the epdsc buddy walk raises more than $50,000! · to support our membership. ... maria floryshak,...
TRANSCRIPT

I would sincerely like to thank all of you who took part in the 12th Annual EPDSC Buddy Walk. What an amazing event!
The day was perfect and we are thankful that the rain held off. More than 900 people, who all joined together to raise more than $50,000 for the EPDSC, attended the event. The funds raised will be used for a combination of operating costs, scholarships, education and social events, NDSS affiliation and to continue to support our membership.
The purpose of the Buddy Walk is to raise awareness of individuals with Down syndrome. The staff and volunteers at the EPDSC strive to meet this goal and provide an environment for families to get to know each other better every time we get together. After all, family support is very valuable. It is the fellowship and support that happens during and outside of EPDSC events that keeps us going and encouraged. We at the EPDSC recognize this since we have had the blessing of other families in our lives. If you would like to get to know more people in the EPDSC network, please contact the Center or join the EPDSC facebook page.
I would like to thank the Buddy Walk volunteer committee who gave their time and energy to make this event such a success. Many thanks to Wendy Carney, Maria Floryshak, Chris Farrell, Steve Neary, Jen Miller, Anne Marie Dolinish-Meltzer and all the other volunteers who helped on the day of the Buddy Walk.
Please know that if you would like to help for 2012 Buddy Walk, we would really love for you to join our committee. Just contact the Center and we’ll get you plugged in. There are many, many families in the EPDSC network and we would love to have more of you involved.
As for next year, we have already begun working and planning! Watch for more information via email, website and newsletter for details. There are exciting and promising developments on the medical side of Down syndrome that we at the EPDSC want to keep you all informed of so that YOU and YOUR family can benefit.
Thanks again. My life is blessed to be a part of the EPDSC and the Buddy Walk. Bobby Lanyon, Buddy Walk Coordinator
Fall 2011
The EPDSCBuddy Walk Raises More Than $50,000!
Where memories are made in the name of a wonderful cause
Dr. Allen C. CrockerRemembering a giant in the Down syndromecommunity.
Enjoying the Season!Read about some of the great autumn events that the EPDSC has hosted.
Medical Assistance NewsFind out what has changed in dental cover-age for those with MA.
Mock My Pants!Dr. Brian Skotko speaks out against an offensive article in GQ magazine.
Behavioral ChallengesGuidelines to determine if your child’s behavior might be significant.
EPDSC Holiday PartyGet details for this event taking place on Saturday, December 10th!
In This Issue
3
4
5
8
10
12
Board of Directors
• Kevin Neiley• Mike Carney• Jason Anderson• Chris Farrell• Steve Neary• Sue Cully• Bobby Lanyon• Ali Heller• Jennifer Miller• Anita Ellsberry• Michelle Levene• Liz DeSantis (at large)• Bill Meltzer (at large)• Keith Frisch (at large)• Sue McGorry (at large)
