the evolving role of i.v. iron in cancer patients – expert ... · epo growth factors + scf, il3,...
TRANSCRIPT

ANEMIA
Parameters

Epo
Growth factors
+ SCF, IL3, GM-CSF
- TGFβ, TNFα, IFNγ
SREFe
ERYTHROPOIESISRegulation
Kidney Bone marrow Macrophages
Hormones (androgens,
thyroid)
Vitamins
(folate, B12)

CirculatingRBC
Liver
Plasma
Intestinalabsorption
Macrophages(RE cells)
Erythroidmarrow
1 mg
3 mg
25 mg25 mg
3 mg
IRON METABOLISMIron compartments
Fe

• GR (106/µL) 4.4-5.7 4.0-5.2
• Hb (gr/dL) 13.5-17.0 12.0-15.0
• Hct (%) 40-52 36-45
• MCV (µ3) 80-100
• MCH (pg) 27-33
• %HYPO (%) < 5%
• Reticulocytes (103/µL) 25-100
• Reticulocytes (%) 0.5-2.5
• CHr (pg) 26-31
RBCRBC parameters
Men Women

• MCV (µ3) : Hct/GR = volume
→ Anemia Microcytic MCV < 80Normocytic MCV 80-100Macrocytic MCV > 100
• MCH (pg) : Hb/GR = amount of Hb per RBC
→ Anemia Hypochromic MCH < 27Normochromic MCH 27-33Hyperchromic MCH > 33
• MCHC (g/dL) : Hb/Hct (not interesting)
RBCRBC parameters
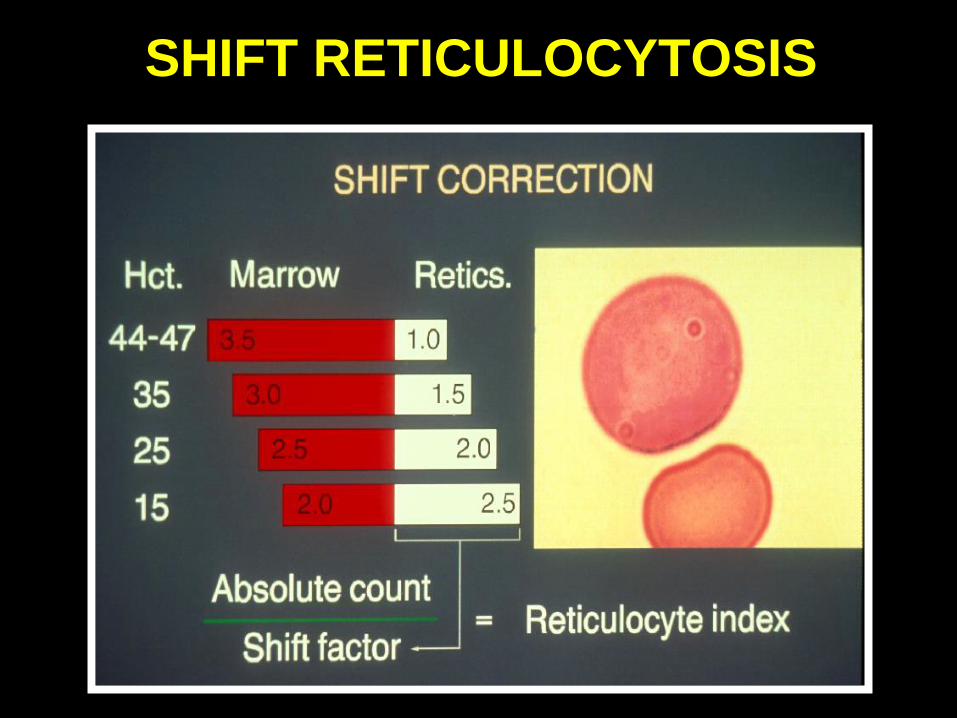
SHIFT RETICULOCYTOSIS

IRON PARAMETERSStorage iron : serum ferritin
CirculatingRBC
Liver
Plasma
Macrophages(RE cells)
Erythroidmarrow
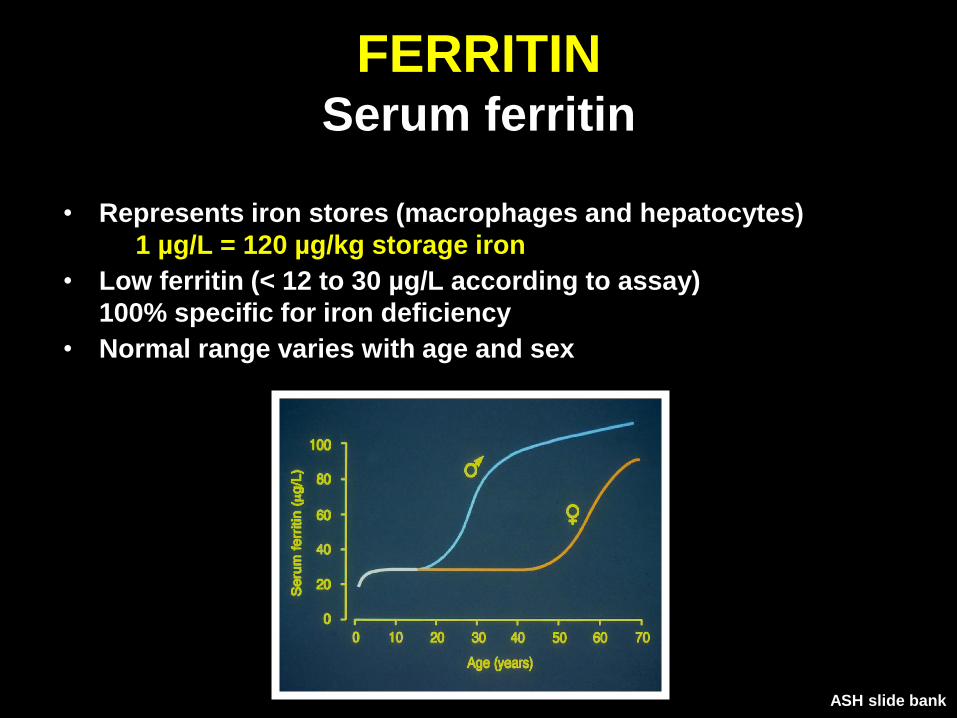
FERRITINSerum ferritin
• Represents iron stores (macrophages and hepatocytes)
1 µg/L = 120 µg/kg storage iron
• Low ferritin (< 12 to 30 µg/L according to assay)
100% specific for iron deficiency
• Normal range varies with age and sex
ASH slide bank
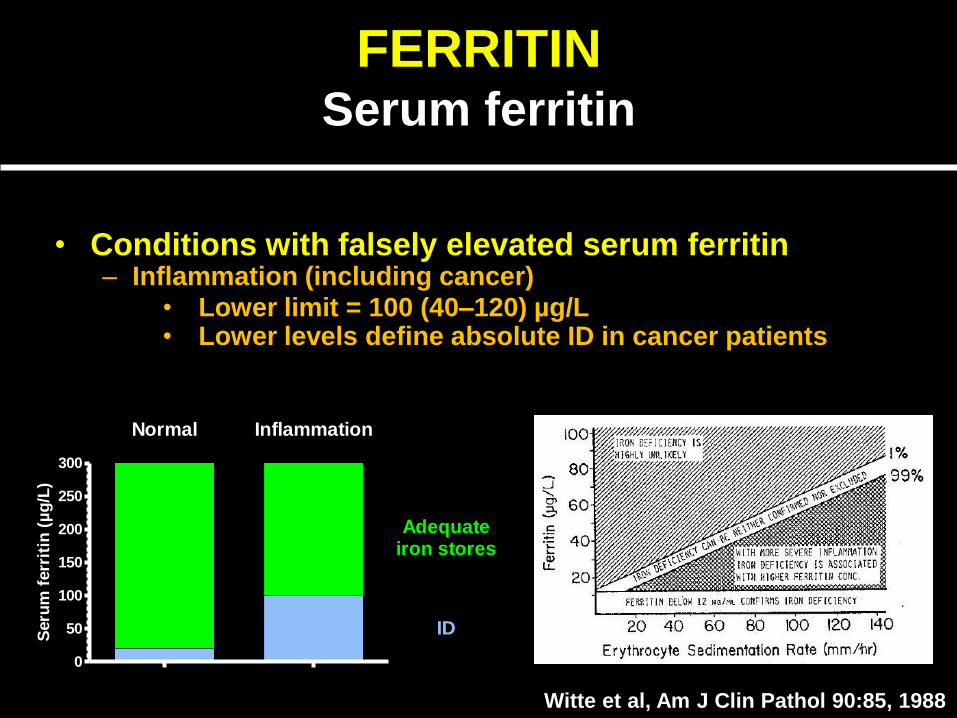
• Conditions with falsely elevated serum ferritin– Inflammation (including cancer)
FERRITINSerum ferritin
Witte et al, Am J Clin Pathol 90:85, 1988
0
50
100
150
200
250
300
Normal Inflammation
ID
Adequateiron stores
Seru
m f
err
itin
(µ
g/L
)
• Lower limit = 100 (40–120) µg/L• Lower levels define absolute ID in cancer patients
FERRITINSerum ferritin
• Conditions with falsely elevated serum ferritin– Inflammation (including cancer)
• Lower limit 40–120 µg/L
• Lower levels define absolute iron deficiency in cancer
patients
– Some forms of cancer (e.g. neuroblastoma)
– Renal failure (lower limit 40–100 µg/L)
– Liver damage
– Hyperthyroidism
– Poorly controlled diabetes mellitus (ferritin glycosylation)
– Hyperferritin-cataract syndrome
– Benign hyperferritinaemia

