triumeq * (dtg/abc/3tc): bioequivalence data · triumeq® * (dtg/abc/3tc): bioequivalence data...
TRANSCRIPT
TRIUMEQ®* (DTG/ABC/3TC):
BIOEQUIVALENCE DATA
UK/TRIM/0048/14(2)
Date of preparation: March2017
Prescribing information is available at the end of this presentation
*In studies supporting TRIUMEQ, DTG 50 mg + ABC 600 mg/3TC 300 mg were used.
Bioequivalence has been demonstrated.
DTG, dolutegravir; ABC, abacavir; 3TC, lamivudine
DECLARATION OF INTEREST
In studies supporting TRIUMEQ, DTG 50 mg + ABC 600 mg/3TC 300 mg were used
Bioequivalence was demonstrated between the TRIUMEQ as a single-pill and the
separate co-administered tablet formulations of DTG + ABC/3TC
INTRODUCTION: TRIUMEQ AND DTG + ABC/3TC –
BIOEQUIVALENCE
TRIUMEQ Summary of Product Characteristics, January 2017; Weller S et al. JAIDS 2014;66:393-8

KEY STUDIES
† DTG 50mg + ABC 600mg/3TC 300mg were
used. Bioequivalence has been
demonstrated.13
* BR - background regimen
** OBR - optimised background regimen
1. Clotet B et al. Lancet. 2014;383(9936):2222-2231. 2. Orrell C et al. Presented at 21st International AIDS Conference, 18th-22nd July, 2016; Durban, South Africa.
Abstract THAB0205LB. 3. Walmsley S et al. N Engl J Med. 2013;369(19):1807-1818. 4. Walmsley S et al. J Acquir Immune Defic Syndr. 2015;70:515-519. 5. Molina
J-M et al. Lancet HIV.2015;2(4):e127-e136. January 2017. 6. Raffi F et al. Lancet Infect Dis. 2013;13:927–935 7. Raffi F et al. Lancet. 2013; 381: 735–743. 8. Cahn P
et al. Lancet. 2013; 382: 700–708. 9. Trottier B et al. Presented at 55th Interscience Conference on Antimicrobial Agents and Chemotherapy, 17th-21st September,
2015; San Diego, CA. LB3271. 10 Lake JE et al. Presented at 21st International AIDS Conference, 18th-22nd July, 2016; Durban, South Africa. Abstract THAB0203.
11. Castagna A et al. J Infect Dis. 2014; 210:354-362.
AT
RIP
LA
®
SINGLE Treatment-naïve patients
TRIUMEQ® † QD vs Atripla® QD (N=833)
SUPERIOR EFFICACY
vs Atripla®
at weeks 48 (primary endpoint),
96 and 144
BO
OS
TE
D P
ls
FLAMINGO Treatment-naïve patients
