the roles of the normal mechanical properties of articular
TRANSCRIPT

University of Calgary
PRISM: University of Calgary's Digital Repository
Graduate Studies The Vault: Electronic Theses and Dissertations
2013-11-14
The Roles of the Normal Mechanical Properties of
Articular Cartilage in the Contact Mechanics of the
Human Knee Joint: a Finite Element Approach
Dabiri, Yaghoub
Dabiri, Y. (2013). The Roles of the Normal Mechanical Properties of Articular Cartilage in the
Contact Mechanics of the Human Knee Joint: a Finite Element Approach (Unpublished doctoral
thesis). University of Calgary, Calgary, AB. doi:10.11575/PRISM/28370
http://hdl.handle.net/11023/1161
doctoral thesis
University of Calgary graduate students retain copyright ownership and moral rights for their
thesis. You may use this material in any way that is permitted by the Copyright Act or through
licensing that has been assigned to the document. For uses that are not allowable under
copyright legislation or licensing, you are required to seek permission.
Downloaded from PRISM: https://prism.ucalgary.ca

UNIVERSITY OF CALGARY
The Roles of the Normal Mechanical Properties of Articular Cartilage in the Contact Mechanics
of the Human Knee Joint: a Finite Element Approach
by
Yaghoub Dabiri
A THESIS
SUBMITTED TO THE FACULTY OF GRADUATE STUDIES
IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE
DEGREE OF DOCTOR OF PHILOSOPHY
DEPARTMENT OF MECHANICAL AND MANUFACTURING ENGINERING
CALGARY, ALBERTA
NOVEMBER, 2013
© Yaghoub Dabiri 2013

Abstract
In spite of numerous research devoted to the study of the mechanical behaviour of
cartilage, few of them considered fluid pressure in an anatomically accurate knee joint model.
Including the fluid phase as a cartilage constituent, this thesis investigated the mechanics of
human knee joint. The main hypothesis of this thesis was that the depth-wise integrity of the
structure of cartilage has an important role in its mechanical performance especially its fluid
pressurization. The roles of depth-dependent properties, local degenerations and defects on the
knee joint mechanics were modeled. Moreover, the effect of individual muscle forces on the
knee joint mechanics was investigated.
In one of our studies, four models including healthy and degenerated cartilage with local
OA progressed from the superficial, to the middle and deep zones were compared. In another
study, the effects of depth-wise progression of a local cartilage defect on the knee contact
mechanics were investigated. A model with individual muscle forces was compared with a
model without muscle forces to examine the effects of muscle forces.
The normal cartilage produced higher surface fluid pressure under a given compression.
The lack of structural integrity, as happened in local cartilage degeneration, resulted in reduced
fluid pressure in the degenerated zone as well as at the cartilage-bone interface. Cartilage defects,
on the other hand, had more complex effects on knee joint mechanics. While a local superficial
defect reduced pressure in the remaining affected cartilage, a defect advanced to the middle zone
increased fluid pressure. Regarding effects of muscle forces, the knee mechanics was noticeably
affected when muscles were included. Contact pressure, for instance, was significantly increased
in a model with muscle forces compared to a model without muscle forces.
ii

The results were in line with previous experimental and computational studies that
reported the importance of the structural integrity and depth-dependent properties of cartilage.
Integrating fluid pressure, complex three-dimensional geometry, depth-dependent properties,
individual muscle forces, and a more realistic treatment of free surface fluid pressure, this project
aimed to better understanding of human knee joint mechanics. Results may contribute to better
understanding of osteoarthritis as well as the design of artificial cartilage.
iii

Acknowledgements
First of all, I would like to give a special thank you to my family for their patience and support.
Among different people who helped me in this project, my supervisor, Dr. LePing Li, had a
crucial role, and I greatly thank him for his efforts during my program. I would like to thank the
supervisory committee members Dr. Steven Boyd and Dr. Simon Park for their comments, and
examiners Dr. Lidan You and Dr. Elena Di Martino for their efforts in reviewing my thesis and
for their questions and comments during the examination. I would like to express my gratitude to
my colleagues Dr. Mojtaba Kazemi and Mr. Sahand Ahsanizadeh for their precious technical
help as well as their friendship. I also would like to thank the previous member of our research
group Mr. Bill Gu for his help when I started the project. I owe a warm thank you to Mr. Stephen
Cull for his assistance in language and friendship. I would like to give thank you to Dr. Doug
Philips and Dr. Hartmut Schmider for their crucial supports with the computational facilities. I
would like to extend my thanks to Dr. Tannin Schmidt, and Dr. Frank Cheng for acting as the
examiners in my candidacy examination.
iv

Dedication
To my parents
v

Table of Contents
ABSTRACT........................................................................................................................II
ACKNOWLEDGEMENTS.............................................................................................. IV
LIST OF TABLES..........................................................................................................VIII
LIST OF FIGURES AND ILLUSTRATIONS................................................................. IX
LIST OF SYMBOLS, ABBREVIATIONS AND NOMENCLATURE .......................... XI
CHAPTER ONE: INTRODUCTION................................................................................12 1.1 Prevalence of Knee Osteoarthritis ...............................................................................12 1.2 Importance of the Mechanical Modeling.....................................................................13 1.3 Thesis Overview ..........................................................................................................16 1.4 Statement of Contribution............................................................................................17
CHAPTER TWO: BACKGROUND.................................................................................18 2.1 Knee Anatomy .............................................................................................................18 2.2 Cartilaginous Tissues ...................................................................................................20
2.2.1 Swelling of Cartilage ............................................................................................22 2.2.2 Macrostructure of Articular Cartilage and Meniscus ...........................................23 2.2.3 Cartilage Mechanical Tests...................................................................................25
2.3 Cartilage Mechanical Models ......................................................................................26 2.3.1 Single-Phase Models.............................................................................................27 2.3.2 Biphasic Models ...................................................................................................27 2.3.3 Fiber Reinforced Models ......................................................................................28
2.4 Knee Joint Numerical Models .....................................................................................28
CHAPTER THREE: INFLUENCES OF THE DEPTH-DEPENDENT MATERIAL INHOMOGENEITY OF ARTICULAR CARTILAGE ON THE FLUID PRESSURIZATION IN THE HUMAN KNEE ................................................................32 3.1 Abstract ........................................................................................................................32 3.2 Introduction..................................................................................................................33 3.3 Methods........................................................................................................................36 3.4 Results..........................................................................................................................41 3.5 Discussion ....................................................................................................................51 3.6 References....................................................................................................................57
CHAPTER FOUR: ALTERED KNEE JOINT MECHANICS IN SIMPLE COMPRESSION ASSOCIATED WITH EARLY CARTILAGE DEGENERATION ....64 4.1 Abstract ........................................................................................................................64 4.2 Introduction..................................................................................................................65 4.3 Methods........................................................................................................................68 4.4 Results..........................................................................................................................73 4.5 Discussion ....................................................................................................................82 4.6 References....................................................................................................................89
vi

CHAPTER FIVE: LOAD BEARING CHARACTERISTICS OF THE KNEE JOINT DETERIORATES WITH THE DEFECT DEPTH OF ARTICULAR CARTILAGE......97 5.1 Abstract ........................................................................................................................97 5.2 Introduction..................................................................................................................98 5.3 Methods......................................................................................................................100 5.4 Results........................................................................................................................103 5.5 Discussion ..................................................................................................................114 5.6 References..................................................................................................................118
CHAPTER SIX: A PROTOCOL TO INCLUDE INDIVIDUAL MUSCLE FORCES IN AN ANATOMICALLY ACCURATE MODEL OF THE HUMAN KNEE JOINT......125 6.1 The Coordinates of Origin and Insertion Points of Muscles......................................126 6.2 The Forces of Muscles ...............................................................................................132
6.2.1 Enforcing Angles ................................................................................................132 6.2.2 Enforcing Moments ............................................................................................134
6.3 The Optimization Process ..........................................................................................134 6.4 Inclusion of Muscle Forces in the ABAQUS Model .................................................136 6.5 MATLAB M-files......................................................................................................138 6.6 Results........................................................................................................................139
CHAPTER SEVEN: FREE-SURFACE FLUID PRESSURE.........................................142 7.1 Subroutines ................................................................................................................143
7.1.1 FLOW Subroutine...............................................................................................143 7.1.2 URDFIL Subroutine ...........................................................................................145
7.2 Result File ..................................................................................................................148 7.3 Testing the algorithm .................................................................................................149 7.4 Application to the Anatomically Accurate Model .....................................................149
CHAPTER EIGHT: CONCLUSION ..............................................................................153 8.1 Summary....................................................................................................................153 8.2 Limitations .................................................................................................................154 8.3 Future Work ...............................................................................................................157
REFERENCES ................................................................................................................160
APPENDIX 1: THE MATLAB CODE DEVELOPED TO TEST THE FORTRAN CODE FOR ZERO FLUID PRESSURE BOUNDARY CONDITION......................................170
APPENDIX 2: THE FORTRAN CODE DEVELOPED TO IMPLEMENT THE ZERO FLUID PRESSURE FOR NON-CONTACTING SURFACES......................................171
APPENDIX 3: THE COPYRIGHT PERMISSION LETTER ........................................177
JOURNAL AND CONFERENCE PAPERS AND ABSTRACTS.................................182
vii

List of Tables
Table (3-1). Material properties for all tissues used in the inhomogeneous model ..........39
Table (3-2). Material properties for the femoral cartilage in the homogeneous model ....41
Table (4-1). Material properties for the normal tissues ....................................................73
Table (5-1). Ten cases investigated in the present study ................................................103
Table (6-1). The coordinates of origin point of muscles in the knee joint.......................129
Table (6-2). The coordinates of insertion point of muscles in the knee joint ..................130
Table (6-3). The coordinates of the intersection point of muscles line of action ............131
Table (6-4). The moment arm and maximum isometric force of three muscles used in this project (yang et al., 2010, o’connor 1993, kellis and baltzopoulos 1999).......................136
viii

List of Figures and Illustrations
Fig. 2.1. The components of the knee joint........................................................................20
Fig. 2.2. The structure of pgs. ............................................................................................22
Fig. 2.3. The depth-dependent structure of cartilage. ........................................................24
Fig. 2.4. Cartilage tests ......................................................................................................25
Fig 3.1. Total reaction force in the knee joint as a function of time..................................42
Fig. 3.2. Variation of fluid pressure and compressive stress (mpa) along the depth of the femoral cartilage ................................................................................................................43
Fig. 3.3. First principal stress or strain along the depth of the femoral cartilage ..............45
Fig. 3.4. Fluid pressure in the sagittal plane of the femoral cartilage that is cut through the medial condyle ...................................................................................................................46
Fig. 3.5. Fluid pressure in the coronal plane of the femoral cartilage that is cut through the medial condyle ...................................................................................................................47
Fig. 3.6. Maximum fluid pressure in a given layer of elements ........................................48
Fig. 3.7. Fluid pressure at 100s as predicted by the inhomogeneous model......................49
Fig. 3.8. Fluid pressure at 100s as predicted by the homogeneous model .........................50
Fig. 4.1. Finite element model of the tibiofemoral joint, showing the distal femur ..........69
Fig. 4.2. Fluid pressure (mpa) at the normalized depth of 1/16 (superficial layer) ...........75
Fig. 4.3. Fluid pressure (mpa) at the normalized depth of 13/16 (deep layer)...................76
Fig. 4.4. Variation of fluid pressure along the depth of the femoral cartilage...................77
Fig. 4.5. Fluid pressure (mpa) in a sagittal plane of the medial condyle. ..........................78
Fig. 4.6. Fluid pressure (mpa) in a coronal plane of the medial condyle...........................79
Fig. 4.7. Lateral strain along the depth of the femoral cartilage........................................80
Fig. 4.8. First principal strain at the normalized depth of 15/16 (deep layer) ...................81
Fig. 4.9. Shear strains at the normalized depth of 15/16 (deep layer) ...............................82
Fig. 5.1. Surface fluid pressure in the femoral cartilage at 500µm compression ............104
Fig. 5.2. Surface fluid pressure in the femoral cartilage during late relaxation...............105
Fig. 5.3. Fluid pressure in the layer of normalized depth of 1/16 at 500µm ...................107
Fig. 5.4. Fluid pressure in a sagittal plane of the femoral cartilage at 500µm.................108
Fig. 5.5. Reaction force in the knee as a function of time. ..............................................110
Fig. 5.6. Surface fluid pressure in the femoral cartilage at 500µm compression ............111
ix

Fig. 5.7. Shear strain in the deepest cartilage layer .........................................................112
Fig. 5.8. Surface fluid pressure in the femoral cartilage at 387.76n ................................113
Fig. 5.9. Reaction force in the knee as a function of time during the loading phase for the cases of creep and stress relaxation .................................................................................114
Fig. 6.1. Seven coordinate systems are shown in this figure. the origin and insertion coordinates are calculated in these frames.......................................................................127
Fig. 6.2: Inclusion of individual muscle forceS...............................................................138
Fig. 6.3: Contact pressure in the femoral cartilage with (a) and without (b) muscles for approximately 40% of the gait cycle. ..............................................................................141
Fig. 7-1: This algorithm is used to distinguish if an integration point is in contact. .......147
Fig. 7-2: A simple model was used to test the algorithm for finding the closest node to an integration point within the master surface......................................................................149
Fig. 7-3: Surface fluid pressure at the femoral cartilage..................................................151
Fig. 7-4: Surface fluid pressure at the femoral cartilage when no boundary condition was enforced for the free surfaces (@3s)................................................................................152
x

List of Symbols, Abbreviations and Nomenclature
Symbol Definition
𝝈𝝈 Total stress 𝝈𝝈𝑒𝑒𝑒𝑒𝑒𝑒 Solid stress, or effective stress −𝝈𝝈𝑒𝑒𝑓𝑓 Component of stress due to fluid pressure 𝑝𝑝 pore pressure 𝝈𝝈𝑚𝑚 Stress in the nonfibrillar matrix 𝝈𝝈𝑒𝑒 Stress in the fibrillar matrix 𝜆𝜆, 𝜇𝜇 Lamé constants 𝑒𝑒 Volumetric strain 𝜺𝜺 Strain 𝐸𝐸𝑥𝑥,𝑦𝑦,𝑧𝑧 Young’s modulus in x, y or z direction 𝐸𝐸𝑚𝑚 Young’s modulus of the nonfibrillar matrix 𝜐𝜐 Poisson’s ratio of the nonfibrillar matrix 𝑘𝑘𝑥𝑥,𝑦𝑦,𝑧𝑧 Permeability in x, y or z direction 𝜐𝜐𝑥𝑥 Fluid velocity in the x direction 𝑝𝑝𝑒𝑒,𝑥𝑥 X component of fluid pressure gradient 𝜏𝜏Rzx Shear strain parallel to cartilage-bone interface and in x direction 𝜏𝜏Rzy Shear strain parallel to cartilage-bone interface and in y direction 𝛾𝛾zx Shear stress parallel to cartilage-bone interface and in x direction 𝛾𝛾zy Shear stress parallel to cartilage-bone interface and in y direction ��𝜃 Angular acceleration at hip, knee or ankle 𝐻𝐻,𝐾𝐾,𝐴𝐴
��𝜃 Angular velocity at hip, knee or ankle 𝐻𝐻,𝐾𝐾,𝐴𝐴
𝑀𝑀𝐻𝐻,𝐾𝐾,𝐴𝐴 Muscle moment at hip, knee or ankle 𝐽𝐽 Performance criterion 𝑎𝑎𝑚𝑚 Activation of muscle number m 𝐹𝐹𝑚𝑚 Force of muscle number m 𝐹𝐹𝑚𝑚0 Maximum isometric force of the muscle number m 𝑓𝑓 Fluid velocity in the direction of outward normal to cartilage surface 𝑘𝑘0 Seepage coefficient 𝛾𝛾𝑤𝑤 specific weight 𝑐𝑐 Characteristic length of an element
POR Fluid pressure (in ABAQUS) S First principal stress (in ABAQUS)
xi

Chapter One: Introduction
1.1 Prevalence of Knee Osteoarthritis
The knee joint is a complex joint of the human body. Daily activities like walking,
jumping, stair ascent and descent require knee joint function. Research that aim to
reproduce the functions of a biological knee with an artificial one encountered numerous
difficulties such as control, strength, cosmetics, and weight of the joint (Dabiri et al.,
2013, Martinez-Villalpando and Herr 2009, Sup et al., 2008). The knee joint is vulnerable
to disease and injury.
In 2003, knee problems were the main reason for visiting an orthopaedic surgeon
(American Academy of Orthopaedic Surgeons (AAOS), 2007). Knee injuries have been
reported to happen in many sport activities (Hashemi et al., 2011, Cheatham and Johnson,
2010, Larson and Grana, 1993, AAOS, 2007). Among the diseases that might occur at
this joint, the following are examples: osteoarthritis, varus, valgus, tear of ligaments of
knee, injuries to meniscus, and fractures in the joint (Cailliet, 1992).
Arthritis is a common disease of the knee joint. This word stems from Greek
“arthron” and “itis”. The first part means joint and the second part means inflammation.
There are different kinds of arthritis. Osteoarthritis is the most common form of arthritis.
In osteoarthritis, cartilage is gradually degenerated, and eventually leads to bone to bone
contact. This bone to bone contact makes the joint painful. In rheumatic arthritis, another
kind of arthritis, the joint is painful and swollen. Infectious arthritis is another kind of
12

arthritis whereby an infection happens in the joint. This infectious arthritis makes the
joint painful as well (Nordqvist, 2009).
Arthritis is the leading cause of disability in the United States (Centers for
Disease Control and Prevention, 2012), and is reported as one of the major causes of
work limitation (Stoddard et al., 1998). The prevalence of arthritis is higher in the older
population. In the United States, almost 80% of people above 65 years of age suffer from
arthritis (Lawrence et al., 1989, Bagge and Brooks, 1995, Manek and Lane, 2000).
Osteoarthritis (OA) of the joints is the most prevalent cause of disability within the
elderly (Manheimer et al., 2007, Peat et al., 2001, Centers for Disease Control and
Prevention, 2001). Among different joints, the knee has the highest incidence
(Manheimer et al., 2007, Felson and Zhang, 1998, Oliveria et al., 1995). OA is
recognized as a disease with noticeable effects on the sociological, the economical and
the well-being aspects of life (Saarakkala et al., 2010). The prevalence and related costs
of knee osteoarthritis are expected to rise during the next 25 years (Manheimer et al.,
2007, Lethbridge-Cejku et al., 2004).
1.2 Importance of the Mechanical Modeling
OA is divided into two categories: primary OA, and secondary OA. The exact cause of
primary OA is not known; however, it develops as a result of cartilage wear, and is
relevant to how long the joint is used. On the other hand, secondary OA develops as a
results of abnormal conditions like injury, and congenital factors (Tsahakis et al., 1993,
13

Mow and Ratcliffe, 1997). In any case, mechanical loading is the leading parameter in
OA initiation and progression.
While OA is a process including mechanical and biological phenomena, it is
defined as the degeneration of a joint caused primarily by mechanical loading (Radin,
1990 adopted from Pauwels, 1976). In primary OA, the cartilage lesion initiates at a
location which is not routinely under load. An initial lesion develops into other load
bearing areas. A lesion at a load bearing area might further progress into deep cartilage
provided the underlying bone has hardened (Radin, 1990). The progression of lesion into
deep layers, finally leads to cartilage loss and bone to bone contact. In secondary OA, the
initiation of OA might happen from cartilage-bone interface (Atkinson and Haut, 1995).
In this case, the mechanical loading causes microfractures at cartilage-bone interface,
which will develop to further cartilage degeneration.
Therefore, the knowledge about the mechanical behavior of the knee joint is an
essential element in understanding the pathogenesis of osteoarthritis. However, the
complexities involved in the structure and function of the joint make the mechanics of the
joint complicated. The mechanical behavior of the knee joint could be assessed in an
experimental approach or in a mathematical modeling approach. Using an experimental
approach is not always feasible due to some limitations pertaining to ethical issues or
difficulties in practical procedures.
Unlike experimental approaches, mathematical approaches are not limited by
ethical issues. However, some simplifying assumptions have to be made in order to
model the knee joint. The more realistic a mathematical model is, the more reliable
14

results will be. Mathematical models could be divided into two subcategories: analytical
and computational models. The former is capable of producing accurate results for
models that are highly simplified. Computational models, however, could overcome
some of the complexities of modeling the biological joint, and avoid some simplifications
made in an analytical model.
This project used the Finite Element Method (FEM) to study the mechanical
behavior of the knee joint. Three hypotheses investigated in this project were: (1) surface
fluid pressure at the cartilage is enhanced by depth-dependent properties; (2) a local
cartilage degeneration in a high load-bearing area in the medial femoral condyle causes
fluid pressure reduction in the cartilage, and a deeper degeneration is associated with a
higher reduction in fluid pressure; (3) a local cartilage defect in a high load-bearing area
in the medial femoral condyle causes fluid pressure reduction in the cartilage, and a
deeper defect is associated with a higher reduction in fluid pressure. The importance of
individual muscle forces in the contact mechanics was modeled as well. Moreover, free
surface fluid pressure boundary condition was improved compared to previous models.
The commercial software ABAQUS (Simulia Inc., Providence, RI, USA) was used to
implement FEM. By eliminating some limitations which were applied to the previous
studies, this project advances the knowledge of knee joint mechanics. The results could
have implications in prevention and treatment of OA. Designing artificial articular
cartilage using the tissue engineering techniques is another application as suggested in the
literature (Ateshian and Hung, 2005).
15

1.3 Thesis Overview
This is a paper-based thesis. Chapters 3, 4, and 5 are published, accepted journal papers,
or submitted manuscript.
Chapter 3:
Dabiri Y, Li LP. Influences of the depth-dependent material inhomogeneity of articular
cartilage on the fluid pressurization in the human knee. Medical Engineering & Physics
2013; 35(11), 1591-1598.1
Chapter 4:
Dabiri Y, Li LP. Altered knee joint mechanics in simple compression associated with
early cartilage degeneration. Computational and Mathematical Methods in Medicine
2013; 2013:1-11, http://dx.doi.org/10.1155/2013/862903.2
Chapter 5:
Dabiri Y, Li LP. Load Bearing Characteristics of the Knee Joint Deteriorates with the
Defect Depth of Articular Cartilage, Submitted.
Chapters 1 and 2 provide the motivations and background of this work. Chapters
3, 4, and 5 present the mechanics of normal and diseased cartilage with the progression of
OA. Considering a normal model, chapter 3 presents the importance of the depth-
dependent structure and integrity of articular cartilage. The models developed in Chapter
3 (including Table 3-1) were based on models developed by our research group
previously (Gu, 2010). Targeting the early stages of OA, chapter 4 discusses the effects
1 The relevant copyright permission license number from Elsevier is 3207701479466 (Appendix 3). 2 Copyright permission was not required by the journal.
16

of depth-wise progression of degeneration on the mechanical behavior of cartilage.
Considering advanced stages of OA, chapter 5 studies cartilage defects representing the
more severe stages of OA.
Chapters 6 and 7 aim to remove two simplifications in the anatomically accurate
models developed in our research group. Chapter 6 describes a method to consider
individual muscle forces. As a suggestion for future work, the resultant knee joint model
from Chapter 6 can be used to analyse daily living activities such as gait. Chapter 7
introduces a methodology that automatically enforces the free-surface pore pressure
boundary conditions during the solution, based on contact conditions. The fixed free-
surface pore pressure condition used in Chapters 3-5 is only suitable for small knee
compression as will be discussed in Chapter 7. Chapter 8 summarizes the thesis and
explains possible future directions. The references provided in Chapters 4, 5, and 6 are
not repeated in the final “Reference” list that provides the references cited in Chapters 1,
2, 6, 7 and 8.
1.4 Statement of Contribution
The author of this thesis and his supervisor are the authors of the papers used to compose
this thesis (Chapters 3, 4, and 5), and they did the pertaining research work including
development of the computational models, simulations, analysing the results, and writing
the papers.
17
Chapter Two: Background
2.1 Knee Anatomy
There are three classifications for the joints in the human body, namely, synovial
(diarthrodial), cartilaginous (amphiarthroses) and fibrous (synarthroses) joints. Knee and
hip joints are examples of synovial joint which enjoy more mobility compared to the two
other classifications. Examples of cartilaginous and fibrous joints are intervertebral and
skull joints, respectively (Mow and Ateshian, 1997).
The knee joint is one of the biggest joints in the body. This joint is composed of
bones, muscles, ligaments, cartilaginous and other soft tissues (Grana and Larson, 1993).
There are four ligaments in the knee joint that stabilize and control its motion: 1- ACL:
Anterior Cruciate Ligament, 2- PCL: Posterior Cruciate Ligament, 3- MCL: Medical
Collateral Ligament, and 4- LCL: Lateral Collateral Ligament.
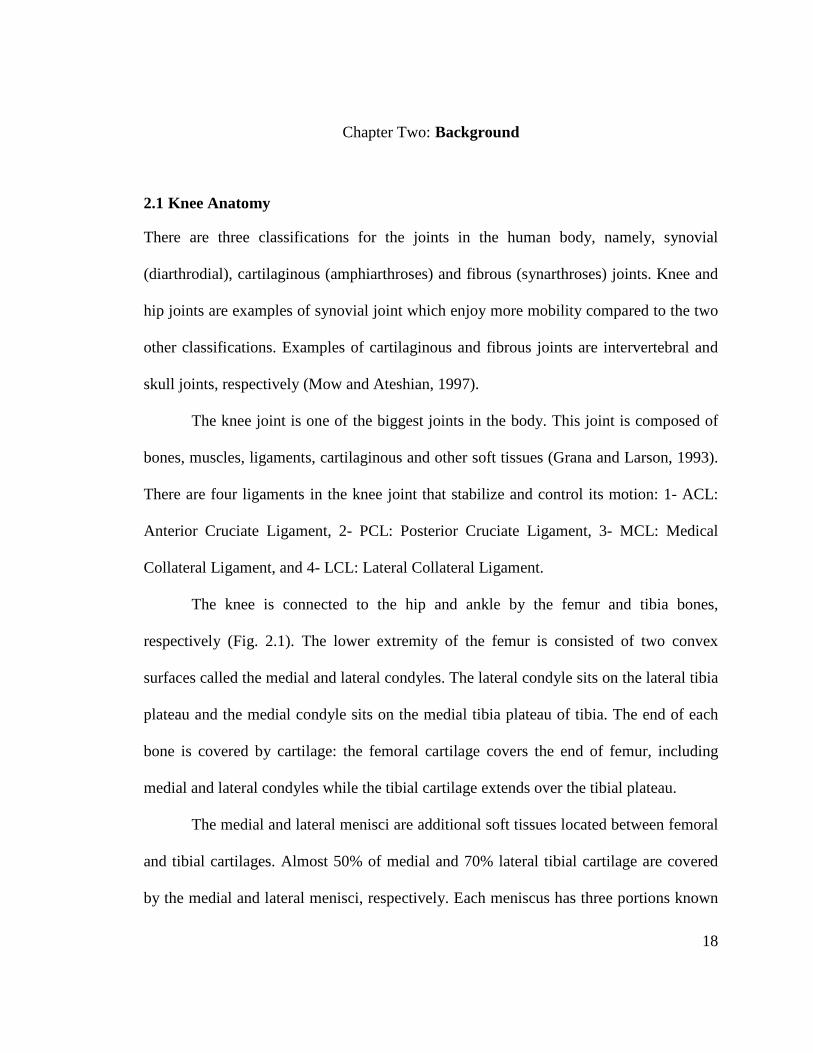
The knee is connected to the hip and ankle by the femur and tibia bones,
respectively (Fig. 2.1). The lower extremity of the femur is consisted of two convex
surfaces called the medial and lateral condyles. The lateral condyle sits on the lateral tibia
plateau and the medial condyle sits on the medial tibia plateau of tibia. The end of each
bone is covered by cartilage: the femoral cartilage covers the end of femur, including
medial and lateral condyles while the tibial cartilage extends over the tibial plateau.
The medial and lateral menisci are additional soft tissues located between femoral
and tibial cartilages. Almost 50% of medial and 70% lateral tibial cartilage are covered
by the medial and lateral menisci, respectively. Each meniscus has three portions known
18

as body, anterior and posterior horns. The medial meniscus is larger, and has a more open
side toward the intercondylar notch. The anterior and posterior horns of medial meniscus
are attached to the tibial plateau. The outer edge of medial meniscus is connected to the
joint capsule. The shape of the lateral meniscus is close to a circle. The anterior horn of
the lateral meniscus is connected to the anterior horn of the medial meniscus through the
transverse ligament. The posterior horn of the lateral meniscus is attached to the posterior
tibia and also has connections with the medial femoral condyle and the popliteus (Rath
and Richmond, 2000, Fox, 2007).
The knee joint is surrounded by a fibrous tissue called the joint capsule lined by
the synovial membrane (synovium). The space within the joint, formed by cartilages and
synovium, is called the joint cavity which is filled with synovial fluid. The synovial fluid,
which is secreted by synovium, plays an important role in lubrication and nourishment of
the joint (Mow and Ateshian, 1997, Nordqvist, 2009).
The third bone in the knee joint is the patella or knee cap. It is located at the
anterior side of the joint and as its primarily function, patella facilitates knee extension.
The fibula is another bone attached proximally to the tibia, and distally to the ankle joint.
At full extension, the femur and tibia define joint mechanics, whereas the patella and
fibula do not play an important role in load support. These components of the knee joint
are depicted in Fig. 2.1.
19

