the journey to high reliability….your flight plan for...
TRANSCRIPT

12/2/2013
1
The Journey to High Reliability….Your Flight Plan for Success
Patrick M. O’Shaughnessy, DO, MBA, FACEP, CHCQM
Senior Vice President & Chief Medical Officer
Catholic Health Services of Long Island
High Reliability Workshop
December 9th, 2013
Session Objectives
Discuss High Reliability concepts from aviation and other HRO’s and applicability to healthcare.
Who’s your Pilot in charge and who are your crew (People)?
What’s your flight plan (process)?
Have you mastered & integrated your avionics and air traffic control (technology and communication)?
Share lessons learned from our organization.
Articulate specific actions you can take to make progress toward high reliability.
Dr. Patrick M. O’Shaughnessy has nothing to discloseNo financial interests or affiliations with any materials presented or distributed at this lecture
P2

12/2/2013
2
Catholic Health Services of Long Island
Healthcare system based out of Rockville Centre, Long Island New York with 1,928 total acute care beds and 790 continuing care beds.
Six Acute Care FacilitiesSaint Francis Hospital; The Heart Center
Mercy Medical Center
Saint Josephs Hospital
Good Samaritan Medical Center
Saint Catherine of Siena Medical Center
Saint Charles Hospital
Collectively the campuses provide clinical services across ALL major surgical and medical service lines, two campuses with OHS programs.
P3
Catholic Health Services of Long Island
Continuing Care Division
Our Lady of Consolation Nursing and Rehabilitative Center
Saint Catherine of Siena Nursing and Rehabilitative Center
Good Samaritan Nursing and Rehabilitative Center
Home Care Division
Care link and Care link plus telemedicine
Clinical Navigator programs
Hospice Division
Maryhaven Center of Hope
Inpatient residence’s for those with developmental disabilities
Outpatient residence’s and day programs
P4

12/2/2013
3
Catholic Health Services of Long Island as a ministry of the Catholic Church, continues Christ’s healing mission,
promotes excellence in care, and commits itself to those in need.
CHS affirms the sanctity of life, advocates for the poor and underserved, and serves the common good. It
conducts its healthcare practice, business, education and innovation with justice, integrity and respect for the
dignity of each person.
CATHOLIC HEALTH SERVICESof Long Island
• Our Reason For BeingMission
• Our Place In The WorldVision
5
An innovative and fully-integrated organization recognized for excellence…
♦ in person-centered compassionate care and community health
♦ as the preferred partner of physicians
♦ by providing exceptional quality while making efficient use of resources
♦ through the dedicated efforts of an engaged, high-performing workforce
Catholic Health Services of Long IslandP6

12/2/2013
4
My Personal Background
Practicing Board Certified Emergency Physician.3 years in Academics
Areas of interest-> Simulation MedicineDisaster Medicine
Prior ED Department Director
3 years as facility Chief Medical OfficerSt. Catherine of Siena Medical Center
CHSLI System CMO, June 2013.
But…… I also like to fly planes!Career began at Embry-Riddle Aeronautical UniversityUpon migration into career of Medicine; was completely shocked to see how complex high risk systems were operated.
P7
Engineering RedundancyP8

12/2/2013
5
Pre flight CheckP9
Computerized ChecklistP10

12/2/2013
6
P11
Computerized ChecklistP12

12/2/2013
7
When all else fails…CAPSP13
High Reliability Aviation: USN
Naval Aircraft Carrier Operations:
Carrier Commanding Officer quotes:“ A hundred things I have no control over could go wrong and wreck my career…..but wherever I go from here, I’ll have no better job than this….This is the best job in the world.”
So you want to understand an aircraft carrier? Well just imagine that it is a busy day, and you shrink SF airport to one short runway. Make planes take off and land at the same time, at half the present time interval, rock the runway from side to side, and require that everyone who leaves in the morning return that same day. Then turn off the radar to avoid detection, impose strict controls on communications, fuel the aircrafts with their engines running, put enemy in the air, and scatter live bombs and rockets around the deck. Now wet the whole thing down with salt water and oil, and man it with 20 year olds, half of whom have never seen an aircraft close up, power the ship with a nuclear reactor; oh and by the way…try to not kill anyone!
P14

