the evaluation of emotional facial expressions in...
TRANSCRIPT

1
Rapport technique : 2010/01/S.GIL
The evaluation of emotional facial expressions in early
postpartum depression mood: A difference between adult
and baby faces?
Sandrine Gil 1, Frédérique Teissèdre 2, Patrick Chambres 2, Sylvie Droit-Volet2
1 Centre de Recherches sur la Cognition et l’Apprentissage – CeRCA, CNRS UMR 6234, Poitiers, France
2 Laboratoire de Psychologie Sociale et Cognitive (LAPSCO), CNRS, UMR 6024, Clermont-Ferrand, France
A paraître dans / To appear in : Gil, S., et al., The evaluation of emotional facial expressions in early postpartum depression mood: A difference between adult and baby faces. Psychiatry Research.
Address for correspondence to the first author at: Sandrine Gil, Université de Poitiers –CNRS Centre de Recherches sur la Cognition et l’Apprentissage (CeRCA) – CNRS UMR 6234 MSHS - Bâtiment A5 - 5 rue Théodore Lefebvre - 86000 Poitiers, France E-mail : [email protected] Tel : 33 (0)5.49.45.44.16 Fax : 33 (0)5.49.45.46.16

KEY-WORDS: Early postpartum depressive mood ; Emotion ; Face ; Anxiety ; Affective disorders.
ABSTRACT
Research suggests that depressive individuals exhibit disturbances in the evaluation of emotional facial expressions.
Owing to the specific character of postnatal depressive mood, the purpose of the present study was to examine
whether postpartum depressive mood intensity in the mothers would involve the same disturbances as depression or a
specific distortion in the emotional evaluation of baby faces as compared to adult faces. Three days after birth, the
participants (N = 79) completed the Edinburgh Postnatal Depression Scale, the State-Trait Anxiety Inventory and the
Toronto Alexithymia Scale. They also evaluated the facial expressions of adults and babies displaying anger, happiness,
sadness and neutrality in terms of the intensity offive emotions: Anger, disgust, sadness, happiness and neutrality. Our
findings suggest thatjudgements of emotional facial expressions depend to a great extent on anxiety, which specifically
increased negative perception of babies' emotions. Moreover, the only difference between mothers with and without
postpartum depressive mood lays in their assessment of the babies' faces, neutral baby faces being judged to be less
neutral, thus demonstrating the specificity of postpartum affective disorders.
INTRODUCTION
The quality of early mother–infant interactions is a determining factor for children's abilities to communicate, for their
emotional development and well-being (Murray, 1992; Weinberg and Tronick, 1994; Papousek and Papousek, 1997;
Tronick and Weinberg, 1997; Field, 2002; Feldman, 2007). Evidence suggests that “linkages detected between maternal
emotional disposition and infant face processing reflect, at least in part, the role of experience in shaping face
processing” (de Haan et al., 2004, p. 1214). However, after childbirth, some mothers suffer from a specific form of
depressive mood that can modify these early relationships.
There are three forms of affective disorders which differ in both their severity and timing: (1) postpartum blues (also
known as baby or maternity blues), (2) postpartum depression, and (3) puerperal psychosis which includes
heterogeneous entities that incorporate all the major psychiatric disorders which occur during the period following
childbirth. The former is the most frequent affective disorder and is experienced by 25% to 85% of mothers.
Postpartum depression affects between 10 and 20% of mothers, while puerperal psychosis affects less than 2 per 1000
(Beck, 2002). The symptoms of postpartum blues consist of common emotional disturbances such as crying, anxiety and a
depressed and unstable mood. These symptoms appear in the first week after childbirth and are limited intime. When
they persist beyond two weeks, or if they are very intense, the diagnosis is one of postpartum depression.
Moreover, the link between early postpartum depressive mood and postpartum depression has been extensively
reported on the basis of the Edinburgh Postnatal Depression Scale (EPDS), which makes it possible to evaluate the
depressive component of the former and to predict the clinical diagnosis of the latter (e.g., Teissèdre and Chabrol,
2004; Gonidakis et al., 2008). Since the way a mother processes the emotional facial information expressed by her
child may help her respond correctly to her infant's physical and social needs, the purpose of our original work was
to examine how mothers suffering from depression symptomatology in the first days after childbirth evaluate
emotional facial expressions. To date, no research has attempted to examine this topic. Indeed, the few experimental
studies on emotion and postpartum depressive mood have focused on disturbances in the emotional
expressiveness of the mothers and/or their children (e.g., Cohn et al., 1990; Lundy et al., 1996; Field, 1997; Lundy et al.,
1997; Striano et al., 2002; Nadel et al., 2005).
As far as depression in general is concerned, two types of disruption to the perception of emotional facial
expressions have been reported on many occasions. Firstly, a number of studies have shown that the recognition of
emotional expressions is less accurate in depressive individuals than in controls (Gur et al., 1992; Rubinow and Post,
1992; George et al., 1998; Suslow et al., 2001; Leppänen et al., 2004; Mendlewicz et al., 2005). Secondly, other studies
have reported a negative bias in emotional evaluations, namely in that depressed individuals attribute negative

3
emotions to neutral or positive facial expressions, or judge negative facial expressions to be more intense (Gur et al.,
1992; Hale, 1998; Gollan et al., 2008). This keeps with the mood congruence effect (Niedenthal et al., 2000): While
someone in love sees life through rose-tinted spectacles, a sad or depressed person sees it through grey spectacles.