Officers
• Kevin Neiley, President• Mike Carney, Vice President• Steve Neary, Treasurer• Sue Cully, Secretary
Staff
• Don Levick, M.D., MBA, Medical Director• Renee Morrow-Connelly, D.O. Pediatrics• Scott Rice, M.D., Pediatrics• Amy Healy, MS, OTR/L• Andrea Meeker, MS, OTR/L• Kelly Nelson, MS, OTR/L• Patti Mertz, Center Coordinator• Maria Floryshak, Center Coordinator• Anne Marie Dolinish-Meltzer, RN,BSN, Center Coordinator• Claire Dainese, Office Assistant• Diana Santoro, Newsletter
theEPDSC
Hello Friends:
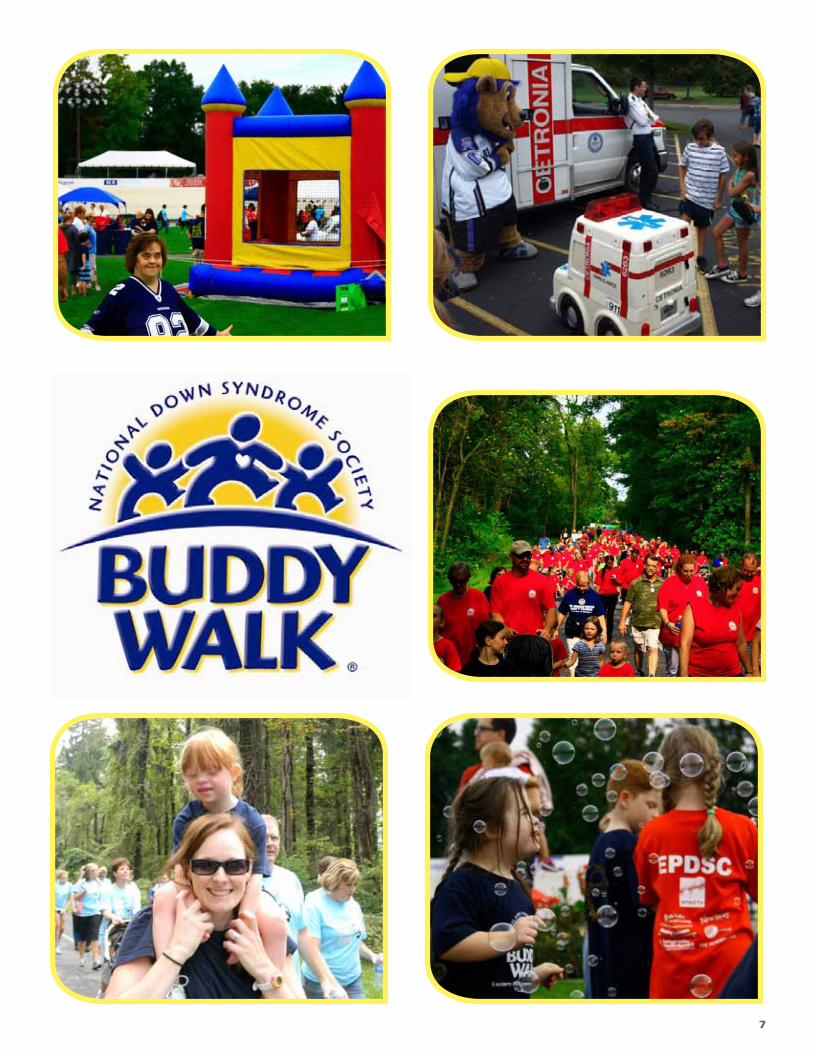
We just completed the Buddy Walk for 2011, I was very happy to see how successful the event was. It was not only a fundraiser, but a time for over 900 people to get together for fellowship and support a cause we all have in common—the wish to provide a better life for our kids and family members.
Preparing for the Buddy Walk took a lot of work by staff and volunteers who worked countless hours to make the Buddy Walk a huge success. Imagine; if only a handful of folks were able to organize all of the activities before, and the day of the Walk, what all of us together could accomplish if everyone gave a little time and volunteered to help our family members and the Center. The difference we could make is enormous.
I welcome and encourage everyone to get involved! We guarantee the time you volunteer will be worthwhile!
I look forward to seeing everyone at the holiday party on December 10th.
Sincerely,
Kevin NeileyPresident, EPDSC
Letter fromthe President

3
On the morning of Sunday, October 23, the medical community, disability community and countless individuals and families who had been touched by his kindness and helped by his medical expertise, lost a giant.
Dr. Crocker’s contribution to disability science and advocacy is almost hard to fathom. In 1967, he opened the Developmental Evaluation Center (DEC) at Children’s, which he continued to direct for 26 years (now known as the
Learning Education in Neurodevelopmental and Related Disabilities program). In 1983, through the publication of a 1,200-page textbook, “Developmental-Behavioral Pediatrics,” he, along with other authors, essentially established the field of developmental pediatrics. He published eight textbooks in all.
He served on the board of directors of the Massachusetts Down
Syndrome Congress for more than 20 years. He also served on the boards of the Boston Institute for Arts Therapy, the Special Olympics, the Marcus Developmental Resource Center, and the National Down Syndrome Congress. He was chairperson of the Adaptive Environments Center, president of the Citizen Advisory Board for Massachusetts’ Department of Developmental Services (formerly DMR). He served on the Advisory Committee for the Office of Health and Disability, the Governor’s Commission on Mental Retardation, and the Advisory Council for Massachusetts Bureau of Family and Community Health. He was a co-founder and co-director of New England Regional Genetics Group. He was an Associate Professor of Maternal and Child Health at the Harvard School of Public Health and Senior Associate in Medicine at Children’s Hospital.
