the late preterm infant family and community medicine grand rounds april 11, 2012 nicole j. urrea,...
TRANSCRIPT
The Late Preterm Infant
Family and Community Medicine Grand Rounds
April 11, 2012
Nicole J. Urrea, M.D.Heather Pratt-Chavez, M.D.
Objectives1. Discuss recent trends in late
preterm births
2. Explain the risk of infant morbidity in the late preterm infant and common complications in this population
3. Discuss the impact of late preterm birth on childhood outcomes
Late Preterm Infants
•Define late preterm infant (LPI) GA. Why do we need a special name for this group?
•Epidemiology
•Etiology
Late Preterm Infants•Morbidity and mortality in NB
period (first 2-4 weeks of life)
•Apnea
•Respiratory distress
•Poor feeding - dehydration
•Hyperbilirubinemia
•Hypoglycemia – hypothermia
•Sepsis - SBI
Case: Baby Hunter27 y.o. G2P1 at 35 0/7 weeks gestation with
severe pre-eclampsia -
Will my baby be OK?
When can I take him home?
Why does he have to stay in the hospital?
Definition•34 0/7 to 36 6/7 weeks gestation
•2005 workshop, Eunice Kennedy Shriver National Institute of Child Health and Human Development
•2007 report by AAP Committee on Fetus and the Newborn
•What happened to draw this attention?
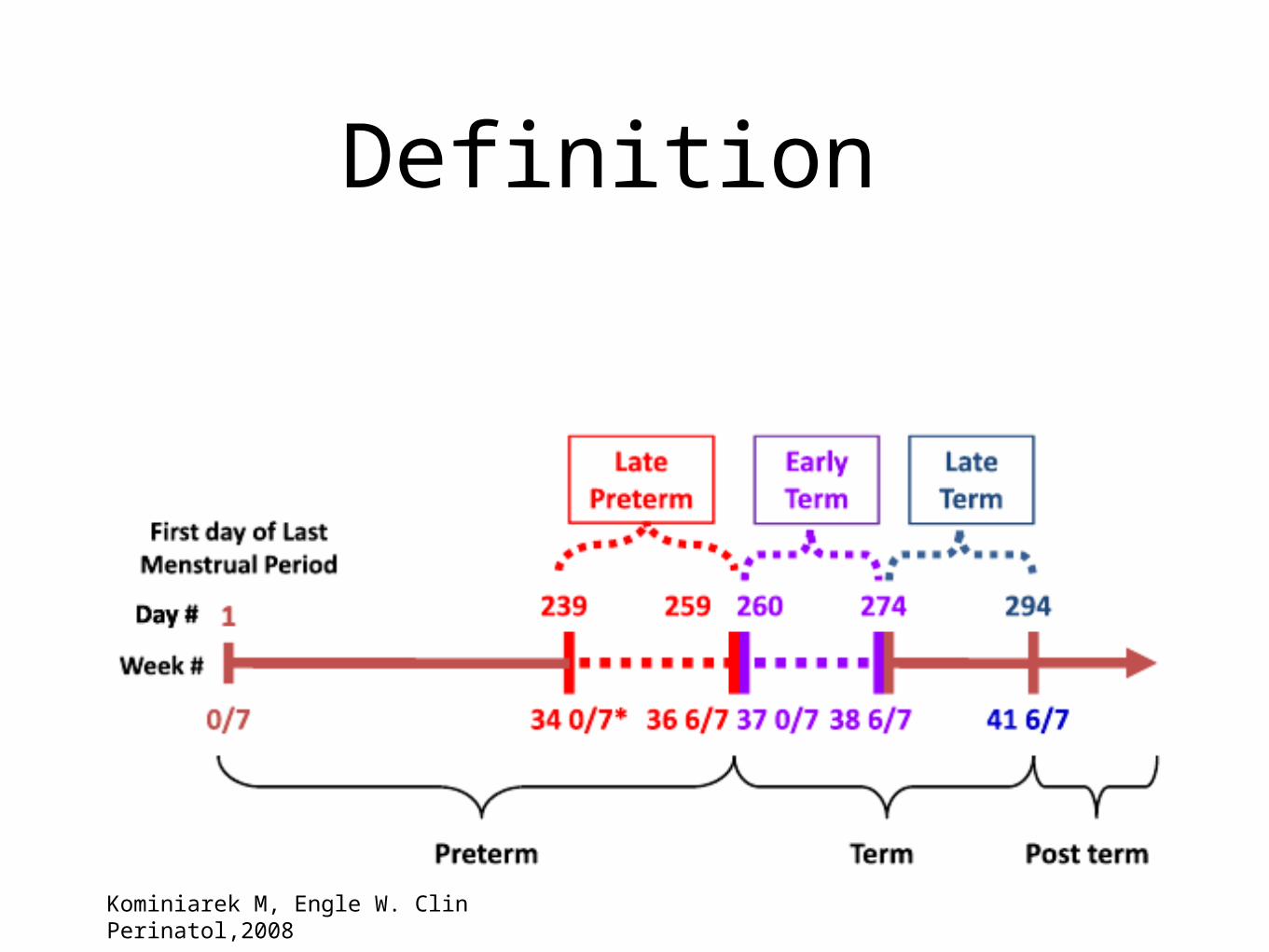
Definition
Kominiarek M, Engle W. Clin Perinatol,2008
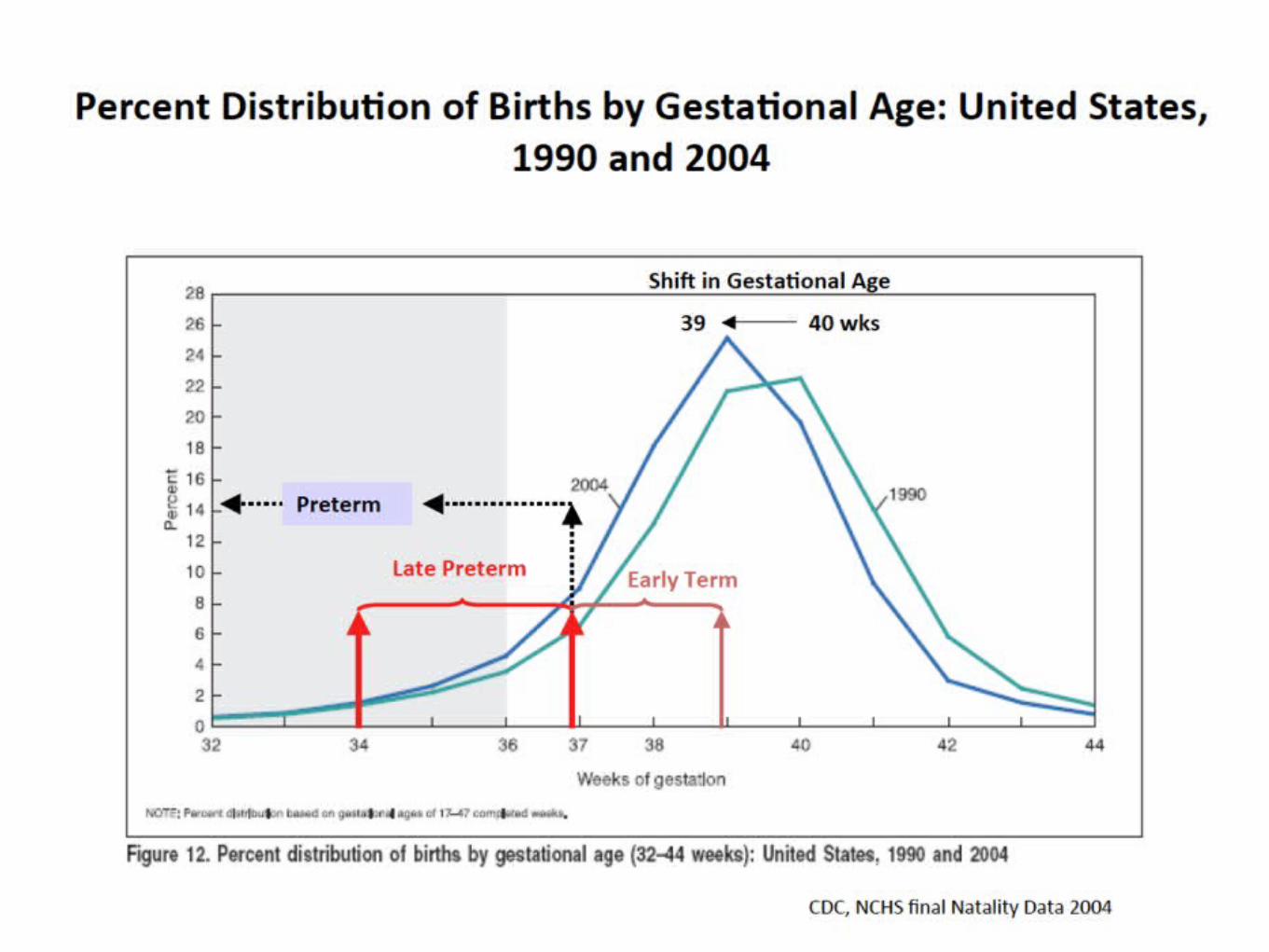


Why the shift?• Increased surveillance - improved ultrasound
technology, (increased form 68.1%-85.4% 1989-2003)
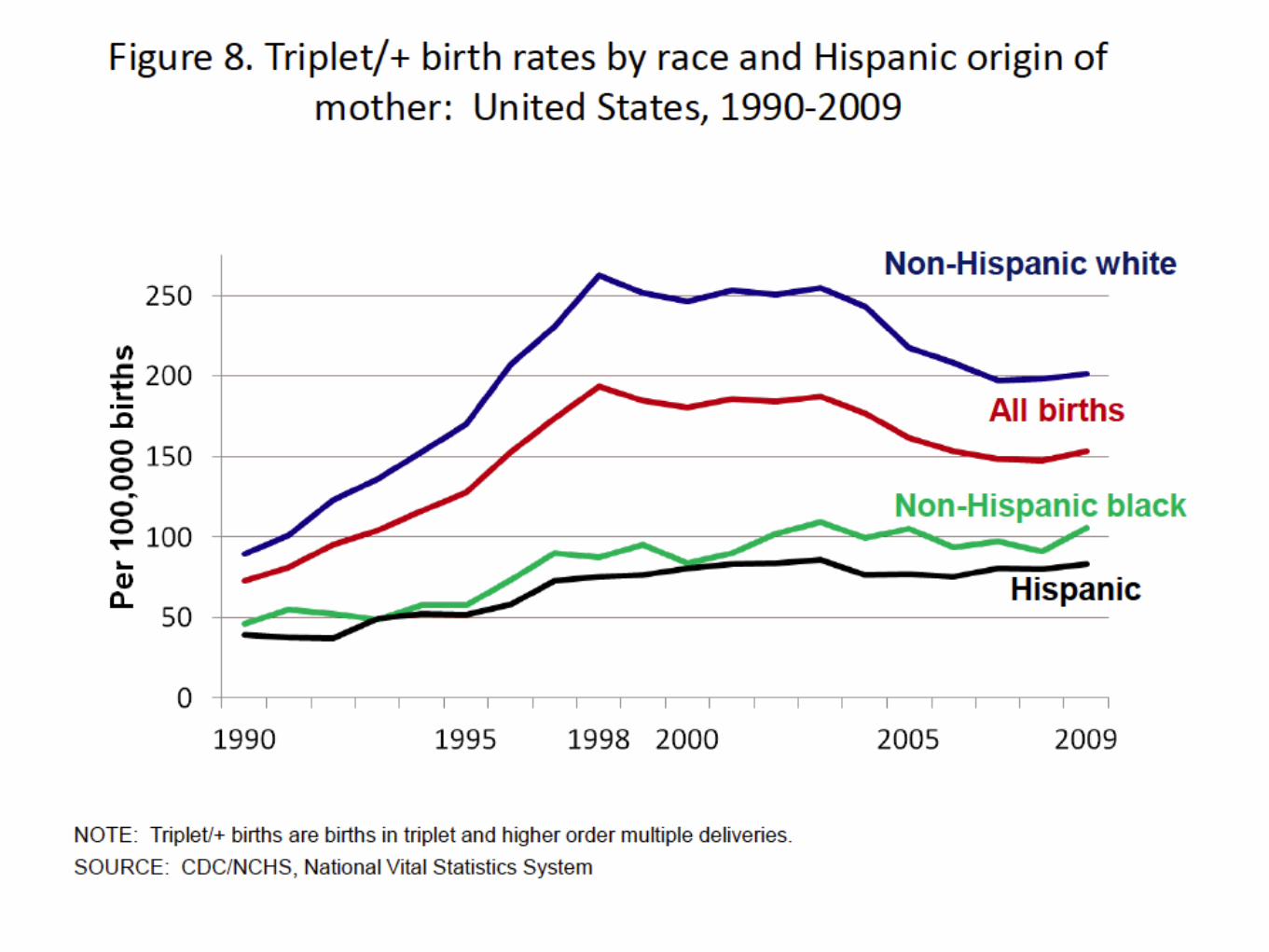
• Infertility treatments - increased multiple gestations (2.4% - 3.2%)
• Increased rates of PROM and preterm labor, PTL increased by 13.8%; PROM by 10.4% (1993-2002)
• Dating problems - iatrogenic• Davidoff MJ, 2006
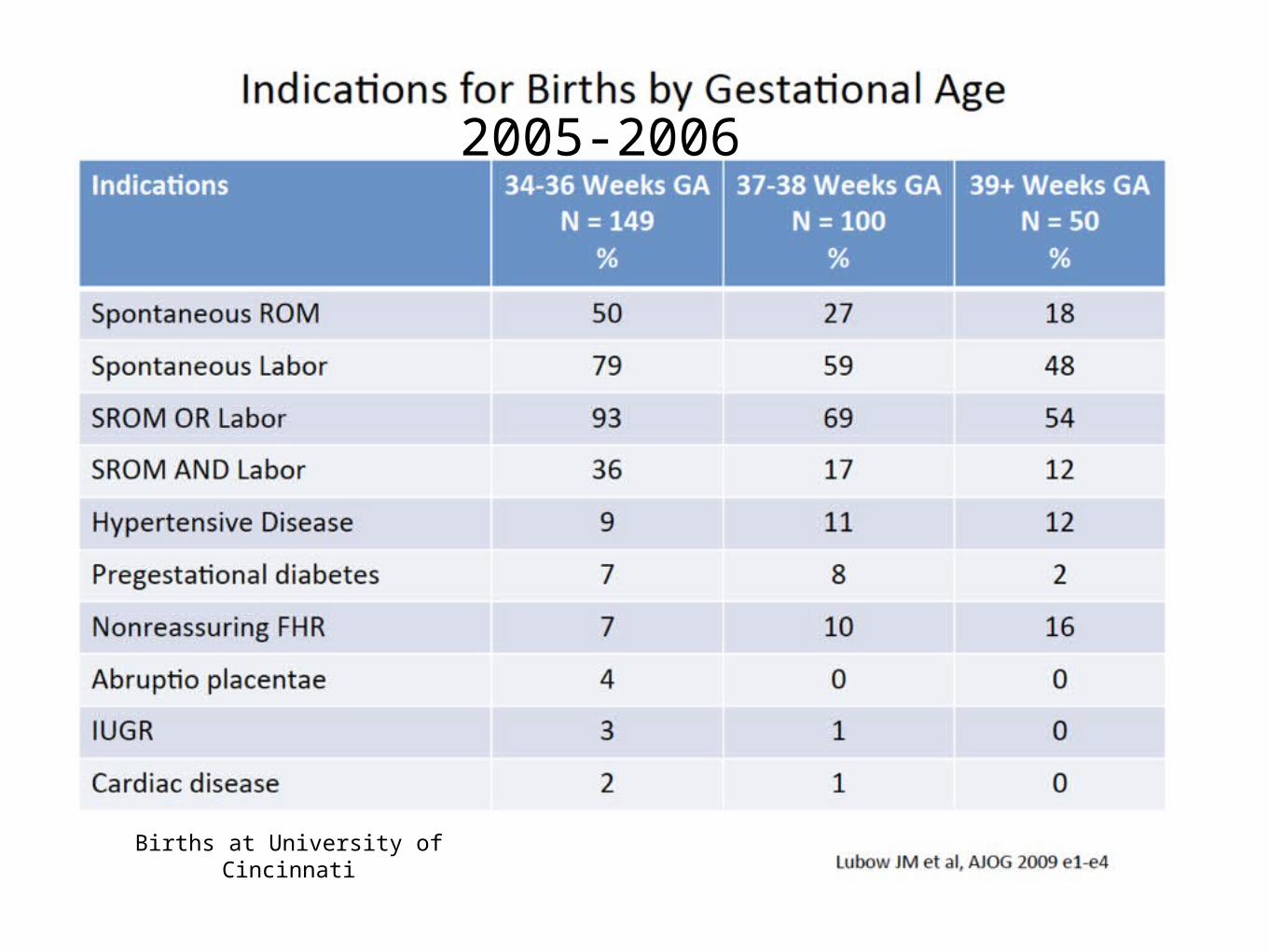
2005-2006
Births at University of Cincinnati
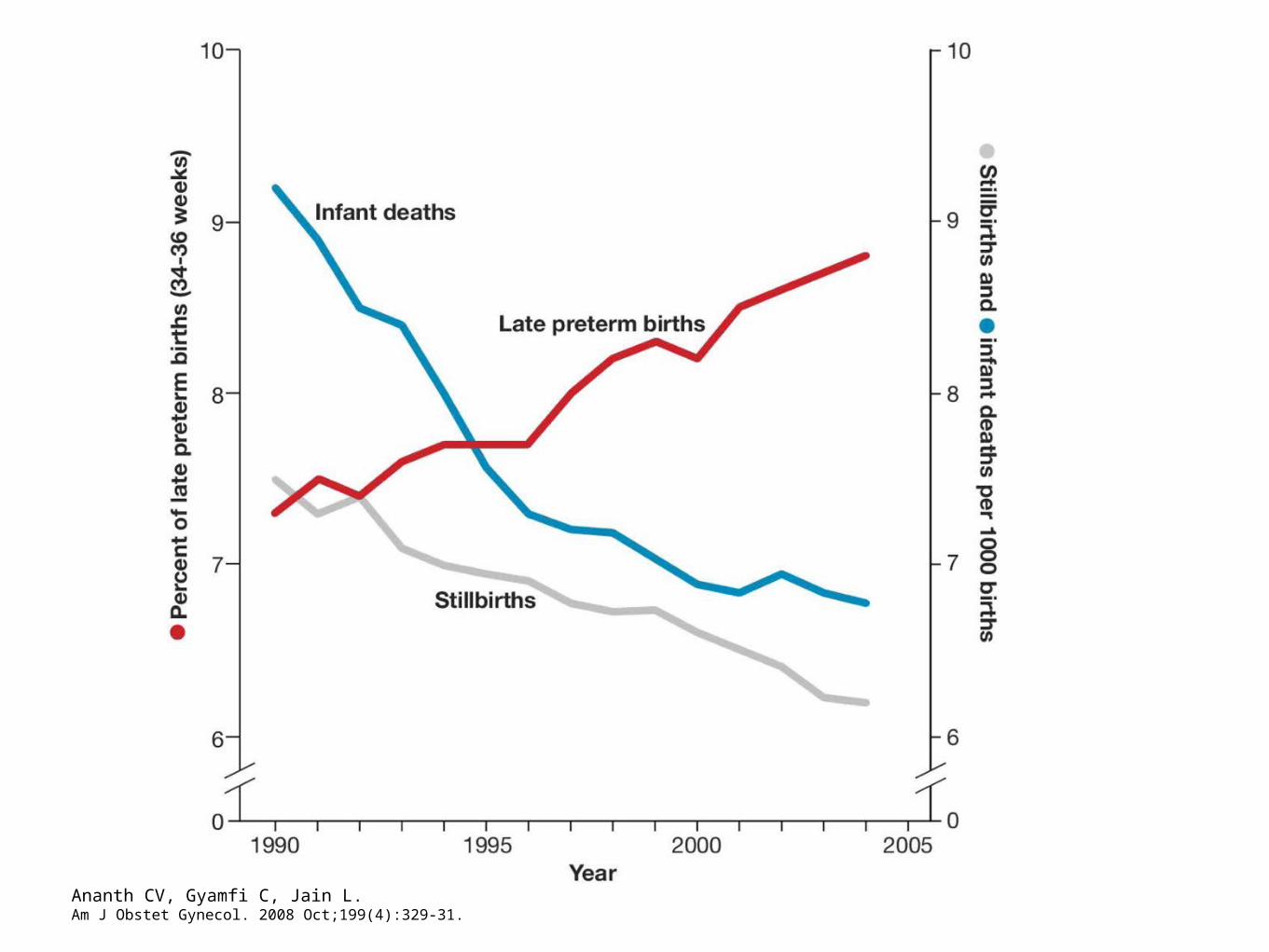
Ananth CV, Gyamfi C, Jain L.Am J Obstet Gynecol. 2008 Oct;199(4):329-31.

Epidemiology Where are we now?
•In US, total births in 2010 = 4,000,279
•Late Preterm Births in 2010 = 339,625 (8.49%)
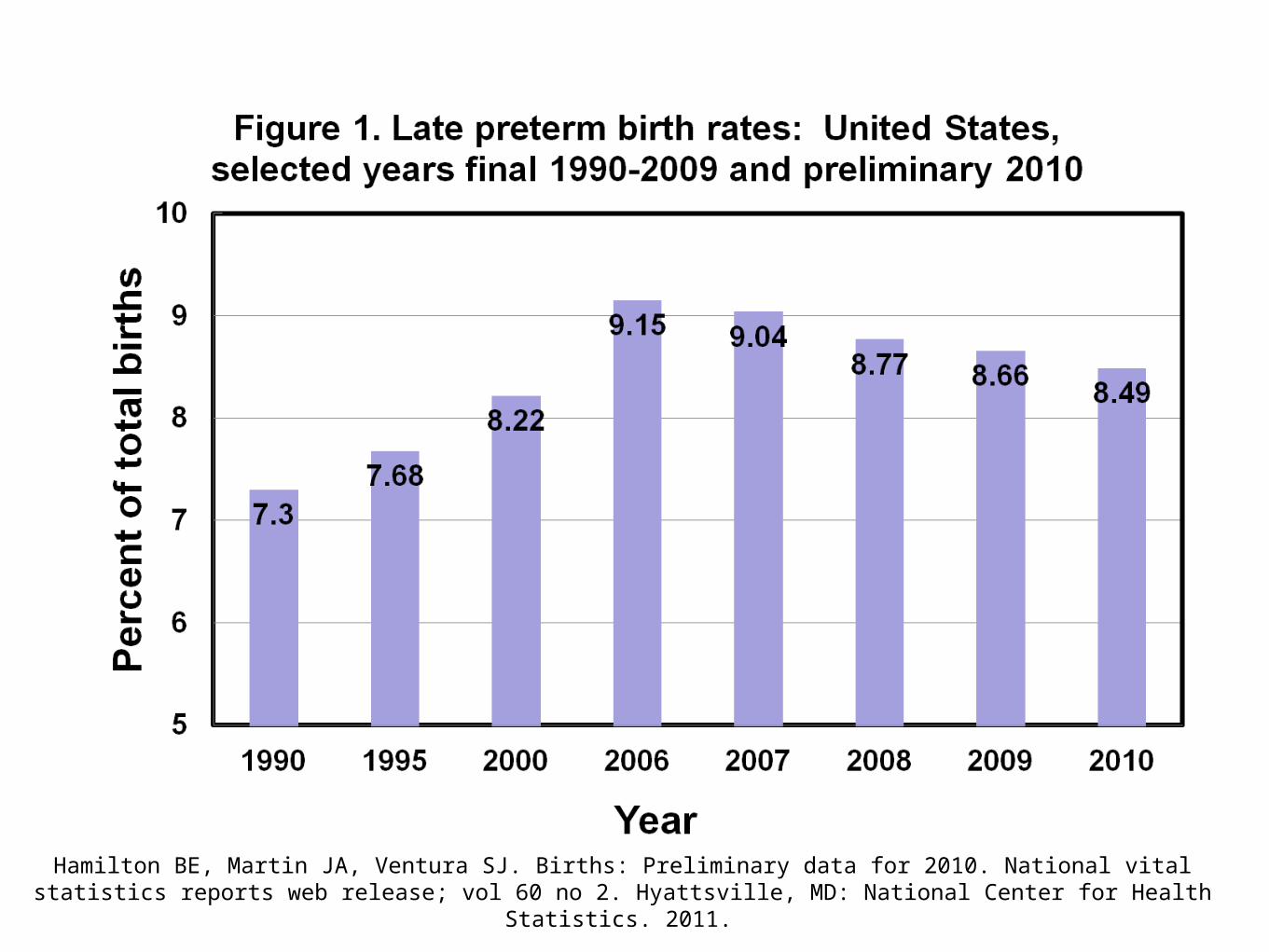
Hamilton BE, Martin JA, Ventura SJ. Births: Preliminary data for 2010. National vital statistics reports web release; vol 60 no 2. Hyattsville, MD: National Center for Health Statistics. 2011.
