the effect of two different immediate loading protocols
DESCRIPTION
The Effect of Two Different Immediate Loading Protocols in Implant-Supported Screw-Retained ProsthesesTRANSCRIPT
The Effect of Two Different ImmediateLoading Protocols in Implant-Supported
Screw-Retained ProsthesesHeba E. Khorshid, BDS, MS,* Hamdy Aboul Fotouh Hamed, BDS, MS, PhD,† and Essam A. Aziz, BDS, MS, PhD‡
The ultimate goal for moderndentistry is to restore the patientto normal facial contour, func-
tion, aesthetics, speech, health, andcomfort.1 Clinical studies on humansand animals have shown that imme-diately loaded implants developbone at the implant surface and areable to tolerate occlusal forces.1,2
The choice of an occlusal scheme forimmediately loaded implant-supportedprosthesis is broad and often controver-sial.3 Because of this controversy, itwould be wise to study the effect ofdifferent occlusal schemes in immedi-ately loaded implants to assess the pos-sible consequences on the supportingstructures of the dental implants.
Various immediate loading pro-tocols for dental implants have beenadvocated4,5:
• Immediate Functional LoadingProtocol (Direct Occlusal LoadingProtocol): where the restorationmakes full contact with the oppos-ing dentition.
• Immediate Nonfunctional Load-ing Protocol (Indirect OcclusalLoading Protocol): where the res- toration makes no direct contact
with the opposing dentition.• Progressive Loading Protocol:
where the restoration is restoredwith light contact initially and thengradually brought into full contactwith the opposing dentition.
The concept of progressive loadingarose in 1980 based on empirical infor-mation supporting the idea that low-grade bone stimulation of gradual loadingwill allow bone to mature, growdenser and improve in quality.6 Non-functional immediate teeth reported by
Misch and Scortecci7 entail a proce-dure that allows progressive loading ofthe implant.
Roberts et al8 and Rotter et al9
described the progressive loading pro-tocol as a method to control the loadapplied onto the dental implant bycontrolling the size of the occlusal ta-ble, the location of the occlusal con-tacts, the firmness of the diet, and theabsence of cantilevers. In a clinicalstudy performed by Appleton et al,10
progressively loaded implants demon-strated less marginal bone height loss
*Assistant Lecturer, Department of Prosthodontics, Faculty ofOral and Dental Medicine, Cairo University, Cairo, Egypt.†Professor, Department of Prosthodontics, Faculty of Oral andDental Medicine, Cairo University, Cairo, Egypt.‡Assistant Professor, Department of Prosthodontics, Facultyof Oral and Dental Medicine, Cairo University, Cairo, Egypt.
Reprint requests and correspondence to: HebaEzzeldin A. Khorshid, BDS, MS, 9 Addey Street,Messaha Square, Dokki, Giza, Egypt 12311, E-mail:[email protected]
ISSN 1056-6163/11/02002-157Implant DentistryVolume 20 • Number 2Copyright © 2011 by Lippincott Williams & Wilkins
DOI: 10.1097/ID.0b013e31820fbd09
Background: The aim of this workwas to evaluate the changes that occurin the supporting structures of implantsplaced bilaterally in the posterior man-dibular region as a result of 2 differentimmediate loading protocols: the imme-diate functional loading protocol andthe immediate progressive loadingprotocol.
Materials and Methods: Thirtyimplants were placed in 5 patientswith unmodified mandibular KennedyClass I. For each patient, 3 implantswere placed on each side of the pa-tient’s dental arch at the premolar/molar mandibular region. At one side,the implants were immediately loadedfollowing an immediate functionalloading protocol, whereas the otherside was loaded following an immedi-ate progressive loading protocol. Ra-diographic evaluation was carried outusing dental computed tomography atintervals of 0, 4, 9, and 24 monthsafter implant surgery.
Results: Statistical analysisshowed a more favorable bone reac-tion with a statistically significantdifference in the crestal bone height(P � 0.011) and in the crestal periim-plant bone density (P � 0.009) in theimmediate progressive loading groupthan the immediate functional loadinggroup.
Conclusion: The immediate pro-gressive loading protocol yields amore predictable bone reaction in theperiimplant crestal bone and ensuresbetter implant prognosis than the im-mediate functional loading protocol;supporting the idea that gradual load-ing or stimulation will allow bone tomature and grow denser in a 2-yearimplant follow-up period. (ImplantDent 2011;20:157–166)Key Words: immediate loading,progressive loading, functionalloading, bone density, computedtomography
IMPLANT DENTISTRY / VOLUME 20, NUMBER 2 2011 157

than conventionally loaded implants.Furthermore, the progressively loadedimplants showed a progressive in-crease in the periimplant bone density.
MATERIALS AND METHODS
Five patients were selected fromthe outpatient Prosthodontics Clinic,Faculty of Oral and Dental Medicine,Cairo University. Patients were withunmodified Class I Kennedy mandib-ular arch with equal bilateral distalextension length showing normalmaxillomandibular relationship (ClassI angle classification), with no para-functional habits and free from anysystemic disease. The average pa-tient’s age was 40.3 years. The oppos-ing arch (maxilla) was completelydentulous either by a complete set ofnatural dentition or restored with sat-isfactory fixed restorations.
