today neuroimaging dementia in aging—get some charts from her lecture ocular changes with...
Post on 19-Dec-2015
216 views
TRANSCRIPT

Today
• Neuroimaging
• Dementia in aging—get some charts from her lecture
• Ocular changes with aging—learn hyperopia

Working Memory is the ability to maintain and manipulate information over short periods of time necessary to guide behavior

200
400
600
800
1000
Mea
n R
eact
ion
Tim
e (m
sec)
Task Condition
70s-80s
50s-60s
20s-30s
ALONE COUNTING DIGIT SPAN
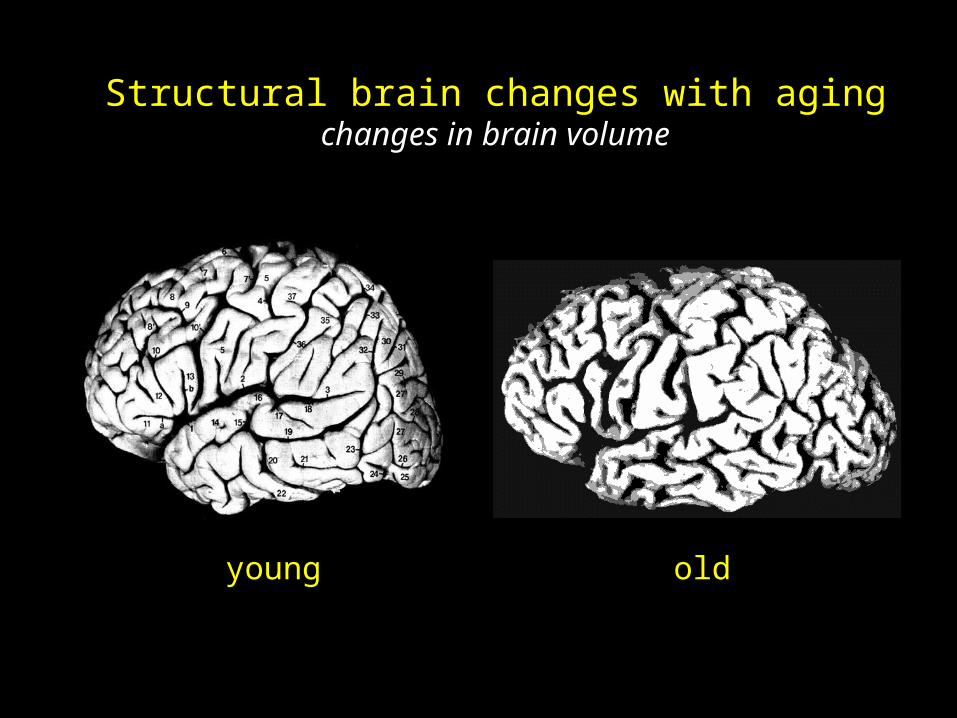
Structural brain changes with agingchanges in brain volume
young old

