the fundamentals of bracing - amazon s3s3.amazonaws.com/dafo/documents/bracing_fundamentals.pdf ·...
TRANSCRIPT
Bracing Fundamentals
Most of the patients who require DAFO braces have neurological or neuromuscular problems resulting from a variety of disorders, including cerebral palsy, spinal bifida, Down syndrome, head injuries and stroke, to name a few. The term “neuro” (as in neurological) refers to the nervous system and brain. The problems associated with these disorders are caused by damage or malformation of the neural systems that control the movement of the muscles and/or provide sensory information about position and movement.
For most of us, our bodies quickly developed the ability to stand upright. Through repeated use, the complex array of muscles and neural control systems required for balance and propulsion became fine tuned to the tasks of supporting the weight of our bodies and, eventually, to shifting that weight from one leg to the other for walking. The bones of our legs and feet positioned themselves in the optimal alignments to perform their supportive roles. They were vigorously held in place by muscles, tendons, and ligaments, all growing and strengthening to the job of standing and walking.
For the neurologically involved DAFO patient, this process of development has been partially or substantially disrupted. Muscle strength or movement has been compromised, inhibiting the development of the skills required for standing and walking. Without normal daily use of the legs and feet, muscles remain underdeveloped and weak. Tendons and ligaments are not stretched and strengthened by the activity of walking. The bones, dependent on the strength of the muscles, tendons and ligaments to hold their structures together, become misaligned.
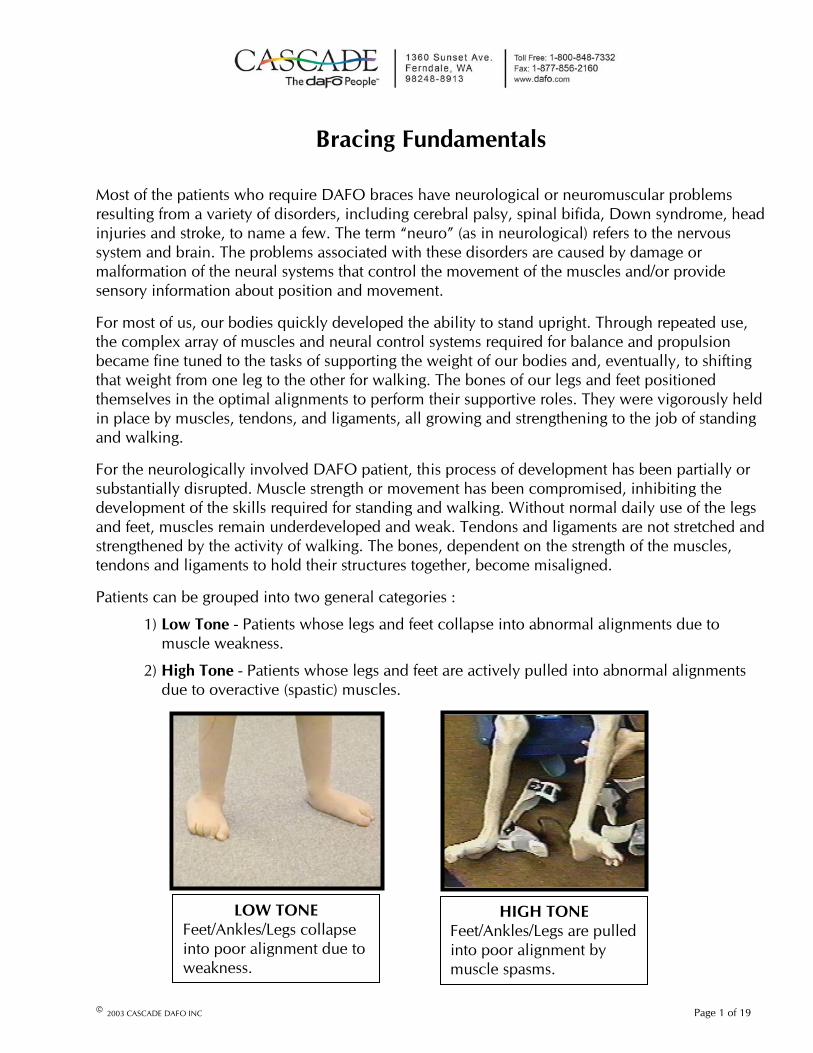
Patients can be grouped into two general categories :
1) Low Tone - Patients whose legs and feet collapse into abnormal alignments due to muscle weakness.
2) High Tone - Patients whose legs and feet are actively pulled into abnormal alignments due to overactive (spastic) muscles.
HIGH TONE Feet/Ankles/Legs are pulled into poor alignment by muscle spasms.
LOW TONEFeet/Ankles/Legs collapseinto poor alignment due to weakness.
© 2003 CASCADE DAFO INC Page 1 of 19

The severity and type of physical problems these patients experience varies considerably. Somehave very minor muscle control problems, perhaps causing a foot to drag a little as they walk. Some are affected on only one side of their bodies (hemiparesis), while the opposite side functions normally. For the most severely involved patients, the legs and feet are so weak or spastic, standing and walking are not possible at all. The closest we may come to experiencing this kind of control or sensory problem is when a leg “falls asleep” or a leg cramp occurs. Control of the leg (and walking) can be severely impaired until sensation is restored or the muscles relax. For the neurological patient, this condition is usually permanent.
The feet of most of our patients look very normal (when misalignments have been corrected) and the joints of the legs and feet are still very flexible. This is most true of younger patients. The abnormal alignments can be corrected and the improved alignments can be maintained with proper support. Over time, the corrected alignments will promote a more normal gait and prevent any permanent deformities.
For those patients afflicted with severe spasm or for those whose poor foot alignment has gone uncorrected for a long time, the feet and ankles begin to loose their flexibility and often develop permanent deformities of the bones and joints. For some of these patients, braces can be supportive enough to allow limited walking and standing, promoting improved joint flexibility and preventing deformities. For those whose condition is severe, the braces are intended to simply maintain a position that will prevent any further deformity.
AMBULATORY
NON-AMBULATORY
© 2003 CASCADE DAFO INC Page 2 of 19

DAFOs Compared to AFOs
The plastic Ankle Foot Orthosis (AFO) is an orthotic design that has been in use for many years. AFOs are rigid plastic shells that partially wrap around the posterior of the lower leg, the heel and under the foot (the Cascade “R” brace is a Regular AFO). Alignment corrections are dependent on straps that pull the patient’s heel and leg back against the rigid shape of the brace. The patient’s lower leg is locked into this rigid position. The muscles that were causing control or gait problems are supported by the brace, so stance and gait may be improved. Those muscles that were functioning well, however, may be over supported by the brace. Once use of the brace becomes routine, these functioning muscles become weaker over time through lack of use.
The Dynamic Ankle Foot Orthosis (DAFO) is a newer design concept using similar technology. The shell of each DAFO brace is formed on a plaster model of the patient’s foot that has been reshaped to a corrected foot alignment. The shell wraps very closely around the patient’s entire foot and ankle. The intimate fit of the shell allows for use of a thinner plastic to precisely correct and control foot position to a degree not possible in a standard AFO. The thinner plastic allows the shell to flex, making the brace more comfortable for the patient. The different DAFO styles offer a range of support and control posibilities that allow a brace to be tuned to the patient’s needs. Those muscles that are well controlled by the patient can remain active while the brace gives an appropriate level of control or support to the muscles that require assistance.
