trends in smoking-related cancer incidence in tarragona, spain, 1980-96
TRANSCRIPT
Trends in Smoking-Related Cancer Incidence in Tarragona, Spain, 1980-96Author(s): Joan Borràs, Josep M. Borràs, Jaume Galceran, Victoria Sánchez, Víctor Morenoand Juan Ramón GonzálezSource: Cancer Causes & Control, Vol. 12, No. 10 (Dec., 2001), pp. 903-908Published by: SpringerStable URL: http://www.jstor.org/stable/3553835 .
Accessed: 15/06/2014 18:16
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
Springer is collaborating with JSTOR to digitize, preserve and extend access to Cancer Causes &Control.
http://www.jstor.org
This content downloaded from 185.2.32.106 on Sun, 15 Jun 2014 18:16:09 PMAll use subject to JSTOR Terms and Conditions

Cancer Causes and Control 12: 903-908, 2001. @ 2001 Kluwer Academic Publishers. Printed in the Netherlands.
903
Trends in smoking-related cancer incidence in Tarragona, Spain, 1980-96
Joan Borris1'3, Josep M. Borras2'*, Jaume Galceran', Victoria S'nchez2, Victor Moreno2 & Juan Ram6n Gonzilez2 1Cancer Registry of Tarragona, Catalonia, Spain; 2lnstitut Catala d'Oncologia, Hospitalet, Barcelona, Spain; 3Hospital de Sant Joan, Universitat Rovira i Virgili, Spain
Received 19 January 2001; accepted in revised form 23 July 2001
Key words: cancer incidence, cancer trends, smoking-related cancer, Spain.
Abstract
Objectives: To analyze recent trends (1980-96) in the incidence of smoking-related cancers among men and women in Tarragona, Spain. Methods: Data were obtained from a population-based cancer registry. Age-standardized incidence rates were computed. Secular trends, between 1980 and 1996, were estimated using a Poisson regression model. From these figures, age, period, and cohort effects were assessed using the method proposed by Holford. Results: The incidence of all smoking-related cancers combined increased significantly in both sexes. The annual increase was 3.0% in men and 4.5% in women. By sites the annual increase was 4.3% in oral cavity, 5.1% in pancreas, 2.5% in lung, 3.2% in bladder, and 7.7% in kidney cancers among men. Among women the corresponding increments were 7.0% in oral cavity, 7.3% in pancreas, 3.1% in lung, 2.1% in bladder, and 6.9% in kidney cancers. The increasing incidence of lung cancer in women was mostly due to the adenocarcinoma histological type. No increase was observed in esophagus and larynx cancer either in men or women. It was not possible to determine whether the increases are due to a period or cohort effect since the curvature analysis was found to be non-significant. Conclusions: All smoking-related cancers combined, except larynx and esophagus, are increasing in both sexes. The effect of tobacco, alcohol, and occupational exposure to carcinogens could explain the high rates of larynx, bladder, and upper digestive tract cancer in men. The rising incidence rates of lung cancer observed in younger women indicate a change in recent trends that is consistent with changes observed in smoking prevalence. Unless recent upward smoking trends in young women can be reversed, lung cancer in women will rise rapidly in the next few years. New smoking prevention strategies aimed at Spanish women, especially in the younger age groups, should be developed.
Introduction
In recent decades, smoking-related cancer incidence and mortality among men in Spain has occupied an inter- mediate rank in Europe, while the rates in women were among the lowest [1-3]. A noticeable exception, how- ever, was the high incidence of larynx and bladder cancer observed in men; a fact that has been related to the interaction between black tobacco smoking and alcohol consumption in southern European countries
[4-7]. Smoking-related cancer trends in incidence and mortality also vary by sex [8]. Among men, a rising trend similar to the pattern seen in northern European countries, but with a time lag of several years, was observed. In contrast, among women the impact of smoking was still not observed [9, 10].
Over the past 15 years, a decrease in smoking prevalence among men, but an increase among women, has been observed in Catalonia, Spain [11, 12]. The proportion of current smoking among men aged 15-64 decreased from 58.3% in 1982 to 39.3% in 1998 [13]. Among women the corresponding figures were 20.0% in 1982 and 30.7% in 1998. These changes began in the 1970s, when Spanish women started to smoke in larger numbers and, since then, smoking prevalence among
* Address for correspondence: Josep M Borris, Cancer Prevention and Control Unit, Institut Catala d'Oncologia, Gran Via s/n Km 2,7, 08907-Hospitalet, Barcelona, Spain. Ph.: 34-93-260 7820; Fax: 34-93- 260 7821; E-mail: [email protected]
This content downloaded from 185.2.32.106 on Sun, 15 Jun 2014 18:16:09 PMAll use subject to JSTOR Terms and Conditions
904 J. Borras et al.
women has increased rapidly. While smoking prevalence among women aged 45 or older was remarkably low during this period, it increased rapidly among younger women, who now show similar figures to men [14-16].
