the chemotherapy of ovarian carcinoma
TRANSCRIPT

Cancer Treatment Reviews ( 1974) 1, 99-110
The chemotherapy of ovarian carcinoma
Robert C. Young, Susan P. Hubbard and Vincent T. DeVita
Medicine Branch, National Cancer Institute, Bethesda, Md 20014, U.S.A.
Introduct ion
Ovarian carcinoma is the fifth most frequent cause of death from cancer among women and approximately 14,000 new cases are diagnosed each year of which 10,400 will even- tually be fatal (46). Although the mortali ty rate has leveled off somewhat in the past decade, the death rate from this disease has tripled in the past 40 years and more than 1 out of every 100 women in the United States will eventually die of ovarian carcinoma. Although surgery and radiotherapy play major roles in the management of many patients with this illness, approximately 60% of patients initially present with advanced disease (F IGO stages I I I and IV) outside the confines of the truepelvis. Evenafter resection of what appears to be localized disease, 20-50 ~o of women will develop recurrent disease requiring further therapy (2, 40). Thus, for most patients with ovarian carcinoma, some kind of systemic therapy will be required either for pr imary or adjuvant management of advanced disease or for subsequent management of recurrent disease. As a consequence, considerable interest in the use of chemotherapy in this illness has developed over the past decade. This review represents an at tempt to collect the available information on the use of single agents and combination chemotherapy in ovarian carcinoma, and to highlight additional chemo- therapeutic agents of potential interest. Finally, a series of studies is proposed which may serve to optimize existing therapy in ovarian carcinoma and provide the basic information required to initiate combined modality studies in a systematic way, comparing newer modalities to optimal existing therapy within each stage.
Single agent chemotherapy
Primary therapy for advanced disease
Historically, single agent chemotherapy, as the initial t reatment of ovarian carcinoma has been restricted almost exclusively to patients with advanced stages (F IGO stages I I I and IV) who have either failed initial at tempts with radiotherapy or who were deemed
99
100 R. C. YOUNG, S. P. HUBBARD AND V. T. DEVITA
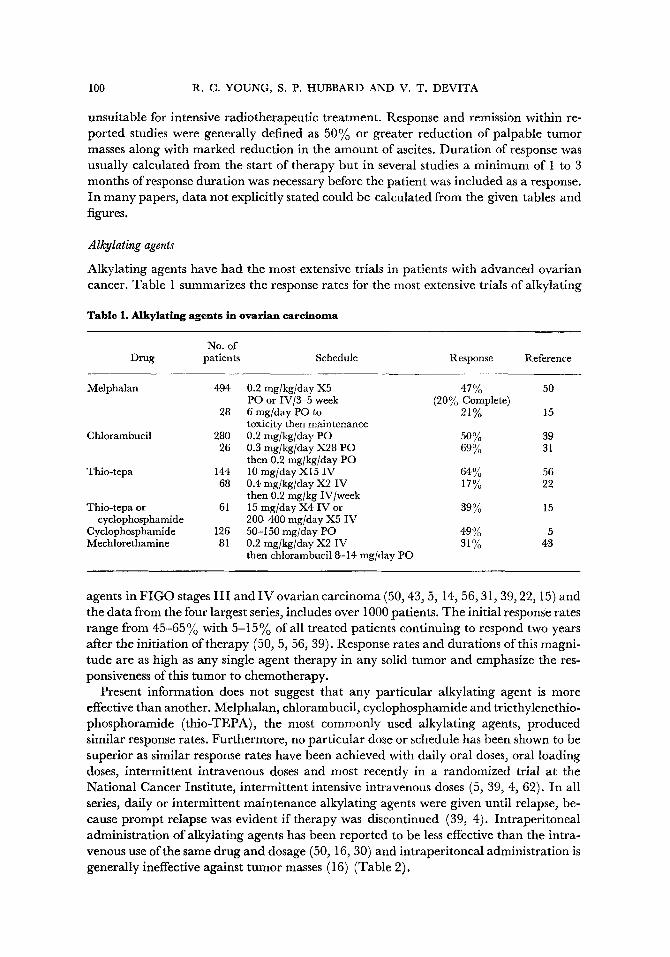
unsuitable for intensive radiotherapeufic treatment. Response and remission within re- ported studies were generally defined as 50% or greater reduction of palpable tumor masses along with marked reduction in the amount of ascites. Duration of response was usually calculated from the start of therapy but in several studies a minimum of 1 to 3 months of response duration was necessary before the patient was included as a response. In many papers, data not explicitly stated could be calculated from the given tables and figures.
