treatment of genotype 2, 3 ,4, and...
TRANSCRIPT
David E. Bernstein, MD, FACG
Treatment of Genotype 2, 3 ,4, and Beyond
David E. Bernstein, MD, FACGVice Chairman of Medicine for Clinical Trials
Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver DiseasesNorthwell Health System
Professor of MedicineHofstra Northwell School of Medicine
2
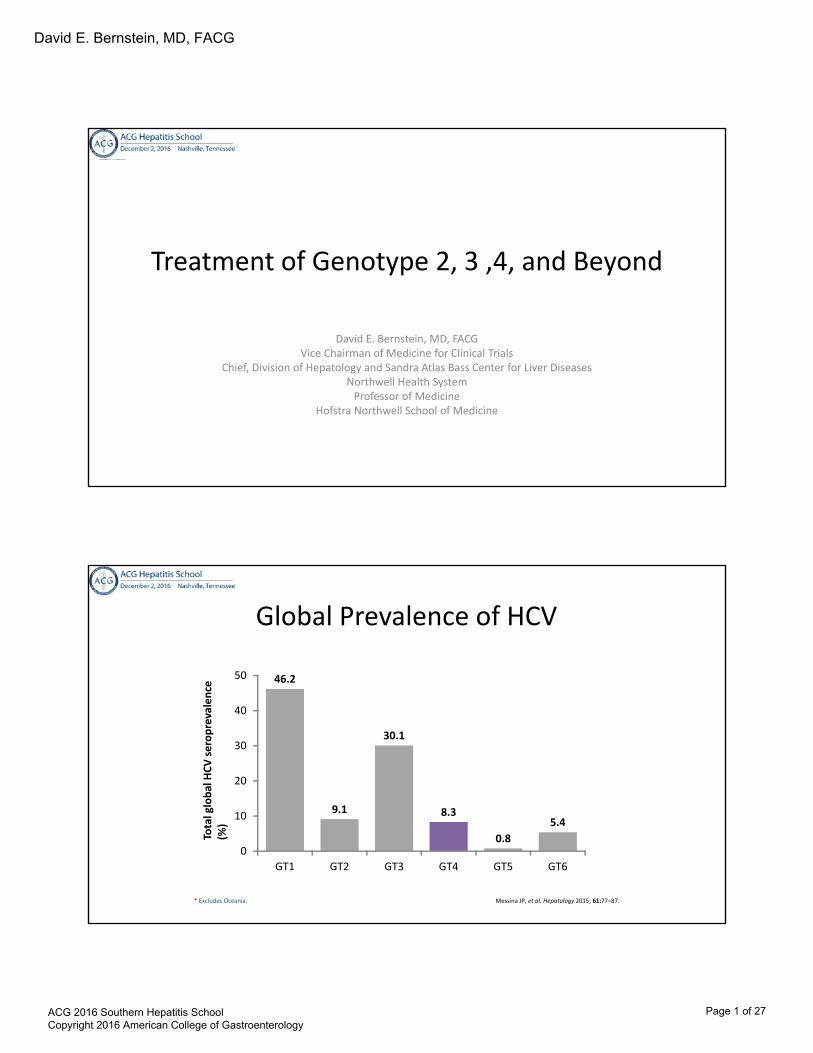
Global Prevalence of HCV
Messina JP, et al. Hepatology 2015; 61:77–87.* Excludes Oceania.
46.2
9.1
30.1
8.3
0.85.4
0
10
20
30
40
50
GT1 GT2 GT3 GT4 GT5 GT6
Tota
l glo
bal H
CV se
ropr
eval
ence
(%)
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 1 of 27
David E. Bernstein, MD, FACG
TREATMENT OF GENOTYPE 2
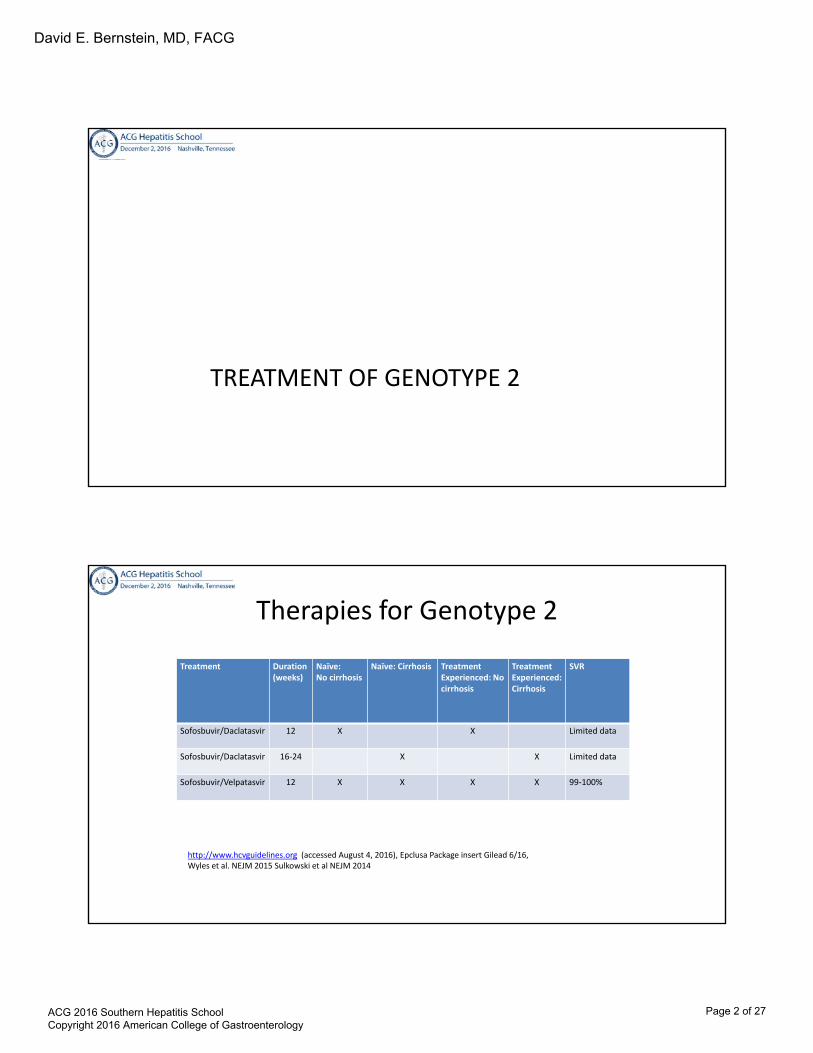
Therapies for Genotype 2
Treatment Duration (weeks)
Naïve:No cirrhosis
Naïve: Cirrhosis Treatment Experienced: No cirrhosis
TreatmentExperienced: Cirrhosis
SVR
Sofosbuvir/Daclatasvir 12 X X Limited data
Sofosbuvir/Daclatasvir 16-24 X X Limited data
Sofosbuvir/Velpatasvir 12 X X X X 99-100%
http://www.hcvguidelines.org (accessed August 4, 2016), Epclusa Package insert Gilead 6/16, Wyles et al. NEJM 2015 Sulkowski et al NEJM 2014
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 2 of 27