ScrewIndirect one-piece implants(ImplantDirect LLC Spectra-SystemDental Implants, Calabasas Hills, CA)were the implants used in this study. Foreach patient, 6 osteotomies were pre-pared to receive 6 implants, 3 on eachside of the patient’s dental arch at thepremolar/molar mandibular region overwhich 3-unit screw-retained fixed/detachable restorations were con-structed. The insertion torque of the im-plants was checked by an adjustabletorque wrench at 30 N cm.11 Patientswere strictly instructed to follow a softdiet protocol for the first month.
48 Hours After Surgery
The provisional restorations weredelivered to the patients. On one side ofthe dental arch, the acrylic resin wasconstructed to be in “infraocclusion”.Infraocclusion was defined as a piece of0.025-mm thick shim stock passingfreely through the occlusal contact re-gion with no resistance. This side wasreferred to as the “Immediate Progres-sive Loading side.”
On the other side of the dentalarch, the acrylic resin was constructedto be in direct (full) occlusal contactwith the opposing maxillary teeth.This side was referred to as the “Im-mediate Functional Loading side”where the following occlusal protocolwas followed:
• Evenly distributed occlusal con-tacts and force (Cusp-fossa/cusp-embrasure occlusal contacts).
• Wide freedom in centric occlu-sion (wide groove and flat fossa).
• Slight reduction of the cusp in-clination especially the buccalinclines of the mandibular buc-cal cusps was performed toavoid interference in lateralexcursive movements of themandible.
• Narrowing the buccolingual and me-siodistal dimensions of the prosthesis.
21⁄2 Months After Surgery
The occlusion of “The ImmediateProgressive Loading Side” was ad-justed into light (point) contact. Asmall mix of self-cure tooth-coloredacrylic resin was adapted over the cen-tral fossae of the occlusal surface ofthe restoration. The patient was thenasked to close lightly over a 0.025-mmshim stock placed on the doughyacrylic resin which was then left tofully polymerize. The 0.025-mm plas-tic shim stock was pulled out withresistance when the patient was apply-ing maximum biting force. Using thistechnique, axial forces are transmittedto the implant body (Fig. 1, A).
3 Months After Surgery
Two weeks later, the occlusalcontacts of “The Immediate Progres-sive loading Side” were adjustedinto full contact (area contact) overthe central fossae only. A normaldiet was allowed 3 months after sur-gery (Fig. 1, B).
31⁄2 Months After Surgery
Two weeks later, the occlusal con-tacts of “The Immediate Progressiveloading Side” were adjusted so as toallow contact over the central fossae andbuccal inclines of the lingual mandibu-lar cusps. No contact was allowed overthe buccal and lingual inclines of thebuccal mandibular cusps (Fig. 1, C).
4 Months After Surgery
The occlusal contacts of “The Im-mediate Progressive loading Side”were adjusted into full contact as thatfollowed in “The Immediate Func-tional Loading Side” (Fig. 1, D).
9 Months After Surgery
The dental implants received thefinal metal ceramic screw-retainedrestoration with an occlusal surface
Fig. 1. A, Occlusal view of the restorations 21⁄2 months after surgery. Note the progressive sidewith slight contact only in the central fossae of the occlusal surface. B, Occlusal view of therestorations 3 months after surgery. Note the progressive side with more contact only in thecentral fossae of the occlusal surface than 2 weeks before. C, Occlusal view of the restorations31⁄2 months after surgery. Note the central fossea and buccal inclines of the lingual cusps in fullcontact with the opposing dentition in the progressive side. D, Four months after surgery,progressive side is placed in full contact with the opposing dentition as in the functional side.
158 EFFECT OF TWO DIFFERENT IMMEDIATE LOADING PROTOCOLS • KHORSHID ET AL
designed to make full occlusal contactwith the opposing dentition.