Alkylating agents
Alkylating agents have had the most extensive trials in patients with advanced ovarian cancer. Table 1 summarizes the response rates for the most extensive trials of alkylating
Table 1. Alkylat ing agents in ovar ian carc inoma
No. of Drug patients Schedule Response Reference
Melphalan 494 0.2 mg/kg/day X5 47% 50 PO or IV/3-5 week (20% Complete)
28 6 mg/day PO to 21% 15 toxicity then maintenance
Chlorambueil 280 0.2 mg[kg[day PO 50% 39 26 0.3 mglkg/day X28 PO 69% 31
then 0.2 mg/kg/day PO Thio-tepa 144 10 mg/day XI5 IV 64% 56
68 0.4 mg/kg/day X2 IV 17% 22 then 0.2 mg/kg IV/week
Thio-tepa or 61 15 rag/day X4 IV or 39% 15 cyclophosphamide 200-400 mg/day X5 IV
Cyclophosphamide I26 50-150 rag/day PO 49% 5 Mechlorethamine 81 0.2 mg/kg/day X2 IV 31% 43
then chlorambucil 8-14 rag]day PO
agents in F I G O stages I I I and I V ovarian carcinoma (50, 43, 5, 14, 56, 31, 39, 22, 15) and the data from the four largest series, includes over 1000 patients. The initial response rates range from 45-65% with 5-15% of all treated patients continuing to respond two years after the initiation of therapy (50, 5, 56, 39). Response rates and durations of this magni- tude are as high as any single agent therapy in any solid tumor and emphasize the res- ponsiveness of this tumor to chemotherapy.
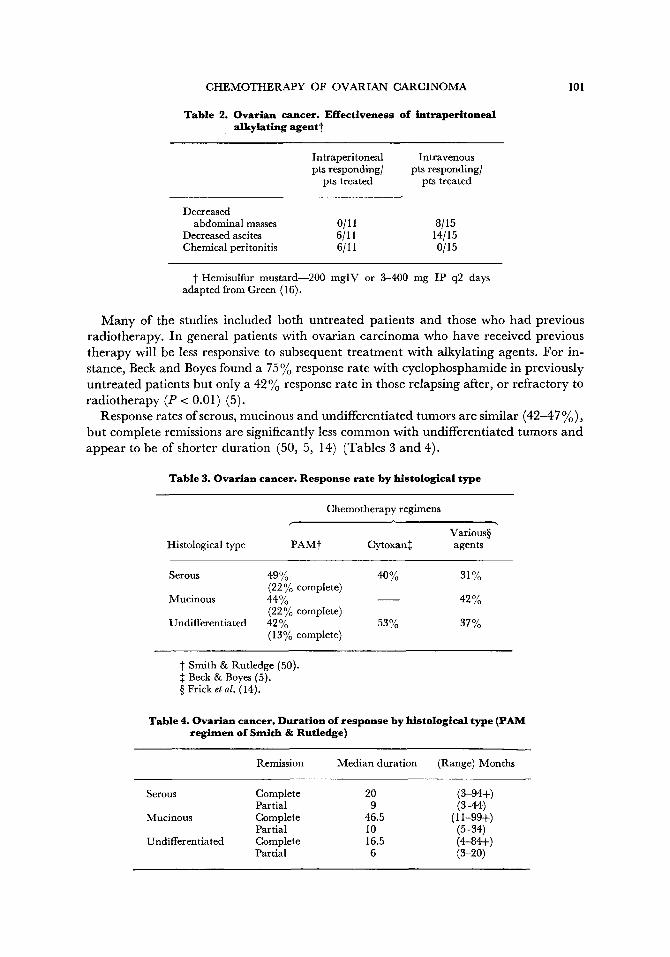
Present information does not suggest that any particular alkylating agent is more effective than another. Melphalan, chlorambucil, cyclophosphamide and triethylenethio- phosphoramide (thio-TEPA), the most commonly used alkylating agents, produced similar response rates. Furthermore, no particular dose or schedule has been shown to be superior as similar response rates have been achieved with daily oral doses, oral loading doses, intermittent intravenous doses and most recently in a randomized trial at the National Cancer Institute, intermittent intensive intravenous doses (5, 39, 4, 62). In all series, daily or intermittent maintenance alkylating agents were given until relapse, be- cause prompt relapse was evident if therapy was discontinued (39, 4). Intraperitoneal administration of alkylating agents has been reported to be less effective than the intra- venous use of the same drug and dosage (50, 16, 30) and intraperitoneal administration is generally ineffective against tumor masses (16) (Table 2).
CHEMOTHERAPY OF OVARIAN CARCINOMA 101
Table 2. Ovarian cancer. Effect iveness of intraperitoneal a lkylat lng agent~
Intraperitoneal Intravenous pts responding/ pts responding]
pts treated pts treated
Decreased abdominal masses 0/11 8/15
Decreased ascites 6/11 14/15 Chemical peritonitis 6/11 0[ 15
I Hemisulfur mustard--200 mglV or 3-400 mg IP q2 days adapted from Green (16).
M a n y of the studies included both unt rea ted patients and those who had previous radiotherapy. I n general patients with ovarian carc inoma who have received previous therapy will be less responsive to subsequent t rea tment with alkylating agents. For in- stance, Beck and Boyes found a 75 % response rate with cyclophosphamide in previously unt rea ted patients but only a 42% response rate in those relapsing after, or refractory to rad io therapy (P < 0.01) (5).
Response rates of serous, mucinous and undifferentiated tumors are similar (42-47 %), bu t complete remissions are significantly less c o m m o n with undifferentiated tumors and appear to be of shorter durat ion (50, 5, 14) (Tables 3 and 4).
Table 3. Ovarian cancer. Response rate by his to logical type
Chemotherapy regimens
Variousw " Histological type PAM t Cytoxan+ + agents
Serous 49 % 40 % 31% (22% complete)
Mucinous 44% 42% (22% complete)
Undifferentiated 42% 53% 37% (13% complete)
~" Smith & Rutledge (50). ++ Beck & Boyes (5). w Frick et al. (14).
