technical assistance to the government of … · figure 8: monitoring ... t l e v e l senior...
TRANSCRIPT

KINGDOM OF LESOTHO
TECHNICAL ASSISTANCE TO THE GOVERNMENT OF LESOTHO
FOR CAPACITY BUILDING, SKILLS TRANSFERS, SCALE UP AND
TRANSITIONAL ARRANGEMENTS UNDER THE LESOTHO
CHILD GRANTS PROGRAMME
CONDITIONAL CASH TRANSFER PILOT
OPERATIONS MANUAL
DECEMBER 2014
PREPARED FOR:
GOVERNMENT OF LESOTHO AND UNICEF
PREPARED BY:
AYALA CO
EUROPEAN UNION
The Lesotho Child Grants Programme
CCT Operations Manual
LIST OF ACRONYMS
ASWO Auxiliary Social WelfareOfficer
CC Community Council
CCT Conditional Cash Transfer
CGP Child Grants Programme
CGP-CCT Child Grants Programme Conditional Cash Transfer
CGP-OU Child Grants Programme Operation Unit
CHAL Christian Health Association of Lesotho
CM Case Management
IEC Information, Education and Communication
HHs Household
M Maloti
M&E Monitoring and Evaluation
MIS Management Information System
MOET Ministry of Education and Training
MOH Ministry of Health
MOSD Ministry of Social Development
OM Operations Manual
SCE Supply Capacity Evaluation
TA Technical Annex
UNICEF United Nations Children’s Fund

The Lesotho Child Grants Programme
CCT Operations Manual
VAC Village Assistance Committees
The Lesotho Child Grants Programme
CCT Operations Manual
TABLE OF CONTENTS
I. INTRODUCTION............................................................................................................ 1
A. OBJECTIVES OF THE PILOT ..................................................................................... 1
B. PURPOSE OF THE OPERATIONS MANUAL ........................................................... 2
C. KEY COMPONENTS OF THE OPERATIONS MANUAL ......................................... 3
II. STAKEHOLDER’S ROLES AND RESPONSIBILITIES .......................................... 4
A. MINISTRY OF SOCIAL DEVELOPMENT (MOSD) .................................................. 5
B. IMPLEMENTATION PARTNERS: MINISTRY OF HEALTH,MINISTRY OF
EDUCATION AND TRAINING AND CHRISTIAN HEALTH ASSOCIATION OF
LESOTHO ........................................................................................................................... 13
C. UNITED NATIONS CHILDREN’S FUND ................................................................ 15
D. LOCAL AUTHORITIES ............................................................................................. 15
E. VILLAGE ASSISTANCE COMMITTEES ................................................................ 15
F. PAYMENT AGENCIES .............................................................................................. 16
G. BENEFICIARY HOUSEHOLDS ................................................................................ 16
III. DESIGN PARAMETERS ............................................................................................. 17
A. ELIGIBILITY CRITERIA ........................................................................................... 17
B. CONDITIONALITIES/CO-RESPONSIBILITIES AND PENALTIES FOR NON-
COMPLIANCE.................................................................................................................... 18
C. PAYMENTS, FREQUENCY OF PAYMENTS AND DELIVERY MECHANISM .. 21
D. DURATION & EXIT POLICY .................................................................................... 21
IV. PROCESS CYCLE ........................................................................................................ 22
A. SUPPLY CAPACITY EVALUATION ....................................................................... 22
B. ENROLMENT ............................................................................................................. 27
C. MONITORING OF CONDITIONALITIES/CO-RESPONSIBILITIES ..................... 34
D. PAYMENTS ................................................................................................................ 36
E. CASE MANAGEMENT .............................................................................................. 40
V. MONITORING AND EVALUATION ........................................................................ 46

The Lesotho Child Grants Programme
CCT Operations Manual
LIST OF FIGURES
Figure 1: Stakeholders in the Implementation of the CCT Pilot ............................................... 5
Figure 2: Pilot Project Cycle .................................................................................................... 22
Figure 3: Flow Chart of the Supply Capacity Evaluation Process .......................................... 23
Figure 4: Flow Chart of the Enrolment Process....................................................................... 28
Figure 5: Flow Chart of the Compliance Monitoring Process ................................................. 34
Figure 6: Flow Chart of the Payments Process ........................................................................ 38
Figure 7: Flow Chart of the Case Management Process .......................................................... 41
Figure 8: Monitoring & Evaluation throughout the Programme Cycle ................................... 46
LIST OF TABLES
Table 1: Treatment Groups and Payment Penalties for Non-Compliance ............................... 19
Table 2: Payments Design Parameters ..................................................................................... 21

The Lesotho Child Grants Programme
CCT Operations Manual
1
I. INTRODUCTION
The Child Grants Programme (CGP) is the current unconditional cash transfer program
implemented by the Ministry of Social Development (MOSD) and directed to extremely poor
and poor households that care for children under 18 years old. The program was initiated in
2007 and it is now operating in all 10 districts of Lesotho. A monthly grant is paid out to
households (HHs) quarterly, and is intended to be used for improving children’s human
capital. However, while the grant is intended to be used for the children’s education and
health, the beneficiary HHs are not monitored in this respect. In order to promote better
investments in human capital, the MOSD decided to implement a Conditional Cash Transfer
(CCT) pilot,a programme operating within the CGP framework but directly linking its cash
transfers to beneficiary children’s usage of education and health services.
The CCT pilot is to be implemented in six community councils (CCs) in three districts.The
pilot implementsfour different treatment groups (with slightly different design parameters).
The education and health conditionality are the same across the six CCs and the fulfilment of
conditionalitiesis monitored for all the beneficiary HHs; however, the link between
conditionalities, payments and case management sets each treatment group aside.
The first treatment group has CCT-specific elements added to the current CGP case
management system: a beneficiary HH failing to meet its conditionsis subject to intense case
management through a specialized Officer and it doesnot suffer any penalties. This intense
case management involves the use of home visits if the household is non-compliant. The
second treatment group has CCT-specific elements added to the CGP payment system: a
beneficiary HH failing to meet its compliancesis subject to incremental penalties levied on
the grant amount. The third treatment group implements a combination of the two previous
interventions: a beneficiary HH failing to meet its conditionsis subject first to intense case
management and then to incremental penalties. The fourth treatment group is monitored
against fulfilment of conditionalities but HHs do not have any penalties levied nor receive
any intense case management. This group is run as the normal CGP as implemented in non-
CCT pilot districts.
A. OBJECTIVES OF THE PILOT
The Lesotho Child Grants Programme
CCT Operations Manual
2
The CCT pilot tests an alternative CGP design which introduces beneficiary
conditionalities/co-responsibilities linked to cash transfers:The main objective of this CGP-
CCT pilot is to encourage participation and expand the use of health and educational services
by poor segments of the population yet to benefit from the advances made by the CGP.
In terms of outcomes, the specific objectives of this programme are to tackle the following
indicators:
1. Education
The education componentaims to:
Improve timely entry into Grade 1;
Decrease drop-out rates;
Increase regular attendance and retention in higher grades; and
Strengthen primary completion.
2. Health
The health component aims to:
Increase number of visits of under 5 year olds to health centres;
Increase immunization rates for under five year olds; and
Prevent prevalence of childhood illnesses.
In addition, the CCT pilot’s secondary objective is to build capacity in MOSD: itnot only
informs the design of other social safety nets in Lesotho by testing innovative operational
mechanisms and various institutional arrangementsbut, if needed, italso allows easy scaling
up of the pilot by having identified the required instruments and institutional arrangements.
B. PURPOSE OF THE OPERATIONS MANUAL
The Operations Manual (OM) provides a summary of all the CGP-CCT processes and serves
the following purposes:
Enable stakeholders to understand the scope, content, organisation, and activities of
the programme;
Describe thoroughly the design parameters and the project cycle;
Provide guidelines for each process within the project cycle; and
The Lesotho Child Grants Programme
CCT Operations Manual
3
Ensure that the requirements for transparency, equity, compliance and accountability
are met.
The OM has been prepared mainly for use by all entities and stakeholders directly involved in
the implementation and administration of the pilot, namely:
The Government of Lesotho;
o Ministry of Social Development;
o Ministry of Health (MOH);
o Ministry of Education and Training (MOET);
o Local Government Authorities;
Christian Health Association of Lesotho (CHAL);
United Nations Children’s Fund (UNICEF);
Village Assistance Committees (VAC); and
All Contracted Entities involved in project implementation
C. KEY COMPONENTS OF THE OPERATIONS MANUAL
The OM is complemented by five (5) Technical Annexes (TAs) which provide detailed
operational procedures along with roles and responsibilities of stakeholders for each process
to ensure proper implementation. The TAs are:
Annex A: Supply Capacity Evaluation
Annex B: Enrolment
Annex C: Monitoring of Conditionalities and Co-Responsibilities
Annex D: Case Management
Annex E: Monitoring and Evaluation
The TAs are accompanied by guidelines describing the method for completing forms relevant
to each process, and the procedures to be carried out at the field level, and training material.
The remainder of the manual is organised into the following sections:
SectionII – Stakeholder’s roles and responsibilities;
Section III - Design Parameters;
Section IV – Process Cycle; and
SectionV – Monitoring and Evaluation.

