the new pharmepa restore and maintain – scientific basis and clinical application
TRANSCRIPT

Pharmepa RESTORE & MAINTAIN®Fast, effective and 100% tailorable
omega-3 treatment protocol
Talk outline
• What is RESTORE & MAINTAIN?
• Role of omega-3 in clinical nutrition
• Using biomarkers to personalise treatment and dosing
• Manipulating Pharmepa for truly personalised support
• Key areas of R&M application
• General dosing guidelines (condition specific)
• Igennus is the only independent manufacturer of specialist Fatty Acid in the UK. Based in Cambridge the medical innovation hub for the UK:
- Seven Seas Merck Pharma Germany- Minami Atrium Pharma Canada- Biocare Elder Pharma India- Eskimo 3 Bringwell Pharma Sweden- Equizen Vifor Pharma Swiss
Pharmepa RESTORE provides 1000 mg pure 90% concentration, rTG EPA wild anchovy oil, in just two easy-to-swallow capsules.
This product provides a loading dose of super strength EPA and is ideal for people who have never supplemented with pure EPA or those who have taken a break from omega-3 EPA supplementation.
• Igennus is the only independent manufacturer of specialist Fatty Acid in the UK. Based in Cambridge the medical innovation hub for the UK:
- Seven Seas Merck Pharma Germany- Minami Atrium Pharma Canada- Biocare Elder Pharma India- Eskimo 3 Bringwell Pharma Sweden- Equizen Vifor Pharma Swiss
Pharmepa MAINTAIN combines 80% concentrated rTG EPA (750mg) plus DHA (250mg) wild anchovy oil with GLA and triterpenes from organic virgin evening primrose oil and vitamins D3 & E.
Pharmepa MAINTAIN protects the structure and function of our cells and helps maintain an optimal AA to EPA ratio, omega-6 to omega-3 ratio and omega-3 index.
Pharmepa MAINTAIN is suitable for long-term use after supplementing with pure EPA.
Long-term users of omega-3 supplements or anyone who is otherwise healthy may skip RESTORE and move straight to MAINTAIN.
• Igennus is the only independent manufacturer of specialist Fatty Acid in the UK. Based in Cambridge the medical innovation hub for the UK:
- Seven Seas Merck Pharma Germany- Minami Atrium Pharma Canada- Biocare Elder Pharma India- Eskimo 3 Bringwell Pharma Sweden- Equizen Vifor Pharma Swiss
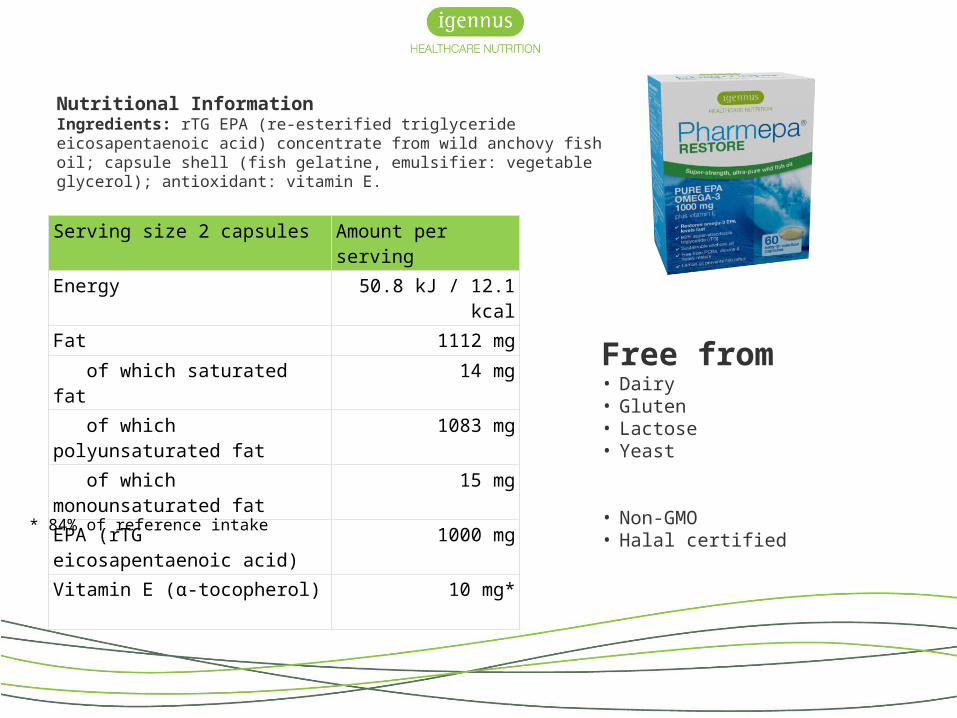
Serving size 2 capsules Amount per serving
Energy 50.8 kJ / 12.1 kcal
Fat 1112 mg
of which saturated fat 14 mg
of which polyunsaturated fat 1083 mg
of which monounsaturated fat 15 mg
EPA (rTG eicosapentaenoic acid) 1000 mg
Vitamin E (α-tocopherol) 10 mg*
Nutritional InformationIngredients: rTG EPA (re-esterified triglyceride eicosapentaenoic acid) concentrate from wild anchovy fish oil; capsule shell (fish gelatine, emulsifier: vegetable glycerol); antioxidant: vitamin E.
Free from• Dairy• Gluten• Lactose• Yeast
• Non-GMO• Halal certified
* 84% of reference intake
• Igennus is the only independent manufacturer of specialist Fatty Acid in the UK. Based in Cambridge the medical innovation hub for the UK:
- Seven Seas Merck Pharma Germany- Minami Atrium Pharma Canada- Biocare Elder Pharma India- Eskimo 3 Bringwell Pharma Sweden- Equizen Vifor Pharma Swiss
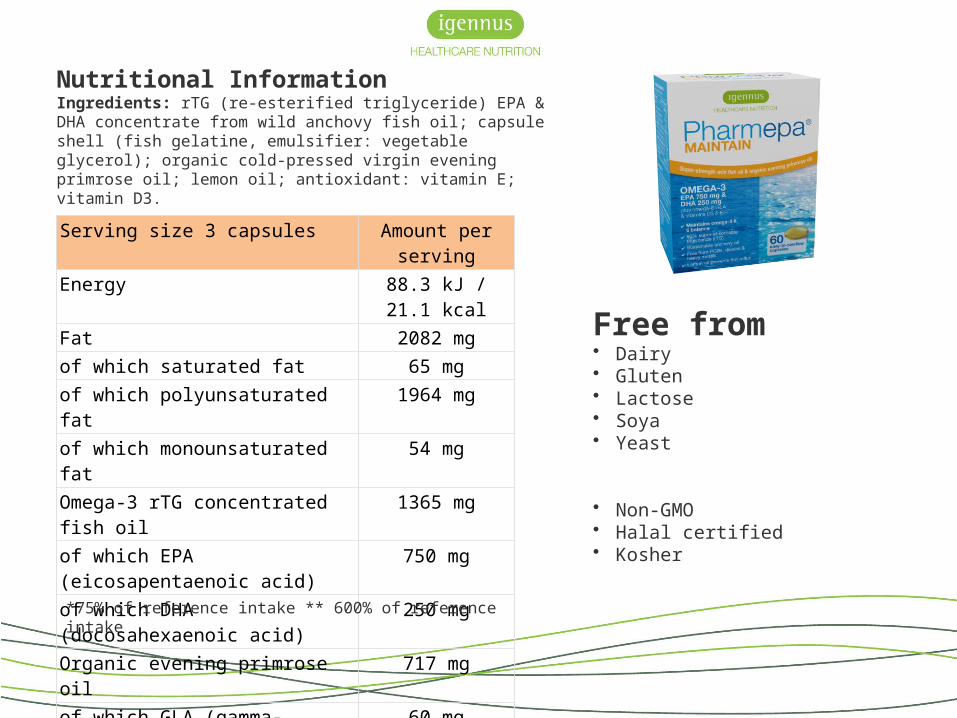
Serving size 3 capsules Amount per serving
Energy 88.3 kJ / 21.1 kcal
Fat 2082 mgof which saturated fat 65 mgof which polyunsaturated fat 1964 mgof which monounsaturated fat 54 mgOmega-3 rTG concentrated fish oil 1365 mgof which EPA (eicosapentaenoic acid) 750 mg
of which DHA (docosahexaenoic acid) 250 mg
Organic evening primrose oil 717 mgof which GLA (gamma-linolenic acid) 60 mgVitamin E (d-alpha tocopherol) 9 mg*Vitamin D3 1200 iu (30 µg)**
Nutritional InformationIngredients: rTG (re-esterified triglyceride) EPA & DHA concentrate from wild anchovy fish oil; capsule shell (fish gelatine, emulsifier: vegetable glycerol); organic cold-pressed virgin evening primrose oil; lemon oil; antioxidant: vitamin E; vitamin D3.
Free from• Dairy• Gluten• Lactose• Soya• Yeast
• Non-GMO• Halal certified• Kosher
*75% of reference intake ** 600% of reference intake
Pharmepa® RESTORE & MAINTAIN™Key product benefits
80-90% concentrated oils = highly efficient absorption
Therapeutic doses achievable in as little as 2 small capsules
rTG for unprecedented bioavailability and fastest increase in cellular omega-3 levels
Small capsules for split dosing to achieve optimum absorption
Sustainable wild anchovy source
Lemon oil infused for reduced fishy reflux (currently MAINTAIN only)
GMP, pharmaceutical grade and toxin free certification
Independently batch tested – meets highest stability and quality levels
Currently being used in major clinical trials (for Cancer Research)
Zero contraindications!
The role of omega-3 in clinical nutrition
EPA and DHA – what, when and how much?
