of the problem of undernutrition
Undernutrition primarily results in loss of body tissue(depletion of body fat stores and muscle wasting) How-ever because nutrient intake is so closely correlatedwith energy intake a deficiency of energy is likely toresult in an inadequate intake of protein vitamins min-erals and trace elements This can cause widespreadmetabolic physiological and functional effects whichmay include
bull Impaired immune function and hence increased sus-ceptibility to infection and sepsis Infection will furtherimpair a malnourished statebull Delayed wound healingbull Increased risk of pressure sores particularly due toloss of cushioning fat storesbull Muscle wasting and weakness which may affect
ndash Respiratory function impaired respiratory musclestrength makes it difficult for a patient to cough andexpectorate effectively so increasing the risk of chestinfection It may also be more difficult to wean apatient off a ventilatorndash Cardiac function this may be impaired resulting inreduced cardiac output and risk of heart failurendash Mobility weakness of skeletal muscles delays areturn to full mobility Reduced mobility increases therisk of thromboembolism and bedsores
bull Altered structure of the small intestine which mayresult in malabsorptionbull Increased risk of postoperative complicationsbull Apathy and depression leading to loss of morale andreduced will to recoverbull General sense of weakness and illness which impairsappetite and physical ability to eat and hence tends toperpetuate and worsen any undernutrition
In summary undernutrition causes considerable mor-bidity delays recovery and increases the risk of death ABMI at or below the 15th percentile has been shown tobe a significant and independent predictor of death inseriously ill patients (Galanos et al 1997) There is alsoan economic cost in terms of increased need of nursingcare and extended hospital stay
There is clear evidence that correcting undernutritionhas many benefits (Potter et al 1998) Improvements inbody weight status and anthropometric parameters areassociated with improvement in immune function(Chandra 1992 Dionigi et al 1988) wound healing(Haydock amp Hill 1987) and muscle function (Fiataroneamp Evans 1993) and in clinical outcomes such asrecovery time and incidence of postoperativecomplications
Hospitals spend approximately pound15 billion on foodannually and studies conducted in one hospital foundthat 30ndash40 of food is discarded (Kelly 1999) This isconsistent with national estimates that 30ndash50 of hos-pital food is wasted with a monetary value calculated tobe pound45 million each year (Edwards amp Nash 1997Fenton et al 1995) With the inclusion of labour andoverheads this cost rises to pound144 million annuallyThere is also the hidden cost of the extra ill health asso-ciated with undernutrition Some hospitals also typicallyspend approximately pound800 000 on enteral andparenteral nutrition (see Sections 92 and 93) TheKingrsquos Fund (1992) report calculated that provision ofcomprehensive nutrition support would result in a 5-day reduction in hospital stay for approximately 10of patients The consequent saving was estimated to bepound266 million annually in the UK A review conducted byBond (1997) in the USA showed a clear relationshipbetween undernutrition and prolonged hospital stayWhen nutritional intervention was introduced 2 daysearlier than usual the result was a 1-day shortening ofhospital stay It was calculated that a more aggressivenutritional intervention policy would save the averagehospital $1 million per year
Key points
bull Between 30 and 50 of hospital food is wastedbull On average food intake is less than 75 of thatrecommended particularly among the elderlybull The monetary value of hospital food wasted eachyear in England alone is calculated to be pound45 millionBy including labour and overheads this cost rises topound144 millionbull There is also the hidden cost of the extra ill healthassociated with undernutrition because it increasesthe risk of complications lowers resistance to infec-tion impairs physical and mental functioning anddelays recovery
6 Why the problem of undernutrition is exacerbated in hospitals
In more than 60 of patients nutritional status deteri-orates during their stay in hospital with those whoare malnourished on admission particularly affectedPennington (1998) demonstrated that progressive nutri-tional depletion occurs for up to 8 weeks after curativesurgery (eg a heart by-pass operation) This thereforeindicates the need to consider nutritional status fromonset of illness through to complete recovery including
98 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
time after discharge However undernutrition remainsundetected in the majority of patients affected becausemany clinicians and nurses still do not consider nutri-tion to be an important factor in the management of dis-ease (Schenker 2000) and so do not routinely monitornutritional status and body weight Economic analysishas demonstrated that appropriate nutritional treatmentis cost-effective but benefits will only be achieved withhigh standards of nutritional care Multi-professionalnutritional support teams best conduct such treatmentbut there is continuing evidence of poor practice anda high incidence of treatment-related complicationswhich negate the benefits of nutritional treatments(Schenker 2000) In the hospital or institutional settingtherefore the problems that cause undernutrition maybe compounded by the fact that nutritional consider-ations may receive little attention from medical andnursing staff Lack of awareness of the prognostic sig-nificance of undernutrition and lack of knowledgeamong doctors and nurses regarding its assessment andmanagement (Nightingale amp Reeves 1999) may meanthat it is neither looked for nor taken into account whentreatment priorities are being set In particular theremay be failure to
bull identify those with or at risk of nutritional depletionbull identify nutritional requirements especially whenthese are increased because of fever surgery or injurybull provide food of an appropriate quality compositionand consistencybull encourage food intake food is of no benefit if noteatenbull monitor what is actually consumed in some circum-stances direct observation of food and fluid consump-tion is essentialbull identify those whose nutritional needs are not beingmet (through regular weighing or the use of otheranthropometric measurements)bull correct inadequate intake
61 Hospital food and feeding
The following factors have been identified as causes forpoor dietary intake in hospital patients
611 Problems with ordering
bull Menus lack clarity dishes should be described accu-rately so that patients have a reasonable idea of what toexpectbull Help with ordering should be available (but in manycases is not) where there are problems with a patientrsquoscomprehension speech or language
bull Menus are often not printed in languages other thanEnglish This is a particular problem in areas with a highimmigrant population Illiteracy may limit usefulness oftranslated menus Verbal translation may be betterbull Ordering from the menu too far in advance A patientmay be discharged after they have ordered food for thenext day resulting in the bedrsquos new occupant receivingfood chosen by someone else which may be unsuitableSame day ordering systems reduce waste and encourageconsumptionbull Patientsrsquo orders are not checked to ensure that thefood received and the portions requested are correct Inthis respect ward hostesses or feeding care attendantsmay be helpful however this does have financialimplicationsbull Inefficient ordering systems and poor two-way com-munication between the wards and the catering depart-ment lead to waste eg food sent to patients who havebeen discharged transferred or have died Such trays arethen either wasted or given to another patient wholeaves most of it because it was not their choice
612 Menu choice
bull Menus do not always take account of the needs tastesand customary eating habits of different groups ofpatients These will vary according to age race or cul-ture or the disease processbull Menus often do not take account of those needingfortified andor modified-consistency mealsbull Inappropriate promotion of lsquohealthy eatingrsquo eglow-fat diets in undernourished or nutritionally at-riskpatientsbull Some elderly patients often adopt a grazing habit andrequire frequent small volume high energy densityfeeds and snacksbull Special needs Although some disease-specific menuseg for renal failure may be provided from a dietkitchen it may be cost-effective to be able to supplementthe standard menu with high-energy high-proteinadditionsbull Nutritional needs and appetites of children differfrom those of adults and also vary according to ageMeals should be made attractive to children
613 Appropriate food choices
bull Food suitable for lsquohealthy eatingrsquo by the overweightpatient with cardiovascular disease is inappropriate forthe depleted malnourished patientbull Pureacuteed or semisolid diets are required by patientswith neurological or mechanical dysphagia who may be
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients
Undernutrition in the UK
89
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
of suitable facilities to store it if it was hot) and there may be no other food availableto them
A major contributor to the worsening nutritional status during hospitalisationhowever is the inadequacy of current catering and feeding practices Hospital cater-ing is beset with all sorts of seemingly trivial problems that add up to one hugeproblem For example the wrong food may arrive for a patient because they werenot able to choose it themselves or they have been given a meal chosen by somebodyelse occupying the bed before them The meal that does come is difficult to eat
eg
the provision of individual butter packs that are difficult for frail arthritic fingers toopen
Although special techniques of enteral and parenteral nutrition support are indi-cated for a minority of patients with failure of swallowing or gastrointestinal func-tion the majority of patients are dependent on hospital food to sustain them duringillness In many hospitals the three meals provided may be of a reasonable standardas the catering officers struggle on the tight budget they have but the range andquality of the snacks (essential to meet increased requirements in many patients) letthem down In many cases proprietary oral supplements or sip feeds may be ofvalue but they should not become a convenient substitute for adequate and appro-priate food provision
Hospital menus and meals should provide sufficient choice to offer healthy bal-anced appetising nutrition for all patients Menus should be designed to meet theneeds of particular patient groups
eg
elderly people children and ethnic minori-ties Adequate choice should be available to meet these needs Special attentionshould be given to the requirements of sick and nutritionally vulnerable patientsand appropriate special therapeutic diets for those who need them should be pro-vided A range of meals specially fortified in energy and protein should also be avail-able in every hospital and snacks and nourishing drinks should be kept in the wardand routinely offered between meals The timing of meals should be reviewed andmade more relevant to patientsrsquo customary meal patterns All methods of food prep-aration
eg
in-house cook-serve or brought-in cook-chill (with ward regeneration)have proved successful but each is highly dependent on the method of distributionand serving With proper management a bulk trolley bedside service servespatientsrsquo needs best Nutritionally vulnerable patients should be placed in wardswith kitchen areas or near ward kitchens so that special meals or snacks can beprepared for them or when possible patients can access the kitchen themselves Theprimary responsibility of the nutritional care of in-patients rests with the nurses incharge of the ward therefore food should be served by nurses supported wherenecessary by other grades of staff trained for this purpose
eg
ward hostesses diettechnicianshelpers Assistance with eating must be provided where necessary Plateor tray collection should be supervised by nursing staff to enable patientsrsquo foodintake to be monitored
Many studies have shown the benefits of nutritional intervention Therefore thepresence of disease whether in hospital or the community should be seen as anindication of the need for nutritional screening to identify those at particular riskand those who might benefit from some form of nutritional intervention In which
90
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
1 Introduction
Serious attention to the problem of undernutrition inhospitals was first given in 1992 with the publication ofthe Kingrsquos Fund report
A Positive Approach to Nutri-tion as Treatment
(Kingrsquos Fund 1992) The report statedthat 66 of all hospital patients were malnourished andcited evidence that undernutrition in hospital patientshad both clinical and financial implications The organ-isation of food and nutrition services in hospitals wasreviewed and a number of recommendations forimproving care were made
Two years later McWhirter amp Pennington (1994)showed that 40 of adults admitted to hospital hadsome degree of undernutrition and in half of them thiswas severe Patients continued to lose weight duringtheir time in hospital yet only 5 were referred for die-tetic help Those who did receive dietetic support gainedweight proving that once identified the problem couldbe treated McWhirter amp Pennington identified a num-ber of contributing factors to the widespread existenceof undernutrition Most importantly they showed thefailure of nurses and doctors to identify patients at riskand to recognise obvious signs and symptoms of under-nutrition There was often no reference in the medicalnotes to the nutritional status of the patient on admis-sion and 23 of patients were not weighed on admis-sion and throughout their stay Also no mention wasmade of the patientrsquos appetite or food intake
Following the publication of the Kingrsquos Fund report anumber of reports have produced recommendationsspecifically addressing the management of food andnutrition in hospitals (Bond 1997 Burke 1997) Thesecover such issues as staff roles and responsibilities train-ing standards for hospital food and the identificationand assessment of undernutrition The latest tworeports
Managing Nutrition in Hospital A Recipe forQuality
(Nuffield Trust 1999) and
Hospital Food asTreatment
(BAPEN 1999) are in almost complete agree-ment as to causes and consequences of undernutrition inhospitals and their subsequent recommendations forimproving the current situation (see Section 7)
Despite an increased awareness and widespread dis-cussion of the issue there is little evidence of generalimprovement in practice either in the provision andorganisation of nutrition care or in the prevalence ofundernutrition among patients The Nuffield Trust(1999) and BAPEN (1999) reports highlighted the con-tinued confusion of roles and responsibilities over nutri-tional care a lack of enforcement of existing guidelinesand a lack of status awarded to the whole area of foodand nutrition in hospitals
The functional clinical and economic consequencesof undernutrition have been well reviewed and demon-strated repeatedly They include impaired mental andphysical function greater risk of death increased com-plication rates during illness and following surgery anddelayed recovery with prolonged convalescence and
case implementing measures such as improved staff training nutritional screeningand assessment and monitoring combined with better catering practices will resultin most patientsrsquo nutritional requirements being met Fortified meals between-mealsnacks and adequate ward staffing have all been shown to contribute to achievingthis goal which leads to better clinical outcome less waste a shorter hospital stayand a more cost-effective service
Recently a number of schemes and initiatives have been set up to help prevent orcombat malnutrition both in hospitals and the community These include the launchof
Better Hospital Food a new menu for the National Health Service
and the estab-lishment of the Malnutrition Advisory Group a group of experts convened to raiseawareness and understanding of issues of undernutrition Community initiativesinclude the establishment of the Neighbourhood Renewal Unit for deprived neigh-bourhoods Sure Start ndash set up to operate local programmes for children and parentsliving in areas of high poverty and Healthy Living Centres ndash set up to run schemessuch as luncheon clubs for older people
Undernutrition in the UK
91
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
hospital stay In some patients undernutrition may bethe main condition that precipitates hospital admissionTrials of nutritional intervention by oral or artificialmeans have shown that in many patients the clinicalconsequences of undernutrition can be avoided orreversed by appropriate nutritional care (Beier-Holgersen amp Boesby 1996 Keele
et al
1995 Larsson
et al
1990 Rana
et al
1992)
2 Definition and classification of undernutrition
Undernutrition can be defined as a disturbance of formor function arising from the deficiency of one or morenutrients Undernutrition can be mild or severe helpful(if it results in appropriate weight loss in someone whois obese) or dangerous Weight loss is a manifestation ofenergy depletion The least essential tissues suffer firstthe adipose tissue cells lose fat which is oxidised to pro-vide energy Essential nutrients protein and micronutri-ents are likely to be depleted at the same time The bodystores of some micronutrients are large while require-ments for others are lower when energy intake isreduced In children who have relatively higher proteinrequirements than adults serious depletion of proteinaccompanies undernutrition
The consequences of protein depletion are apparent intwo main ways somatic protein depletion ndash the loss oftissue as general wasting of muscles and visceral proteindepletion ndash protein loss from the liver pancreas and gutWhen protein is lost from skeletal muscle the musclefibres shrink and the spaces between them are filled withan extracellular watery gel In older people some of theexcess fluid collects in the legs during the day as oedemaIf the loss is not too severe the oedema will disappearwhen the person lies down
In undernutrition the skeleton retains its outward sizeand shape but the fatty marrow disappears and isreplaced with aqueous material The skin loses proteinand becomes easily infected this with the loss of sub-cutaneous fat gives it a loose hanging appearance Theinternal organs particularly the liver lose mass Theheart and kidneys tend to lose mass in parallel withthe rest of the body but the brain retains its size andstructure The gut becomes thin and weight is lost fromboth muscle and mucosa
In spite of these structural changes organ functionand body systems remain normal until a great deal ofweight has been lost The resting metabolic rate per kilo-gram body weight is not greatly reduced in moderateundernutrition but in starvation both metabolic rateand body temperature fall Pulse rate and arterial blood
pressure are low in undernutrition as the body adaptsphysiologically In moderate undernutrition the gutfunctions normally provided there is no infection butin severe undernutrition diarrhoea can be severe (evenwithout infection) and the resulting dehydration canprove fatal
The presence of undernutrition in adults is assessed interms of degrees of weight loss An easy (but not thebest) index is body mass index (BMI) (see Section 833)defined as weight (in kilograms) divided by the square ofthe height (in metres)
ie
weightheight
2
Table 1 givesvalues for defining adult grades of undernutrition
The most sensitive indicator of undernutrition in chil-dren is failure to achieve normal growth compared witha lsquonormalrsquo reference growth rate for the age and sex ofthe child Progression of growth is an important param-eter and can be assessed in terms of height and weightor in infants weight and head circumference in relationto reference standards for age New reference standards(Freeman
et al
1995) have been published to replacethose compiled in the 1950s which take into accountthe upward shift in the average weight and height ofchildren in recent decades However a number of diffi-culties are associated with the use of these data Firstlychildren who cross centiles but never actually reach thecut-off centile defining failure to thrive are not identi-fied For example infants considered large at birthmight fail to grow but because they do not reach thecut-off centile failure to thrive will not be diagnosedSecondly infancy is naturally a period of centile crossing(large for gestational age infants grow more slowly thanthose of small for gestational age) So identifying failureto thrive depends on being able to distinguish poorgrowth from natural changes in growth rate To addressthis problem Cole (1997) has developed a chart thatcan be used to detect growth faltering over any period of4 weeks or longer
Table 1
Classification of undernutrition in adults by body mass index (BMI)
BMI (kgm
2
) Classification
gt
20 Normal185ndash20 Marginal undernutrition17ndash185 Mild undernutrition16ndash17 Moderate undernutrition
lt
16 Severe undernutrition
92
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
3 Causes of undernutrition
Undernutrition is the consequence of a dietary intakethat does not meet nutritional needs and may resultfrom one or more of the following decreased dietaryintake increased nutritional requirementslossesimpaired ability to absorb or utilise nutrients
Undernutrition usually has a slow onset resultingfrom periods of weeks or months when intake has notmatched requirements However in conditions of acutemetabolic stress where nutritional demands are highutilisation of energy and nutrients are disturbed andoral intake is likely to be compromised nutritionaldepletion can occur rapidly and be severe
Many factors can impair dietary intake Theseinclude
bull difficulties with shopping (both access and affordabil-ity) andor preparing cooking or eating food resultingfrom illness lack of mobility or povertybull reduced appetite as a result of the effects of illness orassociated anxiety or depressionbull symptoms associated with a disease or its treatment
eg
nausea vomiting sore mouth abdominal discom-fort or diarrhoeabull lack of interest in food as a result of social isolationsignificant life change (such as bereavement) or mentalillnessbull inadequate or unappetising meals or the provision ofinappropriate foodbull repeated fasting for diagnostic or treatmentproceduresbull problems associated with skipping mealsbull difficulties with eating or chewing
eg
ill-fitting den-tures or poor oral hygiene
bull swallowing difficultiesbull difficulty with self-feeding (
eg
owing to disability ordisorders such as Parkinsonrsquos disease) or inadequatehelp given to those unable to self-feedbull sedation semiconsciousness or coma
These factors can be separated into effects of lifestyleand effects of disease and consequent treatment and areexplored in greater detail below
31 Causes in the community
In this briefing paper causes in the community are con-fined to those undernourished individuals who mayhave previously been patients in hospital and have beendischarged while undernourished or people with onsetof a disease that has yet to be diagnosed or treated andwill enter hospital in due course
311 Poverty
One in four of the UK population nearly 14 millionpeople live in households with incomes below theEuropean poverty line of half the average incomeApproximately 96 million of these people are in house-holds that receive income support and the remainderlive on low or insecure wages Diets in low-incomehouseholds are characterised by less dietary varietywhich is itself associated with poorer nutrient profiles
National Food Survey results have consistently shownlower nutrient intakes in the lowest income groups com-pared to the highest In addition the Dietary and Nutri-tional Survey of British adults (Gregory
et al
1990)found that men and women who were unemployed orliving in households claiming benefit or in social classesIV and V had significantly lower intakes of many vita-mins (especially vitamin C
b
-carotene and vitamin E)and minerals (especially iron) than people not in thesecategories Data from the new NDNS of adults can befound on the FSA website (httpwwwfoodgovuk)
In the National Diet and Nutrition Survey (NDNS) ofyoung children (Gregory
et al
1995) those from man-ual social classes or from less-advantaged homes (wherethe head of the household was unemployed or claimedbenefits) had lower intakes andor blood levels of
b
-carotene niacin vitamin C iron calcium phosphorusand potassium than those from non-manual or more-advantaged households Preschool children from single-parent families had lower levels of
b
-carotene andvitamin C In the NDNS of young people (Gregory
et al
2000) those who received free school meals (and were
Key points
bull Moderate undernutrition leads to fat loss generalwasting of muscles and loss of protein from internalorgansbull Internal organs can function normally in moderateundernutrition but with severe undernutrition gutfunction breaks down causing malabsorption diar-rhoea and infection This can be fatalbull There are a number of methods for the assessmentof undernutrition BMI is routinely used in adultsand growth reference standards are used in children
Undernutrition in the UK
93
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
therefore from households in receipt of benefits) hadlower vitamin and mineral intakes (Buttriss 2002)
Similar findings have been reported from other large-scale surveys in the UK such as the Scottish HeartHealth Study in which the data were controlled forsmoking and education level (Bolton-Smith
et al
1991)and the 36-year follow-up to the National Birth CohortStudy (Braddon
et al
1988) The survey of nutrientintakes in Northern Ireland found similar nutrientdifferences by occupational social class (Barker
et al
1989) These findings are comparable with those fromsmaller surveys looking at nutrient intakes in differentsocioeconomic circumstances (Calvert
et al
1994Moynihan
et al
1993) including the homeless (Rushdenamp Wheeler 1993) A study by Dowler amp Calvert (1995)of nutrient intakes in lone-parent households showedthat where parents had lived for some time on incomesupport and particularly where they had fixed regulardeductions for debt recovery nutrient intakes were halfof the levels of those not living in such circumstances
In terms of dietary variety and overall dietary pat-terns those in poorer households consume less fruitjuice lean meat oily fish and wholemeal products andfewer salads and are more likely to eat white breadpotatoes cheaper fatty meats beans eggs and chips(Anderson amp Hunt 1992 Gregory
et al
1995Whichelow
et al
1991) Those on lower incomes have amuch less diverse food base so their diet is more likelyto lack variety
Many foods that are integral to a healthy diet are per-ceived as a luxury by those on low incomes and are anlsquoexpensiversquo form of energy such foods include fruitsvegetables and fish In addition many healthier alterna-tives carry a price premium
eg
wholemeal bread fatsand spreads low in saturates and lean meat However inaddition to price many factors influence the purchasingand consumption patterns in low-income householdswhich are related to their poor financial status such aslimited food preparation facilities Low income is alsooften associated with lack of knowledge and skillsrelated to food nutrition and cooking
Policies adopted by government local authorities andfood retailers can influence which foods are availableand accessible to people with low incomes For examplethere is the issue of price variability between shopsFood is generally more expensive in corner shops con-venience stores and small independent supermarketsthan in large supermarkets Piachaud amp Webb (1996)found that on average basic foodstuffs cost 24 morein small stores than in supermarkets taking super-market own brands into account the differences in costs
were 60 They calculated that people living in ahousehold on benefits would have to spend 25 moreof their income on food if they could not get to a largesupermarket or street market
Access to shopping facilities in areas where low-income households are concentrated is restricted interms of the physical difficulties or cost of travelling toshops and by a lack of choice of shops Thereforeaccess to a healthy diet becomes a particular problemfor low-income households The number of food retailoutlets is continually decreasing mainly at the expenseof shops such as small grocery retailers butchers fish-mongers and greengrocers The number of large retailoutlets has also decreased mainly because of theincrease in the number of superstores located on the out-skirts of towns and designed for access primarily by carEconomies of scale allow food sold in supermarkets tobe cheaper and cover a wider range than that in smallerhigh street stores The 1998 Independent Inquiry intoInequalities in Health report (Acheson 1998) foundparadoxically that a basket of food cost more in dis-advantaged areas than in affluent areas
The price of a healthy diet and the variation betweenprices of some foods is therefore of major concern forthose living on low incomes Many of the poorest peoplein the UK are concentrated in local authority housing ininner cities and there is evidence to suggest a continuinggeographical polarisation of income inequalities Inmany of these areas shops and banks have withdrawnpartly because the residents spend so little and partlybecause of the retail concentration in superstores(defined as having a total floor surface area of more than7620 m
2
) designed primarily for car access The risein vandalism is another contributing factor In a bidto resolve these problems the supermarket chainSomerfield operates a policy of maintaining small- andmedium-sized high street shops to serve local commu-nities and not to build large out-of town superstoresMany deprived sectors of society suffer from a lack ofaccess to good shopping facilities and in particularfresh fruit and vegetables To avoid these lsquofresh fooddesertsrsquo Somerfield opted to offer a free delivery serviceto village shops and small local stores Unfortunatelythe company had to close some of these small stores insome areas due to vandalism
312 Social and physical factors
Some of the social factors that influence food choice andeating patterns are listed below
94
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Figure 1
Guidelines for estimating the approximate energy and nitrogen requirements for an adult patient receiving artificial nutritional support Reproduced from Garrow
et al
2000 Reproduced with permission from Elsevier
bull Budgeting skillsbull Cultural traditionsbull Religious beliefsbull Educationbull Nutritional knowledgebull Lack of cooking facilities
eg
families housed in bed-and-breakfast accommodationbull Habitsbull Likes and dislikesbull Previous food experiencebull Willingness to experimentbull Time availablebull Eating alonebull Depressionbull Bereavement
For example a recently widowed man may not only besuffering the effects of bereavement and depressionwhich are likely to reduce appetite but he may also sud-denly find himself having to cope alone If his wife hadalways been responsible for shopping cooking and pro-viding food the widower may have difficulty budgetingfor food preparing and cooking food and may find thenew experience of eating alone all too painful
Poor dentition is another factor The NDNS of peopleaged 65 years and over (Finch
et al
1998) reported thatpeople with no natural teeth or few natural teeth ate amore restricted range of foods influenced by their per-ceived inability to chew The survey showed an associ-ation between oral function and nutrient intake andnutritional status Subjects without their own teeth wereless likely to choose foods that need chewing such asfruit and vegetables had lower intakes of iron vitaminsC and E and retinol and had lower plasma levels of vita-min C This was particularly true of those who lived invarious forms of residential care Physical disabilitiesalso influence a personrsquos ability to shop prepare andcook food Something as simple as opening a can ofbaked beans is far from simple for someone witharthritic hands
32 Effect of disease on nutritional status
321 The nutritional requirements of illness
Tissue repair imposes demands on nutritional supplyand an increased activity of body defence mechanismsmay also increase nutritional needs Despite this illhealth is often associated with a decreased desire forfood and decreased nutritional intake
Various changes in the metabolism of carbohydratefat and protein can be observed in illness Proportionalto the severity of illness there is an increase in the bodyrsquosenergy requirement and also an increase in urinarynitrogen loss (Cuthbertson 1980) The scale of thesechanges can be seen in Fig 1 This response to illnesshas been termed a stress response and the state ofincreased energy and protein needs a hypermetabolicstate
The metabolic response to illness traditionally hasthree phases ebb flow and anabolic although these canbe moderated with drug treatment The ebb phase onlylasts for a few hours and there is a depression of meta-bolic function and a reduction in energy expenditure In
Undernutrition in the UK
95
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
the flow phase metabolic rate increases and energyreserves in the form of fat stores are mobilised Visceraland muscle tissue provide amino acids that can be usedfor gluconeogenesis providing glucose for the brain andred blood cells and for wound-healing mechanismsHormonal changes appear to be important determinantsof the stress response Simply stated insulin stimulatesglucose uptake and metabolism and glycogen fat andprotein synthesis During starvation insulin levels arelow and other hormones are effective in mobilisingbody stores (
ie
promote glycogen fat and proteinbreakdown and stimulate gluconeogenesis and ketoge-nesis) In the stress response there is an increased secre-tion of catabolic hormones Especially important arethe glucocorticoids catecholamines and glucagon Theactions of insulin seem to be opposed by the catabolichormones leading to a state of insulin resistance(Cuthbertson 1980)
Another fundamental event is the production of themediator interleukin-1 a polypeptide produced byphagocytic cells (white blood cells that help fight infec-tion) A number of direct effects collectively termed theacute-phase response are ascribed to interleukin-1These include fever which is one of the strategies thebody uses to fight infection and the induction of muscleprotein breakdown leading to increased blood levels ofthe acute-phase proteins prealbumin retinol-bindingprotein (RBP) and C-reactive protein (Casati
et al
1998)
In simple starvation the breakdown of body fat isreversed by feeding with glucose In the hypermetabolicpatient it is found that fat breakdown continues despitegiving glucose and that gluconeogenesis and glucoseoxidation also occur at increased rates Hence theincreased gluconeogenesis can increase the amount ofcarbohydrate that is required to obviate protein break-down Achievement of energy balance fails to alleviatecatabolism in critically ill patients Therefore provisionof energy intake to match energy expenditure is unnec-essary during the flow phase and may even be unhelpful(Frankenfield
et al
1997)The increased nitrogen loss observed in stressed
patients can be accounted for by both a depression ofprotein synthesis and an increase in the rate of proteinbreakdown Provision of adequate protein stimulatesprotein synthesis but it also stimulates breakdown(Campbell 1999)
In the anabolic phase catabolism eventually declinesand is coupled with an increase in appetite and ability tomove This phase provides the opportunity for nutri-tional therapy to restore muscle mass and increase pro-tein synthesis
33 Reaching hospital
On reaching hospital dietary intake may be furtherreduced by one or more of the following problems
bull Confusionbull Fearbull Depressionbull Dysphagia (inability or reduced ability to swallow)bull Loss of appetite taste smell or thirstbull Poor dentitionbull Constipation which is caused by reduced mobilityand the fear that eating will make it worsebull Discomfortbull Dislike of the type of food availablebull Difference in routine and meal patternbull Problems with feedingbull Lack of staff available to help with feeding
Key points
Factors influencing poor dietary intake includebull loss of appetitebull disease or recurrent illness and consequenttreatmentbull impaired ability to absorb or utilise nutrientsbull poverty resulting in lack of car ownership or alter-native transport leading to limited access to bulk buy-ing low-cost foodbull poor housing with poor food storage and prepara-tion facilitiesbull problems of shopping and lack of preparation andcooking skillsbull less education leading to less knowledge and moti-vation to make healthy diet choicesbull unemployment so there is less money available forexpenditure on foodbull social isolation depression and bereavement lowself-esteem
4 Extent of the problem of undernutrition
Undernutrition among patients in UK hospitals wasdocumented in the mid-1970s (Bistrian
et al
1974 Hill
et al
1977) and it remains a common and often unrec-ognised problem that contributes to patient morbidityand mortality (Lennard-Jones 1992 McWhirter ampPennington 1994 Potter
et al
1998)
96
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Many studies over the last 30 years have since empha-sised the presence of disease-related undernutrition inhospitalised patients (Bistrian
et al
1974 Corish
et al
2000 Hill
et al
1977 Kelly
et al
2000 McWhirter ampPennington 1994) However there is controversy aboutits exact prevalence in the hospital setting One of themajor reasons for this is that there is no universal agree-ment about the definition of undernutrition Becausevarious workers have used different criteria to screen forundernutrition the reported magnitude of the problemhas been highly variable ranging from 10 to 60
Corish
et al
(2000) have screened for undernutritionin patients admitted to two teaching hospitals in DublinTo ensure more reliable comparisons they used thesame criteria employed by McWhirter amp Pennington(1994) in a Dundee hospital 6 years earlier In both stud-ies patients were classified as undernourished if theyhad a BMI
lt
20 kgm
2
and a triceps skinfold thicknessor mid-arm muscle circumference (MAMC) below the15th percentile The incidence of undernutrition innewly admitted patients in Dublin was reported to bemore than threefold lower (11) than in Dundee(40)
This striking difference has led other experts in thefield to question the criteria for defining undernutritionElia amp Stratton (2000) suggest that anthropometric cut-off values should not be used as a diagnostic label ofundernutrition but rather to classify an individualrsquosrisk of undernutrition Some healthy subjects have aBMI
lt
20 kgm2 (especially young adults) and are per-fectly well In addition anthropometric criteria alonesuggest a chronic protein-energy deficiency status How-ever a patient showing substantial recent weight loss(eg greater than 10 weight loss over 3ndash6 months) isat risk of undernutrition and impaired bodily functionseven though the anthropometric cut-off values may nothave been reached
The standard data used for anthropometry requireregular review so that they achieve the right balancebetween reflecting what is the norm (which may not bedesirable) and what is desirable (which may not beappropriate to the current generation) Unlike BMIwhich is a fixed criterion percentile values can showsubstantial change over time For example the referencevalues provided by Bishop et al (1981) for arm anthro-pometry were established in the USA about 30 yearsago The secular trends in obesity over that period meanthat these reference values may no longer apply Fur-thermore the choice of the percentile cut-off for use aspart of the screening tool to classify patients as under-nourished may be inappropriately high (since 15 ofthe reference population falls below this cut-off)
While the picture may be incomplete with regard tothe prevalence of undernutrition in hospitals it is clearthat disease-related undernutrition remains a significantclinical problem in hospitals
However the problem of disease-related undernutri-tion is not confined to people in hospital Within thecommunity up to 10 of people with cancer or otherchronic diseases may be significantly malnourished(Edington et al 1996) and many elderly people are alsoat high risk of undernutrition As a result people arecommonly admitted to hospital nutritionally depletedIn a study conducted in four hospitals in EnglandEdington et al (2000) found that one in every fivepatients admitted was malnourished Patients wereassessed using anthropometric measurements and BMIand by recording history of unintentional weight lossThis figure is likely to be an underestimate because it didnot include those who were too ill on admission to beassessed Kelly et al (2000) estimated that undernutri-tion among acute hospital admissions goes unrecognisedin 70 of cases
Once in hospital undernutrition is likely to get worseIn the study by McWhirter and Pennington two-thirdsof the 500 patients who had been assessed on admis-sion and were reassessed on discharge had lost weightA study on a random sample of 150 in-patients foundapproximately half of them to be either at moderate riskor high risk of undernutrition (Reilly et al 1995) Theprevalence and level of risk is probably higher amonghigh dependency medical surgical geriatric and paedi-atric patients (Reilly et al 1995) As illness and hospi-talisation are frequently associated with weight lossdeterioration in nutritional status is inevitable unlessaction is taken to prevent it
Key points
bull It is estimated that 70 of all undernutrition in theUK goes unrecognised and untreatedbull In the community 5 of the population have aBMI lt 20 kgm2 In hospitals this figure is 20ndash25bull It is estimated that 40 of adults and 15 of chil-dren admitted to hospital are malnourished half ofthese severely so and many others become malnour-ished during their stay in hospitalbull It is estimated that at any one time approximately66 of hospital patients are malnourished
Undernutrition in the UK 97
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
5 Cost of the problem of undernutrition
Undernutrition primarily results in loss of body tissue(depletion of body fat stores and muscle wasting) How-ever because nutrient intake is so closely correlatedwith energy intake a deficiency of energy is likely toresult in an inadequate intake of protein vitamins min-erals and trace elements This can cause widespreadmetabolic physiological and functional effects whichmay include
bull Impaired immune function and hence increased sus-ceptibility to infection and sepsis Infection will furtherimpair a malnourished statebull Delayed wound healingbull Increased risk of pressure sores particularly due toloss of cushioning fat storesbull Muscle wasting and weakness which may affect
ndash Respiratory function impaired respiratory musclestrength makes it difficult for a patient to cough andexpectorate effectively so increasing the risk of chestinfection It may also be more difficult to wean apatient off a ventilatorndash Cardiac function this may be impaired resulting inreduced cardiac output and risk of heart failurendash Mobility weakness of skeletal muscles delays areturn to full mobility Reduced mobility increases therisk of thromboembolism and bedsores
bull Altered structure of the small intestine which mayresult in malabsorptionbull Increased risk of postoperative complicationsbull Apathy and depression leading to loss of morale andreduced will to recoverbull General sense of weakness and illness which impairsappetite and physical ability to eat and hence tends toperpetuate and worsen any undernutrition
In summary undernutrition causes considerable mor-bidity delays recovery and increases the risk of death ABMI at or below the 15th percentile has been shown tobe a significant and independent predictor of death inseriously ill patients (Galanos et al 1997) There is alsoan economic cost in terms of increased need of nursingcare and extended hospital stay
There is clear evidence that correcting undernutritionhas many benefits (Potter et al 1998) Improvements inbody weight status and anthropometric parameters areassociated with improvement in immune function(Chandra 1992 Dionigi et al 1988) wound healing(Haydock amp Hill 1987) and muscle function (Fiataroneamp Evans 1993) and in clinical outcomes such asrecovery time and incidence of postoperativecomplications
Hospitals spend approximately pound15 billion on foodannually and studies conducted in one hospital foundthat 30ndash40 of food is discarded (Kelly 1999) This isconsistent with national estimates that 30ndash50 of hos-pital food is wasted with a monetary value calculated tobe pound45 million each year (Edwards amp Nash 1997Fenton et al 1995) With the inclusion of labour andoverheads this cost rises to pound144 million annuallyThere is also the hidden cost of the extra ill health asso-ciated with undernutrition Some hospitals also typicallyspend approximately pound800 000 on enteral andparenteral nutrition (see Sections 92 and 93) TheKingrsquos Fund (1992) report calculated that provision ofcomprehensive nutrition support would result in a 5-day reduction in hospital stay for approximately 10of patients The consequent saving was estimated to bepound266 million annually in the UK A review conducted byBond (1997) in the USA showed a clear relationshipbetween undernutrition and prolonged hospital stayWhen nutritional intervention was introduced 2 daysearlier than usual the result was a 1-day shortening ofhospital stay It was calculated that a more aggressivenutritional intervention policy would save the averagehospital $1 million per year
Key points
bull Between 30 and 50 of hospital food is wastedbull On average food intake is less than 75 of thatrecommended particularly among the elderlybull The monetary value of hospital food wasted eachyear in England alone is calculated to be pound45 millionBy including labour and overheads this cost rises topound144 millionbull There is also the hidden cost of the extra ill healthassociated with undernutrition because it increasesthe risk of complications lowers resistance to infec-tion impairs physical and mental functioning anddelays recovery
6 Why the problem of undernutrition is exacerbated in hospitals
In more than 60 of patients nutritional status deteri-orates during their stay in hospital with those whoare malnourished on admission particularly affectedPennington (1998) demonstrated that progressive nutri-tional depletion occurs for up to 8 weeks after curativesurgery (eg a heart by-pass operation) This thereforeindicates the need to consider nutritional status fromonset of illness through to complete recovery including
98 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
time after discharge However undernutrition remainsundetected in the majority of patients affected becausemany clinicians and nurses still do not consider nutri-tion to be an important factor in the management of dis-ease (Schenker 2000) and so do not routinely monitornutritional status and body weight Economic analysishas demonstrated that appropriate nutritional treatmentis cost-effective but benefits will only be achieved withhigh standards of nutritional care Multi-professionalnutritional support teams best conduct such treatmentbut there is continuing evidence of poor practice anda high incidence of treatment-related complicationswhich negate the benefits of nutritional treatments(Schenker 2000) In the hospital or institutional settingtherefore the problems that cause undernutrition maybe compounded by the fact that nutritional consider-ations may receive little attention from medical andnursing staff Lack of awareness of the prognostic sig-nificance of undernutrition and lack of knowledgeamong doctors and nurses regarding its assessment andmanagement (Nightingale amp Reeves 1999) may meanthat it is neither looked for nor taken into account whentreatment priorities are being set In particular theremay be failure to
bull identify those with or at risk of nutritional depletionbull identify nutritional requirements especially whenthese are increased because of fever surgery or injurybull provide food of an appropriate quality compositionand consistencybull encourage food intake food is of no benefit if noteatenbull monitor what is actually consumed in some circum-stances direct observation of food and fluid consump-tion is essentialbull identify those whose nutritional needs are not beingmet (through regular weighing or the use of otheranthropometric measurements)bull correct inadequate intake
61 Hospital food and feeding
The following factors have been identified as causes forpoor dietary intake in hospital patients
611 Problems with ordering
bull Menus lack clarity dishes should be described accu-rately so that patients have a reasonable idea of what toexpectbull Help with ordering should be available (but in manycases is not) where there are problems with a patientrsquoscomprehension speech or language
bull Menus are often not printed in languages other thanEnglish This is a particular problem in areas with a highimmigrant population Illiteracy may limit usefulness oftranslated menus Verbal translation may be betterbull Ordering from the menu too far in advance A patientmay be discharged after they have ordered food for thenext day resulting in the bedrsquos new occupant receivingfood chosen by someone else which may be unsuitableSame day ordering systems reduce waste and encourageconsumptionbull Patientsrsquo orders are not checked to ensure that thefood received and the portions requested are correct Inthis respect ward hostesses or feeding care attendantsmay be helpful however this does have financialimplicationsbull Inefficient ordering systems and poor two-way com-munication between the wards and the catering depart-ment lead to waste eg food sent to patients who havebeen discharged transferred or have died Such trays arethen either wasted or given to another patient wholeaves most of it because it was not their choice
612 Menu choice
bull Menus do not always take account of the needs tastesand customary eating habits of different groups ofpatients These will vary according to age race or cul-ture or the disease processbull Menus often do not take account of those needingfortified andor modified-consistency mealsbull Inappropriate promotion of lsquohealthy eatingrsquo eglow-fat diets in undernourished or nutritionally at-riskpatientsbull Some elderly patients often adopt a grazing habit andrequire frequent small volume high energy densityfeeds and snacksbull Special needs Although some disease-specific menuseg for renal failure may be provided from a dietkitchen it may be cost-effective to be able to supplementthe standard menu with high-energy high-proteinadditionsbull Nutritional needs and appetites of children differfrom those of adults and also vary according to ageMeals should be made attractive to children
613 Appropriate food choices
bull Food suitable for lsquohealthy eatingrsquo by the overweightpatient with cardiovascular disease is inappropriate forthe depleted malnourished patientbull Pureacuteed or semisolid diets are required by patientswith neurological or mechanical dysphagia who may be
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