Fig. 2.1. The components of the knee joint (http://en.wikipedia.org/wiki/File:Knee_diagram.svg)
2.2 Cartilaginous Tissues
Cartilage is divided into three groups: hyaline cartilage, elastic cartilage and
fibrocartilage. Articular cartilage is the most common type of hyaline cartilage. Articular
cartilage can be found at the end of long bones in articulating joints like the femoral and
tibial cartilages. The external auditory canals is an example of elastic cartilage. The
cartilage in the intervertebral joints and knee meniscus are examples of fibrocartilages
(Mow and Ratcliffe, 1997).
The tensile properties of cartilage are mainly governed by collagens. The collagen
type in articular cartilage is mainly type II, and the collagen type in meniscus is mainly
20

type I. The diameter of collagens in meniscus is larger than in articular cartilage (Mow
and Ratcliffe, 1997).
The cartilaginous tissues (articular cartilage and meniscus) are composed of two
main phases: a liquid phase and a solid phase. The solid phase is mainly composed of
proteoglycans (PGs), collagens, and chondrocytes. The liquid phase is composed of water
and electrolytes.
The compressive stiffness of articular cartilage is mainly due to proteoglycans
(PGs) (Kempson et al., 1970). PGs are composed of a core protein to which the
glycosaminoglycans (GAGs), including keratine and chondroitin sulfate, are attached.
Proteoglycans could aggregate to hyaluronic acids and, as shown in Fig. 2.2, form a
bottle-brush like structure (Mansour, 2004). The GAG chains contain negative charges,
and produce the cartilage fixed charge density or FCD (Mow and Ratcliffe, 1997). As a
result of the PGs’ negative charge, the fluid pressure within cartilage will be higher than
environmental fluid pressure, and their difference will produce Donnan osmotic pressure
(Mow and Ratcliffe, 1997).
PGs constitute almost 30% of cartilage dry weight (Mansour, 2004), and 5-10%
of its wet weight (Mow and Ratcliffe, 1997). The concentration of PGs varies with depth.
At the surface they have the lowest concentration (~15% dry weight), and their highest
concentration (~25% dry weight) is at the middle region (Mow and Ratcliffe, 1997,
Athanasiou et al., 2010).
21

Fig. 2.2. The structure of PGs.
The FCD applies a swelling pressure within cartilage. This swelling pressure
helps cartilage to support higher loads (Mow and Ratcliffe, 1997). Therefore, the
negative charges in the PGs also contribute to the compressive stiffness of articular
cartilage (Mansour, 2004).
2.2.1 Swelling of Cartilage
The repulsion of identical electrical charges of PGs and the higher fluid pressure caused
by them results in cartilage swelling (Mow and Ratcliffe, 1997). As mentioned before,
the identical charges within PGs produce a fluid pressure which is higher than
environmental fluid pressure. Also, the identical charges produce repulsion forces that
contribute to cartilage swelling. These forces play a role in bearing the applied load.
22

2.2.2 Macrostructure of Articular Cartilage and Meniscus
The extracellular matrix (ECM) of articular cartilage is a network of collagen fibers
embedded in a gel built from PGs. Therefore, cartilage can be considered as a fiber
reinforced composite solid (Mizrahi et al., 1986, Mow and Ratcliffe, 1997).
The structure of cartilage varies with depth. As shown in Fig. 2.3, the tissue is
often divided into three zones. The superficial zone comprises ~10-20% of cartilage
thickness. In this zone, the collagen fibers are oriented parallel to the surface according to
the split-lines. The concentration of collagens in this zone is the highest, while the
concentration of PGs is the lowest. The middle (transitional) zone comprises ~40-60% of
cartilage thickness. The collagen fibers are dispersed randomly in this zone. The
concentration of PGs is the highest, and the concentration of collagen fibers is lower
compared to the surface zone. The deep zone comprises ~30% of cartilage tissue in which
the fibers are perpendicular to the cartilage tide mark. The subchondral and cancellous
bones are located below the deep zone and tide mark (Mow and Ratcliffe, 1997). The
mechanical properties of cartilage also vary along the depth, which will be explained in
section 3.2.
23

Fig. 2.3. The depth-dependent structure of cartilage.
As mentioned earlier, similar to articular cartilage, meniscus is also comprised of
the nonfibrillar matrix, fluid, and fibers. The fibers are mainly randomly oriented in the
surface zone of menisci. Almost 100 µm from the surface, within the two-thirds of the
peripheral region, the fibers are oriented circumferentially. These circumferential fibers
are grouped together by supporting radial fibers. In the inner regions, the fibers are
randomly oriented (Mow and Ratcliffe, 1997).
Articular cartilage is an inhomogeneous tissue. The properties of articular
cartilage are both site- and depth-dependent. Site-dependency implies the variation of the
properties of cartilage with location at a specific depth, whereas depth-dependency is
associated with the alteration of the properties in a depth-wise manner.
24

2.2.3 Cartilage Mechanical Tests
In experimental studies of cartilage, four main test configurations can be found (Hasler et
al., 1999, Knecht et al., 2006, Korhonen et al., 2002): unconfined compression, confined
compression, indentation (Fig. 2.4) and tensile testing.
(a) Load (b) Load
Permeable Piston Cartilage Sample Cartilage Impermeable Plates
Sample
Confining Chamber Fig. 2.4. Cartilage tests: (a) confined compression, (b) unconfined (c) Load compression, (c) indentation.
Indenter Cartilage
Subcondral Bone
In a confined setup, the fluid is not allowed to escape through the surrounding
wall, although it can escape through the load-applying piston. The stress-strain results
from confined compression tests can be used to calculate the aggregate modulus and
permeability. For this purpose, based on the biphasic theory (Mow et al., 1980),
compressive stress and applied strain are fitted to the experimental data (Schinagl et al.,
1997, Soltz and Ateshian, 1998). The Young’s modulus can also be calculated from the
confined compression experiment (Korhonen et al., 2002).
25

In unconfined compression, the cartilage sample is under an impermeable plate,
and fluid flow can exude from the lateral sides. This setup can be used to measure the
dynamic modulus of cartilage under a sinusoidal (Park et al., 2004) or instantaneous
deformation step (Saarakkala et al., 2003). After equilibrium is reached, the static
Young’s modulus and Poisson ratio can be calculated.
The indentation test is another experiment used to calculate the mechanical
properties of cartilage. The indentation test can be used to calculate the Young's modulus
and the shear modulus of the cartilage assuming the cartilage is a linear elastic solid
material (Hayes et al., 1972). Compared with the confined and unconfined compression
tests, the advantage of using an indentation test is to keep the integrity of the tissue in the
testing region.
The tensile specimen of cartilage is similar to those discussed in the Mechanics of
Materials, except the cross-section can only be rectangular. Dumbbell shape specimens
are often prepared.
2.3 Cartilage Mechanical Models
Cartilage is generally poromechanical, viscoelastic, anisotropic, and heterogeneous. Its
behavior is strain and strain rate dependent, and its responses differ in tension and
compression (Taylor and Miller, 2006).
Analytical methods could be used to solve the governing equations when the
material model and geometry are sufficiently simplified. Numerical methods, however,
are often used to extract the mechanical parameters from measured data (Carter and
26

Wong, 2003 adopted from Hughes, 1987). For complex testing geometries and realistic
material models, only numerical methods are capable of solving the problem.
2.3.1 Single-Phase Models
Single-phase models assume cartilage as an incompressible or nearly incompressible
solid material (Carter and Wong, 2003). These models can be appropriate for loading
conditions where the fluid flow is not significant such as in short term static loading or
moderate to high frequency cyclic loading (Carter and Wong, 2003).
2.3.2 Biphasic Models
The other approach to model cartilage acknowledges the presence of fluid inside the
tissue. When the fluid exudation is significant, the single phase models fail to predict the
response of articular cartilage, which is time dependent. The poroelastic or consolidation
(Biot, 1941) and biphasic or mixture (Mow et al., 1980) models consider the time-
dependent response produced by the fluid pressurization (Hasler et al., 1999, Taylor and
Miller, 2006, Carter and Wong, 2003). The consolidation approach assumes the material
as a porous solid saturated with fluid. The biphasic approach assumes the material as a
continuum mixture of the solid and fluid parts. Basically, these are two different methods,
but for an incompressible material they are equivalent (Levenston et al., 1998). At each
point of cartilage, the total stress is the sum of the effective stress and the fluid pressure:
𝝈𝝈 = 𝝈𝝈𝑓𝑓𝑓𝑓 + 𝝈𝝈𝑒𝑒𝑓𝑓𝑓𝑓 (2-1)
27

Where σ, σfland σeff are the total stress, fluid stress (the negative of the pore pressure),
and effective stress (or stress in the solid), respectively. Using pore pressure p
𝝈𝝈 = −𝑝𝑝𝐈𝐈 + 𝝈𝝈𝑒𝑒𝑓𝑓𝑓𝑓 (2-2)
2.3.3 Fiber Reinforced Models
In the fiber reinforced model, the collagen fibers are included in the modeling. The tissue
is assumed to be composed of a nonfibrillar matrix and collagen network. The
nonfibrillar matrix supports compression, some tension, and shear and the fibrillar matrix
supports only tension. In mathematical form:
𝝈𝝈𝑒𝑒𝑓𝑓𝑓𝑓 = 𝝈𝝈𝑚𝑚 + 𝝈𝝈𝑓𝑓 (2-3)
Where 𝝈𝝈𝑒𝑒𝑒𝑒𝑒𝑒 is the effective stress in both matrices, 𝝈𝝈𝑚𝑚 is the stress supported by
nonfibrillar matrix, and 𝝈𝝈𝑒𝑒 is the stress in the fibrillar matrix which is zero under
compression. In the fibril-reinforced models, the time-dependent response is accounted
for by the fluid flow and intrinsic viscoelasticity of the collagen network (Li et al., 1999;
Li and Herzog, 2004). The fibril-reinforced poro-viscoelastic models also consider the
intrinsic viscoelasticity of the nonfibrillar (PG) matrix (Wilson et al., 2004).
2.4 Knee Joint Numerical Models
Cartilage models with standard simplified geometry fail to explain important features
inherent to the complex three-dimensional geometry of cartilaginous tissues. Regarding
the knee joint, femoral cartilage, tibial cartilages, and menisci not only are in contact
28

altogether but also they are attached to bones. The multiple contacts between
cartilaginous tissue and their attachments to the bones have important roles in the
mechanical behavior of both the whole knee joint and individual cartilaginous tissues.
For example, the femoral cartilage is in contact with menisci and tibial cartilages, and it
is bonded to the femur. The fluid flow and displacements at the contacting and the
cartilage-bone interface regions influence the mechanical behavior of femoral cartilage.
Those regions, however, are defined by the three-dimensional geometry of the femoral
cartilage as well as the tibial cartilages, the menisci, and the femur distal head. Moreover,
the orientations and locations of individual muscle forces can be defined in a model if the
three-dimensional geometry of the knee joint is considered.
Three-dimensional models have been developed to analyze the mechanical
behavior of the knee joint. They have followed different mathematical approaches to take
geometrical and material properties of the knee joint into consideration. Some studies
implemented more simplifying assumptions. The numerical solutions became more
dominant rather than exact analytical solutions as studies tried to model the knee joint
more realistically. The reader could compare a study by Blankevoort and colleagues and
another report by Bendjaballah and colleagues (Blankevoort et al., 1991, Bendjaballah et
al., 1995). In the former study the bone surfaces were approximated using polynomials
(continuous functions), but the latter study reconstructed bone surfaces from
computerized tomography data using segmented images. In addition, the former study
(Blankevoort et al., 1991) failed to consider cartilages as separate parts in the model but
considered their effect on the contact between bones whereas the latter study
29

(Bendjaballah et al., 1995) analyzed the model with cartilages as additional parts
discretized into finite elements.
Knee joint computational models could be validated using experimental data such
as contact pressure and deformations (Kazemi et al., 2013). For instance, the
patellofemoral contact pressure and area for different knee angles were reported in a
study (Powers et al., 1998), where the mean contact stress under an axial load at 0º knee
flexion angle was 0.62 MPa. The maximum contact pressure in the tibial cartilage was
reported to be 5.5 MPa in another study (Papaioannou et al., 2008). The reported data
depend on the conditions of the experiments including the magnitude of the load,
constraints, and knee joint angle.
Anatomically accurate three-dimensional (3D) models of the knee joint are
developed from imaging data (Kazemi et al., 2013). The geometry of our model was built
based on MRI. Software packages such as Mimics (Materialise, Leuven, Belgium), and
Rhinoceros (Seattle, WA, USA) were used to segment the images and reconstruct the 3D
geometry. The geometry was then meshed for finite element calculations using software
packages such as ABAQUS (Simulia, Providence, USA).
The work presented in this thesis could be considered as a progress in numerical
modeling of the knee joint. Several anatomically accurate finite element models have
been reported in the literature. Each study is based on simplifying assumptions such as
exclusion of fluid pressure, considering cartilaginous tissues as isotropic linear elastic
models, ignoring the depth-dependent properties, neglecting effects of a lesion depth on
the lesion progression, and ignoring the individual muscle forces (Bendjaballah et al.,
30

1995, Peña et al., 2005, Shirazi et al., 2008, Mononen et al., 2012). This project provides
a model where some of these limitations are removed.
31

Chapter Three: Influences of the Depth-dependent Material Inhomogeneity of Articular Cartilage on the Fluid Pressurization in the Human Knee3
3.1 Abstract
The material properties of articular cartilage are depth-dependent, i.e. they differ in the
superficial, middle and deep zones. The role of this depth-dependent material
inhomogeneity in the poromechanical response of the knee joint has not been investigated
with patient-specific joint modeling. In the present study, the depth-dependent and site-
specific material properties were incorporated in an anatomically accurate knee model
that consisted of the distal femur, femoral cartilage, menisci, tibial cartilage and proximal
tibia. The collagen fibers, proteoglycan matrix and fluid in articular cartilage and menisci
were considered as distinct constituents. The fluid pressurization in the knee was
determined with finite element analysis. The results demonstrated the influences of the
depth-dependent inhomogeneity on the fluid pressurization, compressive stress, first
principal stress and strain along the tissue depth. The depth-dependent inhomogeneity
enhanced the fluid support to loading in the superficial zone by raising the fluid pressure
and lowering the compressive effective stress at the same time. The depth-dependence
also reduced the tensile stress and strain at the cartilage–bone interface. The present 3D
modeling revealed a complex fluid pressurization and 3D stresses that depended on the
mechanical contact and relaxation time, which could not be predicted by existing 2D
3 This chapter contains a journal paper published on Medical Engineering and Physics. The relevant copyright permission license number from Elsevier is 3207701479466 (Appendix 3).
32

models from the literature. The greatest fluid pressure was observed in the medial
condyle, regardless of the depth-dependent inhomogeneity. The results indicated the roles
of the tissue inhomogeneity in reducing deep tissue fractures, protecting the superficial
tissue from excessive compressive stress and improving the lubrication in the joint.
KEYWORDS: Articular cartilage mechanics; Cartilage heterogeneity; Collagen fiber
orientation; Finite element analysis; Fluid pressure; Knee joint mechanics
3.2 Introduction
The major components of articular cartilage are collagen fibers, proteoglycans and
synovial fluid (Mow et al., 1980, Mow and Ratcliffe, 1997). The compressive and shear
stiffness of the tissue are governed by the proteoglycan matrix, while the tensile stiffness
is governed by the collagen fibers. The collagen network also greatly contributes to the
apparent compressive stiffness at fast loading through the fluid pressurization, which is
enhanced by fiber reinforcement (Mizrahi et al., 1986, Li et al., 2002). The fluid is also
responsible for the poromechanical behavior of the tissue (Mow et al., 1990): the fluid
pressure supports up to 90% of applied compressive loading (Ateshian and Hung, 2005),
which reduces to an insignificant level at equilibrium. The cartilaginous tissues are
commonly modeled as biphasic (Mow and Mansour, 1977, Mak et al., 1987).
The structure and properties of cartilage, e.g. fiber orientation and hydraulic
permeability, change along the depth of the tissue from the articular surface to the bone
interface (Maroudas and Bullough, 1968, Minns and Steven 1977). This change is
33

referred to as depth-dependent material inhomogeneity, or zonal differences. The
superficial zone is composed of fibers parallel to the articular surface, the fibers in the
middle zone are not oriented in a specific direction, and the fibers in the deep zone are
mainly perpendicular to the bone surface (Weiss et al., 1968, Minns and Steven 1977,
Jeffery et al., 1991). The importance of depth-dependent inhomogeneity has been the
subject of experimental and theoretical studies (Schinagl et al., 1997, Chen et al., 2001a,
Chen et al., 2001b, Mow and Guo, 2002, Julkunen et al., 2007, Federico and Herzog,
2008, Chegini and Ferguson 2010, Saarakkala et al., 2010,). These studies could be
categorized into (1) simplified geometries that pertain to standard testing such as
confined and unconfined compression tests (Schinagl et al., 1997), and (2) three-
dimensional anatomically accurate geometries (Shirazi et al., 2008).
Concerning the first category, previous studies reported the importance of depth-
dependence in the mechanical behavior of articular cartilage in unconfined compression
tests (Korhonen et al., 2008, Li et al., 2000, Li et al., 2002). The mechanical behavior of
cartilage with depth-dependent properties in confined compression was also investigated
simultaneously with unconfined compression (Wilson et al., 2004, Wilson et al, 2005). In
addition, it was reported that the alternation of permeability along the depth affected fluid
pressurization and the mechanical behavior of the tissue (Setton, et al., 1993).
The second category, three-dimensional models of human knee, has been
developed to study the mechanical behavior of the knee in normal and pathological
conditions (Bendjaballah et al., 1995, Périé and Hobatho., 1998, Peña et al., 2005, Peña et
al., 2008). Only two of the 3D models, however, have considered the material properties
34

in a depth-dependent manner. The first one was an elastic model without fluid pressure
(Shirazi et al., 2008). The second one modeled the fluid pressure and zonal dependent
fiber orientation to investigate the short-term load response (Mononen et al., 2012),
which is virtually elastic. The influence of the depth-dependence may not have been
adequately shown in these two studies because of two reasons. First, the mechanical
response of the tissue associated with the collagen network is more significant when
substantial fluid pressure is present (Mizrahi et al., 1986, Oloyede et al., 1992, Li et al.,
2002). Second, the poromechanical response was not investigated. A previous study
indicated more significant influence of fiber orientation during early relaxation (Li et al.,
2009).
Therefore, the objective of the present study was to determine what mechanical
parameters of articular cartilage in the knee were affected by the depth-dependent
material inhomogeneity. We were interested in fluid pressurization and dissipation in the
tissues. An MRI-based knee joint model was used for this purpose. The collagen fibers,
depth-dependent inhomogeneity, and fluid pressure were simultaneously considered for
the cartilaginous tissues. In order to understand the significance of the depth-dependence,
the results from the proposed model were compared with those obtained from a recently
published model that did not include the depth-dependence (Gu and Li, 2011). The
proposed model was otherwise the same as the published model: the fiber and fluid
phases were particularly considered in both models.
35

3.3 Methods
A recently published knee joint model (Gu and Li, 2011) was modified to include depth-
dependent material properties in the femoral cartilage. The proposed model will be
referred to as the inhomogeneous model, because both depth-dependent and site-specific
material properties were incorporated. For the convenience of discussion, the published
model will be referred to as the homogeneous model: it was homogeneous in the
direction of the tissue thickness, although the site-specific material properties were also
considered.
In the literature, the continuous variation of the depth-dependence is often
characterized with three distinct zones. The superficial, middle and deep zones contain,
respectively, 10%-20%, 40%-60% and almost 30% of the cartilage thickness (Mow et al.,
1992, Newman, 1998). For the simplicity of the present inhomogeneous modeling, the
three zones were taken to be approximately 25%, 50% and 25% of the cartilage
thickness. They were further meshed with 2, 4 and 2 layers of elements respectively.
Therefore, there were in total 8 layers of elements in the thickness direction. As the input
of the finite element analysis, the fibers in the superficial zone were assumed to be in
split-line directions (Below et al., 2002); the fibers in the middle zone were randomly
distributed along the three directions, and the fibers in the deep zone were oriented
perpendicular to the bone surface.
For the tibial cartilage, complete measurement data of fiber orientation were not
found from the literature, although split-lines in the submeniscal region were arranged in
a wheel-spoke pattern (Goodwin et al., 2004). Therefore, the mechanical properties were
36

assumed the same for all directions, i.e. no preferred fiber orientation was considered for
the tibial cartilage. For the meniscus, the fibers were incorporated primarily in the
circumferential and secondly in the radial directions (Fithian et al., 1990).
The constitutive behavior of the tissues is described by a fibril-reinforced model
previously published (Li et al., 2000). Some equations are included here for the
convenience of reading. The total stress in the tissue, which is the stress in the mixture, is
determined by the fluid pressure, p, and the effective stress of the solid matrix, σeff
σ = − pI σ+ eff (3-1)
where the effective stress consists of the effective stress of the orthotropic fibrillar matrix,
σ f , and the effective stress of the isotropic nonfibrillar matrix defined by the Lamé
constants λ and µ
eff fσ = λeI + 2µε σ+ (3-2)
where e is the volumetric strain and ε is the strain. The fibrillar matrix mimics the
collagen network, while the nonfibrillar matrix mimics the proteoglycan matrix. As a first
approximation, the fibrillar stress is neglected if the tissue is in compression in the fiber
direction. The tensile stress in the fibrillar matrix is determined by (Li et al., 2009)
dσ f = E f dε (3-3)x x x
where Exf is the fibrillar modulus in the x-direction, which aligns in the direction of
fibers or primary fibers. For the case of small fibrillar strains,
37

E f = E0 + Eε ε (3-4)x x x x
where Ex 0 and Ex
ε are direction- and depth-dependent constants. Replacing x with y and
z, respectively, will derive the corresponding equations for the transverse directions.
Obviously, this formula will not be valid when the tensile strain is large. Fortunately,
when cartilage is compressed from the articular surface, the lateral tensile strain is only a
fraction of the compressive strain. Therefore, this simple formula can approximate
moderate compressions.
The Lamé constants λ and µ in Eq. (3-2) can be replaced by the Young’s modulus
and Poisson’s ratio, Em and νm , of the nonfibrillar matrix. For the inhomogeneous
model, the two parameters for the femoral cartilage were approximated as linear
functions of the tissue depth z
(3-5)Em = E m (1+αE z h) ,νm =ν m (1+ αν z h)
νwhere Em and m are respectively the Young’s modulus and Poisson’s ratio at the
articular surface; h is the tissue thickness; αE and αν are positive constants. This
equation was proposed in a previous study (Li et al., 2000) based on data from the
literature (Schinagl et al., 1996, Schinagl et al., 1997).
Darcy’s law was used to describe the fluid flow in the tissues. The permeability of
the femoral cartilage was assumed to increase from the superficial zone to middle zone,
and then decrease through the deep zone (Maroudas and Bullough, 1968, Muir et al.,
1970, Setton et al., 1993). The material properties for the tibial cartilage, menisci and
bones were the same as what were used in a previous study (Gu and Li, 2011). The 38

material properties for all tissues are summarized in Table (3-1). When these properties
were combined with the site-specific fiber orientation, the spatial inhomogeneity was
incorporated, i.e. both depth-dependence and site-dependence were considered in the
inhomogeneous model.
Table (3-1). Material properties for all tissues used in the inhomogeneous model (modulus: MPa; permeability: 10−3mm4/Ns). The x is the primary fiber direction, i.e. the split-line direction for the superficial zone, the depth direction for the deep zone, and the circumferential direction for the meniscus. The y and z are perpendicular to the primary fiber direction in the local coordinate system. The material properties in the y and z directions are assumed to be the same. Thus a symbol, y/z, is used to denote either y or z direction.
Tissue Fibrillar matrix
Nonfibrillar matrix
Permeability
Ex Ey/z Em νm x y / z
Femoral cartilage
Deep 3+1600ε x
0.9+480εy/z 0.80 0.36 1.0 0.5
Middle 2+1000ε x
2+1000εy/z 0.60 0.30 3.0 1.0
Superficial 4+2200ε x
1.2+660εy/z 0.20 0.16 1.0 0.5
Tibial cartilage 2+1000ε x
2+1000εy/z 0.26 0.36 2.0 1.0
Menisci 28 5 0.50 0.36 2.0 1.0
Bones E = 5000 ν = 0.30
The surface-to-surface contact (ABAQUS manual) was defined between the
following contact pairs: femoral cartilage (master surface) and meniscus, femoral (master 39

surface) and tibial cartilages, and tibial cartilage (master surface) and meniscus. Using the
TIE option in ABAQUS, the following tissues were attached to each other at their
interfaces: femoral cartilage to femoral distal surface, and tibial cartilage to tibial
proximal surface. The ends of menisci were fixed to the tibial proximal surface using the
TIE option, too.
Pore pressure elements were used to mesh cartilages and menisci, and solid
elements were used to mesh bones. The 20-node hexahedral elements (C3D20P) were
used for the femoral cartilage, and 8-node hexahedral elements (C3D8P) were used for
meniscus and tibia cartilage. This choice had the potential of better fluid pressure results
for the femoral cartilage, and yet good numerical convergence in the contact modeling,
since the 20-node elements experienced more difficulties in the contact convergence than
the 8-node elements (as stated in the ABAQUS manual). The femur and tibia were
meshed using 4-node tetrahedral elements to better approximate the surface geometries of
the bones than using the hexahedral elements.
The soil consolidation procedure in ABAQUS was used to simulate the stress
relaxation in the tissues. The procedure was initially developed for the calculation of soil
settlement, but has been widely used to account for the transient response of biological
tissues. A ramp compression of the knee of 0.5 mm was applied at 0.1 mm/s, and then
held unchanged for 400s (stress relaxation). The bottom of tibia was fixed while the
displacement was applied on the top of the femur. The femur was not constrained in
rotations, but its top was constrained against translations in the transverse plane. The part
of distal femur in consideration was 104 mm in height (Gu and Li, 2011). Therefore, the
40

constraints on the top still allowed considerable sliding between the articulating surfaces.
The fluid pressure was given to be zero at the articular surface, if it was not in contact
with its mating surface.
To assess the role of depth-dependent inhomogeneity on the contact mechanics of
the joint, the homogeneous model was also considered with constant properties along the
direction of the tissue thickness. In the homogeneous model, the fiber orientation in all
zones was assumed to be the same as the split-line direction (Below et al., 2002), noting
that the split-lines were site-specific. The material properties for the homogeneous model
(Table 3-2) were chosen so that the reaction forces at maximum compression were
virtually identical for the homogeneous and inhomogeneous models (Fig. 3.1).
Table (3-2). Material properties for the femoral cartilage in the homogeneous model (modulus: MPa; permeability: 10−3mm4/Ns). The x is the primary fiber direction. The properties for the tibial cartilage, menisci and bones are the same as shown in Table (3-1) for the inhomogeneous model.
Tissue
Fibrillar matrix Nonfibrillar matrix Permeability
Ex Ey/z Em νm x y / z
Femoral cartilage 3+1600εx 0.9+480εy/z 0.55 0.36 2.0 1.0
3.4 Results
The results are mainly presented for the femoral cartilage, because the depth-dependent
properties were implemented in this tissue. The total forces obtained from the two models
are very close after careful selection of the material properties for the homogeneous
model (Fig. 3.1). In our preliminary study, we attempted to match the force at 0.1mm
41

compression using a different elastic modulus for the homogeneous model. The two force
curves deviated from each other soon after the ramp compression, resulting in 10%
difference at equilibrium (not shown).
385N @ 500𝜇𝜇m
Fig 3.1. Total reaction force in the knee joint as a function of time. A ramp compression of 500µm was applied in 5s followed by relaxation. The material properties for the homogeneous model were chosen so that the corresponding force obtained was the same as that predicted by the inhomogeneous model at 500µm compression, as marked by the star.
The depth variations of short-term and long-term fluid pressures are shown for a
central contact location (Figs. 3.2a and b). For better understanding of the mechanism of
fluid pressurization, the compressive effective stress is also presented (Figs. 3.2c and d).
The total compressive stress in the tissue thickness direction is the sum of this stress and
42

the fluid pressure (Eq. (3-1)). In either model prediction, the depth variation of the
compressive stress was opposite to that of fluid pressure (Figs. 3.2c vs a; 3.2d vs b). For
instance, the compressive stress increased with the depth (Fig. 3.2d), while the fluid
pressure decreased with the depth (Fig. 3.2b).
Depth Depth
Flui
d Pr
essu
re (M
Pa)
(a) (b)
Depth Depth
Stre
ss (M
Pa)
(c) (d)
Fig. 3.2. Variation of fluid pressure and compressive stress (MPa) along the depth of the femoral cartilage, shown for a location in the central contact region of the lateral condyle. The compressive stress refers to the normal stress of the matrix in the
43

direction of cartilage thickness (positive = compressive). Results were calculated at the centroids of the elements (middle of each layer of elements). The depth is normalized by the thickness (0 = articular surface; 1 = bone interface).
The first principal stress and strain are tensile and mainly produced by the lateral
expansion when it is compressed in the perpendicular direction (Figs. 3.3). However, at
the cartilage-bone interface, they were greatly influenced by the shearing at the interface.
So their variations were different there (Fig. 3.3). The first principal stress here was
calculated from the effective stresses. This stress must be subtracted by the fluid pressure
in order to obtain the total principal stress in the tissue as a mixture, because the effective
stress is now positive but the pressure is negative by nature (Eq. (3-1)).
The fluid pressure contours are shown for a sagittal section and a coronal section
of the contact region (Figs. 3.4 and 3.5). For the case of the inhomogeneous model, the
maximum pressure in each of the contours is shown with the maximum value in the
corresponding legend. For the case of the homogeneous model, the exact value of the
maximum pressure is not actually shown in the figure. They are, therefore, included in
the figure captions.
For both model predictions, the fluid pressures in the central contact region were
generally greater in the superficial zone than that in the deep zone (Figs. 3.6b vs a; Fig.
3.4). However, the pressures also decayed faster in the superficial zone so that the long
term pressures were more uniform along the depth than short-term pressures (Figs. 3.4–
3.6). The maximum fluid pressure occurred in the medial condyle, regardless the layers
and material models that were considered (Figs. 3.7 and 3.8).
44

