transmantle sign and focal cortical dysplasia 1 a. luppi, 1 g. n. simao, 2 l. neder, 2 j. e. h....
TRANSCRIPT

Transmantle sign and focal cortical dysplasia
1A. Luppi, 1G. N. Simao, 2 L. Neder, 2 J. E. H. Pittella, 3T. Velasco, 4C.G. Carlotti Jr., 4H.R. Machado, 3A.C. Sakamoto, 1A.C. Santos
Presentation number: EP-10
1 Radiology Division2 Pathology3 Epilepsy Surgery Center4 Surgery Department
University of Sao Paulo Ribeirao Preto School of MedicineRibeirao Preto – SP ,Brazil

Disclosures
• No disclosures

Background and Purpose
• Focal cortical dysplasia (FCD) was first described by Taylor (1971) and very frequently is associated with refractory epilepsy. It can be diagnosed only by high resolution MRI, but the findings usually are negative.
• Among MRI abnormalities, the transmantle sign is a very useful evidence, frequently related with FCD type IIb. It is characterized by an area of signal abnormality extending radially inward toward the lateral ventricle from the cortical surface and was first described in a subset of FCD.
• In recent years, the concept of long-term epilepsy associated tumors (LEAT) has been introduced. LEAT are low grade, slowly growing, cortically-based tumors, often with a temporal lobe localization. Histopathology includes ganglioglioma (GG) and dysembryoplastic neuroepithelial tumor (DNET), which represent the most common tumors within the spectrum of LEAT.

Background and Purpose
• The advent of high-resolution MRI has revolutionized the research and treatment of these patients, however some focal cortical lesions may occasionally be quite subtle, setting a major challenge for diagnosis.

Background and Purpose
• Grey matter signal abnormalities:– T2 Hyperintensity of the
grey matter.
Sharp demarcation in the cortical-WM junction
• Better evaluated on T2W images.• Likely due to variable myelination in subcortical
WM (due to state of maturation, reactive astrogliosis or malformation itself).

Background and Purpose
• Among the MRI findings, the transmantle sign, an abnormal signal intensity of deep white matter (WM) that focally spans the entire mantle, tapering toward the ventricle, first described by Barkovich (1997) in the subset of the FCD, is often related to type IIb FCD.

ILAE Classification of FCDs

Objective
• To evaluate how sensitive is the presence of the transmantle sign for FCD on MRI and the different types of focal cortical lesions in operated patients with refractory epilepsy, so as to optimize its detection in clinical practice.

Materials and Methods
• We retrospectively reviewed the MR imaging data of all consecutive patients with focal cortical lesion who underwent surgery for intractable epilepsy between January 2009 and January 2014.
• One hundred and seven patients (107) patients (61 males, 35 children) fulfilled these criteria. All lesions were limited to a single lobe and were unilateral.
• Two neuroradiologists (1 and 5 years of experience), aware of the final localization of the operated lesion, retrospectively reviewed the MR images on a dedicated workstation, in consensus to look for the transmantle sign.

Materials and Methods
• After, the patients were divided into five main groups of lesions based on the histological diagnosis, available on medical archives:
1) type I FCD (n = 14, including 5 cases of type Ia, 6 cases of type Ib and three cases of type Ic);
2) type II FCD (n=37, including 19 cases of type IIa and 18 cases of type IIb);
3) tumors (n= 33);
4) tuberous sclerosis (TS) (n=6)
5) others (n=17, including five cases of astrogliosis, three cases of grey matter heterotopia, two cases of type IIId FCD, four cases of vascular malformations, two cases of polimicrogiria and one case of glioneuronal hamartoma).
• The subdivision of FCD was performed according to the new system of classification of the International League Against Epilepsy (ILAE).

Materials and Methods
Figure 1. Coronal FLAIR images of a patient with diagnosis of type IIb FCD in the right frontal lobe show a marked increased signal, tapering gradually from the gray-white matter interface to the superolateral edge of the lateral ventricle, typical of a transmantle sign (arrows).
• Finally, they evaluated the frequency of the transmantle sign (Figure 1) to each group of lesions and in the subgroups of type II FCD. The chi-square test was used to calculate the P value for statistical significance. A probability value < 0.05 was considered statistically significant.

Results
• Transmantle sign was significantly associated to type II FCD and TS compared to other groups (type I FCD, tumors and other lesions).
Type I FCD Type II FCD Tumors Tuberous sclerosis
Others0
5
10
15
20
25
30
35Figure 2. Transmantle signal presence frequency of each group
YESNO
Transmantle sign

Table 1. Transmantle signal presence frequency of each group (significant difference at p <0.05)
Transmantle Signal (count) Transmantle Signal (%)
Group Yes No Total %Type I FCD 0 14 14 0.0Type II FCD 13 24 37 35,1
Tumors 3 30 33 9.1Tuberous sclerosis 5 1 6 83.3
Others 0 17 17 0.0
Groups p value
Type I FCD x Type II FCD 0.01Type I FCD x Tumors 0.24
Type I FCD x Tuberous sclerosis 0.0001Type I FCD x Others ---
Type II FCD x Tumors 0.03Type II FCD x Tuberous sclerosis 0.02
Type II FCD x Others 0.0001Tumors x Tuberous sclerosis 0.0001
Tumors x Others 0.0001Tuberous sclerosis x Others 0.0001
Results