The Lesotho Child Grants Programme
CCT Operations Manual
4
II. STAKEHOLDER’S ROLES AND RESPONSIBILITIES
The implementation of the CCT pilot is led by the Ministry of Social Development through
the CGP Operations Unit (CGP-OU). The MOSD works with various stakeholders in
implementing the programme:
Implementation Partners: MOH, MOET, CHAL;
UNICEF;
Local Authorities;
VACs;
Payment Agencies; and
Beneficiary Households.
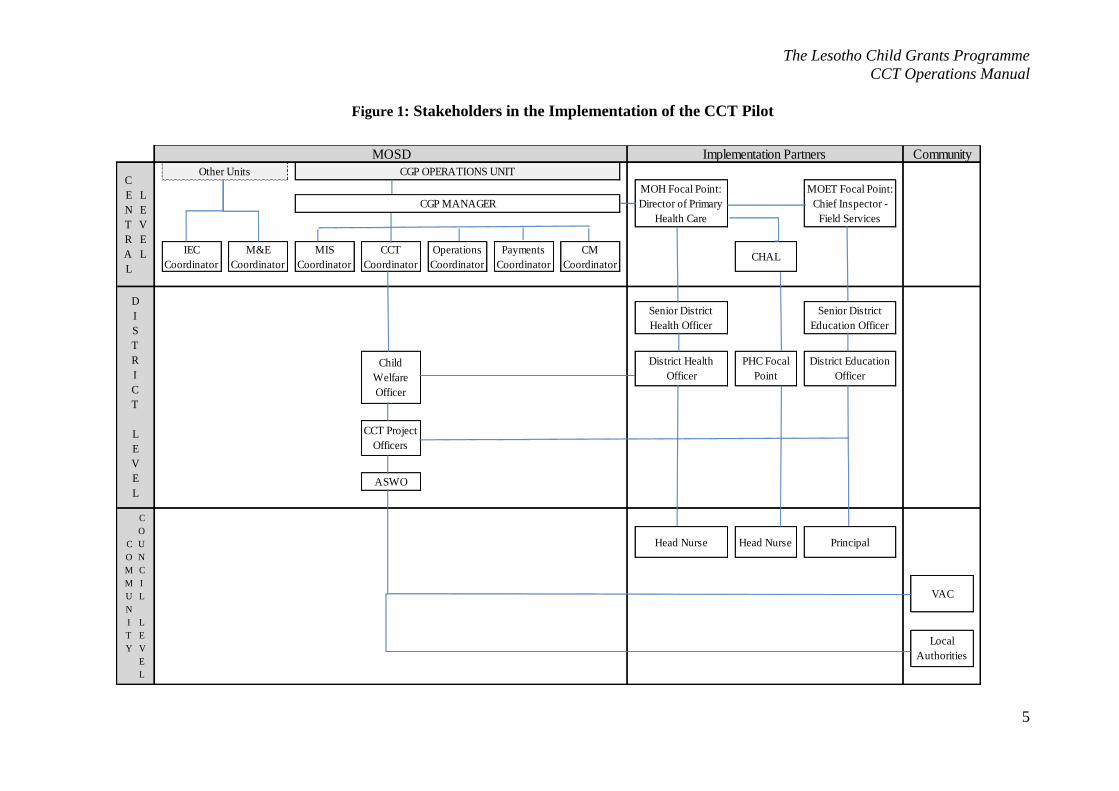
The organisational structure displaying the inter-relationships among main stakeholders in the
programme on central, district and CC level is presented in Figure 1.
The Lesotho Child Grants Programme
CCT Operations Manual
5
Figure 1: Stakeholders in the Implementation of the CCT Pilot
ASWO
Head Nurse Head Nurse PrincipalC
O
M
M
U
N
I
T
Y
C
O
U
N
C
I
L
L
E
V
E
L
VAC
Local
Authorities
CHAL
D
I
S
T
R
I
C
T
L
E
V
E
L
Senior District
Health Officer
Senior District
Education Officer
Child
Welfare
Officer
District Health
Officer
PHC Focal
Point
District Education
Officer
CCT Project
Officers
M&E
Coordinator
MIS
Coordinator
CCT
Coordinator
Operations
Coordinator
Payments
Coordinator
CM
Coordinator
MOSD Implementation Partners Community
C
E
N
T
R
A
L
L
E
V
E
L
Other Units CGP OPERATIONS UNIT
MOH Focal Point:
Director of Primary
Health Care
MOET Focal Point:
Chief Inspector -
Field Services
CGP MANAGER
IEC
Coordinator

The Lesotho Child Grants Programme
CCT Operations Manual
5
A. MINISTRY OF SOCIAL DEVELOPMENT (MOSD)
Through its CGP-OU,the MOSD is the principal coordinating body for the implementation of
the CCT pilot.
The CGP-OU, through its CCT Coordinator, is fully responsible for the CCT’s Process,
including itsdesign and implementation. For this purpose it may undertake relevant activities
itself or through any other qualified external partners.
The general tasks to be carried out by the CGP-OU are to:
Revise and approve all the relevant technical documents and materials to be used;
Ensure the execution of each process is in accordance with the approved procedures
and, if required, make necessary adjustments;
Coordinate the activities for all stakeholders;
Supervise appropriate implementation across treatment groups;
Produce and review various lists/documents/indicators/reports; and
Inform stakeholders and households of the on-going activities and their implications,
and of the monitoring of various outcomes of interest.
The CGP-OU comprises of the following staff: (1) CGP Manager; (2) CCT Coordinator; (3)
Operations Coordinator; (4) Case Management (CM) Coordinator; (5) Payments Coordinator;
(6) Management Information System (MIS) Coordinator; (7) Monitoring and Evaluation
(M&E) Coordinator; (8) Information, Education and Communications (IEC) Coordinator; (9)
CCT Project Officers; (10) District Child Welfare Officers; and (11) Auxiliary Social
Welfare Officers (ASWO).
1. CGP Manager
The CGP Manager heads the CGP-OU and is responsible for overall coordination of the CCT
pilot under the CGP’s framework. He/she is responsible for the coordination with the other
participating Ministries and for facilitating decision-making in the higher policy levels of the
MOSD. The CGP Manager is also directly responsible for procedures requiring the support of
other areas of the MOSD, such as Procurement and Human Resources. The ultimate
responsibility of the CGP Manager is securing the same quality of service delivery for CCT
beneficiaries as for CGP beneficiaries.

The Lesotho Child Grants Programme
CCT Operations Manual
6
2. CCT Coordinator
The CCT Coordinator is responsible for the CCT Pilot Operations, including managing the
day-to-day activities related to the programme. He/she performs the following general duties:
Provide overall guidance for each process, and ensure that all stakeholders and
partners adhere to the rules and procedures set forth in the TA of each process;
Oversee the preparatory activities, general logistical coordination and final
implementation and generation of results of the process at the Central Level;
Conduct activities of each process jointly with the District Level staff;
Coordinate the work in all selected CCs, secure smooth implementation of each
process in coordination with financial partners;
Supervise the use of financial resources and approving the disbursement of funds for
the purchase of material as well as ensuring all required material for the process is
available in a timely fashion;
Ensure that the necessary staff is available, whether through hiring of external staff or
sourcing from within the different levels of the MOSD;
Supervise the design of training modules, schedule training activities and monitor
trainings throughout the pilot Districts;
Train the relevant staff in various processes;
Work closely with the MIS Coordinator to ensure the appropriate use of each
module’s tools; and
Perform M&E activities (spot checks, internal process evaluations) in coordination
with the M&E Coordinator.
3. Operations Coordinator
The Operations Coordinator under direct Supervision of the CGP Manager is responsible for
the following:
Provide overall guidance for each process, to ensure they function smoothly within
CGP procedures;
Support CGP Manager and CCT Coordinator overseeing training and development of
logistics plans;
Supervise communications with ASWOs;

The Lesotho Child Grants Programme
CCT Operations Manual
7
Provide support in the organization of preparatory activities and general logistics,
lending expertise gained from the CGP, including follow-up on the necessary
materials required for the process and overseeing their purchase and distribution;
Oversee the smooth implementation of activities of the process according to its work
plan, in particular for activities that might delay CCT procedures such a as payments;
Implement the communications strategy in collaboration with the IEC Coordinator;
Provide assistance to the CCT Coordinator when necessary; and
Perform any other process-related tasks as detailed in each process’ TA.
4. CM Coordinator
The CM Coordinator is responsible for the appropriate functioning of the CMprocess
throughout the life cycle of the pilot. He/she works closely with the Operations Coordinator
and the CCT Project Officers, indirectly supervises the District Child Welfare Officers and
the ASWOsand reports to the CCTCoordinator. His/her responsibilities are to:
Coordinate the establishment of the CM system at the District and Community
Council;
Monitor the functioning of the CM Process, identifying shortfalls and proposing
solutions;
Develop Rules and Regulations for the District Case Management Committee to be
established in District Offices;
Provide assistance when necessary during the resolution of CM cases, especially
when complaints/exemptions/appeals escalate;
Ensures that payment agencies and other partners at the Central level respond to the
complaints;
Review the quarterly and annual reports on Updates, Appeals, Exemptions and
Complaints produced by the M&E Officer, and discuss them with the CCT
Coordinator;
Direct cases to the Payments Coordinator, Payment Agencies, the Operations
Coordinator, the CCT Coordinator or other relevant staff at Central level for the
corresponding resolution;
Forward responses from Payment Agencies and other partners at the Central level to
the respective CCT Project Officers;

The Lesotho Child Grants Programme
CCT Operations Manual
8
Provide guidance to the CCT Coordinator to solve difficult cases;
PrintCM forms and deliver them to the CCT Project Officers;
Generate/print the notification letters to inform beneficiaries about the result of the
case;
Deliver notification letters to CCT Coordinator to be signed and stamped;
Deliver signed and stamped letters to the CCT Project Officers;
Train the ASWOs and District Child Welfare Officers in performing CM at any
time during the monitoring cycle, as requested;
Supervise the generation of Monthly CCT Case Management Report, Review and
approve the Exemption Requests as solved by the District CM Committees, and
enter them into the MIS with the appropriate status; and
Perform any other process-related tasks as detailed in each process’ TA.
5. Payments Coordinator
The Payment Coordinator is in charge of overseeing the entire payment process including the
preparations of material, dissemination of material, payment events and preparations of
reconciliation. He/she works in close cooperation with the CCT Coordinator, MIS
Coordinator and the Operations Coordinator.
The Payment Coordinator carries out the following activities:
Write letter to the Financial Controller to release funds to payment agencies, and
submit this letter to the CGP Manager;
Generate the payment list;
Generate and print the forms used during the payment process, particularly
payment books, payment book front cover stickers and beneficiary receipts;
Calculate the number of payment amount barcode stickers, generate additional
barcode stickers and send order to print stickers prior to the start of the payment
period;
Delegate the preparation of beneficiary payment books to MIS Officers and/or
CGP Operation Officers at the district level;
Coordinate and supervise the distribution of payment books by the Operation
Officers at the district level;

The Lesotho Child Grants Programme
CCT Operations Manual
9
Monitor and manage the payment process according to this document and the
legal agreements signed with Payment Agencies;
Do spot checks at payment site to monitor whether the process is carried in due
compliance with set up procedures;
Take decision on how to handle unexpected cases that may occur during payment
or refer cases to the CCT Coordinator;
Supervise and instruct the Operation Officers at district level and the Operations
Assistants on the community council level on the payment procedures and their
tasks during payment events;
Upload payment software files into the MIS after payments to prepare
reconciliation report;
Prepare reports regarding the number of beneficiaries that have been paid and the
amount paid out;
On request, prepare reports for the CGP external and internal audits;
Receive Payments Claims from the CM Coordinator, review them and coordinate
with the Payments Agency as needed;
Ensure that Payment Agencies respond to the household complaints and acts as
the communication mediator; and
Perform any other process-related tasks as detailed in each process’ TA.
6. MIS Coordinator
The MIS Coordinator manageshis/her team in order to perform the tasks below. Likewise,
he/sheworks closely with the CCT Coordinator during every step of the process, providing
general support and ensuring the CCT Coordinator is informed of the needs and challenges of
the IT work.
Support the CCT Coordinator in the generation of lists and reports;Define the
hardware and software updating needs for an effective implementation of the CCT on
top of the CGP without negatively affecting the performance of the MIS;
Develop, together with the users, the definition of roles and functionalities required
for the management of each Module within the CCT MIS, taking into account the
process’ design parameters as detailed in this document;
Define the way in which requests for new MIS users areaddressed and administer the
users of the programme;

The Lesotho Child Grants Programme
CCT Operations Manual
10
Keep the MIS users up to date in the changes performed to each Module, perform
trainings on its functions and be responsible for capacity training on the management
of the module for new users;
Keep open and constant communication with the MIS users in order to support their
needs by troubleshooting and answering questions and complaints;
Supervise data entry into the MIS, ensure that it is done as per plan, while ensuring
quality of data entry and privacy of data;
Perform general tasks related to the general administration of each Module and of the
MIS, managing the database, back-ups, and contingency plans in case of emergencies;
and
Perform any other process-related tasks as detailed in each process’ TA.
7. M&E Coordinator
The M&E Coordinator works in close coordination with the CGP Manager and the CCT
Coordinator. He/she is responsible for conducting all activities related to keeping track of and
analysing the progress of the Programme. In specific his/her responsibilities are to:
Lead the overall design of the M&E component of the CCT pilot;
Identify shortfalls in each processbased on data provided through the MIS, and based
on the results of evaluation exercises;
Use the MIS data to identify shortfalls in any of the CCT processes;
Ultimately, use analyses to prepare reports for management, including
recommendations for adjustments and improvements of each process’ design;
Organize and participate in field visits / spot checks during each CCT process and
prepare reports for the CCT and Operations Coordinators;
In coordination with the CCT Coordinator, produce quarterly and annual reports on
each process using data provided by the MIS and results of monitoring visits to the
field; and
Perform any other process-related tasks as detailed in each process’ TA.