Misalignments of the Foot, Ankle and Knee
The goal of DAFO bracing is to support/control the patient’s feet so that:
1) Deformation of the foot structure is prevented or corrected
2) The ability of ambulatory patients to stand and walk is improved
For a brace to be successful, it must comfortably apply sufficient force to correct the alignments of the hindfoot, forefoot and ankle (to the degree they can be corrected) and support the patient in a better position of function. With the DAFO providing an improved base of support, the patient can more confidently progress with the devolopment of standing and walking skills.
For the typical DAFO patient, foot alignment problems fall into two primary categories:
Pronation – Heel everted; Forefoot abducted; Ankle dorsiflexedorSupination – Heel inverted; Forefoot adducted; Ankle plantarflexed
Pronation can generally be described as the use of the medial side of the foot (inside) to support and propel the body, while supination is the use of the lateral side of the foot (outside) to support and propel the body. The average person’s foot and ankle will use a combination of both pronation and supination to facilitate stance and gait, but will rarely use even a moderate degree of either position for long. Some may depend on pronation more than supination and vice versa,depending on factors such as muscle tone, joint flexibility, bone alignment, body weight and the types of activities pursued. As long as stance and gait are relatively efficient, even a moderate degree of pronation or supination may be considered “normal.” When excessive pronation or supination does affect stance or gait, causing discomfort or requiring extra effort to walk, thencorrecting foot alignment can be beneficial.
© 2003 CASCADE DAFO INC Page 3 of 19
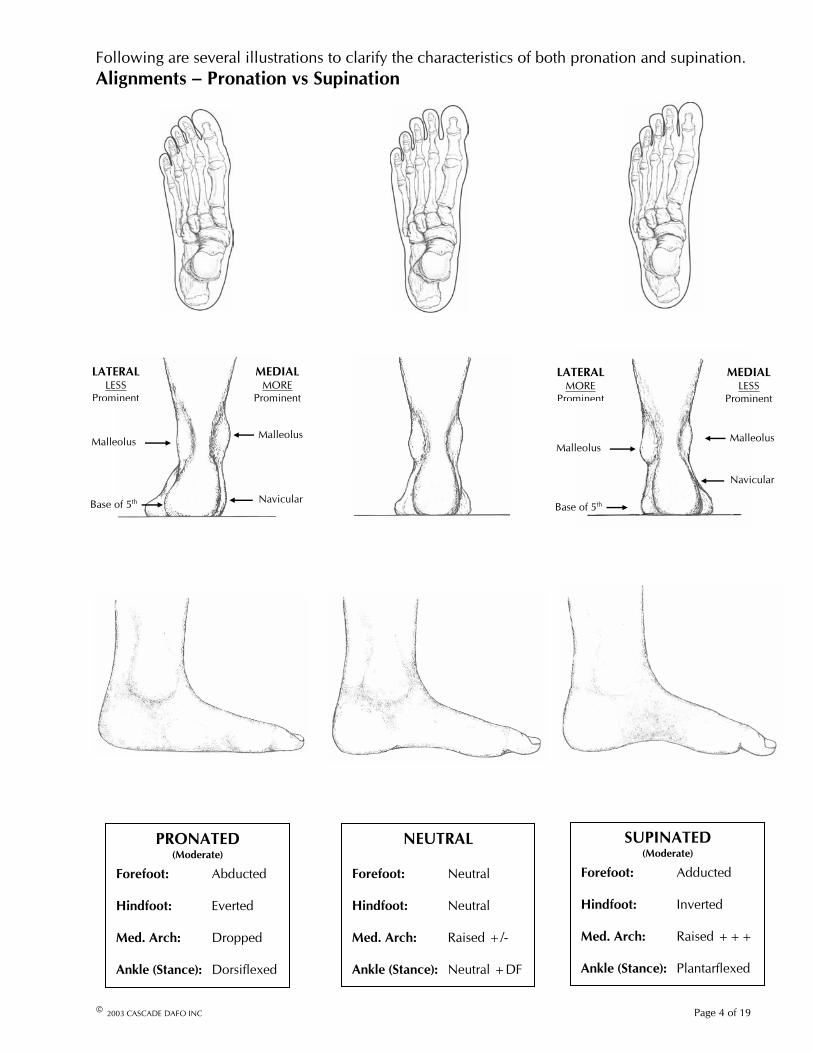
Following are several illustrations to clarify the characteristics of both pronation and supination.Alignments – Pronation vs Supination
Base of 5th
Malleolus
LATERALMORE
Prominent
Navicular
Malleolus
MEDIALLESS
Prominent
Navicular
MEDIALMORE
Prominent
Malleolus
LATERALLESS
Prominent
Base of 5th
Malleolus
SUPINATED(Moderate)
Forefoot: Adducted
Hindfoot: Inverted
Med. Arch: Raised +++
Ankle (Stance): Plantarflexed
NEUTRAL
Forefoot: Neutral
Hindfoot: Neutral
Med. Arch: Raised +/-
Ankle (Stance): Neutral +DF
PRONATED(Moderate)
Forefoot: Abducted
Hindfoot: Everted
Med. Arch: Dropped
Ankle (Stance): Dorsiflexed
© 2003 CASCADE DAFO INC Page 4 of 19

Regions of the Foot
Low Tone Pronation
When a low tone patient attempts to stand or walk, the muscles, tendons and ligaments that control the alignments of the feet are not strong enough to maintain correct alignment while supporting the weight of the body. Eventually, the body’s weight will force the ankle to rotate inward and down and the hindfoot to move outward (evert), stretching the tendons and ligaments. While the forefoot remains supported by the ground, the medial side of the midfoot rotates down and the medial arch flattens. This causes the medial side to lengthen, forcing the forefoot to splay outward into abduction. This pronated alignment causes the medial malleolus and the navicularbones to become more prominent, depending on the degree of pronation. The low tone pronator relies primarily on the medial side of the foot for support. To compensate for the collapsed medial side of the foot , the hip and knee flex and the ankle increases dorsiflexion.
High Tone Pronation
Unlike low tone pronation, where body weight causes the structure of the foot to collapse into pronation, high tone pronation is driven by over active muscles pulling the foot into a pronated position (the foot is externally rotated). The misalignment is often exacerbated by body weight and muscles that are weak despite high tone.
High Tone Supination
Similarly, high tone supination is driven by over active muscles pulling the foot into a supinated position. The medial side of the foot is pulled such that it rotates inward (internal rotation). This pulls the hindfoot into inversion and raises the medial arch, shortening the length of the medial side and pulling the forefoot into adduction. The lateral malleolus and the base of the 5th
metatarsal become more prominent. The high tone supinator relies primarily on the lateral side of the foot for support. To compensate for the lowered lateral side of foot, the hip and knee extend and the ankle increases plantarflexion.