12/2/2013
8
USN Aircraft Carrier OperationsP15
http://www.youtube.com/watch?v=1c0lfwxRpj
0
http://www.youtube.com/watch?v=gXTYQqr2i
34
CHSLI Journey to High Reliability
2009: Beginning of focused Quality restructure
System PI Dashboard with system based quality goals
Sig Sigma black belt recruited; CHSLI system Six
Sigma and Lean program training initiated.
System-wide Six Sigma initiatives began in 2010 with green belt training
Initiatives streamlined to facility-specific projects in 2012
To date, 77 employees have become certified green belts
To date, 22 system sponsored Six sigma quality programs across all
campuses
To date, 18 system sponsored Lean initiatives across all campuses
P16

12/2/2013
9
CHSLI Journey to High Reliability
2010-2011: NO Harm Campaign -> NYS Partnership for Patients • Reduce hospital-acquired conditions by 40%• Reduce preventable readmissions by 20%
NYSPFP FOCUS AREAS NURSING CENTERED INITIATIVES
• Pressure ulcers• Injuries from falls and immobility• Venous thromboembolism• Adverse drug events
INFECTION PREVENTION INITIATIVES• Catheter-associated urinary tract infections• Central line–associated bloodstream infections• Surgical site infections• Ventilator-associated pneumonia
BUILDING CULTURE AND LEADERSHIP PREVENTABLE READMISSIONS INITIATIVE OBSTETRICAL SAFETY INITIATIVE
P17
PEOPLE
High Reliability Healthcare ResourcesCHSLI Resources & Work plan
P18

12/2/2013
10
CHSLI Journey to High Reliability
2010- 2012
The Ongoing Quality Improvement Journey: Next Stop, High Reliability
Incorporated into PI structure locally and from system perspective.
Participation in NYS Partnership for Patients with goal of reducing all Harm and reducing readmissions
Soon realized we needed to take more formal approach and completely reorganized system PI->Quality Program with strategic plan and vision statement for taking active steps toward High Reliability.
Began finalization, roll out and implementation of CHS-e health EMR installation across all facilities (Epic Systems)
P19
High Reliability Healthcare/Aviation
THREE PILLARS TO SUCCESS
People (Our Pilots and Crew ->impacting our Patients/passengers)
Culture of Safety
Through NYSPFP all campuses participated with annual Culture of Safety Survey
12% improvement in participation across the system
Reward transparency and celebrate errors and near misses as opportunities
Leadership at All Levels
Patrick Scollard Award; CHSLI System annual award for leadership
HANYS Healthcare Leadership Academy
Good catch award program instituted in various forms across all campuses
P20

12/2/2013
11
High Reliability Healthcare/ Aviation
People
Our most important resource
Ongoing training and education
Expansion of simulation center
Leadership training (MBA programs, partnership with Adelphi University)
Physician and Nursing leaders
CMO’s/ CNO’s and Departmental leaders exposed to High Reliability concepts and training
BOT/CEO/CAO’s Support and educated on HRO concepts
CAO’s from all campuses part of process
C Suite performance incentives aligned with quality indicators
Good catch and quality awards structured for employees
Physician contracts (Hospitalists and ED) restructured with Quality and HCAHPS based incentives….not just RVU’s!!
P21
High Reliability Healthcare/Aviation
Process - > Robust Process Improvement (Your Flight Plan)
System InitiativesLean/ Six sigma training expansion
Facility specific workflows and processes
Change Acceleration Process trainingGE/ Harvard Business Review
2013 introductory training CHSLI PI leadership team2014 Partnership TJC Center for Transforming Healthcare
Strategic training collaboration
Development of Quality Councils (QC) (PI=Retrospective/QC=Prospective)
IHI Trigger Tools to quantify and reduce harm events
System Board PI – Quality Management Committee of the BoardClinical Excellence (Priority Focus Areas)No Harm Campaign (Priority Focus Areas)System Priority Focus Projects/ Computerized Decisional Support
P22

12/2/2013
12
IHI Trigger ToolsP23
Process->REDUCE HARM
IHI Global Trigger Tool
Department specific tools
Pharmacy – Medication management safety
OR – Procedural safety
ED – High Risk/ returns
OB/ Mother- Baby – delivery safety
IHI Expedition to start off- > Solo
Goals
Get upstream from harm
Move from RCA -> FMEA (Reactive –> Proactive)
P24

12/2/2013
13
Get Up-Stream from HarmP25
HRO..It all starts with a vision……
“Vision without action is a daydream;
action without vision is a
nightmare”…..Japanese proverb
This requires a plan….
Structure ->function
P26

