nuevos fármacos antiretrovirales - fls-science.com · dtg and abc/3tc jean-michel molina, 1...
TRANSCRIPT
Nuevos fármacos
antiretrovirales
Pere Domingo
Malalties Infeccioses
Hospital de la Santa Creu i Sant Pau
Institut del Recerca del HSCSP
Universitat Autonòma de Barcelona


Vacas flacas/lineales
INsTI
Bictegravir switch (Study 380-1844 ) #A022
Bictegravir swicth women (#500)
Bictegravir in adolescents (#844)
ITINAN
Switch a RPV/F/TAF (#504)
Doravirina, Drive-Ahead (#491)
ITIAN
EFdA (MK-8591)(#26, #89LB)
Anticuerpos monoclonales
Ibalizumab (# 561)
ARVs long acting
Implante SC (TAF, #486)
Nanoformulados
MVC, #48, #483
FTC, #484
CBV+RPV, #485
DRV/r, #480
3D (LPV, EFV, TFV) #487
4D (LPV/r, 3TC, TFV) #488
Vacas flacas/lineales
INsTI
Bictegravir switch (Study 380-1844 ) #A022
Bictegravir swicth women (#500)
Bictegravir in adolescents (#844)
ITINAN
Switch a RPV/F/TAF (#504)
Doravirina, Drive-Ahead (#491)
ITIAN
EFdA (MK-8591)(#26, #89LB)
Anticuerpos monoclonales
Ibalizumab (# 561)
ARVs long acting
Implante SC (TAF, #486)
Nanoformulados
MVC, #48, #483
FTC, #484
CBV+RPV, #485
DRV/r, #480
3D (LPV, EFV, TFV) #487
4D (LPV/r, 3TC, TFV) #488
Switch to Bictegravir/F/TAF From DTG and ABC/3TC
Jean-Michel Molina,1 Douglas Ward,2 Indira Brar,3 Anthony Mills,4 Hans Jürgen Stellbrink,5 Luis
López-Cortés,6 Peter Ruane,7 Daniel Podzamczer,8 Cynthia Brinson,9 Joseph Custodio,10 Hui Liu,10
Kristen Andreatta,10 Hal Martin,10 Andrew Cheng,10 Erin Quirk10
1Hôpital Saint Louis, Paris, France; 2Dupont Circle Physicians, Washington DC; 3Henry Ford Hospital, Detroit, MI; 4Southern
California Men’s Medical Group, Los Angeles, CA; 5ICH Study Center, Hamburg, Germany; 6Unidad Clínica de Enfermedades
Infecciosas, Microbiología y Medicina Preventiva, Hospital Universitario Virgen del Rocío/Instituto de Biomedicina de Sevilla,
Spain; 7Peter J. Ruane, MD Inc., Los Angeles, CA; 8Hospital Universitari de Bellvitge, Barcelona, Spain; 9Central Texas Clinical
Research, Austin, TX; 10Gilead Sciences, Inc., Foster City, CA
CROI 2018, Abstract 022 March 4–7, 2018 Boston, MA
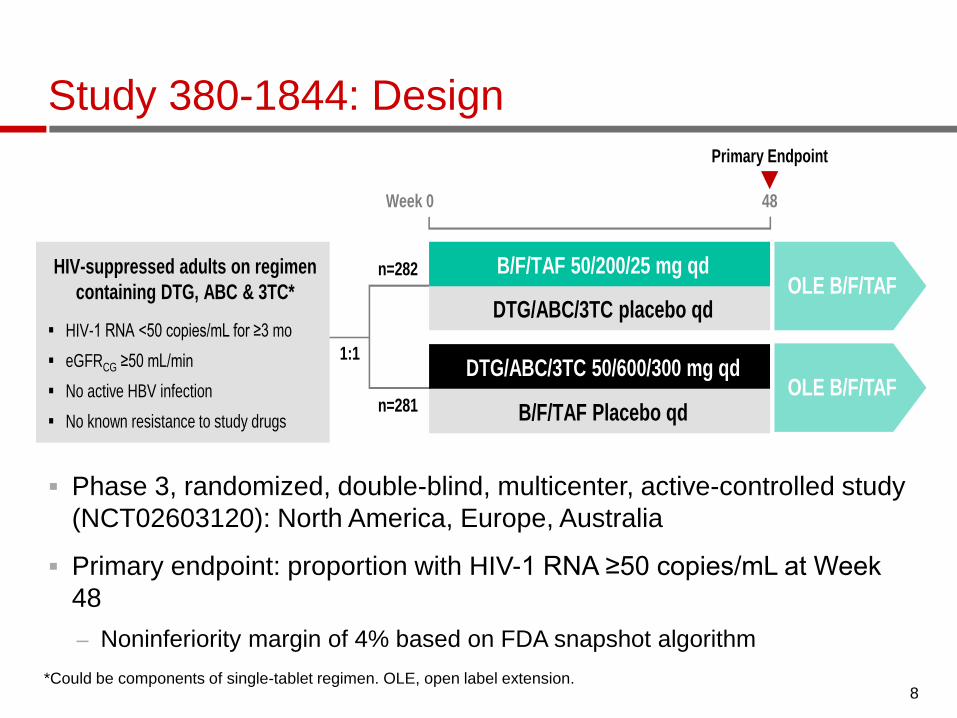
Study 380-1844: Design
Phase 3, randomized, double-blind, multicenter, active-controlled study
(NCT02603120): North America, Europe, Australia
Primary endpoint: proportion with HIV-1 RNA ≥50 copies/mL at Week
48
– Noninferiority margin of 4% based on FDA snapshot algorithm
8 *Could be components of single-tablet regimen. OLE, open label extension.
Week 0 48
HIV-suppressed adults on regimen
containing DTG, ABC & 3TC*
HIV-1 RNA <50 copies/mL for ≥3 mo
eGFRCG ≥50 mL/min
No active HBV infection
No known resistance to study drugs
DTG/ABC/3TC placebo qd
B/F/TAF 50/200/25 mg qd
B/F/TAF Placebo qd
DTG/ABC/3TC 50/600/300 mg qd
n=282
n=281
Primary Endpoint
1:1
OLE B/F/TAF
OLE B/F/TAF