• Our requirements change throughout our life stages
• DHA is primarily a structural component of cell membranes
• Vital for the growth and development of the brain, central nervous system and eye, throughout pregnancy and early infancy
• DHA becomes important again in later life, particularly in conditions affecting brain and CNS structure
• EPA is the main anti-inflammatory and functional fat
• Oily fish consumption throughout life supports optimal EPA and DHA levels in healthy individuals
Herein lies the problem…
Today less than 40% of the population eat the recommended amount of oily fish
The latest EU recommendations support minimum intake of 500mg of omega-3 EPA and DHA daily (split approx. 50/50)
BUT much more is needed for all clinical conditions associated with omega-3
- the American Heart Association dietary guidelines recommend 900 mg per day for those with coronary heart disease
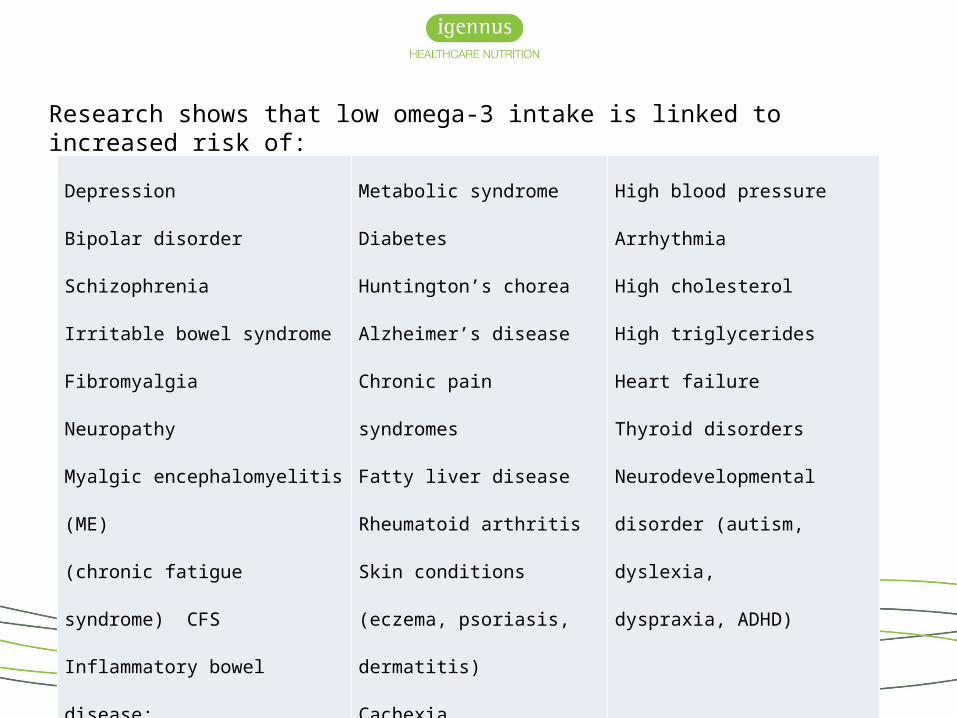
Research shows that low omega-3 intake is linked to increased risk of:
Depression
Bipolar disorder
Schizophrenia
Irritable bowel syndrome
Fibromyalgia
Neuropathy
Myalgic encephalomyelitis (ME)
(chronic fatigue syndrome) CFS
Inflammatory bowel disease:
(Crohn’s disease, ulcerative colitis)
Metabolic syndrome
Diabetes
Huntington’s chorea
Alzheimer’s disease
Chronic pain syndromes
Fatty liver disease
Rheumatoid arthritis
Skin conditions (eczema,
psoriasis, dermatitis)
Cachexia
High blood pressure
Arrhythmia
High cholesterol
High triglycerides
Heart failure
Thyroid disorders
Neurodevelopmental disorder
(autism, dyslexia,
dyspraxia, ADHD)
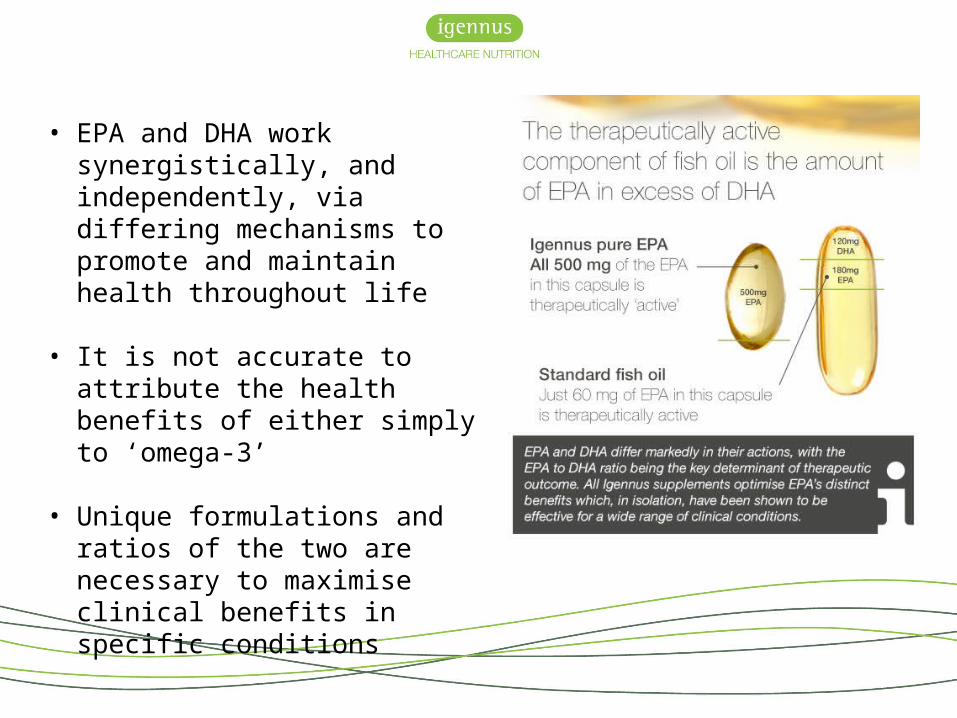
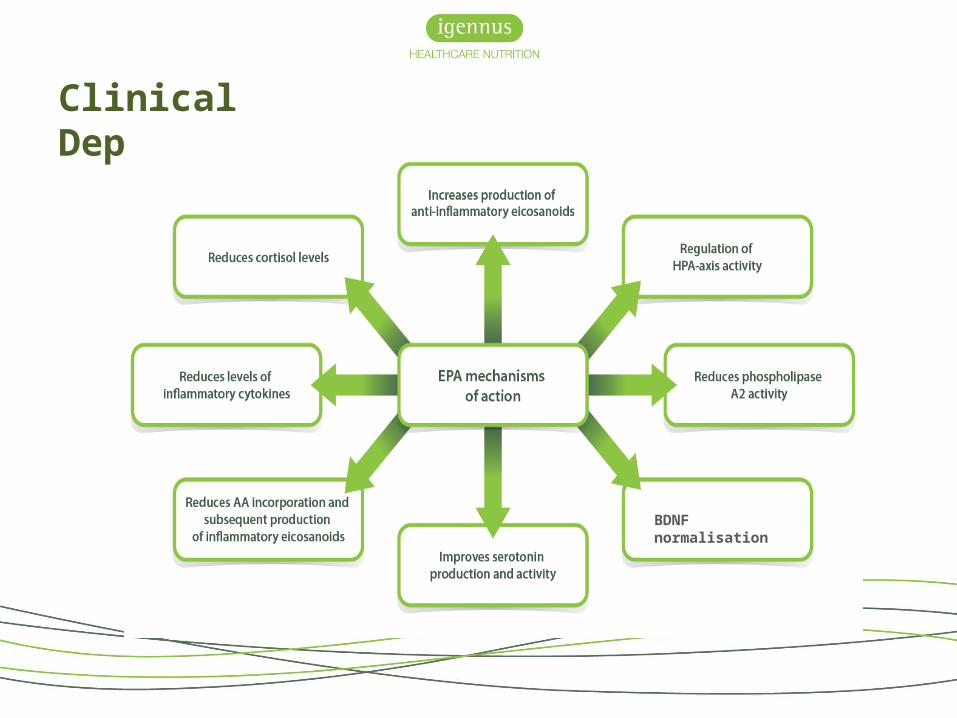
• EPA and DHA work synergistically, and independently, via differing mechanisms to promote and maintain health throughout life
• It is not accurate to attribute the health benefits of either simply to ‘omega-3’
• Unique formulations and ratios of the two are necessary to maximise clinical benefits in specific conditions
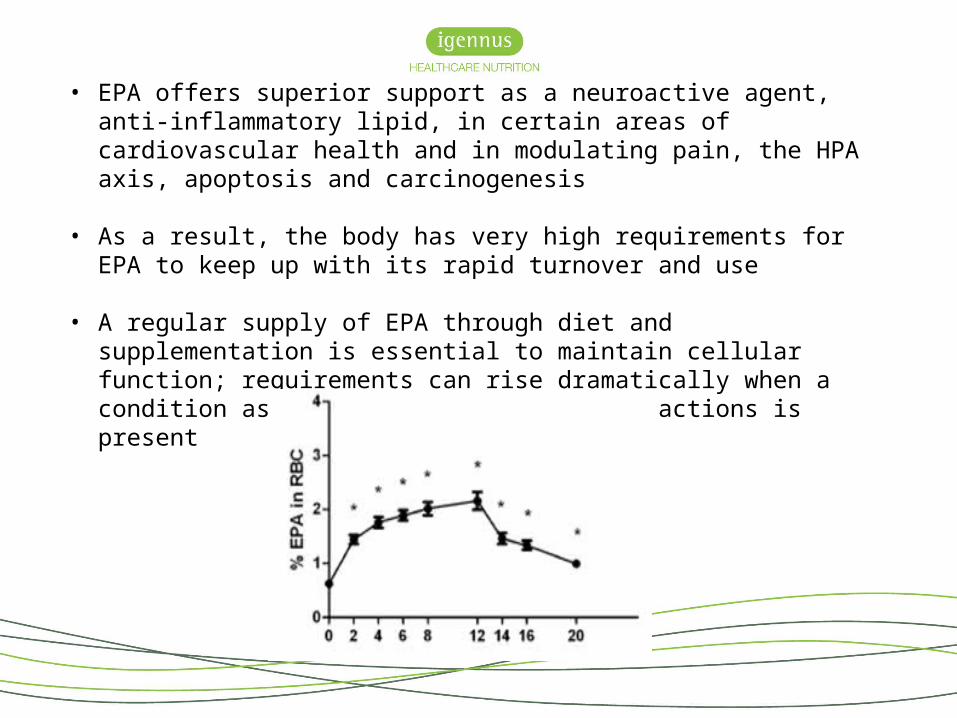
• EPA offers superior support as a neuroactive agent, anti-inflammatory lipid, in certain areas of cardiovascular health and in modulating pain, the HPA axis, apoptosis and carcinogenesis
• As a result, the body has very high requirements for EPA to keep up with its rapid turnover and use
• A regular supply of EPA through diet and supplementation is essential to maintain
cellular function; requirements can rise dramatically when a condition associated with one of EPA’s actions is present
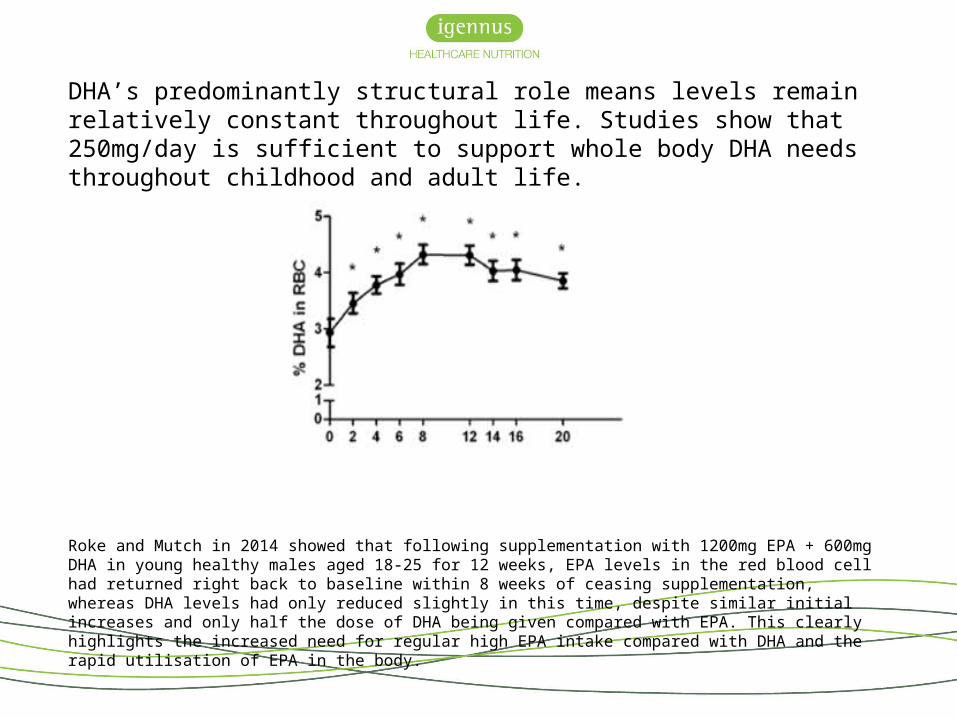
DHA’s predominantly structural role means levels remain relatively constant throughout life. Studies show that 250mg/day is sufficient to support whole body DHA needs throughout childhood and adult life.
Roke and Mutch in 2014 showed that following supplementation with 1200mg EPA + 600mg DHA in young healthy males aged 18-25 for 12 weeks, EPA levels in the red blood cell had returned right back to baseline within 8 weeks of ceasing supplementation, whereas DHA levels had only reduced slightly in this time, despite similar initial increases and only half the dose of DHA being given compared with EPA. This clearly highlights the increased need for regular high EPA intake compared with DHA and the rapid utilisation of EPA in the body.
EPA preserves DHA levels
Optimal EPA intake throughout life helps protect DHA levels
– As DHA’s direct precursor, any excess EPA can be used by the body to ‘make’ DHA therefore keeping levels topped up as necessary
– EPA reduces the activity of the Phospholipase A2 enzyme responsible for ‘releasing’ DHA from cell membranes – maintaining optimal EPA therefore reduces the rate at which DHA is lost and preserves cell membrane DHA levels

DHA levels are tightly regulated – too much is just as bad as not enough
• DHA levels in the cell membrane must be tightly regulated to ensure the correct fluidity is maintained
• Cell membranes too rich in DHA becomes too fluid, also affecting cell function
• When cellular DHA levels are optimal delta-6-desaturase activity is reduced
• Studies often report no increase in DHA levels with pure EPA supplementation, suggesting more DHA is simply not needed. In some cases high DHA supplementation has been shown to worsen health outcomes
• Consuming high-dose DHA when it is not needed switches off the production of EPA, and also GLA, potentially worsening any EPA deficiency and reducing production of the anti-inflammatory omega-6 GLA
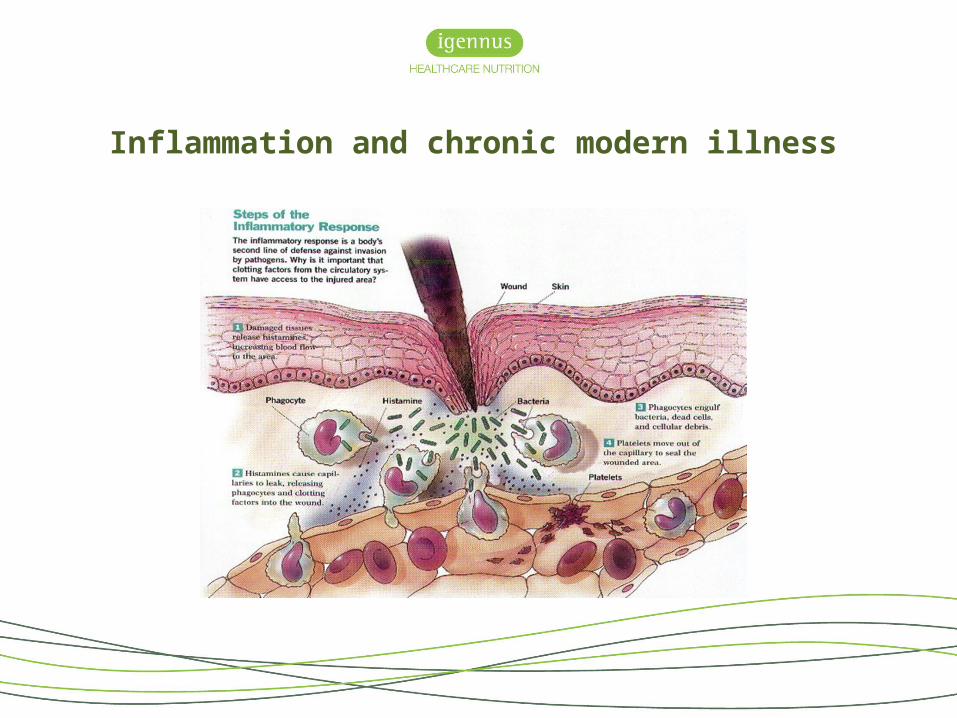
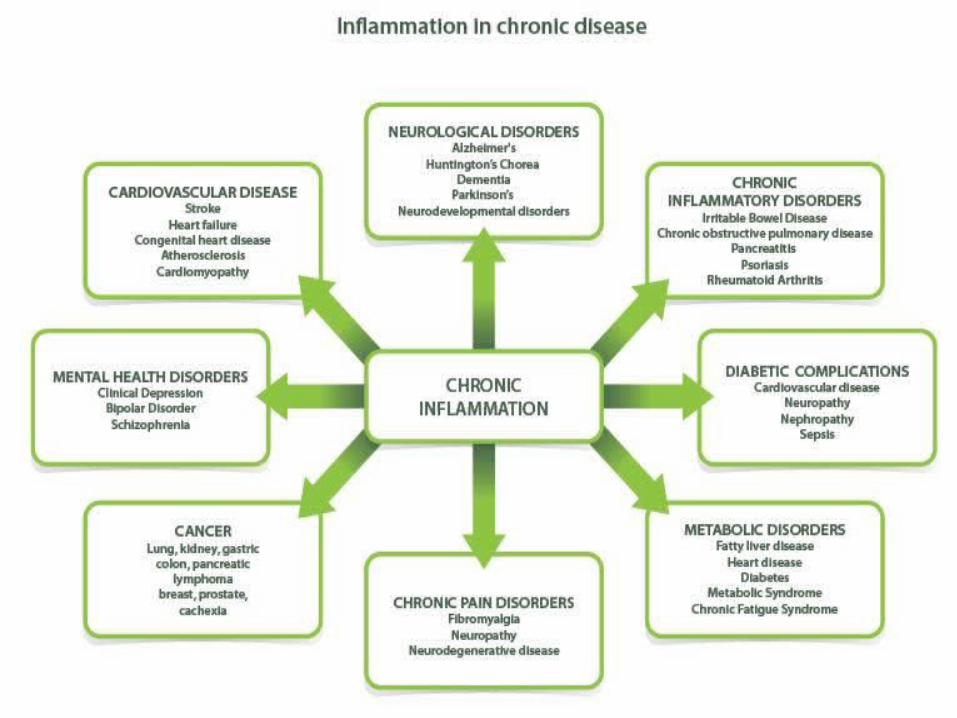
Inflammation and chronic modern illness
What is inflammation?
