the tension between evidence- based and experience-based medicine kent bottles, md president of...
TRANSCRIPT

The Tension Between Evidence-based and Experience-based
Medicine
Kent Bottles, MD
President of ICSI, Bloomington, MN, www.icsi.org
Tufts Summer Institute on Web Strategies for Health Communication
July 20, 2010
Boston, MA

Evidence-based Medicine
• “Evidence-based medicine is the conscientious, explicit and judicious use of current best evidence in making decisions about the care of individual patients.”–Analysis of literature –Pick best treatment–Movement

Evidence-Based Medicine &Patient-Centered Choice
A. Good evidence/Important to patient
B. Good evidence
C. Potential for good evidence
D. Important to patient choice/potential for good evidence
E. Important to patient choice/ No potential for evidence
A B
A. L. Cochrane, from T. Hope Evidence-based patient choice and the doctor patient relationship in But Will it Work Doctor? Kings Fund, London 1997, 20 – 24
CDE
IMPORTANTEVIDENCE

Canadian Cancer Society RFPManske SR, et.al., AJHP 18:409-423, 2004
• Do group counseling programs for smoking cessation work?
• What is the best content for such a session?• How many sessions should be offered?• Who should facilitate such sessions?

Canadian Cancer Society RFPManske SR, et.al., AJHP 18:409-423, 2004
• 40 year comprehensive literature review• Deficiencies in purpose, design, and
reporting• Research could only answer one of the four
questions posed by Cancer Society

Evidence-based MedicineICSI Evidence Grading System
• Primary Reports of New Data Collection– Class A: Randomized, controlled trial– Class B: Cohort study– Class C: Nonrandomized trial, case controlled– Class D: Case series, case reports
• Reports that Synthesize Primary Reports– Class M: Meta-analysis, decision analysis– Class R: Consensus statement, consensus report– Class X: Medical Opinion

Evidence-based MedicineConclusion Grading System
Grade I: Conclusion is supported by good evidenceGrade II: Conclusion is supported by fair evidenceGrade III: Conclusion is supported by limited evidenceGrade not assignable

Guideline Challenges for Patients with Multiple Conditions
• Interactions between illnesses• Interactions between treatments• Tension between therapeutic goals• Multiple providers• Multiple medications
Guidelines and Measures
• We measure what is easy to measure• We do not always identify what is important
clinically and then figure out how to measure the outcome
• We need to place more emphasis on what metrics are important to measure what is important

Clinical Practice Guidelines
• Professional consensus about what to do• Codification of standards of care• Source of legitimacy for quality measures• Educational tool • Strategy to improve quality• Solution to practice variation
Evidence-based Medicine
• Why would anyone be against that?• Demotes ex cathedra statements of experts
to least valid form of evidence

Why Doctors & Patients Do Not Always Select Best Treatments?
• Knowledge gaps• Skills gaps• System barriers• Technology barriers• Misaligned incentives

Why do Some Doctors Reject EBD?
• Psychological immune system that operates unconsciously to maintain our positive image of ourselves
• “When it comes to maintaining a sense of well-being, each of us is the ultimate spin doctor.” Gilbert and Wilson
• Humans are hardwired to think highly of themselves & their abilities as physicians
• Cornell study shows subjects over- estimated their own charity purchases, but were accurate about other people’s action
• MBA students estimate of their own contributions to team projects at 139%

Evidence-based Medicine
– Tonelli believes EBM discounts clinical experience
– Certain groups (women, minorities, pts with multiple conditions, etc) are under-researched
– Funding sources dictate what gets researched– Does measurement and science explain
everything that is important in the world?– EBM does not evaluate tacit knowledge

American Medicine Gets It Right
55% of the time
McGlynn EA, et. al. The quality of health care delivered to adults in the United States. N Engl J Med 2003: 348 (26): 2635-45 (June 26)
RAND Study Details
• Alcohol dependence 11%• Peptic ulcer 33%• Diabetes 45%• Prenatal care 73%• Breast cancer 76% • Cataracts 79%

Improving the Quality of American Health Care in the 21st Century
• Not about motivating clinicians to work harder or be concerned about safety
• “The complexity of modern American medicine exceeds the capacity of the unaided human mind.” D. Eddy, MD
• It is about system leadership providing doctors with the IT data feedback tools to save more lives

• 6,000 articles / day• 150,000 articles / month• 300,000 RCTs• 20,000 biomedical journals
Complexity of MedicineAnn Intern Med 2001;135:309-12
“Asking an individual doctor to rely on his memory to store and retrieve all the facts relevant to patient care is like asking travel agents to memorize airline schedules.”
L. Weed, M.D.
Complexity of Medicine

Protocols Can Improve Care
• Measure, learn from, and eliminate variation arising from professionals; retain variation arising from patients.
• Select a high priority care process.• Adopt an evidence-based best practice guideline.• Blend the guideline into clinical work.• Use the guideline as a shared baseline with
clinicians free to vary based on individual patient .

