the asc is a multi-departmental, collaborative center
TRANSCRIPT
Welcome to the Autism Spectrum Center (ASC) at Boston Children’s Hospital.
The ASC is a multi-departmental, collaborative center providing diagnosis, treatment, continuity of care and support services.
Date: _______________
Dear Parent/Guardian,
Thank you for your interest in the Autism Spectrum Center. The below steps will need to be completed before scheduling an appointment.
1. Complete and return all attached forms to our office by mail, email or fax. Please
note that the more information you can provide us before to your appointment, the more
productive the visit will be. You are also encouraged to make copies of forms for your
own records.
Mail to: Boston Children’s Hospital
Autism Spectrum Center
300 Longwood Avenue, Fegan 11
Boston, MA 02115
Email: [email protected]
Fax: 617-730-4823
2. Please include any relevant early intervention/school testing such as the most recent
copies of:
o IFSP (Individualized Family Service Plan-report from early intervention services)
o IEP (Individualized Education Program)/504 Accommodation Plan
o School district based CORE/TEAM evaluations (could include educational
testing, psychological testing, OT, PT, and/or speech and language evaluations).
o Any private or clinic-based testing (could include psychological testing,
neuropsychological evaluation, past medical diagnostic assessments, OT, PT
and/or speech and language evaluations).
3. Once we receive and review the information, the ASC intake team will contact you to
schedule an appointment.
We know this process can be complex and confusing. Please feel free to contact the Autism Spectrum Center if you have any questions by phone at 617-355-7493 or by email at [email protected]. You can also visit our website for information about our center: http://www.bostonchildrens.org/autismspectrumcenter
SERVICES INCLUDE• A single point of access and a streamlined appointment
process for children with ASD and their families
• Multidisciplinary staff from Neurology, DevelopmentalMedicine, Psychiatry, Psychology, Genetics, Speechand Language, Gastroenterology, Occupational Therapy
• Diagnostic evaluation and follow-up care
• Resource Specialist, Social Work and Child Life Specialiststo better serve our patients
• Educational e-newsletter
• Autism friendly hospital initiative for optimizedpatient experience
• Parent Lecture Series presented by our faculty and guests
LOCATIONSBoston • Lexington • Peabody • Waltham • Weymouth
AUTISM SPECTRUM CENTERBOSTON CHILDREN'S HOSPITAL
A multi-departmental collaborative center providing diagnosis, treatment,
continuity of care, and support services for children with
Autism Spectrum Disorder (ASD) and their families.
617-355-7493
bostonchildrens.org/autismspectrumcenter
FOR MORE INFO
INSURANCE INFORMATION
Your signature below indicates that you have been advised that you may be responsible for paying all charges associated with the visit.
I acknowledge that if any of the above referenced items or services are not considered medically necessary by my insurance company or are non-covered services, I am financially responsible for the full amount should the claim be denied. If I am denied insurance coverage for any service, discounts may be available.
Guarantor Name:
Parent/Guarantor Signature: Date:
1
Web Version
ASC INTAKE QUESTIONNAIRE
Use Plate, Label, or Print:
Name:
CH MRN#:
DOB: Gender: M F
© Boston Children’s Hospital, 2014 All rights reserved 1
Child’s Name: Last First
Date of Birth: __________________________________ Gender (circle): M F
The Autism Spectrum Center does not provide evaluations for child abuse and neglect, custody determination, immediate suicidality, IQ testing for gifted placement or assessment for acute psychiatric conditions. If you need any of the above services, please let us know and we can direct you to an appropriate provider.
Because the Autism Spectrum Center has a waiting list, some problems need more urgent attention. If your child has any of the following problems, please also contact your pediatrician. Please indicate if you have any urgent medical concerns including any of the following:
Y N Seizures Y N Loss of skills, developmental regression Y N Loss of hearing Y N Loss of vision Y N Difficulty swallowing, choking Y N Severe weakness or lack of coordination Y N Inability to tolerate exercise Y N Severe headache Y N Safety of any family members, including this child Y N Suicidal thinking or attempt of child or family members Y N Other (please describe):
___________________________________________________________________________________________
Do any of the following apply to this child: Y N DCF (formerly DSS) involvement Y N DDS (formerly DMR) involvement Y N Lives in residential facility
Please list the question(s) you would like answered by this evaluation (at least one REQUIRED):
1. _____________________________________________________________________________________
2. _____________________________________________________________________________________
3. _____________________________________________________________________________________
Who referred your child to the Autism Spectrum Center? (If a provider, please list name and specialty)
___________________________________________________________________________________________
Child’s Primary Care Provider (e.g. pediatrician, nurse practitioner)
___________________________________________________________________________________________
Date of last physical exam: _____________________________________________________________________
Web Version
ASC INTAKE QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 2
Parent/Caregiver 1 contact information
Full name: First _______________________________________ last ______________________________________
Relationship to child ___________________________________________________________________________
Home address Street___________________________________________________________________________
City/town_________________________________________________________________________
State_____________________________Zip_______________
Telephone (please check preferred number): home_____________ work____________ mobile____________
Email address _______________________________________________________________________________
Parent/Caregiver 2 contact information
Full name: First _______________________________________ last ______________________________________
Relationship to child ___________________________________________________________________________
Home address Street___________________________________________________________________________
City/town_________________________________________________________________________
State_____________________________Zip_______________
Telephone (please check preferred number): home_____________ work____________ mobile____________
Email address _______________________________________________________________________________
Legal guardian (if different from above)
Full name: First _______________________________________ last ______________________________________
Relationship to child ___________________________________________________________________________
Home address Street___________________________________________________________________________
City/town_________________________________________________________________________
State_____________________________Zip_______________
Telephone (please check preferred number): home_____________ work____________ mobile____________
Email address _______________________________________________________________________________
Child’s Living/Custody arrangement: please check if applicable, and complete table on next page
Child in guardianship Child in foster care Child in adoptive family Other (please describe): _____________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
Web Version
ASC INTAKE QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 3
Language(s) spoken in the home:_________________________________________________________________
Y N Do you or your child require an interpreter for this evaluation?
Family religion _______________________________________________________________________________ How would you describe the child’s race or ethnicity? Please check all that apply:
American Indian/Alaska Native Asian Black/African American Native Hawaiian or other Pacific Islander White Latino/Hispanic Other race (please describe): _____________________________________________________________
Y N Has your child had a school (CORE, TEAM) evaluation? If yes, when? __________________________ Y N Does your child have an Individualized Education Plan (IEP)? If yes, date of IEP? _________________ Y N Has your child had any previous psychological testing? If yes, when? ___________________________
Please submit copies of the most recent Individualized Education Plan (IEP), and results of any previous academic, psychological, or school testing from the past 3 years. This information may be necessary for insurance referrals. Please indicate the documents that will be sent in:
Documents to be sent in Who will send these in: IEP, IFSP, IIIP Parent School Other: Academic, psychological, and/or school testing results Parent School Other: Other documents (describe):
Parent School Other:
Name of parent/caregiver or other person with guardianship or medical decision-making authority for the child
Is this person the child’s legal guardian?