CirculatingRBC
Liver
Plasma
Macrophages(RE cells)
Erythroidmarrow
IRON PARAMETERSPlasma iron : transferrin saturation

TRANSFERRIN SATURATIONNormal
Plasma
Transferrin
Macrophages Marrow
Fe
Fe
Red blood
cells
Dynamic equilibrium of
transferrin saturation
Recycling and storage
of iron from red blood
cells
Sufficient iron
available for
erythropoiesis
Senescent RBCs
taken-up by
macrophages
SeFe 8-30 µmol/L
Tsat 20-45 %
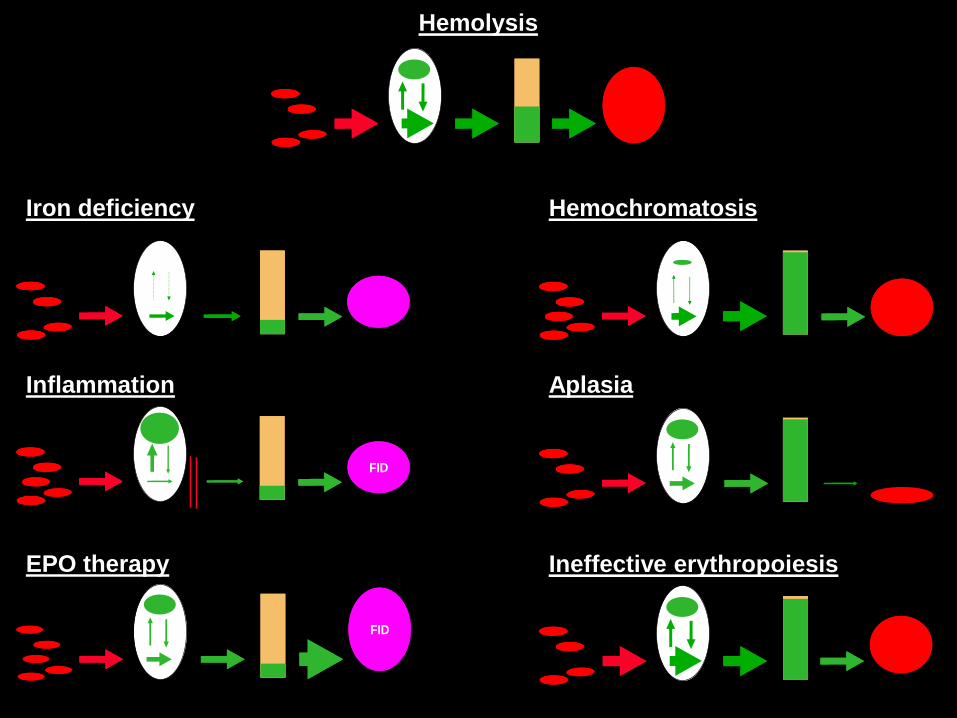
FIDFID
FIDFID
Inflammation
EPO therapy
HemochromatosisIron deficiency
Aplasia
Hemolysis
Ineffective erythropoiesis

CirculatingRBC
Liver
Plasma
Macrophages(RE cells)
Erythroidmarrow
IRON PARAMETERSErythroid marrow: sTfR