90
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
1 Introduction
Serious attention to the problem of undernutrition inhospitals was first given in 1992 with the publication ofthe Kingrsquos Fund report
A Positive Approach to Nutri-tion as Treatment
(Kingrsquos Fund 1992) The report statedthat 66 of all hospital patients were malnourished andcited evidence that undernutrition in hospital patientshad both clinical and financial implications The organ-isation of food and nutrition services in hospitals wasreviewed and a number of recommendations forimproving care were made
Two years later McWhirter amp Pennington (1994)showed that 40 of adults admitted to hospital hadsome degree of undernutrition and in half of them thiswas severe Patients continued to lose weight duringtheir time in hospital yet only 5 were referred for die-tetic help Those who did receive dietetic support gainedweight proving that once identified the problem couldbe treated McWhirter amp Pennington identified a num-ber of contributing factors to the widespread existenceof undernutrition Most importantly they showed thefailure of nurses and doctors to identify patients at riskand to recognise obvious signs and symptoms of under-nutrition There was often no reference in the medicalnotes to the nutritional status of the patient on admis-sion and 23 of patients were not weighed on admis-sion and throughout their stay Also no mention wasmade of the patientrsquos appetite or food intake
Following the publication of the Kingrsquos Fund report anumber of reports have produced recommendationsspecifically addressing the management of food andnutrition in hospitals (Bond 1997 Burke 1997) Thesecover such issues as staff roles and responsibilities train-ing standards for hospital food and the identificationand assessment of undernutrition The latest tworeports
Managing Nutrition in Hospital A Recipe forQuality
(Nuffield Trust 1999) and
Hospital Food asTreatment
(BAPEN 1999) are in almost complete agree-ment as to causes and consequences of undernutrition inhospitals and their subsequent recommendations forimproving the current situation (see Section 7)
Despite an increased awareness and widespread dis-cussion of the issue there is little evidence of generalimprovement in practice either in the provision andorganisation of nutrition care or in the prevalence ofundernutrition among patients The Nuffield Trust(1999) and BAPEN (1999) reports highlighted the con-tinued confusion of roles and responsibilities over nutri-tional care a lack of enforcement of existing guidelinesand a lack of status awarded to the whole area of foodand nutrition in hospitals
The functional clinical and economic consequencesof undernutrition have been well reviewed and demon-strated repeatedly They include impaired mental andphysical function greater risk of death increased com-plication rates during illness and following surgery anddelayed recovery with prolonged convalescence and
case implementing measures such as improved staff training nutritional screeningand assessment and monitoring combined with better catering practices will resultin most patientsrsquo nutritional requirements being met Fortified meals between-mealsnacks and adequate ward staffing have all been shown to contribute to achievingthis goal which leads to better clinical outcome less waste a shorter hospital stayand a more cost-effective service
Recently a number of schemes and initiatives have been set up to help prevent orcombat malnutrition both in hospitals and the community These include the launchof
Better Hospital Food a new menu for the National Health Service
and the estab-lishment of the Malnutrition Advisory Group a group of experts convened to raiseawareness and understanding of issues of undernutrition Community initiativesinclude the establishment of the Neighbourhood Renewal Unit for deprived neigh-bourhoods Sure Start ndash set up to operate local programmes for children and parentsliving in areas of high poverty and Healthy Living Centres ndash set up to run schemessuch as luncheon clubs for older people
Undernutrition in the UK
91
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
hospital stay In some patients undernutrition may bethe main condition that precipitates hospital admissionTrials of nutritional intervention by oral or artificialmeans have shown that in many patients the clinicalconsequences of undernutrition can be avoided orreversed by appropriate nutritional care (Beier-Holgersen amp Boesby 1996 Keele
et al
1995 Larsson
et al
1990 Rana
et al
1992)
2 Definition and classification of undernutrition
Undernutrition can be defined as a disturbance of formor function arising from the deficiency of one or morenutrients Undernutrition can be mild or severe helpful(if it results in appropriate weight loss in someone whois obese) or dangerous Weight loss is a manifestation ofenergy depletion The least essential tissues suffer firstthe adipose tissue cells lose fat which is oxidised to pro-vide energy Essential nutrients protein and micronutri-ents are likely to be depleted at the same time The bodystores of some micronutrients are large while require-ments for others are lower when energy intake isreduced In children who have relatively higher proteinrequirements than adults serious depletion of proteinaccompanies undernutrition
The consequences of protein depletion are apparent intwo main ways somatic protein depletion ndash the loss oftissue as general wasting of muscles and visceral proteindepletion ndash protein loss from the liver pancreas and gutWhen protein is lost from skeletal muscle the musclefibres shrink and the spaces between them are filled withan extracellular watery gel In older people some of theexcess fluid collects in the legs during the day as oedemaIf the loss is not too severe the oedema will disappearwhen the person lies down
In undernutrition the skeleton retains its outward sizeand shape but the fatty marrow disappears and isreplaced with aqueous material The skin loses proteinand becomes easily infected this with the loss of sub-cutaneous fat gives it a loose hanging appearance Theinternal organs particularly the liver lose mass Theheart and kidneys tend to lose mass in parallel withthe rest of the body but the brain retains its size andstructure The gut becomes thin and weight is lost fromboth muscle and mucosa
In spite of these structural changes organ functionand body systems remain normal until a great deal ofweight has been lost The resting metabolic rate per kilo-gram body weight is not greatly reduced in moderateundernutrition but in starvation both metabolic rateand body temperature fall Pulse rate and arterial blood
pressure are low in undernutrition as the body adaptsphysiologically In moderate undernutrition the gutfunctions normally provided there is no infection butin severe undernutrition diarrhoea can be severe (evenwithout infection) and the resulting dehydration canprove fatal
The presence of undernutrition in adults is assessed interms of degrees of weight loss An easy (but not thebest) index is body mass index (BMI) (see Section 833)defined as weight (in kilograms) divided by the square ofthe height (in metres)
ie
weightheight
2
Table 1 givesvalues for defining adult grades of undernutrition
The most sensitive indicator of undernutrition in chil-dren is failure to achieve normal growth compared witha lsquonormalrsquo reference growth rate for the age and sex ofthe child Progression of growth is an important param-eter and can be assessed in terms of height and weightor in infants weight and head circumference in relationto reference standards for age New reference standards(Freeman
et al
1995) have been published to replacethose compiled in the 1950s which take into accountthe upward shift in the average weight and height ofchildren in recent decades However a number of diffi-culties are associated with the use of these data Firstlychildren who cross centiles but never actually reach thecut-off centile defining failure to thrive are not identi-fied For example infants considered large at birthmight fail to grow but because they do not reach thecut-off centile failure to thrive will not be diagnosedSecondly infancy is naturally a period of centile crossing(large for gestational age infants grow more slowly thanthose of small for gestational age) So identifying failureto thrive depends on being able to distinguish poorgrowth from natural changes in growth rate To addressthis problem Cole (1997) has developed a chart thatcan be used to detect growth faltering over any period of4 weeks or longer
Table 1
Classification of undernutrition in adults by body mass index (BMI)
BMI (kgm
2
) Classification
gt
20 Normal185ndash20 Marginal undernutrition17ndash185 Mild undernutrition16ndash17 Moderate undernutrition
lt
16 Severe undernutrition
92
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
3 Causes of undernutrition
Undernutrition is the consequence of a dietary intakethat does not meet nutritional needs and may resultfrom one or more of the following decreased dietaryintake increased nutritional requirementslossesimpaired ability to absorb or utilise nutrients
Undernutrition usually has a slow onset resultingfrom periods of weeks or months when intake has notmatched requirements However in conditions of acutemetabolic stress where nutritional demands are highutilisation of energy and nutrients are disturbed andoral intake is likely to be compromised nutritionaldepletion can occur rapidly and be severe
Many factors can impair dietary intake Theseinclude
bull difficulties with shopping (both access and affordabil-ity) andor preparing cooking or eating food resultingfrom illness lack of mobility or povertybull reduced appetite as a result of the effects of illness orassociated anxiety or depressionbull symptoms associated with a disease or its treatment
eg
nausea vomiting sore mouth abdominal discom-fort or diarrhoeabull lack of interest in food as a result of social isolationsignificant life change (such as bereavement) or mentalillnessbull inadequate or unappetising meals or the provision ofinappropriate foodbull repeated fasting for diagnostic or treatmentproceduresbull problems associated with skipping mealsbull difficulties with eating or chewing
eg
ill-fitting den-tures or poor oral hygiene
bull swallowing difficultiesbull difficulty with self-feeding (
eg
owing to disability ordisorders such as Parkinsonrsquos disease) or inadequatehelp given to those unable to self-feedbull sedation semiconsciousness or coma
These factors can be separated into effects of lifestyleand effects of disease and consequent treatment and areexplored in greater detail below
31 Causes in the community
In this briefing paper causes in the community are con-fined to those undernourished individuals who mayhave previously been patients in hospital and have beendischarged while undernourished or people with onsetof a disease that has yet to be diagnosed or treated andwill enter hospital in due course
311 Poverty
One in four of the UK population nearly 14 millionpeople live in households with incomes below theEuropean poverty line of half the average incomeApproximately 96 million of these people are in house-holds that receive income support and the remainderlive on low or insecure wages Diets in low-incomehouseholds are characterised by less dietary varietywhich is itself associated with poorer nutrient profiles
National Food Survey results have consistently shownlower nutrient intakes in the lowest income groups com-pared to the highest In addition the Dietary and Nutri-tional Survey of British adults (Gregory
et al
1990)found that men and women who were unemployed orliving in households claiming benefit or in social classesIV and V had significantly lower intakes of many vita-mins (especially vitamin C
b
-carotene and vitamin E)and minerals (especially iron) than people not in thesecategories Data from the new NDNS of adults can befound on the FSA website (httpwwwfoodgovuk)
In the National Diet and Nutrition Survey (NDNS) ofyoung children (Gregory
et al
1995) those from man-ual social classes or from less-advantaged homes (wherethe head of the household was unemployed or claimedbenefits) had lower intakes andor blood levels of
b
-carotene niacin vitamin C iron calcium phosphorusand potassium than those from non-manual or more-advantaged households Preschool children from single-parent families had lower levels of
b
-carotene andvitamin C In the NDNS of young people (Gregory
et al
2000) those who received free school meals (and were
Key points
bull Moderate undernutrition leads to fat loss generalwasting of muscles and loss of protein from internalorgansbull Internal organs can function normally in moderateundernutrition but with severe undernutrition gutfunction breaks down causing malabsorption diar-rhoea and infection This can be fatalbull There are a number of methods for the assessmentof undernutrition BMI is routinely used in adultsand growth reference standards are used in children
Undernutrition in the UK
93
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
therefore from households in receipt of benefits) hadlower vitamin and mineral intakes (Buttriss 2002)
Similar findings have been reported from other large-scale surveys in the UK such as the Scottish HeartHealth Study in which the data were controlled forsmoking and education level (Bolton-Smith
et al
1991)and the 36-year follow-up to the National Birth CohortStudy (Braddon
et al
1988) The survey of nutrientintakes in Northern Ireland found similar nutrientdifferences by occupational social class (Barker
et al
1989) These findings are comparable with those fromsmaller surveys looking at nutrient intakes in differentsocioeconomic circumstances (Calvert
et al
1994Moynihan
et al
1993) including the homeless (Rushdenamp Wheeler 1993) A study by Dowler amp Calvert (1995)of nutrient intakes in lone-parent households showedthat where parents had lived for some time on incomesupport and particularly where they had fixed regulardeductions for debt recovery nutrient intakes were halfof the levels of those not living in such circumstances
In terms of dietary variety and overall dietary pat-terns those in poorer households consume less fruitjuice lean meat oily fish and wholemeal products andfewer salads and are more likely to eat white breadpotatoes cheaper fatty meats beans eggs and chips(Anderson amp Hunt 1992 Gregory
et al
1995Whichelow
et al
1991) Those on lower incomes have amuch less diverse food base so their diet is more likelyto lack variety
Many foods that are integral to a healthy diet are per-ceived as a luxury by those on low incomes and are anlsquoexpensiversquo form of energy such foods include fruitsvegetables and fish In addition many healthier alterna-tives carry a price premium
eg
wholemeal bread fatsand spreads low in saturates and lean meat However inaddition to price many factors influence the purchasingand consumption patterns in low-income householdswhich are related to their poor financial status such aslimited food preparation facilities Low income is alsooften associated with lack of knowledge and skillsrelated to food nutrition and cooking
Policies adopted by government local authorities andfood retailers can influence which foods are availableand accessible to people with low incomes For examplethere is the issue of price variability between shopsFood is generally more expensive in corner shops con-venience stores and small independent supermarketsthan in large supermarkets Piachaud amp Webb (1996)found that on average basic foodstuffs cost 24 morein small stores than in supermarkets taking super-market own brands into account the differences in costs
were 60 They calculated that people living in ahousehold on benefits would have to spend 25 moreof their income on food if they could not get to a largesupermarket or street market
Access to shopping facilities in areas where low-income households are concentrated is restricted interms of the physical difficulties or cost of travelling toshops and by a lack of choice of shops Thereforeaccess to a healthy diet becomes a particular problemfor low-income households The number of food retailoutlets is continually decreasing mainly at the expenseof shops such as small grocery retailers butchers fish-mongers and greengrocers The number of large retailoutlets has also decreased mainly because of theincrease in the number of superstores located on the out-skirts of towns and designed for access primarily by carEconomies of scale allow food sold in supermarkets tobe cheaper and cover a wider range than that in smallerhigh street stores The 1998 Independent Inquiry intoInequalities in Health report (Acheson 1998) foundparadoxically that a basket of food cost more in dis-advantaged areas than in affluent areas
The price of a healthy diet and the variation betweenprices of some foods is therefore of major concern forthose living on low incomes Many of the poorest peoplein the UK are concentrated in local authority housing ininner cities and there is evidence to suggest a continuinggeographical polarisation of income inequalities Inmany of these areas shops and banks have withdrawnpartly because the residents spend so little and partlybecause of the retail concentration in superstores(defined as having a total floor surface area of more than7620 m
2
) designed primarily for car access The risein vandalism is another contributing factor In a bidto resolve these problems the supermarket chainSomerfield operates a policy of maintaining small- andmedium-sized high street shops to serve local commu-nities and not to build large out-of town superstoresMany deprived sectors of society suffer from a lack ofaccess to good shopping facilities and in particularfresh fruit and vegetables To avoid these lsquofresh fooddesertsrsquo Somerfield opted to offer a free delivery serviceto village shops and small local stores Unfortunatelythe company had to close some of these small stores insome areas due to vandalism
312 Social and physical factors
Some of the social factors that influence food choice andeating patterns are listed below
94
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Figure 1
Guidelines for estimating the approximate energy and nitrogen requirements for an adult patient receiving artificial nutritional support Reproduced from Garrow
et al
2000 Reproduced with permission from Elsevier
bull Budgeting skillsbull Cultural traditionsbull Religious beliefsbull Educationbull Nutritional knowledgebull Lack of cooking facilities
eg
families housed in bed-and-breakfast accommodationbull Habitsbull Likes and dislikesbull Previous food experiencebull Willingness to experimentbull Time availablebull Eating alonebull Depressionbull Bereavement
For example a recently widowed man may not only besuffering the effects of bereavement and depressionwhich are likely to reduce appetite but he may also sud-denly find himself having to cope alone If his wife hadalways been responsible for shopping cooking and pro-viding food the widower may have difficulty budgetingfor food preparing and cooking food and may find thenew experience of eating alone all too painful
Poor dentition is another factor The NDNS of peopleaged 65 years and over (Finch
et al
1998) reported thatpeople with no natural teeth or few natural teeth ate amore restricted range of foods influenced by their per-ceived inability to chew The survey showed an associ-ation between oral function and nutrient intake andnutritional status Subjects without their own teeth wereless likely to choose foods that need chewing such asfruit and vegetables had lower intakes of iron vitaminsC and E and retinol and had lower plasma levels of vita-min C This was particularly true of those who lived invarious forms of residential care Physical disabilitiesalso influence a personrsquos ability to shop prepare andcook food Something as simple as opening a can ofbaked beans is far from simple for someone witharthritic hands
32 Effect of disease on nutritional status
321 The nutritional requirements of illness
Tissue repair imposes demands on nutritional supplyand an increased activity of body defence mechanismsmay also increase nutritional needs Despite this illhealth is often associated with a decreased desire forfood and decreased nutritional intake
Various changes in the metabolism of carbohydratefat and protein can be observed in illness Proportionalto the severity of illness there is an increase in the bodyrsquosenergy requirement and also an increase in urinarynitrogen loss (Cuthbertson 1980) The scale of thesechanges can be seen in Fig 1 This response to illnesshas been termed a stress response and the state ofincreased energy and protein needs a hypermetabolicstate
The metabolic response to illness traditionally hasthree phases ebb flow and anabolic although these canbe moderated with drug treatment The ebb phase onlylasts for a few hours and there is a depression of meta-bolic function and a reduction in energy expenditure In
Undernutrition in the UK
95
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
the flow phase metabolic rate increases and energyreserves in the form of fat stores are mobilised Visceraland muscle tissue provide amino acids that can be usedfor gluconeogenesis providing glucose for the brain andred blood cells and for wound-healing mechanismsHormonal changes appear to be important determinantsof the stress response Simply stated insulin stimulatesglucose uptake and metabolism and glycogen fat andprotein synthesis During starvation insulin levels arelow and other hormones are effective in mobilisingbody stores (
ie
promote glycogen fat and proteinbreakdown and stimulate gluconeogenesis and ketoge-nesis) In the stress response there is an increased secre-tion of catabolic hormones Especially important arethe glucocorticoids catecholamines and glucagon Theactions of insulin seem to be opposed by the catabolichormones leading to a state of insulin resistance(Cuthbertson 1980)
Another fundamental event is the production of themediator interleukin-1 a polypeptide produced byphagocytic cells (white blood cells that help fight infec-tion) A number of direct effects collectively termed theacute-phase response are ascribed to interleukin-1These include fever which is one of the strategies thebody uses to fight infection and the induction of muscleprotein breakdown leading to increased blood levels ofthe acute-phase proteins prealbumin retinol-bindingprotein (RBP) and C-reactive protein (Casati
et al
1998)
In simple starvation the breakdown of body fat isreversed by feeding with glucose In the hypermetabolicpatient it is found that fat breakdown continues despitegiving glucose and that gluconeogenesis and glucoseoxidation also occur at increased rates Hence theincreased gluconeogenesis can increase the amount ofcarbohydrate that is required to obviate protein break-down Achievement of energy balance fails to alleviatecatabolism in critically ill patients Therefore provisionof energy intake to match energy expenditure is unnec-essary during the flow phase and may even be unhelpful(Frankenfield
et al
1997)The increased nitrogen loss observed in stressed
patients can be accounted for by both a depression ofprotein synthesis and an increase in the rate of proteinbreakdown Provision of adequate protein stimulatesprotein synthesis but it also stimulates breakdown(Campbell 1999)
In the anabolic phase catabolism eventually declinesand is coupled with an increase in appetite and ability tomove This phase provides the opportunity for nutri-tional therapy to restore muscle mass and increase pro-tein synthesis
33 Reaching hospital
On reaching hospital dietary intake may be furtherreduced by one or more of the following problems
bull Confusionbull Fearbull Depressionbull Dysphagia (inability or reduced ability to swallow)bull Loss of appetite taste smell or thirstbull Poor dentitionbull Constipation which is caused by reduced mobilityand the fear that eating will make it worsebull Discomfortbull Dislike of the type of food availablebull Difference in routine and meal patternbull Problems with feedingbull Lack of staff available to help with feeding
Key points
Factors influencing poor dietary intake includebull loss of appetitebull disease or recurrent illness and consequenttreatmentbull impaired ability to absorb or utilise nutrientsbull poverty resulting in lack of car ownership or alter-native transport leading to limited access to bulk buy-ing low-cost foodbull poor housing with poor food storage and prepara-tion facilitiesbull problems of shopping and lack of preparation andcooking skillsbull less education leading to less knowledge and moti-vation to make healthy diet choicesbull unemployment so there is less money available forexpenditure on foodbull social isolation depression and bereavement lowself-esteem
4 Extent of the problem of undernutrition
Undernutrition among patients in UK hospitals wasdocumented in the mid-1970s (Bistrian
et al
1974 Hill
et al
1977) and it remains a common and often unrec-ognised problem that contributes to patient morbidityand mortality (Lennard-Jones 1992 McWhirter ampPennington 1994 Potter
et al
1998)
96
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Many studies over the last 30 years have since empha-sised the presence of disease-related undernutrition inhospitalised patients (Bistrian
et al
1974 Corish
et al
2000 Hill
et al
1977 Kelly
et al
2000 McWhirter ampPennington 1994) However there is controversy aboutits exact prevalence in the hospital setting One of themajor reasons for this is that there is no universal agree-ment about the definition of undernutrition Becausevarious workers have used different criteria to screen forundernutrition the reported magnitude of the problemhas been highly variable ranging from 10 to 60
Corish
et al
(2000) have screened for undernutritionin patients admitted to two teaching hospitals in DublinTo ensure more reliable comparisons they used thesame criteria employed by McWhirter amp Pennington(1994) in a Dundee hospital 6 years earlier In both stud-ies patients were classified as undernourished if theyhad a BMI
lt
20 kgm
2
and a triceps skinfold thicknessor mid-arm muscle circumference (MAMC) below the15th percentile The incidence of undernutrition innewly admitted patients in Dublin was reported to bemore than threefold lower (11) than in Dundee(40)
This striking difference has led other experts in thefield to question the criteria for defining undernutritionElia amp Stratton (2000) suggest that anthropometric cut-off values should not be used as a diagnostic label ofundernutrition but rather to classify an individualrsquosrisk of undernutrition Some healthy subjects have aBMI
lt
20 kgm2 (especially young adults) and are per-fectly well In addition anthropometric criteria alonesuggest a chronic protein-energy deficiency status How-ever a patient showing substantial recent weight loss(eg greater than 10 weight loss over 3ndash6 months) isat risk of undernutrition and impaired bodily functionseven though the anthropometric cut-off values may nothave been reached
The standard data used for anthropometry requireregular review so that they achieve the right balancebetween reflecting what is the norm (which may not bedesirable) and what is desirable (which may not beappropriate to the current generation) Unlike BMIwhich is a fixed criterion percentile values can showsubstantial change over time For example the referencevalues provided by Bishop et al (1981) for arm anthro-pometry were established in the USA about 30 yearsago The secular trends in obesity over that period meanthat these reference values may no longer apply Fur-thermore the choice of the percentile cut-off for use aspart of the screening tool to classify patients as under-nourished may be inappropriately high (since 15 ofthe reference population falls below this cut-off)
While the picture may be incomplete with regard tothe prevalence of undernutrition in hospitals it is clearthat disease-related undernutrition remains a significantclinical problem in hospitals
However the problem of disease-related undernutri-tion is not confined to people in hospital Within thecommunity up to 10 of people with cancer or otherchronic diseases may be significantly malnourished(Edington et al 1996) and many elderly people are alsoat high risk of undernutrition As a result people arecommonly admitted to hospital nutritionally depletedIn a study conducted in four hospitals in EnglandEdington et al (2000) found that one in every fivepatients admitted was malnourished Patients wereassessed using anthropometric measurements and BMIand by recording history of unintentional weight lossThis figure is likely to be an underestimate because it didnot include those who were too ill on admission to beassessed Kelly et al (2000) estimated that undernutri-tion among acute hospital admissions goes unrecognisedin 70 of cases
Once in hospital undernutrition is likely to get worseIn the study by McWhirter and Pennington two-thirdsof the 500 patients who had been assessed on admis-sion and were reassessed on discharge had lost weightA study on a random sample of 150 in-patients foundapproximately half of them to be either at moderate riskor high risk of undernutrition (Reilly et al 1995) Theprevalence and level of risk is probably higher amonghigh dependency medical surgical geriatric and paedi-atric patients (Reilly et al 1995) As illness and hospi-talisation are frequently associated with weight lossdeterioration in nutritional status is inevitable unlessaction is taken to prevent it
Key points
bull It is estimated that 70 of all undernutrition in theUK goes unrecognised and untreatedbull In the community 5 of the population have aBMI lt 20 kgm2 In hospitals this figure is 20ndash25bull It is estimated that 40 of adults and 15 of chil-dren admitted to hospital are malnourished half ofthese severely so and many others become malnour-ished during their stay in hospitalbull It is estimated that at any one time approximately66 of hospital patients are malnourished
Undernutrition in the UK 97
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
5 Cost of the problem of undernutrition
Undernutrition primarily results in loss of body tissue(depletion of body fat stores and muscle wasting) How-ever because nutrient intake is so closely correlatedwith energy intake a deficiency of energy is likely toresult in an inadequate intake of protein vitamins min-erals and trace elements This can cause widespreadmetabolic physiological and functional effects whichmay include
bull Impaired immune function and hence increased sus-ceptibility to infection and sepsis Infection will furtherimpair a malnourished statebull Delayed wound healingbull Increased risk of pressure sores particularly due toloss of cushioning fat storesbull Muscle wasting and weakness which may affect
ndash Respiratory function impaired respiratory musclestrength makes it difficult for a patient to cough andexpectorate effectively so increasing the risk of chestinfection It may also be more difficult to wean apatient off a ventilatorndash Cardiac function this may be impaired resulting inreduced cardiac output and risk of heart failurendash Mobility weakness of skeletal muscles delays areturn to full mobility Reduced mobility increases therisk of thromboembolism and bedsores
bull Altered structure of the small intestine which mayresult in malabsorptionbull Increased risk of postoperative complicationsbull Apathy and depression leading to loss of morale andreduced will to recoverbull General sense of weakness and illness which impairsappetite and physical ability to eat and hence tends toperpetuate and worsen any undernutrition
In summary undernutrition causes considerable mor-bidity delays recovery and increases the risk of death ABMI at or below the 15th percentile has been shown tobe a significant and independent predictor of death inseriously ill patients (Galanos et al 1997) There is alsoan economic cost in terms of increased need of nursingcare and extended hospital stay
There is clear evidence that correcting undernutritionhas many benefits (Potter et al 1998) Improvements inbody weight status and anthropometric parameters areassociated with improvement in immune function(Chandra 1992 Dionigi et al 1988) wound healing(Haydock amp Hill 1987) and muscle function (Fiataroneamp Evans 1993) and in clinical outcomes such asrecovery time and incidence of postoperativecomplications
Hospitals spend approximately pound15 billion on foodannually and studies conducted in one hospital foundthat 30ndash40 of food is discarded (Kelly 1999) This isconsistent with national estimates that 30ndash50 of hos-pital food is wasted with a monetary value calculated tobe pound45 million each year (Edwards amp Nash 1997Fenton et al 1995) With the inclusion of labour andoverheads this cost rises to pound144 million annuallyThere is also the hidden cost of the extra ill health asso-ciated with undernutrition Some hospitals also typicallyspend approximately pound800 000 on enteral andparenteral nutrition (see Sections 92 and 93) TheKingrsquos Fund (1992) report calculated that provision ofcomprehensive nutrition support would result in a 5-day reduction in hospital stay for approximately 10of patients The consequent saving was estimated to bepound266 million annually in the UK A review conducted byBond (1997) in the USA showed a clear relationshipbetween undernutrition and prolonged hospital stayWhen nutritional intervention was introduced 2 daysearlier than usual the result was a 1-day shortening ofhospital stay It was calculated that a more aggressivenutritional intervention policy would save the averagehospital $1 million per year
Key points
bull Between 30 and 50 of hospital food is wastedbull On average food intake is less than 75 of thatrecommended particularly among the elderlybull The monetary value of hospital food wasted eachyear in England alone is calculated to be pound45 millionBy including labour and overheads this cost rises topound144 millionbull There is also the hidden cost of the extra ill healthassociated with undernutrition because it increasesthe risk of complications lowers resistance to infec-tion impairs physical and mental functioning anddelays recovery
6 Why the problem of undernutrition is exacerbated in hospitals
In more than 60 of patients nutritional status deteri-orates during their stay in hospital with those whoare malnourished on admission particularly affectedPennington (1998) demonstrated that progressive nutri-tional depletion occurs for up to 8 weeks after curativesurgery (eg a heart by-pass operation) This thereforeindicates the need to consider nutritional status fromonset of illness through to complete recovery including
98 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
time after discharge However undernutrition remainsundetected in the majority of patients affected becausemany clinicians and nurses still do not consider nutri-tion to be an important factor in the management of dis-ease (Schenker 2000) and so do not routinely monitornutritional status and body weight Economic analysishas demonstrated that appropriate nutritional treatmentis cost-effective but benefits will only be achieved withhigh standards of nutritional care Multi-professionalnutritional support teams best conduct such treatmentbut there is continuing evidence of poor practice anda high incidence of treatment-related complicationswhich negate the benefits of nutritional treatments(Schenker 2000) In the hospital or institutional settingtherefore the problems that cause undernutrition maybe compounded by the fact that nutritional consider-ations may receive little attention from medical andnursing staff Lack of awareness of the prognostic sig-nificance of undernutrition and lack of knowledgeamong doctors and nurses regarding its assessment andmanagement (Nightingale amp Reeves 1999) may meanthat it is neither looked for nor taken into account whentreatment priorities are being set In particular theremay be failure to
bull identify those with or at risk of nutritional depletionbull identify nutritional requirements especially whenthese are increased because of fever surgery or injurybull provide food of an appropriate quality compositionand consistencybull encourage food intake food is of no benefit if noteatenbull monitor what is actually consumed in some circum-stances direct observation of food and fluid consump-tion is essentialbull identify those whose nutritional needs are not beingmet (through regular weighing or the use of otheranthropometric measurements)bull correct inadequate intake
61 Hospital food and feeding
The following factors have been identified as causes forpoor dietary intake in hospital patients
611 Problems with ordering
bull Menus lack clarity dishes should be described accu-rately so that patients have a reasonable idea of what toexpectbull Help with ordering should be available (but in manycases is not) where there are problems with a patientrsquoscomprehension speech or language
bull Menus are often not printed in languages other thanEnglish This is a particular problem in areas with a highimmigrant population Illiteracy may limit usefulness oftranslated menus Verbal translation may be betterbull Ordering from the menu too far in advance A patientmay be discharged after they have ordered food for thenext day resulting in the bedrsquos new occupant receivingfood chosen by someone else which may be unsuitableSame day ordering systems reduce waste and encourageconsumptionbull Patientsrsquo orders are not checked to ensure that thefood received and the portions requested are correct Inthis respect ward hostesses or feeding care attendantsmay be helpful however this does have financialimplicationsbull Inefficient ordering systems and poor two-way com-munication between the wards and the catering depart-ment lead to waste eg food sent to patients who havebeen discharged transferred or have died Such trays arethen either wasted or given to another patient wholeaves most of it because it was not their choice
612 Menu choice
bull Menus do not always take account of the needs tastesand customary eating habits of different groups ofpatients These will vary according to age race or cul-ture or the disease processbull Menus often do not take account of those needingfortified andor modified-consistency mealsbull Inappropriate promotion of lsquohealthy eatingrsquo eglow-fat diets in undernourished or nutritionally at-riskpatientsbull Some elderly patients often adopt a grazing habit andrequire frequent small volume high energy densityfeeds and snacksbull Special needs Although some disease-specific menuseg for renal failure may be provided from a dietkitchen it may be cost-effective to be able to supplementthe standard menu with high-energy high-proteinadditionsbull Nutritional needs and appetites of children differfrom those of adults and also vary according to ageMeals should be made attractive to children
613 Appropriate food choices
bull Food suitable for lsquohealthy eatingrsquo by the overweightpatient with cardiovascular disease is inappropriate forthe depleted malnourished patientbull Pureacuteed or semisolid diets are required by patientswith neurological or mechanical dysphagia who may be
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