The Lesotho Child Grants Programme
CCT Operations Manual
11
8. Information, Education, and Communication Coordinator
The IEC Coordinator works in close coordination with the CG Manager and CCT
Coordinator and is responsible to:
Developa Public Information Campaign for each process, as designed and detailed in
the TAs;
Ensure that appropriate communication materials foreach process have been
developed and distributed to the relevant staff; and
Perform any other process-related tasks as detailed in each process’ TA.
9. CCT Project Officers
The CCT Project Officers operate at Distract level and below and are responsible for the
implementation and supervision of CCT activities within their assigned District. They work
inclose cooperation with and are supervised by the CCT Coordinator. The responsibilities of
the CCT Project Officers are to:
Provide guidance to the District Health and Education Authorities, partner
organizations and the local MOSD staff about the each CCT process;
Attend the appropriate trainings at the central level;
Coordinate and train local actors at the District, community and facility level, as
necessary;
Lead the CCT processes at the District level, which include: planning, managing,
implementing and supervising the various activities;
Work with the District and CC authorities, as well as VACs to ensure community
mobilization is executed in a timely and productive way;
Produce and distribute the materials to support each process, as necessary;
Follow-up with all supply-side cases ensuring that the appropriate CM modality is
implemented;
Send the Monthly CCT Case Management Report to the ASWOs and coordinate
the work of ASWO assigned to the CCT pilot;
Supervise the quality of information collected in forms and entered into the MIS;
Archive the information and documents generated by each process, as necessary;
and

The Lesotho Child Grants Programme
CCT Operations Manual
12
Perform any other process-related tasks as detailed in each process’ TA.
10. District Child Welfare Officer
The District Child Welfare Officer acts as operations coordinator at the District level and is in
charge of instructing and supervising the MOSD district staff and coordinating payments at
the District level.
11. Auxiliary Social Welfare Officers (ASWOs)
The ASWO is involved in the responsible to conduct the intensive case management
according to thegiven rules of the treatment groups and furthermore to support the payments
process. His/her responsibilities are to:
Receive the Monthly CCT Case Management Report from the CCT Project Officer;
Visit the HHs according to their ranking in the report and work with the HHs to
identify the reasons for non-compliance and record the information in the required
material;
Work together with the HHs to find solutions to their challenges, while at the same
time reminding them of the importance of complying because of the welfare of their
children as well as due to the new rules of the CCT pilot;
Pay follow-up visits to recurring non-compliant HHs and, in case he/she finds there is
a valid reason why it is not reasonable to expect the HH or any of its members to
comply with a given component (health or education), file an Exemption Request to
the district CM committee;
Support thePayments Coordinator and the CCT Project Officersat payment events;
Assist the Payment Agencies at the payment site;
Screen whether payees/representative payees have all payment documents at hand
(payment book, identification) and whether documents are properly filled;
Capture case management cases related to payments during Payment Events;
Dissemination of payment relevant information (payment cycle, amount and how the
payment book functions);
Ordering payees by village so that the payment agency can work efficiently (payment
lists is ordered by village); and
The Lesotho Child Grants Programme
CCT Operations Manual
13
Report any suspicious cases to the PaymentsCoordinator for him/her to advise on
solving the case ;
B. IMPLEMENTATION PARTNERS: MINISTRY OF HEALTH,MINISTRY
OF EDUCATION AND TRAININGAND CHRISTIAN HEALTH
ASSOCIATION OF LESOTHO
The implementation partners work at Central, District and Facility level coordinatingwith the
MOSD and performing essential tasks related to the provision of services to beneficiary HHs
and the monitoring of conditionalities/co-responsibilities.
1. Focal points at central level
The focal points within the MOET and MOH/CHAL are individuals already operating within
the structures of the corresponding Ministries/Partner Organizations1, appointed to take on
the additional responsibility of coordinating the implementation of the CCT pilot with the
previously mentioned MOSD staff. Specific responsibilities of the focal points include:
Discuss policy issues, as they arise during each CCT process;
Support the design of each process with technical knowledge of the Ministry/Partner
Organization’s procedures; reviewthe TAs and the corresponding Guidelines for
training on each process;
Coordinate and supervise the provision of complete facility lists as requested by the
CCT Coordinator, as well as of any other information and statistics as needed;
Inform their District Offices about the details of their Ministry’s/Organizations
cooperation with the MOSD, UNICEF and the European Union, and secure their
support;
Receive the list of facilities with no available capacity from the CCT Coordinator, and
make decisions on whether to increase their capacity or not;
Ensure the appropriate local staff attends trainings at central level; and
Ensure facility staff attends trainings at the District level.
1 For the MOH the Focal Point is the Director of Primary Health Care, for the MOET the Focal Point is the
Chief Inspector Field Services.

The Lesotho Child Grants Programme
CCT Operations Manual
14
2. District Staff
The MOET/MOH/CHAL’s contact points at the district levels are:
Senior District Education Officer (MOET), and
Public Health Nurse (MOH/CHAL).
Their specific responsibilities include2:
Inform all the facilities within the selected CCs about the CCT pilot and how the
upcoming activities affect them;
Inform facilities of scheduled visits with enough time in advance, and ensure that the
most knowledgeable persons are available for the interviews or discussions;
Work with the CCT staff to review the facility lists provided by the central level and
validate their quality, and make the appropriate corrections when necessary;
Facilitate the activities of the CCT Project Officers with information and resources, as
available and needed;
Attend all the necessary training sessions;
Assist in the preparation of logistics plans with their knowledge of the area and
conditions;
Assist in the data collection process, and review the quality of data collected;
Analyse and make known the results of the process at the local level;
Provide the information required by the Central level, such as the list of facilities per
selected CC;
Be the link between the Programme and the facilities’ staff, ensuring that these are
properly introduced toeach CCT process; and
Ensure that facilities’ staffattend all the necessary training sessions and the Enrolment
Events.
3. Facility Staff - Head Master/Mistress and Head Nurse
The staff of the Implementing partners at Facility level is responsible to:
Act asthe contact point for the respective school/health facility;
2While the Senior Education Officer and Public Health Nurse are the CCT pilot’s contact points at the District
Level, this does not mean that all tasks must be personally performed by them. They can distribute the tasks
allocated to the district level amongst their staff as they see fit.
The Lesotho Child Grants Programme
CCT Operations Manual
15
Be the main respondent for the supply capacity assessment survey, consulting with
other facility staff as necessary;
Provide the information on catchment areas to the best of their knowledge;
Review the quality of the information provided;
Participate in training events, as necessary;
Participate in the Enrolment Events;
Spread information among CCT beneficiaries about the benefits of children’s
attendance of education and health facilities;
Spread information among CCT beneficiariesattending theirschool/health
facilityabout the CM process, and encourage them to take advantage of it; and
If needed, be prepared to explain more about the details of the education / health
conditionalities/co-responsibilities and their fulfilment.
C. UNITED NATIONS CHILDREN’S FUND
UNICEF provides continuous technical assistance and general support throughout the
implementation of the pilot. UNICEF participates in policy discussions surrounding the
implementation of the CCT pilot and, jointly with the MOSD, reviews technical manuals for
the project process cycle.
D. LOCAL AUTHORITIES
The local government offices provide maps for the CCs involved in the pilot, and support the
process of locating education and health facilities on these maps. The Local Authorities are
instrumental in mobilizing the Community Councillors and enlisting their support.
E. VILLAGE ASSISTANCE COMMITTEES
The VACs are instrumental in the implementation of the pilot. More specifically they support
information dissemination and participate in the pilot’s sensitization and communication
campaigns. Additionally, VACs assist with the verification of beneficiaries during the
payments process, and help with the delivery of beneficiary notification letters associated
with various processes of the program cycle. The village chiefs are instrumental in supporting
the HH in their CM requests, by writing letters of support for the respective cases.
The Lesotho Child Grants Programme
CCT Operations Manual
16
F. PAYMENT AGENCIES
These agencies are charged with the responsibility of handling payments to beneficiaries,
according to the procedures outlined in the Payments Manual. They also assist with the
resolution of payment related claims and complaints as necessary.
G. BENEFICIARY HOUSEHOLDS
Households have the responsibility to abide to all rules of the CCT Programme once they
gave their consent to become beneficiaries:
Attend the Enrolment event and provide truthful information;
Comply with conditionalities/co-responsibilitiesof the CCT Programme;
File cases according to their needs and accept case resolutions;
Attend community mobilization sessions; and
Collect their transfers.

The Lesotho Child Grants Programme
CCT Operations Manual
17
III. DESIGN PARAMETERS
The design parameters of the CCT pilot are the building blocks which allow for uniform
project implementation. The design parameters include eligibility criteria, conditionalities/co-
responsibilities, transfer parameters and the exit policies.
A. ELIGIBILITY CRITERIA
The eligibility criteria provide the basis for inclusion or exclusion of health and education
facilities and beneficiary households in the CCT pilot.
1. Eligibility Criteria for Schools
For a school to be included into the Programme, i.e. to have beneficiary children assigned to
it and monitor their compliance, the following conditions have to be fulfilled:
Be located in one of the selected CCs, or in neighbouring CCs, such that
households enrolled in the pilot would be in the catchment area of these schools;
Be partially or fully funded by the government and offer free primary education;
and
Provide educational services for any of the seven standards of the primary school
cycle.
2. Eligibility Criteria for Health Facilities
For a health facility to be included into the Programme, i.e. to have beneficiary children
assigned to it and monitor their compliance, the following conditions have to be fulfilled:
Be located in one of the selected CCs, or in neighbouring CCs, such that
households enrolled in the pilot would be in the catchment area of these health
facilities; and
Be partially or fully funded by government.
3. Eligibility Criteria for Households
A HH is eligible for Programme entry if the following conditions are fulfilled:
Reside located in one of the selected CCs;
Be already a CGP beneficiary (be in NISSA1 or NISSA2,be validated by
itscommunity and take care of at least one child below 18 years of age); and
Provide care to at least one child 0 to 17 years old (in completed years).