Baseline Characteristics Study 380-1844
B/F/TAF
n=282
DTG/ABC/3TC
n=281
Median age, years (range) 47 (21-71) 45 (20-70)
Male, % 88 90
Race, %
White 73 73
Black or African descent 21 22
Hispanic/Latino Ethnicity, % 16 19
Median CD4 cell count, cells/µL
(IQR) 732 (554,936) 661 (478,874)
Median eGFRCG, mL/min (IQR) 101(84,119) 101(85,122)
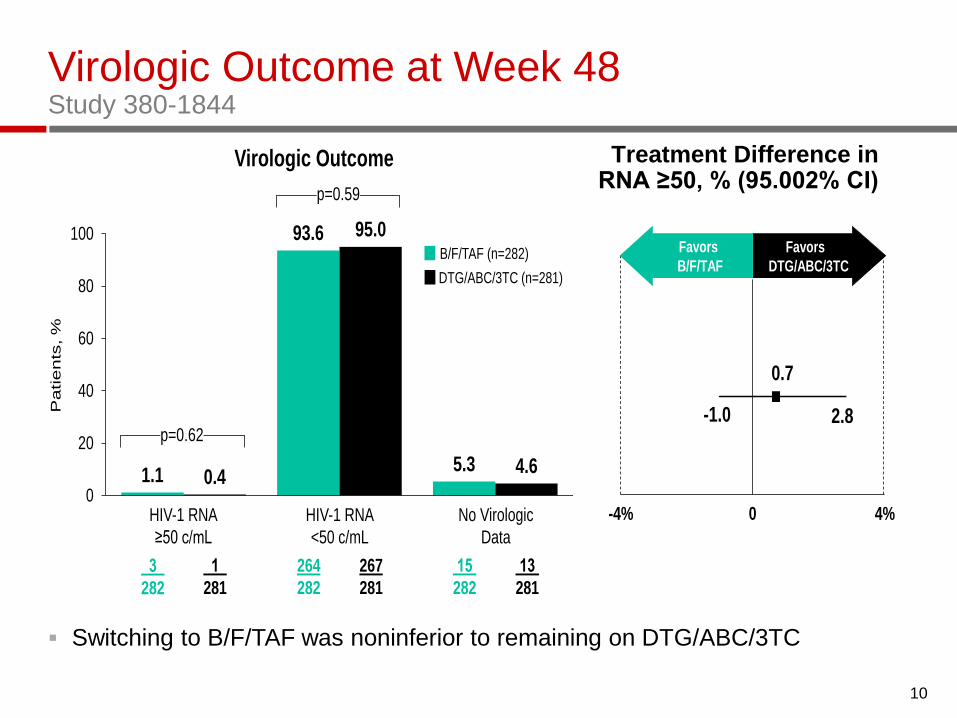
Virologic Outcome at Week 48 Study 380-1844
Switching to B/F/TAF was noninferior to remaining on DTG/ABC/3TC
10
Treatment Difference in RNA ≥50, % (95.002% CI)
-1.0 2.8
0.7
-4% 4%0
Favors
B/F/TAF
Favors
DTG/ABC/3TC
1.1
93.6
5.30.4
95.0
4.6
0
20
40
60
80
100
HIV-1 RNA
<50 c/mL
HIV-1 RNA
≥50 c/mL
No Virologic
Data
3
282
1
281
264
282
267
281
13
281
15
282
DTG/ABC/3TC (n=281)
B/F/TAF (n=282)
Virologic Outcome
Pa
tie
nts
, %
p=0.59
p=0.62

Virologic Outcome at Week 48 Study 380-1844
Switching to B/F/TAF was noninferior to remaining on DTG/ABC/3TC
No participant developed treatment-emergent resistance
11
Treatment Difference in RNA ≥50, % (95.002% CI)
-1.0 2.8
0.7
-4% 4%0
Favors
B/F/TAF
Favors
DTG/ABC/3TC
1.1
93.6
5.30.4
95.0
4.6
0
20
40
60
80
100
HIV-1 RNA
<50 c/mL
HIV-1 RNA
≥50 c/mL
No Virologic
Data
3
282
1
281
264
282
267
281
13
281
15
282
DTG/ABC/3TC (n=281)
B/F/TAF (n=282)
Virologic Outcome
Pa
tie
nts
, %
p=0.59
p=0.62
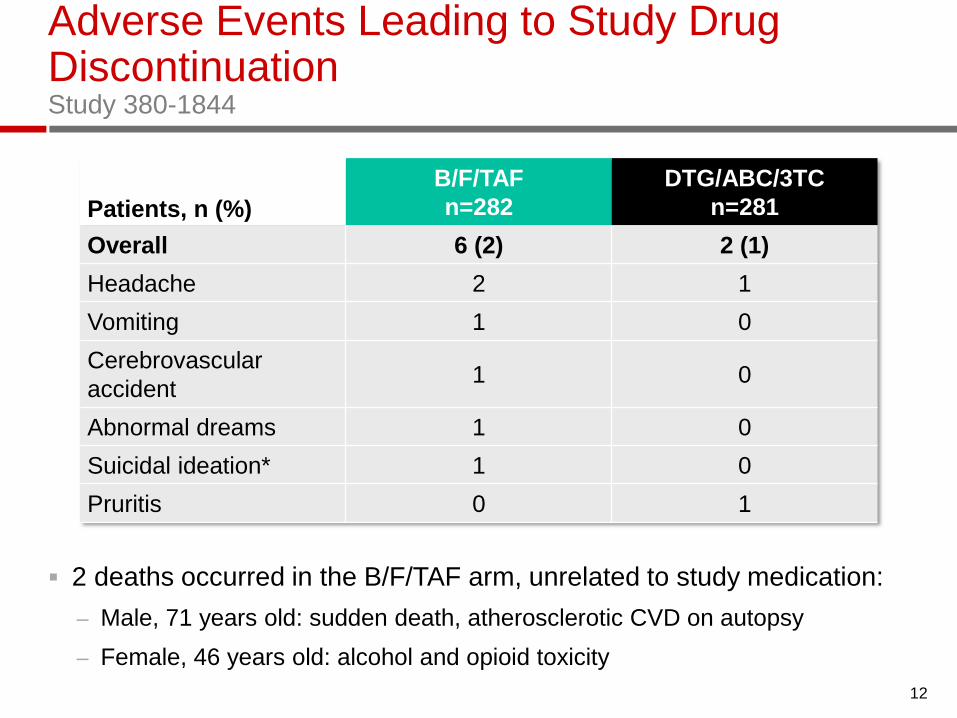
Adverse Events Leading to Study Drug Discontinuation Study 380-1844
2 deaths occurred in the B/F/TAF arm, unrelated to study medication:
– Male, 71 years old: sudden death, atherosclerotic CVD on autopsy
– Female, 46 years old: alcohol and opioid toxicity
12
*Not considered related to study treatment by investigator.
Patients, n (%)
B/F/TAF
n=282
DTG/ABC/3TC
n=281
Overall 6 (2) 2 (1)
Headache 2 1
Vomiting 1 0
Cerebrovascular
accident 1 0
Abnormal dreams 1 0
Suicidal ideation* 1 0
Pruritis 0 1

Most Common Adverse Events Through Week 48 Study 380-1844
Patients, n (%)
B/F/TAF
n=282
DTG/ABC/3T
C
n=281
Any AE (all grades) 225 (79.8) 225 (80.1)
AEs occurring in ≥5% of patients
Upper respiratory tract infection 29 (10) 27 (10)
Nasopharyngitis 20 (7) 22 (8)
Headache 19 (7) 21 (7)
Diarrhea 24 (9) 14 (5)
Arthralgia 19 (7) 10 (4)
Insomnia 8 (3) 14 (5)
13