These changes, initiated in the 1970s, will have an impact on current and future cancer incidence. This paper, that aims to analyze recent trends in the incidence of smoking-related cancers among men and women during the period 1980-1996, can be helpful to other similar countries in order to define strategies of cancer prevention. The study is based on data from the population-based cancer registry of Tarragona, located in the region of Catalonia in the northeast of Spain.
Methods
Incidence data were obtained from the Tarragona Cancer Registry, Spain. This registry covers an area with 541,000 inhabitants in which data on newly diagnosed cancers has been gathered since 1980 [17]. Quality indicators for the registry meet international standards [18]. In 1992, the proportion of cancer cases registered from death certificates only was 2% in men and 3% in women, and 91% of cases in men and 90% in women had morphological verification [2].
Smoking-related cancers included in this study were: oral cavity (ICD-9 codes 140-149), esophagus (150), pancreas (157), larynx (161), lung (162), bladder (188), and kidney (189). The incidence of lung cancer was also analyzed according to histological types: squamous carcinoma, adenocarcinoma, small cell carcinoma, large cell carcinoma, unspecified, and other. The last group contains several histological types of low frequency [19]. Annual and aggregated incidence rates for the period
1980-1996 were computed for 100,000 person-years by sex and for each cancer site, and the results are presented for aggregated 6-year intervals. Age-standard- ized rates (ASR) were calculated by the direct method using the World Standard Population [20].
A Poisson regression model was used to assess age, period, and cohort effects on cancer incidence trends. Due to the non-identifiability of the effects of the parameters studied in the model given the linear relation among them, we analyzed the curvatures of the cohort and period effects, based on the method proposed by Holford [21]. Likelihood-ratio tests were used to assess the significance of each effect. Separate models were fitted for each cancer site, for all smoking-related cancers, and for all cancers (excluding non-melanoma skin cancer and in-situ cancers). Trends were assessed for all ages, for truncated rates (35-64 years old) and for the 65-and-over age group. The annual percentage of change in incidence and the corresponding 95% confi- dence interval were derived from the age-period model.
Results
During the study period (1980-96), 7227 men and 1331 women were diagnosed with a smoking-related cancer in Tarragona. This accounts for 43.6% and 10.4% of the total cancer incidence (except non-melanoma skin can- cer) in men and in women, respectively. Cancer inci- dence rates, as well as the annual percentage of change for age-standardized rates and truncated rates, are presented in Table 1 for men and in Table 2 for women.
In the 1992-96 period, lung cancer was the most common smoking-related cancer among men (ASR of 44.3 per 100,000) followed by bladder cancer (ASR of
Table 1. Incidence trends of smoking-related cancer in men. Cancer Registry of Tarragona, Spain
ICD Cancer Total cases, Age-standardized rate Percentage annual change 1980-96 1980-96
1980-85 1986-91 1992-96 All ages 95% CI 35-64 years 95% CI > 64 years 95% CI
140-149 Oral cavity 691 8.9 11.3 14.4 4.3 (2.7-6.0) 5.0 (3.1-7.0) 1.5 (-2.3-5.4) and pharynx
150 Esophagus 365 5.5 5.4 6.3 0.8 (-1.3-3.0) 3.1 (0.4-5.8) -1.3 (-5.9-3.5) 157 Pancreas 324 3.5 4.4 5.9 5.1 (2.6-7.6) 3.5 (0.3-6.8) 11.0 (-5.8-16.0) 161 Larynx 730 10.3 12.0 12.4 1.1 (-0.4-2.7) 1.3 (-0.5-3.2) 1.0 (-2.3-4.4) 162 Lung 2,783 33.8 43.2 44.3 2.5 (1.7-3.3) 2.1 (1.1-3.1) 2.3 (0.9-3.9) 188 Bladder 1,972 21.8 28.5 32.2 3.2 (2.2-4.2) 3.3 (1.9-4.7) 3.7 (2.1-5.4) 189 Kidney 362 3.2 5.5 7.1 7.7 (5.3-10.0) 8.0 (4.7-12.0) 9.6 (5.1-14.0)
All smoking-related 7,227 87.1 110.3 122.6 3.0 (2.5-3.5) 3.0 (2.3-3.6) 3.2 (2.3-4.2) cancers
All cancersa 16,587 203.2 241.0 271.6 2.5 (2.2-2.8) 2.7 (2.2-3.2) 2.3 (1.7-2.9)
a Excluding non-melanoma skin cancer (173).