Radiographic Follow-Up
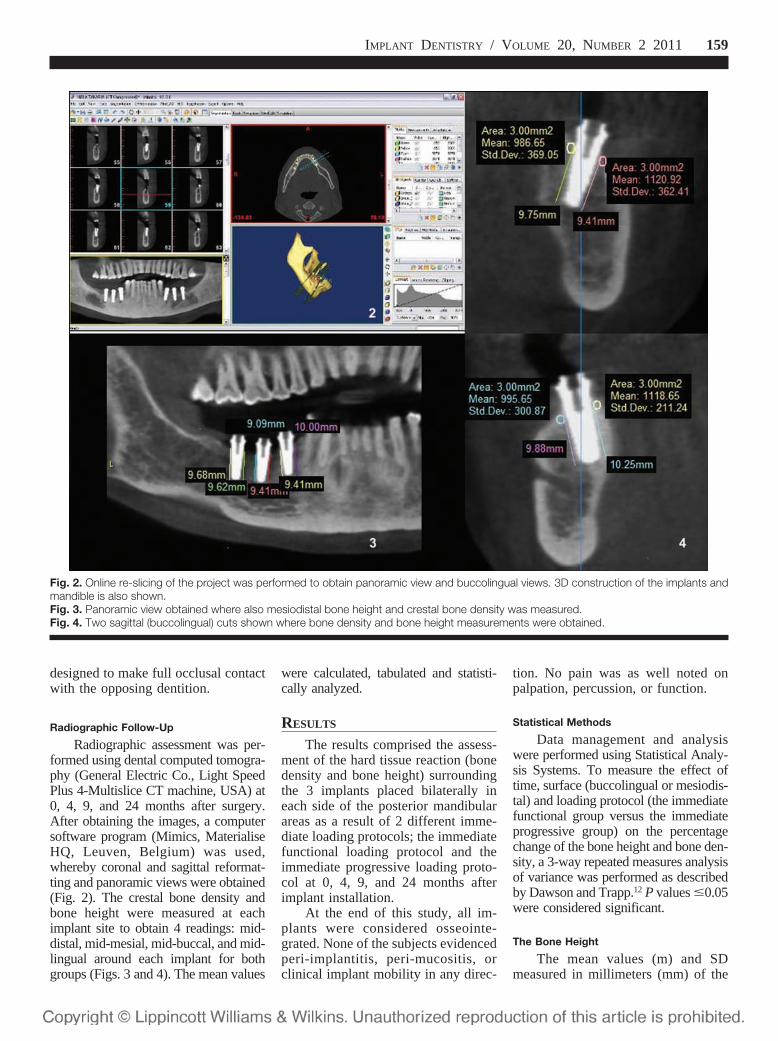
Radiographic assessment was per-formed using dental computed tomogra-phy (General Electric Co., Light SpeedPlus 4-Multislice CT machine, USA) at0, 4, 9, and 24 months after surgery.After obtaining the images, a computersoftware program (Mimics, MaterialiseHQ, Leuven, Belgium) was used,whereby coronal and sagittal reformat-ting and panoramic views were obtained(Fig. 2). The crestal bone density andbone height were measured at eachimplant site to obtain 4 readings: mid-distal, mid-mesial, mid-buccal, and mid-lingual around each implant for bothgroups (Figs. 3 and 4). The mean values
were calculated, tabulated and statisti-cally analyzed.
RESULTS
The results comprised the assess-ment of the hard tissue reaction (bonedensity and bone height) surroundingthe 3 implants placed bilaterally ineach side of the posterior mandibularareas as a result of 2 different imme-diate loading protocols; the immediatefunctional loading protocol and theimmediate progressive loading proto-col at 0, 4, 9, and 24 months afterimplant installation.
At the end of this study, all im-plants were considered osseointe-grated. None of the subjects evidencedperi-implantitis, peri-mucositis, orclinical implant mobility in any direc-
tion. No pain was as well noted onpalpation, percussion, or function.
Statistical Methods
Data management and analysiswere performed using Statistical Analy-sis Systems. To measure the effect oftime, surface (buccolingual or mesiodis-tal) and loading protocol (the immediatefunctional group versus the immediateprogressive group) on the percentagechange of the bone height and bone den-sity, a 3-way repeated measures analysisof variance was performed as describedby Dawson and Trapp.12 P values �0.05were considered significant.
The Bone Height
The mean values (m) and SDmeasured in millimeters (mm) of the
Fig. 2. Online re-slicing of the project was performed to obtain panoramic view and buccolingual views. 3D construction of the implants andmandible is also shown.Fig. 3. Panoramic view obtained where also mesiodistal bone height and crestal bone density was measured.Fig. 4. Two sagittal (buccolingual) cuts shown where bone density and bone height measurements were obtained.
IMPLANT DENTISTRY / VOLUME 20, NUMBER 2 2011 159

buccolingual and mesiodistal boneheight in the immediate functional andthe immediate progressive loadinggroup at 0, 4, 9, and 24 months areshown in Table 1 and Figure 5. Therewas a statistically significant decrease(P � 0.011) in the percentage change
of the crestal bone height of the im-mediate functional loading group thanthe immediate progressive loadinggroup in both the buccolingual andmesiodistal surfaces along the wholestudy period. There was no statisti-cally significant difference (P �
0.208) between the mesiodistal andthe buccolingual surfaces in bothgroups along the whole study period.There was, however, a statistically sig-nificant decrease (P � 0.001) in thetime period of 0 to 4 months thanthe time period of 4 to 9 months.
The Bone Density
The mean values and SD mea-sured in Hounsfield Unit of the buc-colingual and mesiodistal crestal bonedensity in the immediate functionaland the immediate progressive loadinggroups at 0, 4, 9, and 24 months areshown in Table 1 and Figure 6. Therewas a statistically significant decreasein the percentage change of bone den-sity (P � 0.009) of the immediatefunctional loading group than the im-mediate progressive loading group inboth the buccolingual and mesiodistalsurfaces along the whole study period.On the other hand, there was no sta-tistically significant difference (P �0.241) between the mesiodistal andthe buccolingual surfaces in bothgroups along the whole study period.There was, however, a statistically sig-nificant difference (P � 0.023) in thebone density percentage change in thetime period of 0 to 4 months thanthe time period of 4 to 9 months andno statistical difference (P � 0.05) inthe time period of 9 to 24 months inboth surfaces and groups as shownin Figure 6.
