the health of latino communities in the south: challenges and opportunities
DESCRIPTION
The Health of Latino Communities in the South: Challenges and OpportunitiesTRANSCRIPT

NCLRNATIONAL COUNCIL OF LA RAZA
The Health of LatinoCommunities in the South:
Challenges and Opportunities
Report on the Findings of theNational Council of La Raza Institute for Hispanic Health’s
Health in Emerging Latino Communities ProjectFunded by the Department of Health and Human Services – Office of Minority Health
THE HEALTH OF LATINO
COMMUNITIES IN THE SOUTH:CHALLENGES AND OPPORTUNITIES
Report on the Findings of the National Council of La Raza Institute for Hispanic Health’s
Health in Emerging Latino Communities ProjectFunded by the Department of Health and Human Services – Office of Minority Health
National Council of La Raza100 Peachtree Street, NW
Suite 700Atlanta, GA 30303
(404) 658-1711
www.nclr.org
© 2004
Final Version

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
ACKNOWLEDGMENTSi
This report was a collaborative effort of staff of the National Council of La Raza (NCLR) Institute forHispanic Health and Office of Research, Advocacy, and Legislation. Carlos Ugarte, Deputy VicePresident for Health, and Sonia M. Pérez, Deputy Vice President for Research, were the report’s
editors. Liany Elba Arroyo conducted the research and was the principal author of the report.
In addition, the following NCLR colleagues contributed to the publication of the report:
� Jennifer Kadis, Editor, provided expert editorial guidance and prepared the report for publication.
� Magdalena Lezama, Production Assistant, designed and prepared the report’s layout and cover.
The author would like to thank the following individuals and organizations for their cooperation, support,and assistance in conducting this research:
� Patty Alleman-Velez, University of Alabama – School of Public Health
� Dr. Jorge Atiles, University of Georgia
� El Pueblo, Inc., Raleigh, NC
� Latin American Association, Atlanta, GA
� Latino Memphis, Memphis, TN
� Southeast Georgia Communities Project
The research and preparation of this report was made possible by funding from the Department of Healthand Human Services – Office of Minority Health. The final content of the report, as well as errors of logicand fact, is the sole responsibility of NCLR.
Permission to copy, disseminate, or otherwise use information from this report is granted, as long asappropriate credit is given to NCLR.
ACKNOWLEDGMENTS

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
TABLE OF CONTENTS
Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .i
Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Study Design . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
Descriptive Statistics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
Summary of Focus Group Responses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14
Summary of Key Informant Responses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16
Summary of Previous Assessment Findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18
Key Findings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .20
Recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
Appendices . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .24
TABLE OF CONTENTS
NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
EXECUTIVE SUMMARY1
EXECUTIVE SUMMARY
Latino activists and leaders in the South alreadyknow: new Latino communities are establishingroots in the Deep South and Latinos are no longerconcentrated in "traditional" cities and states, likeLos Angeles or Florida.
The growth of the Latino population innontraditional immigrant areas of the U.S., whilenoted by some, took many others by surprise in thelate 1990s and early 2000s, although evidenceexisted that Latinos had settled in the South priorto the release of the 2000 Census. The Latinopresence was felt in area schools in the mid-1990swhen some states nearly doubled the percentage ofLatino students between 1990-1991 and 1996-1997.During that time, Georgia experienced an increasein its percentage of Latinos in public elementaryand secondary schools, from 1.5% to 2.6% of totalenrollment, while North Carolina’s Latino studentpopulation expanded from 1.1% to 2.3% of totalenrollment.5 Likewise, the Latino presence was feltin the agro-industrial sector. In South Carolina,Latinos held 20% of the state’s jobs in the meatindustry despite only officially numbering 41,000people out of a population of 3.7 million.6
The increased attention given to the growingLatino population in the South has brought with ita focus on the barriers Latinos face, particularly inthe area of health care. These population increasesalso challenged an infrastructure that had notplanned or was prepared to deal with a largenumber of newcomers who had specific needs.Uninsurance, immigration status, and languagebarriers long faced by more traditional Latinoimmigrant-receiving states like California, NewYork, and Texas became especially serious barriersfor Latinos in states that were not accustomed todealing with Latinos or immigrant populations.The combination of these factors prompted NCLRand OMH to develop the HELC project.
Overview
The significant increase in the U.S. Hispanic*
population, particularly in nontraditionalregions of the country, such as the South,
has not necessarily been accompanied byproportional increases in information aboutLatinos, their characteristics, and their needs. Toaddress the knowledge gap about this diversepopulation and focus attention on the health carechallenges that the Hispanic community in theSouth faces, the National Council of La Raza(NCLR) and the Department of Health and HumanServices – Office of Minority Health (OMH)partnered to create the "Health in Emerging LatinoCommunities" (HELC) project to assess, for thefirst time, the health care needs, wishes, andrealities of newly emerging Latino communities inthe South.**
The following offers a brief snapshot of relevantdemographic data, a summary of the project, keyfindings, and NCLR conclusions.
A New Demographic Reality
Latino migration to the South in the 1990s wentvirtually unnoticed until the release of the 2000Census data, which showed the tremendous growthof the Hispanic population in many states acrossthe region. For example, from 1990 to 2000, theproportion of the population in Georgia that isLatino grew from 1.7% to 5.3%.1 In NorthCarolina, the community grew to 4.7% of thepopulation in 2000 from just 1.2% ten yearsearlier.2 Specific city data show similar signs ofexpansion. Recent Census estimates found that theLatino community in the metropolitan Atlanta areahas grown 30%,3 and Nashville has experienced a21% surge in its Latino population in just threeyears.4 The 2000 Census and recent Censusestimates serve as confirmation of what many
* The terms "Hispanic" and "Latino" are used interchangeably by the U.S. Census Bureau and throughout this report to identifypersons of Mexican, Puerto Rican, Cuban, Central and South American, Dominican, and Spanish descent; they may be of any race.
** According to the Census, the South includes the states of Alabama, Florida, Georgia, Kentucky, Louisiana, Mississippi, NorthCarolina, South Carolina, Tennessee, Virginia, and West Virginia.
NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
EXECUTIVE SUMMARY
school. The rural group had the lowesteducational level with no participantshaving completed beyond the sixth grade.
◗ Of the employed participants, 31.6% wereemployed in the service sector followed by26.3% in manufacturing.
◗ More than two in five (42%) participantshad either private or government-sponsored insurance. Of note is that morethan two-thirds (68.2%) of North Carolinafocus group participants had insurance,while the number of insured was relativelylow for the other states.
All focus groups were completed by the same NCLRstaff member and tape-recorded.
● Key informant interviews with health careprofessionals who work with Latinos. EachCBO also identified three to five individuals forkey informant interviews. Eighteen keyinformant interviews were completed duringthe course of the needs assessment in all fourareas in which the CBOs were located, as wellas in Birmingham, Alabama. Key informantswere from rural and urban areas. They workedas doctors, health educators, programcoordinators, mental health counselors, andmedical interpreters. Half of the interviewswere conducted in English and the other halfin Spanish. Two-thirds (66%) of the keyinformants were women. The average age ofthe key informants was 42.3 and the medianage was 39. More than half (56%) citedSpanish as their primary language. Half ofthose interviewed were born in the UnitedStates. Eleven of the key informants provideddirect services to Latino clients, while theremaining seven key informants were inmanagement positions with their organizationsor helped to design or manage programs forthe CBOs. With the exception of two keyinformants, all worked at agencies thatprovided some social, educational, or directservice to Latino clients in their area. The
Project Summary
The HELC project consisted of:
● Focus groups with community members.These discussions were coordinated by fourcommunity-based organizations (CBOs) whowere selected to partner with NCLR based oncommunity reputation, reach of theorganization in the community, its urban/rurallocation, prior work in the health care field,and a previous relationship with NCLR. Thefour sites selected were: Latino Memphis(Memphis, TN); El Pueblo, Inc. (Raleigh, NC);Latin American Association (Atlanta, GA); andSoutheast Georgia Communities Project(Lyons, GA). Each focus group consisted ofeight to ten adult clients (age 18 and over) whoagreed to participate in the discussion; this wasnot a random sample and not necessarilyrepresentative of the Latino community of theSouth. A summary of focus group andparticipant characteristics shows that:
◗ There were 50 focus group participants: 24women and 26 men.
◗ Four focus groups were mixed gender andtwo were single sex.
◗ The average age of all participants whoresponded to the question was 35.3.
◗ Close to 75% of the participants weremarried or living with a partner.
◗ Spanish was the primary language of 98%of participants.
◗ Nine in ten (92%) participants wereforeign-born, and half of those were fromMexico.
◗ Four of the participants were born in theUnited States or its territories, includingPuerto Rico.
◗ Three-quarters (73%) of participants hadsome education beyond the eighth grade,were attending, or had attended high
2