Undernutrition in the UK
91
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
hospital stay In some patients undernutrition may bethe main condition that precipitates hospital admissionTrials of nutritional intervention by oral or artificialmeans have shown that in many patients the clinicalconsequences of undernutrition can be avoided orreversed by appropriate nutritional care (Beier-Holgersen amp Boesby 1996 Keele
et al
1995 Larsson
et al
1990 Rana
et al
1992)
2 Definition and classification of undernutrition
Undernutrition can be defined as a disturbance of formor function arising from the deficiency of one or morenutrients Undernutrition can be mild or severe helpful(if it results in appropriate weight loss in someone whois obese) or dangerous Weight loss is a manifestation ofenergy depletion The least essential tissues suffer firstthe adipose tissue cells lose fat which is oxidised to pro-vide energy Essential nutrients protein and micronutri-ents are likely to be depleted at the same time The bodystores of some micronutrients are large while require-ments for others are lower when energy intake isreduced In children who have relatively higher proteinrequirements than adults serious depletion of proteinaccompanies undernutrition
The consequences of protein depletion are apparent intwo main ways somatic protein depletion ndash the loss oftissue as general wasting of muscles and visceral proteindepletion ndash protein loss from the liver pancreas and gutWhen protein is lost from skeletal muscle the musclefibres shrink and the spaces between them are filled withan extracellular watery gel In older people some of theexcess fluid collects in the legs during the day as oedemaIf the loss is not too severe the oedema will disappearwhen the person lies down
In undernutrition the skeleton retains its outward sizeand shape but the fatty marrow disappears and isreplaced with aqueous material The skin loses proteinand becomes easily infected this with the loss of sub-cutaneous fat gives it a loose hanging appearance Theinternal organs particularly the liver lose mass Theheart and kidneys tend to lose mass in parallel withthe rest of the body but the brain retains its size andstructure The gut becomes thin and weight is lost fromboth muscle and mucosa
In spite of these structural changes organ functionand body systems remain normal until a great deal ofweight has been lost The resting metabolic rate per kilo-gram body weight is not greatly reduced in moderateundernutrition but in starvation both metabolic rateand body temperature fall Pulse rate and arterial blood
pressure are low in undernutrition as the body adaptsphysiologically In moderate undernutrition the gutfunctions normally provided there is no infection butin severe undernutrition diarrhoea can be severe (evenwithout infection) and the resulting dehydration canprove fatal
The presence of undernutrition in adults is assessed interms of degrees of weight loss An easy (but not thebest) index is body mass index (BMI) (see Section 833)defined as weight (in kilograms) divided by the square ofthe height (in metres)
ie
weightheight
2
Table 1 givesvalues for defining adult grades of undernutrition
The most sensitive indicator of undernutrition in chil-dren is failure to achieve normal growth compared witha lsquonormalrsquo reference growth rate for the age and sex ofthe child Progression of growth is an important param-eter and can be assessed in terms of height and weightor in infants weight and head circumference in relationto reference standards for age New reference standards(Freeman
et al
1995) have been published to replacethose compiled in the 1950s which take into accountthe upward shift in the average weight and height ofchildren in recent decades However a number of diffi-culties are associated with the use of these data Firstlychildren who cross centiles but never actually reach thecut-off centile defining failure to thrive are not identi-fied For example infants considered large at birthmight fail to grow but because they do not reach thecut-off centile failure to thrive will not be diagnosedSecondly infancy is naturally a period of centile crossing(large for gestational age infants grow more slowly thanthose of small for gestational age) So identifying failureto thrive depends on being able to distinguish poorgrowth from natural changes in growth rate To addressthis problem Cole (1997) has developed a chart thatcan be used to detect growth faltering over any period of4 weeks or longer
Table 1
Classification of undernutrition in adults by body mass index (BMI)
BMI (kgm
2
) Classification
gt
20 Normal185ndash20 Marginal undernutrition17ndash185 Mild undernutrition16ndash17 Moderate undernutrition
lt
16 Severe undernutrition
92
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
3 Causes of undernutrition
Undernutrition is the consequence of a dietary intakethat does not meet nutritional needs and may resultfrom one or more of the following decreased dietaryintake increased nutritional requirementslossesimpaired ability to absorb or utilise nutrients
Undernutrition usually has a slow onset resultingfrom periods of weeks or months when intake has notmatched requirements However in conditions of acutemetabolic stress where nutritional demands are highutilisation of energy and nutrients are disturbed andoral intake is likely to be compromised nutritionaldepletion can occur rapidly and be severe
Many factors can impair dietary intake Theseinclude
bull difficulties with shopping (both access and affordabil-ity) andor preparing cooking or eating food resultingfrom illness lack of mobility or povertybull reduced appetite as a result of the effects of illness orassociated anxiety or depressionbull symptoms associated with a disease or its treatment
eg
nausea vomiting sore mouth abdominal discom-fort or diarrhoeabull lack of interest in food as a result of social isolationsignificant life change (such as bereavement) or mentalillnessbull inadequate or unappetising meals or the provision ofinappropriate foodbull repeated fasting for diagnostic or treatmentproceduresbull problems associated with skipping mealsbull difficulties with eating or chewing
eg
ill-fitting den-tures or poor oral hygiene
bull swallowing difficultiesbull difficulty with self-feeding (
eg
owing to disability ordisorders such as Parkinsonrsquos disease) or inadequatehelp given to those unable to self-feedbull sedation semiconsciousness or coma
These factors can be separated into effects of lifestyleand effects of disease and consequent treatment and areexplored in greater detail below
31 Causes in the community
In this briefing paper causes in the community are con-fined to those undernourished individuals who mayhave previously been patients in hospital and have beendischarged while undernourished or people with onsetof a disease that has yet to be diagnosed or treated andwill enter hospital in due course
311 Poverty
One in four of the UK population nearly 14 millionpeople live in households with incomes below theEuropean poverty line of half the average incomeApproximately 96 million of these people are in house-holds that receive income support and the remainderlive on low or insecure wages Diets in low-incomehouseholds are characterised by less dietary varietywhich is itself associated with poorer nutrient profiles
National Food Survey results have consistently shownlower nutrient intakes in the lowest income groups com-pared to the highest In addition the Dietary and Nutri-tional Survey of British adults (Gregory
et al
1990)found that men and women who were unemployed orliving in households claiming benefit or in social classesIV and V had significantly lower intakes of many vita-mins (especially vitamin C
b
-carotene and vitamin E)and minerals (especially iron) than people not in thesecategories Data from the new NDNS of adults can befound on the FSA website (httpwwwfoodgovuk)
In the National Diet and Nutrition Survey (NDNS) ofyoung children (Gregory
et al
1995) those from man-ual social classes or from less-advantaged homes (wherethe head of the household was unemployed or claimedbenefits) had lower intakes andor blood levels of
b
-carotene niacin vitamin C iron calcium phosphorusand potassium than those from non-manual or more-advantaged households Preschool children from single-parent families had lower levels of
b
-carotene andvitamin C In the NDNS of young people (Gregory
et al
2000) those who received free school meals (and were
Key points
bull Moderate undernutrition leads to fat loss generalwasting of muscles and loss of protein from internalorgansbull Internal organs can function normally in moderateundernutrition but with severe undernutrition gutfunction breaks down causing malabsorption diar-rhoea and infection This can be fatalbull There are a number of methods for the assessmentof undernutrition BMI is routinely used in adultsand growth reference standards are used in children
Undernutrition in the UK
93
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
therefore from households in receipt of benefits) hadlower vitamin and mineral intakes (Buttriss 2002)
Similar findings have been reported from other large-scale surveys in the UK such as the Scottish HeartHealth Study in which the data were controlled forsmoking and education level (Bolton-Smith
et al
1991)and the 36-year follow-up to the National Birth CohortStudy (Braddon
et al
1988) The survey of nutrientintakes in Northern Ireland found similar nutrientdifferences by occupational social class (Barker
et al
1989) These findings are comparable with those fromsmaller surveys looking at nutrient intakes in differentsocioeconomic circumstances (Calvert
et al
1994Moynihan
et al
1993) including the homeless (Rushdenamp Wheeler 1993) A study by Dowler amp Calvert (1995)of nutrient intakes in lone-parent households showedthat where parents had lived for some time on incomesupport and particularly where they had fixed regulardeductions for debt recovery nutrient intakes were halfof the levels of those not living in such circumstances
In terms of dietary variety and overall dietary pat-terns those in poorer households consume less fruitjuice lean meat oily fish and wholemeal products andfewer salads and are more likely to eat white breadpotatoes cheaper fatty meats beans eggs and chips(Anderson amp Hunt 1992 Gregory
et al
1995Whichelow
et al
1991) Those on lower incomes have amuch less diverse food base so their diet is more likelyto lack variety
Many foods that are integral to a healthy diet are per-ceived as a luxury by those on low incomes and are anlsquoexpensiversquo form of energy such foods include fruitsvegetables and fish In addition many healthier alterna-tives carry a price premium
eg
wholemeal bread fatsand spreads low in saturates and lean meat However inaddition to price many factors influence the purchasingand consumption patterns in low-income householdswhich are related to their poor financial status such aslimited food preparation facilities Low income is alsooften associated with lack of knowledge and skillsrelated to food nutrition and cooking
Policies adopted by government local authorities andfood retailers can influence which foods are availableand accessible to people with low incomes For examplethere is the issue of price variability between shopsFood is generally more expensive in corner shops con-venience stores and small independent supermarketsthan in large supermarkets Piachaud amp Webb (1996)found that on average basic foodstuffs cost 24 morein small stores than in supermarkets taking super-market own brands into account the differences in costs
were 60 They calculated that people living in ahousehold on benefits would have to spend 25 moreof their income on food if they could not get to a largesupermarket or street market
Access to shopping facilities in areas where low-income households are concentrated is restricted interms of the physical difficulties or cost of travelling toshops and by a lack of choice of shops Thereforeaccess to a healthy diet becomes a particular problemfor low-income households The number of food retailoutlets is continually decreasing mainly at the expenseof shops such as small grocery retailers butchers fish-mongers and greengrocers The number of large retailoutlets has also decreased mainly because of theincrease in the number of superstores located on the out-skirts of towns and designed for access primarily by carEconomies of scale allow food sold in supermarkets tobe cheaper and cover a wider range than that in smallerhigh street stores The 1998 Independent Inquiry intoInequalities in Health report (Acheson 1998) foundparadoxically that a basket of food cost more in dis-advantaged areas than in affluent areas
The price of a healthy diet and the variation betweenprices of some foods is therefore of major concern forthose living on low incomes Many of the poorest peoplein the UK are concentrated in local authority housing ininner cities and there is evidence to suggest a continuinggeographical polarisation of income inequalities Inmany of these areas shops and banks have withdrawnpartly because the residents spend so little and partlybecause of the retail concentration in superstores(defined as having a total floor surface area of more than7620 m
2
) designed primarily for car access The risein vandalism is another contributing factor In a bidto resolve these problems the supermarket chainSomerfield operates a policy of maintaining small- andmedium-sized high street shops to serve local commu-nities and not to build large out-of town superstoresMany deprived sectors of society suffer from a lack ofaccess to good shopping facilities and in particularfresh fruit and vegetables To avoid these lsquofresh fooddesertsrsquo Somerfield opted to offer a free delivery serviceto village shops and small local stores Unfortunatelythe company had to close some of these small stores insome areas due to vandalism
312 Social and physical factors
Some of the social factors that influence food choice andeating patterns are listed below
94
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Figure 1
Guidelines for estimating the approximate energy and nitrogen requirements for an adult patient receiving artificial nutritional support Reproduced from Garrow
et al
2000 Reproduced with permission from Elsevier
bull Budgeting skillsbull Cultural traditionsbull Religious beliefsbull Educationbull Nutritional knowledgebull Lack of cooking facilities
eg
families housed in bed-and-breakfast accommodationbull Habitsbull Likes and dislikesbull Previous food experiencebull Willingness to experimentbull Time availablebull Eating alonebull Depressionbull Bereavement
For example a recently widowed man may not only besuffering the effects of bereavement and depressionwhich are likely to reduce appetite but he may also sud-denly find himself having to cope alone If his wife hadalways been responsible for shopping cooking and pro-viding food the widower may have difficulty budgetingfor food preparing and cooking food and may find thenew experience of eating alone all too painful
Poor dentition is another factor The NDNS of peopleaged 65 years and over (Finch
et al
1998) reported thatpeople with no natural teeth or few natural teeth ate amore restricted range of foods influenced by their per-ceived inability to chew The survey showed an associ-ation between oral function and nutrient intake andnutritional status Subjects without their own teeth wereless likely to choose foods that need chewing such asfruit and vegetables had lower intakes of iron vitaminsC and E and retinol and had lower plasma levels of vita-min C This was particularly true of those who lived invarious forms of residential care Physical disabilitiesalso influence a personrsquos ability to shop prepare andcook food Something as simple as opening a can ofbaked beans is far from simple for someone witharthritic hands
32 Effect of disease on nutritional status
321 The nutritional requirements of illness
Tissue repair imposes demands on nutritional supplyand an increased activity of body defence mechanismsmay also increase nutritional needs Despite this illhealth is often associated with a decreased desire forfood and decreased nutritional intake
Various changes in the metabolism of carbohydratefat and protein can be observed in illness Proportionalto the severity of illness there is an increase in the bodyrsquosenergy requirement and also an increase in urinarynitrogen loss (Cuthbertson 1980) The scale of thesechanges can be seen in Fig 1 This response to illnesshas been termed a stress response and the state ofincreased energy and protein needs a hypermetabolicstate
The metabolic response to illness traditionally hasthree phases ebb flow and anabolic although these canbe moderated with drug treatment The ebb phase onlylasts for a few hours and there is a depression of meta-bolic function and a reduction in energy expenditure In
Undernutrition in the UK
95
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
the flow phase metabolic rate increases and energyreserves in the form of fat stores are mobilised Visceraland muscle tissue provide amino acids that can be usedfor gluconeogenesis providing glucose for the brain andred blood cells and for wound-healing mechanismsHormonal changes appear to be important determinantsof the stress response Simply stated insulin stimulatesglucose uptake and metabolism and glycogen fat andprotein synthesis During starvation insulin levels arelow and other hormones are effective in mobilisingbody stores (
ie
promote glycogen fat and proteinbreakdown and stimulate gluconeogenesis and ketoge-nesis) In the stress response there is an increased secre-tion of catabolic hormones Especially important arethe glucocorticoids catecholamines and glucagon Theactions of insulin seem to be opposed by the catabolichormones leading to a state of insulin resistance(Cuthbertson 1980)
Another fundamental event is the production of themediator interleukin-1 a polypeptide produced byphagocytic cells (white blood cells that help fight infec-tion) A number of direct effects collectively termed theacute-phase response are ascribed to interleukin-1These include fever which is one of the strategies thebody uses to fight infection and the induction of muscleprotein breakdown leading to increased blood levels ofthe acute-phase proteins prealbumin retinol-bindingprotein (RBP) and C-reactive protein (Casati
et al
1998)
In simple starvation the breakdown of body fat isreversed by feeding with glucose In the hypermetabolicpatient it is found that fat breakdown continues despitegiving glucose and that gluconeogenesis and glucoseoxidation also occur at increased rates Hence theincreased gluconeogenesis can increase the amount ofcarbohydrate that is required to obviate protein break-down Achievement of energy balance fails to alleviatecatabolism in critically ill patients Therefore provisionof energy intake to match energy expenditure is unnec-essary during the flow phase and may even be unhelpful(Frankenfield
et al
1997)The increased nitrogen loss observed in stressed
patients can be accounted for by both a depression ofprotein synthesis and an increase in the rate of proteinbreakdown Provision of adequate protein stimulatesprotein synthesis but it also stimulates breakdown(Campbell 1999)
In the anabolic phase catabolism eventually declinesand is coupled with an increase in appetite and ability tomove This phase provides the opportunity for nutri-tional therapy to restore muscle mass and increase pro-tein synthesis
33 Reaching hospital
On reaching hospital dietary intake may be furtherreduced by one or more of the following problems
bull Confusionbull Fearbull Depressionbull Dysphagia (inability or reduced ability to swallow)bull Loss of appetite taste smell or thirstbull Poor dentitionbull Constipation which is caused by reduced mobilityand the fear that eating will make it worsebull Discomfortbull Dislike of the type of food availablebull Difference in routine and meal patternbull Problems with feedingbull Lack of staff available to help with feeding
Key points
Factors influencing poor dietary intake includebull loss of appetitebull disease or recurrent illness and consequenttreatmentbull impaired ability to absorb or utilise nutrientsbull poverty resulting in lack of car ownership or alter-native transport leading to limited access to bulk buy-ing low-cost foodbull poor housing with poor food storage and prepara-tion facilitiesbull problems of shopping and lack of preparation andcooking skillsbull less education leading to less knowledge and moti-vation to make healthy diet choicesbull unemployment so there is less money available forexpenditure on foodbull social isolation depression and bereavement lowself-esteem
4 Extent of the problem of undernutrition
Undernutrition among patients in UK hospitals wasdocumented in the mid-1970s (Bistrian
et al
1974 Hill
et al
1977) and it remains a common and often unrec-ognised problem that contributes to patient morbidityand mortality (Lennard-Jones 1992 McWhirter ampPennington 1994 Potter
et al
1998)
96
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Many studies over the last 30 years have since empha-sised the presence of disease-related undernutrition inhospitalised patients (Bistrian
et al
1974 Corish
et al
2000 Hill
et al
1977 Kelly
et al
2000 McWhirter ampPennington 1994) However there is controversy aboutits exact prevalence in the hospital setting One of themajor reasons for this is that there is no universal agree-ment about the definition of undernutrition Becausevarious workers have used different criteria to screen forundernutrition the reported magnitude of the problemhas been highly variable ranging from 10 to 60
Corish
et al
(2000) have screened for undernutritionin patients admitted to two teaching hospitals in DublinTo ensure more reliable comparisons they used thesame criteria employed by McWhirter amp Pennington(1994) in a Dundee hospital 6 years earlier In both stud-ies patients were classified as undernourished if theyhad a BMI
lt
20 kgm
2
and a triceps skinfold thicknessor mid-arm muscle circumference (MAMC) below the15th percentile The incidence of undernutrition innewly admitted patients in Dublin was reported to bemore than threefold lower (11) than in Dundee(40)
This striking difference has led other experts in thefield to question the criteria for defining undernutritionElia amp Stratton (2000) suggest that anthropometric cut-off values should not be used as a diagnostic label ofundernutrition but rather to classify an individualrsquosrisk of undernutrition Some healthy subjects have aBMI
lt
20 kgm2 (especially young adults) and are per-fectly well In addition anthropometric criteria alonesuggest a chronic protein-energy deficiency status How-ever a patient showing substantial recent weight loss(eg greater than 10 weight loss over 3ndash6 months) isat risk of undernutrition and impaired bodily functionseven though the anthropometric cut-off values may nothave been reached
The standard data used for anthropometry requireregular review so that they achieve the right balancebetween reflecting what is the norm (which may not bedesirable) and what is desirable (which may not beappropriate to the current generation) Unlike BMIwhich is a fixed criterion percentile values can showsubstantial change over time For example the referencevalues provided by Bishop et al (1981) for arm anthro-pometry were established in the USA about 30 yearsago The secular trends in obesity over that period meanthat these reference values may no longer apply Fur-thermore the choice of the percentile cut-off for use aspart of the screening tool to classify patients as under-nourished may be inappropriately high (since 15 ofthe reference population falls below this cut-off)
While the picture may be incomplete with regard tothe prevalence of undernutrition in hospitals it is clearthat disease-related undernutrition remains a significantclinical problem in hospitals
However the problem of disease-related undernutri-tion is not confined to people in hospital Within thecommunity up to 10 of people with cancer or otherchronic diseases may be significantly malnourished(Edington et al 1996) and many elderly people are alsoat high risk of undernutrition As a result people arecommonly admitted to hospital nutritionally depletedIn a study conducted in four hospitals in EnglandEdington et al (2000) found that one in every fivepatients admitted was malnourished Patients wereassessed using anthropometric measurements and BMIand by recording history of unintentional weight lossThis figure is likely to be an underestimate because it didnot include those who were too ill on admission to beassessed Kelly et al (2000) estimated that undernutri-tion among acute hospital admissions goes unrecognisedin 70 of cases
Once in hospital undernutrition is likely to get worseIn the study by McWhirter and Pennington two-thirdsof the 500 patients who had been assessed on admis-sion and were reassessed on discharge had lost weightA study on a random sample of 150 in-patients foundapproximately half of them to be either at moderate riskor high risk of undernutrition (Reilly et al 1995) Theprevalence and level of risk is probably higher amonghigh dependency medical surgical geriatric and paedi-atric patients (Reilly et al 1995) As illness and hospi-talisation are frequently associated with weight lossdeterioration in nutritional status is inevitable unlessaction is taken to prevent it
Key points
bull It is estimated that 70 of all undernutrition in theUK goes unrecognised and untreatedbull In the community 5 of the population have aBMI lt 20 kgm2 In hospitals this figure is 20ndash25bull It is estimated that 40 of adults and 15 of chil-dren admitted to hospital are malnourished half ofthese severely so and many others become malnour-ished during their stay in hospitalbull It is estimated that at any one time approximately66 of hospital patients are malnourished
Undernutrition in the UK 97
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
5 Cost of the problem of undernutrition
Undernutrition primarily results in loss of body tissue(depletion of body fat stores and muscle wasting) How-ever because nutrient intake is so closely correlatedwith energy intake a deficiency of energy is likely toresult in an inadequate intake of protein vitamins min-erals and trace elements This can cause widespreadmetabolic physiological and functional effects whichmay include
bull Impaired immune function and hence increased sus-ceptibility to infection and sepsis Infection will furtherimpair a malnourished statebull Delayed wound healingbull Increased risk of pressure sores particularly due toloss of cushioning fat storesbull Muscle wasting and weakness which may affect
ndash Respiratory function impaired respiratory musclestrength makes it difficult for a patient to cough andexpectorate effectively so increasing the risk of chestinfection It may also be more difficult to wean apatient off a ventilatorndash Cardiac function this may be impaired resulting inreduced cardiac output and risk of heart failurendash Mobility weakness of skeletal muscles delays areturn to full mobility Reduced mobility increases therisk of thromboembolism and bedsores
bull Altered structure of the small intestine which mayresult in malabsorptionbull Increased risk of postoperative complicationsbull Apathy and depression leading to loss of morale andreduced will to recoverbull General sense of weakness and illness which impairsappetite and physical ability to eat and hence tends toperpetuate and worsen any undernutrition
In summary undernutrition causes considerable mor-bidity delays recovery and increases the risk of death ABMI at or below the 15th percentile has been shown tobe a significant and independent predictor of death inseriously ill patients (Galanos et al 1997) There is alsoan economic cost in terms of increased need of nursingcare and extended hospital stay
There is clear evidence that correcting undernutritionhas many benefits (Potter et al 1998) Improvements inbody weight status and anthropometric parameters areassociated with improvement in immune function(Chandra 1992 Dionigi et al 1988) wound healing(Haydock amp Hill 1987) and muscle function (Fiataroneamp Evans 1993) and in clinical outcomes such asrecovery time and incidence of postoperativecomplications
Hospitals spend approximately pound15 billion on foodannually and studies conducted in one hospital foundthat 30ndash40 of food is discarded (Kelly 1999) This isconsistent with national estimates that 30ndash50 of hos-pital food is wasted with a monetary value calculated tobe pound45 million each year (Edwards amp Nash 1997Fenton et al 1995) With the inclusion of labour andoverheads this cost rises to pound144 million annuallyThere is also the hidden cost of the extra ill health asso-ciated with undernutrition Some hospitals also typicallyspend approximately pound800 000 on enteral andparenteral nutrition (see Sections 92 and 93) TheKingrsquos Fund (1992) report calculated that provision ofcomprehensive nutrition support would result in a 5-day reduction in hospital stay for approximately 10of patients The consequent saving was estimated to bepound266 million annually in the UK A review conducted byBond (1997) in the USA showed a clear relationshipbetween undernutrition and prolonged hospital stayWhen nutritional intervention was introduced 2 daysearlier than usual the result was a 1-day shortening ofhospital stay It was calculated that a more aggressivenutritional intervention policy would save the averagehospital $1 million per year
Key points
bull Between 30 and 50 of hospital food is wastedbull On average food intake is less than 75 of thatrecommended particularly among the elderlybull The monetary value of hospital food wasted eachyear in England alone is calculated to be pound45 millionBy including labour and overheads this cost rises topound144 millionbull There is also the hidden cost of the extra ill healthassociated with undernutrition because it increasesthe risk of complications lowers resistance to infec-tion impairs physical and mental functioning anddelays recovery
6 Why the problem of undernutrition is exacerbated in hospitals
In more than 60 of patients nutritional status deteri-orates during their stay in hospital with those whoare malnourished on admission particularly affectedPennington (1998) demonstrated that progressive nutri-tional depletion occurs for up to 8 weeks after curativesurgery (eg a heart by-pass operation) This thereforeindicates the need to consider nutritional status fromonset of illness through to complete recovery including
98 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
time after discharge However undernutrition remainsundetected in the majority of patients affected becausemany clinicians and nurses still do not consider nutri-tion to be an important factor in the management of dis-ease (Schenker 2000) and so do not routinely monitornutritional status and body weight Economic analysishas demonstrated that appropriate nutritional treatmentis cost-effective but benefits will only be achieved withhigh standards of nutritional care Multi-professionalnutritional support teams best conduct such treatmentbut there is continuing evidence of poor practice anda high incidence of treatment-related complicationswhich negate the benefits of nutritional treatments(Schenker 2000) In the hospital or institutional settingtherefore the problems that cause undernutrition maybe compounded by the fact that nutritional consider-ations may receive little attention from medical andnursing staff Lack of awareness of the prognostic sig-nificance of undernutrition and lack of knowledgeamong doctors and nurses regarding its assessment andmanagement (Nightingale amp Reeves 1999) may meanthat it is neither looked for nor taken into account whentreatment priorities are being set In particular theremay be failure to
bull identify those with or at risk of nutritional depletionbull identify nutritional requirements especially whenthese are increased because of fever surgery or injurybull provide food of an appropriate quality compositionand consistencybull encourage food intake food is of no benefit if noteatenbull monitor what is actually consumed in some circum-stances direct observation of food and fluid consump-tion is essentialbull identify those whose nutritional needs are not beingmet (through regular weighing or the use of otheranthropometric measurements)bull correct inadequate intake
61 Hospital food and feeding
The following factors have been identified as causes forpoor dietary intake in hospital patients
611 Problems with ordering
bull Menus lack clarity dishes should be described accu-rately so that patients have a reasonable idea of what toexpectbull Help with ordering should be available (but in manycases is not) where there are problems with a patientrsquoscomprehension speech or language
bull Menus are often not printed in languages other thanEnglish This is a particular problem in areas with a highimmigrant population Illiteracy may limit usefulness oftranslated menus Verbal translation may be betterbull Ordering from the menu too far in advance A patientmay be discharged after they have ordered food for thenext day resulting in the bedrsquos new occupant receivingfood chosen by someone else which may be unsuitableSame day ordering systems reduce waste and encourageconsumptionbull Patientsrsquo orders are not checked to ensure that thefood received and the portions requested are correct Inthis respect ward hostesses or feeding care attendantsmay be helpful however this does have financialimplicationsbull Inefficient ordering systems and poor two-way com-munication between the wards and the catering depart-ment lead to waste eg food sent to patients who havebeen discharged transferred or have died Such trays arethen either wasted or given to another patient wholeaves most of it because it was not their choice
612 Menu choice
bull Menus do not always take account of the needs tastesand customary eating habits of different groups ofpatients These will vary according to age race or cul-ture or the disease processbull Menus often do not take account of those needingfortified andor modified-consistency mealsbull Inappropriate promotion of lsquohealthy eatingrsquo eglow-fat diets in undernourished or nutritionally at-riskpatientsbull Some elderly patients often adopt a grazing habit andrequire frequent small volume high energy densityfeeds and snacksbull Special needs Although some disease-specific menuseg for renal failure may be provided from a dietkitchen it may be cost-effective to be able to supplementthe standard menu with high-energy high-proteinadditionsbull Nutritional needs and appetites of children differfrom those of adults and also vary according to ageMeals should be made attractive to children
613 Appropriate food choices
bull Food suitable for lsquohealthy eatingrsquo by the overweightpatient with cardiovascular disease is inappropriate forthe depleted malnourished patientbull Pureacuteed or semisolid diets are required by patientswith neurological or mechanical dysphagia who may be
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