DISCUSSION
Analysis of the periimplant boneheight revealed a reduction in the boneheight around the implants in both theimmediate functional loading group
Fig. 5. A histogram showing the mean bone height values in both groups at both the bucco-lingual and mesiodistal surfaces at 0, 4, 9, and 24 months.
Table 1. The Mean Bone Height and Density Values and Standard Deviation Around the Implants in Both Groups
Time Side
ImmediateFunctional Bone
Height (mm)
ImmediateProgressive Bone
Height (mm)
ImmediateFunctional Bone
Density (HU)
ImmediateProgressive Bone
Density (HU)
0 months BL 11.23 � 0.62 11.36 � 0.32 1070 � 136.5 1046.2 � 84.2MD 11.47 � 0.41 11.27 � 0.55 768.8 � 66.3 766.0 � 145.0
4 months BL 10.09 � 0.43 10.28 � 0.38 971.9 � 140.2 1126.0 � 92.7MD 10.32 � 0.32 10.79 � 0.44 663.1 � 55.2 898.3 � 152.6
9 months BL 9.72 � 0.33 9.78 � 0.44 1104.4 � 181.2 1206.7 � 181.2MD 10.03 � 0.13 10.53 � 0.37 833.9 � 117.5 1029.1 � 173.2
24 months BL 8.92 � 0.43 9.12 � 0.39 1125.0 � 191.4 1336.9 � 108.7MD 9.16 � 0.22 9.75 � 0.36 792.9 � 157.8 1019.9 � 204.8
HU indicates Hounsfield unit; BL, buccolingual; MD, mesiodistal.
160 EFFECT OF TWO DIFFERENT IMMEDIATE LOADING PROTOCOLS • KHORSHID ET AL
and the immediate progressive loadinggroup. This might be attributed to thefact that the interface between the im-plants and bone begins to remodel dueto 2 main causes as reported byParfitt13; the surgical trauma and themechanical loading response pro-duced by the immediate delivery ofthe implant prosthesis leading to theinevitable crestal bone resorption.
Statistical analysis showed a morefavorable bone reaction in the imme-diate progressive loading group inboth the buccolingual and mesiodistalsurfaces along the whole study period.This was in accordance with a studyperformed by Appleton et al10 whodemonstrated that progressivelyloaded single osseointegrated implantsplaced in the posterior part of themaxilla showed less marginal bone
height loss than in the convention-ally loaded implants. Roberts et al8
also confirmed in another study thatthe decreased crestal bone lossaround the progressively loaded im-plants together with the increasedbone density are due to the responseto a stress level that stimulates bonegrowth and maturation.
The results also demonstrated thatthere was a statistically significant in-crease in the crestal periimplant boneresorption in the time period from 0 to4 months than the time period of 4 to9 months and in the time period of 4to 9 months than the time period of 9to 24 months. Roberts et al14 explainedthat the surgical process of the implantosteotomy preparation, implant inser-tion and prosthetic loading cause aregional accelerated phenomenon of
bone around the implant-bone inter-face resulting in crestal bone loss dur-ing the first 3 to 4 months. Boneremodeling from mechanical straindoes not only repair damaged bone butalso adapts to its new biomechanicalsituation thus explaining the reasonwhy the amount of bone height reduc-tion decreased in the study period of 9to 24 months. This was in accordancewith Slaets et al15 who also demon-strated that the bone offered good ad-aptation possibilities in immediatelyloaded implants rendering adequateosseointegration. Moreover, Ver-cruyssen and Quirynen16 concludedthat the amount of annual bone resorp-tion is reduced after the first year ofinitial bone remodeling.