DTG + 2 NRTIs QD vs DRV/r + 2 NRTIs QD (N=484)
SUPERIOR EFFICACY
vs darunavir/r
at weeks 48 (primary endpoint)
and 96
ARIA Treatment-naïve women
TRIUMEQ QD vs ATV/r + TDF/FTC QD (N=495)
SUPERIOR EFFICACY
vs atazanavir/r
at week 48 (primary endpoint)
INIs
SPRING-2 Treatment-naïve patients
DTG + 2 NRTIs QD vs RAL + 2 NRTIs BID (N=822)
NON-INFERIOR EFFICACY
vs raltegravir
at weeks 48 (primary endpoint) and 96
SAILING Treatment-experienced,
INI-naïve patients
DTG QD + BR* vs RAL BID + BR* (N=719)
SUPERIOR EFFICACY
vs raltegravir
at week 48 (primary endpoint)
Co
nti
nu
ing
AR
T
STRIIVING Treatment-experienced,
stable-switch patients
TRIUMEQ QD vs continuing ARV regimen (N=551)
NON-INFERIOR EFFICACY
up to weeks 24 (primary endpoint)
and 48
Hea
vily
Trea
tmen
t-
Exp
erie
nce
d
VIKING-3
Heavily treatment experienced
patients with RAL and/or EVG
resistant HIV-1
DTG 50mg BD + OBR** (N=183)-single-arm study
SUSTAINED EFFICACY
up to weeks 24 (primary endpoint)
and 48

BIOEQUIVALENCE
FDCs have greatly simplified the treatment of patients with HIV
DTG is a booster-free INI approved for treatment of HIV-1 infection in combination
with other antiretroviral agents
ABC and 3TC are NRTIs available as a single pill (Kivexa®)
The combination of DTG, ABC and 3TC as a single pill would have several potential
advantages over other FDCs, including fewer drug interactions, once daily dosing,
no need for boosting and no time-of-day or food restrictions
DTG, ABC and 3TC as a single pill is suitable for HLA-B*5701-negative patients
TRIUMEQ (DTG/ABC/3TC) SINGLE PILL
REGIMEN BIOEQUIVALENCE: INTRODUCTION
TRIUMEQ Summary of Product Characteristics, January 2017; Kivexa Summary of Product Characteristics, October 2016; Ramjan R et al. Trop Med Int Health
2014;19:501-13; Weller S et al. JAIDS 2014;66:393-8
Primary objective
Evaluate single-dose bioequivalence in the fasted state between the TRIUMEQ
(DTG/ABC/3TC; 50/600/300 mg) single-pill and DTG 50 mg given with separate
ABC/3TC (600/300 mg) to healthy volunteers (Part A)
Secondary objectives