This content downloaded from 185.2.32.106 on Sun, 15 Jun 2014 18:16:09 PMAll use subject to JSTOR Terms and Conditions

Smoking-related cancer incidence in Spain 905
Table 2. Incidence trends of smoking-related cancer in women. Cancer Registry of Tarragona, Spain
ICD Cancer Total cases, Age-standardized rate Percentage annual change 1980-96 1980-96
1980-85 1986-91 1992-96 All ages 95% CI 35-64 years 95% CI > 64 years 95% CI
140-149 Oral cavity 154 1.3 2.0 2.8 7.0 (3.3-11.0) 8.7 (3.4-14.0) 2.0 (-4.3-8.7) and pharynx
150 Esophagus 39 0.5 0.1 0.5 -2.9 (-9.2-3.7) 6.3 (-6.0-20.0) -0.3 (-11.0-11.0) 157 Pancreas 301 2.0 3.3 4.1 7.3 (4.6-10.0) 4.5 (0.2-9.1) 6.3 (2.0-11.0) 161 Larynx 18 0.2 0.2 0.3 4.1 (-5.7-15.0) 10.0 (-6.7-30.0) 11.0 (-5.5-30.0) 162 Lung 284 2.8 3.0 4.5 3.1 (0.6-5.7) 4.8 (1.0-8.8) 2.3 (-2.0-6.7) 188 Bladder 373 3.0 4.2 4.2 2.1 (0.0-4.4) 5.7 (1.8-9.8) -0.6 (-4.0-2.8) 189 Kidney 162 1.3 2.0 2.9 6.9 (3.4-11.0) 5.5 (0.8-10.0) 9.0 (2.1-16.0)
All smoking-related 1,331 11.2 14.7 19.2 4.5 (3.3-5.7) 5.7 (3.8-7.7) 2.9 (0.9-4.9) cancers
All cancersa 12,816 151.9 167.7 189.8 1.9 (1.6-2.3) 2.1 (1.6-2.6) 0.9 (0.2-1.6)
a Excluding non-melanoma skin cancer (173).
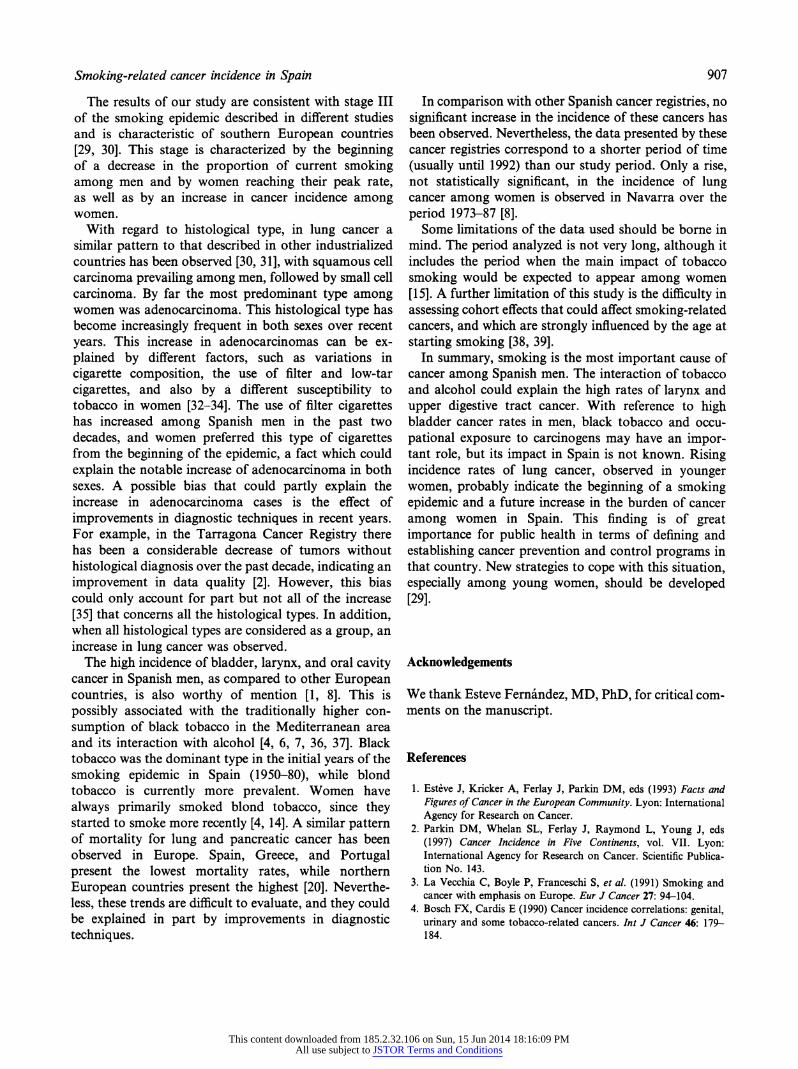
32.2 per 100,000) and oral cavity cancer (ASR of 14.4 per 100,000). Among women, lung cancer was the most frequent smoking-related cancer (ASR of 4.5 per 100,000), followed by bladder cancer (ASR of 4.2 per 100,000) and pancreatic cancer (ASR of 4.1 per 100,000), with quite similar rates. Larynx is by far the cancer with a higher sex ratio, followed by esophagus, lung, and bladder cancers. In men, age-specific rates showed an increase that affects all age groups but which prevailed in those aged 65 and over. In women, it is worthwhile emphasizing an increment in younger age groups (Figure 1).
