tinnitus today september 1997 vol 22, no 3
TRANSCRIPT

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 1/31
September 1997 Volume 22, Number 3
Tinnitus TodayTHE JOURNAL OF THE AMERICAN TINNITUS ASSOCIATION
"To promote relief, prevention, and the eventual cure of tinnitus for
the benefit of present and future generations"
Since 1971Research- Referrals- Resources
In This Issue:Tinnitus and
Homeopathy
Back to School -
Children and Tinnitus
Fad Diets, Quick Fixes,and Tinnitus
New PET Research
7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 2/31
'11/1111
/ l j , j ; / ~ ( 1 !

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 3/31
Tinnitus T o d ~ y Editorial an d Advertising offices: American
Tinnitus Association, P.O. Box 5. Portland,
OR 97207, 503/ 248-9985, 800/ 634-8978,hu pJ I w1"w.telepon.com/ NilW
Execuuve Director & Editor·
Gloria E. Reich, Ph.D.
Associate Editor: Barbara Thbachnick
Ton111rus 7bday is published quarterly in
March, June. September, an d December: It ismailed to members of the American TinnitusA ~ s o c i a t i o n an d a selected list ot tinnitus sur.
fcrcn> an d professionals wh o treat tinnitus.
Cn·wlation is rotated to 75,000 annually.
Th e Publisher reserves the right to r c j ~ c t or
edit an y manuscript received for publication
,111d to reject an y advert1s1ng deemed unsuit·
~ b l e for nnmtus 7bday . Accept.mcc of adver·
tt<ing by Tmnuu.s 7bday does not constitute
endorsement of the advertiser, 1ts products
or ! l e r v i t e ~ . no r does Tlnntt!AS 7bday make
an y cla1ms or guarantees to the accuracy
or validity of the advertiser's offer. Th e
opinions expressed by contributors toTmmrus 7bday are not necessarily those ofthe Publisher, editors, staff, or advertisers
American Tinnitus Associauon is a non·
profit human health and welfJre agency
under 26 USC 501 (c)(3)
Copynght 1997 by American Tinnitus
A<'<Ociation . No pa n of th1s publication may
be reproduced, stOred in a retrie1•al system,
or transmmed in anv form, or bv anv means.
wnhout the prior w;itten permission of the
Pubhsher ISSN: 0897·6368
ScientificAdvisoryCommitteeRonald G. Amedee, M.D., New Orleans. LA
Robert E. Brummett. Ph.D., Portland, OR
Jack D. Clemis. M.D. , Ch1r.ago, IL
The Journal of the American Tinnitus Association
Volume 22 Number 3, September 1997
Tinnitus, ringing in the ears or head noises, is experienced by as many
as 50 million Americans. Medical help is often sought by those whohave it in a severe, stressful, or life-disrupting form.
Table of Contents7 Fad Diets, Quick Fixes, and Tinnitus
by Robert Sweetow, Ph.D.
8 Books at a Glance
by Barbara Thbachnick
9 New PET Research Study of Auditory System
10 Tinnitus and Homeopa thy- My View
by Stephen M. Nagler, M.D.
12 Back to School
by Barbara Thbachnick
14 New ATA Support Network Volunteers
15 ATA's New Board Members16 Announcements

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 4/31

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 5/31
Letters to the Editor
From time to time, we include letters from ourmembers about their experiences with "non
traditional• treatments. We do so in the hope that
the information offered might be helpful. Please
read these anecdotal reports carefully, consult with
your physician or medical advisor, and decide for
yourself if a given treatment might be right for you.
As always, the opinions expressed are strictly those
of the letter writers and do not reflect an opinion orendorsement by ATA.
A a thirty-year tinnitus sufferer, I apprecited Barbara Thbachnick's article on
earing protection aboard airplanes
(June 1997 Tinnitus Tbday). Since I am a professor, I need to fly frequently to attend academic
conferences and always dread i t for fear that
the noise might worsen my already bad ringing.For years I have used foam earplugs of the typeshe recommends. These help some, but they failto cut out the loud low drone of the engines.However, there is a solution: noise cancellationheadphones. I have tri ed several brands and findthat, although all work well, the "Noise-BusterExtremes" work best and are fairly cheap. They
can be purchased from Heartland Americafor $69. (800-229-2901 ). Believe me, once you
try them, you'll never fly (or drive) without
them again!Dr. William Fu.sfield, Pittsburgh, PA
[Editor's Note: According to a United Airlines
spokesperson, major U.S. airlines require passen
gers to turn off all electronic devices during takeoff
and landing, regardless ofa device's electrical output. Noise Cancelation Technologies (NCT), manu
facturer ofNoise-Buster Extremes, claims that this
device should not interfere with critical airplane
controls. However, they cannot state it unequivocal
ly. NCT concedes that it might be hard to convince
flight attendants to allow you to wear any electrical
device during takeof fand landing.]
A!chnique for abating the annoyance of
mnitus, which I have had for most of
y life (I am 67 now) was taught to me
about 20 years ago during a human potentialseminar I attended. The technique was supposed to temporarily sharpen hearing, but Ifound it helpful for my tinnitus. Here it is: The
lower part of the palms of each hand are placed

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 6/31
Letters to the Editor (continued)
over both ears in such a way that virtually no
noise can get through. Fingers are pointing tothe back. The index finger is then used to
thump on the bone at the base of the skull. I t
will sound like a not-unpleasant pounding on awall. I thump with the finger from each hand
simultaneously about 50 times.
Even i f he tinnitus sound doesn't diminish,
there is a considerable immediate sense of relief
that lasts for awhile. The technique doesn't
work as well for me as it did 20 years ago, but
there were many occasions when I thought this
was one of the more valuable coping things Ihave learned.
Otherwise, losing some of my hearing and
the tinnitus have no t prevented me from enjoy
ing an active, productive life about which I feel
most grateful.Murray Cohen, Delphos, OH
I ot a good laugh from J a ~ e d M c L a ~ g h ~ i n ' s letter in the March 1997 1ssue of Tinmtus
Tbday. I'm too old to take up the bag pipes,
but he's right - it's a great "masker."
Marlea Rice Warren, St. Louis Park, MN
ving recently completed my experimental tinnitus therapy, coordinated by
E even years ago I was diagnosed with tinnitus (the intermittent, one-note whistle
variety). I was told there was no known
cure. 'IWo years later, while under chiropractic
care for a slightly herniated disk, I was advised
to take lOOmg. of manganese sulfate and 300mg.
of B-complex daily. This helped my back but
surprisingly cured my tinnitus completely with
in a month. The tinnitus would return only if Istopped taking the manganese. I gradually low
ered the amount as the tinnitus episodes abated.
Thday, I have been tinnitus-free for nine
years and only rarely take manganese. This
"anecdotal cure" also worked for my husband'stinnitus. Dr. Lendon Smith suggests, in his book
Feed Yourself Right (Dell Publishing Co., 1983),
that manganese "five to lOmg. a day for a monthor two" might help nervous tissue.
Barbara Carlson, Ottawa, Ontario, Canada.
Thank you for your very well-written
article, "Air Bag Ruling? - Still Up in the
Air" in the June 1997 issue of Tinnitus
Tbday. I have written to NHTSA several times to
ask that our government require automobile
manufacturers to do the research and development necessary for the production of an air bag
7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 7/31
Fad Diets, Quick Fixes, and Tinnitus
by Robert Sweetow, Ph.D.
There are two conditions affecting millions
of Americans that most of us will go to great
lengths to avoid. One, as all the readers of this
publication are aware, is tinnitus. The other is
obesity. Obesity and some of the medical prob
lems that result from it (like hyperlipidemia)
have been associated with tinnitus. Thus, many
tinnitus patients have tried a variety of diets inwell-intentioned efforts to control their weight
and "get healthy." Recently, one of my tinnitus
patients, who has made a wonderful adaptation
to the symptom, phoned me in a minor panic
because his tinnitus had suddenly increased
"tenfold." One week later, the tinnitus returned
to its baseline. The apparent culprit was the diet
medication he started just before a t rip overseas.Once he stopped taking the pills, the tinnitus
decreased within three days. He asked me to
look into a possible relationship between the
diet and tinnitus.
Ironically, two days after I began my investi
gation, this diet hit the front pages. My patient
was one of over 18 million people who have
taken the very popular Fen-Phen diet medications since 1990. On July 8th of this year, it was
The point of all this is that tinnitus patients
should proceed with fad diets (and, for that mat
ter, any unproven "cures" for tinnitus) with
extreme caution. There is no long-lasting, quick
weight loss scheme. If you lose weight fast, and
then return to your previous eating habits, the
pounds will inevitably return. Long-term exer
cise and reduction in calorie intake is generally
essential. In other words, a behavioral and psy
chological modification must be made. Tinnitus
"cures" will likely meet with similarly short-lived
fates unless you also alter previous behavioral
patterns, including exposure to noise, exposure
to silence (equally as aversive), and make a psy
chological adjustment to your symptom, recog
nizing that regardless of where the tinnitus
originates from, it is the brain that ultimately
perceives it. Thus, you and your health profes
sional must work together toward developing a
strategy to alter your reaction to your tinnitus so
that you might facilitate eventual habituation.
AIRBAGS.. .
Still Waiting

