the concept of diabetes & cv risk: a lifetime risk challenge diabetes & cv risk: routine...
TRANSCRIPT
The concept of Diabetes & CV risk:A lifetime risk challenge
Diabetes & CV Risk:
Routine practice versus guidelines
Eberhard Standl, MDProfessor of MedicineMunich Diabetes Research Group/Diabetes Research Institute.MDMunich, Germany
Cardio Diabetes Master ClassEuropean chapterMunich, GermanyMay 6-8, 2011
Slide lecture prepared and held by:
Presentation topic
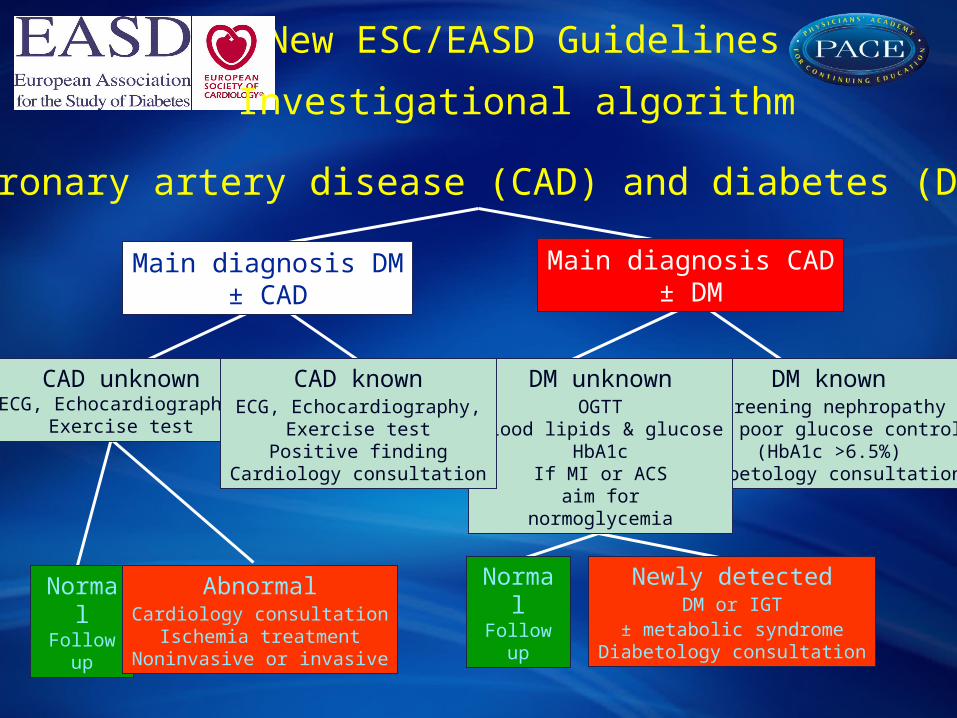
Coronary artery disease (CAD) and diabetes (DM)
Main diagnosis DM± CAD
Main diagnosis CAD± DM
CAD unknownECG, Echocardiography,
Exercise test
DM knownScreening nephropathy If poor glucose control
(HbA1c >6.5%)Diabetology consultation
DM unknownOGTT
Blood lipids & glucoseHbA1c
If MI or ACSaim for
normoglycemia
CAD knownECG, Echocardiography,
Exercise testPositive finding
Cardiology consultation
NormalFollow up
AbnormalCardiology consultation
Ischemia treatmentNoninvasive or invasive
Newly detectedDM or IGT
± metabolic syndromeDiabetology consultation
NormalFollow up
New ESC/EASD Guidelines
Investigational algorithm

Ten important recommendations (1)
To reach (all) treatment targets including those for glycaemic control
To screen for DM and IGT by means of an OGTT in all patients with coronary artery disease and in other high risk individuals
To let life style counselling be the cornerstone in preventing DM and CVD
To offer patients with DM and ACS standard guideline based treatment, early angiography and mechanical revascularisation
To apply strict, when needed insulin based, glucose control in acutely ill DM patients

Ten important recommendations (2)