To create a brace that corrects and controls the patient’s foot alignment, the various components of the foot that affect alignment are repositioned/reshaped during the casting process or on the plaster model of the patient’s foot. In effect, the misalignments characterized above are reversed. The brace shell is then formed on this “corrected” model. When placed on the patient’s foot, the brace shell applies pressure to or “loads” the areas of the foot that are misaligned, forcing the foot into the corrected alignments. If the plaster model has been shaped correctly, the brace will spread this corrective load over as wide an area as possible while unloading sensitive areas of the
© 2003 CASCADE DAFO INC Page 5 of 19

foot. The adjusted alignments must be in a range tolerable to the patient or the brace will put more pressure on the foot than is comfortable. As well, the volume and shape of the foot components must be maintained when being repositioned/reshaped in their new alignments. Too much volume (plaster model is too big) limits the brace’s ability to control position. Too little volume (plaster model is too small) causes the brace to be too tight. Over time, with the alignment corrections appropriately supported, the patient’s muscles, tendons and ligaments responsible for foot alignment will stretch or contract to adapt to the corrected alignment.
For the patient whose feet are fully correctable (near normal flexibility with no deformities), the optimal position of function for the DAFO is most often the neutral or balanced position between pronation and supination. A neutral alignment in the hindfoot of the brace forces the patient’s heel directly under the leg where it can best support the patient’s weight. Although forefoot movement is limited by the brace, there is usually sufficient flexibility to facilitate the activities of even the most active patient.
For the patient whose feet are fixed (tight or unmovable), the neutral position may not be tolerable. An improved alignment (less pronated or less supinated) will add stability and help prevent deformity.
The Ankle
xº Df / Pf AnkleJoint
Central Axisof Leg
Various muscles in the lower leg are responsible for movement of the foot, but the ankle joint controls where and how far the foot can move. The ankle acts like a hinge between the bones of the lower leg and the boney structure of the foot. When we speak of ankle position, we are usually referring to the position of the lower leg in relation to the foot. We characterize ankle position as an angle of the central axis of the leg compared to a plane parallel to the plantar surface of the foot, with the focus or flex point being the ankle joint.
Page 6 of 19
DorsiflexorContracture
PlantarflexorContracture
There are two major muscle groups in the lower legs that control foot movement. The large muscle groups on the back side of the leg (gastrocnemius, soleus) are attached to the heel and plantar (bottom) surface of the foot. When these muscles contract, the foot plantarflexes at the ankle (the foot pivots downwardor the leg pivots rearward). The much smaller muscle groups on the front side of the leg (anterior tibialis, digitorum, hallucis) are attached to the dorsal (top) surface of the foot and the toes. When these muscles contract, the foot dorsiflexes at the ankle (the foot pivots upward or the leg pivots forward).
Normally, these muscle groups make constant adjustments to balance the weight of the body over the feet. When the weight shifts too far forward, the sensory system feels the imbalance and directs the plantarflexion group of muscles to contract. When the weight shifts too far rearward, the dorsiflexion group
Gastrocnemius
Extensor Digitorum
Anterior TibialisSoleus
Extensor Hallucis
© 2003 CASCADE DAFO INC

of muscles contract. This balancing process occurs continuously while standing and becomessignificantly more complex when walking.
If the force exerted by one of these competing muscles groups becomes considerably stronger or weaker than the other, stance and gait are affected. In order to counteract the disproportionate forces exerted by an imbalance in the two muscle groups (or the disproportionate force of gravity on weakened muscles), features of the different brace styles can mechanically control the movement of the foot and leg at the ankle joint. These controlling mechanisms can either resist movement or block movement completely.
A common muscle imbalance treated with DAFOs is a condition commonly called “toe walking” where the plantarflexor muscles are overactive, overpowering the smaller (and weaker) dorsiflexor muscles.
When the child in example 1 walks, over-active calf muscles cause his feet to plantarflex excessively, bringing his heels off the ground. The patient’s weight is carried entirely by the toes and metatarsal heads. When he stops walking, the over-activity of the calf muscles ceases, his heels drop and, although the muscles and tendons are tight, he is able to dorsiflex enough to balance his weight with the aid of a stander.
Example 1
The child in example 2 has the same “toe walking” condition as in the above example. Wearing the DAFO 3 braces, plantarflexion is blocked by the posterior shell of the brace. The child adapts to the flat footed position and balances her body weight over the entire length of the foot. With this position maintained by the brace, dorsiflexion is encouraged, stretching the tight muscles and tendons of the leg.
Example 2
© 2003 CASCADE DAFO INC Page 7 of 19

TURBO DAFO 1
Free PF / DF
DAFO 4
Block PF / Free DF
DAFO 2 DAFO 3
Resist PF / DF
DAFO 3.5
The different DAFO styles vary most in the degree to which they control ankle position. Generally, the higher the brace is on the leg, the more control can be applied to the ankle. The DAFO 4 design allows both plantarflexion and dorsiflexion (no restriction or “free” movement). DAFOs 2 and 3 allow dorsiflexion, but block plantarflexion at a position set at the time of brace fabrication. The DAFO 3.5 offers a variable resistance to both plantarflexion and dorsiflexion. The level of resistance is determined by the size (flexibility) of the strut incorporated into the brace along the posterior side. As the leg (or foot) flexes, the opposing spring force exerted by the strut increases. The same spring like action that resists plantarflexion can also be said to assist dorsiflexion. When the plantarflexion motion or force is stopped, the energy stored in the flexed spring “assists” the leg-foot into dorsiflexion motion.
The DAFO styles mentioned above offer support options for patients with varying degrees of plantarflexion-dorsiflexion control. All make use of the “full wrap” shell for heel and forefoot control. When the patient has very little plantarflexion-dorsiflexion control, whether it involves excessively weak muscles or over active muscles, a more rigid brace design is required.
The DAFO Turbo offers an AFO style rigid posterior shell that can block very strong plantarflexion (high tone of the plantarflexor muscles). When a patient has very weak plantarflexor muscles (posterior calf) or weak leg extensor muscles (front thigh), their own body weight will cause them to sink down into a crouched position (excessive dorsiflexion).The anterior strap attached to the rigid posterior shell of the Turbo will provide support to a patient of moderate size. The Turbo design offers the extra advantage of the inner “full wrap” shell for heel and forefoot control.
For larger patients, severe crouching, or for cases where heel and forefoot control are not a priority, the DAFO 1 provides a very rigid anterior shell that is capable of supporting the full crouching weight of a large patient. Because the patient’s weight is distributed more evenly on the thick anterior shell of the brace (rather than just the anterior strap of the Turbo), more weight can be supported more comfortably. Unlike the designs previously mentioned, however, the DAFO 1 does not control heel or forefoot position as precisely as the full wrap designs.
© 2003 CASCADE DAFO INC Page 8 of 19

The Hindfoot
Because of its orientation directly under the leg, the hindfoot (or heel) provides substantial support of the body’s weight. During stance, it acts as the rear leg of a tripod with the 1st and 5th metheads in front, creating a stable “three point” platform. In non- weight bearing , the normal hindfoot has a flexibility range of 20º inward movement (inversion) to 10º outward movement (eversion). While in the weight bearing mode of walking or running, however, the hindfoot is normally held rigidly in-line with the leg. If allowed to flex too far out from under the leg, the tendons and ligaments that control hindfoot position can be overloaded by body weight and inertia, causing them to stretched and tear (sprained ankle).