VA Tools to Implement Evidence-based Medicine
• Provider education (CME, guidelines)• HIT (Reminders, decision support, registry)• Performance Measurements & Reporting• Pharmacy Benefits Management
(Formulary, pre-approval, co-pay policy)• Patient Education (MyHealthVet, self-
management support)

Developing A Center For Comparative Effectiveness Health Affairs,
11/7/2006
• Australia: Pharmaceutical Benefits Scheme• UK: National Institute for Health and
Clinical Excellence• Canada: Common Drug Review• Germany: Institute for Quality and
Efficiency

National Institute for Health and Clinical Excellence (NICE)
• Postcode lottery scandals• 270 member staff and $50 million per year• Usually does not recommend treatments
whose cost per quality-adjusted-life-year is more than $40,000
• Publishes appraisals of treatments for NHS– Based on clinical effectiveness– Based on cost effectiveness
National Institute for Health and Clinical Excellence (NICE)
• Consultee and commentator organizations• Independent academic center writes
“assessment report”• “Evaluation report”• Independent Appraisal Committee writes
“final appraisal determination”
National Institute for Health and Clinical Excellence (NICE)
• Royal National Institute of Blind People accussed NICE of “incompetence” over delay in approving drug used in Scotland
• Renal Cell Carcinoma treatments– Bevacizumab, sorafenib, sunitinib
• Alzheimer’s disease treatments– Donepezil, galantamine, memantine
Saying No Isn’t NICERobert Steinbrook, NEJM, 359; 19: 1977-1981, November 6, 2008
• “NICE can be viewed as either a heartless rationing agency or an intrepid and impartial messenger for the need to set priorities in health care.”
• NICE has to “be fair to all the patients in the National Health Service…If we spend a lot of money on a few patients, we have less money to spend on everyone else. We are not trying to be unkind or cruel. We are trying to look after everybody”
Uwe E. Reinhardt
• The opposition to cost-effectiveness analysis comes from two distinct groups
• “The first group includes individuals or enterprises that book other people’s health care spending as their own health care income”
• “The second group…includes individuals who sincerely believe that health and life are ‘priceless’ -- for them cost should never be allowed to enter clinical decisions”
Uwe E. Reinhardt
• “It is an utterly romantic notion and, if I may say so, also an utterly silly one. No society could ever act consistently on such a credo”
• “In their daily decisions, American citizens and their political representatives routinely trade health and life for money, which allows economists to infer the value-per-life-year the decision makers had in mind.”