Depth Depth (a) (b)
Depth Depth
Stra
in
Stre
ss
(c) (d)
Fig. 3.3. First principal stress or strain along the depth of the femoral cartilage, shown for a location in the central contact region of the lateral condyle (positive = tensile). Results were calculated at the centroids of the elements (middle of each layer of elements). The depth is normalized by the thickness (0 = articular surface; 1 = bone interface).
45

(a)
(b)
Fig. 3.4. Fluid pressure in the sagittal plane of the femoral cartilage that is cut through the medial condyle. (a) At 20 s and (b) at 400 s. The articular surface is shown at the bottom side; the posterior side is on the left. For the homogeneous case, the maximum pressures at 20 and 400s were 1.617 and 0.459 MPa respectively.
46

(a)
(b)
Fig. 3.5. Fluid pressure in the coronal plane of the femoral cartilage that is cut through the medial condyle only. (a) At 20s and (b) at 400s. The articular surface is shown at the bottom side; the lateral side is on the left. For the homogeneous case, the maximum pressures at 20 and 400s were 1.617 and 0.590 MPa respectively.
47

(a)
(b) Fig. 3.6. Maximum fluid pressure in a given layer of elements. (a) At the normalized depth of 13/16 (center of the 7th layer, deep zone), and (b) at the normalized depth of 3/16 (center of 2nd layer, superficial zone). The peak value shown in (a) are 1.676 and 1.657 MPa, respectively, for the inhomogeneous and homogeneous cases; the peak values shown in (b) are 1.880 and 1.758 MPa, respectively, for the inhomogeneous and homogeneous cases.
48

(a)
(b) Fig. 3.7. Fluid pressure at 100s as predicted by the inhomogeneous model at the normalized depth of (a) 13/16, and (b) 3/16 (0 = articular surface).
49

(a)
(b)
Fig. 3.8. Fluid pressure at 100s as predicted by the homogeneous model at the normalized depth of (a) 13/16, and (b) 3/16 (0 = articular surface).
50

3.5 Discussion
The depth-dependent material inhomogeneity enhanced the fluid pressure and pressure
gradient in the superficial zone of the contact region with less significant influence on the
pressurization in the middle and deep zones. This is observed when the fluid pressures
predicted by the inhomogeneous and homogeneous models are compared (Figs. 3.2a, b,
3.4 and 3.5). With the inhomogeneous material properties, fiber orientations in the tissue
are favorable to the fluid pressurization in the superficial zone. Our results are consistent
with what has been reported for tissue discs under uniform compression (Li et al., 2002)
and for a hexahedral tissue block under indentation (Li et al., 2009). Our results also
support qualitatively the conclusion from an independent study (Krishnan et al., 2003)
that inhomogeneous cartilage properties enhance superficial interstitial fluid support.
However, both our homogeneous and inhomogeneous models predicted slightly higher
pressures in the superficial layer of the central contact region as compared to that in the
deep layer. In the reported study (Krishnan et al., 2003), the homogeneous model
predicted a lower fluid pressure in the superficial layer as compared to that in the deep
zone, while the inhomogeneous model predicted similar fluid pressures in the superficial
and deep layers. This difference in the depth-varying fluid pressures could have been
produced by the different contact geometries and constitutive models considered in the
two studies. In the reported study (Krishnan et al., 2003), the indentation of a flat piece of
tissue with a spherical indentor was simulated using the conewise linear elastic
constitutive model. In the present study, a more realistic knee joint contact was simulated
including the menisci. The use of a fibril-reinforced constitutive model in the present
51

study should also have highlighted the role of the collagen network in the fluid
pressurization in the tissue. It must be noted that the depth variation of the fluid pressure
is different in other regions. For example, the surface pressure is close to zero at the
border of the contact region, but higher in the deep layers there (Figs 3.4 and 3.5).
Articular cartilage in situ exhibited more complex behavior than the explants in
vitro. The present 3D modeling revealed a complex fluid pressurization and 3D stresses
that depended on the mechanical contact and relaxation time, which could not be
predicted by existing 2D models from the literature. The depth-varying fluid pressure in
the outer contact region and noncontact region were different from that in the central
contact region (Figs. 3.4 and 3.5). The pressure distribution in the sagittal plane was
different from that in the coronal plane (Figs. 3.4 and 3.5). Furthermore, the depth-
varying fluid pressure altered with stress relaxation (the results for 5s vs 400s in Fig. 3.4
or 3.5). Both the magnitude and distribution of the fluid pressure were less sensitive to
the depth-dependent inhomogeneity at longer times (Figs. 3.2b, 3.2d, 3.4b and 3.5b,
400s). The tensile strain was the highest in the superficial zone (Fig. 3.3c and d), which
cannot be modeled using a cartilage disk (Li et al., 2000) because of the differences in
boundary conditions. Optical measurement with tissue disks showed maximum tensile
strain in the deep layer, and smallest in the superficial layer (Jurvelin et al., 1997).
The stresses in the tissue matrix were modulated by the fluid pressurization
(Oloyede and Broom, 1991, Oloyede and Broom, 1993). A raised fluid pressure in the
superficial zone reduced the effective stress in the tissue matrix – the depth variation of
the compressive stress was opposite to that of fluid pressure (Fig. 3.2). This fluid pressure
52

mechanism is believed to protect the tissue matrix from excessive stresses. The material
inhomogeneity enhanced this mechanism. When it is not pressurized, the superficial
tissue is softer than the deeper tissue, which is favorable for joint motion. The raised fluid
pressure in the superficial zone enhanced the load support of the softer tissue in the
superficial zone. In general, the ratio of the fluid pressure to solid stress in the superficial
zone was higher in the inhomogeneous model than the homogeneous one (Fig. 3.2a vs. c;
Fig. 3.2b vs. d), which implied reduced frictions by the depth-dependent material
inhomogeneity (McCutchen, 1962, Forster and Fisher, 1996, Ateshian et al., 1998,
Ateshian 2009).
The depth-dependent material inhomogeneity caused a stress concentration
between the superficial and middle zones (Fig. 3.3a and b). This must be partially
produced by the implementation of discontinuous material properties there, especially the
change in the collagen fiber orientation. In reality, however, there is no distinct boundary
between the two zones. Therefore, the stress there must have been overestimated. A more
accurate prediction requires the implementation of material properties that continuously
vary over the tissue thickness. The first principal strain, however, monotonically reduced
with the tissue depth until the cartilage-bone interface (Fig. 3.3c and d). The maximum
tensile strain in the deep zone was less than half of that in the superficial zone. These
results might indicate that the zonal differences protected the deep layers and cartilage–
bone interface from excessive stress and strain (Fig. 3.3), which was in line with the in
vitro result that superficial layers played a protective role for deep layers (Setton et al.,
53

1993). The deep layer fractures occurred frequently (Meachim and Bentley, 1978).
Normal depth-dependent properties may reduce the occurrence of the fractures.
The fluid pressure distribution within a cartilage layer parallel to the articular
surface was similar in pattern for the homogenous and inhomogeneous models (Figs. 3.8
vs. 3.7), but somewhat dependent on the relaxation time (not shown). The distribution
was determined by the site-specific fiber orientation which were the same in the two
material models. These results indicate the possibility of using the homogeneous model
(which is homogenous in the depth direction but site-specific) to predict certain
mechanical responses of the knee, as long as these differences are taken into
consideration when the results are interpreted. When a homogeneous model was used, 4
layers of elements yielded fast converged results (Gu and Li, 2011).
A few limitations exist in the current modeling. First, only 8 layers of elements
were used in the present study, which was not accurate enough for describing the large
depth variations in stresses and pressures (Figs. 3.2 and 3.3). This limitation might have
produced some numerical errors in variables with large gradients in the tissue thickness
direction, such as stress concentrations (Fig. 3.3a and b). When more layers of elements
were used, however, we experienced extremely slow numerical convergence with the
very thin elements. It was not simply the issue with the increased degrees of freedom, but
more trouble with the tolerance of contact convergence. The use of 8 layers of elements
gave us some quality results, although smoother depth variations would be obtained, if
more layers were meshed in the tissue thickness direction. Furthermore, accurate
54

representation of the depth variations requires the segmentation of the three zones with
intensive imaging analysis, although such techniques are available (Potter et al., 2008).
Another limitation of the study was the use of non-physiological loading, which
made it possible to obtain some simple results. Furthermore, we have simulated stress
relaxation other than creep loading in order to speed up the computation, because a creep
testing would take much more time to complete (Li et al., 2008, Kazemi et al., 2013). For
the sake of fast convergence as well, the ramp compression was applied in 5s rather than
in a shorter, realistic time (0.5–1s). Therefore, the fluid pressure and the tensile stresses
have been underestimated. Even with these simplifications, it took approximately one
month to complete a single computation. Our current goal is to understand the
fundamental mechanism of the poromechanical response of the knee joint. We wish to
determine the mechanics under simple loadings and gain experiences in this type of
modeling before moving to more realistic problems. These simplifications do not seem to
compromise this goal.
The use of a small deformation theory is another key factor leading to reduced
convergence complexities. In a previous study (Li et al., 1999), the sensitivity of three
nonlinear factors to the load response was investigated, i.e. nonlinear fibrillar property,
nonlinear permeability and large deformation. It was found that the combined effect of
nonlinear permeability and large deformation on the results was not nearly as significant
as that of the nonlinear fibrillar property. The model was able to describe experimental
data only when the nonlinear fibrillar property was considered. Therefore, the effect of
large deformation was ignored but the fibrillar nonlinearity was considered in the present
55

study. However, this simplification will only affect the magnitudes of the results, e.g. the
predicted fluid pressure could be somewhat underestimated. The qualitative results and
conclusion would remain the same, should a large deformation theory be used.
The constitutive model used in the present study has been previously validated
against multiple experimental data in unconfined compression and tensile testing, such as
simultaneous prediction of creep and relaxation in unconfined compression (Li et al.,
2008). The tissue model was able to account for the great ratios of the transient vs.
equilibrium load responses observed in experiments (Li et al., 1999, Li et al., 2008). The
strong transient response is believed to be caused by the interplay between fibril
reinforcement and fluid pressurization (Li et al., 1999, Li et al., 2003). Therefore,
collagen fibers and fluid pressure were incorporated in the present knee model. Collagen
fibril reinforcement, however, must be interpreted as a mathematical approximation of
the complex structure of the tissues.
Published studies on the mechanical behavior of articular cartilage associated with
the zonal differences were limited to either simple explants geometries with the inclusion
of fluid pressure (Krishnan et al., 2003, Wilson et al., 2005, Korhonen et al., 2008), or
realistic knee contact geometry with elastic or nearly elastic response (Shirazi et al.,
2008, Mononen et al., 2012). We have implemented the depth-dependent material
inhomogeneity in an anatomically accurate knee contact model including the fluid flow
and pressure, as well as the site-specific fiber orientation. The poromechanical response
of the knee joint was also investigated. Some of the present results were qualitatively
similar to those obtained from the explants, e.g. the depth-dependent material
56

inhomogeneity enhanced the fluid pressurization in the superficial zone (Krishnan et al.,
2003). Other results, such as the 3D fluid pressures and 3D stress concentrations, as well
as the spatial distribution of tensile strain reduction at the cartilage-bone interface, could
only be obtained using the current 3D modeling. These findings may be applied in the
studies of osteoarthritis and cartilage tissue engineering (Ateshian and Huang, 2005),
after the modeling has been extended with more realistic loadings.
Acknowledgements
Competing interests: None declared
Funding: Natural Sciences and Engineering Research Council of Canada and the
Canadian Institutes of Health Research.
Ethical approval: E-22593, University of Calgary, for the use of MRI of human subjects.
3.6 References
Ateshian GA. The role of interstitial fluid pressurization in articular cartilage lubrication.
J Biomech 2009;42:1163-76.
Ateshian GA, Hung CT. Patellofemoral joint biomechanics and tissue engineering. Clin
Orthop Relat Res 2005;81:81-90.
Ateshian G, Wang H, Lai W. The role of interstitial fluid pressurization and surface
porosities on the boundary friction of articular cartilage. J Tribo Trans ASME
1998;120:241-248.
57

Below S, Arnoczky SP, Dodds J, Kooima C, Walter N. The split-line pattern of the distal
femur: a consideration in the orientation of autologous cartilage grafts. Arthroscopy
2002;18:613-7.
Bendjaballah MZ, Shirazi-AdI A, Zukor DJ. Biomechanics of the human knee joint in
compression: reconstruction, mesh generation and finite element analysis. Knee
1995;2:69-79.
Chegini S, Ferguson SJ. Time and depth dependent Poisson's ratio of cartilage explained
by an inhomogeneous orthotropic fiber embedded biphasic model. J Biomech
2010;43:1660-6.
Chen AC, Bae WC, Schinagl RM, Sah RL. Depth- and strain-dependent mechanical and
electromechanical properties of full-thickness bovine articular cartilage in confined
compression. J Biomech 2001a;34:1-12.
Chen SS, Falcovitz YH, Schneiderman R, Maroudas A, Sah RL. Depth-dependent
compressive properties of normal aged human femoral head articular cartilage:
relationship to fixed charge density. Osteoarthritis Cartilage 2001b;9:561-9.
Federico S, Herzog W. On the anisotropy and inhomogeneity of permeability in articular
cartilage. Biomech Model Mechanobiol 2008;7:367-78.
Fithian DC, Kelly MA, Mow VC. Material properties and structure-function relationships
in the menisci. Clin Orthop Relat Res 1990;252:19-31.
Forster H, Fisher J. The influence of loading time and lubricant on the friction of articular
cartilage. Proc Inst Mech Eng 1996;210:109-119.
58

Goodwin DW, Wadghiri YZ, Zhu H, Vinton CJ, Smith ED, Dunn JF. Macroscopic
structure of articular cartilage of the tibial plateau: influence of a characteristic matrix
architecture on MRI appearance. AJR Am J Roentgenol 2004;182:311-8.
Gu KB, Li LP. A human knee joint model considering fluid pressure and fiber orientation
in cartilages and menisci. Med Eng Phys 2011;33:497-503.
Jeffery AK, Blunn GW, Archer CW, Bentley G. Three-dimensional collagen architecture
in bovine articular cartilage. J Bone Joint Surg Br 1991;73:795-801.
Julkunen P, Kiviranta P, Wilson W, Jurvelin JS, Korhonen RK. Characterization of
articular cartilage by combining microscopic analysis with a fibril-reinforced finite-
element model. J Biomech 2007;40:1862-70.
Jurvelin JS, Buschmann MD, Hunziker EB. Optical and mechanical determination of
Poisson's ratio of adult bovine humeral articular cartilage. J Biomech 1997;30:235-41.
Kazemi M, Dabiri Y, Li LP. Recent advances in computational mechanics of the human
knee joint. Comput Math Methods Med 2013;2013:1–27,
http://dx.doi.org/10.1155/2013/718423.
Korhonen RK, Julkunen P, Wilson W, Herzog W. Importance of collagen orientation and
depth-dependent fixed charge densities of cartilage on mechanical behavior of
chondrocytes. J Biomech Eng 2008;130:021003.
Krishnan R, Park S, Eckstein F, Ateshian GA. Inhomogeneous cartilage properties
enhance superficial interstitial fluid support and frictional properties, but do not provide a
homogeneous state of stress. J Biomech Eng 2003;125:569-77.
59

Li LP, Buschmann MD, Shirazi-Adl A. A fibril reinforced nonhomogeneous poroelastic
model for articular cartilage: inhomogeneous response in unconfined compression. J
Biomech 2000;33:1533-41.
Li LP, Cheung JT, Herzog W. Three-dimensional fibril-reinforced finite element model
of articular cartilage. Med Biol Eng Comput 2009;47:607-15.
Li LP, Korhonen RK, Iivarinen J, Jurvelin JS, Herzog W. Fluid pressure driven fibril
reinforcement in creep and relaxation tests of articular cartilage. Med Eng Phys
2008;30:182-89.
Li LP, Shirazi-Adl A, Buschmann MD. Alterations in mechanical behaviour of articular
cartilage due to changes in depth varying material properties–a nonhomogeneous
poroelastic model study. Comput Methods Biomech Biomed Engin 2002;5:45-52.
Li LP, Shirazi-Adl A, Buschmann MD. Investigation of mechanical behavior of articular
cartilage by fibril reinforced poroelastic models. Biorheology 2003;40:227-33.
Li LP, Soulhat J, Buschmann MD, Shirazi-Adl A. Nonlinear analysis of cartilage in
unconfined ramp compression using a fibril reinforced poroelastic model. Clin Biomech
(Bristol, Avon) 1999;14:673-82.
Mak AF, Lai WM, Mow VC. Biphasic indentation of articular cartilage–I. Theoretical
analysis. J Biomech 1987;20:703-14.
Maroudas A, Bullough P. Permeability of articular cartilage. Nature 1968;219:1260-1.
McCutchen CW. The frictional properties of animal joints. Wear 1962;5:1-17.
Meachim G, Bentley G. Horizontal splitting in patellar articular cartilage. Arthritis
Rheum 1978;21:669-74.
60

Minns RJ, Steven FS. The collagen fibril organization in human articular cartilage. J Anat
1977;123:437-57.
Mizrahi J, Maroudas A, Lanir Y, Ziv I, Webber TJ. The "instantaneous" deformation of
cartilage: effects of collagen fiber orientation and osmotic stress. Biorheology
1986;23:311-30.
Mononen ME, Mikkola MT, Julkunen P, Ojala R, Nieminen MT, Jurvelin JS, et al.
Effect of superficial collagen patterns and fibrillation of femoral articular cartilage on
knee joint mechanics–a 3D finite element analysis. J Biomech 2012;45:579-87.
Mow VC, Fithian DC, Kelly MA. Fundamentals of articular cartilage and meniscus
biomechanics. In: Ewing JW, editor. Articular cartilage and knee joint function: basic
science and arthroscopy. New York: Raven Press; 1990. p. 1-18.
Mow VC, Guo XE. Mechano-electrochemical properties of articular cartilage: their
inhomogeneities and anisotropies. Annu Rev Biomed Eng 2002;4:175-209.
Mow VC, Kuei SC, Lai WM, Armstrong CG. Biphasic creep and stress relaxation of
articular cartilage in compression? Theory and experiments. J Biomech Eng
1980;102:73-84.
Mow VC, Mansour JM. The nonlinear interaction between cartilage deformation and
interstitial fluid flow. J Biomech 1977;10:31-9.
Mow V, Ratcliffe A. Structure and function of articular cartilage and meniscus. In: Mow
V and Hayes W, editors. Basic orthopaedic biomechanics. second ed. Philadelphia:
Lippincott-Raven, 1997. p. 113-77.
61

Mow VC, Ratcliffe A, Poole AR. Cartilage and diarthrodial joints as paradigms for
hierarchical materials and structures. Biomaterials 1992;13:67-97.
Muir H, Bullough P, Maroudas A. The distribution of collagen in human articular
cartilage with some of its physiological implications. J Bone Joint Surg Br, 1970;52:554
63.
Newman AP. Articular cartilage repair. Am J Sports Med 1998;26:309-24.
Oloyede A, Broom N. Is classical consolidation theory applicable to articular cartilage
deformation? Clin Biomech 1991;6:206-212.
Oloyede A, Broom N. Stress-sharing between the fluid and solid components of articular
cartilage under varying rates of compression. Connect Tissue Res 1993;30:127-41.
Oloyede A, Flachsmann R, Broom ND. The dramatic influence of loading velocity on the
compressive response of articular cartilage. Connect Tissue Res 1992;27:211-24.
Peña E, Calvo B, Martínez MA, Doblaré M. Computer simulation of damage on distal
femoral articular cartilage after meniscectomies. Comput Biol Med 2008;38:69-81.
Peña E, Calvo B, Martínez MA, Palanca D, Doblaré M. Finite element analysis of the
effect of meniscal tears and meniscectomies on human knee biomechanics. Clin Biomech
(Bristol, Avon) 2005;20:498-507.
Périé D, Hobatho MC. In vivo determination of contact areas and pressure of the
femorotibial joint using non-linear finite element analysis. Clin Biomech (Bristol, Avon)
1998;13:394-402.
Potter HG, Black BR, Chong LR. New techniques in articular cartilage imaging. Clin
Sports Med 2009;28:77–94, http://dx.doi.org/10.1016/j.csm.2008.08.004.
62

Saarakkala S, Julkunen P, Kiviranta P, Mäkitalo J, Jurvelin JS, Korhonen RK. Depth-
wise progression of osteoarthritis in human articular cartilage: investigation of
composition, structure and biomechanics. Osteoarthritis Cartilage 2010;18:73-81.
Schinagl RM, Gurskis D, Chen AC, Sah RL. Depth-dependent confined compression
modulus of full-thickness bovine articular cartilage. J Orthop Res 1997;15:499-506.
Schinagl RM, Ting MK, Price JH, Sah RL. Video microscopy to quantitate the
inhomogeneous equilibrium strain within articular cartilage during confined compression.
Ann Biomed Eng 1996;24:500-12.
Setton LA, Zhu W, Mow VC. The biphasic poroviscoelastic behavior of articular
cartilage: role of the surface zone in governing the compressive behavior. J Biomech
1993;26:581-92.
Shirazi R, Shirazi-Adl A, Hurtig M. Role of cartilage collagen fibrils networks in knee
joint biomechanics under compression. J Biomech 2008;41:3340-8.
Weiss C, Rosenberg L, Helfet AJ. An ultrastructural study of normal young adult human
articular cartilage. J Bone Joint Surg Am 1968;50:663-74.
Wilson W, van Donkelaar CC, van Rietbergen R, Huiskes R. The role of computational
models in the search for the mechanical behavior and damage mechanisms of articular
cartilage. Med Eng Phys 2005;27:810-26.
Wilson W, van Donkelaar CC, van Rietbergen B, Ito K, Huiskes R. Stresses in the local
collagen network of articular cartilage: a poroviscoelastic fibril-reinforced finite element
study. J Biomech 2004;37:357-66.
63