To favour CABG over PCI when revascularising DM patients
To use drug-eluting stents in PCI with stent implantation
To include investigations for cardiac autonomic dysfunction, heart failure, arrhythmias, hypotension, PVD (Doppler-Index), eGFR and
(micro) - albuminuria
To use a multifactorial (tight glucose, BP and lipid-control and antiplatelet therapy) approach
To establish a collaboration between cardiologists and diabetologists

110 from 25 countries
n= 4 961
2- 6 weeks per centreFebruary 2003 to January 2004
Euro Heart Survey Diabetes and the HeartParticipating centres
Type of centre:
47% hospital cardiology wards
45% hospital based outpatient clinics
8% outpatient clinics

Prescribed glucose
lowering drugs
77 (17%) 1% 16%
<1%83%
InsulinOral drugsCombinationsNo prescription
Newly detected diabetesn = 452
Not prescribedglucose
lowering drugs
375 (83%)
(Anselmino et al Eur Heart J 2008;29:177)
Glycemic controlExperiences from the Euro Heart SurveyGlucose lowering drugs at follow up in patients with newly detected diabetes
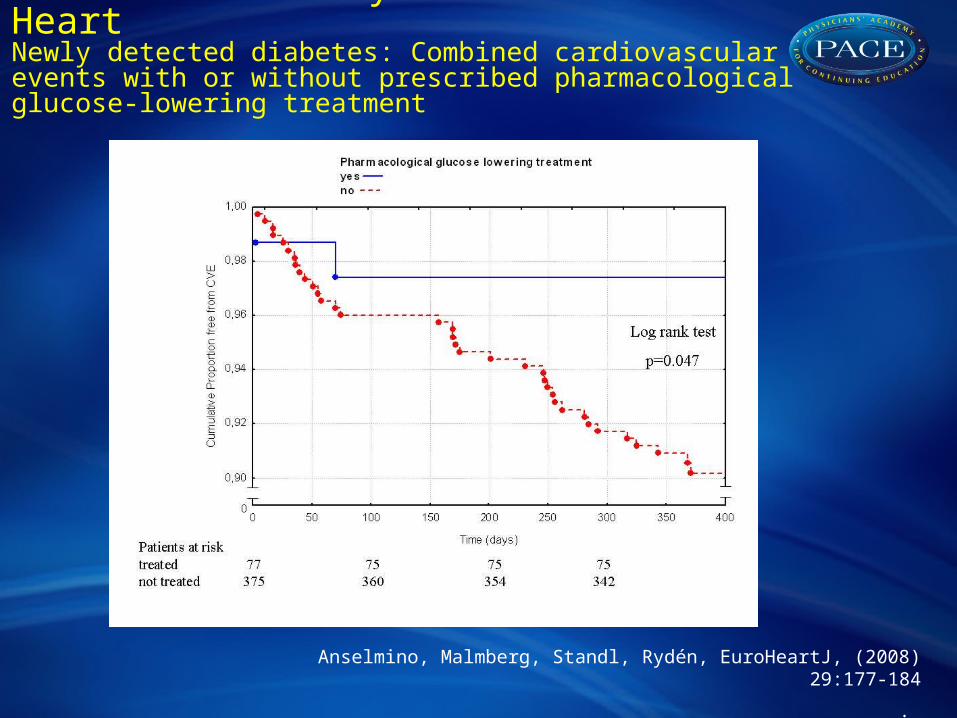
Euro Heart Survey Diabetes and the HeartNewly detected diabetes: Combined cardiovascular events with or without prescribed pharmacological glucose-lowering treatment
Anselmino, Malmberg, Standl, Rydén, EuroHeartJ, (2008) 29:177-184
.

NGT IFG IGT DM
Acuteadmission
n=923
389
(42%)
39
(4%)
294
(32%)
201
(22%)
Electiveconsultation
n=997
486
(49%)
50
(5%)
320
(32%)
141
(14%)
OGTT (0 min) <6.1 6.1 and <7.0 <7.0 7.0
OGTT (2 h) <7.8 <7.8 7.8 and <11.1 or 11.1
Patients with coronary artery disease (CAD) and no diabetes (OGTT cohort n=1920)
Euro Heart Survey Diabetes and theHeart OGTT outcome
Bartnik M et al. Eur Heart J 2004;25:1880–1890.