US to Compare Medical Treatments R. Pear, NY Times, February 16, 2009
• Doubters– Betsy McCaughey– Rush Limbaugh– Congressional Black Caucus– Society for Women’s Health Research
• Proponents– Senator H. Clinton– Rep. Pete Stark– Consumers Union– Dr. Elliott Fisher
Harnessing Comparative Effectiveness:
An Initiative to Improve the Value of Care for Localized Prostate Cancer
For further information:
www.icer-review.org
Steven D. Pearson, MD, MSc, FRCP
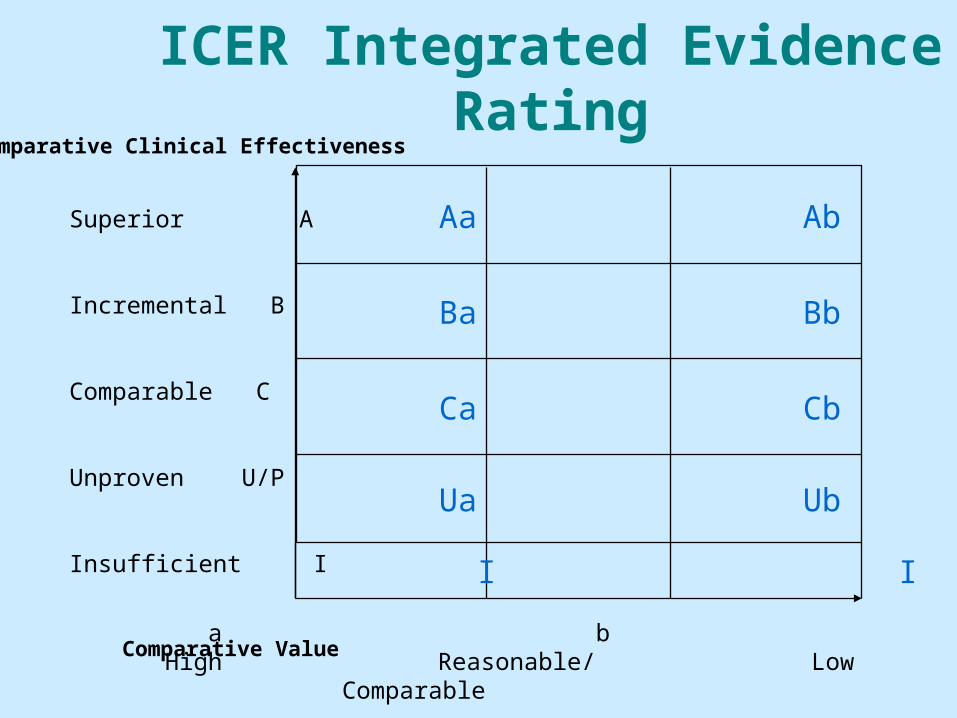
ICER Integrated Evidence Rating
a b c High Reasonable/ Low
Comparable
Superior A
Incremental B
Comparable C
Unproven U/P
Insufficient I
Comparative Clinical Effectiveness
Aa Ab Ac
Ba Bb Bc
Ca Cb Cc
Ua Ub Uc
Comparative Value
I I I

The Project to Improve Prostate Cancer Care
• Localized prostate cancer: the opportunity– Approximately 4,200 new cases per 1 million men– Significant variation in care patterns across the US– Patients and clinicians have time to consider options– Approximate prices paid for radiation therapy options
• 3D-CRT = $10,000• Brachytherapy = $10,000• IMRT = $20,000-$40,000• Proton beam = $50,000-$80,000

a b c High Reasonable/ Low
Comparable
Superior A
Incremental B
Comparable C
Unproven U/P
Insufficient I
Comparative Clinical Effectiveness
Aa Ab Ac
Ba Bb Bc
Ca Cb Cc
Ua Ub Uc
Comparative Value
I I I
BrachytherapyBa
Radiation for prostate cancer
IMRTBc
Proton Beam Therapy = Ic
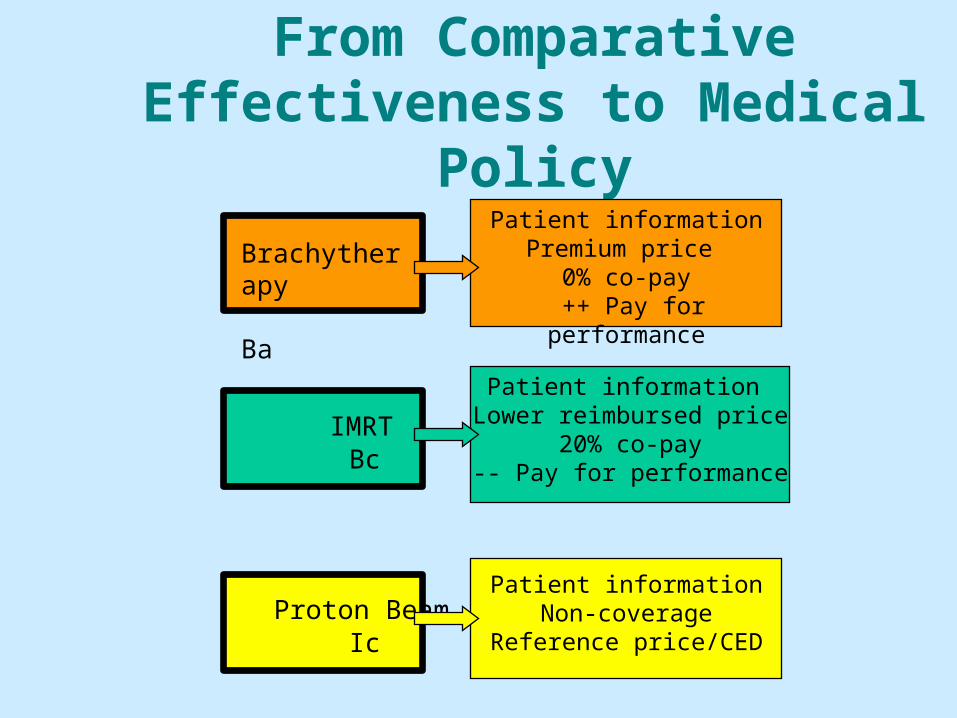
From Comparative Effectiveness to Medical
Policy
IMRT Bc
Patient information Lower reimbursed price
20% co-pay-- Pay for performance
Patient informationPremium price
0% co-pay ++ Pay for performance
Brachytherapy Ba
Proton Beam Ic
Patient informationNon-coverage
Reference price/CED