Table 4. Ovarian cancer. Durat ion of response by his to logical type (PAN/ reg imen of Smith & Rutledge)
Remission Median duration (Range) Months
Serous Complete 20 (3-94+) Partial 9 (3-44)
Mucinous Complete 46.5 (11-99+) Partial 10 (5-34)
Undifferentiated Complete 16.5 (4-84+) Partial 6 (3-20)
102 R.C. YOUNG, S. P. HUBBARD AND V. T. DEVITA
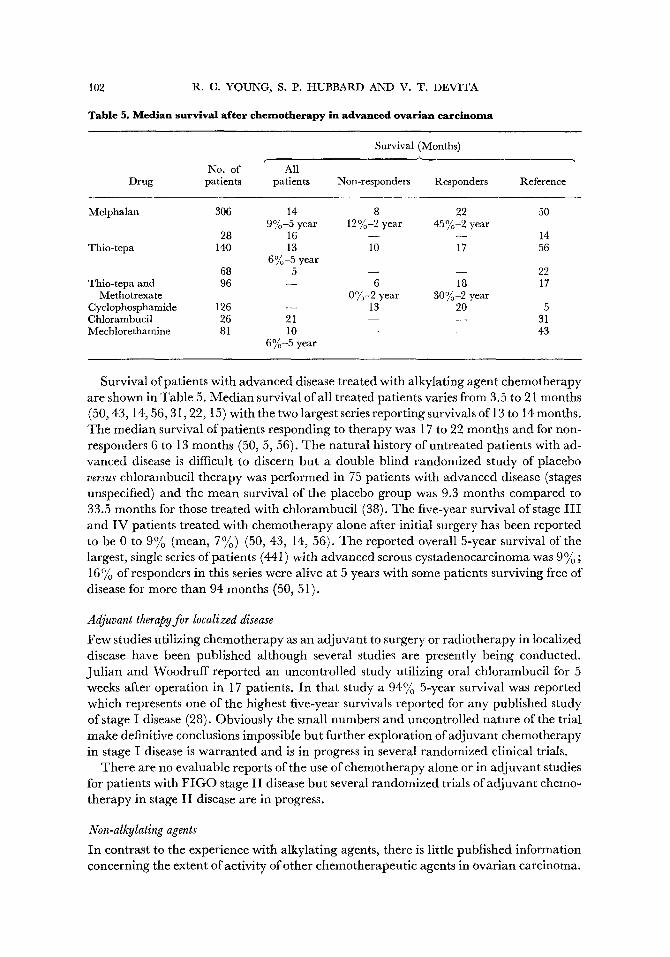
Table 5. Median survival after chemotherapy in advanced ovarian carc inoma
Survival (Months)
No. of All Drug patients patients Non-responders Responders Reference
Melphalan 306 14 8 22 50 9%-5 year 12%-2 year 45%-2 year
28 16 - - - - 14 Thio-tepa 140 13 10 17 56
6%-5 year 68 5 - - - - 22
Thio-tepa and 96 - - 6 18 17 Methotrexate 0%-2 year 30%-2 year
Cyclophosphamide 126 - - 13 20 5 Chlorambucil 2 6 21 - - - - 31 Mechlorethamine 81 10 - - - - 43
6%-5 year
Survival of patients with advanced disease treated with alkylating agent chemotherapy are shown in Table 5. Median survival of all treated patients varies from 3.5 to 21 months (50, 43, 14, 56, 3 I, 22, 15) with the two largest series reporting survivals of 13 to 14 months. The median survival of patients responding to therapy was 17 to 22 months and for non- responders 6 to 13 months (50, 5, 56). The natural history of untreated patients with ad- vanced disease is difficult to discern but a double blind randomized study of placebo versus chlorambucil therapy was performed in 75 patients with advanced disease (stages unspecified) and the mean survival of the placebo group was 9.3 months compared to 33.5 months for those treated with chlorambucil (38). The five-year survival of stage I I I and I V patients treated with chemotherapy alone after initial surgery has been reported to be 0 to 9% (mean, 7%) (50, 43, 14, 56). The reported overall 5-year survival of the largest, single series of patients (441) with advanced serous cystadenocarcinoma was 9 % ; 16 % of responders in this series were alive at 5 years with some patients surviving free of disease for more than 94 months (50, 51).
Adjuvant therapy for localized disease
Few studies utilizing chemotherapy as an adjuvant to surgery or radiotherapy in localized disease have been published although several studies are presently being conducted. Jul ian and Woodruff reported an uncontrolled study utilizing oral chlorambucil for 5 weeks after operation in 17 patients. In that study a 94% 5-year survival was reported which represents one of the highest five-year survivals reported for any published study of stage I disease (28). Obviously the small numbers and uncontrolled nature of the trial make definitive conclusions impossible but further exploration of adjuvant chemotherapy in stage I disease is warranted and is in progress in several randomized clinical trims.
There are no evaluable reports of the use of chemotherapy alone or in adjuvant studies for patients with F I G O stage I I disease but several randomized trials of adjuvant chemo- therapy in stage I I disease are in progress.