A statistically significant increase in the incidence of smoking-related cancers as a group was observed in both men (3.0%) and women (4.5%). This increase is higher than that of all cancers taken together (except non-melanoma skin cancer), 2.5% in men and 1.9% in women. Among men, this rise is observed in the 35-64- year group (3.0%), as well as in men aged 65 and over
1000
S- -* -- Men 1980-85 S*/ Men 1992-96
? --o--Women 1980-85
----
- Women 1992-96 CDo10
30 35 40 45 50 55 60 65 70 75 80 85
Age at diagnosis
Fig. 1. Incidence of lung cancer, 1980-96. Age-specific rates. Cancer Registry of Tarragona (Spain).
(3.2%) (Table 1). Among women, the increase prevails in younger age groups, with an annual percentage of change of 5.7% in the 35-64 year group and of 2.9% in women aged 65 and over (Table 2). By site, all smoking- related cancers increased significantly during the period studied, except cancers of the esophagus and larynx. These increases occurred in both men and women. Only pancreas and kidney cancers showed a statistically significant increase in women aged 65 and over. It is not possible to determine whether the increases are due to a period or cohort effect since the curvature analysis was found to be non-significant.
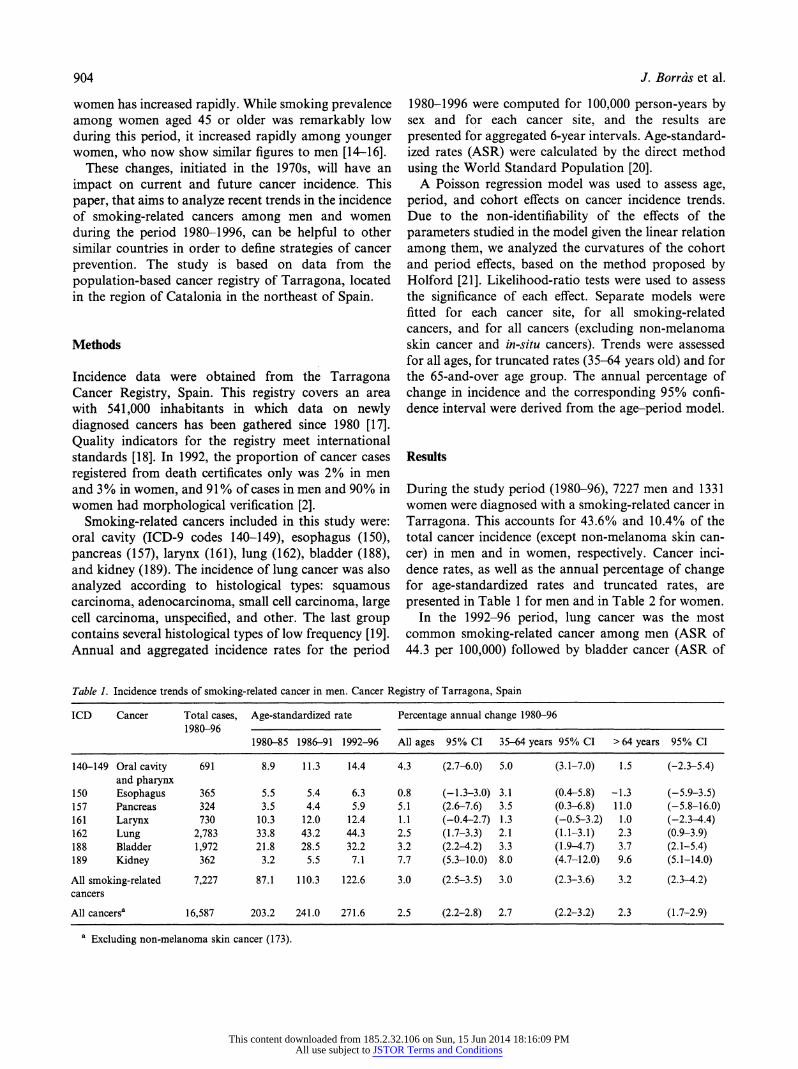
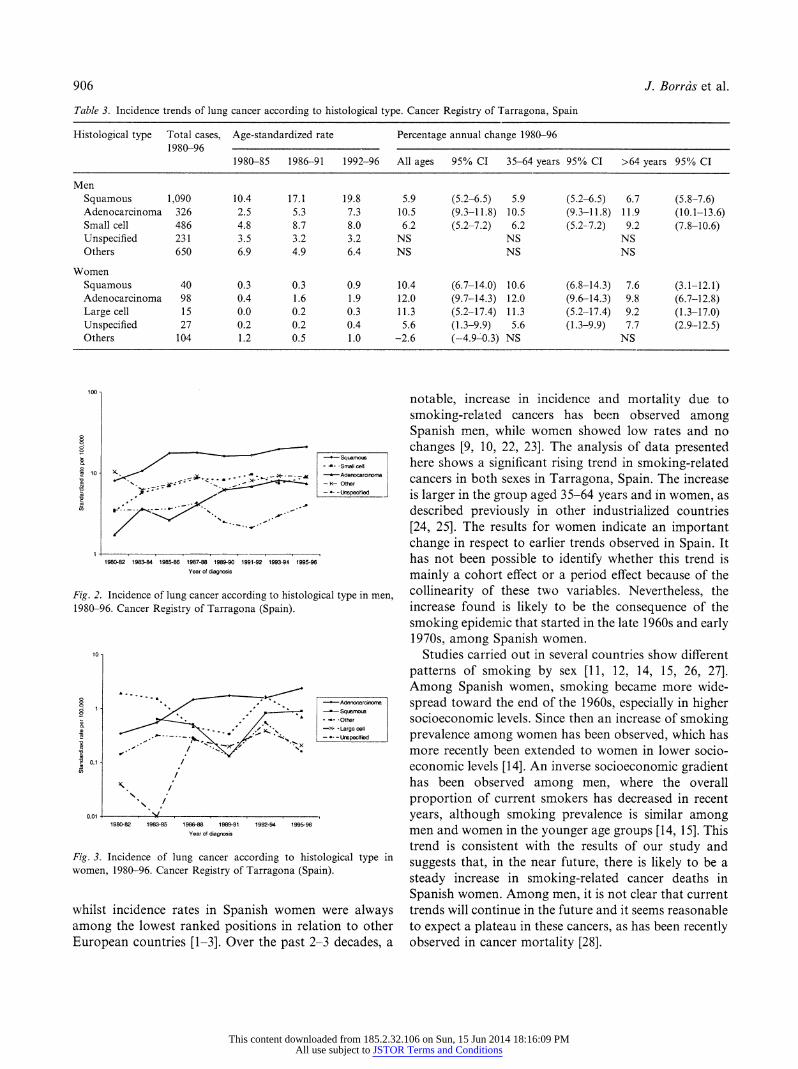
Age-standardized rates and trends of lung cancer by histological type are showed in Table 3 and in Figures 2 and 3. Squamous cell cancer was the most common type among men (ASR of 19.8 per 100,000), followed by small cell cancer (ASR of 8.0 per 100,000) and adeno- carcinoma (ASR of 7.3 per 100,000). Adenocarcinoma showed the greatest increase in incidence rates, with an annual percentage of change of 10.5% since 1980. In women, adenocarcinoma was the most common histo- logical type (ASR of 1.9 per 