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 8/31
Books at aGlance
by Barbara Thbachnick, Client Services Manaverb
Clinical Otology, by Gordon B. Hughes and
Myles L. Pensak, 1997.
Thieme Medical Publishers, Inc., The MaplePress Distribution Center, I-83 Industrial ParkPOB 15100, York, PA 17405. Hardbound I480 pages, $139.
This large, glossy, colorfully illustrated book
is a collection of material by clinicians for clinicians. Two chapters focus on tinnitus. The chapter on non-pulsatile tinnitus by Richard H.Nodar and Thny L. Sahey is a short primer on
case history-taking, evaluating tinnitus mecha-• I
msms of tinnitus, and consulting with patients.The authors advise clinicians to approach tinnitus patients with compassion, to acknowledge
how distressing the condition can be, and i f apatient appears to be at "the very edge of control" to gently ask if he or she would like a referral for counseling. The authors admit that thischapter only scratches the surface of a complexand distressing auditory experience.
Aristides Sismanis delineates the multiple
causes of pulsatile tinnitus in a very technical
and thorough chapter replete with diagrams an d
photographs. The various forms (vascular and
authors . Tinnitus is no t specifically mentioned,?ut t r a u m ~ t i c brain injury is. This type of injuryIS the leadmg cause of death and disability in
the United States for individuals age 40 and
younger. Head trauma has been cited as a com
mon cause of tinnitus.
Hearing Loss, by Peter S. Roland, Bradley F
Marple, and William L. Meyerhoff, 1997.Thieme Medical Publishers, Inc., The Maple
Press Distribution Center, I-83 Industrial ParkPOB 15100, York, PA 17405. Hardbound,
316 pages, $69.This book gives strong focus to the ear's
physiology and what can go wrong with it.Multiple contributors discuss disorders of the
outer ear, tympanic membrane, mastoid, middleear, and inner ear. Vestibular disorders an d rehabilitation are also discussed at length. Tinnitus
is mentioned twice - one paragraph defining itand its relationship with hearing loss, and
another explaining the benefits of hearing aids,maskers, an d tinnitus instruments (hearing aidand masker in one unit). Audiologic tests, like
auditory brainstem response (ABR), electrocochleography (ECoG), an d otoacoustic emissions (OAEs) are clearly explained. This highly

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 9/31
New PET Research Study of
Auditory SystemThe University at Buffalo recently received a
$107,000 grant from the James H. Cummings
Foundation of Buffalo to fund a pioneering
research project that will look at how the brain
transforms the sounds we hear into information.
This three-year study will combine images ofbrain activity using Positron EmissionTomography (PET) scans with images of structures in the brain acquired through MagneticResonance Imaging (MRI) to create a unique
image that links neural activities to specificbrain sites. Through the combined images,researchers hope to gain new insights into how
sounds relayed by the auditory system areunderstood.
Directed by Alan Lockwood, M.D., professorof neurology, the multi-disciplinary project willinvolve the departments of nuclear medicine,neurology, communicative disorders and sciences, linguistics, psychiatry and rehabilitationmedicine, and the Faculty of Social Sciences.
Also participating is the Department of VeteransAffairs through the VA Western New York
between sound and the emotion centers in thebrain, we may also be able to better understand
hearing loss and disorders such as tinnitus or
'ringing' in the ears, which is associated with
adverse psychological symptoms such as depres
sion, anxiety and insomnia." This study willcompare the auditory function of "normal hearing" subjects with that of subjects affected by
various hearing disorders. Lockwood and
Richard Salvi, Ph.D. recently received an ATA
grant to study the neural basis of subjective tinnitus using Positron Emission Tomography.
Unlike other imaging technologies, PET
scans produce images of the body's functionsrather than its structure. Magnetic ResonanceImaging provides a detailed three-dimensionalimage of anatomical structures.
Using newly installed MRI equipment and
powerful computers in the VA Medical Center,the researchers will combine the MRI and PETimages to map the functions observed in the
PET scans onto precise locations in the bodyindicated by the MRI images. Part of the funds

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 10/31
Tinnitus and Homeopathy
MyViewby Stephen M. Nagler; M.D., FA.C.S.
The question regarding the appropriateness
of homeopathic approaches to tinnitus management frequently arises. I thought I might try to
shed some practical light on it from a Western
medicine perspective.First of all, it is important no t to confuse
homeopathic medicine with holistic medicine -
an easy mistake to make because the words start
and end with the same phonetic sounds.
Holistic medicine is based upon the theory that
an organism is not merely equal to the sum of
its parts, but must be perceived or studied as a
whole. This particular philosophy has a lot ofappeal to me for many reasons, not the least of
which is demonstrated by the general observa
tion (and my professional experience) that if apatient has a good relationship with his/her surgeon and has a good self-concept, that patient
tends to recover more quickly from a givenoperation than one who does no t.
Homeopathy is something entirely different.I t is based upon the "law" of similia (likes are
who use "extracts" to build up resistance to,
for instance, various pollens. There are two
differences:1. The pollens from which the extracts are made
elicit no symptoms in healthy individuals -
only in individuals with allergies to the pollensin the first place.2. The dilutions used by homeopaths are purer
than distilled water. Distilled water theoreticallyhas less than 1 part in 109 in impurities- or one
part per billion. Homeopaths frequently usedilutions as pure as 1 part in 10 100
- or one part
per billion billion billion billion billion billion
billion billion billion billion. That dilution mathematically has been judged roughly analogous to
placing a crushed grain of rice in a pool of pure
water the radius of which is the distance fromthe sun to Pluto - then drinking a glass of the
solution to get the effect of the rice. (With this
in mind, whether or not homeopathic remedieshelp you, i t seems highly unlikely that they can
hurt you.)The problems that many of us who practice