The American Recovery and Reinvestment Act of 2009
• $1.1 billion for comparative effectiveness research
• AHRQ: $300 million• NIH: $400 million• Office of the HHS Secretary: $400 million
HHS Definition of CER
• Comparative effectiveness is conducting and synthesizing of research comparing the benefits and harms of different interventions and strategies to prevent, diagnose, treat, and monitor health conditions in “real world” settings.
Money TalksRyan Lizza, The New Yorker, May 4, 2009
“He became obsessed with the findings of a research team at Dartmouth showing some regions…spend far more money on health care than others but that patients in those high-spending areas don’t have better outcomes than those in regions that spend less money”
Money TalksRyan Lizza, The New Yorker, May 4, 2009
“If spending more on health care has no correlation with making people healthier, then there must be enormous savings that a smart government, by determining precisely which medical procedures are worth financing and which are not, could wring out of the system.”

Money TalksRyan Lizza, The New Yorker, May 4, 2009
“At the core of both the stimulus bill and the Obama budget is Orzag’s belief that a government empowered with research on the most effective medical treatments can, using the proper incentives, persuade doctors to become more efficient health-care providers, thus saving billions of dollars.”

Money TalksRyan Lizza, The New Yorker, May 4, 2009
“Paul Ryan and other Republicans had seized on health-cost controls as the issue they believed would bring down Obama’s health-care plan and, with it, they surely hoped, his Presidency.... Orzag’s obession with ‘comparative effectiveness’…will lead to vast government intrusion into the doctor-patient relationship.”
Money TalksRyan Lizza, The New Yorker, May 4, 2009
“Obama is in effect betting his Presidency on Orzag’s thesis.”

Obama InterviewD. Leonhardt, After the Great Recession, NY Times Magazine, May 3, 2009
“There’s always going to be an asymmetry of information between patient and provider. And part of what I think government can do effectively is to be an honest broker in assessing and evaluating treatment options. And certainly that’s true when it come to Medicare and Medicaid, where taxpayers are footing the bill.”
Obama InterviewD. Leonhardt, After the Great Recession, NY Times Magazine, May 3, 2009
“So when Peter Orzag and I talk about the importance of using comparative-effectiveness studies as a way of reining in costs, that’s not an attempt to micromanage the doctor-patient relationship. It is an attempt to say…we’ve looked at some objective studies…concluding that the blue pill, which costs half as much as the red pill, is just as effective, and you might want to go ahead and get the blue one. And if a provider is pushing the red one…, then you should at least ask some important questions.”

Obama InterviewD. Leonhardt, After the Great Recession, NY Times Magazine, May 3, 2009
“If it turns out that doctors in Florida are spending 25% more on treating their patients as doctors in Minnesota, and the doctors in Minnesota are getting outcomes that are just as good -- then us going down to Florida and pointing out that this is how folks in Minnesota are doing it…--I think that conversation will ultimately yield some significant savings and some significant benefits.”

The Big FixDavid Leonhardt, NY Times Magazine, February 1, 2009
• Small area variation in Medicare spending• High spending areas like Miami, Texas,
southern New Jersey• Low spending areas like Minnesota, Iowa,
New Mexico, Virginia
The Big FixDavid Leonhardt, NY Times Magazine, February 1, 2009
• Mitchell Seltzer• Doctors who spend more don’t get better
results than their conservative colleagues• Patients of aggressive doctors stay sick
longer and die sooner because of risks of aggressive care
The Big FixDavid Leonhardt, NY Times Magazine, February 1, 2009
• Mitchell Seltzer• To turn less efficient docs into more
efficient docs need national data from EMRs
• CMS will have to stop reimbursing for some expensive treatments that are not very effective

Medical vs. Semiconductor Research
“When I was doing semiconductor device research, it was expected that I would compare my results with other people’s previously published results and that I would comment on the differences.”