• The normal response of a tissue to injury
• Triggered by a number of causes including infection, invading pathogens (such as bacteria or viruses), trauma or compromised blood flow
Inflammation
Sympathetic nervous system
HPA-axis Immune system
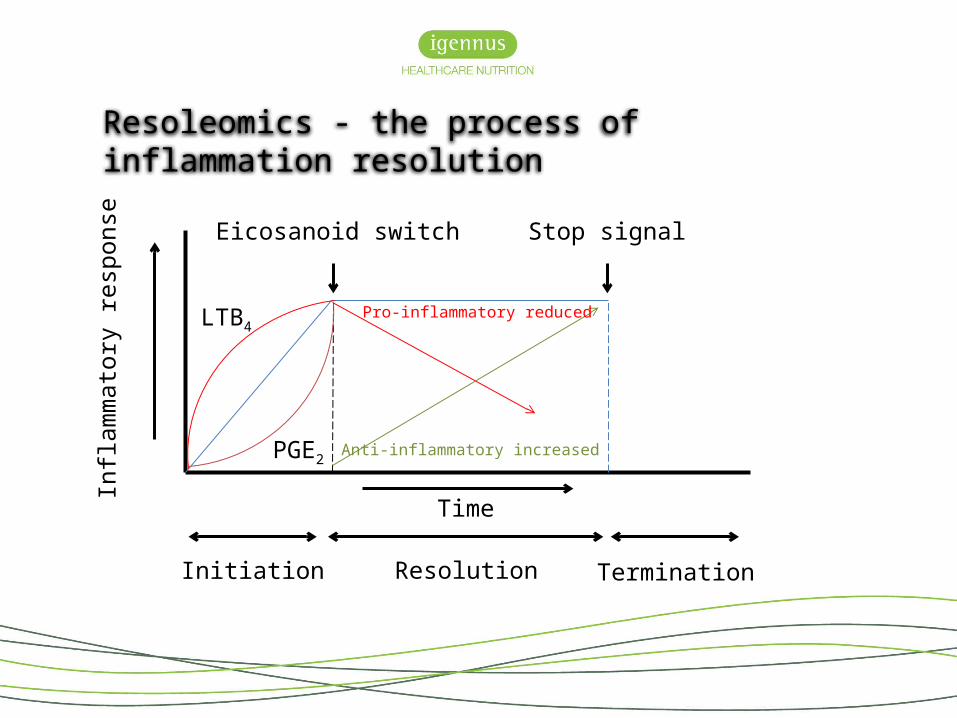
Resoleomics - the process of inflammation resolution In
flam
mat
ory
resp
onse
Initiation Resolution Termination
PGE2
LTB4
Eicosanoid switch Stop signal
Time
Pro-inflammatory reduced
Anti-inflammatory increased
23
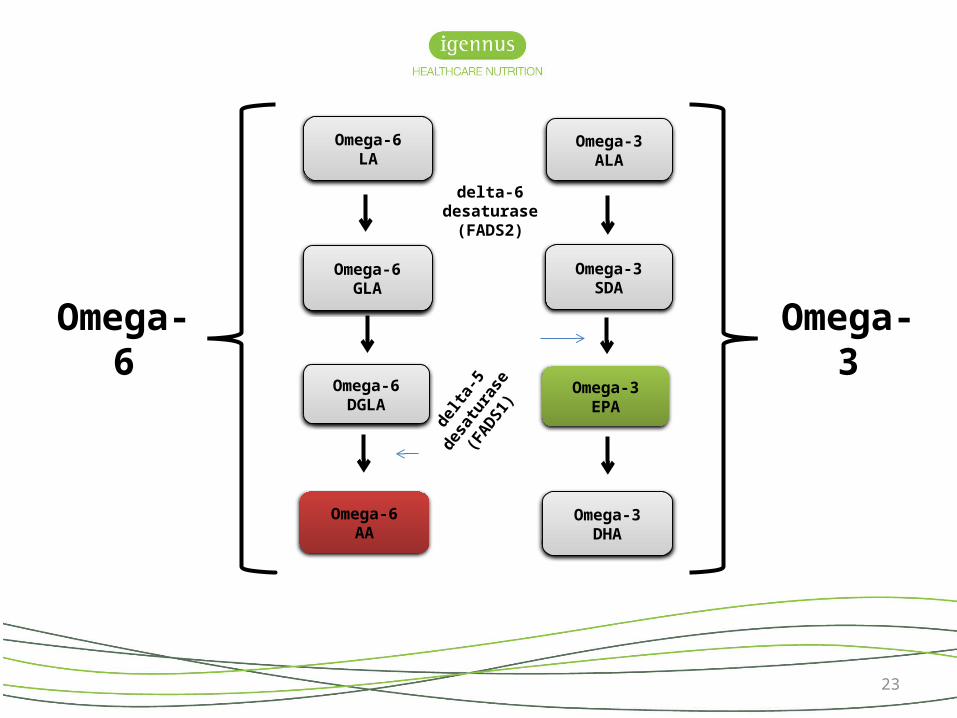
Omega-6LA
Omega-6GLA
Omega-6DGLA
Omega-3ALA
Omega-3EPA
Omega-3SDA
Omega-3DHA
Omega-6AA
delta-6 desaturase(FADS2)
delta
-5 de
satu
rase
(FADS1
)
Omega-6 Omega-3
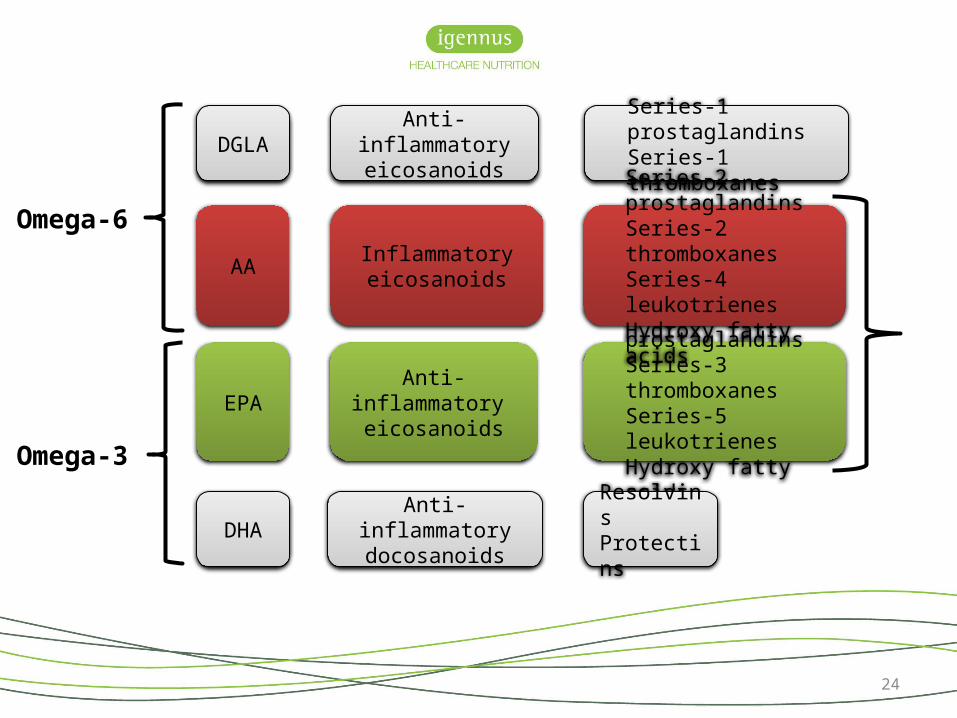
24
Anti-inflammatory eicosanoids
Anti-inflammatory eicosanoids
Anti-inflammatory docosanoids
Inflammatoryeicosanoids
Series-3 prostaglandinsSeries-3 thromboxanesSeries-5 leukotrienesHydroxy fatty acids
Series-1 prostaglandinsSeries-1 thromboxanes
Series-2 prostaglandinsSeries-2 thromboxanesSeries-4 leukotrienesHydroxy fatty acids
Resolvins Protectins
DGLA
EPA
DHA
AA
Omega-6
Omega-3
EPA reduces the pro-inflammatory activity of AA in a number of ways
• EPA is an inhibitor of the enzyme delta-5-desaturase that produces AA
• EPA directly displaces AA from cell membranes
• EPA competes with AA for the enzyme PLA2 necessary to release AA from the membrane phospholipids
• EPA competes with COX and LOX enzymes to prevent the conversion of AA to its eicosanoids
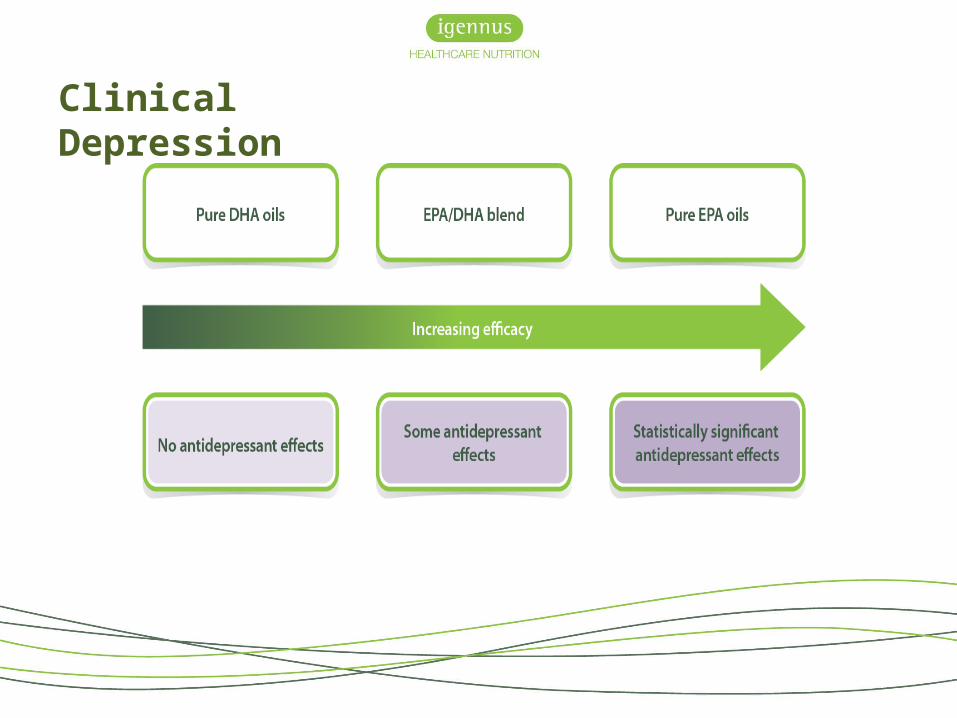
As such, studies show that EPA plus DHA oils are less effective at reducing inflammation than pure EPA oils
Biomarkers for personalised therapeutics
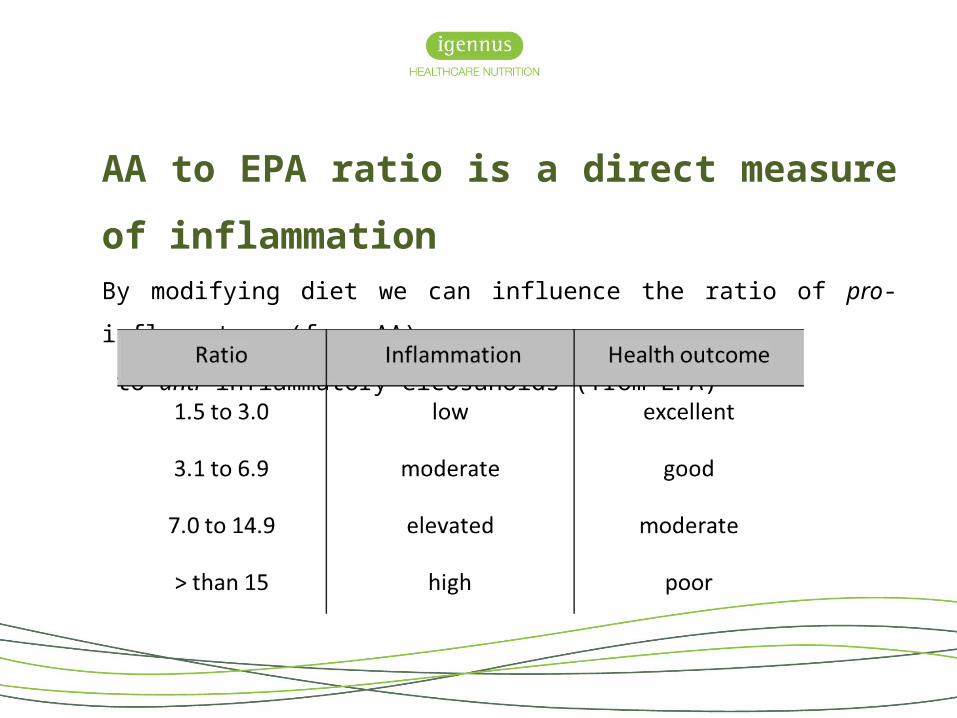
AA to EPA ratio is a direct measure of inflammationBy modifying diet we can influence the ratio of pro-inflammatory (from AA)
to anti-inflammatory eicosanoids (from EPA)
• Depression• Bipolar disorder• Schizophrenia• Myalgic encephalomyelitis• Fibromyalgia• Chronic pain syndromes• Diabetes• Cardiovascular disease• Cancer
• Inflammatory disorders• Inflammatory bowel disease:
(Crohn’s disease, ulcerative colitis)• Neurodevelopmental disorders:
(autism, dyslexia, dyspraxia, ADHD)• Alzheimer’s disease• Huntington’s disease• Skin conditions:
(eczema, psoriasis, dermatitis)