Non-alkylating agents
In contrast to the experience with alkylating agents, there is little published information concerning the extent of activity of other chemotherapeutic agents in ovarian carcinoma.
CHEMOTHERAPY OF OVARIAN CARCINOMA 103
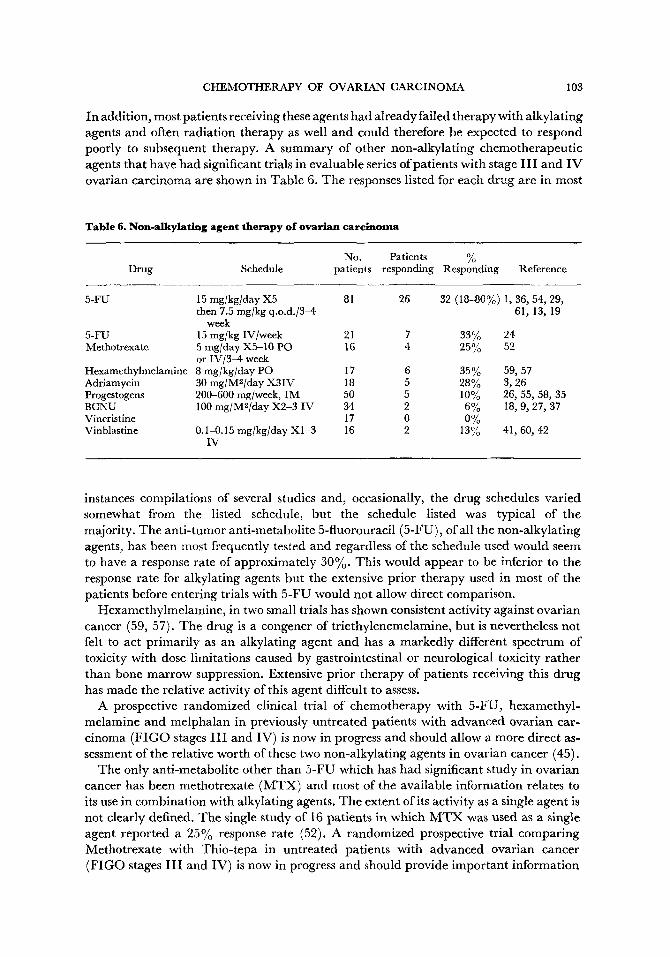
In addition, most patients receiving these agents had already failed therapy with alkylating agents and often radiation therapy as well and could therefore be expected to respond poorly to subsequent therapy. A summary of other non-alkylating chemotherapeutic agents that have had significant trials in evaluable series of patients with stage I I I and I V ovarian carcinoma are shown in Table 6. The responses listed for each drug are in most
Table 6. Non-alkylating agent therapy of ovarian carcinoma
No. Patients % Drug Schedule patients responding Responding Reference
5-FU 15 mg/kg/day X5 81 26 32 (18-80%) 1, 36, 54, 29, then 7.5 mg/kg q.o.d./3-4 61, 13, 19
week 5-FU 15 mg/kg IV/week 21 7 33% 24 Methotrexate 5 mg/day X5-10 PO 16 4 25% 52
or IV/3-4 week Hexamethylmelamine 8 mg/kg/day PO 17 6 35% 59, 57 Adriamycin 30 mg/M2/day X3IV 18 5 28% 3, 26 Progestogens 200-600 nag/week, IM 50 5 10% 26, 55, 58, 35 BCNU 100 mg/M2/day X2-3 IV 34 2 6% 18, 9, 27, 37 Vincristine t 7 0 0% Vinblastine 0.1-0.15 mg/kg/day X1-3 16 2 13% 41, 60, 42
IV
instances compilations of several studies and, occasionally, the drug schedules varied somewhat from the listed schedule, but the schedule listed was typical of the majority. The anti- tumor anti-metabolite 5-fluorouracil (5-FU), of all the non-alkylating agents, has been most frequently tested and regardless of the schedule used would seem to have a response rate of approximately 30%. This would appear to be inferior to the response rate for alkylating agents but the extensive prior therapy used in most of the patients before entering trials with 5-FU would not allow direct comparison.
Hexamethylmelamine, in two small trials has shown consistent activity against ovarian cancer (59, 57). The drug is a congener of triethylenemelamine, but is nevertheless not felt to act primarily as an alkylating agent and has a markedly different spectrum of toxicity with dose limitations caused by gastrointestinal or neurological toxicity rather than bone marrow suppression. Extensive prior therapy of patients receiving this drug has made the relative activity of this agent diffcult to assess.
A prospective randomized clinical trial of chemotherapy with 5-FU, hexamethyl- melamine and melphalan in previously untreated patients with advanced ovarian car- cinoma ( F I G O stages I I I and IV) is now in progress and should allow a more direct as- sessment of the relative worth of these two non-alkylating agents in ovarian cancer (45).