92
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
3 Causes of undernutrition
Undernutrition is the consequence of a dietary intakethat does not meet nutritional needs and may resultfrom one or more of the following decreased dietaryintake increased nutritional requirementslossesimpaired ability to absorb or utilise nutrients
Undernutrition usually has a slow onset resultingfrom periods of weeks or months when intake has notmatched requirements However in conditions of acutemetabolic stress where nutritional demands are highutilisation of energy and nutrients are disturbed andoral intake is likely to be compromised nutritionaldepletion can occur rapidly and be severe
Many factors can impair dietary intake Theseinclude
bull difficulties with shopping (both access and affordabil-ity) andor preparing cooking or eating food resultingfrom illness lack of mobility or povertybull reduced appetite as a result of the effects of illness orassociated anxiety or depressionbull symptoms associated with a disease or its treatment
eg
nausea vomiting sore mouth abdominal discom-fort or diarrhoeabull lack of interest in food as a result of social isolationsignificant life change (such as bereavement) or mentalillnessbull inadequate or unappetising meals or the provision ofinappropriate foodbull repeated fasting for diagnostic or treatmentproceduresbull problems associated with skipping mealsbull difficulties with eating or chewing
eg
ill-fitting den-tures or poor oral hygiene
bull swallowing difficultiesbull difficulty with self-feeding (
eg
owing to disability ordisorders such as Parkinsonrsquos disease) or inadequatehelp given to those unable to self-feedbull sedation semiconsciousness or coma
These factors can be separated into effects of lifestyleand effects of disease and consequent treatment and areexplored in greater detail below
31 Causes in the community
In this briefing paper causes in the community are con-fined to those undernourished individuals who mayhave previously been patients in hospital and have beendischarged while undernourished or people with onsetof a disease that has yet to be diagnosed or treated andwill enter hospital in due course
311 Poverty
One in four of the UK population nearly 14 millionpeople live in households with incomes below theEuropean poverty line of half the average incomeApproximately 96 million of these people are in house-holds that receive income support and the remainderlive on low or insecure wages Diets in low-incomehouseholds are characterised by less dietary varietywhich is itself associated with poorer nutrient profiles
National Food Survey results have consistently shownlower nutrient intakes in the lowest income groups com-pared to the highest In addition the Dietary and Nutri-tional Survey of British adults (Gregory
et al
1990)found that men and women who were unemployed orliving in households claiming benefit or in social classesIV and V had significantly lower intakes of many vita-mins (especially vitamin C
b
-carotene and vitamin E)and minerals (especially iron) than people not in thesecategories Data from the new NDNS of adults can befound on the FSA website (httpwwwfoodgovuk)
In the National Diet and Nutrition Survey (NDNS) ofyoung children (Gregory
et al
1995) those from man-ual social classes or from less-advantaged homes (wherethe head of the household was unemployed or claimedbenefits) had lower intakes andor blood levels of
b
-carotene niacin vitamin C iron calcium phosphorusand potassium than those from non-manual or more-advantaged households Preschool children from single-parent families had lower levels of
b
-carotene andvitamin C In the NDNS of young people (Gregory
et al
2000) those who received free school meals (and were
Key points
bull Moderate undernutrition leads to fat loss generalwasting of muscles and loss of protein from internalorgansbull Internal organs can function normally in moderateundernutrition but with severe undernutrition gutfunction breaks down causing malabsorption diar-rhoea and infection This can be fatalbull There are a number of methods for the assessmentof undernutrition BMI is routinely used in adultsand growth reference standards are used in children
Undernutrition in the UK
93
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
therefore from households in receipt of benefits) hadlower vitamin and mineral intakes (Buttriss 2002)
Similar findings have been reported from other large-scale surveys in the UK such as the Scottish HeartHealth Study in which the data were controlled forsmoking and education level (Bolton-Smith
et al
1991)and the 36-year follow-up to the National Birth CohortStudy (Braddon
et al
1988) The survey of nutrientintakes in Northern Ireland found similar nutrientdifferences by occupational social class (Barker
et al
1989) These findings are comparable with those fromsmaller surveys looking at nutrient intakes in differentsocioeconomic circumstances (Calvert
et al
1994Moynihan
et al
1993) including the homeless (Rushdenamp Wheeler 1993) A study by Dowler amp Calvert (1995)of nutrient intakes in lone-parent households showedthat where parents had lived for some time on incomesupport and particularly where they had fixed regulardeductions for debt recovery nutrient intakes were halfof the levels of those not living in such circumstances
In terms of dietary variety and overall dietary pat-terns those in poorer households consume less fruitjuice lean meat oily fish and wholemeal products andfewer salads and are more likely to eat white breadpotatoes cheaper fatty meats beans eggs and chips(Anderson amp Hunt 1992 Gregory
et al
1995Whichelow
et al
1991) Those on lower incomes have amuch less diverse food base so their diet is more likelyto lack variety
Many foods that are integral to a healthy diet are per-ceived as a luxury by those on low incomes and are anlsquoexpensiversquo form of energy such foods include fruitsvegetables and fish In addition many healthier alterna-tives carry a price premium
eg
wholemeal bread fatsand spreads low in saturates and lean meat However inaddition to price many factors influence the purchasingand consumption patterns in low-income householdswhich are related to their poor financial status such aslimited food preparation facilities Low income is alsooften associated with lack of knowledge and skillsrelated to food nutrition and cooking
Policies adopted by government local authorities andfood retailers can influence which foods are availableand accessible to people with low incomes For examplethere is the issue of price variability between shopsFood is generally more expensive in corner shops con-venience stores and small independent supermarketsthan in large supermarkets Piachaud amp Webb (1996)found that on average basic foodstuffs cost 24 morein small stores than in supermarkets taking super-market own brands into account the differences in costs
were 60 They calculated that people living in ahousehold on benefits would have to spend 25 moreof their income on food if they could not get to a largesupermarket or street market
Access to shopping facilities in areas where low-income households are concentrated is restricted interms of the physical difficulties or cost of travelling toshops and by a lack of choice of shops Thereforeaccess to a healthy diet becomes a particular problemfor low-income households The number of food retailoutlets is continually decreasing mainly at the expenseof shops such as small grocery retailers butchers fish-mongers and greengrocers The number of large retailoutlets has also decreased mainly because of theincrease in the number of superstores located on the out-skirts of towns and designed for access primarily by carEconomies of scale allow food sold in supermarkets tobe cheaper and cover a wider range than that in smallerhigh street stores The 1998 Independent Inquiry intoInequalities in Health report (Acheson 1998) foundparadoxically that a basket of food cost more in dis-advantaged areas than in affluent areas
The price of a healthy diet and the variation betweenprices of some foods is therefore of major concern forthose living on low incomes Many of the poorest peoplein the UK are concentrated in local authority housing ininner cities and there is evidence to suggest a continuinggeographical polarisation of income inequalities Inmany of these areas shops and banks have withdrawnpartly because the residents spend so little and partlybecause of the retail concentration in superstores(defined as having a total floor surface area of more than7620 m
2
) designed primarily for car access The risein vandalism is another contributing factor In a bidto resolve these problems the supermarket chainSomerfield operates a policy of maintaining small- andmedium-sized high street shops to serve local commu-nities and not to build large out-of town superstoresMany deprived sectors of society suffer from a lack ofaccess to good shopping facilities and in particularfresh fruit and vegetables To avoid these lsquofresh fooddesertsrsquo Somerfield opted to offer a free delivery serviceto village shops and small local stores Unfortunatelythe company had to close some of these small stores insome areas due to vandalism
312 Social and physical factors
Some of the social factors that influence food choice andeating patterns are listed below
94
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Figure 1
Guidelines for estimating the approximate energy and nitrogen requirements for an adult patient receiving artificial nutritional support Reproduced from Garrow
et al
2000 Reproduced with permission from Elsevier
bull Budgeting skillsbull Cultural traditionsbull Religious beliefsbull Educationbull Nutritional knowledgebull Lack of cooking facilities
eg
families housed in bed-and-breakfast accommodationbull Habitsbull Likes and dislikesbull Previous food experiencebull Willingness to experimentbull Time availablebull Eating alonebull Depressionbull Bereavement
For example a recently widowed man may not only besuffering the effects of bereavement and depressionwhich are likely to reduce appetite but he may also sud-denly find himself having to cope alone If his wife hadalways been responsible for shopping cooking and pro-viding food the widower may have difficulty budgetingfor food preparing and cooking food and may find thenew experience of eating alone all too painful
Poor dentition is another factor The NDNS of peopleaged 65 years and over (Finch
et al
1998) reported thatpeople with no natural teeth or few natural teeth ate amore restricted range of foods influenced by their per-ceived inability to chew The survey showed an associ-ation between oral function and nutrient intake andnutritional status Subjects without their own teeth wereless likely to choose foods that need chewing such asfruit and vegetables had lower intakes of iron vitaminsC and E and retinol and had lower plasma levels of vita-min C This was particularly true of those who lived invarious forms of residential care Physical disabilitiesalso influence a personrsquos ability to shop prepare andcook food Something as simple as opening a can ofbaked beans is far from simple for someone witharthritic hands
32 Effect of disease on nutritional status
321 The nutritional requirements of illness
Tissue repair imposes demands on nutritional supplyand an increased activity of body defence mechanismsmay also increase nutritional needs Despite this illhealth is often associated with a decreased desire forfood and decreased nutritional intake
Various changes in the metabolism of carbohydratefat and protein can be observed in illness Proportionalto the severity of illness there is an increase in the bodyrsquosenergy requirement and also an increase in urinarynitrogen loss (Cuthbertson 1980) The scale of thesechanges can be seen in Fig 1 This response to illnesshas been termed a stress response and the state ofincreased energy and protein needs a hypermetabolicstate
The metabolic response to illness traditionally hasthree phases ebb flow and anabolic although these canbe moderated with drug treatment The ebb phase onlylasts for a few hours and there is a depression of meta-bolic function and a reduction in energy expenditure In
Undernutrition in the UK
95
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
the flow phase metabolic rate increases and energyreserves in the form of fat stores are mobilised Visceraland muscle tissue provide amino acids that can be usedfor gluconeogenesis providing glucose for the brain andred blood cells and for wound-healing mechanismsHormonal changes appear to be important determinantsof the stress response Simply stated insulin stimulatesglucose uptake and metabolism and glycogen fat andprotein synthesis During starvation insulin levels arelow and other hormones are effective in mobilisingbody stores (
ie
promote glycogen fat and proteinbreakdown and stimulate gluconeogenesis and ketoge-nesis) In the stress response there is an increased secre-tion of catabolic hormones Especially important arethe glucocorticoids catecholamines and glucagon Theactions of insulin seem to be opposed by the catabolichormones leading to a state of insulin resistance(Cuthbertson 1980)
Another fundamental event is the production of themediator interleukin-1 a polypeptide produced byphagocytic cells (white blood cells that help fight infec-tion) A number of direct effects collectively termed theacute-phase response are ascribed to interleukin-1These include fever which is one of the strategies thebody uses to fight infection and the induction of muscleprotein breakdown leading to increased blood levels ofthe acute-phase proteins prealbumin retinol-bindingprotein (RBP) and C-reactive protein (Casati
et al
1998)
In simple starvation the breakdown of body fat isreversed by feeding with glucose In the hypermetabolicpatient it is found that fat breakdown continues despitegiving glucose and that gluconeogenesis and glucoseoxidation also occur at increased rates Hence theincreased gluconeogenesis can increase the amount ofcarbohydrate that is required to obviate protein break-down Achievement of energy balance fails to alleviatecatabolism in critically ill patients Therefore provisionof energy intake to match energy expenditure is unnec-essary during the flow phase and may even be unhelpful(Frankenfield
et al
1997)The increased nitrogen loss observed in stressed
patients can be accounted for by both a depression ofprotein synthesis and an increase in the rate of proteinbreakdown Provision of adequate protein stimulatesprotein synthesis but it also stimulates breakdown(Campbell 1999)
In the anabolic phase catabolism eventually declinesand is coupled with an increase in appetite and ability tomove This phase provides the opportunity for nutri-tional therapy to restore muscle mass and increase pro-tein synthesis
33 Reaching hospital
On reaching hospital dietary intake may be furtherreduced by one or more of the following problems
bull Confusionbull Fearbull Depressionbull Dysphagia (inability or reduced ability to swallow)bull Loss of appetite taste smell or thirstbull Poor dentitionbull Constipation which is caused by reduced mobilityand the fear that eating will make it worsebull Discomfortbull Dislike of the type of food availablebull Difference in routine and meal patternbull Problems with feedingbull Lack of staff available to help with feeding
Key points
Factors influencing poor dietary intake includebull loss of appetitebull disease or recurrent illness and consequenttreatmentbull impaired ability to absorb or utilise nutrientsbull poverty resulting in lack of car ownership or alter-native transport leading to limited access to bulk buy-ing low-cost foodbull poor housing with poor food storage and prepara-tion facilitiesbull problems of shopping and lack of preparation andcooking skillsbull less education leading to less knowledge and moti-vation to make healthy diet choicesbull unemployment so there is less money available forexpenditure on foodbull social isolation depression and bereavement lowself-esteem
4 Extent of the problem of undernutrition
Undernutrition among patients in UK hospitals wasdocumented in the mid-1970s (Bistrian
et al
1974 Hill
et al
1977) and it remains a common and often unrec-ognised problem that contributes to patient morbidityand mortality (Lennard-Jones 1992 McWhirter ampPennington 1994 Potter
et al
1998)
96
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Many studies over the last 30 years have since empha-sised the presence of disease-related undernutrition inhospitalised patients (Bistrian
et al
1974 Corish
et al
2000 Hill
et al
1977 Kelly
et al
2000 McWhirter ampPennington 1994) However there is controversy aboutits exact prevalence in the hospital setting One of themajor reasons for this is that there is no universal agree-ment about the definition of undernutrition Becausevarious workers have used different criteria to screen forundernutrition the reported magnitude of the problemhas been highly variable ranging from 10 to 60
Corish
et al
(2000) have screened for undernutritionin patients admitted to two teaching hospitals in DublinTo ensure more reliable comparisons they used thesame criteria employed by McWhirter amp Pennington(1994) in a Dundee hospital 6 years earlier In both stud-ies patients were classified as undernourished if theyhad a BMI
lt
20 kgm
2
and a triceps skinfold thicknessor mid-arm muscle circumference (MAMC) below the15th percentile The incidence of undernutrition innewly admitted patients in Dublin was reported to bemore than threefold lower (11) than in Dundee(40)
This striking difference has led other experts in thefield to question the criteria for defining undernutritionElia amp Stratton (2000) suggest that anthropometric cut-off values should not be used as a diagnostic label ofundernutrition but rather to classify an individualrsquosrisk of undernutrition Some healthy subjects have aBMI
lt
20 kgm2 (especially young adults) and are per-fectly well In addition anthropometric criteria alonesuggest a chronic protein-energy deficiency status How-ever a patient showing substantial recent weight loss(eg greater than 10 weight loss over 3ndash6 months) isat risk of undernutrition and impaired bodily functionseven though the anthropometric cut-off values may nothave been reached
The standard data used for anthropometry requireregular review so that they achieve the right balancebetween reflecting what is the norm (which may not bedesirable) and what is desirable (which may not beappropriate to the current generation) Unlike BMIwhich is a fixed criterion percentile values can showsubstantial change over time For example the referencevalues provided by Bishop et al (1981) for arm anthro-pometry were established in the USA about 30 yearsago The secular trends in obesity over that period meanthat these reference values may no longer apply Fur-thermore the choice of the percentile cut-off for use aspart of the screening tool to classify patients as under-nourished may be inappropriately high (since 15 ofthe reference population falls below this cut-off)
While the picture may be incomplete with regard tothe prevalence of undernutrition in hospitals it is clearthat disease-related undernutrition remains a significantclinical problem in hospitals
However the problem of disease-related undernutri-tion is not confined to people in hospital Within thecommunity up to 10 of people with cancer or otherchronic diseases may be significantly malnourished(Edington et al 1996) and many elderly people are alsoat high risk of undernutrition As a result people arecommonly admitted to hospital nutritionally depletedIn a study conducted in four hospitals in EnglandEdington et al (2000) found that one in every fivepatients admitted was malnourished Patients wereassessed using anthropometric measurements and BMIand by recording history of unintentional weight lossThis figure is likely to be an underestimate because it didnot include those who were too ill on admission to beassessed Kelly et al (2000) estimated that undernutri-tion among acute hospital admissions goes unrecognisedin 70 of cases
Once in hospital undernutrition is likely to get worseIn the study by McWhirter and Pennington two-thirdsof the 500 patients who had been assessed on admis-sion and were reassessed on discharge had lost weightA study on a random sample of 150 in-patients foundapproximately half of them to be either at moderate riskor high risk of undernutrition (Reilly et al 1995) Theprevalence and level of risk is probably higher amonghigh dependency medical surgical geriatric and paedi-atric patients (Reilly et al 1995) As illness and hospi-talisation are frequently associated with weight lossdeterioration in nutritional status is inevitable unlessaction is taken to prevent it
Key points
bull It is estimated that 70 of all undernutrition in theUK goes unrecognised and untreatedbull In the community 5 of the population have aBMI lt 20 kgm2 In hospitals this figure is 20ndash25bull It is estimated that 40 of adults and 15 of chil-dren admitted to hospital are malnourished half ofthese severely so and many others become malnour-ished during their stay in hospitalbull It is estimated that at any one time approximately66 of hospital patients are malnourished
Undernutrition in the UK 97
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
5 Cost of the problem of undernutrition
Undernutrition primarily results in loss of body tissue(depletion of body fat stores and muscle wasting) How-ever because nutrient intake is so closely correlatedwith energy intake a deficiency of energy is likely toresult in an inadequate intake of protein vitamins min-erals and trace elements This can cause widespreadmetabolic physiological and functional effects whichmay include
bull Impaired immune function and hence increased sus-ceptibility to infection and sepsis Infection will furtherimpair a malnourished statebull Delayed wound healingbull Increased risk of pressure sores particularly due toloss of cushioning fat storesbull Muscle wasting and weakness which may affect
ndash Respiratory function impaired respiratory musclestrength makes it difficult for a patient to cough andexpectorate effectively so increasing the risk of chestinfection It may also be more difficult to wean apatient off a ventilatorndash Cardiac function this may be impaired resulting inreduced cardiac output and risk of heart failurendash Mobility weakness of skeletal muscles delays areturn to full mobility Reduced mobility increases therisk of thromboembolism and bedsores
bull Altered structure of the small intestine which mayresult in malabsorptionbull Increased risk of postoperative complicationsbull Apathy and depression leading to loss of morale andreduced will to recoverbull General sense of weakness and illness which impairsappetite and physical ability to eat and hence tends toperpetuate and worsen any undernutrition
In summary undernutrition causes considerable mor-bidity delays recovery and increases the risk of death ABMI at or below the 15th percentile has been shown tobe a significant and independent predictor of death inseriously ill patients (Galanos et al 1997) There is alsoan economic cost in terms of increased need of nursingcare and extended hospital stay
There is clear evidence that correcting undernutritionhas many benefits (Potter et al 1998) Improvements inbody weight status and anthropometric parameters areassociated with improvement in immune function(Chandra 1992 Dionigi et al 1988) wound healing(Haydock amp Hill 1987) and muscle function (Fiataroneamp Evans 1993) and in clinical outcomes such asrecovery time and incidence of postoperativecomplications
Hospitals spend approximately pound15 billion on foodannually and studies conducted in one hospital foundthat 30ndash40 of food is discarded (Kelly 1999) This isconsistent with national estimates that 30ndash50 of hos-pital food is wasted with a monetary value calculated tobe pound45 million each year (Edwards amp Nash 1997Fenton et al 1995) With the inclusion of labour andoverheads this cost rises to pound144 million annuallyThere is also the hidden cost of the extra ill health asso-ciated with undernutrition Some hospitals also typicallyspend approximately pound800 000 on enteral andparenteral nutrition (see Sections 92 and 93) TheKingrsquos Fund (1992) report calculated that provision ofcomprehensive nutrition support would result in a 5-day reduction in hospital stay for approximately 10of patients The consequent saving was estimated to bepound266 million annually in the UK A review conducted byBond (1997) in the USA showed a clear relationshipbetween undernutrition and prolonged hospital stayWhen nutritional intervention was introduced 2 daysearlier than usual the result was a 1-day shortening ofhospital stay It was calculated that a more aggressivenutritional intervention policy would save the averagehospital $1 million per year
Key points
bull Between 30 and 50 of hospital food is wastedbull On average food intake is less than 75 of thatrecommended particularly among the elderlybull The monetary value of hospital food wasted eachyear in England alone is calculated to be pound45 millionBy including labour and overheads this cost rises topound144 millionbull There is also the hidden cost of the extra ill healthassociated with undernutrition because it increasesthe risk of complications lowers resistance to infec-tion impairs physical and mental functioning anddelays recovery
6 Why the problem of undernutrition is exacerbated in hospitals
In more than 60 of patients nutritional status deteri-orates during their stay in hospital with those whoare malnourished on admission particularly affectedPennington (1998) demonstrated that progressive nutri-tional depletion occurs for up to 8 weeks after curativesurgery (eg a heart by-pass operation) This thereforeindicates the need to consider nutritional status fromonset of illness through to complete recovery including
98 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
time after discharge However undernutrition remainsundetected in the majority of patients affected becausemany clinicians and nurses still do not consider nutri-tion to be an important factor in the management of dis-ease (Schenker 2000) and so do not routinely monitornutritional status and body weight Economic analysishas demonstrated that appropriate nutritional treatmentis cost-effective but benefits will only be achieved withhigh standards of nutritional care Multi-professionalnutritional support teams best conduct such treatmentbut there is continuing evidence of poor practice anda high incidence of treatment-related complicationswhich negate the benefits of nutritional treatments(Schenker 2000) In the hospital or institutional settingtherefore the problems that cause undernutrition maybe compounded by the fact that nutritional consider-ations may receive little attention from medical andnursing staff Lack of awareness of the prognostic sig-nificance of undernutrition and lack of knowledgeamong doctors and nurses regarding its assessment andmanagement (Nightingale amp Reeves 1999) may meanthat it is neither looked for nor taken into account whentreatment priorities are being set In particular theremay be failure to
bull identify those with or at risk of nutritional depletionbull identify nutritional requirements especially whenthese are increased because of fever surgery or injurybull provide food of an appropriate quality compositionand consistencybull encourage food intake food is of no benefit if noteatenbull monitor what is actually consumed in some circum-stances direct observation of food and fluid consump-tion is essentialbull identify those whose nutritional needs are not beingmet (through regular weighing or the use of otheranthropometric measurements)bull correct inadequate intake
61 Hospital food and feeding
The following factors have been identified as causes forpoor dietary intake in hospital patients
611 Problems with ordering
bull Menus lack clarity dishes should be described accu-rately so that patients have a reasonable idea of what toexpectbull Help with ordering should be available (but in manycases is not) where there are problems with a patientrsquoscomprehension speech or language
bull Menus are often not printed in languages other thanEnglish This is a particular problem in areas with a highimmigrant population Illiteracy may limit usefulness oftranslated menus Verbal translation may be betterbull Ordering from the menu too far in advance A patientmay be discharged after they have ordered food for thenext day resulting in the bedrsquos new occupant receivingfood chosen by someone else which may be unsuitableSame day ordering systems reduce waste and encourageconsumptionbull Patientsrsquo orders are not checked to ensure that thefood received and the portions requested are correct Inthis respect ward hostesses or feeding care attendantsmay be helpful however this does have financialimplicationsbull Inefficient ordering systems and poor two-way com-munication between the wards and the catering depart-ment lead to waste eg food sent to patients who havebeen discharged transferred or have died Such trays arethen either wasted or given to another patient wholeaves most of it because it was not their choice
612 Menu choice
bull Menus do not always take account of the needs tastesand customary eating habits of different groups ofpatients These will vary according to age race or cul-ture or the disease processbull Menus often do not take account of those needingfortified andor modified-consistency mealsbull Inappropriate promotion of lsquohealthy eatingrsquo eglow-fat diets in undernourished or nutritionally at-riskpatientsbull Some elderly patients often adopt a grazing habit andrequire frequent small volume high energy densityfeeds and snacksbull Special needs Although some disease-specific menuseg for renal failure may be provided from a dietkitchen it may be cost-effective to be able to supplementthe standard menu with high-energy high-proteinadditionsbull Nutritional needs and appetites of children differfrom those of adults and also vary according to ageMeals should be made attractive to children
613 Appropriate food choices
bull Food suitable for lsquohealthy eatingrsquo by the overweightpatient with cardiovascular disease is inappropriate forthe depleted malnourished patientbull Pureacuteed or semisolid diets are required by patientswith neurological or mechanical dysphagia who may be
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

Undernutrition in the UK
93
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
therefore from households in receipt of benefits) hadlower vitamin and mineral intakes (Buttriss 2002)
Similar findings have been reported from other large-scale surveys in the UK such as the Scottish HeartHealth Study in which the data were controlled forsmoking and education level (Bolton-Smith
et al
1991)and the 36-year follow-up to the National Birth CohortStudy (Braddon
et al
1988) The survey of nutrientintakes in Northern Ireland found similar nutrientdifferences by occupational social class (Barker
et al
1989) These findings are comparable with those fromsmaller surveys looking at nutrient intakes in differentsocioeconomic circumstances (Calvert
et al
1994Moynihan
et al
1993) including the homeless (Rushdenamp Wheeler 1993) A study by Dowler amp Calvert (1995)of nutrient intakes in lone-parent households showedthat where parents had lived for some time on incomesupport and particularly where they had fixed regulardeductions for debt recovery nutrient intakes were halfof the levels of those not living in such circumstances
In terms of dietary variety and overall dietary pat-terns those in poorer households consume less fruitjuice lean meat oily fish and wholemeal products andfewer salads and are more likely to eat white breadpotatoes cheaper fatty meats beans eggs and chips(Anderson amp Hunt 1992 Gregory
et al
1995Whichelow
et al
1991) Those on lower incomes have amuch less diverse food base so their diet is more likelyto lack variety
Many foods that are integral to a healthy diet are per-ceived as a luxury by those on low incomes and are anlsquoexpensiversquo form of energy such foods include fruitsvegetables and fish In addition many healthier alterna-tives carry a price premium
eg
wholemeal bread fatsand spreads low in saturates and lean meat However inaddition to price many factors influence the purchasingand consumption patterns in low-income householdswhich are related to their poor financial status such aslimited food preparation facilities Low income is alsooften associated with lack of knowledge and skillsrelated to food nutrition and cooking
Policies adopted by government local authorities andfood retailers can influence which foods are availableand accessible to people with low incomes For examplethere is the issue of price variability between shopsFood is generally more expensive in corner shops con-venience stores and small independent supermarketsthan in large supermarkets Piachaud amp Webb (1996)found that on average basic foodstuffs cost 24 morein small stores than in supermarkets taking super-market own brands into account the differences in costs
were 60 They calculated that people living in ahousehold on benefits would have to spend 25 moreof their income on food if they could not get to a largesupermarket or street market
Access to shopping facilities in areas where low-income households are concentrated is restricted interms of the physical difficulties or cost of travelling toshops and by a lack of choice of shops Thereforeaccess to a healthy diet becomes a particular problemfor low-income households The number of food retailoutlets is continually decreasing mainly at the expenseof shops such as small grocery retailers butchers fish-mongers and greengrocers The number of large retailoutlets has also decreased mainly because of theincrease in the number of superstores located on the out-skirts of towns and designed for access primarily by carEconomies of scale allow food sold in supermarkets tobe cheaper and cover a wider range than that in smallerhigh street stores The 1998 Independent Inquiry intoInequalities in Health report (Acheson 1998) foundparadoxically that a basket of food cost more in dis-advantaged areas than in affluent areas
The price of a healthy diet and the variation betweenprices of some foods is therefore of major concern forthose living on low incomes Many of the poorest peoplein the UK are concentrated in local authority housing ininner cities and there is evidence to suggest a continuinggeographical polarisation of income inequalities Inmany of these areas shops and banks have withdrawnpartly because the residents spend so little and partlybecause of the retail concentration in superstores(defined as having a total floor surface area of more than7620 m
2
) designed primarily for car access The risein vandalism is another contributing factor In a bidto resolve these problems the supermarket chainSomerfield operates a policy of maintaining small- andmedium-sized high street shops to serve local commu-nities and not to build large out-of town superstoresMany deprived sectors of society suffer from a lack ofaccess to good shopping facilities and in particularfresh fruit and vegetables To avoid these lsquofresh fooddesertsrsquo Somerfield opted to offer a free delivery serviceto village shops and small local stores Unfortunatelythe company had to close some of these small stores insome areas due to vandalism
312 Social and physical factors
Some of the social factors that influence food choice andeating patterns are listed below
94
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Figure 1
Guidelines for estimating the approximate energy and nitrogen requirements for an adult patient receiving artificial nutritional support Reproduced from Garrow
et al
2000 Reproduced with permission from Elsevier
bull Budgeting skillsbull Cultural traditionsbull Religious beliefsbull Educationbull Nutritional knowledgebull Lack of cooking facilities
eg
families housed in bed-and-breakfast accommodationbull Habitsbull Likes and dislikesbull Previous food experiencebull Willingness to experimentbull Time availablebull Eating alonebull Depressionbull Bereavement
For example a recently widowed man may not only besuffering the effects of bereavement and depressionwhich are likely to reduce appetite but he may also sud-denly find himself having to cope alone If his wife hadalways been responsible for shopping cooking and pro-viding food the widower may have difficulty budgetingfor food preparing and cooking food and may find thenew experience of eating alone all too painful
Poor dentition is another factor The NDNS of peopleaged 65 years and over (Finch
et al
1998) reported thatpeople with no natural teeth or few natural teeth ate amore restricted range of foods influenced by their per-ceived inability to chew The survey showed an associ-ation between oral function and nutrient intake andnutritional status Subjects without their own teeth wereless likely to choose foods that need chewing such asfruit and vegetables had lower intakes of iron vitaminsC and E and retinol and had lower plasma levels of vita-min C This was particularly true of those who lived invarious forms of residential care Physical disabilitiesalso influence a personrsquos ability to shop prepare andcook food Something as simple as opening a can ofbaked beans is far from simple for someone witharthritic hands
32 Effect of disease on nutritional status
321 The nutritional requirements of illness
Tissue repair imposes demands on nutritional supplyand an increased activity of body defence mechanismsmay also increase nutritional needs Despite this illhealth is often associated with a decreased desire forfood and decreased nutritional intake
Various changes in the metabolism of carbohydratefat and protein can be observed in illness Proportionalto the severity of illness there is an increase in the bodyrsquosenergy requirement and also an increase in urinarynitrogen loss (Cuthbertson 1980) The scale of thesechanges can be seen in Fig 1 This response to illnesshas been termed a stress response and the state ofincreased energy and protein needs a hypermetabolicstate
The metabolic response to illness traditionally hasthree phases ebb flow and anabolic although these canbe moderated with drug treatment The ebb phase onlylasts for a few hours and there is a depression of meta-bolic function and a reduction in energy expenditure In
Undernutrition in the UK
95
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
the flow phase metabolic rate increases and energyreserves in the form of fat stores are mobilised Visceraland muscle tissue provide amino acids that can be usedfor gluconeogenesis providing glucose for the brain andred blood cells and for wound-healing mechanismsHormonal changes appear to be important determinantsof the stress response Simply stated insulin stimulatesglucose uptake and metabolism and glycogen fat andprotein synthesis During starvation insulin levels arelow and other hormones are effective in mobilisingbody stores (
ie
promote glycogen fat and proteinbreakdown and stimulate gluconeogenesis and ketoge-nesis) In the stress response there is an increased secre-tion of catabolic hormones Especially important arethe glucocorticoids catecholamines and glucagon Theactions of insulin seem to be opposed by the catabolichormones leading to a state of insulin resistance(Cuthbertson 1980)
Another fundamental event is the production of themediator interleukin-1 a polypeptide produced byphagocytic cells (white blood cells that help fight infec-tion) A number of direct effects collectively termed theacute-phase response are ascribed to interleukin-1These include fever which is one of the strategies thebody uses to fight infection and the induction of muscleprotein breakdown leading to increased blood levels ofthe acute-phase proteins prealbumin retinol-bindingprotein (RBP) and C-reactive protein (Casati
et al
1998)
In simple starvation the breakdown of body fat isreversed by feeding with glucose In the hypermetabolicpatient it is found that fat breakdown continues despitegiving glucose and that gluconeogenesis and glucoseoxidation also occur at increased rates Hence theincreased gluconeogenesis can increase the amount ofcarbohydrate that is required to obviate protein break-down Achievement of energy balance fails to alleviatecatabolism in critically ill patients Therefore provisionof energy intake to match energy expenditure is unnec-essary during the flow phase and may even be unhelpful(Frankenfield
et al
1997)The increased nitrogen loss observed in stressed
patients can be accounted for by both a depression ofprotein synthesis and an increase in the rate of proteinbreakdown Provision of adequate protein stimulatesprotein synthesis but it also stimulates breakdown(Campbell 1999)
In the anabolic phase catabolism eventually declinesand is coupled with an increase in appetite and ability tomove This phase provides the opportunity for nutri-tional therapy to restore muscle mass and increase pro-tein synthesis
33 Reaching hospital
On reaching hospital dietary intake may be furtherreduced by one or more of the following problems
bull Confusionbull Fearbull Depressionbull Dysphagia (inability or reduced ability to swallow)bull Loss of appetite taste smell or thirstbull Poor dentitionbull Constipation which is caused by reduced mobilityand the fear that eating will make it worsebull Discomfortbull Dislike of the type of food availablebull Difference in routine and meal patternbull Problems with feedingbull Lack of staff available to help with feeding
Key points
Factors influencing poor dietary intake includebull loss of appetitebull disease or recurrent illness and consequenttreatmentbull impaired ability to absorb or utilise nutrientsbull poverty resulting in lack of car ownership or alter-native transport leading to limited access to bulk buy-ing low-cost foodbull poor housing with poor food storage and prepara-tion facilitiesbull problems of shopping and lack of preparation andcooking skillsbull less education leading to less knowledge and moti-vation to make healthy diet choicesbull unemployment so there is less money available forexpenditure on foodbull social isolation depression and bereavement lowself-esteem
4 Extent of the problem of undernutrition
Undernutrition among patients in UK hospitals wasdocumented in the mid-1970s (Bistrian
et al
1974 Hill
et al
1977) and it remains a common and often unrec-ognised problem that contributes to patient morbidityand mortality (Lennard-Jones 1992 McWhirter ampPennington 1994 Potter
et al
1998)
96
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Many studies over the last 30 years have since empha-sised the presence of disease-related undernutrition inhospitalised patients (Bistrian
et al
1974 Corish
et al
2000 Hill
et al
1977 Kelly
et al
2000 McWhirter ampPennington 1994) However there is controversy aboutits exact prevalence in the hospital setting One of themajor reasons for this is that there is no universal agree-ment about the definition of undernutrition Becausevarious workers have used different criteria to screen forundernutrition the reported magnitude of the problemhas been highly variable ranging from 10 to 60
Corish
et al
(2000) have screened for undernutritionin patients admitted to two teaching hospitals in DublinTo ensure more reliable comparisons they used thesame criteria employed by McWhirter amp Pennington(1994) in a Dundee hospital 6 years earlier In both stud-ies patients were classified as undernourished if theyhad a BMI
lt
20 kgm
2
and a triceps skinfold thicknessor mid-arm muscle circumference (MAMC) below the15th percentile The incidence of undernutrition innewly admitted patients in Dublin was reported to bemore than threefold lower (11) than in Dundee(40)
This striking difference has led other experts in thefield to question the criteria for defining undernutritionElia amp Stratton (2000) suggest that anthropometric cut-off values should not be used as a diagnostic label ofundernutrition but rather to classify an individualrsquosrisk of undernutrition Some healthy subjects have aBMI
lt
20 kgm2 (especially young adults) and are per-fectly well In addition anthropometric criteria alonesuggest a chronic protein-energy deficiency status How-ever a patient showing substantial recent weight loss(eg greater than 10 weight loss over 3ndash6 months) isat risk of undernutrition and impaired bodily functionseven though the anthropometric cut-off values may nothave been reached
The standard data used for anthropometry requireregular review so that they achieve the right balancebetween reflecting what is the norm (which may not bedesirable) and what is desirable (which may not beappropriate to the current generation) Unlike BMIwhich is a fixed criterion percentile values can showsubstantial change over time For example the referencevalues provided by Bishop et al (1981) for arm anthro-pometry were established in the USA about 30 yearsago The secular trends in obesity over that period meanthat these reference values may no longer apply Fur-thermore the choice of the percentile cut-off for use aspart of the screening tool to classify patients as under-nourished may be inappropriately high (since 15 ofthe reference population falls below this cut-off)
While the picture may be incomplete with regard tothe prevalence of undernutrition in hospitals it is clearthat disease-related undernutrition remains a significantclinical problem in hospitals
However the problem of disease-related undernutri-tion is not confined to people in hospital Within thecommunity up to 10 of people with cancer or otherchronic diseases may be significantly malnourished(Edington et al 1996) and many elderly people are alsoat high risk of undernutrition As a result people arecommonly admitted to hospital nutritionally depletedIn a study conducted in four hospitals in EnglandEdington et al (2000) found that one in every fivepatients admitted was malnourished Patients wereassessed using anthropometric measurements and BMIand by recording history of unintentional weight lossThis figure is likely to be an underestimate because it didnot include those who were too ill on admission to beassessed Kelly et al (2000) estimated that undernutri-tion among acute hospital admissions goes unrecognisedin 70 of cases
Once in hospital undernutrition is likely to get worseIn the study by McWhirter and Pennington two-thirdsof the 500 patients who had been assessed on admis-sion and were reassessed on discharge had lost weightA study on a random sample of 150 in-patients foundapproximately half of them to be either at moderate riskor high risk of undernutrition (Reilly et al 1995) Theprevalence and level of risk is probably higher amonghigh dependency medical surgical geriatric and paedi-atric patients (Reilly et al 1995) As illness and hospi-talisation are frequently associated with weight lossdeterioration in nutritional status is inevitable unlessaction is taken to prevent it
Key points
bull It is estimated that 70 of all undernutrition in theUK goes unrecognised and untreatedbull In the community 5 of the population have aBMI lt 20 kgm2 In hospitals this figure is 20ndash25bull It is estimated that 40 of adults and 15 of chil-dren admitted to hospital are malnourished half ofthese severely so and many others become malnour-ished during their stay in hospitalbull It is estimated that at any one time approximately66 of hospital patients are malnourished
Undernutrition in the UK 97
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
5 Cost of the problem of undernutrition
Undernutrition primarily results in loss of body tissue(depletion of body fat stores and muscle wasting) How-ever because nutrient intake is so closely correlatedwith energy intake a deficiency of energy is likely toresult in an inadequate intake of protein vitamins min-erals and trace elements This can cause widespreadmetabolic physiological and functional effects whichmay include
bull Impaired immune function and hence increased sus-ceptibility to infection and sepsis Infection will furtherimpair a malnourished statebull Delayed wound healingbull Increased risk of pressure sores particularly due toloss of cushioning fat storesbull Muscle wasting and weakness which may affect
ndash Respiratory function impaired respiratory musclestrength makes it difficult for a patient to cough andexpectorate effectively so increasing the risk of chestinfection It may also be more difficult to wean apatient off a ventilatorndash Cardiac function this may be impaired resulting inreduced cardiac output and risk of heart failurendash Mobility weakness of skeletal muscles delays areturn to full mobility Reduced mobility increases therisk of thromboembolism and bedsores
bull Altered structure of the small intestine which mayresult in malabsorptionbull Increased risk of postoperative complicationsbull Apathy and depression leading to loss of morale andreduced will to recoverbull General sense of weakness and illness which impairsappetite and physical ability to eat and hence tends toperpetuate and worsen any undernutrition
In summary undernutrition causes considerable mor-bidity delays recovery and increases the risk of death ABMI at or below the 15th percentile has been shown tobe a significant and independent predictor of death inseriously ill patients (Galanos et al 1997) There is alsoan economic cost in terms of increased need of nursingcare and extended hospital stay
There is clear evidence that correcting undernutritionhas many benefits (Potter et al 1998) Improvements inbody weight status and anthropometric parameters areassociated with improvement in immune function(Chandra 1992 Dionigi et al 1988) wound healing(Haydock amp Hill 1987) and muscle function (Fiataroneamp Evans 1993) and in clinical outcomes such asrecovery time and incidence of postoperativecomplications
Hospitals spend approximately pound15 billion on foodannually and studies conducted in one hospital foundthat 30ndash40 of food is discarded (Kelly 1999) This isconsistent with national estimates that 30ndash50 of hos-pital food is wasted with a monetary value calculated tobe pound45 million each year (Edwards amp Nash 1997Fenton et al 1995) With the inclusion of labour andoverheads this cost rises to pound144 million annuallyThere is also the hidden cost of the extra ill health asso-ciated with undernutrition Some hospitals also typicallyspend approximately pound800 000 on enteral andparenteral nutrition (see Sections 92 and 93) TheKingrsquos Fund (1992) report calculated that provision ofcomprehensive nutrition support would result in a 5-day reduction in hospital stay for approximately 10of patients The consequent saving was estimated to bepound266 million annually in the UK A review conducted byBond (1997) in the USA showed a clear relationshipbetween undernutrition and prolonged hospital stayWhen nutritional intervention was introduced 2 daysearlier than usual the result was a 1-day shortening ofhospital stay It was calculated that a more aggressivenutritional intervention policy would save the averagehospital $1 million per year
Key points
bull Between 30 and 50 of hospital food is wastedbull On average food intake is less than 75 of thatrecommended particularly among the elderlybull The monetary value of hospital food wasted eachyear in England alone is calculated to be pound45 millionBy including labour and overheads this cost rises topound144 millionbull There is also the hidden cost of the extra ill healthassociated with undernutrition because it increasesthe risk of complications lowers resistance to infec-tion impairs physical and mental functioning anddelays recovery
6 Why the problem of undernutrition is exacerbated in hospitals
In more than 60 of patients nutritional status deteri-orates during their stay in hospital with those whoare malnourished on admission particularly affectedPennington (1998) demonstrated that progressive nutri-tional depletion occurs for up to 8 weeks after curativesurgery (eg a heart by-pass operation) This thereforeindicates the need to consider nutritional status fromonset of illness through to complete recovery including
98 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
time after discharge However undernutrition remainsundetected in the majority of patients affected becausemany clinicians and nurses still do not consider nutri-tion to be an important factor in the management of dis-ease (Schenker 2000) and so do not routinely monitornutritional status and body weight Economic analysishas demonstrated that appropriate nutritional treatmentis cost-effective but benefits will only be achieved withhigh standards of nutritional care Multi-professionalnutritional support teams best conduct such treatmentbut there is continuing evidence of poor practice anda high incidence of treatment-related complicationswhich negate the benefits of nutritional treatments(Schenker 2000) In the hospital or institutional settingtherefore the problems that cause undernutrition maybe compounded by the fact that nutritional consider-ations may receive little attention from medical andnursing staff Lack of awareness of the prognostic sig-nificance of undernutrition and lack of knowledgeamong doctors and nurses regarding its assessment andmanagement (Nightingale amp Reeves 1999) may meanthat it is neither looked for nor taken into account whentreatment priorities are being set In particular theremay be failure to
bull identify those with or at risk of nutritional depletionbull identify nutritional requirements especially whenthese are increased because of fever surgery or injurybull provide food of an appropriate quality compositionand consistencybull encourage food intake food is of no benefit if noteatenbull monitor what is actually consumed in some circum-stances direct observation of food and fluid consump-tion is essentialbull identify those whose nutritional needs are not beingmet (through regular weighing or the use of otheranthropometric measurements)bull correct inadequate intake
61 Hospital food and feeding
The following factors have been identified as causes forpoor dietary intake in hospital patients
611 Problems with ordering
bull Menus lack clarity dishes should be described accu-rately so that patients have a reasonable idea of what toexpectbull Help with ordering should be available (but in manycases is not) where there are problems with a patientrsquoscomprehension speech or language
bull Menus are often not printed in languages other thanEnglish This is a particular problem in areas with a highimmigrant population Illiteracy may limit usefulness oftranslated menus Verbal translation may be betterbull Ordering from the menu too far in advance A patientmay be discharged after they have ordered food for thenext day resulting in the bedrsquos new occupant receivingfood chosen by someone else which may be unsuitableSame day ordering systems reduce waste and encourageconsumptionbull Patientsrsquo orders are not checked to ensure that thefood received and the portions requested are correct Inthis respect ward hostesses or feeding care attendantsmay be helpful however this does have financialimplicationsbull Inefficient ordering systems and poor two-way com-munication between the wards and the catering depart-ment lead to waste eg food sent to patients who havebeen discharged transferred or have died Such trays arethen either wasted or given to another patient wholeaves most of it because it was not their choice
612 Menu choice
bull Menus do not always take account of the needs tastesand customary eating habits of different groups ofpatients These will vary according to age race or cul-ture or the disease processbull Menus often do not take account of those needingfortified andor modified-consistency mealsbull Inappropriate promotion of lsquohealthy eatingrsquo eglow-fat diets in undernourished or nutritionally at-riskpatientsbull Some elderly patients often adopt a grazing habit andrequire frequent small volume high energy densityfeeds and snacksbull Special needs Although some disease-specific menuseg for renal failure may be provided from a dietkitchen it may be cost-effective to be able to supplementthe standard menu with high-energy high-proteinadditionsbull Nutritional needs and appetites of children differfrom those of adults and also vary according to ageMeals should be made attractive to children
613 Appropriate food choices
bull Food suitable for lsquohealthy eatingrsquo by the overweightpatient with cardiovascular disease is inappropriate forthe depleted malnourished patientbull Pureacuteed or semisolid diets are required by patientswith neurological or mechanical dysphagia who may be
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