Conditions associated with a high AA to EPA ratio
• As a biomarker, the AA to EPA ratio gives an indication of the inflammatory status
• Diet has the capacity to influence the amount of polyunsaturated fats within our cell membranes, so we also need a structural biomarker
• The omega-3 index = biomarker of intake, but also as risk marker, a risk factor and target for therapy
• Combining the AA to EPA ratio with the omega-3 index gives us a comprehensive overview of health status
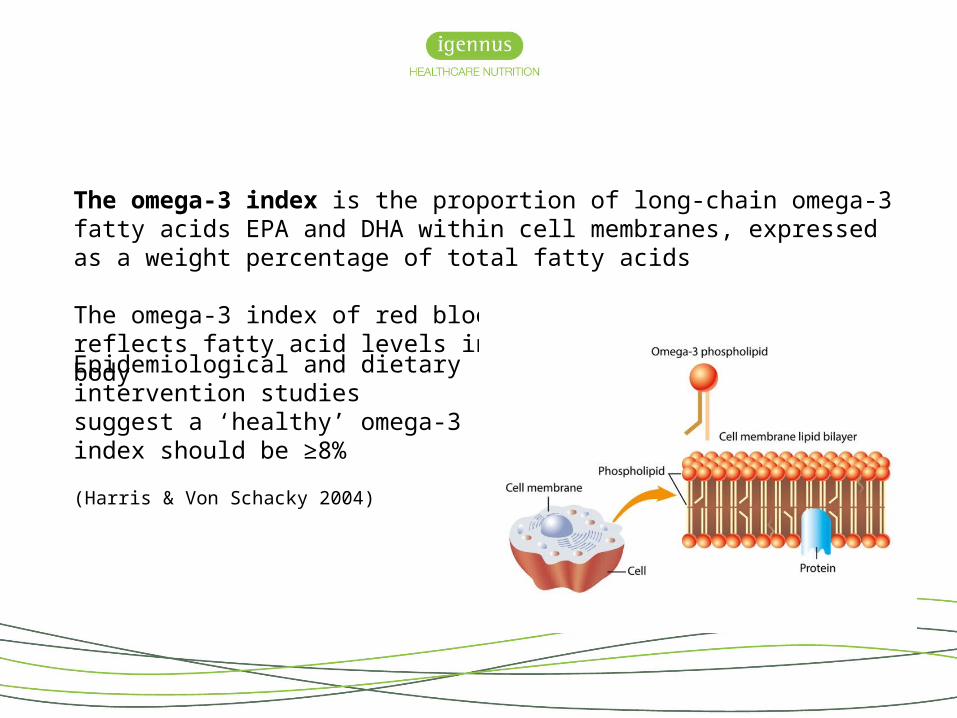
The omega-3 index is the proportion of long-chain omega-3 fatty acids EPA and DHA within cell membranes, expressed as a weight percentage of total fatty acids
The omega-3 index of red blood cells most accurately reflects fatty acid levels in the body
Epidemiological and dietary intervention studies suggest a ‘healthy’ omega-3 index should be ≥8%
(Harris & Von Schacky 2004)
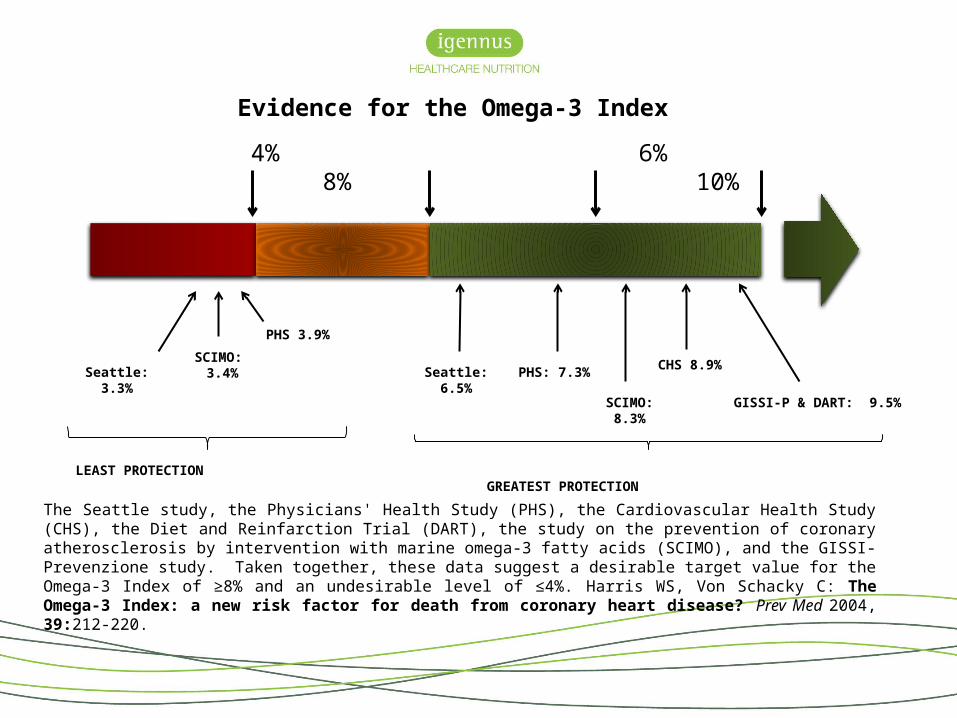
The Seattle study, the Physicians' Health Study (PHS), the Cardiovascular Health Study (CHS), the Diet and Reinfarction Trial (DART), the study on the prevention of coronary atherosclerosis by intervention with marine omega-3 fatty acids (SCIMO), and the GISSI-Prevenzione study. Taken together, these data suggest a desirable target value for the Omega-3 Index of ≥8% and an undesirable level of ≤4%. Harris WS, Von Schacky C: The Omega-3 Index: a new risk factor for death from coronary heart disease? Prev Med 2004, 39:212-220.
4% 6% 8% 10%
GISSI-P & DART: 9.5%
CHS 8.9%
PHS 3.9%
SCIMO: 3.4%Seattle: 3.3%
SCIMO: 8.3%
PHS: 7.3%Seattle: 6.5%
LEAST PROTECTION GREATEST PROTECTION
Evidence for the Omega-3 Index
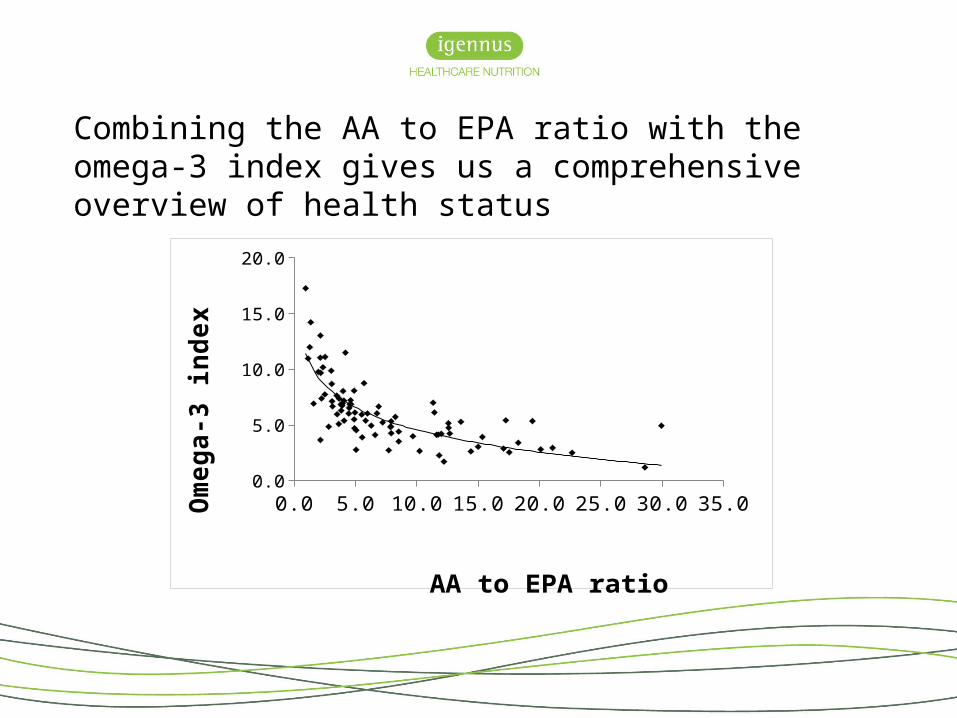
0.0 5.0 10.0 15.0 20.0 25.0 30.0 35.00.02.04.06.08.0
10.012.014.016.018.020.0
AA to EPA ratio
Om
ega-
3 in
dex
Combining the AA to EPA ratio with the omega-3 index gives us a comprehensive overview of health status
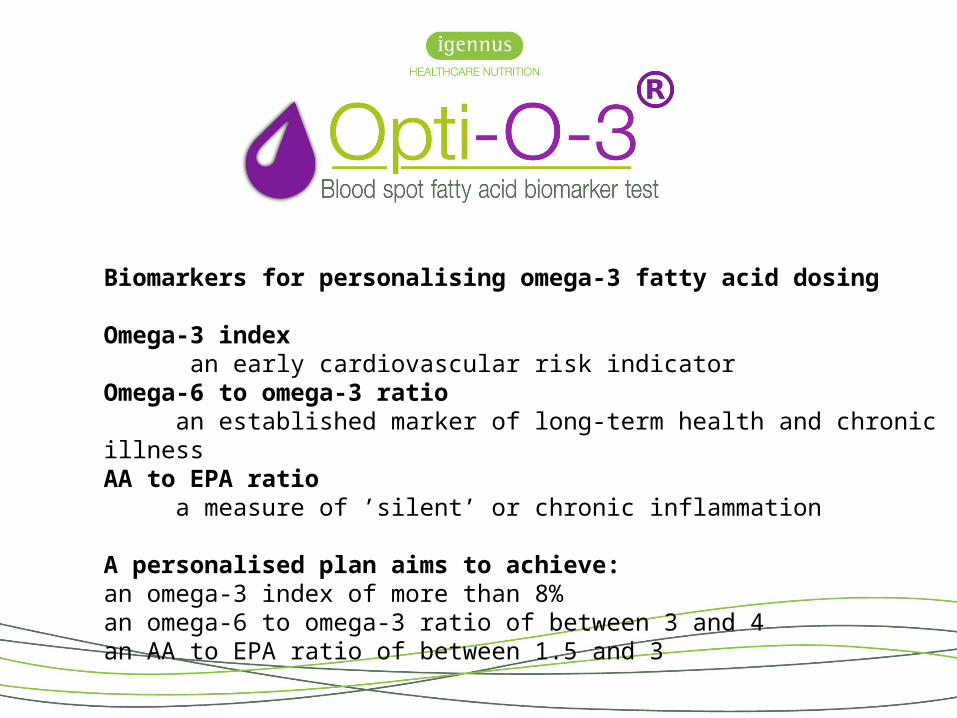
Biomarkers for personalising omega-3 fatty acid dosing
Omega-3 index an early cardiovascular risk indicatorOmega-6 to omega-3 ratio an established marker of long-term health and chronic illnessAA to EPA ratio a measure of ’silent’ or chronic inflammation
A personalised plan aims to achieve:an omega-3 index of more than 8% an omega-6 to omega-3 ratio of between 3 and 4an AA to EPA ratio of between 1.5 and 3