The only anti-metabolite other than 5-FU which has had significant study in ovarian cancer has been methotrexate (MTX) and most of the available information relates to its use in combination with alkylating agents. The extent of its activity as a single agent is not clearly defined. The single study of 16 patients in which M T X was used as a single agent reported a 25% response rate (52). A randomized prospective trial comparing Methotrexate with Thio-tepa in untreated patients with advanced ovarian cancer (FIGO stages I I I and IV) is now in progress and should provide important information

104 R. C. YOUNG, S. P. HUBBARD AND V. T. DEVITA
on the relative activity of this potentially important anti-metabolite in advanced ovarian cancer (44).
Anti-tumor antibiotics have not received any significant trial as single agents in ovarian cancer with the exception of the new agent adriamycin (6, 3). Initial information would suggest some activity (28% responses in 17 patients) for this agent and should stimulate further use of this agent in prospective trials (6).
Progestogens, of various kinds have been reported to have activity in this disease in several trials, but the collected objective response rate in 50 patients was only 10Yo (26, 55, 58, 35). A recent study reporting two extremely good responses, out of nine patients treated with complete remissions lasting 30+ and 45+ months, make further study of the compound warranted (35).
The nitrosourea, BCNU, has been investigated in 34 patients with ovarian carcinoma in four separate trials and the 6% overall response rate with short durations of response would seem to indicate minimal activity of this agent (18, 9, 29, 37).
The vinca alkaloids, vincristine and vinblastine, have received some investigation in ovarian cancer and both appear to have minimal activity in the small number of patients thus far studied (21, 41, 60, 42).
Because so few patients have been treated and there is such great variability of prior treatment and extent of disease, it is impossible to provide meaningful information on median duration of responses or median survival for those patients treated with non- alkylating agents. One of the most important unanswered questions regarding manage- ment of advanced ovarian cancer is the extent of activity of non-alkylating drugs which have different mechanisms of action and types of toxicity. Only this information will allow rational design of potentially useful combination chemotherapy programs.
Potential agents for experimental drug trials
A series of chemotherapeutic agents are presently available which are attractive for study in patients with ovarian carcinoma who have failed on previous "standard" therapy. They are included because (1) they have shown activity in scattered reports where a few patients with ovarian cancer (less than 10) were included, or (2) they are active in many human tumors but have not been tried in ovarian carcinoma. In addition, interest is heightened in any such agent which does not have bone marrow suppression as its dose- limiting toxicity, as such drugs might be particularly useful in combination chemotherapy programs. A list of potential drugs for experimental drug trials appear in Table 7.
Cytembena has been fairly extensively investigated by Czechoslovakian workers and appears to be active against a wide range of gynecological malignancies including ovarian cancer (47, 12). In comparing 55 patients with ovarian cancer treated with Cytembena and 10 patients treated with eyclophosphamide, the tumor-inhibitory activity of the two agents was approximately equal but less toxicity was encountered with Cytembena (12). The mechanism of action of the drug is not completely known but the agent appears to inhibit purine biosynthesis as well as vital folate metabolizing enzymes (48, 49).
Procarbazine is of potential interest as it is active in several human solid tumors in- cluding mesothelioma which is embryologically related to the ovarian epithelium. Fur- thermore when administered on an intermittent intravenous regimen its dose-limiting toxicity is neurologic rather than hematopoietic (8).
CHEMOTHERAPY OF OVARIAN CARCINOMA 105
Table 7. Potential drugs for experimental trials in ovarian earelnoma
Cytembena Procarbazine Actlnomycin D Porfiromycin Streptozotocin DTIG Bleomycln Hydroxyurea Mithramycin Mitomycin C
Actinomycin D has been used extensively in a number of combination chemotherapy programs in ovarian cancer (50, 51) but has never been investigated as a single agent. Considerable toxicity would be added to any regimen which included actinomycin D and hence the therapeutic contribution of this agent should be assessed before its further use in combination can be recommended. Its known activity in germinal tumors of the ovary and testis may not predict for activity in the more common epithelial tumors of the ovary.
Porfiromycin, an anti-tumor antibiotic has been studied in two separate clinical trials in which ovarian patients refractory to alkylating agents have been included. Of the 21 ovarian patients treated, six demonstrated some response to the compound and further studies seem warranted (34, 23).
Streptozotocin and bleomycin have been included because their activity has not been investigated in patients with ovarian cancer and their dose-limiting toxicity is not bone marrow suppression.
DTIC, hydroxyurea, mithramycin and mitomycin C, have all shown activity in several human solid tumors but have not been studied in patients with ovarian cancer. All have significant bone marrow as well as other toxicities.
C o m b i n a t i o n c h e m o t h e r a p y i n a d v a n c e d o v a r i a n c a n c e r
A few trials of combination drug therapy have been reported, however, only one has been a randomized trial comparing the combination with an effective single agent. Smith and Rutledge reported 38~o responses (9% complete) in 47 patients refractory to melphalan with a three drug combination including cyclophosphamide, actinomycin D and 5- fluorouracil (50). In a subsequent randomized prospective trial comparing the three drug combination with melphalan, however, the overall response rate to the combination in 47 patients was 45 ~ compared with 42 % for the 50 patients treated with melphalan alone (51). In addition the toxicity of the combination was more severe than the toxicity ofmel- phalan alone (51).
