©ufs dental benefits – u.s. market june 2010 dr. alan vogel metlife, vp dental products
TRANSCRIPT
©UFS
Dental Benefits – U.S. Market
June 2010Dr. Alan VogelMetLife, VP Dental Products
2
Today’s Topics
• US Dental Market – Statistics
• Dental Plan Evolution – Design & Administration– Initial approach - Cost Drivers
• Plan Design and Contract Provisions• Plan Administration• Provider Networks
– Current approach – Cost & Value Drivers• Research based / Evidenced Based Dentistry• Consumer Directed Plans • Tools – Employee
– Future• Wellness / Disease Management• Data management
3
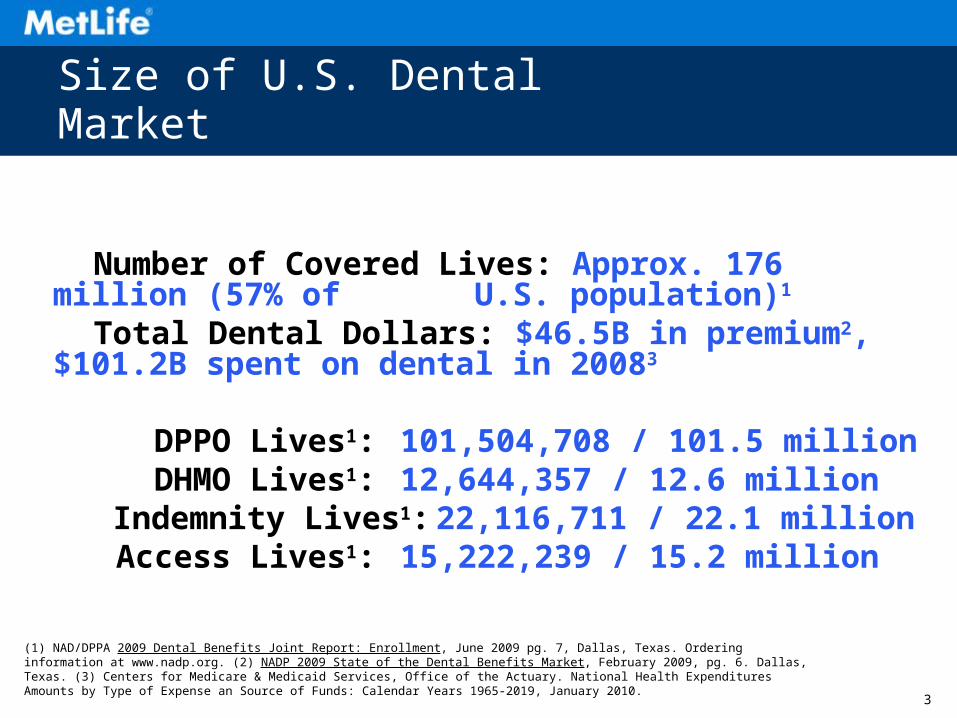
Number of Covered Lives: Approx. 176 million (57% of U.S. population)1
Total Dental Dollars: $46.5B in premium2, $101.2B spent on dental in 20083
DPPO Lives1: 101,504,708 / 101.5 million DHMO Lives1: 12,644,357 / 12.6 million Indemnity Lives1: 22,116,711 / 22.1 million Access Lives1: 15,222,239 / 15.2 million
Size of U.S. Dental Market
(1) NAD/DPPA 2009 Dental Benefits Joint Report: Enrollment, June 2009 pg. 7, Dallas, Texas. Ordering information at www.nadp.org. (2) NADP 2009 State of the Dental Benefits Market, February 2009, pg. 6. Dallas, Texas. (3) Centers for Medicare & Medicaid Services, Office of the Actuary. National Health Expenditures Amounts by Type of Expense an Source of Funds: Calendar Years 1965-2019, January 2010.
