the importance of recognizing pathology associated with ... · gies such as ameloblastoma or ......
TRANSCRIPT
JCDA • www.cda-adc.ca/jcda • February 2006, Vol. 72, No. 1 • 41
Clinical S H O W C A S E
“Clinical Showcase” is a series
of pictorial essays that focus on
the technical art of clinical
dentistry. The section features
step-by-step case demonstrations
of clinical problems encountered
in dental practice. If you would
like to propose a case or
recommend a clinician who
could contribute to this
section, contact editor-in-chief
Dr. John O’Keefe at
The presence of either partially eruptedor fully impacted third molars oftenprompts a visit to the dental office.
Patients may experience symptomsranging from pain to mild or moderatetrismus or even acute infection withpurulence at the site of the involved tooth.In such instances, immediate treatment isoften necessary to alleviate or resolve thepatients’ presenting complaint. In the sit-uation of completely impacted thirdmolars, the clinician must make thepatient aware of the presence of theimpacted wisdom teeth and the presenceor absence of any associated pathology.The prophylactic removal of impactedwisdom teeth is often suggested to preventproblems such as infection, cariouslesions, destruction of adjacent teeth,periodontal defects involving adjacentteeth, cysts or tumours.1 Because a largenumber of wisdom teeth remain impactedor partially impacted (84%) rather thanerupting completely (16%), it is impor-tant that retained wisdom teeth be care-fully monitored for signs of pathology.2 Asa result, it is important that patientsundergo panoramic radiography as part
of the initial evaluation when third molarsymptoms are part of the chief complaint.Also, the need for proper referral ifpathology is suspected, as well as appro-priate radiographic follow-up, must berecognized.
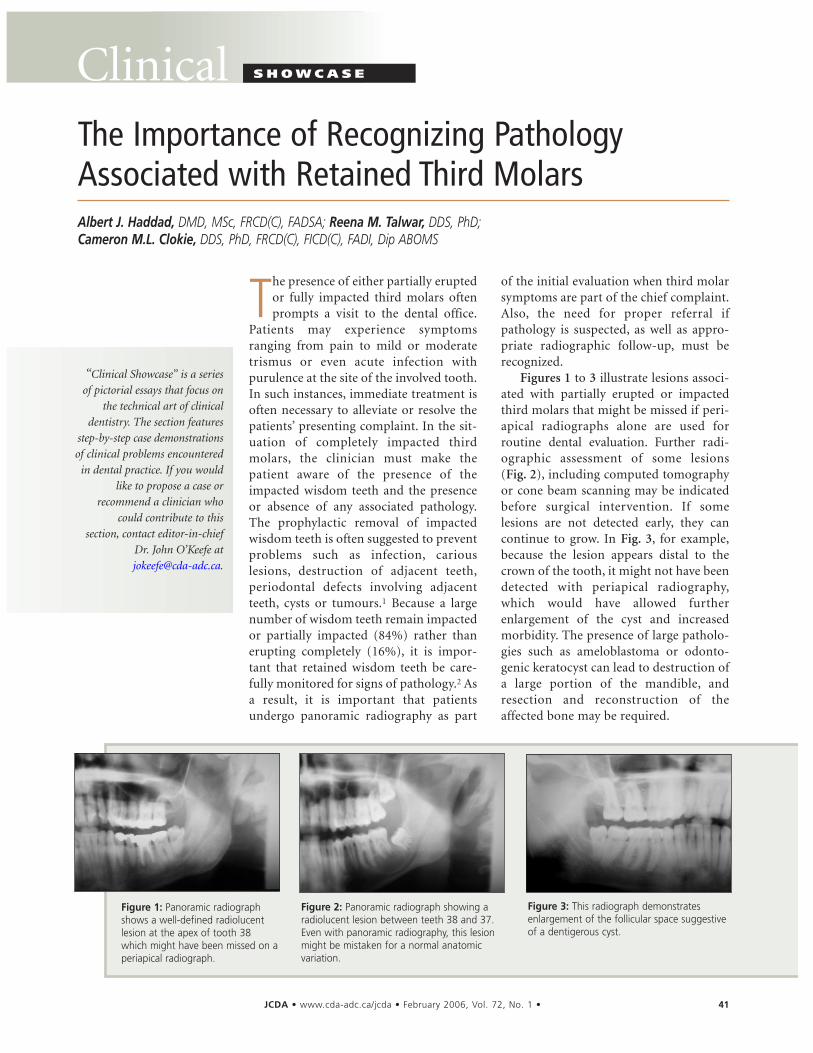
Figures 1 to 3 illustrate lesions associ-ated with partially erupted or impactedthird molars that might be missed if peri-apical radiographs alone are used for routine dental evaluation. Further radi-ographic assessment of some lesions (Fig. 2), including computed tomographyor cone beam scanning may be indicatedbefore surgical intervention. If somelesions are not detected early, they cancontinue to grow. In Fig. 3, for example,because the lesion appears distal to thecrown of the tooth, it might not have beendetected with periapical radiography,which would have allowed furtherenlargement of the cyst and increasedmorbidity. The presence of large patholo-gies such as ameloblastoma or odonto-genic keratocyst can lead to destruction ofa large portion of the mandible, andresection and reconstruction of theaffected bone may be required.