SOLUBLE TRANSFERRIN RECEPTORErythropoiesis
AA CRF Chemo0
2
4
6
8
10
(n=20) (n=61)(n=58)
Normals
TfR
(m
g/L
)
AIHA HS Thal HbH PC0
10
20
30
40
50
60
70
(n=20) (n=11)(n=72)
Normal
(n=12)(n=8)
sT
fR (
mg
/L)
Hyperplastic Hypoplastic
sTfR 3-7 µg/l
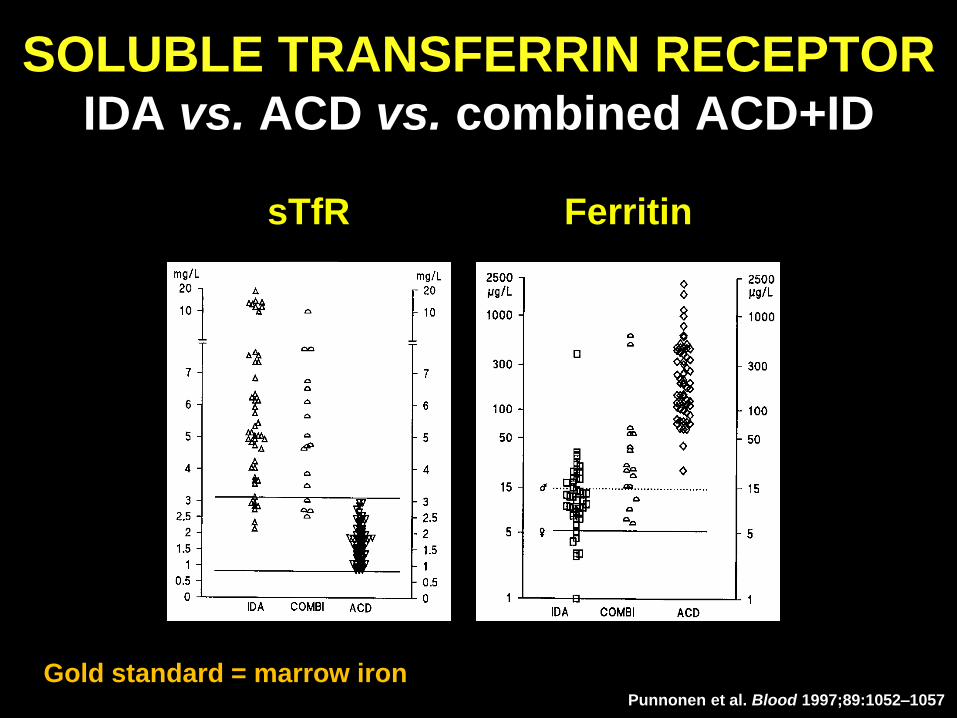
Punnonen et al. Blood 1997;89:1052–1057
sTfR Ferritin
Gold standard = marrow iron
SOLUBLE TRANSFERRIN RECEPTORIDA vs. ACD vs. combined ACD+ID
CirculatingRBC
Liver
Plasma
Macrophages(RE cells)
Erythroidmarrow
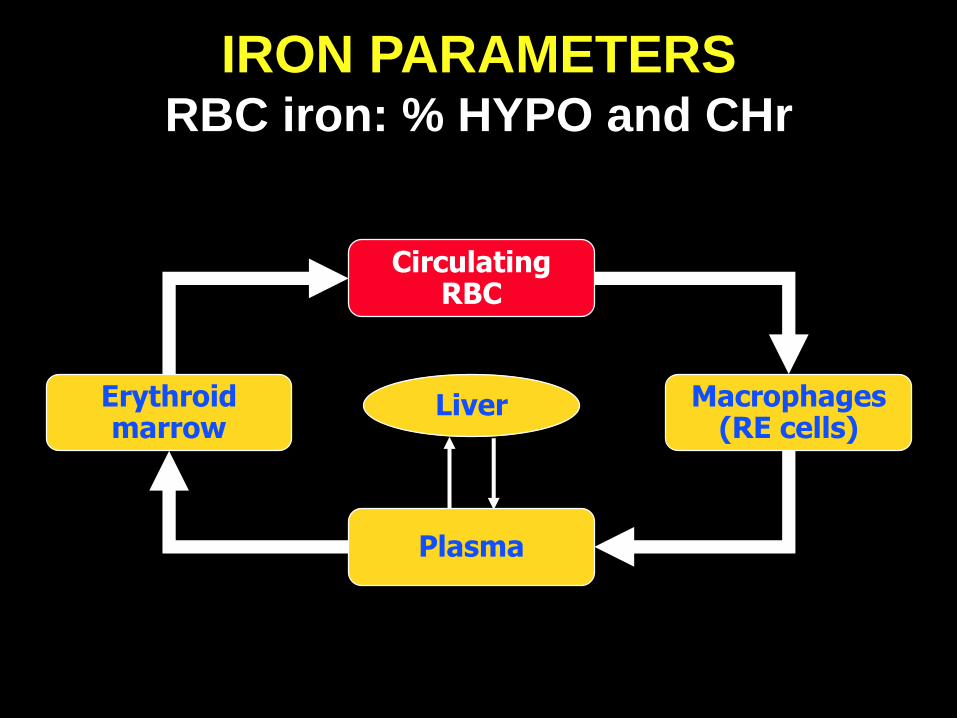
IRON PARAMETERSRBC iron: % HYPO and CHr
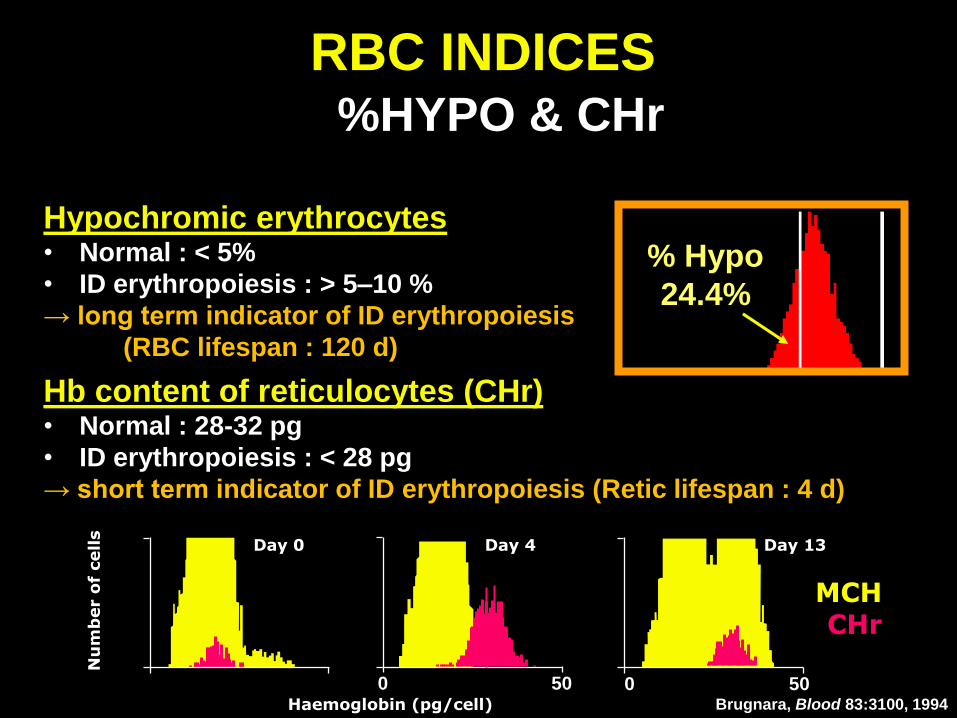
Hypochromic erythrocytes• Normal : < 5%
• ID erythropoiesis : > 5–10 %
→ long term indicator of ID erythropoiesis
(RBC lifespan : 120 d)
% Hypo
24.4%
Hb content of reticulocytes (CHr)• Normal : 28-32 pg
• ID erythropoiesis : < 28 pg
→ short term indicator of ID erythropoiesis (Retic lifespan : 4 d)
Nu
mb
er o
f cells
Haemoglobin (pg/cell)
Day 13
500
Day 4
500
Day 0
MCHCHr
Brugnara, Blood 83:3100, 1994
RBC INDICES%HYPO & CHr
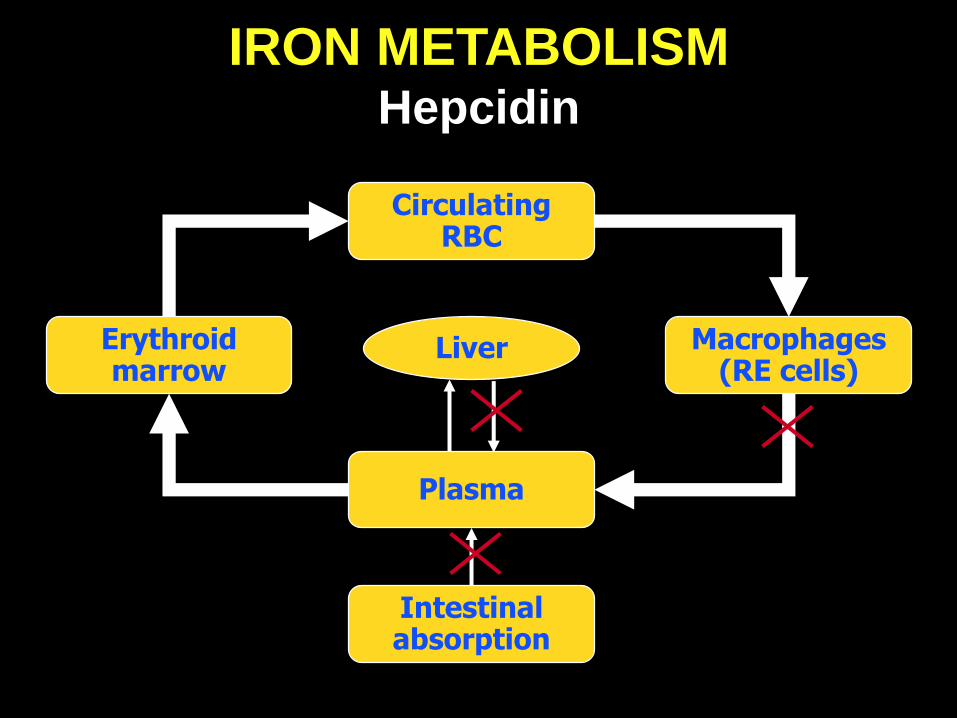
CirculatingRBC
Liver
Plasma
Intestinalabsorption
Macrophages(RE cells)
Erythroidmarrow
IRON METABOLISMHepcidin
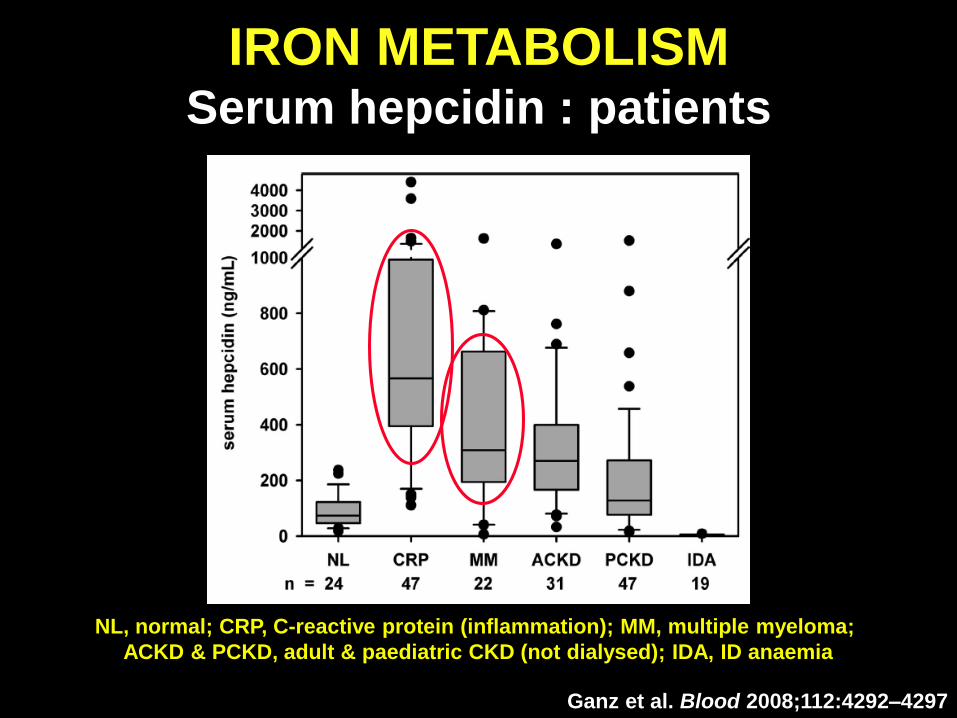
Ganz et al. Blood 2008;112:4292–4297
NL, normal; CRP, C-reactive protein (inflammation); MM, multiple myeloma;
ACKD & PCKD, adult & paediatric CKD (not dialysed); IDA, ID anaemia
IRON METABOLISMSerum hepcidin : patients

ERYTHROPOIETINSerum erythropoietin
Serum EPO 10-20 U/ml
Relative to degree of anemia !
Cazzola et al,
Blood 89:4250, 1997