4
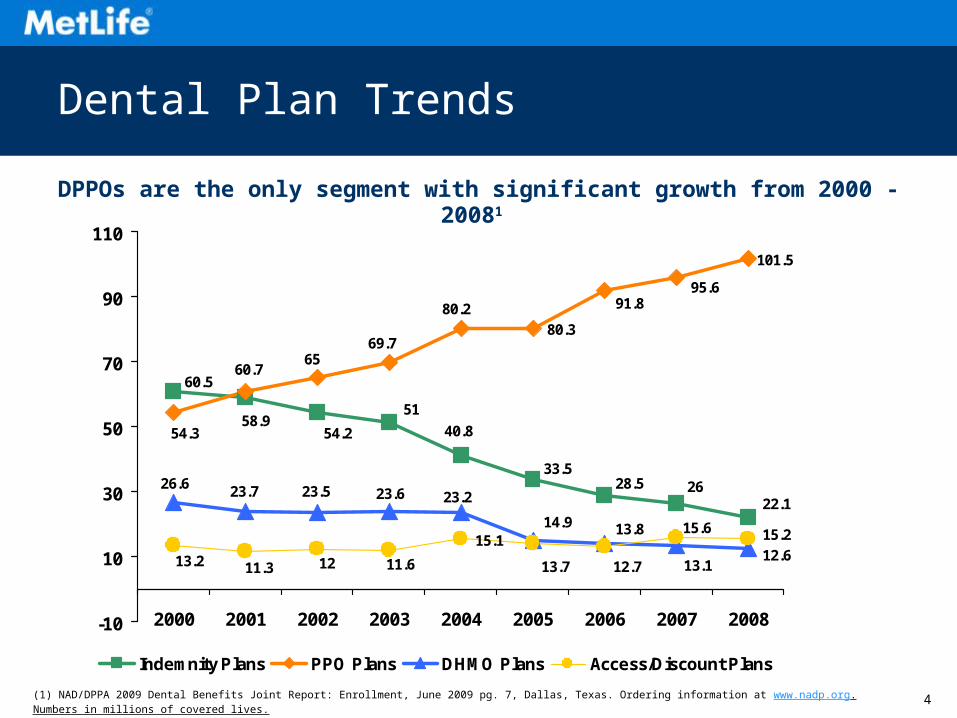
Dental Plan Trends
80.3
101.5
15.1
22.1
33.528.5 26
60.5
40.8
51
54.258.9
95.691.8
54.3
60.765
69.7
80.2
12.6
13.8
13.1
14.9
26.6 23.7 23.5 23.6 23.2
15.215.6
12.713.711.61211.313.2
-10
10
30
50
70
90
110
2000 2001 2002 2003 2004 2005 2006 2007 2008
Indemnity Plans PPO Plans DHMO Plans Access/Discount Plans
(1) NAD/DPPA 2009 Dental Benefits Joint Report: Enrollment, June 2009 pg. 7, Dallas, Texas. Ordering information at www.nadp.org. Numbers in millions of covered lives.
DPPOs are the only segment with significant growth from 2000 - 20081
5
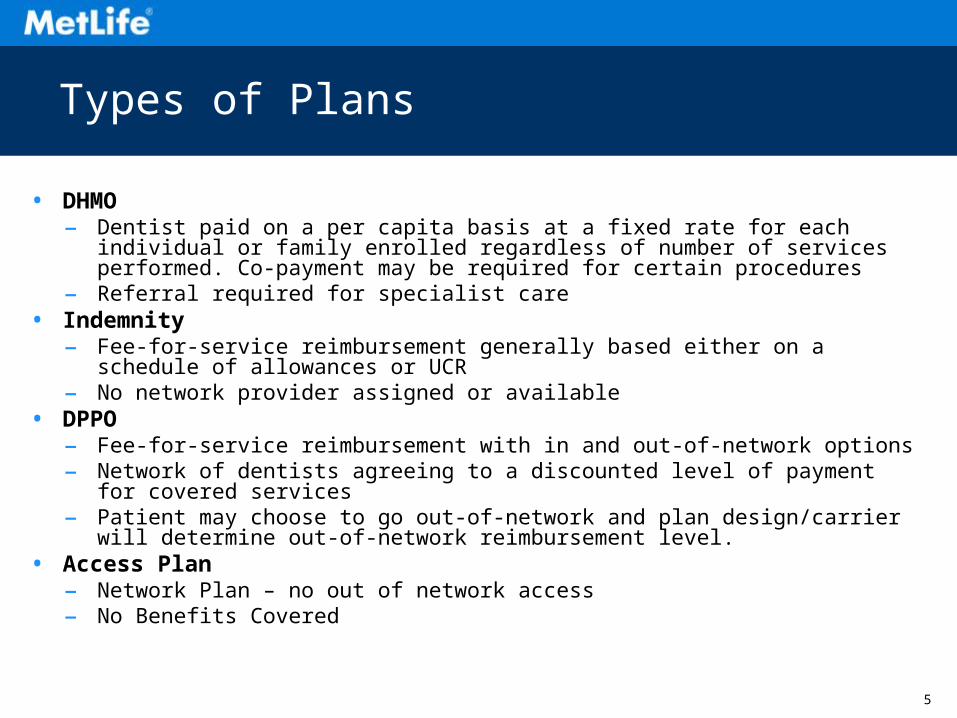
Types of Plans
• DHMO– Dentist paid on a per capita basis at a fixed rate for each individual or family
enrolled regardless of number of services performed. Co-payment may be required for certain procedures
– Referral required for specialist care• Indemnity
– Fee-for-service reimbursement generally based either on a schedule of allowances or UCR
– No network provider assigned or available• DPPO
– Fee-for-service reimbursement with in and out-of-network options– Network of dentists agreeing to a discounted level of payment for covered