Study Drug-Related AEs Through Week 48 Study 380-1844
14
All Grades
B/F/TAF
n=282
DTG/ABC/3
TC
n=281 p-Value
Any study drug-related AE,
n (%) 23 (8) 44 (16) 0.01
Study drug-related AE in
≥1%, n (%)
Headache 7 (3) 8 (3)
Abnormal dreams 1 (<1) 5 (2)
Flatulence 0 5 (2)
Nausea 0 5 (2)
Diarrhea 2 (<1) 4 (1)
Fatigue 1 (<1) 3 (1)
Insomnia 0 3 (1)
p-value from Fisher exact test
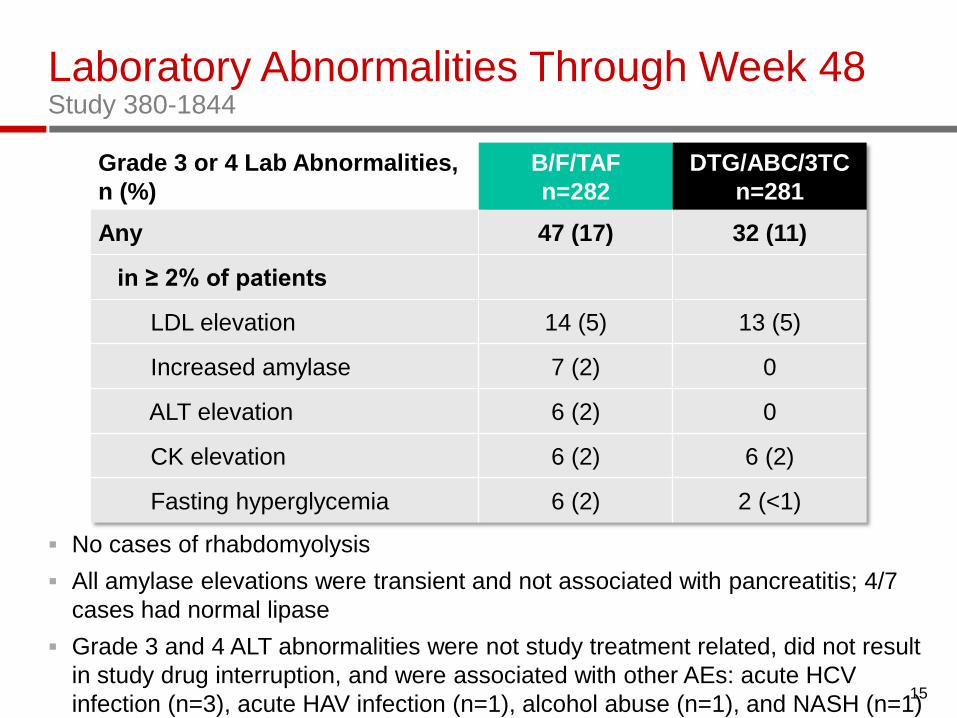
Laboratory Abnormalities Through Week 48 Study 380-1844
No cases of rhabdomyolysis
All amylase elevations were transient and not associated with pancreatitis; 4/7
cases had normal lipase
Grade 3 and 4 ALT abnormalities were not study treatment related, did not result
in study drug interruption, and were associated with other AEs: acute HCV
infection (n=3), acute HAV infection (n=1), alcohol abuse (n=1), and NASH (n=1) 15
Grade 3 or 4 Lab Abnormalities,
n (%)
B/F/TAF
n=282
DTG/ABC/3TC
n=281
Any 47 (17) 32 (11)
in ≥ 2% of patients
LDL elevation 14 (5) 13 (5)
Increased amylase 7 (2) 0
ALT elevation 6 (2) 0
CK elevation 6 (2) 6 (2)
Fasting hyperglycemia 6 (2) 2 (<1)

Change in eGFRCG Over Time Study 380-1844
No discontinuations due to renal AEs and no cases of renal tubulopathy in
either arm 16 *From 2-sided Wilcoxon rank-sum test.
1.0 mL/min
-1.8 mL/min
p <0.001*
Me
dia
n C
ha
ng
e F
rom
Ba
se
lin
e e
GF
RC
G,
mL
/min
(Q
1, Q
3)
Week
0
1 0
2 0
- 1 0
- 2 0
B / F / T A F
0 4 8 1 2 2 4 3 6 4 8
A B C / D T G / 3 T CB/F/TAF DTG/ABC/3TC

Changes in Quantitative Proteinuria at Week 48 Study 380-1844
17 *From 2-sided Wilcoxon rank-sum test for % change from baseline at Week 48 for each marker for treatment comparison.
14 20 21
9
29
17
-50
-25
0
25
50
75
100
-34
β2-microglobulin:CreatinineRetinol-Binding
Protein:Creatinine
Me
dia
n %
Ch
an
ge
Fro
m B
ase
lin
e (
Q1
, Q
3)
Albumin:Creatinine
B/F/TAF
DTG/ABC/3TC
6372
-6
-19-22 -20
66
-7
p=0.74*
Baseline 5.6 mg/g 5.4 mg/g
p=0.31* p=0.53*
8496
75
99 μg/g 96 μg/g 75 μg/g 77 μg/g

Changes in Spine and Hip BMD Through Week 48 Study 380-1844
18 *From ANOVA model for comparison of B/F/TAF vs DTG/ABC/3TC at Week 48.
B/F/TAF n=256
DTG/ABC/3TC n=262
244
253
233
244
256
265
246
253
229
242
-1
1
2
-2
0
0.30
0.16
0.69
0.42
HipSpine
-1
1
2
-2
0
Me
an
% C
ha
ng
e
Fro
m B
ase
lin
e(9
5%
CI)
WeekWeek
24 48 24 480 0
p=0.33*
p=0.47*
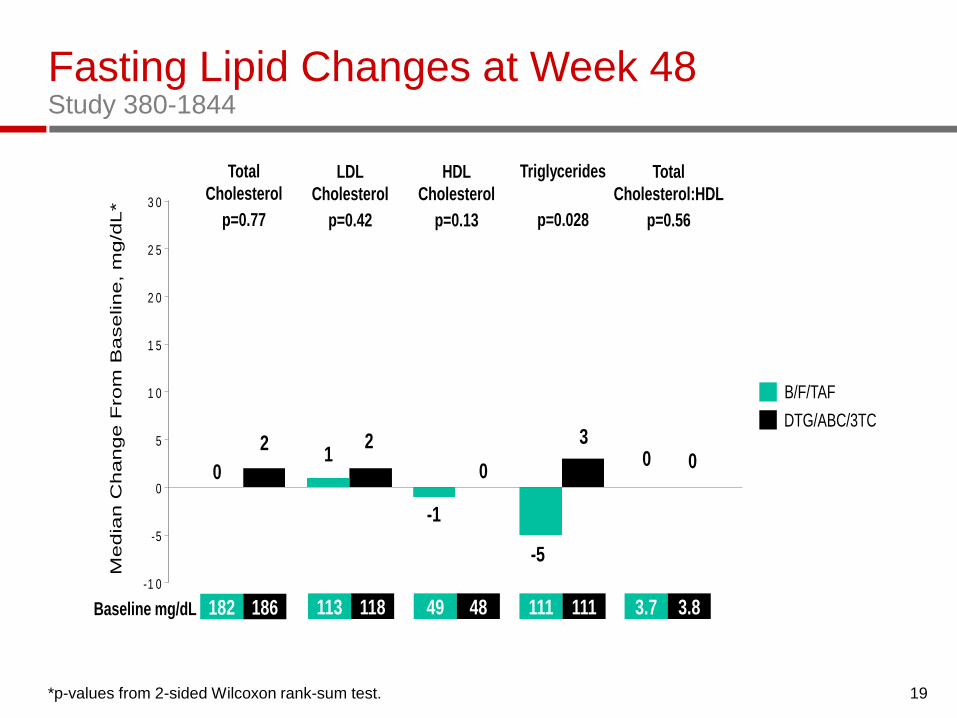
Fasting Lipid Changes at Week 48 Study 380-1844
19 *p-values from 2-sided Wilcoxon rank-sum test.
-1 0
-5
0
5
1 0
1 5
2 0
2 5
3 0
0
21
2
-1
-5
3
Total
Cholesterol
LDL
Cholesterol
TriglyceridesHDL
Cholesterol
B/F/TAF
DTG/ABC/3TC
113 118 49 48 111 111Baseline mg/dL 182 186
Media
n C
hange F
rom
Baseline, m
g/d
L*
0
p=0.77 p=0.42 p=0.13 p=0.028
3.7 3.8
0 0
Total
Cholesterol:HDL
p=0.56