ERYTHROPOIETINSerum Epo & erythropoietic activity

ERYTHROID FUNCTIONParameters
Retic (effective erythropoiesis)
Hb - Hct - RBC
MCV - MCH
SeFe
Tf sat(marrow iron supply)
sTfR(total erythropoiesis)
Ferritin(iron stores)
Macrophages
EPO
CHr
Hypochromic RBC(marrow iron supply)

ANEMIA
Anemias due to
defective red cell production
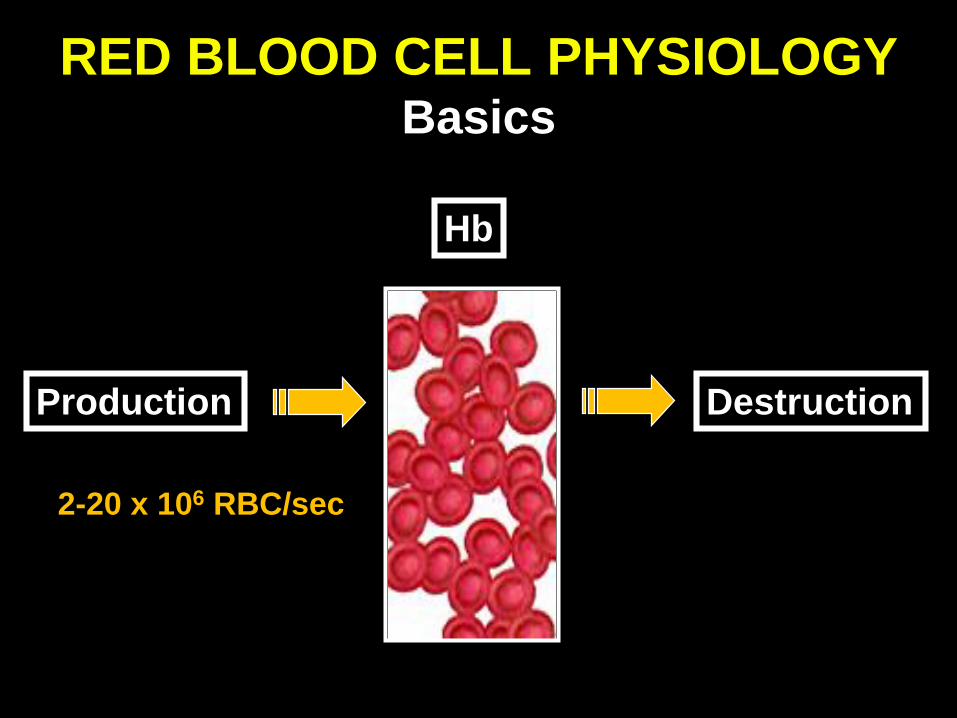
RED BLOOD CELL PHYSIOLOGYBasics
Production Destruction
2-20 x 106 RBC/sec
Hb

• Red cell production- Erythroid marrow- Erythropoietin- Iron
ANEMIA3 major mechanisms
• Red cell loss - Hemolysis
- Hemorrhage
• Maturation defects
- DNA (folate, B12, …)
- Hb • Globin
• Heme
- Myelodysplasia

• Decreased erythroid precursors - Marrow damage :
• Global : SAA, chemotherapy, …
• Pure red cell aplasia
- Marrow replacement : myelofibrosis, tumor cells
- Marrow inhibition
• Decreased Epo production- Renal failure
- Hypothyroidism, hypopituitarism
• Decreased iron availability- Absolute : ID
- Functional : inflammation
ANEMIADefective red cell production

• Microcytic : serum iron / TSat- Low : ID or inflammation
- High : maturation defect (globin, heme)
• Normocytic : reticulocytes- N/low : acute hemorrhage or ↓ erythropoiesis
- High : subacute hemorrhage or hemolysis
• Macrocytic : reticulocytes- N/low : maturation defect (DNA, MDS, alcohol)
- High : hemolysis
ANEMIADifferential diagnosis
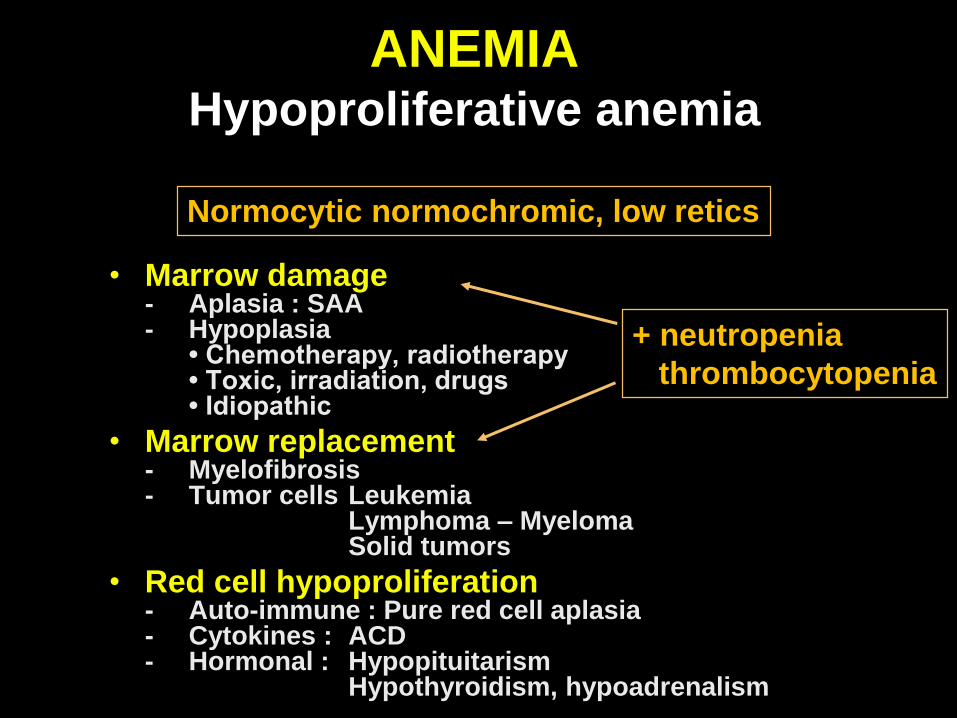
• Marrow damage - Aplasia : SAA - Hypoplasia
• Chemotherapy, radiotherapy • Toxic, irradiation, drugs • Idiopathic
• Marrow replacement- Myelofibrosis- Tumor cells Leukemia
Lymphoma – MyelomaSolid tumors
• Red cell hypoproliferation- Auto-immune : Pure red cell aplasia - Cytokines : ACD- Hormonal : Hypopituitarism
Hypothyroidism, hypoadrenalism
ANEMIAHypoproliferative anemia
Normocytic normochromic, low retics
+ neutropenia
thrombocytopenia

HYPOPLASTIC ANEMIAPRCA (1)
• Isolated RBC aplasia, normal WBC/platelets
• Etiology- Congenital : Diamond-Blackfan anemia
- Acquired :
* Transient erythroblastopenia of childhood
* Idiopathic auto-immune
* Secondary chronic Thymoma
CLL
Biermer, B6 deficiency
SLE, RA
Some solid tumors
Anti-rHuEpo Ab (SC Eprex® in CRF)
* Secondary transient Parvovirus B19, CMV, HIV
Dapsone, sulfasalazine, rifampicin
Thiamphenicol, chloramphenicol
HYPOPLASTIC ANEMIAPRCA (2)
• Biological features- Normocytic normochromic anemia
- Reticulocytes < 1%
- Normal WBC & platelets
- BM : normocellular without erythroblasts
• Management- Transfusion
- Treat underlying condition
- Thymoma : surgery
- Parvovirus : IV Ig
- Immunosuppression :
steroids, ciclosporin, cyclophosphamide, ATG, azathioprim …
• Prognosis→ 15% spontaneous CR, 65% respond to IS, 50% relapse
ERYTHROPOIETINInadequate endogenous Epo
• Chronic renal disease
• Chronic inflammatory disease
• HIV infection
• Cancer
• Premature infants
• Early pregnancy
• Allogeneic bone marrow transplantation
• Congestive heart failure
Normocytic normochromic, low retics
Treatment = rHuEpo
ANEMIA IN CANCER Epo deficit : serum Epo levels
• Normal - Solid tumors
- Leukemia
• Reduced - Multiple myeloma
- Lymphoma
• Highly variable - MDS