However, compared to depression, postpartum depressive symptoms have to be considered as being related to a
specific context, because they appear in reaction to childbirth. We may thus suppose that the depressionbased
disturbances in the evaluation of the emotions expressed by faces might be specific to baby faces or more important
for baby than for adult faces. Furthermore, there is some evidence that interindividual variations in the external
context (e.g. having low mother esteem) might exacerbate the depressive symptoms and their effects (Kendell et al.,
1984; O'Hara et al., 1991; Tamaki et al., 1997; Robertson et al., 2004; Séjourné et al., 2008). Certain external variables
might therefore modulate the effect of depressive mood on the evaluation of emotional faces. Consequently, in our
study, we have also taken into account many external variables of sociobiographical, psychosocial and obstetrical
nature.
Furthermore, with regard to postnatal symptoms, an increasing number of studies have provided empirical evidence
that childbirth is associated not only with depression but also with other affective styles, especially anxiety disorders
(Heron et al., 2004; Gonidakis et al., 2008; Mota et al., 2008; Skouteris et al., 2009) and alexithymia (Le et al., 2007;
Gonidakis et al., 2008), the later often being found to be related to depression (Taylor et al., 2000; Kojima et al., 2003).
In the present study, we thus investigated whether, as has been shown for depressive mood, early postpartum
depressive mood is associated with disturbances in the evaluation of emotional facial expressions, and whether these
disturbances are observed at a higher rate in response to baby faces. In this framework, we examined also whether
affective styles (anxiety and alexithymia), as external variables associated with postnatal depressive mood intensity
explain, at least partly, the distortions in emotional expression evaluation.
METHOD
STUDY DESIGN
The study was conducted in two hospitals near Clermont-Ferrand. Seventy-nine female volunteers were seen
individually in their rooms on the third day after delivery. The inclusion criteria consisted of an adequate knowledge of
French language and the delivery of a healthy baby.
CLINICAL SYMPTOMS QUESTIONNAIRES
The French version (Guedeney and Fermanian, 1998) of the Edinburgh Postnatal Depression Scale (EPDS) (Cox et al.,
1987) was used to assess postpartum depression symptomatology on the third day after childbirth. This questionnaire
consists of 10-item self-report statements which investigate the mother's mood, the level of anxiety, the feeling of
guilt, the feeling of lacking ability, sleep problems and the desire to end one's own life. The score range is between 0
and 30. This questionnaire is acknowledged as making it possible to screen for postnatal depressive mood at an early
stage and identify mothers at risk (Beck, 2001; Chabrol and Teissèdre, 2004).
The intensity and the frequency of anxiety were measured with the State-Trait Anxiety Inventory (STAI) (Spielberger et
al., 1983; French version by Schweitzer and Paulhan, 1990). This commonly employed self-report instrument, which
consists of 4-point Likert scales, allowed us to assess state anxiety and trait anxiety independently on two different 20-
item subscales. The anxiety score on each subscale provides information about the general probability of experiencing
anxiety symptoms and ranges from 20to 80.
The French version (Loas et al., 1996) of the 20-item Toronto Alexithymia Scale (TAS-20) (Bagby et al., 1994) was also
administered. In this extensively validated scale, subjects were asked to indicate the degree to which they agree with
each of the 20 statements on a 5-point Likert scale. The scores range from 20 to 100, with higher scores indicating a
higher level of alexithymia.

THE EMOTIONAL FACIAL EXPRESSION TASK
Because there are no pictures of the facial expressions of adults and babies taken under the same conditions, we had
developed our own stimuli1. Adults and babies exhibiting facial expressions of basic emotions that are widely
recognized in adults—anger, happiness, sadness and neutrality—were therefore photographed from the shoulders
up. To standardize the photographs, all wore a grey pullover, and were photographed against a light-blue
background. We consequently selected 452 photographs that were judged to represent recognizable facial
expressions. Each photograph was then evaluated by 25 undergraduate students who, in each case, had to judge the
intensity of 8 emotions (anger, happiness, sadness, neutrality, disgust, fear, surprise, and shame) on a 7-point scale
ranging from 0 “The face in no way expresses this emotion” to 6 'The face fully expresses this emotion”. This larger
panel of emotions was used in order to exclude ambiguous facial expressions. The order of presentation of both the
photographs and the emotion scale was randomised across the participants. These evaluations allowed us to identify
the best photographs2 that expressed a specific emotion3 at a high level of intensity (>3.5). The final set of stimuli
consisted of 48 colour photographs displaying 4 different kinds of emotional facial expressions—anger, happiness,
sadness, and neutrality (see Fig. 1 for an example). There were 12 photographs for each emotion tested. Six
photographs represented an adult's emotional facial expression (3 males and 3 females) and six photographs
represented a baby's emotional facial expression (two babies). Each target expressed the 4 emotion expressions once.
PROCEDURE
All the women, who volunteered to take part in the study, gave their informed consent and were asked to complete
a questionnaire relating to their demographic, obstetric and psychosocial details4 (see Table 1).