94
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Figure 1
Guidelines for estimating the approximate energy and nitrogen requirements for an adult patient receiving artificial nutritional support Reproduced from Garrow
et al
2000 Reproduced with permission from Elsevier
bull Budgeting skillsbull Cultural traditionsbull Religious beliefsbull Educationbull Nutritional knowledgebull Lack of cooking facilities
eg
families housed in bed-and-breakfast accommodationbull Habitsbull Likes and dislikesbull Previous food experiencebull Willingness to experimentbull Time availablebull Eating alonebull Depressionbull Bereavement
For example a recently widowed man may not only besuffering the effects of bereavement and depressionwhich are likely to reduce appetite but he may also sud-denly find himself having to cope alone If his wife hadalways been responsible for shopping cooking and pro-viding food the widower may have difficulty budgetingfor food preparing and cooking food and may find thenew experience of eating alone all too painful
Poor dentition is another factor The NDNS of peopleaged 65 years and over (Finch
et al
1998) reported thatpeople with no natural teeth or few natural teeth ate amore restricted range of foods influenced by their per-ceived inability to chew The survey showed an associ-ation between oral function and nutrient intake andnutritional status Subjects without their own teeth wereless likely to choose foods that need chewing such asfruit and vegetables had lower intakes of iron vitaminsC and E and retinol and had lower plasma levels of vita-min C This was particularly true of those who lived invarious forms of residential care Physical disabilitiesalso influence a personrsquos ability to shop prepare andcook food Something as simple as opening a can ofbaked beans is far from simple for someone witharthritic hands
32 Effect of disease on nutritional status
321 The nutritional requirements of illness
Tissue repair imposes demands on nutritional supplyand an increased activity of body defence mechanismsmay also increase nutritional needs Despite this illhealth is often associated with a decreased desire forfood and decreased nutritional intake
Various changes in the metabolism of carbohydratefat and protein can be observed in illness Proportionalto the severity of illness there is an increase in the bodyrsquosenergy requirement and also an increase in urinarynitrogen loss (Cuthbertson 1980) The scale of thesechanges can be seen in Fig 1 This response to illnesshas been termed a stress response and the state ofincreased energy and protein needs a hypermetabolicstate
The metabolic response to illness traditionally hasthree phases ebb flow and anabolic although these canbe moderated with drug treatment The ebb phase onlylasts for a few hours and there is a depression of meta-bolic function and a reduction in energy expenditure In
Undernutrition in the UK
95
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
the flow phase metabolic rate increases and energyreserves in the form of fat stores are mobilised Visceraland muscle tissue provide amino acids that can be usedfor gluconeogenesis providing glucose for the brain andred blood cells and for wound-healing mechanismsHormonal changes appear to be important determinantsof the stress response Simply stated insulin stimulatesglucose uptake and metabolism and glycogen fat andprotein synthesis During starvation insulin levels arelow and other hormones are effective in mobilisingbody stores (
ie
promote glycogen fat and proteinbreakdown and stimulate gluconeogenesis and ketoge-nesis) In the stress response there is an increased secre-tion of catabolic hormones Especially important arethe glucocorticoids catecholamines and glucagon Theactions of insulin seem to be opposed by the catabolichormones leading to a state of insulin resistance(Cuthbertson 1980)
Another fundamental event is the production of themediator interleukin-1 a polypeptide produced byphagocytic cells (white blood cells that help fight infec-tion) A number of direct effects collectively termed theacute-phase response are ascribed to interleukin-1These include fever which is one of the strategies thebody uses to fight infection and the induction of muscleprotein breakdown leading to increased blood levels ofthe acute-phase proteins prealbumin retinol-bindingprotein (RBP) and C-reactive protein (Casati
et al
1998)
In simple starvation the breakdown of body fat isreversed by feeding with glucose In the hypermetabolicpatient it is found that fat breakdown continues despitegiving glucose and that gluconeogenesis and glucoseoxidation also occur at increased rates Hence theincreased gluconeogenesis can increase the amount ofcarbohydrate that is required to obviate protein break-down Achievement of energy balance fails to alleviatecatabolism in critically ill patients Therefore provisionof energy intake to match energy expenditure is unnec-essary during the flow phase and may even be unhelpful(Frankenfield
et al
1997)The increased nitrogen loss observed in stressed
patients can be accounted for by both a depression ofprotein synthesis and an increase in the rate of proteinbreakdown Provision of adequate protein stimulatesprotein synthesis but it also stimulates breakdown(Campbell 1999)
In the anabolic phase catabolism eventually declinesand is coupled with an increase in appetite and ability tomove This phase provides the opportunity for nutri-tional therapy to restore muscle mass and increase pro-tein synthesis
33 Reaching hospital
On reaching hospital dietary intake may be furtherreduced by one or more of the following problems
bull Confusionbull Fearbull Depressionbull Dysphagia (inability or reduced ability to swallow)bull Loss of appetite taste smell or thirstbull Poor dentitionbull Constipation which is caused by reduced mobilityand the fear that eating will make it worsebull Discomfortbull Dislike of the type of food availablebull Difference in routine and meal patternbull Problems with feedingbull Lack of staff available to help with feeding
Key points
Factors influencing poor dietary intake includebull loss of appetitebull disease or recurrent illness and consequenttreatmentbull impaired ability to absorb or utilise nutrientsbull poverty resulting in lack of car ownership or alter-native transport leading to limited access to bulk buy-ing low-cost foodbull poor housing with poor food storage and prepara-tion facilitiesbull problems of shopping and lack of preparation andcooking skillsbull less education leading to less knowledge and moti-vation to make healthy diet choicesbull unemployment so there is less money available forexpenditure on foodbull social isolation depression and bereavement lowself-esteem
4 Extent of the problem of undernutrition
Undernutrition among patients in UK hospitals wasdocumented in the mid-1970s (Bistrian
et al
1974 Hill
et al
1977) and it remains a common and often unrec-ognised problem that contributes to patient morbidityand mortality (Lennard-Jones 1992 McWhirter ampPennington 1994 Potter
et al
1998)
96
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Many studies over the last 30 years have since empha-sised the presence of disease-related undernutrition inhospitalised patients (Bistrian
et al
1974 Corish
et al
2000 Hill
et al
1977 Kelly
et al
2000 McWhirter ampPennington 1994) However there is controversy aboutits exact prevalence in the hospital setting One of themajor reasons for this is that there is no universal agree-ment about the definition of undernutrition Becausevarious workers have used different criteria to screen forundernutrition the reported magnitude of the problemhas been highly variable ranging from 10 to 60
Corish
et al
(2000) have screened for undernutritionin patients admitted to two teaching hospitals in DublinTo ensure more reliable comparisons they used thesame criteria employed by McWhirter amp Pennington(1994) in a Dundee hospital 6 years earlier In both stud-ies patients were classified as undernourished if theyhad a BMI
lt
20 kgm
2
and a triceps skinfold thicknessor mid-arm muscle circumference (MAMC) below the15th percentile The incidence of undernutrition innewly admitted patients in Dublin was reported to bemore than threefold lower (11) than in Dundee(40)
This striking difference has led other experts in thefield to question the criteria for defining undernutritionElia amp Stratton (2000) suggest that anthropometric cut-off values should not be used as a diagnostic label ofundernutrition but rather to classify an individualrsquosrisk of undernutrition Some healthy subjects have aBMI
lt
20 kgm2 (especially young adults) and are per-fectly well In addition anthropometric criteria alonesuggest a chronic protein-energy deficiency status How-ever a patient showing substantial recent weight loss(eg greater than 10 weight loss over 3ndash6 months) isat risk of undernutrition and impaired bodily functionseven though the anthropometric cut-off values may nothave been reached
The standard data used for anthropometry requireregular review so that they achieve the right balancebetween reflecting what is the norm (which may not bedesirable) and what is desirable (which may not beappropriate to the current generation) Unlike BMIwhich is a fixed criterion percentile values can showsubstantial change over time For example the referencevalues provided by Bishop et al (1981) for arm anthro-pometry were established in the USA about 30 yearsago The secular trends in obesity over that period meanthat these reference values may no longer apply Fur-thermore the choice of the percentile cut-off for use aspart of the screening tool to classify patients as under-nourished may be inappropriately high (since 15 ofthe reference population falls below this cut-off)
While the picture may be incomplete with regard tothe prevalence of undernutrition in hospitals it is clearthat disease-related undernutrition remains a significantclinical problem in hospitals
However the problem of disease-related undernutri-tion is not confined to people in hospital Within thecommunity up to 10 of people with cancer or otherchronic diseases may be significantly malnourished(Edington et al 1996) and many elderly people are alsoat high risk of undernutrition As a result people arecommonly admitted to hospital nutritionally depletedIn a study conducted in four hospitals in EnglandEdington et al (2000) found that one in every fivepatients admitted was malnourished Patients wereassessed using anthropometric measurements and BMIand by recording history of unintentional weight lossThis figure is likely to be an underestimate because it didnot include those who were too ill on admission to beassessed Kelly et al (2000) estimated that undernutri-tion among acute hospital admissions goes unrecognisedin 70 of cases
Once in hospital undernutrition is likely to get worseIn the study by McWhirter and Pennington two-thirdsof the 500 patients who had been assessed on admis-sion and were reassessed on discharge had lost weightA study on a random sample of 150 in-patients foundapproximately half of them to be either at moderate riskor high risk of undernutrition (Reilly et al 1995) Theprevalence and level of risk is probably higher amonghigh dependency medical surgical geriatric and paedi-atric patients (Reilly et al 1995) As illness and hospi-talisation are frequently associated with weight lossdeterioration in nutritional status is inevitable unlessaction is taken to prevent it
Key points
bull It is estimated that 70 of all undernutrition in theUK goes unrecognised and untreatedbull In the community 5 of the population have aBMI lt 20 kgm2 In hospitals this figure is 20ndash25bull It is estimated that 40 of adults and 15 of chil-dren admitted to hospital are malnourished half ofthese severely so and many others become malnour-ished during their stay in hospitalbull It is estimated that at any one time approximately66 of hospital patients are malnourished
Undernutrition in the UK 97
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
5 Cost of the problem of undernutrition
Undernutrition primarily results in loss of body tissue(depletion of body fat stores and muscle wasting) How-ever because nutrient intake is so closely correlatedwith energy intake a deficiency of energy is likely toresult in an inadequate intake of protein vitamins min-erals and trace elements This can cause widespreadmetabolic physiological and functional effects whichmay include
bull Impaired immune function and hence increased sus-ceptibility to infection and sepsis Infection will furtherimpair a malnourished statebull Delayed wound healingbull Increased risk of pressure sores particularly due toloss of cushioning fat storesbull Muscle wasting and weakness which may affect
ndash Respiratory function impaired respiratory musclestrength makes it difficult for a patient to cough andexpectorate effectively so increasing the risk of chestinfection It may also be more difficult to wean apatient off a ventilatorndash Cardiac function this may be impaired resulting inreduced cardiac output and risk of heart failurendash Mobility weakness of skeletal muscles delays areturn to full mobility Reduced mobility increases therisk of thromboembolism and bedsores
bull Altered structure of the small intestine which mayresult in malabsorptionbull Increased risk of postoperative complicationsbull Apathy and depression leading to loss of morale andreduced will to recoverbull General sense of weakness and illness which impairsappetite and physical ability to eat and hence tends toperpetuate and worsen any undernutrition
In summary undernutrition causes considerable mor-bidity delays recovery and increases the risk of death ABMI at or below the 15th percentile has been shown tobe a significant and independent predictor of death inseriously ill patients (Galanos et al 1997) There is alsoan economic cost in terms of increased need of nursingcare and extended hospital stay
There is clear evidence that correcting undernutritionhas many benefits (Potter et al 1998) Improvements inbody weight status and anthropometric parameters areassociated with improvement in immune function(Chandra 1992 Dionigi et al 1988) wound healing(Haydock amp Hill 1987) and muscle function (Fiataroneamp Evans 1993) and in clinical outcomes such asrecovery time and incidence of postoperativecomplications
Hospitals spend approximately pound15 billion on foodannually and studies conducted in one hospital foundthat 30ndash40 of food is discarded (Kelly 1999) This isconsistent with national estimates that 30ndash50 of hos-pital food is wasted with a monetary value calculated tobe pound45 million each year (Edwards amp Nash 1997Fenton et al 1995) With the inclusion of labour andoverheads this cost rises to pound144 million annuallyThere is also the hidden cost of the extra ill health asso-ciated with undernutrition Some hospitals also typicallyspend approximately pound800 000 on enteral andparenteral nutrition (see Sections 92 and 93) TheKingrsquos Fund (1992) report calculated that provision ofcomprehensive nutrition support would result in a 5-day reduction in hospital stay for approximately 10of patients The consequent saving was estimated to bepound266 million annually in the UK A review conducted byBond (1997) in the USA showed a clear relationshipbetween undernutrition and prolonged hospital stayWhen nutritional intervention was introduced 2 daysearlier than usual the result was a 1-day shortening ofhospital stay It was calculated that a more aggressivenutritional intervention policy would save the averagehospital $1 million per year
Key points
bull Between 30 and 50 of hospital food is wastedbull On average food intake is less than 75 of thatrecommended particularly among the elderlybull The monetary value of hospital food wasted eachyear in England alone is calculated to be pound45 millionBy including labour and overheads this cost rises topound144 millionbull There is also the hidden cost of the extra ill healthassociated with undernutrition because it increasesthe risk of complications lowers resistance to infec-tion impairs physical and mental functioning anddelays recovery
6 Why the problem of undernutrition is exacerbated in hospitals
In more than 60 of patients nutritional status deteri-orates during their stay in hospital with those whoare malnourished on admission particularly affectedPennington (1998) demonstrated that progressive nutri-tional depletion occurs for up to 8 weeks after curativesurgery (eg a heart by-pass operation) This thereforeindicates the need to consider nutritional status fromonset of illness through to complete recovery including
98 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
time after discharge However undernutrition remainsundetected in the majority of patients affected becausemany clinicians and nurses still do not consider nutri-tion to be an important factor in the management of dis-ease (Schenker 2000) and so do not routinely monitornutritional status and body weight Economic analysishas demonstrated that appropriate nutritional treatmentis cost-effective but benefits will only be achieved withhigh standards of nutritional care Multi-professionalnutritional support teams best conduct such treatmentbut there is continuing evidence of poor practice anda high incidence of treatment-related complicationswhich negate the benefits of nutritional treatments(Schenker 2000) In the hospital or institutional settingtherefore the problems that cause undernutrition maybe compounded by the fact that nutritional consider-ations may receive little attention from medical andnursing staff Lack of awareness of the prognostic sig-nificance of undernutrition and lack of knowledgeamong doctors and nurses regarding its assessment andmanagement (Nightingale amp Reeves 1999) may meanthat it is neither looked for nor taken into account whentreatment priorities are being set In particular theremay be failure to
bull identify those with or at risk of nutritional depletionbull identify nutritional requirements especially whenthese are increased because of fever surgery or injurybull provide food of an appropriate quality compositionand consistencybull encourage food intake food is of no benefit if noteatenbull monitor what is actually consumed in some circum-stances direct observation of food and fluid consump-tion is essentialbull identify those whose nutritional needs are not beingmet (through regular weighing or the use of otheranthropometric measurements)bull correct inadequate intake
61 Hospital food and feeding
The following factors have been identified as causes forpoor dietary intake in hospital patients
611 Problems with ordering
bull Menus lack clarity dishes should be described accu-rately so that patients have a reasonable idea of what toexpectbull Help with ordering should be available (but in manycases is not) where there are problems with a patientrsquoscomprehension speech or language
bull Menus are often not printed in languages other thanEnglish This is a particular problem in areas with a highimmigrant population Illiteracy may limit usefulness oftranslated menus Verbal translation may be betterbull Ordering from the menu too far in advance A patientmay be discharged after they have ordered food for thenext day resulting in the bedrsquos new occupant receivingfood chosen by someone else which may be unsuitableSame day ordering systems reduce waste and encourageconsumptionbull Patientsrsquo orders are not checked to ensure that thefood received and the portions requested are correct Inthis respect ward hostesses or feeding care attendantsmay be helpful however this does have financialimplicationsbull Inefficient ordering systems and poor two-way com-munication between the wards and the catering depart-ment lead to waste eg food sent to patients who havebeen discharged transferred or have died Such trays arethen either wasted or given to another patient wholeaves most of it because it was not their choice
612 Menu choice
bull Menus do not always take account of the needs tastesand customary eating habits of different groups ofpatients These will vary according to age race or cul-ture or the disease processbull Menus often do not take account of those needingfortified andor modified-consistency mealsbull Inappropriate promotion of lsquohealthy eatingrsquo eglow-fat diets in undernourished or nutritionally at-riskpatientsbull Some elderly patients often adopt a grazing habit andrequire frequent small volume high energy densityfeeds and snacksbull Special needs Although some disease-specific menuseg for renal failure may be provided from a dietkitchen it may be cost-effective to be able to supplementthe standard menu with high-energy high-proteinadditionsbull Nutritional needs and appetites of children differfrom those of adults and also vary according to ageMeals should be made attractive to children
613 Appropriate food choices
bull Food suitable for lsquohealthy eatingrsquo by the overweightpatient with cardiovascular disease is inappropriate forthe depleted malnourished patientbull Pureacuteed or semisolid diets are required by patientswith neurological or mechanical dysphagia who may be
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients
Undernutrition in the UK
95
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
the flow phase metabolic rate increases and energyreserves in the form of fat stores are mobilised Visceraland muscle tissue provide amino acids that can be usedfor gluconeogenesis providing glucose for the brain andred blood cells and for wound-healing mechanismsHormonal changes appear to be important determinantsof the stress response Simply stated insulin stimulatesglucose uptake and metabolism and glycogen fat andprotein synthesis During starvation insulin levels arelow and other hormones are effective in mobilisingbody stores (
ie
promote glycogen fat and proteinbreakdown and stimulate gluconeogenesis and ketoge-nesis) In the stress response there is an increased secre-tion of catabolic hormones Especially important arethe glucocorticoids catecholamines and glucagon Theactions of insulin seem to be opposed by the catabolichormones leading to a state of insulin resistance(Cuthbertson 1980)
Another fundamental event is the production of themediator interleukin-1 a polypeptide produced byphagocytic cells (white blood cells that help fight infec-tion) A number of direct effects collectively termed theacute-phase response are ascribed to interleukin-1These include fever which is one of the strategies thebody uses to fight infection and the induction of muscleprotein breakdown leading to increased blood levels ofthe acute-phase proteins prealbumin retinol-bindingprotein (RBP) and C-reactive protein (Casati
et al
1998)
In simple starvation the breakdown of body fat isreversed by feeding with glucose In the hypermetabolicpatient it is found that fat breakdown continues despitegiving glucose and that gluconeogenesis and glucoseoxidation also occur at increased rates Hence theincreased gluconeogenesis can increase the amount ofcarbohydrate that is required to obviate protein break-down Achievement of energy balance fails to alleviatecatabolism in critically ill patients Therefore provisionof energy intake to match energy expenditure is unnec-essary during the flow phase and may even be unhelpful(Frankenfield
et al
1997)The increased nitrogen loss observed in stressed
patients can be accounted for by both a depression ofprotein synthesis and an increase in the rate of proteinbreakdown Provision of adequate protein stimulatesprotein synthesis but it also stimulates breakdown(Campbell 1999)
In the anabolic phase catabolism eventually declinesand is coupled with an increase in appetite and ability tomove This phase provides the opportunity for nutri-tional therapy to restore muscle mass and increase pro-tein synthesis
33 Reaching hospital
On reaching hospital dietary intake may be furtherreduced by one or more of the following problems
bull Confusionbull Fearbull Depressionbull Dysphagia (inability or reduced ability to swallow)bull Loss of appetite taste smell or thirstbull Poor dentitionbull Constipation which is caused by reduced mobilityand the fear that eating will make it worsebull Discomfortbull Dislike of the type of food availablebull Difference in routine and meal patternbull Problems with feedingbull Lack of staff available to help with feeding
Key points
Factors influencing poor dietary intake includebull loss of appetitebull disease or recurrent illness and consequenttreatmentbull impaired ability to absorb or utilise nutrientsbull poverty resulting in lack of car ownership or alter-native transport leading to limited access to bulk buy-ing low-cost foodbull poor housing with poor food storage and prepara-tion facilitiesbull problems of shopping and lack of preparation andcooking skillsbull less education leading to less knowledge and moti-vation to make healthy diet choicesbull unemployment so there is less money available forexpenditure on foodbull social isolation depression and bereavement lowself-esteem
4 Extent of the problem of undernutrition
Undernutrition among patients in UK hospitals wasdocumented in the mid-1970s (Bistrian
et al
1974 Hill
et al
1977) and it remains a common and often unrec-ognised problem that contributes to patient morbidityand mortality (Lennard-Jones 1992 McWhirter ampPennington 1994 Potter
et al
1998)
96
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Many studies over the last 30 years have since empha-sised the presence of disease-related undernutrition inhospitalised patients (Bistrian
et al
1974 Corish
et al
2000 Hill
et al
1977 Kelly
et al
2000 McWhirter ampPennington 1994) However there is controversy aboutits exact prevalence in the hospital setting One of themajor reasons for this is that there is no universal agree-ment about the definition of undernutrition Becausevarious workers have used different criteria to screen forundernutrition the reported magnitude of the problemhas been highly variable ranging from 10 to 60
Corish
et al
(2000) have screened for undernutritionin patients admitted to two teaching hospitals in DublinTo ensure more reliable comparisons they used thesame criteria employed by McWhirter amp Pennington(1994) in a Dundee hospital 6 years earlier In both stud-ies patients were classified as undernourished if theyhad a BMI
lt
20 kgm
2
and a triceps skinfold thicknessor mid-arm muscle circumference (MAMC) below the15th percentile The incidence of undernutrition innewly admitted patients in Dublin was reported to bemore than threefold lower (11) than in Dundee(40)
This striking difference has led other experts in thefield to question the criteria for defining undernutritionElia amp Stratton (2000) suggest that anthropometric cut-off values should not be used as a diagnostic label ofundernutrition but rather to classify an individualrsquosrisk of undernutrition Some healthy subjects have aBMI
lt
20 kgm2 (especially young adults) and are per-fectly well In addition anthropometric criteria alonesuggest a chronic protein-energy deficiency status How-ever a patient showing substantial recent weight loss(eg greater than 10 weight loss over 3ndash6 months) isat risk of undernutrition and impaired bodily functionseven though the anthropometric cut-off values may nothave been reached
The standard data used for anthropometry requireregular review so that they achieve the right balancebetween reflecting what is the norm (which may not bedesirable) and what is desirable (which may not beappropriate to the current generation) Unlike BMIwhich is a fixed criterion percentile values can showsubstantial change over time For example the referencevalues provided by Bishop et al (1981) for arm anthro-pometry were established in the USA about 30 yearsago The secular trends in obesity over that period meanthat these reference values may no longer apply Fur-thermore the choice of the percentile cut-off for use aspart of the screening tool to classify patients as under-nourished may be inappropriately high (since 15 ofthe reference population falls below this cut-off)
While the picture may be incomplete with regard tothe prevalence of undernutrition in hospitals it is clearthat disease-related undernutrition remains a significantclinical problem in hospitals
However the problem of disease-related undernutri-tion is not confined to people in hospital Within thecommunity up to 10 of people with cancer or otherchronic diseases may be significantly malnourished(Edington et al 1996) and many elderly people are alsoat high risk of undernutrition As a result people arecommonly admitted to hospital nutritionally depletedIn a study conducted in four hospitals in EnglandEdington et al (2000) found that one in every fivepatients admitted was malnourished Patients wereassessed using anthropometric measurements and BMIand by recording history of unintentional weight lossThis figure is likely to be an underestimate because it didnot include those who were too ill on admission to beassessed Kelly et al (2000) estimated that undernutri-tion among acute hospital admissions goes unrecognisedin 70 of cases
Once in hospital undernutrition is likely to get worseIn the study by McWhirter and Pennington two-thirdsof the 500 patients who had been assessed on admis-sion and were reassessed on discharge had lost weightA study on a random sample of 150 in-patients foundapproximately half of them to be either at moderate riskor high risk of undernutrition (Reilly et al 1995) Theprevalence and level of risk is probably higher amonghigh dependency medical surgical geriatric and paedi-atric patients (Reilly et al 1995) As illness and hospi-talisation are frequently associated with weight lossdeterioration in nutritional status is inevitable unlessaction is taken to prevent it
Key points
bull It is estimated that 70 of all undernutrition in theUK goes unrecognised and untreatedbull In the community 5 of the population have aBMI lt 20 kgm2 In hospitals this figure is 20ndash25bull It is estimated that 40 of adults and 15 of chil-dren admitted to hospital are malnourished half ofthese severely so and many others become malnour-ished during their stay in hospitalbull It is estimated that at any one time approximately66 of hospital patients are malnourished
Undernutrition in the UK 97
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
5 Cost of the problem of undernutrition
Undernutrition primarily results in loss of body tissue(depletion of body fat stores and muscle wasting) How-ever because nutrient intake is so closely correlatedwith energy intake a deficiency of energy is likely toresult in an inadequate intake of protein vitamins min-erals and trace elements This can cause widespreadmetabolic physiological and functional effects whichmay include
bull Impaired immune function and hence increased sus-ceptibility to infection and sepsis Infection will furtherimpair a malnourished statebull Delayed wound healingbull Increased risk of pressure sores particularly due toloss of cushioning fat storesbull Muscle wasting and weakness which may affect
ndash Respiratory function impaired respiratory musclestrength makes it difficult for a patient to cough andexpectorate effectively so increasing the risk of chestinfection It may also be more difficult to wean apatient off a ventilatorndash Cardiac function this may be impaired resulting inreduced cardiac output and risk of heart failurendash Mobility weakness of skeletal muscles delays areturn to full mobility Reduced mobility increases therisk of thromboembolism and bedsores
bull Altered structure of the small intestine which mayresult in malabsorptionbull Increased risk of postoperative complicationsbull Apathy and depression leading to loss of morale andreduced will to recoverbull General sense of weakness and illness which impairsappetite and physical ability to eat and hence tends toperpetuate and worsen any undernutrition
In summary undernutrition causes considerable mor-bidity delays recovery and increases the risk of death ABMI at or below the 15th percentile has been shown tobe a significant and independent predictor of death inseriously ill patients (Galanos et al 1997) There is alsoan economic cost in terms of increased need of nursingcare and extended hospital stay
There is clear evidence that correcting undernutritionhas many benefits (Potter et al 1998) Improvements inbody weight status and anthropometric parameters areassociated with improvement in immune function(Chandra 1992 Dionigi et al 1988) wound healing(Haydock amp Hill 1987) and muscle function (Fiataroneamp Evans 1993) and in clinical outcomes such asrecovery time and incidence of postoperativecomplications
Hospitals spend approximately pound15 billion on foodannually and studies conducted in one hospital foundthat 30ndash40 of food is discarded (Kelly 1999) This isconsistent with national estimates that 30ndash50 of hos-pital food is wasted with a monetary value calculated tobe pound45 million each year (Edwards amp Nash 1997Fenton et al 1995) With the inclusion of labour andoverheads this cost rises to pound144 million annuallyThere is also the hidden cost of the extra ill health asso-ciated with undernutrition Some hospitals also typicallyspend approximately pound800 000 on enteral andparenteral nutrition (see Sections 92 and 93) TheKingrsquos Fund (1992) report calculated that provision ofcomprehensive nutrition support would result in a 5-day reduction in hospital stay for approximately 10of patients The consequent saving was estimated to bepound266 million annually in the UK A review conducted byBond (1997) in the USA showed a clear relationshipbetween undernutrition and prolonged hospital stayWhen nutritional intervention was introduced 2 daysearlier than usual the result was a 1-day shortening ofhospital stay It was calculated that a more aggressivenutritional intervention policy would save the averagehospital $1 million per year
Key points
bull Between 30 and 50 of hospital food is wastedbull On average food intake is less than 75 of thatrecommended particularly among the elderlybull The monetary value of hospital food wasted eachyear in England alone is calculated to be pound45 millionBy including labour and overheads this cost rises topound144 millionbull There is also the hidden cost of the extra ill healthassociated with undernutrition because it increasesthe risk of complications lowers resistance to infec-tion impairs physical and mental functioning anddelays recovery
6 Why the problem of undernutrition is exacerbated in hospitals
In more than 60 of patients nutritional status deteri-orates during their stay in hospital with those whoare malnourished on admission particularly affectedPennington (1998) demonstrated that progressive nutri-tional depletion occurs for up to 8 weeks after curativesurgery (eg a heart by-pass operation) This thereforeindicates the need to consider nutritional status fromonset of illness through to complete recovery including
98 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
time after discharge However undernutrition remainsundetected in the majority of patients affected becausemany clinicians and nurses still do not consider nutri-tion to be an important factor in the management of dis-ease (Schenker 2000) and so do not routinely monitornutritional status and body weight Economic analysishas demonstrated that appropriate nutritional treatmentis cost-effective but benefits will only be achieved withhigh standards of nutritional care Multi-professionalnutritional support teams best conduct such treatmentbut there is continuing evidence of poor practice anda high incidence of treatment-related complicationswhich negate the benefits of nutritional treatments(Schenker 2000) In the hospital or institutional settingtherefore the problems that cause undernutrition maybe compounded by the fact that nutritional consider-ations may receive little attention from medical andnursing staff Lack of awareness of the prognostic sig-nificance of undernutrition and lack of knowledgeamong doctors and nurses regarding its assessment andmanagement (Nightingale amp Reeves 1999) may meanthat it is neither looked for nor taken into account whentreatment priorities are being set In particular theremay be failure to
bull identify those with or at risk of nutritional depletionbull identify nutritional requirements especially whenthese are increased because of fever surgery or injurybull provide food of an appropriate quality compositionand consistencybull encourage food intake food is of no benefit if noteatenbull monitor what is actually consumed in some circum-stances direct observation of food and fluid consump-tion is essentialbull identify those whose nutritional needs are not beingmet (through regular weighing or the use of otheranthropometric measurements)bull correct inadequate intake
61 Hospital food and feeding
The following factors have been identified as causes forpoor dietary intake in hospital patients
611 Problems with ordering
bull Menus lack clarity dishes should be described accu-rately so that patients have a reasonable idea of what toexpectbull Help with ordering should be available (but in manycases is not) where there are problems with a patientrsquoscomprehension speech or language
bull Menus are often not printed in languages other thanEnglish This is a particular problem in areas with a highimmigrant population Illiteracy may limit usefulness oftranslated menus Verbal translation may be betterbull Ordering from the menu too far in advance A patientmay be discharged after they have ordered food for thenext day resulting in the bedrsquos new occupant receivingfood chosen by someone else which may be unsuitableSame day ordering systems reduce waste and encourageconsumptionbull Patientsrsquo orders are not checked to ensure that thefood received and the portions requested are correct Inthis respect ward hostesses or feeding care attendantsmay be helpful however this does have financialimplicationsbull Inefficient ordering systems and poor two-way com-munication between the wards and the catering depart-ment lead to waste eg food sent to patients who havebeen discharged transferred or have died Such trays arethen either wasted or given to another patient wholeaves most of it because it was not their choice
612 Menu choice
bull Menus do not always take account of the needs tastesand customary eating habits of different groups ofpatients These will vary according to age race or cul-ture or the disease processbull Menus often do not take account of those needingfortified andor modified-consistency mealsbull Inappropriate promotion of lsquohealthy eatingrsquo eglow-fat diets in undernourished or nutritionally at-riskpatientsbull Some elderly patients often adopt a grazing habit andrequire frequent small volume high energy densityfeeds and snacksbull Special needs Although some disease-specific menuseg for renal failure may be provided from a dietkitchen it may be cost-effective to be able to supplementthe standard menu with high-energy high-proteinadditionsbull Nutritional needs and appetites of children differfrom those of adults and also vary according to ageMeals should be made attractive to children
613 Appropriate food choices
bull Food suitable for lsquohealthy eatingrsquo by the overweightpatient with cardiovascular disease is inappropriate forthe depleted malnourished patientbull Pureacuteed or semisolid diets are required by patientswith neurological or mechanical dysphagia who may be
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