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
EXECUTIVE SUMMARY
services. Reasons ranged from lack ofknowledge of available resources, lack ofinterpreters, lack of insurance, lack of trust inthe medical system, and immigration status (i.e.,not being legally present in the United States).Focus group participants and key informantscited use of over-the-counter medicines, homeremedies, and the emergency room as methodsof care used by Latinos who do not seek out orknow of available sources of health care.Participants in the focus group and interviewsmentioned that Latinos receive differenttreatment by health care staff. Specifically, theynoted that Latinos experience longer waits andare denied services due to language barriers, lackof insurance, and lack of cultural understandingon the part of providers and their staff.
● Spanish-language media is the best means todistribute information to the Latinocommunity. The majority of respondents statedthat, while most Latinos get information abouthealth services in their community by word ofmouth, the Spanish-language media was thebest method to reach the Latino community.Word of mouth was also mentioned as a meansto share information in relation to door-to-dooroutreach efforts. Previous local assessmentssupported this finding.
● The primary barrier to accessing health care isrelated to language and communication issues.The barrier most often cited by Latinos whenaccessing health care is limited Englishproficiency and difficulty communicating withhealth care personnel. Focus group respondentswere aware of a law requiring interpreters butfelt that providers did not always follow the law.While other barriers such as lack of insurance,lack of transportation, and in some casesdiscriminatory behavior by health care staff werementioned, all respondents and previousassessments felt that language challenges werethe biggest barrier faced by Latinos.
remaining two informants worked atorganizations that conducted research andprovided public information and advocacy.
In total, 16 different agencies were represented. Eightof the organizations represented provided servicesonly to Latinos while the remaining eight providedservices to everyone. However, while they providedservices to everyone, five had a majority of Latinoclients or offered some services only in Spanish.
● A literature review of previous assessments***
on Latino health and Latino health statistics.NCLR staff gathered and reviewed prior needsassessments and health reports from Alabama,Tennessee, North Carolina, and Georgia tosupplement information obtained from thefocus groups.
● A meeting with key stakeholders fromthroughout the South was convened to gatheradditional perspectives and validate theassessment’s findings.
Key Findings
The focus groups answered questions in threemajor areas: use of existing services by Latinos,barriers to obtaining health care services, and thegap between what is needed and what is currentlyavailable. A fourth area of questions concerningdiscrimination was added if the focus groupbrought up differential treatment as an issue. Thefollowing are the key themes that emerged fromthe focus groups and key informant interviews.
● Latinos are reluctant to use available sources ofhealth care and are treated differently from otherpatients when accessing care. While focus groupparticipants and key informants were not incomplete agreement over whether the majorityof Latinos used existing services, there is aperception by focus group participants – whichis reinforced by some of the other assessments –that Latinos do not use available health care
3***For a complete listing of the previous assessments, please see the full report.

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
EXECUTIVE SUMMARY
than reactively to ensure that health providers hadthe resources and information needed to complywith the law. Its work can be used as a model forother southern states.
Nonprofit Organizations:
● Local nonprofits should create a regionalPromotores de Salud Institute.
The Institute would train local CBOs on how todevelop promotores programs and on the latestcommunity health education techniques. Theseprograms provide a vehicle for using localcommunity resources to educate the largercommunity about health issues.† The Institutewould also conduct train-the-trainers sessions soCBOs could train their own promotores in theirlocal area. In order to address the larger issue ofaccess, the training would include information onthe rights of citizens and noncitizens to accessservices as well as general information on the U.S.health care system.
Professional Medical Associations:
● Medical professionals should create a culturalcompetency curriculum for distribution tomedical and allied health schools in theSouth. In addition, doctors’ associationsshould offer continuing education coursesdealing with cultural competency to ensurethat all doctors have an opportunity toincrease their knowledge of culturally andlinguistically diverse populations.
Although the number of Latinos in the Southcontinues to climb, the number of Latino healthcare professionals is not keeping pace with thisgrowth.7 Therefore, it is important to ensure thatyoung medical professionals and new graduates inthe South are adequately prepared to deal with thechanging demographics in this region. To help inthis effort, the government and nonprofit sectorsshould collaborate to develop a curriculum that
Recommendations
Based on the findings of the HELC project, theNational Council of La Raza Institute for HispanicHealth recommends the following:
Government Agencies:
● Federal and state governments should create ahealth awareness and education publicservice/information campaign specific to theSouth.
The federal government should work inconjunction with state and local healthdepartments, CBOs, and local media outlets todesign and implement a comprehensive media-based campaign that provides information on localservices available to listeners, viewers, and readers.The campaign should include information ondiseases and illnesses that affect Latinosdisproportionately, information on the rights ofimmigrants to access services, and information onlocal clinics.
● Federal, state, and local governments andhealth insurers should establish and fundmechanisms through which appropriatelanguage services are available when needed.In addition, recipients of federal funds must beaccountable for providing language services asrequired under Executive Order 13166 and TitleVI of the Civil Rights Act of 1964. The Office forCivil Rights (OCR) should increase its efforts tomonitor and enforce Title VI violations relatedto language access and discrimination.
A mechanism should be established between theOffice for Civil Rights, state and local healthdepartments, and local CBOs, which would allowfor the reporting and investigation of suspectedTitle VI violations before a noncompliance order isissued. In North Carolina, El Pueblo, Inc. workedwith the state health department proactively rather
4
† For a full description and models of promotores programs, see "Promotores Energizing Communities for Heart Health:Findings from the Salud Para Su Corazón Implementation Projects" by the National Heart, Lung, and Blood Institute, theNational Council of La Raza, and the University of North Texas – School of Public Health, July 2002.
NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
EXECUTIVE SUMMARY
Similarly, Latino CBOs and individuals shouldnetwork with existing services and communityleaders to continue to express their needs,wishes, and demands, and to advocate for equalaccess to and fair treatment from healthservices.
● Use existing resources to publicize informationand services. Spanish- and English-languagemedia should play a role in highlighting thecontributions, strengths, and needs of thegrowing Latino population in the South, aswell as highlight and disseminate informationthat points to solutions and successes.
Ensuring the integration of Latinos into the socialfabric of the South United States will require ashared effort among service providers, government,and the Latino community. As demographicchanges suggest, the health and status of Hispanicsin the South will increasingly be tied to andinfluence the overall well-being of the region.NCLR believes that the recommendations outlinedabove to improve health care access and care arewithin reach and is hopeful that service providers,government, CBOs, and Latinos themselves willwork in partnership to ensure fair treatment,quality services, and healthy outcomes for Latinochildren, families, and all residents in the South.
addresses Latino cultural beliefs but also theunique situation in the South. This curriculumshould be adapted and offered as a course forcontinuing education credits so that currentproviders can increase their knowledge andimprove their treatment of their diverse clients.
The Latino Community:
NCLR believes that the Latino community also hasa role to play in improving service delivery andoutreach and focusing policy-maker attention onhealth issues of importance to Latinos in theSouth. In particular, the Latino communityshould:
● Increase education and public awarenessefforts related to health issues. Latinos shouldbecome as informed as possible about thehealth conditions affecting them and theirfamilies, and the community at large, andshare this information with the broadercommunity to begin to take steps to improvetheir well-being.
● Participate in health forums and fairs that maybe sponsored by "mainstream" organizations intheir community to represent the realities andneeds of Latinos as a growing and importantcitizenry of the South, and increase the voiceand presence of Latino families in this region.
● Share information and research. NCLR, othernonprofits, CBOs, and researchers shoulddistribute and promote widely the findings ofthis report and other related research insideand outside the community to raise awarenessand promote change.
● Coordinate efforts between Latino andmainstream service providers and resources toenhance health advocacy. Existing Latino orLatino-serving "gatekeeper" organizationsshould coordinate efforts and mobilizetraditionally "mainstream" national healthorganizations to create the environment anddedicate resources within their ownorganizations to become part of the solution.
5

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
EXECUTIVE SUMMARY
1. U.S. Census Bureau, The Hispanic Population:Census 2001 Brief,http://www.census.gov/prod/2001pubs/c2kbr01-3.pdf
2. Ibid.
3. Scott, Jeffry, "Influx of Hispanics, Asians marksmetro area’s growth," The Atlanta JournalConstitution, August 26, 2004.
4. Wadhwani, Anita, "Nashville area leads state inHispanic population growth," The Tennessean,August 28, 2004.
5. Torres, Cruz, "Emerging Latino communities:A new challenge for the rural South." August2000.
6. Butler, Pat, "Hispanics add another thread toSouth Carolina’s cultural fabric: Immigrantpopulation outpaces state’s general growth,"The State. April 18, 1998.
7. PR Newswire, "Commission addressesunderrepresentation of minority healthprofessionals," Hispanic Business.http://www.hispanicbusiness.com/news/newsbyid.asp?id=12367, September 5, 2004. AccessedSeptember 9, 2004.
6
ENDNOTES