Epidemiology
•In New Mexico total births in 2010 = 27,028
•Late Preterm total = 2,352 (8.7% of total births)

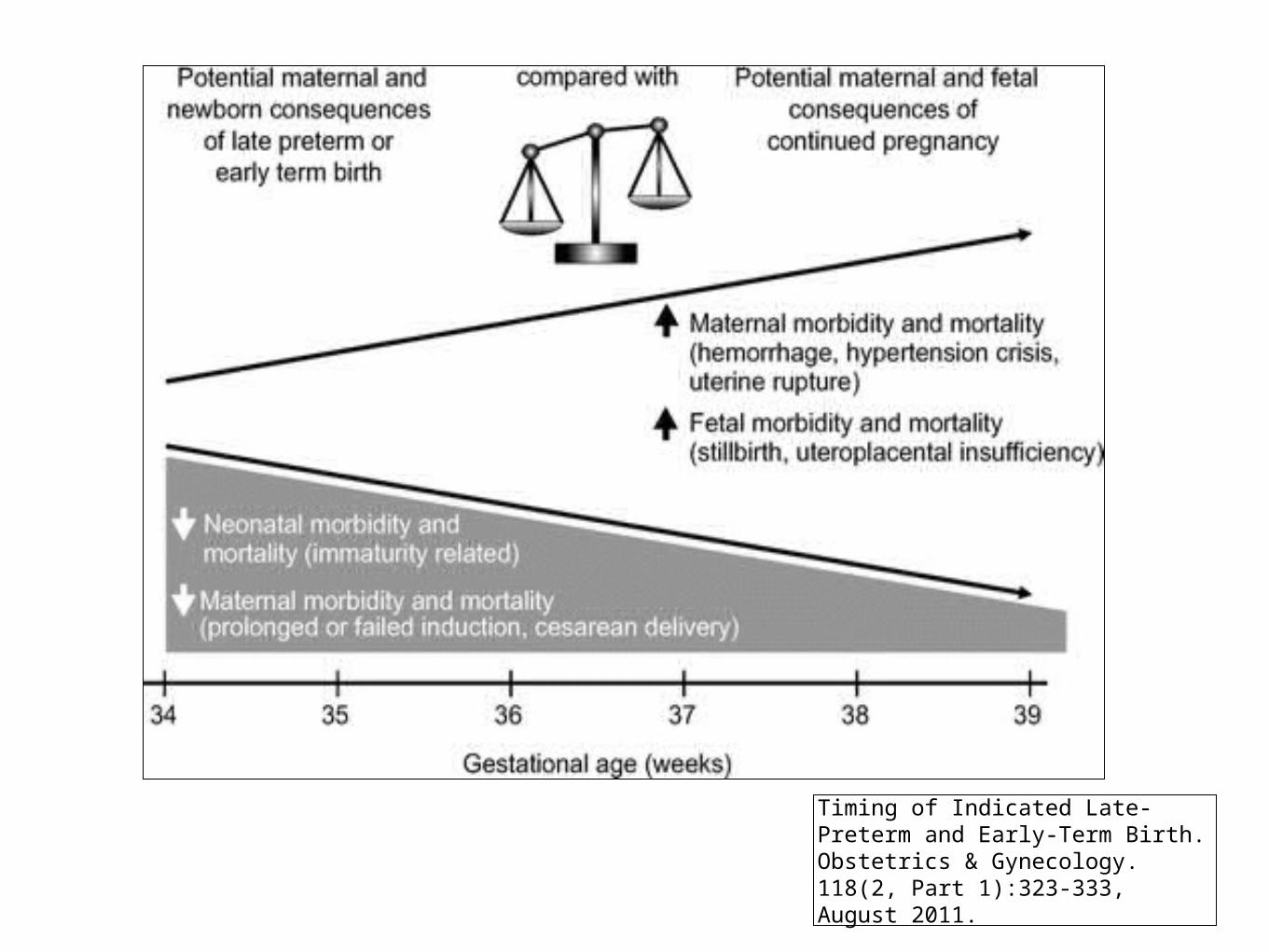
Timing of Indicated Late-Preterm and Early-Term Birth.Obstetrics & Gynecology. 118(2, Part 1):323-333, August 2011.
© 2011 The American College of Obstetricians and Gynecologists. Published by The American College of Obstetricians and Gynecologists.
3
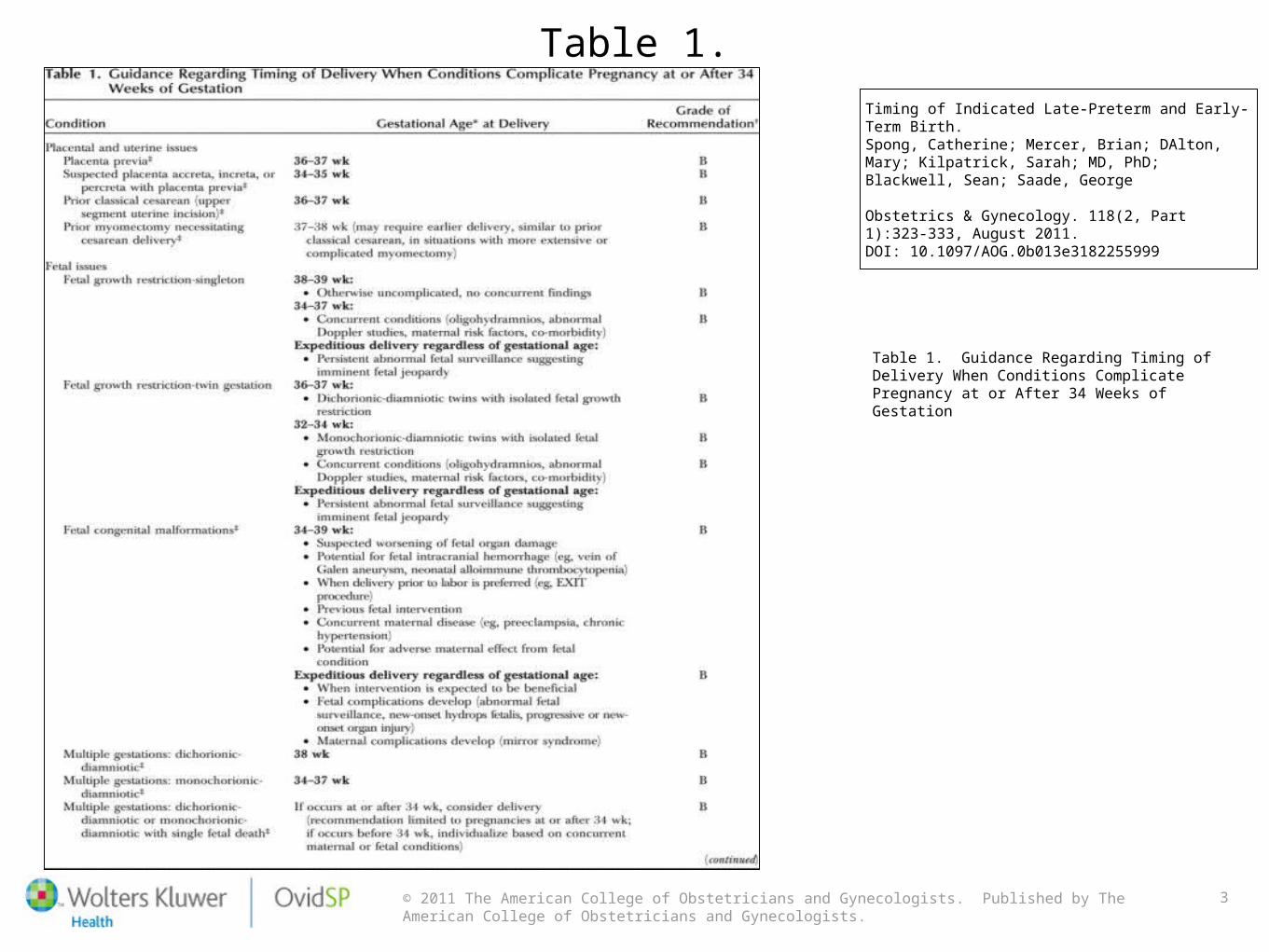
Table 1.Timing of Indicated Late-Preterm and Early-Term Birth.Spong, Catherine; Mercer, Brian; DAlton, Mary; Kilpatrick, Sarah; MD, PhD; Blackwell, Sean; Saade, George
Obstetrics & Gynecology. 118(2, Part 1):323-333, August 2011.DOI: 10.1097/AOG.0b013e3182255999
Table 1. Guidance Regarding Timing of Delivery When Conditions Complicate Pregnancy at or After 34 Weeks of Gestation
© 2011 The American College of Obstetricians and Gynecologists. Published by The American College of Obstetricians and Gynecologists.
4
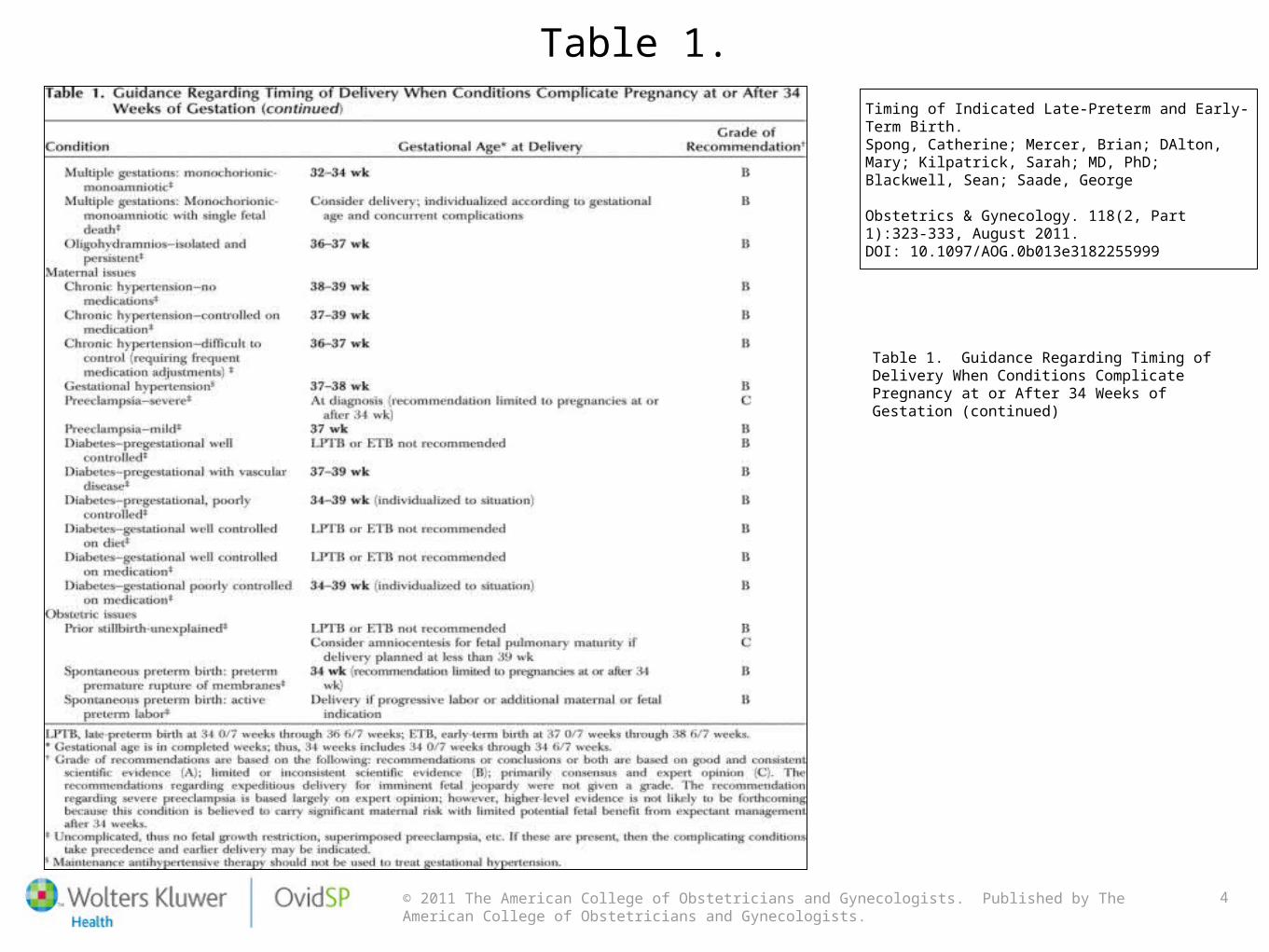
Table 1.Timing of Indicated Late-Preterm and Early-Term Birth.Spong, Catherine; Mercer, Brian; DAlton, Mary; Kilpatrick, Sarah; MD, PhD; Blackwell, Sean; Saade, George
Obstetrics & Gynecology. 118(2, Part 1):323-333, August 2011.DOI: 10.1097/AOG.0b013e3182255999
Table 1. Guidance Regarding Timing of Delivery When Conditions Complicate Pregnancy at or After 34 Weeks of Gestation (continued)

Early Morbidity
and Mortality
What milestones are missed by
infants born late preterm?