Medical vs. Semiconductor Research
“But it seemed to be different in medicine. Medical practitioners primarily tended to publish their own data; they often didn’t compare their data with the data of other practitioners, even in their own field, let alone with the results of other types of treatments for the same condition.”
Andy Grove, Forbes 5/13/96

Though Results Are Unproven Robotic Surgery Wins Converts G. Kolata, NY Times, Feb 14, 2010
• Robotic surgery costs more• $1,500 to $2,000 per patient• Not clear if outcomes are better, worse, or
the same as surgery without robot• No large studies planned or under way
Though Results Are Unproven Robotic Surgery Wins Converts G. Kolata, NY Times, Feb 14, 2010
• Medicare study 2003 to 2007• Compared 6,899 4 inch incision v. 1,983
laparoscopic surgery (many with robot)• Lap: shorter stays, less blood, less resp/surg
complications, more incontinence and impotence

Though Results Are Unproven Robotic Surgery Wins Converts G. Kolata, NY Times, Feb 14, 2010
• Marketing has driven demand• 2009
– 85,000 had prostate surgery– 73,000 had robotic surgery– 86%– 8 years ago 5,000 had robotic surgery
Though Results Are Unproven Robotic Surgery Wins Converts G. Kolata, NY Times, Feb 14, 2010
• “There is no question there is a lot of marketing hype. I just think that in this particular instance, with this particular robot there hasn’t been a quantum leap in anything.” Dr. Gerald Andriole,
Wash U• “I say robotic surgery has to be better to justify its
learning curve, to justify its unknown cancer control, to justify its increased cost.” Dr. H. Lepor
NYU
Though Results Are Unproven Robotic Surgery Wins Converts G. Kolata, NY Times, Feb 14, 2010
• “From Day 1, when I sat down at that robotic console, I knew we would give patients a better outcome.” Dr. Vipul Patel
• It takes 200 to 300 robot-assisted surgeries to become highly proficient
• “The battle is lost. Marketing is driving the case here.” Dr. Jeffrey Cadedu

Though Results Are Unproven Robotic Surgery Wins Converts G. Kolata, NY Times, Feb 14, 2010
• “Doctors and medical centers advertise it, and patients demand it….[creating a] “folie a deux.” Dr. Michael J. Barry, MGH
• “With the stream of prostate cancer patients that come through this is a big, big business.” Dr. Jason Engel, GWU
• Hospital investment– $1.39 million for the robot– $140,000 a year for the service contract

A Simple Health Care Fix Fizzles OutKeith J. Winstein, WSJ, Feb 11, 2010
• Courage Study, NEJM, 2007• 2,287 patients studied for 5 years• Patients with chronic chest pain usually
receive no benefit from stents when used with cocktail of generic drugs
• Cardiac stress testing should be done before stent placement to see what causes pain

A Simple Health Care Fix Fizzles OutKeith J. Winstein, WSJ, Feb 11, 2010
• Boston Scientific shares fell on day study published
• US stent implants declined 13% in the month after the study published
• “Most haven’t voluntarily incorporated the Courage criteria into their practice. What’s going to continue to drive practice is reimbursement.” Dr. William Boden

A Simple Health Care Fix Fizzles OutKeith J. Winstein, WSJ, Feb 11, 2010
• Steven Nissen, MD called study a “blockbuster”
• “It’s certainly remarkable that nothing has been done to put some checks and balances. I have a very strong disagreement with cardiologists who see no reason to do the stress test.” Eric Topol, MD, CAO Scripps

A Simple Health Care Fix Fizzles OutKeith J. Winstein, WSJ, Feb 11, 2010
• Sanjay Kaul, cariologist at Cedars Sinai estimates US could save $5 billion a year if all doctors follow Courage criteria
• Most pts do not receive stress test before receiving stent
• Courage’s finding apply to 1/3 of pts receiving stents
A Simple Health Care Fix Fizzles OutKeith J. Winstein, WSJ, Feb 11, 2010
• Invasive cardiologists average $500,000 a year in 2008
• Up 22% from 1998• Pts have little incentive to decline stent• Cardiologist get $900 per stent procedure• Medicare is legally barred from considering
treatment benefit when deciding how much to pay MD for procedure