Pharmepa® RESTORE & MAINTAIN™
The fastest, most effective, clinical omega-3
Maximising therapeutic success:
A combination of factors determine omega-3 intervention success:
Dose – must be determined according to participant baseline levels in EPA+DHA body
Strength/concentration of the active ingredient within the total oil volume
Bioavailability of the omega-3 form used
(Von Schacky 2015)
Dose
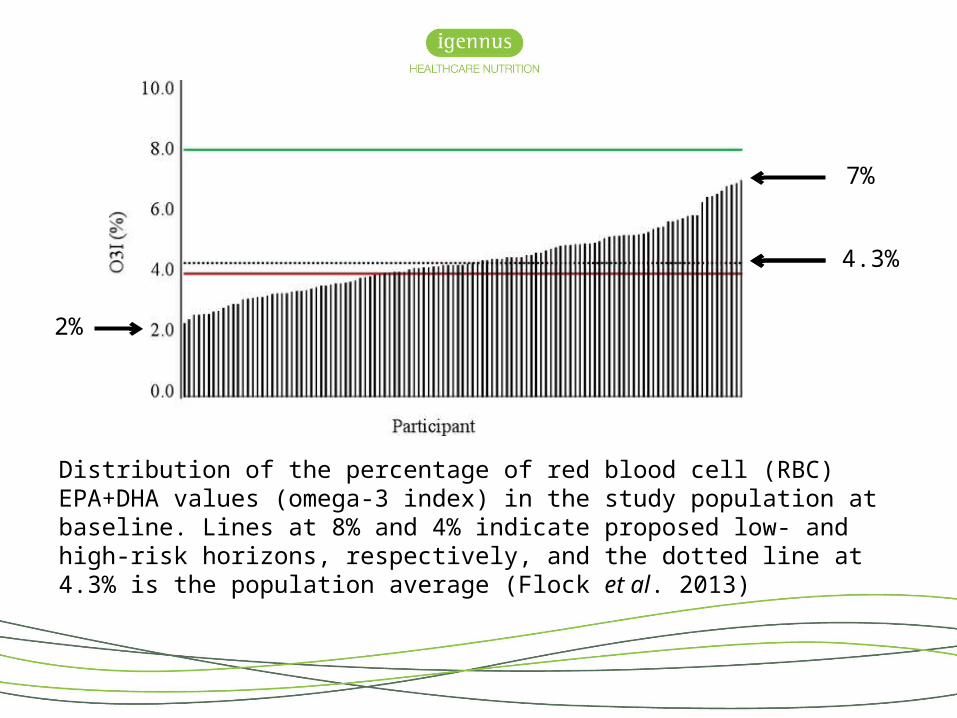
Distribution of the percentage of red blood cell (RBC) EPA+DHA values (omega 3 ‐index) in the study population at baseline. Lines at 8% and 4% indicate proposed low and high risk horizons, respectively, and the dotted line at 4.3% is the ‐ ‐population average (Flock et al. 2013)
7%
2%
4.3%
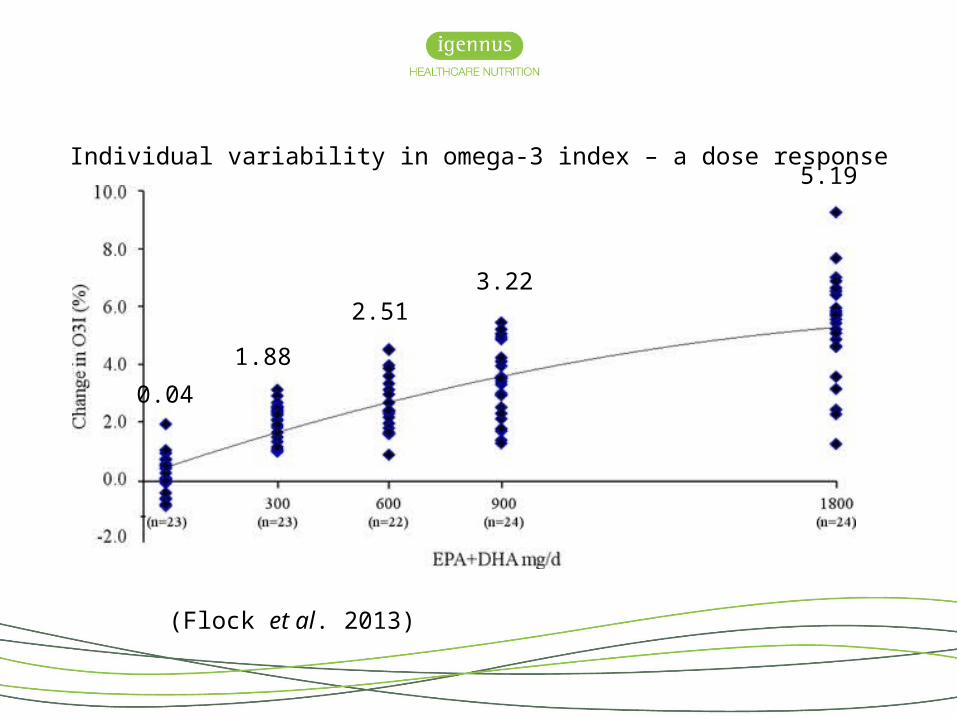
Individual variability in omega-3 index – a dose response
(Flock et al. 2013)
2.51
5.19
3.22
0.04
1.88
Variability was influenced by baseline omega-3 index, age, sex and physical activity
Lower omega-3 index status and older age each predicted greater increases in omega-3 index
Increased physical activity level was associated with a higher omega-3 index
Female subjects had a non-significant increase in omega-3 compared to males
However, body weight was the greatest influencer
(Flock et al., 2013)
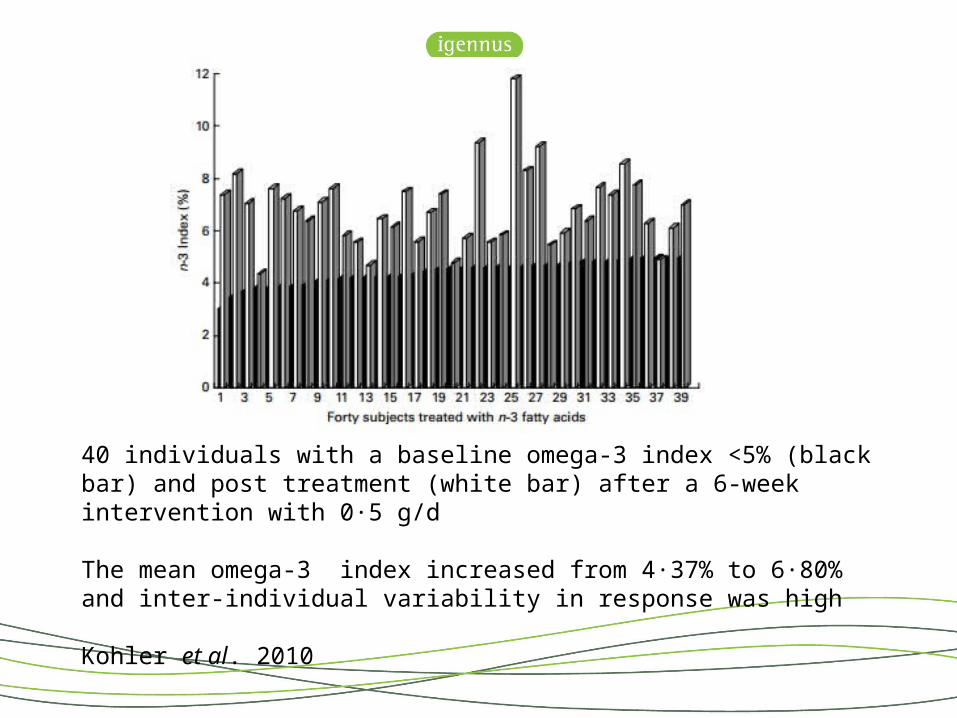
40 individuals with a baseline omega-3 index <5% (black bar) and post treatment (white bar) after a 6-week intervention with 0·5 g/d
The mean omega-3 index increased from 4·37% to 6·80% and inter-individual variability in response was high
Kohler et al. 2010
Concentration
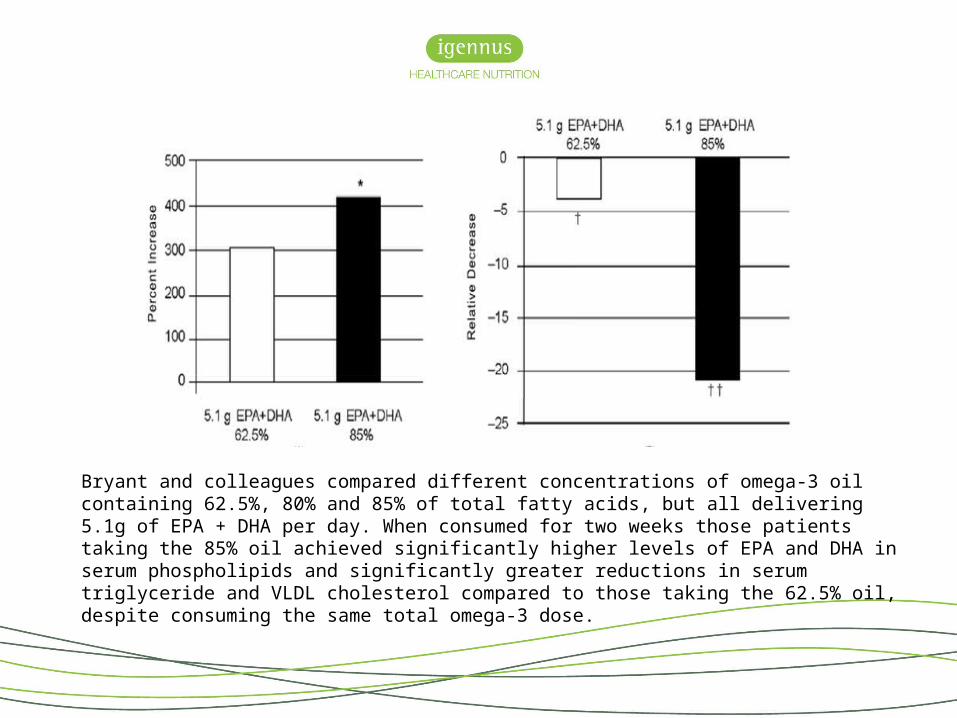
Bryant and colleagues compared different concentrations of omega-3 oil containing 62.5%, 80% and 85% of total fatty acids, but all delivering 5.1g of EPA + DHA per day. When consumed for two weeks those patients taking the 85% oil achieved significantly higher levels of EPA and DHA in serum phospholipids and significantly greater reductions in serum triglyceride and VLDL cholesterol compared to those taking the 62.5% oil, despite consuming the same total omega-3 dose.
Beware of ‘strength’
• Many companies boast ‘double strength’ ‘high strength’ ‘maximum strength’
• But they are actually referring to the dose
• Taking 3 times the volume does not make the oil 3 times the strength
– or 3 x as effective!