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
BACKGROUND
a focus on the barriers Latinos face, particularly inthe area of health care. The growth of the Latinopopulation in nontraditional immigrant areas ofthe U.S., while noted by some, took many others bysurprise in the late 1990s and early 2000s andchallenged an infrastructure that had not plannedor was prepared to deal with a large number ofnewcomers who had specific needs. Uninsurance,immigration status, and language barriers longfaced by more traditional Latino immigrant-receiving states like California, New York, andTexas became especially serious barriers for Latinosin states that were not accustomed to dealing withLatinos or immigrant populations.
As the Latino community grew the challenges inserving this diverse population also grew, andgreater information and insight was neededregarding the characteristics of the population andthe challenges that the Hispanic community in theSouth faced. In 2001, the National Council of LaRaza (NCLR) and the Department of Health andHuman Services – Office of Minority Health (OMH)partnered to create the "Health in Emerging LatinoCommunities" (HELC) project to assess, for thefirst time, the health care needs, wishes, andrealities of newly emerging Latino communities inthe South. Previous assessments were either state-or county-based and did not compare thechallenges across state lines.
To accomplish this goal, the project worked withfour Latino community-based organizations(CBOs) in the South to conduct focus groups withcommunity members and key informant interviewswith individuals currently working with Latinos inthe health care arena. Prior needs assessmentreports on Latino health and Latino healthstatistics were also collected in order to comparefindings with data obtained from the focus groupsand interviews.
Hispanic* migration to the South in the 1990swent virtually unnoticed until the release ofthe 2000 Census data, which showed the
tremendous growth of the Hispanic population inmany states across the South.** For example, from1990 to 2000, the proportion of the population inGeorgia that is Latino grew from 1.7% to 5.3%.1
In North Carolina, the community grew to 4.7% ofthe population in 2000 from just 1.2% ten yearsearlier.2 Specific city data show similar signs ofexpansion. Recent Census estimates found that theLatino community in the metropolitan Atlanta areahas grown 30%,3 and Nashville has experienced a21% surge in its Latino population in just threeyears.4 The 2000 Census and recent Censusestimates serve as confirmation of what manyLatino activists and leaders in the South alreadyknow: new Latino communities are establishingroots in the Deep South and Latinos are no longerconcentrated in "traditional" cities and states, likeLos Angeles or Florida.
Despite the surprise felt by many in the Southconcerning this growth, evidence existed thatLatinos had settled in the South prior to therelease of the 2000 Census. The Latino presencewas felt in area schools in the mid-1990s whensome states nearly doubled the percentage ofLatino students between 1990-1991 and 1996-1997.During that time, Georgia experienced an increasein its percentage of Latinos in public elementaryand secondary schools, from 1.5% to 2.6% of totalenrollment, while North Carolina’s Latino studentpopulation expanded from 1.1% to 2.3% of totalenrollment.5 Likewise, the Latino presence was feltin the agro-industrial sector. In South Carolina,Latinos held 20% of the state’s jobs in the meatindustry despite only officially numbering 41,000people out of a population of 3.7 million.6
The increased attention given to the growingLatino population in the South has brought with it
7
BACKGROUND
* The terms "Hispanic" and "Latino" are used interchangeably by the U.S. Census Bureau and throughout this report to identifypersons of Mexican, Puerto Rican, Cuban, Central and South American, Dominican, and Spanish descent; they may be of any race.
** According to the Census, the South includes the states of Alabama, Florida, Georgia, Kentucky, Louisiana, Mississippi, NorthCarolina, South Carolina, Tennessee, Virginia, and West Virginia.

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
STUDY DESIGN
participants were selected by the CBOs from theirpool of clients. The sample was a conveniencesample and thus not necessarily representative ofthe Latino community of the South. The focusgroups were originally planned as single-gendergroups; however, several CBOs felt that havingboth genders participate in the same focus groupwould not inhibit participation from individuals.Only one site, Latino Memphis, held single genderfocus groups. In addition, El Pueblo had one focusgroup with more than ten participants, andSoutheast Georgia Communities Project’s focusgroup had four participants.
The same NCLR staff person, using a focus groupguide designed in conjunction with a consultant,conducted all focus groups. All focus groups weretape-recorded. For their participation in the HELCproject, each site was given a grant to coveremployee time, focus group participant stipends,and refreshments for the day of the focus group.
Key informant interviews took place in all fourareas in which the CBOs were located in additionto Birmingham, Alabama. All key informants wereover age 18, involved in the health field, andworking with Latinos. Key informants were fromrural and urban areas. They worked as doctors,health educators, program coordinators, mentalhealth counselors, and medical interpreters.
Once all the focus groups and key informantinterviews were completed, a contractortranscribed the data. However, the women’s focusgroup in Memphis was not transcribed as the tape,upon review by the transcriber, was inaudible. Thedata from this group were obtained using the focusgroup moderator’s notes.
Prior needs assessments and health reports weregathered from Alabama, Tennessee, North Carolina,and Georgia. Focus groups and interviews wereconducted from April 2003 through August 2003 withreport-gathering continuing through the end of theyear. All individuals were asked to sign an informedconsent form and a Participant Information sheetprior to the start of the focus group or interview.
Additionally, a meeting to convene keystakeholders – service providers, elected officials,and agency heads – from throughout the regionwas also held as part of the project. The meeting’spurpose was to provide feedback, serve as anexternal mechanism to validate the report’sfindings, and seek input on strategies to addressthe concerns highlighted in the report. Themeeting agenda, participants and their affiliations,as well as a summary of their comments andrecommendations are included as Appendix A, B,and C, respectively.
The assessment was intended to be a snapshot ofthe needs of Latinos in the South. Although thefinal sample size was small, its findings were foundto be representative of the concerns of the regionas supported by the attendees of the meeting. Theattendees represented 19 organizations with aclient base of thousands of individuals fromthroughout the region.
STUDY DESIGNSite Selection
Selection of CBOs that would collaborate on theproject was based on community reputation, reachof the organization in the community, urban/rurallocation, prior work in the health care field, andprevious relationship with NCLR. Based on thesecriteria, four CBOs were selected to participate inthe needs assessment. The four sites selected were:Latino Memphis (Memphis, TN); El Pueblo, Inc.(Raleigh, NC); Latin American Association (Atlanta,GA); and Southeast Georgia Communities Project(Lyons, GA). The Southeast Georgia CommunitiesProject allowed for collection of data from a ruralcommunity.
Data Collection
Each site arranged one or two single-gender focusgroups with eight to ten adult clients (age 18 andover) and assisted in identifying three to fiveindividuals for key informant interviews. The
8

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
DESCRIPTIVE STATISTICS
Focus Groups
Between April and June six focus groups in threestates were completed. A total of 50 individualsparticipated in the focus groups. All six focusgroups were conducted in Spanish.
North Carolina
Two mixed-gender focus groups of ten and 12participants were conducted in April 2003. Thefirst focus group had four women and six men.The second focus group had five women and sevenmen. Each focus group contained participantsfrom throughout the state. The average age of thefocus group participants was 34.6. The average ageof the men was 35.3 and the average age of thewomen was 33.6. The majority of the participantswere married (15). Two were living with a partner,three were divorced or separated, one was widowed,and one was single. Twenty-one (95.5%) citedSpanish as their primary language. Oneparticipant did not answer the language question.
The countries of birth varied in the focus groups.Seven participants were born in Mexico, whilethree were born in the United States, including onein Puerto Rico. Colombia and Argentina were thecountries of birth for three participants each.Venezuela and the Dominican Republic were thecountries of birth for two participants. Guatemalaand Peru were the countries of birth for oneparticipant each. The average length of time in theU.S. for all participants not born in the U.S. was6.2 years (including the participant born in PuertoRico). Length of time in the U.S. ranged from sixmonths to 17 years not including those born onthe United States mainland. All participants livedin the U.S. year-round.
9
DESCRIPTIVE STATISTICS
NUMBER OFCOUNTRY PARTICIPANTS
Argentina 3
Colombia 3
Dominican Republic 2
Guatemala 1
Peru 1
Mexico 7
United States (including Puerto Rico) 3
Venezuela 2
NUMBER OFEMPLOYMENT STATUS PARTICIPANTS
Employed 19
Unemployed 3
Nineteen of the participants were employed at thetime of the focus groups. Their occupationsranged from manufacturing to paraprofessionaland professional work, such as vocationalrehabilitation and teaching at a local communitycollege and a Head Start program. The majority ofthe participants were occupied in paraprofessionalroles followed by manufacturing work. Two menand one woman were not employed at the time ofthe focus groups.
Employment Status – NC
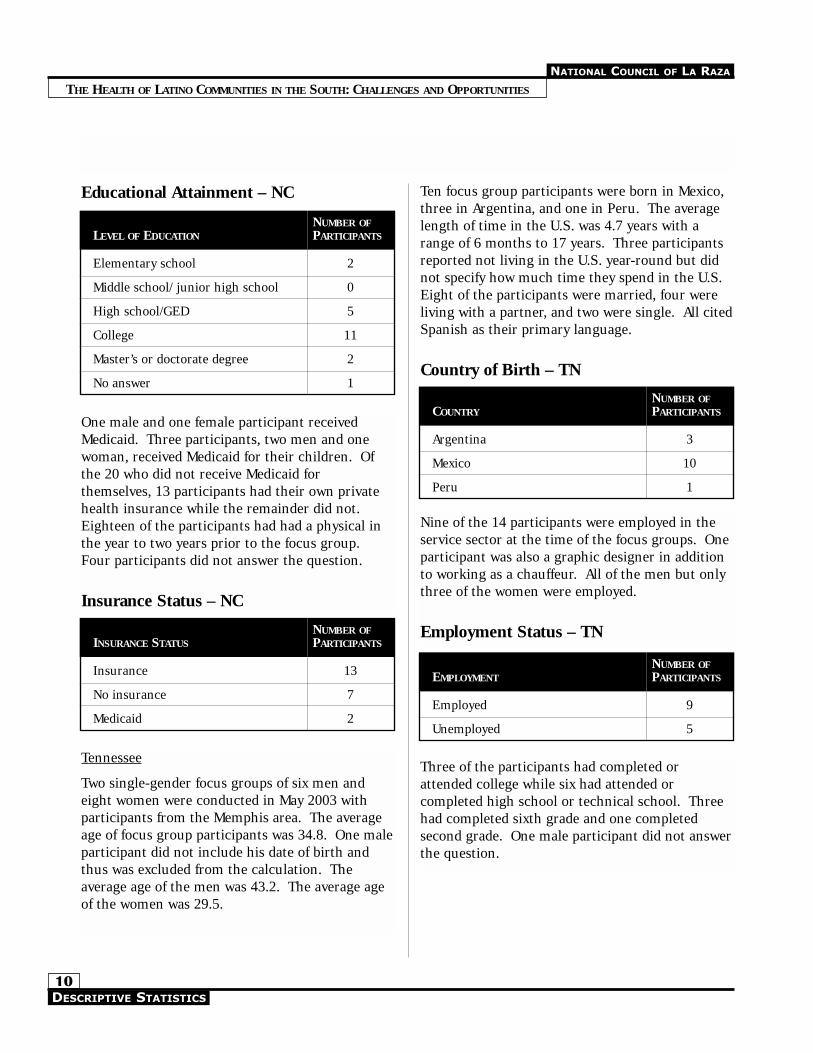
Eleven participants had completed, attended, orwere currently attending college. One participanthad a master’s degree and another had a doctorate.Five had completed or attended high school or arecurrently completing a GED. Two had only anelementary school education and one did notanswer the education question.
Country of Birth – NC
NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
Ten focus group participants were born in Mexico,three in Argentina, and one in Peru. The averagelength of time in the U.S. was 4.7 years with arange of 6 months to 17 years. Three participantsreported not living in the U.S. year-round but didnot specify how much time they spend in the U.S.Eight of the participants were married, four wereliving with a partner, and two were single. All citedSpanish as their primary language.
Country of Birth – TN
Educational Attainment – NC
10
NUMBER OFLEVEL OF EDUCATION PARTICIPANTS
Elementary school 2
Middle school/ junior high school 0
High school/GED 5
College 11
Master’s or doctorate degree 2
No answer 1
NUMBER OFINSURANCE STATUS PARTICIPANTS
Insurance 13
No insurance 7
Medicaid 2
One male and one female participant receivedMedicaid. Three participants, two men and onewoman, received Medicaid for their children. Ofthe 20 who did not receive Medicaid forthemselves, 13 participants had their own privatehealth insurance while the remainder did not.Eighteen of the participants had had a physical inthe year to two years prior to the focus group.Four participants did not answer the question.
Insurance Status – NC
Tennessee
Two single-gender focus groups of six men andeight women were conducted in May 2003 withparticipants from the Memphis area. The averageage of focus group participants was 34.8. One maleparticipant did not include his date of birth andthus was excluded from the calculation. Theaverage age of the men was 43.2. The average ageof the women was 29.5.
NUMBER OFCOUNTRY PARTICIPANTS
Argentina 3
Mexico 10
Peru 1
Nine of the 14 participants were employed in theservice sector at the time of the focus groups. Oneparticipant was also a graphic designer in additionto working as a chauffeur. All of the men but onlythree of the women were employed.
Employment Status – TN
NUMBER OFEMPLOYMENT PARTICIPANTS
Employed 9
Unemployed 5
Three of the participants had completed orattended college while six had attended orcompleted high school or technical school. Threehad completed sixth grade and one completedsecond grade. One male participant did not answerthe question.
DESCRIPTIVE STATISTICS