David E. Bernstein, MD, FACG
Sofosbuvir + Velpatasvir
1. Jacobson IM, et al. New Engl J Med 2013;368:1867-77; 2. Lawitz E, et al. New Engl J Med 2013;368:1878-87; 3. Cheng G, et al. EASL 2013, poster 1191; 4. German P, et al. EASL 2013, poster 1195; 5. Lawitz E, et al. EASL 2013, poster 1082. 6. Everson G, et al. EASL 2014, oral presentation. 3
SOF Nucleotide polymerase inhibitor
♦ Sofosbuvir (SOF)1,2
‒ Potent antiviral activity against HCV GT 1‒6
‒ Once-daily, oral, 400-mg tablet
♦ Velpatasvir3-5
– Picomolar potency against HCV GT 1‒6– PK supports once-daily dosing
♦ SOF + Velpatasvir6
– Treatment for 12 weeks resulted in high SVR in treatment-naïve patients with HCV GT 1‒6 without cirrhosis
GS-5816NS5A inhibitor
SOF GS-5816+
The ASTRAL Phase 3 Program (N=1408)
6
ASTRAL-1GT 1, 2, 4‒6
TN, TENC, CC
ASTRAL-2GT 2
TN, TENC, CC
ASTRAL-3GT 3
TN, TENC, CC
ASTRAL-4GT 1‒6TN, TE
CTP-B Cirrhosis
‡
Primary endpoints– SVR12– Discontinuations due to AEs
n=624
n=116
Wk 0 Wk 12
n=134
n=132
Wk 0 Wk 12
n=277
n=275
Wk 0 Wk 12
SOF + RBV
SOF/VEL
Wk 24 Wk 0
Wk 12
SOF/VEL
Wk 24
n=90
n=87
n=90
SOF/VEL+ RBV
SOF/VEL
SOF/VEL
Placebo
SOF/VEL
SOF+RBV
ASTRAL-5
GT 1‒4
TN, TE
NC, CCHIV/HCV Co-Infection
n=106
Wk 0 Wk 12
SOF/VEL
Feld, AASLD, 2015, LB-2. Feld JJ, et al. N Engl J Med. 2015; Sulkowski, AASLD, 2015, 205. Foster GR, et al. New Engl J Med. 2015.; Mangia, AASLD, 2015, 249. Foster GR, et al. New Engl J Med. 2015, Charlton, AASLD, 2015, LB-13. Curry MP, et al. New Engl J Med.2015. Wyles, EASL 2016, PS104
