the current state of covid litigation
TRANSCRIPT

1
The Current State of COVID Litigation
1
Nichole L. HairHall Booth Smith, PC
Peter CridlandTrans RE
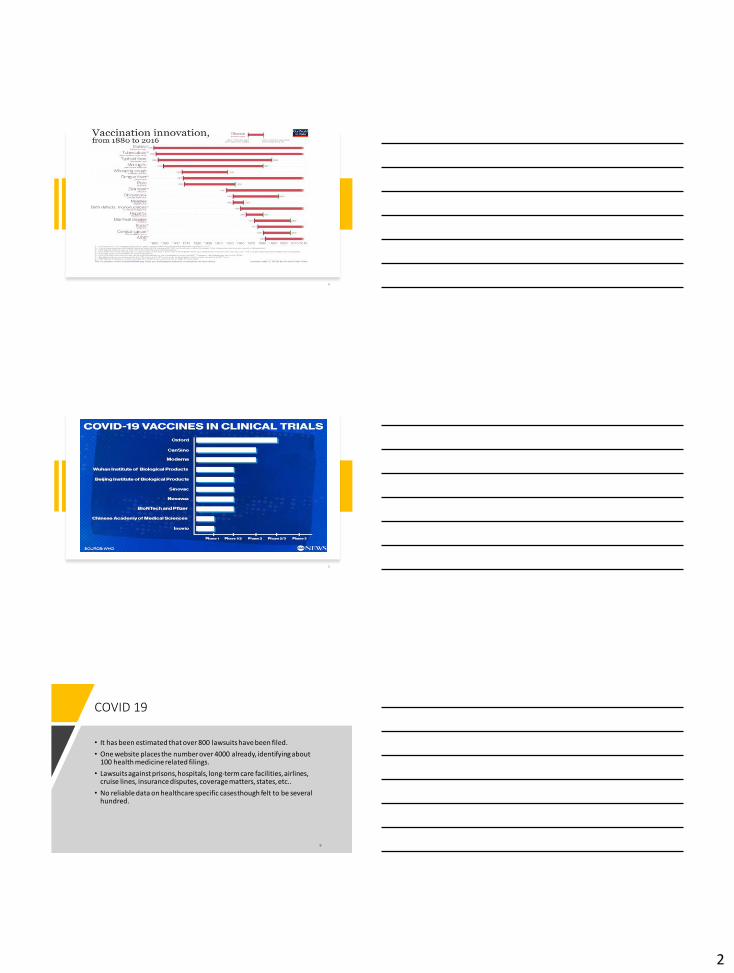
COVID 19
• Global cases: Around 31 million
• Global deaths: More than 962,000
• United States cases: Around 6.8 million
• United States deaths: Approximately 200,000
• The data above was compiled by Johns Hopkins University as of 2:30 p.m. on September 21, 2020
3
2
4
5
COVID 19
• It has been estimated that over 800 lawsuits have been filed.
• One website places the number over 4000 already, identifying about 100 health medicine related filings.
• Lawsuits against prisons, hospitals, long-term care facilities, airlines, cruise lines, insurance disputes, coverage matters, states, etc..
• No reliable data on healthcare specific cases though felt to be several hundred.

3
Progression of Claims
1. LTC Facilities – NOW
2. Outrageous facts in provider or hospital care - NOW
3. General claims against providers – 1-2 years from NOW.
7
DISCUSSION OF PREP ACT AND STATE IMMUNITY ORDERS
WHAT IS THE PREP ACT? WHAT IMMUNITY DOES IT PROVIDE?
WHAT ARE THE IMPLICATIONS FOR PROVIDERS IN HOSPITALS?
LTC? OUTPATIENT? HOME HEALTH?
WHICH STATES HAVE IMMUNITY ORDERS?
WHAT IMMUNITY ORDERS ARE IN-PROCESS, BUT NOT PASSED?
WHAT CAN WE EXPECT TO SEE IN LITIGATION?
8
Should Seek Removal to Federal Court
• One case so far. Maglioli remanded to state court
• Judge (Schummer brother in law very liberal)
• Remand grounds relied on federal officer
• Believe complete preemption is better route
• Not binding/will have multiple rulings soon