Study 380-1844 Conclusions
Switching to B/F/TAF was non-inferior to remaining on
DTG/ABC/3TC
No treatment emergent resistance was observed in
either arm
B/F/TAF was well tolerated
– Adverse events were comparable between arms at Week
48
The lipid, bone and renal safety profiles of switching to
B/F/TAF were comparable to remaining on
DTG/ABC/3TC through 48 weeks of treatment
B/F/TAF offers an effective and safe alternative to
DTG/ABC/3TC
Study 380-1961: Switching to B/F/TAF in women (Kityo
et al. Poster 500)
20

Switching to B/E/TAF in Women
Kytio C, et al. #500

Disposition
Kytio C, et al. #500

Baseline characteristics
Kytio C, et al. #500
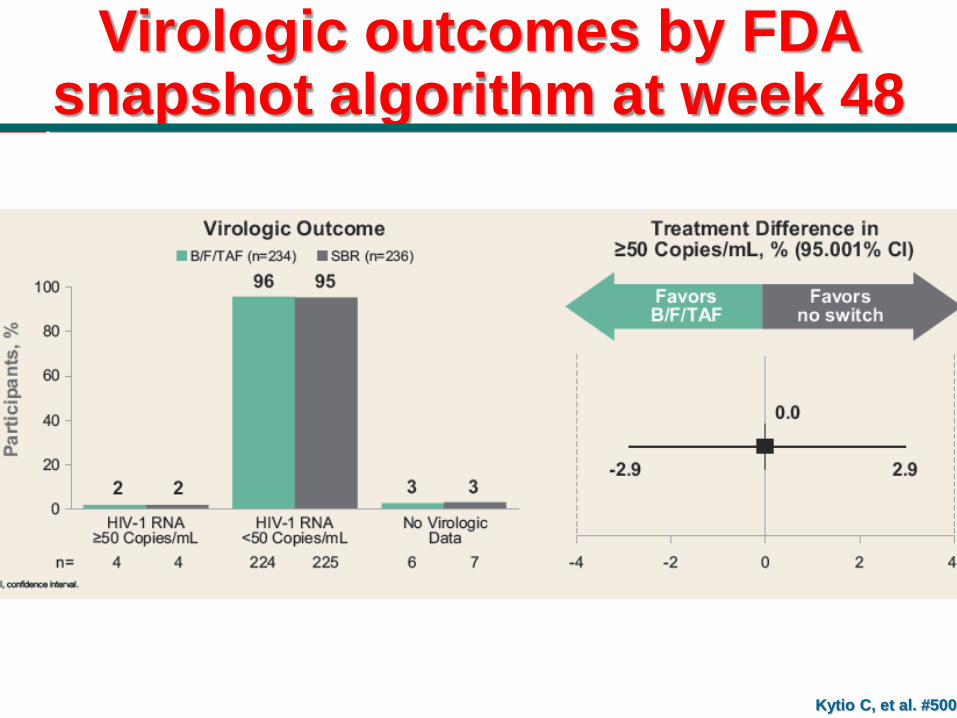
Virologic outcomes by FDA snapshot algorithm at week 48
Kytio C, et al. #500
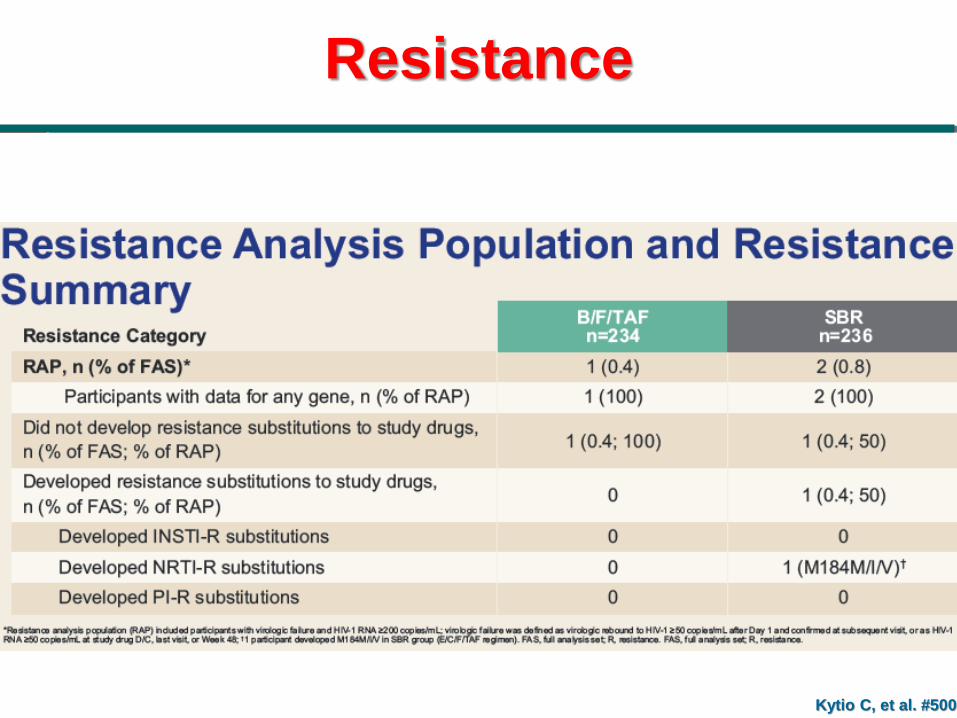
Resistance
Kytio C, et al. #500
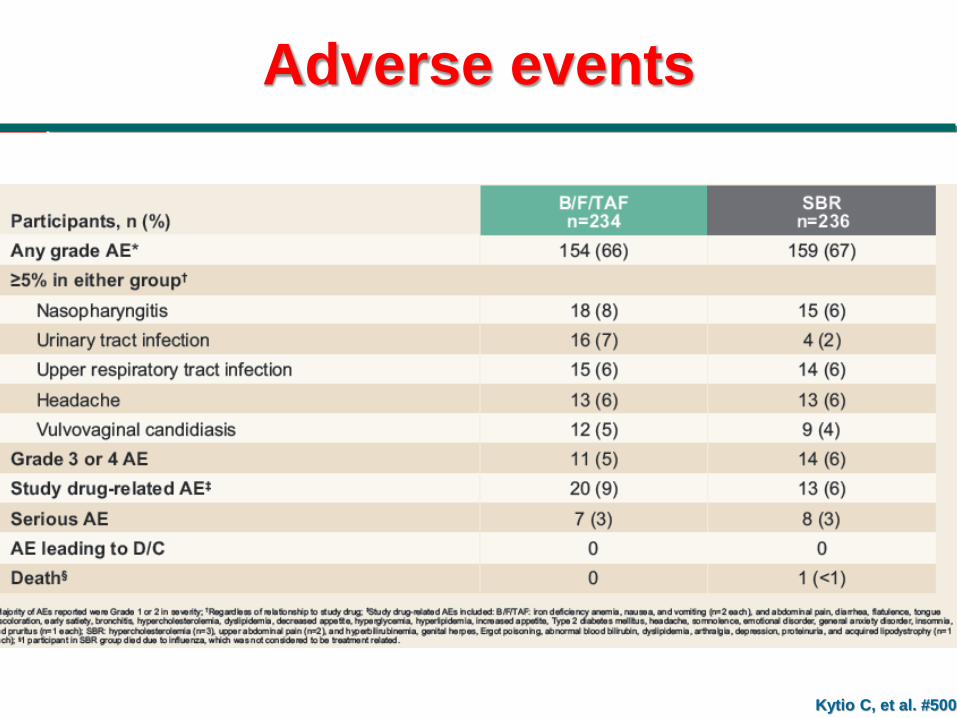
Adverse events
Kytio C, et al. #500
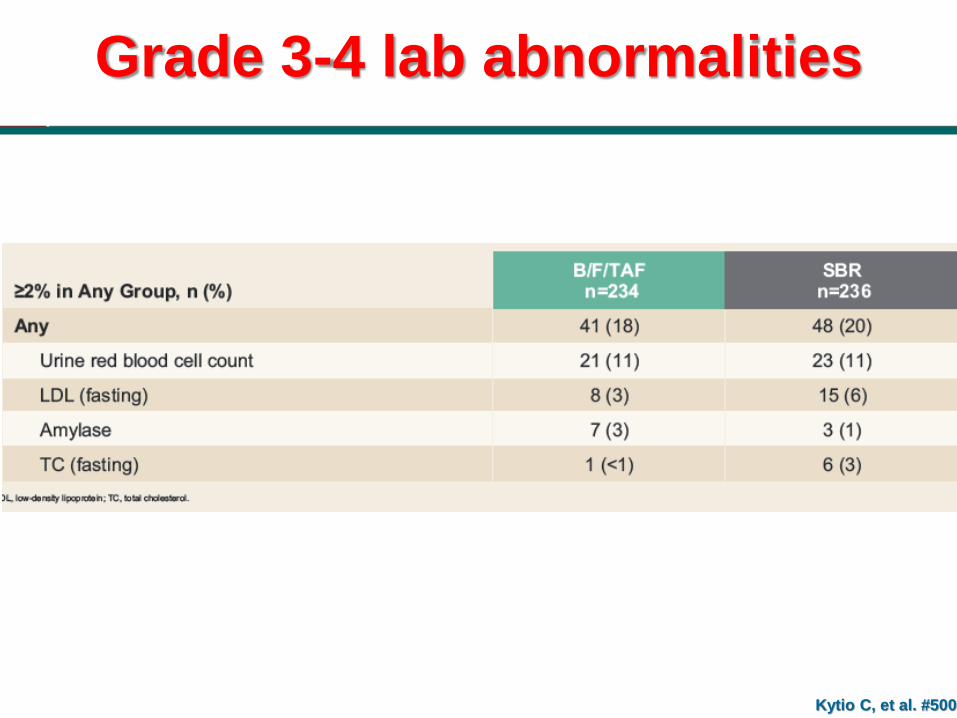
Grade 3-4 lab abnormalities
Kytio C, et al. #500
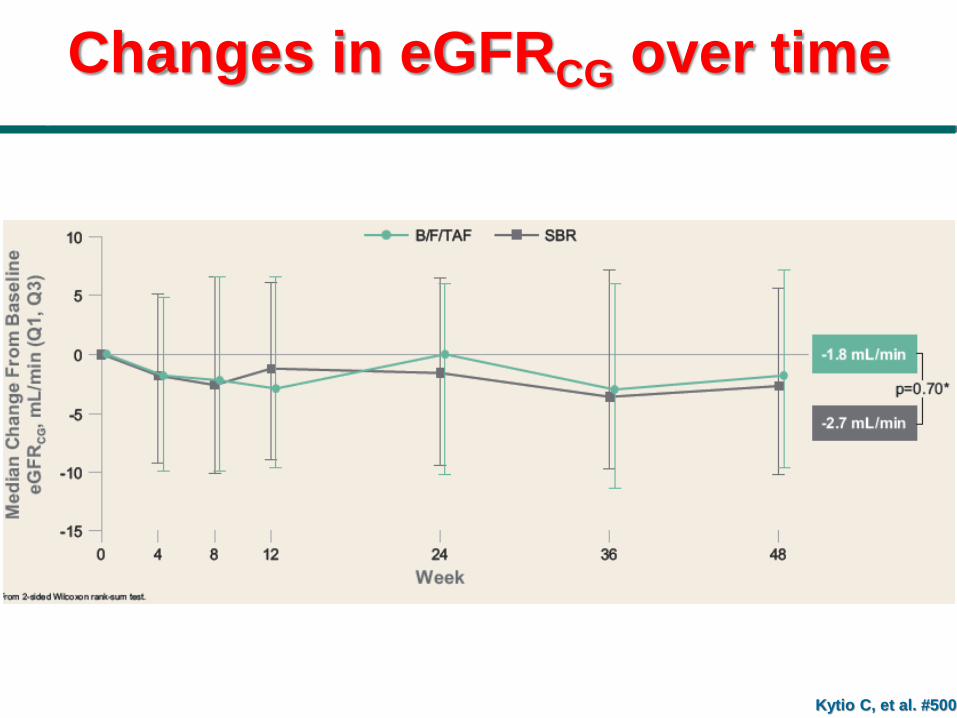
Changes in eGFRCG over time
Kytio C, et al. #500