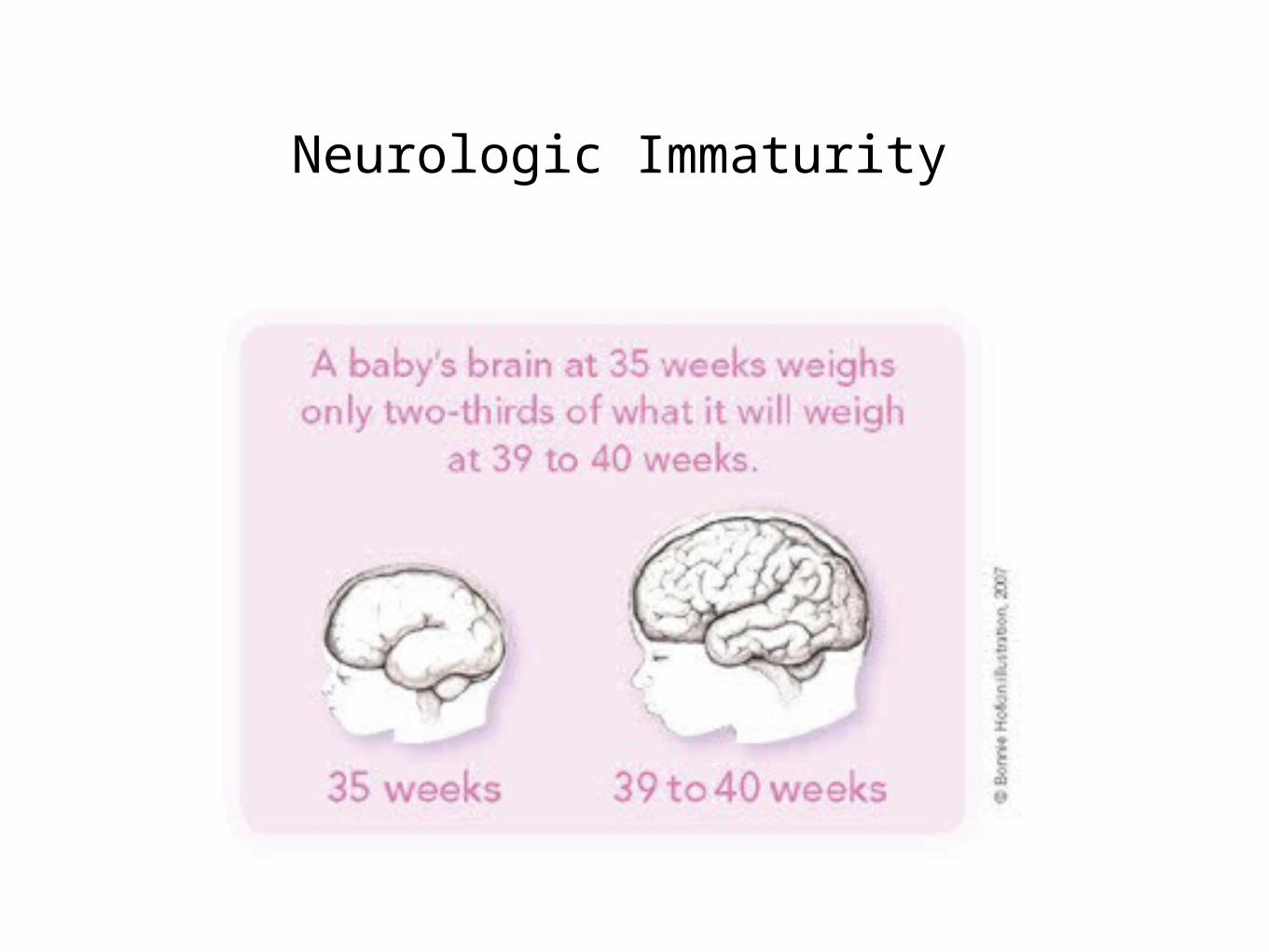
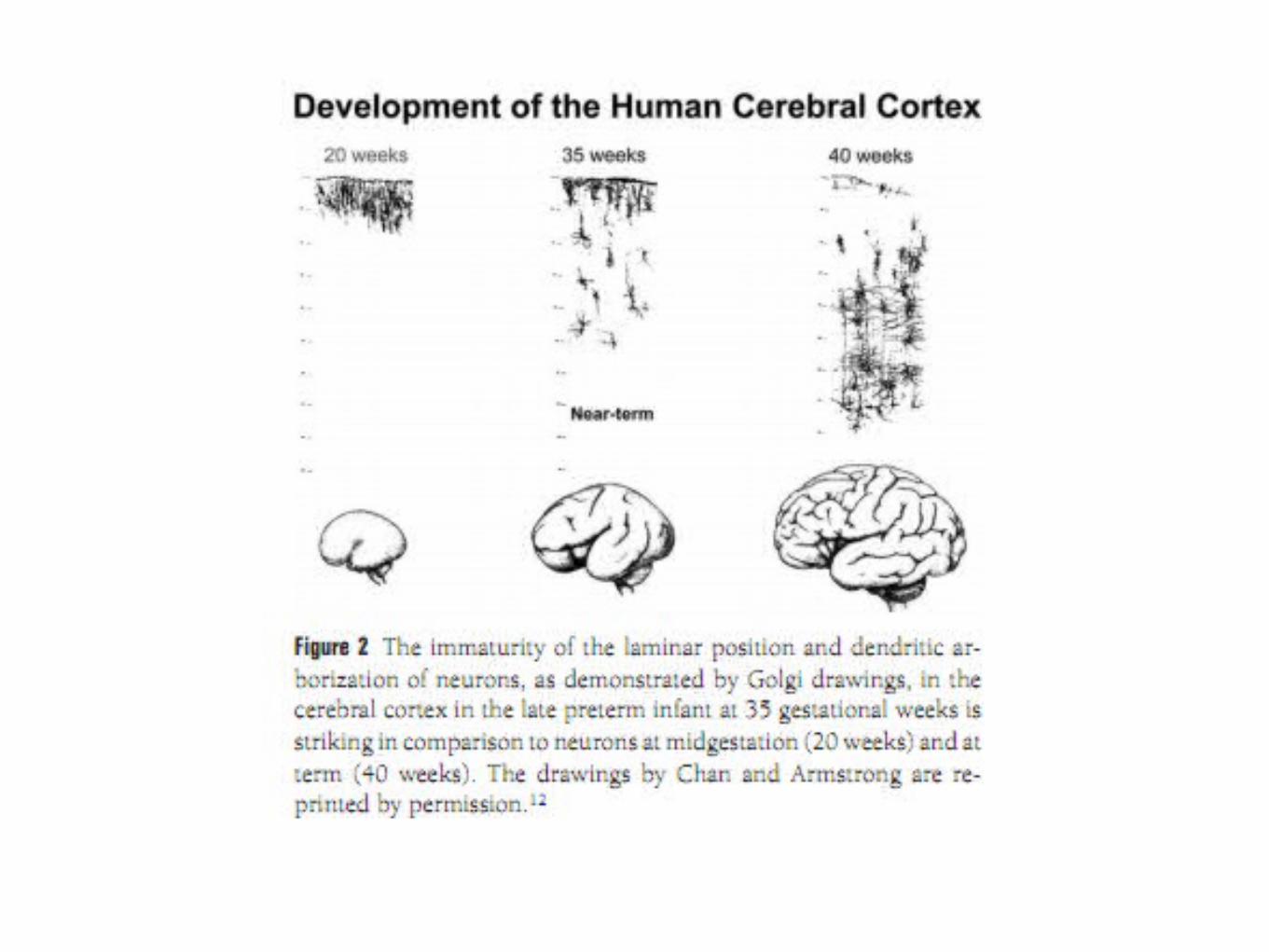
Neurologic Immaturity
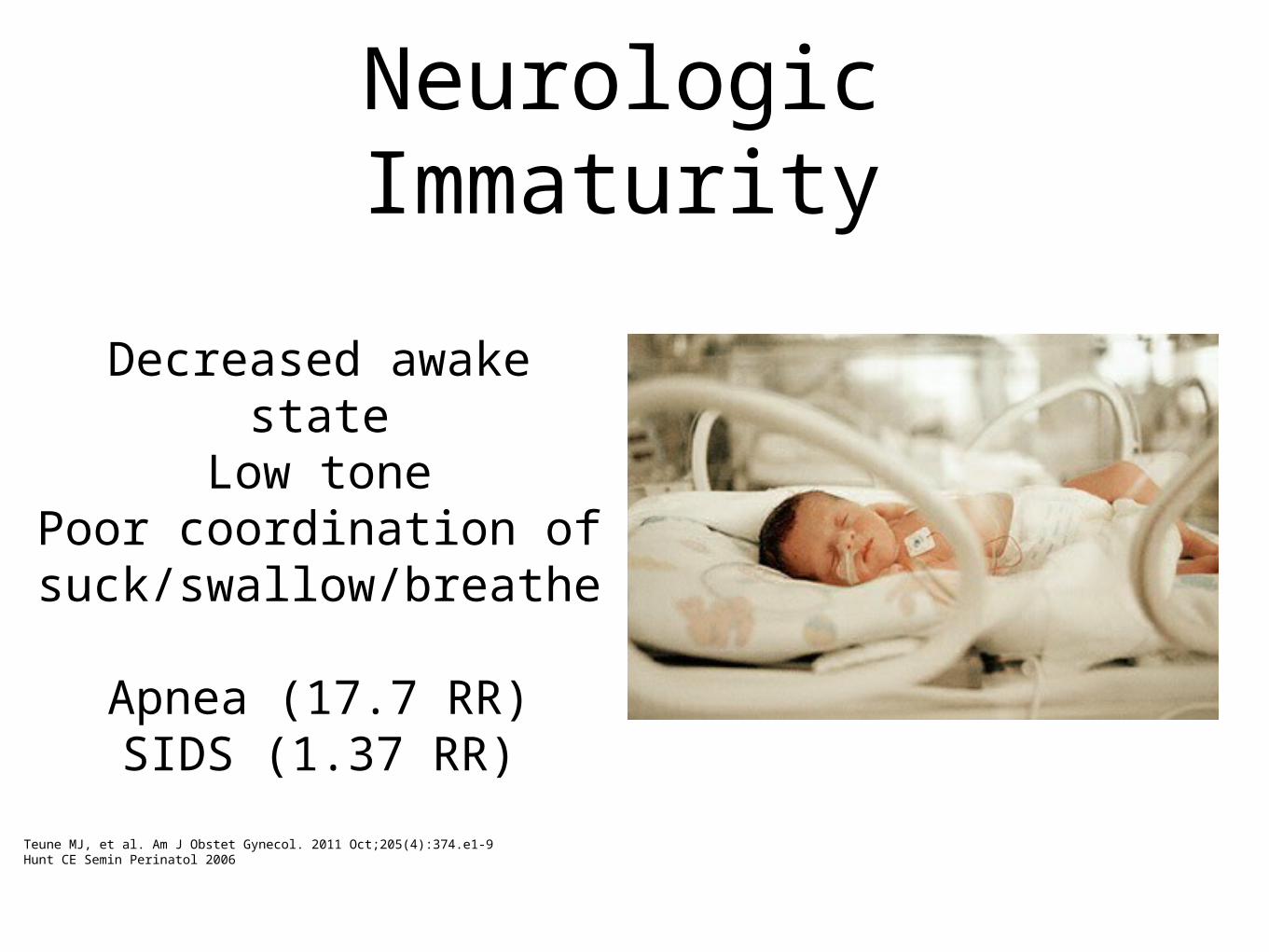
Neurologic Immaturity
Decreased awake state
Low tonePoor coordination of
suck/swallow/breathe
Apnea (17.7 RR)SIDS (1.37 RR)
Teune MJ, et al. Am J Obstet Gynecol. 2011 Oct;205(4):374.e1-9Hunt CE Semin Perinatol 2006
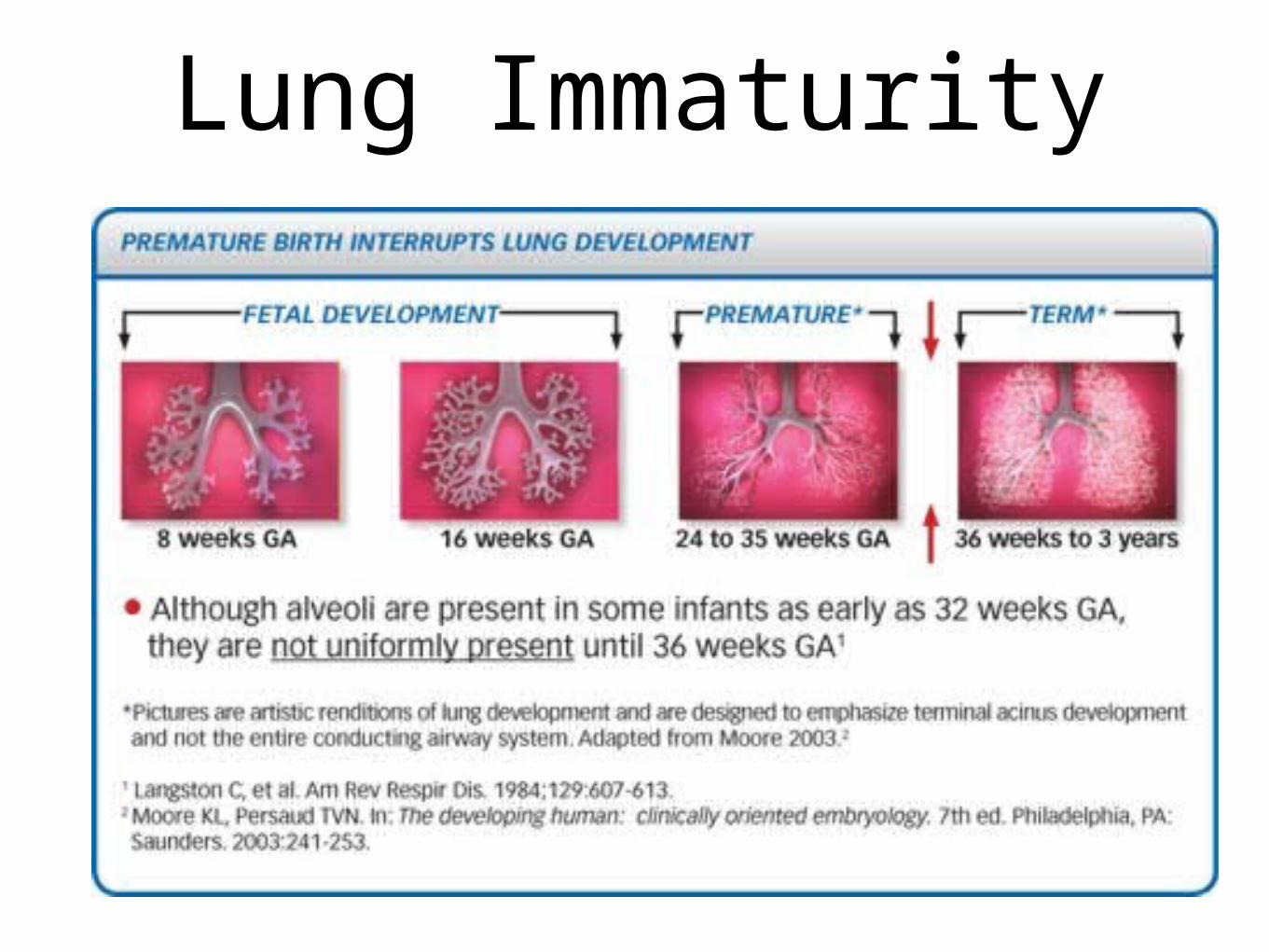
Lung Immaturity

Lung Immaturity
Use of nasal oxygen - 6% of late preterms
(24.4 RR)
RDS - 5.3% (17.3 RR)
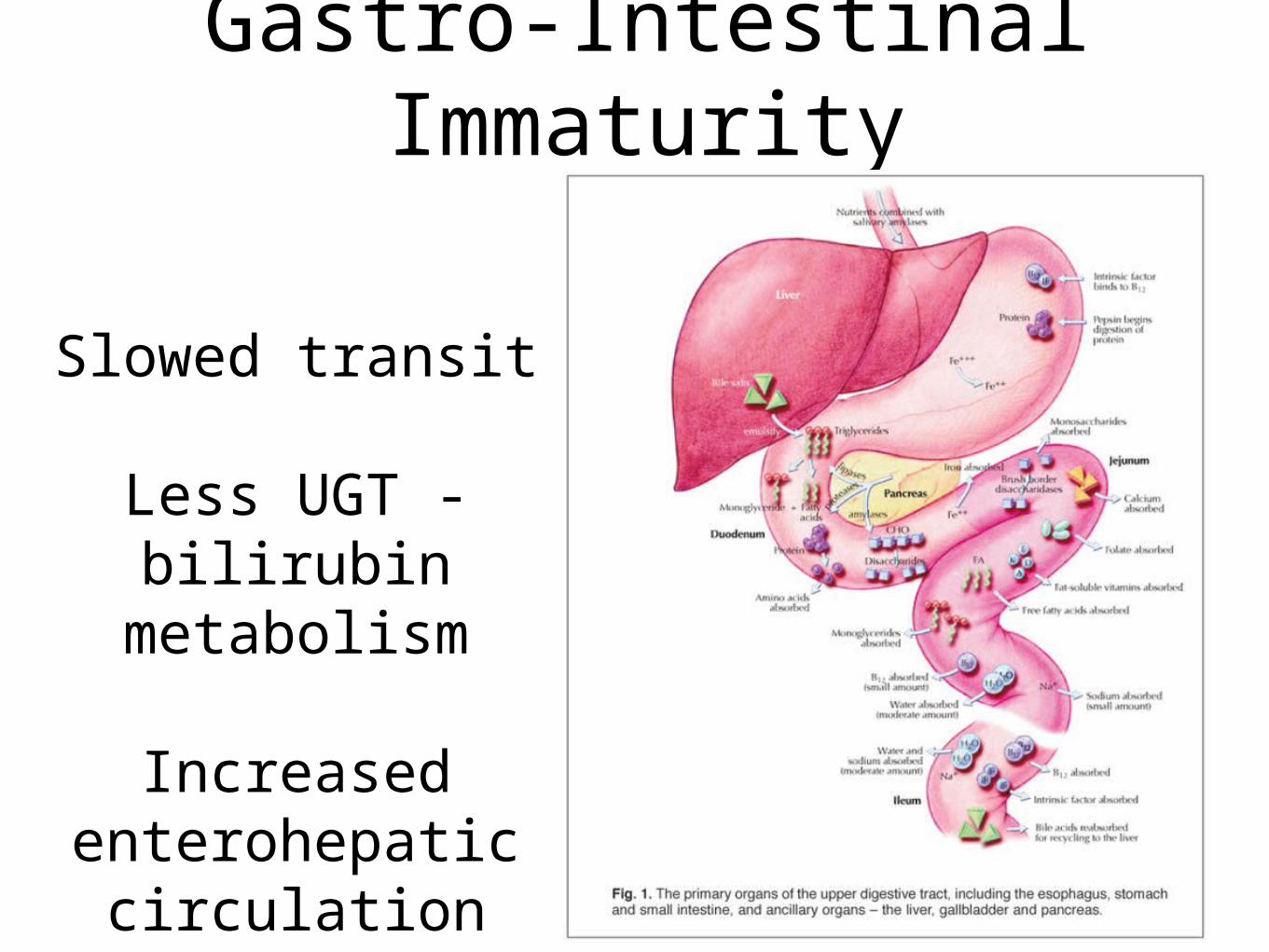
Gastro-Intestinal Immaturity
Slowed transit
Less UGT - bilirubin
metabolism
Increased enterohepatic
circulation
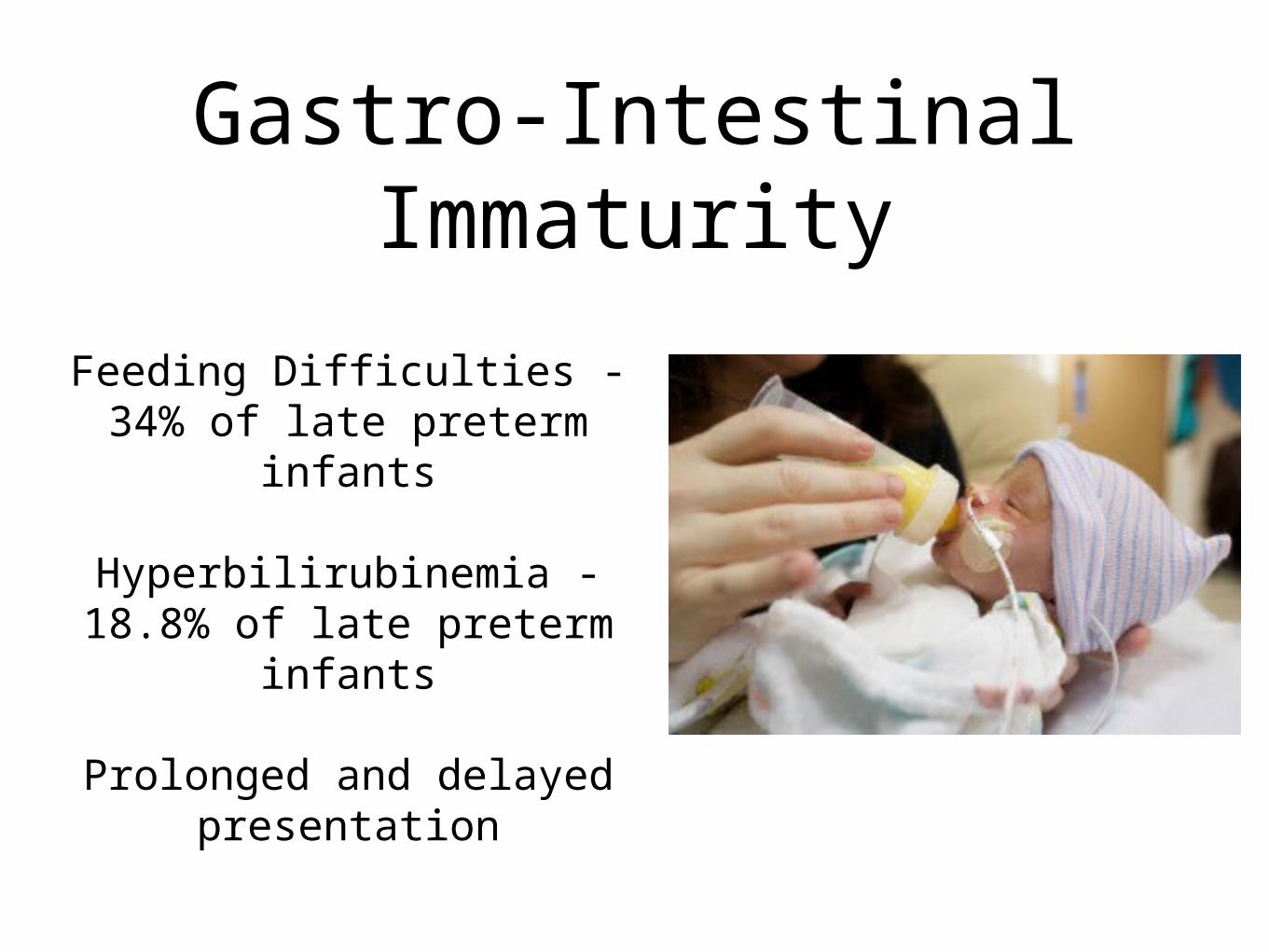
Gastro-Intestinal Immaturity
Feeding Difficulties - 34% of late preterm infants
Hyperbilirubinemia - 18.8% of late preterm
infants
Prolonged and delayed presentation