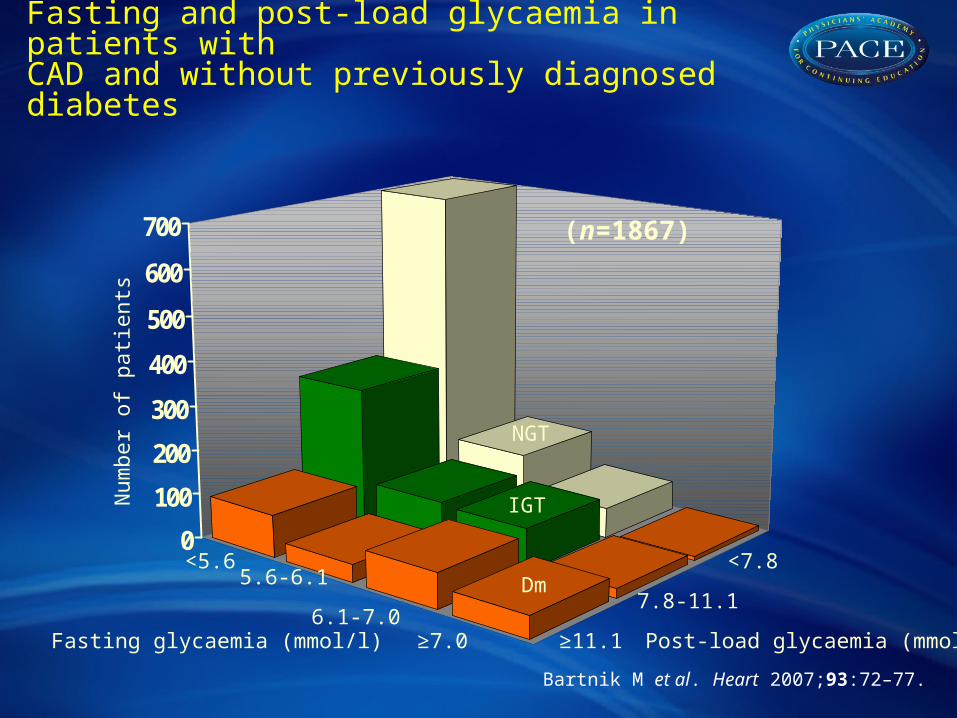
Euro Heart Survey Diabetes and the HeartFasting and post-load glycaemia in patients withCAD and without previously diagnosed diabetes
0
100
200
300
400
500
600
700
Fasting glycaemia (mmol/l) Post-load glycaemia (mmol/l)
<5.65.6-6.1
6.1-7.0≥7.0 ≥11.1
7.8-11.1
<7.8
(n=1867)
Num
ber o
f pat
ient
s
Dm
IGT
NGT
Bartnik M et al. Heart 2007;93:72–77.
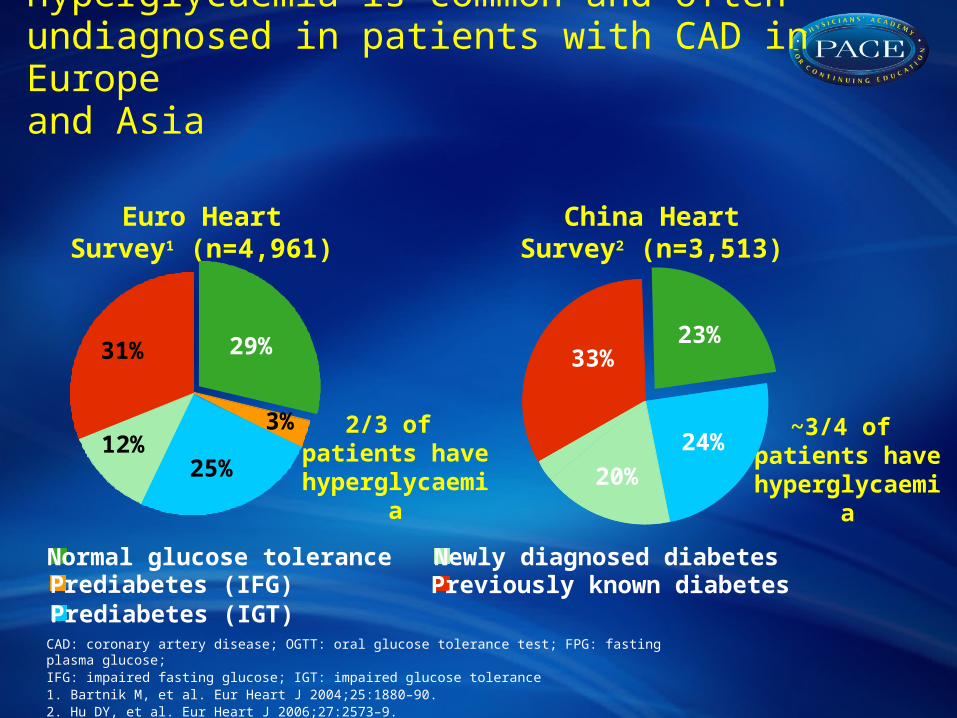
CAD: coronary artery disease; OGTT: oral glucose tolerance test; FPG: fasting plasma glucose; IFG: impaired fasting glucose; IGT: impaired glucose tolerance1. Bartnik M, et al. Eur Heart J 2004;25:1880–90. 2. Hu DY, et al. Eur Heart J 2006;27:2573–9.