Changes in quantitative proteinuria at week 48 by prior regimen
Kytio C, et al. #500
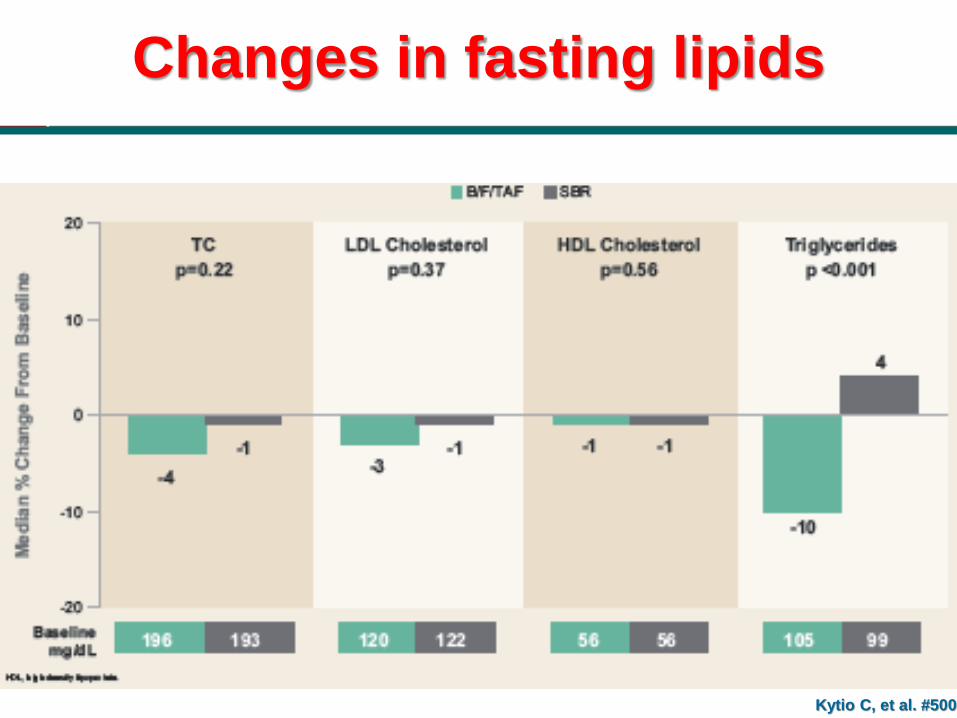
Changes in fasting lipids
Kytio C, et al. #500

Conclusions
Kytio C, et al. #500
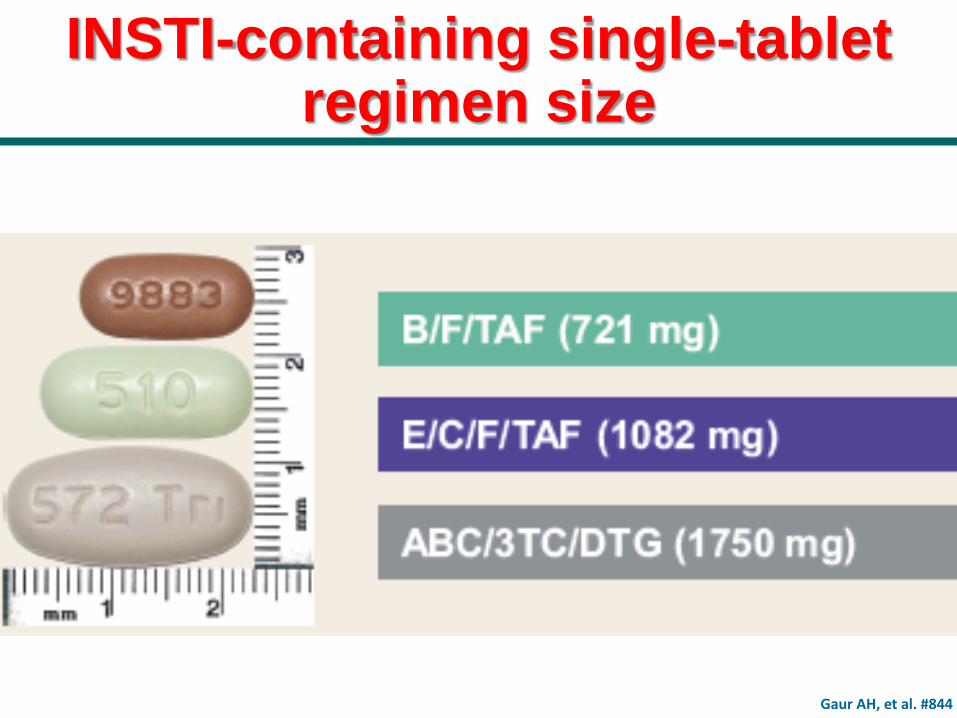
INSTI-containing single-tablet regimen size
Gaur AH, et al. #844