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 11/31
Tinnitus and Homeopathy (continued)
Since I question the basis of the theory and
since simple double-blind experiments have not
been done to any statistical satisfaction, I find it
difficult to recommend homeopathy as a treatment for tinnitus. Still, some tinnitus sufferers
report that homeopathy occasionally seems to
help them. This observation is termed "anecdo
tal evidence" - a phrase that unfortunately car
ries a lighthearted connotation. But there is
nothing remotely lighthearted about a treatment
that might in certain circumstances be benefi
cial in alleviating the discomfort oftinnitus. In
my experience: No tinnitus sufferer who found
even a small amount of relief ever cared one iota
whether or not the treatment which resulted in that
relief was based on "science. n (Nagler's Law.)
So,how does a reasonable person reconcilethe above apparently conflicting positions - no
scientific basis or solid evidence vs. anecdotalreports of successful treatment? And what posi
tion should a responsible health care profession
al take when faced with this question?
Doctors who state that they depend strictly
on the results of double-blind randomized
prospective studies when they make recommen-dations to patients are either naive or forgetful.Most of us have tricks that "seem to work well
indicated, and in general developing a meaning
ful relationship with the afflicted. This sounds
like what M.D!s used to do years ago beforesome began to sacrifice time at the "bedside" for
quantity of patients treated. Whether this grad
ual change in posture in modern American
medicine is a result of the onslaught of managed
care, or economic reality, or advancing science,
or just plain greed (I suspect a combination of
each), many of our patients have ultimately had
to pay the price. To the homeopath's credit, no
significant compromise has been made withrespect to the time spent with each patient.
Herein might lie the answer to the homeopath's
occasional anecdotal success.
The philosophy of homeopathy cannot readi
ly be measured by traditional double-blind randomized prospective methodology, which may
in part explain the reluctance of the homeopath
ic community to subject their treatment proto
cols to this type of rigorous testing. It does not,
however, explain the reluctance of the homeopathic community to report even retrospectively
specific success rates backed by good data.
If a tinnitus patient told me that he hadexperienced success with homeopathy foranother ailment and wanted to include a home
7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 12/31
Back to School
by Barbara Tabachnick, Client Services Manager
I walk into the second grade classroom laden
with a large and mysterious cardboard box.
Despite their curiosity, the seated children there
ask no questions and I give no clues. I put the
box down, take ou t a video and put it in the
VCR. I do not press the "play" button just yet.
With the teacher's permission, I erase some
space on the blackboard then wait to be intro
duced. "I have an important question for you,"I begin. "How many of you have ears?"
I can tell by the giggles and the 25 hands
that shoot up in the ai r that this is not going
to be a tough crowd. I continue, "Oh good. I
came to the
right room . Ihave another
question: How
many ofyou
like your ears?"All hands shoot
up again. I
smile and take
a long, hard
look at the
young faces - and at the trust written all over
them. These eight-year-olds are ready to learn
hearing aids but won't. And some children have
tinnitus - intermittent, pulsatile, and sometimes constant to the point that they cannot
sleep at night. Alarmingly, their parents don'talways know. Also alarming is the data I unwit
tingly gather: an average of two children per
classroom confide in me that they have tinnitus.
Children With Tinnitus
The actual number of children with tinnitusis not known, and for a number of very goodreasons: Children have a difficult time convinc
ing adults of their condition. Children are often
afraid to tell adults that they hear noises.
Children who are born with tinnitus have no
frame of reference and do not know that it is
un usual. When children are given hearing tests,
they typically give positive answers to pleasethe testers. (This makes it hard for testers to
identify what children really hear.) Children alsolikely under-report the condHion because their
busy and distracted lifestyles help them get past
the problems associated with tinnitus.
Dr. Richard Nodar conducted a study in
1972 to approximate the prevalence of tinnitus
- - - - - - - - - - in children.Ofthe 2000
7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 13/31
Back to School <continued)
In another study, Graham found that only two
out of 78 hearing-impaired school-age children
with tinnitus reported their tinnitus to be con
stant. "This suggests," he writes, "that where the
electrical'-' ' activity asso-
ciated with
tinnitus has
been present
since birth, it
generally
needs to be
intermittent
to be per
ceived."
Researchers speculate that children's intermit
tent tinnitus might become constant when they
reach adulthood.When it comes to avoiding environmental
noise, like the kind in school gyms or movie
theaters, children have relatively little power -
and they know it. I encourage them to exercise
that power anyway, however slight it might be .
"Ask for your world to be quieter. Ask for the
noise to be turned down. Grown-ups are out
there asking too," I assure them. "We can'tchange everything, but we can change some
message across and short enough to ge t it across
before we lose our audience's attention. We ask
questions, draw on the board, watch a video, do
an earplug demonstration, play a game. Every
week from September through June, we present
the program to a different school. And by
request, we send Hearing Conservation kits tovolunteers across the U.S.
Teaching is a slow process. I t is also won
drously rewarding. Thousands of children arenow putting earplugs in their ears properly (or
close to it) who had not done so before. Childrentell us that now they understand why their ears
ring after they go to basketball games. One
seven-year-old who complained about his broth
er's loud stereo before the presentation said to
me excitedly afterwards, "I know what I'll do. 1'11tell him to TURN IT DOWN! But I'll have toshout it, 'cause if I don't, he won't hear me."
How critical is it that we disseminate this
information? Completely. Children and their
parents, grandparents, and teachers are still in
the dark about the unforgiving consequences of
excessive noise: permanent hearing damage,
tinnitus, learning disabilities, other health ills,and the concomitant damage to the emotionalwell-being of everyone concerned.

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 14/31
Back to School (continued)
ResourcesBoodman, Sandra G., Researchers say airplane noise curbs
reading skill, The Washington Post.
Gabriels, Pam, Children with tinrtitus, Proceedings
of he Fifth International Tinn itus Seminar, editors,
Gloria Reich and Jack Vernon, 1995.
Graham, J.M., Tinnitus in hearing-impaired children,
Tinnitus, 1987; 131-143.
Graham, John, Paediatric Tinnitus, Journal of Laryngology
an d Otology, Supplement 4, 1981; 117-120.
Graham, John, and Jane Butler, Tinnitus in children,
Joumal of Laryngology and Otology, Supplement 9, 1984;236-241.
Mills, R.P., and D.M. Albert, C.E. Drain, Tinnitus in child
hood, Clinical Otolaryngology, 1986, l l ; 431-434.
Nodar, Richard H., Tinnitus aurium in school age children:
a survey, Journal of Auditory Research, 1972; 12, 133-135.
Nodar, Richard H., and Mary H. W. LeZak, Pediatric titmitus
(a thesis revisited), Journal ofLaryngology and Otology,
Supplement 9, 1984; 234 -235.
Stouffer, J.L., and R.S. 1Jier, J.C. Booth, B. Buckrell,Tinnitus in normal-hearing an d hearing-impaired children,
Proceedings o f he Fourth International Tinn itus Seminar, edi
tors, Jean-Marie Aran and Rene Dauman, 1991.
How can you get the free
Elementary School
NewATA Support
NetworkVolunteers
Support groups commonly reassemble in thefall after their summer hiatus. This fall, several
new groups are beginning too. Welcome back,
and welcome all!
The Tinnitus Support Network is designed
to offer one-on-one contact between those
who have found treatments and coping ski11s
that work and those who are still looking for
answers. Thousands of people use this resourceevery year.
Are you ready to help others? Please let
us know. We will gladly send you a packet of
materials to help you become a telephone
contact or support group leader.
New Support Group Leaders
Sharon Weinhaus
425 E. 58th St. #40B
New York, NY 10022
212/758-0791
Larry Maurer
9680 Glenstone Dr.
Kirtland, OH 44094
216/256-8023
Edna Young
1808-C N.W O'Brien Rd.
Lee's Summit,
MO 64081
816/246-4644
(near Kansas City)
Mitzi Cahn
1439 Bonita Ave.
Berkeley, CA 94709510/527-9075
7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 15/31
ATA's New Board MembersStephen Nagler, M.D.,
F.A.C.S.
Dr. Nagler writes:
"After my graduation in
1975 from Northwestern
University Medical School,I completed an internship
and residency in GeneralSurgery and surgical subspe
cialties. I am a Diplomate ofStephen M. Nagler, M.D. the American Board of
Surgery and a Fellow of the American College of
Surgeons. As a surgeon, I am intimately familiar
with the physical impact of disease as well as its
emotional consequences upon patients and their
loved ones."Prior to becoming Director of the new
Southeastern Comprehensive Tinnitus clinic, Ispent two years studying the anatomy, physiolo
gy, and pathology of the auditory system as they
relate to the etiology of tinnitus and the efficacyof various treatment modalities. I have lectured
on numerous tinnitus-related topics - includingthe multi-modality approach to tinnitus patient
management, the role of pharmacologic agentsin tinnitus therapy, and the place of hypnosis in
tinnitus treatment.
Sidney Kleinman
Sid writes:"I believe that each day is a'gift,' sometimes wonderful
and marvelous, and some
times no t so great. But it isa gift to be enjoyed and
experienced. Furthermore,one cannot just take from
the World and Life in aSidney Kleinman
narcissistic manner. One
must give back and try to assi st others.
"As a result, throughout my professionalcareer, I have always made a commitment toothers as - among other roles - a volunteer
working with emotionally disturbed teenagers; avolunteer attorney representing rent strike build
ings in Chicago's inner city; a co-founder of achamber symphony; an active member of theAdvisory Board of the DePaul University School
of Music; and now as a member of the Board of
the American Tinnitus Association."It is my hope that I will be able to assist ATA
in its role as the advocate for th e silent tinnitussufferers of this country - in advancing continue d research to find the mechanisms of tinnitus
and the means to ameliorate its symptoms -