Evaluate the effect of food on the bioavailability of single-dose TRIUMEQ (Part B)
Assess the safety and tolerability of single-dose administration of DTG, ABC and 3TC
in healthy volunteers either fasted or with food
TRIUMEQ SINGLE PILL REGIMEN
BIOEQUIVALENCE: OBJECTIVES
Weller S et al. JAIDS 2014;66:393-8
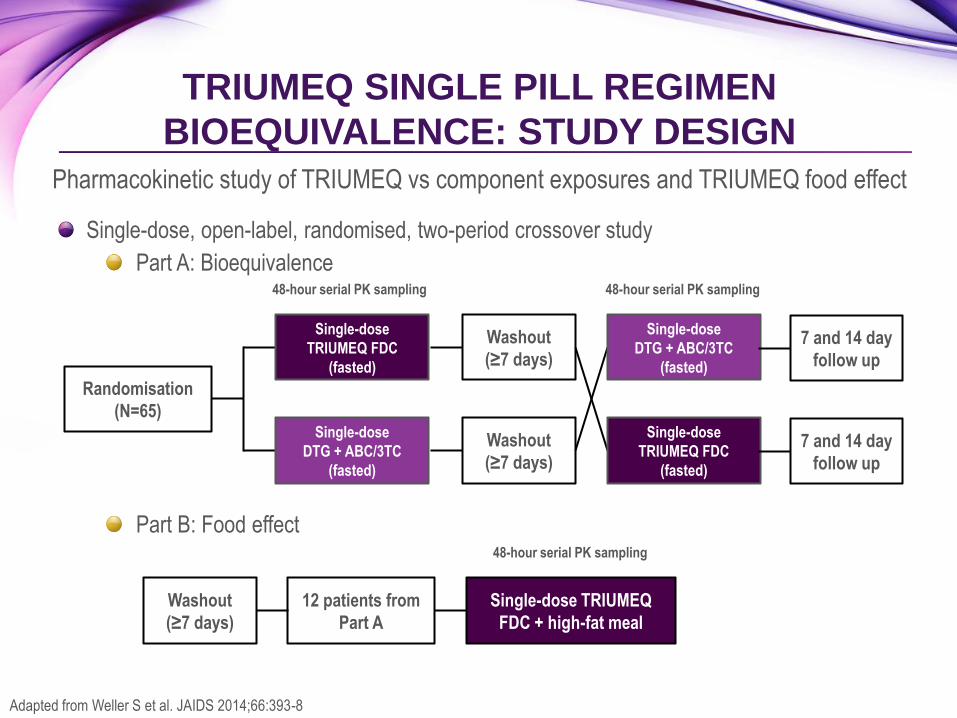
Single-dose, open-label, randomised, two-period crossover study
Part A: Bioequivalence
Part B: Food effect
TRIUMEQ SINGLE PILL REGIMEN
BIOEQUIVALENCE: STUDY DESIGN
Pharmacokinetic study of TRIUMEQ vs component exposures and TRIUMEQ food effect
Randomisation
(N=65)
Single-dose
TRIUMEQ FDC
(fasted)
Single-dose
DTG + ABC/3TC
(fasted)
Washout
(≥7 days)
Washout
(≥7 days)
Single-dose
DTG + ABC/3TC
(fasted)
Single-dose
TRIUMEQ FDC
(fasted)
48-hour serial PK sampling 48-hour serial PK sampling
12 patients from
Part A
Single-dose TRIUMEQ
FDC + high-fat meal
Washout
(≥7 days)
48-hour serial PK sampling
Adapted from Weller S et al. JAIDS 2014;66:393-8
7 and 14 day
follow up
7 and 14 day
follow up
TRIUMEQ SINGLE PILL REGIMEN
BIOEQUIVALENCE: STUDY DESIGN
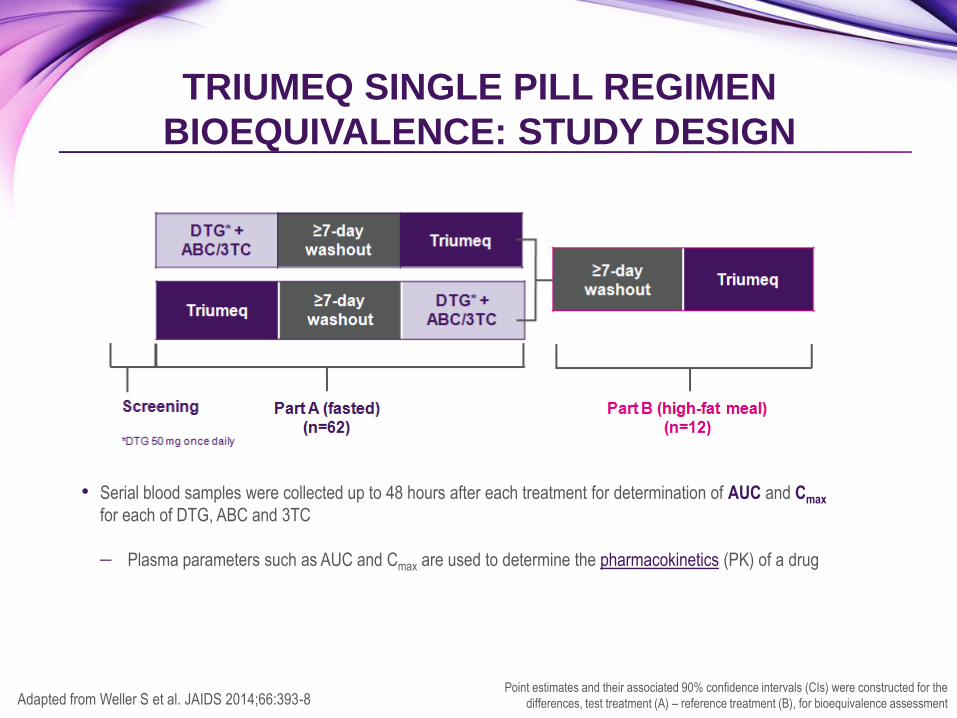
Point estimates and their associated 90% confidence intervals (CIs) were constructed for the
differences, test treatment (A) – reference treatment (B), for bioequivalence assessment Adapted from Weller S et al. JAIDS 2014;66:393-8
• Serial blood samples were collected up to 48 hours after each treatment for determination of AUC and Cmax
for each of DTG, ABC and 3TC
Plasma parameters such as AUC and Cmax are used to determine the pharmacokinetics (PK) of a drug
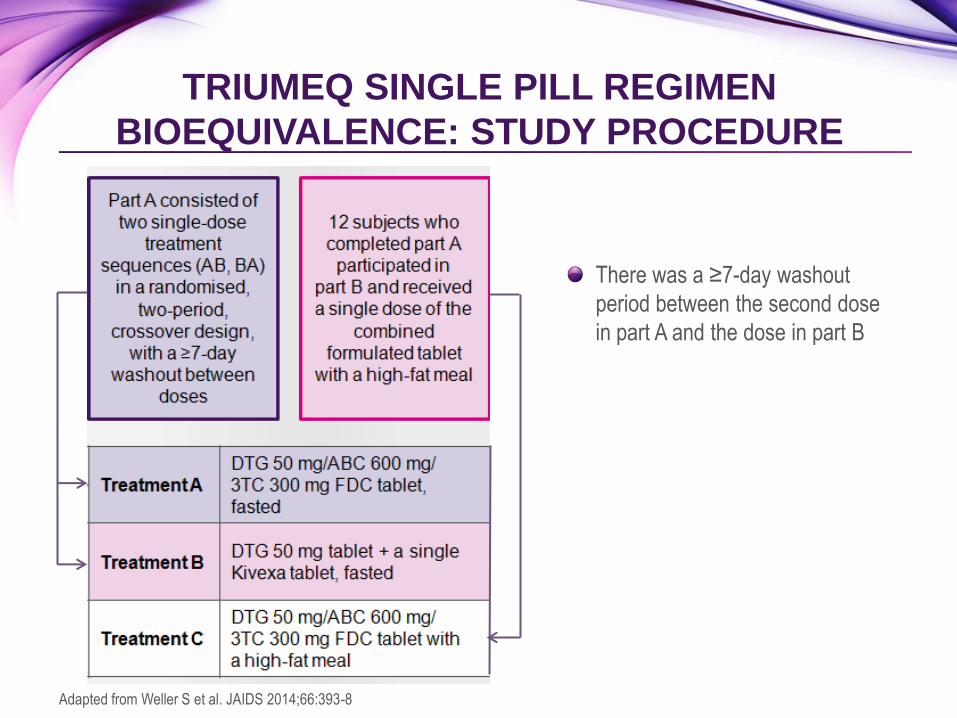
There was a ≥7-day washout
period between the second dose
in part A and the dose in part B
TRIUMEQ SINGLE PILL REGIMEN
BIOEQUIVALENCE: STUDY PROCEDURE
Adapted from Weller S et al. JAIDS 2014;66:393-8
65 subjects randomised to either Group 1 or Group 2
Group 1 received a single dose of Triumeq FDC followed by DTG +
ABC/3TC
Group 2 received DTG + ABC/3TC followed by a single dose of TRIUMEQ
FDC
62 subjects completed the study
TRIUMEQ SINGLE PILL REGIMEN