Metabolic Immaturity
Small size
SGA
Less brown fat
Less white
adipose
Metabolic Immaturity
Hypoglycemia - 7.1% of LPIs
Hypothermia - 1.5% of LPIs
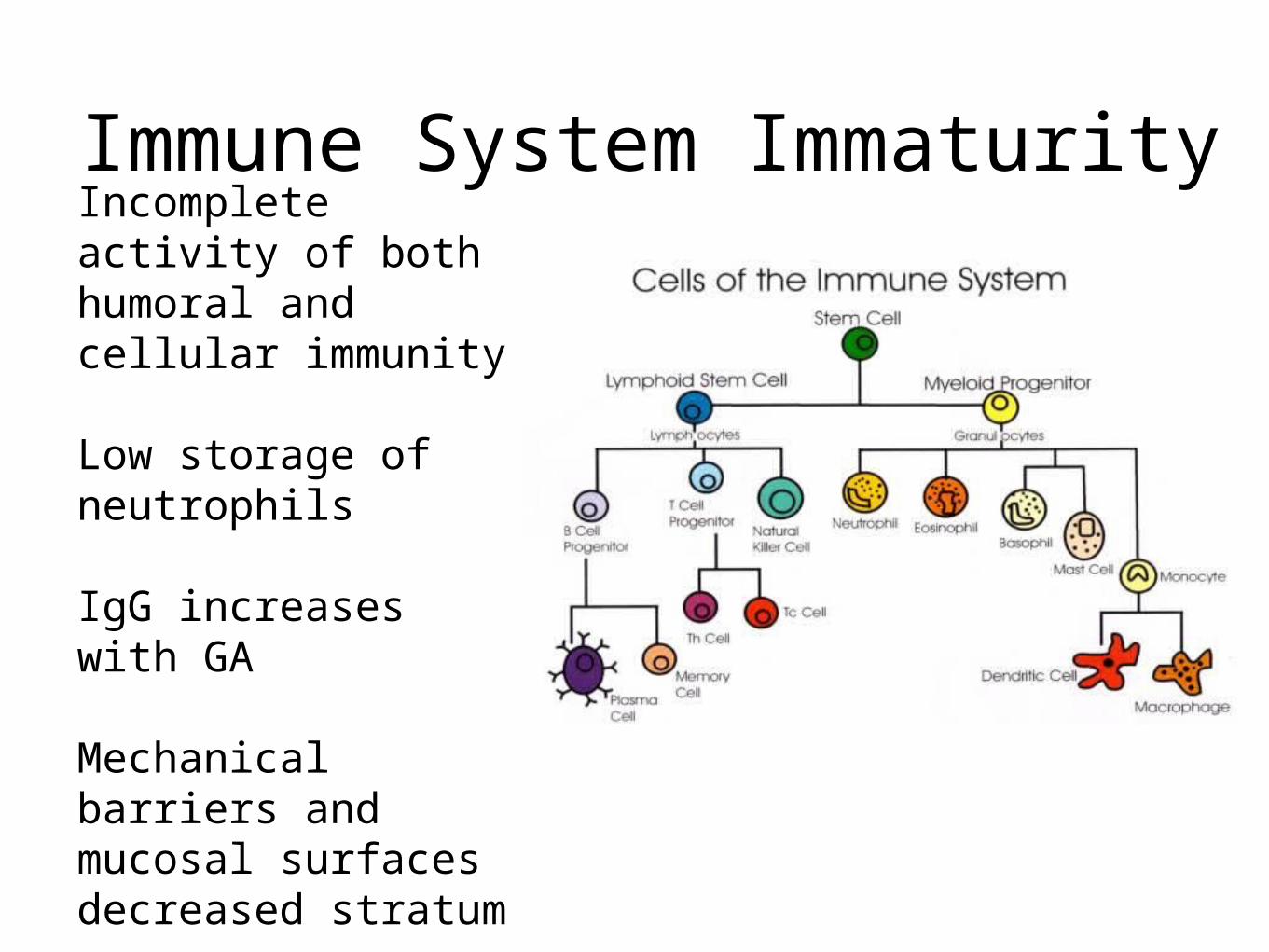
Immune System ImmaturityIncomplete activity of both humoral and cellular immunity
Low storage of neutrophils
IgG increases with GA
Mechanical barriers and mucosal surfaces decreased stratum corneum

Immune System Immaturity
More sepsis work-ups - 19.7% of late preterms
Sepsis (RR 5.6) Meningitis (RR 21)
PNA (RR 3.5) NEC (RR 7.5)
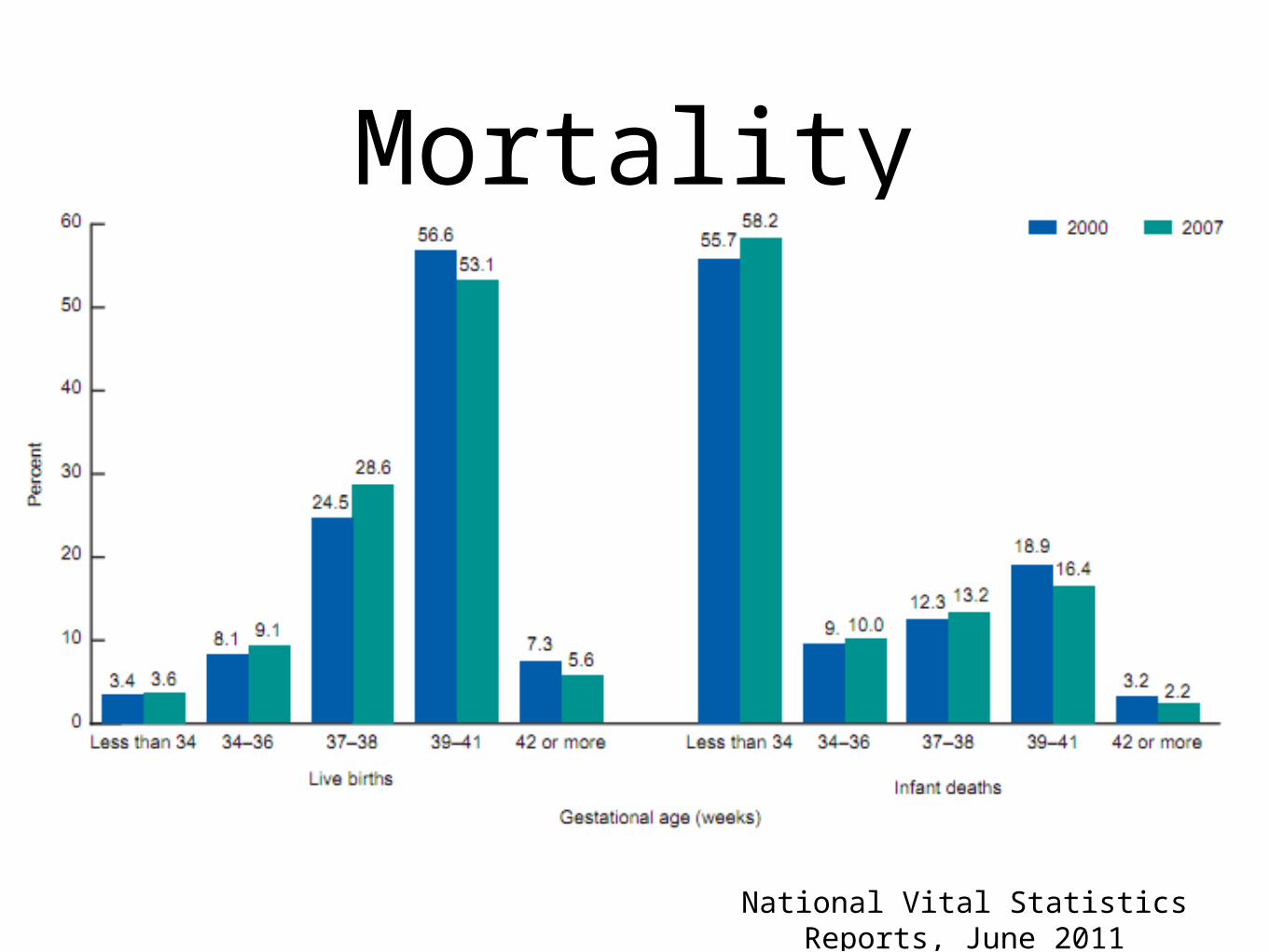
Mortality
National Vital Statistics Reports, June 2011
Newborn Period
•Missed events of development in last 6 weeks of gestation = morbidity risks in newborn period
Newborn period
•Tell families their baby will stay until close to their due date
•Every baby is different