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 16/31
Announcements
ATA To Receive $5000 FromBarry Manilow
As the result of a court settlement, BarryManilow - the man who "writes the songs" -has also written a check to ATA. Philip Espinosa,an Arizona Court of Appeals judge and ATA
member, brought suit against the famous performer after a 1993 concert left him with severe
tinnitus. "I expected soft amplified music,"Espinosa stated, but the music was too loud and
he now has a constant "screeching" in his ears.
While neither Manilow nor his production
company admits any fault, Espinosa believes the
suit will be helpful in raising consciousnessabout the serious problem of high volume levelsat entertainment events. "Unfortunately in our
society, large industries like the music business
do not listen to you unless you file a lawsuit,"he said. "It (the money) is not a large amount
in terms of a permanent injury, but it's a very
significant amount for the American Tinnitus
Association."
MedWatchThe U.S. Food and Drug Administration
(FDA) has a way for the public to confidentiallyreport problems with any medication (prescrip
a recognized pioneer in tinnitus research. In thisvideo of that lecture, Dr. Vernon discusses theorigins of tinnitus treatment and the contemporary applications of masking, hearing aid use,and other treatments for tinnitus remediation.His formidable knowledge, practical experience,and gracious manner highlight the hour.
Cost.· $20 (shipping included), Running time: 59minutes, 20 seconds
Send check to: OHSU, Office of Community
Relations, Attn: Thrry Erb, 3181 Sam Jackson
Park Rd., L101, Portland, OR 97201-3098
The Third Course on Tinnitus
Retraining Therapy for Management of
Tinnitus & HyperacusisSeptember 28-30 1997Organizers: Pawel J. Jastreboff, Ph.D., Sc.D., and
Margaret M. Jastreboff, Ph.D.Tinnitus & Hyperacusis Center, University of
Maryland, Baltimore, MD 21201 USA
This course will cover the following topics:+ An outline of common methods for treating
tinnitus and hyperacusis
+ Theory and clinical implications of ourapproach

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 17/31
Back Issues of Tinnitus TodayYour interest in Tinnitus Tbday back issues
has been tremendous. Thank you!The following is a list of the featured topics
in each issue. Almost every issue contains ·Dr. Jack Vernon's Q & A column, information
about self-helping, research updates, and (fromSeptember 1994 to the present) Letters to the
Editor.
The cost per issue:$2.50 (member price); $5.00 (non-member price)See the table below for shipping cost.For orders outside the U.S., please add $5to the total shipping cost.
Supplies are still ample for most issues
listed. A few, however, are available only as
photocopies. Every effort will be made to send
the originals.
J une 1997 Barometric Changes and the Ear;Elderly People and Tinnitus; Air Bag update
March 1997 NIDCD-funded Tinnitus Research,Treatments for Subjective Tinnitus; Similaritiesbetween Tinnitus and Chronic Pain; Air Bagupdate
Dec. 1996 Air Bag Safety- Air Bag Risk;
Interview with researcher Jos Eggermont, Ph .D.Sept. 1996 Ototoxic medications; Silent Dental
September 1993 How Tinnitus is Generated;
HypnosisJune 1993 1Jpes of Hearing LossMarch 1993 Anatomy of the Ear; Researchreport (PHOTOCOPIES ONLY)
December 1992 TMJ
September 1992 Industrial Liability CaseJune 1992 ATA history; Monitoring YourTinnitus
March 1992 Interaction of Earmold Acoustics,Real Ear Resonances, and Tinnitus MaskerResponsesDecember 1991 Fourth International Tinnitus
Seminar; Personal Injury lawsuitsSeptember 1991 Tinnitus in the Nursing
Home; Research report; Cochlear Implants
June 1991 VA Info; Hyperacusis; Researchhighlights (PHOTOCOPIES ONLY)
March 1991 Noise and Tinnitus; There is Hope;Tbny RandallDecember 1990 Tinnitus Measurement; Drug
Therapies
September 1990 Older Americans and
Tinnitus; Research Report; ADAJune 1990 Cognitive Therapy; AmplificationMar ch 1990 Noise-induced Hearing Loss in
Musicians; Vestibular Disorders; Tinnitus in the
14th CenturyDecember 1989 Tinnitus Patient Management;

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 18/31
ATXs Passport to Progressby Cora Lee (Corky) Stewart,
Program Development Director
While i t is often fun to impulsively take off
on a quick trip to an undetermined destination
a real journey requires careful planning. YouI
need to know where you are going, how you
will get there and, perhaps most importantly,
why you are going there. For the past year, the
ATA Board of Directors and staff members havebeen planning what could be classified "a major
journey" for ATA. As such, it's bound to be the
trip of the century, so hop on board for ATA's
Big Adventure.
What I'm referring to is, of course, ATA's
Strategic Plan, which sounds like a rather boring
business document bu t is really an exciting
itinerary that defines ATA's direction, approach,and focus for the next five years. On July 1 (the
start of this fiscal year), the Plan became our
roadmap.
This is not to imply that ATA has been drift
ing aimlessly; far from it - as a non-profit
organization, i t is in an enviable position. With
a diverse membership, it is financially stable,
recognized internationally as a credible sourcefor tinnitus information, and is the leading advo
formed an incredibly intense inspection of
everything ATA has done and wants to do· what
similar organizations are doing; and what needs
aren't being met in the tinnitus arena at large.They agreed, disagreed, discussed, and even
cussed. But the result is a clearly defined Planfor ATA, complete with measurable objectives,
workable projects, and reachable time lines.
The good news is that there was consensuson the major points and considerable validation
of much of ATA's past activities. The bad news is
that we had to accept the fact that our resources
are limited and we can't continue to be allthings to all people. This clarity of focus is
reflected in the new ATA mission statement:
Th promote relief, prevention and the eventualcure of tinnitus for the benefit of present and
future generations.
Naturally, finding a cure for tinnitus was
(and is) the number one priori ty for everyone,so investing i n - and advocating for - research
will continue to be the most important compo
nent for ATA. And until the cure is found, there
is clearly a continuing need for an organization
that provides programs tohelp people
avoid getting tinnitus and that supports those who have
it. Thus we've ended up with the EARS Plan