The Importance of Recognizing PathologyAssociated with Retained Third MolarsAlbert J. Haddad, DMD, MSc, FRCD(C), FADSA; Reena M. Talwar, DDS, PhD; Cameron M.L. Clokie, DDS, PhD, FRCD(C), FICD(C), FADI, Dip ABOMS
Figure 1: Panoramic radiographshows a well-defined radiolucentlesion at the apex of tooth 38which might have been missed on aperiapical radiograph.
Figure 2: Panoramic radiograph showing aradiolucent lesion between teeth 38 and 37.Even with panoramic radiography, this lesionmight be mistaken for a normal anatomicvariation.
Figure 3: This radiograph demonstratesenlargement of the follicular space suggestiveof a dentigerous cyst.

42 JCDA • www.cda-adc.ca/jcda • February 2006, Vol. 72, No. 1 •
–––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase ––––
Case ReportFigures 4 to 24 illustrate a situation in
which an abnormality associated with animpacted third molar tooth went undetectedfor several years because of a lack of appro-priate radiographic assessment. As a result, thepatient had to undergo significant surgicalresection and reconstruction.
An otherwise healthy 17-year-old womanpresented with a large radiolucent lesion of theright mandibular body and ramus, involvingthe coronoid process and sigmoid notch area.Radiographic examination revealed that tooth48 was impacted within the lesion. There wasalso evidence of radicular resorption of teeth 46and 47. Clinical examination revealed expan-sion of the mandibular body, which was pal-pable intraorally and along the inferior borderof the mandible. The examination was supple-
mented by computed tomography, whichhelped to define the extent of the pathology.
Before a definitive treatment plan was estab-lished, incisional biopsy was performed, and adiagnosis of follicular-type ameloblastoma wasconfirmed. The treatment plan included resec-tion of the mandibular ramus and body andimmediate reconstruction of a microvascularfibular flap. To help minimize functional andesthetic deficits, a 3-D acrylic model was fabri-cated preoperatively to assist in the overall sur-gical plan.
The surgical treatment involved a multidis-ciplinary approach: a plastic surgical team har-vested the fibular flap, and the mandible wasresected by the oral and maxillofacial surgeryteam. Figures 7 to 22 illustrate the step-by-stepremoval of the lesion and reconstruction of themandible.
–––– Clinical Showcase ––––
Figure 7: An incision is made around theintraoral extension of the lesion where thebiopsy was performed. Frozen sections weretaken to confirm that the soft tissues werefree of pathology.
Figure 8: The teeth anterior to the plannedresection margin are removed, as is the soft-tissue portion of the lesion to allow for clo-sure over the defect.
Figure 9: The area is sutured to pre-vent communication between theintraoral and extraoral approaches tothe mandible.