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 3 of 27
David E. Bernstein, MD, FACG
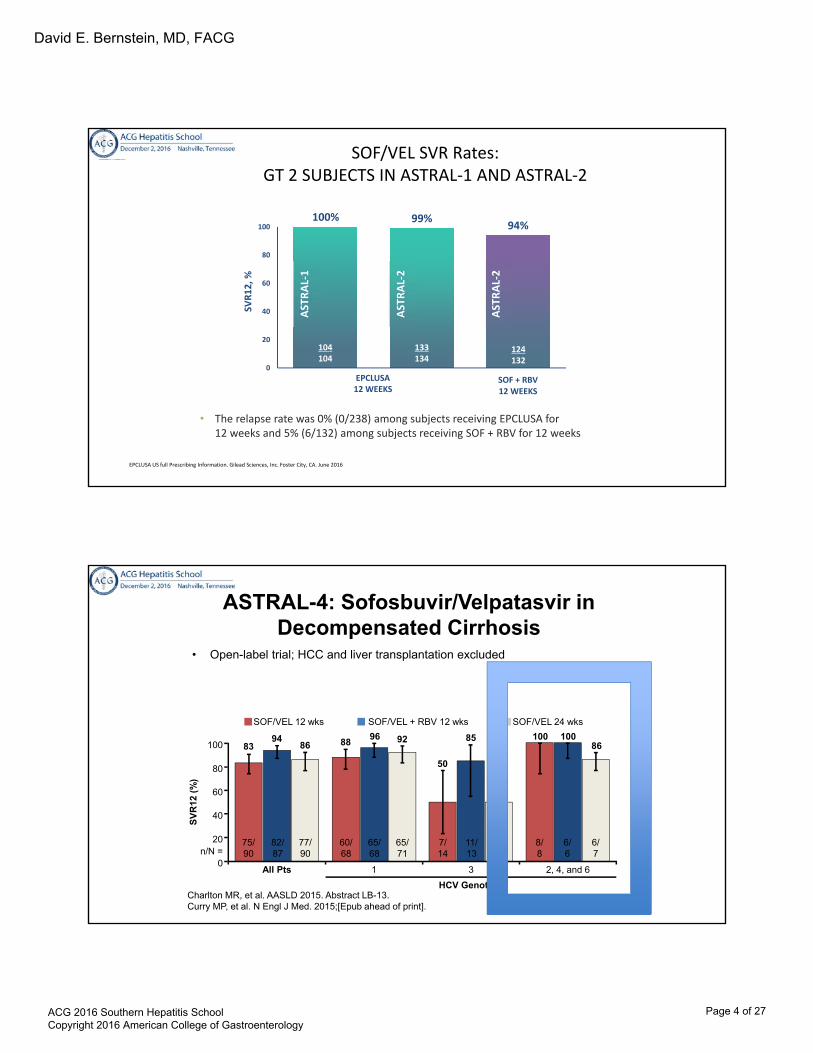
SOF/VEL SVR Rates:GT 2 SUBJECTS IN ASTRAL-1 AND ASTRAL-2
100% 99% 94%
0
20
40
60
80
100
SOF + RBV12 WEEKS
SVR1
2, %
ASTR
AL-1
ASTR
AL-2
ASTR
AL-2
133134
104104
124132
EPCLUSA12 WEEKS
• The relapse rate was 0% (0/238) among subjects receiving EPCLUSA for 12 weeks and 5% (6/132) among subjects receiving SOF + RBV for 12 weeks
EPCLUSA US full Prescribing Information. Gilead Sciences, Inc. Foster City, CA. June 2016
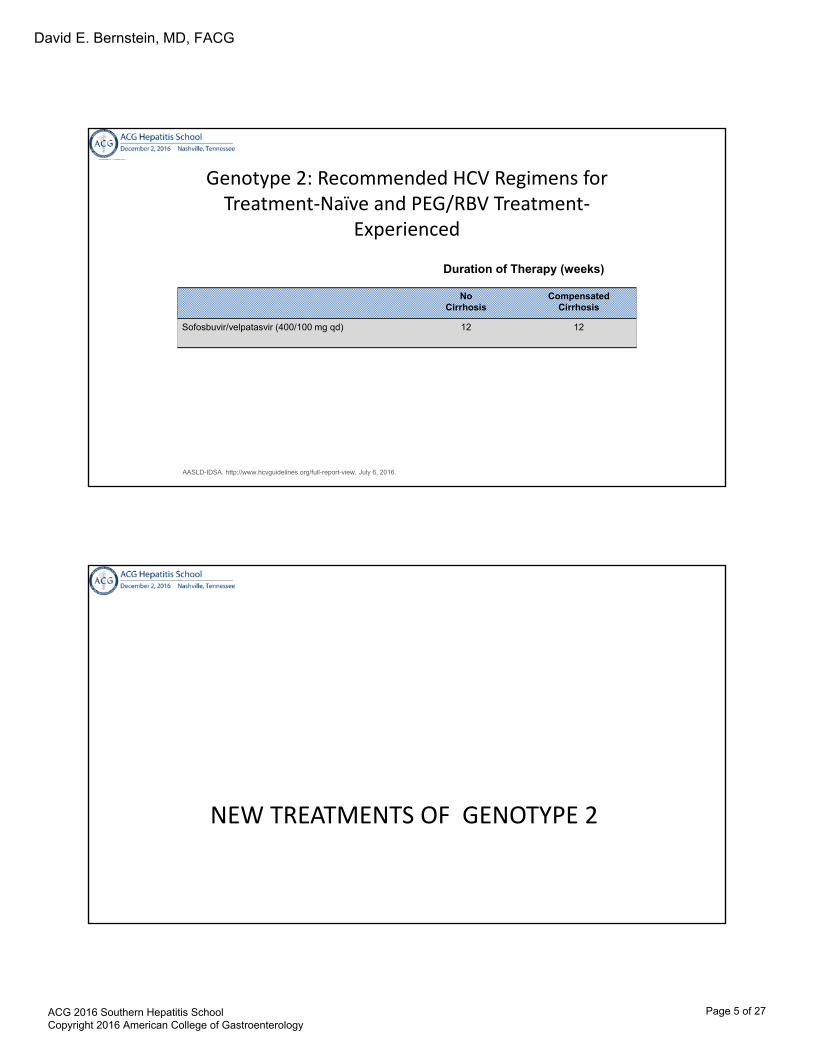
ASTRAL-4: Sofosbuvir/Velpatasvir in Decompensated Cirrhosis
• Open-label trial; HCC and liver transplantation excluded
Charlton MR, et al. AASLD 2015. Abstract LB-13.Curry MP, et al. N Engl J Med. 2015;[Epub ahead of print].
All Pts 1 3
HCV Genotype
n/N =
SV
R12
(%
)
SOF/VEL 12 wks SOF/VEL + RBV 12 wks SOF/VEL 24 wks
2, 4, and 6
100
80
60
40
20
0
8394
86 8896 92
50
85
50
100 10086
75/90
82/87
77/90
60/68
65/68
65/71
7/14
11/13
6/12
8/8
6/6
6/7
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 4 of 27
David E. Bernstein, MD, FACG
NoCirrhosis
CompensatedCirrhosis
Sofosbuvir/velpatasvir (400/100 mg qd) 12 12
Genotype 2: Recommended HCV Regimens forTreatment-Naïve and PEG/RBV Treatment-
Experienced
Duration of Therapy (weeks)
AASLD-IDSA. http://www.hcvguidelines.org/full-report-view. July 6, 2016.
NEW TREATMENTS OF GENOTYPE 2
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 5 of 27