96
Sarah Schenker
copy 2003 British Nutrition Foundation
Nutrition Bulletin
28
87ndash120
Many studies over the last 30 years have since empha-sised the presence of disease-related undernutrition inhospitalised patients (Bistrian
et al
1974 Corish
et al
2000 Hill
et al
1977 Kelly
et al
2000 McWhirter ampPennington 1994) However there is controversy aboutits exact prevalence in the hospital setting One of themajor reasons for this is that there is no universal agree-ment about the definition of undernutrition Becausevarious workers have used different criteria to screen forundernutrition the reported magnitude of the problemhas been highly variable ranging from 10 to 60
Corish
et al
(2000) have screened for undernutritionin patients admitted to two teaching hospitals in DublinTo ensure more reliable comparisons they used thesame criteria employed by McWhirter amp Pennington(1994) in a Dundee hospital 6 years earlier In both stud-ies patients were classified as undernourished if theyhad a BMI
lt
20 kgm
2
and a triceps skinfold thicknessor mid-arm muscle circumference (MAMC) below the15th percentile The incidence of undernutrition innewly admitted patients in Dublin was reported to bemore than threefold lower (11) than in Dundee(40)
This striking difference has led other experts in thefield to question the criteria for defining undernutritionElia amp Stratton (2000) suggest that anthropometric cut-off values should not be used as a diagnostic label ofundernutrition but rather to classify an individualrsquosrisk of undernutrition Some healthy subjects have aBMI
lt
20 kgm2 (especially young adults) and are per-fectly well In addition anthropometric criteria alonesuggest a chronic protein-energy deficiency status How-ever a patient showing substantial recent weight loss(eg greater than 10 weight loss over 3ndash6 months) isat risk of undernutrition and impaired bodily functionseven though the anthropometric cut-off values may nothave been reached
The standard data used for anthropometry requireregular review so that they achieve the right balancebetween reflecting what is the norm (which may not bedesirable) and what is desirable (which may not beappropriate to the current generation) Unlike BMIwhich is a fixed criterion percentile values can showsubstantial change over time For example the referencevalues provided by Bishop et al (1981) for arm anthro-pometry were established in the USA about 30 yearsago The secular trends in obesity over that period meanthat these reference values may no longer apply Fur-thermore the choice of the percentile cut-off for use aspart of the screening tool to classify patients as under-nourished may be inappropriately high (since 15 ofthe reference population falls below this cut-off)
While the picture may be incomplete with regard tothe prevalence of undernutrition in hospitals it is clearthat disease-related undernutrition remains a significantclinical problem in hospitals
However the problem of disease-related undernutri-tion is not confined to people in hospital Within thecommunity up to 10 of people with cancer or otherchronic diseases may be significantly malnourished(Edington et al 1996) and many elderly people are alsoat high risk of undernutrition As a result people arecommonly admitted to hospital nutritionally depletedIn a study conducted in four hospitals in EnglandEdington et al (2000) found that one in every fivepatients admitted was malnourished Patients wereassessed using anthropometric measurements and BMIand by recording history of unintentional weight lossThis figure is likely to be an underestimate because it didnot include those who were too ill on admission to beassessed Kelly et al (2000) estimated that undernutri-tion among acute hospital admissions goes unrecognisedin 70 of cases
Once in hospital undernutrition is likely to get worseIn the study by McWhirter and Pennington two-thirdsof the 500 patients who had been assessed on admis-sion and were reassessed on discharge had lost weightA study on a random sample of 150 in-patients foundapproximately half of them to be either at moderate riskor high risk of undernutrition (Reilly et al 1995) Theprevalence and level of risk is probably higher amonghigh dependency medical surgical geriatric and paedi-atric patients (Reilly et al 1995) As illness and hospi-talisation are frequently associated with weight lossdeterioration in nutritional status is inevitable unlessaction is taken to prevent it
Key points
bull It is estimated that 70 of all undernutrition in theUK goes unrecognised and untreatedbull In the community 5 of the population have aBMI lt 20 kgm2 In hospitals this figure is 20ndash25bull It is estimated that 40 of adults and 15 of chil-dren admitted to hospital are malnourished half ofthese severely so and many others become malnour-ished during their stay in hospitalbull It is estimated that at any one time approximately66 of hospital patients are malnourished
Undernutrition in the UK 97
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
5 Cost of the problem of undernutrition
Undernutrition primarily results in loss of body tissue(depletion of body fat stores and muscle wasting) How-ever because nutrient intake is so closely correlatedwith energy intake a deficiency of energy is likely toresult in an inadequate intake of protein vitamins min-erals and trace elements This can cause widespreadmetabolic physiological and functional effects whichmay include
bull Impaired immune function and hence increased sus-ceptibility to infection and sepsis Infection will furtherimpair a malnourished statebull Delayed wound healingbull Increased risk of pressure sores particularly due toloss of cushioning fat storesbull Muscle wasting and weakness which may affect
ndash Respiratory function impaired respiratory musclestrength makes it difficult for a patient to cough andexpectorate effectively so increasing the risk of chestinfection It may also be more difficult to wean apatient off a ventilatorndash Cardiac function this may be impaired resulting inreduced cardiac output and risk of heart failurendash Mobility weakness of skeletal muscles delays areturn to full mobility Reduced mobility increases therisk of thromboembolism and bedsores
bull Altered structure of the small intestine which mayresult in malabsorptionbull Increased risk of postoperative complicationsbull Apathy and depression leading to loss of morale andreduced will to recoverbull General sense of weakness and illness which impairsappetite and physical ability to eat and hence tends toperpetuate and worsen any undernutrition
In summary undernutrition causes considerable mor-bidity delays recovery and increases the risk of death ABMI at or below the 15th percentile has been shown tobe a significant and independent predictor of death inseriously ill patients (Galanos et al 1997) There is alsoan economic cost in terms of increased need of nursingcare and extended hospital stay
There is clear evidence that correcting undernutritionhas many benefits (Potter et al 1998) Improvements inbody weight status and anthropometric parameters areassociated with improvement in immune function(Chandra 1992 Dionigi et al 1988) wound healing(Haydock amp Hill 1987) and muscle function (Fiataroneamp Evans 1993) and in clinical outcomes such asrecovery time and incidence of postoperativecomplications
Hospitals spend approximately pound15 billion on foodannually and studies conducted in one hospital foundthat 30ndash40 of food is discarded (Kelly 1999) This isconsistent with national estimates that 30ndash50 of hos-pital food is wasted with a monetary value calculated tobe pound45 million each year (Edwards amp Nash 1997Fenton et al 1995) With the inclusion of labour andoverheads this cost rises to pound144 million annuallyThere is also the hidden cost of the extra ill health asso-ciated with undernutrition Some hospitals also typicallyspend approximately pound800 000 on enteral andparenteral nutrition (see Sections 92 and 93) TheKingrsquos Fund (1992) report calculated that provision ofcomprehensive nutrition support would result in a 5-day reduction in hospital stay for approximately 10of patients The consequent saving was estimated to bepound266 million annually in the UK A review conducted byBond (1997) in the USA showed a clear relationshipbetween undernutrition and prolonged hospital stayWhen nutritional intervention was introduced 2 daysearlier than usual the result was a 1-day shortening ofhospital stay It was calculated that a more aggressivenutritional intervention policy would save the averagehospital $1 million per year
Key points
bull Between 30 and 50 of hospital food is wastedbull On average food intake is less than 75 of thatrecommended particularly among the elderlybull The monetary value of hospital food wasted eachyear in England alone is calculated to be pound45 millionBy including labour and overheads this cost rises topound144 millionbull There is also the hidden cost of the extra ill healthassociated with undernutrition because it increasesthe risk of complications lowers resistance to infec-tion impairs physical and mental functioning anddelays recovery
6 Why the problem of undernutrition is exacerbated in hospitals
In more than 60 of patients nutritional status deteri-orates during their stay in hospital with those whoare malnourished on admission particularly affectedPennington (1998) demonstrated that progressive nutri-tional depletion occurs for up to 8 weeks after curativesurgery (eg a heart by-pass operation) This thereforeindicates the need to consider nutritional status fromonset of illness through to complete recovery including
98 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
time after discharge However undernutrition remainsundetected in the majority of patients affected becausemany clinicians and nurses still do not consider nutri-tion to be an important factor in the management of dis-ease (Schenker 2000) and so do not routinely monitornutritional status and body weight Economic analysishas demonstrated that appropriate nutritional treatmentis cost-effective but benefits will only be achieved withhigh standards of nutritional care Multi-professionalnutritional support teams best conduct such treatmentbut there is continuing evidence of poor practice anda high incidence of treatment-related complicationswhich negate the benefits of nutritional treatments(Schenker 2000) In the hospital or institutional settingtherefore the problems that cause undernutrition maybe compounded by the fact that nutritional consider-ations may receive little attention from medical andnursing staff Lack of awareness of the prognostic sig-nificance of undernutrition and lack of knowledgeamong doctors and nurses regarding its assessment andmanagement (Nightingale amp Reeves 1999) may meanthat it is neither looked for nor taken into account whentreatment priorities are being set In particular theremay be failure to
bull identify those with or at risk of nutritional depletionbull identify nutritional requirements especially whenthese are increased because of fever surgery or injurybull provide food of an appropriate quality compositionand consistencybull encourage food intake food is of no benefit if noteatenbull monitor what is actually consumed in some circum-stances direct observation of food and fluid consump-tion is essentialbull identify those whose nutritional needs are not beingmet (through regular weighing or the use of otheranthropometric measurements)bull correct inadequate intake
61 Hospital food and feeding
The following factors have been identified as causes forpoor dietary intake in hospital patients
611 Problems with ordering
bull Menus lack clarity dishes should be described accu-rately so that patients have a reasonable idea of what toexpectbull Help with ordering should be available (but in manycases is not) where there are problems with a patientrsquoscomprehension speech or language
bull Menus are often not printed in languages other thanEnglish This is a particular problem in areas with a highimmigrant population Illiteracy may limit usefulness oftranslated menus Verbal translation may be betterbull Ordering from the menu too far in advance A patientmay be discharged after they have ordered food for thenext day resulting in the bedrsquos new occupant receivingfood chosen by someone else which may be unsuitableSame day ordering systems reduce waste and encourageconsumptionbull Patientsrsquo orders are not checked to ensure that thefood received and the portions requested are correct Inthis respect ward hostesses or feeding care attendantsmay be helpful however this does have financialimplicationsbull Inefficient ordering systems and poor two-way com-munication between the wards and the catering depart-ment lead to waste eg food sent to patients who havebeen discharged transferred or have died Such trays arethen either wasted or given to another patient wholeaves most of it because it was not their choice
612 Menu choice
bull Menus do not always take account of the needs tastesand customary eating habits of different groups ofpatients These will vary according to age race or cul-ture or the disease processbull Menus often do not take account of those needingfortified andor modified-consistency mealsbull Inappropriate promotion of lsquohealthy eatingrsquo eglow-fat diets in undernourished or nutritionally at-riskpatientsbull Some elderly patients often adopt a grazing habit andrequire frequent small volume high energy densityfeeds and snacksbull Special needs Although some disease-specific menuseg for renal failure may be provided from a dietkitchen it may be cost-effective to be able to supplementthe standard menu with high-energy high-proteinadditionsbull Nutritional needs and appetites of children differfrom those of adults and also vary according to ageMeals should be made attractive to children
613 Appropriate food choices
bull Food suitable for lsquohealthy eatingrsquo by the overweightpatient with cardiovascular disease is inappropriate forthe depleted malnourished patientbull Pureacuteed or semisolid diets are required by patientswith neurological or mechanical dysphagia who may be
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients
Undernutrition in the UK 97
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
5 Cost of the problem of undernutrition
Undernutrition primarily results in loss of body tissue(depletion of body fat stores and muscle wasting) How-ever because nutrient intake is so closely correlatedwith energy intake a deficiency of energy is likely toresult in an inadequate intake of protein vitamins min-erals and trace elements This can cause widespreadmetabolic physiological and functional effects whichmay include
bull Impaired immune function and hence increased sus-ceptibility to infection and sepsis Infection will furtherimpair a malnourished statebull Delayed wound healingbull Increased risk of pressure sores particularly due toloss of cushioning fat storesbull Muscle wasting and weakness which may affect
ndash Respiratory function impaired respiratory musclestrength makes it difficult for a patient to cough andexpectorate effectively so increasing the risk of chestinfection It may also be more difficult to wean apatient off a ventilatorndash Cardiac function this may be impaired resulting inreduced cardiac output and risk of heart failurendash Mobility weakness of skeletal muscles delays areturn to full mobility Reduced mobility increases therisk of thromboembolism and bedsores
bull Altered structure of the small intestine which mayresult in malabsorptionbull Increased risk of postoperative complicationsbull Apathy and depression leading to loss of morale andreduced will to recoverbull General sense of weakness and illness which impairsappetite and physical ability to eat and hence tends toperpetuate and worsen any undernutrition
In summary undernutrition causes considerable mor-bidity delays recovery and increases the risk of death ABMI at or below the 15th percentile has been shown tobe a significant and independent predictor of death inseriously ill patients (Galanos et al 1997) There is alsoan economic cost in terms of increased need of nursingcare and extended hospital stay
There is clear evidence that correcting undernutritionhas many benefits (Potter et al 1998) Improvements inbody weight status and anthropometric parameters areassociated with improvement in immune function(Chandra 1992 Dionigi et al 1988) wound healing(Haydock amp Hill 1987) and muscle function (Fiataroneamp Evans 1993) and in clinical outcomes such asrecovery time and incidence of postoperativecomplications
Hospitals spend approximately pound15 billion on foodannually and studies conducted in one hospital foundthat 30ndash40 of food is discarded (Kelly 1999) This isconsistent with national estimates that 30ndash50 of hos-pital food is wasted with a monetary value calculated tobe pound45 million each year (Edwards amp Nash 1997Fenton et al 1995) With the inclusion of labour andoverheads this cost rises to pound144 million annuallyThere is also the hidden cost of the extra ill health asso-ciated with undernutrition Some hospitals also typicallyspend approximately pound800 000 on enteral andparenteral nutrition (see Sections 92 and 93) TheKingrsquos Fund (1992) report calculated that provision ofcomprehensive nutrition support would result in a 5-day reduction in hospital stay for approximately 10of patients The consequent saving was estimated to bepound266 million annually in the UK A review conducted byBond (1997) in the USA showed a clear relationshipbetween undernutrition and prolonged hospital stayWhen nutritional intervention was introduced 2 daysearlier than usual the result was a 1-day shortening ofhospital stay It was calculated that a more aggressivenutritional intervention policy would save the averagehospital $1 million per year
Key points
bull Between 30 and 50 of hospital food is wastedbull On average food intake is less than 75 of thatrecommended particularly among the elderlybull The monetary value of hospital food wasted eachyear in England alone is calculated to be pound45 millionBy including labour and overheads this cost rises topound144 millionbull There is also the hidden cost of the extra ill healthassociated with undernutrition because it increasesthe risk of complications lowers resistance to infec-tion impairs physical and mental functioning anddelays recovery
6 Why the problem of undernutrition is exacerbated in hospitals
In more than 60 of patients nutritional status deteri-orates during their stay in hospital with those whoare malnourished on admission particularly affectedPennington (1998) demonstrated that progressive nutri-tional depletion occurs for up to 8 weeks after curativesurgery (eg a heart by-pass operation) This thereforeindicates the need to consider nutritional status fromonset of illness through to complete recovery including
98 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
time after discharge However undernutrition remainsundetected in the majority of patients affected becausemany clinicians and nurses still do not consider nutri-tion to be an important factor in the management of dis-ease (Schenker 2000) and so do not routinely monitornutritional status and body weight Economic analysishas demonstrated that appropriate nutritional treatmentis cost-effective but benefits will only be achieved withhigh standards of nutritional care Multi-professionalnutritional support teams best conduct such treatmentbut there is continuing evidence of poor practice anda high incidence of treatment-related complicationswhich negate the benefits of nutritional treatments(Schenker 2000) In the hospital or institutional settingtherefore the problems that cause undernutrition maybe compounded by the fact that nutritional consider-ations may receive little attention from medical andnursing staff Lack of awareness of the prognostic sig-nificance of undernutrition and lack of knowledgeamong doctors and nurses regarding its assessment andmanagement (Nightingale amp Reeves 1999) may meanthat it is neither looked for nor taken into account whentreatment priorities are being set In particular theremay be failure to
bull identify those with or at risk of nutritional depletionbull identify nutritional requirements especially whenthese are increased because of fever surgery or injurybull provide food of an appropriate quality compositionand consistencybull encourage food intake food is of no benefit if noteatenbull monitor what is actually consumed in some circum-stances direct observation of food and fluid consump-tion is essentialbull identify those whose nutritional needs are not beingmet (through regular weighing or the use of otheranthropometric measurements)bull correct inadequate intake
61 Hospital food and feeding
The following factors have been identified as causes forpoor dietary intake in hospital patients
611 Problems with ordering
bull Menus lack clarity dishes should be described accu-rately so that patients have a reasonable idea of what toexpectbull Help with ordering should be available (but in manycases is not) where there are problems with a patientrsquoscomprehension speech or language
bull Menus are often not printed in languages other thanEnglish This is a particular problem in areas with a highimmigrant population Illiteracy may limit usefulness oftranslated menus Verbal translation may be betterbull Ordering from the menu too far in advance A patientmay be discharged after they have ordered food for thenext day resulting in the bedrsquos new occupant receivingfood chosen by someone else which may be unsuitableSame day ordering systems reduce waste and encourageconsumptionbull Patientsrsquo orders are not checked to ensure that thefood received and the portions requested are correct Inthis respect ward hostesses or feeding care attendantsmay be helpful however this does have financialimplicationsbull Inefficient ordering systems and poor two-way com-munication between the wards and the catering depart-ment lead to waste eg food sent to patients who havebeen discharged transferred or have died Such trays arethen either wasted or given to another patient wholeaves most of it because it was not their choice
612 Menu choice
bull Menus do not always take account of the needs tastesand customary eating habits of different groups ofpatients These will vary according to age race or cul-ture or the disease processbull Menus often do not take account of those needingfortified andor modified-consistency mealsbull Inappropriate promotion of lsquohealthy eatingrsquo eglow-fat diets in undernourished or nutritionally at-riskpatientsbull Some elderly patients often adopt a grazing habit andrequire frequent small volume high energy densityfeeds and snacksbull Special needs Although some disease-specific menuseg for renal failure may be provided from a dietkitchen it may be cost-effective to be able to supplementthe standard menu with high-energy high-proteinadditionsbull Nutritional needs and appetites of children differfrom those of adults and also vary according to ageMeals should be made attractive to children
613 Appropriate food choices
bull Food suitable for lsquohealthy eatingrsquo by the overweightpatient with cardiovascular disease is inappropriate forthe depleted malnourished patientbull Pureacuteed or semisolid diets are required by patientswith neurological or mechanical dysphagia who may be
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

98 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
time after discharge However undernutrition remainsundetected in the majority of patients affected becausemany clinicians and nurses still do not consider nutri-tion to be an important factor in the management of dis-ease (Schenker 2000) and so do not routinely monitornutritional status and body weight Economic analysishas demonstrated that appropriate nutritional treatmentis cost-effective but benefits will only be achieved withhigh standards of nutritional care Multi-professionalnutritional support teams best conduct such treatmentbut there is continuing evidence of poor practice anda high incidence of treatment-related complicationswhich negate the benefits of nutritional treatments(Schenker 2000) In the hospital or institutional settingtherefore the problems that cause undernutrition maybe compounded by the fact that nutritional consider-ations may receive little attention from medical andnursing staff Lack of awareness of the prognostic sig-nificance of undernutrition and lack of knowledgeamong doctors and nurses regarding its assessment andmanagement (Nightingale amp Reeves 1999) may meanthat it is neither looked for nor taken into account whentreatment priorities are being set In particular theremay be failure to
bull identify those with or at risk of nutritional depletionbull identify nutritional requirements especially whenthese are increased because of fever surgery or injurybull provide food of an appropriate quality compositionand consistencybull encourage food intake food is of no benefit if noteatenbull monitor what is actually consumed in some circum-stances direct observation of food and fluid consump-tion is essentialbull identify those whose nutritional needs are not beingmet (through regular weighing or the use of otheranthropometric measurements)bull correct inadequate intake
61 Hospital food and feeding
The following factors have been identified as causes forpoor dietary intake in hospital patients
611 Problems with ordering
bull Menus lack clarity dishes should be described accu-rately so that patients have a reasonable idea of what toexpectbull Help with ordering should be available (but in manycases is not) where there are problems with a patientrsquoscomprehension speech or language
bull Menus are often not printed in languages other thanEnglish This is a particular problem in areas with a highimmigrant population Illiteracy may limit usefulness oftranslated menus Verbal translation may be betterbull Ordering from the menu too far in advance A patientmay be discharged after they have ordered food for thenext day resulting in the bedrsquos new occupant receivingfood chosen by someone else which may be unsuitableSame day ordering systems reduce waste and encourageconsumptionbull Patientsrsquo orders are not checked to ensure that thefood received and the portions requested are correct Inthis respect ward hostesses or feeding care attendantsmay be helpful however this does have financialimplicationsbull Inefficient ordering systems and poor two-way com-munication between the wards and the catering depart-ment lead to waste eg food sent to patients who havebeen discharged transferred or have died Such trays arethen either wasted or given to another patient wholeaves most of it because it was not their choice
612 Menu choice
bull Menus do not always take account of the needs tastesand customary eating habits of different groups ofpatients These will vary according to age race or cul-ture or the disease processbull Menus often do not take account of those needingfortified andor modified-consistency mealsbull Inappropriate promotion of lsquohealthy eatingrsquo eglow-fat diets in undernourished or nutritionally at-riskpatientsbull Some elderly patients often adopt a grazing habit andrequire frequent small volume high energy densityfeeds and snacksbull Special needs Although some disease-specific menuseg for renal failure may be provided from a dietkitchen it may be cost-effective to be able to supplementthe standard menu with high-energy high-proteinadditionsbull Nutritional needs and appetites of children differfrom those of adults and also vary according to ageMeals should be made attractive to children
613 Appropriate food choices
bull Food suitable for lsquohealthy eatingrsquo by the overweightpatient with cardiovascular disease is inappropriate forthe depleted malnourished patientbull Pureacuteed or semisolid diets are required by patientswith neurological or mechanical dysphagia who may be
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients
Undernutrition in the UK 99
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
unable to cope with either liquid or solid food Suchdiets can have low-energy contents and this may needattention
614 Quality and presentation
bull The general appearance and presentation of food isoften poor in hospitals These aspects are very impor-tant and influence whether or not food is consumedbull Lack of variety may be a problem for longer-staypatientsbull In many hospitals the kitchens are situated far awayfrom the wards This has implications for how far inadvance food is prepared and how it is transported tothe wards In addition some hospitals buy in externallyprepared food which is heated up on the premises againpotentially affecting taste and presentationbull Methods used are not always most conducive to pres-ervation of nutrient content and palatabilitybull Food served from trolleys by the bedside may aidchoice and induce greater consumption than provisionof a plated meal where the patient has little control overportion size Some patients find receiving a large mealvery off-putting
615 Quality portion control
bull Insufficient account is taken of the evidence fromnutritional science of the differing energy and proteinrequirements of patients of different age sex size cur-rent nutritional status and disease processbull Portion control is often poor or non-existent
616 Interference with meal times by ward rounds investigations and procedures
bull Delayed meals may spoil and become unappetisingbull Meals are often missed rather than saved or a substi-tute providedbull Patients are reluctant to eat after others have finishedThe social encouragement to eat is lostbull lsquoNil-by-mouthrsquo orders may be used inappropriately orprolonged unnecessarily A patient may be kept nil-by-mouth all morning only to find that their treatment hasbeen cancelled or delayed
617 Timing
bull Meal times are often inflexible and ill-adapted topatientsrsquo normal habitsbull There can be long gaps between some meals eg 12 hbetween the evening meal and breakfast and narrow
gaps between others eg 4 h between breakfast andlunch ndash more suited to administrative convenience thanpatient needsbull Preferences of the local patient population should besought and adoptedbull Lack of access to nutritious snacks and drinksbetween meals
618 Medication (see Section 62 for more details)
bull Many drugs cause anorexia taste changes nauseavomiting or constipation thereby reducing food intakeSuch drugs can sometimes be stopped or changed fol-lowing discussion between medical and pharmacy staffwithout detriment to treatment
619 Physical problems
bull As a result of paralysis fractures arthritis or othermusculo-skeletal problems a patient may be unable tounwrap or access food and drinkbull Eating utensils may be ill-suited to the needs ofpatients with disability who require utensils that areeasier to holdbull False teeth may be lost misplaced or not fitted atmealtimesbull False teeth may be poor fittingbull Patients with impaired hearing or vision may have dif-ficulty ordering food or eating it when it arrives
6110 Position
bull The tray may be placed by untrained staff out ofreach of the patient who may be too ill to botherreaching out for it or because of a disability be unableto do sobull The patient may not have been positioned properly tofacilitate manipulation eating and swallowing of foodEating lying down is difficult and can be dangerous(Royal Institute of Public Health 2002)
6111 Help with eating
bull Sick people give up easily and need encouragementbull Patients who need special help are not alwaysidentifiedbull Nurses rarely have time to help patients eatbull Few hospitals employ trained ward hostesses or careassistants to help patients with food choices and to pro-vide encouragement and help at meal timesbull Insufficient staff are available at meal times to assistor monitor patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients
100 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bull Untrained orderlies care assistants or volunteers maynot report uneaten meals but simply place the trayat the bedside and remove it unquestioningly if it isuntouched
6112 Environment
bull This has an important effect on meal consumptionEating is a social activity and may be enhanced ifpatients on the ward eat togetherbull Patients who are able to move about are likely to eatmore in an attractive dining area with social interactionbull Those eating at the bedside may be put off by unpleas-ant odours and the behaviour or medical condition ofother patients The use of commodes should be discour-aged at meal timesbull Some patients with disabilities are embarrassed bytheir own messy eating and avoid this by leaving food
6113 Communication
bull There is often poor communication between cateringand nursing staff over menus ordering food and servingmealsbull Staff who serve meals may not tell nursing staff whenpatients leave most of their meal and nurses may notdiscover or record the fact through pressure of otherwork or lack of motivation or understanding of theclinical importance of such observationsbull There is often poor communication between dieteticnursing and catering staff
6114 Failure of management
bull The provision of policies design of protocols and set-ting of standards for food service in hospitals is gener-ally inadequatebull Cost is often cited unjustifiably as a reason for notimplementing change in food service or mealtimeroutines
6115 Education
bull Previous surveys have shown the low standard ofnutritional knowledge among medical and nursing staffto be one of the main impediments to improving patientnutrition (see Section 74 for how this problem is nowbeing addressed)bull Education of catering and domestic staff in basicnutrition is essential if they are to appreciate andexecute their vital role in the provision of food as atreatment
Despite the enormous complexities involved in feedingpatients and despite its vital role in patient recovery theplanning and delivery of a good food service is oftenoverlooked Some hospitals have introduced smallyet effective measures to aid patient feeding Theseinclude employing dietetic helpers to assist with feedingpatients on the wards or serving the main meal of theday in the evening rather than at mid-day which is morefamiliar and comfortable for the majority of patientsMany hospitals have changed from plated meals to bulktrolley service giving the patient a better choice andensuring that food is still hot by the time it is served InNorthern Ireland one Health Authority has ruled thatduring lunchtimes no other ward activity should takeplace and all staff effort should concentrate on feedingpatients
62 Drugndashnutrient interactions
Drugs and nutrients interact in many ways because theyare absorbed from similar sites and metabolised andend products excreted by similar processes Food intakecan be altered or decreased as a consequence of theside-effects of drugs It is therefore important to assessthe effect of patientsrsquo medication on their nutritionalstatus
While the greatest impact on nutritional status is fromprescribed drugs some over-the-counter preparationsexert pharmacological effects that have nutritionalimplications These include
bull indigestion remedies analgesics and laxatives that canimpact on nutrition as well as being an indication ofpoor eating habitsbull herbal remediesbull misuse of nutritional supplements or mega-dosing ofvitamins or minerals
621 Effect of nutrition on drugs
Nutritional factors influence drug absorption actionand effectiveness The presence or absence of food caneither delay or enhance the rate and extent to whichan orally administered drug is absorbed through effectson gastric emptying gastrointestinal pH competitionfor binding sites and the presence of components offood such as iron and calcium ions Some drugs shouldbe taken on an empty stomach to maximise theirabsorption rate Conversely other drugs must betaken with food to achieve a slower sustained rate ofabsorption
Periods of short-term starvation or prolonged periods
Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

Undernutrition in the UK 101
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
of poor nutritional intake can influence the effectivenessor safety of a drug Body weight determines the amountof drug required to produce a certain pharmacologicaleffect Therefore sudden weight loss or dehydration canresult in an overdose Undernutrition also reduces theactivity of microsomal drug-metabolising enzymes andthis can diminish a drugrsquos effectiveness by reducing therate of synthesis of an active metabolite or enhancing itstoxicity by reducing the rate of its excretion (Truswell2000) This emphasises the importance of ensuring goodnutrition during an illness that is being treated withdrugs
622 Effects of drugs on nutrition
Food intake may be reduced as a result of the followingside-effects
bull Anorexia ndash either as a direct effect of the drug onappetite or as a result of side-effects such as drowsinessor lethargybull Nausea or vomitingbull Effect on the gastrointestinal tract ndash such asindigestion heartburn or gastritis bloating earlysatiety (feeling full after eating very little) or abdominalpainbull Taste changesbull Dry or sore or painful mouthbull Confusionbull Specific interference eg some antibiotics on theabsorption of folate
Furthermore nutrient absorption can then be impairedas a result of the following
bull Formation of insoluble complexes ndash many drugs canchelate with minerals and trace elementsbull Competition for binding sites within the intestinalmucosabull Damage to the absorptive surface of the intestinalmucosabull Lack of bile acids ndash affecting the absorption of fat sol-uble vitaminsbull Increased intestinal motility ndash causing diarrhoea
It is important to recognise that poor nutritionalstatus can impair drug metabolism and that drugtreatment can have a detrimental effect on nutritionalstatus Although in many instances losses in nutrientavailability or drug action will be small or short-livedthose most at risk from interactions are patients ina nutritionally compromised state those who haveexperienced recent weight loss or who are dehydrated
7 What can and is being done
Improvements are on-going at every level of patient careto help combat undernutrition in hospitals New strat-egies include changes within the National Health Service(NHS) to help identify patients at risk of malnutritionsetting up government bodies to develop standards fortreating malnutrition improvements in hospital foodand its provision improvements in teaching nutrition tomedical nursing and other health care professionalsgovernment initiatives being conducted in the commu-nity to reduce the prevalence of undernutrition whichwill in turn help reduce the number of patients who areundernourished on admission Each of these strategies isdiscussed further below
71 Changes within the NHS
The NHS Plan (Department of Health 2000) detailsfuture reforms for the NHS There is planned action tointroduce a hospital nutrition policy to improve the out-come of care for patients
Both the Nuffield Trust (1999) and BAPEN (1999)reports recommended that robust indicators concerningnutritional care of nutritionally at-risk or malnourishedpeople in hospital to fit the National Service Framework(NSF) should be developed and agreed NSFs have beenset out by the National Institute for Clinical Excellencewhich has been set up in England to develop standardsof best practice in health care (NHS Executive 1998)The frameworks provide a plan of action by which totackle major health issues and important diseases Cur-rently a framework is being set up to include require-ments for best practice in food service The frameworkwill need to be consistent with similar frameworks thathave been developed for related aspects of care eg careof elderly people (httpwwwdohgovuknsf) This willmean that authorities will have their own explicit writ-
Key pointsbull In many hospitals the quality of the food has beenpoor (see Section 72) and existing feeding policiesare inadequatebull Such problems include the limited choice the wayfood is served and the lack of help for those unableto feed themselves properlybull Others need additional nutritional support but thisoften goes unrecognisedbull Food intake can be altered or decreased as a con-sequence of drug side-effects
102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

102 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ten nutritional standards and guidelines based on offi-cial national standards Appropriate funding will haveto be made available to attain these standards For nutri-tion to have the status it deserves within the trustmanagement environment trust boards must be fullycommitted to the notion of food provision being a keycomponent of clinical care and subject to the clinicalgovernance programme The inspection body that willenforce NSFs is The Commission for Health Improve-ment and this has the ultimate sanction to dismiss theboard of a hospital trust
72 Improvements in hospital food
In May 2001 the government launched Better HospitalFood a new menu for the NHS as part of a pound40 millionscheme to overhaul hospital food The emphasis is onproviding calorific and nutritious food and a 24-hsnack box service of chocolate and crisps with fruit isavailable for patients who miss meals The NHS menuoffers more choices more fresh food and more optionsfor vegetarians and others with specialised diets (seebelow) Forty-three of the new dishes known as lsquoChefrsquosSpecialsrsquo have been designed by expert chefs andinclude lsquosteak and kidney pie with olive oil mashrsquo lsquocau-liflower with very cheesy saucersquo and lsquoposh pear andchocolate crumblersquo These dishes are part of theNational Dish Selector and have been extensively tri-alled and tested with patients hospital chefs and dieti-tians Each dish costs approximately 80 p per servingAccompanying the menu are guidelines for the deliveryof services timing availability flexibility and presen-tation have all been considered Introduction of thenational menu and the national dish list is the first stepin the process of revitalising NHS catering the menu hasbeen sent out as a national cookery book to all hospitaltrusts (Better Hospital Food 2001)
Better Hospital Food is part of a long-term pro-gramme to continually improve catering services in hos-pitals The three objectives are
bull to ensure all hospitals meet the required standardsbull to bring all hospitals to existing levels of excellencebull to develop and introduce across the NHS new cater-ing systems which provide modern services that areboth efficient and responsive to the needs of patients
Better Hospital Food is a blueprint for the revitalisa-tion of NHS catering across the country reflectingchanges in social patterns the way we eat and our evolv-ing tastes for a wider variety of foods The aim is to pro-vide patients with a service that encourages them to eatenough food to satisfy their nutritional requirements by
offering them foods that they will want to eat at timesthey want to eat them Each hospital will receive anImplementation Support Pack which has been designedto assist hospitals in meeting the challenge set out in theNHS Plan and offers a practical source of help andadvice
In addition to those for whom a lsquotraditionalrsquo diet issuitable The NHS Menu includes options for childrenvegetarians those preferring a soft diet those with spe-cial dietary needs because of religious or cultural obser-vance certain patients who have to follow a medicallymodified diet The menu also has an lsquoAll Hoursrsquo sectionsetting out the 24-h catering service Hospitals shouldensure that the range of meals available in each sectionhas been specifically designed to reflect the needs ofpatients within those groups
All dishes have been designed to meet adequate nutri-tional standards including meeting criteria for
bull dietary reference values (Department of Health1991)bull coding for common therapeutic dietsbull food textures and consistencybull food rules of different religions
The National Dish Selector contains dishes designedby both expert chefs (see above) and the NHS group ofcatering managers dietitians and nurses Trusts areencouraged to adopt dishes from the Dish Selectorwhenever possible thus alleviating the need to continu-ally develop recipes and undertake nutritional analysisof these at every hospital With the exception of thoselabelled lsquoChefrsquos Specialsrsquo that have been developed bythe expert chefs use of which is mandatory it is notcompulsory for hospitals to use the exact recipes
The Better Hospital Food plan also proposes that inorder to reflect changes in modern eating habits themain meal of the day should be served in the eveningHowever some groups of patients particularly olderpatients still prefer their main meal at mid-day Trustsare therefore encouraged to ensure that delivery ofthe main meal continues to meet the needs of thehospital population in the short term but that intime adjustments are made to meet the requirementsof the plan Serving the main meal of the day in theevening should have been implemented in all trusts byDecember 2002
However it is important to recognise that improve-ment in provision is only the first step in helping toreduce the incidence of undernutrition in hospitals TheRoyal College of Nursing welcomed the initiative butstressed that it was important to recognise that therewere many other problems related to the practical
Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

Undernutrition in the UK 103
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
aspects of feeding patients in hospitals other than thenutritional content quality and variety of foods served(Royal College of Nursing personal communication)Once a suitable meal that is both appetising and of anadequate nutritional standard is served to the patienthelp with eating must also be provided when necessaryThis is one of the most important problems faced byhospitals as there are staffing implications (eg feeding apatient who has had a stroke can take 30 min) Thepatient should be in a comfortable position in a pleas-ant environment and practical issues such as use ofspecial cutlery and good fitting dentures should be con-sidered If a patient does not eat a meal it is importantfor the nurse or carer to identify the problem and itssolution
Information about Better Hospital Food can be foundat httpwwwbetterhospitalfoodcom
73 Improvements in the provision of hospital food
The Nuffield Trust (1999) and BAPEN (1999) reportsboth called for a nutrition steering group to be set upwithin each trust A named senior health professionalshould have responsibility for co-ordinating nutritionalcare services across the entire trust The steering groupshould give consideration to
bull transferring the catering and nutritional care servicefrom the domestic facilities budget to the clinical sup-port and treatment service budgetbull setting up a new nutrition directorate with overallresponsibility for all aspects of nutritional care
The steering group should have the power to makerecommendations and implement change It should con-sist of a core group including the chief dietitian the chiefcatering officer a manager from the finance section asenior clinician with a special interest in nutrition asenior nurse or nutrition nurse specialist and a phar-macist The steering group must be involved in contrac-tual arrangements for catering or in the development ofin-house catering services from the beginning It shouldalso be responsible for evaluating the experience ofother centres and seeking expert advice The chief die-titian should have executive not just advisory input intothe catering services
Another set of recommendations made by theNuffield Trust (1999) and BAPEN (1999) focus on wardpracticalities
bull The timing of meals should be reviewed and mademore relevant to patientsrsquo customary meal patterns Allfood preparation methods (eg in-house cook-serve or
brought-in cook-chill ndash heated up and served at wardlevel) have proved successful but are highly dependenton the method of distribution and service With propermanagement a bulk trolley bedside service best servespatientsrsquo needs and is the recommended methodbull Nutritionally vulnerable patients should be placed inwards with kitchen areas or near ward kitchens In thisway special meals or snacks can be prepared forpatients or when possible they can access the kitchenthemselvesbull Delivering the food to the patient is one thing ensur-ing that it has been eaten is quite another The nurses incharge of the ward have primary responsibility for thenutritional care of in-patients BAPEN and the NuffieldTrust advise that food should be served by nurses sup-ported where necessary by other grades of staff trainedfor this purpose (eg ward hostesses diet technicianshelpers) Assistance with eating must be provided whereit is needed Plate or tray collection should be supervisedby nursing staff to enable patientsrsquo food intake to bemonitored
Both the BAPEN and Nuffield Trust reports recognisethat all members of the multi-disciplinary team butnursing staff in particular should be aware of drugs thatcause anorexia nausea or gastrointestinal side-effectsand should seek to stop or minimise the use of suchdrugs where possible Polypharmacy in the elderly isparticularly culpable in this respect In some cases of ter-minal disease nutritional status inevitably continues todeteriorate and over-aggressive nutritional interventionmay not be appropriate
Thirty years after they were abolished the govern-ment has re-introduced matrons as a step towards driv-ing up standards of nutrition and feeding practices onwards Among matronsrsquo responsibilities will be toensure that the food is good and patients are fedproperly The aim is to have 2000 matrons in place by2004
74 Improvements in the nutrition education of health professionals and care workers
741 Health professionals
The Malnutrition Advisory Group (MAG) launched in1999 was established to combat undernutrition in theUK (Elia 2001) MAG consists of hospital doctors aca-demics dietitians and other members of the primaryhealth care team and seeks to raise awareness andunderstanding of undernutrition to ensure the issue isgiven priority by health care professionals and policy
104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