The Lesotho Child Grants Programme
CCT Operations Manual
18
B. CONDITIONALITIES/CO-RESPONSIBILITIES AND PENALTIES FOR
NON-COMPLIANCE
CCT beneficiaries are required to comply with conditionalities/co-responsibilities
thuspromotingthe expansion in the usage of public health and educational services.They
present a unique opportunity for investing in the human capital of programme beneficiaries.
HHs in Treatment Group Oneare subject to co-responsibilities in the sense that they areonly
be subject to monitoring and intense case management, with no payment related penalties
should they not comply with the co-responsibilities. However, HHs in Treatment Groups
Twoand Three are subject to conditionalities wherein they face payment related penalties
should they fail to comply with these conditionalities.HHs in Treatment Group Four are
subject to co=responsibilities but no penalties or intense case management is carried out.
Below are the programme rules (co-responsibilities and conditionalities) with which
beneficiary HH are expected to comply, and the penalties applied when HHs are non-
compliant.
1. EducationConditionalities/Co-responsibilities
The education conditionalities/co-responsibilities apply to children between the ages 6 and 17
(in completed ages). The children have to comply with the following:
Be formally enrolled in any of the Grades 1 to 7 in an eligible primary school; and
Attend at least 85% of effective school days per monitoring quarter.
2. HealthConditionalities/Co-responsibilities
The health conditionalities/co-responsibilities apply for children below 60 months of age (5
years). The children have to comply with the following:
Conduct regular visits to eligible health facilities according to the EPI Immunisation
Schedule of the MOH.
Conduct visits to health facilities monthly for growth monitoring visits, or attend
monthly growth monitoring events carried out by village health workers.3
3Additionally, at the early childhood stage (age 3 to 5 years old) children should visit the health facility for
routine check-ups every six months.

The Lesotho Child Grants Programme
CCT Operations Manual
19
However, the type of visit is not monitored; rather it is monitored whether a visit has been
conducted each month.
There are programme beneficiaries who can be exempt from these education and health co-
responsibilities. The categories of beneficiaries along with the justifications for exemptions
are described below:
Children who are 60 months old or above but below 72 months old (5 years in
completed years) are excluded from compliance monitoring because they are too
old for the health component, but too young to be enrolled in primary school (pre-
school not included);
Children 5 years old who are not enrolled in school during the current academic
year, but turned 6 after the current academic year began. These children are
required to enrol in the following academic year, before they turn 7.
Children at least 14 but less than 18 years old who dropped out of primary school,
and left school at least 2 years ago;
Children who graduated the primary school levels (Standards 1-7);
Children who are disabled;
Children who are enrolled in schools/health facilities that fall more than ten (10)
km outside of the selected CCs’ boundaries or are not government funded. In this
case, proof of enrolment has to be collected/provided; and
Children who live in areas where no facilities are available for new enrolment or
no facilities are available in general in the catchment area of the village.4
3. Penalties
According to the rules described above, penalties do only apply to Households in Treatment
Group 2 and 3. A HH is considered as non-complied if at least one beneficiary child did not
fulfilits conditionality in the monitoring quarter. The penalty is then applied on HH level, i.e.
the combined transfer amount according to all children of the HH is penalized.
The table belowillustrates the penalties applied according to the HH’s Treatment Group.
Table 1: Treatment Groups and Payment Penalties for Non-Compliance
4 Whereas all other exemptions are identified during enrolment, this exemption can be applied to via the Case
Management and is approved on a case-to-case basis. For more details refer to the Case Management Manual.

The Lesotho Child Grants Programme
CCT Operations Manual
20
Treatment Group
Payment Penalties Across Monitoring Cycles (MC)
1stconsecutive
non-compliance
2nd consecutive
non-compliance
3rd consecutive
non-compliance
4thconsecutive no-
compliance
One
(Intense CM, no
penalties)
0 0 0 0
Two
(Penalties) 25% 50% 100%
100% Reinstated
if Compliant;
100% Penalty if
Non-compliant
Three
(Intense CM and
Penalties)
0 25% 50% 100%
Four
(No intense CM, no
penalties)
0 0 0 0
A HHin Treatment Group Two whichdid not comply with the health and/oreducation
conditionalities for the first time loses 25% of itstransfer amount during that respective
payment cycle. The penalty increases to 50% if the HHisnon-compliant for a second
consecutive quarter, and to 100 % if non-compliance follows for a third consecutive quarter.
The first quartera HHin Treatment Group Three is non-compliant with any of the health
and/or education conditionalities no payment penalty is applied but intense case management
is carried out. However, a 25% penalty is levied if non-compliance follows for a second

The Lesotho Child Grants Programme
CCT Operations Manual
21
monitoring period. The penalty increases to 50% for the third consecutive non-compliant
quarter, and to 100 % for the fourth consecutive non-compliant quarter.
Once a non-compliant HH becomes compliant in a given quarter, the full payment amount is
restored regardless of the penalty levied in the previous quarter.
C. PAYMENTS, FREQUENCY OF PAYMENTS AND DELIVERY
MECHANISM
Beneficiaries of the CCT pilot receive a quarterly payment betweenM 360 and 750 per
household, depending on the number of children in the household. The payments are
embedded in the CG payment schedule. Below are the design parameters for payments:
Table 2:Payments Design Parameters
Cash Transfer Amount
Between Maloti (M) 360-750:
- M 360 for 1-2 children
- M 600 for 3-4 children
- M 750 for 5+ children
Transfer Frequency Every 3 months (four transfers per year)
Transfer Mechanism Payment Agencies
D. DURATION & EXIT POLICY
The CCT pilot is implemented over a period of two years. The exit policies for the
programme are as follows:
HH misses three consecutive payments;
HH relocates to an area not covered by the pilot;
A child no longer lives in the HH;
and
HH misusespayment
The Lesotho Child Grants Programme
CCT Operations Manual
22
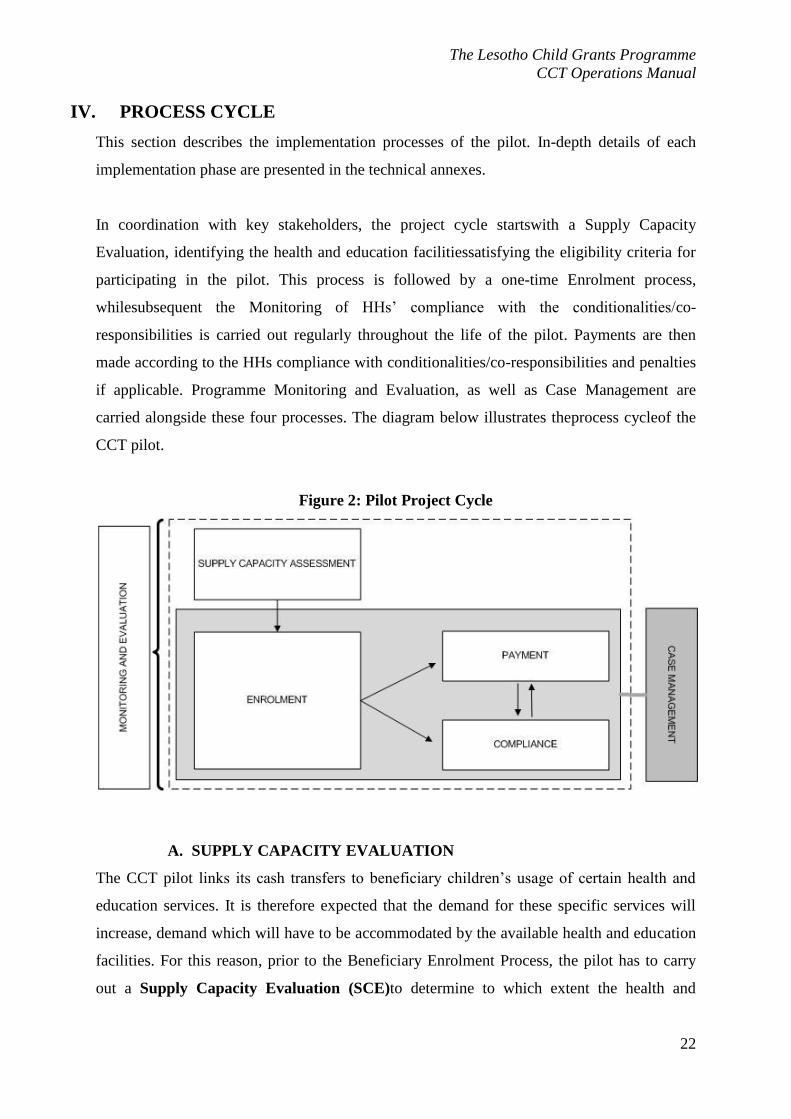
IV. PROCESS CYCLE
This section describes the implementation processes of the pilot. In-depth details of each
implementation phase are presented in the technical annexes.
In coordination with key stakeholders, the project cycle startswith a Supply Capacity
Evaluation, identifying the health and education facilitiessatisfying the eligibility criteria for
participating in the pilot. This process is followed by a one-time Enrolment process,
whilesubsequent the Monitoring of HHs’ compliance with the conditionalities/co-
responsibilities is carried out regularly throughout the life of the pilot. Payments are then
made according to the HHs compliance with conditionalities/co-responsibilities and penalties
if applicable. Programme Monitoring and Evaluation, as well as Case Management are
carried alongside these four processes. The diagram below illustrates theprocess cycleof the
CCT pilot.
Figure 2: Pilot Project Cycle
A. SUPPLY CAPACITY EVALUATION
The CCT pilot links its cash transfers to beneficiary children’s usage of certain health and
education services. It is therefore expected that the demand for these specific services will
increase, demand which will have to be accommodated by the available health and education
facilities. For this reason, prior to the Beneficiary Enrolment Process, the pilot has to carry
out a Supply Capacity Evaluation (SCE)to determine to which extent the health and

The Lesotho Child Grants Programme
CCT Operations Manual
23
education facilities have enough capacity to absorb this expected additional demand of their
services.
For schools, the main determinant of capacity is the student to teacher ratio, which should be
less than 45:1. For health centres, the assessment looks at how many patients the health
workers could attend to vs. how many they are currently attending. All the information
obtained from the SCEprovides the CCT pilot with information on both the accessibility of
schools and health facilities in the selected CCs, and their ability to meet increases in
demand. The facilities able to meet these increases in demand are recommended, during the
Enrolment process, to be utilized by new entrants. However, it is the beneficiaries’ choice
which facilities they will ultimately use.
A number of steps have to be taken to assess the capacity ofschools and health facilitiesto
respond to programme service needs. An overview of these activities is provided in this
section.
Figure 3:Flow Chart of the Supply Capacity Evaluation Process

The Lesotho Child Grants Programme
CCT Operations Manual
24
PREPARATORY
ACTIVITIES
Fieldwork
Data entry into MIS
Logistics Coordination
Production and distribution of materials
Visit District and Council Offices
Visit schools and health facilities
Fill corresponding forms
Data entry into MIS
Schools results lists
Training
Close fieldwork
Generate results
Results analysisGenerate indicators
Health facilities results lists
Follow-upFollow-up with respective Ministries on
“problem” facilities
1. Preparatory Activities
These include all activities that are carried out before data collection for the SCEtakes place
in the field. It involves the preparation of a logistics plan, preparation and distribution of
required work material and training.
The logistics plan is an essential implementation tool that allows for smooth implementation
of field activities. While Central Level programme staff is in charge of the overall logistics
plan, the District programme staff is required to prepare their own plan and submit it to the
Central Level, who then monitor its implementation. The logistics plan includes:
(i) Basic Information Gathering –Information to be collected from the health and
education authorities regarding the facilities that satisfy the pre-eligibility criteria.
(ii) Fieldwork Coordination – Verification of basic data,establishing contact with the
central and local district authorities, logistics coordination, organizing trainings,
developing a schedule for all the field activities to take place during the SCE.