David E. Bernstein, MD, FACG
ABT-493 + ABT-530 in G2
• SURVEYOR-II: 70% G2b, 87% TN, 82% F0-F1
Poordad F, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. SAT-157.
P/R. pegIFN/RBv; pegIFN, pegylated interferon; RBV, ribavirin.
SURVEYOR-II Study Design8-week Treatment Arms Only
0 8 24
ABT-493 (300 mg)+ ABT-530 (120 mg)
SURVERYOR-IIG2 without cirrhosis
• Open-label study• Treatment-naïve or
P/R experienced
SVR12
Week
ABT-493 + ABT-530: SVR Rates after 8 weeks of Treatment
Poordad F, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. SAT-157.
98
0
20
40
60
80
100
GT2
SVR
12 IT
T (%
)
3334
5354
ABT-493 (300mg) + ABT-530 (120mg)8weeks
100
0
20
40
60
80
100
GT2
SVR
12 m
ITT
(%)
3333
5353
ABT-493 (300mg) + ABT-530 (120mg)8weeks
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 6 of 27

David E. Bernstein, MD, FACG
TREATMENT OF GENOTYPE 2: WHAT TO DO WITH DAA FAILURES
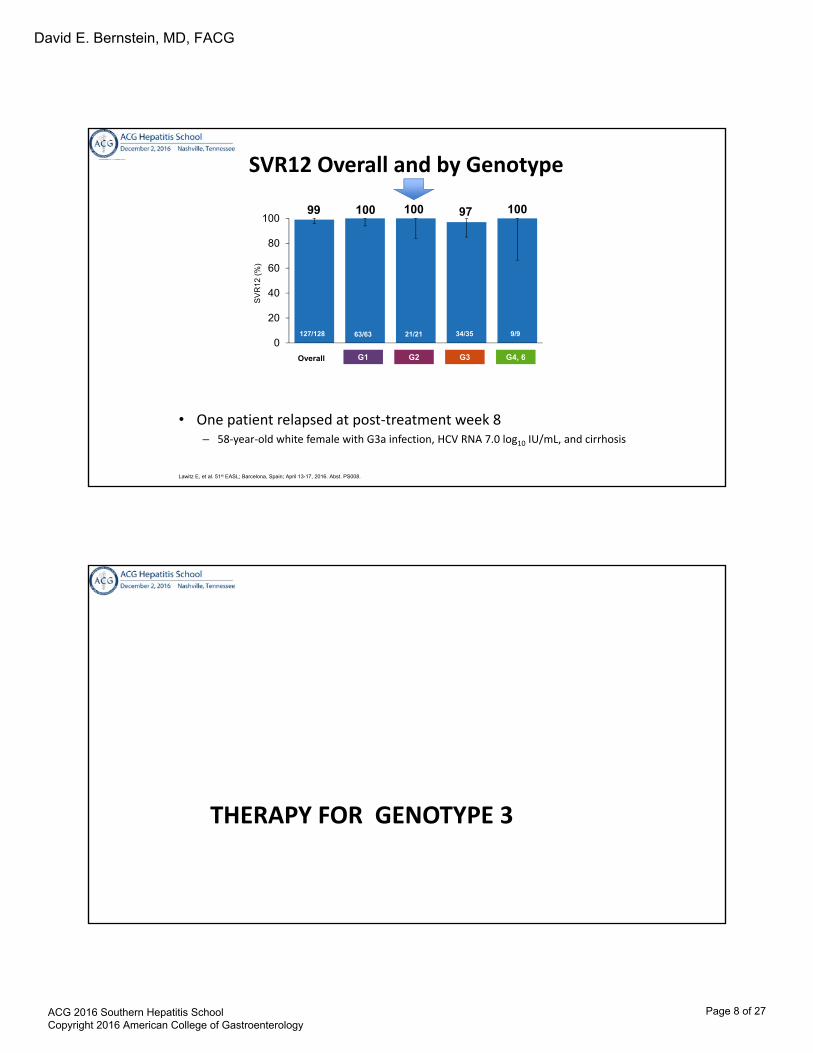
SOF/VEL + GS-9857 (VOX) - Study Design
• GS-9857 – voxilaprevir Protease inhibitor• Two Phase 2, multicenter, open-label studies
(US, New Zealand) – GS-US-367-1168: G1 – GS-US-367-1169: G2, 3, 4, 5, 6
• Broad inclusion criteria– HCV treatment experienced, including DAA experienced
• G1: NS5A inhibitor or ≥2 DAA classes • G2–6: Peg-IFN + RBV or any DAA
– 50% with compensated cirrhosis
0 12 24
SVR12SOF/VEL + GS-9857N=128
Week
Lawitz E, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. PS008.
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 7 of 27
David E. Bernstein, MD, FACG
99 100 100 97 100
0
20
40
60
80
100
SVR12 Overall and by Genotype
• One patient relapsed at post-treatment week 8– 58-year-old white female with G3a infection, HCV RNA 7.0 log10 IU/mL, and cirrhosis
SV
R1
2 (
%)
Overall G3G2 G4, 6G1
63/63127/128 9/934/3521/21
Lawitz E, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. PS008.
THERAPY FOR GENOTYPE 3
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 8 of 27

David E. Bernstein, MD, FACG
Genotype 3 Is Associated With a Significantly Higher Risk of Cirrhosis and HCC vs GT 1
• VA HCV Clinical Case Registry (2000-2009)– 88,348 patients with genotype 1 (80%)
– 13,077 genotype 2 (12%)
– 8,337 genotype 3 (7.5%)
– Mean follow-up 5.4 years
Conclusion: GT 3 is associated with a significantly higher risk of cirrhosis and HCC vs GT 1, independent of age, diabetes, BMI or antiviral treatment
Kanwal F et al, Hepatology 2014;60:98-105
Hazard RatioConfidence
Interval
Cirrhosis 1.31 1.22-1.39
HCC 1.80 1.61-2.03
Therapies for Genotype 3
Treatment Duration (weeks)
Naïve: No cirrhosis
Naïve: Compensated cirrhosis
Treatment Experienced: No cirrhosis
Treatment experienced: Compensated Cirrhosis
SVR
Sofosbuvir/Daclatasvir 12 X X 94-97%Sofosbuvir/Daclatasvir/+/-Ribavirin**
24 X 86%
Sofosbuvir/Daclatasvir/+/-Ribavirin
X Limited data
Sofosbuvir/Velpatasvir 12 X 98%Sofosbuvir/Velpatasvir/+/- ribavirin**
12 X 94%
Sofosbuvir/Velpatasvir 12 X 93%Sofosbuvir/Velpatasvir 12 X 89%
Nelson et al. Hepatology 2015, http://www.hcvguidelines.org (accessed August 4, 2016),Epclusa package insert Gilead 6/16
**RAV testing is indicated for Y93H and add ribavirin if present
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 9 of 27

David E. Bernstein, MD, FACG
Follow-upDCV 60 mg +SOF 400 mg QD
Day 1 Week 24 Week 36
DCV 60 mg +SOF 400 mg QD
Week 12
Treatment-naiveN = 101
Treatment-experiencedN = 51
SVR12
Genotype 3: ALLY-3 Study Design
• Primary endpoint: SVR12• Eligible patients
– Age ≥ 18 years with chronic GT 3 infection and HCV RNA ≥ 10,000 IU/mL– Treatment-naive or -experienced (prior treatment failures), including patients
with cirrhosis– Those who received prior treatment with NS5A inhibitors were excluded
Nelson et al. Hepatology 2015; 61:1127-35
0
20
40
60
80
100 90 86
SV
R12
(%
)
Treatment-naive Treatment-experienced
91/101 44/51
DCV/SOF for GT 3: SVR12 in Treatment-naïve and Treatment-experienced patients Treated for 12 Weeks (ALLY-3)
Nelson DR, Hepatology 2015; 61: 1127-1135
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 10 of 27