China Heart Survey2 (n=3,513)
~3/4 of patients have
hyperglycaemia
Euro Heart Survey1 (n=4,961)
2/3 of patients have
hyperglycaemia
Previously known diabetesNormal glucose tolerance
Prediabetes (IGT)
Newly diagnosed diabetes
33%23%
24%
20%21%
Hyperglycaemia is common and often undiagnosed in patients with CAD in Europeand Asia
25%
31%
12%3%
29%
Prediabetes (IFG)
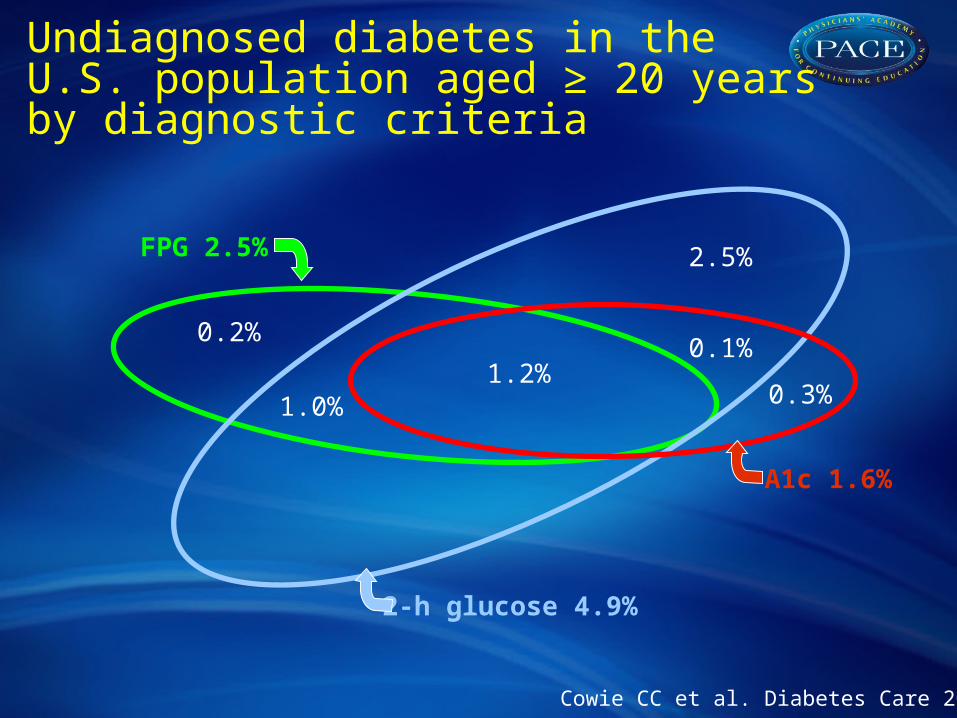
Undiagnosed diabetes in the U.S. population aged ≥ 20 years by diagnostic criteria
0.2%
1.0%1.2%
0.1%
0.3%
2.5%FPG 2.5%
A1c 1.6%
2-h glucose 4.9%
Cowie CC et al. Diabetes Care 2010

International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes
• A1C ≥ 5.7% to < 6,5% high risk for Diabetes
• A1C ≥ 6,5% undiagnosed diabetes
• ADA : or FPG > 7.0 mmol/l and/or post load ≥ 11.1 mmol/l
Diabetes Care 200932: 1327 -1334
WHO position statement 2011: HbA1c > 6.5 diagnostic for DM, levels below do not exclude diagnosis using glucose tests, no formal recommendation to interprete levels < 6.5 %

Type 2 Diabetes: some evidence based recommendations in primary CV prevention 2011
• Evidence for CHD risk equivalence: controversial, but total risk has decreased, i.e. to 10-15% over 10y in the best case scenario vs some 25% with silent myocardial ischemia
• Should every diabetic be on low dose aspirin? – probably not (bleeding hazards), however rather limited data base