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 19/31
AMERICAN TINNITUS ASSOCIATIONStrategic Plan- July 1997 through June 2000
Mission:
PROGRAM S:
7b promote relief, prevention, and the eventual cure of tinnitus for the benefit ofpresent and future generations
Education Goal: To further awareness and understanding of tinnitus through education
Thrgets: Hearing health professionals, primary care physicians, general public'Ibols: Tinnitus Today and ATA brochures, professional workshops, workplaceand classroom seminars, exhibits at conventions, targeted mailings, media
placementsMeasurements: Currently there are no statistics pertaining to actualawareness of tinnitus, so the first step will be to conduct a survey to establishbenchmarks. (Education efforts work: In 1986, patients were told to "learn to
live with it" ahout 83% of the time. By 1996, the figure was down to 74%.Similarly, in 1986 only 33.7% felt their physicians were helpful, but that
improved to 58.2% by 1996. In 1986, only 31% of the people surveyed had tried
any form of tinnitus treatment. By 1996 that number had jumped to 60%.)
Advocacy Goal: To advocate for tinnitus in the development and implementation of
public and private policies'Ibols: Participation in federal meetings and policy making for the NationalInstitute on Deafness and other Communication Disorders (NIDCD) or similaragencies; direct contact with health insurance providers and with manufacturers
of noisy products.Measurements: While 83.7% of the respondents to ATA's 1986 survey receivedpartial or complete insurance coverage for their tinnitus treatments, claimprocessing is often complicated and sometimes litigious. ATA will work to
establish a liaison/advisory role with major insurers to improve this situation.Many manufacturers of noisy products provide cautionary information, but few
7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 20/31
Questions and Answers
by Jack A. Vernon, Ph.D.
[Q]Mr. S. from Hawaii writes to report an
unusual aspect about his pulsatiletinnitus. He indicates that his pulsatile
tinnitus can be 99% eliminated by extendedneck flexion, that is, placing the chin firmly on
the chest. What, he asks, is the possible mean-
ing of this effect?
It may mean that the pulsatile tinnitus
is coming from a partial occlusion in the
carotid artery and that the neck flexioncauses that blockage to be somehow relieved.Mr. S., may I ask you i f any physician has
listened to your neck region to see if he or she
can hear your pulsatile tinnitus? You describe it
as a high-pitched whine, thus the listener would
need to have good high frequency hearing inorder to detect your pulsatile tinnitus. If your
pulsatile tinnitus is an objective tinnitus
(detectable by others), then a surgical exploration of the neck region using temporary liga
tion (a tying-off) of the possibly offending artery
may lead to a cure for you. Note that this is amajor procedure! I do know of one case where a
surgeon did essentially that. With a stethoscope,the surgeon explored the opened neck area and
There is a significant difference between
pink noise and white noise. White noisecontains all frequencies from 20Hz
through 20,000Hz. Pink noise contains frequencies from 200Hz through 6000Hz. The purpose
of the listening exercise is to establish normalloudness tolerance for everyday ordinarysounds. Remember hyperacusis is no t the lowered threshold for sound detection but rather it
is a collapse of loudness tolerance. The usualsounds to which we are exposed are composed
of frequencies from around 200Hz to around
4000Hz. Also recall that hyperacusis is inverselyrelated to the pitch of the sound: The higher thepitch, the less the loudness tolerance. Sometime back, a patient in our hyperacusis treatment program questioned our use of white
noise for desensitizing hyperacusis ears on thegrounds that the high frequency portion of the
white noise would delay the recovery process.Instead the patient suggested that we use pinknoise which contains those frequencies foundin normal environmental sounds and does notcontain the high frequencies. Our patient'sreasoning seemed reasonable to us and we have
been using pink noise ever since. I t is criticallyimportant for hyperacusis patients to not over
7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 21/31
Questions and Answers (continued)
[Q]Ms. G. from Ohio writes that one health
care professional said she did not needhearing aids, another said that she does,
and a third said that she needs both tinnitus
maskers and hearing aids. Naturally she isconfused.
Regarding hearing aids, the way todetermine whether or not you need
them is to try them. You can do this with
a 30-day money-back guarantee. In some cases,a hearing aid is all that is necessary for relief
of tinnitus. Mostly it will depend upon the kind
of hearing loss you have and the pitch of your
tinnitus. If the tinnitus is low-pitched and if the
hearing loss extends into the low frequencies
then perhaps hearing aids are all you need .If, on the other hand, you have a high-pitchedtinnitus and a high-pitched hearing loss then
the combination of hearing aids and tinnitusmaskers (called tinnitus instruments) are what
you should try. Many physicians believe that
the high frequency loss does not interfere with
normal hearing. And they are correct - so longas the patient is in a quiet place and speaking
one-on-one. Unfortunately we are more commonly in the presence of background noise.
relief from the use of vinpocetine. Hopefully
someone here in the U.S. will conduct a pair ofstudies of this drug. First, an open study shouldbe done where everyone gets the drug. If that
turns out to produce positive effects in high
enough numbers, then a double-blind placebocontrolled study should be done. If you don'twant to wait for the results from such studies,you can write to Interlab, BCM Box 5890,
London WCIN 3XX, England and request an
order form. Vinpocetine (or Cavinton) is an
over-the-counter drug in England and SouthAmerica but you still might need a physician'sprescription to order it. Vinpocetine sells for$26 per 100. If you order and use vinpocetinewe will be most interested in your results.
[Q]Mr. B. from California, who noticedcomments in Tinnitus 1bday suggestinga relationship between pain and tinnitus,
offers direct evidence of such a relationship.Mr. B is cursed with otalgia (ear pain) and tinnitus which started eight years ago. The cause of
his otalgia has not been discovered but the paincan be relieved by narcotics. Severe chronic pain
haskept Mr. B.
on Demerolwhich
has beeneffective not only for the pain but has also

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 22/31
Questions and Answers (continued)
[Q]Mr. B. from Michigan was told that his
hearing was so impaired that maskingwould not help him. He further states
that even with hearing aids, he can hear peoplespeaking but cannot understand what they are
saying.
Regarding masking, never judge in
advance. Always conduct a trial. Mostlikely the best chance for success for
you, Mr. B., is with tinnitus instruments. Ifyou
try the tinnitus instrument remember that it isessential to adjust the hearing aid portion first.Only after that do you add in the maskingsound.
Speech comprehension is a common complaint,especially among elderly patients with hearing
losses. The act of understanding speech involvesnot only hearing the speech sounds but also processing those sounds in the brain. The processing actually requires a certain amount of time to
achieve. Apparently as we age, that processing
Learn Lip Reading
with this Fun,Self-Help,
of speech sounds (like many other things) simply slows down. And it doesn't have to slowdown much for speech to become an incomprehensible mess. Dr. David Lilly of OHSU conducted a study where the time interval between
utterances was increased by 250 milliseconds.The delayed timing as compared to the normal
timing of speech improved speech comprehension significantly for the elderly hearing
impaired. Unfortunately, as yet there is no
wearable electronic device available that can
effect the slower presentation. I t will be helpfulto you, however, i f you suggest that those speaking to you do so not louder but more slowly.
Notice: Many ofyo u have left messages requestingthat I phone you . I simply cannot afford to meet
those requests. Please feel free to call me on any
Wednesday, 9:30a.m.- noon and 1:30-4:30 p.m.
(503/494-2187). Please send your questions to:
Dr. Jack Vernon c/o ATA, Tinnitus 7bdayPO Box 5, Portland, OR 97207-0005.
7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 23/31
Tinnitus Transformation
from Sufferer to Survivor
by Thomas J. DA.iuto
I had never heard the word
tinnitus uttered until the
day of my injury. And after
15 years as a police officer, Iwish I could say I was
injured in some heroic way.But my injury was the result
of a weight-lifting accident
in the police fitness room.
The medical diagnosis was"perilymph fistula," but basically I pushed toohard on the bench press and exploded my inner
ear. I clearly remember that other than the sen
sation of a pop and a clogged feeling, the firstsymptom was a ringing sound which I thought
was a phone in the gym!
When I got up from the weight bench, I wasnauseous and off-balance. I stumbled back tomy office to call my doctor but there was no dialtone when I picked up the phone. Now sick and
mad that the phones were broken, I asked my
secretary to check her phone. I t worked. As Itried her phone I discovered that I was deaf in
now know feeds directly from and supports thetinnitus. It is depression.
Until my audiologist told me about the .ATA,
I had been on a two-year downward spiral, with
what appeared to be no help in sight. I can
clearly remember receiving my first issue of
Tinnitus Tbday and how I read it from cover tocover as if it were food for a starving individual.1 also can remember sitting there alone and crying, realizing that I was not crazy or unique in
my pain. Tinnitus Tbday has become my "lifepreserver." And it seems to always be thrown
my way just when I most need it.I began and continue to receive counseling
and drug treatment for depression. Stil1, when
the depression starts to clear and I feel activeand alive, the tinnitus reminds me that living in
this noisy, busy world extracts a hefty price. I t is
a vicious circle in that when I do feel well and
in need of stimuli, it is the stimuli that willdrive me back to seclusion which starts the
cycle over. Although I know my major tinnitus
triggers, there is no way to eliminate them
entirely without eliminating my quality of life.This is where tinnitus and depression appear to