Does this person have physical custody (child lives with this person)?
If yes, at what age did child come into home?
Caregiver 1 above Y N Y N
Caregiver 2 above Y N Y N
Other Y N Y N
Other Y N Y N
Web Version
ASC INTAKE QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 4
Please check off any that apply to this child:
I have concerns about
Child has been diagnosed with
Medical, developmental, or psychological problem
Autism spectrum disorder, Asperger’s, Pervasive developmental disorder (PDD) ADHD, ADD Behavior Problems Developmental delay Emotional or psychiatric problem Learning problem Intellectual disability (formerly mental retardation) Speech/language delay, communication problems Fine motor problem Gross motor problem Epilepsy, seizures Problems with coordination, ataxia Severe weakness or inability to tolerate exercise Tics/Tourette’s Toileting problem (problems toilet training, bedwetting, soiling) Genetic or chromosomal condition Anxiety, Obsessive-Compulsive Disorder (OCD) Bipolar disorder or mood swings Depression
Please list any other current medical disorders (e.g. cerebral palsy, Down syndrome, sickle cell, asthma):
Y N Has your child ever been prescribed medication(s) for the concerns or diagnoses checked off above?
If yes, please list medication(s) and dose(s) if possible
Approximate dates of use
Did this medication effectively treat your child’s problem(s)?
Y N Not sure
Y N Not sure
Y N Not sure
Y N Not sure
Y N Not sure
Y N Not sure
Y N Not sure
Y N Not sure
Web Version
ASC INTAKE QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 5
Y N Has your child ever received any mental health/counseling services?
If yes, please list type of service, provider’s name, and location/clinic
Approximate dates of service
Did this service effectively treat your child’s problem(s)?
Y N Not sure
Y N Not sure
Y N Not sure
Y N Not sure
Y N Not sure
Y N Is there anything else we should know about your child or your family?
___________________________________________________________________________________________
___________________________________________________________________________________________
___________________________________________________________________________________________
Parent/Guardian Sign Print Date Completed
Relationship to Patient
Web Version
CHILD AND FAMILY HISTORY QUESTIONNAIRE
Use Plate, Label, or Print:
Name:
CH MRN#:
DOB: Gender: M F
© Boston Children’s Hospital, 2014 All rights reserved 1
Child’s Name: Last First
Date of Birth: __________________________________ Gender (circle): M F
CHILD’S LIVING SITUATION Please list all those living in the child’s home: Name Relationship to
child Birthdate Highest grade or
degree completed Occupation (if applicable)
Are there any siblings not listed above? Y N If yes, please list names, ages, and where they live:
If one or both biological parents are not living in the home, how often does the child see the parent(s) not in the
home?
___________________________________________________________________________________________
Is there anything you would like us to know about the religious, spiritual, cultural beliefs, traditions, or practices of
your family or extended family?
___________________________________________________________________________________________
___________________________________________________________________________________________
Web Version
CHILD AND FAMILY HISTORY QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 2
CHILD’S BIRTH HISTORY Check if birth history is unknown
Age of mother at delivery: ______
Number of previous pregnancies (including miscarriages or terminations): _________
During pregnancy, did the mother: Y N Take prenatal vitamins
Y N Use tobacco If yes: how much?
Y N Drink alcohol If yes: how much?
Y N Take drugs or medications
If yes: what drug(s) or medication(s), and during which trimester(s):
Birth weight____________ Birth length ____________ Head circumference_________
Apgar score (if known): 1 minute ___ 5 minute ____
Was the baby born at term? Y N OR _____ number of weeks
Was the delivery vaginal cesarean (C-section)?
If cesarean, please describe why:
Were there any prenatal or neonatal complications? Y N
If yes, please describe:
Was a NICU or extended hospital stay required? Y N
If yes, please describe:
Was initial feeding formula breast milk
If breastfed, for how long? _______________
CHILD’S MEDICAL HISTORY
Check if child’s entire medical history is unknown Does the child have, or has the child ever had, any of the following DEVELOPMENTAL OR LEARNING PROBLEMS? Please describe or explain
Developmental delay or intellectual disability Y N Don’t know
Behavior problems Y N Don’t know
Attention or hyperactivity problems, ADHD, ADD Y N Don’t know
Autism spectrum disorder, Asperger’s, Pervasive Developmental Disorder (PDD)
Y N Don’t know
Learning problems, dyslexia Y N Don’t know
Speech or language delays Y N Don’t know
Web Version
CHILD AND FAMILY HISTORY QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 3
Does the child have, or has the child ever had, any of the following MENTAL HEALTH PROBLEMS? Please describe or explain
Anxiety, Obsessive-Compulsive Disorder, Post-Traumatic Stress Disorder Y N Don’t know
Attachment disorder Y N Don’t know
Depression Y N Don’t know
Suicidal thoughts or attempts Y N Don’t know
Bipolar disorder Y N Don’t know
Schizophrenia or psychosis Y N Don’t know
Does the child have, or has the child ever had any of the following CONGENITAL, METABOLIC, OR SENSORY PROBLEMS?
Please describe or explain
Down syndrome/Trisomy 21 Y N Don’t know
Other genetic or chromosomal disorder Y N Don’t know
Metabolic disorder Y N Don’t know
Frequent ear infections Y N Don’t know
Problems with ears or hearing Y N Don’t know
Problems with eyes or vision Y N Don’t know
Does the child have, or has the child ever had, any of the following NEUROLOGIC PROBLEMS? Please describe or explain
Frequent headaches, migraines Y N Don’t know
Head injury, concussion, loss of consciousness Y N Don’t know
Epilepsy, convulsions, or seizures Y N Don’t know
Tics or Tourette’s Y N Don’t know
Meningitis Y N Don’t know
Cerebral Palsy Y N Don’t know
Fine or gross motor delays Y N Don’t know
Does the child have, or has the child ever had, any of the following HEART (CARDIAC) PROBLEMS? Please describe or explain
Heart murmur Y N Don’t know
Heart rhythm problem, irregular heart rate, long QT syndrome, Wolff-Parkinson-White
Y N Don’t know
Congenital heart problem Y N Don’t know
Cardiomyopathy Y N Don’t know
Other (specify): Y N Don’t know
Web Version
CHILD AND FAMILY HISTORY QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 4
Does the child have, or has the child ever had, any of the following OTHER HEALTH PROBLEMS? Please describe or explain
Dental decay Y N Don’t know
Sleep problems, snoring, restless sleep, apnea Y N Don’t know
Allergies Y N Don’t know
Chronic or recurrent skins problems (e.g. eczema, acne) Y N Don’t know
Asthma, bronchitis, bronchiolitis, pneumonia Y N Don’t know
Overweight, obesity Y N Don’t know
Diabetes Y N Don’t know
Thyroid or other endocrine problems Y N Don’t know
Growth problems Y N Don’t know
Feeding problems Y N Don’t know
For
girls:
Age of first period (menses) Not applicable Age:
Problems with periods (menses) Not applicable Y N
Pregnancy Not applicable Y N
Daytime bowel or urine accidents (over age 5) Y N Don’t know
Nighttime bedwetting (over age 5) Y N Don’t know
Frequent abdominal pain Y N Don’t know
Constipation requiring doctor visits Y N Don’t know
Celiac disease Y N Don’t know
Kidney disease or urologic problem Y N Don’t know
Anemia or bleeding problem Y N Don’t know
Immune deficiency or HIV Y N Don’t know
Cancer Y N Don’t know
Joint disease, arthritis, rheumatologic
problem Y N Don’t know
Alcohol or drug use Y N Don’t know
Tobacco use Y N Don’t know
Other health problems (please specify):
Web Version
CHILD AND FAMILY HISTORY QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 5
Has the child ever experienced any of the following? If yes, when and where? Hospitalized overnight Y N Don’t know
Surgery Y N Don’t know
Injuries, fractures, ingestions Y N Don’t know
Elevated lead level Y N Don’t know
Family violence Y N Don’t know
Has the child ever had any of the following screening/diagnostic tests or procedures?