12/2/2013
14
CHSLI Quality & Safety Vision Statement
and Goal
“To consistently deliver superior patient clinical outcomes
across the full continuum of care through creation of a
high-reliability culture and through embracing patient
safety as our core value.”
CHSLI’s goal:
Perform in the top 10% nationally in key quality and service indicators by 2017 through adherence of its system quality and safety plan.
27
28

12/2/2013
15
Quality Management Committee of the Board
Three System Pillars
I) Clinical Excellence
> Selected CMS / Joint Commission quality and safety measures (Priority Focus Areas or PFA’s)
• Core Measures
• PSI 90 measures
II) No Harm Campaign (Priority Focus Areas or PFA’s)
> NYSPFP select measures
• CAUTI/CLABSI/ SSI
29
Quality Management Committee of the Board
Three Pillars
III a) System Priority Focus Projects (Operational)
* projects tied to measures in other two pillars with
alignment of incentives
* quarterly updates to System QMC grid
- Surgical Safety Checklist Initiative (WHO toolkit/Life wings)
- Hand Hygiene Campaign (Joint Commission CFTH TST)
- HF Readmission Reduction(Joint Commission CFTH TST)
30

12/2/2013
16
Quality Management Committee of the
Board
III b) CHS- e Health Decisional Support and Forced Functionality(Operational)
•Hand Off Communication
•Medication Safety
•Fall Reduction
•CPOE
•Documentation improvement
•Triggers!!
P31
32
SIGN-IN TIME-OUT SIGN-OUT
Brief Prior to: STOP Prior to: Debrief Prior to:
Sedation/Induction Procedure/Incision Leaving the Procedure Room/OR
KNOW ME
Nurse:
� I would like to introduce (Patient’s Name).
� The patient’s medical record number is:
� Please tell us what surgery you are having
today.
� Please point to the area.
� I can see the site is marked.
� The consent is complete, accurate and signed.
� The patient is allergic to (medication)
Anesthesia:
� EBL (minimal or >500ml and preparation
confirmed) (adequate IV access, blood
products, fluids available).
� Airway status is (adequate or enhanced and
preparation confirmed) (equipment/assistance
available).
� Anesthesia assessment ,equipment and safety
checks complete
� Beta-Blockers (have been given or are not
needed)
� Consideration has been given for VTE
prophylaxis, Glycemic control and
Normothermia measures.
CARE FOR ME
RN/ST:
� Is everyone ready for the timeout?
� Can the Team Members please identify
themselves by name and role?
Surgeon:
� This is (patient's name)
� I am performing (proposed procedure).
� The correct site is marked and visible to me.
� Positioning is correct
� Images are (available/correctly labeled and
oriented/site &side confirmed with radiologist*)
* Confirmation with radiologist required for high
risk procedures including, but not limited to:
craniotomy, endarterectomy, pneumonectomy,
adrenalectomy, nephrectomy, amputation.
� Needed implants, devices and equipment are
available.
� I (do/do not) expect to need blood products.
� I have no special concerns at this time.
Anesthesia:
� The appropriate antibiotic(s) has (have) been
given and properly timed. Redosing plan is:
� Risk for fire is: (low or high and preparation
confirmed).
� I have no special concerns at this time.
Nurse:
� Baseline counts have been completed
� Sterilization indicators have been confirmed
� Does anyone have any questions?
� Since we are all in agreement then the “time-out”
is complete and we can proceed.
EASE MY WAY
Nurse:
� The sponge, sharps and instrument counts
(are/are not) complete and correct.
� The wound class is (wound class).
� There are (#) specimens labeled as (read
label)
� What are the key concerns for recovery and
management?
Surgeon:
� We performed a (name of procedure).
� I have no concerns at this time.
(postoperative ventilation, pain management,
nausea/vomiting, glucose control, temperature,
et al)
Anesthesia:
� The disposition for this patient is
(disposition).
� I have no concerns at this time.
(postoperative ventilation, pain management,
nausea/vomiting, glucose control, temperature,
et al)
CHSLI Surgical Safety Checklist Initiative
Checklists
Save lives!