A Simple Health Care Fix Fizzles OutKeith J. Winstein, WSJ, Feb 11, 2010
• Washington State Health Technology Assessment Program tried to put Courage criteria into practice
• “We don’t want to end up being our own willing executioners”
• “There were some sincere and also probably some not-so-sincere questions” about definition of stable chest pain
A Simple Health Care Fix Fizzles OutKeith J. Winstein, WSJ, Feb 11, 2010
• Blue Cross Blue Shield of western and northeast New York
• Requires stress test before stent will be paid for
• Patients must try drug therapy for 1 year before receiving elective stent
• “Bill Bolden has been telling me, we’re looking at a potential of $8 billion in savings,” Cynthia Ambres, CMO

Participatory Medicine/Experienced-based
Medicine
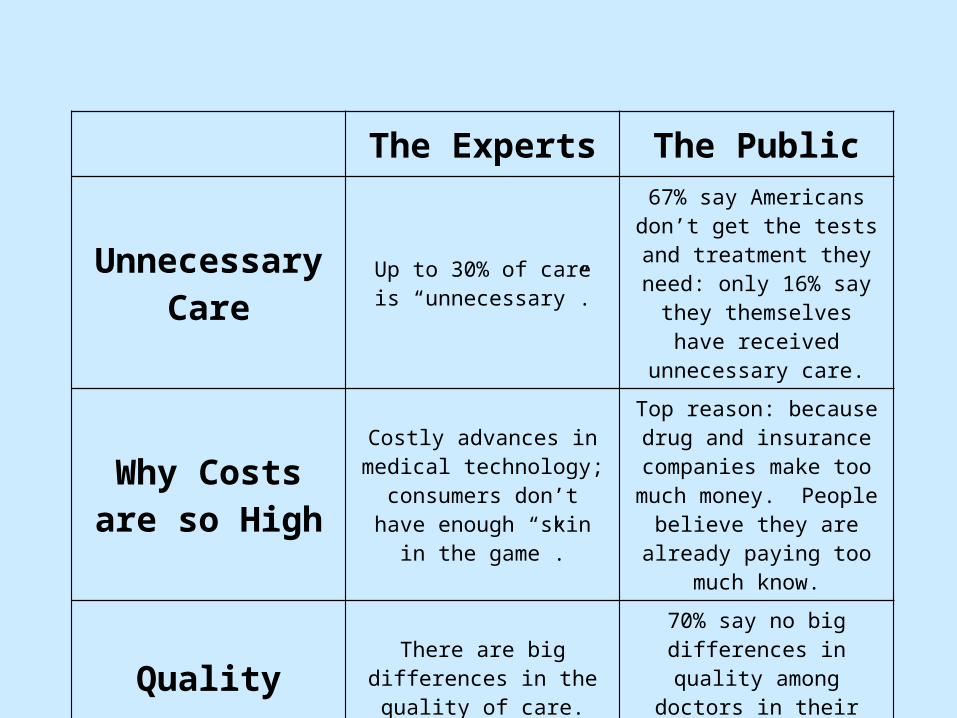
The Experts The Public
Unnecessary Care
Up to 30% of care is “unnecessary”.
67% say Americans don’t get the tests and treatment they
need: only 16% say they themselves have received
unnecessary care.
Why Costs are so High
Costly advances in medical technology; consumers don’t
have enough “skin in the game”.