Results
• In assessing the transmantle sign presence between the subtypes of type II FCD, this sign was significantly associated to type IIb FCD (10 in 18 cases – 55%) compared to type IIa (3 in 19 cases – 15%).
Type IIA FCD Type IIB FCD02468
1012141618
Figure 3. Frequency of transmantle sign in groups type IIa FCD and type IIB FCD
YESNO
Transmantle sign
p = 0.011

Type IIB FCD
Figure 4. Coronal FLAIR and IR images of a patient with diagnosis of type IIb FCD show the classic transmantle sign in the left frontal lobe, with linear and convergent aspect, extending from the inner cortical surface, narrowing while coursing to the edge of the lateral ventricle (arrows).
(a)
(c)

Tuberous sclerosis
Figure 5. Coronal FLAIR images in a patient with tuberous sclerosis with multiple cortical tubers, one of them with the classic transmantle sign (arrows).
F

Results
• It was also observed another type of abnormal sign of WM that spans the entire cerebral mantle from the ventricle to the cortical surface, more thickened than the classic transmantle, without the characteristic linear and convergent aspect, called by the authors “pseudotransmantle sign”, significantly more frequent in tumors compared to other groups, probably being related to tumor dissemination by white matter.
Type I FCD Type II FCD Tumors Tuberous sclerosis
Others0
5
10
15
20
25
30
35Figure 6. Pseudotransmantle sign presence frequency of each group
YESNO
Pseudotransmantle sign
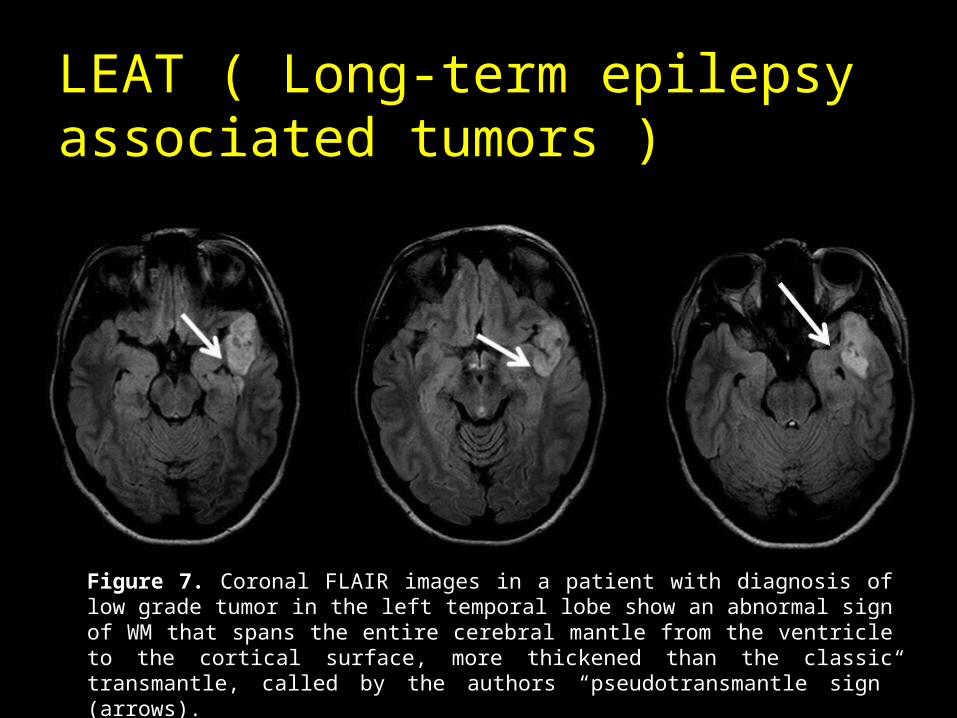
LEAT ( Long-term epilepsy associated tumors )
Figure 7. Coronal FLAIR images in a patient with diagnosis of low grade tumor in the left temporal lobe show an abnormal sign of WM that spans the entire cerebral mantle from the ventricle to the cortical surface, more thickened than the classic transmantle, called by the authors “pseudotransmantle sign” (arrows).

Results• Furthermore, it was observed an abnormal diffuse sign of the WM, that spans the
entire cerebral mantle from the ventricle to the cortical surface, but doesn’t respect a distribution pattern and shows imprecise limits.
• This was more frequent observed in the group others and there was significant difference between the groups others and tumors, TS, type I FCD and type II FCD (p < 0,05).
Type I FCD Type II FCD Tumors Tuberous sclerosis
Others05
101520253035
Figure 8. Diffuse abnormal sign presence frequency of each group
YESNO

Others lesions
Figure 9. Axial FLAIR images in a patient with diagnosis of astrogliosis in the left frontal lobe show an abnormal diffuse sign of WM, extending from the inner cortical surface, of imprecise limits, narrowing while coursing to the edge of the lateral ventricle (arrows).
(a)
(c)
Diffuse pseudotransmantle sign

Results
• Besides, it was observed that in the absence of an abnormal sign of WM, it was significantly associated to type I FCD compared to other groups.
Type I FCD Type II FCD Tumors Tuberous sclerosis
Others0
5
10
15
20
25
Figure 10. Absent sign frequency of each group
YESNO

Figure 11. reduced volume and mild blurring of the subcortical WM at the left frontal superior gyrus (arrow).