•Some presentation is delayed, need to follow closely
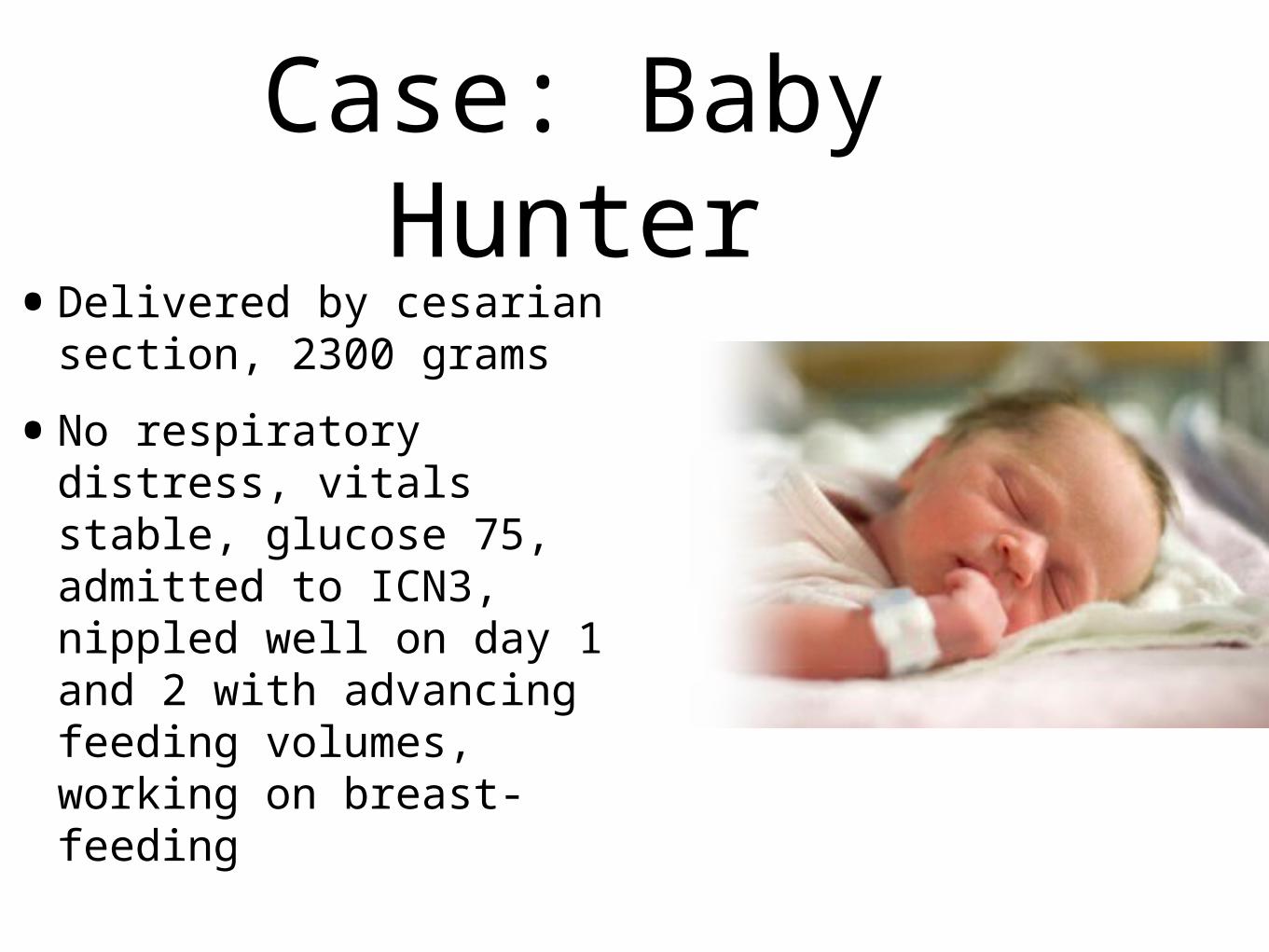
Case: Baby Hunter•Delivered by cesarian
section, 2300 grams
•No respiratory distress, vitals stable, glucose 75, admitted to ICN3, nippled well on day 1 and 2 with advancing feeding volumes, working on breast-feeding
Case
•Day 3 and 4, Hunter is more easily fatigued with nippling, some lower temps recorded, naso-gastric tube placed, nippling now once per shift, mom expressing breast milk
Case
•Day 5, Hunter’s needs phototherapy for increasing bilirubin, still working on feeds, poor weight gain
•Day 6-8, Hunter’s mom has to return to Gallup to care for 2 y.o. at home, still trying to express and store breast milk
Case
•Day 12, taking full feeds, waking every 2-3 hours to feed, gaining weight, passed car seat trial, ready for discharge
Nutrition
•Breastmilk
•Human-milk fortifier?