Top reason: because drug and insurance companies make too much money. People believe they are already paying too much know.
Quality There are big differences in the quality of care.
70% say no big differences in quality among doctors in
their area.
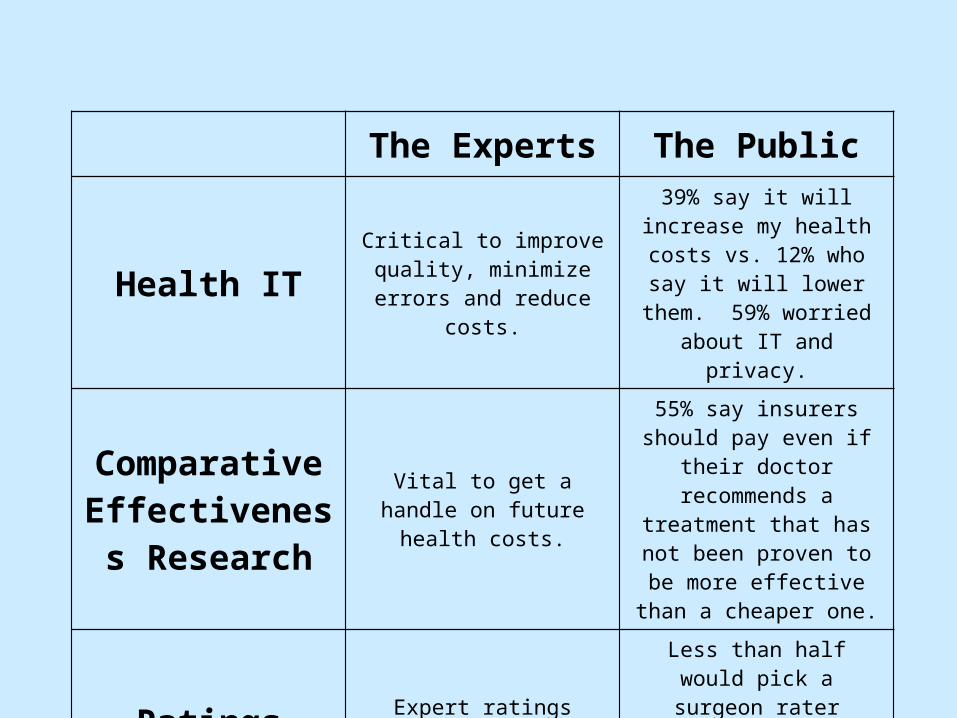
The Experts The Public
Health ITCritical to improve quality, minimize errors and reduce
costs.
39% say it will increase my health costs vs. 12% who say
it will lower them. 59% worried about IT and privacy.
Comparative Effectiveness
Research
Vital to get a handle on future health costs.
55% say insurers should pay even if their doctor
recommends a treatment that has not been proven to be
more effective than a cheaper one.
Ratings Expert ratings should matter.
Less than half would pick a surgeon rater higher by
experts than one they/their family know well.
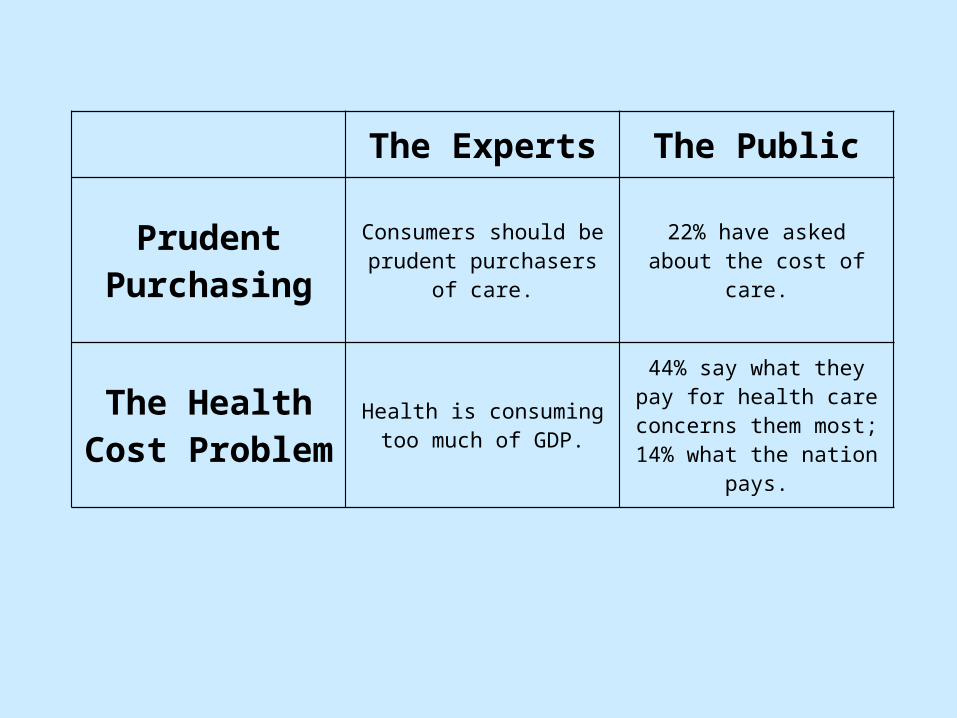
The Experts The Public
Prudent Purchasing
Consumers should be prudent purchasers of care.
22% have asked about the cost of care.
The Health Cost Problem
Health is consuming too much of GDP.
44% say what they pay for health care concerns them most; 14% what the nation
pays.