But as everyone who knew Dr. Crocker could attest, he was even more than the sum of his remarkable achievements. He was advocate, an activist and a friend, standing up for and behind those who he realized were unseen, misunderstood, unrepresented, or undersold by mainstream society.
You will be missed dearly, Dr. Crocker!
Allen C. Crocker Self-Advocate Internship Fund
A living memorial has been created for Dr. Allen C. Crocker to honor his legacy and lifelong work. Donations in his memory may be made to the Massachusetts Down Syndrome Congress (payable to MDSC) for the Allen C. Crocker Self-Advocate Internship Fund to 20 Burlington Mall Road, Suite 261, Burlington, MA 01803 or by visiting http://mdsc.kintera.org/crockerfund.
Through the Dr. Crocker Intership Program, self-advocates with Down syndrome will have the opportunity to continue Dr. Crocker’s lifelong mission of promoting the acceptance and inclusion of all people, including those with Down syndrome.
The Life of Dr. Allen C. Crocker (1925-2011)
EPDSC Activities
The beginning of the school year brings many changes and a desire to understand the diverse learning needs of all the students. Patti Mertz, our Educational Consultant, provided professional development seminars for educators and school personnel at both the middle school and high school of Northampton School District. Patti was also involved in providing support and technical assistance to family and school in the Northern Lehigh School District that was interested in implementing an inclusive environment.
Advocating on behalf of individuals with Down syndrome, Patti has observed several students in their school environment in order to provide support, recommendations, and resources during IEP meetings.
The staff of the Center has also been fortunate to meet and welcome several new families into our network. Maria and Patti recently met with families and their newborns with Down syndrome. The meetings consisted of a tour of the Center, a brief preview of our lending library, a lengthy discussion about the services the Center provides, and anopportunity to answer questions. Separate meetings with new families are a common occurrence due to the time period it takes to schedule new appointments at the Center.
New parent packets have recently been distributed to our area hospitals so that families experiencing the birth of a new baby with Down syndrome have the most up-to-date information possible. We are proud to be able to provide the packets so that their newborns get off on the best foot possible.
The Conference Committee has been very busy contacting and confirming speakers for “Home. Health and Future 2012”. Next year’s conference will be held at the Lehigh Valley Hospital Center, Cedar Crest and I-78 in Allentown, PA. The committee has reserved Saturday, March 31, 2012 for the parent/professional date and is working on the Self-Advocate Conference as well. “We are focusing on getting speakers that were requested in last year’s surveys, as well as presenting new information that has developed within the last 12 months. We’re very excited!” Please save the date and plan on attending “Home, Health and Future 2012”.

Trick or Treat started early this year at the Iron Pigs “Suites and Treats” night on October 26th. Children, decked out in their Halloween finest, were treated to all different kinds of goodies in the upstairs suites which were decorated in themes that ranged from Candyland to Hogwarts to disco to Santa’s Workshop. Refreshments were served in the dining area. It was a howling success!
Say YES! to ScarecrowsThe Eastern PA Down Syndrome Center joined in the annual “Say Yes to Scarecrows” event in Emmaus on October 8, 2011. Local non profit agencies are invited to build a scarecrow to compete for top prizes and donations from the community.
The EPDSC scarecrow this year is Spiderman and he is enjoying his view from the porch of Janet’s Stained Glass Shop. Please stop by Janet’s shop and thank her for supporting the EPDSC.
EPDSC Events
Suites and Treats

News You Should Know
5
Department of Public Welfare Announces Medical Assistance Dental Benefits Changes The September 24, 2011 edition of the PA Bulletin includes a Department of Public Welfare (DPW) notice announcing benefit package changes for certain dental services for adult Medical Assistance recipients 21 years of age and older, effective September 30, 2011. This is one of the first regulatory Notices under the authority of Act 22 of 2011 which gives the Department the ability to change certain benefits simply by issuing a “notice” of the change. While the Department is allowing a 30-day public comment period on this notice, these comments will only be “reviewed and considered for any subsequent revision of the dental benefit package.”
The implications of Act 22 for the service system was discussed in detail at PAR’s September 22 General Membership meeting by former DPW Chief Counsel Allen Warshaw, Esq. of Rhoads and Sinon. PAR is keeping a close watch on the Department’s implementation of Act 22 and will be alerting members as issues arise.Excerpts from the notice are in italics below:
The Department has taken steps to identify cost containment initiatives that will have the least detrimental impact on the health care needs of the Medical Assistance population.