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 24/31
Tinnitus Transformation (continued)
bring tinnitus out of the closet and in turn and if
possible, help prevent someone else from suffer
ing from this affliction, maybe even help find a
cure. Since tinnitus is not a fatal illness, it is
hard for many to take it seriously. I am con
vinced that it's up to us - people with tinnitus
- to push for acceptance, understanding and,
ultimately treatment. This has been a huge fac
tor in my transformation from tinnitus suffererto tinnitus survivor.
I am also blessed in having a wonderful and
understanding family- my wife, Lindy, and my
son, Tony - who perceive my discomfort level
when we're ou t socially and are completely sup
portive i f I need to leave when the noise
becomes unbearable. Both Lindy and Tony arewell-educated about tinnitus, and volunteer
their time and efforts at our monthly support
group meetings and by taking support phone
calls when I'm not able to. This is another major
positive factor in living with this disease.
Now with the help of excellent therapists
and rehabilitation counselors, I am back in
Guidelines for Writers
school full-time (and pulling straight A's) work
ing towards a paralegal degree. I know I cannot
work in a traditional work environment due to
the severity of my tinnitus but I can utilize new
computer technology to work from home. I've
learned through vocational counseling and mar
ket surveys that there are many local employers
who will accommodate my needs. I look forward
to making the transition from a police criminal
investigator to a criminal and litigation
researcher. The tools will change - from hand
cuffs and a gun to a computer mouse and theInternet- but the skills remain the same.
So I try to enjoy the good days, and know
that even on the deepest, darkest days, just over
the next cresting wave is a lifeboat. Inside are
fellow survivors (not sufferers) smiling, as one
tosses the next copy of Tinnitus Tbday my way.
While I yearn for the day my "life preserver"
carries the headline TINNITUS CURED, the
warmth, compassion, and understanding of
these survivors rescue me and 1 know that
I am not alone.

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 25/31
SPECIAL DONORS and TRIBUTES
ATA's Champions of Silence are a remarkable
group of donors who have demonstrated their commitment in the fight against tinnitus by making acontribution or research donation of $500 or more.Sponsor Members and Professional Associates
have contributed at the $100-$499 level. ResearchDonors have made research-restricted contributionsin any amount up to $499.
acknowledged with an appropriate card to the
honoree or family of the honoree. The gift amount isnever disclosed.
Our heartfelt thanks to all of these specialdonors!
All contributions to the American TinnitusAssociation are tax-deductible.
GIFTS FROM 4-16-97 to 7-15-97.A T ~ s Tribute fund is designated 100% forresearch. 'Ihbute contributions are promptly
Champions of
Silence(Contributions of$500 and above)Julia R. AmaralAllen R. BernsteinRobert w. BoothRichard Burnat
Rob M. Crichton
Glen R. CuccinelloCornelius R. DuffieJosephine K. Gump
David W. Hopkins,Fonnit PrintManagement
W. F. Samuel
Hopmeier, BC-HISHarry G. an d Marion
KeiperJohn Malcolm
Bruce MartinJohn E. Meehan
Raymond L. Buse, Jr.Raymond L. BuseMemorialFoundation, Inc.
John F. CaddvBarbara Young CampStan ColeMichael L. ConnollyRichard R. Cortright
CliffordS.
CraigGeorge Crandall, Jr.Carole DesnoesIrene DuffieldA. T. EvansRobert Fasic and Roy
GrieshaberBernard FishmanDavid E. FlatowMary A. FloydFrancine and Ray
FosterElliot S. FrankfortRobin R. Fuller
Marvin KowitE. Joseph KubatAllan S. KushenHenry G. LargeyFred R. LawsonEvelyn Schrader LeeRuth T. LelszGary W. LightnerGary L. Lombardi
Peter ManasseAugusto MarcianteEllen Anne MarksPeter A. MarrinanAndy MatthiesenMr. and Mrs. M.
Richard MayGudrun Wallgren
MerrillJohn M. MeyerAlexander Miller
Judith MmerMatt MinningerPhilip 0. Morton
Forrest ShookDavid J. Simm
Raymond C. SimonJoel Smith
Connie StantonRichard H. StecklerVeronica
SteffensmeierDouglas H. Steves
William an d Cora Lee(Corky) StewartElsebeth S. StrykerRichard W. SullivanAntril C. Suydam
Robert L. SzaboFred D. Thompson
James C. TottenJack WallnerDavid J . WalshJ . Michael Wiggins
MaryB.
WilliamsonShirley L. WiremanStephane W. Wratten
Carlos Herraiz, M.D.David T. Malicke, D.O.
Sol Marghzar. M.S.,CCC-A
Ernest E. Mhoon, Jr.,M.D.
Stephen E. Mock,Ph.D.
Kenneth E. Mooney,
M.D.Philip A. Rosenfeld,M.D.
'Thnit Ganz Sanchez,M.D.
Martin SmithDr. Blair R. Swanson
Corporationswith
Matching GiftsAmerican Express
Chase ManhattanCPC InternationalHoechst Celanese

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 26/31
SPECIAL DONORS and TRIBUTES (continued )
TRIBUTES
In Memory OfFlorence Angello
Mary G. KalilMrs. Louise Barrows
Mark Jurich
'f rudy Drucker,Ph.D .
Barbara M. Handy
Mary R. KokesHazel V. Fingal
John H. And Faye L.SchleterBernhard GarfinkleShirlie Kesselman
Lydia KonitzerJames KonitzerIrene Lomax
Kolbrenner &Alexander, L.L.C.
Jerry PragerSybil BarzilayEd ThnnienJoella and Lester
SatterthwaiteMary J. McGorray'Thd Van Sloote nArlo and Phyllis Nash
In Honor OfJack Harary
(for Father's Day)Bob and Debbie
Harary and Family
Ronald W. BocksrukerJoyce C. BodigDarlene K. BohincMildred S. BonwitRichard C. BorellaChristina BourdaaTheodore T. BoutisBessie M. BowensSr. Antoinette BoykinTrene E. Brennan
Kathleen M. BrockElaine F. BrodeyBarbara F. BrownGay BrowneHarry A. Bruhn
J. Ben BuckPaul Bunts
Michael W. Burnham
Abigail H. BurrDaniel M. CahillMiriam W. CampbellMichelle CanzioDaniel J . Carlin
Joh n CarloStuart A. ChalfantSusan P. ChizeckLorime r T.
Christensen
Jean CinaderC. Dennis Clardy
Thomas R. Coffey, I IArthur P. Coletta, CVS-
LifeArthur B. CollierE.
Landon CollinsMary J. CollinsEileen T. Corcoran
Elaine Gannon
David J. GaudieriMark S. GellerOtto GenoniJu dith M. GillErwi11 C. GotschPeggy B. Gouldman
Seymour GreensteinNorman GrolmanJack A. GubancJohn F. HallgrenJohn R. Hammond
Laura E. HardyCharles T. Hawn
Mrs. F. W. HeesBetty J . Reisch
Geraldine Herrs. Dale HessE. Alan Hildstrom
Paul G. HillCirel HillmanLouise M. HirasawaSara Jean Hoffmann
LorettaL.
HughesDorothy Ikemeyer
David P. Ja nkofskyBarry V. JohnsonHoward W. Johnson
Christopher A. KaelinRebecca B. KaisermanR. L. KeheleyFrank L. Kellogg, Jr.Fred F. KentopWayne M. Kern
MichaelW.
KerschenDavid Kiecker
John E. Kinney
Byron R. MannLillian P. MarkowitzJohn MasciaJulianne MattimoreJohnathon R.
McCartneyMarvin MeskerShirley A. MillerWard T. MilnerGladys V. MooreWalter N. MorganFranco MormandoHarry H. MorrittE. Susan MortonDavid E. MotternElayne MyersMae Nachmanlan L. Natkin
Vivian NewillJerome H. Newman
Regine R. NexsenRobert NicholsDonald G. O'Brien, Sr.
WilliamD.
OdbertCurtis S. OlsonRobert OroszBenjamin OssmanKarl E. Owen
John PalazzoEdward PalinJan ie L. Palmer
Carl J . PaluckiThmmy Kells Parker
Kanti S. Patel
Sharon PayneRobert PecciniH. w. Pedersen
Richard S. SchonwaldWilliam SchwartzArlan R. SchwoyerJim Shawn
Norma T. SheldMark W. SholofskySylvia K. ShugrueKatherine L. SimmonsSherwood L. SimmonsRaymond C. SimonMark A. SniegowskiMildred F. SohnJean
SpenceElizabeth H. SpencerMaureen T. SprohgeJames J. SteponikDouglas H. StevesJim StokesJames E. StorerLyle E. StrahanSteven Strong, M.D.Elsebeth S. StrykerRaymond L. Sullivan
Ronald Swid1erHelen K. ThylorKaren M. Thomson
Eugene F. TI:uaxLen UflandWayne VaughnMaxine VincentLee K. VorisekMichael VucelichMildred WadJerMark K. Wallack, M.D.
Marc WeinsteinRichard L. WeisErik Wennermark