BIOEQUIVALENCE: STUDY POPULATION

TRIUMEQ SINGLE PILL REGIMEN
BIOEQUIVALENCE: PATIENT DEMOGRAPHICS
Demographics
TRIUMEQ
fasted
(n=65)
DTG + ABC/3TC
fasted
(n=65)
TRIUMEQ
fed
(n=12)
Age, mean (SD), years 29.3 (9.59) 29.3 (9.55) 33.8 (11.06)
Sex, n (%)
Female 22 (34%) 22 (34%) 4 (33%)
Male 43 (66%) 43 (66%) 8 (67%)
BMI, mean (SD), kg/m2 25.03 (3.72) 25.16 (3.71) 26.48 (3.09)
Height, mean (SD), cm 172.55 (10.01) 172.58 (9.97) 175.86 (11.64)
Weight, mean (SD), kg 74.69 (13.72) 75.05 (13.48) 82.29 (14.75)
Race, n (%)
African American/African heritage 25 (38%) 25 (38%) 5 (42%)
White – White/Caucasian/European heritage 34 (52%) 34 (52%) 7 (58%)
Part A Part B
BMI, body mass index; SD, standard deviation
Adapted from Weller S et al. JAIDS 2014;66:393-8
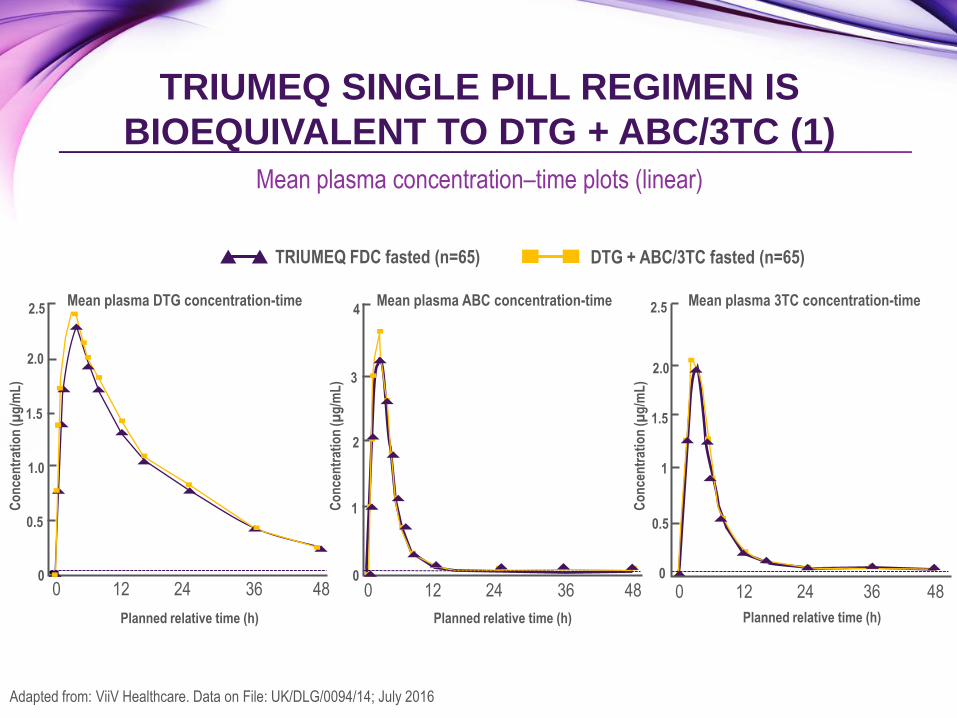
Mean plasma concentration–time plots (linear)
TRIUMEQ SINGLE PILL REGIMEN IS
BIOEQUIVALENT TO DTG + ABC/3TC (1)
Adapted from: ViiV Healthcare. Data on File: UK/DLG/0094/14; July 2016
Mean plasma DTG concentration-time Mean plasma ABC concentration-time Mean plasma 3TC concentration-time
Planned relative time (h)
Co
nce
ntr
atio
n (µ
g/m
L)
2.5
2.0
1.5
1.0
0.5
0 24 0 12 36 48
1.5
0.5
2.0
24 0 12 36 48
2.5
1
0
24 0 12 36 48
4
3
2
1
0
Co
nce
ntr
atio
n (µ
g/m
L)
Co
nce
ntr
atio
n (µ
g/m
L)
Planned relative time (h)
DTG + ABC/3TC fasted (n=65) TRIUMEQ FDC fasted (n=65)
Planned relative time (h)
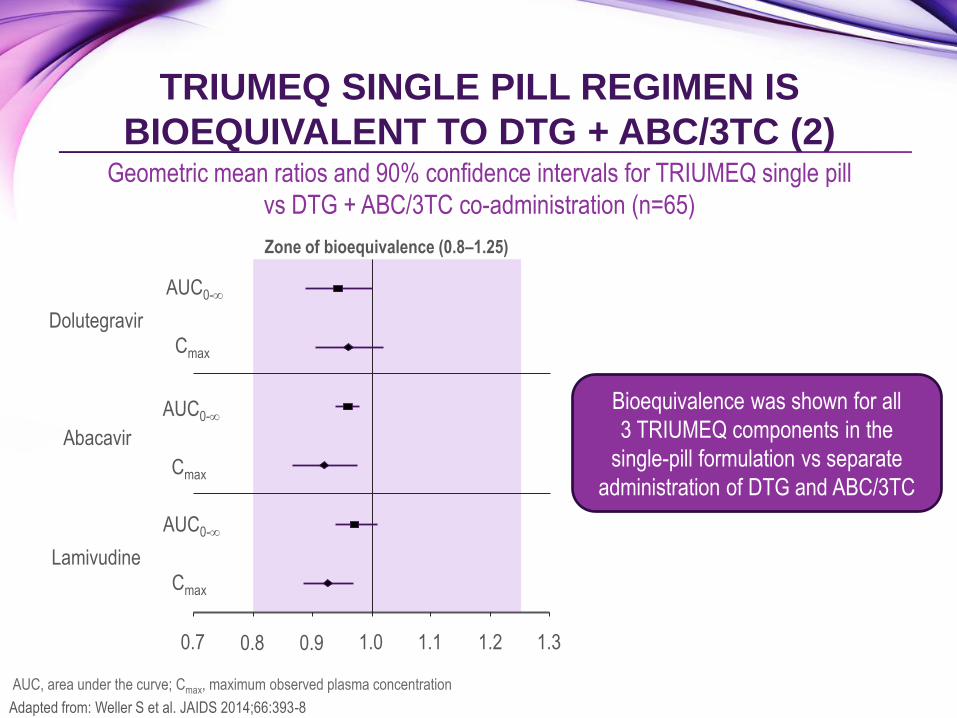
Geometric mean ratios and 90% confidence intervals for TRIUMEQ single pill
vs DTG + ABC/3TC co-administration (n=65)
TRIUMEQ SINGLE PILL REGIMEN IS
BIOEQUIVALENT TO DTG + ABC/3TC (2)
Adapted from: Weller S et al. JAIDS 2014;66:393-8
Zone of bioequivalence (0.8–1.25)
0.7 0.8 0.9 1.0 1.1 1.2 1.3
Dolutegravir
AUC0-
Cmax
AUC0-
Cmax
AUC0-
Cmax
Abacavir
Lamivudine
Bioequivalence was shown for all
3 TRIUMEQ components in the
single-pill formulation vs separate
administration of DTG and ABC/3TC
AUC, area under the curve; Cmax, maximum observed plasma concentration
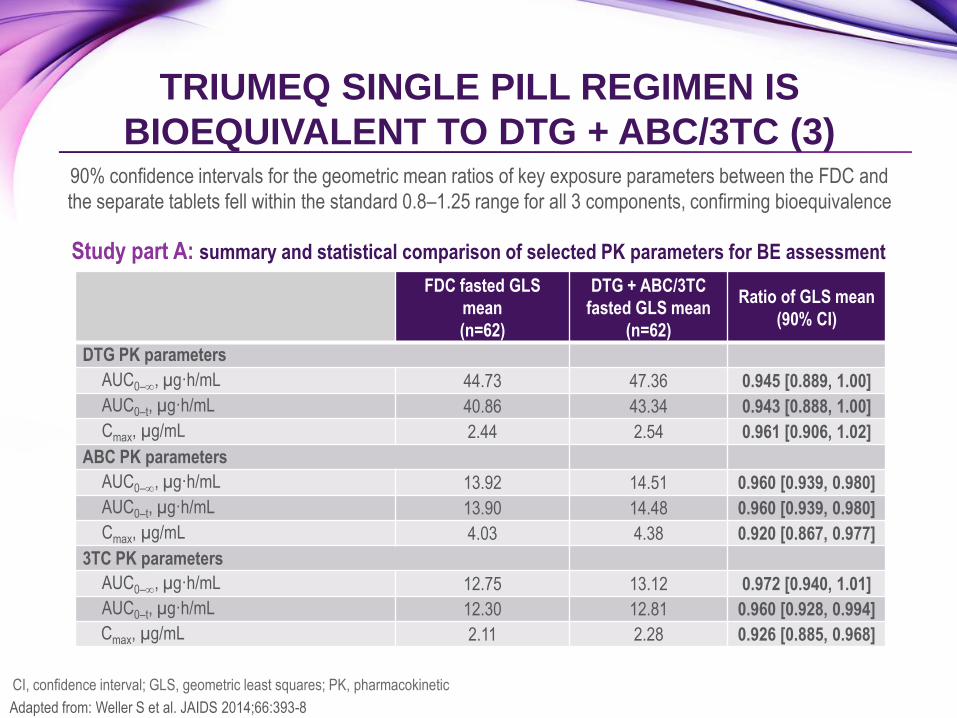