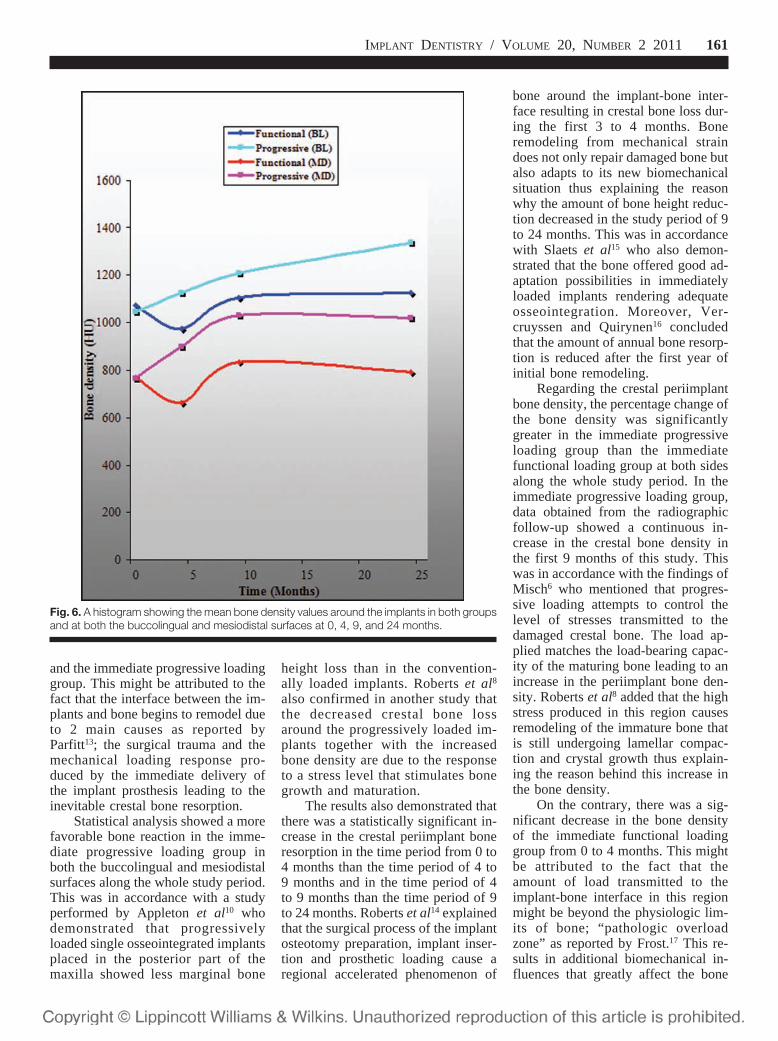
Regarding the crestal periimplantbone density, the percentage change ofthe bone density was significantlygreater in the immediate progressiveloading group than the immediatefunctional loading group at both sidesalong the whole study period. In theimmediate progressive loading group,data obtained from the radiographicfollow-up showed a continuous in-crease in the crestal bone density inthe first 9 months of this study. Thiswas in accordance with the findings ofMisch6 who mentioned that progres-sive loading attempts to control thelevel of stresses transmitted to thedamaged crestal bone. The load ap-plied matches the load-bearing capac-ity of the maturing bone leading to anincrease in the periimplant bone den-sity. Roberts et al8 added that the highstress produced in this region causesremodeling of the immature bone thatis still undergoing lamellar compac-tion and crystal growth thus explain-ing the reason behind this increase inthe bone density.
On the contrary, there was a sig-nificant decrease in the bone densityof the immediate functional loadinggroup from 0 to 4 months. This mightbe attributed to the fact that theamount of load transmitted to theimplant-bone interface in this regionmight be beyond the physiologic lim-its of bone; “pathologic overloadzone” as reported by Frost.17 This re-sults in additional biomechanical in-fluences that greatly affect the bone
Fig. 6. A histogram showing the mean bone density values around the implants in both groupsand at both the buccolingual and mesiodistal surfaces at 0, 4, 9, and 24 months.
IMPLANT DENTISTRY / VOLUME 20, NUMBER 2 2011 161

maturation as explained by Bragger etal.18 This is also in agreement with thefindings of Piattelli et al19,20 who re-ported that the increase in bone den-sity around loaded implants is abiological response to the mechanicalstress below a certain threshold,whereas loss of marginal bone anddecrease in the periimplant bone den-sity may be the result of a mechanicalstress beyond this threshold.
CONCLUSION
Immediate progressive loadingof implants yielded a more favorablebone reaction at the bone-implant in-terface than the immediate func-tional loading throughout a 2-yearstudy period as it controlled the levelof stresses transmitted to the dam-aged crestal bone thus preserved theperiimplant bone height and im-proved the periimplant crestal bonedensity. There was, however, an im-provement in bone height and den-sity over time in both groups due tothe bone accommodation.
Disclosure
The authors claim to have nofinancial interest in any company orany of the products mentioned in thisarticle.
ACKNOWLEDGMENTS
The authors thank Professor Dr.Gerald A. Niznick for his invaluablehelp and support and for supplying thedental implants used in this study (Im-plantDirect LLC, Calabasas Hills, CA).
REFERENCES
1. Misch CE. Rationale for Dental Im-plants. 3rd ed. St. Louis, MO: ElsevierMosby; 2008;1:3-25.
2. Romanos G, Toh CG, Siar CH, et al.Peri-implant bone reactions to immediatelyloaded implants. An experimental study inmonkeys. J Periodontol. 2001;72:506-511.
3. Zarb G, Schmitt A. The edentulouspredictament. I. A prospective study of theeffectiveness of implant supported fixedprostheses. J Am Dent Assoc. 1996;127:59-65.
4. Morton D, Jaffin R, Weber HP. Im-mediate restoration and loading of dentalimplants: Clinical considerations and pro-tocol. Int J Oral Maxillofac Implants. 2004;19(suppl):103-108.
5. Wang H, Ormianer Z, Palti A, et al.Consensus conference on immediateloading: The single tooth and partial eden-tulous area. Implant Dent. 2006;15:324-333.
6. Misch CE. Progressive bone load-ing. St Louis, MO: Elsevier Mosby; 2005;26:511-530.
7. Misch CE, Scortecci GM. Immedi-ate Load and Restoration in ImplantDentistry: Rationale and Treatment. 3rded. St Louis, MO: Elsevier Mosby; 2008;35:799-838.