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 27/31
Noise, either of short or long duration was jump in 1996 to 60%. People also reported getting
7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 28/31
associated with the onset of tinnitus for 36.8% of
the respondents. Another 36% did not know wheretheir tinnitus came from. 12% reported it from ear
infections. Various other causes were reported in
small numbers.
Nearly 70% of people responding reporthaving a hearing loss. Strikingly 75% of thesepeople do not wear hearing aids. The majority
considers tinnitus a greater problem than hearing
loss.
Almost everyone, 97%, has health
insurance. Only 16% report no coverage for tinnitus,83.7% received either partial or complete payment
Tinnitus has a significant effec t on the lives
of those completing this survey. It interfered with
work for 56.8%, with social interaction for 69.3%,and with general enjoyment of life for 85.7%.
Additionally, 70.8% of the respondents reportedbeing depressed. In spite of these numbers onlyabout 12% have had to quit work because of
tinnitus.
Ninety people reported their tinnitus led to
litigation, bu t most have taken no steps to achievea settlement. Ten have begun litigation. Twenty-sixreported receiving a favorable settlement and 33
reported receiving an unfavorable settlement.
It appears that some headway is being
made in educating both professionals and thegeneral public. Patients in 1986 were told to "learnto live with it" about 83% of the time. That haddecreased to about 7 4% by 1996. Physicians will be
pleased to note that respondents now consider
them 58.2% helpful with tinnitus - a dramaticincrease from 33.7% ten years ago. However,91.7% of the respondents did not think they hadbeen offered effective relief!
In 1986 only 31% of the people had triedany form of tinnitus treatment, that number
increased a little in 1992, to 34%, but took a big
relief from what they'd tried. Masking in its variousforms, including retraining therapy and bedside
masking accounted for most of the successes.Drugs for tinnitus accounted for considerable relief,but not as much as in 1992.
More than 10% of he respondents reportedattending ATA self-help group meetings with themajority rating them good to excellent.
HOW CAN I FIND HELP FOR MY TINNITUS?
The American Tinnitus Association, a non-profitorganization, supported solely by private donations,is dedicated to helping tinnitus patients andsupporting tinnitus research. Activities include the
production and distribution of public awarenessmaterials, educational programs for the professionaland lay communities, establishment and guidancefor self-help groups and their leaders, and thepromotion of community hearing protectionprograms.
For further information and membership benefits:
AMERICAN TINNITUS ASSOCIATION
Post Office Box 5
Portland, OR 97207-0005
Tel: (503) 248-9985 Fax:(503) 248-0024http://www.teleport.com/-ata
e-mail: [email protected]
A non-profitvoluntary human health and welfare agency under
26USC 501 (c)(3) @ATA 0997
RESULTS OF THE
1996 TINNITUS
PATIENT SURVEY
FROM THE
AMERICAN
TINNITUS
ASSOCIATION
I GENERAL INFORMATION 7. Employment status: I TINNITUS DESCRIPTION

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 29/31
1.Age: Mean 59.76, Range 19-91
2. Sex: 62.3% male, 37.4% female
3. Marital Status:MarriedNot married
4. Ethnicity:WhiteNon-white
5. Education level:
72.1%27.9%
96.3%3.7%
Grade schoolHigh/vocnl school
1.0%22.8%
6. Where residence located by geographiccensus area:
NortheastMidwestSouthWest
27%20%25%
28%
Full time 36.9%Part time 7.8%Retired 42.8%UnempiJDisabled 4.7%Not empl.outside home 7.8%
Major Lifetime Occupation
8. Major occupation throughout life:Sales/officeTeacher/student/creativeHomemaker/farmerAdmin/managerScientist/medical
Mechanic/const.lfactoryFire/Police/Military
9. Annual family income:Under $25,000$25,000 to $49,999Over $50,000
10. General Health Level:Excellent 34.6 %Good 52.6%Fair 11.0%
Poor 1.8% .
13.0%33.8%53.2%
23.8%18.9%15.6%15.1%14.9%
6.7%4.9%
11 . How long have you been aware of your
tinnitus?:Up to 1 yr
1 up to 2 yr
up to 5 yr
5 up to 10 yr
10 up to 20 yr
20+ years
5.9%8.7%19.4%22 .7%23.8%19.4%
12. Did the tinnitus come on gradually or
suddenly?:GraduallySuddenlyUnsure
34.2%51.0%14.8%
13. Where does your tinni tus seem to belocated?:
Lef t ear 15.7%Right ear 11.0%Both ears 54.6%
In head 7.7%In head & ears 10.0%
14.1s your tinnitus constant or ntermittent?:Hear it part time 16.6%Constantly there 83.4%
15. What does your tinnitus usually soundlike?:
RingingHissing
Transformer noiseBuzzingClear ToneSizzlingPulsatingWhistleHigh TensionOcean RoarHum
29.3%22.2%
8.7%5.3%5.3%4.1%3.1%3.1%2.3%2.3%1.7%
16. Tinni tus loudness rating on a scale 1 to 10,where 10 is the loudest.:
Mode 5; Mean 5.95; Median 4.92