The Lesotho Child Grants Programme
CCT Operations Manual
25
(iii) Composition of Evaluation Teams – Decision on number of individuals required
to carry out data collection and the allocation of responsibilities among these
individuals.
(iv) Estimation of Required Materials– Estimation on the number of data collection
forms, maps, stationery, list of villages in CC, based on the number of facilities
identified during the Basic Information Gathering stage.
(v) Detail Training Requirements – A plan for training ensuring that processes in the
field are implemented according to the procedures set out in the Supply Capacity
Evaluation TA.
This logistics plan lays the groundwork for the preparationand distribution of materials and
the necessary training that takes place before the field work.
Preparation and distribution of materials include: (i) procurement of detailed maps for the
Community Councils where the CCT pilot is being implemented; and (ii) preparation of the
Evaluation Materials Kit for every Community Council, which includes maps, forms and
stationery.
The training for the teams carrying out the actual data collection in the field is carried out at
Central level, and its objective is that all team membersperformtheir designated role in the
process.The training includes both theoretical (a review of the general aspects of the
evaluation and a thorough practice of data collection procedures) and practical aspects (mock
interviews in order to master the correct way to fill out the SCE forms).
2. Fieldwork
Fieldwork defines the data collection aspect of the Supply Capacity Evaluation. It includes
three main activities:
(i) Visits to District and Council Offices – to provide district and council authorities
with information on the CCT pilot,to verify the data provided by health and
education authorities, and ensure that the existent lists of villages in the pilot
Community Councils are complete and that the villages are located on the
respective maps.
The Lesotho Child Grants Programme
CCT Operations Manual
26
(ii) Visits to Schools and Health Facilities – to collect information on the capacity and
the catchment area of these facilities(villages using a certain facility and their
distance to facility) by completing the SCE forms.
(iii) Fieldwork Closure–to ascertain the quality of the data, and to decide on actions to
be taken if data collection forms are incomplete/in need of revisions.
(iv)
3. Data Entry
The data entry process takes place after the appropriate data entry staff is trained, and the data
collected in the field is verified by the CCT Coordinator and eventual corrections are
made.Upon receiving access to the MIS, the trained data entry staff entersthe data into the
appropriate MIS module. The data is once more checked by the MIS, and corrections are
made as necessary.
4. Generation of Results
Using the data entered into the MIS, each facility is assigned one of the following supply
capacity statuses:
(i) Evaluated, Sufficient - the MIS has all the essential information5 on the facility, and it
evaluates that the facility has available capacity to absorb new entrants;
(ii) Evaluated, Deficient - the MIS has all the essential information on a facility, and it
evaluates that the facility does not have available capacity to absorb new entrants;
(iii)Not Evaluated, Incomplete - some of the essential information on the facility is
missing. The MIS keeps this status until the information is corrected; and
(iv) Not Evaluated, Annulled - facilities which have been eliminated from the CCT pilot
due to a policy-level decision. Even if the information on these facilities is complete,
their available capacity isnot further computed and displayed.
Based on these statuses, the MIS generates the following on-demand result lists:
(i) Overall School and Health Facilities Results – This list provides results for all the
facilities for which essential information was gathered and entered into the MIS.
5Consult the SCE TA for details on which information on the SCE forms is deemed as essential.

The Lesotho Child Grants Programme
CCT Operations Manual
27
(ii) Results by Facility6 – This list contains information on the geographic location,
staffing, available capacity and indicators pertaining to the SCE, by facility.
(iii) Results by Village7 – This list contains information on the education and health
facilities which are within the catchment area of each village, together with the
facilities computed available capacity.
Additionally, the MIS also generates lists that allow for the analysis of catchment areas for
both health and education facilities. These results can be generated by facility or per village.8
5. Follow-Up
Based on the results generated, the programmemanagerfollowsup with the MOET and
MOHin order to present them the overall results and to make them aware of the facilities with
deficient capacity and catchment area challenges.
6. Generation of Indicators
This activity can be carried out during or after the SCE, and is useful for the monitoring and
evaluation of the process. During the SCE, the indicators accessed should focus on
monitoring the progress of the fieldwork, namely on the percentages of facilities covered in
different locations. After the SCE, the indicators focus on the status of facilities, available
capacity, coverage and accessibility.
B. ENROLMENT
The Enrolment Process of the CCT pilot is meant to inform the beneficiary HHs about the
pilot’s launch and the new programme rules, and enrol in the CCT pilot those beneficiaries
HHs which agree to participate. BeneficiaryHHs in the selected CCs whichdo not enrol in the
CCT pilot by choice or they don’t have children in the appropriate age groups anymore
areremoved from CGP-CCT pilot.
6 To be included in the MIS developed by Local IT Firm . 7 To be included in the MIS developed by Local IT Firm. 8 To be included in the MIS developed by Local IT Firm.
The Lesotho Child Grants Programme
CCT Operations Manual
28
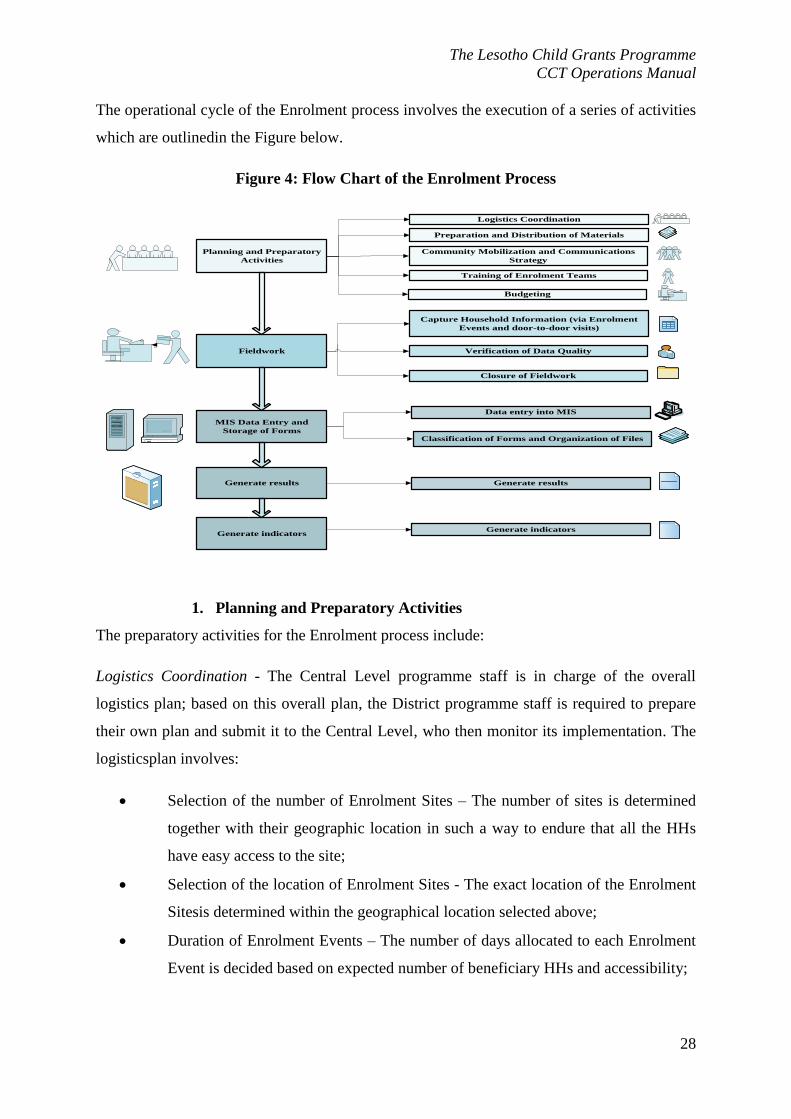
The operational cycle of the Enrolment process involves the execution of a series of activities
which are outlinedin the Figure below.
Figure 4: Flow Chart of the Enrolment Process
Planning and Preparatory
Activities
Fieldwork
MIS Data Entry and
Storage of Forms
Logistics Coordination
Preparation and Distribution of Materials
Capture Household Information (via Enrolment
Events and door-to-door visits)
Verification of Data Quality
Community Mobilization and Communications
Strategy
Training of Enrolment Teams
Budgeting
Generate results Generate results
Closure of Fieldwork
Data entry into MIS
Generate indicatorsGenerate indicators
Classification of Forms and Organization of Files
1. Planning and Preparatory Activities
The preparatory activities for the Enrolment process include:
Logistics Coordination - The Central Level programme staff is in charge of the overall
logistics plan; based on this overall plan, the District programme staff is required to prepare
their own plan and submit it to the Central Level, who then monitor its implementation. The
logisticsplan involves:
Selection of the number of Enrolment Sites – The number of sites is determined
together with their geographic location in such a way to endure that all the HHs
have easy access to the site;
Selection of the location of Enrolment Sites - The exact location of the Enrolment
Sitesis determined within the geographical location selected above;
Duration of Enrolment Events – The number of days allocated to each Enrolment
Event is decided based on expected number of beneficiary HHs and accessibility;

The Lesotho Child Grants Programme
CCT Operations Manual
29
Staff Requirements – The number of persons needed as well as the composition of
the Enrolment Teams is decided at this stage;
Dates of Enrolment –The dates for each Enrolment Event are decided
consideringthe remoteness of enrolment site;
Calendar of Enrolment Events, or Enrolment Plan – This compiles the information
on Enrolment Sites and Dates of Enrolment Events, taking into consideration any
public holidays/festivities, transportation time, and allowing for door-to-door
enrolment visits at the end of the enrolment in a selected community council.
Preparation and Distribution of materials: Then, the following materials are prepared
and distributed during this planning phase: Call Enrolment Lists and Invitation Letters
for Enrolment;List of Partner Facilities;Bukana/Health Cards;Enrolment Forms;Forms
monitoring the progress of the fieldwork;Training materials; andEnrolment Plan.
Community Mobilization - The objective of the community mobilization campaign is to
provide the community information about the pilot, its objectives and requirements, and the
upcoming plans for enrolment. The communications strategy is centrally designed, and the
best method(s) of dissemination are selected (brochures, posters, flyers, banners,
billboards).The strategy is then rolled out with the respective materials produced in advance.
Training -To ensure a smooth implementation in the field, trainingof allkey participants of
the enrolment process is a key element of the preparatory stage. There are two separate
training audiences: (i) the headmasters and head nurses on the facilities’ side, and (ii) the
Enrolment Teams on the MOSD side.
Budgeting -all human resources, materials, transportation, accommodation and training are
estimated and analysed in order to facilitate financial controlof the actions carried out during
the Enrolment process.
2. Fieldwork
This phase includes:
(i) Data Collection;
(ii) Verification of Data Quality; and
(iii) Closure of Fieldwork.