Bioavailability
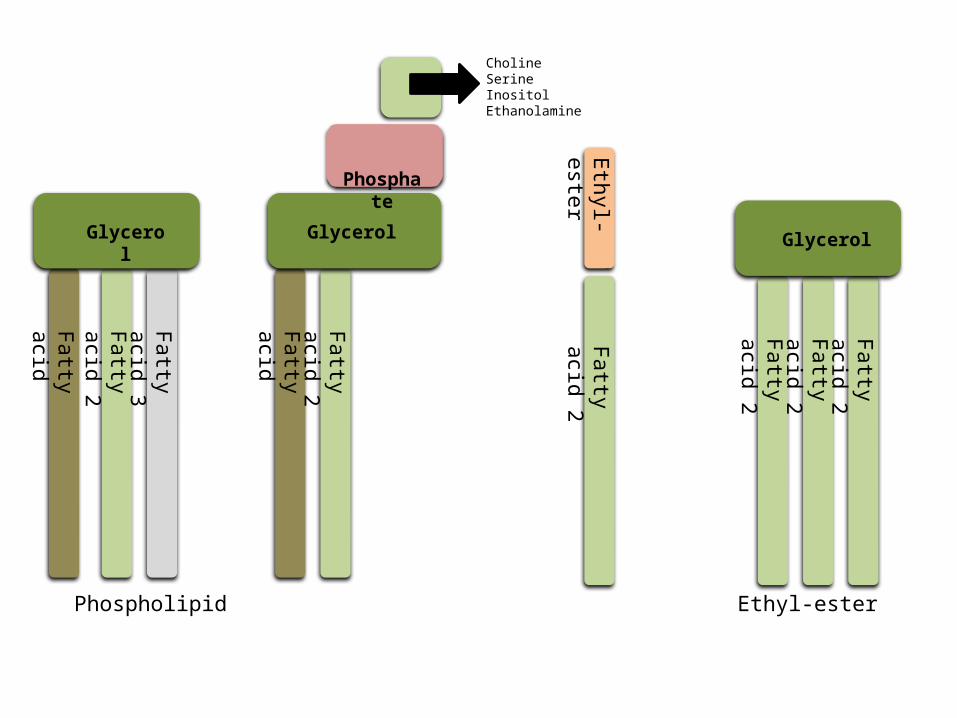
Fatty acid
Fatty acid 2
Phosphate
Glycerol
Ethyl-esterFatt
y acid 2
Fatty acid 2
Fatty acid 2
Fatty acid 2
Glycerol
Fatty acid 2
Fatty acid 3
Glycerol
Triglyceride Phospholipid Ethyl-ester Re-esterified triglyceride
Fatty acid
CholineSerineInositolEthanolamine
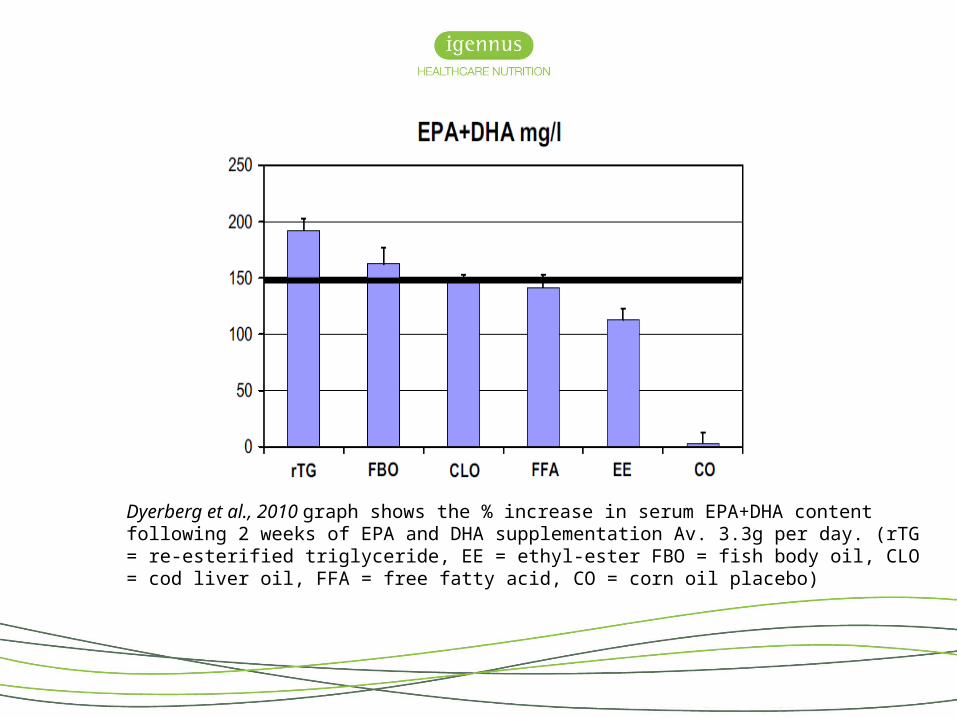
Dyerberg et al., 2010 graph shows the % increase in serum EPA+DHA content following 2 weeks of EPA and DHA supplementation Av. 3.3g per day. (rTG = re-esterified triglyceride, EE = ethyl-ester FBO = fish body oil, CLO = cod liver oil, FFA = free fatty acid, CO = corn oil placebo)
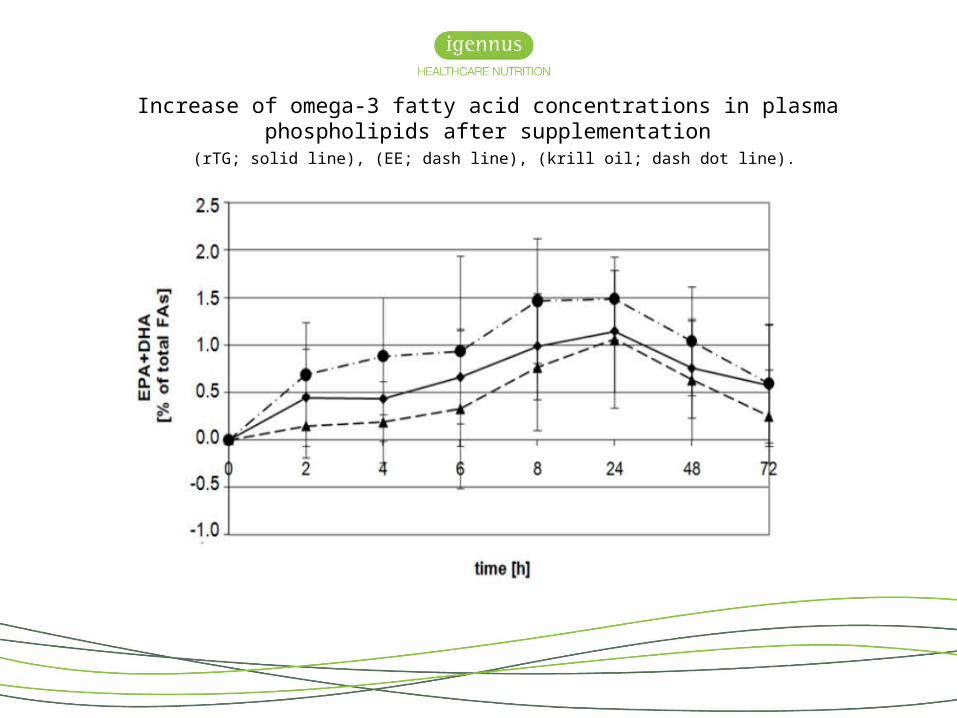
Increase of omega-3 fatty acid concentrations in plasma phospholipids after supplementation (rTG; solid line), (EE; dash line), (krill oil; dash dot line).

Dose + concentration + bioavailability=
benefits
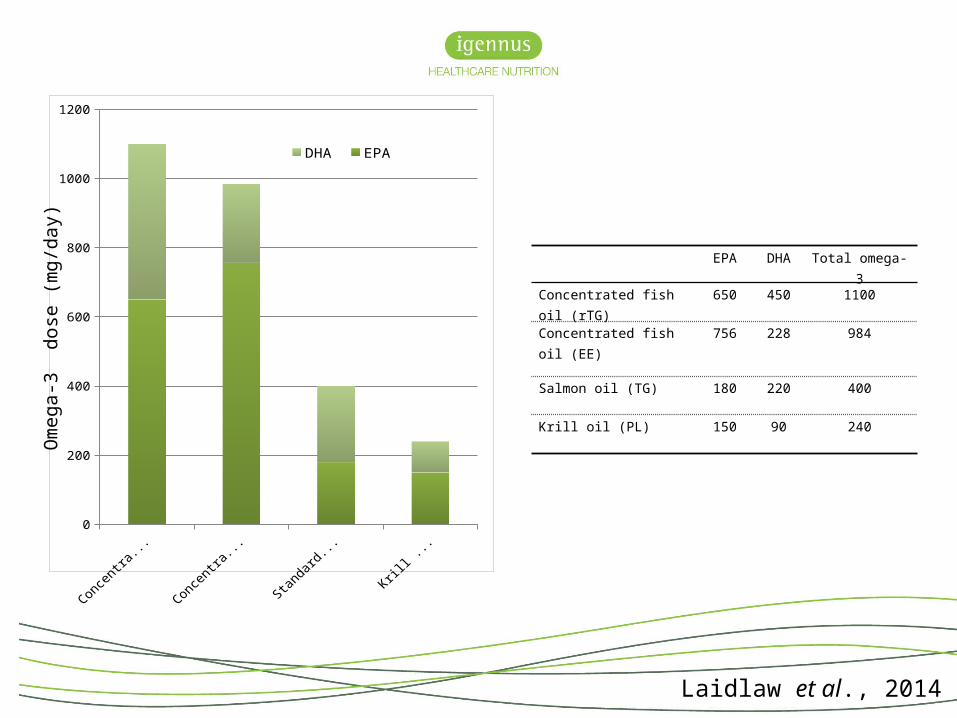
Concentrated fish oil (rTG)
Concentrated fish oil (EE)
Standard fish oil (TG)
Krill oil (PL) 0
200
400
600
800
1000
1200
DHA EPA
Om
ega-
3 d
ose
(mg/
day)
EPA DHA Total omega-3
Concentrated fish oil (rTG) 650 450 1100
Concentrated fish oil (EE) 756 228 984
Salmon oil (TG) 180 220 400
Krill oil (PL) 150 90 240
Laidlaw et al., 2014
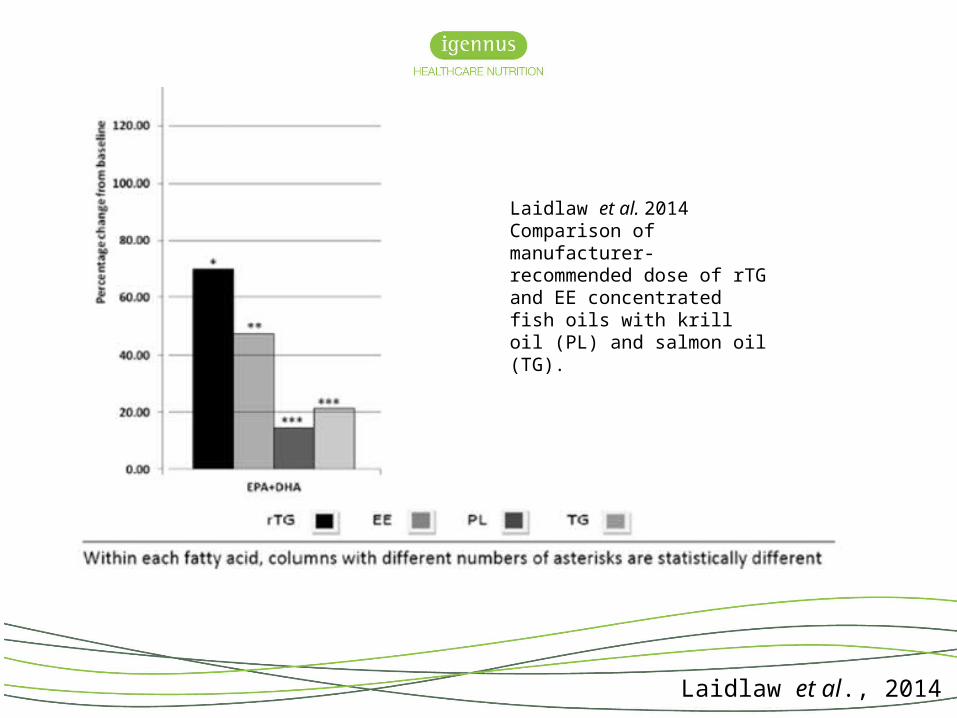
Laidlaw et al., 2014
Laidlaw et al. 2014 Comparison of manufacturer-recommended dose of rTG and EE concentrated fish oils with krill oil (PL) and salmon oil (TG).