4
Congressional Research Service
• The PREP Act and COVID-19: Limiting Liability for Medical Countermeasures Updated July 20, 2020
• Courts have characterized PREP Act immunity as “sweeping.” It applies to all types of legal claims under state and federal law.
Federal Immunity: The PREP Act
The Public Readiness Emergency Preparedness (PREP) Act was enacted in 2005 by Congress. The PREP Act authorizes the Secretary of the US Department of Health and Human Services to issue a PREP Act declaration in response to a public health emergency.
The PREP Act authorizes the Secretary of Health and Human Services (HHS) to declare that certain “covered persons” are immune from liability (i.e., loss sounding in tort or contract) for taking certain “covered countermeasures” that are necessary to combat a public-health emergency such as COVID-19.
On March 10, 2020, Secretary of HHS Alex Azar issued such a declaration, effective February 4, 2020 (“Declaration”)
12

5
The PREP Act Declaration: Scope of Immunity
• Immunity includes:
• Any claim, under federal or state law, for loss that has a causal relationship with the administration to or use by an individual covered by a countermeasure.
• A loss is defined to include: death, personal injury, emotional injury, property damage, business interruption and fear of personal injury.
• The protection is very broad and applies “without regard to the date of the occurrence, presentation or discovery of the loss.” With few exceptions.
• Immunity from liability under the PREP Act is not available for death or serious physical injury caused by willful misconduct.
13
The PREP Act Declaration: Covered Persons
• Declaration provides immunity for "covered persons" who include:
• Program planners (individuals and entities involved in planning, administering, or supervising programs for distribution of a countermeasure)
• Qualified persons
• Defined as licensed health care professionals or other individuals authorized to prescribe, administer, or dispense covered countermeasures under the law of the state in which the covered countermeasure is prescribed.
• Officials, agents and employees of any of these entities or persons
14
The PREP Act Declaration: Recommended Activities
• "Recommended Activities" are to prescribe, administer, deliver, distribute, or dispense the Covered Countermeasures following a Declaration of an emergency.
• "Administration" is :
• “physical provision of the countermeasures to recipients, or activities and decisions directly relating to public and private delivery, distribution, and dispensing of the countermeasures to recipients; management and operation of countermeasure programs; or management and operation of locations for purposes of distributing and dispensing countermeasures. “
15

6
The PREP Act Declaration: Continuing Guidance
• On April 3, 2020, the FDA issued Emergency Use Authorizations, under the PREP Act, for:
• Non-NIOSH-approved KN95 respirators made in China
• Hydroxychloroquine in the use for treatment of COVID-19.
• On April 8, 2020, HHS issued guidance extending federal immunity under the PREP Act to licensed pharmacists administering approved COVID-19 testing.
• On April 14, 2020, HHS General Counsel issued an advisory opinion setting forth its view that federal immunity under the PREP Act may apply to certain persons employing certain countermeasures in the fight against COVID-19, even though they are technically not covered by the PREP Act, if one could have reasonably believed the persons or countermeasures were covered.
16
Additional Federal Protections and Regulatory Waivers
• The VPA establishes that volunteer healthcare professionals of non-profit organizations or governmental entities are not liable for economic damages stemming from medical care provided within the scope of their volunteer responsibilities.
Volunteer Protection Act of 1997 (VPA)
• On March 17, 2020, the United States Secretary of Health and Human Services, Alex Azar, issued a limited waiver of certain HIPAA sanctions for healthcare providers to improve data sharing and expand telehealth patient care during the pandemic.
• HHS did not waive or extend the 60-day time limit for medical providers to notify affected patients of a breach of their protected health information.
Limited Waiver of HIPAA to Expand Telehealth
17
18
Update on State Immunities

7
States with Immunity Executive
Orders
19
20
Overview of Senate Relief Bill Immunity Provisions
SAFE TO WORK ACT(Proposed)
WHERE IT STANDS:
• In Committee (Senate – Judiciary)
• Negotiations are currently stalled over funding
• Mitch McConnell was the Original Sponsor
• Now 18 Co-Sponsors (All Republicans)
TWO TYPES OF IMMUNITY:
• For businesses (if in interstate commerce)• Covers Alleged Exposure to COVID-19
• For health care providers• Covers healthcare liability claims
21