If yes, when, where, and results? (Please send in copies of results if available)
Genetic testing Y N Don’t know
EEG Y N Don’t know
CT scan or MRI of the head Y N Don’t know
Sleep study Y N Don’t know
Hearing test Y N Don’t know
Vision test Y N Don’t know
BIRTH (BIOLOGICAL) FAMILY MEDICAL HISTORY
Check if the entire birth family history is unknown
Are there any birth family members who have had any the following DEVELOPMENTAL OR LEARNING PROBLEMS?
If yes: please indicate who and whether on mother’s or father’s side of the family
Developmental disability or intellectual disability Y N Don’t know
Attention or hyperactivity problems, ADHD, ADD Y N Don’t know
Autism spectrum disorder, Asperger’s, Pervasive Developmental Disorder (PDD)
Y N Don’t know
Learning problems, dyslexia Y N Don’t know
Speech or language problems Y N Don’t know
Are there any birth family members who have had any the following MENTAL HEALTH PROBLEMS?
If yes: please indicate who and whether on mother’s or father’s side of the family
Anxiety, Obsessive-Compulsive Disorder, Post-Traumatic Stress Disorder Y N Don’t know
Depression Y N Don’t know
Suicide or attempted suicide Y N Don’t know
Bipolar disorder Y N Don’t know
Schizophrenia or psychosis Y N Don’t know
Other (please specify): Y N Don’t know
Web Version
CHILD AND FAMILY HISTORY QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 6
Are there any birth family members who have had any of the following CONGENITAL, METABOLIC, OR SENSORY PROBLEMS?
If yes: please indicate who and whether on mother’s or father’s side of the family
Down syndrome/Trisomy 21 Y N Don’t know
Other genetic or chromosomal disorder Y N Don’t know
Metabolic disorder Y N Don’t know
Childhood hearing loss Y N Don’t know
Visual impairment Y N Don’t know
Other (please specify):
Are there any birth family members who have had any of the following NEUROLOGIC PROBLEMS?
If yes: please indicate who and whether on mother’s or father’s side of the family
Frequent headaches, migraines Y N Don’t know
Epilepsy, convulsions, or seizures Y N Don’t know
Tics or Tourette’s Y N Don’t know
Dementia or Alzheimer’s Y N Don’t know
Other (please specify):
Are there any birth family members who had had any of the following HEART-RELATED (CARDIAC) PROBLEMS?
If yes: please indicate who and whether on mother’s or father’s side of the family
Heart disease (before 55 years old) Y N Don’t know
Heart rhythm problem, irregular heart beats, long QT syndrome, Wolff-Parkinson-White
Y N Don’t know
Hypertrophic cardiomyopathy Y N Don’t know
High cholesterol or takes cholesterol medication
Y N Don’t know
High blood pressure Y N Don’t know
Sudden unexplained death Y N Don’t know
Marfan syndrome Y N Don’t know
Other (please specify):
Web Version
CHILD AND FAMILY HISTORY QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 7
Are there any birth family members who have had any of the following OTHER HEALTH PROBLEMS?
If yes: please indicate who and whether on mother’s or father’s side of the family
Allergies Y N Don’t know
Immune problems, HIV, or AIDS Y N Don’t know
Asthma Y N Don’t know
Obstructive sleep apnea Y N Don’t know
Cancer (before 55 years old) Y N Don’t know
Overweight, obesity Y N Don’t know
Diabetes Y N Don’t know
Thyroid or other endocrine problems Y N Don’t know
Growth problems Y N Don’t know
Liver disease Y N Don’t know
Kidney or bladder disease Y N Don’t know
Bedwetting (after 5 years old) Y N Don’t know
Muscle disease (e.g. Duchenne) Y N Don’t know
Alcohol or drug use Y N Don’t know
Tobacco use Y N Don’t know
Other health problem (please specify):
Web Version
CHILD AND FAMILY HISTORY QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 8
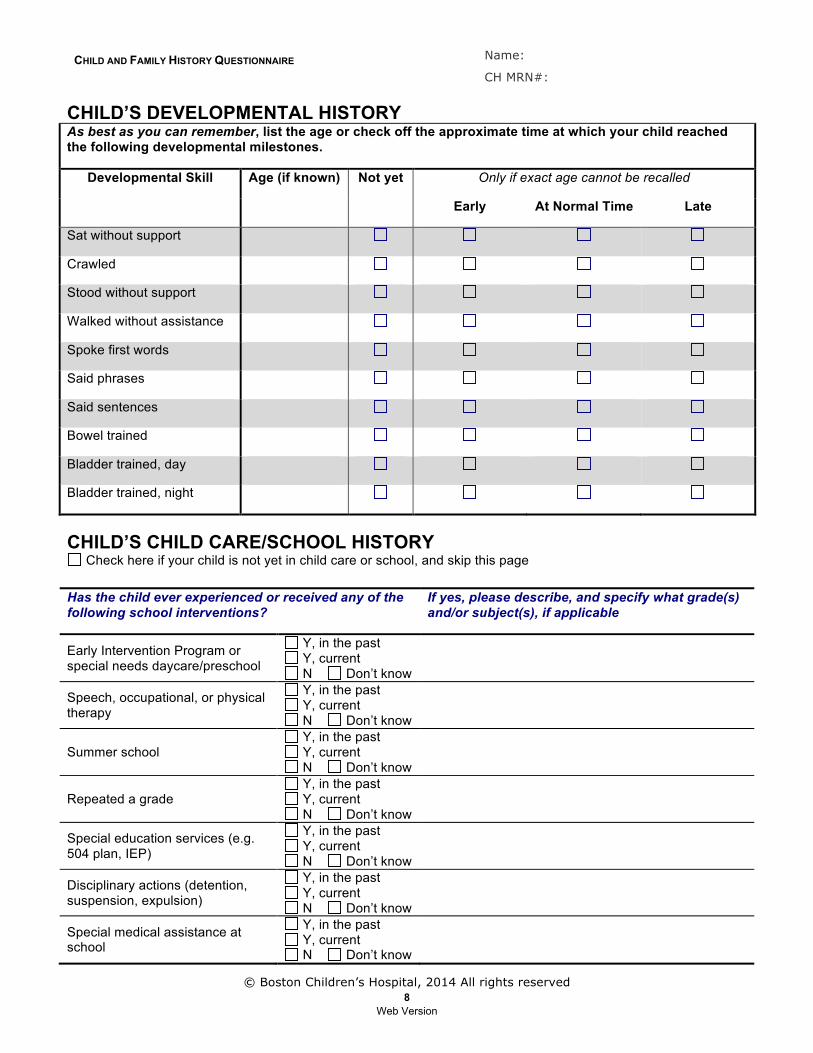
CHILD’S DEVELOPMENTAL HISTORY As best as you can remember, list the age or check off the approximate time at which your child reached the following developmental milestones.