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
respectively. Five participants were living with apartner, three participants were married, and threewere single. One participant was widowed, anotherwas divorced, and one participant did not answerthe question. Thirteen of the 14 participants citedSpanish as their primary language.
Six participants were born in Mexico, five inColombia, and one each in Uruguay, Guatemala,and Texas. The average length of time in the U.S.,excluding the U.S.-born participant, was 4.5 yearswith a range of three months to 14 years. All livedin the U.S. year-round.
Country of Birth – GA
Educational Attainment – TN
11
NUMBER OFLEVEL OF EDUCATION PARTICIPANTS
Elementary school 1
Middle school/ junior high school 3
High school/GED 6
College 3
No answer 1
One male participant received Medicaid. Twowomen participants received Medicaid for theirchildren. Of those who did not receive Medicaidfor themselves, none had private medicalinsurance. Eight participants had a physical in thetwo years prior to the focus group. Fiveparticipants did not remember the last time theyhad a physical, and one participant did not answerthe question.
Insurance Status – TN
NUMBER OFINSURANCE STATUS PARTICIPANTS
Insurance 0
No insurance 13
Medicaid 1
Georgia
Two mixed-gender focus groups were conducted inGeorgia: one in rural Lyons in May 2003 and theother in Atlanta in June 2003. The participants ineach group were from the city or town andsurrounding areas. The Lyons focus group hadfour participants and the Atlanta focus group hadten participants. In total there were seven menand seven women focus group participants. Theaverage age of the focus group participants was37.0 excluding one man and one woman who didnot include their date of birth. The average age ofthe men and women was 29.7 and 44.3,
NUMBER OFCOUNTRY PARTICIPANTS
Colombia 5
Guatemala 1
Mexico 6
United States 1
Uruguay 1
Ten of the participants were employed at the timeof the focus groups. Two men and two womenparticipants were not employed at the time of thefocus groups. Those employed were all employedin the service sector as housekeeping staff, retailworkers, dishwashers, or field workers.
Employment Status – GA
NUMBER OFEMPLOYMENT PARTICIPANTS
Employed 10
Unemployed 4
Four of the participants had completed or attendedcollege. Five had attended or completed highschool or technical school. Two had completedsixth grade and one had completed fifth grade.
DESCRIPTIVE STATISTICS

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
participants, one woman and two men, did notrespond to the question and were excluded fromthe calculations. The majority (26) of theparticipants were married while 11 lived with apartner. Out of the 49 participants who answeredthe language questions, 48 cited Spanish as theirprimary language.
Twenty-three of the participants were born inMexico with eight participants born in Colombiaand six in Argentina. The United States, includingPuerto Rico, was the country of birth for four ofthe participants. The countries of Peru, theDominican Republic, Venezuela, and Guatemalawere the countries of birth for two participantseach. Uruguay was the country of birth for oneparticipant.
Country of Birth – All Participants
Two participants reported no formal education. Ofnote is that the participants in Lyons had thelowest educational attainment level of all. Thehighest grade completed by the four participants inthe Lyons focus group was sixth grade.
Educational Attainment – GA
12
NUMBER OFLEVEL OF EDUCATION PARTICIPANTS
Elementary school 3
High school/GED 5
College 4
No formal education 2
One man and one woman participant receivedMedicaid. Two participants have children whoreceived Medicaid. Of those who did not receiveMedicaid for themselves, only three participantshad private medical insurance. Thirteen of the 14participants had received a medical examination inthe three years prior to the focus group beingconducted, with the overwhelming majority havinghad an exam in the two years prior. Only oneparticipant could not remember when his lastmedical examination had taken place.
Insurance Status – GA
NUMBER OFINSURANCE STATUS PARTICIPANTS
Insurance 3
No insurance 9
Medicaid 2
Summary Statistics
In total, there were 50 focus group participants: 24women and 26 men. The average age of allparticipants who responded to the question was35.3. The average age for women was 35.0. Theaverage age for the men was 35.5. A total of three
NUMBER OFCOUNTRY PARTICIPANTS
Argentina 6
Colombia 8
Dominican Republic 2
Guatemala 2
Uruguay 1
Peru 2
Mexico 23
United States(including 1 born in Puerto Rico) 4
Venezuela 2
Overall, the focus group participants had someeducation beyond the eighth grade. Eleven hadattended or completed elementary and junior highschool. Fifteen had completed, were attending, orhad attended high school. Eighteen had some levelof college education or had completed college, andtwo other participants had graduate degrees. Twoparticipants had no formal schooling and twoparticipants did not answer the question.
DESCRIPTIVE STATISTICS

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
Insurance Status – All ParticipantsEducational Attainment – All Participants
13
NUMBER OFEMPLOYMENT PARTICIPANTS
Employed 38
Unemployed 12
NUMBER OFLEVEL OF EDUCATION PARTICIPANTS
Elementary/junior high school 11
High school/GED 15
College 18
Graduate school 2
No formal education 2
No answer 2
Out of the 38 participants who were employed, themajority of the participants (31.6%) were employedin the service sector followed by the manufacturingsector at 26.3%. A number of participants (18.4%)were employed as paraprofessionals/skilled workersin schools, health departments, or smallnewspapers, and 13.2% were employed asprofessionals in the health field or as teachers.
Employment Status – All Participants
Only five (10%) participants received Medicaid forthemselves. Seven (14%) received it for theirchildren. Out of the remaining 45 participantswho did not receive Medicaid for themselves, only16 had private medical insurance. Of note is that68.2% of North Carolina focus group participantshad insurance, while the number of insured wasrelatively low for the other states.
INSURANCE STATUS NUMBER OFPARTICIPANTS
Insurance 16
No insurance 29
Medicaid 5
Key Informant Descriptive Statistics
Eighteen key informant interviews were completedduring the course of the needs assessment. Halfwere conducted in English and half wereconducted in Spanish or a mixture of both. Fiveinterviews were conducted in the Atlanta area andfive in Raleigh, three in South Georgia, four inBirmingham, Alabama, and one in Memphis.Twelve women and six men were interviewed. Allworked in the health care field in some capacity.The average age of the key informants was 42.3with a median age of 39. The average age for thewomen was 55.2 with a median age of 40.5. Theaverage age for the men was 34.8 with a medianage of 33.5. Twelve of the key informants weremarried, and ten cited Spanish as their primarylanguage.
Half of the key informants were born in the UnitedStates. Of those not born in the U.S., four wereborn in Colombia, and one each was from Mexico,Brazil, Uruguay, Cuba, and the DominicanRepublic. The average length of time in the UnitedStates for those born outside the United States was21.9 years with a range from two years to 40 years.
Two held high school diplomas, five held collegedegrees, and one had attended college. Five heldmaster’s degrees and two had doctorate degrees.The remaining three held medical degreesalthough one medical degree was from a foreigncountry and the participant was not practicing inthe U.S.
DESCRIPTIVE STATISTICS