Chapter Four: Altered Knee Joint Mechanics in Simple Compression Associated with Early Cartilage Degeneration4
4.1 Abstract
The progression of osteoarthritis can be accompanied by depth dependent changes in the
properties of articular cartilage. The objective of the present study was to determine the
subsequent alteration in the fluid pressurization in the human knee using a three-
dimensional computer model. Only a small compression in the femur-tibia direction was
applied to avoid numerical difficulties. The material model for articular cartilages and
menisci included fluid, fibrillar and nonfibrillar matrices as distinct constituents. The
knee model consisted of distal femur, femoral cartilage, menisci, tibial cartilage, and
proximal tibia. Cartilage degeneration was modeled in the high load-bearing region of the
medial condyle of the femur with reduced fibrillar and nonfibrillar elastic properties and
increased hydraulic permeability. Three case studies were implemented to simulate (1)
the onset of cartilage degeneration from the superficial zone, (2) the progression of
cartilage degeneration to the middle zone, and (3) the progression of cartilage
degeneration to the deep zone. As compared with a normal knee of the same
compression, reduced fluid pressurization was observed in the degenerated knee.
Furthermore, faster reduction in fluid pressure was observed with the onset of cartilage
degeneration in the superficial zone and progression to the middle zone, as compared to
progression to the deep zone. On the other hand, cartilage degeneration in any zone
4 This chapter contains a paper published on Computational and Mathematical Methods in Medicine that does not require copyright permission.
64
would reduce the fluid pressure in all three zones. The shear strains at the cartilage-bone
interface were increased when cartilage degeneration was eventually advanced to the
deep zone. The present study revealed, at the joint level, altered fluid pressurization and
strains with the depth-wise cartilage degeneration. The results also indicated
redistribution of stresses within the tissue and relocation of the loading between the tissue
matrix and fluid pressure. These results may only be qualitatively interesting due to the
small compression considered.
KEYWORDS: Articular cartilage mechanics; Finite element analysis; Fluid pressure;
Human knee; Joint mechanics; Osteoarthritis; Zonal differences
4.2 Introduction
Osteoarthritis (OA) is the most prevalent cause of disability among the elderly ( CDC,
2001; Peat et al., 2001, Manheimer et al., 2007). Among all joints, the knee has the
highest incidence of OA ( Oliveria et al., 1995, Felson and Zhang, 1998, Manheimer et
al., 2007). The onset and progression of OA is related to the mechanical environment of
articular cartilage (Griffin and Guilak, 2005). In fact, the cartilage morphology,
biosynthesis, and pathogenesis are strongly associated with its mechanical loading
(Guilak and Mow, 2000). Therefore, the better the mechanical behavior of cartilage is
understood, the better treatment and prevention strategies could be planned.
Osteoarthritis has been reported to initiate with deterioration from cartilage
surface or cartilage-bone interface (Meachim and Bentley, 1978). The former is believed
to be a result of surface wear or splitting, and the latter a result of high stiffness gradient
65

at cartilage-bone interface (Meachim and Bentley, 1978; Carter et al., 2004). An altered
mechanical environment, such as by stress, strain, and fluid flow, affects the biosynthesis
of chondrocytes (Wong and Carter, 2003), and eventually leads to tissue degeneration
and loss, and exposure of bone surface to direct joint contact.
When OA is initiated from the surface, it progresses layer by layer, from the
superficial zone, to the middle and eventually deep zones (Arokoski et al., 2000). During
this process, each layer of the tissue suffers from an altered mechanical environment, e.g.
the stress, strain, and fluid pressure in the deeper layer can be altered by degenerated
superficial layers.
The mechanics of depth-wise (layer by layer) progression of OA in the knee joint
must be affected by the multiple contacts between the cartilaginous tissues, including
femoral cartilage, meniscus, and tibial cartilage. A few factors may be important in the
contact mechanics of the knee. First, the 3D geometry of these tissues is obviously a
dominant parameter that determines the contact area and distribution of contact loading.
Second, the fluid pressurization in these tissues plays an essential role in the mechanical
functions of the knee, because the knee compression is associated with high fluid
pressure in these cartilaginous tissues (Ateshian and Hung, 2005). Additionally, the
depth-dependent tissue properties, often being characterized by three discrete zones, may
also affect the mechanical behavior of the joint.
Great progress has been made in computational OA modeling, with major
simplifications on the geometry including unrealistic boundary conditions, and on the
material properties including absence of fluid and fiber properties. For those studies with
66

fluid pressure considered, some assumed a spherical contact in the knee with no meniscus
(Wu et al., 2000, Federico et al., 2004, 2005); others modeled unconfined compression
testing only. The effect of PG depletion and collagen degradation was investigated by
reducing the modulus of the two constituents, respectively (Korhonen et al., 2003).
Unconfined geometry was used with a fibril reinforced model (Li et al., 1999). In another
study, OA was modeled in a depth-dependent manner (Saarakkala et al., 2010). The
depth-dependent properties were used for cartilage based on values reported in the
literature (Wilson et al., 2006). Again, unconfined compression geometry was used in the
study. A major progress was made recently in knee OA modeling when both 3D
geometry and fluid pressure in articular cartilage were implemented (Mononen et al.,
2012). In this latest study the fluid flow in the menisci was ignored, which could possibly
affect the prediction of the contact mechanics of the joint. Furthermore, the depth-
dependent mechanical properties were not incorporated in the study.
Computer modeling may provide an effective tool to examine the effect of
cartilage degeneration on contact mechanics and especially fluid pressure within the
intact joint. We attempted to study the contact mechanics with an anatomically accurate
finite element (FE) model of the normal and osteoarthritic knee joint. The material model
for the cartilaginous tissues included nonfibrillar matrix, fibers, fluid and depth-
dependent properties. We hypothesized that, due to perturbations induced by OA, the
fluid pressure in the tissue would be reduced with a given knee compression
(displacement-control). To examine this hypothesis a normal model was compared with
case studies whereby depth-wise progression of cartilage degeneration was implemented.
67

As a first step for our OA modeling of the knee, cartilage degeneration was assumed in
the high load-bearing region of the medial condyle. This is one of the regions where the
lesions are more likely progressed to deep layers (Seedholm et al., 1979, Andriacchi et
al., 2004, Carter et al., 2004), although OA lesions were also found in other sites of
femoral cartilage (Seedholm et al., 1979, Bae et al., 2010). The medial condyle was
chosen because it was believed to carry higher load compared to the lateral condyle
(Brown and Shaw, 1984). The medial condyle was reported to be more susceptible to OA
development in both normal (Temple et al., 2007) and ligament-deficient knees ( Maffulli
et al., 2003, Strobel et al., 2003, Tandogan et al., 2004). The medial condyle experienced
the most rapid lesion progression (Biswal et al., 2002).
4.3 Methods
The geometry of the model was reconstructed from MRI images of the right knee of a 27
year-old male subject, who had no symptoms of OA (SPGR sequence, 625×625µm
resolution, Sagittal scan). The model included the distal femur, femoral cartilage,
meniscus, tibial cartilage, and proximal tibia (Fig. 4.1). The maximum thickness of the
femoral cartilage was approximately 2.8mm, and the maximum thickness of the menisci
was 8.4mm (Gu and Li, 2011).
68

Fig. 4.1. Finite element model of the tibiofemoral joint, showing the distal femur, proximal tibia, menisci, femoral and tibial cartilages. The tibial cartilage on the medial side is essentially covered by the medial meniscus (right knee, medial side shown on the left of the figure). The femoral cartilage is further shown with 8 layers of elements.
The cartilaginous tissues, i.e. femoral cartilage, menisci, and tibial cartilage, were
assumed as fibril-reinforced fluid-saturated materials. A fibril-reinforced constitutive law
was used which models the solid of the tissue as a linear nonfibrillar matrix that is
reinforced by a nonlinear fibrillar matrix (Li et al., 1999). Hence, two material properties
were required to define the nonfibrillar matrix, i.e. the elastic modulus Em and Poisson’s
ratio νm. The fibrillar matrix was characterized by elastic moduli in three orthogonal
directions. For the case of small deformations considered in the present study, these
69

moduli were simplified as linear functions of the corresponding tensile strain, e.g. for the
local x-direction
0 εε (4-1)Ex + Ex x , if ε x ≥ 0Ex =
0 , if ε x < 0
The compressive stiffness of the fibrillar matrix was neglected because the fibers
mainly support tensile loading. Note that the x-direction could be oriented in different
directions for different sites. Therefore, a 3D collagen orientation could be thus
incorporated. In order to describe the interstitial fluid flow, an orthotropic hydraulic
permeability was introduced per Darcy’s law, e.g. for the local x-direction
= −k p x (4-2)vx x f ,
where kx is the x-component of the permeability, which is the negative ratio of the x-
component of the fluid velocity, vx, and the x-component of the fluid pressure gradient,
pf ,x . Simply replacing the subscript x in Eqs. (4-1) and (4-2) with y or z would obtain the
relevant equations for the y or z direction.
The depth-dependent properties were incorporated for the femoral cartilage, i.e.
the tissue properties varied with the superficial, middle and deep zones, in the way
approximated previously (Li et al., 2000). In the superficial zone, the fibers were oriented
according to the split lines recorded from the surface (Below et al., 2002, adopted from
Fig. 2 in Gu and Li, 2011). In the middle zone, the fibers did not have any specific
orientation. In the deep zone, they were vertical to the cartilage-bone interface. In the
meniscus, the primary fibers were oriented in the circumferential direction. No preferred
fiber directions were considered for the tibial cartilage due to lack of data. 70

The surface-to-surface contact was defined between articulating surfaces using ABAQUS
6.10. Namely, contact was defined between: femoral cartilage and meniscus, femoral
cartilage and tibial cartilage, meniscus and tibial cartilage. No fluid flow was assumed
between cartilage and bone. The cartilages and bones were meshed independently.
However, in reality, the cartilage is firmly attached to the bone. There is no relative
motion at the cartilage-bone interface. This interface condition was modeled using the
TIE contact option provided by ABAQUS, i.e., femoral cartilage was tied to femur,
medial and lateral tibial cartilages were tied to tibia, and meniscus horns were tied to the
tibial cartilage at both ends of each meniscus.
A ramp compression of 0.1mm was applied in 1s on top of the femur while the
bottom of the tibia was fixed. The knee was in full extension. As a boundary condition,
the free articulating surface (which was not in contact) was assigned to zero fluid
pressure.
The consolidation procedure in ABAQUS was used to analyze the quasi-static
problem. For cartilaginous tissues, porous elements with fluid pressure were used. The
20-node quadratic elements were used for the femoral cartilage, and the 8-node linear
elements were used for tibial cartilage and meniscus. The choice of using different
element types for the cartilages was a result of compromise between faster contact
convergence and better fluid pressure distribution. The 20-node elements provide better
numerical accuracy for the fluid pressure but significantly slow down the contact
convergence. We used the 20-node elements for the femoral cartilage, because that was
the focus for results. The bones were meshed with solid elements. The fluid pressure in
71

the bones was not considered, because it is less significant in load support as compared to
that in cartilaginous tissues due to a 3-order higher stiffness of the bones.
In order to understand the mechanics of the depth-wise progression of OA, the
normal and three degenerative case studies were implemented computationally. In Case
1, the perturbations were implemented only in the superficial zone. In Case 2, the
perturbations were implemented in superficial and middle zones, and in Case 3, the
perturbations were implemented in all three zones. As discussed earlier, local cartilage
degeneration was implemented within the high load-bearing region of the medial condyle
of the femoral cartilage (Fig. 4.2, bounded by the dash line). All other tissues were
assumed normal. These three cases simulated the onset of cartilage degeneration from the
superficial zone and progression to the deep zone.
The following perturbations were implemented for the degenerated cartilage: the
permeability was increased by 50%, the Young’s modulus of fibrillar matrix was
decreased by 70%, the Young’s modulus of nonfibrillar matrix was decreased by 65%,
and the orientation of fibers was not set in any particular direction. The material
properties of normal tissues are summarized in Table (4-1), which were mainly based on
previous fibril-reinforced modeling with tissue explants (Li et al., 2000, Li et al., 2009).
We assumed no changes in the thickness of the degenerated cartilage, because only early
degeneration was considered. Therefore, the same tissue geometry was used for the
normal and three case studies.
72

Table (4-1). Material properties for the normal tissues (Modulus: MPa; Permeability: 10−3mm4/Ns). The x is the primary fiber direction, i.e. the split-line direction for the superficial zone, the depth direction for the deep zone for articular cartilage, and the circumferential direction for the meniscus. The y and z are normal to the primary fiber direction. The properties are the same in the y and z directions.
Tissue
Fibrillar matrix, Eq (4-1) Nonfibrillar matrix
Permeability, Eq (4-2)
Ex Ey or Ez Em 𝜐𝜐Rm kx ky or kz
Femoral cartilage
Deep zone
3 + 1600𝜀𝜀𝑥𝑥 0.9 + 480𝜀𝜀𝑦𝑦/𝑧𝑧 0.80 0.36 1.0 0.5
Middle
zone
2 + 1000𝜀𝜀𝑥𝑥 2 + 1000𝜀𝜀𝑦𝑦/𝑧𝑧 0.60 0.30 3.0 1.0
Superficial zone
4 + 2200𝜀𝜀𝑥𝑥 1.2 + 660𝜀𝜀𝑦𝑦/𝑧𝑧 0.20 0.16 1.0 0.5
Tibial cartilage 2 + 1000𝜀𝜀𝑥𝑥 2 + 1000𝜀𝜀𝑦𝑦/𝑧𝑧 0.26 0.36 2.0 1.0
Menisci 28 5 0.50 0.36 2.0 1.0
Bones E = 5000 𝜐𝜐 = 0.30
4.4 Results
All results presented here are for the end of ramp compression prior to relaxation. The
fluid pressure in the femoral cartilage is shown in Fig. 4.2 for a superficial layer and Fig.
4.3 for a deep layer. In either layer, no significant alteration in the pressure was seen in
the lateral condyle (left in figure) when cartilage degeneration advanced in the medial
condyle from the superficial to middle and then deep zones (Normal → Case 1 → Case 2
→ Case 3). The pore pressure in the medial condyle was substantially reduced with the
73

progression of degeneration. This again was true for the fluid pressure in either
superficial or deep layer.
The depth variation of the fluid pressure in the degeneration site is shown in Figs.
4.4-4.6. The pressure decreased with the tissue depth in all cases. However, the pressure
gradient in the tissue thickness direction reduced progressively with cartilage
degeneration for a given knee compression, with larger reduction in the superficial zone
(Fig. 4.4). The depth variation was also site-specific; it can be more easily seen in the
high load-bearing region (Figs. 4.5 and 4.6).
74

Normal Case 1
Fluid Pressure (MPa)
Case 2 Case 3
Fig. 4.2. Fluid pressure (MPa) at the normalized depth of 1/16 (superficial layer) for the normal femoral cartilage and three cases of local cartilage degeneration. Case 1: degeneration in the superficial zone; Case 2: degeneration in both superficial and middle zones; and Case 3: degeneration in all three zones. The site of degeneration is indicated with the dash lines (inferior view of the right knee, i.e. the medial condyle on the right).
75

Normal Case 1
Fluid Pressure (MPa)
Case 2 Case 3
Fig. 4.3. Fluid pressure (MPa) at the normalized depth of 13/16 (deep layer) for the normal femoral cartilage and three cases of local cartilage degeneration as defined in Fig. 4.2.
76

Depth
Flui
d Pr
essu
re (M
Pa)
Fig. 4.4. Variation of fluid pressure along the depth of the femoral cartilage, shown for a location in the central contact region of the medial condyle where cartilage degeneration occurred. The depth was normalized by the tissue thickness (0 = articulating surface; 1 = cartilage-bone interface). The pressure was calculated at the centroid of each element.
77

Normal Case 1
Fluid Pressure (MPa)
Case 3 Case 2
Fig. 4.5. Fluid pressure (MPa) in a sagittal plane of the medial condyle (cut position shown in Fig. 4.2) for the normal femoral cartilage and three cases of local cartilage degeneration as defined in Fig. 4.2. The articulating surface is at bottom and the anterior side is on the right.
78

Normal Case 1
Fluid Pressure (MPa)
Case 3 Case 2
Fig. 4.6. Fluid pressure (MPa) in a coronal plane of the medial condyle (cut position shown in Fig. 4.3) for the normal femoral cartilage and three cases of local cartilage degeneration as defined in Fig. 4.2. The articulating surface is at bottom and the lateral side is on the left.
The distribution of normal strain along the tissue depth was also altered with
degeneration in the medial condyle (Fig. 4.7). This strain was associated with the lateral
expansion of the tissue when compressed in the thickness direction. The strain was
smaller in the superficial zone because more tangentially oriented fibers there restrained
the lateral expansion. However, the first principal strain was actually higher in the
superficial zone than in the middle and most deep zones due to high shear strains at the
surface (not shown). The first principal strain in the deepest layer was the largest in Case
79

3 (Fig. 4.8), mostly because of large shear strains at the cartilage-bone interface in Case 3
(the lateral strain shown in Fig. 4.7 was not the largest at the deepest layer).
Depth
Late
ral S
train
Fig. 4.7. Lateral strain along the depth of the femoral cartilage, shown for a location in the central contact region of the medial condyle where cartilage degeneration occurred. This normal strain was in the direction parallel to the articulating surface and perpendicular to the split-line. The depth was normalized by the tissue thickness (0 = articulating surface; 1 = cartilage-bone interface). The normal strain was calculated at the centroid of each element.
As compared to the normal case, the shear strains at the cartilage-bone interface
were reduced by cartilage degeneration in the superficial zone (Fig. 4.9, Case 1 vs
Normal), and further reduced when degeneration progressed into the middle zone (Fig.
4.9, Case 2 vs Case 1). However, the shear strains were eventually raised above normal
when cartilage degeneration progressed into the deep zone (Fig. 4.9, Case 3 vs Normal).
80

Note that these shear strains were associated with shear stresses τzx and τz y , which might
cause shear failure at the cartilage-bone interface (z is the tissue thickness direction).
Normal Case 1
Principal Strain
Case 2 Case 3
Fig. 4.8. First principal strain at the normalized depth of 15/16 (deep layer) for the normal femoral cartilage and three cases of local cartilage degeneration as defined in Fig. 4.2. This is an inferior view of the right knee, i.e. the medial condyle is on the right.
81

Strain 𝛾𝛾𝑧𝑧𝑥𝑥 Strain 𝛾𝛾𝑧𝑧𝑦𝑦
Normal
Case 1
Case 2
Case 3
Fig. 4.9. Shear strains at the normalized depth of 15/16 (deep layer) for the normal femoral cartilage and three cases of local cartilage degeneration as defined in Fig. 4.2. This is shown for part of the medial condyle. The local xy-plane is parallel to the cartilage-bone interface. The corresponding shear stresses for the strains are τzx and τzy , which are parallel to the interface.
4.5 Discussion
The fluid pressurization in all cartilaginous tissues was considered in the proposed model
of cartilage degeneration in the human knee with anatomically accurate geometry of the
82

joint. The zonal differences were considered in order to simulate the progression of
degeneration from the superficial to deep zones. Our hypothesis was positively tested: for
a given compression (displacement-control), the model predicted reduced fluid
pressurization (Figs. 4.2-4.6) although water content increased with cartilage
degeneration. The fluid pressure can support a large portion of the load applied to
cartilage (Ateshian and Hung, 2005), which is believed to be part of the mechanism to
reduce the joint friction (McCutchen, 1962), and thus to reduce the chances of OA
initiation from the tissue surface. Furthermore, the reduction in the fluid pressure
observed in the present study for the case of displacement-control indicated increased
joint friction and increased load support by the tissue matrix in the case of joint-force
control. Both may cause further progression of OA and deterioration of the tissue.
The onset of cartilage degeneration in an upper zone also resulted in reduced fluid
pressure in the lower zone, e.g. a degenerated superficial zone would reduce the fluid
pressure in both middle and deep zones (Fig. 4.4, Case 1). Since fluid pressurization
bears high loading for the tissue, this result agrees with the protective role of the surface
layer for the deep layer, as suggested by both experimental and computational studies
(Setton et al., 1993, Shirazi et al., 2008).
Furthermore, the fluid pressure reduced quickly when the degeneration started
from the superficial zone and progressed to the middle zone, then reduced at a lower rate
when the degeneration advanced to the deep zone (Fig. 4.4). This was most likely a
consequence of different fiber orientations in the three zones. In the superficial zone, the
fibers are oriented tangentially to resist lateral expansion under knee compression, and
83

thus great fluid pressure is produced. Some tangential fibers in the middle zone should
also contribute to increased fluid pressure. In the deep zone, however, the vertical fibers
are in compression, and thus do not significantly contribute to fluid pressurization.
Therefore, collagen degeneration in the deep zone would cause less fluid pressure change
in the tissue than degeneration in the superficial and middle zones.
The shear strains at the cartilage-bone interface were increased substantially with
cartilage degeneration to the deep zone (Fig. 4.9, Case 3 vs Normal). This was probably
because cartilage degeneration in the deep zone further increased the high gradient of the
material properties from deep cartilage to underlying bone. Great shear strains at the
cartilage-bone interface could cause microfractures, which eventually leads to OA (Radin
and Rose, 1986, Vener et al., 1992, Burr and Radin, 2003). The high gradients of material
properties are believed to increase the possibility of damage to the cartilage-bone
interface (Meachim and Bentley, 1978, Radin and Rose, 1986). Surprisingly, the shear
strains at the interface were reduced in Cases 1 and 2 prior to the progression of
degeneration into the deep zone (Fig. 4.9, Case 1 or 2 vs Normal). The reason was
probably due to the reduction of fluid pressure and its gradient in the tissue depth
direction while the material properties in the deep zone remained unchanged in Cases 1
and 2. Note that knee compression was given in the present study (displacement control).
The shear strains might not have been reduced in Cases 1 and 2, if the joint force had
been given (force-control).
Lower Young’s moduli and higher permeability were used in the present study to
simulate cartilage degeneration, in agreement with data from the literature (Armstrong
84

and Mow, 1982, Knecht et al., 2006). The compressive modulus of cartilage was reduced,
respectively, by 18% and 87.5%, and the water content was increased, respectively, by
79.9-81.6% and 84.1%, in moderate and advanced OA (Nieminen et al., 2004, Knecht et
al., 2006). According to another study, as a result of OA, the compressive and tensile
moduli of human articular cartilage were decreased by 55-68% and 72-83% respectively,
and the permeability was increased by 60-80% (Boschetti and Peretti, 2008). For the
human tibial cartilage, the compressive stiffness was decreased by 29% (Ding et al.,
1998); the compressive compliance was increased by 71% as a result of OA (Obeid et al.,
1994). Six months after anterior cruciate ligament transection, the compressive modulus
of canine cartilage was decreased by 25%, while the permeability was increased by ~48%
twelve weeks after the surgery (Setton et al., 1994, Setton et al., 1999). We have used
moderate values from these measurements.
Reduced surface fluid pressure with OA was also reported in the only similar
existing study (Mononen et al., 2012). It was found in that study that the stress
distribution through cartilage depth was also influenced by the orientation of superficial
fibers. The additional features of the present study included the fluid pressure in all
cartilaginous tissues and full consideration of the depth-dependent mechanical properties.
We further simulated the depth-wise cartilage degeneration from the superficial to deep
zones. As a consequence, the present results suggest that not only the degeneration in the
superficial layer reduced the fluid pressure in the deeper layers, which agrees with the
existing study (Mononen et al., 2012), but also that degeneration in the deeper layers
lowered the fluid pressure in the superficial layer.
85

A major limitation of the present study was due to the small knee compression
(100 µm) that was applied at a rather low rate (100 µm/s) in the computer simulation.
Our choice was a consequence of slow contact convergence and high demand in
computational time resulting from a high resolution of element mesh associated with the
zonal differences. Eight layers of elements were meshed in the tissue thickness direction
so there were 2, 4 and 2 layers of elements, respectively, for the superficial, middle and
deep zones. This mesh required several times more computational time, as compared to
the previous 4-layer mesh when the zonal differences were ignored (Gu and Li, 2011,
Kazemi et al., 2011). It took about a week to complete 1s simulation on a 4-CPU
workstation. In addition, we sometimes failed to obtain convergent results when larger or
faster compressions were applied. Further verifications are in progress. Because of the
small compression considered, one primary concern is whether the results were
compromised by the geometrical errors introduced during MRI segmentation and element
meshing, such as errors in surface curvature and tissue thickness. While such errors
indeed existed, they were probably at a lower level as compared to 100 µm. (The quality
of surface construction can be positively seen from the continuous variation in pore
pressure. The errors in geometry construction have been examined by independent
research groups, e.g. Li et al., 2001.) Other limitations included the omission of osmotic
pressure and the use of lab loading conditions.
The same compression was used in the present study, i.e. a displacement-control
was used for comparison. While the force-control loading protocol is often considered
more realistic, a knee joint with different stages of OA may not experience the same
86

force. As the OA develops, the patient tends to apply lower load on the diseased side
(Kaufman et al., 2001). On the other hand, it is more convenient and easier to interpret
the results when using a displacement-control in both computer simulations and lab tests.
Theoretically, the results from displacement control can be qualitatively interpreted to
that of force-control. Therefore, we chose the displacement control for simplicity.
The results presented here should be qualitatively correct, although the
magnitudes are not realistic because of the use of small and slow compression in the
present study. The alterations due to degeneration would be amplified in the case of a
physiologically realistic compression. This is because of the nonlinear and compression-
rate dependent load response of the joint. If a larger compression were applied, the fluid
pressure in the healthy cartilage would nonlinearly increase due to the normal collagen
network in the tissue, while the pressure in the degenerated cartilage would increase more
slowly due to a weak collagen network. For the same reason, if the same compression
were applied faster, the fluid pressure would increase faster in the healthy cartilage than
in the degenerated cartilage. In other words, the difference in the fluid pressurization in
the healthy and degenerated cartilages would be enlarged with the compression-
magnitude and compression-rate. This is understood from previous studies on cartilage
explants: both nonlinearity and strain-rate dependence of the load response of cartilage
are predominantly determined by the properties of collagen network (Li et al., 1999,
2003a, b).
The results of this investigation shed light on the effect of perturbation of material
properties and fibers orientation on knee joint mechanics, in the course of progression of
87

OA from cartilage surface to the cartilage-bone interface. Clinical studies suggest the
depth of cartilage defect as a parameter that characterizes OA severity (Brittberg and
Winalski, 2003). Computational modeling can be used to study the effect of this
parameter on the mechanics of knee joint. Furthermore, the role of defect depth in knee
joint mechanics can be better understood if computational models consider depth-
dependent properties embedded in an anatomical accurate geometry, as this study
showed. The findings of this study could be implemented in characterizing OA severity
based on the depth of cartilage injury. In fact, the development of OA is a multifactorial
phenomenon including alteration of tissue mechanical properties, perturbation of fiber
orientation, cartilage tissue loss, and the size and location of cartilage lesion (Brittberg
and Winalski, 2003, Guettler et al., 2004, Peña et al., 2007, Mononen et al., 2012). In this
study, the effect of the first two parameters was investigated, whereas the importance of
other factors will be investigated in future.
In summary, we have determined the alterations of fluid pressure and strains in
articular cartilage for the local tissue degeneration in the medial condyle of the femur.
These results may provide new information in understanding the progression of
osteoarthritis. As discussed earlier, cartilage degeneration resulted in reduced capability
of fluid pressurization and reduced pressure gradients in the tissue, which suggest
reduced lubrication in the joint and increased load support for the tissue matrix. Results
also suggest that once cartilage degeneration is initiated from the articulating surface, it
will eventually advance to the deep layer. This facilitation is achieved through the
reduction of fluid pressurization in all three zones with greater reduction in the superficial
88

zone, and damage to the depth-dependent structure of the tissue. In particular, cartilage
degeneration in the superficial zone may increase the possibility of damage to cartilage-
bone interface.
ACKNOWLEDGEMENTS
The present study was partially supported by the Natural Sciences and Engineering
Research Council of Canada, and the Canadian Institutes of Health Research.
CONFLICT OF INTEREST
The authors have no conflict of interest to disclose.
4.6 References
Andriacchi TP, Mündermann A, Smith RL, Alexander EJ, Dyrby CO, Koo S. A
framework for the in vivo pathomechanics of osteoarthritis at the knee. Ann Biomed Eng
2004;32:447-57.
Armstrong CG, Mow VC. Variations in the intrinsic mechanical properties of human
articular cartilage with age, degeneration, and water content. J Bone Joint Surg Am
1982;64:88-94.
Arokoski JP, Jurvelin JS, Väätäinen U, Helminen HJ. Normal and pathological
adaptations of articular cartilage to joint loading. Scand J Med Sci Sports 2000;10:186
98.
Ateshian GA, Hung CT. Patellofemoral joint biomechanics and tissue engineering. Clin
Orthop Relat Res 2005;81:81-90.
89

Bae WC, Payanal MM, Chen AC, Hsieh-Bonassera ND, Ballard BL, Lotz MK, Coutts
RD, Bugbee WD, Sah RL. Topographic Patterns of Cartilage Lesions in Knee
Osteoarthritis. Cartilage 2010;1:10-19.
Below S, Arnoczky SP, Dodds J, Kooima C, Walter N. The split-line pattern of the distal
femur: A consideration in the orientation of autologous cartilage grafts. Arthroscopy
2002;18:613-7.
Biswal S, Hastie T, Andriacchi TP, Bergman GA, Dillingham MF, Lang P. Risk factors
for progressive cartilage loss in the knee: a longitudinal magnetic resonance imaging
study in forty-three patients. Arthritis Rheum 2002;46:2884-92.
Boschetti F, Peretti GM. Tensile and compressive properties of healthy and osteoarthritic
human articular cartilage. Biorheology 2008;45:337-44.
Brittberg M, Winalski CS. Evaluation of cartilage injuries and repair. J Bone Joint Surg
Am 2003;85-A Suppl 2:58-69.
Brown TD , Shaw DT. In vitro contact stress distribution on the femoral condyles. J
Orthop Res 1984;2:190-9.
Burr DB, Radin EL. Microfractures and microcracks in subchondral bone: are they
relevant to osteoarthrosis? Rheum Dis Clin North Am 2003;29:675-85.
Carter DR, Beaupré GS, Wong M, Smith RL, Andriacchi TP, Schurman DJ. The
mechanobiology of articular cartilage development and degeneration. Clin Orthop Relat
Res 2004;427:S69-77.
90