Normal Hindfoot Range of Motion
The bones of the hindfoot, midfoot and forefoot are connected by ligaments in a flexible series of jBecause of these connections, position of the hindfoot can significantly influence the position and alignment of the midfoot and forefoot. Withthe task of supporting the entire weight of the body during stance and gait, as well as its influenon position of the rest of the foot, it is crucial to the success of a brace that the hindfoot be properly positioned and well secured. The shell of the brace will correct and maintain the medlateral position of the heel. The instep strap and heel lock features built into the shell prevent the heel from rising up out of its corrected position in the brace.
oints.
ce
ial-
Again, for the patient whose feet are fully correctable, the best alignment for the hindfoot is in the neutral position (vertical) so that the weight of the body can be efficiently and confidently supported. For the patient whose hindfoot is fixed (tight or unmovable), the neutral position may not be tolerable. An improved alignment (less everted or less inverted) securely supported by the brace shell will promote stability and patient confidence.
Everted Heel - In Fig. 1, the patient’s body weight pushes down on the ankles and feet. Due to lack of muscle tone or control, the patient’s weight causes the ankles to rotate inward and down, shifting the hindfoot into an everted alignment.
Fig. 2 Fig. 1
© 2003 CASCADE DAFO INC Page 9 of 19
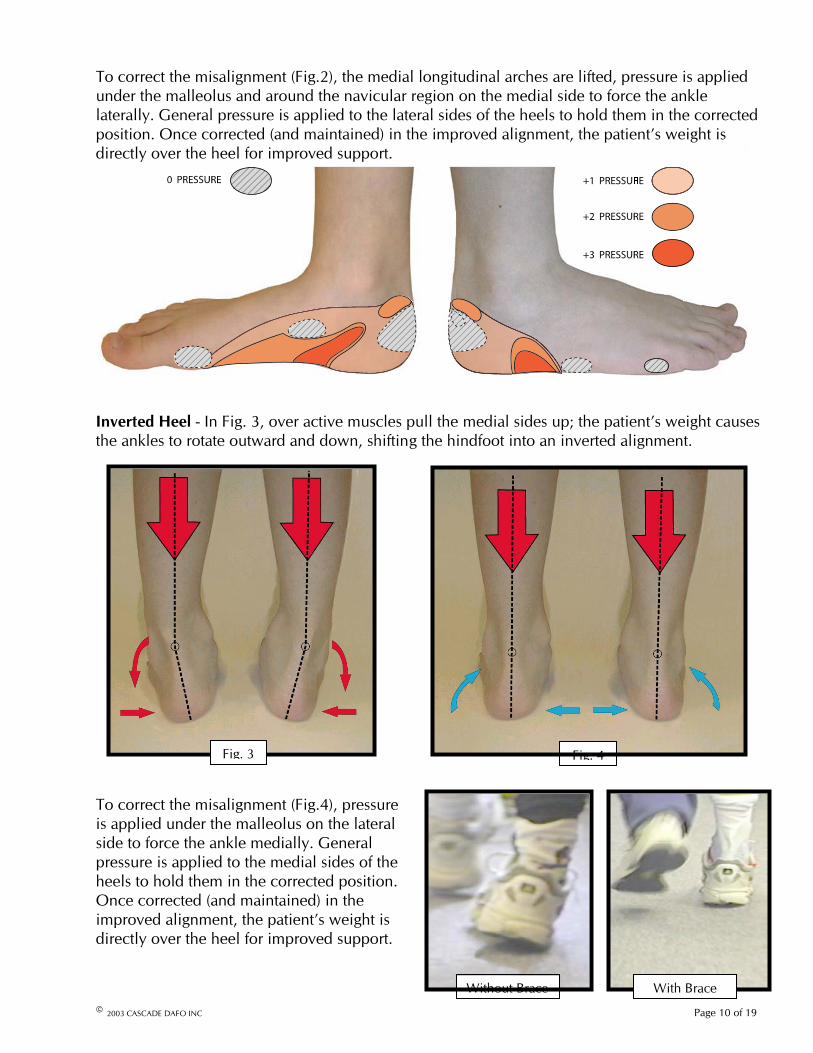
Fig. 3 Fig. 4
To correct the misalignment (Fig.2), the medial longitudinal arches are lifted, pressure is applied under the malleolus and around the navicular region on the medial side to force the ankle laterally. General pressure is applied to the lateral sides of the heels to hold them in the corrected position. Once corrected (and maintained) in the improved alignment, the patient’s weight is directly over the heel for improved support.
Inverted Heel - In Fig. 3, over active muscles pull the medial sides up; the patient’s weight causes the ankles to rotate outward and down, shifting the hindfoot into an inverted alignment.
To correct the misalignment (Fig.4), pressure is applied under the malleolus on the lateral side to force the ankle medially. General pressure is applied to the medial sides of the heels to hold them in the corrected position. Once corrected (and maintained) in the improved alignment, the patient’s weight is directly over the heel for improved support.
With Brace Without Brace
© 2003 CASCADE DAFO INC Page 10 of 19
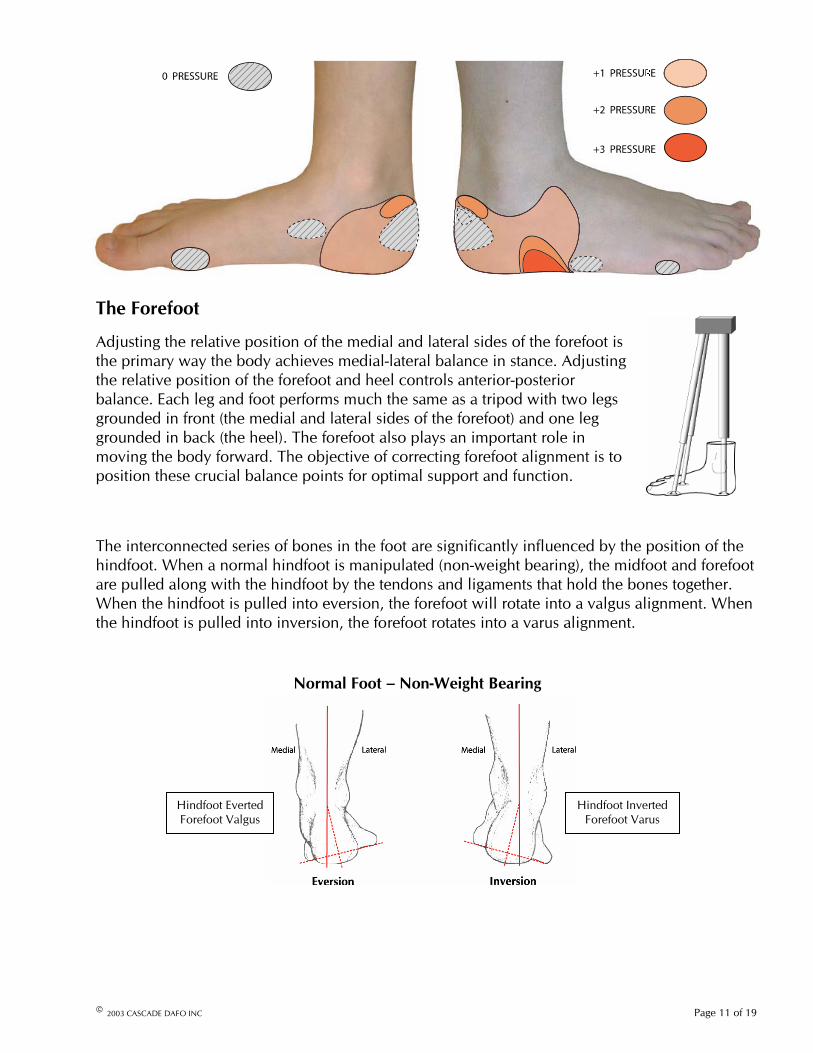
The Forefoot
Adjusting the relative position of the medial and lateral sides of the forefoot is the primary way the body achieves medial-lateral balance in stance. Adjusting the relative position of the forefoot and heel controls anterior-posterior balance. Each leg and foot performs much the same as a tripod with two legs grounded in front (the medial and lateral sides of the forefoot) and one leg grounded in back (the heel). The forefoot also plays an important role in moving the body forward. The objective of correcting forefoot alignment is to position these crucial balance points for optimal support and function.