100,000) followed by squamous cell cancer (ASR of 0.9 per 100,000). Adeno- carcinoma accounted for almost all of the increase observed in women, with an annual percentage of change of 12.0% (p < 0.05). The overall increase in incidence of this histological type in women is largely accounted for by the rise in incidence in the 35-64 year age group (Table 3).
Discussion
Incidence rates of smoking-related cancers in Spanish men were generally ranked in an intermediate position
This content downloaded from 185.2.32.106 on Sun, 15 Jun 2014 18:16:09 PMAll use subject to JSTOR Terms and Conditions
906 J. Borrais et al.
Table 3. Incidence trends of lung cancer according to histological type. Cancer Registry of Tarragona, Spain
Histological type Total cases, Age-standardized rate Percentage annual change 1980-96 1980-96
1980-85 1986-91 1992-96 All ages 95% CI 35-64 years 95% CI >64 years 95% CI
Men
Squamous 1,090 10.4 17.1 19.8 5.9 (5.2-6.5) 5.9 (5.2-6.5) 6.7 (5.8-7.6) Adenocarcinoma 326 2.5 5.3 7.3 10.5 (9.3-11.8) 10.5 (9.3-11.8) 11.9 (10.1-13.6) Small cell 486 4.8 8.7 8.0 6,2 (5.2-7.2) 6.2 (5.2-.7.2) 9.2 (7.8-10.6) Unspecified 231 3.5 3.2 3.2 NS NS NS Others 650 6.9 4.9 6.4 NS NS NS
Women
Squamous 40 0.3 0.3 0.9 10.4 (6.7-14.0) 10.6 (6.8-14.3) 7.6 (3.1-12.1) Adenocarcinoma 98 0.4 1.6 1.9 12.0 (9.7-14.3) 12.0 (9.6-14.3) 9.8 (6.7-12.8) Large cell 15 0.0 0.2 0.3 11.3 (5.2-17.4) 11.3 (5.2-17.4) 9.2 (1.3-17.0) Unspecified 27 0.2 0.2 0.4 5.6 (1.3-9.9) 5.6 (1.3-9.9) 7.7 (2.9--12.5) Others 104 1.2 0.5 1.0 -2.6 (-4.9-0.3) NS NS
100
-- Squamus - .Small cell
S,,,810 ~ -- - Adenocarcirnom-a . ; --- Other
- *- -Urepecif ed
1980-82 1983-84 1985-86 1987-88 1989-90 1991-92 1993.94 1995-96 Year of diagnosis
Fig. 2. Incidence of lung cancer according to histological type in men, 1980-96. Cancer Registry of Tarragona (Spain).