Centers for Disease Control and Prevention. Prevalence of self-reported arthritis or
chronic joint symptoms among adults--United States, MMWR Morb Mortal Wkly Rep
2002;51:948-50.
Ding M, Dalstra M, Linde F, Hvid I. Changes in the stiffness of the human tibial
cartilage-bone complex in early-stage osteoarthrosis. Acta Orthop Scand 1998;69:358-62.
Federico S, Herzog W, and Wu JZ. Erratum: effect of fluid boundary conditions on joint
contact mechanics and applications to the modelling of osteoarthritic joints, J Biomech
Eng 2005;127: 208–209.
Federico S, La Rosa G, Herzog W, and Wu JZ. Effect of fluid boundary conditions on
joint contact mechanics and applications to the modelling of osteoarthritic joints, J
Biomech Eng 2004;126:220–225.
Felson DT, Zhang Y. An update on the epidemiology of knee and hip osteoarthritis with
a view to prevention. Arthritis Rheum 1998;41:1343-55.
Griffin TM, Guilak F. The role of mechanical loading in the onset and progression of
osteoarthritis. Exerc Sport Sci Rev 2005;33:195-200.
Gu KB, Li LP. A human knee joint model considering fluid pressure and fiber orientation
in cartilages and menisci. Med Eng Phys 2011;33:497-503.
Guettler JH, Demetropoulos CK, Yang KH, Jurist KA. Osteochondral defects in the
human knee: influence of defect size on cartilage rim stress and load redistribution to
surrounding cartilage. Am J Sports Med 2004;32:1451-8.
91

Guilak F, Mow VC. The mechanical environment of the chondrocyte: a biphasic finite
element model of cell-matrix interactions in articular cartilage. J Biomech 2000;33:1663
73.
Kaufman KR, Hughes C, Morrey BF, Morrey M, AN KN. Gait characteristics of patients
with knee osteoarthritis. J Biomech 2001;34:907-15.
Kazemi M, Li LP, Savard P, Buschmann MD. Creep behavior of the intact and
meniscectomy knee joints. J Mech Behav Biomed Mater 2011;4:1351-8.
Knecht S, Vanwanseele B, Stüssi E. A review on the mechanical quality of articular
cartilage - implications for the diagnosis of osteoarthritis. Clin Biomech (Bristol, Avon)
2006;21: 999-1012.
Korhonen RK, Laasanen MS, Töyräs J, Lappalainen R, Helminen HJ, Jurvelin JS. Fibril
reinforced poroelastic model predicts specifically mechanical behavior of normal,
proteoglycan depleted and collagen degraded articular cartilage. J Biomech
2003;36:1373-9.
Krishnan R, Park S, Eckstein F, Ateshian GA. Inhomogeneous cartilage properties
enhance superficial interstitial fluid support and frictional properties, but do not provide a
homogeneous state of stress. J Biomech Eng 2003;125:569-77.
Li LP, Buschmann MD, Shirazi-Adl A. A fibril reinforced nonhomogeneous poroelastic
model for articular cartilage: inhomogeneous response in unconfined compression. J
Biomech 2000;33:1533-1541.
Li LP, Buschmann MD, Shirazi-Adl A. Strain-rate dependent stiffness of articular
cartilage in unconfined compression. J Biomech Eng 2003;125,161-168.
92

Li LP, Buschmann MD and Shirazi-Adl A. Erratum: Strain-rate dependent stiffness of
articular cartilage in unconfined compression. J Biomech Eng 2003;125,566.
Li LP, Cheung JTM, Herzog W. Three-Dimensional Fibril-Reinforced Finite Element
Model of Articular Cartilage. Med Biol Eng Comput 2009;47:607-615.
Li G, Lopez O, Rubash H. Variability of a three-dimensional finite element model
constructed using magnetic resonance images of a knee for joint contact stress analysis. J
Biomech Eng 2001;123:341-346.
Li LP, Soulhat J, Buschmann MD, Shirazi-Adl A. Nonlinear analysis of cartilage in
unconfined ramp compression using a fibril reinforced poroelastic model. Clin Biomech
(Bristol, Avon) 1999;14:673-82.
Maffulli N, Binfield PM, King JB. Articular cartilage lesions in the symptomatic anterior
cruciate ligament-deficient knee. Arthroscopy 2003;19:685-90.
Manheimer E, Linde K, Lao L, Bouter LM, Berman BM. Meta-analysis: acupuncture for
osteoarthritis of the knee. Ann Intern Med 2007;146:868-77.
Mccutchen CW. The frictional properties of animal joints. Wear 1962;5:1-17.
Meachim G, Bentley G. Horizontal splitting in patellar articular cartilage. Arthritis
Rheum 1978;21:669-74.
Mononen ME, Mikkola MT, Julkunen P, Ojala R, Nieminen MT, Jurvelin JS, Korhonen
RK. Effect of superficial collagen patterns and fibrillation of femoral articular cartilage
on knee joint mechanics-a 3D finite element analysis. J Biomech 2012;45:579-87.
93

Nieminen HJ, Saarakkala S, Laasanen MS, Hirvonen J, Jurvelin JS, Töyräs J. Ultrasound
attenuation in normal and spontaneously degenerated articular cartilage. Ultrasound Med
Biol 2004;30:493-500.
Obeid EM, Adams MA, Newman JH. Mechanical properties of articular cartilage in
knees with unicompartmental osteoarthritis. J Bone Joint Surg Br 1994;76:315-9.
Oliveria SA, Felson DT, Reed JI, Cirillo PA, Walker AM. Incidence of symptomatic
hand, hip, and knee osteoarthritis among patients in a health maintenance organization.
Arthritis Rheum 1995;38:1134-41.
Peat G, Mccarney R, Croft P. Knee pain and osteoarthritis in older adults: a review of
community burden and current use of primary health care. Ann Rheum Dis 2001;60:91-7.
Peña E, Calvo B, Martínez MA, Doblaré M. Effect of the size and location of
osteochondral defects in degenerative arthritis. A finite element simulation. Comput Biol
Med 2007;37:376-87.
Radin EL, Rose RM. Role of subchondral bone in the initiation and progression of
cartilage damage. Clin Orthop Relat Res 1986;213:34-40.
Saarakkala S, Julkunen P, Kiviranta P, Mäkitalo J, Jurvelin JS, Korhonen RK. Depth-
wise progression of osteoarthritis in human articular cartilage: investigation of
composition, structure and biomechanics. Osteoarthritis Cartilage 2010;18:73-81.
Seedholm BB, Takeda T, Tsubuku M, Wright V. Mechanical factors and patellofemoral
osteoarthrosis. Ann Rheum Dis 1979;38:307-16.
94

Setton LA, Elliott DM, Mow VC. Altered mechanics of cartilage with osteoarthritis:
human osteoarthritis and an experimental model of joint degeneration. Osteoarthritis
Cartilage 1999;7:2-14.
Setton LA, Mow VC, Müller FJ, Pita JC, Howell DS. Mechanical properties of canine
articular cartilage are significantly altered following transection of the anterior cruciate
ligament. J Orthop Res 1994;12:451-63.
Setton LA, Zhu W, Mow VC. The biphasic poroviscoelastic behavior of articular
cartilage: role of the surface zone in governing the compressive behavior. J Biomech
1993;26:581-92.
Shirazi R, Shirazi-Adl A. Computational biomechanics of articular cartilage of human
knee joint: effect of osteochondral defects. J Biomech 2009;42:2458-65.
Shirazi R, Shirazi-Adl A, Hurtig M. Role of cartilage collagen fibrils networks in knee
joint biomechanics under compression. J Biomech 2008;41:3340-8.
Strobel MJ, Weiler A, Schulz MS, Russe K, Eichhorn HJ. Arthroscopic evaluation of
articular cartilage lesions in posterior-cruciate-ligament-deficient knees. Arthroscopy
2003;19:262-8.
Tandogan RN, Taşer O, Kayaalp A, Taşkiran E, Pinar H, Alparslan B, Alturfan A.
Analysis of meniscal and chondral lesions accompanying anterior cruciate ligament tears:
relationship with age, time from injury, and level of sport. Knee Surg Sports Traumatol
Arthrosc 2004;12:262-70.
95

Temple MM, Bae WC, Chen MQ, Lotz M, Amiel D, Coutts RD, Sah RL. Age- and site-
associated biomechanical weakening of human articular cartilage of the femoral condyle.
Osteoarthritis Cartilage 2007;15:1042-52.
Vener MJ, Thompson RC, Lewis JL, Oegema TR. Subchondral damage after acute
transarticular loading: an in vitro model of joint injury. J Orthop Res 1992;10:759-65.
Wilson W, Van Burken C, Van Donkelaar C, BUMA P, Van Rietbergen B, Huiskes R.
Causes of mechanically induced collagen damage in articular cartilage. J Orthop Res
2006;24:220-8.
Wong M, Carter DR. Articular cartilage functional histomorphology and
mechanobiology: a research perspective. Bone 2003;33:1-13.
Wu JZ, Herzog W, Epstein M. Joint contact mechanics in the early stages of
osteoarthritis. Med Eng Phys 2000;22:1-12.
96

Chapter Five: Load Bearing Characteristics of the Knee Joint Deteriorates with the Defect Depth of Articular Cartilage
5.1 Abstract
Osteoarthritis is associated with alterations in cartilage mechanical properties and tissue
loss. The focal cartilage defect is a typical type of tissue loss. The present study
investigated the altered mechanics of human knee joint due to focal defects. The focus
was on the fluid pressurization and its load support in cartilage. Ten normal and defect
cases were analyzed using an anatomically accurate finite element model of the knee.
Fluid pressurization, anisotropic fibril-reinforcement, and depth-dependent mechanical
properties were modeled for articular cartilages and menisci. The focal defects were
considered in both condyles within high load-bearing regions. Both displacement and
force controls were simulated. A reduced load bearing capacity was seen in the vicinity
of the defect region, which was similar to the case of cartilage degeneration investigated
previously. A deeper defect caused more fluid pressure reduction in the surrounding
region. However, a partial defect did not necessarily cause a fluid pressure reduction in
the remaining underlying cartilage: the fluid pressure could increase in some scenarios,
which was different from the case of cartilage degeneration. Cartilage defects also
increased the shear strain at the cartilage-bone interface, which was more significant with
a full-thickness defect. The remaining defect tissue could still support substantial loading,
when it was in contact with the mating surface. The consequence of cartilage defect also
depended on the defect sites. Finally, the creep response could be interpreted from the
97

relaxation response with knowledge of the nonlinear and strain-rate dependent behavior
of articular cartilage.
KEYWORDS: Articular cartilage mechanics; Cartilage focal defect; Finite element
analysis; Fluid pressure; Knee joint mechanics
5.2 Introduction
Osteoarthritis (OA) is a leading cause of disability among the elderly, and it has been
reported as the most prevalent joint disease in the USA (Peat et al., 2001, Manheimer et
al., 2007). One scenario of OA is to start from the surface of articular cartilage, and attack
deeper layer until reach the bone (Andriacchi et al., 2004, Saarakkala et al., 2010). Once
deep layers of cartilage are destroyed, bone is exposed to the joint contact. The knee joint
has the highest prevalence of OA (Oliveria et al., 1995, Felson and Zhang, 1998,
Manheimer et al., 2007). The prevalence and cost of knee OA was high in the past and is
expected to remain high in at least the next two decades (Lethbridge-Cejku et al., 2004,
Manheimer et al., 2007). The development of OA is not yet fully understood. The
interplay between cartilage structure and mechanical loading, however, is believed to be a
pathway in the OA development.
Perturbation of the composition and structure of cartilage may be a necessary step
to initiate OA (McDevitt and Muir, 1976, Stockwell et al., 1983, Guilak et al., 1994).
Cartilage is mainly composed of a solid matrix and a fluid (Mow and Ratcliffe, 1997).
The solid matrix is composed of collagen fibers and nonfibrillar proteoglycan matrix that
98

mostly support the tensile and compressive loading, respectively. Cartilage is often
divided into three zones: superficial, middle, and deep zones (Mow et al., 1980, Mow and
Ratcliffe, 1997). Fibers are mostly parallel to the surface in the superficial zone,
randomly-oriented in the middle zone, and perpendicular to the cartilage-bone interface
in the deep zone.
Fluid pressurization plays an essential role in the mechanics of a joint, lubricating
the joint and preventing the matrix of cartilage from excessive loading (McCutchen,
1962, Walker et al., 1968, Ateshian and Hung, 2005). Fluid pressurization contributes to
load support of the joint at different scales during different loading phases (Mow et al.,
1984, Herberhold et al., 1999, Li et al., 2002). For example, load is applied on the knee
joint in a fraction of a second during gait which is associated with high fluid
pressurization, whereas standing for a long time might be associated with a lower fluid
pressure in the knee. Moreover, the alteration in fluid pressurization is one of the
symptoms in the early OA (Maroudas, 1976, Maroudas and Venn, 1977, Venn and
Maroudas, 1977, Maroudas et al., 1985). Recently, we demonstrated a weaker fluid
pressurization in a degenerated knee, using an anatomically accurate model of the knee
joint (Dabiri and Li, 2013).
Several parameters may play roles in the interplay between defect progression and
mechanical loading including defect depth, size, location, and properties of cartilage
associated with the defect (Seedholm et al., 1979, Noyes and Stabler, 1989, Brittberg and
Winalski, 2003). Experimental studies encounter difficulties when investigating the effect
of each of these parameters. The consequence of each parameter is difficult to
99

differentiate as they often evolve simultaneously. Numerical simulation can be recruited
to study the development of OA and the role of each parameter in the progression of OA,
as has been reported in the literature (Haut Donahue et al., 2003, Ramaniraka et al., 2005,
Peña et al., 2007). In a recent study, the contact mechanics of the knee joint was
investigated in the presence of cartilage degeneration with alterations in mechanical
properties including fiber orientation (Mononen et al., 2012). The study, however, did not
consider the fluid pressure in menisci and full depth-dependent properties of cartilages,
and only considered the short-term behavior of the knee joint. The significance of defect
size in the mechanics of the knee joint was reported using an elastic model (Peña et al.,
2007). The mechanics of cartilage defect has also been investigated with two-dimensional
explant geometries (Duda et al., 2005).
The defect depth is a criterion to categorize the severity of a cartilage defect
(Noyes and Stabler, 1989, Brittberg and Winalski, 2003). For example, the International
Cartilage Repair Society (ICRS) has a classification system for cartilage defect which is
based on the progression of defect from cartilage surface to cartilage-bone interface
(Brittberg and Winalski, 2003). Therefore, the objective of the present study was to
determine the alteration in fluid pressurization in the human knee joint in different stages
of defect progression from cartilage surface to cartilage-bone interface.
5.3 Methods
The geometry of the knee model was reconstructed from the MRI images of the right leg
of a male subject who was 27 years old with no leg injury (Gu and Li, 2011, Kazemi et
100

al., 2011, Kazemi et al., 2012). The model was composed of femur, femoral cartilage,
menisci, tibial cartilage, and tibia. The commercial finite element package ABAQUS
6.10 (Simulia, Providence, USA) was used for the finite element analysis with custom
defined material model. The femur and tibia were modeled as linearly elastic. Articular
cartilages and menisci were considered fluid-saturated materials reinforced by a nonlinear
fiber network, using a previously developed fibril-reinforced model of cartilage (Li et al.,
2002). The depth-varying tissue properties of the femoral cartilage were also incorporated
as per a recent study (Dabiri and Li, 2013)
The surface-to-surface contact modeling in ABAQUS was considered between
femoral cartilage and tibial cartilage, femoral cartilage and menisci, and tibial cartilage
and menisci. Using the TIE option in ABAQUS, the femoral cartilage was fixed to the
femur, and the tibial cartilage was fixed to the tibia. The horns of menisci were also tied
to the tibia.
Two loading conditions were considered: (1) Ramp compression of 500 µm
applied in 5s followed by relaxation up to 1000s; and (2) Ramp compressive force of
387.76 N applied in 5s followed by creep. This force was taken to be the same as
obtained at 500 µm compression. In either case, the compressive displacement or force
was applied on the top of femur with fixed bottom of tibia.
Cartilage defects can be developed in different sites (Seedholm et al., 1979, Bae et
al., 2010). We focused on the depth-wise advancement of defect in the medial femoral
cartilage as this region is more vulnerable to the development of lesions (Biswal et al.,
2002, Maffulli et al., 2003, Strobel et al., 2003, Tandogan et al., 2004, Temple et al.,
101

2007). Three types of cartilage defect were considered: (1) Superficial defect refers to the
defect in the superficial zone only (tissue loss in the zone); (2) Middle defect refers to the
defect in the superficial and middle zones; and (3) Deep defect refers to the defect in all
three zones (full-thickness loss). A superficial defect in the lateral femoral cartilage was
also examined for comparison.
In addition to the loading conditions, site and depth of defect, another factor
considered was the contact condition of the defect cartilage to its mating surface. Both
scenarios were implemented in the modeling: defect contact or no defect contact. Both
scenarios are possible, because patients tend to adjust their gait when OA develops
(Kaufman et al., 2001). Considering the combinations of all these factors, 10 cases were
investigated in this study (Table 5-1).
102

Table (5-1). Ten cases investigated in the present study. Three cartilage conditions were considered: normal cartilage, defects in the medial and lateral condyles, respectively; three defect depths were also assumed for the medial condyle defect: the defect in the superficial zone only, the defect up to the middle zone and the defect up to the deep zone. Both force and displacement controls (creep and relaxation) were simulated. In cases 6 and 7, no contact was assumed between the defected cartilage and its mating surface.
Loading & Normal Medial condyle defect Lateral condyle defect
contact cartilage
conditions Superficial Middle Deep Superficial
Displacement Case 1 Defect Case 2 Case 3 Case 4 Case 5
control contact
No Case 6 Case 7
defect
contact
Force control Case 8 Defect Case 9 Case 10
contact
5.4 Results
For the same knee compression, the short-term surface fluid pressure in the medial
condyle decreased with the defect depth (Fig. 5.1). The long-term fluid pressure
experienced less alteration with the defect, with some alteration in the pressure
distribution, surprisingly a little more significant with the middle defect (Fig. 5.2).
Furthermore, the fluid pressure in the lateral condyle was merely affected by the defect in
the medial condyle. A redistribution of the fluid pressure was more obvious when the
103

defect was progressed to full-thickness (Fig. 5.1). Note only the fluid pressures in the
unaffected cartilage are shown in Figs. 5.1 and 5.2.
(a) Case 1 (b) Case 2
Fluid Pressure (MPa)
(d) Case 4 (c) Case 3
Fig. 5.1. Surface fluid pressure in the femoral cartilage at 500µm compression prior to relaxation. (a) Normal model (Case 1), (b) Superficial defect model (Case 2), (c) Middle defect model (Case 3), and (d) Full-thickness defect model (Case 4). Defect contact was assumed in the three defect models (Cases 2-4). The medial condyle is on the right. This is an inferior view of the right knee.
104

(a) Case 1 (b) Case 2
Fluid Pressure (MPa)
(d) Case 4 (c) Case 3
Fig. 5.2. Surface fluid pressure in the femoral cartilage during late relaxation of 500µm compression (at 1000s). These are the same cases as shown in Fig. 5.1.
105

When the defect cartilage was in contact with its mating surface (Cases 2-4), a
decreased fluid pressure in the defect region was observed in the case of the superficial
defect as compared to the normal case (Fig. 5.3a vs 5.3b). However, a drastically raised
pressure in the defect region was seen in the case of middle defect (Fig. 5.3). On the other
hand, if the defect cartilage was not in contact with its mating surface (Cases 6 and 7), the
fluid pressure in the vicinity of defect decreased with defect depth (Fig. 5.4). The depth
variation of the pressure was also altered with the defect depth (Fig. 5.4)
106

(a) Case 1 (b) Case 2
(c) Case 3 (d) Case 4
Fluid Pressure (MPa)
Fig. 5.3. Fluid pressure in the layer of normalized depth of 1/16 at 500µm compression prior to relaxation. For the partial-thickness defect models, the fluid pressure in the defect region is shown for the new surface layer, i.e. at the depth of 5/16 (Case 2) and 13/16 (Case 3) respectively. Defect contact was assumed in the three defect models (Cases 2-4). The medial condyle is on the right.
107

Fluid Pressure (MPa)
(a) Case 1
(b) Case 6
(c) Case 7
Fig. 5.4. Fluid pressure in a sagittal plane of the femoral cartilage at 500µm compression prior to relaxation, shown for the high load bearing region of the medial condyle. (a) Normal model (Case 1), (b) Superficial defect model (Case 6), and (c) Middle defect model (Case 7). No defect contact was assumed in the defect models (Cases 6-7). The anterior side is on the left.
The reaction force of the defect joint could increase to above or decrease to below
the normal value depending on the contact condition at the defect region and the loading
phase (Fig. 5.5, displacement control). When the defect contact was considered (Cases 2
4), the short-term reaction force was the highest in the case of middle defect, but the
long-term reaction force reduced with the defect depth (Fig. 5.5a). When the defect
108

contact was not considered (Cases 6-7), the reaction force was virtually the same for the
two defect cases, which was also close to the one for Case 4 (Fig. 5.5b).
The effect of a lateral defect on fluid pressure contours was more noticeable as
compared to a medial defect (Fig. 5.6). Specifically, two high-fluid pressure regions were
observed in the lateral defect while there was only one high-fluid pressure region in the
normal model.
The shear strain component in the cartilage-bone interface was altered by the
defect depth (Fig. 5.7). The superficial defect did not cause noticeable change in the shear
strain. However, the middle and deep defects produced obvious changes in the shear
strain. The location of peak shear strain moved toward defect rim as the defect advanced
to the deeper layer, and also the distribution of shear strain was altered.
For the cases of force control (Cases 8-10), the increase in the fluid pressure in the
defect region was more obvious than for the displacement control, especially for the
defect in the lateral condyle (Fig. 5.8).
109

(a)
(b) Fig. 5.5. Reaction force in the knee as a function of time for the ramp compression of 500µm followed by relaxation. (a) Defect contact was assumed in the defect models (Peak forces: Case 1: 387.764; Case 2: 363.614; Case 3: 396.252; Case 4: 288.13N); and (b) No defect contact was assumed in Cases 6 and 7 (Peak forces: Case 6: 309.457; Case 7: 293.578N).
110

Fluid Pressure (MPa)
(a) Case 1
(b) Case 2
(c) Case 5 Fig. 5.6. Surface fluid pressure in the femoral cartilage at 500µm compression prior to relaxation. (a) Normal model (Case 1), (b) Superficial defect in the medial condyle (Case 2), and (c) Superficial defect in the lateral condyle (Case 5). Defect contact was assumed in the defect models.
111

(a) Case 1 (b) Case 2
Shear strain
(c) Case 3 (d) Case 4
Fig. 5.7. Shear strain in the deepest cartilage layer during late relaxation of 500µm compression (at 1000s). (a) Normal model (Case 1), (b) Superficial defect model (Case 2), (c) Middle defect model (Case 3), and (d) Deep defect model (Case 4). Defect contact was assumed in the defect models (Cases 2-4). The medial condyle is on the right.
112

Fluid Pressure (MPa)
(a) Case 8
(b) Case 9
(c) Case 10
Fig. 5.8. Surface fluid pressure in the femoral cartilage at 387.76N compressive force prior to creep in the layer of normalized depth of 1/16. (a) Normal model (Case 8), (b) Superficial defect in the medial condyle (Case 9), and (c) Superficial defect in the lateral condyle (Case 10). For the defect models, the fluid pressure in the defect region is shown for the new surface layer, i.e. at the depth of 5/16. Defect contact was assumed in the two defect models (Cases 9-10). The medial condyle is on the right.
113

Forc
e (N
) 400
300 Loading Phase for creep (constant loading rate)
200
100 Loading Phase for relaxation (loading rate increases with time)
0 0 1 2 3 4 5
Time (s)
Fig. 5.9. Reaction force in the knee as a function of time during the loading phase for the cases of creep and stress relaxation. In the case of relaxation, the knee joint experienced a loading rate that started at a small value then increased with time, while in the case of creep, the loading rate was constant. The curve for the case of relaxation was taken from Fig. 5.5 for the normal joint.
5.5 Discussion
Generally speaking, the load bearing capacity associated with fluid pressurization was
weakened in the vicinity of the defect region (Figs. 5.1 and 5.2), but the remaining defect
cartilage may be more pressurized on the spot (Fig. 5.3c), if it was in contact with its
mating surface. In the case of displacement control, it meant lowered fluid pressure in the
vicinity of the defect region, which further decreased with the defect depth (Fig. 5.1). In
114

the case of force control, a weakened load bearing from fluid pressurization in the
vicinity of the defect meant increased fluid pressure in the remaining defect cartilage
(Fig. 5.8), in order to maintain the load support in the joint. In any case, a redistribution
of the fluid pressure has been observed in the defect region and its vicinity (Figs. 5.1-5.4,
5.6 and 5.8), as a result of load reallocation in the joint.
The reduced load bearing capability from fluid pressurization was not obviously
seen in the case of creep (Fig. 5.8), because the same force was maintained in the normal
and defect joints, as mentioned above. In other words, larger compressive displacement
or faster compression must be produced in the defect joint in order to produce the same
reaction force as that for the normal joint. In fact, a higher peak fluid pressure was seen in
creep than in relaxation for the normal joint (Fig. 5.8a vs 5.1a), although the same force
was applied in 5s in both creep and relaxation (Fig. 5.9). This phenomenon can be
explained by the nonlinear response of the knee (Li and Gu, 2011) and strain-rate
dependent response of articular cartilage (Li and Herzog, 2004). For the case of
relaxation, the compression rate (displacement/time) was constant, corresponding to a
lower loading rate (force/time) at the beginning and a higher loading rate at the end of the
loading phase (Fig. 5.9). For the case of creep, however, the loading rate was constant
during the loading phase, resulting in a higher compression rate at the beginning (but a
lower compression rate at the end) of the loading phase as compared to the case of
relaxation. The faster early compression in turn produced a higher fluid pressure during
early compression due to the strain-rate dependence of cartilage (Li and Herzog, 2004).
This higher fluid pressure did not have sufficient time to dissipate although the
115

compression was slowed down in the late loading phase. Therefore, we see a higher peak
fluid pressure in creep than in relaxation even the reaction forces were identical at the end
of the loading phase.
As indicated above, the creep behavior can be somehow understood from the
relaxation behavior, although they might look differently. On the other hand, modeling
stress relaxation is computationally less expensive than modeling creep, because a faster
increasing fluid pressure in creep results in a slower numerical convergence and also
because creep takes much longer time to complete (Li et al., 2008). Therefore, the present
study was focused on the stress relaxation (displacement-controlled) behavior of the knee
joint while creep response (force-controlled) was also modeled.
The contact condition at the defect region played a significant role in the load
support of the joint although the defect size was small (Figs. 5.4 and 5.5). The remaining
defect cartilage still supported substantial loading when it was in contact with its mating
surface (Fig. 5.5a, Cases 2 and 3 compared to Case 1). The reaction force in the knee was
significantly lower, if the remaining defect cartilage lost contact with its mating surface,
even the rest normal surfaces remained in contact (Fig. 5.5, Cases 6 and 7 vs Cases 2 and
3). This result indicated significant load changes in the defect joint from a slight gait
adjustment by a patient, as people often do when they suffer from OA (Kaufman et al.,
2001).
The effect of cartilage defect on the fluid pressurization was also dependent on
the defect site (Figs. 5.6 and 5.8). More results for the defect in the medial condyle are
presented in this paper, because this region is considered more vulnerable to the
116

development of lesions (Biswal et al., 2002, Maffulli et al., 2003, Strobel et al., 2003,
Tandogan et al., 2004, Temple et al., 2007).
The effect of cartilage defect on the fluid pressurization diminished with
relaxation and creep time (Figs. 5.1 vs 5.2), which was expected as fluid pressurization in
the tissue decays with stress relaxation and creep. However, one would still expect the
negative impact of the defect on the long-term stresses and strains of the tissue matrix, as
we see the shear strains in the region increased with the defect depth (Fig. 5.7). This
escalated shear strain may increase the chances of OA following microfracture at the
cartilage-bone interface (Radin and Rose, 1986, Vener et al., 1992, Burr and Radin,
2003). These results agree with previous studies on the importance of the tissue integrity
(Setton et al., 1993, Shirazi et al., 2008).
The effects of focal cartilage defect and degeneration on fluid pressurization were
similar in some ways and different in other ways. Both caused the reduced capacity of
fluid pressurization in the vicinity of the defect or degeneration; the reductions were
positively correlated to the depth of degeneration or defect (the effect of cartilage
degeneration was reported in Dabiri and Li, 2013). However, partial cartilage defects did
not necessarily cause fluid pressure reduction in the remaining underlying layers (Figs.
5.3 and 5.8) as it occurred in cartilage degeneration (Dabiri and Li, 2013). A defect
advanced to the middle zone resulted in a substantially higher fluid pressure in the deep
zone (Fig. 5.3c), but a degeneration advanced to the same zone caused lower fluid
pressure in the deep zone (Dabiri and Li, 2013), as compared to the normal case.
117