The women then completed the emotional facial expression task. They were told that they would see faces of
different individuals, and that they had to indicate the intensity of a given emotion ona 7-point scale from 0 'The face
in no way expresses this emotion” to 6 'The face fully expresses this emotion”. For each photograph, they had to judge
the intensity of 5 emotions: the four actually expressed emotion (anger, happiness, sadness and neutrality) and, in
order to avoid overloading the experiment, only one additional emotion, namely disgust, because literature
highlights that this emotion plays an critical role in some affective styles, particularly anxiety (Marzillier and Davey,
2005). The order of the emotions was counterbalanced between each photograph. The 48 emotional facial
expressions were therefore presented one by one centered on the computer screen. After judging a photograph, the
participant had to press a key on the computer keyboard to see the next photograph. The order of the photographs
1 To produce the facial expressions of anger, happiness and sadness, we asked the adults to think of an event which induces a specific emotion, (e.g., for happiness, thinking of a party with friends). In addition, we presented them with examples of pilot-tested emotional facial expressions from Beaupré and Hess's (2005) study. In the case of the babies, the photos were taken as a function of the baby's spontaneous mood. In others words, the experimenter waited for the baby to laugh (e.g., when he was happy to play with his mother), or cry (e.g., when he was hungry). 2 The photographs were tested by an additional sample of participants and selected and assessed following 3 phases: (1) a preliminary selection of photographs considered by the participants as representing a given emotion at a high level of intensity (i.e., mean>3.5 on a 7-point scale) was run; (2) A series of analyses of variance (ANOVAs) and T-tests were performed to examine whether the selected photographs differed as a function of the category of expressed emotion, and were similar in each emotional category; (3) A principal component analyses for each emotion and for all selected photographs was also run in order to confirm that the sample of photographs expressing a particular emotion was homogeneous. 3 Regarding the evaluations of babies' facial expressions, the data revealed that baby photographs evaluated as strongly expressing anger were also systematically evaluated as expressing sadness. Consequently, in our experiment, the 'angry baby faces” category actually corresponded to an 'angry/sad baby faces” category. This blending of anger and sadness is usually observed in emotional baby faces (e.g., Matias and Cohen, 1993; Sullivan and Lewis, 2003). The other categories (i.e., happy, sad, neutral) corresponded to a specific emotion. 4 Since 11% of women reported to have already used antidepressants, we carried out an independent-sample T-test in order to control that these women did not obtain an EPDS score significantly higher than the other women. The results showed no difference between women who have already used antidepressants (M= 9.11; S.D.= 4.45) and the others (M= 8.76; S.D.= 5.57, t(73) = —.18, P>0.10). Because the question was not precise, we can supposed that these women took antidepressants at a more or less remote point intime, with this former antidepressant intake having no impact on the results obtained in our study.

5
was counterbalanced for each participant. Finally, the participants completed the three self -report scales for
postnatal depression symptoms, anxiety, and alexithymia. The entire session lasted about 1 h.
Figure 1. Examples of adults' and babies' facial expression for each emotion: happiness, neutrality, sadness and anger.
Table 1. Sample characteristics.
DATA ANALYSIS
Analyses of data were performed using SPSS version 16. Analyses included all participants. Concerning the stimuli,
because previous statistical analyses showed no effect of the sex of adult faces (P<0.05), we thus considered adult faces
independently of sex.
First (point 3.1), we examined the relationship between the clinical measures (EPDS, STAI state, STAI trait) and the