Rather than eliminating all dental services for the Medical Assistance adult population, the Department closely evaluated the utilization of, and payments for, particular dental services to determine which services could be limited with minimal impact. Based on medical Assistance utilization and claims data from state fiscal year 2009-2010, the most recent year for which complete data is available, the changes to the dental benefit package would have had no impact on over 96% of the total Medical Assistance eligible adult population eligible for dental benefits who received services in that fiscal year. The Department will therefore realize significant cost savings while maintaining core preventative services as well as some other dental services for recipients.Effective September 30, 2011, adult Medical Assistance recipients 21 years of age and older will be eligible for the following:
• One partial upper denture or one full upper denture and one partial lower denture or one full lower denture per lifetime. Additional dentures will require a benefit limit exception.
• One dental exam and prophylaxis per 180 days, per adult recipient. Additional dental exams and prophylaxis will require a benefit limit exception.
• Crowns and adjunctive services, periodontal and endodontic services if the recipient receives a benefit limit exception.
The Department will grant benefit limit exceptions to the dental benefit package when one of the following criteria is met:
1. The Department determines that the recipient has a serious chronic systemic illness or other serious health condition and denial of the exception will jeopardize the life of the recipient.
2. The Department determines that the recipient has a serious chronic systemic illness or other serious health condition and denial of the exception will result in the rapid, serious deterioration of the health of the recipient.
3. The Department determines that granting a specific exception is a cost effective alternative for the Medical Assistance Program.
4. The Department determines that granting an exception is necessary to comply with Federal law.
The specified dental benefit package changes do not apply to Medical Assistance recipients under 21 years of age or to Medical Assistance recipients who live in a nursing facility, in an intermediate care facility for persons with mental retardation or in intermediate care facilities for persons with other related conditions.
The complete notice can be found at: http://www.pabulletin.com/secure/data/vol41/41-39/1672.html
5

7

Mock my pants, not my sisterby CHILDRENS HOSPITAL BOSTON STAFF on 7/18/11
The following was written by Brian Skotko , MD, MPP, a Physician at Children’s Hospital Boston’s Down Syndrome Program. It’s in response to a feature in GQ magazine that used insensitive language.
On July 15, John B. Thompson of GQ magazine slammed Bostonians as the worst dressed in the nation. Evidently, our beloved Beantown is actually a “bad-taste storm sewer” where all the worst fashion ideas come to “stagnate and putrefy.” He further decries, “Boston suffers from a kind of Style Down Syndrome , where a little extra ends up ruining everything.”
Go ahead, GQ, and mock my blue whale-emblemed Nantucket-red pants. Laugh if you want at the loud argyles that I prefer to wear with my black suit. I don’t even care if you dismiss the sexy pink polka-dotted tie that I like to wear with my blue-checkered shirt in clinic. But, whatever you do, do not mess with my sister.
My sister, Kristin, has Down syndrome, and let me explain what “Style Down Syndrome” really is.
“Style Down Syndrome” is smiling when everyone else prefers to frown. It’s spending three summers, in sheer determination, learning to ride a bike because you want the freedom to be like everyone else. It’s singing tunes from Grease at the top of your lungs with your friends. It’s celebrating a third-place victory at a swim meet with as much gusto as the gold medalist.
Style Down Syndrome is strong-willed, persevering, and forgiving—because it has to be.
People with Down syndrome are ridiculed on a daily basis. Although not as obvious as GQ’s sport, children with Down syndrome do not always get invited to birthday parties just because they have Down syndrome. Young adults, freshly minted from high school, sometimes have trouble finding post-secondary opportunities. And, adults with Down syndrome are often the first to be fired when the economy tanks.
All of this comes at a time when people with Down syndrome are achieving previously unimagined successes. They are graduating, working, living and loving within our communities. So, why do people underestimate their abilities? It must be because they do not know someone with Down syndrome. Because, if they did, they would come to appreciate the life lessons that accompany their extra chromosome.