STRUCTURAL FUNCTIONAL
Magnetic Resonance ImagingPositron Emission Tomography
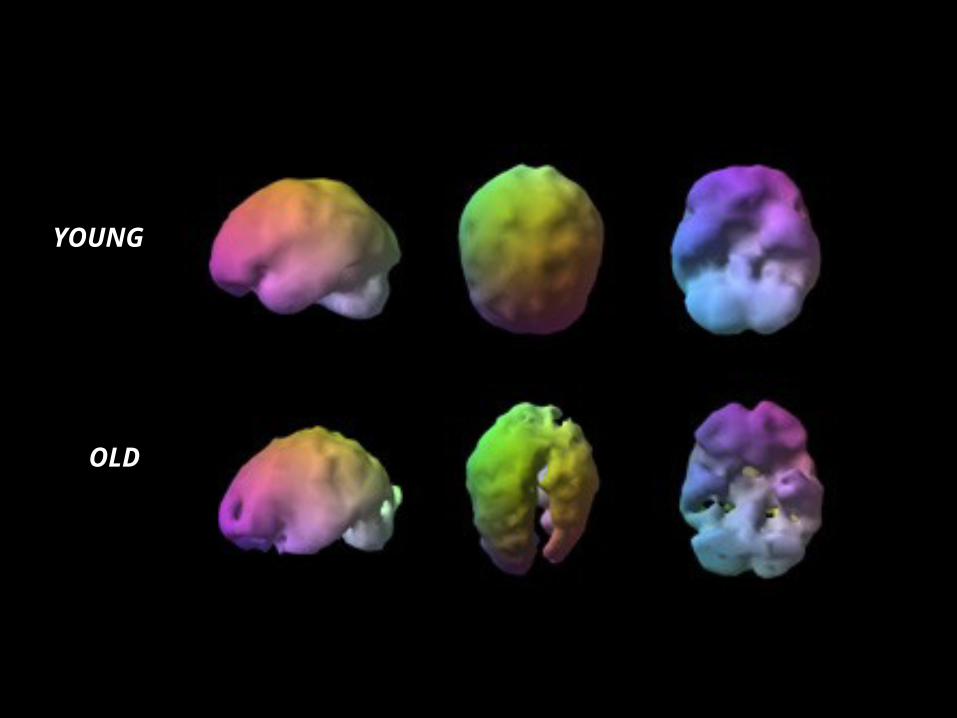
OLD
YOUNG


YOUNG ELDERLYUNDER
RECRUITMENTOVER
RECRUITMENT
YOUNG
OLD
NON-SELECTIVE RECRUITMENT


Memory Load2 6 2 6
500
750
1000
1250
1500
Young Old
React
ion
Tim
e (
mse
c)

FASTEST SLOWEST
YOUNG
OLD

Summary
• Age-related decline in selective cognitive processes
• Functional MRI is a powerful method with excellent spatialand temporal resolution to study the physiological basis ofcognitive decline in normal aging
• Evidence for selective prefrontal cortical dysfunction(I.e. under-recruitment) with normal aging
• Possible neural as well as behavioral compensation

Questions
• What is fMRI? What is it used for and how does it work?
• What area of the brain has been shown to have change in older people?

AGING OF THE NERVOUS SYSTEM—FUNCTIONAL CHANGES
Again, in the normal aging brain the changes are relatively few. However impaired function and
increased pathology do occur. Major functional deficits/ pathologies involve:
Motility (e.g. Parkinson’s Disease)
Senses and communication
Cognition (e.g. dementias)
Affect and mood (e.g. depression)
Blood circulation (stroke, multi-infarct dementia)
Parkinson’s Disease: Chapter 8, pp. 110-113Dementias: Chapter 8, pp. 130-136

Dementia
• Dementia: global deterioration of intellectual and cognitive function characterized by 5 major mental functions:– Orientation
– Memory
– Intellect
– Judgment
– affect
– (But clear consciousness)

Dementia (cont.)
• There are two types of dementia:– Reversible– Irreversible

TABLE 8-7 Underlying and Reversible Causes of Dementia
D Drugs E Emotional disorders M Metabolic or endocrine disorders E Eye and ear dysfunctions N Nutritional deficiencies T Tumor and trauma I Infections A Arteriosclerotic complications
i.e., myocardial infarction, stroke or heart failure