Figure 6: This photograph shows thereconstruction plate bent to repro-duce an appropriate mandibular con-tour. The expansion of the mandibularbody at the site of the abnormalitycan also be appreciated in this view.
Figure 5: This mirror-image model allowedfor prebending of the reconstruction plate,which was needed for fixation of the vascu-larized fibular flap to the native mandible.
Figure 4: Impacted tooth 48 is apparentwithin a large radiolucent lesion of the rightmandibular body and ramus. There is also evi-dence of radicular resorption of teeth 46 and47.
–––– Clinical Showcase ––––

JCDA • www.cda-adc.ca/jcda • February 2006, Vol. 72, No. 1 • 43
–––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase –––––––– Clinical Showcase ––––
Figure 11: The fibula is harvested through alateral approach while the mandible is beingresected.
Figure 10: The mandible is placedinto intermaxillary fixation to preventpostoperative malocclusion after themandibular reconstruction.
Figure 13: The platysma muscle isexposed through the submandibularapproach to the mandibular body.Careful dissection is necessary to pro-tect the mandibular portion of thefacial nerve as well as the facialartery and vein.
Figure 14: The mandible is exposed and themental nerve identified as it exits the mentalforamina (arrow). The nerve will be sectionedand marked to allow for repair after themandibular resection.
Figure 15: An anterior resection osteotomy iscreated to allow removal of the affectedramus and body.
Figure 12: Landmarks are identified to protectstructures such as the marginal mandibularbranch and the temporal branch of the facialnerve.
Figure 17: A digital radiograph of the spec-imen after its removal.
Figure 18: The fibula is harvested with thevascular pedicle intact (arrow).
Figure 16: A medial view of theresected specimen shows expansionof the mandibular body and obliteration of the coronoid processand sigmoid notch.
44 JCDA • www.cda-adc.ca/jcda • February 2006, Vol. 72, No. 1 •
–––– Clinical Showcase ––––
DiscussionProper assessment of retained third molars,
especially when local symptoms are present,should include a comprehensive clinical andradiographic evaluation. Obtaining apanoramic radiograph at the time of initialevaluation is highly recommended. The limita-tions of periapical radiography in assessingpartially or fully impacted third molarsinclude, but are not limited to, the inability toproperly assess the relationship of the tooth tothe inferior alveolar nerve canal, the limitedability to evaluate the morphology of the thirdmolar root and the inability to detect abnor-
malities associated with the tooth or teeth inquestion.