If my friends who are black were mocked, they would not take it. If my friends who are gay were slurred, they would not take it. My 400,000 fellow Americans with Down syndrome have been cheapened, and I will not take it. I invite GQ magazine to introduce its readers to real people with Down syndrome through the My Great Story campaign of the National Down Syndrome Society.
* Editor’s note: Mock my pants not my sister has created a lot of dialogue on the subject of advocacy for the Down syndrome community as well as the use of insensitive language, and resulted in plenty of mainstream media attention to the issue. To date the blog has been referenced in the Washington Post, Boston Business Journal, Boston Magazine, the Boston Globe and FOX News. To learn more about the many social and mainstream media platforms Dr. Skotko’s post has influenced, please visit the following web site: http:// http://childrenshospitalblog.org/childrens-blog-makes-headlines
Brian Skotko and his sister, Kristen

9
School buses carry approximately 24 million children each year and collectively travel more than four billion miles. At nearly eight times safer than passenger vehicles, school buses are the safest way for children to get to and from school. Unfortunately, accidents involving school buses can occur.
Approximately 25 children are killed each year in school bus crashes or while getting on or off the bus. Most of these children are between the ages of five and seven.
Children most likely to be involved in a school bus-related accident are those who are rushing toget on or off the bus or have limited experience with traffic.
Other factors that put children at risk foraccidents include assuming other drivers will stop for them, not staying within the bus driver’s line of sight and picking up something that has been dropped in the path of the bus.
Parents can teach their children some basic rules about school bus safety to help preventaccidents and injuries.
• Make sure children are at the bus stop at least five minutes before the bus is due to arrive. As the bus approaches, children should stand approximately six feet away from the curb and line up away from the street.
• Wait until bus comes to a complete stop, the door opens and the bus driver signals the children to board the bus. Children crossing the street to get on the bus must look both ways for oncoming traffic and then walk at least 10 feet in front of the bus to make sure the bus driver sees them.
• Children should always get on and off the bus at safe, designated locations.
• When boarding or exiting the bus, children should use handrails to avoid falls and make sure no backpack strap or loose item of clothing such as a drawstring gets caught in a handrail or door.
• On the bus, children should sit down, not rush around or push, and put on safety belts if the bus is equipped with them.
They must always follow the bus driver’s instructions• If children drop something when exiting the bus, they should not stop to pick it up because the bus driver may not see them.
School bus safety is important for adults too. Drivers need to look out for children walking or biking to school while backing out of a driveway or leaving a garage. They also should slow down andwatch for children who are congregating near bus stops
or are walking in the street if there are no sidewalks. Be aware that children may dart into the street without looking for traffic.
Motorists should slow down and prepare to stop when they see flashing yellow lights on the school bus and drivers must stop and not pass the school bus when the lights are flashing red and the stop signal arm is extended.
By learning and following these simple guidelines, both children and adults can work together to make sure school bus transportation is safer for everyone.
For more information about school bus safety, visit the National Highway Traffic Safety Administration Web site at www.nhtsa.gov.
July 27, 2011, St. Christopher’s Hospital News
The Importance of School Bus Safety

the child’s behavior during a typical day at home or school can sometimes help to identify an event that may have triggered the non-compliant behavior. At times the oppositional behavior may the child’s way of communicating frustration or lack of understanding due to their communication/language problems. Children with Down syndrome become very good at distracting parents or teachers when they are challenged with a difficult task.
Attention problems—children with Down syndrome can have ADHD but they should be evaluated for attention span and impulsivity based on developmental age and not strictly chronological age. The use of parent and teacher rating scales such as the Vanderbilt and the Connors Parent and Teacher Rating Scales can be helpful in diagnosis. Anxiety disorders, language processing problems and hearing loss can also present as problems with attention.
Obsessive/compulsive behaviors—these can be as simple as always wanting the same chair at the table to repetitive behaviors such as dangling beads or belts when not engaged directly in an activity. This type of behavior is
seen more commonly in younger children with Down syndrome and while the number of compulsive behaviors is no different than those in typical children at the same mental age the frequency and intensity of the behavior is often more in children with Down syndrome.
Autism Spectrum Disorder—autism is seen in approximately 5-7% of children with Down syndrome. The diagnosis is usually made at a later age (6-8 years of age) then in the general population and regression of language skills if present also occurs later (3-4 years of age). The interventions strategies are the same as for any child with autism and it is important for the child to
be identified as early as possible so he/she can receive the most appropriate therapeutic and educational services. How should parents approach behavior issues in their child with Down syndrome?