The interconnected series of bones in the foot are significantly influenced by the position of the hindfoot. When a normal hindfoot is manipulated (non-weight bearing), the midfoot and forefoot are pulled along with the hindfoot by the tendons and ligaments that hold the bones together. When the hindfoot is pulled into eversion, the forefoot will rotate into a valgus alignment. When the hindfoot is pulled into inversion, the forefoot rotates into a varus alignment.
Normal Foot – Non-Weight Bearing
Fig. 5 Hindfoot Inverted Forefoot Varus
Hindfoot Everted Forefoot Valgus
© 2003 CASCADE DAFO INC Page 11 of 19
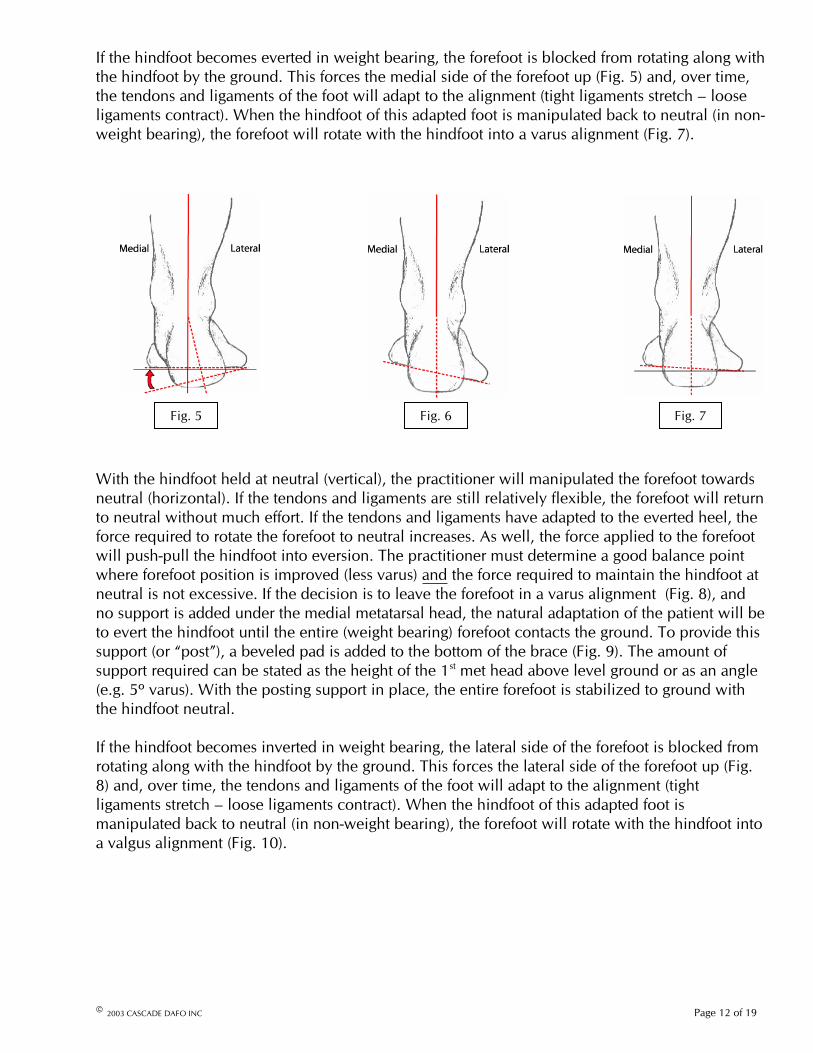
If the hindfoot becomes everted in weight bearing, the forefoot is blocked from rotating along with the hindfoot by the ground. This forces the medial side of the forefoot up (Fig. 5) and, over time, the tendons and ligaments of the foot will adapt to the alignment (tight ligaments stretch – looseligaments contract). When the hindfoot of this adapted foot is manipulated back to neutral (in non-weight bearing), the forefoot will rotate with the hindfoot into a varus alignment (Fig. 7).
Fig. 5 Fig. 6 Fig. 7
With the hindfoot held at neutral (vertical), the practitioner will manipulated the forefoot towards neutral (horizontal). If the tendons and ligaments are still relatively flexible, the forefoot will return to neutral without much effort. If the tendons and ligaments have adapted to the everted heel, the force required to rotate the forefoot to neutral increases. As well, the force applied to the forefoot will push-pull the hindfoot into eversion. The practitioner must determine a good balance point where forefoot position is improved (less varus) and the force required to maintain the hindfoot at neutral is not excessive. If the decision is to leave the forefoot in a varus alignment (Fig. 8), and no support is added under the medial metatarsal head, the natural adaptation of the patient will be to evert the hindfoot until the entire (weight bearing) forefoot contacts the ground. To provide thissupport (or “post”), a beveled pad is added to the bottom of the brace (Fig. 9). The amount ofsupport required can be stated as the height of the 1st met head above level ground or as an angle (e.g. 5º varus). With the posting support in place, the entire forefoot is stabilized to ground with the hindfoot neutral.
If the hindfoot becomes inverted in weight bearing, the lateral side of the forefoot is blocked from rotating along with the hindfoot by the ground. This forces the lateral side of the forefoot up (Fig. 8) and, over time, the tendons and ligaments of the foot will adapt to the alignment (tight ligaments stretch – loose ligaments contract). When the hindfoot of this adapted foot is manipulated back to neutral (in non-weight bearing), the forefoot will rotate with the hindfoot into a valgus alignment (Fig. 10).