Developmental Skill Age (if known) Not yet Only if exact age cannot be recalled
Early At Normal Time Late
Sat without support
Crawled
Stood without support
Walked without assistance
Spoke first words
Said phrases
Said sentences
Bowel trained
Bladder trained, day
Bladder trained, night
CHILD’S CHILD CARE/SCHOOL HISTORY
Check here if your child is not yet in child care or school, and skip this page Has the child ever experienced or received any of the following school interventions?
If yes, please describe, and specify what grade(s) and/or subject(s), if applicable
Early Intervention Program or special needs daycare/preschool
Y, in the past Y, current N Don’t know
Speech, occupational, or physical therapy
Y, in the past Y, current N Don’t know
Summer school Y, in the past Y, current N Don’t know
Repeated a grade Y, in the past Y, current N Don’t know
Special education services (e.g. 504 plan, IEP)
Y, in the past Y, current N Don’t know
Disciplinary actions (detention, suspension, expulsion)
Y, in the past Y, current N Don’t know
Special medical assistance at school
Y, in the past Y, current N Don’t know
Web Version
CHILD AND FAMILY HISTORY QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 9
HISTORY OF SCHOOL PROBLEMS: Please describe any problems that occurred during each of the following grades
Academics Behavior
Preschool
Kindergarten, first grade
Second and third grades
Fourth and fifth grades
Sixth through eighth grade
High School
Parent/Guardian Sign Print Date Completed
Relationship to Patient
Web Version
CURRENT FUNCTIONING UNDER 5
Use Plate, Label, or Print:
Name:
CH MRN#:
DOB: Gender: M F
© Boston Children’s Hospital, 2014 All rights reserved 1
Child’s Name: Last First
Date of Birth: __________________________________ Gender (circle): M F CHILD’S GENERAL HEALTH When was the child’s last visit with his or her primary care provider? ______________________
Y N Has the child seen a dentist in the last year? Y N Are the child’s immunizations up to date?
CHILD’S MEDICATIONS
Child does not take any medications Name of medication Strength Dose Frequency, when
given Comments
Example: Concerta 36 mg 1 tablet Once each morning
Only on school days
Does the child currently take or use any of the following:
Vitamins (list):
Herbal preparations (list):
Dietary supplements (e.g. melatonin, omega 3) (list):
Special diets (describe):
CHILD’S ALLERGIES Please list any FOODS or MEDICATIONS to which the child has an allergy:
Child does not have any known allergies to foods or medications
Food or medication Describe reaction Example: amoxicillin Rash
Web Version
CURRENT FUNCTIONING UNDER 5 Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 2
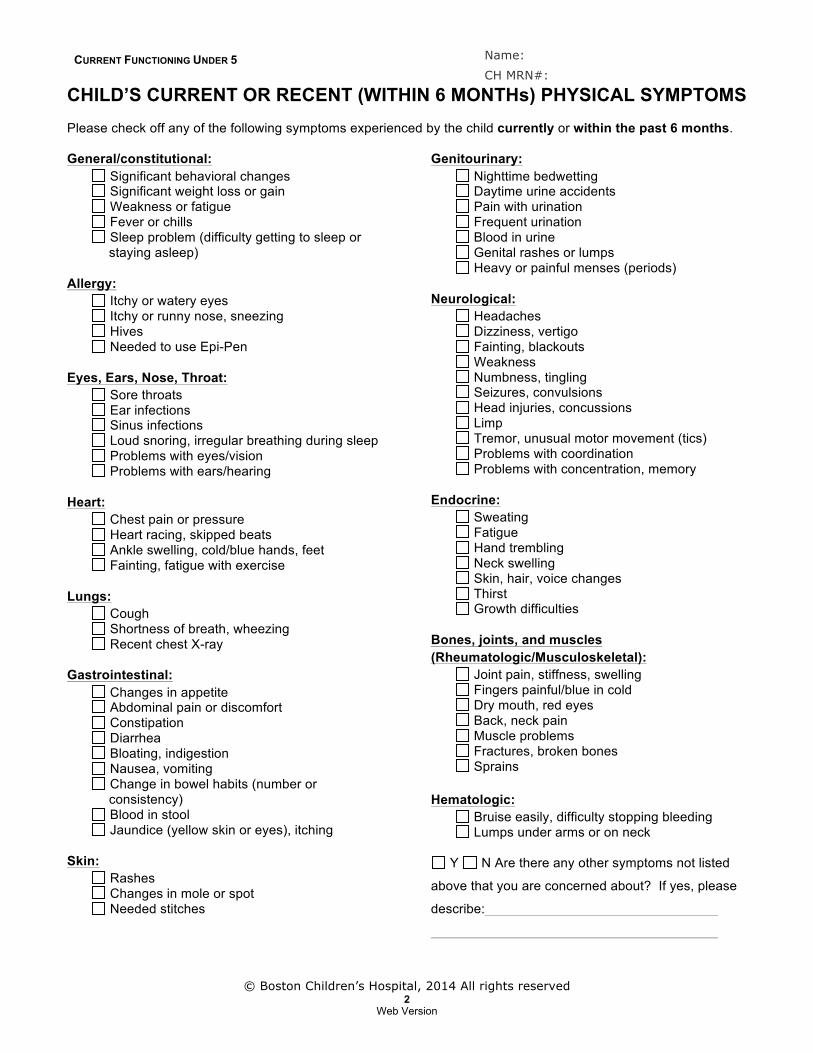
CHILD’S CURRENT OR RECENT (WITHIN 6 MONTHs) PHYSICAL SYMPTOMS Please check off any of the following symptoms experienced by the child currently or within the past 6 months. General/constitutional:
Significant behavioral changes Significant weight loss or gain Weakness or fatigue Fever or chills Sleep problem (difficulty getting to sleep or
staying asleep) Allergy:
Itchy or watery eyes Itchy or runny nose, sneezing Hives Needed to use Epi-Pen
Eyes, Ears, Nose, Throat:
Sore throats Ear infections Sinus infections Loud snoring, irregular breathing during sleep Problems with eyes/vision Problems with ears/hearing
Heart:
Chest pain or pressure Heart racing, skipped beats Ankle swelling, cold/blue hands, feet Fainting, fatigue with exercise
Lungs:
Cough Shortness of breath, wheezing Recent chest X-ray
Gastrointestinal:
Changes in appetite Abdominal pain or discomfort Constipation Diarrhea Bloating, indigestion Nausea, vomiting Change in bowel habits (number or
consistency) Blood in stool Jaundice (yellow skin or eyes), itching
Skin:
Rashes Changes in mole or spot Needed stitches
Genitourinary:
Nighttime bedwetting Daytime urine accidents Pain with urination Frequent urination Blood in urine Genital rashes or lumps Heavy or painful menses (periods)
Neurological:
Headaches Dizziness, vertigo Fainting, blackouts Weakness Numbness, tingling Seizures, convulsions Head injuries, concussions Limp Tremor, unusual motor movement (tics) Problems with coordination Problems with concentration, memory
Endocrine:
Sweating Fatigue Hand trembling Neck swelling Skin, hair, voice changes Thirst Growth difficulties
Bones, joints, and muscles (Rheumatologic/Musculoskeletal):
Joint pain, stiffness, swelling Fingers painful/blue in cold Dry mouth, red eyes Back, neck pain Muscle problems Fractures, broken bones Sprains
Hematologic:
Bruise easily, difficulty stopping bleeding Lumps under arms or on neck
Y N Are there any other symptoms not listed
above that you are concerned about? If yes, please
describe:
Web Version
CURRENT FUNCTIONING UNDER 5 Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 3
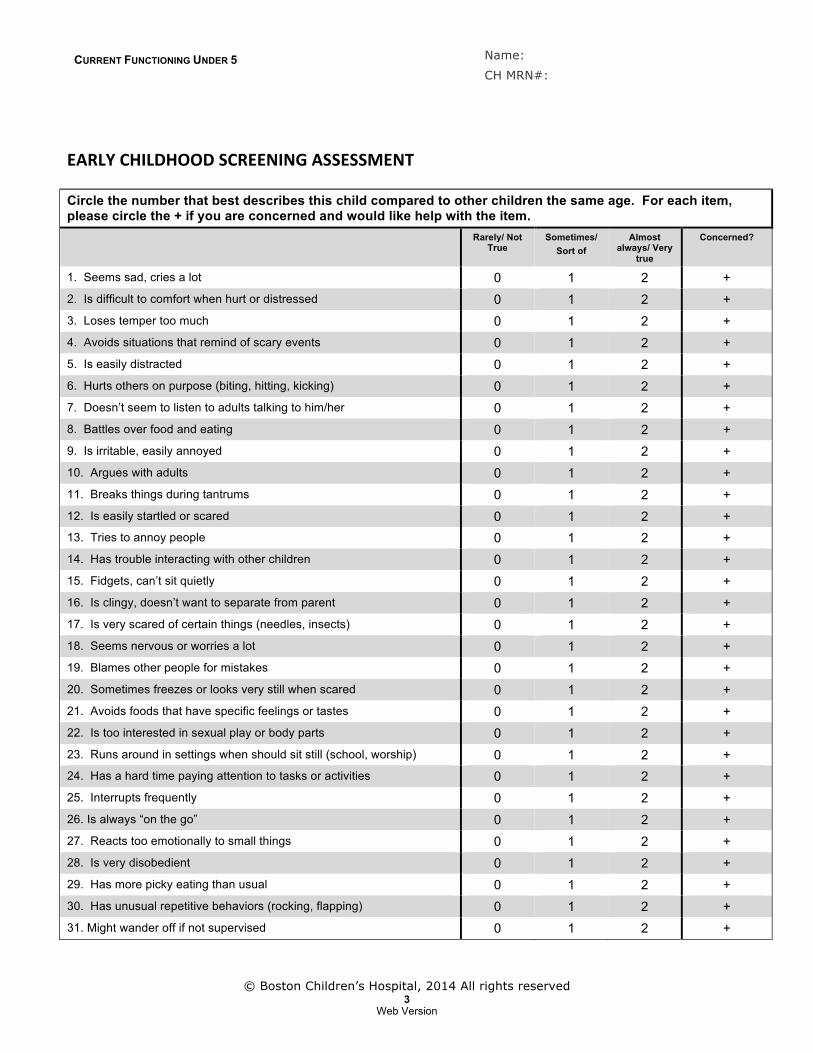
EARLY CHILDHOOD SCREENING ASSESSMENT Circle the number that best describes this child compared to other children the same age. For each item, please circle the + if you are concerned and would like help with the item.
Rarely/ Not True
Sometimes/ Sort of
Almost always/ Very
true
Concerned?
1. Seems sad, cries a lot 0 1 2 + 2. Is difficult to comfort when hurt or distressed 0 1 2 + 3. Loses temper too much 0 1 2 + 4. Avoids situations that remind of scary events 0 1 2 + 5. Is easily distracted 0 1 2 + 6. Hurts others on purpose (biting, hitting, kicking) 0 1 2 + 7. Doesn’t seem to listen to adults talking to him/her 0 1 2 + 8. Battles over food and eating 0 1 2 + 9. Is irritable, easily annoyed 0 1 2 + 10. Argues with adults 0 1 2 + 11. Breaks things during tantrums 0 1 2 + 12. Is easily startled or scared 0 1 2 + 13. Tries to annoy people 0 1 2 + 14. Has trouble interacting with other children 0 1 2 + 15. Fidgets, can’t sit quietly 0 1 2 + 16. Is clingy, doesn’t want to separate from parent 0 1 2 + 17. Is very scared of certain things (needles, insects) 0 1 2 + 18. Seems nervous or worries a lot 0 1 2 + 19. Blames other people for mistakes 0 1 2 + 20. Sometimes freezes or looks very still when scared 0 1 2 + 21. Avoids foods that have specific feelings or tastes 0 1 2 + 22. Is too interested in sexual play or body parts 0 1 2 + 23. Runs around in settings when should sit still (school, worship) 0 1 2 + 24. Has a hard time paying attention to tasks or activities 0 1 2 + 25. Interrupts frequently 0 1 2 + 26. Is always “on the go” 0 1 2 + 27. Reacts too emotionally to small things 0 1 2 + 28. Is very disobedient 0 1 2 + 29. Has more picky eating than usual 0 1 2 + 30. Has unusual repetitive behaviors (rocking, flapping) 0 1 2 + 31. Might wander off if not supervised 0 1 2 +