The Lesotho Child Grants Programme
CCT Operations Manual
30
During the data collection, HH leveland individual data is collected by the Enrolment Teams
using the Enrolment Form. The data is expected to be collected during the Enrolment Events.
However, separate provisions are made for HHs who cannot attend the Enrolment Events:
first, at the end of the Enrolment Events in a certain Community Council, the Enrolment
Teams carry out door-to-door visits in order to enrol these HHs. If the HHs are not present
during this visits, they can visit the district office of the MOSD within 14 days from the end
of enrolment in their council, and request they are enrolled.
The Enrolment Officers and the Enrolment Coordinator, both part of the Enrolment
Teams,are in charge of the data quality control during the fieldwork. The objective of this
activity is to verify during the fieldwork that the forms filled out are complete, legible and do
not contain obvious errors. As such, this activity ensures the collected information complies
with the minimum quality requirements.
The closure of fieldworkis a process that actually begins during implementation and is
finalized once all the HHs have left the enrolment site. The process of closure is detailed
below:
(i) Completion of Supervision Formsby Enrolment Officers and the Enrolment
Coordinator
(ii) Collection of Enrolment Forms by the Enrolment Coordinator
(iii) Packaging and Labellingby the whole Enrolment Team, supervised by the
Enrolment Coordinator
(iv) Submission of Forms to the Central Level by the Enrolment Coordinator
The submission of Forms to the Central Level takes place ideally as work is finalized for each
enrolment site. However, this might not be possible due to logistical difficulties; in this case,
the forms are submitted either at the finalization of work in a certain council or, at most, at
the finalization of work in a certain district.
3. MIS Data Entry and Storage of Forms
Before the first batch of completed forms reaches the Central Level, specialized data entry
staff (either MOSD or external consultants, as needed) is trained on the specifics of entering
the data in the Enrolment module of the MIS. Once the documents reach the programme

The Lesotho Child Grants Programme
CCT Operations Manual
31
manager at the central level, the Enrolment Forms are sorted and the MIS data entryis
conducted by these dedicated staff.
In parallel with the data entry, it is recommended that two concomitant types of storage of
the formsare used: (i) forms are scanned and stored electronically at Central Level, so that
the loss of information is prevented; and (ii) forms are physically classified and stored at
District Level, after the data entry and the electronic storage are completed.
4. Generation of Results
Using the data entered into the MIS, each child 0-17 years old (in completed years) is
assigned one of the following enrolment statuses:
a. Enrolled, Active: child in a beneficiary HH who is held liable for fulfilling
conditionalities/co-responsibilities;
b. Enrolled, Exempt: child in a beneficiary HH who, for well-determined
reasons,isnot be held liable for fulfilling conditionalities/co-responsibilities;
c. Incomplete: child in a beneficiary HH for whom at least one piece of the
essential information is missing/ineligible/mistaken, and thus he/she can be
categorized as neither active nor exempt; and
d. Excluded: child in a beneficiary HH for whom no official identification was
provided before the grace period expired.
Based on these individual statuses, a HH can be categorized as:
a. Beneficiary, active: all the HH members 0-17 years old are successfully
categorized as either “enrolled, active” or “enrolled, exempt” or “incomplete”
but at least one child is “enrolled, active”;
b. Beneficiary, exempt: all the HH members under 18 years old are successfully
categorized as “enrolled, exempt” or “incoplete” but at least one child is
“enrolled, exempt”;
c. Incomplete: all the HH members under 18 years old are categorized as
“incomplete.”
d. Restricted:HH which has failed to take the opportunities granted to register
into the CCT pilot and which is restricted from the CCT upon the expiring of
the final date for enrollment (14 days or longer after the first round of
The Lesotho Child Grants Programme
CCT Operations Manual
32
enrolment has been completed); or HH which opted out of the CCT pilot; or
beneficiary HH which currently does not care for any child younger than 18
years old; or HHs which do not reside in a CCT CC anymore; or HH which
did not present official identification forms for all the children; or HH which
presented fraudulent information.
At any time, as needed, the MIS should generate lists of active, exempt, and incomplete
children, overall and by education or health conditionality, sorted by district, CC, Electoral
Division and village (and HH), together with basic personal information (e.g. unique HH and
personal number, age and gender or the child). The list of exempt children should also
differentiate between the various types of exemptions.
Similarly, as needed, the MIS should generate lists of enrolled, incomplete, missing, and
restricted HHs, all by district, CC, Electoral Division and village. The lists should also
contain few other HH level variables (e.g. the unique HH number, the reason for having a
“restricted” status, demographic characteristics).
At any time, the MIS should keep track of the children with no birth certificates in the system
and the time lapse since enrolment. This list should be generated, as needed, by any
geographical division, and contain some other specific HH level information.
5. Generation of Indicators
The MIS is capable of generating statistical reports at the household or child level. These
reports contain indicators that can be used to monitor and assess the implementation of
enrolment process.
The reports provide statistics of how many beneficiaries were called for enrolment and how
many were enrolled, and the respective percentages. The statistics at HH level should be both
for the overall population and disaggregated by geographic location (by district, constituency,
CC, electoral division, village), status (active, exempt, incomplete, restricted), and
component (education only, health only, both). The statistics at individual/child level should
be both overall and disaggregated by geographic location (by district, constituency, CC,
electoral division, village), gender (male, female),age, status (active, incomplete and exempt)
and component of the CCT-pilot (education and health).