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
SUMMARY OF FOCUS GROUP RESPONSES
services from doctors, clinics, the hospital, healthdepartment, or the emergency room. Respondentsin one group mentioned using medications fromtheir home country as the first alternative beforeseeking medical care due to cost concerns.
In their home countries,respondents mentioned that theysought services at the doctor orclinic because they had insurance intheir countries or health serviceswere provided free of charge. Twofocus groups mentioned the use ofhome remedies as the first stepbefore going to the doctor. Thedistinction was made by the groups
between an emergency and a minor illness thatcould first be treated by home remedies or withover-the-counter drugs.
All six focus groups were well aware of the healthorganizations, health programs, resources, andproviders available in their communities. Allgroups mentioned local private clinics and thehealth department and their clinics as services. Inaddition, hospitals, urgent care clinics, andnumerous health maintenance organizations werementioned as service providers. Two groupsmentioned local CBOs as providers of healthinformation or resources. While participantsmentioned using the emergency room when theyor a family member became ill, none viewed it as ahealth resource.
Although respondents were aware of the healthservices, providers, resources, and programsavailable to them and the community, theoverwhelming majority of participants in all focusgroups did not feel that many Latinos used theseservices. The reasons for not using these servicescentered around lack of information or knowledgeabout services, fear of paperwork, no interpretersavailable, being undocumented, lack of insurance,and lack of trust in the U.S. medical system.
Instead, all groups, except for the SoutheastGeorgia focus group, mentioned self-medicating
Eleven (61.1%) of the key informants provideddirect services to Latino clients. Two providedmental health counseling and two providedmedical services to Latinos, while the remainingfive provided health education services. Inaddition, ten of the 11 also hadmanagement or programcoordinating duties. The remainingseven key informants were inmanagement positions with theirorganizations or helped to design ormanage programs for the CBOs.
In total, 16 different agencies wererepresented. With the exception oftwo key informants, all worked atagencies that provided some social, educational, ordirect service to Latino clients in their area. Theremaining two informants worked at organizationsthat conducted research and provided publicinformation and advocacy.
Eight of the organizations represented providedservices only to Latinos while the remaining eightprovided services to everyone. However, while theyprovided services to everyone, five had a majorityof Latino clients or offered some services only inSpanish.
SUMMARY OF FOCUS GROUPRESPONSESThe focus groups answered questions in threemajor areas: use of existing services by Latinos,barriers to obtaining health care services, and thegap between what is needed and what is currentlyavailable. A fourth area, discrimination, was addedif the focus group brought up differentialtreatment as an issue. The following is a summaryof the responses and the themes that emerged fromtheir responses.
Use of Existing Health Services:
When respondents or family members became ill inthe U.S., all groups mentioned obtaining medical
14
“The situation (in the U.S.)is difficult and you have tolook for alternative homeremedies…It is easier tohave a house than to pay
for health care here." — Atlanta participant

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
in all six groups mentioned radio, followed bynewspapers and then television. Three groupsmentioned outreach via pamphlets sent home ordoor-to-door as well as school as an opportunity toobtain information. Mexican tiendas, CBOs, andwork were also mentioned.
Participants were asked about any groups orindividuals that make it difficult to obtain care.Most mentioned system barriers, but the Atlantagroup did mention that the government made itdifficult to obtain care by the cuts they weremaking to health care funding. A North Carolinaparticipant stated, "I know of a clinic in a ruralarea and if the person does not pay theirinterpreter they will not receive service in thatclinic."
The overwhelming response to what barriers existfor Hispanics in accessing health care services waslanguage. It was acknowledged that Latinos shouldmake an effort to learn English, but one North
Carolina focus group mentionedpossible violations of the lawrequiring interpreters and the lackof available interpreters. A majorityof respondents also mentionedmoney and lack of insurance asbarriers to accessing health care.Some individuals mentionedcultural barriers, legal status, and
transportation to facilities as additional barriers toaccessing health care. Four groups mentioneddiscrimination or different treatment as barriers.
The Gap:
The majority of respondents, except for the NorthCarolina focus groups, did not have healthinsurance. Those whose employers provided healthinsurance felt that the cost was too high. Thosewhose employers did not provide insurance alsofelt that the cost was high but also mentioned theirinability to obtain other insurance because of lackof legal status in this country. Participants whodid not work cited the same reasons for lackinghealth insurance.
with medicines from Mexico or their countries oforigin or using other home remedies they knew orwere mentioned to them by friends and family.Returning to their home country was alsomentioned as an alternative due to lower cost oftreatment. One group mentioned the use ofsanteros (traditional healers) as a means oftreatment for some individuals, and anothermentioned going to individuals who do not have alicense to practice medicine in this country buthave a license from their country of origin.
One participant from Atlanta stated, "…it is cheaperto go to Colombia. I went one time to a dentist(here in the United States) and they told me itwould cost $2,500, until I met a Colombian womanworking with the (medical) license of someone elseand I did the crown with her and it costs $250."
Barriers to Health Care Access:
Participants were asked how they find out aboutservices in their area. Word of mouth was themost mentioned means of obtaininginformation about health care. Thiswas followed by use of the radio andother forms of media such as thenewspapers and television. Mexicantiendas (stores) were mentioned as ameans for finding out about healthcare. Lastly, pamphlets or flyers, thechurch, promotores (community health outreachworkers), and local CBOs were also mentioned asmethods for finding out about health care.
While churches were only mentioned by one focusgroup as a means of finding out about health care,the majority of the groups mentioned thatchurches assisted them with obtaining or accessinghealth care. Local CBOs and promotores were alsomentioned, as well as employees at some of theclinics or hospitals they visited.
When asked about the best way for groups oragencies to let them and the community knowabout the health services they offer, the media wasthe response most often mentioned. Respondents
15SUMMARY OF FOCUS GROUP RESPONSES
"We are in a differentcountry and we should
all learn English." — North Carolina
participant

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
All groups had key points they wanted healthprofessionals to know. Participants want to be treatedbetter and not face discrimination or bad treatmentwhen seeking services. Some stated that they simplywant to be treated as humans. Many want doctors tohave a better understanding of their circumstances andbetter education for both doctors and the communityabout prevention, health, and culture. Additionally,they want health professionals to understand thatimmigrants, despite not residing here legally, haverights. Better access to insurance as well as better-trained interpreters were also requested.
SUMMARY OF KEY INFORMANTRESPONSESThe questions for the key informants mirrored thequestions that were asked in the focus groups. Allquestions addressed the three main areas addressedby the focus groups. However, all key informantswere asked about discrimination as well asbackground questions on their agencies.
Use of Existing Health Services:
Overall the informants mentioned the samecommunity health providers, resources, andprograms as the focus group participants.Informants, presumably because of their work,were able to identify additional resources notmentioned by the focus groups. There wasconsistency between both groups with regard tohospitals, clinics, and the health department beingmentioned as resources in the community. Keyinformants mentioned more often than the focusgroup participants the use of the emergency roomas a source of care.
Key informants differed on the perception ofwhether many Latinos used the resources,providers, and programs mentioned. The majorityof the informants felt that many Latinos used theprograms because there were no other resources,particularly with regards to use of the emergencyroom. Only one informant felt that many Latinosdid not use the available resources and providers in
Respondents felt that there were a large number ofservices that Latinos in their areas needed. Manyof the responses across all three states weresimilar. All except one group mentioned the needfor dental services. The same was true for the needfor interpreters. In general, there was a lack ofinterpreters available, and a need for training ofinterpreters was also mentioned. Vision serviceswere also mentioned as being needed by threegroups. Two groups cited a need for better qualitygeneral health services as well. Family healthservices and a clinic for Latino adults were viewedas necessary, in addition to children’s and women’sservices. In addition, the groups mentioned theneed for prevention information, recreation sites,access to specialists, and more clinics.
Respondents were asked about their use ofmedicines prescribed by doctors. While many didfill prescriptions from the pharmacy whenprescribed, many others did not. The reasons fornot filling prescriptions varied from lack of money,not trusting that the medicines would work, lack ofinsurance, and preferring to obtain somethingcheaper even though it may not work. Somerespondents preferred to get medicines from theirhome countries because of cost and having moreconfidence in those drugs. One participantmentioned not understanding the prescription whenit is filled because the label is in English. Mostgroups mentioned that home remedies and over-the-counter medicines were used when they wereunable to get prescriptions filled.
While only four groups mentioned discriminationor differential treatment by providers, not all wereattributed to race. One woman mentioned havingbeen the victim of inappropriate comments abouther body by her doctor. Others mentioned thatemployees, such as front desk staff, mistreatedclients by yelling at them, denying them servicesbased on lack of interpreters, or asking for theirlegal status when accessing services. Others feltthat they were treated well only if they spokeEnglish. Only two respondents mentioned race orethnicity as a reason for the differential treatment.
16SUMMARY OF KEY INFORMANT RESPONSES