ACD
=
Anemia
of
inflammation
Associated
diseases

Anemia in cancer patientsPathogenesis
Anemia due to
other causes
Treatment-induced
anemia
Anemia of cancer
(AOC)
• Chemotherapy(CIA)
• Radiotherapy
• Bone marrow infiltration
• ACD :- Hemodilution- Decreased RBC survival- Decreased RBC production
Defective Epo productionInhibition of erythropoiesisIron sequestration
Increased RBC loss• Hemodilution (spleen, hyper-γ…)• Hemolysis (AIHA, µ-angiopathic…)• Hemophagocytosis• Hypersplenism• Bleeding (GI, gynecologic…)
Impaired RBC production• Nutrition. defic. (B12, folate…)• Iron deficiency• Renal dysfunction• Marrow impairment (MDS, BM
necrosis, PRCA…)FIDHypochromic microcytic anemia
↓ SeFe & TSat
↑ Ferritin
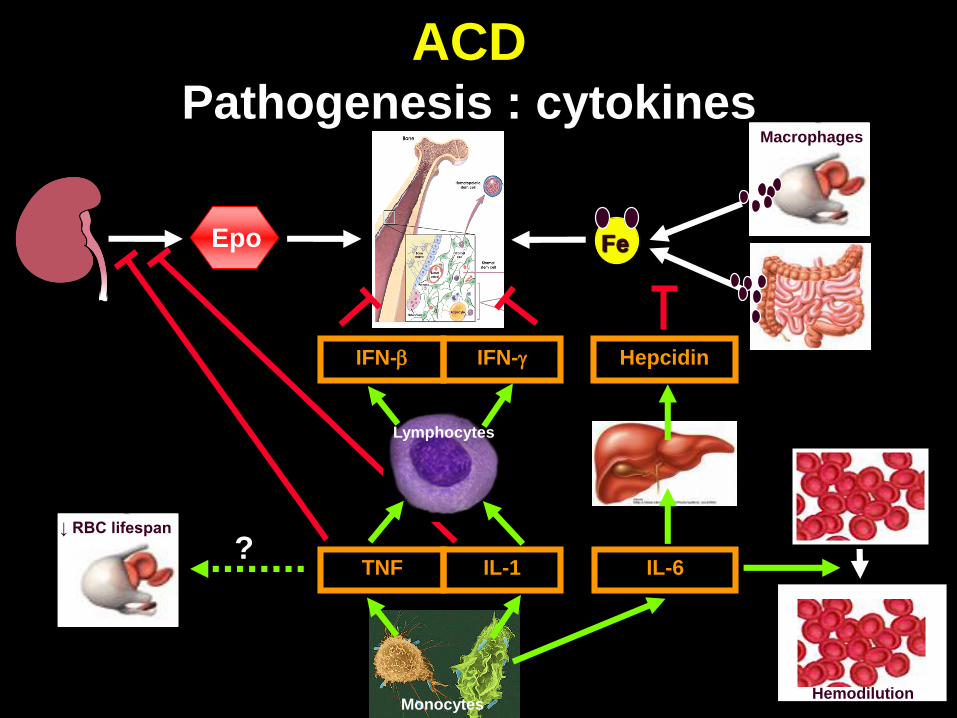
ACDPathogenesis : cytokines
Hepcidin
TNF IL-1 IL-6
Monocytes
Epo Fe
Macrophages
Hemodilution
?↓ RBC lifespan
IFN- IFN-
Lymphocytes

HEPCIDINMediator of iron blockade
IL-6 Hepcidin
Ferroportin
Macrophage
Transferrin
ANEMIA
Anemia of cancer
Treatment
CASES
Iron & Epo therapy
IRON OR EPO ?Case 1
• 25-yr-old female
• Hodgkin, stage IV, ABVD
• Hb 9.5 g/dL, normocytic
• Serum ferritin 856 µg/L
• Tsat 14%
IRON OR EPO ?Case 1
• 25-yr-old female
• Hodgkin, stage IV, ABVD
• Hb 9.5 g/dL, normocytic
• Serum ferritin 856 µg/L
• Tsat 14%1. EPO
2. Oral iron
3. IV iron
4. EPO + oral iron
5. EPO + IV iron
6. None

IRON OR EPO ?Case 2
• 65-yr-old female
• Active rhumatoid arthritis, CRP 184 mg/L
• Hb 11.5 g/dL, microcytic
• Serum ferritin 42 µg/L
• Tsat 17%
IRON OR EPO ?Case 2
• 65-yr-old female
• Active rhumatoid arthritis, CRP 184 mg/L
• Hb 11.5 g/dL, microcytic
• Serum ferritin 42 µg/L
• Tsat 17%1. EPO
2. Oral iron
3. IV iron
4. EPO + oral iron
5. EPO + IV iron
6. None
IRON OR EPO ?Case 3
• 15-yr-old female
• Asthenia, dyspnea when running
• Hb 9.5 g/dL, microcytic
• Serum ferritin 12 µg/L
• Tsat 8%
IRON OR EPO ?Case 3
• 15-yr-old female
• Asthenia, dyspnea when running
• Hb 9.5 g/dL, microcytic
• Serum ferritin 12 µg/L
• Tsat 8%1. EPO
2. Oral iron
3. IV iron
4. EPO + oral iron
5. EPO + IV iron
6. None
ACDTreatment
• Treat underlying disease
• Transfusions
• rHuEpo
• IV iron
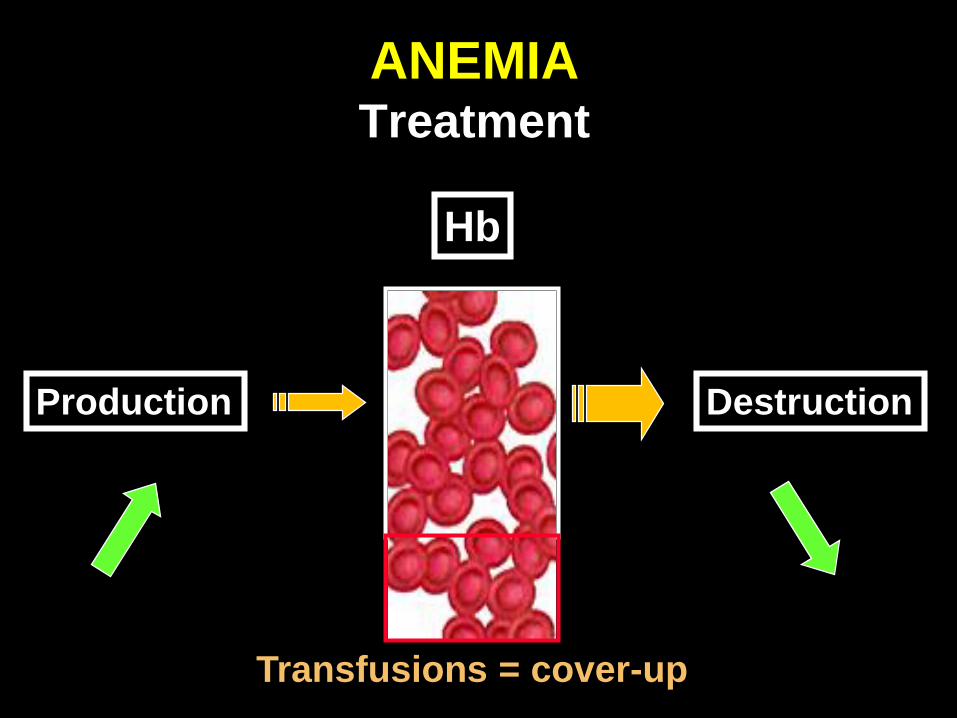
ANEMIATreatment
Production Destruction
Hb
Transfusions = cover-up

EPO THERAPY IN CANCER EPO vs transfusions : slow vs fast
Vaupel et al, The Oncologist 13(Suppl 3):21, 2008
Hb + 1 g/dL : 4 wks
Hb + 2 g/dL : 8 wks