90% confidence intervals for the geometric mean ratios of key exposure parameters between the FDC and
the separate tablets fell within the standard 0.8–1.25 range for all 3 components, confirming bioequivalence
TRIUMEQ SINGLE PILL REGIMEN IS
BIOEQUIVALENT TO DTG + ABC/3TC (3)
Adapted from: Weller S et al. JAIDS 2014;66:393-8
Study part A: summary and statistical comparison of selected PK parameters for BE assessment
FDC fasted GLS
mean
(n=62)
DTG + ABC/3TC
fasted GLS mean
(n=62)
Ratio of GLS mean
(90% CI)
DTG PK parameters
AUC0–, µg·h/mL 44.73 47.36 0.945 [0.889, 1.00]
AUC0–t, µg·h/mL 40.86 43.34 0.943 [0.888, 1.00]
Cmax, µg/mL 2.44 2.54 0.961 [0.906, 1.02]
ABC PK parameters
AUC0–, µg·h/mL 13.92 14.51 0.960 [0.939, 0.980]
AUC0–t, µg·h/mL 13.90 14.48 0.960 [0.939, 0.980]
Cmax, µg/mL 4.03 4.38 0.920 [0.867, 0.977]
3TC PK parameters
AUC0–, µg·h/mL 12.75 13.12 0.972 [0.940, 1.01]
AUC0–t, µg·h/mL 12.30 12.81 0.960 [0.928, 0.994]
Cmax, µg/mL 2.11 2.28 0.926 [0.885, 0.968]
CI, confidence interval; GLS, geometric least squares; PK, pharmacokinetic
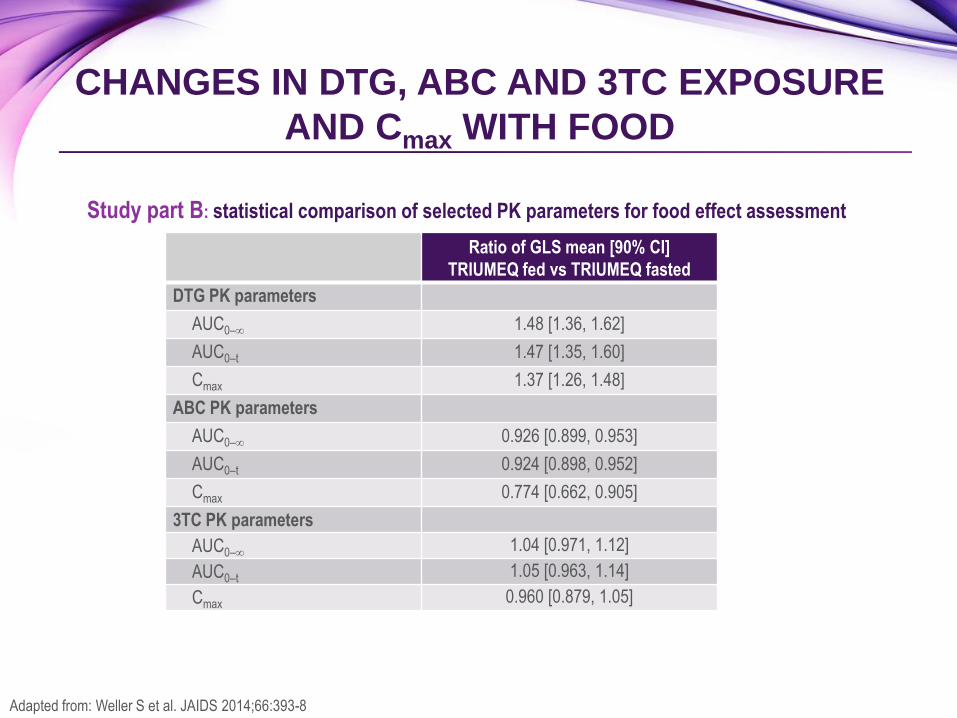
CHANGES IN DTG, ABC AND 3TC EXPOSURE
AND Cmax WITH FOOD
Study part B: statistical comparison of selected PK parameters for food effect assessment
Ratio of GLS mean [90% CI]
TRIUMEQ fed vs TRIUMEQ fasted
DTG PK parameters
AUC0– 1.48 [1.36, 1.62]
AUC0–t 1.47 [1.35, 1.60]
Cmax 1.37 [1.26, 1.48]
ABC PK parameters
AUC0– 0.926 [0.899, 0.953]
AUC0–t 0.924 [0.898, 0.952]
Cmax 0.774 [0.662, 0.905]
3TC PK parameters
AUC0– 1.04 [0.971, 1.12]
AUC0–t 1.05 [0.963, 1.14]
Cmax 0.960 [0.879, 1.05]
Adapted from: Weller S et al. JAIDS 2014;66:393-8
DTG plasma exposures with a high-fat meal
Approximately 48% higher for AUC and 37% higher for Cmax than in the fasted condition
Indicate that TRIUMEQ can be taken with or without food
ABC and 3TC plasma exposures with a high-fat meal
Generally similar to fasted exposures
Cmax for ABC was 23% lower with food
Consistent with prior results for ABC/3TC, which may be taken with or without food
TRIUMEQ AND FOOD