to-
. - Adeanoarcoirrrna
.8
-- Squamous
. " -X- -Large cell
- ---
- -- - --Lnspecdred
o,1 /
0,01 0,01
,
, 1980-82 1983-85 1986-88 1989-91 1992-94 1995-96 Year of diagnosis
Fig. 3. Incidence of lung cancer according to histological type in
women, 1980-96. Cancer Registry of Tarragona (Spain).
whilst incidence rates in Spanish women were always among the lowest ranked positions in relation to other European countries [1-3]. Over the past 2-3 decades, a
notable, increase in incidence and mortality due to smoking-related cancers has been observed among Spanish men, while women showed low rates and no changes [9, 10, 22, 23]. The analysis of data presented here shows a significant rising trend in smoking-related cancers in both sexes in Tarragona, Spain. The increase is larger in the group aged 35-64 years and in women, as described previously in other industrialized countries [24, 25]. The results for women indicate an important change in respect to earlier trends observed in Spain. It has not been possible to identify whether this trend is mainly a cohort effect or a period effect because of the collinearity of these two variables. Nevertheless, the increase found is likely to be the consequence of the smoking epidemic that started in the late 1960s and early 1970s, among Spanish women.
Studies carried out in several countries show different patterns of smoking by sex [11, 12, 14, 15, 26, 27]. Among Spanish women, smoking became more wide- spread toward the end of the 1960s, especially in higher socioeconomic levels. Since then an increase of smoking prevalence among women has been observed, which has more recently been extended to women in lower socio- economic levels [14]. An inverse socioeconomic gradient has been observed among men, where the overall proportion of current smokers has decreased in recent years, although smoking prevalence is similar among men and women in the younger age groups [14, 15]. This trend is consistent with the results of our study and suggests that, in the near future, there is likely to be a steady increase in smoking-related cancer deaths in Spanish women. Among men, it is not clear that current trends will continue in the future and it seems reasonable to expect a plateau in these cancers, as has been recently observed in cancer mortality [28].
This content downloaded from 185.2.32.106 on Sun, 15 Jun 2014 18:16:09 PMAll use subject to JSTOR Terms and Conditions
Smoking-related cancer incidence in Spain 907
The results of our study are consistent with stage III of the smoking epidemic described in different studies and is characteristic of southern European countries [29, 30]. This stage is characterized by the beginning of a decrease in the proportion of current smoking among men and by women reaching their peak rate, as well as by an increase in cancer incidence among women.
With regard to histological type, in lung cancer a similar pattern to that described in other industrialized countries has been observed [30, 31], with squamous cell carcinoma prevailing among men, followed by small cell carcinoma. By far the most predominant type among women was adenocarcinoma. This histological type has become increasingly frequent in both sexes over recent years. This increase in adenocarcinomas can be ex- plained by different factors, such as variations in cigarette composition, the use of filter and low-tar cigarettes, and also by a different susceptibility to tobacco in women [32-34]. The use of filter cigarettes has increased among Spanish men in the past two decades, and women preferred this type of cigarettes from the beginning of the epidemic, a fact which could explain the notable increase of adenocarcinoma in both sexes. A possible bias that could partly explain the increase in adenocarcinoma cases is the effect of improvements in diagnostic techniques in recent years. For example, in the Tarragona Cancer Registry there has been a considerable decrease of tumors without histological diagnosis over the past decade, indicating an improvement in data quality [2]. However, this bias could only account for part but not all of the increase [35] that concerns all the histological types. In addition, when all histological types are considered as a group, an increase in lung cancer was observed.
The high incidence of bladder, larynx, and oral cavity cancer in Spanish men, as compared to other European countries, is also worthy of mention [1, 8]. This is possibly associated with the traditionally higher con- sumption of black tobacco in the Mediterranean area and its interaction with alcohol [4, 6, 7, 36, 37]. Black tobacco was the dominant type in the initial years of the smoking epidemic in Spain (1950-80), while blond tobacco is currently more prevalent. Women have always primarily smoked blond tobacco, since they started to smoke more recently [4, 14]. A similar pattern of mortality for lung and pancreatic cancer has been observed in Europe. Spain, Greece, and Portugal present the lowest mortality rates, while northern European countries present the highest [20]. Neverthe- less, these trends are difficult to evaluate, and they could be explained in part by improvements in diagnostic techniques.