David E. Bernstein, MD, FACG
96 97 94
63 5869
0
20
40
60
80
100
SV
R12
(%)
YesNo
Cirrhosis
YesNo YesNo
Overall Tx-naive Tx-experienced
SVR12 in Patients With and Without Cirrhosis Treated for 12 Weeks (ALLY-3)
Nelson DR, Hepatology 2015; 61: 1127-1135
Ally-3 and Ally-3+: SVR 12 in advanced fibrosis
22
All 12 week 16 week12 week
93
SVR1
2 (%
) + 9
5% C
I
ALLY-3(DCV+SOF)
ALLY-3+(DCV+SOF+RBV)
0102030405060708090
100100
1 relapsePrior SOF+RBV failure
NS5A-Y93H at baselineBaseline HCV RNA:
8.8 × 106 IU/mL
1415
1414
66
88
100 100
Kowdley et el. EASL 2016
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 11 of 27
David E. Bernstein, MD, FACG
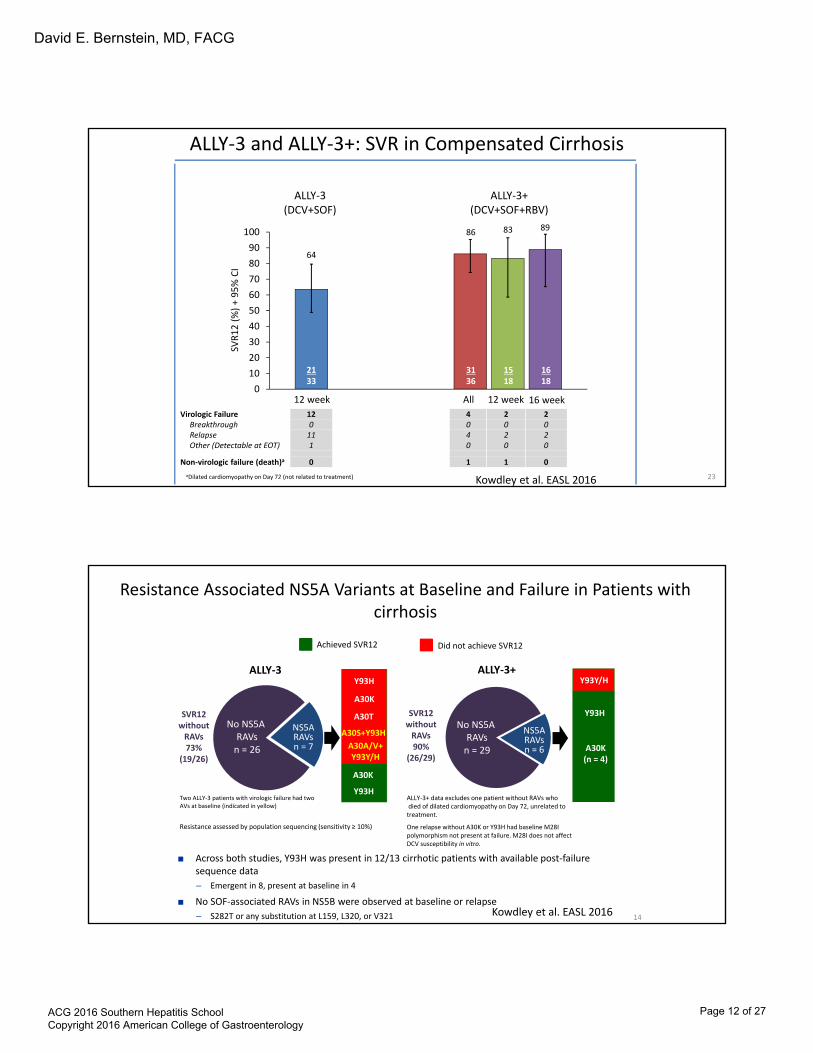
ALLY-3 and ALLY-3+: SVR in Compensated Cirrhosis
23
0102030405060708090
100
64
86 83 89
2133
3136
1518
1618
ALLY-3+(DCV+SOF+RBV)
ALLY-3(DCV+SOF)
All 12 week 16 week12 weekVirologic Failure 12 4 2 2
Breakthrough 0 0 0 0Relapse 11 4 2 2Other (Detectable at EOT) 1 0 0 0
Non-virologic failure (death)a 0 1 1 0aDilated cardiomyopathy on Day 72 (not related to treatment)
SVR1
2 (%
) + 9
5% C
I
Kowdley et al. EASL 2016
Resistance Associated NS5A Variants at Baseline and Failure in Patients with cirrhosis
■ Across both studies, Y93H was present in 12/13 cirrhotic patients with available post-failure sequence data– Emergent in 8, present at baseline in 4
■ No SOF-associated RAVs in NS5B were observed at baseline or relapse– S282T or any substitution at L159, L320, or V321
Resistance assessed by population sequencing (sensitivity ≥ 10%)
No NS5A RAVs
n = 26
NS5ARAVsn = 7
14
Y93H
A30S+Y93H
A30K
A30TSVR12without
RAVs73%
(19/26)
4550
No NS5A RAVs
n = 12NS5A RAVs
n = 2 A30K(n = 4)
Y93H
A30T (n=1)
SVR12without
RAVs90%
(26/29)A30A/V+Y93Y/H
A30K
Y93H
Y93Y/HALLY-3 ALLY-3+
No NS5A RAVs
n = 29
NS5ARAVsn = 6
ALLY-3+ data excludes one patient without RAVs whodied of dilated cardiomyopathy on Day 72, unrelated to
treatment.
One relapse without A30K or Y93H had baseline M28I polymorphism not present at failure. M28I does not affect DCV susceptibility in vitro.
Two ALLY-3 patients with virologic failure had two AVs at baseline (indicated in yellow)
Achieved SVR12 Did not achieve SVR12
Kowdley et al. EASL 2016
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 12 of 27

David E. Bernstein, MD, FACG
The ASTRAL Phase 3 Program
25
ASTRAL-1GT 1, 2, 4‒6
TN, TENC, CC
ASTRAL-2GT 2
TN, TENC, CC
ASTRAL-3GT 3
TN, TENC, CC
ASTRAL-4GT 1‒6TN, TE
CTP-B Cirrhosis
‡
Primary endpoints– SVR12– Discontinuations due to AEs
n=624
n=116
Wk 0 Wk 12
n=134
n=132
Wk 0 Wk 12
n=277
n=275
Wk 0 Wk 12
SOF + RBV
SOF/VEL
Wk 24 Wk 0
Wk 12
SOF/VEL
Wk 24
n=90
n=87
n=90
SOF/VEL+ RBV
SOF/VEL
SOF/VEL
Placebo
SOF/VEL
SOF+RBV
ASTRAL-5
GT 1‒4
TN, TE
NC, CCHIV/HCV Co-Infection
n=106
Wk 0 Wk 12
SOF/VEL
Feld, AASLD, 2015, LB-2. Feld JJ, et al. N Engl J Med. 2015; Sulkowski, AASLD, 2015, 205. Foster GR, et al. New Engl J Med. 2015.; Mangia, AASLD, 2015, 249. Foster GR, et al. New Engl J Med. 2015, Charlton, AASLD, 2015, LB-13. Curry MP, et al. New Engl J Med.2015. Wyles, EASL 2016, PS104
Study DesignASTRAL-3
• Open-label, active-comparator trial • Broad inclusion criteria• 1:1 randomization to SOF/VEL or SOF + RBV
– Stratified by prior treatment (TN/TE) and cirrhosis (presence/absence)• Conducted at 76 sites in US, Canada, UK, Germany, France, Italy, Australia,
and New Zealand
Foster et al. NEJM 2016 26
n=250
n=250
Week 0 12 24
SVR12
SVR12SOF + RBV
36
SOF/VEL
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 13 of 27