Weller S et al. JAIDS 2014;66:393-8; TRIUMEQ Summary of Product Characteristics, January 2017
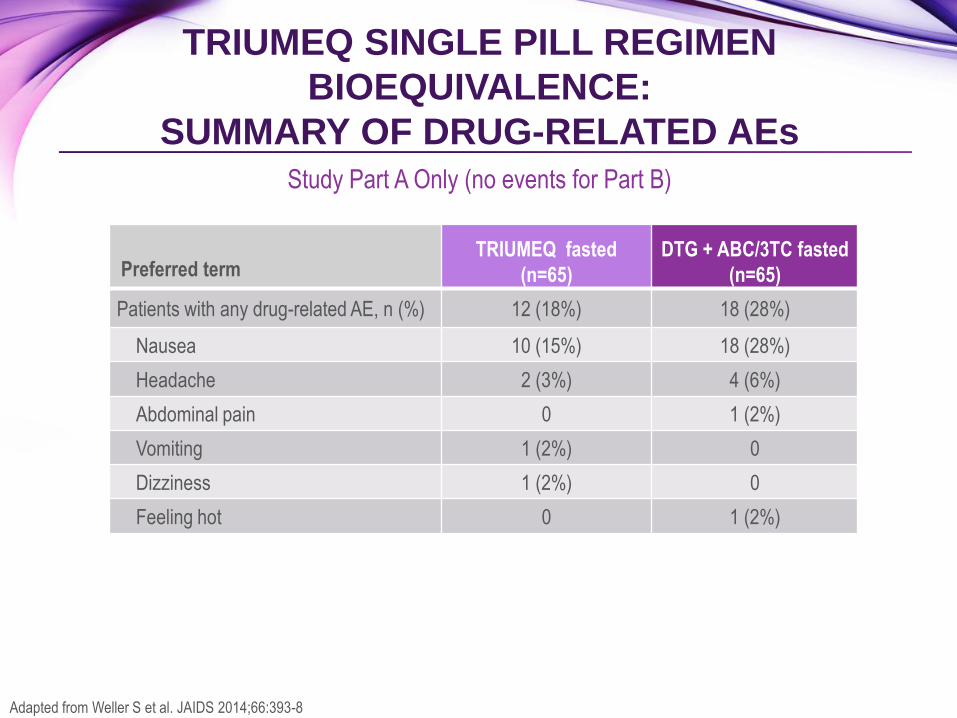
Study Part A Only (no events for Part B)
TRIUMEQ SINGLE PILL REGIMEN
BIOEQUIVALENCE:
SUMMARY OF DRUG-RELATED AEs
Preferred term TRIUMEQ fasted
(n=65)
DTG + ABC/3TC fasted
(n=65)
Patients with any drug-related AE, n (%) 12 (18%) 18 (28%)
Nausea 10 (15%) 18 (28%)
Headache 2 (3%) 4 (6%)
Abdominal pain 0 1 (2%)
Vomiting 1 (2%) 0
Dizziness 1 (2%) 0
Feeling hot 0 1 (2%)
Adapted from Weller S et al. JAIDS 2014;66:393-8
Bioequivalence was demonstrated between TRIUMEQ as a single pill and the
separate co-administered tablet formulations of DTG + ABC/3TC
TRIUMEQ may be taken with or without food
Tolerability results (single-dose, healthy volunteers)
Part A: numerically fewer drug-related AEs with TRIUMEQ compared with separate
DTG + ABC/3TC (18% vs 28%, respectively)
Part B: no adverse events were reported
TRIUMEQ SINGLE PILL REGIMEN
BIOEQUIVALENCE: CONCLUSIONS
Weller S et al. JAIDS 2014;66:393-8; TRIUMEQ Summary of Product Characteristics. January 2017
TRIUMEQ is indicated for the treatment of HIV-infected adults and adolescents who:
are above 12 years of age, and
weigh at least 40 kg
TRIUMEQ is not recommended for use in patients with:
HLA-B*5701 allele
a creatinine clearance below 50 ml/min, or
moderate or severe hepatic impairment
TRIUMEQ is contraindicated:
in patients with hypersensitivity to dolutegravir, abacavir, lamivudine or to any of the
tablet excipients
for use with dofetilide* co-administration
TRIUMEQ INDICATION
TRIUMEQ Summary of Product Characteristics, January 2017
*Dofetilide is not licensed in the UK or Ireland
HLA / HYPERSENSITIVITY CONSIDERATIONS
Hypersensitivity reactions have been observed more commonly with abacavir, some of
which have been life-threatening, and in rare cases fatal, when not managed
appropriately. The risk for abacavir HSR to occur is high for patients who test positive for
the HLA‐B*5701 allele. However, abacavir HSRs have been reported at a low frequency
in patients who do not carry this allele.