The major limitation of the present study was the use of non-physiological
loadings, which were relatively small (< 400 N) and slowly applied to the joint (5 s).
These loading protocols were used to avoid slow numerical convergence. While the fluid
pressures obtained were still low (0-4 MPa), they were close to measured contact
pressures in the knee joints. Therefore, the results presented here are still practically
interesting. Furthermore, the qualitative results would remain the same, if larger and
faster loadings were used.
In summary, focal cartilage defects substantially compromise the capability of the
fluid pressurization in articular cartilage and the load-bearing in the joint. Furthermore,
load bearing characteristics of the knee joint deteriorates with the defect depth of articular
cartilage. The altered mechanics of the knee are also influenced by the sites of defects
and the contact conditions in the defect regions.
Acknowledgments
Funding: the Natural Sciences and Engineering Research Council of Canada.
Conflict of Interests: the authors have no conflict of interest to declare.
Ethical approval: E-22593, University of Calgary, for the use of MRI of human subjects.
5.6 References
Andriacchi TP, Mündermann A, Smith RL, Alexander EJ, Dyrby CO, Koo S. A
framework for the in vivo pathomechanics of osteoarthritis at the knee. Ann Biomed Eng
2004;32:447-57.
118

Ateshian GA, Hung CT. Patellofemoral joint biomechanics and tissue engineering. Clin
Orthop Relat Res 2005;436:81-90.
Bae WC, Payanal MM, Chen AC, Hsieh-Bonassera ND, Ballard BL, Lotz MK, Coutts
RD, Bugbee WD, Sah RL. Topographic Patterns of Cartilage Lesions in Knee
Osteoarthritis. Cartilage 2010;1:10-19.
Biswal S, Hastie T, Andriacchi TP, Bergman GA, Dillingham MF, Lang P. Risk factors
for progressive cartilage loss in the knee: a longitudinal magnetic resonance imaging
study in forty-three patients. Arthritis Rheum 2002;46:2884-92.
Brittberg M, Winalski CS. Evaluation of cartilage injuries and repair. J Bone Joint Surg
Am 2003;85-A Suppl 2:58-69.
Burr DB, Radin EL. Microfractures and microcracks in subchondral bone: are they
relevant to osteoarthrosis? Rheum Dis Clin North Am 2003;29:675-85.
Dabiri Y, Li LP. Altered knee joint mechanics in simple compression associated with
early cartilage degeneration. Comput Math Methods Med 2013;2013:1-11,
http://dx.doi.org/10.1155/2013/862903.
Duda GN, Maldonado ZM, Klein P, Heller MO, Burns J, Bail H. On the influence of
mechanical conditions in osteochondral defect healing. J Biomech 2005;38:843-51.
Felson DT, Zhang Y. An update on the epidemiology of knee and hip osteoarthritis with
a view to prevention. Arthritis Rheum 1998;41:1343-55.
Gu KB, Li LP. A human knee joint model considering fluid pressure and fiber orientation
in cartilages and menisci. Med Eng Phys 2011;33:497-503.
119
Guilak F, Ratcliffe A, Lane N, Rosenwasser MP, Mow VC. Mechanical and biochemical
changes in the superficial zone of articular cartilage in canine experimental osteoarthritis.
J Orthop Res 1994;12:474-84.
Haut Donahue TL, Hull ML, Rashid MM, Jacobs CR. How the stiffness of meniscal
attachments and meniscal material properties affect tibio-femoral contact pressure
computed using a validated finite element model of the human knee joint. J Biomech
2003;36:19-34.
Herberhold C, Faber S, Stammberger T, Steinlechner M, Putz R, Englmeier KH, Reiser
M, Eckstein F. In situ measurement of articular cartilage deformation in intact
femoropatellar joints under static loading. J Biomech 1999;32:1287-95.
Kaufman KR, Hughes C, Morrey BF, Morrey M, An KN. Gait characteristics of patients
with knee osteoarthritis. J Biomech 2001;34:907-15.
Kazemi M, Li LP, Buschmann MD, Savard P. Partial meniscectomy changes fluid
pressurization in articular cartilage in human knees. J Biomech Eng 2012;134:021001.
Kazemi M, Li LP, Savard P, Buschmann MD. Creep behavior of the intact and
meniscectomy knee joints. J Mech Behav Biomed Mater 2011;4:1351-58.
Korhonen RK, Laasanen MS, Töyräs J, Lappalainen R, Helminen HJ, Jurvelin JS. Fibril
reinforced poroelastic model predicts specifically mechanical behavior of normal,
proteoglycan depleted and collagen degraded articular cartilage. J Biomech
2003;36:1373-79.
Lethbridge-Cejku M, Schiller JS, Bernadel L. Summary health statistics for U.S. adults:
National Health Interview Survey, 2002. Vital Health Stat 2004;10:1-151.
120

Li LP, Buschmann MD, Shirazi-Adl A. The role of fibril reinforcement in the mechanical
behavior of cartilage. Biorheology 2002;39:89-96.
Li LP, Gu KB. Reconsideration on the use of elastic models to predict the instantaneous
load response of the knee joint. Proc Inst Mech Eng H 2011;225:888-96.
Li LP, Herzog W. Strain-rate dependence of cartilage stiffness in unconfined
compression: the role of fibril reinforcement versus tissue volume change in fluid
pressurization. J Biomech 2004;37:375-82.
Li LP, Korhonen RK, Iivarinen J, Jurvelin JS, Herzog W. Fluid pressure driven fibril
reinforcement in creep and relaxation tests of articular cartilage. Med Eng Phys
2008;30:182-89.
Maffulli N, Binfield PM, King JB. Articular cartilage lesions in the symptomatic anterior
cruciate ligament-deficient knee. Arthroscopy 2003;19:685-90.
Manheimer E, Linde K, Lao L, Bouter LM, Berman BM. Meta-analysis: acupuncture for
osteoarthritis of the knee. Ann Intern Med 2007;146:868-77.
Maroudas AI. Balance between swelling pressure and collagen tension in normal and
degenerate cartilage. Nature 1976;260:808-09.
Maroudas A, Venn M. Chemical composition and swelling of normal and osteoarthrotic
femoral head cartilage. II. Swelling. Ann Rheum Dis 1977;36:399-406.
Maroudas A, Ziv I, Weisman N, Venn M. Studies of hydration and swelling pressure in
normal and osteoarthritic cartilage. Biorheology 1985;22:159-69.
Mccutchen CW. The frictional properties of animal joints. Wear 1962;5:1-17.
121

Mcdevitt CA, Muir H. Biochemical changes in the cartilage of the knee in experimental
and natural osteoarthritis in the dog. J Bone Joint Surg Br 1976;58:94-101.
Mononen ME, Mikkola MT, Julkunen P, Ojala R, Nieminen MT, Jurvelin JS, Korhonen
RK. Effect of superficial collagen patterns and fibrillation of femoral articular cartilage
on knee joint mechanics-a 3D finite element analysis. J Biomech 2012;45:579-87.
Mow V, Ratcliffe A. Structure and function of articular cartilage and meniscus. In: Mow
V, Hayes W, editors. Basic orthopaedic biomechanics. second ed. Philadelphia:
Lippincott-Raven; 1997. p. 113-77.
Mow VC, Holmes MH, Lai WM. Fluid transport and mechanical properties of articular
cartilage: a review. J Biomech 1984;17:377-94.
Mow VC, Kuei SC, Lai WM, Armstrong CG. Biphasic creep and stress relaxation of
articular cartilage in compression: Theory and experiments. J Biomech Eng 1980;102:73
84.
Noyes FR, Stabler CL. A system for grading articular cartilage lesions at arthroscopy.
Am J Sports Med 1989;17:505-13.
Oliveria SA, Felson DT, Reed JI, Cirillo PA, Walker AM. Incidence of symptomatic
hand, hip, and knee osteoarthritis among patients in a health maintenance organization.
Arthritis Rheum 1995;38:1134-41.
Peat G, Mccarney R, Croft P. Knee pain and osteoarthritis in older adults: a review of
community burden and current use of primary health care. Ann Rheum Dis 2001;60:91-7.
122

Peña E, Calvo B, Martínez MA, Doblaré M. Effect of the size and location of
osteochondral defects in degenerative arthritis. A finite element simulation. Comput Biol
Med 2007;37:376-87.
Radin EL, Rose RM. Role of subchondral bone in the initiation and progression of
cartilage damage. Clin Orthop Relat Res 1986;213:34-40.
Ramaniraka NA, Terrier A, Theumann N, Siegrist O. Effects of the posterior cruciate
ligament reconstruction on the biomechanics of the knee joint: a finite element analysis,
Clin Biomech (Bristol, Avon) 2005;20:434-42.
Saarakkala S, Julkunen P, Kiviranta P, Mäkitalo J, Jurvelin JS, Korhonen RK. Depth-
wise progression of osteoarthritis in human articular cartilage: investigation of
composition, structure and biomechanics. Osteoarthritis Cartilage 2010;18:73-81.
Seedholm BB, Takeda T, Tsubuku M, Wright V. Mechanical factors and patellofemoral
osteoarthrosis. Ann Rheum Dis 1979;38:307-16.
Setton LA, Zhu W, Mow VC. The biphasic poroviscoelastic behavior of articular
cartilage: role of the surface zone in governing the compressive behavior. J Biomech
1993;26:581-92.
Shirazi R, Shirazi-Adl A, Hurtig M. Role of cartilage collagen fibrils networks in knee
joint biomechanics under compression. J Biomech 2008;41:3340-48.
Stockwell RA, Billingham ME, Muir H. Ultrastructural changes in articular cartilage
after experimental section of the anterior cruciate ligament of the dog knee. J Anat
1983;136:425-39.
123

Strobel MJ, Weiler A, Schulz MS, Russe K, Eichhorn HJ. Arthroscopic evaluation of
articular cartilage lesions in posterior-cruciate-ligament-deficient knees. Arthroscopy
2003;19:262-8.
Tandogan RN, Taşer O, Kayaalp A, Taşkiran E, Pinar H, Alparslan B, Alturfan A.
Analysis of meniscal and chondral lesions accompanying anterior cruciate ligament tears:
relationship with age, time from injury, and level of sport. Knee Surg Sports Traumatol
Arthrosc 2004;12:262-70.
Temple MM, Bae WC, Chen MQ, Lotz M, Amiel D, Coutts RD, Sah RL. Age- and site-
associated biomechanical weakening of human articular cartilage of the femoral condyle.
Osteoarthritis Cartilage 2007;15:1042-52.
Vener MJ, Thompson RC, Lewis JL, Oegema TR. Subchondral damage after acute
transarticular loading: an in vitro model of joint injury. J Orthop Res 1992;10:759-65.
Venn M, Maroudas A. Chemical composition and swelling of normal and osteoarthrotic
femoral head cartilage. I. Chemical composition. Ann Rheum Dis 1977;36:121-9.
Walker PS, Dowson D, Longfield MD, Wright V. "Boosted lubrication" in synovial
joints by fluid entrapment and enrichment. Ann Rheum Dis 1968;27:512-20.
124

Chapter Six: A Protocol to Include Individual Muscle Forces in an Anatomically Accurate Model of the Human Knee Joint
As an active joint, the mechanical performance of the knee joint is determined by the
contact forces, inertia forces, and muscle and other soft tissue forces. Individual muscles
stabilize the knee joint for each activity by appropriate sequence of individual activations.
From a mechanical engineering perspective, the presence of individual muscles (and not
an integrated muscle force) has another effect on the stability of the knee joint: the knee
joint is statically over-constrained. In other words, the number of muscles required to
accomplish a task are more than those required to make the joint statically determined.
The higher the number of muscles considered in a model is, the more complex the
mathematical modeling will be. Major muscles are normally included in a
musculoskeletal model of a joint. For example, Piazz and Delp considered 12 muscles for
a musculoskeletal model of the lower extremity (Piazza and Delp, 1996). Various
muscles get activated in different stages of a gait cycle (Perry, 1992), and a complete
simulation of an activity such as gait should include all major muscles. The long-term
goal of this research is to model the behavior of the knee joint during different activities.
For that purpose, the geometry of the model should be reoriented for different motions
including gait phases. When the gait cycle is simulated, the contacting components will
be different at each phase. The boundary and load conditions will be different as well. An
example of altering loading and boundary condition is that the body weight will not be
present during the swing phase of gait in contrast to the stance phase. A protocol should
125

be planned to decide how to include individual muscle forces before the entire gait cycle
is simulated. The purpose of this section is to develop that protocol.
6.1 The Coordinates of Origin and Insertion Points of Muscles
The major muscles were considered when the origin and insertion points of different
muscles were calculated, to provide a framework for future work. The muscles were: 1
rectus femoris (RF), 2- semimembranosus (SEMIMEM), 3- semitendinosus (SEMITEN),
4- long head of biceps femoris (BIFEMLH), 5- short head of biceps femoris (BIFEMSH),
6- vastus medialis (VASMED), 7- vastus intermedius (VASINT), 8- vastus lateralis
(VASLAT), 9- medial head of gastrocnemius, 10- lateral head of gastrocnemius. Delp
has reported the origin and insertion points of major muscles of the lower extremity
(Delp, 1990a). Seven coordinate systems were located at pelvis, femur, tibia, patella,
talus, calcaneus, and toe as shown in Fig. 6.1.
126

Fig. 6.1. Seven coordinate systems are shown in this figure. The origin and insertion
X Y
Z Pelvis
Femur
Patella
Tibia
Talus Toes
Calcanus
coordinates are calculated in these frames.
127

The origin and insertion point of each muscle is known at a coordinate system.
The coordinate data were transferred to pelvis coordinate system for all muscles. Then,
the coordinate data of the origin and insertion points of each muscle were converted to
the ABAQUS assembly coordinate system (Tables 6-1, 6-2). The line of action of each
muscle was calculated. To include the muscles in the three-dimensional knee model, a
plate was artificially created at the top femur. The intersect point of the plate and each
muscle line of action was calculated in the ABAQUS assembly coordinate system.
Finally, the coordinates of intersect point were transferred to the plate local coordinate
system. The direction of each muscle force was parallel to a unit vector calculated using
the origin and insertion point data of each muscle (Table 6-3). Section 6-4 explains the
calculation of each muscle force location with more details.
128
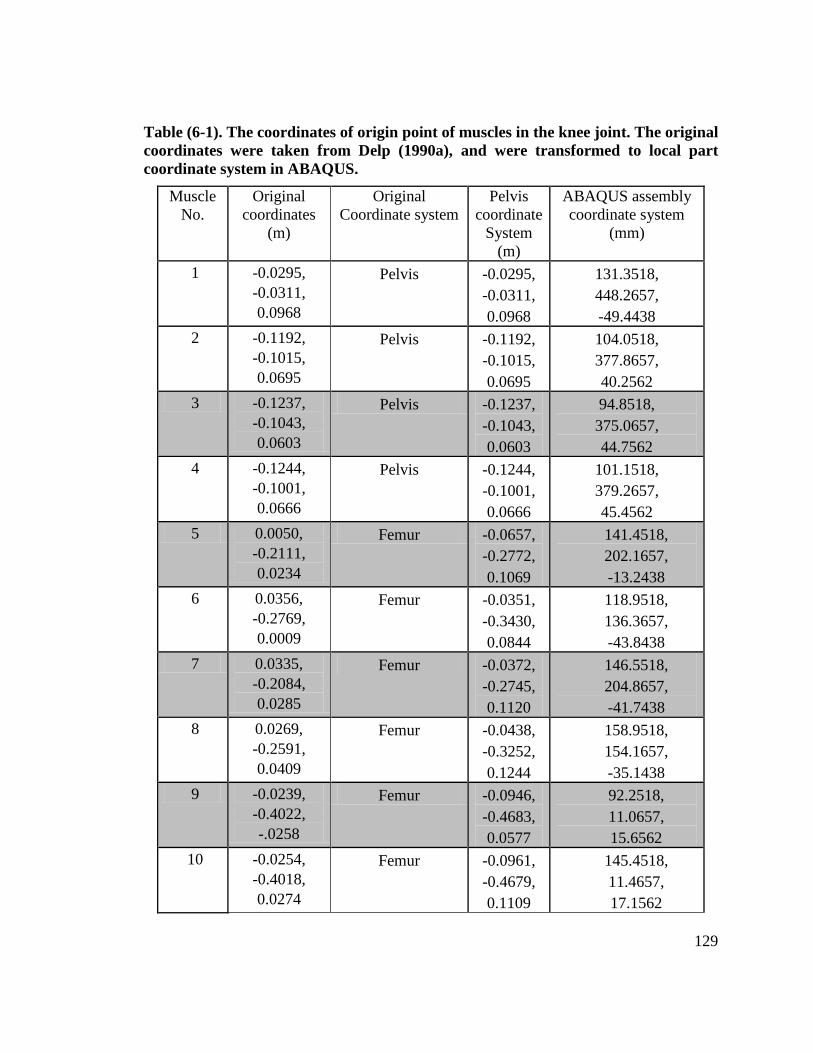
Table (6-1). The coordinates of origin point of muscles in the knee joint. The original coordinates were taken from Delp (1990a), and were transformed to local part coordinate system in ABAQUS.
Muscle No.
Original coordinates
(m)
Original Coordinate system
Pelvis coordinate
System (m)
ABAQUS assembly coordinate system
(mm)
1 -0.0295, -0.0311, 0.0968
Pelvis -0.0295, -0.0311, 0.0968
131.3518, 448.2657, -49.4438
2 -0.1192, -0.1015, 0.0695
Pelvis -0.1192, -0.1015, 0.0695
104.0518, 377.8657, 40.2562
3 -0.1237, -0.1043, 0.0603
Pelvis -0.1237, -0.1043, 0.0603
94.8518, 375.0657, 44.7562
4 -0.1244, -0.1001, 0.0666
Pelvis -0.1244, -0.1001, 0.0666
101.1518, 379.2657, 45.4562
5 0.0050, -0.2111, 0.0234
Femur -0.0657, -0.2772, 0.1069
141.4518, 202.1657, -13.2438
6 0.0356, -0.2769, 0.0009
Femur -0.0351, -0.3430, 0.0844
118.9518, 136.3657, -43.8438
7 0.0335, -0.2084, 0.0285
Femur -0.0372, -0.2745, 0.1120
146.5518, 204.8657, -41.7438
8 0.0269, -0.2591, 0.0409
Femur -0.0438, -0.3252, 0.1244
158.9518, 154.1657, -35.1438
9 -0.0239, -0.4022, -.0258
Femur -0.0946, -0.4683, 0.0577
92.2518, 11.0657, 15.6562
10 -0.0254, -0.4018, 0.0274
Femur -0.0961, -0.4679, 0.1109
145.4518, 11.4657, 17.1562
129

Table (6-2). The coordinates of insertion point of muscles in the knee joint. The original coordinates were taken from Delp (1990a), and were transformed to local part coordinate system in ABAQUS.
Muscle No.
Original coordinates
(m)
Original coordinate
system
Pelvis coordinate System
(m)
ABAQUS assembly
coordinate system (mm)
1 0.0121, 0.0437, -0.0010
Patella -0.0142, -0.4411, 0.0849
119.4518, 38.2657, -64.7438
2 -0.0243, -0.0536, -0.0194
Tibia -0.1003, -0.5157, 0.0641
98.6518, -36.3343, 21.3562
3 -0.0314, -0.0545, -0.0146
Tibia -0.1074, -0.5166, 0.0689
103.4518, -37.2343, 28.4562
4 -0.0081, -0.0729, 0.0423
Tibia -0.0841, -0.5350, 0.1258
160.3518, -55.6343,
5.1562 5 -0.0101,
-0.0725, 0.0406
Tibia -0.0861, -0.5346, 0.1241
158.6518, -55.2343,
7.1562 6 0.0063,
0.0445, -0.0170
Patella -0.0200, -0.4403, 0.0689
103.4518, 39.0657, -58.9438
7 0.0058, 0.0480, -0.0006
Patella -0.0205, -0.4368, 0.0853
119.8518, 42.5657, -58.4438
8 0.0103, 0.0423, 0.0141
Patella -0.0161, -0.4425, 0.1000
134.5518, 36.8657, -62.8438
9 0.0044, 0.0310, -0.0053
Calcanus -0.1203, -0.9031, 0.0861
120.6518, -423.7343,
41.3562 10 0.0044,
0.0310, -0.0053
Calcanus -0.1203, -0.9031, 0.0861
120.6518, -423.7343,
41.3562
130

Table (6-3). The coordinates of the intersection point of muscles line of action and the plate (second and third columns). Data were transferred from assembly coordinate system to plate (local part) coordinate system using MATLAB. The last column contains coordinates of unit vectors to which muscle forces were parallel.
Muscle No. Assembly coordinate system (mm)
Plate coordinate system (mm)
Unit vector
1 120.2306, 65.1000, -63.7424
-11.6324, -5.0000, 44.6141
-0.0290, -0.9989, -0.0373
2 99.9742, 65.1000, 25.9847
78.0947, -5.0000, 64.8705
-0.0130, -0.9989, -0.0456
3 101.3172, 84.6119, 0.0208, 65.1000, -5.0000, -0.9990, 32.5019 63.5275 -0.0395
4 143.9171, 65.1000, 16.3440
68.4540, -5.0000, 20.9276
0.1343, -0.9867, -0.0914
5 150.6108, 49.7292, 0.0665, 65.1000, -5.0000, -0.9947, -2.3808 14.2339 0.0788
6 107.5991, 65.1000, -54.9035
-2.7935, -5.0000, 57.2456
-0.1555, -0.9762, -0.1515
7 123.5589, -4.0151, -0.1615, 65.1000, -5.0000, -0.9817, -56.1251 41.2858 -0.1010
8 140.4249, 65.1000, -56.1764
-4.0664, -5.0000, 24.4198
-0.1984, -0.9539, -0.2253
9 99.1680, -16.8623, -0.0651, -94.8200, 5.0000, 0.9961, 21.9149 13.5885 -0.0589
10 139.3951, -94.8200, 23.0664
-18.0138, 5.0000, 53.8156
0.0568, 0.9968, -0.0554
131

6.2 The Forces of Muscles
The muscle forces create an over-constrained system for the knee joint. An optimization
method is used along with momentum equations to calculate muscle forces (Anderson
and Pandy, 2001). Two optimization methods can be implemented: dynamic optimization
and static optimization. In the first method a forward dynamic approach is used to
determine muscle forces, whereas in the second method an inverse method is used. These
methods give similar results when simulating the gait cycle (Anderson and Pandy, 2001).
In this project the second method was implemented as it is computationally more
efficient (Anderson and Pandy, 2001).
Two sets of equations will be used to determine muscle forces. The first equation
is an optimization criterion which minimizes a function of muscle activations. The
second equation enforces either the simulated angle or the momentum at the knee joint to
be close to the experimentally measured angle or momentum at this joint, as is explained
in the following sections.
6.2.1 Enforcing Angles
The muscle forces are determined so that the calculated angles at the joints are close to
experimentally determined angles within a tolerance. The lower extremity is considered
as a linkage with the hip, the knee and the ankle rotations as its degrees of freedom.
Using the Lagrange method, and considering the motions in the sagittal plane, the
equations of motion for the system are (Piazza and Delp, 1996):
132

2��𝜃 𝐻𝐻 ⎡��𝜃 𝐻𝐻⎤ −��𝜃 𝐻𝐻��𝜃 𝐾𝐾 𝑀𝑀𝐻𝐻⎢ 2 ⎥𝑀𝑀 −��𝜃 𝐾𝐾 = 𝐶𝐶 ⎢��𝜃 𝐾𝐾⎥ + 𝑉𝑉 ��𝜃 𝐻𝐻��𝜃 𝐴𝐴 + 𝐺𝐺 + −𝑀𝑀𝐾𝐾 (6-1) ⎢ ⎥ 𝑀𝑀𝐴𝐴𝜃𝜃𝐴𝐴 ⎣��𝜃 𝐴𝐴
2 ⎦ −𝜃𝜃𝐾𝐾𝜃𝜃𝐴𝐴
In this equation 𝜃𝜃𝐾𝐾 , 𝜃𝜃𝐻𝐻 and 𝜃𝜃𝐴𝐴 are the knee, the hip and the ankle angles, respectively.
Dots are used to refer to time derivatives. One dot represents angular velocity, and two
dots represents angular acceleration. 𝑀𝑀𝐻𝐻, 𝑀𝑀𝐾𝐾 and 𝑀𝑀𝐴𝐴 are the moments produced by
muscles, and matrices 𝑀𝑀, 𝐶𝐶, 𝑉𝑉, and 𝐺𝐺 are related to effects such as inertial and gravity
forces (Piazza and Delp, 1996). The moments at the knee is produced by muscles and
other soft tissues. We assume that the moments caused by other soft tissues is negligible
compared to the moments produced by muscles. This equation can be written in the
following form:
2��𝜃 𝐻𝐻 ⎡𝜃𝜃𝐻𝐻⎤ −��𝜃 𝐻𝐻��𝜃 𝐾𝐾 𝑀𝑀𝐻𝐻⎢ 2 ⎥−��𝜃 𝐾𝐾 = 𝑀𝑀−1𝐶𝐶 ⎢��𝜃 𝐾𝐾⎥ + 𝑀𝑀−1𝑉𝑉 ��𝜃 𝐻𝐻��𝜃 𝐴𝐴 + 𝑀𝑀−1𝐺𝐺 + 𝑀𝑀−1 −𝑀𝑀𝐾𝐾 (6-2) ��𝜃 𝐴𝐴
⎢⎣��𝜃 2 ⎥⎦ −��𝜃 𝐾𝐾��𝜃 𝐴𝐴
𝑀𝑀𝐴𝐴𝐴𝐴
The nonlinear terms in the right-hand side are calculated based on the data from a
previous time step. After this equation is solved, the angular velocity at the knee joint can
be determined once the initial angular velocity is known at this joint, as follows:
𝜏𝜏 𝜏𝜏−∆𝑡𝑡 (6-3)��𝜃 𝐾𝐾 = ∆𝑡𝑡 × ��𝜃 𝐾𝐾 + ��𝜃 𝐾𝐾
And then the angle can be found:
𝜏𝜏 𝜏𝜏−∆𝑡𝑡 (6-4)𝜃𝜃𝐾𝐾 = ∆𝑡𝑡 × ��𝜃 𝐾𝐾 + 𝜃𝜃𝐾𝐾
The knee angle can be calculated for all time steps in a similar manner.
133