David E. Bernstein, MD, FACG
*p-value for superiority of SOF/VEL compared with SOF+ RBV. Error bars represent 95% confidence intervals.
Results: SVR12ASTRAL-3
27
95
80
0
20
40
60
80
100SV
R12
(%)
264/277 221/275
p <0.001*
SOF/VEL12 Weeks
SOF + RBV24 Weeks
Foster et al NEJM 2016
97 91 97 9087
66
86
63
0
20
40
60
80
100
SOF/VEL SOF + RBV
SVR1
2 (%
)
Results: SVR12 by Cirrhosis or Treatment HistoryASTRAL-3
Error bars represent 95% confidence intervals.
191197
7380
5583
200206
176204
6471
4571
163187
No Yes Naïve Experienced
Cirrhosis Status Treatment History
28NEJM 2016
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 14 of 27
David E. Bernstein, MD, FACG
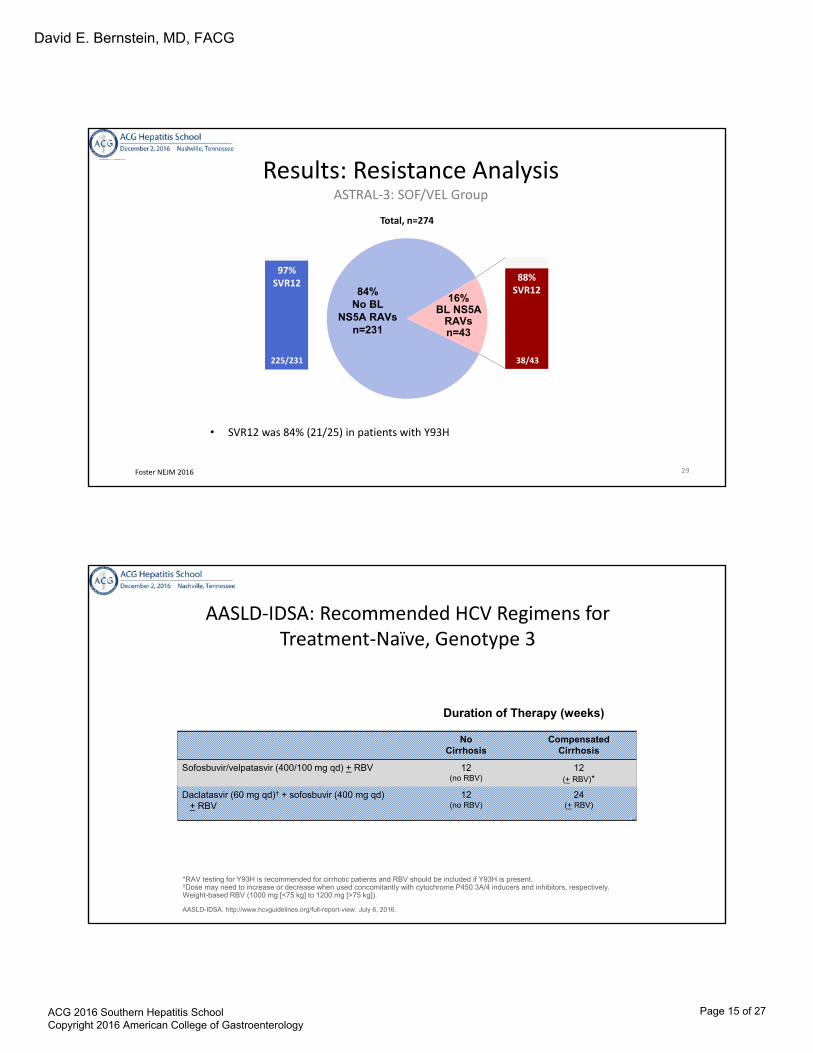
Results: Resistance AnalysisASTRAL-3: SOF/VEL Group
• SVR12 was 84% (21/25) in patients with Y93H
Foster NEJM 2016 29
84% No BL
NS5A RAVsn=231
16% BL NS5A
RAVsn=43
Total, n=274
97% SVR12
225/231
88% SVR12
38/43
NoCirrhosis
CompensatedCirrhosis
Sofosbuvir/velpatasvir (400/100 mg qd) + RBV 12(no RBV)
12(+ RBV)*
Daclatasvir (60 mg qd)† + sofosbuvir (400 mg qd)+ RBV
12(no RBV)
24(+ RBV)
AASLD-IDSA: Recommended HCV Regimens forTreatment-Naïve, Genotype 3
Duration of Therapy (weeks)
*RAV testing for Y93H is recommended for cirrhotic patients and RBV should be included if Y93H is present.†Dose may need to increase or decrease when used concomitantly with cytochrome P450 3A/4 inducers and inhibitors, respectively.Weight-based RBV (1000 mg [<75 kg] to 1200 mg [>75 kg]).
AASLD-IDSA. http://www.hcvguidelines.org/full-report-view. July 6, 2016.
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 15 of 27

David E. Bernstein, MD, FACG
AASLD-IDSA: Recommended HCV Regimens forPrior PR Failure, Genotype 3
Duration of Therapy (weeks)
AASLD-IDSA. http://www.hcvguidelines.org/full-report-view. July 6, 2016.
NoCirrhosis
CompensatedCirrhosis
Sofosbuvir/velpatasvir (400/100 mg qd) + RBV 12(+ RBV)*
12(with RBV)
Daclatasvir (60 mg qd)† + sofosbuvir (400 mg qd)+ RBV
12(+ RBV)*
24(with RBV)
*RAV testing for Y93H is recommended for non-cirrhotic patients and RBV should be included if Y93H is present.†Dose may need to increase or decrease when used concomitantly with cytochrome P450 3A/4 inducers and inhibitors, respectively.Weight-based RBV (1000 mg [<75 kg] to 1200 mg [>75 kg]).PR: pegIFN/RBV.
NEW THERAPIES ON THE HORIZON FOR GENOTYPE 3
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 16 of 27