It is the responsibility of the clinician toproperly diagnose and manage any pathlogyassociated third molars that are removed. Inthe case of local pericoronal or periapicallesions associated with impacted third molars,removal of the tooth and biopsy of the soft-tissue lesion should be performed simultane-ously. If there is suspicion of a more aggressivepathologic process, appropriate referral shouldbe considered. In this situation, the patientshould be made aware of the clinical findings,the various treatment modalities available andthe overall prognosis. C
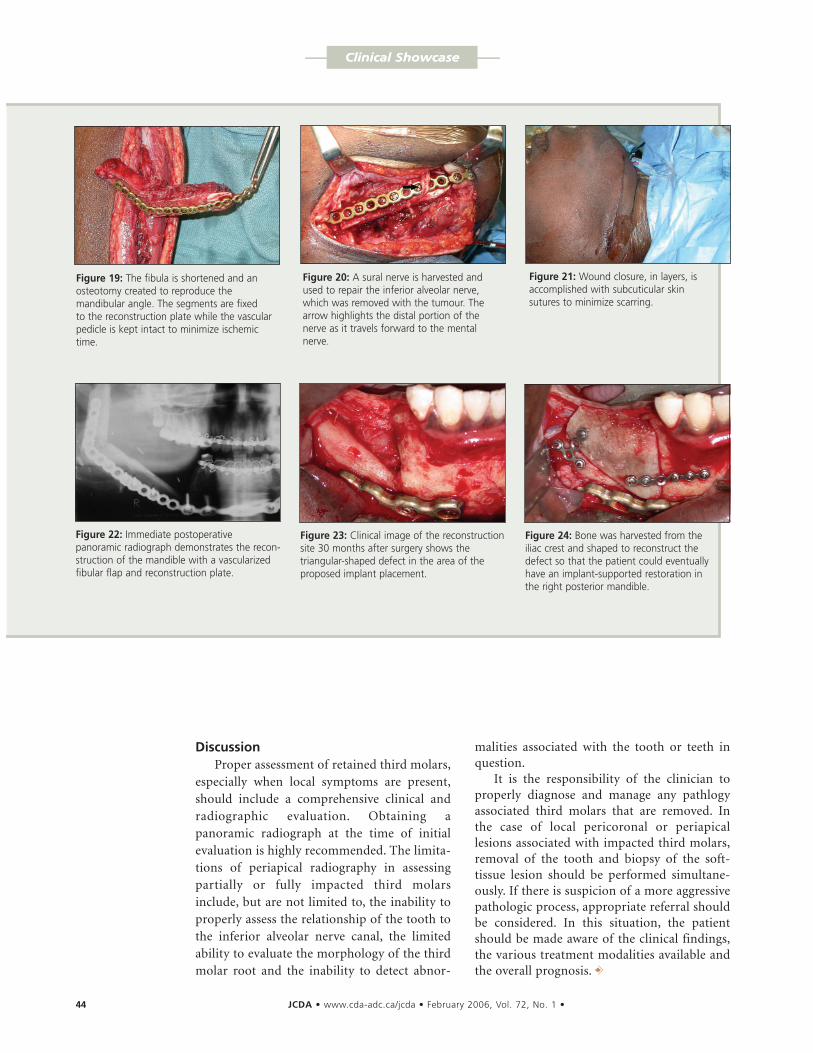
Figure 19: The fibula is shortened and anosteotomy created to reproduce themandibular angle. The segments are fixed to the reconstruction plate while the vascularpedicle is kept intact to minimize ischemictime.
Figure 20: A sural nerve is harvested andused to repair the inferior alveolar nerve,which was removed with the tumour. Thearrow highlights the distal portion of thenerve as it travels forward to the mentalnerve.
Figure 21: Wound closure, in layers, isaccomplished with subcuticular skinsutures to minimize scarring.
Figure 22: Immediate postoperativepanoramic radiograph demonstrates the recon-struction of the mandible with a vascularizedfibular flap and reconstruction plate.
Figure 23: Clinical image of the reconstructionsite 30 months after surgery shows the triangular-shaped defect in the area of the proposed implant placement.
Figure 24: Bone was harvested from theiliac crest and shaped to reconstruct thedefect so that the patient could eventuallyhave an implant-supported restoration inthe right posterior mandible.
–––– Clinical Showcase ––––

References1. Knutsson K, Brehmer B, Lysell L, Rohlin M. Pathoses associatedwith mandibular third molars subjected to removal. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1996; 82(1):10–7.
2. Venta I, Murtomaa H, Ylipaavalniemi P. A device to predictlower third molar eruption. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1997; 84(6):598–603.
JCDA • www.cda-adc.ca/jcda • February 2006, Vol. 72, No. 1 • 45
–––– Clinical Showcase –––––––– Clinical Showcase ––––
Dr. Haddad is in private practice in Toronto,Ontario. He is an associate in dentistry, disci-pline of oral and maxillofacial surgery, at thefaculty of dentistry, University of Toronto,Toronto, Ontario.
Dr. Talwar is an assistant professor, discipline oforal and maxillofacial surgery, at the faculty ofdentistry, University of Toronto, Toronto,Ontario.
Dr. Clokie is a professor and head of oral andmaxillofacial surgery at the faculty of dentistry,University of Toronto, Toronto, Ontario.
THE AUTHORS Correspondence to: Dr. Cameron Clokie, Oral andMaxillofacial Surgery, Faculty of Dentistry, University ofToronto, 124 Edward St., Toronto, ON M5G 1G6. Email:[email protected].
The authors have no declared financial interests.
Dr. Clokie’s full-day session at the ODA annual meeting,titled “Oral surgery for the general practitioner”, will be pre-sented on Friday, April 7.