12/2/2013
17
Clinical ExcellenceP33
No HarmP34

12/2/2013
18
Weighted indicator scoringP35
CHS Performance vs. Targets
36

12/2/2013
19
Detail
37
Significant Event Trending
38

12/2/2013
20
CHS E-Health Examples (ATC and Avionics)
Triage Triggers and Best Practice Advisories39
Safety First Best Practice Advisories
WHAT IS YOUR PERSONAL MINIMUM? 40

12/2/2013
21
Sepsis Evidence-Based Order Set
AUTOMATICALLY PRE-SELECTED 41
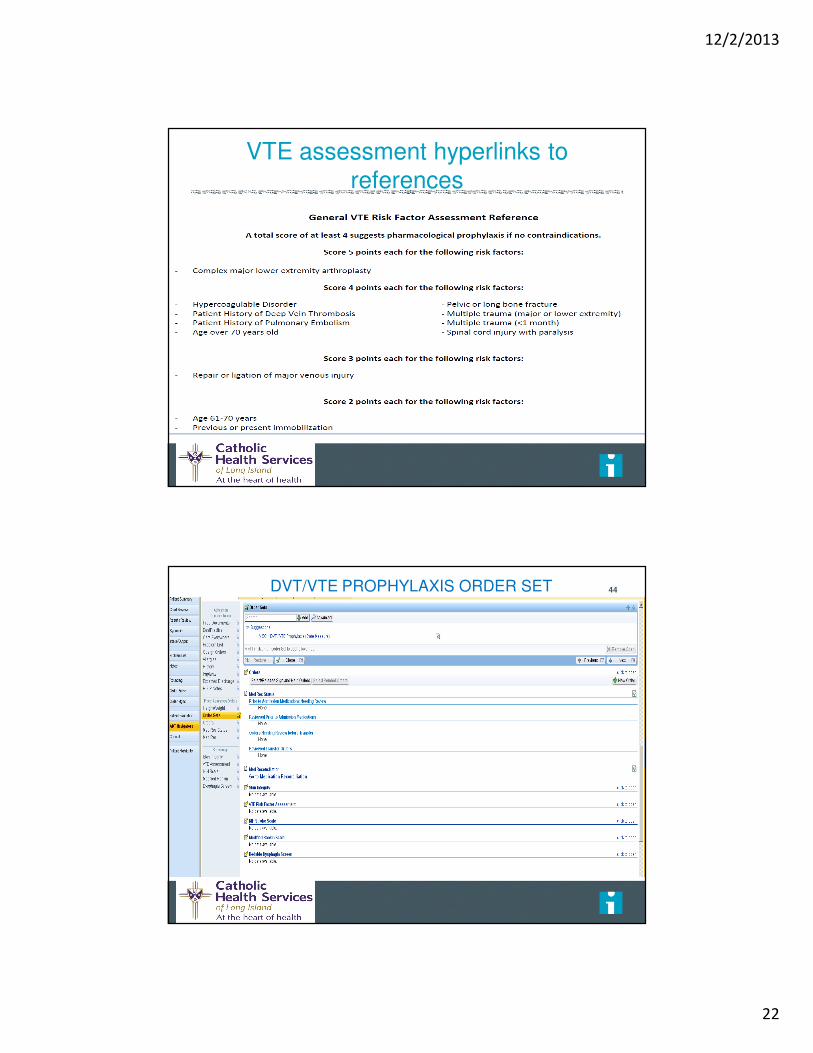
CHS E Health ExamplesVTE ASSESSMENT 42
12/2/2013
22
VTE assessment hyperlinks to
references
DVT/VTE PROPHYLAXIS ORDER SET
ISAUTOMATICALLY SUGGESTED ON ALL ADULT
PATIENTS
44

12/2/2013
23
High Risk Medication Hard StopMEDICATION MANAGEMENT SAFETY 45
Titration Soft Stop Guidance
Parameters46

12/2/2013
24
Medication Safety - Dual Verification by Pharmacists for Neonatal, Pediatrics and Chemotherapy
Medication Safety - Dual Verification (continued)

12/2/2013
25
High Risk Medication Safety
Forced Functionality
49
Barcode Medication Administration Warnings
Return to Table of Contents

12/2/2013
26
SBAR Handoff Report
SBAR Handoff Report

12/2/2013
27
Morse Fall Risk Assessment
IHI Fall Risk for Injury

12/2/2013
28
The Journey of 1000 miles………starts first with
PEOPLE…then Process…then Technology ……
The CHSLI RPI Team
P55