EPO THERAPY IN CANCER 2/3 patients respond
0
100
80
60
40
20
Weeks
rHuEpo 30,000 IU/week
67%
8 10 12 14 16
27%
Placebo
4 6
p<0.0001
Österborg et al.
J Clin Oncol 2002; 20: 2486–2494
Patients with lymphoproliferative malignancies achieving
haemoglobin increase of ≥2.0 g/dL from baseline
K-M
% p
ati
en
ts (
95
% C
I)
0
10
20
30
40
50
60
70
80
Lymphoma Myeloma
64%
23%
p<0.001
56%
13%
p<0.001
Aranesp®
Placebo
K-M
% p
ati
en
ts (
95
% C
I)
0
10
20
30
40
50
60
70
80
Lymphoma Myeloma
64%
23%
p<0.001
56%
13%
p<0.001
Aranesp®
Placebo
Hedenus M et al.
Br J Haematol 2003;122:394–403
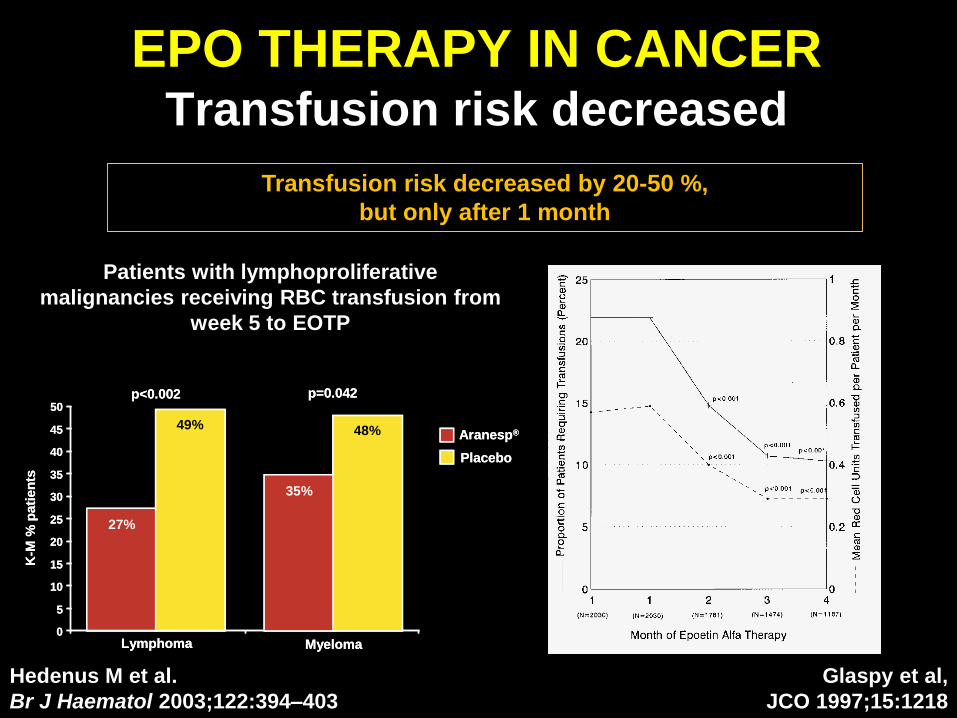
EPO THERAPY IN CANCER Transfusion risk decreased
Glaspy et al,
JCO 1997;15:1218
Hedenus M et al.
Br J Haematol 2003;122:394–403
K-M
% p
ati
en
ts
0
5
10
15
20
25
30
35
40
45
50
Lymphoma
27%
49%
Myeloma
p<0.002 p=0.042
35%
48% Aranesp®
Placebo
K-M
% p
ati
en
ts
0
5
10
15
20
25
30
35
40
45
50
Lymphoma
27%
49%
Myeloma
p<0.002 p=0.042
35%
48% Aranesp®
Placebo
Patients with lymphoproliferative
malignancies receiving RBC transfusion from
week 5 to EOTP
Transfusion risk decreased by 20-50 %,
but only after 1 month
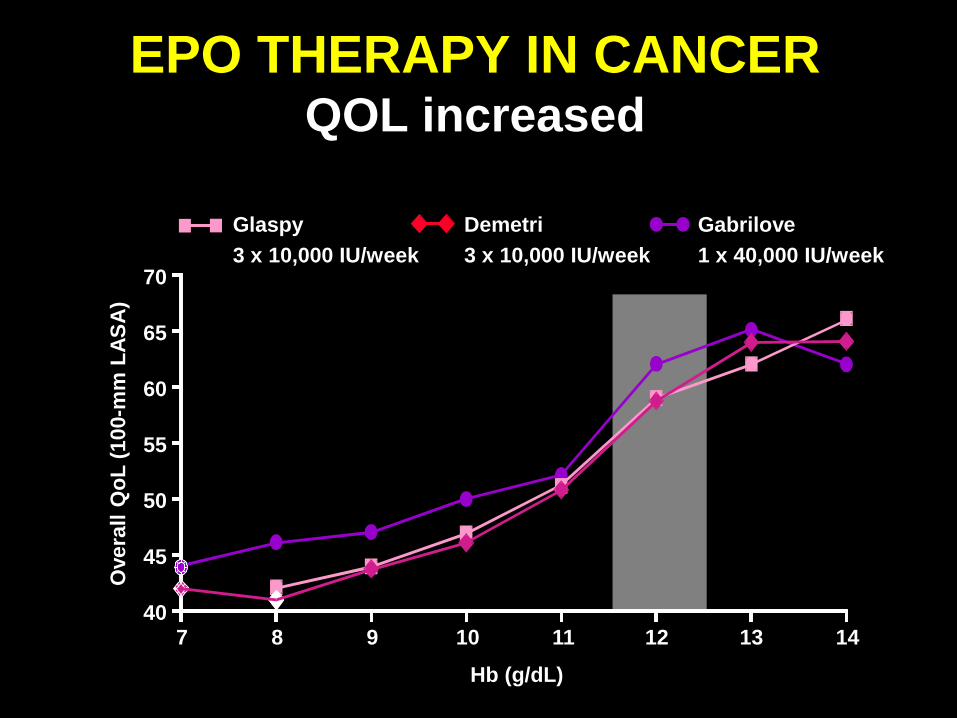
EPO THERAPY IN CANCER QOL increased
Overa
ll Q
oL
(10
0-m
m L
AS
A)
Hb (g/dL)
7 8 9 10 11 12 13 14
70
65
60
55
50
45
40
Gabrilove
1 x 40,000 IU/week
Glaspy
3 x 10,000 IU/week
Demetri
3 x 10,000 IU/week

EPO THERAPY IN CANCER Resistance
• Infections, inflammation, surgery
• Bleeding, hemolysis
• Intensive chemotherapy, limited residual
hematopoiesis
• Marrow fibrosis, major marrow involvement
• Anti-Epo antibodies
• Folate/B12 deficiency
• (Functional) iron deficiency

EPO THERAPY IN CANCERResistance : inflammation
0 100 200 300 4000
3000
6000
9000
12000
15000
6
8
10
12
14
16Acute pancreatitis
Transfusions
rHuEpo
Days post-transplant
sT
fR (
µg
/L) Hb
(g/d
L)
Hb
sTfR
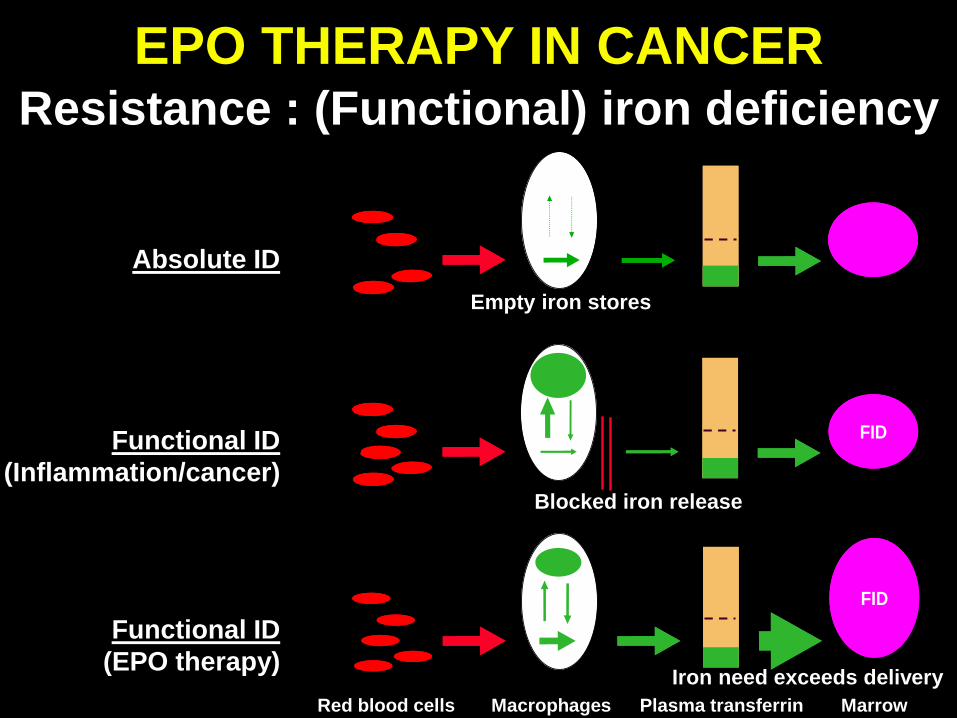
Absolute ID
Empty iron stores
FIDFIDFunctional ID
(Inflammation/cancer)Blocked iron release
FIDFID
Functional ID
(EPO therapy)Iron need exceeds delivery
MacrophagesRed blood cells Plasma transferrin Marrow
EPO THERAPY IN CANCERResistance : (Functional) iron deficiency

• Absolute iron deficiency
= no iron stores
• Functional iron deficiency
= iron stores present but ID in erythroid bone marrow
a) Iron sequestration in macrophages
- Inflammation (ACD, anemia of chronic disease)
b) Increased iron requirements
- EPO therapy
IRON DEFICIENCYEtiology