On the other hand, the experimentally determined values can be obtained from gait
analysis experiments, as reported in the literature (for example, Perry, 1992, Allard et al.,
1997).
The muscle forces are determined so that:
𝑆𝑆𝑆𝑆𝑚𝑚𝑆𝑆𝑓𝑓𝑎𝑎𝑡𝑡𝑒𝑒𝑆𝑆 − 𝜃𝜃𝐾𝐾 (6-5)𝐸𝐸𝐸𝐸𝑝𝑝𝑒𝑒𝐸𝐸𝑆𝑆𝑚𝑚𝑒𝑒𝐸𝐸𝑡𝑡𝑎𝑎𝑓𝑓 < 𝑇𝑇𝑇𝑇𝑓𝑓𝑒𝑒𝐸𝐸𝑎𝑎𝐸𝐸𝑐𝑐𝑒𝑒 𝜃𝜃𝐾𝐾
6.2.2 Enforcing Moments
In this method, moments resultant from calculated muscle forces are enforced to be close
to experimentally determined joint moments (for example, Perry, 1992, Allard et al.,
1997). Similar to the previous section, we assume the moment at the knee joint is
produced mainly by muscles. In other words, moments produced by other soft tissues is
negligible compared to the moment caused by muscles. The equation used in this section
can be written in the following form:
𝐸𝐸𝐸𝐸𝑝𝑝𝑒𝑒𝐸𝐸𝑆𝑆𝑚𝑚𝑒𝑒𝐸𝐸𝑡𝑡𝑎𝑎𝑓𝑓 < 𝑇𝑇𝑇𝑇𝑓𝑓𝑒𝑒𝐸𝐸𝑎𝑎𝐸𝐸𝑐𝑐𝑒𝑒 𝑆𝑆𝑆𝑆𝑚𝑚𝑆𝑆𝑓𝑓𝑎𝑎𝑡𝑡𝑒𝑒𝑆𝑆 − 𝑀𝑀𝐾𝐾 (6-6)𝑀𝑀𝐾𝐾
𝑆𝑆𝑆𝑆𝑚𝑚𝑆𝑆𝑓𝑓𝑆𝑆𝑆𝑆𝑒𝑒𝑆𝑆 Where 𝑀𝑀𝐾𝐾 , the simulated moment at the knee joint, becomes close to
𝑀𝑀𝐾𝐾𝐸𝐸𝑥𝑥𝐸𝐸𝑒𝑒𝐸𝐸𝑆𝑆𝑚𝑚𝑒𝑒𝐸𝐸𝑆𝑆𝑆𝑆𝑓𝑓 within 𝑇𝑇𝑇𝑇𝑓𝑓𝑒𝑒𝐸𝐸𝑎𝑎𝐸𝐸𝑐𝑐𝑒𝑒. This approach is adopted in this project, and it will be
explained in the next section with more details.
6.3 The Optimization Process
As mentioned earlier, two sets of equations are simultaneously included in the
optimization process. The first equation is the performance criterion as follows:
134

𝐸𝐸
𝐽𝐽 = 𝑎𝑎𝑚𝑚2 (6-7) 𝑚𝑚=1
Where 𝐸𝐸 is the number of muscles, and 𝑎𝑎𝑚𝑚 is the activation of muscle number 𝑚𝑚. From a
physiological point of view function 𝐽𝐽 is related to musculoskeletal endurance.
Musculoskeletal endurance is maximized when 𝐽𝐽 is minimized (Crowninshield and Brand,
1981). The activation of each muscle is bounded to be equal or between 0 and 1:
0 ≤ 𝑎𝑎𝑚𝑚 ≤ 1 (6-8)
The other equation (Eq. 6-6) enforces the calculated moment at the joint be close to the
experimentally measured moment within a tolerance:
𝑆𝑆𝑆𝑆𝑚𝑚𝑆𝑆𝑓𝑓𝑎𝑎𝑡𝑡𝑒𝑒𝑆𝑆 − 𝑀𝑀𝐾𝐾 (6-6)𝐸𝐸𝐸𝐸𝑝𝑝𝑒𝑒𝐸𝐸𝑆𝑆𝑚𝑚𝑒𝑒𝐸𝐸𝑡𝑡𝑎𝑎𝑓𝑓 < 𝑇𝑇𝑇𝑇𝑓𝑓𝑒𝑒𝐸𝐸𝑎𝑎𝐸𝐸𝑐𝑐𝑒𝑒 𝑀𝑀𝐾𝐾
The simulated moment is calculated as follows:
𝐸𝐸 (6-9)𝑆𝑆𝑆𝑆𝑚𝑚𝑆𝑆𝑓𝑓𝑎𝑎𝑡𝑡𝑒𝑒𝑆𝑆 𝑀𝑀𝐾𝐾 = 𝐹𝐹𝑚𝑚 × 𝐸𝐸𝑚𝑚
𝑚𝑚=1
Where 𝐹𝐹𝑚𝑚 and 𝐸𝐸𝑚𝑚 are the force and moment arm for muscle number 𝑚𝑚 about the knee
joint. The moment arms can be calculated from the kinematic data of the knee joint when
the gait cycle is simulated (Delp, 1990b). The formulation to include individual muscle
forces presented in this chapter is general, and it can be used for a gait cycle. However, as
it will explained in the next paragraph, we used 40% gait cycle as an example.
Consequently, in this project, the moment arm data from the literature was used as the
angle of the knee joint was constant. 𝐹𝐹𝑚𝑚 is calculated from muscle activations as follows: 135

0 (6-10)𝐹𝐹𝑚𝑚 = 𝑎𝑎𝑚𝑚 × 𝐹𝐹𝑚𝑚
where 𝐹𝐹𝑚𝑚0 is the maximum isometric force of the muscle number 𝑚𝑚.
The knee joint angle of the current model reconstructed from MRI is almost zero.
On the other hand, the knee joint angle at almost 40% of the gait cycle is zero (Sup et al.,
2008 adopted from Perry, 1992). Consequently, for the analysis of the anatomically
accurate model, only rectus femoris, medial head of gastrocnemius and lateral head of
gastrocnemius were considered. These muscles were included because the forces of
other muscles were almost zero at 40% of the gait cycle (Besier et al., 2009). The
moment arms and maximum isometric forces of these muscles are summarized in Table
(6-4). It should be emphasized that the method to include individual muscle forces
discussed in this chapter can be used for a whole gait cycle, and data for 40% was used as
an example to explain how the method works. The knee moment at 40% gait cycle was
approximated as 20N.m (Sup et al., 2008 adopted from Winter, 1991).
Table (6-4). The moment arm and maximum isometric force of three muscles used in this project (O’Connor 1993, Kellis and Baltzopoulos 1999, Yang et al., 2010).
Muscle Moment arm (m) Maximum isometric force (N)
Rectus femoris 0.0369 854.09 Medial head of gastrocnemius 0.025 1112.2 Lateral head of gastrocnemius 0.025 487.86
6.4 Inclusion of Muscle Forces in the ABAQUS Model
As shown in Fig. 6-2, the anatomically accurate model included distal femur, proximal
tibia and fibula, femoral and tibial cartilages, menisci, and ligaments. This model and the 136

constitutive material behavior of its components were developed by a researcher in our
group (Kazemi, 2013). A plate was created above the femur for the purpose of applying
muscle forces in the model. The Young's modulus of the plate was much higher than
cartilages and menisci (almost rigid). The intersect point of each muscle action line and
the bottom face of the plane was calculated. Three points of the bottom surface of the
plate were obtained in ABAQUS. Assume these points are 𝑎𝑎1, 𝑎𝑎2, 𝑎𝑎3. The origin and
insertion point of each muscle was also calculated in ABAQUS assembly coordinate
system (Tables 6-1 and 6-2). Assume the coordinates of these points for a muscle are
𝑏𝑏1and 𝑏𝑏2. Then the intersect point of the line passing through 𝑏𝑏1and 𝑏𝑏2 and the plate will
be:
−1𝑡𝑡1 𝐸𝐸𝑏𝑏1 − 𝐸𝐸𝑏𝑏2 𝐸𝐸𝑎𝑎2 − 𝐸𝐸𝑎𝑎1 𝐸𝐸𝑎𝑎3 − 𝐸𝐸𝑎𝑎1 𝐸𝐸𝑏𝑏1 − 𝐸𝐸𝑎𝑎1
𝑡𝑡2 = 𝑦𝑦𝑏𝑏1 − 𝑦𝑦𝑏𝑏2
𝑦𝑦𝑎𝑎2 − 𝑦𝑦𝑎𝑎1
𝑦𝑦𝑎𝑎3 − 𝑦𝑦𝑎𝑎1 𝑦𝑦𝑏𝑏1
− 𝑦𝑦𝑎𝑎1 (6-11) 𝑡𝑡3 𝑧𝑧𝑏𝑏1 − 𝑧𝑧𝑏𝑏2 𝑧𝑧𝑎𝑎2 − 𝑧𝑧𝑎𝑎1 𝑧𝑧𝑎𝑎3 − 𝑧𝑧𝑎𝑎1 𝑧𝑧𝑏𝑏1 − 𝑧𝑧𝑎𝑎1
The intersect location of the flowing muscle forces were determined: rectus
femoris, vastus lateralis, vastus medialis, vastus intermedius, short head of biceps
femoris, long head of biceps femoris, semitendinosus, and semimembranosus. Medial
gastrocnemius and lateral gastrocnemius forces were applied at the posterior side of
medial and lateral condyles. The location of the intersecting point of a muscle line and
the plate was calculated in the plate coordinate system after it was found in assembly
coordinate system (Table 6-3). The coordinates of the intersecting point were used to
define a node where the muscle force was applied. The force was applied in the direction
of a unit vector whose components were calculated based on the insertion and origin
point of each muscle (Table 6-3). As it was explained in section 6.3, three muscles rectus
137

femoris, medial head of gastrocnemius and lateral head of gastrocnemius were considered
for the finite element analysis.
1 2 3 4
7 8 5 6
Fig. 6.2: Inclusion of individual muscle forces in an anatomically accurate three-dimensional knee model. The numbers correspond to muscles as follows: 1- vastus lateralis, 2- vastus intermedius, 3-rectus femoris, 4- vastus medialis, 5semitendinosus, 6- semimembranosus, 7- long head of biceps femoris, 8- short head of biceps femoris. Medial and lateral heads of gastrocnemius forces are applied on the posterior side of femoral condyles. Table (6-3) contains the intersection point coordinates in ABAQUS.
6.5 MATLAB M-files
MATLAB (Mathworks, Natick, Massachusett, USA) programming language was used in
this part of the project. MATLAB codes were used to transfer coordinates between
138

different coordinate systems and also for optimization. These MATLAB files had the
following roles:
- calculations of the components of a unit vector in the direction of each muscle force.
These data were used when a concentrated force was defined for a muscle force in
ABAQUS.
- calculation of the coordinates of the intersection point between a muscle force line of
action and the bottom face of the plate. This location was used to define the location
where the muscle force was applied.
- the transfer of the coordinates of muscle insertion and origin points between different
coordinate systems.
- enforcing the simulated knee moment to be close to the experimental moment (Eq. 6-6).
- calculation of the optimization function (Eq. 6-7).
- optimization of the performance function.
6.6 Results
The model under a 150N compressive load without muscle forces was analyzed. As it
was discussed in section 6.3, the geometry of our model approximately corresponds to
40% of gait cycles. At 40% of the gait cycle, muscles other than rectus femoris, lateral
gastrocnemius, and medial gastrocnemius are almost inactive (Besier et al., 2009).The
muscle forces including rectus femoris, lateral gastrocnemius, and medial gastrocnemius
were then included along with the vertical force to examine the effect of muscle forces on
139

the contact mechanics of the knee joint. Contact pressure at the femoral cartilage is
shown for both cases in Fig. 6.3.
The pattern of contact pressure is the same; however, the contact pressures are
significantly higher when muscle forces are included. The contours would also be
different if the whole gait cycle was considered as the orientation of bones and muscle
forces are considerably altered during different phases of gait. The noticeable effect of
muscle forces on the contact pressure is in line with previous studies that reported the
knee joint is under a much higher burden when muscles are activated (Kuster et al.,
1997).
140

(a)
(b) Fig. 6.3: Contact pressure in the femoral cartilage with (a) and without (b) muscles for approximately 40% of the gait cycle.
141

Chapter Seven: Free-Surface Fluid Pressure
The contact surfaces change as a result of deflections. It is important to adjust the fluid
pressure boundary conditions due to these changes in contact surfaces. As mentioned
earlier, contact surfaces are the interfaces between the femoral cartilage, menisci, and
tibial cartilages. The contact area of each component varies when applied load increases
from zero to a given value.
The models, described so far, assumed no fluid pressure boundary changes during
the solution. The free surfaces were approximated at the beginning of an analysis, and a
node set included in those surfaces was defined. The pore pressure at those nodes was
enforced to be zero during the analysis, as boundary conditions. This method could be
suitable for small knee compressions, but for large knee compressions some of the nodes
which were not in contact initially could become in contact after further deformation.
In this chapter, based on a previous study (Pawaskar et al., 2010), an algorithm is
developed to adjust the free-surface pore pressure as a solution variable. As it will be
explained in the next sections, the pore pressure boundary condition was defined to be
dependent upon contact status, and based on the contact status a seepage coefficient was
used to update the pore pressure at each surface integration point.
142

7.1 Subroutines
To implement the zero fluid pressure condition at the surface two subroutines were used:
FLOW and URDBFIL. The former implements the fluid velocity or fluid pressure
condition at a surface. The latter provides the contact condition of the surface.
7.1.1 FLOW Subroutine
This subroutine uses a seepage coefficient 𝑘𝑘0 and a constant 𝑆𝑆0 (which can be zero) to
enforce the fluid flow condition at a surface. The relation among fluid flow, seepage
coefficient and a reference fluid pressure is:
𝑓𝑓 = 𝑘𝑘0(𝑆𝑆 − 𝑆𝑆0) (7-1)
Where 𝑓𝑓 is fluid velocity in the direction of outward normal to the surface, 𝑘𝑘0 is seepage
coefficient, 𝑆𝑆 is fluid pressure and 𝑆𝑆0 is a reference fluid pressure. If the surface is in
contact with another surface (e.g. two cartilage layers are in contact), and the pore
pressure is equal on both sides of the contact surface, letting k0 be zero will satisfy the
zero velocity condition at the interface. On the other hand, if the surface is free, the fluid
pressure condition should be 𝑆𝑆 = 𝑆𝑆0. This condition will be approximately enforced, if
𝑘𝑘𝑘𝑘0 ≫
𝛾𝛾𝑤𝑤𝑐𝑐 (7-2)
Where 𝑘𝑘 is the permeability of the underlying material, 𝛾𝛾𝑤𝑤 is the specific weight, and 𝑐𝑐 is
the characteristic length of the underlying elements (ABAQUS manual). For standard
geometries (disks and spheres) by two previous studies, 𝑘𝑘0 = 1 𝑚𝑚𝑚𝑚3
was chosen 𝑁𝑁𝑁𝑁
(Pawaskar et al., 2010, Federico et al., 2004, 2005), but our model was not convergent
when that value was used (the base units used are N for force, mm for length and s for
143

time). This could be due to the complexity of the geometry in our model compared to
those studies as well as different element lengths used in our model. When 𝑘𝑘0 =
0.001 𝑚𝑚𝑚𝑚3
was chosen for our model, reasonable results were obtained. According to the 𝑁𝑁𝑁𝑁
ABAQUS manual values of 𝑘𝑘0 set too high might cause “poor conditioning of the
model”, which explains why 𝑘𝑘0 = 1 𝑚𝑚𝑚𝑚3
was not appropriate for our model. In other 𝑁𝑁𝑁𝑁
words, the characteristic seepage coefficient 𝛾𝛾𝑤𝑤
𝑘𝑘
𝑐𝑐 in our model is lower than those in
aforementioned previous models (Pawaskar et al., 2010, Federico et al., 2004, 2005).
The sign of 𝑓𝑓 is another feature that affects the convergence of our model when adjusting
the surface fluid pressure by the method described in this section. When an element is not
in contact, the normal velocity can be outward or inward in respect to the surface. If the
velocity direction is inward, the model will not converge if equation (7-1) is used.
Therefore, the velocity is forced to be zero in that case. In other words, the drainage only
flow is implemented, which corresponds to the non-cyclic loading used in our
simulations.
The FLOW subroutine is activated with 2 command lines in the ABAQUS input file:
*SFLOW
SURFACENAME, QNU
SURFACENAME is the surface name, and QNU is an identifier that tells ABAQUS the
seepage coefficient and a reference fluid pressure will be given for the surface. FLOW
implements Eq. (7-1) at every integration point of the surface. Whether an integration
point is in contact should be determined as the zero fluid pressure was expected to be
144

implemented in non-contacting points. Unfortunately, ABAQUS does not pass the
contact information to this subroutine. As a result, we have to implement an algorithm to
determine if an integration point is in contact or not.
ABAQUS passes the contact pressure at slave surface nodes to URDFIL subroutine, but
ABAQUS does not do so for master surface nodes. Therefore, for a slave surface, the
closest node to an integration point was found. For a master surface, the closest node in
the mating surfaces was found for each integration point. URDFIL was used in both
cases. If the closest node to an integration point was in contact (contact pressure was
larger than zero in the closest node), the pertinent integration point was assumed to be in
contact as well.
7.1.2 URDFIL Subroutine
This subroutine reads the information from the result file. A result file is generated by
ABAQUS if the user requests that in the input file (section 7-2). For example, the nodal
coordinates and pore pressures are written in the result file for a node set called
FEMURE, by the command below:
*NODE FILE, NSET=FEMURE
COORD, POR
The type of written data in the result file depends upon the requests in the input
file. The coordinates of all nodes and also contact pressures in all slave surfaces were
written in the result file in our case. The coordinates of each integration point in the
master surface were known in the FLOW subroutine. As it was explained in section 7.1.1,
145

the code described in this chapter finds the closest node to an integration point and stores
the contact pressure at the node in the memory. As the first step, for each integration
point the contact pressure for the closest node from the previous increment is read. If the
contact pressure is greater than zero, this means the integration point is in contact, and
then the following assignments are done:
= 0 𝑚𝑚𝑚𝑚3
𝑘𝑘0 𝑆𝑆𝑆𝑆
𝑆𝑆0 = 0 𝑀𝑀𝑀𝑀𝑎𝑎 (7-3)
If the contact pressure at the closest node is zero or negative, this means the
integration point is not in contact. In this case, the sign of the velocity component in the
direction of the outward normal to the surface is determined. If that sign is negative, the
adjustments in Eq. (7-3) are done; otherwise, the following assignments are enforced:
= 0.001 𝑚𝑚𝑚𝑚3
𝑘𝑘0 𝑆𝑆𝑆𝑆
𝑆𝑆0 = 0 (7-4)
Figure (7-1) shows this approach for a master surface, in a flowchart format.
146

Read the coordinates of the current integration point
Assume: MINDIS = 2E10
DIS = the distance between current integration point and the next node within the slave surfaces
No DIS > MINDIS
Yes
MINDIS = DIS
No Is this the last node?
𝑓𝑓 < 0
Yes No Yes
Yes
Contact pressure of this node > 0
𝑘𝑘0 = 0, 𝑆𝑆0 = 0 𝑘𝑘0 = 0.001, 𝑆𝑆0 = 0 No
Fig. 7-1: This algorithm is used to distinguish if an integration point in a master surface is in contact or not, and adjust the seepage coefficient accordingly. MINDIS is the distance between the current integration point and the closest node. 𝒌𝒌𝟎𝟎(𝒎𝒎𝒎𝒎
𝟑𝟑)
𝑵𝑵𝑵𝑵 is seepage coefficient, 𝒇𝒇(𝒎𝒎𝒎𝒎 ) is fluid velocity, 𝒖𝒖 is fluid pressure and 𝒖𝒖𝟎𝟎 is a
𝑵𝑵 reference fluid pressure (𝑴𝑴𝑴𝑴𝑴𝑴). "Yeas" means the condition in valid whereas "No" means the condition is not valid.
147

7.2 Result File
The result file must be requested if URDFIL subroutine is used. There is a heading
associated with any type of result data. For instance, the coordinates of nodes is
associated with a heading that specifies the name of the node set for which the
coordinates are written. A key is also associated with any data. For example, pore
pressure is associated with key 108. Results data could be divided into three categories:
integer, real or characters. Arrays “ARRAY” and “JRRAY” contain these data. If the data
is integer or character type “JRRAY” and if the data type is real type, “ARRAY” should
be read. The following example shows how the pore pressure data are written to the result
files, and how they are stored in proper variables in a program.
Data lines to request fluid pressure results in the result file:
NODE FILE, NSET=Femural_Cartilage
POR
Data lines to read and store the number of a node:
INTEGER NODE_NUMBER
NODE_NUMBER = JRRAY(1,2)
Note that node number is the second entry in the JRRAY matrix.
Data lines to read and store the pore pressure of a node:
REAL POR_PRESS
POR_PRESS = ARRAY(4)
Note that pore pressure is the forth entry in the ARRAY vector.
148

7.3 Testing the algorithm
A simple contact model was constructed to test different features of the written code, as
shown in Fig. 7-2. The closest node in the pool of nodes located in the slave surfaces
node set was to be found. To test if the code finds the closest node, a MATLAB program
was also written (Appendix 1). This code was designed to read the coordinates of all
nodes within the slave surface (which was one in this case), and find a node among them,
as close as possible to a given node in the master surface (which was one in this case).
The results obtained from Fortran and MATLAB codes were identical.
Fig. 7-2: A simple model was used to test the algorithm for finding the closest node to an integration point within the master surface.
7.4 Application to the Anatomically Accurate Model
The algorithm was applied on a three-dimensional anatomically accurate model of the
knee joint. For this purpose, no zero fluid pressure boundary condition at the surface was
manually given, but the fluid pressure at the femoral cartilage was defined to be 149

determined according to the algorithm described in section (7-2). The result is shown in
Fig. 7-3. From this figure, we can at least conclude that the algorithm defined the zero
and nonzero fluid pressure zones as expected.
To examine the importance of zero fluid pressure boundary condition at the non-
contact surfaces, another case was studied. In that case, no fluid pressure boundary
conditions were specified for non-contacting surfaces. The resulting fluid pressure is
shown in Fig. 7-4 which is noticeably similar to Fig. 7-3. Even the contour pressures
obtained in Chapters 3, 4, and 5 for the normal model are similar to Figs. 7-3 and 7-4 (see
for example, Fig. 4-2). In Chapters 3, 4, and 5 the fluid pressure at non-contacting
surfaces was implemented by defining a set of nodes, and fluid pressure was manually
enforced to be zero in these nodes. Therefore, a boundary condition to enforce zero fluid
pressure may not affect the results significantly for problems with small simple knee
compression, where the deformation is localized and the contact area does not change
much. However, we indeed need to adjust the boundary conditions per contact conditions
when the knee compression is large or significant sliding and flexion is involved.
150

Fig. 7-3: Surface fluid pressure at the femoral cartilage when the algorithm shown in Fig. 7-1 was used to enforce the fluid pressure boundary conditions (@3s).
151

Fig. 7-4: Surface fluid pressure at the femoral cartilage when no boundary condition was enforced for the free surfaces (@3s).
152

Chapter Eight: Conclusion
8.1 Summary
The effect of normal and pathological properties of articular cartilage on the mechanical
behavior of the human knee joint was studied with emphasize on the fluid pressurization.
Depth-dependent structure and integrity are two of the important features of cartilage.
The hypotheses were: (1) the depth-dependent structure enhances cartilage surface fluid
pressure; (2) a local degeneration in a high load-bearing area in the medial femoral
condyle reduces the surface fluid pressure and the deeper the degeneration is, the more
reduced fluid pressure will be; (3) a local cartilage defect in a high load-bearing area in
the medial femoral condyle reduces fluid pressure and a deeper defect has more
destructive effects on the fluid pressurization. An anatomically accurate finite element
model of the knee joint was constructed using ABAQUS software package to test the
hypotheses.
Depth-dependent properties improved the load bearing capability of the knee
joint. The contribution of fluid pressurization to the applied load significantly reduces the
burden on the solid part of cartilage. Fluid pressurization plays more important roles at
the cartilage surface compared to the deeper zones, as the surface zone has more parallel
collagen fibres. Results showed the depth-dependent properties of cartilage produce
higher surface fluid pressure, supporting our first hypothesis.
Our second hypothesis was also supported. Degenerations leading to advanced
OA could develop from cartilage surface. Advancing layer by layer, degeneration alters
153

the mechanical properties of the tissue including Young's modulus and permeability. As
results showed, degeneration advancement to a layer is associated with decreased fluid
pressure within all other layers including the surface layer. This result implies that the
development of degeneration from the surface facilitates its further development. The
deep cartilage layers close to the cartilage-bone interface experience higher shear strains
as a result of depth-wise advancement of degeneration, increasing the risks of
microfractures occurring at cartilage-bone interface.
The destructive effects due to cartilage defect was also studied using the
anatomically accurate geometry of the knee joint. The effects of cartilage defects on the
knee joint mechanics are more complex compared to cartilage degeneration. Depth-wise
progression of the degeneration was associated with decreased fluid pressure within all
layers, whereas higher fluid pressures were obtained when a defect progressed to the
middle zone of cartilage. Therefore, our third hypothesis was not supported by the results.
8.2 Limitations
A numerical model could be interpreted as a product extracted from a real phenomenon
after simplifying assumptions have been implemented. These simplifying assumptions
cause the major portion of the limitations of any numerical model including the
anatomically accurate normal and pathological models developed in this project. This
section describes the limitations, some of which were discussed in Chapters 3, 4, and 5.
One weak point of the present modelling is the computational time. The analysis
of depth-dependent normal model took almost one week to complete the first second of
154

simulations (loading phase) on a desktop computer with 4 CPUs and 12 GB RAM. When
the number of elements is increased or the loading conditions become more complex the
simulation time increases dramatically. The issue of simulation time becomes more
apparent when the restrictions on the number of ABAQUS licenses are taken into
consideration. Multiple simulations were run in parallel as each one needed a long time to
complete. As a result, too many licenses had to be used simultaneously for long periods,
which was hardly possible using available computational facilities at the University. Due
to long simulation time, local cartilage degeneration (Chapter 4) was modeled for 1s. A
better comparison between effects of degenerations and defects would be possible if the
degenerated case studies were modeled for higher loads as it was done for defects
(Chapter 5).
Simplified loading and boundary conditions are other aspects of the limitations.
Realistic loadings resulting from daily living activities such as gait should be
implemented to make the results more applicable. In this study, however, standard lab
testing loadings including compressive load and displacement were used. Although these
standard loadings provided important insights to the mechanics of the knee joint, some
phenomena will not be seen in the modeling unless loading conditions resembling daily
living activities are considered. For instance, a complex transient loading combined with
forces and moments are applied during a gait cycle in 0.8s. These combined loadings and
their durations have effects on pore pressure, stress, and strain distribution that are not
captured in this project.
155