evaluations of facial expressions. In this vain, we used Spearman correlations and, then, when emotional evaluations
were correlated with more than one clinical measure, we conducted Stepwise linear regression analyses in order to
determine which was the predictor. As multiple regression analysis can inflate the familywise error rate, the regression
analyses were interpreted after applying the Bonferroni correction (α= 0.05/2).
Second (point 3.2), we investigated whether emotional distortions observed due to clinical dimensions should be also
related to external variables (demographic , obstetric and psychosocial variables). Consequently, we used Spearman
correlations, and then Stepwise linear regression analyses (conducted with a Bonferroni correction, α = 0.05/6) for the
emotional evaluations which were significantly correlated with a clinical score, by entering both clinical variables and
external variables as predictors.
RESULTS
CLINICAL VARIABLES AND EMOTIONAL EVALUATIONS
In line with the values reported in the literature, 30.38% of the women in our sample corresponded to the criteria
defined for the Edinburgh Postnatal Depression Scale. As stated in the Introduction, our aim was to investigate whether
there was any relationship between postpartum depressive mood intensity in the mothers and its related affective
styles (i.e., anxiety and alexithymia) on the one hand, and the evaluations of facial expressions, on the other hand. To
this end, we began by calculating Spearman correlations between depressive mood intensity, anxiety and alexithymia
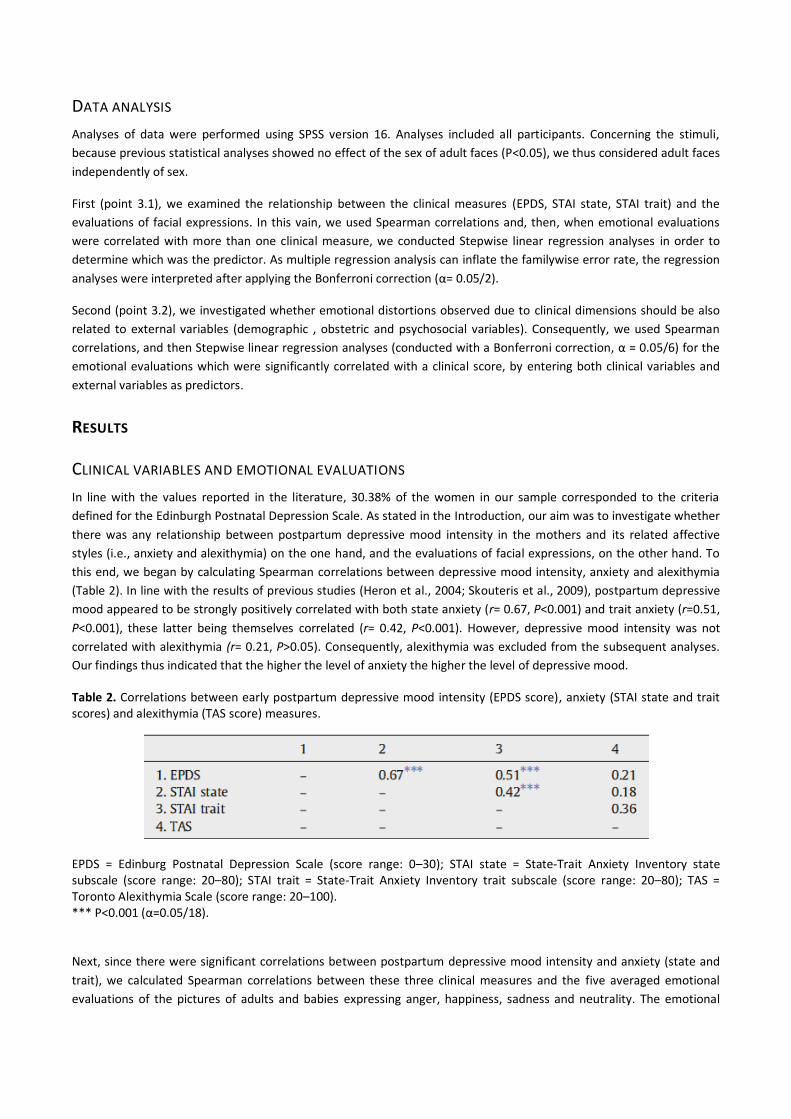
(Table 2). In line with the results of previous studies (Heron et al., 2004; Skouteris et al., 2009), postpartum depressive
mood appeared to be strongly positively correlated with both state anxiety (r= 0.67, P<0.001) and trait anxiety (r=0.51,
P<0.001), these latter being themselves correlated (r= 0.42, P<0.001). However, depressive mood intensity was not
correlated with alexithymia (r= 0.21, P>0.05). Consequently, alexithymia was excluded from the subsequent analyses.
Our findings thus indicated that the higher the level of anxiety the higher the level of depressive mood.
Table 2. Correlations between early postpartum depressive mood intensity (EPDS score), anxiety (STAI state and trait scores) and alexithymia (TAS score) measures.
EPDS = Edinburg Postnatal Depression Scale (score range: 0–30); STAI state = State-Trait Anxiety Inventory state subscale (score range: 20–80); STAI trait = State-Trait Anxiety Inventory trait subscale (score range: 20–80); TAS = Toronto Alexithymia Scale (score range: 20–100). *** P<0.001 (α=0.05/18). Next, since there were significant correlations between postpartum depressive mood intensity and anxiety (state and
trait), we calculated Spearman correlations between these three clinical measures and the five averaged emotional
evaluations of the pictures of adults and babies expressing anger, happiness, sadness and neutrality. The emotional
7
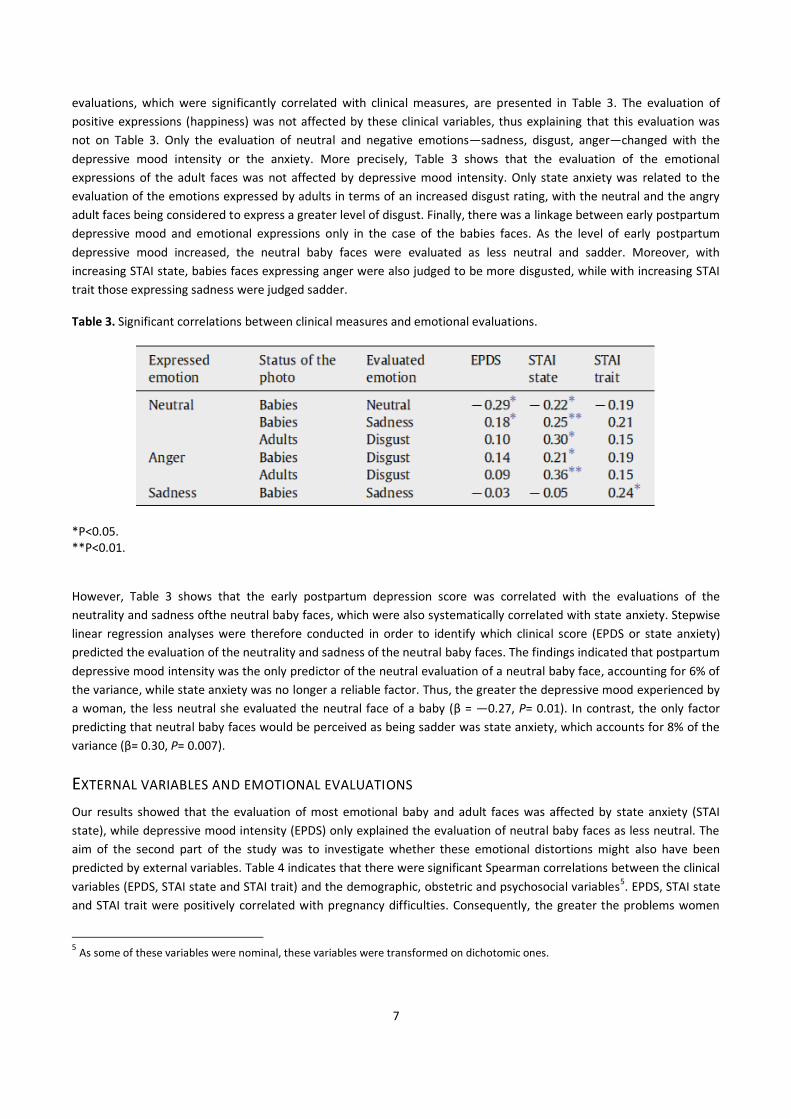
evaluations, which were significantly correlated with clinical measures, are presented in Table 3. The evaluation of
positive expressions (happiness) was not affected by these clinical variables, thus explaining that this evaluation was
not on Table 3. Only the evaluation of neutral and negative emotions—sadness, disgust, anger—changed with the
depressive mood intensity or the anxiety. More precisely, Table 3 shows that the evaluation of the emotional
expressions of the adult faces was not affected by depressive mood intensity. Only state anxiety was related to the
evaluation of the emotions expressed by adults in terms of an increased disgust rating, with the neutral and the angry
adult faces being considered to express a greater level of disgust. Finally, there was a linkage between early postpartum
depressive mood and emotional expressions only in the case of the babies faces. As the level of early postpartum
depressive mood increased, the neutral baby faces were evaluated as less neutral and sadder. Moreover, with
increasing STAI state, babies faces expressing anger were also judged to be more disgusted, while with increasing STAI
trait those expressing sadness were judged sadder.