Conclusions
• In our study, the transmantle sign was significantly associated with type II FCD and tuberous sclerosis compared to other groups of focal cortical lesions in refractory epilepsy, as well as in type IIb compared to type IIa.
• Furthermore, we also observed other two types of abnormal sign of WM related to focal cortical lesions in refractory epilepsy: a thickened abnormal sign extending radially from the cortical surface toward the lateral ventricle, named “pseudotransmantle sign”, significantly associated to tumors, and a diffuse abnormal sign from the cortical surface until the ventricle, significantly associated to the group of miscellaneous lesions.
• Finally, the absence of abnormal sign of WM was significantly associated to type I FCD.
• In this way, the advances in neuroimaging may help us to localize the epileptogenic lesion in epilepsy surgery candidates and to provide more successful treatment and surgical planning.

References
1. Barkovich AJ, Kuzniecky RI, Bollen AW, Grant PE. Focal transmantle dysplasia: a specific malformation of cortical development. Neurology. 1997 Oct; 49:1148–52.
2. Taylor D.C., Falconer M.A., Bruton C.J., Corsellis J.A. Focal dysplasia of the cerebral cortex in epilepsy. J Neurol Neurosurg Psychiatry. 1971;34, 369-38.
3. Bronen RA, Vives KP, Kim JH, Fulbright RK, Spencer SS, Spencer DD. Focal Cortical Dysplasia of Taylor, Balloon Cell Subtype: MR Differentiation from Low-Grade Tumors. AJNR Am J Neuroradiol. 1997 June; 18:1141–1151.
4. Blümcke I, Vinters HV, Armstrong D, Aronica E, Thom M, Spreafico R. Malformations of cortical development and epilepsies: neuropathological findings with emphasis on focal cortical dysplasia. Epileptic Disord. 2009. Sep; 11 (3): 181-93.
5. Colombo N, Salamon N, Raybaud C, Özkara Ç, Barkovich AJ. Imaging of malformations of cortical development. Epileptic Disord. 2009 Sep;11 (3): 194-205.
6. Blümcke I, Thom M, Aronica E, Armstrong DD, Vinters HV, Palmini A, et al. The clinicopathologic spectrum of focal cortical dysplasias: a consensus classification proposed by an ad hoc Task Force of the ILAE Diagnostic Methods Commission. Epilepsia. 2011 Jan; 52(1):158–74.
7. Shepherd C, Liu J, Goc J, Martinian L, Jacques ST, Sisodiya SM, Thom A. A quantitative study of white matter hypomyelination and oligodendroglial maturation in focal cortical dysplasia type II. Epilepsia. 2013;54(5):898–908.

References
8. Colombo N, Tassi L, Deleo F, Citterio A, Bramerio M, Mai R, et al. Focal cortical dysplasia type IIa and IIb: MRI aspects in 118 cases proven by histopathology. Neuroradiology. 2012 Jun;54:1065–1077.
9. Cossu M., Fuschillo D., Bramerio M, Galli C, Gozzo F, Pelliccia V, et al. Epilepsy surgery of focal cortical dysplasia–associated tumors. Epilepsia. 2013;54(Suppl. 9):115–122.
10. Leach JL, Greiner HM, Miles L, Mangano FT. Imaging Spectrum of Cortical Dysplasia in Children. Seminars in Roentgenology. 2014;49,99-111.
11. Wang DD, Deans AE, Barkovich AJ, Tihan T., Barbaro NM, Garcia PA, Chang EF. Transmantle sign in focal cortical dysplasia: a unique radiological entity with excellent prognosis for seizure control. J Neurosurg. 2013 Feb;118:337–344, 2013.
12. Lee SK, Kim DW. Focal Cortical Dysplasia and Epilepsy Surgery. Journal of Epilepsy Research. 2013; 3:43-47.
13. Mellerio C, Labeyrie M-A, Chassoux F, Daumas-Duport C, et al. Optimizing MR Imaging Detection of Type 2 Focal Cortical Dysplasia: Best Criteria for Clinical Practice. AJNR Am J Neuroradiol. 2012 Nov; 33: 1932-1938.
14. Mellerio C, Labeyrie M-A, Chassoux F, Roca P, Alami O, Plat M., et al. 3T MRI improves the detection of transmantle sign in type 2 focal cortical dysplasia. Epilepsia. 2014; 55(1):117–122.
15. Aronica E, Crino PB. Epilepsy Related to Developmental Tumors and Malformations of Cortical Development. Neurotherapeutics. 2014 Jan;11(2):251-68.