8. Roberts WE, Smith RK, Zilberman Y,et al. Osseous adaptation to continuousloading of rigid endosseous implants.Am J Orthod. 1984;86:95-111.
9. Rotter BE, Blackwell R, Dalton G.Testing progressive loading of endostealimplants with the Periotest: A pilot study.Implant Dent. 1996;5:28-32.
10. Appleton RS, Nummikoski PV,Pigno MA, et al. A radiographic assess-ment of progressive loading on bonearound single osseointegrated implants inthe posterior maxilla. Clin Oral ImplantsRes. 2005;16:161-167.
11. O’Sullivan D, Sennerby L, MeredithN. Measurements comparing the initial sta-
bility of five designs of dental implants: Ahuman cadaver study. Clin Implant DentRelat Res. 2000;2:85-92.
12. Dawson B, Trapp GT. Basic andClinical Biostatistics. 3rd ed. Lange Medi-cal Book. Norwalk, CT: Appleton & Lange;2001.
13. Parfitt AM. The physiological andclinical significance of bone histomor-phometric data. In: Reck RR, ed. BoneHistomorphometry, Techniques and In-terpretation. Boca Raton, FL: CRCPress; 1983:143-223.
14. Roberts WE, Turley PK, BrezniakN, et al. Implants: Bone physiology andmetabolism. J Calif Dent Assoc. 1987;15:54-61.
15. Slaets E, Naert I, Carmeliet G, et al.Early cortical bone healing around loadedtitanium implants: A histological study inthe rabbit. Clin Oral Implants Res. 2009;20:126-134.
16. Vercruyssen M, Quirynen M. Long-term, retrospective evaluation (implant andpatient-centered outcome) of the two-implants-supported overdenture in themandible. Part 2: Marginal bone loss. ClinOral Impl Res. 2010;21:466-472.
17. Frost HM. A 2003 update of bonephysiology and Wolff’s Law for clinicians.Angle Orthod. 2004;74:3-15.
18. Bragger U, Burgin W, Lang NP, etal. Digital subtraction radiography for theassessment of changes in the peri-implantbone density. Int J Oral Maxillofac Im-plants. 1991;6:160-166.
19. Piattelli A, Corigliano M, Scarano A,et al. Immediate loading of titaniumplasma-sprayed implants: An histologicanalysis in monkeys. J Periodontol. 1998;69:321-327.
20. Piattelli A, Corigliano M, ScaranoA, et al. Bone reactions to early occlusalloading of two-stage titanium plasma-sprayed implants: A pilot study in mon-keys. Int J Periodontics Restorative Dent.1997;17:162-169.
162 EFFECT OF TWO DIFFERENT IMMEDIATE LOADING PROTOCOLS • KHORSHID ET AL

Abstract Translations
GERMAN / DEUTSCHAUTOR(EN): Heba E. Khorshid, BDS, MS, Hamdy AboulFotouh Hamed, BDS, MS, PhD, Essam A. Aziz, BDS, MS,PhDAuswirkung zweier unterschiedlicher Protokolle mit unmittel-barer Belastung bei Implantatgestutzten und Schraubenge-haltenen Prothesen
ZUSAMMENFASSUNG: Hintergrund: Die vorliegendeArbeit zielte darauf ab, die Veranderungen zu beurteilen, diebei den stutzenden Strukturen von bilateral in den hinterenUnterkiefer eingepflanzten Implantaten auftreten, und diesals Ergebnis zweier unterschiedlicher Protokolle zur unmit-telbaren Belastung: das Protokoll der unmittelbaren funktio-nellen Belastung und das Protokoll der unmittelbarenprogressiven Belastung. Materialien und Methoden: Beifunf Patienten mit unveranderter Kennedy-Klasse I im Un-terkiefer wurden dreißig Implantate eingepflanzt. Bei jedemPatienten wurden drei Implantate auf jeder Seite des Zahn-bogens an der pramolaren/molaren Unterkieferregion eingep-flanzt. Auf der einen Seite wurden die Implantate unmittelbargemaß dem Protokoll zur unmittelbaren funktionellen Belas-tung belastet, wahrend die Implantate auf der anderen Seitegemaß Protokoll zur unmittelbaren progressiven Belastungbelastet wurden. Uber zahntechnischen CT wurde eine ront-genologische Bewertung nach 0, 4, 9, sowie 24 Monaten nachdem Implantierungseingriff durchgefuhrt. Ergebnisse: Diestatistische Analyse wies bei Vergleich der Gruppe mit un-mittelbarer progressiver Belastung mit der Gruppe mitunmittelbarer funktionaler Belastung eine bessere Kno-chengewebsreaktion bei einer statistisch bedeutsamen Differ-enz in der krestalen Knochendicht im das Implantatumlagernden Gewebe (P � 0.009) fur die Belastungsgruppemit progressiver Belastung auf. Schlussfolgerung: Das Pro-tokoll mit sofortiger progressiver Belastung erzielt einebesser vorhersagbare Knochengewebsreaktion im das Im-plantat umgebenden krestalen Knochen und stellt einebessere Implantatprognose sicher als das Protokoll mit un-mittelbarer funktionaler Belastung. Es wird die These unter-stutzt, dass eine allmahliche Belastung oder Stimulation denKnochen reifen lasst und in einer uber zwei Jahre laufendenNachfolgezeit ein dichteres Knochenwachstum fordert.