1. Rule out a medical problem that could be related to the behavior.
2. Consider emotional stresses at home/school/work that may impact behavior.
3. Work with a professional (psychologist, behavioral pediatrician, counselor) to develop a behavior treatment plan using the ABC’s of behavior. (Antecedent, Behavior, Consequence of the behavior)
4. Medication may be indicated in particular cases such as ADHD and autism.
Intervention strategies for treatment of behavior problems are variable and dependent on the child’s age, severity of the problem and the setting in which the behavior is most commonly seen. Local parent support programs can often help by providing suggestions,support and information about community treatment programs. Psychosocial services in the primary care physician’s office can be used for consultative care regarding behavior issues. Chronic problems warrant referral to a behavioral specialist experienced inworking with children and adults with special needs.
By Bonnie Patterson, MD, NDSS Guest Author
Behavioral Challenges in People with Down Syndrome
The definition of a “behavior problem” varies but certain guidelines can be helpful in determining if a behavior has become significant.
1. Does the behavior interfere with development and learning?
2. Are the behaviors disruptive to the family/school/work place?
3. Is the behavior harmful to the child/adult or others?4. Is the behavior discrepant from what might be
typically displayed by someone of comparable developmental age?
The first step in evaluation of a child/adult with Down syndrome who presents with a behavior concern is to determine if there are any acute or chronic medical problems related to the identified behavior. The following is a list of the more common medical problems that may be associated with behavior changes.
1. Vision or hearing deficits.2. Thyroid function3. Celiac disease4. Sleep apnea5. Anemia6. Gastro esophageal reflux7. Constipation8. Depression9. Anxiety
Evaluation by the primary care physician is an important component of the initial work-up for behavior problems in children or adults with Down syndrome.
The behavioral challenges seen in children with Down syndrome are usually not all that different from those seen in typically developing children. However, they may occur at a later age and last somewhat longer. For example temper tantrums are common in 2-3 year olds, for a child with Down syndrome temper tantrums may begin at 3-4. When evaluating behavior in a child with Down syndrome it is important to look at the behavior in the context of the child’s developmental age, not only their chronological age. It is also important to know the child’s receptive and expressive language skill level as many behavior problems are related to frustration with communication. Many times the behavior issues can be addressed by finding ways to help the child communicate more effectively. The following are some of the common behavior concerns reported by parents/teachers.
Wandering/running off—the most important thing is the safety of the child. This would include good locks and door alarms at home and a plan written into the IEP at school regarding what each person’s role is in the event the child leaves the classroom or playground. Visual supports such as a STOP sign on the door and/or siblings asking permission to go out the door can be a reminder to the child to ask permission before leaving the house.
Stubborn/oppositional behavior—a description of

Autism Can Be Diagnosed in Down Syndrome
Children with Down syndrome can be diagnosed with autism via the autism spectrum disorder criteria from the Diagnostic and Statistical Manual of Mental Disorders, based on results of a cluster analysis of 293 children with Down syndrome.
Previous studies have suggested that autism spectrum disorders (ASD) can’t be effectively diagnosed in children with Down syndrome (DS) because of the cognitive impairment already associated with DS, said Dr. N.Y. Ji of Johns Hopkins University, Baltimore.
In this study, Dr. Ji and colleagues used the Aberrant Behavior Checklist to show that children with both DS and ASD match the DSM criteria for autism diagnoses (J. Intellect. Disabil. Res. 2011 Aug. 30 [doi:10.1111/j.1365-2788.2011.0465.x]).
The researchers assessed more than 1,000 children aged 0-21 years who visited the Down syndrome clinic of the Kennedy Krieger Institute in Baltimore during 1992-2008. They identified 293 children for cluster analysis and used the Aberrant Behavior Checklist–Community (ABC-C) and the Autism Behavior Checklist to identify autism features. For comparison, the researchers also identified children with DS and two other common DS comorbidities: disruptive behavior disorder (DBS) and stereotypic movement disorder (SMD).
Overall, 114 children (39%) met criteria for ASD, 104 (36%) met criteria for DBS, and 43 (15%) had SMD. Another 32 children (11%) did not meet criteria for any coexisting major psychiatric condition in addition to DS.