104 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
makers As part of this process MAG has producedguidelines for the treatment and identification of under-nutrition in the community with the aim of improvingpatient care and reducing NHS costs
Previously the training in nutrition for health careprofessionals was fragmentary MAG has highlightedthe need for further education and training for healthcare professionals particularly doctors and nurses toraise the awareness of the importance of food and nutri-tion This followed a MORI survey that MAG commis-sioned which showed that doctors would like furthertraining and education in nutrition 60 of generalpractitioners (GPs) felt they needed further training indetection of undernutrition and 74 of GPs had noundergraduate training in nutrition
A working party of the Royal College of Physicianshas recently published a report (Royal College ofPhysicians 2002) focusing on the responsibility of doc-tors for the nutritional care of patients The reporthighlights the impact of both undernutrition and over-nutrition on disease processes the influence of illness onnutrition and the potential for nutritional interventionto contribute to disease management and preventionRecommendations are made for clinical governance toaddress potential shortcomings in patient care and toprovide methods for improving the nutritional knowl-edge and skills of doctors
A core curriculum which has been accepted by allundergraduate medical schools has been developed forundergraduates to provide a standard for training thatensures safe practice The curriculum identifies 18 keylearning points including the principles of nutritionalscience public health nutrition clinical nutrition andnutritional support The Royal Colleges have responsi-bility for the postgraduate training of doctors An inter-collegiate group on nutrition has been formed and runsthree 1-week foundation courses for doctors at differ-ent centres around the country For more informationsee httpwwwicgnutritionorguk
742 Care workers
The Caroline Walker Trust has been pivotal in thenutritional education of care workers working indifferent establishments The work of the trust isparticularly targeted towards nutritionally vulnerablegroups and people who need special help with feedingNutritional and practical guidelines have been producedfor
bull school meals (Caroline Walker Trust 1992)bull older people in residential and nursing homes
(Caroline Walker Trust 1995) including special guide-lines for those with dementia (Caroline Walker Trust1998a)bull under-5s in childcare (Caroline Walker Trust 1998b)
The most recent project (Caroline Walker Trust 2001)is a report on the nutritional and practical guidelines forlooked-after children and young people and is aimed tohelp carers provide a nutritionally balanced varied andtasty diet The report is accompanied by a training man-ual and a computer program CHOMP for planningmenus for under-5s in childcare was launched in 2001This is to help users produce varied and interestingmenus to satisfy the nutritional guidelines detailed in thereport The program is similar to the CORA menu plan-ner for those catering in residential and nursing homesfor older people
For more information on the Caroline WalkerTrust and details of other publications see httpwwwcwtorguk
75 Community initiatives
The Womenrsquos Royal Voluntary Service has been themain body for the running of the Meals on Wheelsscheme across the UK which has been in operation since1943 The majority of meals are provided by three maincatering companies which are required to meet nutri-tional criteria specified by either the Caroline WalkerTrust or the Advisory Body of Social Services CateringFor further information see httpwwwwrvsorguk
In the last few years the problems associated with apoor dietary intake have received government attentionA number of reports have been published including theNutrition Task Force Eat Well II (Department of Health1996a) the Low Income Project Teamrsquos Report(Department of Health 1996b) the Independent Inquiryinto Inequalities in Health (Acheson 1998) BringingBritain Together (Social Exclusion Unit 1998) andSaving Lives Our Healthier Nation (Department ofHealth 1999a) These reports identify the link betweendiet and health and consider the difficulties of thoseliving on a low income They have resulted in a numberof action plans and policies designed to tackle all thethings which make people ill (Department of Health1999b) by taking a holistic approach which includesnutrition
The Neighbourhood Renewal Unit was set up withthe aim of narrowing the gap between deprived neigh-bourhoods and the rest of the country by delivering bet-ter health as well as better education and better housingamong other services It is hoped that better health will
Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

Undernutrition in the UK 105
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
be achieved through the Renewal Neighbourhood FundNew Deal for Communities and the Single Regenera-tion Budget For more information see httpwwwneighbourhooddtlrgovuk Related to this the Depart-ment of Health has recently issued proposals to revisethe Welfare Foods Scheme which currently benefitspregnant women and children under 5 years living infamilies receiving income support and Job SeekersAllowance (Department of Health 2002ab) Thescheme currently benefits pregnant women and under-5sliving in families receiving Income Support and Job-seekers allowance and also provides milk for nurseryschool children (See httpwwwdohgovukcomawelfarefoodsreviewpdf)
Sure Start has been set up by the government to tacklechild poverty and social exclusion The aim is to have500 Sure Start local programmes in operation by 2004concentrated in areas where a high proportion of chil-dren are living in poverty Local programmes will workwith parents and parents-to-be to improve childrenrsquoslife chances through better access to health servicesamong others For more information see httpwwwsurestartgovuk Again related to this is Welfare FoodsScheme (Department of Health 2002ab)
Education Action Zones and Health Action Zoneshave been launched by the Department for Educationand Skills and the Department of Health respectivelyBoth initiatives include poor diet and nutritional intakeas a problem to be tackled in improving performance inschool and improving the health of those who are worstoff For further information see httpwwwdfesgovukand httpwwwdohgovukpricarehazhtm
The Healthy Living Centre initiative was set up in1999 under the New Opportunities Fund the lotterybody established under the National Lottery Act Theprogramme promotes health in its broadest sense andtargets areas and groups in the most disadvantaged sec-tors of the population Funds are awarded to someapplicants from Healthy Action Zones Schemes includecommunity cafes luncheon clubs for older people andactivities such as swimming classes and lsquowalking forhealthrsquo schemes For further information visit httpwwwdohgovukhlcindexhtm
The Low Income Project Team set up by the govern-mentrsquos Nutrition Task Force in the early 1990s identi-fied strategic priorities that will help low-incomehouseholds gain access to an adequate variety of good-quality food that is within their financial grasp to haveinformation to help them make appropriate foodchoices and to obtain the skills and facilities to preparefood (Department of Health 1996b) The followingobjectives contribute to this goal
bull To increase the control that people living on lowincomes have in matters related to food ensuring morereal choice and affordable good-quality foodbull To develop and improve opportunities for the UKrsquosfood manufacturing and retailing industriesbull To increase opportunities for choice by diverse meanswhether retailing competition different pricing policiesbetter individual and collective skills and educationimproved shopping access and involvement by localpeoplebull To increase the collective money available for food bymaximising income through better take-up of availablebenefitsbull To nurture local food partnerships influencing wherewhen and at what price people can buy their food
Numerous individual projects have been set up as aresult of these objectives including
bull food co-operatives and mobile shopsbull cookery and shopping skills coursesbull development and provision of healthy recipe leafletsbull community cafes and lunch clubs providing healthyfood at low costbull food and nutrition education coursesbull meal provision for those with special needsbull food couponsbull transport to shops
The overall aim is to reduce inequalities and improvehealth including nutritional status thus reducing theincidence and prevalence of undernutrition in thecommunity Details of these sorts of projects andinformation about their effectiveness can be found onSustainrsquos website httpwwwsustainweborg and theHealth Development Agencyrsquos website httpwwwhda-onlineorguk
Key points
bull There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being metbull Fortified meals between-meal snacks and adequateward staffing have all been shown to contribute toachieving this goal which leads to better clinical out-come less waste shorter hospital stay and a morecost-effective service
Continued
106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

106 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
8 Screening for undernutrition
81 Nutritional screening and assessment of patients in hospitals
It has been recommended that all patients admitted tohospital are assessed for nutritional risk using one of themany available protocols (Sizer 1996) The use of a for-mal nutritional screening tool for every admission isprobably inappropriate and ineffective but it may bemore realistic to screen for nutritional risk (Lennard-Jones et al 1995) More formal clinical assessment maythen be carried out by a dietitian or nutrition nurse Theobjectives of the assessment are
bull to accurately define the nutritional status of thepatientbull to define clinically relevant undernutritionbull to monitor changes in nutritional status during nutri-tional support
Clinically relevant undernutrition has been defined aslsquothe state of altered nutritional status that is associatedwith an increased risk of adverse clinical events such ascomplications or deathrsquo (Dempsey amp Mullen 1987) Ide-ally nutritional assessment should help determine thetype and aggressiveness of nutritional support requiredfor an individual patient which should be timely andcost-effective
There is no consensus on the best method for theaccurate assessment of nutritional status The most fre-quently used methods include dietary anthropometricbiochemical and functional indices
Specific patient groups have been studied and identi-fied as being at risk of protein-energy undernutritionNutritional screening has become more common inmany clinical areas and many tools have been devel-oped for this purpose However there remains a needfor a published universally accepted and validatedscreening tool Lennard-Jones et al (1995) found thathalf of the 454 ward nurses and two-thirds of the 319junior doctors questioned had asked their patients
about recent unintentional weight loss before admissionto hospital This survey led to the identification of fourbasic questions which it is recommended are asked ofevery patient admitted to hospital patients These are
bull Have you unintentionally lost weight recentlybull Have you been eating less than usualbull What is your normal weightbull How tall are you
Following these questions all patients should beweighed All answers and measurements should be doc-umented in case notes and those patients considered tobe at risk of nutritional depletion should be referred forspecialist assessment and advice
82 Measurement of nutritional status
The World Health Organization defines nutritionalstatus as the condition of the body resulting from theintake absorption and utilisation of food as well asfrom factors of pathological significance Nutritionalassessment allows measurement of changes in bodycomposition variables and associated functionalchanges that adversely affect clinical outcome The mea-surement of height and weight and calculation of BMIoften relies on the willingness of staff to comply Lack ofcompliance may be due to a lack of insight into the needto record such data or simply that the necessary equip-ment is not available in clinics or on wards Further-more available equipment may not be regularlycalibrated or maintained Lennard-Jones et al (1995)found that most of the nurses and doctors who wereasked questions about the height and weight measure-ments of their patients had not taken measurementsbecause they regarded the information as unimportantOf the wards surveyed 86 had weighing scales butonly just over half the hospitals had a service contractfor their maintenance
There is no single or standard way of assessing nutri-tional status This is a dynamic state which reflectsphysiological requirements nutritional intake bodycomposition and body function Methods used to eval-uate these parameters include
bull Clinical factorsndash Increased nutrient requirementndash Increased nutrient lossndash Impaired nutrient digestion and absorption
bull Physical factorsndash Appearance of patientndash Mobility of patientndash Mood of patient
Key points (continued)
bull There is increasing evidence that those who live onlow incomes for long periods cannot afford a healthydiet A number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs
Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

Undernutrition in the UK 107
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
ndash Breathing difficultiesndash Pressure sores and wound healingndash Oedema
bull Dietary factorsndash Change in appetitendash Change in meal patternndash Change in food choice or food consistency
bull Anthropometry (see Section 83)bull Biochemical measurements (see Section 84)
Various assessment tools have been developed whichmay be disease specific (Stall et al 1996) age specific(Boosalis amp Stiles 1995) or are simple tools such asthe Mini Nutritional Assessment designed for those atrisk of undernutrition and which can be predictiveof mortality and hospital cost (Vellas et al 1999)However no single assessment tool is appropriate for allcircumstances
83 Body composition
Foe the purpose of this briefing paper body compositioncan be considered to comprise lean body mass (ie mus-cle and organs) fat stores and body water Accurateresults are highly dependant on the quality of the mea-surements taken the experience and skill of the personconducting the measurements and whether or not themethod is indeed suitable Accurate monitoring ofchanges using techniques such as skinfold thickness ishighly dependent on the measurements being made bythe same observer It should be noted that all methods ofassessing body composition in humans are indirect theonly direct method is complete chemical analysis ofcadavers Therefore measurement of changes ratherthan attempts to measure absolute values will give moreuseful information
Bedsideclinic techniques to assess lean body massinclude
bull MAMCbull grip strengthbull nitrogen balancebull plasma proteins and urea
Bedsideclinic techniques to assess fat stores include
bull tricep skinfold thicknessbull BMI
There are a number of other techniques to measurebody composition generally used in clinical researchbecause the equipment is laboratory-based Theseinclude bioimpedance analysis total body water anddual-energy X-ray absorptiometry (DXA) In the past
few years DXA scanners have been developed that canassess lean and fat tissue they were originally developedto measure bone mineral density only More rarelyother scanning techniques such as computer-assistedtomography magnetic resonance imaging nuclearmagnetic resonance neutron inelastic scattering andgamma-ray resonance are also used to assess body com-position Only those techniques that are commonly usedin clinical practice will be discussed here For a review ofbody composition techniques their appropriate appli-cation for different circumstances and the equipmentand facilities required see Jebb amp Elia (1993)
831 Height
The accurate measurement of a patientrsquos height dependson the availability of a fixed or a portable stadiometerand on the ability of the patient to stand upright In asurvey of the nutritional status of 500 patients 200were undernourished Of these only 155 hadtheir height measured at a clinic visit and one patienthad height recorded on admission (McWhirter ampPennington 1994) Not all hospitalised patients are ableto have their height measured so an estimate of staturecan be made if necessary One method which has a highcorrelation with total height is knee height (Baxter1999) This is particularly useful in elderly people thosewith severe spinal curvature or patients who are unableto stand Knee height is more accurate than arm span(Mitchell amp Lipschitz 1982) with less interobservervariation (Chumlea et al 1985) Knee height is mea-sured with a caliper on the left leg with the knee bent ata 90infin angle Equations are then used to estimate heightin men and women with a 90 error of approximately80 mm in both sexes
832 Weight
Actual body weight and percentage weight loss areprobably the most important indices of nutritionalassessment and the most readily obtainable marker ofenergy reserves However because weight also reflectsbody water interpretation of weight and its fluctuationsbecomes more difficult in those patients in whom thereis a relative increase in total body water such as in liverkidney and heart disease
Percentage weight change is the most commonly useddynamic measurement of nutritional status with acuteunintentional weight loss particularly associated withincreased morbidity and mortality Weight loss can eas-ily be determined if measurements are made on at leasttwo occasions Difficulties arise when the preillness
108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

108 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
weight is unknown particularly as patients at nutri-tional risk have already lost weight Discrepancybetween actual and recalled weight is likely (Pirie et al1981) However there is evidence that estimation ofweight loss by patient recall is more useful than the useof published ideal-weight tables (Morgan et al 1980) Itis important that the composition the rate and the causeof weight loss are investigated Percentage weight lossdetects patients who were previously overweight buthave unintentionally lost weight quickly Such individ-uals may have lost mainly lean body mass rather thanbody fat (Garrow 1980)
The significance of weight loss as a percentage ofpreillness weight (Heymsfield amp Matthews 1994) hasbeen defined as
bull lt 5 weight loss ndash not significantbull 5ndash9 weight loss ndash only clinically significant if weightloss was rapidbull 10ndash20 weight loss ndash clinically significant nutri-tional support indicatedbull gt 20 weight loss ndash severe needs aggressive nutri-tional support
833 Body mass index
BMI is not a sensitive indicator of protein-energy under-nutrition because changes do not distinguish betweendepletion of fat and protein stores However individualswith a BMI of less than 20 kgm2 may be at risk of nutri-tional depletion (see Table 1)
834 Other anthropometric measurements
Anthropometric measurements can be used in two wayseither as a measure of change in body composition usingserial measurements in an individual with a baseline forreference or in epidemiological studies where values arecompared with values according to age and gendergiven in tables Unfortunately the accuracy of relativelysimple measurements can be compromised by a numberof errors in technique Furthermore standard tablesmust be used with caution as many were derived fromdata from narrowly defined healthy populations
In experienced hands the clinical use of MAMCusing a non-stretchy measuring tape and triceps skin-fold thickness using skinfold calipers to estimate storesof muscle protein and fat in the mid-arm is a useful com-ponent of nutritional assessment It is the accessibility ofthe upper arm that makes these useful techniques Bothmeasurements may be used in patients who are immo-bile are too ill to be weighed or have fluid imbalance
which makes a weight measurement unreliableAlthough changes in values occur slowly it is usefulto monitor MAMC and tricep skinfold thickness ofpatients who are on long-term nutritional support inorder to assess efficacy
Interpretation of nutritional assessment in diseasestates may be difficult There is a lack of sensitivity pro-vided by individual nutritional indices percentage idealbody weight has been shown to be less than 85 ofstandard in most patients reflecting increased bodywater mean triceps skinfold thickness measurementswere 49 of standard and MAMC was 78 of stan-dard In a survey of 54 patients with cancer cachexia42 had triceps skinfold thickness below 80 of stan-dard and 23 had MAMC below 80 of standard(Nixon et al 1980) In a study of 43 type I diabeticpatients on haemodialysis MAMC was below the 5thpercentile in almost half and 26 of patients had bodyweights below 85 of ideal (Miller et al 1983)
835 Dual-energy X-ray absorptiometry
Bone and other tissues are able to absorb energy from aphoton beam This means that the mass of bone mineralin the body can be estimated by scanning the wholebody with a photon beam of known energy and mea-suring the difference between energy absorbed andenergy not absorbed This technique can also be used tomeasure the lean to fat ratio in the soft tissue The sub-ject is exposed to radiation but the dose is extremelylow DXA scanning is now quite a common techniquefor assessing body composition because of its primarywidespread use for measuring bone mineral density
836 Bioelectrical impedance analysis (BIA)
Lean tissue is a good conductor of electricity whereas fatis not It is this difference that is measured in BIA Twopairs of electrodes are attached to a subjectrsquos left handand left foot A very small electric current is passedthrough the outer electrodes and the voltage drop ismeasured at the proximal electrodes from which theresistance (impedance) of the tissues is calculated Theimpedance value is then entered into a regression equa-tion with other data including height weight genderand age This gives a prediction of total body water andhence fat-free mass It is usually assumed that fat-freemass is about 73 water BIA measurements are signif-icantly affected by dehydration which is common inmany undernourished patients so general equationsmay not be appropriate
Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

Undernutrition in the UK 109
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
84 Biochemical assessment
There is no single universally accepted objective bio-chemical marker of nutritional status Commonly usedindices include albumin and prealbumin transferrin andretinol-binding protein (RBP)
841 Albumin
Protein-energy undernutrition causes a decrease in therate of albumin synthesis (Fleck et al 1985) Albuminhas a half-life of 21 days and responds slowly to alteredprotein intake so it will not reflect recent changes innutritional intake (Klein 1990) In the classic Minnesotastudy (Keys et al 1950) after 24 weeks of semistarva-tion serum albumin concentrations had fallen by only10 and the total circulating albumin by 2 It wasconcluded that the decrease in circulating plasma levelscommonly seen in disease is not due to simple under-nutrition If oedema is present there is a dilution effecton plasma albumin concentrations Low concentrationshave been correlated with increased morbidity and mor-tality in hospital patients and with longer hospital stays(Dreblow et al 1981 Inglebleek et al 1975) Albuminis not a good marker of nutritional status
842 Transferrin
The main function of transferrin is to bind and transportiron It is therefore affected by iron status Concentra-tions are affected by the acute-phase response so the use-fulness of transferrin measurements in nutritionalassessment is limited Iron deficiency results in anincrease in transferrin synthesis in the liver and conse-quent low concentrations are seen in many inflamma-tory states
843 Thyroxine-binding pre-albumin
Pre-albumin is synthesised in the liver and has a shorterhalf-life than albumin (2 days) Pre-albumin respondsacutely when energy andor protein intakes are low Itssensitivity to nutritional therapy means that it is morelikely to be an indicator of recent dietary intake than anaccurate measure of nutritional status (Casati et al1998)
844 Retinol-binding protein
RBP is also produced by the liver and has an extremelyshort half-life (12 h) As RBP is responsible for thetransport of vitamin A it is affected by vitamin A defi-
ciency as well as hyperthyroidism zinc deficiency liverdisease and the acute-phase response Although RBP hasbeen investigated and used as a nutritional marker itis present in very low concentrations and is difficultto measure RBP is similar to pre-albumin in that itresponds to recent dietary intake rather than being amarker of nutritional status (Casati et al 1998)
845 Insulin-like growth factor 1 (IGF-1)
A number of studies have suggested that IGF-1 whichhas a half-life of a few hours may be a useful objectiveindicator of nutritional status However at present thisis not used routinely The mechanism for the reportedfall in concentration in undernutrition is unknown itmay simply be a reflection of the general decrease in pro-tein synthesis Unlike albumin and the other markersIGF-1 is unaffected by the acute-phase response andmay therefore be a more accurate reflection of nutri-tional status independent of disease activity Untermanet al (1985) measured IGF-1 levels in 37 malnourishedpatients and compared these to conventional nutritionalindices (albumin transferrin and lymphocyte count)The level of IGF-1 correlated well and levels rose in sixpatients who were provided with nutritional supportHowever poor correlation was found when IGF-1 levelswere used as a marker in patients in whom undernutri-tion was determined by anthropometry (McWhirteret al 1995)
85 Functional assessment
851 Grip strength
Measurement of muscle function is important in theassessment of nutritional status but the laboratorymethods are not suitable for practice in the clinical set-ting Undernutrition results in reduced muscle functionwhich may be reversed during nutritional supportalthough measurement of nutritional indices may takelonger to improve (Lopez et al 1982) Maximum vol-untary grip strength measured using a dynamometer is auseful functional measurement and is related to whole-body muscle mass assessed by creatine excretion limbmuscle circumference and anthropometry (Hunt et al1985) Specificity and sensitivity are improved if age andsex standardised values are used for comparison A gripstrength of less than 85 of standard could be evidenceof muscle protein depletion (Klidjian et al 1980) Gripstrength cannot be assessed in patients with arthritisthose who are critically ill or prescribed muscle relax-ants Up to 10 of patients in the acute setting may be
110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

110 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
86 Nutritional screening and assessment of patients in the community
A patientrsquos health often deteriorates before admission tohospital while they are still in the community bringingwith it a concomitant deterioration in their nutritionalstatus (see Section 31) This often remains unrecognisedby the primary health care team for a number of rea-sons The first problem is one of identifying who needsnutritional screening as this should happen automati-cally for patients on admission to hospital Both Ham(1994) and Chernoff (1994) have recommended thatelderly people should be screened routinely particularlythose in nursing homes those attending GP clinics andthose requiring home care In the USA it has beenshown that 74 of meals-on-wheels recipients were atrisk of poor nutritional status (Coulston et al 1996)Furthermore McWhirter amp Pennington (1994) haveshown that 43 of elderly patients in the UK admittedto hospital from the community were malnourished
Other groups of patients who require regular screen-ing and assessment are the chronically ill and those withcancer and neurological disorders many of whom areelderly (Barrocas et al 1995) Children with develop-mental disabilities are also at increased nutritional risk(Campbell amp Kelsey 1994)
In the community practice and community nurses seethe majority of at-risk patients Grindel amp Costello(1996) suggest that these members of the primary healthcare team should conduct routine nutrition screening oftheir patients But if screening and assessment are totake place in the community the primary health careteam must be provided with simple tools and training inhow to use them The problem of how patients shouldbe screened is a major one As discussed in Sections 84and 85 currently there are no national standards bywhich to measure nutritional status and these areurgently needed to ensure consistency in screening andassessment
Despite the many published papers describing nutri-tional screening tools that are used in hospitals thereare few describing tools that have been developedfor use in the community (Green amp McLaren 1998)Hickson amp Hill (1997) describe the adaptation for usein the community of a tool that was originally designedfor hospital use This tool requires nurses to measureBMI which could create difficulties if patients are beingseen at home and scales and stadiometers are not avail-able Several tools have been developed in the USA andEurope for screening nutritional risk in the elderly(Guigoz et al 1994 The Nutrition Screening Initiative1994) In the UK dietitians from the Nutrition AdvisoryGroup for Elderly People have produced a nutritionassessment checklist for community care workers toidentify the potential nutritional problems of elderlyclients (Nutrition Advisory Group for Elderly People1992) The list covers general questions about eatinghabits weight change use of supplements and laxativesand has four sections aimed at identifying deficiencies ofparticular nutrients iron vitamin C calcium andvitamin D and fibre Advice is given in each section onhow to take appropriate action to improve intakeReliability and validity of the checklist have not beenestablished
Children with developmental problems are a vulner-able group whose nutritional status needs to be moni-tored regularly Campbell amp Kelsey (1994) in the USAhave developed the Parent Eating and Nutrition Assess-ment for Children with Special Needs (PEACH) surveywhich is a checklist of questions designed to be admin-istered by the childrsquos primary caregiver Six developmen-tal paediatricians assessed the questions for content andface validity then assigned scores to each question Thetool was validated in 79 children by comparing the totalscore obtained using the PEACH survey with a nutri-tional survey by a dietitian The tool was found to havea sensitivity of 886 and a specificity of 909 withan overall predictive value of 886 The authors con-
Key points
bull If there is no request to measure a patientrsquos heightor weight it is often not carried out and lack of thenecessary equipment and skills is an important issueto be addressedbull An action plan of appropriate nutritional caretogether with follow-up measures taken to evaluatethe effect of the nutritional support is then neededbull Simple bedside techniques (eg tricep skinfoldthickness) of measuring nutritional status should beused to determine those patients at risk of developingnutrition-related complicationsbull The ideal nutritional assessment should be rela-tively inexpensive minimally invasive and the resultsshould be accurate and reproduciblebull Measurements such as height weight and BMI tri-cep skinfold thickness and MAMC are quick cheapand non-invasive methods of estimating weight-for-height subcutaneous fat and protein stores
unable to comply with dynamometry (McWhirter1995) It may be useful in patients receiving long-termnutritional support
Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

Undernutrition in the UK 111
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
cluded that in children with developmental problemsthe PEACH tool provides a quick method of screeningout unnecessary referrals and maximises effective use ofthe dietitianrsquos time
To date in the UK only Bryan et al (1998) havedeveloped and validated a screening tool for clients withlearning difficulties The form has questions about foodfrequency weight and nutrition-related problems Thistool requires the patient to be weighed and measuredwhich could create difficulties for clients in wheelchairs
Ward et al (1998) have developed a screening tool foruse in general practice in the UK It has been constructedusing a list of questions that require only lsquoyesrsquo or lsquonorsquoanswers which are predictive of nutritional risk Thevalidity of the tool was tested by comparing the ques-tions administered by a community nurse to a fullnutritional assessment conducted by a dietitian within4 days of each other Discriminant analysis and multipleregression analysis were then used to determine whichquestions were predictive of nutritional risk and toassign weightings to each question Patients are categor-ised according to their level of risk There are threecategories of scores (0ndash6 not at risk 7ndash16 possible orprobable risk 17 or more malnourished) The tool has apositive predictive value of 946 and a negative pre-dictive value of 811
Once patients have been found to be at nutritionalrisk the community dietitian takes responsibility forconducting a full assessment in the community Asdiscussed previously there are no national referencestandards by which to measure nutritional status Inaddition the reference standards for anthropometrythat are currently used for those over 65 years of age arestandards derived in the USA and the UK in the 1980s(Bishop et al 1981 Burr amp Philips 1984)
Klein et al (1997) have reviewed nutritional assess-ment methods and conclude that there is no goldstandard because there is no universally accepted defi-nition of undernutrition The dietitian must use theirclinical expertise to determine each individual patientrsquosnutritional status and consider the following problemsassessment of patients with oedema fluid overloadheart failure or dehydration decreasing height with oldage assessment of patients with neurological problemsleading to undernutrition as degeneration will notreverse with nutrition and assessment of bed-boundpatients
87 Recommendations
bull A definition of undernutrition needs to be establishedand accepted
bull National reference standards for anthropometricmeasurements by which to evaluate body compositionneed to be established for both young and elderlypopulations since the body size of the population haschanged over the last 20 years and those currently usedare outdatedbull If BMI is to be used as a standard measurement ofnutritional status universally accepted cut-off points forlow BMIs need to be agreedbull Nutritional screening needs to be incorporated as aroutine part of yearly check-ups for people over75 years (Caroline Walker Trust 1995) and for allpatients deemed to be at risk because of their diseasestatus In addition all health care professionals shouldbe educated about the contribution of nutritional statusto general health of all patients in their care and the det-rimental effect poor nutritional status can have if it isleft untreatedbull Different ranges for anthropometric measurementsthat are age andor disease specific for certain popula-tion groups may be more useful in predicting undernu-trition particularly when used in addition to clinicalmeasurements of body function such as serum albuminlevel
Key points
bull Difficulties exist in defining undernutrition as theanthropometric measurements used are neither agenor disease specificbull Ranges and cut-off points to define normal or idealhave been based on healthy young individuals but areapplied to the whole population Different rangesthat are age andor disease specific for certain popu-lation groups may be more useful in predictingundernutrition
9 Specialised feeding
Appendix 2 gives a short comprehensive overview of theprinciples involved in specialised feeding and coversthe three main types of specialised feeding techniquesincluding indications and contraindications for theiruse energy needs and some of the practical issuesinvolved in nutrition support More detailed informa-tion can be obtained from specialised textbooks such asManual of Dietetic Practice (Thomas 2001) and HumanNutrition and Dietetics (Garrow et al 2000)
112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