services– Patient may choose to go out-of-network and plan design/carrier will determine
out-of-network reimbursement level.• Access Plan
– Network Plan – no out of network access– No Benefits Covered
6
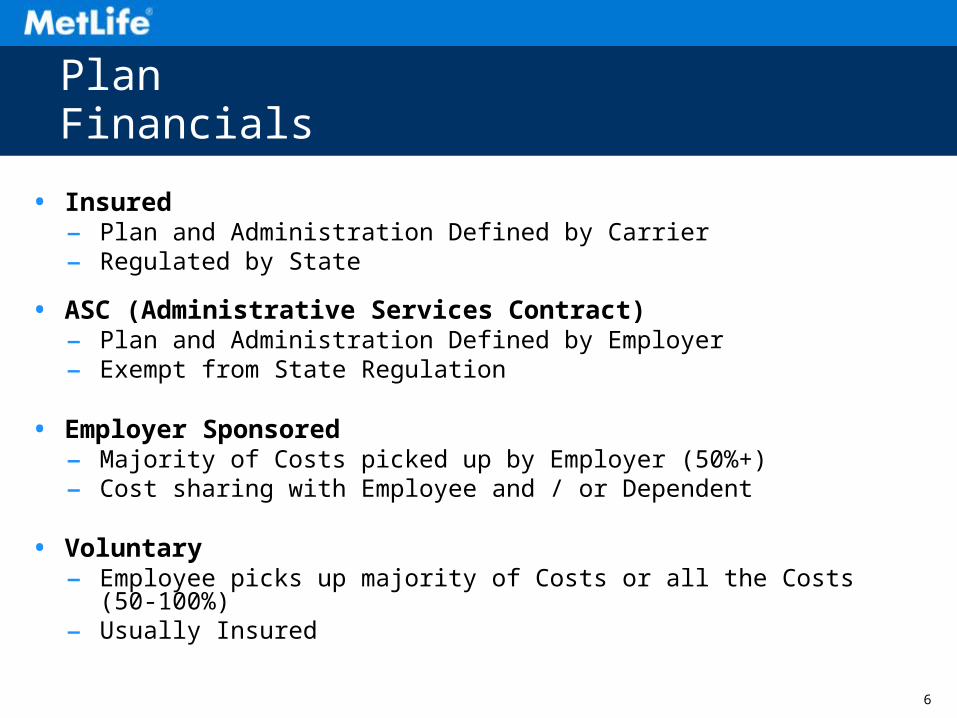
Plan Financials
• Insured– Plan and Administration Defined by Carrier– Regulated by State
• ASC (Administrative Services Contract)– Plan and Administration Defined by Employer– Exempt from State Regulation
• Employer Sponsored– Majority of Costs picked up by Employer (50%+)– Cost sharing with Employee and / or Dependent
• Voluntary– Employee picks up majority of Costs or all the Costs (50-100%)– Usually Insured
7
©UFS
Evolution of Dental Plans Examining the Present and Future
8
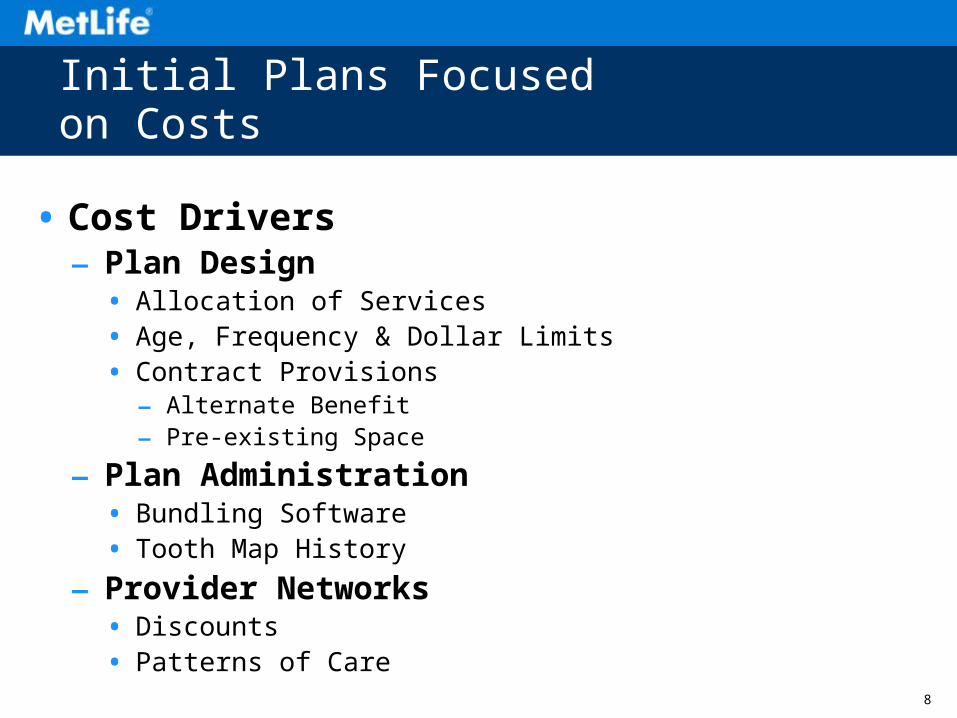
Initial Plans Focused on Costs
• Cost Drivers – Plan Design
• Allocation of Services• Age, Frequency & Dollar Limits• Contract Provisions
– Alternate Benefit– Pre-existing Space
– Plan Administration• Bundling Software• Tooth Map History
– Provider Networks• Discounts• Patterns of Care
9
Costs -Plan Design Components - DPPO / Indemnity
• Allocation of Services & Coinsurance percentages
– Preventive: Cleanings, Routine X-rays (100%)