Table 3. Significant correlations between clinical measures and emotional evaluations.
*P<0.05. **P<0.01. However, Table 3 shows that the early postpartum depression score was correlated with the evaluations of the
neutrality and sadness ofthe neutral baby faces, which were also systematically correlated with state anxiety. Stepwise
linear regression analyses were therefore conducted in order to identify which clinical score (EPDS or state anxiety)
predicted the evaluation of the neutrality and sadness of the neutral baby faces. The findings indicated that postpartum
depressive mood intensity was the only predictor of the neutral evaluation of a neutral baby face, accounting for 6% of
the variance, while state anxiety was no longer a reliable factor. Thus, the greater the depressive mood experienced by
a woman, the less neutral she evaluated the neutral face of a baby (β = —0.27, P= 0.01). In contrast, the only factor
predicting that neutral baby faces would be perceived as being sadder was state anxiety, which accounts for 8% of the
variance (β= 0.30, P= 0.007).
EXTERNAL VARIABLES AND EMOTIONAL EVALUATIONS
Our results showed that the evaluation of most emotional baby and adult faces was affected by state anxiety (STAI
state), while depressive mood intensity (EPDS) only explained the evaluation of neutral baby faces as less neutral. The
aim of the second part of the study was to investigate whether these emotional distortions might also have been
predicted by external variables. Table 4 indicates that there were significant Spearman correlations between the clinical
variables (EPDS, STAI state and STAI trait) and the demographic, obstetric and psychosocial variables5. EPDS, STAI state
and STAI trait were positively correlated with pregnancy difficulties. Consequently, the greater the problems women
5 As some of these variables were nominal, these variables were transformed on dichotomic ones.

experience during pregnancy, the higher the level of depressive mood and anxiety symptoms that they exhibit. This
finding is consistent with published studies (O Hara and Swain, 1996; Verdoux et al., 2002). However, the anxiety state
intensity was significantly reduced in women who have already had children. In addition, anxiety trait was negatively
related to pregnancy satisfaction, and depressive mood intensity with mother s confidence.
Table 4. Correlations between clinical variables and external variables.
***P<0.001. **P<0.003 (α= 0.05/18).
To test the degree to which the external variables were involved in the clinical variable-related emotional distortions,
we conducted stepwise linear regression analyses for the emotional evaluations, which were significantly correlated
with a clinical score (see Section 3.1 and Table 3), by entering both the clinical variables (EPDS, STAI state and trait) and
the external variables as predictor variables. Those external variables that were not significantly correlated with the
clinical scores were not considered in these analyses. The analyses revealed that none ofthe external variables was a
reliable predictor of emotion distortion in the evaluation of emotional expressions (all P>0.05).
DISCUSSION
Studies of emotions have shown that depressive individuals attribute negative emotions to neutral and positive faces,
and judge negative facial expressions to be more negative (Gur et al., 1992; Hale, 1998; Gollan et al., 2008). Our results
suggest that depressive mothers mood intensity has not the same effect on the perception of emotional expressions.
Indeed, postpartum depressive mood did not change the perception of facial expressions, all mothers (i.e., both those
exhibiting and those who did not exhibit these symptoms) having similar perception of the positive and negative
expressions. In contrast, and as expected, our main result demonstrated that the intensity of depressive mood in the
mothers has a specific impact on baby faces perception (i.e., the neutral baby faces were judged to be less neutral and
sadder). This specific emotional distortion with regard to baby faces may be related to the role of women in the
upbringing of children. Although widely speculative at this point, it seems possible that distress feelings of women
suffering from mood disorders may involve negative perception of neutrality (i.e., mood congruence effect), but that
this distortion may be primarily directed towards infants because women s crucial responsibility towards their children
is salient. Whatever the case, this early postpartum depression mood-related distortion in the perception of neutral
baby faces might represent an indicator of a potential risk of developing disturbances within the mother–children
interaction. It would be interesting to investigate if this emotional distortion is maintained only in the few number of
mothers who develop postpartum depression or if it is also maintained in the other mothers, those who do not develop
depression but remain anxious.