I N U I I I I ~ O [11• U L I I I Z I ( . U I I I U I I I ~ i ~ L I U I I b L M U I K ; b l l C t b l l I % I U U K ; U O.11 ( ; V C L I U I : ~ U I ~ I ~ U I I L I U I L ~ l U U l J u I
patients treated with conventional chemotherapy. Greenspan employed triethylenethio- phosphoramide (thio-TEPA) and methotrexate in intermittent loading-dose schedules and reported 63 ~o good to excellent responses in 96 patients (17). There were, however, frequent side effects and three deaths due to drug toxicity and the overall survival was similar to that achieved with single agents (17).
Brandl, utilizing a regimen of cyclophosphamide, vinblastine and triaziquone (Trenimon) a quinone derivative that may act as an alkylating agent, reported 80~

106 R. C. YOUNG, S. P. HUBBARD AND V. T. DEVITA
"objective" responses (two complete) in 26 patients with no prior therapy (7). Finally, there are a series of reports of various combinations which have been used in ovarian carcinoma, but so few ovarian patients have been included that one is unable to assess the worth of the regimens in the overall management of the disease (9, 33, 32, 53, 20).
At present no combination chemotherapy regimen has been demonstrated to be more efficacious than an alkylating agent used alone and even those unrandomized trials where high initial response rates have been reported have had durations of maintained responses similar to those obtained with alkylating agents alone. There are, nevertheless, important theoretical reasons for considering combination chemotherapy in this disease (11), but the worth of such combinations will only be evaluable when compared directly with a parallel group treated with alkylating agents alone. The design of new combinations for ovarian cancer will rest on combining drugs which (a) have different mechanisms of action and different types of toxicity, (b) have proven anti- tumor activity in ovarian epithelial tumors when used as single agents and (c) can be combined with acceptable toxicity and ease of administration. The identification of significant anti- tumor activity of new drugs is an important step in further clinical trials.
Combination radiotherapy and chemotherapy
Although there are many reports of survival data where both radiotherapy and chemo- therapy have been administered, only prospective studies of thoroughly staged patients, systematically given simultaneous or closely sequential radiotherapy and chemotherapy would be expected to demonstrate synergistic effects of the two modalities, if such a synergy exists. Unfortunately only four reasonably large series meet these criteria. Hreshchyshyn and Graham reported an 11.5 month median survival in 41 stage I I I patients compared to four months for retrospective controls treated by radiotherapy alone (22). In two other studies, patients with stage I I I disease were randomized to total abdominal radiotherapy with or without alkylating agent therapy (30, 10). Median survivals of 13 and 14 months were found for patients on combined therapy compared to 7 and 8 months for those treated with radiotherapy alone although patients relapsing after radiotherapy alone subsequently received chemotherapy. Johnson et al., in a randomized trial of patients with
Figure I. Controlled trials in ovarian cancer treatment.
Definitions : SST--Standardized surgical therapy
must remain the same within any trial. May be:
(a) Resection of existing disease
(b) Panhysterectomy (c) Panhysterectomy plus
omentectomy
SRT--Standardized radiotherpy must remain the same within any trial. May be:
(a) Pelvic plus lower abdominal (b) Total abdominal-spray (c) Total abdominal-moving
strip
Alkylating agent-- must remain the same within trial. May be :
(a) PAM (b) Thio-TEPA (c) Cytoxan (d) Chlorambucil
Non-alkylating agent May be :
(a) 5-FU (b) I-Iexamethylmelamine (c) Adriamycin (d) Procarbazine (e) Cytembena
OST-- Optimal surgical treatment'~
OIT-- Optimal irradiation treatment'~
ODT--Optimal drug Treatment~ Will be generated by the pro-
posed randomized clinical trials

GHEMOTHERAPY OF OVARIAN CARCINOMA 107
~=~-~'~ ~i ~ ~ ~ [
ii ~il !~i~ ~ -~- ~ ~
Lana i

108 R. (3. YOUNG, S. P. HUBBARD AND V. T. DEVITA
stage I I I disease, compared cyclophosphamide alone with cyclophosphamide and total abdominal radiotherapy and found an insignificant difference between the regimens with survivals of 10.5 months and 14.0 months, respectively (25). Although trials with combined modalities have not been strikingly effective, most of the trials have demon- strated that chemotherapy has been the equivalent of or has added some benefit to radiotherapy. As suggested by these data, there is no evidence that radiotherapy is su- perior to chemotherapy either for palliation of the median patient or for producing im- proved five year survivals of patients with advanced disease. Likewise, there is no evidence that simultaneous radiotherapy and chemotherapy is superior to chemotherapy alone. In one study, the addition of radiation therapy after a melphalan-induced remission failed to improve survival when compared to melphalan maintenance and the authors felt the additional radiation therapy was detrimental (51). In addition, the available data sug- gests that the complications of total abdominal radiotherapy are at least as frequent and severe as the complications of chemotherapy. Clearly, prospective studies, randomizing stage I I I and IV patients to radiotherapy or chemotherapy alone will be necessary to determine definitively the relative merits of each.