– Basic Restorative: Fillings, Periodontics, Surgery, Endodontics (80%)
– Major Restorative: Crowns, Bridges/Dentures (50%)
• Plan maximums ($)
– Annual Max and Orthodontia Lifetime Max
• Deductibles (individual & Family)
• Reimbursement Design
• Age & Frequency Limitations
• Exclusions
10
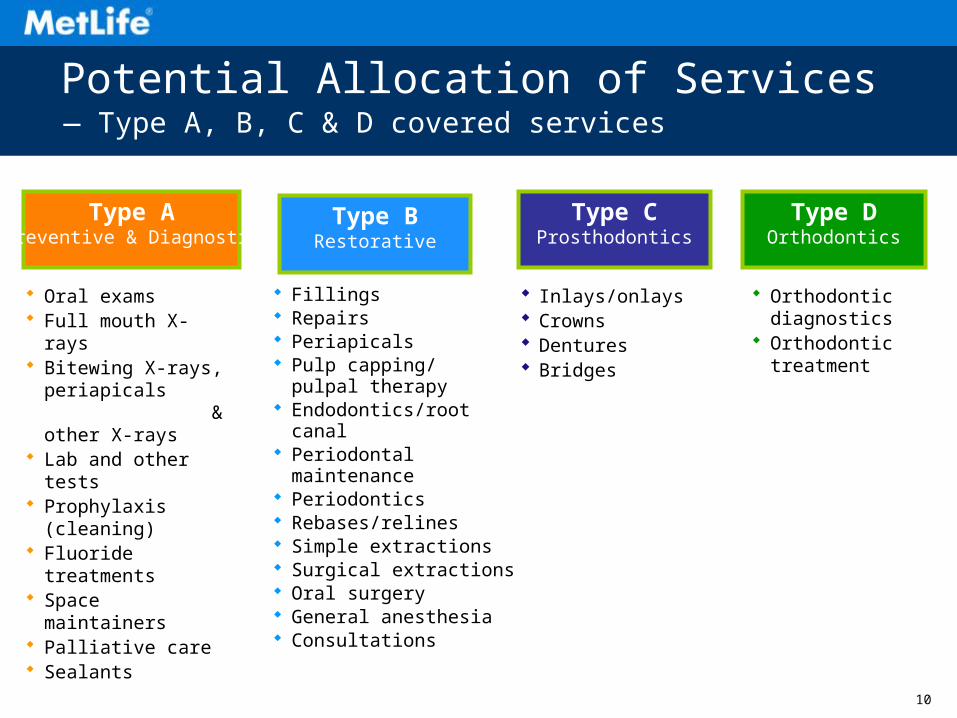
Fillings Repairs Periapicals Pulp capping/
pulpal therapy Endodontics/root canal Periodontal maintenance Periodontics Rebases/relines Simple extractions Surgical extractions Oral surgery General anesthesia Consultations
Potential Allocation of Services
Orthodontic diagnostics
Orthodontic treatment
Type CProsthodontics
Inlays/onlays Crowns Dentures Bridges
Type DOrthodontics
Type BRestorative
Type APreventive & Diagnostic
Oral exams Full mouth X-rays Bitewing X-rays,
periapicals & other X-rays
Lab and other tests Prophylaxis (cleaning) Fluoride treatments Space maintainers Palliative care Sealants
— Type A, B, C & D covered services
11
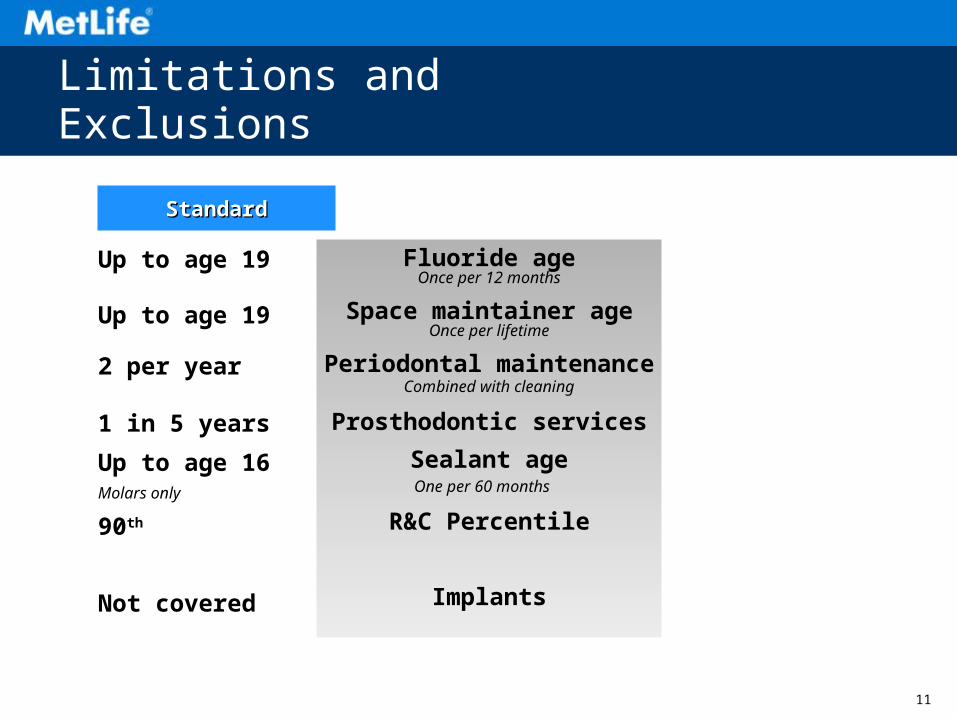
Fluoride ageOnce per 12 months
Space maintainer ageOnce per lifetime
Periodontal maintenanceCombined with cleaning
Prosthodontic services
Sealant ageOne per 60 months
R&C Percentile
Implants
StandardStandard
Up to age 19
Up to age 19
2 per year
1 in 5 years
Up to age 16Molars only
90th
Not covered
Limitations and Exclusions
12
Costs - Plan Administration - PPO / Indemnity
• Unbundling software
• Claim Review
• Reimbursement amounts
• Alternate benefits
• Pre existing conditions
• Prior History (Tooth Map History)
13
Costs - Networks - PPO
• Provider Selection & Credentialing
– Practice Patterns
• Contract
– Defines Relationship to Carrier
– Defines Relationship to Plans
• Fee Schedule
– Creates maximum reimbursement amounts
– Defines many plan requirements
• Access to Providers
– Geo-Access reports – Generalist & Specialist
14
Current Plans Focus on Value & Costs
• Value Drivers (Evidence Based Benefits)– Researched Based Plan Design
• Build Research into Age, Frequency Limits• Build Research into Guidelines & Covered Services
– Consumer Based Plan Ideas• Cover Services That Treat Disease at Higher Levels• Patient makes “Bad Choice” = Higher Costs
– Employee Tools• Oral Health Library• Decision Support
15
Value- Covered Services – Researched based
• Implants
• White Fillings on Molars
• Bruxing Appliances
Add These Services Without Increasing Costs, How?