SCHLUSSELWORTER: Unmittelbare Belastung, progres-sive Belastung, funktionale Belastung, Knochengewebsdi-chte, Computertomografie
SPANISH / ESPAÑOLAUTOR(ES): Heba E. Khorshid, BDS, MS, Hamdy AboulFotouh Hamed, BDS, MS, PhD, Essam A. Aziz, BDS, MS, PhD
El efecto de dos protocolos diferentes de carga inmediata enprotesis retenidas con tornillos y apoyadas en implantes
ABSTRACTO: Antecedentes: El objetivo de este trabajo fueevaluar los cambios que ocurren en las estructuras de apoyode implantes colocados bilateralmente en la region mandib-ular posterior como resultado de dos protocolos distintos decarga inmediata: El protocolo de carga funcional inmediata yel protocolo de carga progresiva inmediata. Materiales ymetodos: Se colocaron treinta implantes en cinco pacientescon una mandíbula sin modificacion Kennedy Clase I. Encada paciente, se colocaron tres implantes en cada costado delarco dental del paciente en la region mandibular molar/premolar. En un costado, los implantes se cargaron inmedia-tamente usando un protocolo de carga funcional inmediatamientras que en el otro costado se cargaron usando un pro-tocolo de carga progresiva inmediata. La evaluacion ra-diografica se realizo usando una tomografía computadadental en intervalos de 0, 4, 9, y 24 meses luego de lacolocacion quirurgica de los implantes. Resultados: El anali-sis estadístico demostro una reaccion mas favorable del huesocon una diferencia estadísticamente significativa en la alturadel hueso crestal (P � 0.011) así como en la densidad delhueso crestal periimplante (P � 0.009) en el grupo de cargaprogresiva inmediata que en el grupo de carga funcionalinmediata. Conclusion: El protocolo de carga progresivainmediata produce una reaccion mas predecible del hueso enel hueso crestal periimplante y asegura una mejor prognosisdel implante que el protocolo de carga funcional inmediata; loque apoya la idea de que una carga o estimulacion gradualpermitira que el hueso madure y adquiera mayor densidad enel período de dos anos de seguimiento del implante.
PALABRAS CLAVES: Carga inmediata, carga progresiva,carga funciona, densidad del hueso, tomografía computada
PORTUGUESE / PORTUGUÊSAUTOR(ES): Heba E. Khorshid, Bacharel em Cirurgia Den-taria, Mestre em Ciencia, Hamdy Aboul Fotouh Hamed,Bacharel em Cirurgia Dentaria, Mestre em Ciencia, PhD,Essam A. Aziz, Bacharel em Cirurgia Dentaria, Mestre emCiencia, PhDO Efeito de Dois Diferentes Protocolos de CarregamentoImediato em Proteses Retidas por Parafuso e Suportadaspor Implante
RESUMO: Antecedentes: O objetivo deste trabalho era aval-iar as alteracoes que ocorrem nas estruturas de suporte deimplantes colocados bilateralmente na regiao mandibularposterior como resultado de dois diferentes Protocolos deCarregamento Imediato: o Protocolo de Carregamento Fun-
IMPLANT DENTISTRY / VOLUME 20, NUMBER 2 2011 163
cional Imediato e o Protocolo de Carregamento ProgressivoImediato. Materiais e Metodos: Trinta implantes foram co-locados em cinco pacientes com Kennedy Class I mandibularnao modificada. Para cada paciente, tres implantes foramcolocados em cada lado da arcada dentaria do paciente naregiao mandibular pre-molar/molar. De um lado, os implantesforam carregados imediatamente em seguida a um Protocolode Carregamento Funcional Imediato, enquanto o outro ladofoi carregado em seguida a um Protocolo de CarregamentoProgressivo Imediato. Foi realizada avaliacao radiograficausando tomografia computadorizada dentaria a intervalos de0, 4, 9, e 24 meses apos a cirurgia de implante. Resultados:A analise estatística mostrou uma reacao ossea mais fa-voravel, com uma diferenca estatisticamente significativa naaltura da crista ossea (P � 0.011), bem como na densidade doosso de peri-implante da crista (P � 0.009) no grupo decarregamento progressivo imediato do que no grupo de car-regamento funcional imediato. Conclusao: O protocolo decarregamento progressivo imediato produz uma reacao osseamais previsível no osso da crista de peri-implante e garantemelhor prognostico de implante do que o protocolo de car-regamento funcional imediato, apoiando a ideia de que ocarregamento ou estímulo gradual permitira que o osso ama-dureca e cresca mais denso em um período de acompanha-mento de implante de dois anos.