In comparison with other Spanish cancer registries, no significant increase in the incidence of these cancers has been observed. Nevertheless, the data presented by these cancer registries correspond to a shorter period of time (usually until 1992) than our study period. Only a rise, not statistically significant, in the incidence of lung cancer among women is observed in Navarra over the period 1973-87 [8].
Some limitations of the data used should be borne in mind. The period analyzed is not very long, although it includes the period when the main impact of tobacco smoking would be expected to appear among women [15]. A further limitation of this study is the difficulty in assessing cohort effects that could affect smoking-related cancers, and which are strongly influenced by the age at starting smoking [38, 39].
In summary, smoking is the most important cause of cancer among Spanish men. The interaction of tobacco and alcohol could explain the high rates of larynx and upper digestive tract cancer. With reference to high bladder cancer rates in men, black tobacco and occu- pational exposure to carcinogens may have an impor- tant role, but its impact in Spain is not known. Rising incidence rates of lung cancer, observed in younger women, probably indicate the beginning of a smoking epidemic and a future increase in the burden of cancer among women in Spain. This finding is of great importance for public health in terms of defining and establishing cancer prevention and control programs in that country. New strategies to cope with this situation, especially among young women, should be developed [29].
Acknowledgements
We thank Esteve Fernandez, MD, PhD, for critical com- ments on the manuscript.
References
1. Est~ve J, Kricker A, Ferlay J, Parkin DM, eds (1993) Facts and Figures of Cancer in the European Community. Lyon: International Agency for Research on Cancer.
2. Parkin DM, Whelan SL, Ferlay J, Raymond L, Young J, eds (1997) Cancer Incidence in Five Continents, vol. VII. Lyon: International Agency for Research on Cancer. Scientific Publica- tion No. 143.
3. La Vecchia C, Boyle P, Franceschi S, et al. (1991) Smoking and cancer with emphasis on Europe. Eur J Cancer 27: 94-104.
4. Bosch FX, Cardis E (1990) Cancer incidence correlations: genital, urinary and some tobacco-related cancers. Int J Cancer 46: 179- 184.
This content downloaded from 185.2.32.106 on Sun, 15 Jun 2014 18:16:09 PMAll use subject to JSTOR Terms and Conditions

908 J. Borrds et al.
5. Tuyns AJ, Estbve J, Raymond L, et al. (1987) Cancer of the larynx/hypopharynx, tobacco and alcohol: IARC international case-control study in Turin and Varese (Italy), Zaragoza and Navarra (Spain), Geneva (Switzerland) and Calvados (France). Int J Cancer 41: 483-491.
6. Tuyns AJ (1990) Alcohol-related cancers in Mediterranean coun- tries. Tumori 76: 315-320.
7. Tuyns AJ, Sasco AJ (1997) Incidence of tobacco and alcohol- related cancers in western Europe. Eur J Cancer Prey 6: 560-561.
8. Coleman MP, Esteve J, Damiecki P, Arslan A, Renard H, eds (1993) Trends in Cancer Incidence and Mortality. Lyon: Interna- tional Agency for Research on Cancer. Scientific Publication No. 121.
9. Lopez-Abente G, Pollin M, Jimenez M (1993) Female mortality trends in Spain due to tumors associated with tobacco smoking. Cancer Causes Control 4: 539-545.
10. Peto R, Lopez A, Boreham J, Thun MJ, Heath CW (1992) Mortality from tobacco in developed countries: indirect estima- tions from national vital statistics. Lancet 339: 1268-1278.
11. Fernandez E, Salt6 E, Pardell H, Tresserras R, Junc S (1998) Smoking prevalence decreases in males but not in females. The case of Catalonia (Spain). (Letter). Eur J Epidemiol 14: 629-630.
12. Pardell H, Salt6 E, Tresserras R, et al. (1997) La evoluci6n del
hibito tabiquico en Catalufia, 1982-1994. Med Clin (Barc) 109: 125-129.
13. Pla de Salut de Catalunya 1999-2000 (1999) Barcelona: Generalitat de Catalunya; Departament de Sanitat i Seguretat Social, pp. 65- 67.
14. Borrts JM, Fernandez E, Schiaffino A, Borrell C, La Vecchia C (2000) Pattern of smoking initiation in Catalonia, Spain, from 1948 to 1992. Am J Publ Health 90: 1459-1462.
15. Fernandez E, Garcia M, Schiaffino A, Borr.s
JM, Nebot M, Segura A (2001) Smoking initiation and cessation by gender and educational level in Catalonia, Spain. Prey Med 32: 218-223.