•Formula?
•Many challenges in the breastfeeding late preterm infant
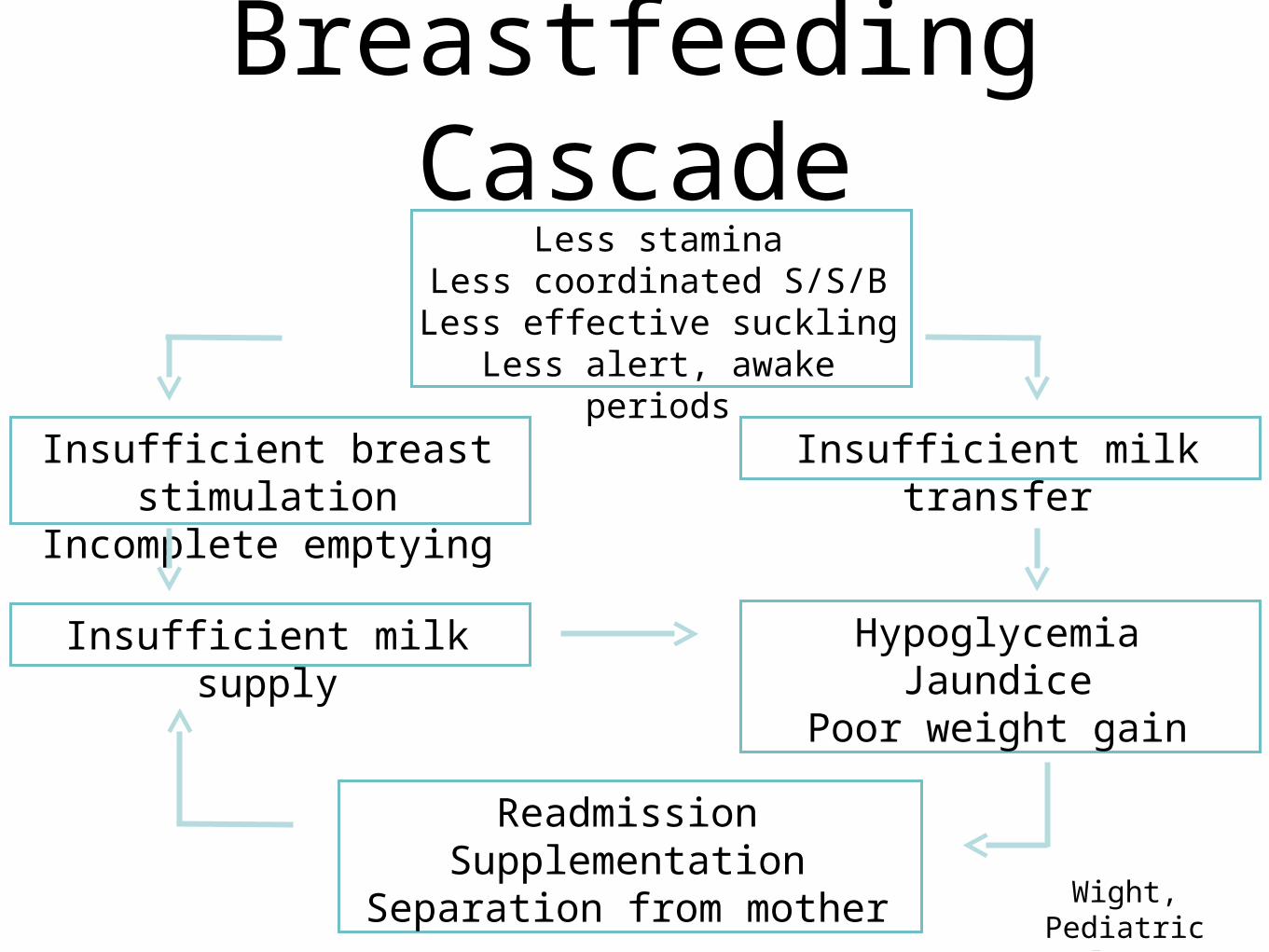
Breastfeeding CascadeLess stamina
Less coordinated S/S/BLess effective suckling
Less alert, awake periods
Insufficient breast stimulation
Incomplete emptying
Insufficient milk transfer
Insufficient milk supply HypoglycemiaJaundice
Poor weight gain
ReadmissionSupplementation
Separation from mother Wight, Pediatric Annals 2003;
32:5
Breastfeeding Management Strategies
• Kangeroo skin-to-skin contact
• Strong evidence of increased breastfeeding at 1 month after discharge (RR 4.76, 95% CI 1.19 to 19.1) and for more than 6 wks (RR 1.95, 95% CI 1.03 to 3.7)
• Minimize pain during painful procedures
• Peer support
• Simultaneous pumping
• Multidisciplinary staff training
• Baby Friendly accreditationRenfrew et al., Health Technol Assess, 2009

Growth• Catch up growth
• Abnormal growth patterns may be associated with adult morbidity
• Limited investigations on the growth development of LPIs
• Santos et al. BMC Pediatrics, 2009
• Risk of being underweight was at least two folds higher for LPIs
Readmission•LPIs are readmitted 2 to 3 times more
often than term infants
•Common reasons:
• Jaundice, infection, feeding issues, failure to thrive
•Risk factors:
•Primigravida mother, breastfeeding, maternal complications, public insurance and Asian/Pacific Island heritage
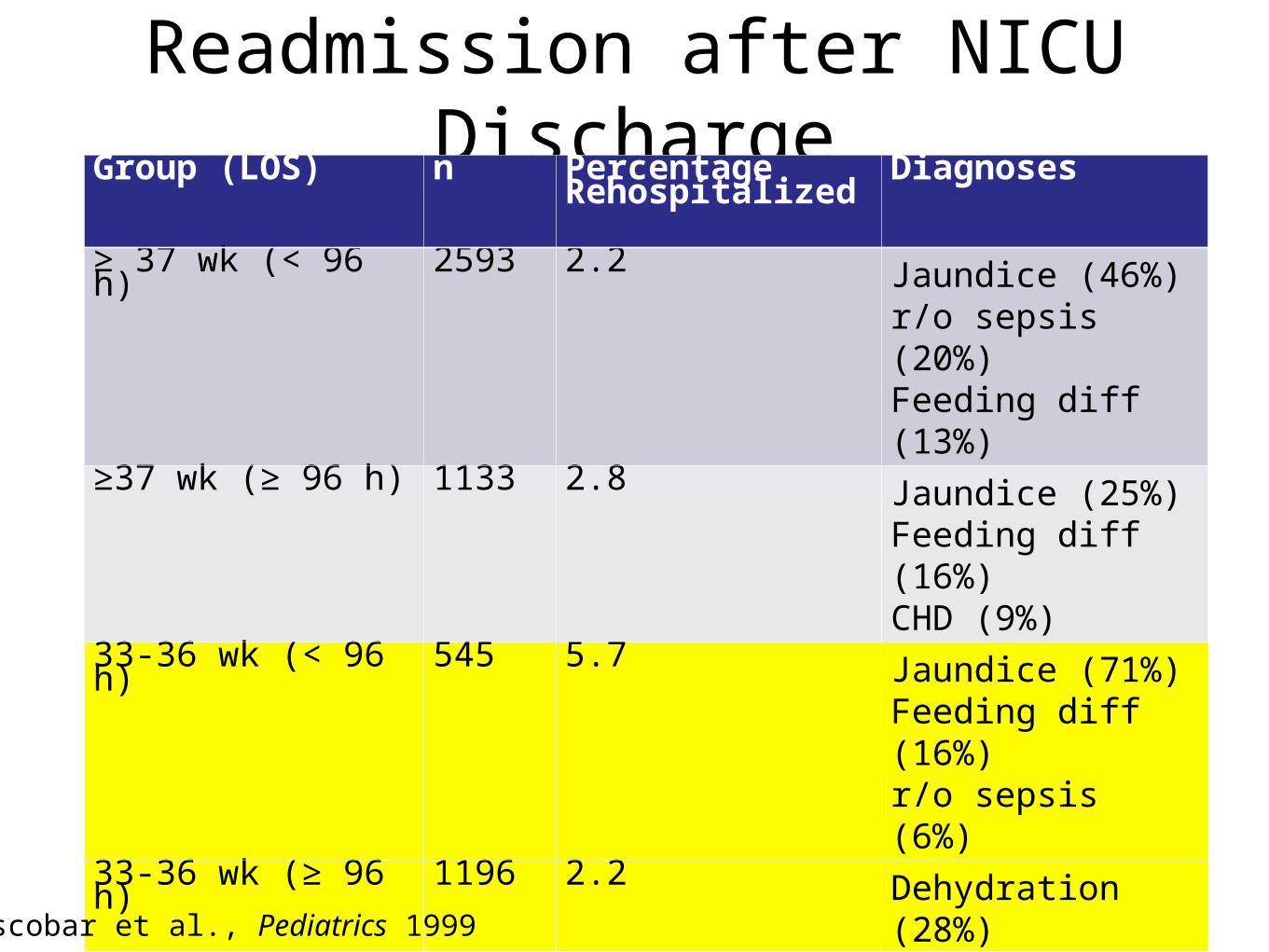
Readmission after NICU DischargeGroup (LOS) n Percentage
RehospitalizedDiagnoses
≥ 37 wk (< 96 h) 2593 2.2 Jaundice (46%)r/o sepsis (20%)Feeding diff (13%)
≥37 wk (≥ 96 h) 1133 2.8 Jaundice (25%)Feeding diff (16%)CHD (9%)
33-36 wk (< 96 h) 545 5.7 Jaundice (71%)Feeding diff (16%)r/o sepsis (6%)
33-36 wk (≥ 96 h) 1196 2.2 Dehydration (28%)Jaundice (20%)r/o sepsis (20%)
< 32 wk (all LOS) 587 3.4 Bronchiolitis (21%)GER (16%)Hernia repair (10%)
Escobar et al., Pediatrics 1999

Neurodevelopmental Outcomes

Neurodevelopmental Outcomes
• Few studies
• Neurologic abnormalities, learning difficulties, poor scholastic achievement, and behavioral problems have been reported
• CP is three times more likely