Indeed, our results revealed that, at an early stage of the postpartum, the depressive mood intensity was strongly
correlated with state anxiety, and that it was this anxiety in the mothers that produced larger distortion in the
perception of other people s emotion, especially the perception of emotion in babies. This finding is entirely consistent
with the growing body of evidence indicating that state anxiety is more or less related to depressive symptoms through
both pregnancy and the initial period after childbirth (Heron et al., 2004; Gonidakis et al., 2008; Mota et al., 2008;

9
Skouteris et al., 2009). For example, studies have shown that anxiety level may predict the risk of developing major
postpartum depression 6 weeks after childbirth (Stuart et al., 1998; Teissèdre and Chabrol, 2003). Moreover, Brown
(1993) has highlighted that 84% of mothers suffering from postpartum depression have experienced a recent episode
of intense stress. Consistent with this idea, our results showed that postpartum depressive mood and anxiety were
positively correlated with pregnancy difficulties. In our study, the pregnancy difficulties were the only reliable external
variable systematically associated with our clinical measures. Experiencing a difficult pregnancy could therefore be an
important source involved in the emergence of postpartum depression. However, our study was not concerned with
postpartum depression, but depressive mood just after childbirth day. It nevertheless revealed that, at this early stage,
state anxiety was already associated to distortions in the judgment of emotional expressions. With adult faces as
targets, when state anxiety increased, mothers perceived more disgust in the adult faces expressing anger or neutrality.
However, more specifically, with baby faces as targets, mothers not only perceived more disgust in the babies when
they expressed anger, but also more sadness for neutral baby faces. Mothers with anxious personalities (trait anxiety)
also perceived more sadness in sad baby faces. Mothers' anxiety after childbirth therefore increased the negative
perception of babies' emotions. It would be now interesting to investigate the evolution of this negative emotional
perception at different points in time during the first year after childbirth in order to better understand its eventual
impact on the mother–infant relationship. It might be possible that these anxious mothers would experience more
difficulties to adapt to their infants' need and to communicate with him. In this case, an early and systematic diagnostic
of anxiety in the mothers would be important for an early care.
Moreover, it is interesting to note that, in the present study, anxiety was related to the evaluation of disgust, with the
higher the level anxiety the more disgust perceived, be it with an adult or a baby as target. This is consistent with
numerous studies indicating the relationship between the emotion of disgust and anxious psychopathologies (e.g.,
phobias or eating disorders) (Davey et al., 1998; Phillips et al., 1998; Woody and Tolin, 2002). Recently, Schofield et al.
(2007) showed that anxiety may induce interaction difficulties (i.e., a high interaction cost as evaluated by the
individuals themselves, in the presence of a facial expression of disgust). More interestingly, recent findings revealed
that inducing anxiety in participants led to an increase in self-reported disgust (Marzillier and Davey, 2005), or,
conversely, inducing disgust led to an increase in self-reported anxiety (Davey et al., 2008). The question is why anxious
individuals perceive more disgust in other people's faces. It is likely that anxious mothers attribute their own feeling of
disgust to others. An alternative explanation is that perceiving disgust in another person is a means of protecting one's
child against that person. Within an evolutionist perspective, disgust is conceived as a powerful adaptive emotion
allowing us to reduce the risk of contact with a contaminating object (Lazarus, 1991; Rozin and Fallon, 1987). Following
the observation of selective attention to threats in anxious states (Öhman et al., 2001; Surcinelli et al., 2006; Rossignol
et al., 2007), it is conceivable that a mother's anxiety after childbirth could produce emotional distortions which allow
her to protect her children against a potential danger: all other people could be a potential source of contamination.
To summarize, although further research testing mothers at different times after childbirth and with different level of
depression needs to be performed to examine the evolution of emotional evaluation perforrmance, the observed
pattern of results raises the question of the need to screen mothers who have recently given birth for both depression
and anxiety symptomatology.
ACKNOWLEDGEMENTS
The authors would like to thank Pierre -Jean Marescaux for advising on the statistical analyses in the revised version of
the manuscript, Anaïs Beaudoux and Noémie Christol for their assistance during data collection, and Serban C. Musca for English
proofreading the revised version of the manuscript. We extend our thanks to the women who participated to this
research. This research was supported by the French National Research Agency (ANR Blan06-2- 145908 FaceExpress).

RÉFÉRENCES
Bagby, R.M., Parker, J.D.A., Taylor, G.J., 1994. The Twenty-Item Toronto Alexithymia Scale. I. Item selection and cross-validation of the factor structure. Journal of Psychosomatic Research 38, 23–32.
Beaupré, M.G., Hess, U., 2005. Cross-cultural emotion recognition among Canadian ethnic groups. Journal of Cross-Cultural Psychology 26, 355–370.
