t he l ung n odule rohit kumar, md assistant professor of medicine thomas jefferson university
TRANSCRIPT

THE LUNG NODULE
Rohit Kumar, MD Assistant Professor of Medicine
Thomas Jefferson University

OUTLINE
Definition Risks of malignancy Approach to diagnosis Current guidelines for follow up Cases
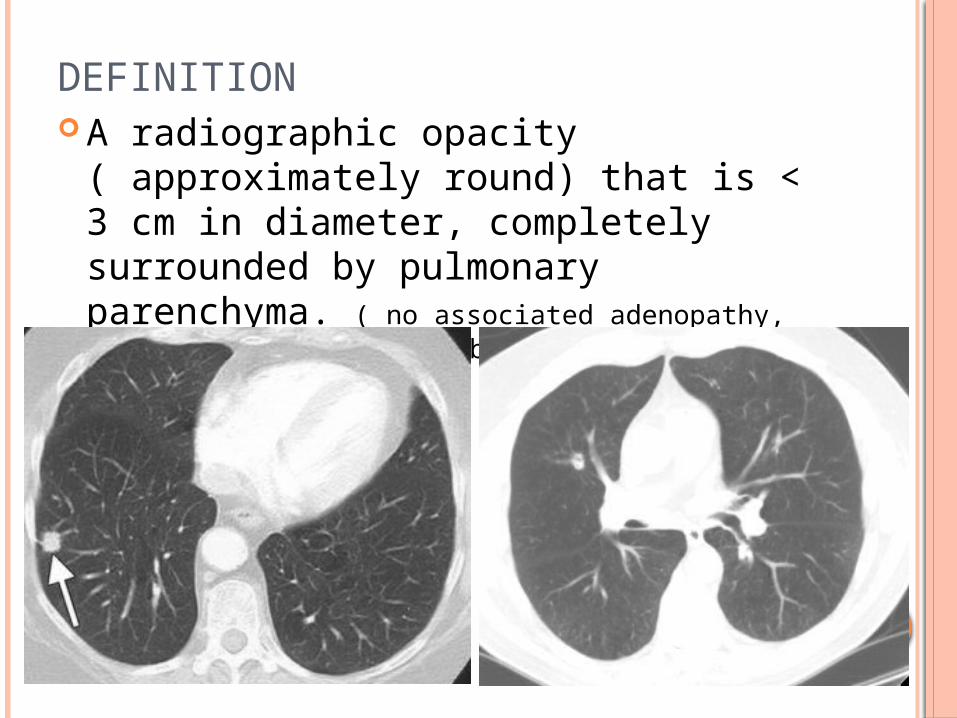
DEFINITION A radiographic opacity ( approximately
round) that is < 3 cm in diameter, completely surrounded by pulmonary parenchyma. ( no associated adenopathy, atelectesis or pleural abnormalities)
.

WHY SHOULD WE FIND NODULES?
Smoking continues to be a highly prevalent
Most lung cancer presents at a later stage
Survival for late stage lung cancer is still poor
Malignant nodules represent a potentially curable form of lung cancer
Recent trials indicate screening might be beneficial

CXR STUDIES
4 Randomized Clinical Trials in 1970s Mayo Clinic Study Czech Study
Sloan Kettering study Johns Hopkins study
CXR + Sputum cytology vs.
Usual Care
CXR + Sputum cytology vs.
CXR alone

PLCO
Smoker +Non-smokerAge 55-74
CXR
Randomize
150,000
No Screen
Year 0 1 2 3 ………… 20

NATIONAL LUNG SCREENING TRIAL
30 pack yearsAge 55-74
CT
Randomize
52,000
CXR
Year 0 1 2 3 4 5 6 7

NLST – STUDY POPULATION
Inclusion criteria
55 to 74 years At least 30 pack-year
smoking history If former smokers, had
quit within previous 15 years
Exclusion criteria
Previous lung cancer CT chest within 18
months before enrollment
Hemoptysis Unexplained weight
loss of more than 15 lbs in last year60%Males
90%Whites50%former
smokers75%less than 64
years old

NLST- RESULTS
20% reduction in lung cancer specific mortality
247 deaths/ 100,000 person-years
compared to 309 deaths/ 100,000
person-years
6.7% reduction in overall mortality
443
356
1060
941
Number Needed to Screen – 320

EPIDEMIOLOGY
1 in 500 CXR’s demonstrates a lung nodule
>150,000 nodules are identified each year Incidence of cancer in nodules ranges
between 10% to 70% ( 35%) Most nodules are benign- infection /
hamartoma ELCAP – 23% subjects had nodules, 2.7%
malignant Mayo Clinic – 1500 pts: 70% had nodules,
1.4% malignant

DDX “BENIGN” LESIONS
Vascular AV malformations Pulmonary artery
aneurysm Infectious
Tuberculosis MAI Aspergilloma Histoplasmosis Echinococcus Blastomycosis Cryptococcus Coccidiomycosis Ascariasis Difofilaria
Inflammatory Rheumatoid nodule Sarcoidosis
Wegener’s granuloma Congenital
Bronchogenic cyst Other
Rounded atelectasis Pulmonary Amyloidosis
Tumors Hamartoma Lipoma Fibroma