Future role for chemotherapy in ovarian adenocarclnoma
In spite of the deaths of 100,000 women from ovarian adenocarcinoma in the United States in the past decade, the optimal therapy of this disease is still unknown. The impres- sive responses of some patients with advanced ovarian cancer to single alkylating agents has suggested an expanding role for chemotherapy in this disease. However, the overall experience with the disease continues to be discouraging even in spite of the sometimes effective chemotherapy, surgery and radiotherapy. Fundamental to improved therapy in this disease will be the determination of the optimal existing therapy for each stage of the disease which can only be accomplished by prospective randomized clinical trials. A series of such trials will involve chemotherapy either as an adjuvant for localized disease, as a combined modality with radiotherapy, or as a primary therapy in single agent or combination chemotherapy programs. An outline of some of the considerations for such chemotherapy trials appears in Figure I.
As shown in Figure 1, inherent in clinical trials of chemotherapy in both early and ad- vanced stages of disease is the determination of optimal radiotherapeutic management of the disease as well as optimal chemotherapy. These optimal single modality therapies can then be compared to each other and to combination approaches as listed. Prior deter- mination of important prognostic factors such as staging, histologic type, histologic grade and extent of residual disease after surgery will be necessary in order to insure compar- ability of randomized groups.
In stage Ia and Ib disease, the therapeutic dilemma centers around the benefit of addi- tional prophylactic therapy after primary resection. The relative merits of the several alkylating agents must be compared to optimal radiotherapy and eventually to a com- bined modality approach. I f new drugs or drug combinations become established as more effective than alkylating agents in trials in advanced disease they would then become ap- propriate for subsequent comparative trials.
For patients with stage Ic and II disease, the central questions are what is the optimal existing radiation treatment and is chemotherapy equivalent or can it improve the five year survival of optimal radiotherapy ?

CHEMOTHERAPY OF OVARIAN CARCINOMA 109
For patients with advanced disease (stages I I I a nd IV) it will be necessary to define the opt imal form of i r radia t ion t rea tment and to establish the relat ive mer i t of a d j u v a n t chemotherapy. Second, it will be impor tan t to establish the relative meri t of chemotherapy alone compared to radio therapy alone. F ina l ly it will be necessary to compare s t andard alkylat ing agent therapy, with new active agents, combina t ion chemotherapy regimens and in addi t ion to search for new agents active against ovar ian carcinoma. Such trials will allow physicians m a n a g i n g this disease to s tudy newer therapeut ic and combined
modal i ty approaches in a systematic way, compar ing newer therapies to opt imal existing t rea tment wi th in each stage. Such studies will define the role of chemotherapy in the
m a n a g e m e n t of ovar ian carcinoma.
R e f e r e n c e s
1. Ansfield, F.J., Shroeder, J. M. & Curreri, A. R. (1962). J. Am. med. Ass. 181:295. 2. Bagley, C. M., Young, R. C., Canellos, G. P. & DeVita (1972). New Engl. 3". Med. 287:856. 3. Barlow, J. J., Piver, M. S., Chuang, J. T., Cortes, E. P., Ohnuma, T. & Holland, J. F. (1973). Cancer,
N.Y. 32:735. 4. Barr, W., Cowell, M. A. C. & Chatfield, W. R. (1970). Scott. med. J . 15:250-256. 5. Beck, R. E. & Boyes, D. A. (1968). Can. reed. Ass. J . 98:539. 6. Bonadonna, G. (1973). Proc. 8th Int. Congr. Chemother., Athens. Vol. I. (Abstr. B VII-3). 7. Brandl, K. (1970). Zentbl. Gyna'k. 92:233. 8. Chabner, B. A., Sponzo, R., Hubbard, S., Canellos, G. P., Young, R. C., Schein, P. S. & DeVita, V. T.
(1963). Cancer Chemother. Rep. 57, Part 1 : 361. 9. Cohen, S. M., Weiner, M.J. & Greenspan, E. M., (1972). Cancer Chemother. Rep. 56, Part 1:751.
10. Decker, D. G., Mussey, E., Malkasian, G. D. et al. (1967). Am. J. Obstet. Gynee. 97: 171. 11. DeVita, V. T. & Schein, P. S. (1973). New Engl. 3". Med. 288:998. 12. Dvorak, O. (1971). Neoplasma 18:461. 13. Field, J. G. (1963). Cancer Chemother. Rep. 33:45. 14. Frick, H. C., Atchoo, N., Adamsons, K. & Taylor, H. C. (1965). Am. J. Obstet. Gynee. 93:1112. 15. Frick, H. C., Tretter, P., Tretter, W. & Hymen, G. A. (1968). Cancer, N.Y. 21:508. 16. Green, T. H. (1959). Obstet. Gynec., N.Y. 13:383. 17. Greenspan, E. M. (1968). J. M t Sinai Hosp. 35:52. 17(a). Greenspan, E. See (44). 18. Godfrey, T. E., King A. & Rentschler, R. (1973). Am. J. Obster. Gynec. 115:576. 19. Hall, B. E. & Good, J. W. (1962). CancerChemother. Rep. 16:369. 20. Hanham, I. W. F., Newton, K. A. & Westbury, G. (1971). Br. J. Cancer 25:462. 21. Holland, J. F., Scharlau, C., Gailani, S. et al. (1973). Cancer Res. 33: 1258. 22. Hreschchyshyn, M. M. & Graham, J. B. (1967). Int. Surg. 47:398. 23. Izbicki, R., A1-Sarraf, M., Reed, M. L., Vaughn, C. B. & Vaitkevicius, V. K. (1972) Cancer Chemother.