Lack of experimental validation of the whole knee model is another limitation.
The results from simulations were in line with experimental and numerical reports. The
constitutive model has been extensively validated against experimental measurements (Li
et al., 1999, 2008). Consequently, the results are qualitatively ascertained to reflect the
mechanical behavior of the knee joint in real situations. However, the results would be
more trustworthy if the model is quantitatively validated at the whole joint level.
The sensitivity of the models was not performed for all parameters. The size of
finite element meshes, material properties, fiber orientations, the amplitude and rate of
the loads, boundary conditions, and errors due to the model reconstruction and other
parameters can be altered to investigate how they affect the results. Examples of model
sensitivity analysis can be found in a previous study conducted in our research group
(Kazemi 2013).
The interface between cartilage and bone plays an important role. The current
model assumes the cartilage thickness to be composed of three zones: superficial, middle
and deep zones. Calcified cartilage which is below the deep zone could improve the
accuracy of results when included in a depth-dependent model. This zone of cartilage
becomes more important when the effect of bone stiffness on the mechanics of cartilage
is modeled. The interface between bone and cartilage which includes the calcified zone
significantly influences the development of osteoarthritis (Burr and Radin, 2003, Burr,
2004), but the calcified zone was not modelled in our studies.
Loads, boundary conditions, degeneration area and depth, and defected regions
are altered simultaneously during the development of OA. As a result of this disease, the
156

patient adjusts his/her kinematics and kinetics during activities such as gait (Kaufman et
al., 2001), which means the applied loads and boundary conditions are not constant with
the advancement of OA. Moreover, the areas of degenerated and lost cartilage are
varying with the progression of the disease. However, these changes have not been
considered simultaneously in our studies.
As a last remark, modeling can never be performed without simplifications.
Therefore, limitations will be a part of the model. For example, since the knee joint is one
part of the whole body, another limitation is not to have considered the joint as an
integrated part of the whole body, or at least the lower extremity (Beillas et al., 2004).
8.3 Future Work
Validation of the results obtained for the anatomically accurate model is one of future
directions. Due to the invasive nature of the required procedure, direct in vivo
measurement of parameters such as stress and pore pressure currently seems to be
infeasible. However, measurement of deformation can be performed with medical
imaging. Some measurements can be performed on cadaveric samples and used to
validate the computational results. For instance, contact pressure is a parameter that can
be experimentally measured in cadaveric knee joints using pressure sensors, which could
be compared with computed contact pressures from the model (Papaioannou et al., 2008,
Fukubayashi and Kurosawa, 1980).
Improving the load and boundary conditions according to the kinematics and
kinetics of the lower limb during the gait cycle is a topic of future research. Gait analysis
157

experiments should be conducted to obtain the motions of different joints as well as the
reactions between the ground and the foot. Using inverse dynamics methods, the forces
and moments applied to the knee joint can be calculated (Zajac et al., 2002). These
loading data along with motions obtained for different joints can be used to model the
knee joint mechanics during a whole gait cycle. Modeling the knee joint as a part of a
larger model of the lower extremity will help to implement the loading conditions more
realistically (Beillas et al., 2004). These improvements will deal with challenges such as
numerical difficulties in convergence of the model, high demand in computational
facilities, and problems with capturing the geometry of the lower extremity during a gait
cycle.
The transient nature of muscle forces should be considered in the model as they
vary with time during different activities. The individual muscle forces vary during
different stages of the gait cycle. These forces can be determined according to the
protocol explained in Chapter 6 to model the contact mechanics of the knee joint. Other
activities such as sitting to standing motions, running, or pathological motions such as
gait of below-the-knee amputees can be analyzed to determine kinematic and kinetics of
the lower extremity including muscle forces. These data can then be incorporated in the
finite element anatomically accurate model to get a better understanding about the
development of osteoarthritis in the knee joint.
The depth-dependent structure of cartilage is important when designing artificial
cartilage. Tissue-engineered cartilage might be used as a replacement to biological
cartilage. Knowledge of the structure and properties of cartilage is necessary to design the
158

implanted cartilage so that it mimics the mechanical behavior of native cartilage.
Modeling the depth-dependent structure of cartilage in an anatomically accurate model
provides more accurate results when compared to the case of standard geometries. The
results reported in this thesis could be used as a reference when designing tissue-
engineered cartilage (Ateshian and Hung, 2005).
159

References
Allard P, Cappozzo A, Lundberg A, Vaughan ChL. Three-dimensional analysis of human
locomotion, West Sussex: John Wiley & Sons; 1997.
American Academy of Orthopaedic Surgeons (AAOS). Common Knee Injuries [Online].
Available: http://orthoinfo.aaos.org/topic.cfm?topic=A00325 2007 [Accessed July 6,
2012].
Anderson FC, Pandy MG. Static and dynamic optimization solutions for gait are
practically equivalent. J Biomech 2001;34:153-61.
Ateshian GA, Hung CT. Patellofemoral joint biomechanics and tissue engineering. Clin
Orthop Relat Res 2005;436:81-90.
Athanasiou K, Darling E, and Hu J. Articular cartilage tissue engineering. San Rafael,
Morgan and Claypool Publishers; 2010.
Atkinson PJ, Haut RC. Subfracture insult to the human cadaver patellofemoral joint
produces occult injury. J Orthop Res 1995;13:936-44.
Bagge E, Brooks P. Osteoarthritis in older patients. Optimum treatment. Drugs Aging
1995;7:176-83.
Beillas P, Papaioannou G, Tashman S, Yang KH. A new method to investigate in vivo
knee behavior using a finite element model of the lower limb. J Biomech 2004; 37: 1019
30.
Bendjaballah MZ, Shirazi-Adi A, Zukor DJ. Biomechanics of the human knee joint in
compression: reconstruction, mesh generation and finite element analysis. Knee
1995;2:69-79.
160

Besier TF, Fredericson M, Gold GE, Beaupré GS, Delp SL. Knee muscle forces during
walking and running in patellofemoral pain patients and pain-free controls. J Biomech
2009;42:898-905.
Biot M. General theory of three-dimensional consolidation. Journal of Applied Physics
1941;12:155-164.
Blankevoort L, Kuiper JH, Huiskes R, Grootenboer HJ. Articular contact in a three-
dimensional model of the knee. J Biomech 1991;24:1019-31.
Burr DB. The importance of subchondral bone in the progression of osteoarthritis. J
Rheumatol Suppl 2004;70:77-80.
Burr DB, Radin EL. Microfractures and microcracks in subchondral bone: are they
relevant to osteoarthrosis? Rheum Dis Clin North Am 2003;29:675-85.
Cailliet R. Knee Pain and Disability. third ed. Philadelphia: F. A. Davis Company; 1992.
p. 70-261.
Carter D, Wong M. Modelling cartilage mechanobiology. Philosophical Transactions of
the Royal Society of London Series B-Biological Sciences 2003;358:1461-71.
Centers for Disease Control and Prevention. Athritis [Online]. Available:
http://www.cdc.gov/arthritis/ 2012 [Accessed July 6, 2012].
Centers for Disease Control and Prevention. Prevalence of self-reported arthritis or
chronic joint symptoms among adults--United States, 2001. MMWR Morb Mortal Wkly
Rep 2002, 51, 948-50.
Cheatham SA, Johnson DL. Current concepts in ACL Injuries. Phys Sportsmed
2010;38:61-8.
161

Crowninshield RD, Brand RA. A physiologically based criterion of muscle force
prediction in locomotion, J Biomech 1981;14:793-801.
Dabiri Y, Najarian S, Eslami MR, Zahedi S, Moser D. A powered prosthetic knee joint
inspired from musculoskeletal system, Biocybern Biomed Eng 2013; 33:118-24.
Delp SL. Surgery simulation: A computer-graphics system to analyze and design
musculoskeletal reconstructions of the lower limb. Stanford University, Ph.D. Thesis,
1990a; p.89-105.
Delp SL. Surgery simulation: A computer-graphics system to analyze and design
musculoskeletal reconstructions of the lower limb. Stanford University, Ph.D. Thesis,
1990b; p.22-4.
Federico S, La Rosa G, Herzog W, and Wu JZ. Effect of fluid boundary conditions on
joint contact mechanics and applications to the modelling of osteoarthritic joints, J
Biomech Eng 2004;126:220–25.
Federico S, Herzog W, and Wu JZ. Erratum: effect of fluid boundary conditions on joint
contact mechanics and applications to the modelling of osteoarthritic joints, J Biomech
Eng 2005;127:208–9.
Felson DT, Zhang Y. An update on the epidemiology of knee and hip osteoarthritis with
a view to prevention. Arthritis Rheum 1998;41:1343-55.
Fukubayashi T, Kurosawa H. The contact area and pressure distribution pattern of the
knee. A study of normal and osteoarthrotic knee joints. Acta Orthop Scand 1980;51:871
9.
162

Gu K, An anatomically-accurate finite element knee model accounting for fluid pressure
in articular cartilage, the University of Calgary, M.Sc. Thesis, 2010.
Hashemi J, Mansouri H, Chandrashekar N, Slauterbeck JR, Hardy DM, Beynnon BD.
Age, sex, body anthropometry, and ACL size predict the structural properties of the
human anterior cruciate ligament. J Orthop Res 2011;29:993-1001.
Hasler EM, Herzog W, Wu JZ, Müller W, Wyss U. Articular cartilage biomechanics:
theoretical models, material properties, and biosynthetic response. Crit Rev Biomed Eng
1999;27:415-88.
Hayes WC, Keer LM, Herrmann G, Mockros LF. A mathematical analysis for
indentation tests of articular cartilage. J Biomech 1972;5:541-51.
Hughes T. The Finite Element Method. Englewood Cliffs: Prentice-Hall; 1987.
Kaufman KR, Hughes C, Morrey BF, Morrey M, An KN. Gait characteristics of patients
with knee osteoarthritis. J Biomech 2001;34:907-15.
Kazemi M. Finite Element Study of the Healthy and Meniscectomized Knee Joints
Considering Fibril-Reinforced Poromechanical Behaviour for Cartilages and Menisci, the
University of Calgary, Ph.D. Thesis,2013.
Kazemi M, Dabiri Y, Li LP. Recent advances in computational mechanics of the human
knee joint. Comput Math Methods Med 2013;2013:1–27,
http://dx.doi.org/10.1155/2013/718423.
Kellis E, Baltzopoulos V. 1999. In vivo determination of the patella tendon and
hamstrings moment arms in adult males using videofluoroscopy during submaximal knee
extension and flexion. Clin Biomech 1999;14:118–24.
163

Kempson GE, Muir H, Swanson SA, Freeman MA. Correlations between stiffness and
the chemical constituents of cartilage on the human femoral head. Biochim Biophys Acta
1970;215:70-7.
Knecht S, Vanwanseele B, Stüssi E. A review on the mechanical quality of articular
cartilage - implications for the diagnosis of osteoarthritis. Clin Biomech (Bristol, Avon)
2006;21:999-1012.
Korhonen RK, Laasanen MS, Töyräs J, Rieppo J, Hirvonen J, Helminen HJ, Jurvelin JS.
Comparison of the equilibrium response of articular cartilage in unconfined compression,
confined compression and indentation. J Biomech 2002;35:903-9.
Kuster MS, Graeme AW, Stachowiak GW, G chter A. Joint load considerations in total
knee replacemnet. J Bone Joint Surg Br 79;1:109-13.
Larson RL, Grana WA. The knee form, function, pathology, and treatment. Philadelphia:
W.B. Saunders; 1993.
Lawrence RC, Hochberg MC, Kelsey JL, Mcduffie FC, Medsger TA, Felts WR, Shulman
LE. Estimates of the prevalence of selected arthritic and musculoskeletal diseases in the
United States. J Rheumatol 1989;16:427-41.
Lethbridge-Cejku M, Schiller JS, Bernadel L. Summary health statistics for U.S. adults:
National Health Interview Survey, 2002. Vital Health Stat 2004;10:1-151.
Levenston M, Frank E, Grodzinsky A. Variationally derived 3-field finite element
formulations for quasistatic poroelastic analysis of hydrated biological tissues. Computer
Methods in Applied Mechanics and Engineering 1998;156:231-46.
164

Li LP, Herzog W. Strain-rate dependence of cartilage stiffness in unconfined
compression: the role of fibril reinforcement versus tissue volume change in fluid
pressurization, J Biomech 2004; 37: 375–82.
Li LP, Korhonen RK, Iivarinen J, Jurvelin JS, Herzog W. Fluid pressure driven fibril
reinforcement in creep and relaxation tests of articular cartilage. Med Eng Phys
2008;30:182–9.
Li LP, Soulhat J, Buschmann MD, Shirazi-Adl A. Nonlinear analysis of cartilage in
unconfined ramp compression using a fibril reinforced poroelastic model. Clin Biomech
(Bristol, Avon) 1999;14:673-82.
Manek NJ, Lane NE. Osteoarthritis: current concepts in diagnosis and management. Am
Fam Physician 2000;61:1795-804.
Manheimer E, Linde K, Lao L, Bouter LM, Berman BM. Meta-analysis: acupuncture for
osteoarthritis of the knee. Ann Intern Med 2007;146:868-77.
Mansour JM. Biomechanics of cartilage. In: Oatis CA, editors. Kinesiology: the
Mechanics and Pathomechanics of Human Movement. Philadelphia: Lippincott Williams
and Wilkins; 2004. p. 66-79.
Martinez-Villalpando EC, Herr H. Agonist-antagonist active knee prosthesis: a
preliminary study in level-ground walking, J Rehabil Res 2009;46:361-73.
Mononen ME, Mikkola MT, Julkunen P, Ojala R, Nieminen MT, Jurvelin JS, Korhonen
RK. Effect of superficial collagen patterns and fibrillation of femoral articular cartilage
on knee joint mechanics-a 3D finite element analysis. J Biomech 2012;45:579-87.
165

Mow V, Ateshian G. Lubrication and wear of diarthrodial joints. In: Mow V, Hayes W,
editors. Basic orthopaedic biomechanics. second ed. Philadelphia: Lippincott-Raven;
1997. p. 275-316.
Mow VC, Kuei SC, Lai WM, Armstrong CG. Biphasic creep and stress relaxation of
articular cartilage in compression: theory and experiments. J Biomech Eng 1980;102:73
84.
Mow V, Ratcliffe A. Structure and function of articular cartilage and meniscus. In: Mow
V, Hayes W, editors. Basic orthopaedic biomechanics. second ed. Philadelphia:
Lippincott-Raven; 1997. p. 113-77.
Nordqvist C. What is Arthritis? What Causes Arthritis? [Online]. Available:
http://www.medicalnewstoday.com/articles/7621.php 2009 [Accessed July 6, 2012
2012].
Oliveria SA, Felson DT, Reed JI, Cirillo PA, Walker AM. Incidence of symptomatic
hand, hip, and knee osteoarthritis among patients in a health maintenance organization.
Arthritis Rheum 1995;38:1134-41.
Papaioannou G, Nianios G, Mitrogiannis C, Fyhrie D, Tashman S, Yang KH. Patient-
specific knee joint finite element model validation with high-accuracy kinematics from
biplane dynamic Roentgen stereogrammetric analysis. J Biomech 2008;41:2633-8.
Park S, Hung CT, Ateshian GA. Mechanical response of bovine articular cartilage under
dynamic unconfined compression loading at physiological stress levels. Osteoarthritis
Cartilage 2004;12:65-73.
166

Pauwels F. Biomechanics of the normal and diseased hip. Theoretical foundation.
Techniques and results of treatment, an atlas. Berlin: Springer-Verlag; 1976.
Pawaskar SS, Fisher J, Jin Z. Robust and general method for determining surface fluid
flow boundary conditions in articular cartilage contact mechanics modeling, J Biomech
Eng 2010;132:031001.
Peat G, Mccarney R, Croft P. Knee pain and osteoarthritis in older adults: a review of
community burden and current use of primary health care. Ann Rheum Dis 2001;60:91-7.
Peña E, Calvo B, Martínez MA, Palanca D, Doblaré M. Finite element analysis of the
effect of meniscal tears and meniscectomies on human knee biomechanics. Clin Biomech
(Bristol, Avon) 2005;20:498-507.
Perry J. Gait analysis: normal and pathological function. Thorofare: Slack; 1992.
Piazza SJ, Delp SL. 1996. The influence of muscles on knee flexion during the swing
phase of gait. J Biomech 1996;29:723-33.
Powers CM, Lilley JC, Lee TQ. The effects of axial and multi-plane loading of the
extensor mechanism on the patellofemoral joint. Clin Biomech (Bristol,
Avon) 1998;13:616-624.
Radin EL. Factors influencing the progression of osteoarthritis. In: Ewing J, editors.
Articular cartilage and knee joint function basic science and arthroscopy. New York:
Raven Press; 1990. p. 301-09.
Saarakkala S, Julkunen P, Kiviranta P, Mäkitalo J, Jurvelin JS, Korhonen RK. Depth-
wise progression of osteoarthritis in human articular cartilage: investigation of
composition, structure and biomechanics. Osteoarthritis Cartilage 2010;18:73-81.
167

Saarakkala S, Laasanen MS, Jurvelin JS, Törrönen K, Lammi MJ, Lappalainen R, Töyräs
J. Ultrasound indentation of normal and spontaneously degenerated bovine articular
cartilage. Osteoarthritis Cartilage 2003;11:697-705.
Schinagl RM, Gurskis D, Chen AC, Sah RL. Depth-dependent confined compression
modulus of full-thickness bovine articular cartilage. J Orthop Res 1997;15:499-506.
Shirazi R, Shirazi-Adl A, Hurtig M. Role of cartilage collagen fibrils networks in knee
joint biomechanics under compression. J Biomech 2008;41:3340-8.
Soltz MA, Ateshian GA. Experimental verification and theoretical prediction of cartilage
interstitial fluid pressurization at an impermeable contact interface in confined
compression. J Biomech 1998;31:927-34.
Stoddard S, Jans L, Ripple J, Kraus L. Chartbook on Work and Disability in the United
States. An InfoUse Report. Washington, D.C.: U.S. National Institute on Disability and
Rehabilitation Research 1998.
Sup F, Bohara A, Goldfarb M. Design and control of a powered transfemoral prosthesis.
Int J Robot Res 2008;27:263-73.
Taylor ZA, Miller K. Constitutive modeling of cartilaginous tissues: a review. J Appl
Biomech 2006;22:212-29.
Tsahakis PJ, Brick GW, Thornhill ThS. Arthritis and Arthroplasty. In: Larson RL, Grana
WA, editors. The knee form, function, pathology, and treatment. Philadelphia: W.B.
Saunders; 1993. P. 273-322.
168

Wilson W, Van Donkelaar CC, Van Rietbergen B, Ito K, Huiskes R. Stresses in the local
collagen network of articular cartilage: a poroviscoelastic fibril-reinforced finite element
study. J Biomech 2004;37:357-66.
Winter DA. The Biomechanics and motor control of human gait: normal, elderly and
pathological, second ed. Waterloo: University of Waterloo Press; 1991.
Yang NH, Canavan PK, Nayeb-Hashemi H, Najafi B, Vaziri A. 2010. Protocol for
constructing subject-specific biomechanical models of knee joint. Comput Methods
Biomech Biomed Engin 2010;13:589-603.
Zajac FE, Neptune RR, Kautz SA. Biomechanics and muscle coordination of human
walking. Part I: introduction to concepts, power transfer, dynamics and simulations. Gait
Posture 2002; 16:215-32.
169

Appendix 1: The MATLAB code developed to test the Fortran code for zero fluid pressure boundary condition
function D = testclose()
load the coordinates data of slave surfaces.
for count2 = 1:number of slave surfaces
store the coordinate data of all slave nodes in a matrix.
end
read the coordinates of a master node.
Set the initia guess for the minimum distance.
MINDIS = 5000;
for count1 = 1:number of slave nodes;
store the coordinates of the current slave node in a vector.
Calculate the length of the vector obtained by subtracting the vector of master node
coordinates from the vector of current slave node coordinates (dis);
if(dis < MINDIS)
MINDIS = dis;
row = count1;
end
end
store MINDIS and row
end
170

Appendix 2: The FORTRAN code developed to implement the zero fluid pressure for non-contacting surfaces
SUBROUTINE FLOW(H, SINK, U, KSTEP, KINC, TIME, NOEL, NPT, COORDS,
1 JLTPY, SNAME)
C
INCLUDE 'ABA_PARAM.INC'
C Establish the data in the common block.
COMMON /VECTORS/ V1,V2,V3,V4,V5,V6,V7,V8
C######################################################################
Set a high value for the minimum distance between a master node and a slave node
(MINDIS2).
MINDIS2 = 10e20;
c These are the coordinates of the current integration point.
Read the coordinates of the current integration point (COORDS(1), COORDS(2),
COORDS(3)).
XI = V11(NPT)
YI = V12(NPT)
ZI = V13(NPT)
DO COUNT9=1, 100000 (a number equal to or greater than the number of slave nodes)
Determine the surface to which this slave node belongs, from the common block.
Recall the coordinates of the current slave nodes from common block.
XN = V3(COUNT9)
YN = V4(COUNT9) 171

ZN = V5(COUNT9)
IF this node does not belong to the master surface:
Determine the distance between the current integration point and the current slave node.
DIS2 = SQRT((XI-XN)**2 + (YI-YN)**2 + (ZI-ZN)**2)
IF (MINDIS2.GT.DIS2) THEN
MINDIS2 = DIS2
Store the number of current slave node.
ENDIF
ENDIF
ENDDO
C######################################################################
Read the number of closest node to the current integration point, from previous section.
NEAREST_NODE = V14(NPT)
Read the value of the contact pressure for the nearest node to the current integration
point.
IF (contact pressure.GT.0) Then
Set the appropriate values for seepage coefficient (H) and reference pore pressure (SINK)
H = 0
SINK = 0
ELSEIF (contact pressure.LT.0.OR.contact pressure.EQ.0) THEN
IF (normal outflow velocity.LT.0) THEN
H = 0
172
SINK = 0
ELSE
H= 0.001
SINK=0
ENDIF
ENDIF
ENDIF
RETURN
END
C######################################################################
SUBROUTINE URDFIL(LSTOP, LOVRWRT, KSTEP, KINC, DTIME, TIME)
C
INCLUDE 'ABA_PARAM.INC'
C
DIMENSION ARRAY(513),JRRAY(NPRECD,513),TIME(2)
EQUIVALENCE (ARRAY(1),JRRAY(1,1))
Establish the common block.
COMMON /VECTORS/ V1,V2,V3,V4,V5,V6,V7,V8
C**********************************************************************
DO K1=1, 999999
CALL DBFILE(0, ARRAY, JRCD)
IF (JRCD .NE. 0) GO TO 110
173
KEY = JRRAY(1,2)
IF (KEY.EQ.1503) THEN
KEY 1503 has the information of the name of contacting surfaces.
Store the name of master and slave nodes.
C**********************************************************************
ELSEIF (KEY.EQ.1504.AND. this is the tibial cartilage) THEN
KEY 1504 has the node numbers of contacting surfaces.
Store the number of the current node
ELSEIF (KEY.EQ.1511.AND. this is the tibial cartilage) THEN
KEY 1511 has the contact pressure on a slave node.
ELSEIF (KEY.EQ.1911) THEN
KEY 1911 has the names of node sets.
ELSEIF (KEY.EQ.107.AND.the node set is the tibial cartilage node set) THEN
KEY 107 has the node number and its coordinates.
Store the coordinates of the node.
ELSEIF (KEY.EQ.108.AND.the node set is the tibial cartilage node set) THEN
KEY 108 has the pore pressure at a node.
Store the value of pore pressure at this node
READING DATA OF THE SECOND SLAVE SURFACE (Tibia Cartilages).
IF (KEY.EQ.1504.AND. this is the menisci surface) THEN
KEY 1504 has the node numbers of contacting surfaces.
Store the number of the current node
C
174

ELSEIF (KEY.EQ.1511.AND. this is the menisci surface) THEN
KEY 1511 has the contact pressure on a slave node.
Store the value of contact pressure
ELSEIF (KEY.EQ.107.AND.the node set is the menisci node set) THEN
Store the coordinates of the node.
ELSEIF (KEY.EQ.108.AND.the node set is the menisci node set) THEN
Store the value of pore pressure at this node
C READING DATA OF THE MASTER SURFACE.
IF (KEY.EQ.1504.AND. this is the femoral cartilage surface) THEN
Store the number of the current node
ELSEIF (KEY.EQ.107.AND.the node set is the femoral cartilage node set) THEN
KEY 107 has the node number and its coordinates.
Store the coordinates of the node.
C THE CONTACT PRESSURE IS UPDATED FOR MASTER NODES HERE.
C######################################################################
MINDIS = 10e20;
C These are the coordinates of the current master node.
X1 = COOR1
Y1 = COOR2
Z1 = COOR3
DO COUNT5=1,2000 (a number equal to or greater than the number of all nodes)
IF the current node is not in the femoral cartilage
175

Recall the coordinates of the current slave node from stored data.
Determine the distance between the current slave node and the master node.
DIS = SQRT((X1-X2)**2 + (Y1-Y2)**2 + (Z1-Z2)**2)
IF (MINDIS.GT.DIS) THEN
MINDIS = DIS
Set the contact pressure at the current master node equal to contact pressure at the closest
slave node.
ENDIF
ENDIF
ENDDO
C**********************************************************************
110 CONTINUE
RETURN
END
176

Appendix 3: The Copyright Permission Letter
177

178

179

180

181

Journal and Conference Papers and Abstracts
Journal Papers
Dabiri Y, Li LP. Influences of the depth-dependent material inhomogeneity of articular
cartilage on the fluid pressurization in the human knee. Medical Engineering &
Physics 2013; 35(11), 1591-1598.
Dabiri Y, Li LP. Altered knee joint mechanics in simple compression associated with
early cartilage degeneration. Computational and Mathematical Methods in Medicine
2013; 2013: 1-11, http://dx.doi.org/10.1155/2013/862903.
Dabiri Y, Li LP. Load Bearing Characteristics of the Knee Joint Deteriorates with the
Defect Depth of Articular Cartilage, submitted to Medical & Biological Engineering
& Computing.
Kazemi M, Dabiri Y, Li LP. Recent advances in computational mechanics of the human
knee joint. Comput Math Methods Med 2013; 2013: 1–27,
http://dx.doi.org/10.1155/2013/718423.
Conference Papers and Abstracts
Dabiri Y, Li LP. Comparison of Cartilage Degeneration and Defect on Fluid
Pressurization in the Human Knee, Saskatoon, Canada, June 2-6, 2013.
Dabiri Y, Ahsanizadeh S, Li LP. Effects of the depth of cartilage defect on the knee joint
mechanics: a depth-dependent fiber-reinforced depth-dependent poroelastic model, Salt Lake
City, Utah, USA, April 3-6, 2013.
182

Dabiri Y, and Li LP. A numerical model of mechanics of osteoarthritis in human knee joint,
ASME 2012 International Mechanical Engineering Conference and Exposition, Houston,
Texas, USA, November 9-15, 2012.
Dabiri Y, Li LP. Effect of depth-dependent cartilage properties on cartilage bone interface
mechanics, Canadian Society of Mechanical Engineering, Winnipeg, Canada, June 4-6,
2012.
Dabiri Y, Kazemi M, Li LP. A finite element model of mechanical behaviour of human
knee with osteoarthritis, Canadian Society of Biomechanics, Vancouver, Canada,
June 6-9, 2012.
Dabiri Y, Li LP. The mechanical role of the zonal differences of intact human knee
cartilage, European Society of Biomechanics, Lisbon, Portugal, July 1-4, 2012.
Dabiri Y, Li LP, Mechanical response of human knee joint to sinusoidal compression –
influence of fluid pressurization in soft tissues, ASME summer bioengineering
conference, Puerto Rico, USA, June 20-23, 2012.
Zheng H, Dabiri Y, Kazemi M, Li LP, 3D Knee Joint Reconstruction from MR Images,
12th Alberta biomedical engineering conference, 2011, Banff, Canada, October 21
23, 2011.
Dabiri Y, Kazemi M, Li LP. Influence of the zonal differences on the mechanics of
articular cartilage in the knee joint. WACBE 5th World Congress on Bioengineering,
Tainan, Republic of China, August 18-21, 2011.
183