• Evidenced Based Dentistry - Modify
– Age & frequency limits
– Allocation of Services
– Replacement Limits
16
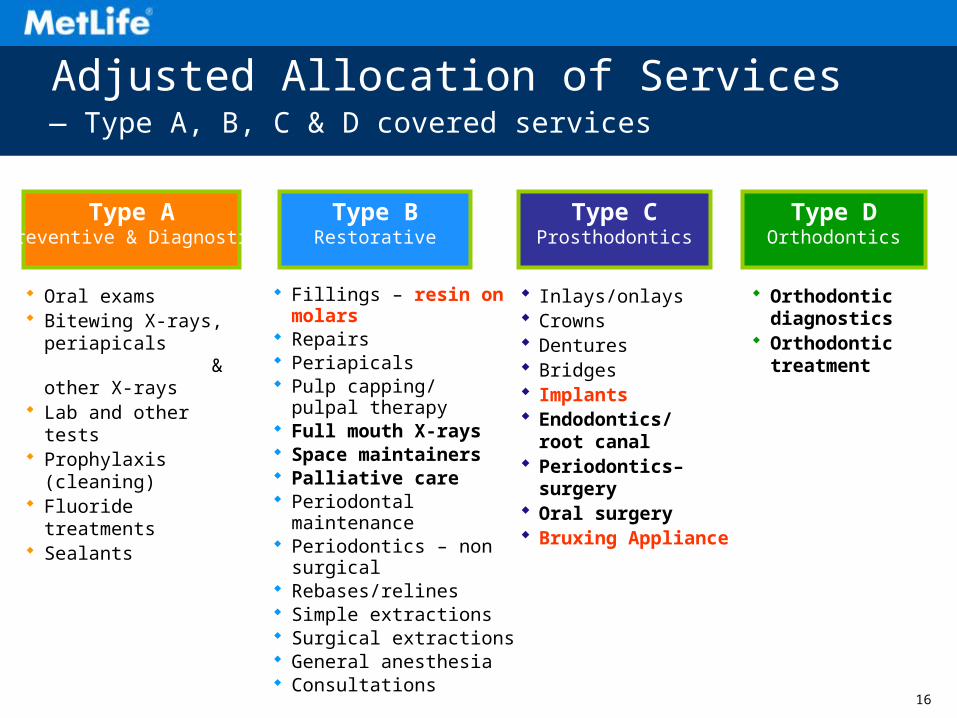
Fillings – resin on molars Repairs Periapicals Pulp capping/
pulpal therapy Full mouth X-rays Space maintainers Palliative care Periodontal maintenance Periodontics – non surgical Rebases/relines Simple extractions Surgical extractions General anesthesia Consultations
Adjusted Allocation of Services
Orthodontic diagnostics
Orthodontic treatment
Type CProsthodontics
Inlays/onlays Crowns Dentures Bridges Implants Endodontics/
root canal Periodontics–surgery Oral surgery Bruxing Appliance
Type DOrthodontics
Type BRestorative
Type APreventive & Diagnostic
Oral exams Bitewing X-rays,
periapicals & other X-rays
Lab and other tests Prophylaxis (cleaning) Fluoride treatments Sealants
— Type A, B, C & D covered services
17
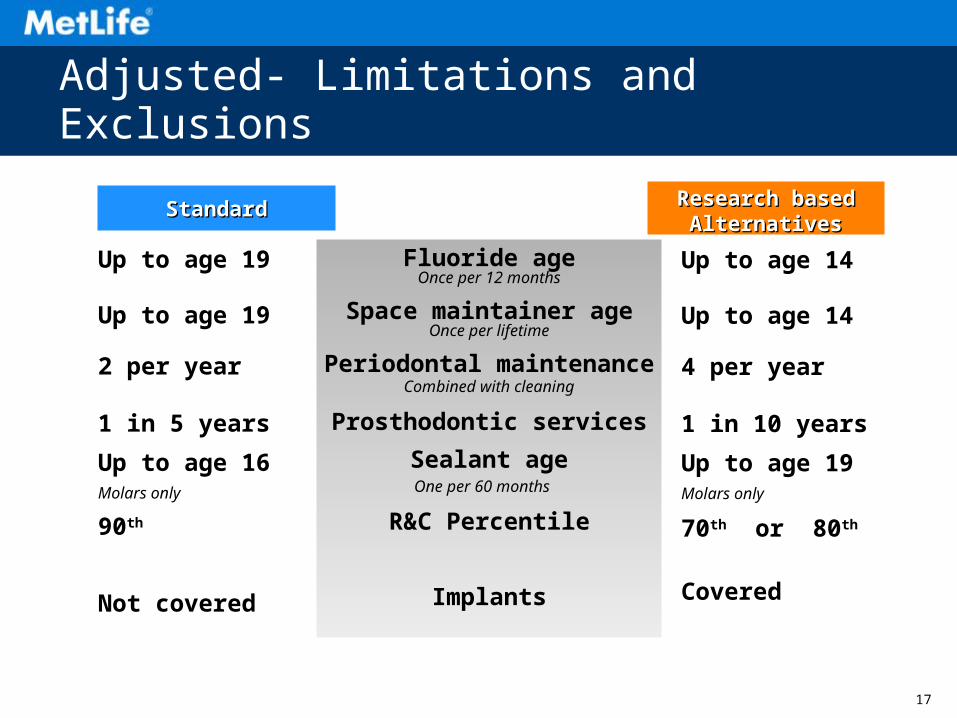
Fluoride ageOnce per 12 months
Space maintainer ageOnce per lifetime
Periodontal maintenanceCombined with cleaning
Prosthodontic services
Sealant ageOne per 60 months
R&C Percentile
Implants
Up to age 14
Up to age 14
4 per year
1 in 10 years
Up to age 19Molars only
70th or 80th
Covered