The Lesotho Child Grants Programme
CCT Operations Manual
33
The Lesotho Child Grants Programme
CCT Operations Manual
34
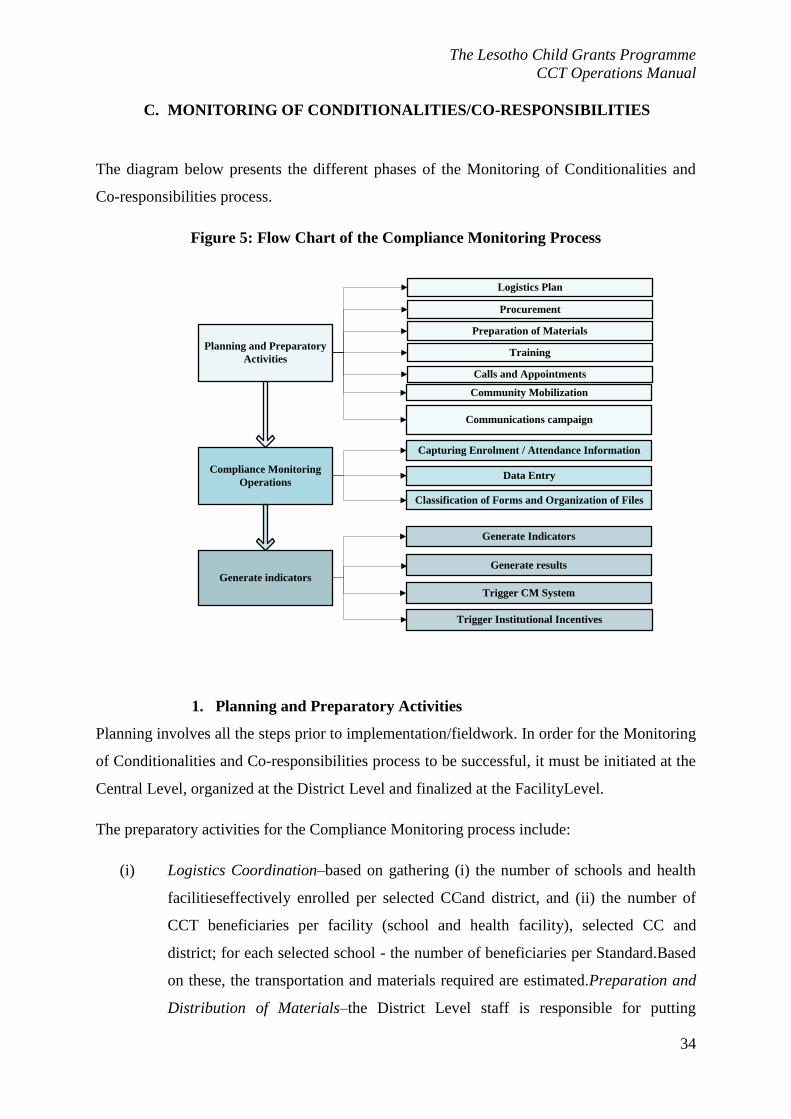
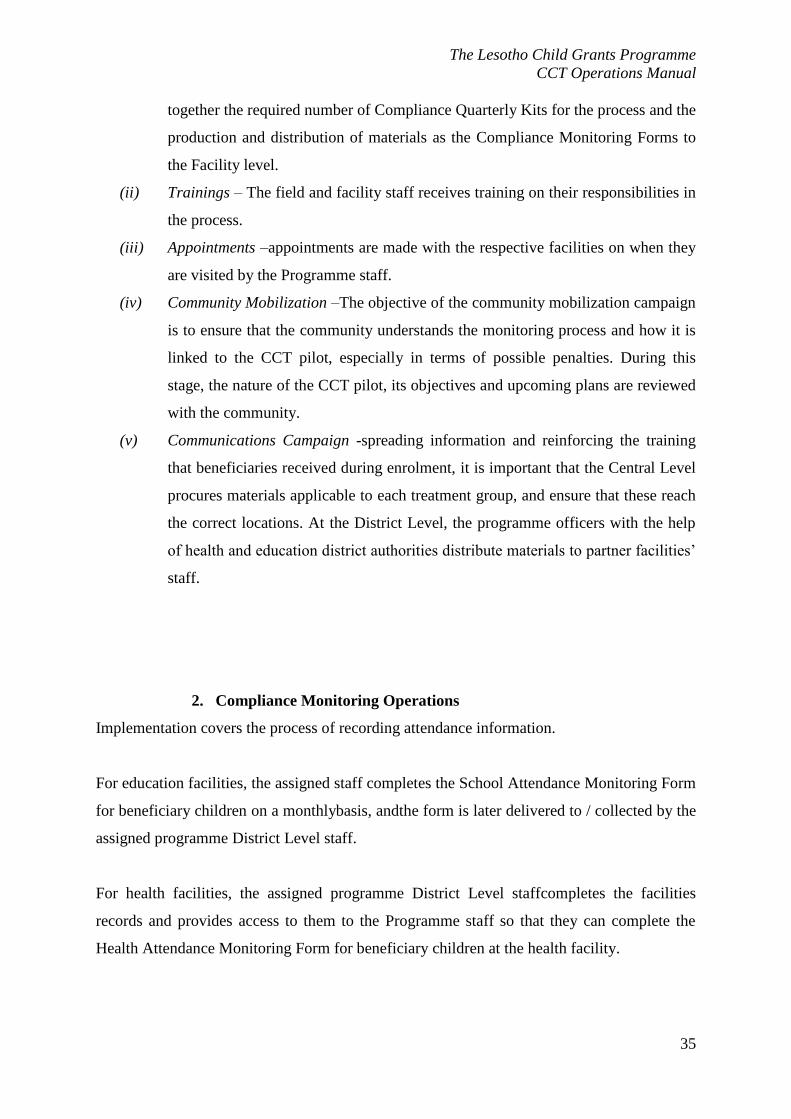
C. MONITORING OF CONDITIONALITIES/CO-RESPONSIBILITIES
The diagram below presents the different phases of the Monitoring of Conditionalities and
Co-responsibilities process.
Figure 5: Flow Chart of the Compliance Monitoring Process
Planning and Preparatory
Activities
Compliance Monitoring
Operations
Logistics Plan
Procurement
Capturing Enrolment / Attendance Information
Data Entry
Preparation of Materials
Communications campaign
Generate indicators
Trigger Institutional Incentives
Classification of Forms and Organization of Files
Community Mobilization
Training
Calls and Appointments
Generate Indicators
Generate results
Trigger CM System
1. Planning and Preparatory Activities
Planning involves all the steps prior to implementation/fieldwork. In order for the Monitoring
of Conditionalities and Co-responsibilities process to be successful, it must be initiated at the
Central Level, organized at the District Level and finalized at the FacilityLevel.
The preparatory activities for the Compliance Monitoring process include:
(i) Logistics Coordination–based on gathering (i) the number of schools and health
facilitieseffectively enrolled per selected CCand district, and (ii) the number of
CCT beneficiaries per facility (school and health facility), selected CC and
district; for each selected school - the number of beneficiaries per Standard.Based
on these, the transportation and materials required are estimated.Preparation and
Distribution of Materials–the District Level staff is responsible for putting
The Lesotho Child Grants Programme
CCT Operations Manual
35
together the required number of Compliance Quarterly Kits for the process and the
production and distribution of materials as the Compliance Monitoring Forms to
the Facility level.
(ii) Trainings – The field and facility staff receives training on their responsibilities in
the process.
(iii) Appointments –appointments are made with the respective facilities on when they
are visited by the Programme staff.
(iv) Community Mobilization –The objective of the community mobilization campaign
is to ensure that the community understands the monitoring process and how it is
linked to the CCT pilot, especially in terms of possible penalties. During this
stage, the nature of the CCT pilot, its objectives and upcoming plans are reviewed
with the community.
(v) Communications Campaign -spreading information and reinforcing the training
that beneficiaries received during enrolment, it is important that the Central Level
procures materials applicable to each treatment group, and ensure that these reach
the correct locations. At the District Level, the programme officers with the help
of health and education district authorities distribute materials to partner facilities’
staff.
2. Compliance Monitoring Operations
Implementation covers the process of recording attendance information.
For education facilities, the assigned staff completes the School Attendance Monitoring Form
for beneficiary children on a monthlybasis, andthe form is later delivered to / collected by the
assigned programme District Level staff.
For health facilities, the assigned programme District Level staffcompletes the facilities
records and provides access to them to the Programme staff so that they can complete the
Health Attendance Monitoring Form for beneficiary children at the health facility.

The Lesotho Child Grants Programme
CCT Operations Manual
36
3. MIS Data Entry and Closure
Once data collection has been completed in the field and all completed forms are with the
relevant District Level staff at the MOSD District offices, the classification of forms and their
organization for storage is carried out in parallel with data entry activities.
Attendance data collected by the health and education service providersis entered into the
MIS by the relevant District Level staff, and it is monitored and supervisedby the Data Entry
Coordinator assigned from Central Level.Once the data entry process is closed for a
monitoring quarter, no information can be entered or altered for that monitoring cycle.
4. Generation of Results
The MIS generates the following lists every quarter, and these lists should be easily sorted by
or generated for various geographical breakdowns (district, constituency, CC, electoral
division, village):
List of beneficiaries in the education component of the CCT;
List of beneficiaries in the health component of the CCT;
List of beneficiaries who have complied with the required conditionalities/co-
responsibilities;
List of beneficiaries who have not complied (partially or fully) with the required
conditionalities/co-responsibilities;
List of active beneficiaries; and
List of exempt beneficiaries.
5. Generation of Indicators
A list of indicators is generated as a result of the process of compliance monitoring; to be
used by the higher management levels of the CGP as a tool to evaluate, supervise, monitor
the process, make decisions and estimate the results of the process.
D. PAYMENTS
At the end of each monitoring cycle, payments are made to the beneficiary HHby contracted
payment agencies. The process is summarised in three broad activities in the figure below:

The Lesotho Child Grants Programme
CCT Operations Manual
37

The Lesotho Child Grants Programme
CCT Operations Manual
38
Figure 6: Flow Chart of the Payments Process
1. Preparatory Activities
During this phase of implementation the MOSD has to ensure that:
(i) Payment Agencies are trained;
(ii) Payment Lists and offline file for paymentsoftware are generated and delivered to
payment agencies;
(iii) Letter for Release of Funds is prepared;
(iv) Payment Barcode Stickers are obtained and printed;
(v) Beneficiaries are informed about the process via ASWOs and VACs/Village
Chiefs; and
(vi) Payment Books are prepared and distributed.
PAYMENT
PROCESS
PREPARATORY
ACTIVITIES
PAYMENT TO
BENEFICIARIES
ACTIVITIES
AFTER THE
PAYMENT
Training to Payment Agencies
Generation of payment lists
Generation of Payment amountbarcodes stickers
Development of offline file for software
Dissemination of information to beneficiaries
Check if payee documents are complete
Check ID of payee/ representative (scan or
manually)
Affix payment amount barcode stickers payment
list and payment book
Scan payment amount barcode sticker and verify
amount
Pay out the respective amounts
(Scan payment list in case not done during
payment)
Deliver payment software file and reconciliation
file to DSW
Upload payment software file into MIS
Beneficiaries sign payment list for receipt of
money
Generate reconciliation report
Agree and sign reconciliation report

The Lesotho Child Grants Programme
CCT Operations Manual
39
2. Payment to Beneficiaries
With the groundwork laid during the preparatory activities, the MOSD works closely with the
Payment Agencies to ensure programme beneficiaries receive their quarterly payment in a
regular manner (March, June, September, and December). The following activities take place
during the payment event:
(i) Beneficiaries visit their designated payment points and present ID and Payment
Book;
(ii) The assigned Payment Officer verifies identification and cross checks beneficiary
details in the payment book with offline software;
(iii) In the case of positive identification, the payment amount is verified based on
information in the payment software and a payment receipt is filled out by the
payment agency representative;
(iv) The corresponding payment barcode sticker is affixed to the payment book and a
duplicate barcode sticker is placed on the payment list;
(v) The barcode sticker in the payment book is stamped and payment date entered in
both payment book and payment list;
(vi) The payment software is updated with the amount being paid out on that specific
date and
(vii) The payment agency representative gives the payment amount to the beneficiary,
who signs on the payment list to confirm receipt of funds.
Aside from collecting payments, beneficiaries can also present a case for Case Management
at the payment event by completing the appropriate form with a programme officer.
3. Reconciliation
These activities take place after the payment event has closed. The following actions are
carried out:
(i) Scanning of payment lists with ID barcodes and payment amount barcode stickers,
if this was not done during the process of making payments to beneficiaries;
(ii) Delivery of payment software files and payment lists to MOSD by Payment
Agency;
(iii) Uploading of the software files to the MIS and Generation of Reconciliation
Report; and