Table 8-10 Selected Characteristics of Alzheimer’s Dementia
Anatomo-Histology Pathology Metabolism
Brain atrophy, flattening of gyri, widening of sulci,
& cerebral ventricles
Loss of cholinergic neurons, in nucleus of Meynert,
hippocampus & association cortices
Loss of adrenergic neurons,
in locus ceruleus
Denudation of neurons, stripping of dendrites,
damage to axons
Increased microglia
Accumulation of cell
inclusions: lipofuscin, Hirano and Lewy bodies,
altered cytoskeletal Tau proteins,
ubiquitin
Neurofibrillary tangles, neuritic plaques with
amyloid,
Perivascular amyloid, distributed throughout the
brain, but especially in frontal, prefrontal lobes,
Hippocampus, association cortices
Decreased oxidative
metabolism, slower enzyme activity (Ch. 7)
Free-radical
accumulation (Ch. 5)
Impaired iron homeostasis (Ch. 7) Other minerals, zinc,
aluminum
Reduced level/ metabolism/ activity of
neurotransmitters
Increased amyloid peptide with accumulation of
amyloid proteins
Increased prion protein
Altered immune response

TABLE 8-9 Characteristics of Multi-Infarct Dementia
History of abrupt onset or stepwise deterioration History of transient ischemic attack or stroke Presence of hypertension or arrhythmia Presence of any neurologic focal symptoms or signs

Amyloid Connections
• In Alzheimer’s, amyloids are made and accumulate in brain tissues and cause disturbances.
• Maybe these could be a point of intervention to prevent progression of alzheimers.

Characteristics of Multi Infarct Dementia (table 8.9)
• Transient ischemic attack or stroke
• Hypertension, arrythmia
• Focal neurological signs
• Stepwise deterioration

Questions
• What are the causes of reversible dementia?
• What are the characteristics of multi-infarct dementia?
• What are the major functional deficits/pathologies in aging?

Aging of the Visual System

Definitions
• To look at a near source, the lens has to accommodate (become more round); to look at a far source it doesn’t have to accommodate.
• Myopia: nearsightedness because eyeball is too long or lens is too strong. Corrected with concave lens.
• Hyperopia: farsightedness due to eye too short or lens is not strong enough. Corrected with convex lens
• Presbyopia: loss of focusing power of lens because it has stiffened—results in difficulty seeing objects close up which necessitates lens to accommodate.

Aging of the Visual System• Structural Changes (See handout given in class)
– Tear Film: • Dry eyes or tearing
– Sclera: • Fat deposits – yellowing
• Thinning – blueing
– Cornea• Diameter does not change after age 1
• Shape changes
– Retina• Photoreceptor density decreases; other layers become disordered
(rod density decreases with age, cone density remains)
• Illuminance decreases with age
– Lens• Increased size and thickness
• Becomes more yellow
Aging of the Visual System• Function
– Corneal and Lens• Decreased accommodation power (loss of presbyopia: loss of
focusing power of lens because it has stiffened—results in difficulty seeing objects close up.)
• Increased accommodation reflex latency• Refractive error becomes more hyperopic with age• Corneal sensitivity decreases• Scatter increases
– Pupil• Size decreases with age, particularly for dim light conditions.

Aging of the Visual System
– Retinal (MANY changes due to decreased amt of light reaching retina)• Decreased critical flicker frequency• Visual acuity declines• Visual Field decreases• Color vision changes• Darkness adaptation is slowed• Increased glare problems, longer time to recover from glare• Decreased light reaches retina• Visual acuity declines most with age when tested in low contrast with dim
light. The difference as compared to young people is very significant in this case. (not as significant if tested with high contrast, bright light)
• Attentional visual field size decrease• Stereopsis (close-up depth perception) shows large loss with age due to
difference in function of 2 eyes. • Face recognition impaired

Other changes
• Words per minute decrease in reading
• Increased hyperopia: (farsightedness because eye is short)
• Increased astigmatism (cornea of eye is asymmetrically curved causing out of focus vision)

Graph from handout—summary of some main points
• Most change with age in:– acuity in glare 18x worse with aging– Next: glare recovery 15x– Next: attentional field 12x– Etc…

Aging of the Visual System
• Recommendation to Accommodate Problems: (she didn’t discuss in too much detail, but good to know)– Wear appropriate optical correction– Increase ambient light– Make lighting even and reduce glare– Improve contrast in critical areas– Avoid rapid changes in light level– Avoid Pastel– Allow more time