StandardStandard Research basedResearch basedAlternativesAlternatives
Up to age 19
Up to age 19
2 per year
1 in 5 years
Up to age 16Molars only
90th
Not covered
Adjusted- Limitations and Exclusions
18
Value- Employee Tools
• Self Service
– Claim information
– Plan information
– Network Providers
• Oral Health Library
– Educational on Services
– Educational on Risks
• Fee Estimator

1919
What’s Driving Dental Plan Design Evolution?
Do the dental plans you recommend recognize and incorporate these trends?
Dental Standards & Market Practice
Dental BenefitsEnvironment
Research & Risk
Changing Benefits
Objectives & Demands
Dental Plan Design
20
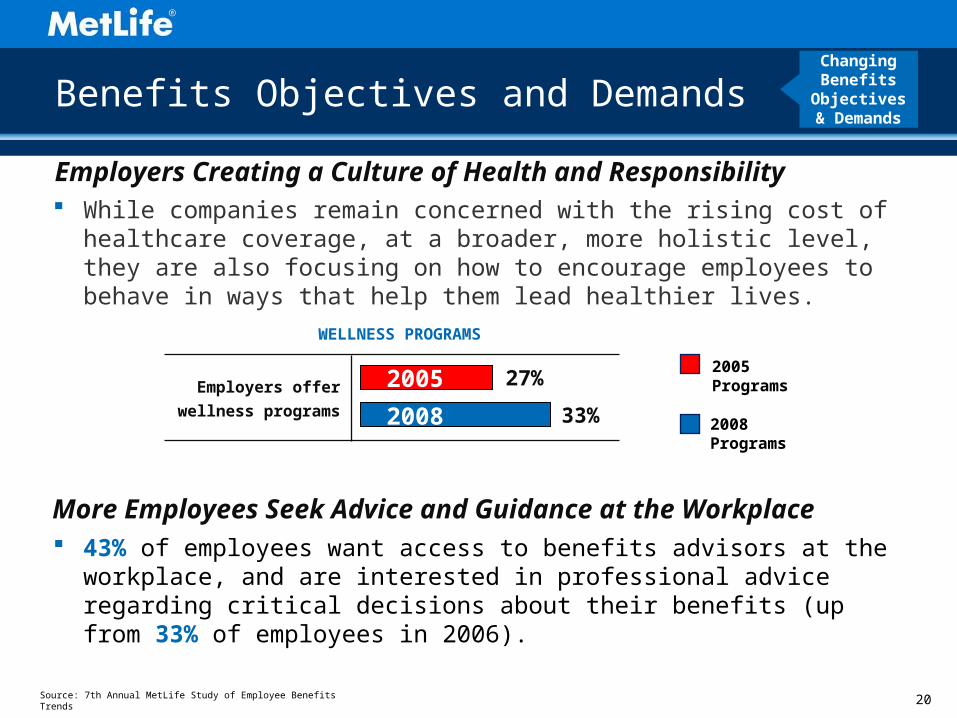
More Employees Seek Advice and Guidance at the Workplace
Source: 7th Annual MetLife Study of Employee Benefits Trends
Benefits Objectives and Demands
Employers Creating a Culture of Health and Responsibility
2005 Programs
2008 Programs
WELLNESS PROGRAMS
Employers offer
wellness programs
27%
33%
2005
2008
While companies remain concerned with the rising cost of healthcare coverage, at a broader, more holistic level, they are also focusing on how to encourage employees to behave in ways that help them lead healthier lives.