Rep. 56:615. 24. Jacobs, E. M., Reeves, W.J., Wood, D. A., Pugh, R., Braunwald, J. & Bateman, J. R. (1971). Cancer,
N.Y. 27:1302. 25. Johnson, C. E., Decker, D. G., Van Herik, M., Mussey, E., Malkasian, G. D. & Jorgensen, E. O. (1972).
Am. J. Roentg. 114:136. 26. Jolles, B. (1962). Br. J. Cancer 16:209. 27. Jorgensen, E. O., Malkasian, G. D., Webb, M. J. & Hahn, R. G. (1973). Am. J. Obstet. Gynec. 116:769 28. Julian, C. G. & Woodruff, J. D. (1969). Obstet. Gynec. Surv. 24:1307. 29. Kennedy, B.J. & Theologides, A. (1961). Ann. intern. Med. 55:719. 30. Kottmeier, H. L. (1968). Clin. Obstet. Gynec. 11:428. 31. Lebharz, T. B., Huston, J. W., Austin, J. A. & Boyce, C. R. (1965). Obstet. Gynec. N.Y. 25:475478. 32. Li, M. C. & Hsu, K. (1970). Clin. Obstet. Gynee. 13:928. 33. Lokich, J. J., Skarin, A. T. (1972). Cancer Chemother. Rep. 56, Part 1 : 761. 34. Loo, R. V., Vaitkevieius, V. K. Reed, M. L. & Vaughn, C. B. (1967). Cancer Chemother. Rep. 51:497. 35. Malkasian, G. D., Decker, D. G.,Jorensen, E. O. & Webb, M.J. (1973). Cancer Chemother. Rep. Part 1.
57: 241. 36. Malkasian, G. D., Decker, D. G., Mussey, E. &Johnson, C. E. (1968). Am. J. Obstet. Gqnee. 100:1021.

110 R . C . YOUNG, S. P. HUBBARD AND V. T. DEVITA
37. Marsh, J. C., DeConti, R. C. & Hubbard, S. P. (1971). Cancer Chemotlwr. Rep. 55, Part 1 : 599. 38. Masterson, J. G. Discussion of Burns, B. C., Jr. Rutledge, F. N., Smith, J. P. et al. (1967). Am. J . Obstet.
Gynec. 98:374. 39. Masterson, J. G. & Nelson, J. H. (1965). Am. J . Obstet. Gynee. 93: 1102. 40. Munnell, E. W. (1968). Am. J . Obstet. Gynec. 100:790. 41. Midwest Cooperative Chemotherapy Group (1963). Cancer Res. 23: 169. 42. Neoplastic Disease Treatment with Vinblastine: a Cooperative Study. (1965). Archs intern. Med. 116:
846. 43. Parker, R. T., Parker, C. H. & Wilbanks, G. D. (1970). Am. J . Obstet. Gynec. 100:878. 44. Personal Communication, Greenspan, E. 45. Personal Communication, Smith, J. P. 46. Silverberg, E & Holleb, A. I. (1972). Cancer Statistics. CA 22:2. 47. Skoda, V., Jandova, A. & Novotna, J. (i970). Neoplasma 17:175. 48. Slavikova, V., Semonsky, M., Slavik, K. & Volejnikova, J. (1966). Biochem. Pharmac. 15:763. 49. Slavikova, S., Semonsky, M., Slavik, K., Zikan, V. & Volejnikova,J. (1969). Biochem. Pharmac. 18: 1455. 50. Smith, J. P. & Rutledge, F. (1970). Am. J. Obstet. Gynec. 107: 691. 51. Smith, J. P., Rutledge, F. &Wharton, J. T. (1972). Cancer. N.Y. 30: 1565. 51(a). Smith, J. P. See (45). 52. Sullivan, R. D., Miller, E., Zurek, W. Z., Oberfeld, R. A. & Ojima, Y. (1967). Surgery. Gynec. Obstet.
125:819. 53. Vahrson, H. (1973). Geburtsh. Frauenheilk. 33:293. 54. Vaitkevicuis, V. K., Brennen, M.J. , Beckett, V. L., Kelly, J. E. & Talley, R. W. (1961). Cancer, N.Y.
14: 131. 55. Varga, A. & Henriksen, E. (1964). Obstet. Gynec., N.Y. 23:51. 56. Wallach, R. C. Kabakow, B., Blinick, G. et al. (1970). Obstet. Gynec., N.Y. 35:278. 57. Wampler, G. L., Mellette, S.J., Kupermine, M. & Regelson, W. (1972). CancerChemother. Rep. 56, Part
1 : 505. 58. Ward, H. W. C. (1972). 3". Obstet. Gynec. Br. Commun. 79:555. 59. Wilson, W. L., Bisel, H. F., Cole, D. et al. (1970). Cancer N.Y. 25:568. 60. Wright, T. L., Hurley, J., Korst, D. R., Monto, R. W., Rohn, R. J., Will, J. J. & Louis, J. (1963).
Cancer Res. 23:169. 61. Young, C. W., Ellison, R. R., Sullivan, R. D. etal. (1960). CancerChemother. Rep. 6: 17. 62. Young, R. C. & DeVita, V. T. Unpublished observations.