© 2003 CASCADE DAFO INC Page 12 of 19

Fig.10Fig.9Fig.8
d
The force applied to correct the forefoot will push-pull the hindfoot into inversion. The practitioner determines a good balance point where forefoot position is improved (less valgus) athe force required to maintain the hindfoot at neutral is notexcessive. If the forefoot is left in a valgus alignment (Fig. 12), the raised forefoot is supported by adding a beveled pad to the bottom of the brace (Fig. 11). The amount of support required can be stated as the height of the 5th met head above level ground or as an angle (e.g. 5º valgus – from bottom of 1st to bottom of 5th).With the posting support in place, the entire forefoot is stabilized to ground with the hindfoot neutral.
n
Fig. 11 - Extrinsic Valgus Post
To correct forefoot alignment, the forefoot region of the plaster model is reshaped with the “new” forefoot in the corrected alignment (Fig.12). The shell of the brace takes on the corrected shape. With the shell wrapped very closely around the forefoot (and the strap cinched tight) the brace material pulls the forefoot into the corrected position and resists the forefoot’s tendency to rotate back to the improper alignment (Fig.13). In order for the brace to maintain control, the cross-sectional shape of the forefoot region must be accurate so that the shell fits very close to the surface of the foot. If it is too loose around the foot (Fig.14), the forefoot will not be held inposition properly. If it is too tight, the brace is uncomfortable to wear.
Fig.13GAP
Poor FitCorrect Fit
Fig.14
Corrected ModelUncorrected Model
Fig.12
© 2003 CASCADE DAFO INC Page 13 of 19
Alignment Corrections: Evaluation of the Plaster Positive
Creation of an accurate model of a patient’s foot and lower leg is the first step in the production of a DAFO brace. The accuracy of the fit and alignment of the finished DAFO is dependent on the skills and experience of the practitioner casting the patient, as well as the judgment of the modifier that prepares the positive created from the cast. The experience of the practitioners that cast patients varies considerably, so it is not surprising that the quality of casts received varies considerably as well. Even for the highly skilled practitioner, the task of casting a frightened and combative patient will often result in below average cast quality.
The following are general guidelines when evaluating a rough plaster positive:
• Most of the feet we make braces for are normal in proportions and contours.
• Most of the feet we make braces for can be corrected to neutral (vertical heel, horizontal forefoot, 3 degrees dorsiflexion).
• The smaller the foot, the more likely it is normal in shape and correctable.
• Features on positives that look odd are usually casting defects (but not always).
• Smaller feet cast with less accuracy.
• Larger feet cast with more accuracy.
• Good Cast Quality: details are more meaningful; less shaping is necessary.
• Poor Cast Quality: details are less meaningful; more shaping is necessary.
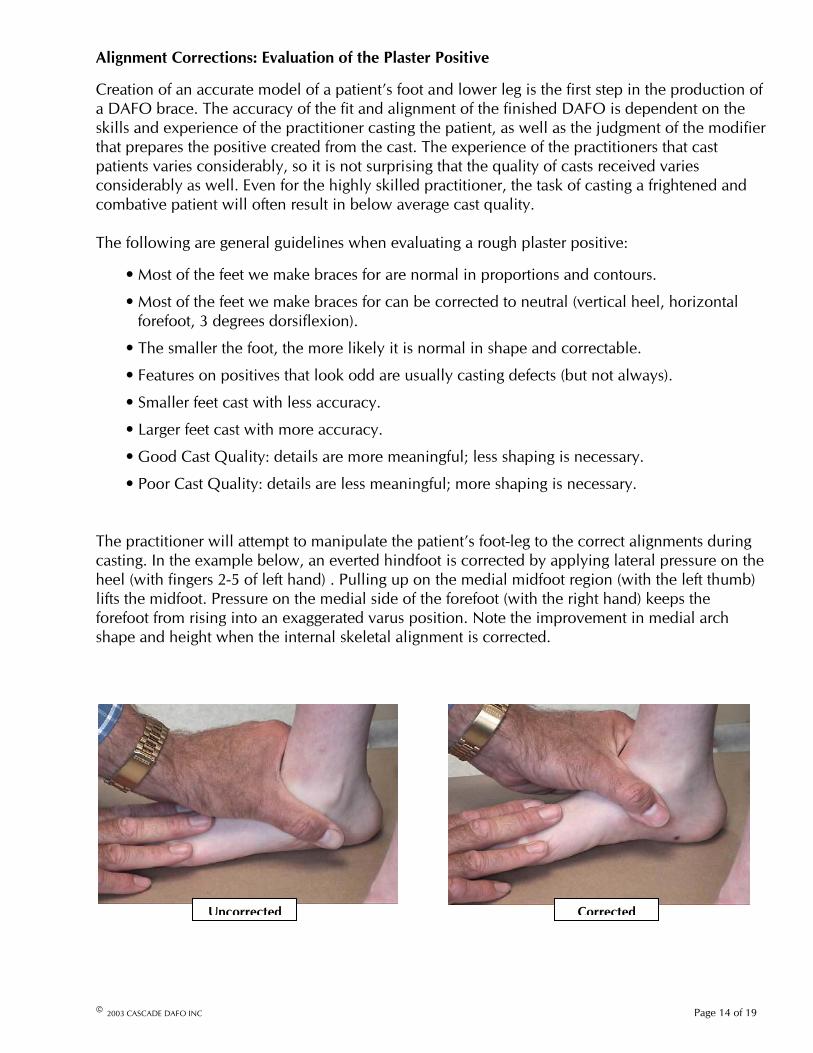
The practitioner will attempt to manipulate the patient’s foot-leg to the correct alignments during casting. In the example below, an everted hindfoot is corrected by applying lateral pressure on the heel (with fingers 2-5 of left hand) . Pulling up on the medial midfoot region (with the left thumb) lifts the midfoot. Pressure on the medial side of the forefoot (with the right hand) keeps the forefoot from rising into an exaggerated varus position. Note the improvement in medial arch shape and height when the internal skeletal alignment is corrected.
CorrectedUncorrected
© 2003 CASCADE DAFO INC Page 14 of 19

If the corrected alignments have not been captured in the cast, further corrections to the cast before filling or to the positive produced from the cast may be needed. The requirements of the three most important alignments – Ankle, Hindfoot and Forefoot – are noted on each order form. Other alignment or support corrections (e.g. medial arch support, ST support, forefoot ab / adduction correction, etc.) will be noted on the order form.
A preliminary examination of the plaster positive and order form is essential to assess the accuracy of the plaster positive(s) and to develop a sensible plan for modification. Obviously, a relatively high quality cast increases the likelihood that the plaster positive is an accurate rendering of the foot, requiring only the minimal amount of shaping by the modifier. As the quality of the plaster positive decreases, the final shape becomes more dependent on the modifier’s contribution. If the contours and features of the positive are obscured or distorted due to poor casting, then it is up to the modifier to apply his knowledge of the structures, contours and proportions of the foot to sensibly (and conservatively) shape the less-than-perfect positives. For the positives of poorest quality, the modifier must decide whether or not there is enough “good shape” to proceed or whether it’s more prudent to ask for a recast or assistance in developing a sensible plan.
Successful shaping of the plaster positive depends on an understanding of:
1) The normal structure, proportions and contours of the foot and leg.