The findings add to the field of Down syndrome research because they confirm the DSM diagnostic criteria of autism spectrum disorder in children with Down syndrome. The researchers divided the children into four clusters based on the ABC-C and Autism Behavior Checklist.
Participants in clusters 1 and 4 had lower levels of intellectual functioning than did those in clusters 2 and 3, although there was no significant difference in the median age among the groups, the researchers noted.
In addition, children in cluster 1 had a broad range of behavioral problems, including self-injury and highly disruptive behavior.
Children in cluster 2 had the lowest ABC-C scores and the mildest levels of maladaptive behavior.
Children in cluster 3 had high disruptive behavior scores similar to those seen in cluster 1, but significantly less severe autistic behaviors.
Children in cluster 4 had the most severe autistic behaviors, compared with the other clusters.
Children in clusters 1 and 4 underwent additional analysis to confirm that they resembled the original DS plus ASD diagnostic group. This additional analysis confirmed that children with DS and ASD with “more irritable and hyperactive behaviors as well as high levels of self-injury” were more likely to fall into cluster 1, whereas children with more severe autistic behavior fell into cluster 4. In addition, significantly more children in cluster 4 had a history of late onset ASD, compared with those in cluster 1.
“These data also support the existence of ASD subtypes in DS, in line with the heterogeneity of the behavioral disorder in the general population,” the researchers noted.
The study was limited by the relatively small number of children in each category and by the use of only the ABC-C data for the primary analysis, the researchers said.
However, the findings add to the field of DS research because they confirm the DSM diagnostic criteria of ASD in children with DS. Additional longitudinal studies could examine whether the DSM diagnoses remain stable over time. Better behavioral instruments are needed to help clinicians recognize comorbidities and suggest targeted interventions, they added.
“We have known for some time that Down syndrome is associated with a range of neurodevelopmental and behavioral outcomes,” said Dr. George T. Capone, a study coauthor. “We hypothesized that the association between developmental function and behavior was not random; rather, the two are related in such a manner that distinct behavioral clusters can be identified.”
The study underscores the point that children with Down syndrome are not all alike, he explained, which has “direct implications for our understanding of brain organization and possibly the relationship between genotype and phenotype in young children with the diagnosis.”
He and his colleagues were not particularly surprised by the findings, he added, because “it has long been our observation that children with Down syndrome and maladaptive behavior differ from their typical peers with the diagnosis.” These differences are obvious and measurable both to parents who respond to validated behavioral questionnaires and to neurodevelopmental pediatricians who use a DSM classification to identify behavior and mental health disorders.
Increased vigilance, screening, and evaluation for atypical development and behavior problems have recently received greater emphasis in the American Academy of Pediatrics’ updated “Health Supervision for Children with Down Syndrome” guidelines (Pediatrics 2011 128:393-406).
“Our study findings support the existence of well-delineated behavior clusters in children with DS, and in our clinic we have witnessed educational success when these issues are recognized and addressed. Pediatricians can do families a great service by recognizing that a coexisting neurobehavioral condition may be present,” said Dr. Capone of the department of pediatrics at Johns Hopkins University, who is also director of the Down syndrome clinic at the Kennedy Krieger Institute, both in Baltimore. With proper evaluation and treatment, he noted, children with DS and disruptive behaviors or ASD can benefit from a combination of medication and behavior management, in addition to an educational program emphasizing functional communication and social skills development.
The study was supported in part by grants from Autism Speaks, a nonprofit association. The researchers had no relevant financial conflicts disclosures.
By Heidi Splete, Family Practice News Digital Network 11

Mark Your Calendars
PO Box 606900 Hamilton BoulevardTrexlertown, PA 18087
Phone: 610.402.0184Fax: 610.402.0187Email: [email protected]: www.epdsc.net
Contact Us
2011 EPDSC Holiday Party
You are invited to celebrate the holidays with good food, great friends, & Santa!
To guarantee your seat, please RSVP to the EPDSC as soon as possible (but no later
than Thursday, December 1)
[email protected] or (610) 402-0184
FREE for current members and their children!
Non-members: Adults $15, Children $10
Date: Saturday, December 10th
Time: 9:30am - 12:00pm
Place: The Hamilton Room @ Allentown Brew Works 812 Hamilton Street, Allentown, PA 18101
** Plenty of FREE parking **