8
SAFE TO WORK ACT(Proposed)
Immunity for Businesses:
• Creates an Exclusive Federal Cause of Action (“Coronavirus Exposure Action”)
• Plaintiff Must Prove:• Failure to make Reasonable Efforts to Comply with
Applicable Standards/Guidance;
• Gross Negligence or Willful Misconduct;
• Actual Exposure to COVID-19; and
• Causation and Personal Injury.
• Covers Businesses Engaged in Interstate Commerce (or Otherwise Subject to Federal Regulation under the Spending Clause)
22
SAFE TO WORK ACT(Proposed)
Immunity for Health Care Providers:
• Creates an Exclusive Federal Cause of Action (“Coronavirus-Related Medical Liability Action”)
• Plaintiff must prove:• Gross Negligence or Willful Misconduct;
• Direct Causation; and
• Personal Injury.
• Covers any HCP engaged in “Coronavirus-Related Health Care Services”:• Diagnosis, prevention, assessment of COVID-19; or
• Care of any individual during the federal emergency, if the care is impacted by COVID-19
• “HCP” Includes SNF, but Unclear if it Includes AL
23
SAFE TO WORK ACT(Proposed)
Common Features of Both Actions:
• Burden of Proof is “Clear and Convincing Evidence”
• Removable at Will by Any Defendant
• 1 Year Statute of Limitations;
• Heightened Pleading Requirements;
• Limited Discovery until Defendants have a Chance to Dismiss;
• No Non-Economic Damages Allowed (unless willful);
• Punitive Damages are Capped (1x Compensatory)
• Enhanced Appellate Rights; and
• No Joint & Several Liability (unless intent/fraud).
24

9
Anticipated Claims
• The plaintiffs’ bar will attempt to circumscribe the scope of the immunity provided by targeting their efforts on alleged claims of malpractice in the treatment of COVID-19 and non-COVID-19 patients in hospitals.
• Although the statutory immunity is not limited to COVID-19 patients, there must be a connection to the COVID-19 crisis for the immunity to be applied to the alleged injury of a non-COVID-19 patient. It is in this grey area where the legal battle will be fought.
25
Anticipated Claims
• We expect to experience a range of claims, such as:
• Failure to diagnose COVID-19.
• Delay or denial of deemed “elective” or “non-essential” care to patients that is later asserted to be critical in the course of treatment.
• Alleged negligence whereby patients and family members are infected with COVID-19 by “community spread” in a clinic or office setting.
• Alleged negligent mistreatment of COVID-19 (e.g., overutilization of ventilators in patient protocols).
• Delay or denial of care due to lack of facility capacity (e.g., bed shortages) or access to medical equipment (ventilators, PPE etc.) caused by patient overload.
• Asserted negligence in “community spread” of COVID-19 in sensitive areas, such as ICU, cardiology, surgery, oncology, etc.
26
Ongoing Litigation Non-CovidClaims
• Current cases – including those not related to Covid-19 – will be affected by the pandemic.
• Court closures by State, District
• Convening juries during a pandemic
• Flagler holds state’s first in-person jury trial since coronavirus while Orange business court goes remote
• By MONIVETTE CORDEIRO
• ORLANDO SENTINEL |/AUG 31, 2020 AT 1:02 PM
• Aiken County holds first jury trial since onset of coronavirus pandemic
• By Matthew Enfinger [email protected]/Aug 25, 2020
• First Brooklyn trial since COVID-19 pandemic starts without jury, delayed so defendant could get a mask
• By ANNA CHOI and NOAH GOLDBERG
• NEW YORK DAILY NEWS |/JUL 29, 2020 AT 6:55 PM
27

10
COVID –issues relating to Risk Management
• Coordinate creating a timeline. Incorporate all the waivers and changes by CMS, FDA, OIG (re: HIPAA, EMTALA), so that the healthcare entities’ responses are documented in the same timeline that these waivers came about in your repository of information. Document your actions now!
• Review the FDA temporary policy (“loosened rule”) on compounding pharmacies. The drugs addressed are mostly IV drugs and many are high risk and assist in guidelines development. https://www.fda.gov/media/137031/download
• Consolidate maintenance of Tracked staffing allocation, PPE supplies, and ventilators through your hospitals and assure that those records are maintained for the years of litigation to come in your repository of information.
28
COVID –issues relating to Risk Management
• Determine witnesses that can authenticate these documents and the need to be identified and prepare for their part in upcoming litigation.
• Work with department heads and experts within your hospital to document the “day in the life” of a health care worker in all units of a hospital during the COVID-19 emergency.
• Spearhead a team to document all infectious disease safety measures implemented and track to your repository of information
• Foster experts to study the medicine related to COVID-19 and chronicle the standard of care so they can provide affidavits regarding its impact on the treatment of non-COVID-19 patients to support summary judgment motions and testimony at the time of trial.
29
COVID –issues relating to Risk Management
• Intercept the anticipated claim of physicians practicing out of specialty, and treatment decisions due to shortness of staff & resources.
• If possible, work with managers to encourage training to address documentation with language which is contemporaneous during the period of the COVID-19 crisis to help give context in the future of what treatment was being provided even if it was not COVID-19 treatment.
• Again, flip the model; you assume the burden of proof and demonstrate the positive steps you have taken in your healthcare system to meet a crisis standard of care.
• Consider modifying your consent forms during this crisis to provide sample language
• Proactively prepare for the “The Reptile Strategy”
30