2) “Normal” differences in the structure, proportions and contours of the chronically misaligned foot and leg.
3) Casting errors (and how to correct them).
4) Contour alterations to improve alignment and promote comfort in the finished brace.
It is not a coincidence that sculptors and painters study human and animal anatomy. To accuratelyrender a sculpture or painting of a body one must understand the internal structures to understand their influence on the external shape. While each foot is unique, the basic structure and proportions of the feet are consistent. Variations due to chronic low tone or misalignment are also relatively consistent. Accurately approximating the size and position of a “missing piece” ispossible when one has sufficient knowledge of normal anatomical structure and proportion, an understanding of the variations that occur, and sufficient accurate anatomical landmarks on which to base the approximation. The more “good” information there is available on the plaster positive, the more confident one can be of an accurate approximation. Understanding the limitations of the casting process can help identify flawed or distorted features on the positive resulting from the casting process.
© 2003 CASCADE DAFO INC Page 15 of 19
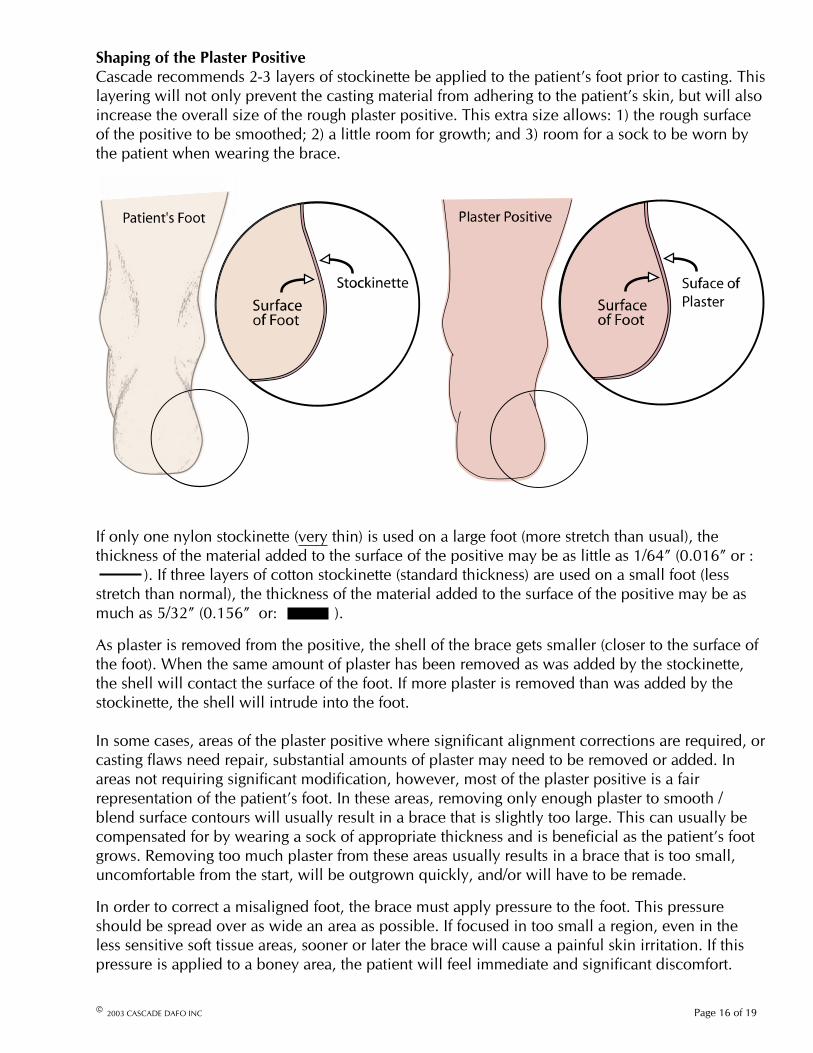
Shaping of the Plaster PositiveCascade recommends 2-3 layers of stockinette be applied to the patient’s foot prior to casting. This layering will not only prevent the casting material from adhering to the patient’s skin, but will also increase the overall size of the rough plaster positive. This extra size allows: 1) the rough surface of the positive to be smoothed; 2) a little room for growth; and 3) room for a sock to be worn by the patient when wearing the brace.
If only one nylon stockinette (very thin) is used on a large foot (more stretch than usual), the thickness of the material added to the surface of the positive may be as little as 1/64” (0.016” or : ). If three layers of cotton stockinette (standard thickness) are used on a small foot (less stretch than normal), the thickness of the material added to the surface of the positive may be as much as 5/32” (0.156” or: ).
As plaster is removed from the positive, the shell of the brace gets smaller (closer to the surface of the foot). When the same amount of plaster has been removed as was added by the stockinette, the shell will contact the surface of the foot. If more plaster is removed than was added by the stockinette, the shell will intrude into the foot.
In some cases, areas of the plaster positive where significant alignment corrections are required, or casting flaws need repair, substantial amounts of plaster may need to be removed or added. In areas not requiring significant modification, however, most of the plaster positive is a fairrepresentation of the patient’s foot. In these areas, removing only enough plaster to smooth /blend surface contours will usually result in a brace that is slightly too large. This can usually be compensated for by wearing a sock of appropriate thickness and is beneficial as the patient’s foot grows. Removing too much plaster from these areas usually results in a brace that is too small,uncomfortable from the start, will be outgrown quickly, and/or will have to be remade.
In order to correct a misaligned foot, the brace must apply pressure to the foot. This pressure should be spread over as wide an area as possible. If focused in too small a region, even in theless sensitive soft tissue areas, sooner or later the brace will cause a painful skin irritation. If this pressure is applied to a boney area, the patient will feel immediate and significant discomfort.
© 2003 CASCADE DAFO INC Page 16 of 19

Boney areas should be:
1) Protected ( not shaved down during modification)and / or
2) Built-Up (Covered with Additional Plaster)
Soft tissue areas should be:
1) Used as key areas to apply correction pressuresand
2) Shaped naturally in order to spread the correction pressure over a wider area (avoid point loading).
The following drawings illustrate the how proper and improper modification of the plaster positive will affect brace fit:
Protected
In Figure 15 (A), a boney prominence is shown surrounded by soft tissue.
A
The boney prominence is evident and relatively accurate in the plaster positive (B). B
The boney prominence is protected and the soft tissue areas around the bone are shaved down (C). C
The plastic shell is pulled over the plaster positive. The plastic shell takes on the same shape as the modified plaster positive (D). D
When the brace is placed on the actual foot, little or no pressure is placed on the protected boney prominence,while the force required to correct foot alignment is spread out on the soft tissues surrounding the bone (E).