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
views. Key informants mentioned the attitude of thegeneral community, other minority groups, Latinopractitioners, immigration reform groups, the statelegislatures, and departments including the healthdepartment, employers, and the media. The reasonsgiven were the policies of some of the governmentagencies and community not allowing time off to
obtain care, Latino practitioners"putting down" other Latinopractitioners, and the use of the mediato create anti-immigrant sentiment.
Similar to the focus groups, themost mentioned barrier that existsfor Latinos is language. Every
informant mentioned language as a barrier.Informants mentioned transportation, lack ofinsurance, and cost of services as the next largestbarriers. In addition, legal status, attitudes ofproviders and the public, cultural barriers, hours ofoperation, and lack of bilingual providers,interpreters, and information were listed asadditional barriers. Many of the barriers were thesame as those listed by the focus groups.
Lastly, 15 of the 18 informants believe that Latinosare treated differently than others when obtaininghealth care. Their sense was that because oflanguage, lack of insurance, and culturalunderstanding, Latinos are made to wait longer,denied services, and treated as second-classcitizens. Three informants felt that perception andbureaucratic red tape contribute to Latinos feelingas if they are treated differently.
The Gap:
Key informants felt that there was a need to expandservices to Latinos in a number of areas. Basic accessto services, insurance access, healtheducation/promotion, prenatal care, migrant care,and substance abuse services were the most frequentanswers with three to five informants mentioningthem. Other areas in which informants felt servicesshould be expanded was sexually transmitted diseaseinformation, mental health, and cultural sensitivitytraining. These answers differed somewhat from focusgroup participants. While there was some overlap,
their community because of the cost and the lackof trained interpreters.
Key informant answers more closely mirroredfocus group participants when asked what Latinoswho don’t access the available services do when ill.The use of home remedies, self-medication, andhealers was mentioned byinformants in addition to the factthat some do nothing and suffer insilence. Most informants mentionedthe use of the emergency room.
Barriers to Health Care Access:The majority of key informants (12out of the 18) stated that the manner in whichmost Latinos in the community find out abouthealth care services is through word of mouth.This was the same response as the focus groups.CBOs, including the church, and communityoutreach were mentioned by many of theinformants followed by media, the healthdepartment, and health fairs.
The informants’ answers regarding how Latinos findout about health services in their communitycoincided with which organizations they believe assistLatinos in accessing health care. All informantsmentioned some type of CBO or organization thatassisted Latinos in accessing health care such aschurches, universities, health departments, localCBOs, and individuals in the community.
The best way to reach the community, according toinformants, was the use of the Spanish-languagemedia. Nine informants mentioned the media inall forms (radio, print, and television) as one of thebest ways to get information to the community.This echoes the responses from focus groupparticipants. Word of mouth, the workplace,outreach and outreach workers, churches, CBOs,clinics, government services, and schools were alsomentioned. Some of these were mentioned by thefocus groups as well.
Overall, key informants felt that many groups made itdifficult for Latinos to access health care services. Thiswas in marked contrast to focus group participants’
17SUMMARY OF KEY INFORMANT RESPONSES
"If you are blondethey treat you better."
— North Carolinaparticipant

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
focus only on the barriers to access highlight theneed for more state-based health data on Latinos.
Overall, the findings of the 16 reports wereconsistent with the findings of the HELC reportand show agreement between the concerns andchallenges facing the Latino community in theSouth U.S. However, there were some areas ofdivergence between some of the reports and theHELC assessment. What follows is an overview ofthe concerns and challenges raised by the HELCassessment compared to the previous reports.
Utilization of Services:
While HELC focus groupparticipants and key informantresponses did not overlap on thequestion of whether many Latinosused the health resources andprograms available in their areas,focus group participants raisedconcerns similar to the findings of
other reports. HELC focus group participants feltthat many Latinos did not use the availableresources because of lack of knowledge of existingservices, fear of paperwork, no interpretersavailable, being undocumented, and lack of trust inthe U.S. medical system. Some of these concernswere echoed in the collected reports.
For example, the Duke University Access to HealthCare by Durham’s Low Income Latinos7 cited lackof knowledge about where to obtain services, andthe Atlanta Regional Health Forum Town Hall8
cited lack of interpreters and immigration status aswell. In addition, a Whitfield County HealthDepartment9 focus group also found lack ofknowledge and documentation to be a concern forLatinos not accessing health care, and the LatinoHealth Task Force of the North Carolina Instituteof Medicine10 (NC IOM Report) citeddocumentation as a barrier to seeking services.
The issue of lack of trust of the U.S. medicalsystem can stem from the lack of knowledge of thesystem, which could potentially lead Latinos toturn away from seeking medical care or possibly
focus group participants mentioned more concreteservices such as dental and vision services which theyfelt were missing, while informants mentioned morepreventative information and access issues.
Key informants were asked what type of healthcampaign they think the Latino community wasready for and what type of campaign they wouldlike to see. The most cited answers were STD/HIVinformation, health awareness/prevention, andinsurance access campaigns. Other responsesincluded diabetes, substance abuse, domesticviolence, nutrition, and sexual education, amongnumerous others. When asked forthe campaigns they would like tosee, there was more agreement. Themost cited response was an STD/HIVcampaign followed by domesticviolence, substance abuse, andaffordable primary care campaigns.The most common responses forwhat the campaigns should includewere outreach by individuals (promotores) or viamobile units, prevention messages, and includinggovernment officials and the media.
In closing the interview, informants were asked ifthere was anything that they felt was the mostimportant issue to address. While answers variedfrom person to person, some mutual concerns didemerge from the interviews, including the need fordomestic violence and substance abuse education.Other concerns with multiple responses were theneed for primary care, more bilingual staff, andcommunity education and leadership training.
SUMMARY OF PREVIOUSASSESSMENT FINDINGSA total of 16 state, county, or local Latino health-specific reports were obtained during the projectyear. Nine were from Georgia, with three fromNorth Carolina, two from Alabama, and one eachfrom Tennessee and South Carolina. The smallnumber of Latino health-specific reports, theirsmall sample size, and the fact that many reports
18SUMMARY OF PREVIOUS ASSESSMENT FINDINGS
"If you speak English they treat you withquality attention." — North Carolina
participant

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
Only four reports addressed the best way for healthinformation to reach the community. HELCrespondents cited the media, particularly the radio,in all of its forms as the best mechanism to reachthe Latino community. The Gwinnett CountyHispanic Focus Group, the Health Needs andResources of the Greater Birmingham AlabamaLatino Community Survey,18 the Whitfield CountyHealth Department Focus Group, and the NorthCarolina IOM Report addressed the use of themedia as a means to disseminate healthinformation.
In contrast to the HELC findings, the Birminghamreport found that, among providers and thecommunity, the best means to disseminate healthinformation was the church. However, providerssurveyed mentioned media such as newspapers,radio, and television as their next three answers.Radio was the last method indicated by theBirmingham community. Other mechanisms citedby HELC participants to get information to thecommunity included promotores de salud,community workshops, schools, markets, andworksites. Many of these responses were cited inthe previously mentioned reports as well.
The Gap:
Latino respondents in all reports, excluding theNorth Georgia LEP Survey, felt they needed moreservices or information on a variety of issues. TheHELC report found that focus group participantswanted more dental services, interpreters, visionservices, and better quality health care, as well asprevention information. While these responsesdiffered from the key informants who felt that theexpansion of services to Latinos should include basicaccess issues, health education/health promotion,prenatal care, migrant care, and substance abuseinformation and services, just about all responsesfrom both groups were included in the reports thataddressed the question. Although no report askedthe question in the same format as the HELCreport, reports that did address the need forinformation and services overlapped with some ofthe responses from HELC participants.
seek medicines and remedies native to their homecountries. The use of home remedies wasacknowledged in the NC IOM Report and TheNeeds of Georgia’s New Latinos11 and documentedin the HELC report.
Barriers to Health Care Access:
The barriers faced by Latinos when accessinghealth care are similar throughout the South.While language, cost of services, and lack ofinsurance were the most often cited barriers byHELC participants, other barriers such astransportation, legal status, and cultural barrierswere mentioned as well. These same barriers werementioned by the ten reports that addressedbarriers to health care access. The final report wasa survey on limited-English-proficient (LEP)services available in the North Georgia HealthDistrict12 (North GA LEP Survey).
Language as a barrier to access was mentioned by11 reports. As early as 1999, the North CarolinaOffice of Minority Health and State Center forHealth Statistics13 cited language as a barrier forLatinos. This was echoed by a study in Memphis,Working for Culturally Sensitive Health Care forLatinos in Memphis,14 which found that out of 27%of their survey respondents needing interpreterservices, 93% "did not find an interpreter to bereadily available." Finally, The Needs of Georgia’sNew Latinos and the Findings from theHispanic/Latino Ad Hoc Committee15 of SouthCarolina also cited language as a barrier.
The North Georgia LEP Survey documentedSpanish as the top language spoken by clients whoreceive LEP services. Indigenous Guatemalanlanguages were the second most cited, indicatingthat Latinos moving from Central and SouthAmerica are a diverse group. Additionally, theinterrelated barriers of cost and lack of insurancewere mentioned by all reports. The Obstacles toMedical Care for Latino Children in GwinnettCounty, Georgia16 focus group report and theHealth Survey of Migrant Population in ApplingCounty, Georgia17 mirrored these results inaddition to addressing transportation.
19SUMMARY OF PREVIOUS ASSESSMENT FINDINGS