Similar Efficacy and Safety By
Subgroup in DRIVE-AHEAD: DOR/3TC/TDF vs EFV/FTC/TDF
Orkin C, et al. #491
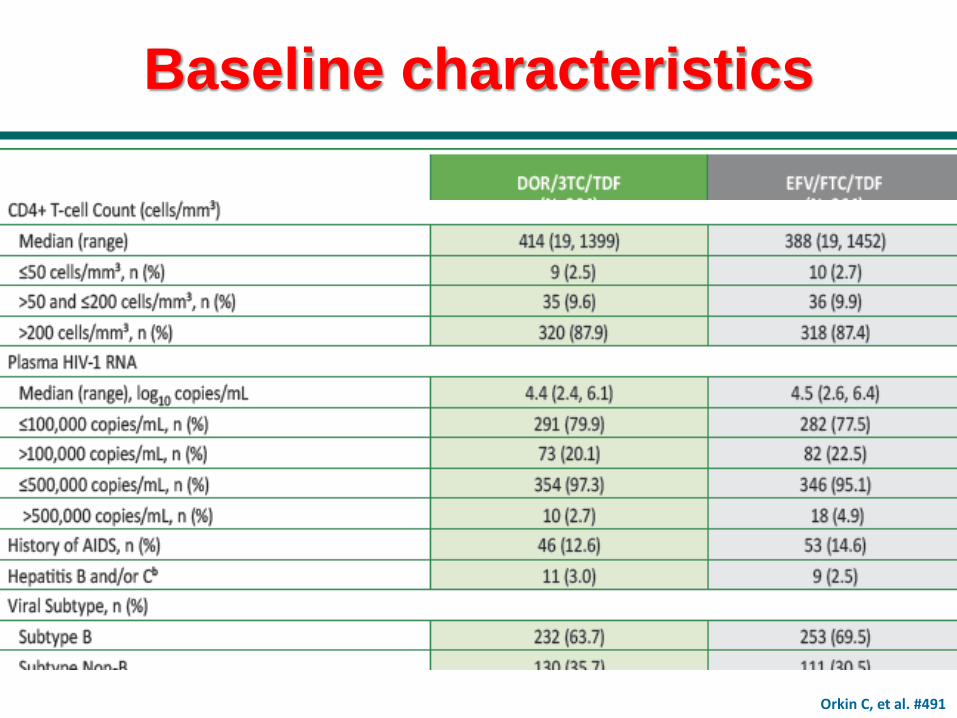
Baseline characteristics
Orkin C, et al. #491
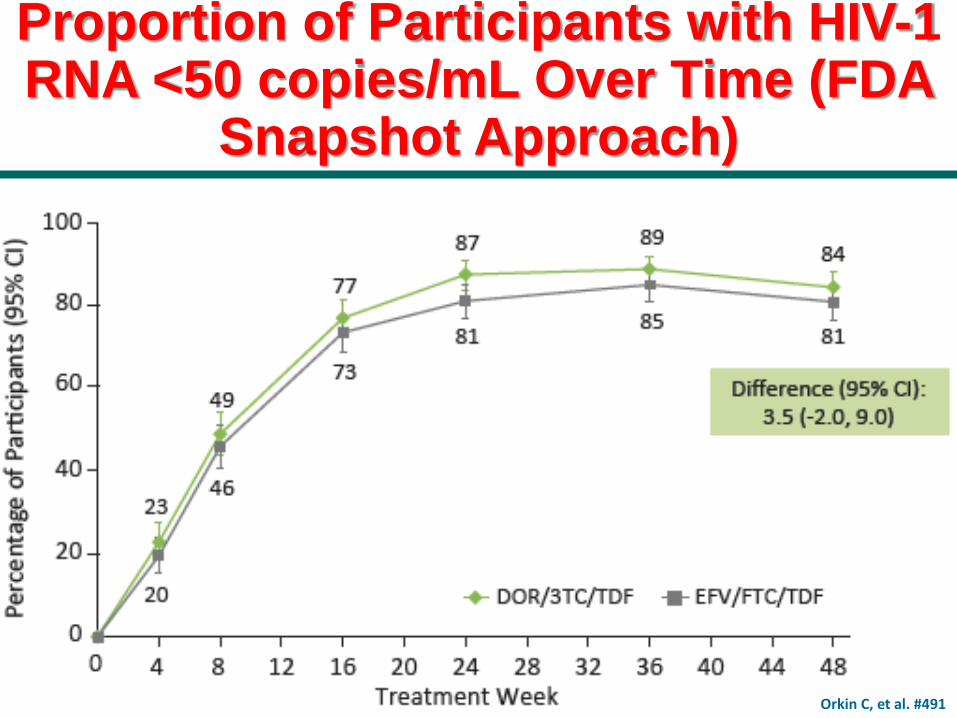
Proportion of Participants with HIV-1 RNA <50 copies/mL Over Time (FDA
Snapshot Approach)
Orkin C, et al. #491
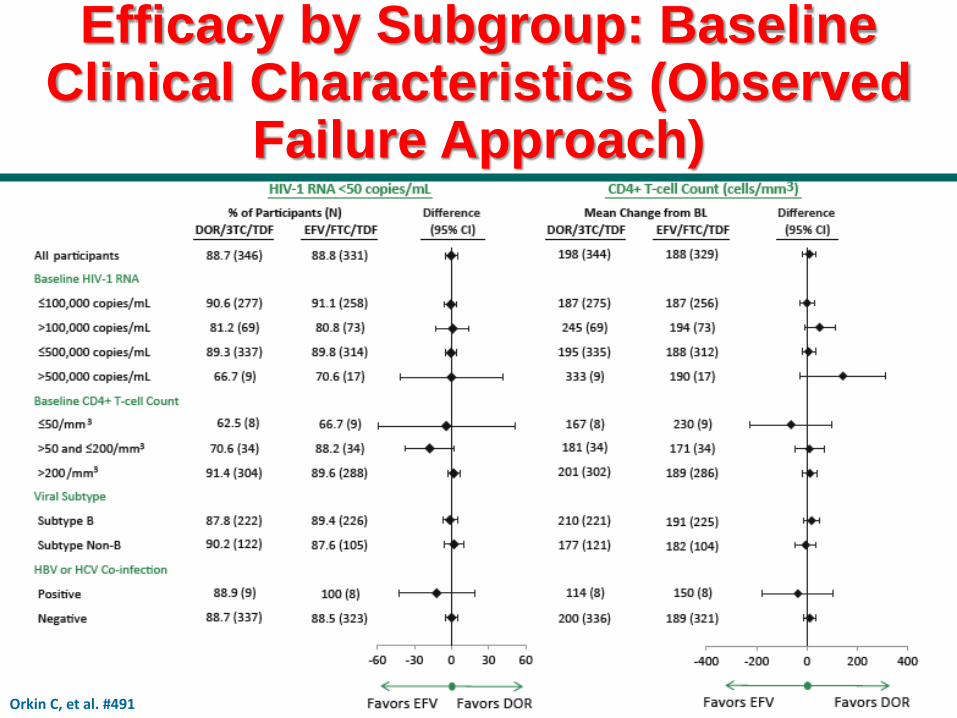
Efficacy by Subgroup: Baseline Clinical Characteristics (Observed
Failure Approach)
Orkin C, et al. #491

Efficacy by Subgroup: Demographic Factors (Observed Failure Approach)
Orkin C, et al. #491

Clinical Adverse Events (%) by Gender
Orkin C, et al. #491

Clinical Adverse Events (%) by Race/Ethnicity
Orkin C, et al. #491

Clinical Adverse Events (%) by Baseline CD4+ T-cell Count
Orkin C, et al. #491

Conclusions
Orkin C, et al. #491

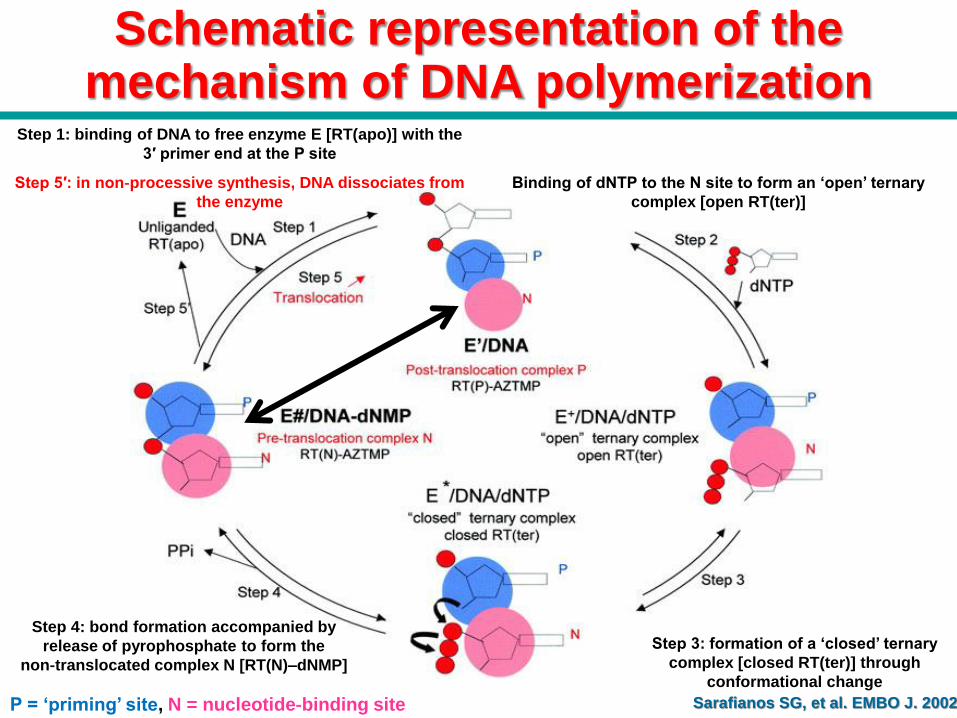
Schematic representation of the mechanism of DNA polymerization
Sarafianos SG, et al. EMBO J. 2002
Step 1: Binding of DNA to free enzyme E [RT(apo)] with the
3′ primer end at the P site
Binding of dNTP to the N site to form an ‘open’ ternary
complex [open RT(ter)]
Formation of a ‘closed’ ternary complex
[closed RT(ter)] through conformational
change
Bond formation accompanied by release of
pyrophosphate to form the non‐translocated
complex N [RT(N)–dNMP]
Step 5: in processive synthesis, the primer translocates
from the N site to the P site
P = ‘priming’ site, N = nucleotide‐binding site