Beck, C.T., 2001. Predictors of postpartum depression: an update. Nursing Research 50, 275–285. Beck, C.T., 2002. Postpartum depression: a metasynthesis. Qualitative Health Research 12, 453–472. Brown, G.W., 1993. The role of life events in the aetology of depressive and anxiety disorders. In: Stanford, S.C., Salmon, P. (Eds.),
Stress: From Synapse to Syndrome. Academic Press, London, pp. 23–50. Chabrol, H., Teissèdre, F., 2004. Relation between Edinburgh Postnatal Depression Scale scores at 2–3 days and 4–6 weeks
postpartum. Journal of Reproductive and Infant Psychology 22, 33–39. Cohn, J.F., Campbell, S.B., Matias, R., Hopkins, J., 1990. Face-to-face interactions of postpartum depressed and nondepressed
mother–infant pairs at 2 months. Developmental Psychology 26, 15–23. Cox, J.L., Holden, J.M., Sagovsky, R., 1987. Detection of postnatal depression: development of the 10-item Edinburgh Postnatal
Depression Scale. The British Journal of Psychiatry 150, 782–786. Davey, G.C.L., Buckland, G., Tantow, B., Dallos, R., 1998. The effect of disgust on anxiety ratings to fear-relevant, disgust-relevant and
fear-irrelevant stimuli. Journal of Anxiety Disorders 6, 201–211. Davey, G.C.L., MacDonald, B.A., Brierley, L., 2008. The effect of disgust on anxiety ratings to fear-relevant, disgust-relevant and fear-
irrelevant stimuli. Journal of Anxiety Disorders 22, 1347–1354. de Haan, J., Belsky, J., Reid, V., Volein, A., Johnson, M., 2004. Maternal personality and infant's neural and visual responsivity to facial
expressions of emotion. Journal of Child Psychology and Psychiatry 45, 1209–1218. Feldman, R., 2007. Parent–infant synchrony and the construction of shared timing; physiological precursors, developmental
outcomes, and risk conditions. Journal of Child Psychology and Psychiatry 48, 329–354. Field, T., 1997. The treatment of depressed mothers and their infants. In: Murray, L., Cooper, P.J. (Eds.), Postpartum Depression and
Child Development. The Guilford Press, NY, pp. 221–236. Field, T., 2002. Early interactions between infants and their postpartum depressed mothers. Infant Behavior & Development 7, 527–
532. George, M.S., Huggins, T., Mcdermut, W., Parekh, P.I., Rubinow, D., Post, R.M., 1998. Abnormal facial emotion recognition in
depression: serial testing in an Ultra-RapidCycling Patient. Behavior Modification 22, 192–204. Gollan, J.K., Pane, H.T., McCloskey, M.S., Coccaro, E.F., 2008. Identifying differences in biased affective information processing in
major depression. Psychiatry Research 159, 18–24. Gonidakis, F., Rabavilas, A.D., Varsou, E., Kreatsas, G., Christodoulou, G.N., 2008. A 6- month study of postpartum depression and
related factors in Athens Greece. Comprehensive Psychiatry 49, 275–282. Guedeney, A., Fermanian, J., 1998. Validation study of the French version of the Edinburgh Postnatal Depression Scale (EPDS): new
results about use and psychometric properties. European Psychiatry 13, 83–89. Gur, R.C., Erwin, R.J., Gur, R.E., Zwil, A.S., Heimberg, C., Kraemer, H.C., 1992. Facial emotion discrimination: II. Behavioral findings in
depression. Psychiatry Research 42, 241–251. Hale, W.W., 1998. Judgement of facial expressions and depression persistence. Psychiatry Research 80, 265–274. Heron, J., O'Connor, T., Evans, J., Golding, J., Glover, J., 2004. The course of anxiety and depression through pregnancy and the
postpartum in a community sample. Journal of Affective Disorders 80, 65–73. Kendell, R.E., Mackenzie, W.E., West, C., McGuire, R.J., Cox, J.L., 1984. Day-to-day mood changes after childbirth: further data. The British Journal of Psychiatry 145, 620–625. Kojima, M., Senda, Y., Nagaya, T., Tokudome, S., Furukawa, T., 2003. Alexithymia, depression and social support among Japanese
workers. Psychotherapy and Psychosomatics 72, 307–314. Lazarus, R.S., 1991. Emotion and Adaptation. Oxford University Press, NY. Le, H.N., Ramos, M.A., Munoz, R.F., 2007. The relationship between alexithymia and perinatal depressive symptomatology. Journal of
Psychosomatic Research 62, 215–222. Leppänen, J.M., Milders, M., Bell, J.S., Terriere, E., Hietanen, J.K., 2004. Depression biases the recognition of emotionally neutral
faces. Psychiatry Research 128, 123–133. Loas, G., Otmani, O., Verrier, A., Fremaux, D., Marchand, M.P., 1996. Factor analysis of the French version of the 20-item Toronto
Alexithymia Scale (TAS-20). Psychopathology 29, 139–144. Lundy, B., Field, T., Pickens, J., 1996. Newborns of mothers with depressive symptoms are less expressive. Infant Behavior &
Development 19, 419–424. Lundy, B., Field, T., Cigales, M., Cuadra, A., 1997. Vocal and facial expression matching in infants of mothers with depressive
symptoms. Infant Mental Health Journal 18, 265–273. Marzillier, S., Davey, G.C.L., 2005. Anxiety and disgust: evidence for a unidirectional relationship. Cognition and Emotion 19, 729–750.

11
Matias, R., Cohen, J.F., 1993. Are Max-specified infant facial expressions during face-to-face interaction consistent with differential emotions theory? Developmental Psychology 29, 524–531.
Mendlewicz, L., Linkowski, P., Bazelmans, C., Philippot, P., 2005. Decoding emotional facial expressions in depressed and anorexic patients. Journal of Affective Disorders 89, 195–199.
Mota, N., Cox, B., Enns, M.W., Calhoun, L., Sareen, J., 2008. The relationship between mental disorders, quality of life, and pregnancy: findings from a nationally representative sample. Journal of Affective Disorders 109, 300–304.