11
Uniform Chart Language
• General documentation to be in every chart• Please note that this care is given at a time of national
public health emergency due to the pandemic caused by COVID-19 (Novel Coronavirus). As a result, It is acknowledged and understood that the spread of COVID-19 within our communities places an incomprehensible strain on our providers, hospital systems and the resources, equipment, beds, treatment options, and services available in support of patient care.
• It is further acknowledged and understood that the Hospital and provider, during the COVID-19 pandemic, endeavor to remain operational and provide care to all patients commensurable with the resources available to the Hospital existing at that time. Further, it is acknowledged that the transmittable risks, treatment process and diagnosis are novel without well-defined guidelines.
• It is further acknowledged due to the novel and emergency nature of this pandemic, treatment is provided utilizing the best judgment and currently known practices, within the limitation of resources.”
31
COVID –issues relating to Risk Management
• Reach out to other hospitals in your area, through your counsel, to ascertain their efforts to set down their journey creating experts that can be shared by way of affidavits to support summary judgments or eventual trial testimony outside your respective hospital.
• Coordinate contacting your marketing department and capture video footage or photos of departments built to respond to COVID-19, Emergency Departments built, and all safety measures taken to respond for social distancing. Provide attorney-client protection, and in anticipation of litigation.
32
COVID –issues relating to Risk Management
• Identify experts in specialties based on current experiences and have them ready on COVID cases.
• Maintain a legal medical data base
• Maintain a current social media to help recreate this “reality”
• Maintain a current and ongoing medical research into area and challenges such as staffing and end of life decisions
33

12
COVID – Hospital Checklist
• The following is a checklist of items you may consider maintaining if and when the Hospital is asked at a later date for documentation related to services provided during the COVID-19 pandemic. The form that each piece of information is maintained will depend on the hospital’s current document management processes and the extent of readily available electronic storage. Regardless of the format, the hospital should consider maintaining the documentation in an easily accessible format for no less than ten (10) years.
34
COVID –issues relating to Risk Management
With the PREP Act and state executive orders and immunities, there is a new range of defenses that should be raised on any COVID related cases, including claims tangentially associated with COVID.
This can more economically be done by A PRE-DRAFTED MOTIONS AND RESEARCH and distributed to your panel counsel, with
oversight if needed on prosecuting the same.
35
COVID –issues relating to Risk Management
We are developing a Uniform Strategy approach to be proactive in these areas. In considering this approach, we can forecast effective implementation of methods and strategies related to:
1. consistent discovery responses
2. deposition answers
3. spoliation arguments4. arguments made on motions for summary judgment
36

13
COVID –issues relating to Risk Management
• The concept of crisis standards of care should be pursued, developed, and prepared for summary judgments
37
COVID –issues relating to Risk Management
• Draft uniform defenses to be filed with answers and considered in evaluation along with removal motions (where applicable)
• Draft standard removal practice
• Draft (Prepare) Federal and State Immunity motions to dismiss or application of applicable standard motions
• Draft discovery that would ferret out COVID defenses
• Draft current notice provisions that can be placed in current charts to preserve the awareness of the “COVID reality”
38
COVID –issues relating to Risk Management
• Plan for the Correct 30(b)(6) Witness: We can foresee that your hospital will eventually have to produce a witness to testify about information known or reasonably available to the organization with respect to your COVID-19 response.
• We recommend you seize the opportunity to identify that witness and start to prepare the witness based on all the information developed in your Global COVID-19 Defense Strategy Road Map.
• This will afford your healthcare system a plausible and consistent message down the road in litigation, and to aggressively jump start your defense plans.
39

14
https://data.cms.gov/stories/s/COVID-19-Nursing-Home-Data/bkwz-xpvg
CMS Covid-19 Response:Increase Nursing Home Transparency
41
Litigation Trends: Survey of Plaintiff Attorney Advertising for COVID cases
North Carolina
42

15
Texas
43
Conclusion
Questions & Answers and responses.
44