• Should every diabetic be on a statin with a LDL target of 70 mg/dl? – probably yes, but more studies warranted
• Should every diabetic be on anti-RAS therapy? Probably yes, but avoid hypotension, especially with preexisting CVD
• Silent myocardial ischemia in totally asymptomatic patients with diabetes – is frequent, some 30 %, and with high risk (see above). Appropriate multifactorial therapy plus good medical monitoring for signs and symptoms of CHD effective and economic approach

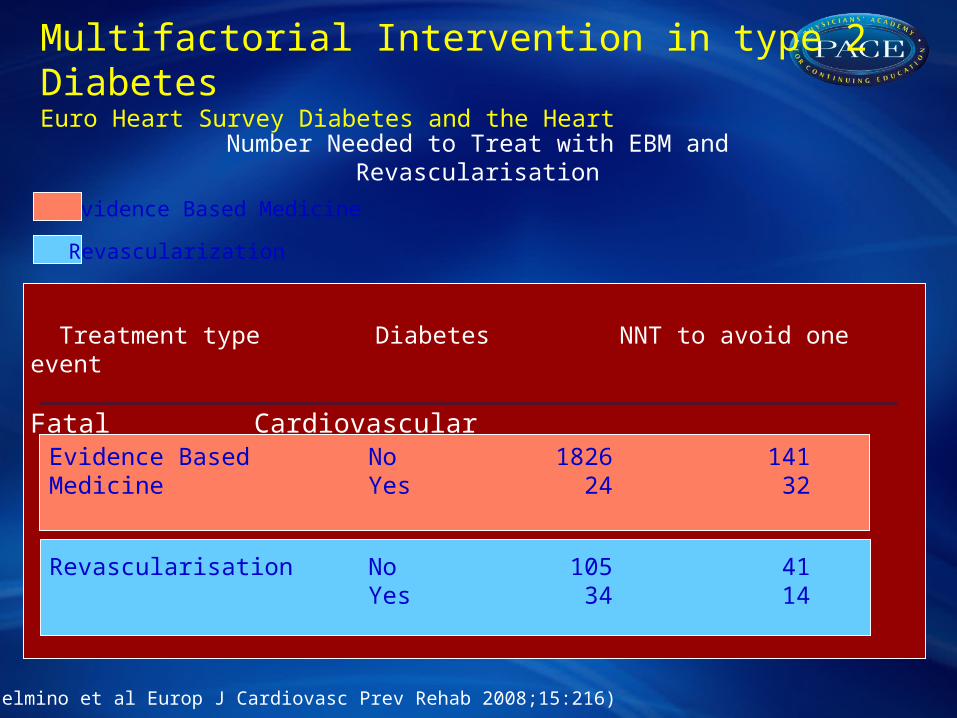
Multifactorial Intervention in type 2 DiabetesEuro Heart Survey Diabetes and the Heart
(Anselmino et al Europ J Cardiovasc Prev Rehab 2008;15:216)
0 100 200 300 4000,91
0,92
0,93
0,94
0,95
0,96
0,97
0,98
0,99
1,00
No DM EBM +
No DM EBM -
DM EBM +
DM EBM -
Time of follow up (days)
Cu
mu
lativ
e s
urv
iva
lImpact of Evidence Based Medicine (EBM) on 1-year mortality
Multifactorial Intervention in type 2 DiabetesEuro Heart Survey Diabetes and the Heart
(Anselmino et al Europ J Cardiovasc Prev Rehab 2008;15:216)
Treatment type Diabetes NNT to avoid one event Fatal Cardiovascular
Evidence Based No 1826 141Medicine Yes 24 32
Revascularisation No 105 41Yes 34 14
Evidence Based Medicine
Revascularization
Number Needed to Treat with EBM and Revascularisation