7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 30/31
17. Onset association:Not known 36.0%
Noise exposure/long time 18.5%Noise exposure/brief 18.3%Ear Infection 12.0%Drugs 5.6%
Illness 5.1%
Head Injury 3.1 o/o
Whiplash 1.4%
18. Do you also have a hearing loss?:No 21.8%
Yes 69.9%
Unsure 9.7%
19. Do you currently wear a hearing-aid?:No 74.9%
Left ear 8.1%
Right ear 6.3%
Both ears10.7'1/o
20. Which is more of a problem?:Tinnitus 59.4%
Hearing loss 14.6%Equal bother 22.8%
Unsure 3.1%
• TINNITUS AND HEALTH CARE
21. Do you have health insurance?:
No 2.9%Yes 97.0%
22. Were the costs of your tinnitus visits
covered by insurance?:No 16.0%Partial 54.4%
Yes 29.3%
23. How many tinnitus visits to any health careprofessionals have you made in the last 12
months?:Mean 1.11
24. How many visits since tinni tus onset?:Mean4.3
25. Were health care professionals helpful andsympathetic?:
AgreeDisagree
58.2%41.5%
26. The treatment offered reduced or
eliminated tinnitus:AgreeDisagree
8.0%91 .7%
27. The treatment offered was ineffective:Agree 58.5%
Disagree 41 .0%
28. Only treatment offered was "Learn to Jive
with it":
Agree
Disagree
74.1%
25.3%
29. Have you tried any form of treatment for
your tinnitus?:No 39.5%Yes 60.0%
Listanyproviding relief:
Bedside maskersAuditory HabituationMaskersDrug TherapyHearing-aids
BiofeedbackAcupunctureOther
65.0%
50.0%
47.3%
42.8%
37.4%
31.8%19.1%38.1%
30. Visited a health professional on ATAreferral list?:
NoYes
81.5%
18.2%
31. Rate care received from that referral: (248people reporting)
Excellent29.4%
Fair17.6%
Good 37.3% Poor 12.9%
IV TINNTUS AND THEQUAliTY OF UFE
32 . How much effort to ignore tinnitus?:Easily ignored 16.8%Ignored with effort 41.5%
Considerable effort to ignore 26.9%
Can never ignore 14.9%
33. Feel irritable due to tinnitus?:NeverSometimesOftenAlways
16.5%57.3%
21.4%
4.9%
34. Sleep problems due to tinnitus?:NeverSometimesOftenAlways
31.0%
48.4%
11.6%9.0%
35. Ever feel depressed due to tinnitus?:Never 28.24'/o
Sometimes 51.8%
Often 14.9%Always 5.1%
36. How much does tinni tus interfere withwork?:
NoneSlight amountModerate
Great
37. Ever quit work due to tinnitus?:NoYes TemporarilyYes Permanently
43.1%
31.3%
16.7%
8.8%
88 .0%6.8%
5.3%
38 . How much does tinnitus interfere withsocial activity?:
NoneSlight amount
ModerateGreat
30 .8%30.24'/o
22.S0.4
16.6%
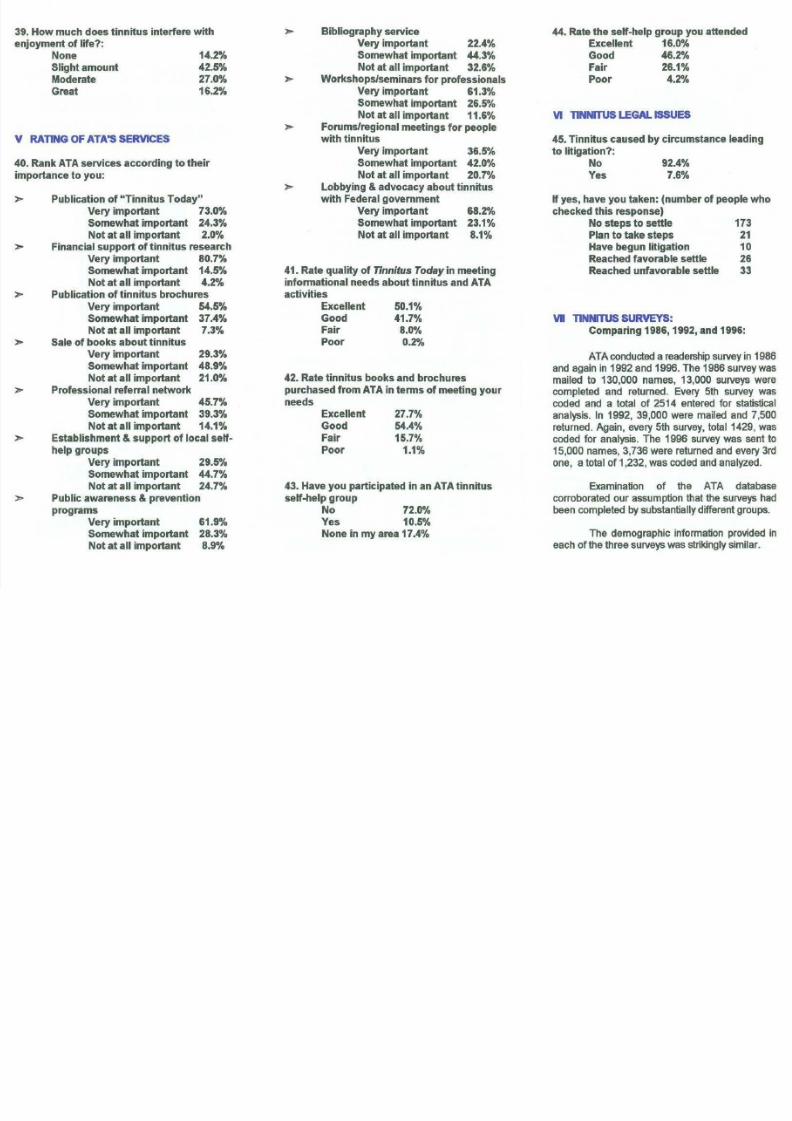
39. How much does tinni tus interfere with Bibliography service 44. Rate the self-help group you attended
7/23/2019 Tinnitus Today September 1997 Vol 22, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1997-vol-22-no-3 31/31
enjoyment of ife?:NoneSlight amountModerateGreat
14.2%
42.5%
27.0%
16.2%
V RATING OF ATA'S SERVICES
40. Rank ATA services according to their
importance to you:
> Publication of "Tinnitus Today"Very important 73.0%
Somewhat important 24.3%
Not at all important 2.0%
Financial support of tinnitus researchVery important 80.7%
Somewhat important 14.5%
Not at all important 4.2%Publication of tinnitus brochuresVery important 54.5%
Somewhat important 37.4%
Not at all important 7.3%
Sale of books about tinnitusVery important 29.3%
Somewhat important 48.9%
Not at all important 21 .0%
Professional referral networkVery important 45.7%
Somewhat important 39.3%
Not at all important 14.1%Establishment & support of local selfhelp groups
Very important 29.5%
Somewhat important 44.7%
Not at all important 24.7%
Public awareness & preventionprograms
Very important 61.9%
Somewhat impor tant 28.3%
Not at all important 8.9%
Very important 22.4%
Somewhat important 44.3%
Not at all important 32 .6%
Workshops/seminars fo r professionalsVery important 61 .3%
Somewhat important 26.5%
Not at all important 11.6%
Forums/regional meetings fo r peoplewith tinnitus
Very important 36.5%
Somewhat important 42.0%
Not at all important 20.7%
Lobbying & advocacy about tinni tuswith Federal government
Very importantSomewhat importantNot at all important
68.2%
23.1%
8.1%
41. Rate quality of Tinnitus Today in meeting
informationa l needs about tinn itus and ATAactivitiesExcellentGoodFairPoor
50.1%
41.7%
8.0%
0.2%
42. Rate tinni tus books and brochurespurchased from ATA in terms of meeting your
needsExcellent
GoodFairPoor
27.7%
54.4%15.7%
1.1%
43. Have you participated in an ATA tinnitu sself-help group
No 72.0%
Yes 10.5%
None in my area 17.4%
Excellent 16.0%
Good 46.2%
Fair 26.1%
Poor 4.2%
VI TlNNmJS LEGAL ISSUES
45. Tinnitus caused by circumstance leadingto litigation?:
NoYes
92.4%
7.6%
If yes, have you taken: (number of people who
checked this response)No steps to settle 173
Plan to take steps 21
Have begun litigation 10
Reached favorable settle 26
Reached unfavorable settle 33
VI TlNNRUS SURVEYS:Comparing 1986, 1992, and 1996:
ATA conducted a readership survey in 1986and again in 1992 and 1996. The 1986 survey was
mailed to 130,000 names, 13,000 surveys werecompleted and returned. Every 5th survey wascoded and a total of 2514 entered for statisticalanalysis. In 1992, 39,000 were mailed and 7,500
returned. Again, every 5th survey, total 1429, wascoded for analysis. The 1996 survey was sent to15,000 names, 3,736 were returned and every 3rdone, a total of 1 232, was coded and analyzed.
Examination of the ATA databasecorroborated our assumption that the surveys hadbeen completed by substantially different groups.
The demographic information provided in
each of the three surveys was strikingly similar.