PALAVRAS-CHAVE: carregamento imediato, carregamentoprogressivo, carregamento funcional, densidade do osso, to-mografia computadorizada
RUSSIAN /������: Heba E. Khorshid, �������� ������� ��� ����������, ��� �� � �� ������� ���, HamdyAboul Fotouh Hamed, �������� ������� ��� ����������, ��� �� � �� ������� ���, ���������� ����, Essam A. Aziz, �������� ������� ��� ����������, ��� �� � �� ������� ���, ���������� ��������� �� �������� ���� �������� ��������� ��������� ������� � ������ �������� ����� ��� � � ���� � �� ������
�!"#$!. %������������� ����. ����������� ������ ���� ������ ���������, ����������� ����� � ������� ������� �����������, ����������� ����� ����� � ������ ���� �������� ���� ��, � ��������� � ����������� ������������ ���������� ����������� ��������:��������� ������������� ������������������� � ��������� ����� ���������������� ��������. $�������� � ������.���� ��������� ���� ��������� ������������������� (������������������ ��� I ��������� �� ������ ���� ��). ������ ����������� ��������� �� ��� ���������� ������
������ ����� �� � ���� �� ���������/������������ ���� ��. ����� ������ ���������� �������������� ������� ��� �� ��������������������� ����������� ��������, � ���� ������ �������� ��������� � ��� ���������� ����� ����� �������������������. ��������� � ������������� ��������� ����!�� ����� ��������� ����������� 0, 4, 9 � 24 �� ��� �� �� �������� �������������. ����������. ���� ���� ��� ������������� ����� ����������� �� ��� ������� � ���� ���� �� �������� ��������� � �� ��������������� ����� (p � 0,011), � ����� ������� �� ������������ ���������������� �� ��(p � 0,009) � ���� ����� ����� �������������������� �� �������� ����� ������������� ����������� ���������.�����. �������� ����� ����� ������������������� ��� �������� ����� ������������� ��� ������� � ���������������������������� ����� � ���� ����� ������������������ ���� ������� ����������, ��� ��������������������� ����������� ��������, ��������������� ������������� � ���, ����� �������� �������� ��� �������� ���������� �� ������ � �������� � �� ������������������� ������� �� ����!�� ���������� �������������.
&'#(!��! )'���: ����������� ��������,����� ����� ��������, ���������������������, ������ �� �� ��, ���������������������
TURKISH / TURKCEYAZARLAR: Heba E. Khorshid, BDS, MS, Hamdy AboulFotouh Hamed, BDS, MS, PhD, Essam A. Aziz, BDS, MS,PhDImplantla Desteklenen ve Vida ile Baglanan Protezlerde IkiFarklı Hemen Yukleme Protokolunun Etkisi
OZET: Bilgi: Bu calısmanın amacı, iki farklı Hemen Yukl-eme Protokolu ile posterior alt cenenin iki tarafındayerlestirilen implantların destek yapılarında olusandegisiklikleri degerlendirmekti. Calısmada, Hemen Fonksiy-onel Yukleme Protokolu ile Hemen Progresif Yukleme Pro-tokolu degerlendirildi. Gerec ve Yontem: Degistirilmemismandibuler Kennedy Sınıf I olan 5 hastada toplam 30 implantyerlestirildi. Her bir hastada, hastanın dis arkının premolar/molar alt cene bolgesinin her bir tarafına ucer implantyuklendi. Bir tarafta implantlar Hemen Fonksiyonel YuklemeProtokolu ile yerlestirilirken diger tarafta Hemen ProgresifYukleme Protokolu kullanıldı. Bilgisayarlı dental tomografiile implant cerrahisinden 0, 4, 9, ve 24 ay sonra radyografikdegerlendirmeler gerceklestirildi. Bulgular: Istatistiksel
164 EFFECT OF TWO DIFFERENT IMMEDIATE LOADING PROTOCOLS • KHORSHID ET AL

analizlere gore hemen progresif yukleme grubu, hemenfonksiyonel yukleme grubuna nazaran daha olumlu kemikreaksiyonu vererek, kret kemik yuksekliginde (P � 0.011) vekret peri-implant kemik yogunlugunda (P � 0.009) istatis-tiksel acıdan anlamlı bir farklılık gosterdi. Sonuc: Hemenprogresif yukleme protokolu, peri-implant kret kemigindedaha onceden tahmin edilebilir bir kemik reaksiyonuolusturdugu gibi, hemen fonksiyonel yukleme protokolune
nazaran daha olumlu implant prognozu da saglar. Bu da,progresif yukleme veya uyarının iki yıllık implant takip done-minde kemigin olgunlasmasına ve yogunlasmasına olanaksagladıgı dusuncesini desteklemektedir.
ANAHTAR KELIMELER: hemen yukleme, progresif yukl-eme, fonksiyonel yukleme, kemik yogunlugu, bilgisayarlıtomografi
JAPANESE /
IMPLANT DENTISTRY / VOLUME 20, NUMBER 2 2011 165

CHINESE /
KOREAN /
166 EFFECT OF TWO DIFFERENT IMMEDIATE LOADING PROTOCOLS • KHORSHID ET AL