Web Version
CURRENT FUNCTIONING UNDER 5 Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 4
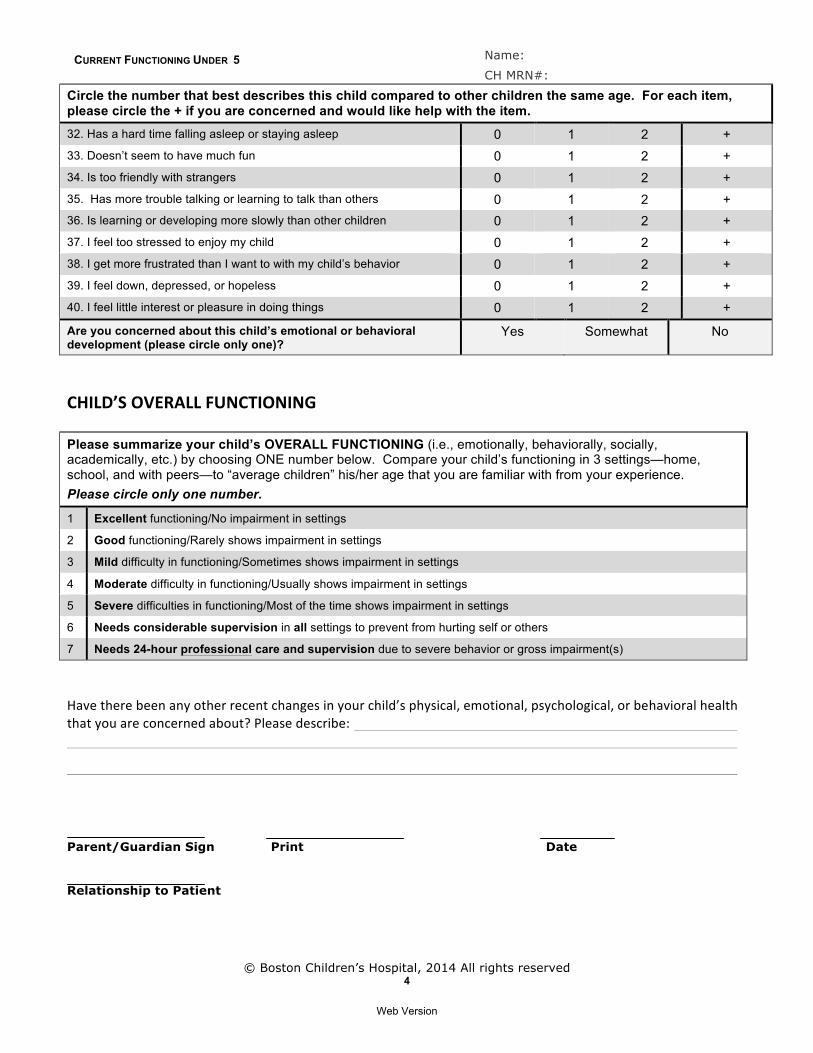
Circle the number that best describes this child compared to other children the same age. For each item, please circle the + if you are concerned and would like help with the item. 32. Has a hard time falling asleep or staying asleep 0 1 2 + 33. Doesn’t seem to have much fun 0 1 2 + 34. Is too friendly with strangers 0 1 2 + 35. Has more trouble talking or learning to talk than others 0 1 2 + 36. Is learning or developing more slowly than other children 0 1 2 + 37. I feel too stressed to enjoy my child 0 1 2 + 38. I get more frustrated than I want to with my child’s behavior 0 1 2 + 39. I feel down, depressed, or hopeless 0 1 2 + 40. I feel little interest or pleasure in doing things 0 1 2 + Are you concerned about this child’s emotional or behavioral development (please circle only one)?
Yes Somewhat No
CHILD’S OVERALL FUNCTIONING Please summarize your child’s OVERALL FUNCTIONING (i.e., emotionally, behaviorally, socially, academically, etc.) by choosing ONE number below. Compare your child’s functioning in 3 settings—home, school, and with peers—to “average children” his/her age that you are familiar with from your experience. Please circle only one number.
1 Excellent functioning/No impairment in settings
2 Good functioning/Rarely shows impairment in settings
3 Mild difficulty in functioning/Sometimes shows impairment in settings
4 Moderate difficulty in functioning/Usually shows impairment in settings
5 Severe difficulties in functioning/Most of the time shows impairment in settings
6 Needs considerable supervision in all settings to prevent from hurting self or others
7 Needs 24-hour professional care and supervision due to severe behavior or gross impairment(s)
Have there been any other recent changes in your child’s physical, emotional, psychological, or behavioral health that you are concerned about? Please describe:
Parent/Guardian Sign Print Date Relationship to Patient
Web Version
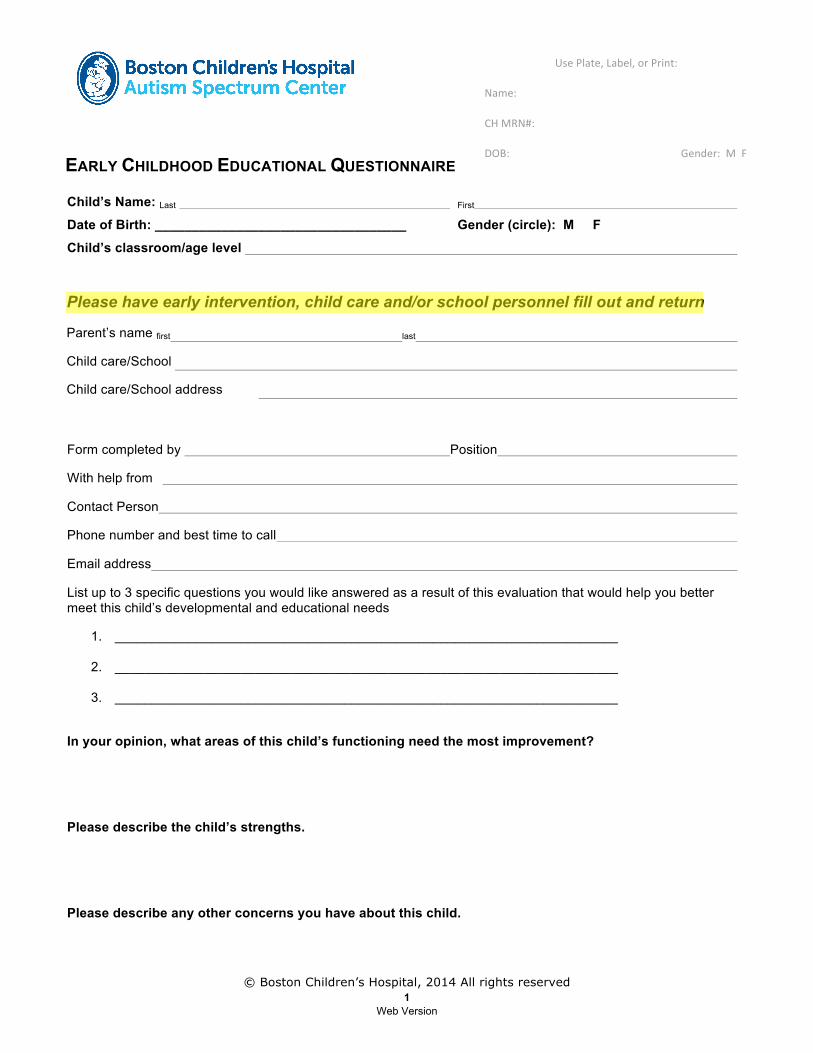
EARLY CHILDHOOD EDUCATIONAL QUESTIONNAIRE
Use Plate, Label, or Print:
Name:
CH MRN#:
DOB: Gender: M F
© Boston Children’s Hospital, 2014 All rights reserved 1
Child’s Name: Last First
Date of Birth: __________________________________ Gender (circle): M F
Child’s classroom/age level
Please have early intervention, child care and/or school personnel fill out and return
Parent’s name first last
Child care/School
Child care/School address
Form completed by Position
With help from
Contact Person
Phone number and best time to call
Email address
List up to 3 specific questions you would like answered as a result of this evaluation that would help you better meet this child’s developmental and educational needs
1. ____________________________________________________________________
2. ____________________________________________________________________
3. ____________________________________________________________________
In your opinion, what areas of this child’s functioning need the most improvement?