Before initiating treatment with TRIUMEQ▼, screening for carriage of the HLA-B*5701
allele should be performed in any HIV-infected patient, irrespective of racial origin
TRIUMEQ should never be initiated in patients with a positive HLA-B*5701 status, nor in
patients with a negative HLA-B*5701 status who had a suspected abacavir HSR on a
previous abacavir-containing regimen
TRIUMEQ Summary of Product Characteristics, January 2017
TRIUMEQ▼: SPECIAL WARNINGS AND
PRECAUTIONS FOR USE
Liver disease
Patients with chronic hepatitis B or C
Immune Reactivation Syndrome
Mitochondrial dysfunction
Myocardial infarction
Weight and metabolic parameters
Osteonecrosis
Opportunistic infections
Drug resistance
Drug interactions
TRIUMEQ Summary of Product Characteristics, January 2017
3TC, lamivudine
ABC, abacavir
AE, adverse event
AUC, area under the curve
BE, bioequivalence
BID, twice daily
BMI, body mass index
CI, confidence interval
CL/F, Apparent total clearance of the drug
from plasma after oral administration
Cmax, maximum observed plasma
concentration
CNS, central nervous system
DRV, darunavir
DRV/r, darunavir/ritonavir
ABBREVIATIONS
DTG, dolutegravir
EFV, efavirenz
EVG, elvitegravir
FDC, fixed-dose combination
FTC, emtricitabine
GLS, geometric least squares
HIV, human immunodeficiency virus
INI, integrase inhibitor
NRTI, nucleoside reverse transcriptase inhibitor
PK, pharmacokinetic
QD, once daily
RAL, raltegravir
SD, standard deviation
TDF, tenofovir disoproxil fumarate
PRESCRIBING INFORMATION TRIUMEQ® ▼ (DOLUTEGRAVIR 50MG/ABACAVIR 600MG/LAMIVUDINE 300MG TABLETS)
(SEE SUMMARY OF PRODUCT CHARACTERISTICS BEFORE PRESCRIBING)
Indication: HIV in over 12 years and > 40kg. Screen for HLA-B*5701
prior to use. Do not use if HLA-B*5701 positive. Dose: one tablet once
daily with or without food. Elderly: Limited data in 65+ yrs. Creatinine
clearance <50ml/min or moderate/severe hepatic impairment: Not
recommended. Monitor closely in mild hepatic impairment.
Contraindications: Hypersensitivity to any ingredient. Co-administration
with dofetilide. Warnings/precautions: Both abacavir and dolutegravir
are associated with risk of hypersensitivity reactions (HSR). Do not
initiate in HLA-B*5701+ or previous suspected abacavir HSR. Stop
Triumeq without delay if HSR suspected. Never reintroduce any
dolutegravir- or abacavir-containing product after suspected HSR. Risks
of immune reactivation syndrome, osteonecrosis, increased weight,
lipids, glucose. Monitor LFTs in Hepatitis B/C co-infection. Inconclusive
data on relationship between abacavir and MI; minimise all modifiable CV
risk factors (e.g. smoking, hypertension, hyperlipidaemia). Not
recommended if dolutegravir required b.d. (with etravirine [without
boosted PI], efavirenz, nevirapine, rifampicin, boosted tipranavir,
carbamazepine, oxcarbazepine, phenytoin, phenobarbital and St John’s
Wort). Use with cladribine not recommended. Use
with Mg/Al-containing antacids, calcium, multivitamins or iron requires
dosage separation. Caution with metformin: monitor renal function and
consider metformin dose adjustment. Pregnancy/lactation: Not
recommended. Avoid breast-feeding. Side effects: See SPC for details.
Headache, insomnia, sleep/dream disorders, GI disturbance, fatigue,
hypersensitivity, anorexia, depression, dizziness, somnolence, lethargy,
malaise, cough, nasal symptoms, rash, pruritus, alopecia, arthralgia,
myalgia, asthenia, fever, elevations of ALT, AST and CPK, blood
dyscrasias, suicidal ideation or suicide attempt, rhabdomyolysis, lactic
acidosis, erythema multiforme, Stevens-Johnson syndrome, toxic
epidermal necrolysis. Basic NHS costs: 30 tablets: £798.16
EU/1/14/940/001. MA holder: ViiV Healthcare UK Ltd, 980 Great West
Road, Brentford, Middlesex TW8 9GS. Further information is available
from Customer Contact Centre, GlaxoSmithKline UK Ltd, Stockley Park
West, Uxbridge, Middlesex UB11 1BT.
S1A
Triumeq is a registered trademark of the ViiV Healthcare Group of
Companies.
Date of approval: January 2017 Zinc code: UK/TRIM/0037/14(7)
POM
Adverse events should be reported. For the UK, reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should
also be reported to GlaxoSmithKline on 0800 221 441.
Adverse events should be reported. For Ireland, adverse events should be reported directly to the HPRA; Freepost, Pharmacovigilance Section, Health
Products Regulatory Authority, Earlsfort Terrace, Dublin 2, Tel: +353 1 676 4971, [email protected]. Adverse events should also be reported to
GlaxoSmithKline on 1800 244 255.