The Lesotho Child Grants Programme
CCT Operations Manual
40
(iv) Signing of Reconciliation Report by MOSD and Payment Agency.
E. CASE MANAGEMENT
The basic Case Management (CM) system is a series of protocols which respond to specific
beneficiary requests and programme alerts. Its purpose is to provide solutions to:(i) demand-
side cases where beneficiaries require to file updates, complaints, claims, eligibility appels,
replacement of documents, or denouncements;; and (ii) supply-side cases arising from
restrictions, alerts and warnings produced automatically by the MIS.
The Case Management is handled across the Enrolment, Compliance Monitoring and
Payments processes. The process consists of the following stages:
Planning and preparatory activities;
Operations: fieldwork, data entry and processing of information, case management;
Generate indicators.
An illustration of the process is presented below.
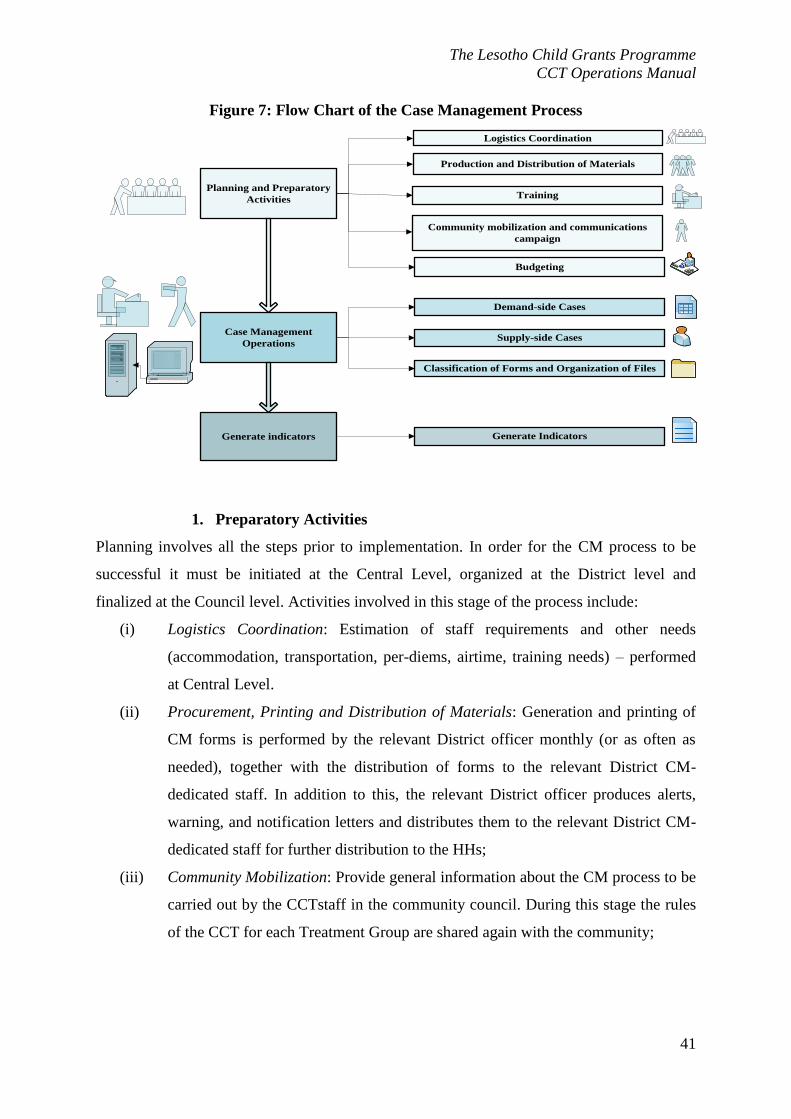
The Lesotho Child Grants Programme
CCT Operations Manual
41
Figure 7: Flow Chart of the Case Management Process
Planning and Preparatory
Activities
Case Management
Operations
Logistics Coordination
Production and Distribution of Materials
Demand-side Cases
Supply-side Cases
Training
Community mobilization and communications
campaign
Generate indicators Generate Indicators
Classification of Forms and Organization of Files
Budgeting
1. Preparatory Activities
Planning involves all the steps prior to implementation. In order for the CM process to be
successful it must be initiated at the Central Level, organized at the District level and
finalized at the Council level. Activities involved in this stage of the process include:
(i) Logistics Coordination: Estimation of staff requirements and other needs
(accommodation, transportation, per-diems, airtime, training needs) – performed
at Central Level.
(ii) Procurement, Printing and Distribution of Materials: Generation and printing of
CM forms is performed by the relevant District officer monthly (or as often as
needed), together with the distribution of forms to the relevant District CM-
dedicated staff. In addition to this, the relevant District officer produces alerts,
warning, and notification letters and distributes them to the relevant District CM-
dedicated staff for further distribution to the HHs;
(iii) Community Mobilization: Provide general information about the CM process to be
carried out by the CCTstaff in the community council. During this stage the rules
of the CCT for each Treatment Group are shared again with the community;

The Lesotho Child Grants Programme
CCT Operations Manual
42
(iv) Communication Campaign: Selection of the best method(s) of dissemination (e.g.
brochures, posters, flyers) for information on the main characteristics of the CCT
pilot and the CM procedures available for the HHs to take advantage of;
(v) Training: Organization of various sessions based on audiences: (a) for CM-
dedicated staff and all levels; (b) for VACs and Village Chiefs; and (c) for
relevant data entry officers;
(vi) Budgeting: All human resources, materials, transportation, accommodation,
airtime and training needs estimated at the logistics stage are now analysed and
budgeted in order to facilitate financial control of the actions carried out during
the CM process. Forecasting of cost implications of the CM process is also
performed.
2. Case Management Operations
This phase of the CM process captures the reporting or detection of demand and supply side
cases respectively.
Sixtypes of demand side cases are handled by the programme:
(i) Updates – HH reports the update and relevant programme staff updates the MIS.
Changes are verified at the central level,and beneficiary notificationsare generated
and sent, containing information on the implications of the update.
(ii) Payment Claims – HH reports this case to the relevant programmerepresentative, a
Payments Claim Form is completed, and relevant programme staff updates the
MIS. All these forms are later reviewed by the CCT Project Officer and cross-
checked with Health Care Attendance and Monitoring of School Attendance
Forms as necessary. Following resolution of the case, the beneficiary is presented
with a notification letter.
(iii) Quality Complaints –HH reports the case and is required to complete the relevant
complaints form. The CCT Project Officer enters the data into the MIS and the
case is then handled by the Case Management Coordinator. Following resolution,
the beneficiary is notified by way of letter.
(iv) Eligibility Appeals- HH is instructed to complete the respective CM form, and the
CCT Project Officer enters this data into the MIS.The Case Management
Coordinator reviews the validity of the case and a resolution is derived. A
notification letter is generated through the MIS to inform households of outcome
of the appeal.

The Lesotho Child Grants Programme
CCT Operations Manual
43
(v) Denouncements – Beneficiaries or non-beneficiaries file this case which is then
entered into the MIS. The case is reviewed by the Case Management
Coordinatorand the outcome is communicated to the HH by way of letter.
(vi) Requests for Replacement ID/Payment Books – The HH completes the respective
CM form and case is reviewed byCase Management Coordinator and then
forwarded to the Payments Coordinator. The Payment Coordinator generates ID
and Payment Book as necessary and dispatches them for delivery to beneficiaries.
For supply side cases, two types of cases are handled by the programme:
(i) Exits: – The following lists are generated at various points in time: (a) list of HHs
missing 3 consecutive payments (generated at the end of every payment cycle);
(b) list of HHs which no longer have children in the household (before each
payment cycle); (d) list of HHs who moved to locations not covered by the pilot.
All these lists are reviewed by the Case Management Coordinator for resolution,
and the beneficiaries are informed via notificationletters.
(ii) Restrictions: A list of households which are restricted due to consecutive non-
compliance and dueto failing to present child birth certificates in the required time
(before each payment cycle); is generated.
(iii) Alerts–The Case Management Coordinator generates alerts (reminders to attend
payment events and/or to submit birth certificates). The Case Management
Coordinator generates the reminder letters and the HH notification letters, and
sends them for distribution to the HHs.
Additionally, a quarterly Case Management report containing alerts linked to non-compliance
of co-responsibilities is also generated from the CM Module. Necessary steps are taken to
remedy situation based on the Treatment Group a HH belongs to.
3. Case Management Resolution
Once the case is presented, data is entered, and the data entry quality is checked, the actual
resolution of the case starts. Below is a description of how each case is resolved.
a) Demand-Side Cases
The general steps are the following:
Once the Data Supervision status is “Complete”, MIS sends a notification to the
District Coordinator for handling (containing number of new cases to be taken care of,
The Lesotho Child Grants Programme
CCT Operations Manual
44
by case type). The MIS allows District Coordinator to forward these notifications to
various other actors in charge of dealing with various CM cases (e.g. he/she should be
able to send a notification to the Payments Coordinator that x Payment Claims and y
Requests for Payment Books are awaiting his response);
The relevant MOSD staff handles the case;
If there is a change in eligibility, then written approval from the Case Management
Coordinator and CCT Coordinator is needed for the resolution to be entered and for
the case to be assigned a closed status. If the Case Management Coordinator and/or
the CCT Coordinator do not agree with the resolution, the case is sent back for re-
consideration, while its status in the MIS remains Pending.
The resolution of the case is communicated with the HH via letter.
b) Supply-Side Cases:
i. Restrictions and Exits
At the appropriate time, the Case Management Coordinator receives notification about HHs
which should be restricted or removed from the programme. After one more review, he/she
accepts the cases and then the MIS automatically changes the HH status from “Beneficiary”
to “Restricted” or “Exited.”
ii. Alerts
The most critical alerts are:
Warning Letters for HHs;
Cases Pending to be monitored and closed by CCT Coordinator; and
Significant Quality Complaints.
Alerts are generated for two levels:
a) Internal Alerts9: To notify the relevant MOSD staff (e.g. the CCT Coordinator) of the need
to monitor, take action and/or close cases; and
b) External Alerts: To notify HHs to take remedial actions to avoid being restricted from the
programme.
9 To be developed by local IT Firm

The Lesotho Child Grants Programme
CCT Operations Manual
45
c) Delivery of Notification
As soon as the resolution is entered into the MIS and the case is closed, the MIS should
automatically generate internally a Notification /Warning Letter as appropriate. The
appropriate user (CM and/or District Coordinator) reviews the letter, makes changes if
necessary, and approves it for printing. At this stage, the letter is ready to be printed at any
time.
In order to order to maximize efficiency, every effort should be made to ensure the delivery
of Notification and Warning Letters to the beneficiary during one of the various events. For
the HHs which do not get their Notification Letter during one of these events, the MOSD
should plan for case-by-case delivery no later than 15 days after the letters were generated.
Only in extreme cases should the MOSD use the VACs or Village Chiefs for delivery.
4. Generation of Indicators
For each type of case the MIS produces the number and percentages of accepted, rejected and
pending cases, as well as the average time to solve a case and the percentage of cases solved
within the recommended time.

The Lesotho Child Grants Programme
CCT Operations Manual
46
V. MONITORING AND EVALUATION
The monitoring and evaluation process involves gathering information about the programme
implementation and evaluating the performance of the programme relative to its intended
objectives.
Monitoring describes the records of activities, their results and associated problems during
programme implementation. Evaluation provides explanations of the factors accounting for
the performance of the programme. As presented in the figure below, Monitoring and
Evaluationcan take place throughout the implementation of the CCT.
Figure 8: Monitoring & Evaluation throughout the Programme Cycle
1. Programme Planning
During the programme planning phase, an ex-ante evaluation may be carried out. This
evaluation could provide data on programme feasibility by examining supporting policies,
institutions and financial resources required for the implementation of the programme.
Likewise, a baseline study could also be carried out during this phase of the programme.
Gathering baseline information provides the data needed to conduct an impact evaluation at
the end of the programme.
2. Programme Implementation
During the programme implementation stage, the various programme processes can be
assessed through process evaluations, spot checks and rapid assessments. The process
•Ex-Ante Evaluation
•Baseline Study (part of an Impact Evaluation)Programme Planning
•Process Evaluation
•Rapid Assessment
•Monitoring
•Spot Checks
Programme Implementation
•Follow-up Survey (part of Impact Evaluation)
•Rapid AssessmentProgramme Completion
The Lesotho Child Grants Programme
CCT Operations Manual
47
evaluation can help to determine whether target populations are being reached and if services
are being provided as intended. Indicators for the processes within the pilot project cycle are
monitored throughout the project implementation. It is through this continuous monitoring
process that programme achievements can be assessed.
3. Programme Completion
At this stage, a follow-up survey can be conducted, to serve for finalizing the impact
evaluation. This can provide programme implementers with information on how the
implementation of the project affected programme beneficiaries and service provision in the
participating institutions. This impact has to be compared to the baseline data, which
demands the collection of baseline data before the implementation of the project.