E
Fig. 15
© 2003 CASCADE DAFO INC Page 17 of 19
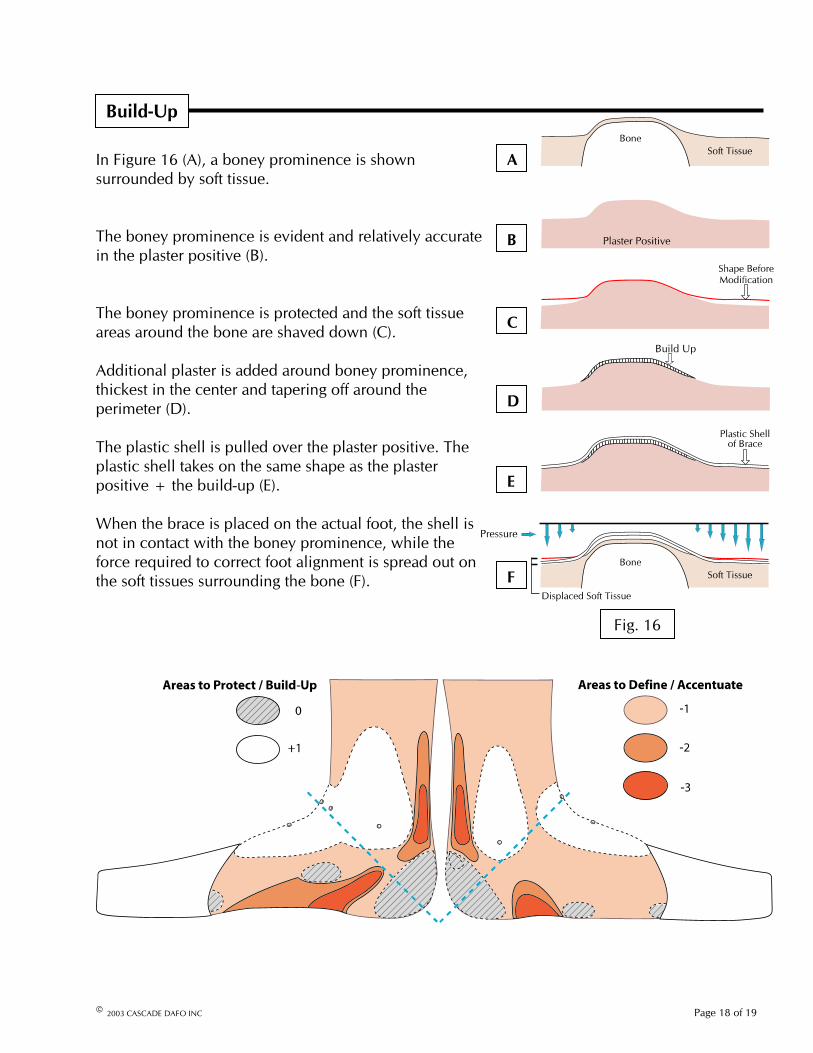
AIn Figure 16 (A), a boney prominence is shown surrounded by soft tissue.
The boney prominence is evident and relatively accurate in the plaster positive (B).
B
The boney prominence is protected and the soft tissue areas around the bone are shaved down (C).
Additional plaster is added around boney prominence, thickest in the center and tapering off around the perimeter (D). D
The plastic shell is pulled over the plaster positive. Theplastic shell takes on the same shape as the plaster positive + the build-up (E).
Build-Up
C
E
When the brace is placed on the actual foot, the shell is not in contact with the boney prominence, while the force required to correct foot alignment is spread out on the soft tissues surrounding the bone (F). F
Fig. 16
© 2003 CASCADE DAFO INC Page 18 of 19
© 2003 CASCADE DAFO INC Page 19 of 19
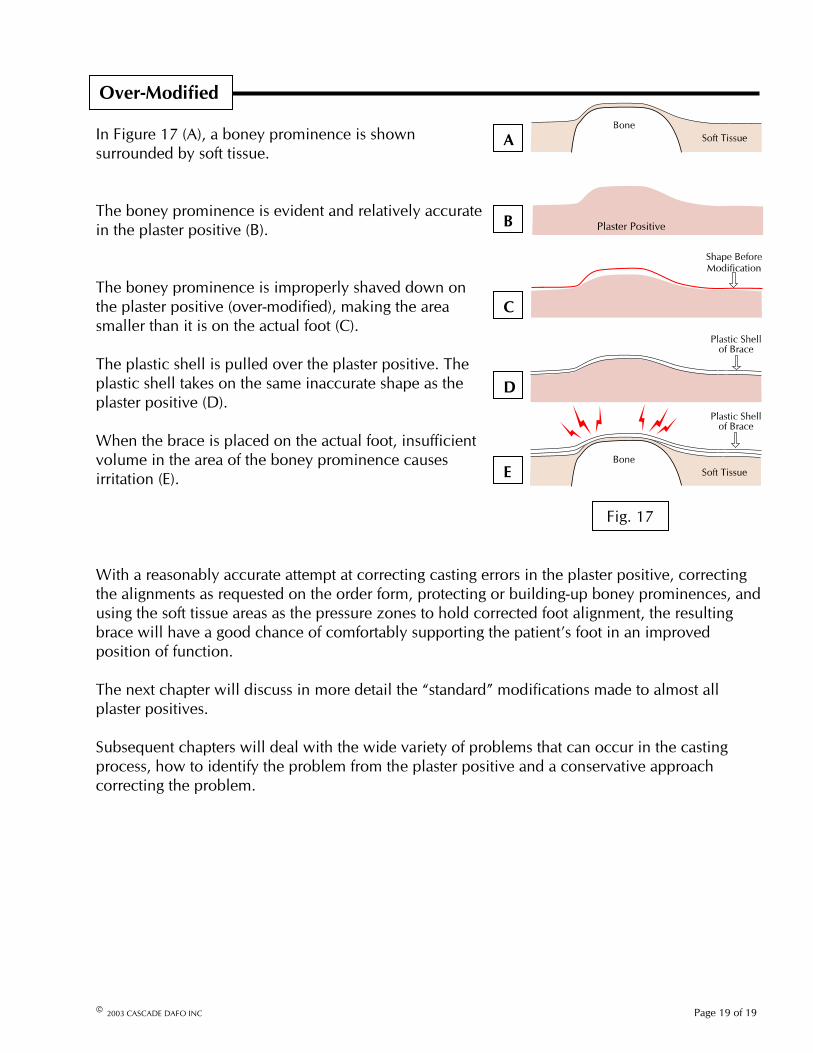
In Figure 17 (A), a boney prominence is shown surrounded by soft tissue.
A
The boney prominence is evident and relatively accurate in the plaster positive (B). B
The boney prominence is improperly shaved down on the plaster positive (over-modified), making the area smaller than it is on the actual foot (C).
Over-Modified
C
The plastic shell is pulled over the plaster positive. The plastic shell takes on the same inaccurate shape as the plaster positive (D).
D
When the brace is placed on the actual foot, insufficient volume in the area of the boney prominence causes irritation (E). E
Fig. 17
With a reasonably accurate attempt at correcting casting errors in the plaster positive, correctingthe alignments as requested on the order form, protecting or building-up boney prominences, and using the soft tissue areas as the pressure zones to hold corrected foot alignment, the resulting brace will have a good chance of comfortably supporting the patient’s foot in an improved position of function.
The next chapter will discuss in more detail the “standard” modifications made to almost all plaster positives.
Subsequent chapters will deal with the wide variety of problems that can occur in the casting process, how to identify the problem from the plaster positive and a conservative approach correcting the problem.