What Patient-Centered Should MeanDonald M. Berwick, Health Affairs, 28, no. 4 (2009)
• Eliot Freidson posits society cedes authority to profession to judge quality of its own work
• Altruism• Expertise• Self-regulation
What Patient-Centered Should MeanDonald M. Berwick, Health Affairs, 28, no. 4 (2009)
• “They give me exactly the help I need and want exactly when and how I need and want it.”
• “I eschew compromise words like partnership”
• “We should behave not as hosts in the care system, but as guests in their lives.”

What Patient-Centered Should MeanDonald M. Berwick, Health Affairs, 28, no. 4 (2009)
• Patient centeredness improves health status outcomes
• Golomb statin drug takers initiate discussions of symptoms related to drug
• O’Connor on shared decision making found a 23% reduction in surgical interventions
• Patient education can increase compliance

What Patient-Centered Should MeanDonald M. Berwick, Health Affairs, 28, no. 4 (2009)
• The needs of the patient comes first (Mayo)• Nothing about me without me• Every patient is the only patient

What Patient-Centered Should MeanDonald M. Berwick, Health Affairs, 28, no. 4 (2009)
• The experience (to the extent the informed, individual patient desires it) of transparency, individualization, recognition, respect, dignity, and choice in all matters, without exception, related to one’s person, circumstances, and relationships in health care.
What Patient-Centered Should MeanDonald M. Berwick, Health Affairs, 28, no. 4 (2009)
• Hospitals should have no restrictions on visiting
• Patients would choose food and clothes• Patients should participate in rounds• Patients would participate in design of
health care processes and services• Medical records belong to the patient• Shared decision-making used universally

What Patient-Centered Should MeanDonald M. Berwick, Health Affairs, 28, no. 4 (2009)
• Should patient-centeredness trump EBM?• Is physician steward of social resources?• What about clinicians’ needs and wants?

Letting the Patient Call the ShotsPauline Chen, MD, NY Times, June 4, 2009
• “We have built a technocratic castle, and when people come into it, they are intimidated.”
• “When you make someone helpless, in a funny way you make them sicker”
• “Noncompliance is a control word, a power word, and we need a slightly different one”
Letting the Patient Call the ShotsPauline Chen, MD, NY Times, June 4, 2009
• “Speak up and be prepared. Patients who write down questions do better. Bring your digital recorder to the meeting so you can listen to the conversation several times after. Bring a companion along to be your sentinel, your advisor”

Letting the Patient Call the ShotsPauline Chen, MD, NY Times, June 4, 2009
• Shared decision making mandatory• Patients participate in design of processes• Medical records belong to patient• Compliance would become obsolete

Mort Orman, MDMedical Director, Capital BlueCross
• “I couldn’t disagree more with its thesis”• Berwick is for an unequal relationship with
regards to power and control with patient in charge
• I prefer to have an unequal relationship with airline pilot with the pilot in charge
• “I would be just as foolish to think I could better direct my own health care decisions, compared to a trusted professional”

Mort Orman, MDMedical Director, Capital BlueCross
• “The best type of doctor-patient relationship is an unequal one, with the majority of the power and control vested in the professional”
• Gawande identifies why the trust for this to work has vanished

Mort Orman, MDMedical Director, Capital BlueCross
• New version of Hippocratic Oath• “to be both personally and collectively
accountable to improving quality and decreasing costs of health care and to do no harm to the health care system.”
• “to be absolutely worthy of our patients’ trust at all times, both personally and professionally.”
J. Rainey, LA Times on Backlash against debunking vaccine/autism link http://ow.ly/28ziE
• “Citizens armed with information are sure they know better. Readers who brush up against expertise believe they have become experts. The common man rebels against the notion that anyone — not professionals, not the government and certainly not the media — speaks with special authority.”
J. Rainey, LA Times on Backlash against debunking vaccine/autism link http://ow.ly/28ziE
• “Where it stops, nobody knows. But already we see a wave of amateurs convinced they can write a pithier movie review, arrange a catchier song, even assess our planet’s shifting weather conditions, better than the professionals trained to do the job.”