DDX MALIGNANT NODULES
Primary Lung CancerNon-small cell
Squamous cell Adenocarcinoma Large cell Bronchoalveolar
carcinomaSmall cell CarcinoidLymphoma
Metastatic CancersColonTesticularBreastMelanomaSarcomaRenal Cell
Carcinoma
DECISION TO PERFORM FOLLOW UP STUDIES SHOULD DEPEND ON ….
Nodule Size Nodule characteristics ( morphology) Growth rate ( doubling time) Patient risk profile

NODULE SIZE
> 3 cm – Mass ► should be biopsied/ removed
Size Likelihood of malignancy < 3 mm 0.2% 4-7 mm 0.9% 8-20 mm 18% > 20 mm 50%
Midthun et al. Lung cancer 2003

NODULE GROWTH RATE
A 30% increase in diameter represents doubling of volume ( assuming lesions are spherical)
Depends on nodule morphology: Solid nodules – 149 days Sub solid nodules – 457 days Pure Ground Glass – 813 days
Doubling time of malignant tumors is rerely less than a month or more than a year
Stability of a solid nodule over 2 years is considered a sign of benignity

NODULE MORPHOLOGY
Opacification of underlying parenchymaSolid Ground Glass
Borders Calcification Fat - benign
Cavitation Air bronchograms Location in the Upper Lobes
malignant

BORDERS
Spiculated Scalloped Smooth
Corona radiata sign
80-90% of spiculated nodules are malignant !

CALCIFICATION Malignant Benign
Eccentric/ Stippled
Popcorn
Central/ Laminated

THE SUB SOLID NODULE
Atypical Adenomatous Hyperplasia BAC Adenocarcinoma

PATIENT FACTORS
Age Smoking Various prediction models:
Family history of lung cancer Pneumonia Occupational exposure

Risks of Malignancy___________________________________

SPN-CHANCE OF MALIGNANCY
0
10
20
30
40
50
60
% M
alig
nanc
y
35 - 39 40-49 50-59 >60
Age
% Malignant
Cummings, ARRD 1986;134:453 & Toomes, Cancer 1983;51:534

Factors Affecting Malignant Probability of SPN
Spiculated Margins 5.54
Age > 70 years old 4.16
Size 2.1-3.0 cm 3.67
Doubling time < 465 days 3.40
Smoker 2.27
Age 50-69 years old 1.90
Size 1.1 to 2.0 cm 0.74
< 1 cm 0.52
Smooth Margins 0.30
Never Smoked 0.19
Doubling Time > 465 days 0.01Gurney JW. Radiology, 1993.
Likelihood Ratio

RISK FACTORS
Ost et al, NEJM: June 2003

Management___________________________________

KEY NOTES
Compare OLD films Compare OLD films Compare OLD films
Assess patient risk Assess operability

SPN MANAGEMENT STRATEGY Excision
High risk lesion, low risk pt Biopsy
Intermediate risk Observation
Low risk lesion, high risk pt Requires serial CT scans Bx if change
When in doubt, take it out.

MANAGEMENT OF NODULES < 8 MM

FLEISCHNER SOCIETY GUIDELINES

THIS DOES NOT APPLY TO…..
Patients with known or suspected malignant/ metastatic disease.
Patients < 35 yrs – unless other cancer. Patients with unknown fever.

MANAGEMENT OF NODULES > 8 MM

MANAGEMENT OF NODULES > 8 MM

FOLLOWING SUBSOLID NODULES
2 year rule does not apply Change in the solid component TBNA indicated for non surgical pts, multifocal
disease, and where proof of malignancy needed before surgery.

FOLLOWING SUBSOLID NODULES
Pure GGO: < 5 mm : No follow up 5-10 mm : 3-6 month, then annually for 3-5 year > 10 mm : 3-6 month, then surgery
GGO with Solid component: > 10 mm: Consider PET scan, then Surgery

32 YEAR OLD, NON-SMOKER, WITH RECURRENT SINUS INFECTIONS
Differential Diagnosis? Work-up?
ANSWER
Differential DiagnosisWegener’s
GranulomatosisCavitary PneumoniaTBSquamous Cell
CarcinomaOther lung cancer
ApproachLab tests (ANCA)Sputum culture &
cytologyFOBTrial of antibiotics
PET less likely to help in diagnosis
PET good for disease outside the chest

65 YEAR-OLD SMOKER; 2 CM NODULE
Peripheral or central?
Approach?

ANSWERS
Peripheral lesion Best approach:
Assess for surgical candidacy PFTs PET scan +/- Head CT/MRI
If good candidate VATS If not good CT-guided biopsy

42 YEAR-OLD SMOKER FROM OHIO
Differential Diagnosis? What next?
PET SCAN – DOES IT HELP YOU?
SUV 2.0

ANSWER:
Blastomycosis

42 YEAR OLD SMOKER WITH WEIGHT LOSS
Differential Diagnosis? Next Step?

CT SCAN
What next?

ANSWER
PET scan Surgical Candidate? VATS vs. TTNA
Diagnosis: Lymphoma

CASES
66 yr male smoker with FEV1 0.7L

CASES
57 yr asthmatic female from Puerto Rico with cough


ELCAP PET sensitivity CT sensitivity Yield of bronchoscopy vs needle vs
navigation/ ebus