• DD and MR have been found to be 1.3-2 times more likely
• No evidence of increased risk of autism has been reported
Arpino et al, Childs Nerv Syst, 2010
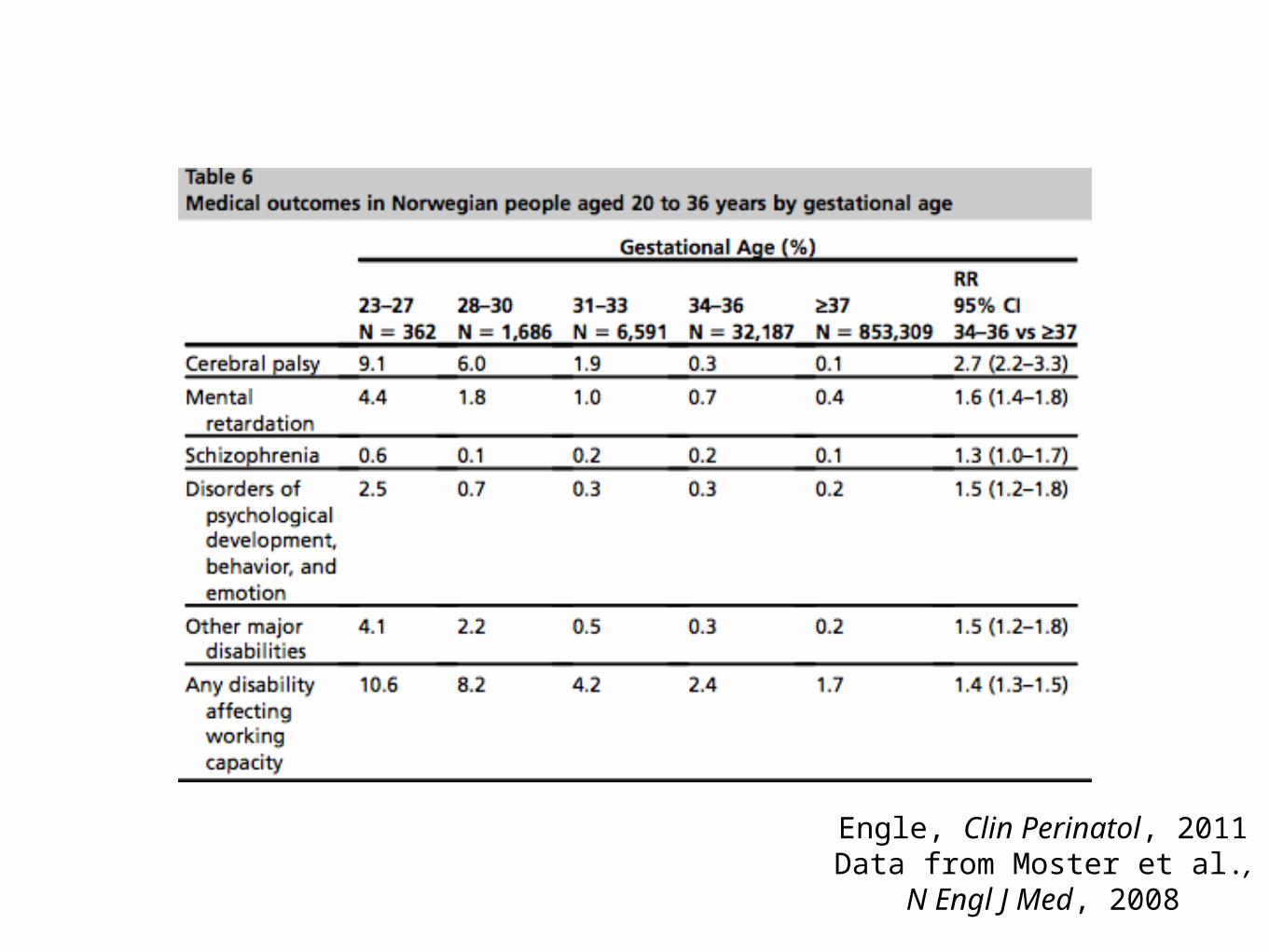
Engle, Clin Perinatol, 2011Data from Moster et al., N
Engl J Med, 2008
Learning Disability•Compared to full
term:
•LPIs have 24% increased odds for reading scores below average in the first grade of education
•1.4-2.1 risk for special education Arpino et al, Childs Nerv Syst,
2010

Morse et al., Pediatrics, 2009

Early School and Developmental
Outcomes
•61 healthy infants born between 33-36 weeks gestation
•At 12 and 18 months corrected GA, LPI showed a mean developmental index similar to term infants
Romeo et al., Euro Ped Neur Soc, 2010
Case: Baby Hunter•Hunter is seen by his pediatrician for his
9 month well child check
•He continues to breastfeed and mom has introduced solids without difficulty
•He babbles, says “mama”, and likes to play “peek-a-boo”
•On exam his physician notes that he is unable to sit without support
•He is referred to Early Intervention
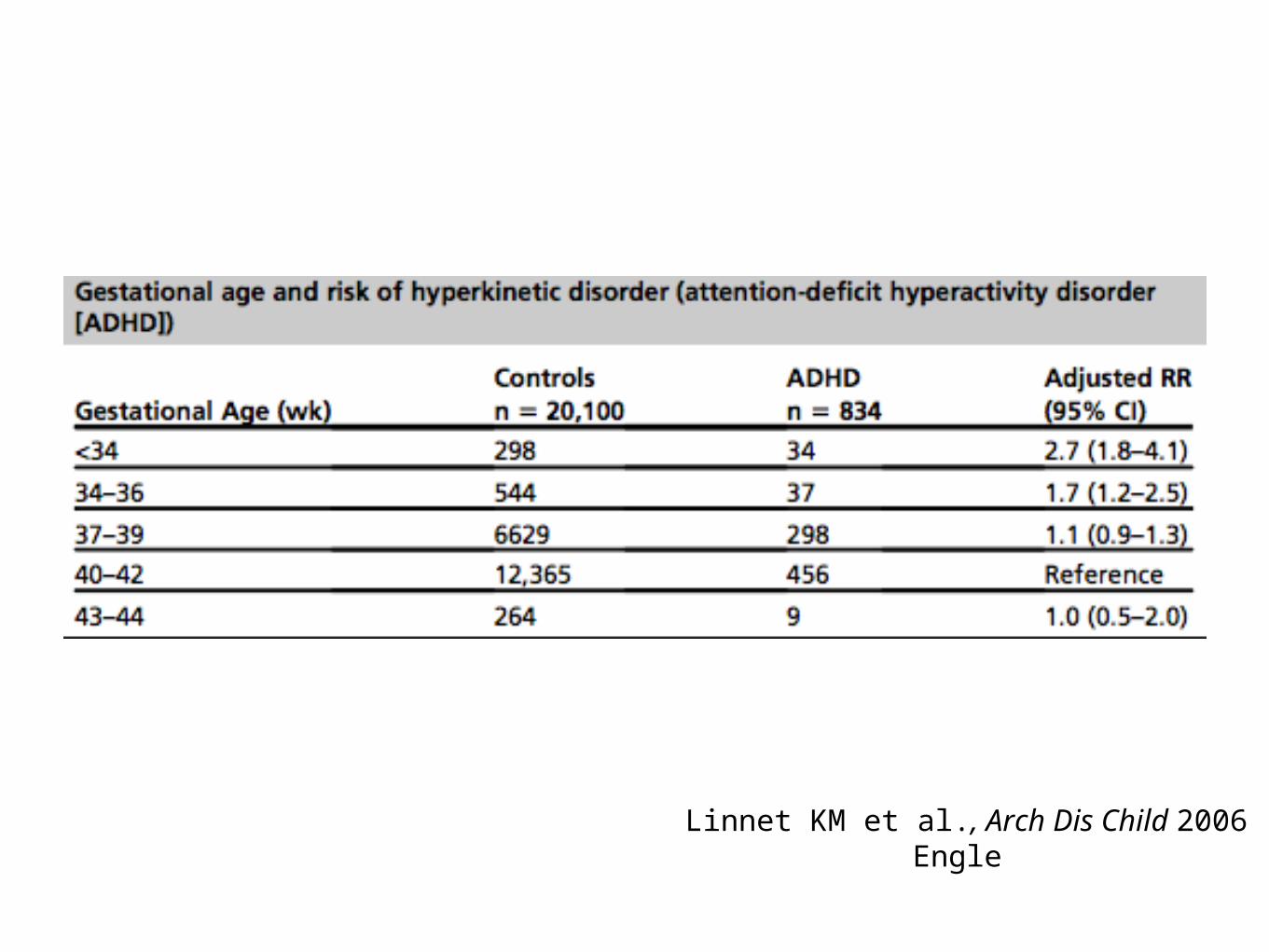
Linnet KM et al., Arch Dis Child 2006Engle
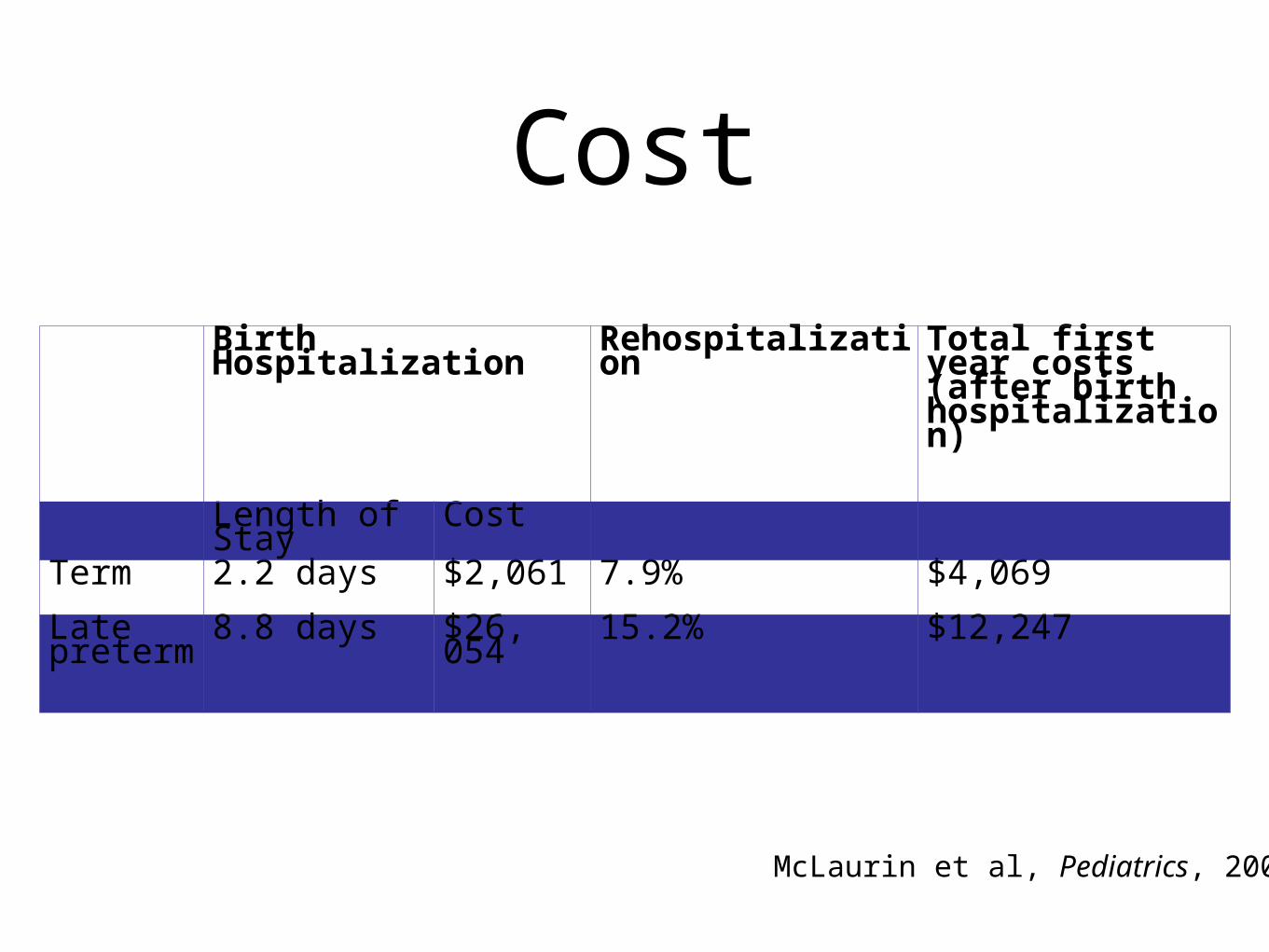
Cost
Birth Hospitalization
Rehospitalization
Total first year costs (after birth hospitalization)
Length of Stay
Cost
Term 2.2 days $2,061 7.9% $4,069
Late preterm
8.8 days $26, 054
15.2% $12,247
McLaurin et al, Pediatrics, 2009

Future ResearchNational Institute of Child Health and Human
Development: Optimizing Care and Outcome for Late-Preterm Infants
•Education
•Epidemiology and Etiology
•Gestational-age-specific morbidities and mortalities
•Evidence-based intervention guidelines
•Assessing the total cost of LPI birth
•Outcomes of LPIs and relationship to indication for delivery
Conclusions•Although the risk of poor outcome is
less than that of an early preterm infant, LPIs are a vulnerable population.
•Early discharge should not occur in these infants and diligent follow up is important, both in the post neonatal period and for continued long-term care.
•More research is needed
Questions?