Functional ID
Iron
demand
Iron
supply
Adequate iron supply
Iron
consumption
Storage
iron
release
IV iron
EPO THERAPYFunctional iron deficiency
May occur even with
increased iron stores
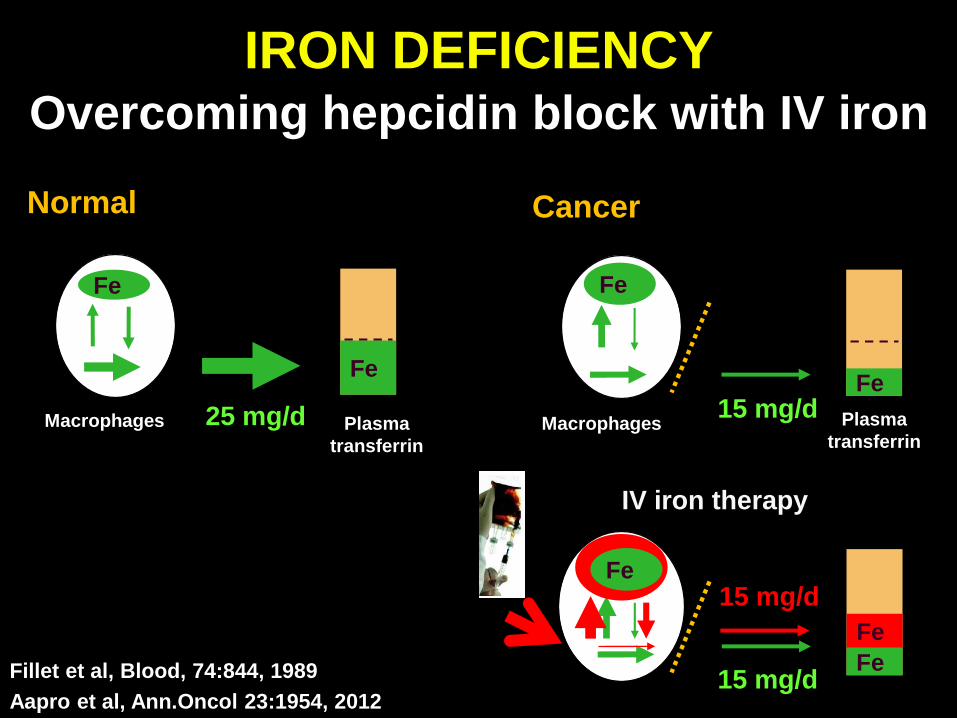
IRON DEFICIENCYOvercoming hepcidin block with IV iron
15 mg/dFe
15 mg/d
Fe
Fe
IV iron therapy
Fillet et al, Blood, 74:844, 1989
Aapro et al, Ann.Oncol 23:1954, 2012
Fe
Fe
25 mg/d
Normal
Macrophages Plasma
transferrin
Fe
Fe
15 mg/d
Cancer
Macrophages Plasma
transferrin

EPO THERAPY IN CANCER IV iron
Henry et al,
Oncologist 12:231-242, 2007
No iron Oral iron IV iron0
20
40
60
80
100
p=.0029p=.0099
All patients : rHuEPO
% r
es
po
ns
e
No iron Oral iron IV iron0
20
40
60
80
100
p=.0029p=.0099
All patients : rHuEPO
% r
es
po
ns
e
Bastit et al,
JCO 26:1611, 2008
Hedenus et al,
Leukemia 21:627, 2007
More
responses
Fewer
transfusions
Less
Epo use
All patients : DA
All patients : DA

EPO THERAPY IN CANCER IV iron gluconate
Henry et al, Oncologist 12:231-242, 2007
TSAT <20%(serum ferritin mostly over 100 ng/mL)
TSAT ≥20%(regardless of serum ferritin level)
100
80
60
40
20
0
Eva
lua
ble
po
pu
lati
on
(%
)
p=0.0091, oral vs ferric gluconate
p=0.0027, no iron vs ferric gluconate
p=0.535, oral vs no iron
Ferric
gluconate
Oral iron No iron
100
80
60
40
20
0
Eva
lua
ble
po
pu
lati
on
(%
)
Ferric
gluconate
Oral iron No iron
4852
68
27
37
81

Cazzola et al., Blood 1996, 87:4824
Hb sTfR Ferritin
ANEMIA IN JUVENILE ARTHRITISIV iron therapy

PlasmaMacrophages Marrow
Venofer 300 mg IV in 1 H
qow x 3 doses
Injectafer 1000 mg IV in 30 min
Faster response
Higher response rate
Fewer transfusions
Less EPO used
EPO THERAPY IN CANCERIV iron

PlasmaMacrophages Marrow
IV iron
EPO THERAPY IN CANCERExcessive IV iron
Hepatocytes& others
Acute reactions
Organ damage
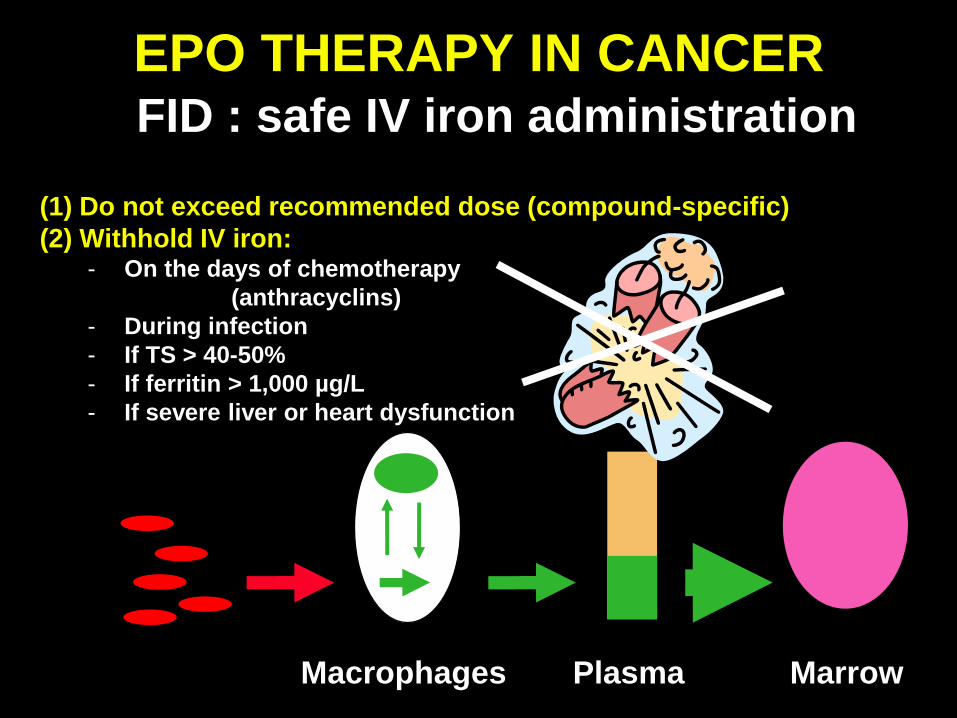
EPO THERAPY IN CANCERFID : safe IV iron administration
PlasmaMacrophages Marrow
(1) Do not exceed recommended dose (compound-specific)
(2) Withhold IV iron:- On the days of chemotherapy
(anthracyclins)
- During infection
- If TS > 40-50%
- If ferritin > 1,000 µg/L
- If severe liver or heart dysfunction
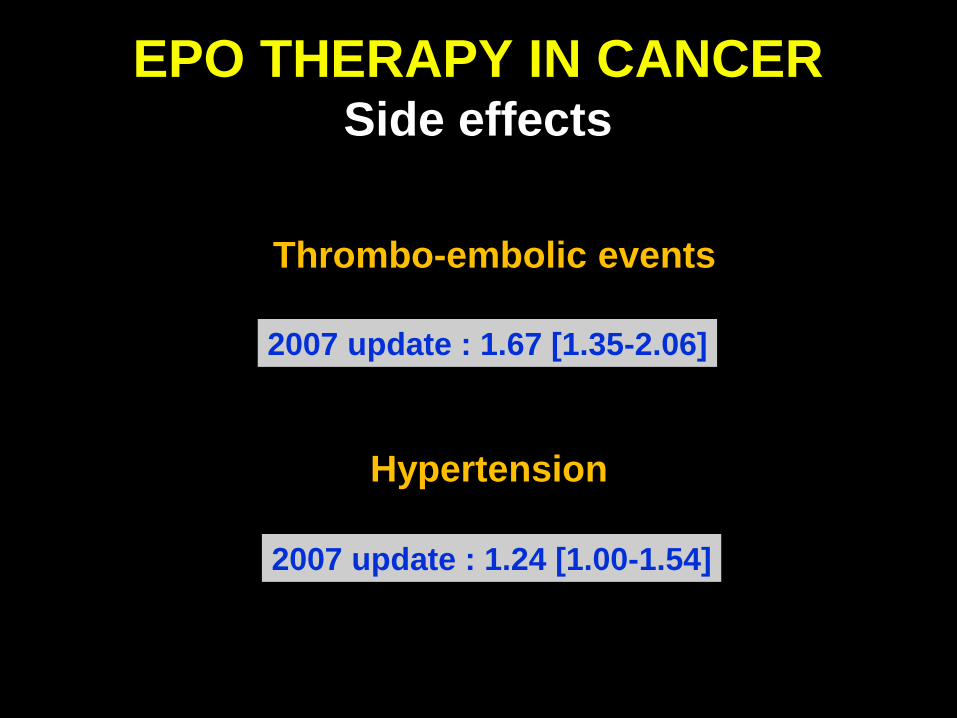
EPO THERAPY IN CANCER Side effects
2007 update : 1.67 [1.35-2.06]
2007 update : 1.24 [1.00-1.54]
Thrombo-embolic events
Hypertension