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
KEY FINDINGS
KEY FINDINGSThe following discussion highlights the key themesthat emerged from the HELC focus groups and keyinformant interviews.
● Latinos are reluctant to use available sourcesof health care and are treated differently fromother patients when accessing care.
While focus group participants and key informantswere not in complete agreement over whether themajority of Latinos use existing services, there is aperception by focus group participants – which isreinforced by some of the other assessments – thatLatinos do not use available health care services.Reasons ranged from lack of knowledge of availableresources, lack of interpreters, lack of insurance,lack of trust in the medical system, andimmigration status (i.e., not being legally presentin the United States). Focus group participantsand key informants cited use of over-the-countermedicines, home remedies, and the emergencyroom as methods of care used by Latinos who donot seek out or know of available sources of healthcare. Participants in the focus group andinterviews mentioned that Latinos receive differenttreatment by health care staff. Specifically, theynoted that Latinos experience longer waits and aredenied services due to language barriers, lack ofinsurance, and lack of cultural understanding onthe part of providers and their staff.
● Spanish-language media is the best means todistribute information to the Latinocommunity.
The majority of respondents stated that, whilemost Latinos get information about health servicesin their community by word of mouth, theSpanish-language media was the best method toreach the Latino community. Word of mouth wasalso mentioned as a means to share information inrelation to door-to-door outreach efforts. Previouslocal assessments supported this finding.
For example, in the Floyd County HealthDepartment Hispanic Survey,19 respondents wantedinformation on family planning and nutrition,prenatal care, domestic violence, sexuallytransmitted diseases (STDs), and immunizations.The lack of information on STDs was highlighted bya report on a syphilis outbreak in Decatur, Alabamain which Latino males accounted for half of thecases found.20 Atlanta Regional Health Forumparticipants cited dental and vision services as wellas access to primary care and preventive services asimportant health issues that challenge them or theirfamilies. The NC IOM Report and a report on Latinomigrant farmworkers21 also cited insufficientresources to address the health, behavioral, anddental health needs of Latinos.
Of note is the lack of Latino-specific mental healthinformation. Only one report, Treatment andEthnographic Data in Latino Substance AbuseServices,22 contained data on Latino admissionsinto an outpatient substance abuse program.Although recognized by key informants as a serviceneed for Latinos, there is a lack of southern state-specific data on the topic.
Overall, the findings of the HELC project echothose found in other reports, but also provide somenew information on how Latinos view the healthcare system. Latinos want access to quality andaffordable health care like all Americans. They donot view the emergency room as a health resourcebut rather as the last stop for obtaining neededcare, and they have a need for culturallyappropriate health care information. Many of thefindings defy the conventional wisdom whichsuggests that Latinos do not care about theirhealth or that health is not an important issue tothem. Despite the nature of the challengespresented by the HELC project, the findings alsoindicate areas for opportunity.
20

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
RECOMMENDATIONS
● Federal, state, and local governments andhealth insurers should establish and fundmechanisms through which appropriatelanguage services are available when needed.In addition, recipients of federal funds must beaccountable for providing language services asrequired under Executive Order 13166 andTitle VI of the Civil Rights Act of 1964. TheOffice for Civil Rights (OCR) should increaseits efforts to monitor and enforce Title VIviolations related to language access anddiscrimination.
A mechanism should be established between theOffice for Civil Rights, state and local healthdepartments, and local CBOs which would allowfor the reporting and investigation of suspectedTitle VI violations before a noncompliance order isissued. In North Carolina, El Pueblo, Inc. workedwith the state health department proactively ratherthan reactively to ensure that health providers hadthe resources and information needed to complywith the law. Its work can be used as a model forother southern states.
Nonprofit Organizations:
● Local nonprofits should create a regionalPromotores de Salud Institute.
The Institute would train local CBOs on how todevelop promotores programs and on the latestcommunity health education techniques. Theseprograms provide a vehicle for using localcommunity resources to educate the largercommunity about health issues.*** The Institutewould also conduct train-the-trainers sessions soCBOs could train their own promotores in theirlocal area. In order to address the larger issue ofaccess, the training would include information onthe rights of citizens and noncitizens to accessservices as well as general information on the U.S.health care system.
● The primary barrier to accessing health care isrelated to language and communicationissues.
The barrier most often cited by Latinos whenaccessing health care is limited Englishproficiency and difficulty communicating withhealth care personnel. Focus grouprespondents were aware of a law requiringinterpreters but felt that providers did notalways follow the law. While other barrierssuch as lack of insurance, lack oftransportation, and in some casesdiscriminatory behavior by health care staffwere mentioned, all respondents and previousassessments felt that language challenges werethe biggest barrier faced by Latinos.
RECOMMENDATIONSBased on the findings of the HELC project, theNational Council of La Raza Institute for HispanicHealth recommends the following:
Government Agencies:
● Federal and state governments should create ahealth awareness and education publicservice/information campaign specific to theSouth.
The federal government should work inconjunction with state and local healthdepartments, CBOs, and local media outlets todesign and implement a comprehensive media-based campaign that provides information on localservices available to listeners, viewers, and readers.The campaign should include information ondiseases and illnesses that affect Latinosdisproportionately, information on the rights ofimmigrants to access services, and information onlocal clinics.
21
***For a full description and models of promotores programs, see "Promotores Energizing Communities for Heart Health:Findings from the Salud Para Su Corazón Implementation Projects" by the National Heart, Lung, and Blood Institute, theNational Council of La Raza, and the University of North Texas – School of Public Health, July 2002.

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
RECOMMENDATIONS
● Share information and research. NCLR, othernonprofits, CBOs, and researchers shoulddistribute and promote widely the findings ofthis report and other related research inside andoutside the community to raise awareness andpromote change.
● Coordinate efforts between Latino andmainstream service providers and resources toenhance health advocacy. Existing Latino orLatino-serving "gatekeeper" organizations shouldcoordinate efforts and mobilize traditionally"mainstream" national health organizations tocreate the environment and dedicate resourceswithin their own organizations to become partof the solution. Similarly, Latino CBOs andindividuals should network with existing servicesand community leaders to continue to expresstheir needs, wishes, and demands, and toadvocate for equal access to and fair treatmentfrom health services.
● Use existing resources to publicize informationand services. Spanish- and English-languagemedia should play a role in highlighting thecontributions, strengths, and needs of thegrowing Latino population in the South, as wellas highlight and disseminate information thatpoints to solutions and successes.
Ensuring the integration of Latinos into the socialfabric of the South will require a shared effort amongservice providers, government, and the Latinocommunity. As demographic changes suggest, thehealth and status of Hispanics in the South willincreasingly be tied to and influence the overall well-being of the region. NCLR believes that therecommendations outlined above to improve healthcare access and care are within reach and is hopefulthat service providers, government, CBOs, andLatinos themselves will work in partnership toensure fair treatment, quality services, and healthyoutcomes for Latino children, families, and allresidents in the South.
Professional Medical Associations:
● Medical professionals should create a culturalcompetency curriculum for distribution tomedical and allied health schools in theSouth. In addition, doctors’ associationsshould offer continuing education coursesdealing with cultural competency to ensurethat all doctors have an opportunity toincrease their knowledge of culturally andlinguistically diverse populations.
Although the number of Latinos in the Southcontinues to climb, the number of Latino health careprofessionals is not keeping pace.23 Therefore, it isimportant to ensure that young medical professionalsand new graduates in the South are adequatelyprepared to deal with the changing demographics inthis region. To help in this effort, the governmentand nonprofit sectors should collaborate to develop acurriculum that addresses Latino cultural beliefs butalso the unique situation in the South. Thiscurriculum should be adapted and offered as a coursefor continuing education credits so that currentproviders can increase their knowledge and improvetheir treatment of their diverse clients.
The Latino Community:
NCLR believes that the Latino community also has arole to play in improving service delivery andoutreach and focusing policy-maker attention onhealth issues of importance to Latinos in the South.In particular, the Latino community should:
● Increase education and public awareness effortsrelated to health issues. Latinos should becomeas informed as possible about the healthconditions affecting them and their families, andthe community at large, and share thisinformation with the broader community tobegin to take steps to improve their well-being.
● Participate in health forums and fairs that maybe sponsored by "mainstream" organizations intheir community to represent the realities andneeds of Latinos as a growing and importantcitizenry of the South, and increase the voiceand presence of Latino families in this region.
22

NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
ENDNOTES23
ENDNOTES
14. Access Project, "Working for CulturallySensitive Health Care for Latinos in Memphis,"http://www.accessproject.org/st_6.htm, 2000.Accessed September 8, 2003.
15. The South Carolina Commission for MinorityAffairs, "Findings from the Hispanic/Latino AdHoc Committee," http://www.state.sc.us/cma/Hispanic_Report/htm, 2003. AccessedMarch 3, 2004.
16. American Academy of Pediatrics, "Obstacles toMedical Care for Latino Children in GwinnettCounty, Georgia," 2001.
17. Zhang, Pidi and Andrea Cruz, "Health Surveyof Migrant Population in Appling County,Georgia, 2000," 2001.
18. Alleman-Velez, Patty, Joseph Telfair, and JoAnaDodson Stallworth, "Health Needs andResources of the Greater Birmingham,Alabama Latino Community: A Survey ofGeneral Health, Substance Abuse and HIVKnowledge Among Young Latino Adults," 2003.
19. Floyd County Health Department, Floyd CountyHealth Department Hispanic Health Survey, 2000.
20. Paz-Bailey, Gabriela, Silvia Teran, WilliamLevine, and Lauri E. Markowitz, "SyphilisOutbreak Among Hispanic Immigrants inDecatur, AL: Association with Commercial Sex,"Sexually Transmitted Diseases, January 2004.
21. Perilla, Julia L., Astrid H. Wilson, Judith L.Wold, and Lorine Spencer, "Listening toMigrant Voices: Focus Groups on Health Issuesin South Georgia," Journal of CommunityHealth Nursing, 1998.
22. Mancini, Pierluigi. "Treatment and EthnographicData in Latino Substance Abuse Services." 2003.
23. PR Newswire, "Commission addressesunderrepresentation of minority healthprofessionals," Hispanic Business.http://www.hispanicbusiness.com/news/newsbyid.asp?id=12367, September 5, 2004. AccessedSeptember 9, 2004.
1. U.S. Census Bureau, The Hispanic Population:Census 2001 Brief,http://www.census.gov/prod/2001pubs/c2kbr01-3.pdf
2. Ibid.
3. Scott, Jeffry, "Influx of Hispanics, Asians marksmetro area’s growth," The Atlanta JournalConstitution, August 26, 2004.
4. Wadhwani, Anita, "Nashville area leads state inHispanic population growth," The Tennessean,August 28, 2004.
5. Torres, Cruz, "Emerging Latino communities: Anew challenge for the rural South," August 2000.
6. Butler, Pat, "Hispanics add another thread toSouth Carolina’s cultural fabric: Immigrantpopulation outpaces state’s general growth,"The State. April 18, 1998.
7. Denman, Susan, "Access to Health Care byDurham’s Low Income Latinos,"http://www.nursing.duke.edu/research/latinos.html,1998. Accessed July 24, 2003.
8. Atlanta Regional Health Forum Town HallMeeting Summary, 2003.
9. Whitfield County Health Department,"Hispanic Health Care Needs/Hispanic HealthCare Workers," 2003.
10. NC Latino Health, Durham, NC: NorthCarolina Institute of Medicine, February 2003.
11. Atiles, Jorge H. and Stephanie A. Bohon, TheNeeds of Georgia’s New Latinos: A PolicyAgenda for the Decade Ahead. Athens, GA:Carl Vinson Institute of Government,September 2002.
12. Survey of North Georgia Health DistrictLanguage Assistance Services: County HealthDepartments and District Programs, July 2003.
13. Office of Minority Health and State Center forHealth Statistics. (1999). North CarolinaMinority Health Facts: Hispanics/Latinos,September 1999.
ENDNOTES
National Council of La RazaHealth in Emerging Latino Communities (HELC) Project Meeting
March 11, 2004
AGENDA
I. Welcome(10:00-10:15 a.m.)Carlos Ugarte, Deputy Vice President, National Council of La Raza – Washington, DC
II. Introductions(10:15-10:30 a.m.)
III. Overview of Findings(10:30-11:15 a.m.)Liany Elba Arroyo, Project Coordinator, National Council of La Raza – Atlanta, GA
IV. Latino Health in NC: Status and Policy Efforts from an Advocacy Perspective(11:15 a.m.-12:00 noon)Andrea Bazán-Manson, Executive Director, El Pueblo – Raleigh, NC
V. Lunch and Networking(12:00 noon-1:00 p.m.)
VI. Participant Discussion on Findings(1:00-1:45 p.m.)Facilitated by Liany Elba Arroyo
VII. Participant Recommendations(1:45-2:30 p.m.)Facilitated by Liany Elba Arroyo
VIII.Next Steps(2:30-3:00 p.m.)Carlos Ugarte
NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
APPENDIX A24
APPENDIX AMeeting Agenda

Health in Emerging Latino Communities Project
1. Edgar Angulo – Georgia Department of Community Health – Office of Minority Health, Atlanta, GA
2. Andrea Bazán-Manson – El Pueblo, Inc., Raleigh, NC
3. Carolina Caseres – National Center for Primary Care, Morehouse School of Medicine, Atlanta, GA
4. Andres Crowley – El Pueblo, Inc., Raleigh, North Carolina
5. Andrea Cruz – South Georgia Communities Project, Lyons, GA
6. Delma de la Fuente – Georgians for Healthcare, Atlanta, GA
7. Alina Flores – Centers for Disease Control and Prevention
8. Corina Florez – South Georgia Communities Project, Lyons, GA
9. Jerry Gonzalez – Georgia Association of Latino Elected Officials
10. Chris Griffin – Department of Health and Human Services, Office for Civil Rights, Atlanta, GA
11. Julia Hayes – Alabama Department of Health – Office of Minority Health, Huntsville, AL
12. Dr. Pierluigi Mancini – Clinic for the Education, Prevention and Treatment of Addiction, Atlanta, GA
13. Yolanda Martínez – Children’s Health Insurance Program, State of Alabama
14. Lisa Reddington – St. Vincent’s Hospital, Birmingham, AL
15. Michael Rhein – National AIDS Fund, Washington, DC
16. Angel Roca – Centers for Disease Control and Prevention
17. Dr. Isabel Scarinci – University of Alabama-Birmingham
18. Blanca Torres – Centers for Disease Control and Prevention
19. Dr. Henrie Treadwell – National Center for Primary Care, Morehouse School of Medicine, Atlanta, GA
20. Rogelio Valencia – North Carolina Department of Health and Human Services
21. Dr. José Velazquez – Latino Memphis, Memphis, TN
22. Charles Walker – United Way of Metropolitan Atlanta – Cobb County, Marietta, GA
23. Kirsten Witt – Coca-Cola Company, Atlanta, GA
24. Melissa Wolowicz – Community Foundation of Greater Memphis
NCLR Staff
Carlos Ugarte, MSPH – Deputy Vice President, Institute for Hispanic Health
Lynda Barros – Director, Emerging Latino Communities Initiative
Liany Elba Arroyo, MPH – Project Coordinator, Southeast Health Program Office – Institute for Hispanic Health
Natalie Hernandez – Consultant
NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
APPENDIX B25
APPENDIX BMeeting Participants
Meeting Background:
The Health in Emerging Latino Communities meeting was held March 11, 2004 in Atlanta, Georgia.The Latin American Association, the largest provider of services to Latinos in metropolitan Atlanta,hosted the meeting in its facilities. A total of 24 individuals attended from the four states
represented in the assessment. In all, 65 individuals from Alabama, Georgia, Mississippi, North Carolina,South Carolina, and Tennessee were invited. Participants did not receive the draft of the report in advance.
Two presentations were made during the meeting. The first was an overview of the Health in EmergingLatino Communities project. The overview was followed by a presentation on North Carolina’s approach toLatino health from the perspective of a state-based Latino advocacy organization and a National Council ofLa Raza affiliate.
Participants were invited to give input and discuss the report findings as well as give theirrecommendations to improve Latino health in the South United States. What follows is a summary of thediscussion and their recommendations.
Summary of Participant Comments:
1. Do the findings mirror what you encounter in your work? How so?Overall, meeting participants felt that the findings of the HELC project mirrored what they found intheir own work. Participants felt that it reflected the situation in the South.
2. If not, how do they differ?While the report reflected the challenges and barriers encountered by Latinos in the South, meetingparticipants stated that they did see some differences in their own work not reflected in theassessment. First, participants felt that the sample population was not truly reflective of the overallLatino community. Examples of this included the level of insurance and education. In the assessment,the education level and insured rate were higher than what most providers found in their work.
3. General CommentsParticipants had many insights to share regarding Latino health in the South. Some felt that morefunding was necessary to conduct adequate research on a representative sample. Likewise, thatfunding should also make its way down to the community level. Participants recognized that, whilefunds that are being expended are targeted for the Latino community, these funds were not making itto the community level.
Participants felt that the community needed to be more engaged in the programs targeting theircommunities as well. One participant stated, "Who better knows the community than the communityitself? The community needs to define needs…how can you solve problems? You solve them byempowering the community." Promotores were mentioned as a means to work with the community asthey come from and share the same values as the community. However, it was stated that agencies neededto find bicultural and bilingual staff as well.
NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
APPENDIX C26
APPENDIX CSummary of Participant Comments and Recommendations

Participant Recommendations:
Research:
1. Examine differences between Latinos living in rural and urban areas.
2. Identify social and political determinants of health for Latinos in the South.
3. Examine the intensity of the needs of Latinos.
4. Define core elements of a multicultural health system.
Policy:
1. Promote the development of Latino human resources in the South.
2. Create a system of continuing education for medical interpreters.
3. Extend Title VI by incorporating cultural competency standards.
4. Require that existing providers receive continuing education in cultural competency.
NATIONAL COUNCIL OF LA RAZA
THE HEALTH OF LATINO COMMUNITIES IN THE SOUTH: CHALLENGES AND OPPORTUNITIES
APPENDIX C27