• To raise the omega-3 index from 5.2 to 10 requires an omega-3 dose of 21.2mg/kg/day
• A 70kg individual would therefore require a daily omega-3 dose of 1.48g
• 3 capsules RESTORE provides 500mg omega-3 per capsule at a daily cost of £1.50 (£45/month = £270 for full treatment phase)
• 28 capsules MegaRed provides 52.5mg omega-3 per capsule at a daily cost of around £10 (£300/month = £1800 for full treatment phase)
Manipulating Pharmepa® RESTORE & MAINTAIN™
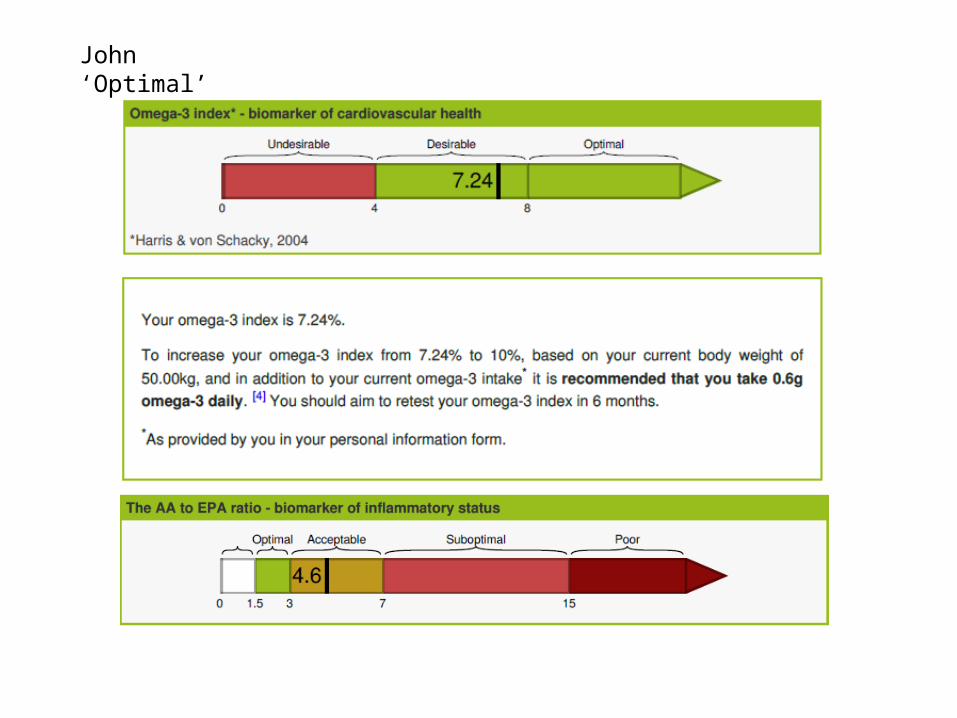
John ‘Optimal’
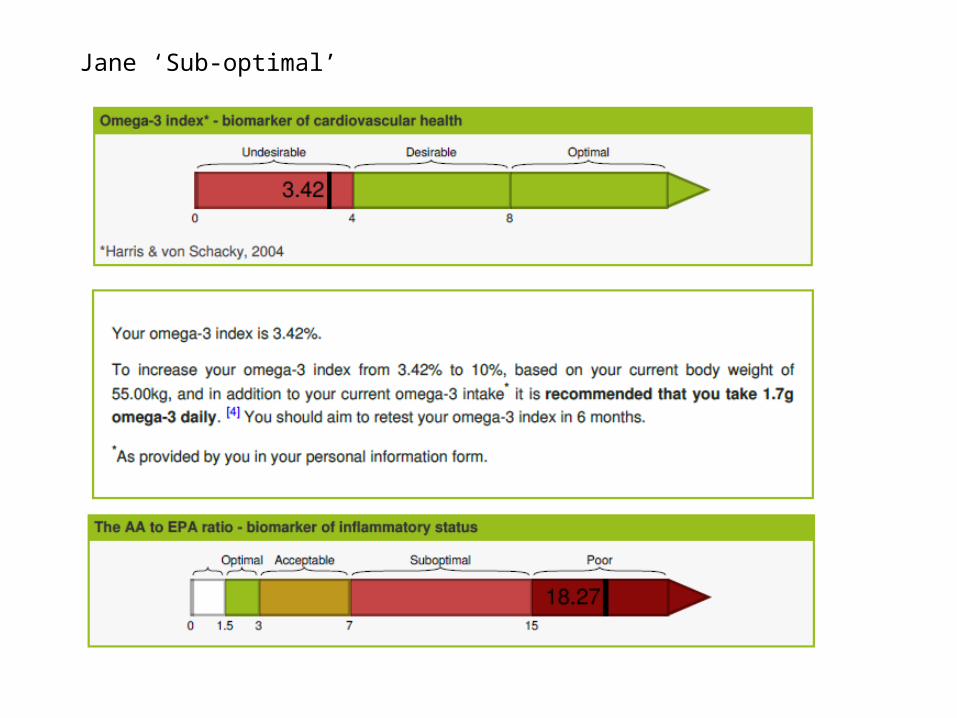
Jane ‘Sub-optimal’


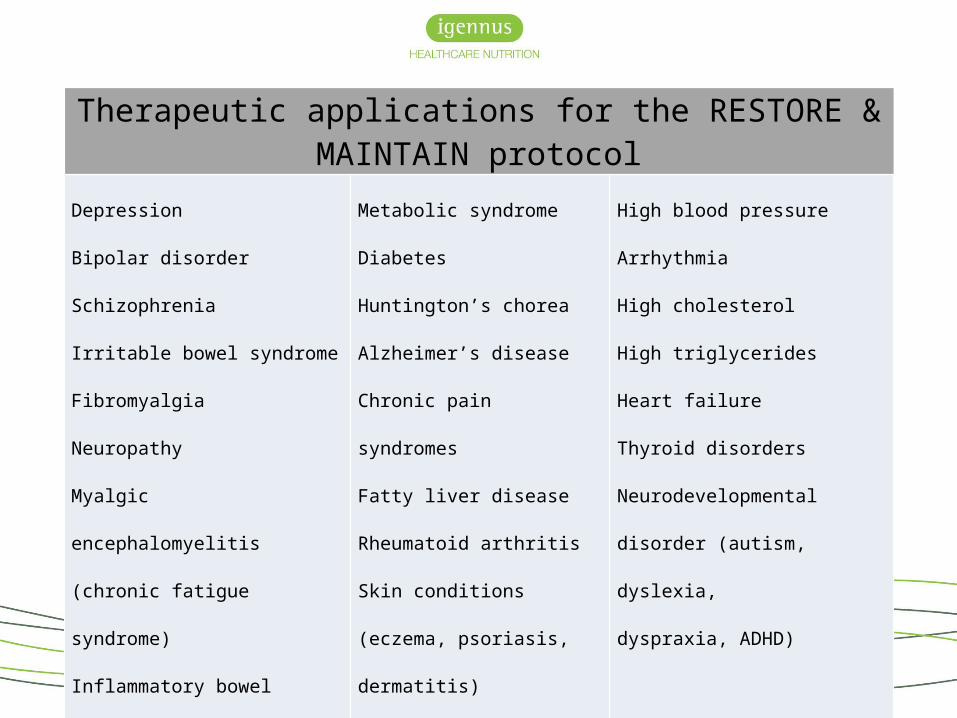
Therapeutic applications for the RESTORE & MAINTAIN protocol
Depression
Bipolar disorder
Schizophrenia
Irritable bowel syndrome
Fibromyalgia
Neuropathy
Myalgic encephalomyelitis
(chronic fatigue syndrome)
Inflammatory bowel disease:
(Crohn’s disease, ulcerative colitis)
Metabolic syndrome
Diabetes
Huntington’s chorea
Alzheimer’s disease
Chronic pain syndromes
Fatty liver disease
Rheumatoid arthritis
Skin conditions (eczema,
psoriasis, dermatitis)
Cachexia
High blood pressure
Arrhythmia
High cholesterol
High triglycerides
Heart failure
Thyroid disorders
Neurodevelopmental disorder
(autism, dyslexia,
dyspraxia, ADHD)
http://igennus.com/professionals/reference-materials/
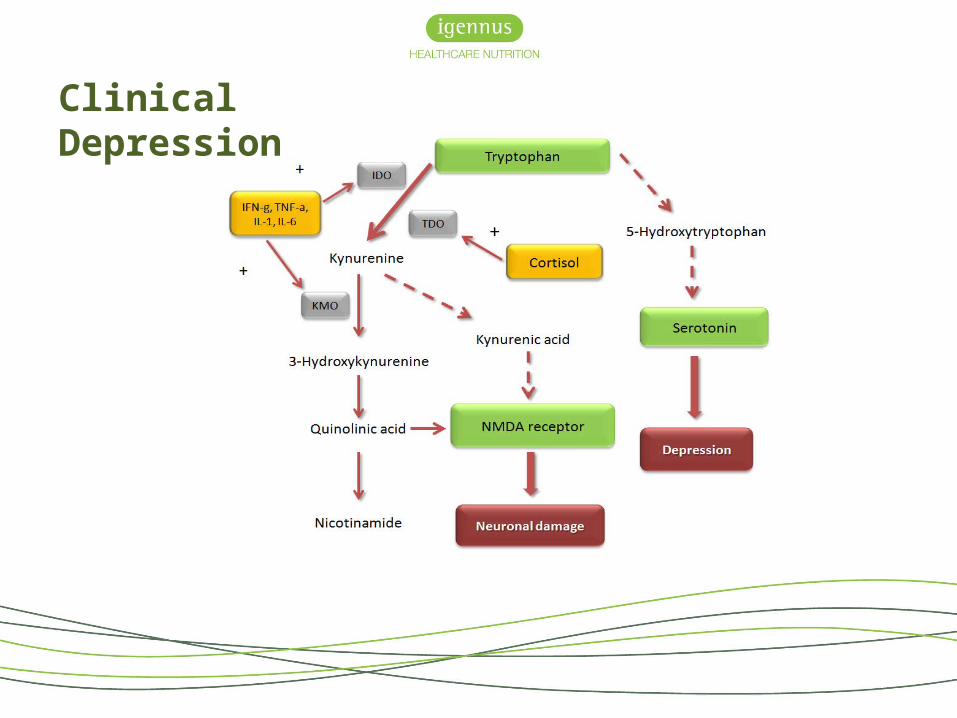
Clinical Depression
Clinical Depression
BDNF normalisation
Clinical Depression
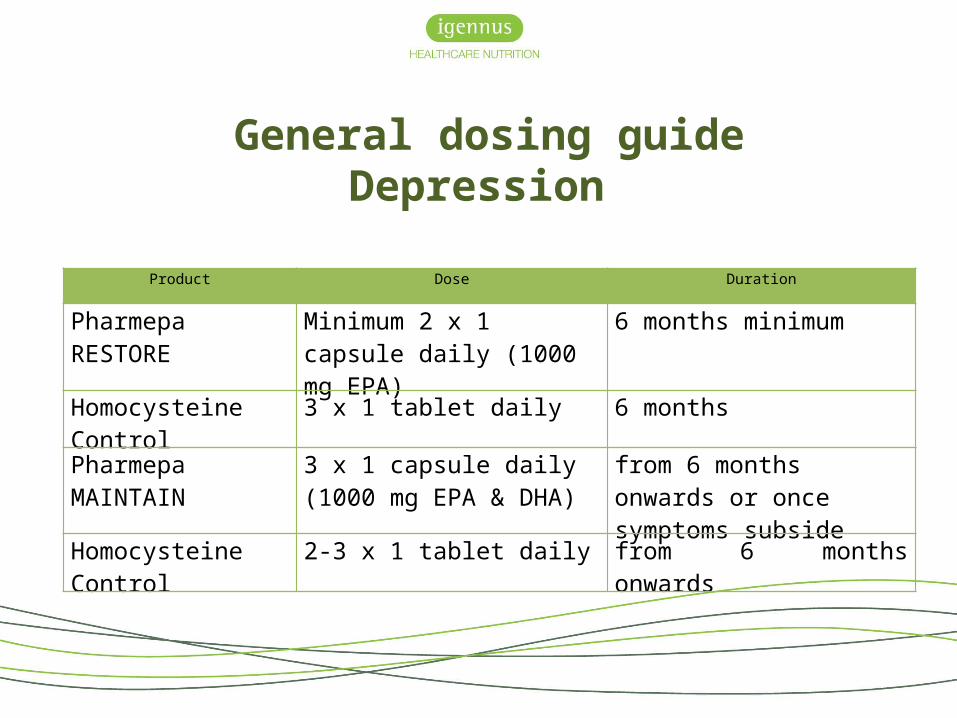
General dosing guideDepression
Product Dose Duration
Pharmepa RESTORE Minimum 2 x 1 capsule daily (1000 mg EPA)
6 months minimum
Homocysteine Control 3 x 1 tablet daily 6 monthsPharmepa MAINTAIN 3 x 1 capsule daily (1000 mg
EPA & DHA)from 6 months onwards or once symptoms subside
Homocysteine Control 2-3 x 1 tablet daily from 6 months onwards
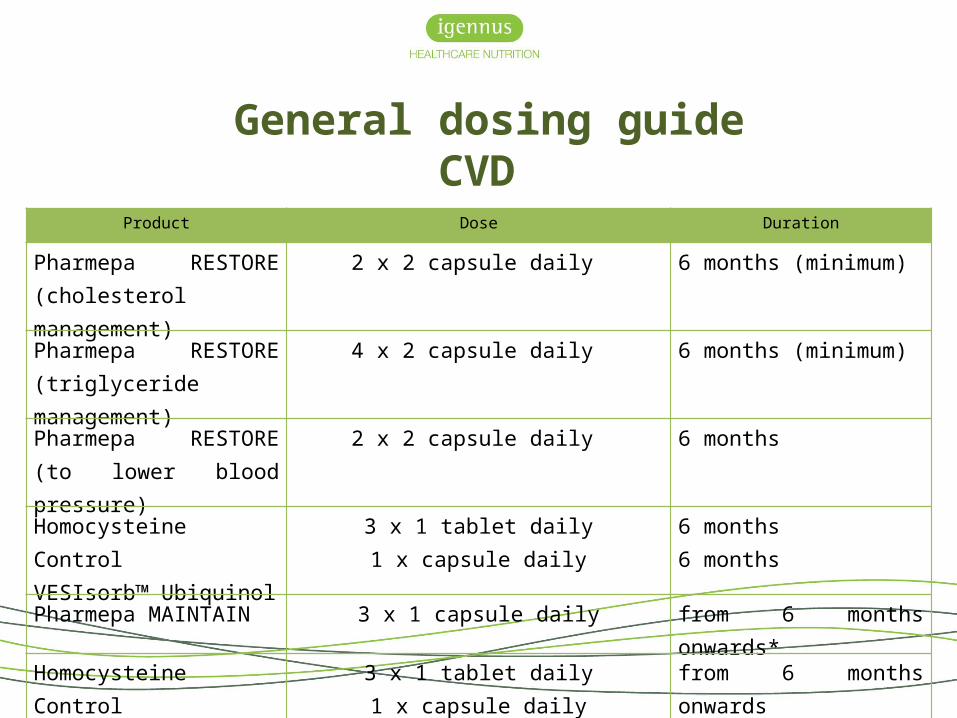
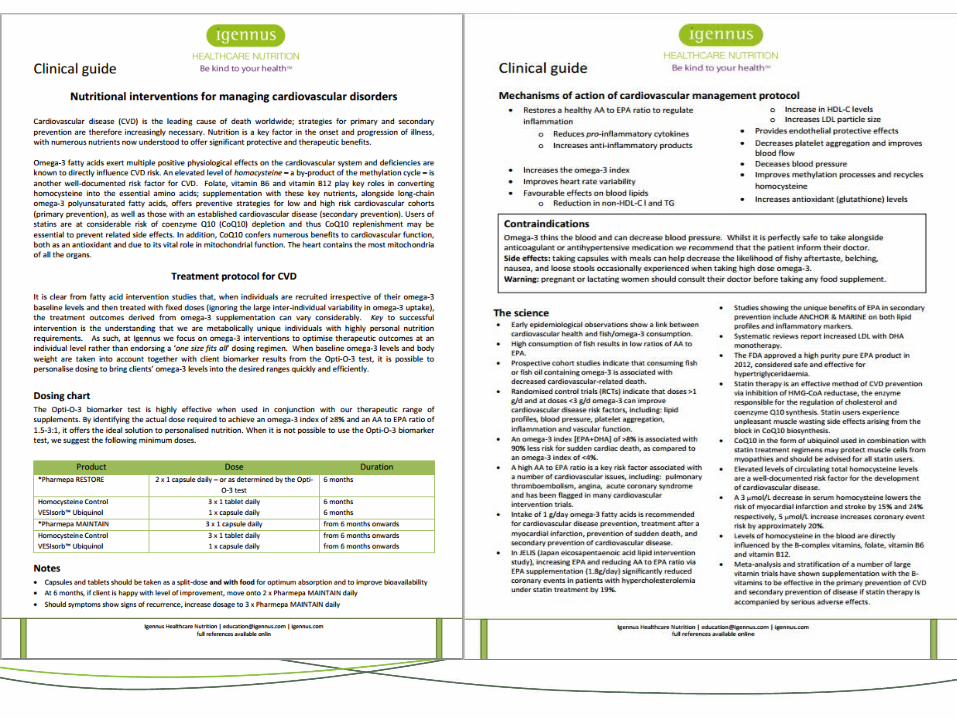
General dosing guideCVD
Product Dose Duration
Pharmepa RESTORE (cholesterol management)
2 x 2 capsule daily 6 months (minimum)
Pharmepa RESTORE (triglyceride management)
4 x 2 capsule daily 6 months (minimum)
Pharmepa RESTORE (to lower blood pressure)
2 x 2 capsule daily 6 months
Homocysteine Control VESIsorb™ Ubiquinol
3 x 1 tablet daily1 x capsule daily
6 months6 months
Pharmepa MAINTAIN 3 x 1 capsule daily from 6 months onwards*Homocysteine Control VESIsorb™ Ubiquinol
3 x 1 tablet daily1 x capsule daily
from 6 months onwardsfrom 6 months onwards
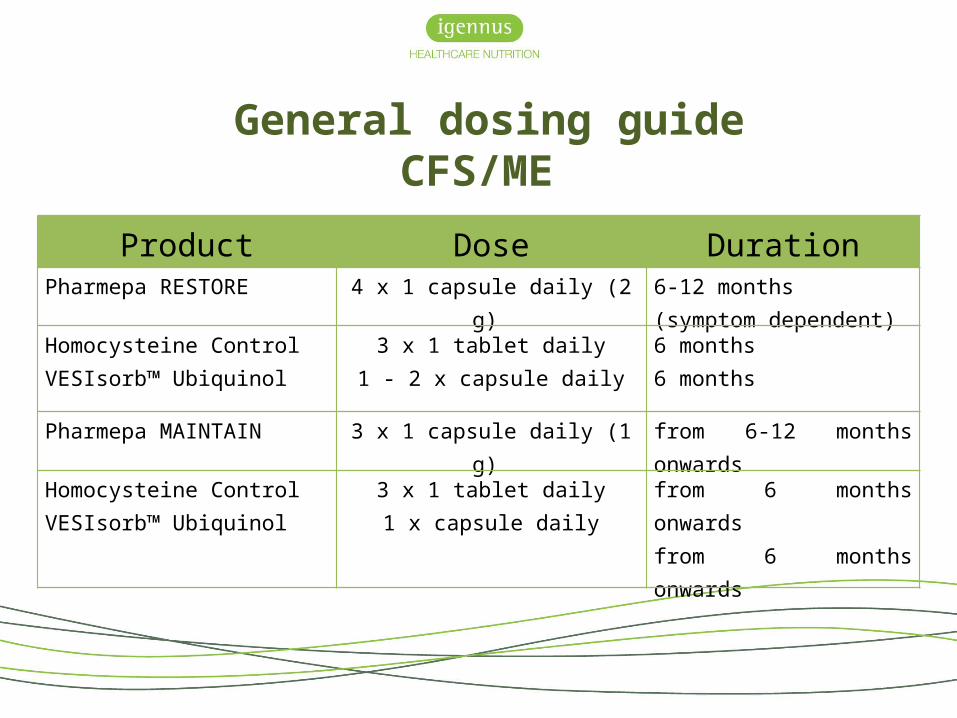
General dosing guideCFS/ME
Product Dose DurationPharmepa RESTORE 4 x 1 capsule daily (2 g) 6-12 months
(symptom dependent)
Homocysteine Control VESIsorb™ Ubiquinol
3 x 1 tablet daily1 - 2 x capsule daily