rHuEpo during radiotherapy for H&N Ca
EPO & SURVIVAL IN CANCERH&N cancer and radiotherapy
Tumor hypoxia
Henke et al, Lancet 362:1255, 2003
Loco-regional PFS
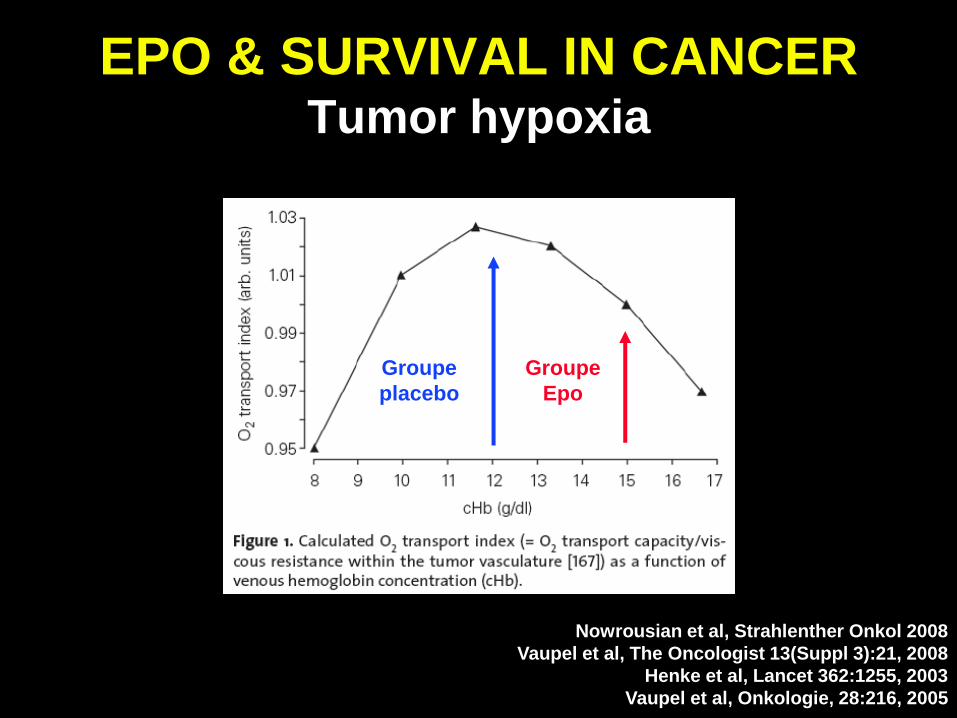
EPO & SURVIVAL IN CANCER Tumor hypoxia
Nowrousian et al, Strahlenther Onkol 2008
Vaupel et al, The Oncologist 13(Suppl 3):21, 2008
Henke et al, Lancet 362:1255, 2003
Vaupel et al, Onkologie, 28:216, 2005
Groupe
placebo
Groupe
Epo

COCHRANE REVIEWMortality
Group No pts RR p value
All patients on-study 13,933 1.17 (1.06-1.30) 0.003
long-term 1.06 (1.00-1.12) 0.046
Chemo on-study 10,441 1.10 (0.98-1.24) 0.12
long-term 1.04 (0.97-1.11) 0.26
Bohlius et al, Lancet 373: 1532–1542, 2009

EPO & SURVIVAL IN CANCERDLBCL
Delarue R et al. J Clin Oncol 2011;29 (suppl): Abstr 9048GELA LNH03-6B trial
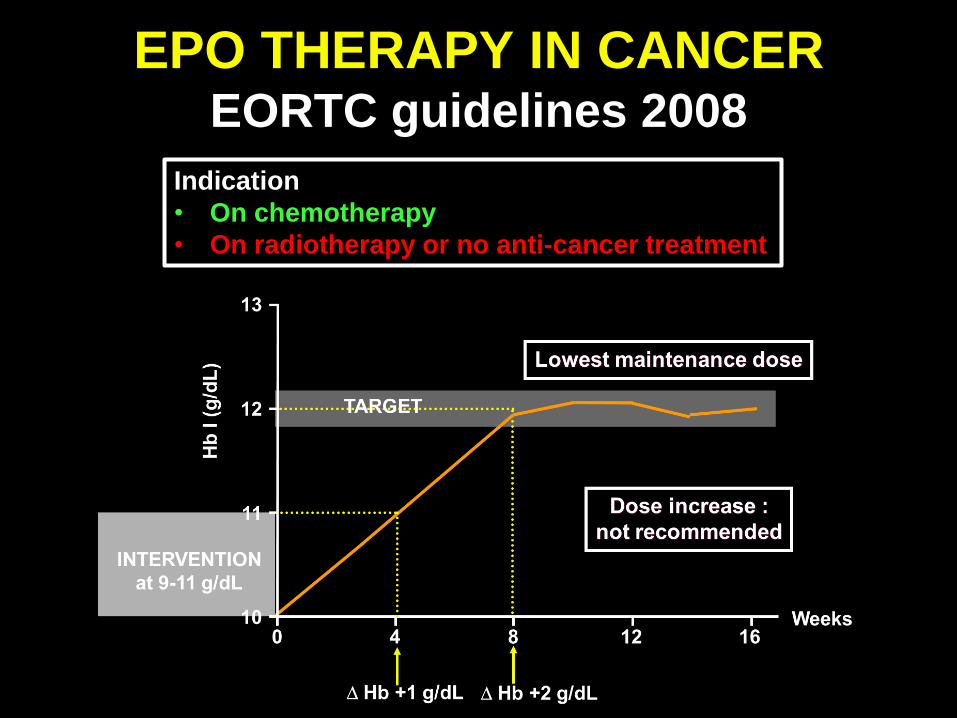
EPO THERAPY IN CANCEREORTC guidelines 2008
Indication
• On chemotherapy
• On radiotherapy or no anti-cancer treatment

EPO THERAPY IN CANCER EORTC guidelines 2008
• Recommended : treatment of cancer patients receiving
chemotherapy (chemo-radiotherapy ?)
• Not recommended :
– Anemia due to other causes (ID…)
– Prophylactic use (normal Hb)
– Radiotherapy alone
– No cancer treatment
((EORTC : careful assessment of need !))
Bokemeyer et al. Eur J Cancer 2007; 43: 258-271
Aapro et al. The Oncologist 2008; 13(Suppl.3): 33-36

EPO THERAPY IN CANCERRecommendations
• Dose : SC - rHuEPO 30-40,000 U/wk (500 U/kg/wk)
(Neorecormon®, Eprex®)- Darbepoetin 150 µg/1 wk (2.25 µg/kg/1 wk)
300 µg/2 wks * (4.5 µg/kg/2 wks) 500 µg/3 wks (6.75 µg/kg/3 wks)
(Aranesp®)
• In case of no response- do not increase dose- verify and treat causes of resistance (iron !)- stop EPO
• IV iron supplements (Venofer / Injectafer)in case of functional iron deficiency
* Not on SmPC

CASES
Iron & Epo therapy

IRON OR EPO ?Case 1
• 25-yr-old female
• Hodgkin, stage IV, ABVD
• Hb 9.5 g/dL, normocytic
• Serum ferritin 856 µg/L
• Tsat 14%1. EPO
2. Oral iron
3. IV iron
4. EPO + oral iron
5. EPO + IV iron
6. None

IRON OR EPO ?Case 2
• 65-yr-old female
• Active rhumatoid arthritis, CRP 184 mg/L
• Hb 11.5 g/dL, microcytic
• Serum ferritin 42 µg/L
• Tsat 17%1. EPO
2. Oral iron
3. IV iron
4. EPO + oral iron
5. EPO + IV iron
6. None
IRON OR EPO ?Case 3
• 15-yr-old female
• Asthenia, dyspnea when running
• Hb 8.5 g/dL, microcytic
• Serum ferritin 12 µg/L
• Tsat 8%1. EPO
2. Oral iron
3. IV iron
4. EPO + oral iron
5. EPO + IV iron
6. None