Murray, L., 1992. The impact of postnatal depression on infant development. Journal of Child Psychology and Psychiatry 33, 543–561. Nadel, J., Soussignan, R., Canet, P., Libert, G., Gérardin, P., 2005. Two-month-old infants of depressed mothers show mild, delayed
and persistent change in emotional state non-contingent interaction. Infant Behavior & Development 28, 418–425. Niedenthal, P.M., Halberstadt, J.B., Margolin, J., Innes-Ker, A.H., 2000. Emotional state and the detection of change in facial
expression of emotion. European Journal of Social Psychology 30, 211–222. O'Hara, M.W., Swain, A.M., 1996. Rates and risk of postpartum depression: a metaanalysis. International Review of Psychiatry 8, 37–
54. O'Hara, M.W., Schlechte, J.A., Lewis, D.A., Wright, E.J., 1991. Prospective study of postpartum blues: biologic and psychosocial
factors. Archives of General Psychiatry 48, 801–806. Öhman, A., Flykt, A., Esteves, F., 2001. Emotion drives attention: detecting the snake in the grass. Journal of Experimental
Psychology: General 130, 466–478. Papousek, H., Papousek, M., 1997. Fragile aspects of early social integration. In: Murray, L., Cooper, P. (Eds.), Post Partum Depression
and Child Development. The Guilford Press, New York, pp. 35–53. Phillips, M.L., Senior, C., Fahy, T., David, A.S., 1998. Disgust: the forgotten emotion in psychiatry. The British Journal of Psychiatry 172,
373–375. Robertson, E., Grace, S., Wallington, T., Stewart, E., 2004. Antenatal risk factors for postpartum depression: a synthesis of recent
literature. General Hospital Psychiatry 26, 289–295. Rossignol, M., Anselme, C., Vermeulen, N., Philippot, P., Campanella, S., 2007. Categorical perception of anger and disgust facial
expression is affected by nonclinical social anxiety: an ERP study. Brain Research 1132, 166–176. Rozin, P., Fallon, A.E., 1987. A perspective on disgust. Psychological Review 94, 23–41. Rubinow, D.R., Post, R.M., 1992. Impaired recognition of affect in facial expression in depressed patients. Biological Psychiatry 31,
947–953. Schofield, C.A., Coles, M.E., Gibb, B.E., 2007. Social anxiety and interpretation biases for facial displays of emotion: emotion
detection and ratings of social cost. Behaviour Research and Therapy 45, 2950–2963. Schweitzer, M.B., Paulhan, I., 1990. Manuel pour l'Inventaire d'Anxiété Trait - Etat (forme Y). Editions du Centre de Psychologie
Appliquée, Paris. Séjourné, N., Denis, A., Theux, G., Chabrol, H., 2008. The role of some psychological, psychosocial and obstetrical factors in the
intensity of postpartum blues. L'Encéphale 34,179–182. Skouteris, H., Wertheim, E.H., Rallis, S., Milgrom, J., Paxton, S.J., 2009. Depression and anxiety through pregnancy and the early
postpartum: an examination of prospective relationships. Journal of Affective Disorders. 113, 303–308. Spielberger, C.D., Gorsuch, R.L., Lusthene, R.E., 1983. Manual for the State-Trait Anxiety Inventory. Consulting Psychologist Press,
Palo Alto. Striano, T., Brennan, P.A., Vanman, E.J., 2002. Maternal depressive symptoms and 6-monthold infants' sensitivity to facial
expressions. Infancy 3,115–126. Stuart, S., Couser, G., Schilder, K., O'Hara, M., Gorman, L.,1998. Post-partum anxiety and depression: onset and comorbidity in a
community Sample. The Journal of Nervous and Mental Disease 186, 420–424. Sullivan, M.W., Lewis, M., 2003. Contextual determinants of anger and other negative expressions in young infants. Developmental
Psychology 39, 693–705. Surcinelli, P., Codispoti, M., Montebarocci, O., Rossi, N., Baldaro, B., 2006. Facial emotion recognition in trait anxiety. Journal of
Anxiety Disorders 20, 110–117. Suslow, T., Junghanns, K., Arolt, V., 2001. Detection of facial expressions of emotions in depression. Perceptual and Motor Skills 92,
857–868. Tamaki, R., Murata, M., Okano, T., 1997. Risk factors for postpartum depression in Japan. Psychiatry and Clinical Neurosciences 51,
93–98. Taylor, G.J., Bagby, R.M., Luminet, O., 2000. Assessment of alexithymia: self-report and observer-rated measures. In: Bar-On, R.,
Parker, J.D.A. (Eds.), The Handbook of Emotional Intelligence: Theory, Development, Assessment, and Application at Home, School, and in the Workplace. Jossey-Bass, San Francisco, pp. 301–319.
Teissèdre, F., Chabrol, H., 2003. Postnatal depression: a study of the predictive effects of postnatal anxiety. Irish Journal of Psychological Medecine 20, 111–114.
Teissèdre, F., Chabrol, H., 2004. Detecting women at risk of postnatal depression using the EPDS at 2 to 3 days postpartum. Canadian Journal of Psychiatry 49, 51–54.
Tronick, E.Z., Weinberg, M.K., 1997. Depressed mothers and infants: failure to form dyadic states of consciousness. In: Cooper, P., Murray, L. (Eds.), Post Partum Depression and Child Development. The Guilford Press, New York, pp. 54–81.
Verdoux, H., Sutter, A.L., Glatigny-Dallay, E., Minisini, A., 2002. Obstetrical complications and the development of postpartum depressive symptoms: a prospective survey of the MATQUID cohort. Acta Psychiatrica Scandinavica 106, 212–219.

Weinberg, M.K., Tronick, E.Z., 1994. Beyond the face: an empirical study of infant affective configurations of facial, vocal, gestural, and regulatory behaviours. Child Development 65, 1495–1507.
Woody, S.R., Tolin, D.F., 2002. The relationship between disgust sensitivity and avoidant behavior: studies of clinical and nonclinical samples. Journal of Anxiety Disorders 16, 543–559.