Schematic representation of the mechanism of DNA polymerization
Chain terminator
Sarafianos SG, et al. EMBO J. 2002
Step 1: binding of DNA to free enzyme E [RT(apo)] with the
3′ primer end at the P site
Binding of dNTP to the N site to form an ‘open’ ternary
complex [open RT(ter)]
Formation of a ‘closed’ ternary complex
[closed RT(ter)] through conformational
change
Bond formation accompanied by release of
pyrophosphate to form the non‐translocated
complex N [RT(N)–dNMP]
Step 5: in processive synthesis, the primer translocates
from the N site to the P site
P = ‘priming’ site, N = nucleotide‐binding site
Schematic representation of the mechanism of DNA polymerization
Sarafianos SG, et al. EMBO J. 2002
Step 1: binding of DNA to free enzyme E [RT(apo)] with the
3′ primer end at the P site
Binding of dNTP to the N site to form an ‘open’ ternary
complex [open RT(ter)]
Step 3: formation of a ‘closed’ ternary
complex [closed RT(ter)] through
conformational change
Step 4: bond formation accompanied by
release of pyrophosphate to form the
non‐translocated complex N [RT(N)–dNMP]
Step 5′: in non‐processive synthesis, DNA dissociates from
the enzyme
P = ‘priming’ site, N = nucleotide‐binding site

Multiple Daily Doses of MK-8591 as Low as 0.25 mg Are Expected to
Suppress HIV
Randolph P. Matthews1; Deanne Jackson Rudd1; Vanessa Lev'ine1; Sandra Zhang1; Laura Sterling2; Jay A. Grobler1; Ryan Vargo1; S. Aubrey Stoch1; Mar'ian
lwamoto1

MK-8591 (4'-Ethynyl-2-Fluoro-2'-Deoxyadenosine, EFdA)

MK-8591 Demonstrates PK Suitable for Multiple Dosing Regimens and Has High
Antiviral Potency

Use of MK-8591 as a daily antiretroviral

MK-8591 PN009: Multiple daily Dose Study
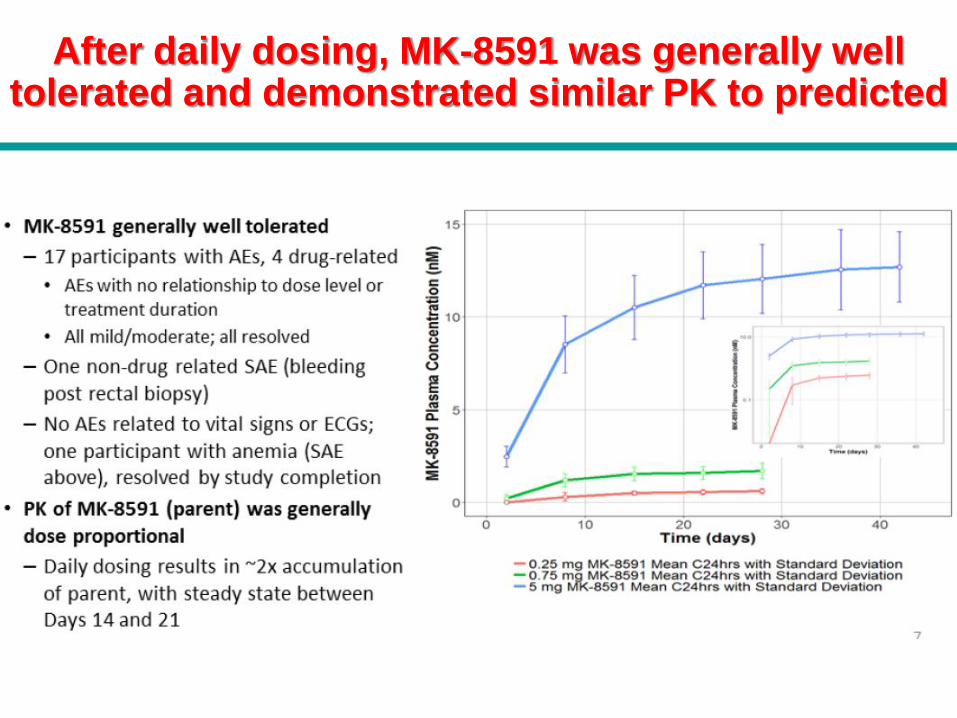
After daily dosing, MK-8591 was generally well tolerated and demonstrated similar PK to predicted

MK-8591-TP achieves PK target on day 1 at 8,25 mg

MK-8591-TP QD PK in healthy adults
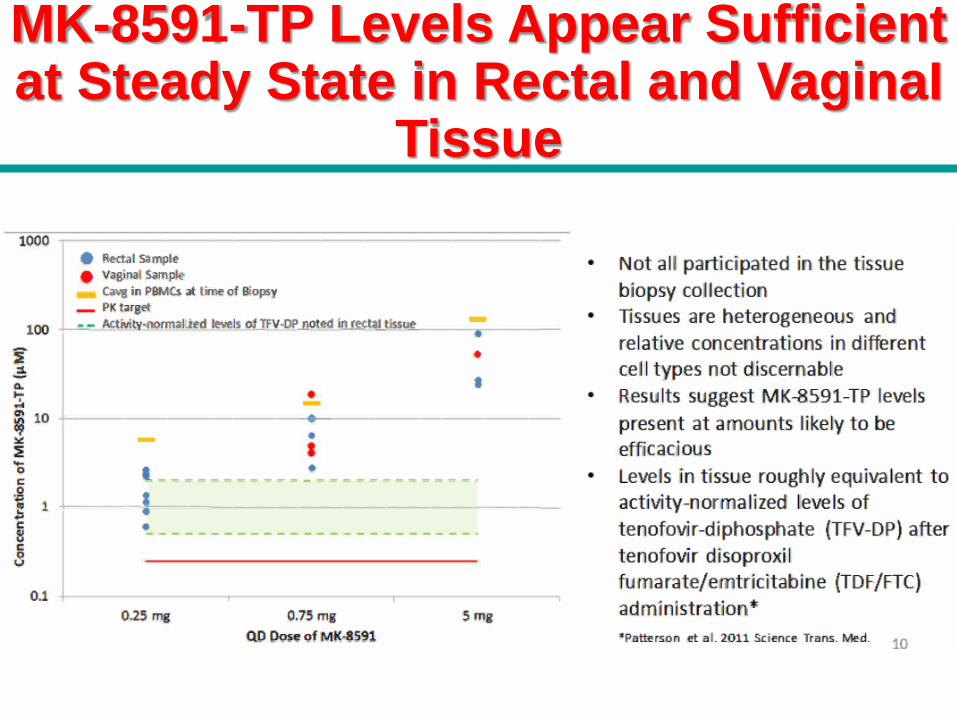
MK-8591-TP Levels Appear Sufficient at Steady State in Rectal and VaginaI
Tissue

Conclusions

LOW DOSE MK-8591 PROTECTS RHESUS MACAQUES AGAINST
RECTAL SHIV INFECTION

Rhesus macaques treated with 3.9 mg/kg MK-859I weekly and challenged intrarectally with low dose SHIV 109CP3 weekly were completely protected

Protection against infection
“The intelligent people are
full of doubt, while the
stupid are full of
confidence”
Charles Bukowski
(1888-1959)