Please describe the child’s strengths.
Please describe any other concerns you have about this child.
Web Version
PRE K SCHOOL QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 2
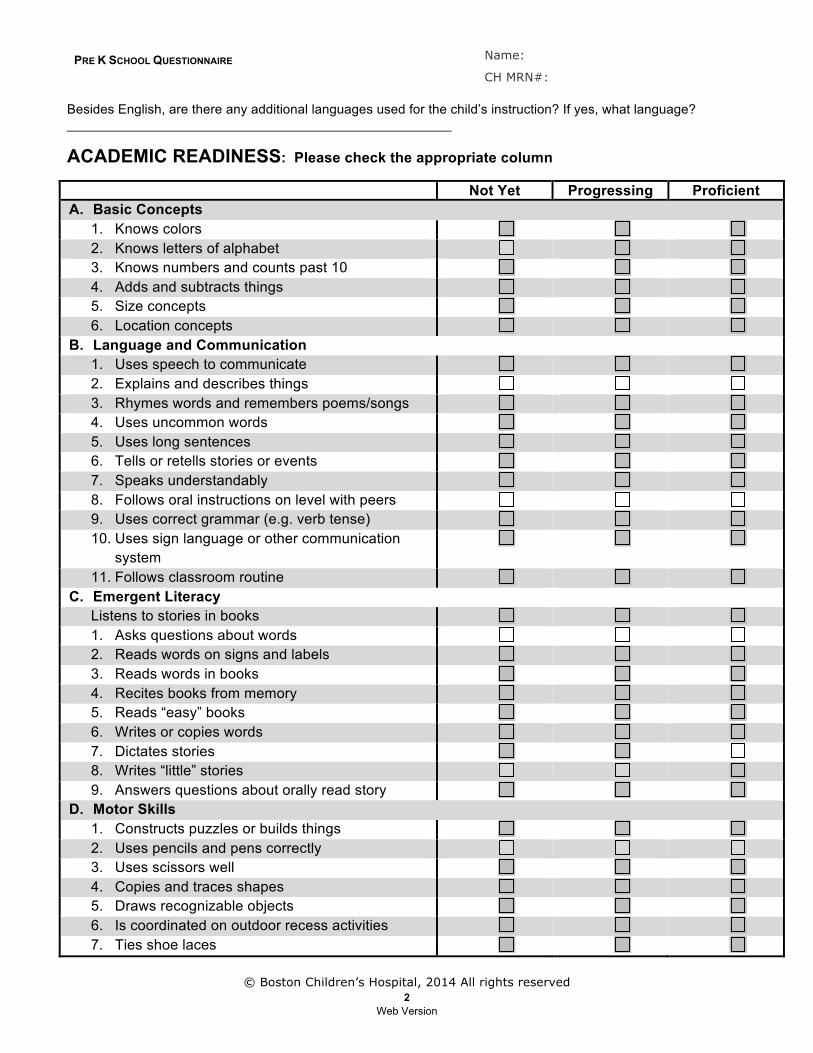
Besides English, are there any additional languages used for the child’s instruction? If yes, what language? ____________________________________________________
ACADEMIC READINESS: Please check the appropriate column
Not Yet Progressing Proficient A. Basic Concepts
1. Knows colors 2. Knows letters of alphabet 3. Knows numbers and counts past 10 4. Adds and subtracts things 5. Size concepts 6. Location concepts
B. Language and Communication 1. Uses speech to communicate 2. Explains and describes things 3. Rhymes words and remembers poems/songs 4. Uses uncommon words 5. Uses long sentences 6. Tells or retells stories or events 7. Speaks understandably 8. Follows oral instructions on level with peers 9. Uses correct grammar (e.g. verb tense) 10. Uses sign language or other communication
system
11. Follows classroom routine C. Emergent Literacy
Listens to stories in books 1. Asks questions about words 2. Reads words on signs and labels 3. Reads words in books 4. Recites books from memory 5. Reads “easy” books 6. Writes or copies words 7. Dictates stories 8. Writes “little” stories 9. Answers questions about orally read story
D. Motor Skills 1. Constructs puzzles or builds things 2. Uses pencils and pens correctly 3. Uses scissors well 4. Copies and traces shapes 5. Draws recognizable objects 6. Is coordinated on outdoor recess activities 7. Ties shoe laces
Web Version
PRE K SCHOOL QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 3
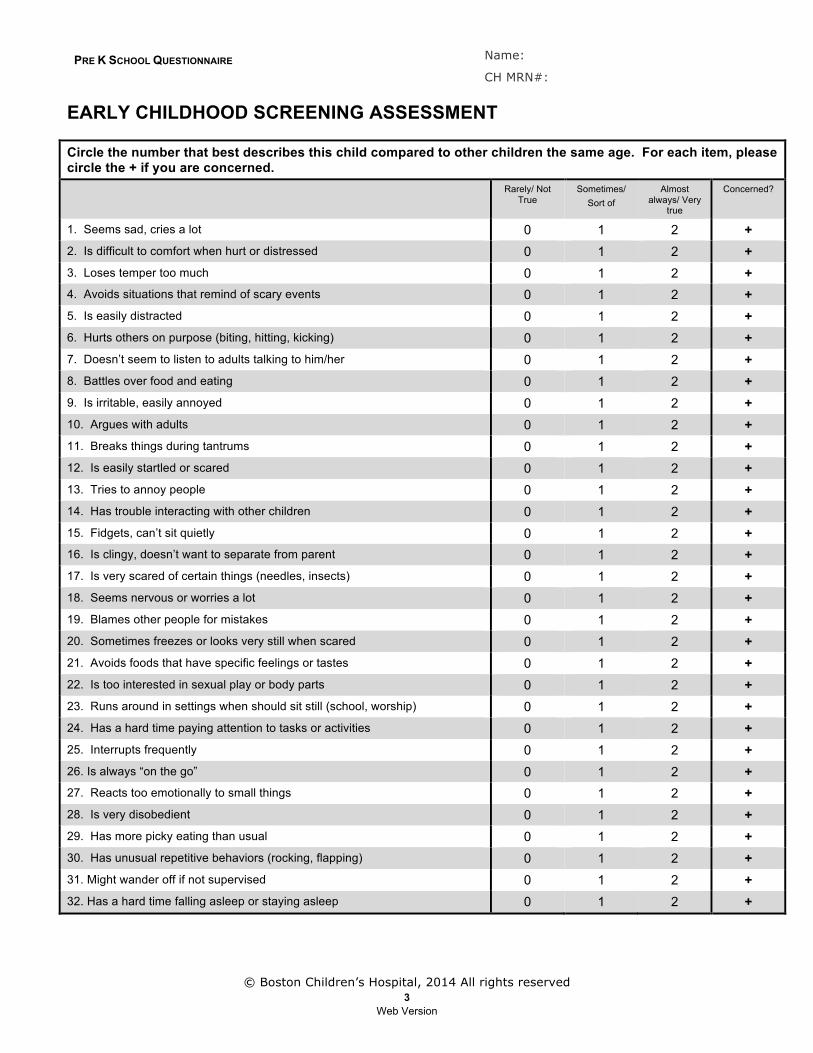
EARLY CHILDHOOD SCREENING ASSESSMENT
Circle the number that best describes this child compared to other children the same age. For each item, please circle the + if you are concerned.