43% of employees want access to benefits advisors at the workplace, and are interested in professional advice regarding critical decisions about their benefits (up from 33% of employees in 2006).
Changing Benefits
Objectives & Demands
21
Risk Is Playing a More Important Role inDental Plan Design
(1) Khader YS, Ta’ani Q. Periodontal diseases and the risk of preterm birth and low birth weight: a meta-analysis. Evid Based Dent 2005 Feb; 76(2):161-5. (2) Mealey B.L. Oates T.V. Diabetes Mellitus and Periodontal Diseases. AAP-Commissioned Review. J Periodontal 2006;77:1289-1303.. (3) Humphrey LL, Fu R Buckley DI, Freeman M, Helfand M. J Gen Intern Med. 2008;23(12):2079-86; (4) Keene, Joseph J. Jr., et al. “Antidepressant use in psychiatry and medicine — Importance for dental practice,” Journal of the American Dental Association, Vol. 134, January 2003; (5) Dirix, Piet, et al. “Radiation-Induced Xerostomia in Patients with Head and Neck Cancer,” Cancer, Vol. 107, number 11, December 2006; (6) Migliorati et al. “Managing the care of patients with bisphosphonate-associated osteonecrosis: An American Academy of Oral Medicine Position Paper.” Journal of the American Dental Association. Vol. 136, December 2005; (7) Ioannidou et al. Elevated Serum Interleukin-6 (IL-6) in Solid-Organ Transplant Recipients Is Positively Associated With Tissue Destruction and IL-6 Gene Expression in the Periodontium.” Journal of Periodontology, 2006, Vol. 77, No. 1, pg 1871-1878.
21
People taking Antidepressants or Cancer Patients undergoing radiation — In some cases antidepressants and radiation may cause Xerostomia (dry mouth), which can compromise oral health.4,5
Women taking Bisphosphonates for Osteoporosis (Injectable) — Bisphosphonates may contribute to osteonecrosis of the jaw in some cases6
People in need of organ transplants — One study suggests they may have a better chance for success of the transplant if their oral health is good7 (a link between chronic periodontitis and the risk for rejection)
Research has suggested a relationship between oral and overall health, and has associated periodontal disease with conditions such as preterm births1, diabetes2, and coronary heart disease3.
However, studies have suggested additional relationships between oral and overall health for which further research is underway:
Research & Risk
22
Do you know?
It’s estimated 35% of adults have periodontal disease1, and up to 13% have moderate or severe periodontal disease2.
Q: and what percent is attributed to smoking?
A: Half2,3
(1) Quality Resource Guide, “Assessing Risk for Chronic Periodontitis in Adults, Dr. Ray Williams, DMD, Chair Department of Periodontology, University of North Carolina School of Dentistry. (2) Center for Disease Control, Oral Health at a Glance, 2010 (3) Journal of the American Dental Association, “Risk assessment and management of periodontal disease”, Douglass, 2006 (4) Tobacco and healthy teeth don’t mix. Canadian Dental Association website. www.healthyteeth.org/tobacco. Accessed October 2, 2009.
23
Do you know?
So what?
Research suggests there is a two-way connection between diabetes and periodontal disease – not only are diabetics more susceptible (to periodontal disease), but the presence (of perio disease) may also make glycemic control more difficult.2
(1) Center for Disease Control, National Diabetes Fact Sheet, 2007(2) Department of Health and Human Services, “Working Together to Manage Diabetes”, 2007
24
Do you know?
Q: Among the 50 most prescribed medications, this percent had the capacity to cause xerostomia1, or dry mouth, as a side effect?
A: Half
(1) Quality Resource Guide, “Recognition and Management of Patients with Xerostomia”, James Guggenheimer, DDS, University of Pittsburgh School of Dental Medicine
25
Future Plan Focus
• Disease Management / Wellness– Medical / Dental Integration – Patient Information– Education – To Risks for Disease– Variable Benefits – Based on Individual Risk
• Data Mining– Outcome Measures – Network Selection Process– Provider (Dentist) Profiles – Focused Claim Review– Utilization Statistics – Show Value of Program to:
• Patients• Dentists• Payor
26
WHY???
So A Carrier Can: Analyze and challenge plan designs
– Look deeper than 100/80/50 and question where services are allocated
– Understand limitations, exclusions, contract language — and ask questions!
Understand what adds value to a plan and what is questionable
Educate your clients on “why change plans”
Present the best plans and alternatives to meet your customers’ unique needs
27
Questions?