David E. Bernstein, MD, FACG
C-Crest 1 & 2: Part B: MK-3682/GRZ/MK-8408 with and without RBV in non-cirrhotic and cirrhotics with genotype 1,2, and 3
95
98
87
96
100 100 100
98
100
97
80
82
84
86
88
90
92
94
96
98
100
GT 1a GT 1b G2 G3
Per Protocol Analysis
8 weeks 12 weeks 16 weeks
Lawitz et al. AASLD 2016. abstract 110
C-Crest 1 & 2: Part B: MK-3682/GRZ/MK-8408 with and without RBV in non-cirrhotic and cirrhotics with genotype 3
94
95
96
97
98
99
100
101
TN TE
GT3 BY PRIOR TREATMENT EXPERIENCE
8 weeks 12 weeks 16 weeks
Lawitz et al AASLD 2016; abstract 110
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 17 of 27

David E. Bernstein, MD, FACG
C-Crest 1 & 2: Part B: MK-3682/GRZ/MK-8408 with and without RBV in G3 cirrhotics
100 100 100
96
94
95
96
97
98
99
100
12 week, No RBV 12 week, RBV 16 week, No RBV 16 week, RBV
Lawitz et al. AASLD 2016; abstract 110
ABT-493 (glecaprevir) + ABT-530 (pibrenasvir) SVR Rate – G3 Non-cirrhotics
• No virologic failures• 1 patient withdrew consent after
treatment week 6 due to intolerance of blood draws and had an undetectable HCV RNA at the time of discontinuation
• Safe and well tolerated
Muir AJ, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. PS098.
mITT SVR12 rate excludes non-virologic failures
97 100
0
20
40
60
80
100
.SVR12 mITTSVR12
SVR1
2, %
Pat
ient
s
28 / 29
28 / 28
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 18 of 27

David E. Bernstein, MD, FACG
Kwo P, et al. 51st EASL; Barcelona, Spain; April 13-17, 2016. Abst. LB01.
ABT-493 + ABT-530 :Genotype 3 Cirrhotics SVR 12 by ITT Analysis
100 100
0
20
40
60
80
100
.ABT-493+ ABT-530
ABT-493+ ABT-530 + RBV
SVR1
2, %
Pat
ient
s
24 /24
24 / 24
Surveyor –II, part 3: Glecaprevir/pibrenasvir in genotype 3
• Non-cirrhotic, TE subjects• Cirrhotics, regardless of Naïve or TE
Non-cirrhotic TE SVR12 weeks 91% (n=22)16 weeks 96% (n=22)
Cirrhotics SVRTN 12 weeks 98%TE 16 weeks 96%
Wyles et al. AASLD 2016, abstract 113
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 19 of 27

David E. Bernstein, MD, FACG
Polaris 3: SOF/VEL/VOX vs SOF/VEL for genotype 3 and cirrhosis
• Genotype 3, cirrhotic• Two arms
– SOF/VEL/VOX for 8 weeks– SOF/VEL for 12 weeks
• 30% failed previous IFN tx• 219 patients• All Y93H had SVR
– 6 in SOF/VEL/VOX– 4 in SOF/VEL
• No treatment emergent RAS’s developed
0
10
20
30
40
50
60
70
80
90
100
SOF/VEL VOX 8wks
SOF/VEL 12wks
SVR rates96% 96%
Foster et al. AASLD 2016 Abstract 258
TREATMENT OF GENOTYPE 4
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 20 of 27
David E. Bernstein, MD, FACG
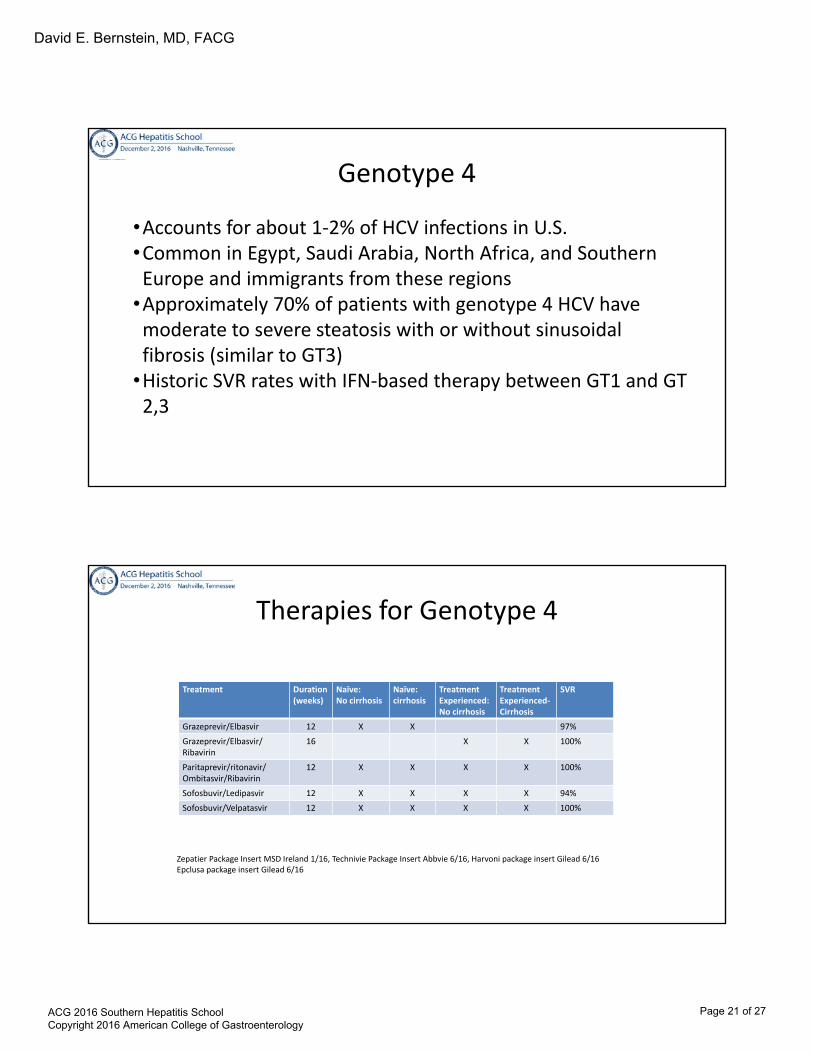
Genotype 4
•Accounts for about 1-2% of HCV infections in U.S.•Common in Egypt, Saudi Arabia, North Africa, and Southern Europe and immigrants from these regions
•Approximately 70% of patients with genotype 4 HCV have moderate to severe steatosis with or without sinusoidal fibrosis (similar to GT3)
•Historic SVR rates with IFN-based therapy between GT1 and GT 2,3
Therapies for Genotype 4
Treatment Duration (weeks)
Naïve:No cirrhosis
Naïve:cirrhosis
Treatment Experienced: No cirrhosis
Treatment Experienced-Cirrhosis
SVR
Grazeprevir/Elbasvir 12 X X 97%Grazeprevir/Elbasvir/Ribavirin
16 X X 100%
Paritaprevir/ritonavir/Ombitasvir/Ribavirin
12 X X X X 100%
Sofosbuvir/Ledipasvir 12 X X X X 94%Sofosbuvir/Velpatasvir 12 X X X X 100%
Zepatier Package Insert MSD Ireland 1/16, Technivie Package Insert Abbvie 6/16, Harvoni package insert Gilead 6/16Epclusa package insert Gilead 6/16
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 21 of 27