PRESCRIBING INFORMATION TIVICAY® ▼ (DOLUTEGRAVIR 50MG TABLETS)
(SEE SUMMARY OF PRODUCT CHARACTERISTICS BEFORE PRESCRIBING)
Indication: HIV in >12 years and >40kg as part of combination
therapy. Dosing: 50mg once daily with or without food if no proven/
suspected integrase resistance. 50mg twice daily with efavirenz,
nevirapine, tipranavir/ritonavir, etravirine (without boosted PI),
carbamazepine, oxcarbazepine, phenytoin, phenobarbital, St John’s
Wort or rifampicin. Adults with proven/ suspected integrase resistance:
50mg twice daily preferably with food. Elderly: Limited data in 65+ yrs.
Caution in severe hepatic impairment. Contraindications:
Hypersensitivity to any ingredient. Co-administration with dofetilide.
Warnings/precautions: Risk of hypersensitivity reactions. Discontinue
dolutegravir and other suspect agents immediately if suspected. Risks
of osteonecrosis, immune reactivation syndrome. Monitor LFTs in
Hepatitis B/C co-infection and ensure effective Hepatitis B therapy.
Caution with metformin: monitor renal function and consider metformin
dose adjustment. Use with etravirine requires boosted PI or increased
dose of dolutegravir. Use with Mg/Al-containing antacids, calcium,
multivitamins or iron requires dosage separation.
Pregnancy/ lactation: Not recommended. Avoid breast-feeding. Side
effects: See SPC for full details. Headache, GI disturbance, insomnia,
abnormal dreams, depression, dizziness, rash, pruritus, fatigue,
elevations of ALT, AST and CPK, arthralgia, myalgia, hypersensitivity,
suicidal ideation or suicide attempt. Basic NHS costs: 30 tablets
£498.75 EU/1/13/892/001. MA holder: ViiV Healthcare UK Ltd, 980
Great West Road, Brentford, Middlesex TW8 9GS. Further information
available from Customer Contact Centre, GlaxoSmithKline UK Ltd,
Stockley Park West, Uxbridge, Middlesex UB11 1BT.
Tivicay is a registered trademark of the ViiV Healthcare Group of
Companies
Date of approval: January 2017. Zinc code: UK/DLG/0055/13(9)
POM
Adverse events should be reported. For the UK, reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events
should also be reported to GlaxoSmithKline on 0800 221 441.
Adverse events should be reported. For Ireland, adverse events should be reported directly to the HPRA; Freepost, Pharmacovigilance Section,
Health Products Regulatory Authority, Earlsfort Terrace, Dublin 2, Tel: +353 1 676 4971, [email protected]. Adverse events should also be
reported to GlaxoSmithKline on 1800 244 255.
S1A
PRESCRIBING INFORMATION
KIVEXA ® (ABACAVIR 600MG/LAMIVUDINE 300MG TABLETS)
(SEE SUMMARY OF PRODUCT CHARACTERISTICS BEFORE PRESCRIBING)
Indications: HIV in adults, adolescents and children weighing at
least 25 kg as part of combination therapy. Screen for HLA-
B*5701 prior to use. Dose: one tablet daily with or without food.
Elderly: No pharmacokinetic data in 65+ yrs. Renal impairment:
Creatinine clearance <50ml/min: not recommended. Hepatic
impairment: not recommended in moderate or severe hepatic
impairment. Monitor closely in mild hepatic impairment.
Contraindications: Hypersensitivity to any ingredient.
Warnings/precautions: Risk of hypersensitivity reactions (HSR).
Do not initiate in HLA-B*5701+ or previous suspected abacavir
HSR. Stop Kivexa without delay if HSR suspected. Never re-
introduce any abacavir-containing product after suspected HSR.
Risks of virological failure, immune reactivation syndrome,
osteonecrosis, increased weight, lipids, glucose. Monitor LFTs in
Hepatitis B/C co-infection. Inconclusive data on relationship
between abacavir and MI; minimise modifiable CV risk factors
(e.g. smoking, hypertension, hyperlipidaemia). Use with cladribine,
emtricitabine or high doses of co-trimoxazole
not recommended. Pregnancy/lactation: Not recommended. Avoid
breast-feeding. Side effects: See SPC for full details.
Hypersensitivity, GI disturbance, headache, anorexia, insomnia,
rash, fever, lethargy, fatigue, malaise, arthralgia, muscle disorders,
nasal symptoms, cough, alopecia, blood dyscrasias,
rhabdomyolysis, lactic acidosis, erythema multiforme, Stevens-
Johnson syndrome and toxic epidermal necrolysis. Basic NHS
costs: 30 tablets: £299.41 EU/1/04/298/002. MA holder: ViiV
Healthcare UK Ltd, 980 Great West Road, Brentford, Middlesex
TW8 9GS. Further information is available from Customer Contact
Centre, GlaxoSmithKline UK Ltd, Stockley Park West, Uxbridge,
Middlesex UB11 1BT.
Kivexa is a registered trademark of the ViiV Healthcare Group of
Companies
Date of approval: October 2016 Zinc code: UK/ABC3TC/0008/13(9)
POM
Adverse events should be reported. For the UK, reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events
should also be reported to GlaxoSmithKline on 0800 221 441.
Adverse events should be reported. For Ireland, adverse events should be reported directly to the HPRA; Freepost, Pharmacovigilance Section,
Health Products Regulatory Authority, Earlsfort Terrace, Dublin 2, Tel: +353 1 676 4971, [email protected]. Adverse events should also be
reported to GlaxoSmithKline on 1800 244 255.
S1A