6 months6 months
Pharmepa MAINTAIN 3 x 1 capsule daily (1 g) from 6-12 months onwards
Homocysteine Control VESIsorb™ Ubiquinol
3 x 1 tablet daily1 x capsule daily
from 6 months onwardsfrom 6 months onwards
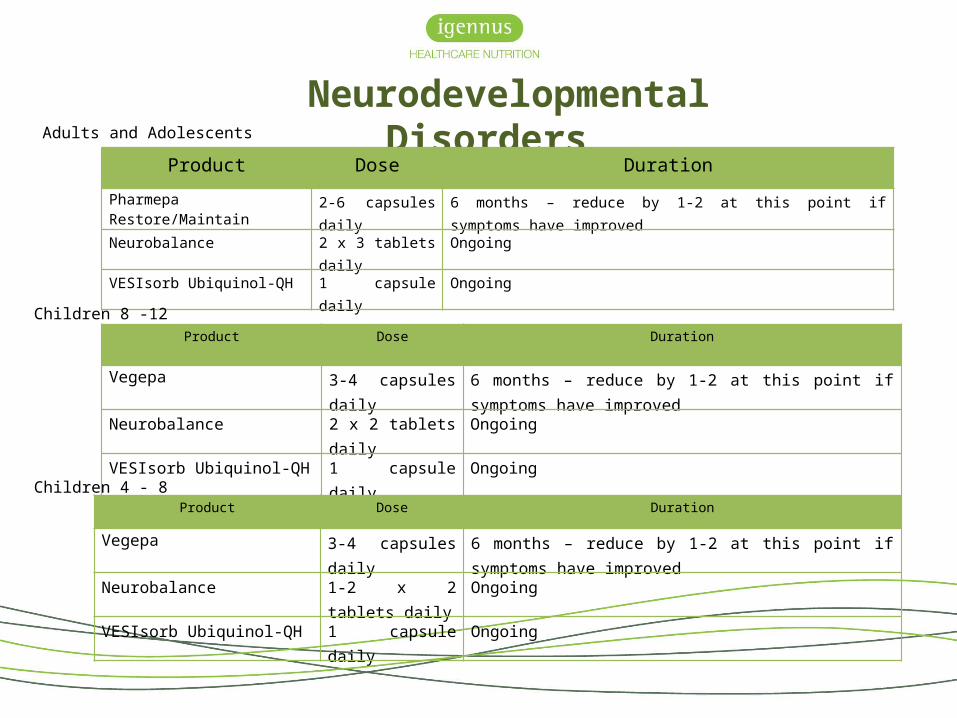
Neurodevelopmental Disorders
Product Dose Duration
Pharmepa Restore/Maintain 2-6 capsules daily 6 months – reduce by 1-2 at this point if symptoms have improved
Neurobalance 2 x 3 tablets daily Ongoing
VESIsorb Ubiquinol-QH 1 capsule daily Ongoing
Product Dose Duration
Vegepa 3-4 capsules daily 6 months – reduce by 1-2 at this point if symptoms have improved
Neurobalance 2 x 2 tablets daily Ongoing
VESIsorb Ubiquinol-QH 1 capsule daily Ongoing
Product Dose Duration
Vegepa 3-4 capsules daily 6 months – reduce by 1-2 at this point if symptoms have improved
Neurobalance 1-2 x 2 tablets daily OngoingVESIsorb Ubiquinol-QH 1 capsule daily Ongoing
Adults and Adolescents
Children 8 -12
Children 4 - 8

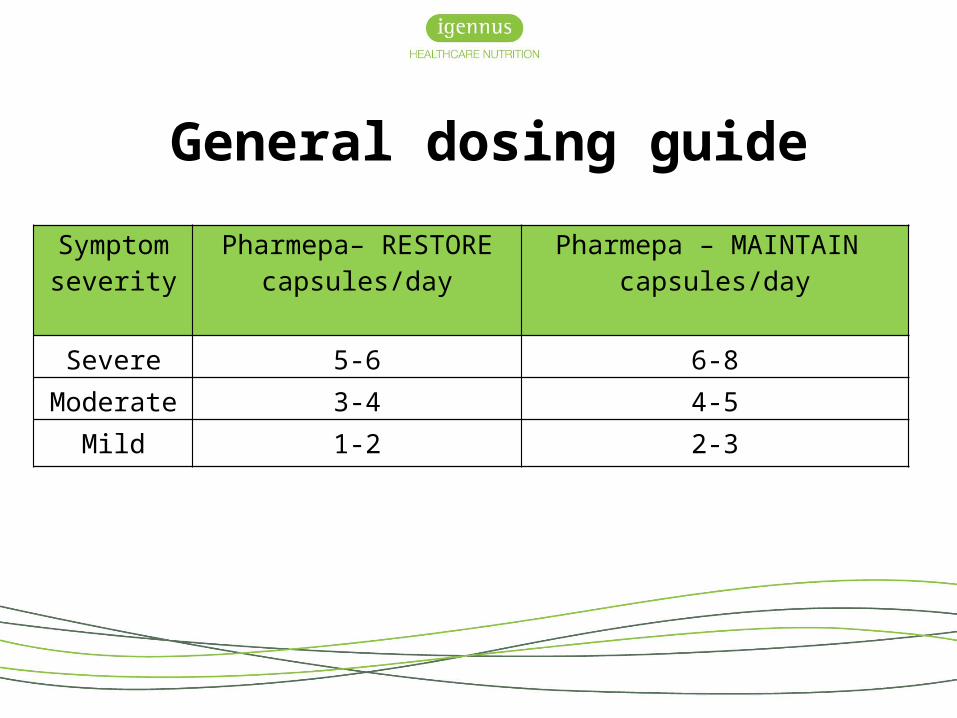
Symptom severity
Pharmepa– RESTOREcapsules/day
Pharmepa – MAINTAIN capsules/day
Severe 5-6 6-8Moderate 3-4 4-5
Mild 1-2 2-3
General dosing guide
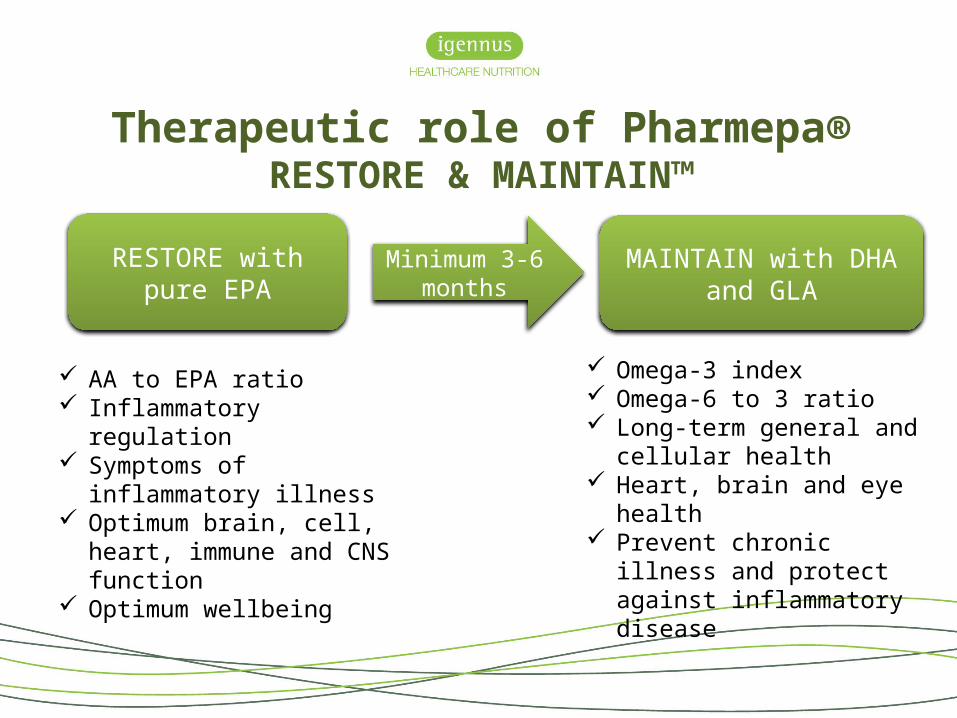
RESTORE with pure EPA
MAINTAIN with DHA and GLA
Minimum 3-6 months
Therapeutic role of Pharmepa®RESTORE & MAINTAIN™
AA to EPA ratio Inflammatory regulation Symptoms of inflammatory
illness Optimum brain, cell, heart,
immune and CNS function Optimum wellbeing
Omega-3 index Omega-6 to 3 ratio Long-term general and
cellular health Heart, brain and eye health Prevent chronic illness and
protect against inflammatory disease
RESTORE & MAINTAIN™
AA to EPA ratio omega-3 index
omega-6 to 3 ratio
Pharmepa RESTORE provides ultra-pure, highly concentrated and preformed omega-3 isolate to restore and replenish deficiencies that may have occurred through the inadequate in-vivo production of EPA or through inadequate intake from common dietary sources
Pharmepa MAINTAIN helps to maintain long-term cellular and total body health by maintaining optimal eicosanoid balance, regulation of inflammatory mediators, optimal cell structure and a healthy omega-6 to 3 ratio
• Igennus is the only independent manufacturer of specialist Fatty Acid in the UK. Based in Cambridge the medical innovation hub for the UK:
- Seven Seas Merck Pharma Germany- Minami Atrium Pharma Canada- Biocare Elder Pharma India- Eskimo 3 Bringwell Pharma Sweden- Equizen Vifor Pharma Swiss
Resources and reading
http://igennus.com/nutrition/omega-3-science/
http://igennus.com/professionals/
http://www.dhaomega3.org/Overview/DHA-+-EPA-for-Other-Health-Benefits-and-Chronic-Disorders
http://www.efsa.europa.eu/en/search.htm?search=EPA&text=EPA