David E. Bernstein, MD, FACG
PEARL-I Study: Ombitasvir/Paritaprevir/r + RBV in HCV Genotype 4
• Open-label, phase 2b study– Ombitasvir/paritaprevir/r + RBV
for 12 weeks– Treatment-naïve and
experienced (no prior DAAs)• HCV RNA: 6.1 IU/mL
– No cirrhosis– Primary efficacy endpoint: SVR12
• Baseline NS5A RAVs (58% of patients) did not impact SVR12 rates
• Virologic failures (n=3)– Genotype 4d
0
20
40
60
80
100
SV
R12
(%
)
91%100%
Ombitasvir/Paritaprevir/r
(n=44)
100%
SVR Rates
Hezode C, et al. Lancet. 2015;385:2502-2509.
Ombitasvir/Paritaprevir/r+ RBV (n=42)
Ombitasvir/Paritaprevir/r+ RBV (n=49)
TreatmentNaive
TreatmentExperienced
Astral 1: Velpatasvir (NS5A) + SOF for 12 weeks- Genotype 4, 5 and 6
100 97 100
0
20
40
60
80
100
GT 4 GT 5 GT 6
SVR
Feld et al. NELM 2015
116/116 34/35 41/41
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 22 of 27

David E. Bernstein, MD, FACG
NoCirrhosis
CompensatedCirrhosis
Sofosbuvir/velpatasvir (400/100 mg qd) 12 12
Ledipasvir/sofosbuvir (90/400 mg qd) 12 12
Elbasvir/grazoprevir (50/100 mg) 12 12
Ombitasvir/paritaprevir/r (25/150/100 mg qd) + RBV 12 12
AASLD-IDSA: Recommended HCV Regimens forTreatment-Naïve, Genotype 4
Duration of Therapy (weeks)
Weight-based RBV (1000 mg [<75 kg] to 1200 mg [>75 kg]).
AASLD-IDSA. http://www.hcvguidelines.org/full-report-view. July 6, 2016.
NoCirrhosis
CompensatedCirrhosis
Sofosbuvir/velpatasvir (400/100 mg qd) 12 12
Ledipasvir/sofosbuvir (90/400 mg qd) 12 12
Elbasvir/grazoprevir (50/100 mg) 16 16
Ombitasvir/paritaprevir/r (25/150/100 mg qd) + RBV 12 12
AASLD-IDSA: Recommended HCV Regimens forTreatment-Experienced, Genotype 4
Duration of Therapy (weeks)
Weight-based RBV (1000 mg [<75 kg] to 1200 mg [>75 kg]).
AASLD-IDSA. http://www.hcvguidelines.org/full-report-view. July 6, 2016.
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 23 of 27

David E. Bernstein, MD, FACG
NEW TREATMENTS OF GENOTYPE 4
Surveyor-II, Part 4: Glecaprevir/pibrentasvir in genotype 2,4,5,6 without cirrhosis
• 203 subjects treated for 8 weeks
97
98
100 100
95.5
96
96.5
97
97.5
98
98.5
99
99.5
100
G2 G4 G5 G6
SVR
141/145 44/45 2/2 10/10Hassenian et al. AASLD 2016. Abstract LB-15
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 24 of 27

David E. Bernstein, MD, FACG
Endurance 4: Glecaprevir/pibrentasvir for genotype 4, 5 ,6
• Non-cirrhotics• 12 week regimen• 99% (120/121) of GT 4-6 patients achieved SVR
Asselah et al. AASLD 2016; Abstract 114
TREATMENT OF GENOTYPE 5 AND 6
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 25 of 27

David E. Bernstein, MD, FACG
NoCirrhosis
CompensatedCirrhosis
Sofosbuvir/velpatasvir (400/100 mg qd) 12 12
Ledipasvir/sofosbuvir (90/400 mg qd) 12 12
Genotype 5 and 6:Recommended HCV Regimens for
Treatment-Naïve and PEG/RBV Treatment Experienced, Genotype 5 and 6
Duration of Therapy (weeks)
AASLD-IDSA. http://www.hcvguidelines.org/full-report-view. July 6, 2016.
General Outcomes With AASLD-IDSA Recommended HCV Regimens for Genotype 5 and 6 Patients
Genotype 5: Treatment-Naïve, Treatment-Experienced
Sofosbuvir/velpatasvir: 12 weeks (ASTRAL-1).Ledipasvir/sofosbuvir (12 weeks): genotype 5 (study 1119) and genotype 6 (ELECTRON).
Feld JJ, et al. N Engl J Med. 2015;373:2599-2697.Abergel A, et al. Lancet Infect Dis. 2016;16:459-464.Gane EJ, et al. Gastroenterology. 2015;149:1454-1461.
Percent (n/N)
SVR12Rate
Relapse Rate
DiscontinuationsDue to Adverse Events
Sofosbuvir/velpatasvir 12 weeksNo cirrhosis/compensated cirrhosis 96 (23/24) 0 (0/24) 0 (0/24)
Ledipasvir/sofosbuvir 12 weeksNo cirrhosisCompensated cirrhosis
97 (31/32)
89 (8/9)
3 (1/32)
11 (1/9)
0 (0/32)
0 (0/9)
Sofosbuvir/velpatasvir 12 weeksNo cirrhosis/compensated cirrhosis 100 (38/38) 0 (0/38) 0 (0/38)
Ledipasvir/sofosbuvir 12 weeksNo cirrhosis/compensated cirrhosis 96 (24/25) 4 (1/25) 0 (0/25)
Genotype 6: Treatment-Naïve, Treatment-Experienced
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 26 of 27

David E. Bernstein, MD, FACG
Summary
• All oral DAA’s highly effective for all non-genotype 1 genotypes• What’s ahead in the future
– Pangenotypic therapies– Shorter duration of treatment?
ACG 2016 Southern Hepatitis School Copyright 2016 American College of Gastroenterology
Page 27 of 27