112 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
10 Conclusions
It is estimated that 70 of undernutrition in the UKgoes unrecognised and untreated and that in the com-munity 5 of the population has a BMI lt 20 kgm2Poverty is a major contributory factor To address thisproblem a number of community food initiatives havebeen developed in an attempt to improve the eatingbehaviours of those living on a low income Theseinitiatives include lsquocook and eatrsquo groups food co-operatives community cafes and breakfast clubs How-ever it should be recognised that the success of theseinitiatives depend upon appropriate advice and supportbeing offered to people living on a low income as well aswhether they have enough money to implement thedietary changes that are advocated
In hospitals the prevalence of underweight(BMI lt 20 kgm2) rises to 20ndash25 It is also estimatedthat 40 of adults and 15 of children admitted tohospital are malnourished half of these severely so andmany others become malnourished during their stay inhospital Undernutrition increases the risk of complica-tions lowers resistance to infection impairs physicaland mental functioning and delays recovery
For patients already undernourished or those whoare at risk of undernutrition on admission the problemsmay become worse often owing to the quality of hospi-tal food and the inadequacy of current feeding policiesSuch problems include the limited choice the way foodis served and the lack of help for those unable to feedthemselves properly Others need additional nutritionalsupport but this often goes unrecognised Between 30and 50 of hospital food is wasted and average foodintake is less than 75 of that recommended particu-larly among the elderly As well as impairing clinicaloutcome this wastes resources The monetary value ofhospital food wasted each year in England alone is cal-culated to be pound45 million By including labour and over-heads this cost rises to pound144 million There is also thehidden cost of the extra ill health associated withundernutrition
There is strong evidence that measures such asimproved staff training nutritional screening andassessment and monitoring combined with bettercatering practices can result in most patientsrsquo nutri-tional requirements being met Fortified meals between-meal snacks and adequate ward staffing have all beenshown to contribute to achieving this goal which leadsto better clinical outcome less waste shorter hospitalstay and a more cost-effective service Many of theseproblems are now being tackled with the establishmentof new schemes such as Better Hospital Food and imple-
mentation of guidelines such as those produced by theCaroline Walker Trust on the nutritional education ofcare workers
Difficulties exist in defining undernutrition specifi-cally undernutrition as the anthropometric measure-ments used are neither age nor disease specific Rangesand cut-off points to define normal or ideal have beenbased on healthy young individuals but are applied tothe whole population Different ranges that are age andor disease specific for certain population groups may bemore useful in predicting undernutrition Compoundingthis problem is the fact that many clinicians GPs nursesand other health care professionals have had no trainingin the detection and management of undernutrition oron the guidance of prescribing nutritional supplementsThus despite the widespread use of oral nutritional sup-plements in the community their effectiveness is ques-tionable The nutrition education of doctors has beenaddressed by the Royal Colleges and an intercollegiategroup on nutrition has now been established and runsregular training courses
Since most patients are discharged from hospital witha worse nutritional status than they entered it this theninjects into the community a further group of under-nourished individuals setting up a vicious circle There-fore the presence of disease whether in hospital or thecommunity should be seen as an indication of the needfor nutritional screening to identify those at particularrisk and those who might benefit from some form ofnutritional intervention Clinical governance should beused to ensure appropriate nutritional management forpatients The National Institute of Clinical Excellence iscurrently setting up a new NSF to include standards ofbest practice in food service in hospitals
Acknowledgements
This briefing paper has been drafted by Dr SarahSchenker The British Nutrition Foundation wishes tothank the members of the Foundationrsquos Scientific Advi-sory and Industrial Scientists Committees who helpedto shape the contents of this briefing paper
References
Acheson D (1998) Inequalities in Health An Independent Inquiry The Stationery Office London
American Gastroenterological Association (1995) American Gastro-enterological Association Medical Position Statement guidelines for the use of enteral nutrition Gastroenterology 108 1280ndash301
Anderson A amp Hunt K (1992) Who are the healthy eaters Eating pat-terns and health promotion in the west of Scotland Health Educa-tion Journal 51 3ndash10
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients
Undernutrition in the UK 113
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
British Association for Parenteral and Enteral Nutrition (1999) Hos-pital Food as a Treatment A Report by the British Association of Parenteral and Enteral Nutrition (Allison SP ed) BAPEN Maidenhead
Barker M McClean S McKenna P et al (1989) Diet Lifestyle and Health in Northern Ireland A Report of the Health Promotion Research Trust University of Ulster Coleraine
Barrocas A Belcher D Champagne C amp Jastram C (1995) Nutrition assessment practical approaches Clinics in Geriatric Medicine 11 675ndash713
Baxter JP (1999) Problems of nutritional assessment in the acute set-ting Proceedings of the Nutrition Society 58 39ndash46
Beier-Holgersen R amp Boesby S (1996) Influence of postoperative enteral nutrition on postsurgical infections Gut 39 833ndash53
Better Hospital Food (2001) Better Hospital Food The Stationery Office London
Bishop CW Bowen PE amp Ritchley PI (1981) Norms for nutritional assessment of American adults by upper arm anthropometry American Journal of Clinical Nutrition 34 2530ndash9
Bistrian BR Blackburn GL Hallowell E amp Heddle R (1974) Protein status of general surgical patients Journal of the American Medical Association 230 858ndash60
Bolton-Smith C Smith W Woodward M amp Tunstall-Pedoe H (1991) Nutritional intakes in different social class groups results from the Scottish Heart Study British Journal of Nutrition 65 321ndash5
Bond S ed (1997) Eating Matters a Resource for Improving Dietary Care in Hospitals Centre for Health Services Research University of Newcastle upon Tyne Newcastle upon Tyne
Boosalis MG amp Stiles NJ (1995) Nutritional assessment in the elderly biochemical analyses Clinical and Laboratory Science 8 31ndash3
Braddon F Wadsworth M Davies J amp Cripps H (1988) Social and regional differences in food and alcohol consumption and their measurement in a national birth cohort Journal of Epidemiology and Community Health 42 341ndash9
British Nutrition Foundation (2002) Briefing Paper Nutrition Health and Schoolchildren British Nutrition Foundation London
Bryan F Jones JM amp Russell L (1998) Reliability and validity of a nutrition screening tool to be used with clients with learning diffi-culties Journal of Human Nutrition and Dietetics 11 41ndash50
Burke A (1997) Hungry in Hospitals News Briefing Association of Community Health Councils for England and Wales London
Burr ML amp Philips KM (1984) Anthropometric norms in the elderly British Journal of Clinical Nutrition 51 165ndash9
Calvert C Rushton C amp Dowler E (1994) Dietary intakes of female lone parents in London energy and micronutrients Proceedings of the Nutrition Society 53 97A
Campbell IT (1999) Limitations of nutrient intake The effect of stres-sors trauma sepsis and multiple organ failure European Journal of Clinical Nutrition 53 S143ndash7
Campbell MK amp Kelsey KS (1994) The PEACH survey a nutrition screening tool for use in early intervention programs Journal of the American Dietetic Association 94 1156ndash8
Caroline Walker Trust (1992) Nutritional Guidelines for School Meals Caroline Walker Trust London
Caroline Walker Trust (1995) Eating Well for Older People Caroline Walker Trust London
Caroline Walker Trust (1998a) Eating Well for Older People with Dementia Caroline Walker Trust London
Caroline Walker Trust (1998b) Eating Well for Under-5s in Child Care Caroline Walker Trust London
Caroline Walker Trust (2001) Eating Well for Looked After Children and Young People Caroline Walker Trust London
Casati A Muttini S Leggieri C et al (1998) Rapid turnover proteins in critically ill ICU patients Negative acute phase proteins or nutri-tional indicators Minerva Anesteiologica 64 345ndash50
Chandra RK (1992) Effect of vitamin and trace element supplemen-tation on immune responses and infection in elderly subjects Lan-cet 340 1124ndash7
Chernoff R (1994) Meeting the nutritional needs of the elderly in the institutional setting Nutrition Reviews 52 132ndash6
Chumlea WC Roche AF amp Steinbaugh ML (1985) Estimating stature from knee height for persons 60 to 90 years of age Journal of the American Geriatric Society 33 116ndash20
Cole T (1997) 3-in-1 weight-monitoring chart Lancet 349 102ndash3Corish CA Flood P Mulligan S amp Kennedy NP (2000) Apparent low
frequency of undernutrition in Dublin hospital in-patients should we review the anthropometric thresholds for clinical practice Brit-ish Journal of Nutrition 84 325ndash35
Coulston AM Craig L amp Voss AC (1996) Meals-on-wheels applicants are a population at risk for poor nutritional status Journal of the American Dietetic Association 96 570ndash3
Cuthbertson DP (1980) Alterations in metabolism following injury Injury 11 175ndash89 286ndash303
Dempsey DT amp Mullen JL (1987) Prognostic value of nutritional indices Journal of Parenteral and Enteral Nutrition 11 109Sndash14S
Department of Health (1991) Dietary Reference Values for Food Energy and Nutrient Intakes in the UK Report on Health Social Subjects 41 HMSO London
Department of Health (1996a) Eat well II A Progress Report from the Nutrition Task Force on the Action Plan to Achieve the Health of the Nation Targets on Diet and Nutrition Department of Health London
Department of Health (1996b) Low Income Project Team Depart-ment of Health London
Department of Health (1999a) Saving Lives Our Healthier Nation The Stationery Office London
Department of Health (1999b) Reducing Health Inequalities An Action Report Department of Health London
Department of Health (2000) The NHS Plan The Stationery Office London
Department of Health (2002a) Healthy Start Proposals for reform to the Welfare Food Scheme Department of Health London (httpwwwdohgovukhealthystart)
Department of Health (2002b) Scientific Review of the Welfare Food Scheme Report on health social subjects 51 Report of the panel on child health and maternal nutrition of the Committee on Medical Aspects of Food and Nutrition Policy The Stationery Office London
Dionigi R Zonta A Dominioni L et al (1988) The effects of total parenteral nutrition on immunodepression due to malnutrition Annals of Surgery 185 467ndash74
Dowler E amp Calvert C (1995) Nutrition and Diet in Lone Parent Families in London Family Policy Studies Centre London
Dreblow DM Anderson CF amp Moxness K (1981) Nutritional assessment of orthopedic patients Mayo Clinic Proceedings 56 51ndash5
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients
114 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Edington J Boorman J Durrant ER et al (2000) Prevalence of mal-nutrition on admission to four hospitals in England Clinical Nutri-tion 19 191ndash5
Edington J Kon P amp Martyn CN (1996) Prevalence of malnutrition in patients in general practice Clinical Nutrition 15 60ndash3
Edwards J amp Nash A (1997) Catering services Measuring the was-teline Health Service Journal 107 26ndash7
Elia M (1995) Changing concepts of nutrient requirements in disease implications for artificial nutritional support Lancet 345 1279ndash83
Elia M (2000) Nutritional support in sepsis and trauma In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) pp 483ndash9 Churchill Livingstone Edinburgh
Elia M (2001) The Malnutrition Advisory Group consensus guidelines for the education and management of malnutrition in the commu-nity Nutrition Bulletin 26 81ndash4
Elia M amp Jebb S (1992) Changing concepts of energy requirements of critically ill patients current medical literature Clinical Nutrition 11 35
Elia M amp Stratton RJ (2000) How much undernutrition is there in hospitals British Journal of Nutrition 84 257ndash9
Fenton J Eves A Kipps M amp OrsquoDonnell CC (1995) The nutritional implications of food wastage in continuing care wards for elderly patients with mental health problems Journal of Human Nutrition and Dietetics 8 239ndash48
Fiatarone MA amp Evans WJ (1993) The etiology and reversibility of muscle dysfunction in the aged Journal of Geriatrics 48 77ndash83
Finch S Doyle W Lowe C et al (1998) National Diet and Nutrition Survey People Aged 65 Years and Over Report of the Diet and Nutrition Survey The Stationery Office London
Fleck A Colley CM amp Myers MA (1985) Liver export proteins and trauma British Medical Bulletin 41 265ndash73
Frankenfield DC Smith JS amp Cooney RN (1997) Accelerated nitrogen loss after traumatic injury is not attenuated by achievement of energy balance Journal of Enteral and Parenteral Nutrition 21 324ndash9
Freeman J Cole T Chinn S et al (1995) Cross sectional stature and weight reference curves for the UK 1990 Archives of Disease in Childhood 73 17ndash24
Galanos AN Pieper CF Kussin PS et al (1997) Relationship of body mass index to subsequent mortality among seriously ill hospitalised patients SUPPORT Investigators The study for understanding prognoses and preferences for outcome and risks of treatment Crit-ical Care Medicine 25 1962ndash8
Garrow JS (1980) Combined medical-surgical approaches to treat-ment of obesity American Journal of Clinical Nutrition 33 425ndash30
Garrow JS James WPT amp Ralph A (2000) Human Nutrition and Die-tetics Churchill Livingstone Edinburgh
Green SM amp McLaren SG (1998) Nutritional assessment and screen-ing instrument selection British Journal of Community Nursing 1 335ndash9
Gregory J Collins R Davies P Hughes J amp Clarke P (1995) National Diet and Nutrition Survey Children Aged 112 to 412 Years HMSO London
Gregory J Foster K Tyler H amp Wiseman M (1990) The Dietary and Nutritional Survey of British Adults HMSO London
Gregory J Lowe S Bates C et al (2000) National Diet and Nutrition Survey Children Aged 4 to 18 Years The Stationery Office London
Grindel CG amp Costello MC (1996) Nutrition screening an essential assessment parameter MEDSURG Nursing 5 145ndash56
Guigoz Y Vellas B amp Garry PJ (1994) Mini Nutritional Assessment a practical assessment tool for grading the nutritional state of eld-erly patients Facts Research and Intervention in Geriatrics 4 15ndash59
Ham RJ (1994) The signs and symptoms of poor nutritional status Primary Care Clinics in Office Practice 21 33ndash54
Haydock DA amp Hill GL (1987) Improved wound healing response in surgical patients receiving intravenous nutrition British Journal of Surgery 74 320ndash4
Herberer M amp Marx A (1995) Complications of enteral nutrition In Artificial Nutritional Support in Clinical Practice (Payne-James J Grimble G amp Silk D eds) Edward Arnold London
Heymsfield SB amp Matthews D (1994) Body composition research and clinical advances Journal of Parenteral and Enteral Nutrition 18 91ndash103
Hickson M amp Hill M (1997) Implementing a nutritional assessment tool in the community a report describing the process audit and problems encountered Journal of Human Nutrition and Dietetics 10 373ndash7
Hill G Blackett RL Pickford I et al (1977) Malnutrition in surgical patients An unrecognised problem Lancet 1 89ndash92
Hunt D Rowlands B amp Johnston D (1985) Hand grip strength ndash a simple prognostic indicator in surgical patients Journal of Parenteral and Enteral Nutrition 9 701ndash4
Inglebleek Y Van den Schneck HG amp De Nayer P (1975) Albumin transferrin and the thyroxine binding pre-albuminretinol binding protein (TBPA-RPB) complex in the assessment of malnutrition Clinica Chimica Acta 63 61ndash5
Jebb SA amp Elia M (1993) Techniques for the measurement of body composition a practical guide International Journal of Obesity 17 611ndash21
Keele AM Bray MJ Emery PW amp Silk DBA (1995) A randomised controlled clinical trial of postoperative oral dietary supplements in surgical patients Journal of Parenteral and Enteral Nutrition 19 215
Kelly L (1999) Audit of food wastage differences between a plated and bulk system of meal provision Journal of Human Nutrition and Dietetics 12 415ndash24
Kelly IE Tessier S Cahill A et al (2000) Still hungry in hospital iden-tifying malnutrition in acute hospital admissions Quarterly Journal of Medicine 93 93ndash8
Keys AJ Brozek J Henchel O Michelson O amp Taylor HL (1950) In The Biology of Human Starvation University of Minnesota Press Minneapolis MN
Kingrsquos Fund (1992) A Positive Approach to Nutrition as a Treatment Report of a Working Party on the Role of Enteral and Parenteral Feeding in Hospital and at Home (Lennard-Jones JE ed) Kingrsquos Fund London
Klein S (1990) The myth of albumin as a measure of nutritional status Gastroenterology 99 1845ndash6
Klein S Kinner J Jeejeebhoy K et al (1997) Nutrition support in clin-ical practice review of published data and recommendations for future research Journal of Parenteral and Enteral Nutrition 21 133ndash56
Klidjian AM Foster KJ Kammering RM Cooper A amp Karran SJ (1980) Relationship of anthropometric variables to serious post operative complications British Medical Journal 281 899ndash901
Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

Undernutrition in the UK 115
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Larsson J Unosson M Ek A-C et al (1990) Effect of dietary supple-ment on nutritional status and clinical outcome on 501 geriatric patients ndash a randomized study Clinical Nutrition 9 179ndash84
Lennard-Jones JE (1992) A Positive Approach to Nutrition as a Treat-ment Kingrsquos Fund Centre London
Lennard-Jones JE Arrowsmith H Davison C Denham AF amp Micklewright A (1995) Screening by nurses and junior doctors to detect malnutrition when patients are first assessed in hospital Clin-ical Nutrition 14 336ndash40
Lopez J Russell DM Whitwell J amp Jeejeebhoy K (1982) Skeletal mus-cle function in malnutrition American Journal of Malnutrition 36 602ndash10
McCombie L (1999) Sip feed prescribing in primary care an audit of current practice in Greater Glasgow Health Board Glasgow UK Journal of Human Nutrition and Dietetics 12 210ndash12
McWhirter JP (1995) The clinical significance of malnutrition MPhil Thesis Glasgow Caledonian University
McWhirter JP Hill K Richards J amp Pennington CR (1995) The use efficacy and monitoring of artificial nutritional support in a teach-ing hospital Scottish Medical Journal 40 179ndash83
McWhirter JP amp Pennington CR (1994) Incidence and recognition of malnutrition in hospital British Medical Journal 308 945ndash8
Miller D Levine S Bistrian BR amp Elia J (1983) Diagnosis of protein calorie malnutrition in diabetic patients on haemodialysis and peritoneal dialysis American Journal of Clinical Nutrition 41 810ndash17
Mitchell DO amp Lipschitz DA (1982) Detection of protein caloric mal-nutrition in the elderly American Journal of Clinical Nutrition 35 398ndash406
Morgan DB Hill GL amp Burkinshaw L (1980) The assessment of weight loss from a single measurement of body weight the prob-lems and limitations American Journal of Clinical Nutrition 33 2101ndash5
Moynihan P Adamson A Skinner R et al (1993) The intake of nutri-ents by Northumbrian adolescents from one-parent families and from unemployed families Journal of Human Nutrition and Die-tetics 6 433ndash41
National Health Service Executive (1998) A First Class Service Con-sultation Document on Quality in the New NHS Health Service Circular 1998113 Department of Health London
Nightingale JM amp Reeves J (1999) Knowledge about assessment and management of undernutrition a pilot questionnaire in a UK teach-ing hospital Clinical Nutrition 18 23ndash7
Nixon DW Heymsfield SB Cohen AE et al (1980) Protein-calorie undernutrition in hospitalised cancer patients American Journal of Medicine 68 683ndash90
Nuffield Trust (1999) Managing Nutrition in Hospital A Recipe for Quality (Maryon Davis A amp Bristow A eds) Nuffield Trust London
Nutrition Advisory Group for Elderly People (1992) Eating Through the 90s NAGE Leeds
Pennington CR (1998) Disease-associated malnutrition in the year 2000 Postgraduate Medical Journal 74 65ndash71
Piachaud D amp Webb J (1996) The Price of Food Missing Out on Mass Consumption STICERD occasional Paper 20 London School of Economics London
Pirie P Jacobs D Jeffrey R amp Hannan P (1981) Distortion of self
reported height and weight data Journal of the American Dietetic Association 78 601ndash6
Potter J Langhorne P amp Roberts M (1998) Routine protein energy supplementation in adults systematic review British Medical Jour-nal 317 495ndash501
Rana SK Bray J Menzies-Gow N et al (1992) Short term benefits of postoperative oral dietary supplements in surgical patients Clinical Nutrition 11 337ndash44
Reilly HM Martineau JK Moran A amp Kenenedy H (1995) Nutri-tional screening ndash Evaluation and implementation of a simple Nutri-tion Risk Score Clinical Nutrition 34 269ndash73
Royal College of Physicians (2002) Nutrition and Patients a Doctorrsquos Responsibility Royal College of Physicians London
Royal Institute of Public Health (2002) Eating for Health in Care Homes A practical nutrition handbook Royal Institute of Public Health London
Rushden C amp Wheeler E (1993) The dietary intake of homeless males sleeping rough in Central London Journal of Human Nutrition and Dietetics 6 443ndash56
Schenker S (2000) Malnutrition in the UK Conference Report Nutri-tion Bulletin 25 175ndash8
Sizer T ed (1996) Standards and Guidelines for Nutritional Support of Patients in Hospital A report of a BAPEN working party BAPEN Maidenhead Berks
Social Exclusion Unit Cabinet Office (1998) Bringing Britain Together The Stationery Office London
Stall SH Ginsberg NS DeVita MV et al (1996) Comparison of five body composition methods in peritoneal dialysis patients American Journal of Clinical Nutrition 64 125ndash30
Stratton RJ (2000) Summary of a systematic review on oral nutritional supplement use in the community Proceedings of the Nutrition Society 59 469ndash76
Stratton RJ amp Elia M (1999) A critical systematic analysis of the use of oral nutritional supplements in the community Clinical Nutri-tion 18 29ndash84
The Nutrition Screening Initiative (1994) Incorporating Nutrition Screening and Intervention into Medical Practice A Monograph for Physicians no 1-73 Ross Products Division Abbott Laboratories Columbus OH
Thomas B (2001) Manual of Dietetic Practice Blackwell Science Oxford
Truswell AS (2000) Drugndashdiet interactions In Human Nutrition and Dietetics (Garrow JS James WPT amp Ralph A eds) Churchill Livingstone Edinburgh
Unterman TG Vazquez RM Slas AJ et al (1985) Nutrition and Somatomedin XIII Usefulness of somatomedin-C in nutritional assessment American Journal of Medicine 78 228ndash34
Vellas B Guigoz Y Garry PJ et al (1999) The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients Nutrition 15 116ndash22
Ward J Close J Little L et al (1998) Development of a screening tool for assessing risk of undernutrition in patients in the community Journal of Human Nutrition and Dietetics 11 323ndash30
Whichelow M Erzinclioglu S amp Cox B (1991) Some regional varia-tions in dietary patterns in a random sample of British adults European Journal of Clinical Nutrition 45 253ndash62
116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

116 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Appendix 1 Useful addresses and websites
Addresses
bull British Association for Parenteral and EnteralNutrition (BAPEN) PO Box 922 Maidenhead BerksSL6 4SH httpwwwbapenorgukbull British Dietetic Association 5th Floor CharlesHouse 1489 Great Charles Street QueenswayBirmingham B3 3HT httpwwwbdaukcombull Caroline Walker Trust 22 Kindersley WayAbbots Langley Hertfordshire WD5 0DQ httpwwwcwtorgukbull Kingrsquos Fund Centre 11ndash13 Cavendish SquareLondon W1M 0AN httpwwwkingsfundorgukbull National Institute for Clinical Excellence 11 StrandLondon WC2N 5HR httpwwwniceorgukbull Nuffield Trust 59 New Cavendish Street LondonW1M 7RD httpwwwnuffieldtrustorgukbull Patients Association 7 Milton Street NorthamptonNN2 7JG httpwwwpatients-associationcombull Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN httpwwwrcnorgukbull WRVS Milton Hill House Steventon AbingdonOxon OX13 6AD httpwwwwrvsorguk
Websites
bull httpwwwbetterhospitalfoodcombull httpwwwdfesgovukbull httpwwwdohgovukcomawelfarefoodsreviewpdfbull httpwwwdohgovukhlcindexhtmbull httpwwwdohgovuknsfbull httpwwwdohgovukpricarehazhtmbull httpwwwhda-onlineorgukbull httpwwwicgnutritionorgukbull httpwwwintercollegiateorgukbull httpwwwneighbourhooddtlrgovukbull httpwwwoxfamorgukbull httpwwwsignacukbull httpwwwsurestartgovukbull httpwwwsustainweborg
Appendix 2 Specialised feeding
This section is designed to give a short comprehensiveoverview of the principles involved in specialised feed-ing The three main types of specialised feeding tech-niques including indications and contraindications fortheir use energy needs and some of the practical issuesinvolved in nutrition support are covered briefly Moredetailed information can found in specialised textbooks(Garrow et al 2000 Thomas 2001)
Once specialised feeding of a patient has been agreedupon it is the responsibility of the dietitian to assessnutritional requirements and decide on how these canbest be met through a variety of different feeding meth-ods Combinations of methods can be used and the die-titian must co-ordinate these to ensure they complementeach other The dietitian not only calculates nutrientrequirements but also must take into account the phys-ical and mental condition of the patient other treatmentbeing received and the predicted length of time that thepatient will require special feeding
Use of oral nutrition supplements
If sufficient energy intake cannot be achieved withnormal foods proprietary supplements can be a usefuladdition to the diet Some types can be purchaseddirectly from chemists and supermarkets They are usu-ally in powdered form and made up with milk to makemilkshakes or soups They are not nutritionally com-plete however as they lack trace elements The majorityof the nutritionally complete supplements are prescrib-able on FP 10 forms The Advisory Committee onBorderline Substances lists the conditions for whicheach product is prescribable in the Monthly Index ofMedical Specialities and the British National FormularyMost come ready-to-drink in cartons and in a variety offlavours Prescribable soups and puddings are alsoavailable
Prescribed supplementary oral nutrition products arecostly to the NHS so it is important that they are notused unnecessarily They can be effective in somepatients when used properly but auditing procedureshave shown these products are often prescribed withoutthe involvement of a dietitian and before any attempthas been made to improve dietary intake by conven-tional foods (McCombie 1999) Supplements should notbe regarded as an easier option than providing highnutrient density meals or extra snacks Supplementationshould only be considered when dietary measures areinsufficient to sustain or improve intake They should beregarded as an addition to normal intake and not as asubstitute except on days when food cannot be faced atall Patients should always be given simple writtenguidance on the use of supplements and should beencouraged to consume supplements at intervalsthroughout the day and not before meals to avoidimpairing appetite
In the community GPs are able to prescribe supple-ments in response to requests from district or palliativecare nurses as well as dietitians and this has led to wide-spread use of oral nutritional supplements in the com-
Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

Undernutrition in the UK 117
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
munity However there is uncertainty regarding thevalue of their use because it is often inappropriate andunnecessary A critical systematic review has beenconducted by Stratton (2000) to gain insights into theeffects of supplements on body weight and structurespontaneous food intake and body function The authorreviewed 84 trials categorised into different patientgroups The results showed that following supplemen-tation weight gain varied considerably and dependedon the duration and amount of supplementation and onthe disease status of patients Percent weight changewas greater in patients with a mean BMI lt 20 kgm2
than with a mean BMI gt 20 kgm2 Total energy intakeincreased during supplementation and the energy fromthe supplement was largely additional to rather thansubstituting for food eaten Additional energy intake viasupplementation also varied considerably depending onthe disease state and BMI of the patient This highlightsthe need for better guidelines regarding supplement use(Stratton amp Elia 1999)
Enteral nutrition
Enteral tube feeding is the preferred route for patientswith a functioning gastrointestinal tract but who cannotswallow or for those who cannot obtain adequate nutri-tion from the intake of food andor dietary supplementsEnteral nutrition is simpler cheaper and physiologicallypreferable to parenteral nutrition (see the section onlsquoParenteral nutritionrsquo) because it maintains the integrityof the gut barrier better which prevents bacteria fromentering the systemic circulation
Guidelines for the use of enteral tube feeding are givenin Table 2 Contraindications to its use include pro-longed gastrointestinal failure such as bowel stasiseritonitis severe and recurrent pancreatitis high intes-tinal fistulae short bowel syndrome or severe inflam-matory disease of the bowel such as mucositis followingcytotoxic therapy or Crohnrsquos disease complicated byfistulae
Table 2 Clinical guidelines for the use of enteral nutrition in the adult patient
Where artificial enteral nutrition should bepart of routine care
Protein-energy undernutrition (greater than 10 weight loss) with little or no oral intake for theprevious 5 days
Less than 50 of the required oral nutrient intake for the previous 7ndash10 daysSwallowing-related difficulties eg head injury strokes motor neurone diseaseMajor full-thickness burnsMassive small bowel resection in combination with parenteral nutrition (in patients with 50ndash90
small bowel resection enteral nutrition is given to hasten gut regeneration and return to oralintake)
Low-output enterocutaneous fistulae (less than 500 mLday) (elemental diets may hasten closureof fistula)
Where enteral nutrition would normallybe helpful
Major traumaRadiation therapyMild chemotherapy
Where enteral nutrition is of limited orundetermined value
Intensive chemotherapyImmediate postoperative period or poststress period (especially if an adequate oral intake will be
resumed within 5ndash7 days)Acute enteritisLess than 10 of small intestine remaining after surgery
Where enteral nutrition should not be used Complete mechanical intestinal obstructionPoor muscle movement of the intestinal tractSevere uncontrollable diarrhoeaHigh-output fistulae ndash a leaking hole in the intestinal tractSevere acute pancreatitisShockNot desired by the patient or legal guardian and such action being in accordance with hospital
policy and existing lawPrognosis not warranting aggressive nutritional support
Source Elia (2000)
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients
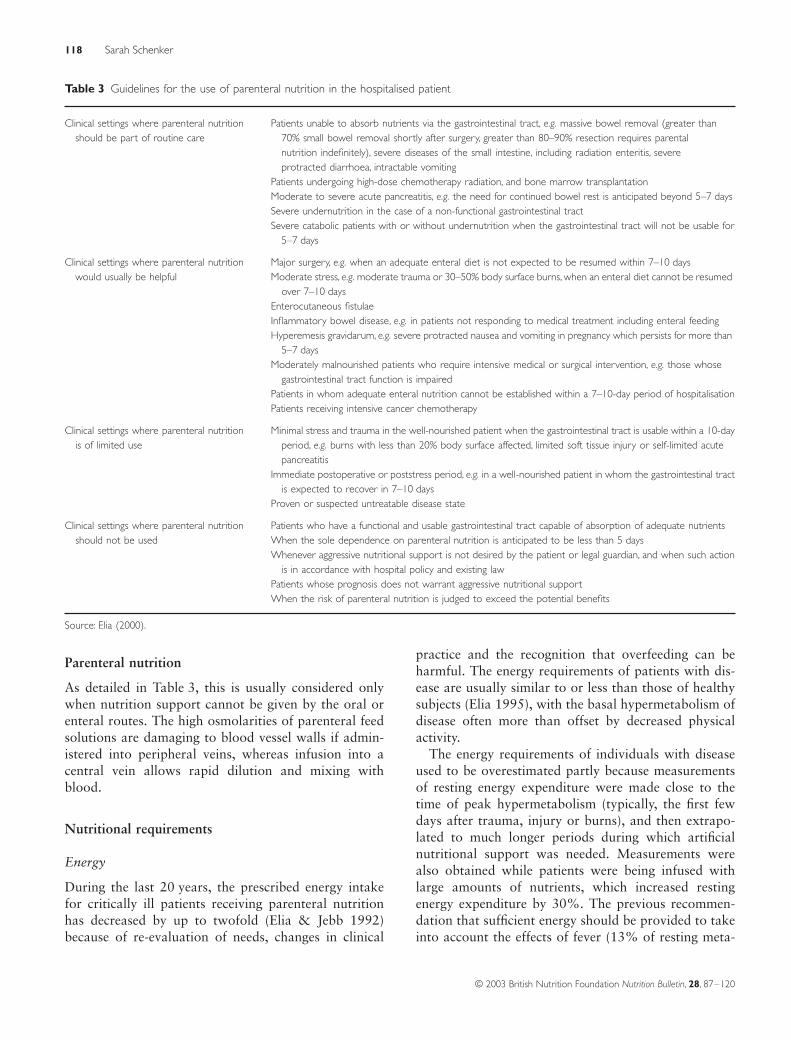
118 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
Parenteral nutrition
As detailed in Table 3 this is usually considered onlywhen nutrition support cannot be given by the oral orenteral routes The high osmolarities of parenteral feedsolutions are damaging to blood vessel walls if admin-istered into peripheral veins whereas infusion into acentral vein allows rapid dilution and mixing withblood
Nutritional requirements
Energy
During the last 20 years the prescribed energy intakefor critically ill patients receiving parenteral nutritionhas decreased by up to twofold (Elia amp Jebb 1992)because of re-evaluation of needs changes in clinical
practice and the recognition that overfeeding can beharmful The energy requirements of patients with dis-ease are usually similar to or less than those of healthysubjects (Elia 1995) with the basal hypermetabolism ofdisease often more than offset by decreased physicalactivity
The energy requirements of individuals with diseaseused to be overestimated partly because measurementsof resting energy expenditure were made close to thetime of peak hypermetabolism (typically the first fewdays after trauma injury or burns) and then extrapo-lated to much longer periods during which artificialnutritional support was needed Measurements werealso obtained while patients were being infused withlarge amounts of nutrients which increased restingenergy expenditure by 30 The previous recommen-dation that sufficient energy should be provided to takeinto account the effects of fever (13 of resting meta-
Table 3 Guidelines for the use of parenteral nutrition in the hospitalised patient
Clinical settings where parenteral nutritionshould be part of routine care
Patients unable to absorb nutrients via the gastrointestinal tract eg massive bowel removal (greater than70 small bowel removal shortly after surgery greater than 80ndash90 resection requires parentalnutrition indefinitely) severe diseases of the small intestine including radiation enteritis severeprotracted diarrhoea intractable vomiting
Patients undergoing high-dose chemotherapy radiation and bone marrow transplantationModerate to severe acute pancreatitis eg the need for continued bowel rest is anticipated beyond 5ndash7 daysSevere undernutrition in the case of a non-functional gastrointestinal tractSevere catabolic patients with or without undernutrition when the gastrointestinal tract will not be usable for
5ndash7 days
Clinical settings where parenteral nutritionwould usually be helpful
Major surgery eg when an adequate enteral diet is not expected to be resumed within 7ndash10 daysModerate stress eg moderate trauma or 30ndash50 body surface burns when an enteral diet cannot be resumed
over 7ndash10 daysEnterocutaneous fistulaeInflammatory bowel disease eg in patients not responding to medical treatment including enteral feedingHyperemesis gravidarum eg severe protracted nausea and vomiting in pregnancy which persists for more than
5ndash7 daysModerately malnourished patients who require intensive medical or surgical intervention eg those whose
gastrointestinal tract function is impairedPatients in whom adequate enteral nutrition cannot be established within a 7ndash10-day period of hospitalisationPatients receiving intensive cancer chemotherapy
Clinical settings where parenteral nutritionis of limited use
Minimal stress and trauma in the well-nourished patient when the gastrointestinal tract is usable within a 10-dayperiod eg burns with less than 20 body surface affected limited soft tissue injury or self-limited acutepancreatitis
Immediate postoperative or poststress period eg in a well-nourished patient in whom the gastrointestinal tractis expected to recover in 7ndash10 days
Proven or suspected untreatable disease state
Clinical settings where parenteral nutritionshould not be used
Patients who have a functional and usable gastrointestinal tract capable of absorption of adequate nutrientsWhen the sole dependence on parenteral nutrition is anticipated to be less than 5 daysWhenever aggressive nutritional support is not desired by the patient or legal guardian and when such action
is in accordance with hospital policy and existing lawPatients whose prognosis does not warrant aggressive nutritional supportWhen the risk of parenteral nutrition is judged to exceed the potential benefits
Source Elia (2000)
Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients

Undernutrition in the UK 119
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
bolic rate per degC rise in temperature) is also inappropri-ate if resting metabolic rate is measured while thepatient has a high temperature The energy cost ofbreathing normally 2ndash3 of resting metabolic rateincreases up to 10-fold in patients with acute respiratorydistress but is included in direct measures of restingmetabolic rate
Changes in clinical practice have reduced energyneeds (Elia 1995) The early surgical removal of necrotictissue in burns rather than leaving it intact to form ascab has decreased the energy requirements of patientswith burns Patients in burn and intensive care units donot wear clothes and are consequently nursed at higherambient temperatures so reducing energy expenditure
More aggressive management of infections (egdrainage of abscesses) has reduced both the magnitudeand duration of hypermetabolism in various clinical set-tings Thus patients in an intensive care unit with sys-temic infections could have a resting metabolic rate ofonly 15 above that predicted even though the mea-surements were made while enteral feeds were infused ata rate of 15 times the metabolic rate
Adverse effects of overfeeding
Animal models of sepsis have shown that overfeedingcan produce huge increases in mortality (Elia amp Jebb1992) Clinically excess carbohydrate and excess lipidhave both been linked to hepatic fat accumulation andabnormal liver function Lipids may also be deposited inthe lungs and impair diffusion of gases and produceinfusional hyperlipidaemia Overfeeding with excesscarbohydrate induces excess carbon dioxide produc-tion which can precipitate respiratory failure in patientswith poor respiratory reserve In critically ill patientshyperglycaemia is common and blood glucose control ismore difficult during overfeeding with high carbohy-drate loads
The rationale for reducing the intake of large amountsof energy in patients with acute illnesses has been rein-forced by the measurement of energy expenditure by24 h continuous indirect calorimetry (eg in ventilatedpatients in intensive care units) and by tracer techniquesThe daily energy expenditure in adults is generally 30ndash35 kcal per kilogram body weight This is irrespective ofwhether the patients are preoperative or postoperativereceiving parenteral nutrition in hospital or at home orare in intensive care units Even children with severeburns may expend similar amounts or less energy thanhealthy children
Hypocaloric feeding may be practised in the earlystages of injury to reduce the risk of metabolic instabil-
ity and its consequences This form of nutritional sup-port while not preventing loss of lean or fat tissue willlimit the loss An emphasis on repletion is then made inthe recovery phase
Further information on nutrient requirements inenteral and parenteral feeding is given in Elia (2000)
Practical aspects of nutrition support
Once the method of feeding has been agreed by the clin-ical nutrition team a number of factors will influencethe specific site of feeding the type of feed used andthe common complications associated with both themethod and physical and psychological state of thepatient
Tube feeding
The use of fine-bore feeding tubes has reduced the extentof complications such as rhinitis oesophagitis andoesophageal strictures that were formerly associatedwith large-bore nasogastric Rylersquos tubes Nasogastricfeeding is not suitable for patients who may regurgitateandor aspirate feed into the lungs so passing the tubefurther into the small intestine may then help Gastros-tomy feeding (feeding directly into the stomach via a finetube) is used for long-term (greater than 30 days) or per-manent enteral feeding Gastrostomies may be madesurgically but this requires laparotomy and a generalanaesthetic therefore percutaneous endoscopic gastros-tomy is now performed using a local anaesthetic anda fibreoptic endoscope Jejunostomies (feeding tubesdirectly into the jejunum) are used in patients prone toaspiration pneumonia
Line feeding
Central vein parenteral nutrition is considered forpatients who require prolonged nutrition support orwho have poor venous access Peripheral vein parenteralnutrition is being increasingly used for providing nutri-tional support to the majority of patients who requireshort-term parenteral nutrition Mechanical problemswith the catheter and catheter-related sepsis are signifi-cantly less than with peripheral parental nutrition Thismethod of feeding is often satisfactory for 1ndash2 weeksbut the incidence of thrombophlebitis after this periodis high Thrombophlebitis is the main disadvantage ofperipheral vein parenteral nutrition and there are anumber of factors that can affect the incidence of thiscondition most important is the high osmolality ofparenteral feeds The carbohydrate content can be
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients
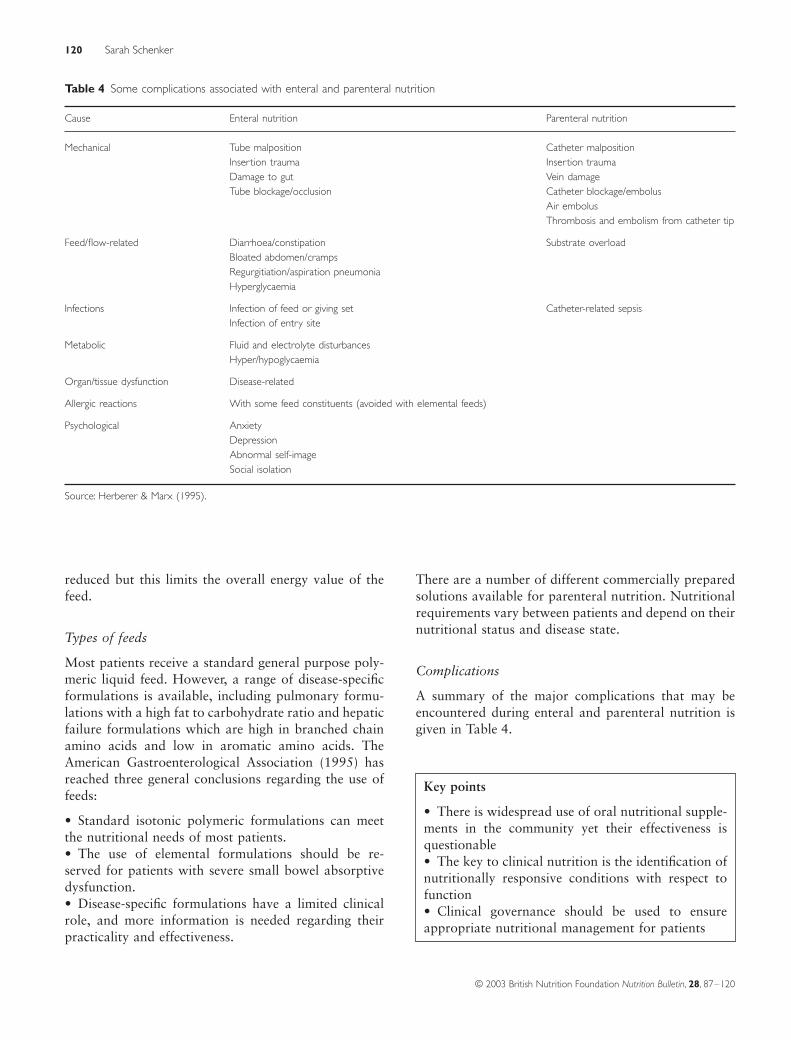
120 Sarah Schenker
copy 2003 British Nutrition Foundation Nutrition Bulletin 28 87ndash120
reduced but this limits the overall energy value of thefeed
Types of feeds
Most patients receive a standard general purpose poly-meric liquid feed However a range of disease-specificformulations is available including pulmonary formu-lations with a high fat to carbohydrate ratio and hepaticfailure formulations which are high in branched chainamino acids and low in aromatic amino acids TheAmerican Gastroenterological Association (1995) hasreached three general conclusions regarding the use offeeds
bull Standard isotonic polymeric formulations can meetthe nutritional needs of most patientsbull The use of elemental formulations should be re-served for patients with severe small bowel absorptivedysfunctionbull Disease-specific formulations have a limited clinicalrole and more information is needed regarding theirpracticality and effectiveness
There are a number of different commercially preparedsolutions available for parenteral nutrition Nutritionalrequirements vary between patients and depend on theirnutritional status and disease state
Complications
A summary of the major complications that may beencountered during enteral and parenteral nutrition isgiven in Table 4
Table 4 Some complications associated with enteral and parenteral nutrition
Cause Enteral nutrition Parenteral nutrition
Mechanical Tube malposition Catheter malpositionInsertion trauma Insertion traumaDamage to gut Vein damageTube blockageocclusion Catheter blockageembolus
Air embolusThrombosis and embolism from catheter tip
Feedflow-related Diarrhoeaconstipation Substrate overloadBloated abdomencrampsRegurgitiationaspiration pneumoniaHyperglycaemia
Infections Infection of feed or giving set Catheter-related sepsisInfection of entry site
Metabolic Fluid and electrolyte disturbancesHyperhypoglycaemia
Organtissue dysfunction Disease-related
Allergic reactions With some feed constituents (avoided with elemental feeds)
Psychological AnxietyDepressionAbnormal self-imageSocial isolation
Source Herberer amp Marx (1995)
Key points
bull There is widespread use of oral nutritional supple-ments in the community yet their effectiveness isquestionablebull The key to clinical nutrition is the identification ofnutritionally responsive conditions with respect tofunctionbull Clinical governance should be used to ensureappropriate nutritional management for patients