16. Onis M, Villar J (1991) La consommation de tabac chez la femme espagnole. Rapp trimest statist sanit mond 44: 80-88.
17. Muir CS, Watherhouse J, Mack T, Powell J, Whelan S, eds (1987) Cancer Incidence in Five Continents, vol. V. Lyon: International
Agency for Research on Cancer. Scientific Publication No. 88. 18. Parkin DM, Chen VW, Ferlay J, Galceran J, Storm HH, Whelan
SL, eds (1994) Comparability and Quality Control in Cancer
Registration. Lyon: International Agency for Research on Cancer. 19. Parkin DM, Shanmugaratnam K, Sobin L, Ferlay J, Whelan SL,
eds (1998) Histological Groups for Comparative Studies. Lyon: International Agency for Research on Cancer.
20. Boyle P, Parkin DM (1991) Statistical methods for registries. In: Jensen OM, Parkin DM, MacLennan R, Muir CS, Skeet RG, eds Cancer Registration: Principles and Methods. Lyon: International
Agency for Research on Cancer. Scientific Publication No. 95, pp. 126-158.
21. Holford TR (1983) The estimation of age period and cohort effects for vital rates. Biometrics 39: 311-324.
22. Moreno V, Sanchez V, Galceran J, Borris JM, Borras J, Bosch FX (1998) Riesgo de enfermar y morir por cancer en Catalufia. Med Clin (Barc) 110: 86-93.
23. Sainchez V, Borris JM, Mingot M (1994) Evolucion de la mortalidad por cancer en Catalufia: 1975-1990. Med Clin (Barc) 102: 606-612.
24. Ernster VL (1994) The epidemiology of lung cancer in women. Ann Epidemiol 4: 102-110.
25. La Vecchia C, Levi F, Decarli A, Wietlisbach V, Gutzwiller F (1998) Trends in smoking and lung cancer mortality in Switzer- land. Prey Med 17: 712-724.
26. Espinis JA, Moreno V, Borris JM, Pujol C, Marti M (1999) Determinantes sociodemogrificos del haibito tabaquico y de su abandono en la poblaci6n de Cornellai de LLobregat. Gac. Sanit 13: 126-134.
27. Fernandez E, Schiaffino A, La Vecchia C, et al. (1999) Age at starting smoking and number of cigarettes smoked in Catalonia, Spain. Prey Med 28: 1-6.
28. Fernandez E, Gonzalez JR, Borris JM, Moreno V, Sanchez V, Peris M (2001) Recent decline in cancer mortality in Catalonia (Spain). A joinpoint regression analysis. Eur J Cancer (in press).
29. Amos A (1996) Women and smoking. Br Med Bull 52: 74-89. 30. Lopez A, Collishaw NE, Piha T (1994) A descriptive model of the
cigarette epidemic in developed countries. Tobacco Control 3: 242- 247.
31. Thun MJ, Lally CA, Flannery JT, Calle EE, Flanders WD, Heath CW (1997) Cigarette smoking and changes in the histopathology of lung cancer. J Natl Cancer Inst 89: 1580-1586.
32. Kreuzer M, Kreienbrock L, Mfiller KM, Gerken M, Wichmann E (1999) Histologic types of lung carcinoma and age at onset. Cancer 85: 1958-1965.
33. Lam S, LeRiche JC, Zheng Y, et al. (1999) Sex-related differences in bronchial epithelial changes associated with tobacco smoking. J Natl Cancer Inst 91: 691-696.
34. Risch HA, Howe GR, Jain M, Burch JD, Holowaty EJ, Miller AB (1993) Are female smokers at higher risk for lung cancer than male smokers? Am J Epidemiol 138: 281-293.
35. Chaloux A, Quoix E, Wolkove N, Small D, Pauli G, Kreisman H (1997) The increasing incidence of lung adenocarcinoma: reality or artefact? A review of the epidemiology of lung adenocarcinoma. Int J Epidemiol 26: 14-23.
36. Boyle P (1997) Cancer, cigarette smoking and premature death in Europe: a review including the recommendations of European Cancer Experts Consensus Meeting, Helsinki, October 1996. Lung Cancer 17: 1-60.
37. La Vecchia C, Boyle P (1993) Trends in tobacco-related cancer epidemic in Europe. Cancer Detect Prev 17: 495-506.
38. Spitz MR, Andrade M, Giovanni J (1999) Molecular dosimeters of smoking damage in the lung. J Natl Cancer Inst 91: 578-579.
39. Wiencke JK, Thurston SW, Kelsey KT, et al. (1999) Early age at smoking initiation and tobacco carcinogen DNA damage in the lung. J Natl Cancer Inst 91: 614-619.
This content downloaded from 185.2.32.106 on Sun, 15 Jun 2014 18:16:09 PMAll use subject to JSTOR Terms and Conditions