Rarely/ Not True
Sometimes/ Sort of
Almost always/ Very
true
Concerned?
1. Seems sad, cries a lot 0 1 2 + 2. Is difficult to comfort when hurt or distressed 0 1 2 + 3. Loses temper too much 0 1 2 + 4. Avoids situations that remind of scary events 0 1 2 + 5. Is easily distracted 0 1 2 + 6. Hurts others on purpose (biting, hitting, kicking) 0 1 2 + 7. Doesn’t seem to listen to adults talking to him/her 0 1 2 + 8. Battles over food and eating 0 1 2 + 9. Is irritable, easily annoyed 0 1 2 + 10. Argues with adults 0 1 2 + 11. Breaks things during tantrums 0 1 2 + 12. Is easily startled or scared 0 1 2 + 13. Tries to annoy people 0 1 2 + 14. Has trouble interacting with other children 0 1 2 + 15. Fidgets, can’t sit quietly 0 1 2 + 16. Is clingy, doesn’t want to separate from parent 0 1 2 + 17. Is very scared of certain things (needles, insects) 0 1 2 + 18. Seems nervous or worries a lot 0 1 2 + 19. Blames other people for mistakes 0 1 2 + 20. Sometimes freezes or looks very still when scared 0 1 2 + 21. Avoids foods that have specific feelings or tastes 0 1 2 + 22. Is too interested in sexual play or body parts 0 1 2 + 23. Runs around in settings when should sit still (school, worship) 0 1 2 + 24. Has a hard time paying attention to tasks or activities 0 1 2 + 25. Interrupts frequently 0 1 2 + 26. Is always “on the go” 0 1 2 + 27. Reacts too emotionally to small things 0 1 2 + 28. Is very disobedient 0 1 2 + 29. Has more picky eating than usual 0 1 2 + 30. Has unusual repetitive behaviors (rocking, flapping) 0 1 2 + 31. Might wander off if not supervised 0 1 2 + 32. Has a hard time falling asleep or staying asleep 0 1 2 +
Web Version
PRE K SCHOOL QUESTIONNAIRE Name:
CH MRN#:
© Boston Children’s Hospital, 2014 All rights reserved 4
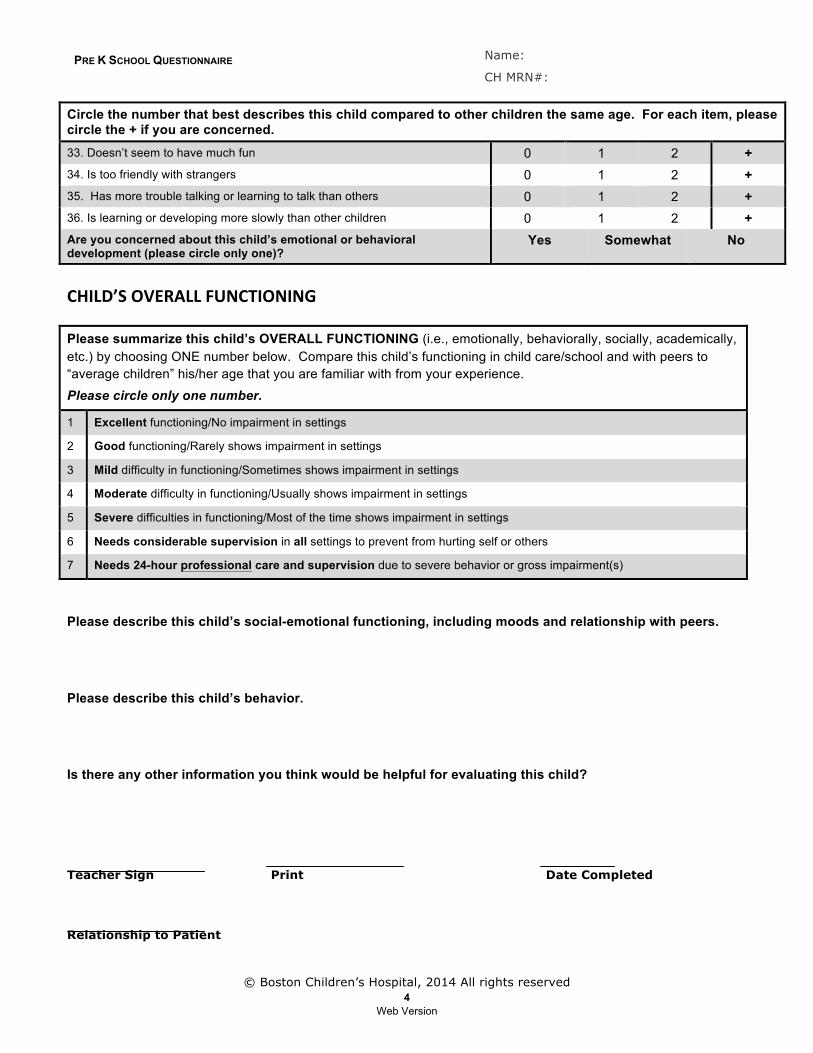
Circle the number that best describes this child compared to other children the same age. For each item, please circle the + if you are concerned. 33. Doesn’t seem to have much fun 0 1 2 + 34. Is too friendly with strangers 0 1 2 + 35. Has more trouble talking or learning to talk than others 0 1 2 + 36. Is learning or developing more slowly than other children 0 1 2 + Are you concerned about this child’s emotional or behavioral development (please circle only one)?
Yes Somewhat No
CHILD’S OVERALL FUNCTIONING Please summarize this child’s OVERALL FUNCTIONING (i.e., emotionally, behaviorally, socially, academically, etc.) by choosing ONE number below. Compare this child’s functioning in child care/school and with peers to “average children” his/her age that you are familiar with from your experience. Please circle only one number.
1 Excellent functioning/No impairment in settings
2 Good functioning/Rarely shows impairment in settings
3 Mild difficulty in functioning/Sometimes shows impairment in settings
4 Moderate difficulty in functioning/Usually shows impairment in settings
5 Severe difficulties in functioning/Most of the time shows impairment in settings
6 Needs considerable supervision in all settings to prevent from hurting self or others
7 Needs 24-hour professional care and supervision due to severe behavior or gross impairment(s)
Please describe this child’s social-emotional functioning, including moods and relationship with peers. Please describe this child’s behavior. Is there any other information you think would be helpful for evaluating this child?
Teacher Sign Print Date Completed
Relationship to Patient
Web Version